Physiology of Exercise
 Oxygen consumption during exercise
Oxygen consumption during exerciseIntroduction
Physiology of exercise has generated significant interest and has gained importance because of:
• The current concern with physical conditioning and improvement in performance of athletes, sports persons, military and paramilitary personnels all over the world.
• Role of exercise in prevention of cardiovascular diseases and physical fitness among population groups.
• Role of exercise (stress tests) in evaluation of the cardiovascular and respiratory systems.
• Role of exercise in rehabilitation of the cardiac invalids.
Exercise: types and grading
Types of exercise
Exercise may be dynamic or isotonic and static or isometric.
Dynamic exercise involves isotonic muscle contractions. External work is involved in this type of exercise.
Grading of exercise
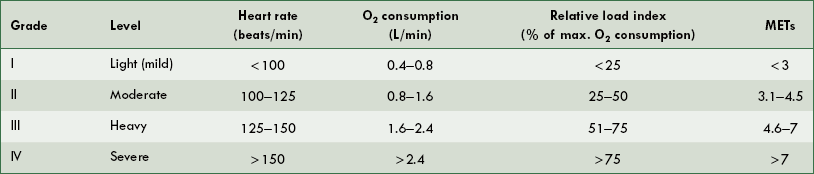
WHO (1978) has classified muscular exercise into four grades depending upon the heart rate and oxygen consumption. Oxygen consumption can be expressed as litres per minute or as relative load index (RLI), i.e. percentage of maximum O2 utilization. The oxygen utilization can also be expressed as metabolic energy expenditure (MET) test. One MET is equivalent to resting O2 uptake of 250 mL/min for an average adult man and 200 mL/min for an average adult woman. The four grades of exercise are shown in Table 5.8-1.
Responses to exercise
Exercise, basically, is a period of enhanced energy expenditure. The energy for muscular exercise is provided by the increased fuel consumption, which is reflected as greater O2 consumption and CO2 production. The increased O2 delivery to the tissues and removal of CO2 from the tissues is achieved by:
In addition, endocrine responses to exercise occur and play a regulatory role by regulating the water loss and availability of fuel during exercise.
Oxygen consumption during exercise
Oxygen consumption during exercise. The energy for muscular work during exercise is provided by the increased fuel consumption, which is reflected in greater O2 consumption and CO2 production.
Oxygen consumption (VO2) during rest is about 250 mL/min, which increases linearly with severity of exercise up to a certain limit, beyond which a plateau is reached (Fig. 5.8-1).
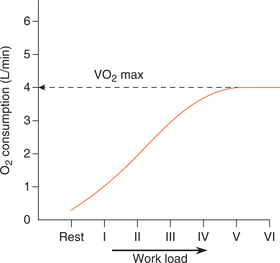
Maximal oxygen consumption (VO2 max) is the term used to define the level of oxygen consumption beyond which no further increase in O2 consumption occurs with further increase in the severity of exercise.
Oxygen deficit and O2 debt
The period of muscular exercise can be divided into three phases (Fig. 5.8-2).
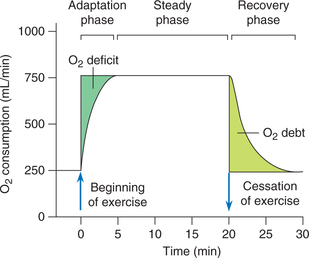
1. Adaptation phase refers to the beginning of muscular exercise (first 2–4 min) during which oxygen consumption increases linearly and reaches the maximal O2 consumption (VO2 max). The VO2 max at this stage is much less than the oxygen demand; thus an oxygen deficit is established. So, the energy requirement over and above the limits of O2 consumption is met with by the anaerobic pathway.
2. Steady phase of exercise is characterized by a maximum O2 consumption (VO2 max) throughout, i.e. a plateau phase of O2 consumption and work done relationship. During this phase also, as mentioned above, the excess energy requirement is met with by the anaerobic pathway, i.e. by breakdown of creatine phosphate and muscle glycogen. As a result of anaerobic release of energy in the muscles, the blood levels of lactic acid begin to rise steeply.
