CANCER IN CHILDREN


Cancer in children is rare, but is still the leading cause of death from disease. Survival rates in children with cancer have dramatically improved in the past 30 years. Some of the factors leading to improved cure rates in children with cancer include the use of combination chemotherapy, clinical trials, and multimodal treatment for childhood solid tumors.
INCIDENCE AND TYPES OF CANCER
In 2004 the mortality rates of children with cancer were 2.4 per 100,000 in children ages 1 to 4 years and 2.5 per 100,000 in children ages 5 to 14 years. In comparison, cancer is the second leading cause of death from disease in adults (second to heart disease), with an overall mortality rate of 187.4 per 100,000 individuals.1
The types of malignancies in children are vastly different from those that affect adults. The most common types of cancer among adults include prostate, breast, lung, and colon. Children tend to develop leukemias, brain tumors, and sarcomas. Although many adult cancers have associated lifestyle factors that could theoretically be avoided, such as smoking and exposure to sun, very few environmental factors have been linked to pediatric malignancies. Yet more data are emerging that the developing child may be affected by parental exposures prior to conception, exposures in utero, and the contents of breast milk (see What’s New? Increased Emphasis on Child Health and Environmental Contaminants).2,3
Most recently, cancer incidence and treatment in adolescents and young adults have become of interest and concern in pediatric oncology. The incidence of cancer among adolescents and young adults represents only 2% of all invasive cancers. However, the malignancy rate in this age group (15- to 29-year-olds) is three times higher than that in children younger than 15 years. The most common cancers among the 15- to 19-year-old population in the United States are Hodgkin lymphoma, germ cell tumors, central nervous system (CNS) tumors, non-Hodgkin lymphoma, thyroid cancer, malignant melanoma, and acute lymphocytic leukemia (ALL). This pattern is different than in younger as well as older populations. Many of the common malignancies in children younger than 5 years of age are virtually absent in the 15- to 19-year-old group.4 Similarly, cancers that predominate in adults are unusual among adolescents.
Most childhood cancers originate from the mesodermal germ layer that gives rise to connective tissue, bone cartilage, muscle, blood, blood vessels, gonads, kidney, and the lymphatic system. Thus the more common childhood cancers are leukemias, sarcomas, and embryonic tumors. Embryonic tumors originate during intrauterine life. These tumors contain abnormal cells that appear to be immature embryonic tissue, unable to mature or differentiate into fully developed functional cells. Embryonic tumors are diagnosed early in life (usually before 5 years of age). Embryonic tumors often contain the term blast cell in their name, which refers to the immature nature of the cells.
Leukemia is the most common malignancy in children and the most common type of leukemia is ALL, which represents three fourths of all pediatric leukemia cases. Although the presenting signs of the various types of leukemia may be similar, the treatment and response to treatment of childhood leukemias vary greatly.
CNS tumors are the most common types of solid tumors in children. Not all brain tumors are malignant by histology, but even a benign tumor can have devastating effects on a child. The treatment for brain tumors in children often presents difficulties because therapies, such as radiation, may have debilitating effects on the developing brain.
Lymphoma, including non-Hodgkin lymphoma and Hodgkin lymphoma, is a malignancy common in children and adults. However, the subtypes of lymphoma and treatments in the two populations often differ.
Many pediatric solid tumors usually develop only in the pediatric population but, in rare instances, may occur in adults. These tumors include neuroblastoma, Wilms tumor, rhabdomyosarcoma, retinoblastoma, osteosarcoma, and Ewing sarcoma.
Childhood cancers are most often diagnosed during peak times of physical growth. In general, they are extremely fast growing, with 80% having distant spread (metastases) at diagnosis. Overall, cancer is 10% to 25% more common in white than in black children. Boys are more likely to develop cancer than girls.