3. Recovery phase refers to the period after the cessation of exercise during which an extra amount of O2 is consumed. The amount of extra O2 consumed during recovery phase is called O2 debt and is proportionate to the extent to which oxygen deficit occurred during exercise. In other words, the O2 deficit which occurs during exercise is repaid during the recovery phase, in the form of O2 debt. The extra amount of O2 consumed during the recovery phase (O2 debt) is used:
Cardiovascular responses to exercise
To meet the increased energy demand of muscles during exercise the primary cardiovascular response is in the form of:
• Increase in the skeletal muscle blood flow,
• Redistribution of blood flow in the body,
Skeletal muscle blood flow
At rest the blood flow to the skeletal muscle is about 2–4 mL/100 g/min of muscle tissue. During strenuous exercise muscle blood flow can increase up to 20 times, i.e. about 50–80 mL/100 g/min muscle tissue. This is called exercise hyperaemia. This tremendous increase in the muscle blood flow during exercise is made possible by:
• Opening up of the closed capillaries which greatly increase the surface area and the rate of blood flow (page 196).
Redistribution of blood flow
As mentioned earlier the tremendous increase in the skeletal muscle blood flow is possible due to increased cardiac output (discussed later in detail) and redistribution of cardiac output in following manner (Table 5.8-2).
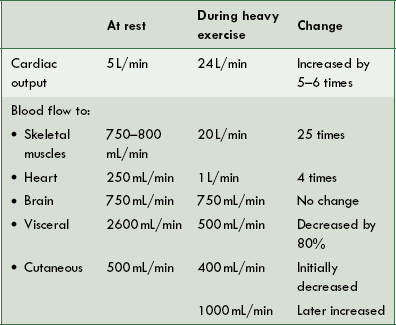
Coronary blood flow. During exercise coronary blood flow is increased by four to five times with 100% O2 utilization (page 191).
Visceral blood flow is temporarily curtailed in co-ordination with increase in muscle blood flow. It is brought about by the increased sympathoadrenal discharge.
Splanchnic blood flow is decreased by 80% in severe exercise.
Renal blood flow is also decreased by 50%–80% in severe exercise.
Cutaneous blood flow at rest is about 500 mL/min.
• Decrease in cutaneous blood flow occurs initially in the beginning of exercise due to reflex vasoconstriction.
• Increase in cutaneous blood flow is noted in sustained exercise when body temperature rises to dissipate the heat generated during exercise, as the blood flow through the skin is controlled predominantly by the requirements of temperature regulation.
Cerebral blood flow at rest is about 750 mL/min and remains unchanged during any grade of muscular exercise.
Adipose tissue blood flow is increased by four times during exercise. This helps to deliver fatty acids mobilized from triglyceride stores to the working muscles.
Increase in cardiac output
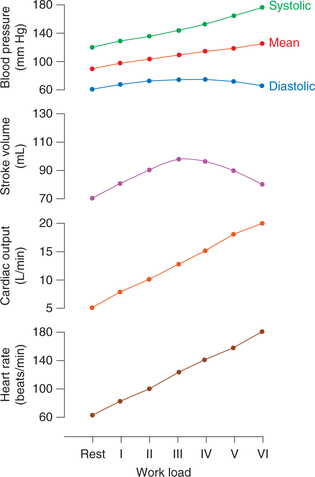
Normal cardiac output is about 5–6 L/min. During exercise, the cardiac output is increased depending upon the severity of exercise. In maximum exercise it may increase by five to six times. Since cardiac output is the product of heart rate and stroke volume, an increase in both contributes to the increase in a cardiac output during exercise (Fig. 5.8-3).
Increase in heart rate
Heart rate increases linearly with the severity of exercise. The increase in heart rate occurs as soon as the exercise begins or may be seen even before the exercise begins (anticipatory tachycardia).
Factors contributing to tachycardia during exercise are the following:
• Increased sympathetic discharge.
• Peripheral reflexes originating from the exercising muscles (muscle spindles, muscle-tendon receptors and organ of Corti) and joints.
• Local metabolic factors. Muscle tissue has free nerve endings which are stimulated by the lactic acid, potassium ions and other metabolites which collect in exercising muscles possibly contribute to the sustained increase in heart rate during prolonged exercise.
• Humoral factors, such as release of adrenaline and noradrenaline and possibly thyroid hormones during exercise.
• Intrinsic factors. Stimulation of sinoatrial node (SA) in the right atrium due to increased venous return increases the heart rate during exercise. This is known as Bainbridge reflex.