ETIOLOGY
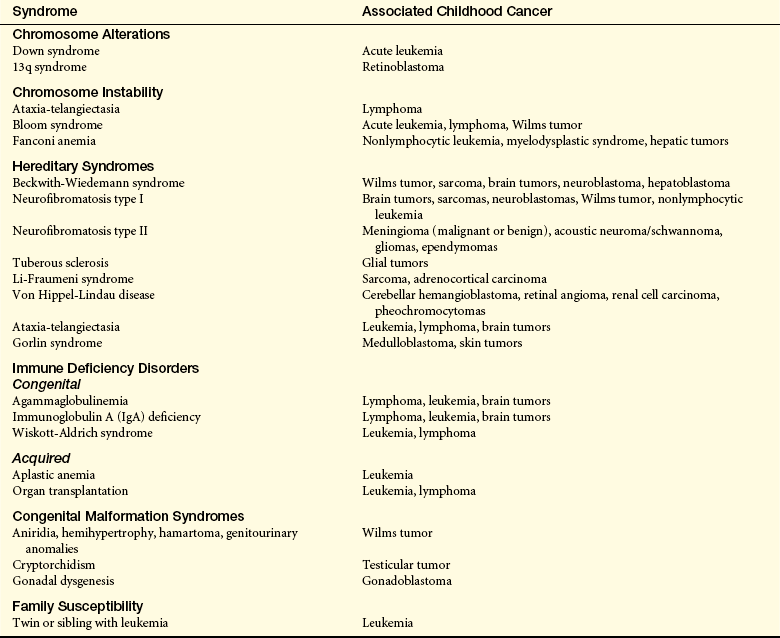
The causes of cancer in children are largely unknown. A few environmental factors are known to predispose a child to cancer, but causal factors have not been established for most childhood cancers. A number of host factors, many of which are genetic risk factors or congenital conditions, have been implicated in the development of childhood cancer (Table 13-1). Because the cell types often identified in tumors in children closely resemble undifferentiated cells noted during normal development, it is hypothesized that these genetic changes alter such cells’ ability to fully differentiate.5 It is probably the interaction of many factors that produces cancer, a concept referred to as multiple causation or multifactorial etiology. In this view, cancer develops because of the predisposing characteristics of the person who is interacting with the environment.
The multiple causation concept is useful when the results of epidemiologic studies are interpreted. For example, laboratory and epidemiologic studies may indicate that exposure to a certain chemical can cause leukemia, but not all children exposed to that chemical will develop leukemia. Additional studies will be needed to determine what other factors must interact with chemical exposure to cause the disease.
Genetic Factors
Oncogenes and tumor-suppressor genes have been associated with childhood malignancies (Table 13-2; also see Chapter 11). Proto-oncogenes have a role in normal cell division and growth through a signaling process that orchestrates the cell cycle. If they are mutated, proto-oncogenes become carcinogenic oncogenes. Changes produced by specific oncogenes cause the cell cycle to go out of control. An example of an oncogene in pediatric cancer is N-myc, which is involved in neuroblastoma and glioblastoma. Tumor-suppressor genes arise from genes that normally suppress cancer cell proliferation but have lost their suppressor function, thus leading to uncontrolled growth. Some childhood cancers identified with tumor-suppressor genes include osteosarcoma, leukemia, rhabdomyosarcoma, retinoblastoma, and Wilms tumor.6
Table 13-2
Selected Oncogenes and Tumor-Suppressor Genes Associated with Childhood Cancer
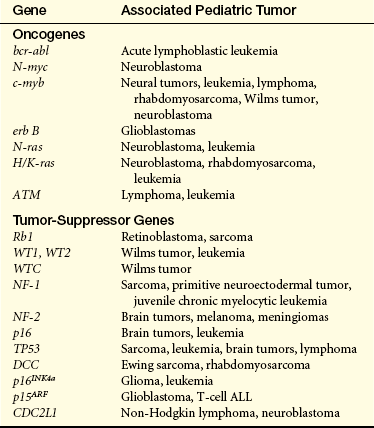
ALL, Acute lymphocytic leukemia.
Data from Dome JS, Coppes MS: Curr Opin Pediat 14(1):5-11, 2002; Linblom A, Nordenskjold M: Sem Cancer Biol 10(4):251-254, 2000; Tischkowitz M, Rosser E: Eur J Cancer 40:2459-2470, 2004; Look A, Kirsch IR: Molecular basis of childhood cancer. In Pizzo PA, Poplack DG, editors: Principles and practices of pediatric oncology, ed 4, Philadelphia, 2002, Lippincott Williams & Wilkins.