• Increased temperature in the myocardium due to increased activity of the heart during exercise may directly increase the rhythmicity of the pacemaker.
Increase in stroke volume
Under normal conditions the average stroke volume is about 80 mL/beat and may increase up to twice the normal value during exercise (Fig. 5.8-3).
Blood pressure changes during exercise (Fig. 5.8-4)
In systemic circulation
Systolic blood pressure is always raised by exercise since it depends upon the cardiac output which is increased in exercise. The blood pressure remains elevated during exercise and is not reflexly corrected by baroreceptor reflex. This has been explained by the fact that the neurons descending from the hypothalamic defence centre inhibit the baroreceptor afferents.
Diastolic blood pressure which primarily depends upon the peripheral resistance may mildly increase or decrease or remain unchanged depending upon the change in total peripheral resistance. Mostly, the vasodilatation in the skeletal muscles balances the vasoconstriction in other tissues, so diastolic blood pressure is usually not changed much.
Mean blood pressure is usually increased. It helps to increase the skeletal muscle blood flow by providing greater pressure head in the face of dilated resistance vessels.
Changes in blood volume during exercise
Blood volume during exercise is decreased by 15% resulting in haemoconcentration. Blood volume is decreased due to more plasma loss at the capillary level due to following reasons:
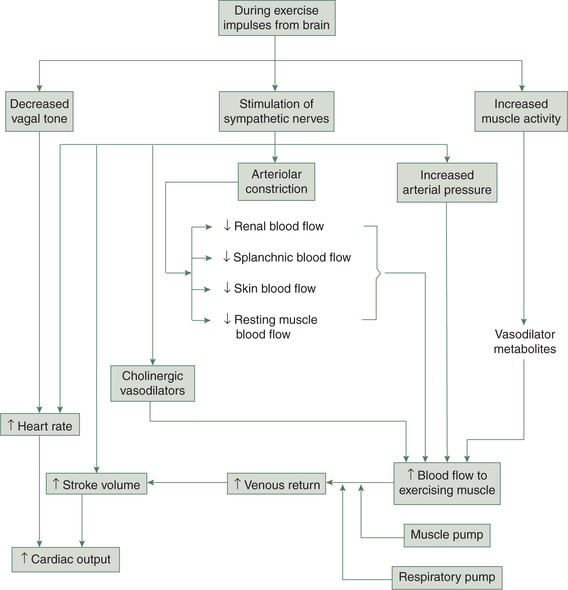
Summary of cardiovascular responses to exercise
The cardiovascular responses to exercise are summarized in Figure 5.8-4.
Respiratory responses to exercise
I. Increase in pulmonary ventilation
The pulmonary ventilation increases linearly with the increase in intensity of exercise (O2 consumption) until the anaerobic threshold is reached. The anaerobic threshold occurs at approximately 60% of the maximal exercise level, regardless of the level of physical fitness. Above the anaerobic threshold, the pulmonary ventilation increases out of proportion to the increase in O2 consumption because lactic acid that is generated imposes an additional respiratory drive.
Mechanism of increased pulmonary ventilation
There are several factors which can account for the marked increase in the pulmonary ventilation occurring in severe exercise. The probable factors are given below.
1. Neural control mechanisms Neural control mechanisms which have been suggested to make contribution to exercise hyperpnoea are:
• Cerebral cortex, the seat of conscious thought and voluntary activity may be responsible for the anticipatory hyperpnoea, which may occur due to psychic stimuli just before the beginning of exercise.
• Afferent impulses from proprioceptors in the muscles and joints are at least partly responsible for exercise hyperpnoea.
• Increase in body temperature during sustained exercise may also make some contribution to the exercise hyperpnoea through neural mechanism.
2. Chemical mechanism does not play the main role in exercise hyperpnoea, as the alveolar and arterial pO2 and pCO2 are well maintained during exercise however:
Changes at the tissue level
The changes at the tissue level which facilitate transfer of a large amount of O2 from the blood to the exercising muscles and that of CO2 from the tissues to the blood are:
Blood flow to the skeletal muscles is increased during strenuous exercise which brings more O2 to the tissue per minute. Capillary bed of the contracting muscles is dilated and many previously closed capillaries are open. Because of these changes the mean distance from the blood to the tissues cells is greatly decreased; this facilitates movement of O2 from the blood to the cells.