Other genetic factors involve chromosome aberrations or single-gene defects. These chromosome abnormalities include aneuploidy, amplifications, deletions, translocations, and fragility. A well-known chromosomal abnormality is the Philadelphia chromosome found in chronic and acute myelogenous leukemias.7 Chromosomal deletions are often observed in retinoblastoma and osteosarcoma.
Some congenital malformations herald the onset of pediatric malignancies. For example, certain syndromes involve easily diagnosed abnormalities and the child can then be followed closely and screened for tumor development.
Trisomy 21 (Down syndrome) is the most common genetic defect linked to the development of acute leukemia. Children with Down syndrome have a 10- to 20-fold increased risk of developing acute lymphoblastic and myelogenous leukemia and a higher risk for developing acute megakaryocytic leukemia. The risk is highest between 1 and 4 years of age.8 Wilms timor is associated with several congenial syndromes; aniridia, or congenital absence of the iris of the eye; ambiguous genitalia and mental retardation (AGR), neurofibromatosis, and Beckwith-Wiedemann syndrome.9 Retinoblastoma, a malignant embryonic tumor of the eye, occurs as an inherited defect or as an acquired mutation (see Chapter 19).
Several single-gene defects have been associated with the subsequent development of childhood cancers. Fanconi anemia and Bloom syndrome, two autosomal recessive conditions, are risk factors for the development of ALL.
Although not determined to be genetically transmitted, a child who has a sibling with leukemia has a risk for the development of leukemia that is two to four times greater than for children with healthy siblings. The occurrence of leukemia in monozygous twins is estimated as being as high as 25%.
In families with Li-Fraumeni syndrome (LFS) (an autosomal dominant disorder involving the TP53 tumor-suppressor gene), the risk of developing cancer as a child or adult is significantly higher than the unaffected population. Children and adults in Li-Fraumeni families are at risk for soft-tissue sarcoma, breast cancer, leukemia, osteosarcoma, melanoma, and cancer of the colon, pancreas, adrenal cortex, and brain. Individuals with LFS are at increased risk for developing multiple primary cancers.10
Environmental Factors
Although many adult cancers are associated with environmental agents, few childhood tumors share a similar strong association. Because of the lengthy latency period required between exposure and development of cancer; presumably early exposure to carcinogens does not result in cancer until the child is an adult.
Prenatal Exposure
Prenatal exposure to some drugs and to ionizing radiation has been linked to childhood cancers. The most well-described drug is diethylstilbestrol (DES), which was prescribed by physicians to prevent spontaneous miscarriage (in women with previous miscarriage). In 1971, DES was identified as a transplacental chemical carcinogen because a small percentage of the daughters of the women who took DES developed adenocarcinomas of the vagina. Since then, other studies have attempted to identify other drugs taken by pregnant women that may cause cancer in their offspring, but no other drugs have been found. Prior research suggested an association between antenatal x-ray exposure and childhood cancer but have not been replicated or supported in recent literature.
Childhood Exposure
Childhood exposure to ionizing radiation, drugs, or viruses has been associated with the risk of developing cancer. Retrospective research has shown a significant correlation between radiation-induced malignancies from radiotherapy (cancer treatment) or from radiation exposure from diagnostic imaging.11 In addition to the drug and environmental agents that are known to cause cancer in adults and therefore also are risks for exposure during childhood, a few drugs may particularly increase cancer risk during childhood (Table 13-3).

The relationship between childhood cancer and electromagnetic fields, small appliances, radon, and so on, has been the focus of many epidemiologic studies, yet no conclusive evidence has been observed.11
The strongest association between viruses and the development of cancer in children has been the Epstein-Barr virus (EBV), Burkitt lymphoma, nasopharyngeal carcinoma, and Hodgkin disease. Children with acquired immunodeficiency syndrome (AIDS) have an increased risk of developing non-Hodgkin lymphoma and Kaposi sarcoma. However, with the use of highly active antiretroviral therapy in the developed world, the incidence of AIDS-related malignancies has declined dramatically.12
PROGNOSIS
More than 70% of children diagnosed with cancer are cured. Survival rates for children younger than 15 years of age have increased at a rate of 1.5% per year. Similar improvements have been noted in the survival rates of adults older than 50 years of age. However, adolescents and young adults between 15 and 24 years of age have experienced increases in survival of less than 0.5% per year.4 A partial explanation for the relative lack of progress in curing the adolescent population at the same rate as that realized in the younger pediatric population is the lack of participation in clinical trials. Between 1997 and 2003, the rate of 15- to 19-year-olds with cancer participating in clinical trials was estimated at 10% to 15%. This rate is roughly one fourth the clinical trial participation rate of children younger than 15 years of age.4 The National Cancer Institute (NCI) and pediatric and adult cooperative groups sponsored by the NCI have launched a national initiative to increase the numbers of adolescents and young adults in clinical trials.
Blast cell 437
Embryonic tumors 437
Mesodermal germ layer 437
Multifactorial etiology 437
Multiple causation 437
Proto-oncogenes 438
Some of the factors leading to improved cure rates in pediatric oncology include the use of combination chemotherapy, multimodal treatment for childhood solid tumors, improvements in nursing and supportive care, development of research centers for comprehensive childhood cancer treatment, cooperation among treatment institutions and the development of cooperative study groups, recognition of the psychologic effects of cancer treatment, and continued follow-up to track trends in the late effects of cancer treatment. Young children are particularly prone to long-term sequelae of cancer therapy. It is imperative that more effective, targeted therapies with fewer side effects be found.
REFERENCES
1. Miniño AM, Heron MP, Smith BL: Deaths: preliminary data for 2004. National vital statistics reports. Available at www.cdc.gov/nchs/data/nvsr/nvsr54/nvsr54_19.pdf Retrieved July 14, 2008.
2. Clapp, R.W., Howe, G.K., Jacobs, M.M. Environmental and occupational causes of cancer: a call to act on what we know. Biomed Pharmacother. 2007;61(10):631–639.
3. Wigle, D.T., et al. Epidemiologic evidence of relationships between reproductive and child health outcomes and environmental chemical contaminants. J Toxicol Environ Health B Crit Rev. 2008;11(5-6):373–517.
4. Bleyer, A., Budd, T., Montello, M. Adolescents and young adults with cancer: the scope of the problem and criticality of clinical trials. Cancer. 2006;107(7 Suppl):1645–1655.
5. Look, A.T., Aplan, P.D. Molecular and genetic basis of childhood cancer. In Pizzo P.A., Poplack D.G., eds.: Principles and practice of pediatric oncology, ed 5, Philadelphia: Lippincott Williams & Wilkins, 2006.
6. Plon, S.E., Malkin, D. Childhood cancer and heredity. In Pizzo P.A., Poplack D.G., eds.: Principles and practice of pediatric oncology, ed 5, Philadelphia: Lippincott Williams & Wilkins, 2006.
7. Soupir, C.P., et al. Philadelphia chromosome-positive acute myeloid leukemia: a rare aggressive leukemia with clinicopathologic features distinct from chronic myeloid leukemia in myeloid blast crisis. Am J Clin Pathol. 2007;127(4):642–650.
8. Margolin, J.F., Steuber, C.P., Poplack, D.G. Acute lymphoblastic leukemia. In Pizzo P.A., Poplack D.G., eds.: Principles and practice of pediatric oncology, ed 5, Philadelphia: Lippincott Williams & Wilkins, 2006.
9. Dome, J.S., et al. Childhood cancer and heredity. In: Pizzo P.A., Poplack D.G., eds. Principles and practice of pediatric oncology. ed 5. Philadelphia: Lippincott Williams & Wilkins; 2006:905–932.
10. Tabori, U., Malkin, D. Risk stratification in cancer predisposition syndromes: lessons learned from novel molecular developments in Li-Fraumeni syndrome. Cancer Res. 2008;68(7):2053–2057.
11. Buka, I., Koranteng, S., Osomio Vargas, A.R. Trends in childhood cancer incidence: review of environmental linkages. Pediatr Clin North Am. 2007;54(1):177–203.
12. Powles, T., et al. Head and neck cancer in patients with human immunodeficiency virus-1 infection: incidence, outcome and association with Epstein-Barr virus. J Laryngol Otol. 2004;118(3):207–212.