Gradient of pO2 between capillary blood and tissue fluid is increased. Due to the increased gradient of pO2 between capillaries and tissue fluid more O2 is removed from the capillary blood into the tissue fluid.
O2–Hb dissociation curve shifts to the right due to accumulation of CO2, rise in temperature and rise in red blood cell 2,3-DPG. This results in a threefold increase in O2 extraction from each unit of blood.
Endocrinal responses to exercise
Endocrines play an important role in adjustment to exercise. The hormones which are increased during exercise along with the role played by them are given.
1. Antidiuretic hormone (ADH) secretion is markedly increased during exercise. It helps to maintain fluid balance by reducing urine flow.
2. Adrenocorticotrophic hormone (ACTH) is released during the endurance events and probably helps by mobilizing fats for providing energy directly as well as by stimulating glucocorticoid secretion.
3. Endorphin secretion is significantly increased during exercise. They improve tolerance to discomfort associated with exercise by relieving pain. They also relieve mental stress and induce a feeling of well-being.
4. Cortisol secreted during exercise is helpful in reducing exercising stress. It also mobilizes protein and fats. Fatty acids are particularly useful as fuel during exercise. Consequently, carbohydrates are spared to be used by brain.
5. Aldosterone secreted during exercise reduces urinary loss of water and sodium like ADH. This helps to maintain fluid balance in the presence of excessive sweating during exercise.
6. Adrenaline and noradrenaline secretion is increased significantly in intense exercise. These hormones mobilize fatty acids and glucose, and thus improve the availability of fuel.
7. Insulin secretion is decreased during exercise. However due to training tissue sensitivity to insulin improves at rest. The improved sensitivity at rest accounts for the improvement in glucose tolerance test seen as a result of regular exercise. Because of this effect exercise is considered one of the most useful components of treatment of diabetes.
8. Glucagon. Prolonged exercise stimulates secretion of glucagon. It mobilises glucose from glycogen and fatty acids from the adipose tissue, and thereby improves fuel availability during prolonged exercise.
Effects of training
Training to the body tissues is provided by different sets of exercise regimes. Endurance training (aerobic) produces different effects in the skeletal muscles. Only aerobic exercises produce cardiovascular conditioning.
Usefulness of training to the body systems is highlighted:
• Training is most essential for the performance by athletes and sports persons, and forms the main aspect of sports physiology.
• Training by regular physical exercise is likely to slow the ageing process, which helps to prevent several degenerative and metabolic diseases, and thereby make life healthier and longer.
• Patients who exercise regularly ’feel better’. Such effects may also be attributed to the release of endorphins during exercise, which are reported to relieve mental stress and induce a sense of well-being.
• Regular exercise is one of the most useful components of treatment of diabetes because it reduces the insulin requirement by virtue of improvement in the glucose tolerance.
• There is some evidence that regular exercise decreases the incidence and severity of myocardial infarctions.
Effects of training on the body tissues can be described as:
• Effects of training on cardiovascular system,
• Effects of training on respiratory system,
Effects of training on cardiovascular system
Athletic training produces following effects on cardiovascular system.
1. Low resting heart rate. Consequently, trained athletes have low resting heart rate (50–60/min) due to increase in the vagal tone. This is useful during exercise because it increases the range through which the heart rate can increase.
2. Higher resting stroke volume. The aerobic athletic training leads to a cardiac hypertrophy and an increase in end-diastolic volume, which increases the resting stroke volume to about 105 mL as compared to about 75 mL in an untrained individual.
3. Much larger cardiac output during exercise. Because of the low resting heart rate and higher resting stroke volume, a trained athlete can achieve much larger cardiac output during exercise than an untrained individual.
Effects of training on respiratory system
1 Increase in maximal oxygen consumption
Maximal O2 consumption (VO2 max) increases by 5%–20% by conditioning (athletic training).
Effects of training on skeletal muscles
Increased muscle strength due to training results from:
• Increase in muscle mass, which is due to an increase in the size of muscle fibres (hypertrophy) and not due to increase in the number of muscle fibres (hyperplasia).
Changes in the muscle fibres, which enhance the capacity of the muscles to extract more O2 and improve the ability of the muscle fibres to provide energy during prolonged exercise are: