The gastrointestinal history
To study the phenomena of disease without books is to sail an uncharted sea, while to study books without patients is not to go to sea at all.
Gastroenterologists and gastrointestinal surgeons concern themselves with the entire length of the gut, the exocrine pancreas, the liver and the peripheral effects of alimentary disease.
Presenting symptoms (see List 13.1)
ABDOMINAL PAIN
There are many causes of abdominal pain, and careful history taking will often lead to the correct diagnosis. The following should be considered.
Frequency and duration
Try to determine whether the pain is acute or chronic, when it began and how often it occurs.
Site and radiation
The site of the pain is important. Ask the patient to point to the area affected by pain and to the point of maximum intensity. Parietal peritoneal inflammation that causes pain usually does so in a localised area. Ask about radiation of pain. Pain that radiates through to the back suggests pancreatic disease or a penetrating peptic ulcer. Pain due to diaphragmatic irritation may radiate to the shoulder and that due to oesophageal reflux or spasm may radiate to the throat.
Character and pattern
The pain may be colicky (coming and going in waves and related to peristaltic movements) or steady. Colicky pain comes from obstruction of the bowel or the ureters. Colicky pain arises because of complete or partial blockage of the bowel which triggers intestinal receptors. Classically, colicky pain occurs in small intestinal obstruction. If the pain is chronic, ask about the daily pattern of pain.
Aggravating and relieving factors
Pain due to peptic ulceration may or may not be related to meals. Eating may precipitate ischaemic pain in the gut. Antacids or vomiting may relieve peptic ulcer pain or that of gastro-oesophageal reflux. Defecation or passage of flatus may temporarily relieve the pain of colonic disease. Patients who obtain some relief by rolling around vigorously are more likely to have a colicky pain, while those who lie perfectly still are more likely to have peritonitis.
PATTERNS OF PAIN
Peptic ulcer disease
This is classically a dull or burning pain in the epigastrium that is relieved to a degree by food or antacids. It is typically episodic and may occur at night, waking the patient from sleep. This combination of symptoms is suggestive of the diagnosis. The pain is not always related to meals, despite classical teaching to the contrary. It is not possible to distinguish duodenal ulceration from gastric ulceration clinically. Many patients with epigastric pain related to meals have no evidence of peptic ulcer on investigation (referred to as non-ulcer or functional dyspepsia).
Pancreatic pain
This is a steady epigastric pain that may be partly relieved by sitting up and leaning forwards. There is often radiation of the pain to the back, and vomiting is common.
Biliary pain
Although usually called ‘biliary colic’, this pain is rarely colicky. Obstruction of the cystic duct often causes epigastric pain. It is usually a severe, constant pain that can last for hours. There may be a history of episodes of similar pain in the past; although pain episodes can occur after fatty meals, they are usually unpredictable. If cholecystitis develops, the pain typically shifts to the right upper quadrant and becomes more severe. Biliary colic is often associated with nausea and vomiting.
Renal colic
This is a colicky pain superimposed on a background of constant pain in the renal angle, often with radiation towards the groin. It can be very severe indeed.
Bowel obstruction
This is colicky pain. Periumbilical pain suggests a small bowel origin but colonic pain can occur anywhere in the abdomen. Small bowel obstruction tends to cause more frequent colicky pain (with a cycle every 2–3 minutes) than large bowel obstruction (every 10–15 minutes). Obstruction is often associated with vomiting, constipation and abdominal distension.
APPETITE AND WEIGHT CHANGE
Loss of appetite (anorexia) and weight loss are important gastrointestinal symptoms. The presence of both anorexia and weight loss should make one suspicious of an underlying malignancy, but they may also occur with depression and in other diseases. The combination of weight loss with an increased appetite suggests malabsorption of nutrients or a hypermetabolic state (e.g. thyrotoxicosis). It is important to document when the symptoms began and how much weight loss has occurred over this period. Liver disease can sometimes cause disturbance of taste. This may cause smokers with acute hepatitis and jaundice to give up smoking.
EARLY SATIATION AND POSTPRANDIAL FULLNESS
Inability to finish a normal meal (early satiation) may be a symptom of gastric diseases, including gastric cancer and peptic ulcer. A feeling of inappropriate fullness after eating can also be a symptom of functional dyspepsia.
NAUSEA AND VOMITING
Nausea is the sensation of wanting to vomit.a Heaving and retching may occur but there is no expulsion of gastric contents. Vomiting refers to the explosive ejection of stomach contents through the mouth; it is involuntary.
There are many possible causes for these complaints. Gastrointestinal tract infections (e.g. from food poisoning by Staphylococcus aureus) or small bowel obstruction can cause acute symptoms. In patients with chronic symptoms, pregnancy and drugs (e.g. digoxin, opiates, dopamine agonists, chemotherapy) should always be ruled out. In the gastrointestinal tract, peptic ulcer disease with gastric outlet obstruction, motor disorders (e.g. gastroparesis from diabetes mellitus, or after gastric surgery), acute hepatobiliary disease and alcoholism are important causes. Finally, psychogenic vomiting, eating disorders (e.g. bulimia) and, rarely, increased intracranial pressure should be considered in patients with chronic unexplained nausea and vomiting.
Asking about the timing of the vomiting (see Questions box 13.1) can be helpful; vomiting delayed more than 1 hour after the meal is typical of gastric outlet obstruction or gastroparesis, while early morning vomiting before eating is characteristic of pregnancy, alcoholism and raised intracranial pressure. Also ask about the contents of the vomitus (e.g. bile indicates an open connection between the duodenum and stomach, old food suggests gastric outlet obstruction, while blood suggests ulceration). Vomiting due to bowel obstruction may occur with little or no nausea.
Questions box 13.1
Questions to ask a patient presenting with recurrent vomiting
 denotes symptoms for the possible diagnosis of an urgent or dangerous problem
denotes symptoms for the possible diagnosis of an urgent or dangerous problem
1. Describe what happens during a typical episode (rule out rumination).
2. How long have you been having attacks of vomiting (distinguish acute from chronic)?
3. Does the vomiting occur with nausea preceding it, or does it occur without any warning?
4. Is the vomiting usually immediately after a meal or hours after a meal?
5. Do you have vomiting early in the morning or late in the evening?
6. What does the vomit look like? Is it bloodstained, bile-stained or feculent? (Gastro-intestinal bleeding or bowel obstruction)
7. Do you have specific vomiting episodes followed by feeling completely well for long periods before the vomiting episode occurs again? (Cyclical vomiting syndrome)
8. Is there any abdominal pain associated with the vomiting?
9. Have you been losing weight?
10. What medications are you taking?
11. Do you have worsening headaches? (Neurological symptoms suggest a central cause)
Vomiting is different from rumination. Rumination is effortless regurgitation of food into the mouth after eating; patients often call this vomiting when asked to describe what they mean. The food is spat out or re-swallowed; the taste is, apparently, not unpleasant.
HEARTBURN AND ACID REGURGITATION
Heartburn refers to the presence of a burning pain or discomfort in the retrosternal area. Typically, this sensation travels up towards the throat and occurs after meals or is aggravated by bending, stooping or lying supine (see Questions box 13.2). Antacids usually relieve the pain, at least transiently. This symptom is due to regurgitation of stomach contents into the oesophagus. Usually these contents are acidic, although occasionally alkaline reflux can induce similar problems. Associated with gastro-oesophageal reflux may be acid regurgitation, in which the patient experiences a sour or bitter-tasting fluid coming up into the mouth. This symptom strongly suggests that reflux is occurring. Some patients complain of a cough that troubles them when they lie down. In patients with gastro-oesophageal reflux disease, the lower oesophageal sphincter muscle relaxes inappropriately. Reflux symptoms may be aggravated by alcohol, chocolate, caffeine, a fatty meal, theophylline, calcium channel blockers and anticholinergic drugs, as these lower the oesophageal sphincter pressure.
Questions box 13.2
Questions to ask the patient with acid reflux or suspected gastro-oesophageal reflux disease (GORD)
denotes symptoms for the possible diagnosis of an urgent or dangerous problem
1. Do you have heartburn (a burning pain under the sternum radiating up towards the throat)? How often does this occur? (More than once a week suggests GORD)
2. Does your heartburn occur after meals or when you lean forwards or lie flat in bed (typical of acid reflux)?
3. Does the pain radiate across your chest down your left arm or into your jaw? (Suggests myocardial ischaemia)
4. Is the pain relieved by antacids or acid-blocking drugs? (Typical of acid reflux)
5. Do you experience suddenly feeling bitter-tasting fluid in your mouth? (Acid regurgitation; typical of acid reflux)
6. Have you experienced the sudden appearance of a salty tasting or tasteless fluid in your mouth? (Waterbrash, not GORD)
7. Have you had trouble swallowing? (Dysphagia; see Questions box 13.3)
Waterbrash refers to excessive secretion of saliva into the mouth and should not be confused with regurgitation; it may occur, uncommonly, in patients with peptic ulcer disease or oesophagitis.
DYSPHAGIA
Dysphagia is difficulty in swallowing. Such difficulty may occur with solids or liquids. The causes of dysphagia are listed in List 13.2. If a patient complains of difficulty swallowing, it is important to differentiate painful swallowing from actual difficulty.1 Painful swallowing is termed odynophagia and occurs with any severe inflammatory process involving the oesophagus. Causes include infectious oesophagitis (e.g. Candida, herpes simplex), peptic ulceration of the oesophagus, caustic damage to the oesophagus or, rarely, oesophageal perforation.
If the patient complains of difficulty initiating swallowing (see Questions box 13.3), fluid regurgitating into the nose or choking on trying to swallow, this suggests that the cause of the dysphagia is in the pharynx (pharyngeal dysphagia). Causes of pharyngeal dysphagia can include neurological disease (e.g. motor neurone disease, resulting in bulbar or pseudobulbar palsy).
Questions box 13.3
Questions to ask a patient who reports difficulty swallowing
denotes symptoms for the possible diagnosis of an urgent or dangerous problem
1. Do you have trouble swallowing solids or liquids, or both? (Solids and liquids suggests a motor problem, e.g. achalasia; solids only suggests a mechanical problem like cancer or a stricture)
2. Where does the hold-up occur (please point to the area)? (Pointing to the lower oesophagus suggests mechanical obstruction in the lower oesophagus)
3. Is the trouble swallowing intermittent or persistent? (Intermittent suggests eosinophilic oesophagitis [EoE], a lower oesophageal ring or a motor problem; EoE also causes acute food impaction)
4. Has the problem been getting progressively worse? (This suggests cancer or a stricture)
5. Do you cough or choke on starting to swallow? (This suggests oropharyngeal dysphagia)
6. Is it painful to swallow (odynophagia)? (This suggests acute inflammation of the oesophagus)
7. Do you have any heartburn or acid regurgitation? (Yes suggests GORD)
8. Have you been losing weight? (Worry about cancer)
9. Do you have asthma or hay fever? (This would be further supportive of EoE)
If the patient complains of food sticking in the oesophagus, it is important to consider a number of anatomical causes of oesophageal blockage.1 Ask the patient to point to the site where the solids stick. If there is a mechanical obstruction at the lower end of the oesophagus, most often the patient will localise the dysphagia to the lower retrosternal area. However, obstruction higher in the oesophagus may be felt anywhere in the retrosternal area. If heartburn is also present, for example, this suggests that gastro-oesophageal reflux with or without stricture formation may be the cause of the dysphagia.
The actual course of the dysphagia is also a very important part of the history to obtain. If the patient states that the dysphagia is intermittent or is present only with the first few swallows of food, this suggests either a lower oesophageal ring, eosinophilic oesophagitis or, rarely, diffuse oesophageal spasm. However, if the patient complains of progressive difficulty swallowing, this suggests a stricture, carcinoma or achalasia. If the patient states that both solids and liquids stick, then a motor disorder of the oesophagus is more likely, such as achalasia or diffuse oesophageal spasm.
DIARRHOEA
The symptom diarrhoea can be defined in a number of different ways. Patients may complain of frequent stools (more than three per day or a change from previous frequency is abnormal) or they may complain of a change in the consistency of the stools, which have become loose or watery. There are a large number of possible causes of diarrhoea.
Ask about the frequency and volume. Some patients pass small amounts of formed stool more than three times a day because of an increased desire to defecate. The stools are not loose and stool volume is not increased. This is not true diarrhoea. It can occur because of local rectal pathology, incomplete rectal emptying or a psychological disturbance that leads to an increased interest in defecation.
When a history of diarrhoea is obtained (see Questions box 13.4), it is also important to determine whether this has occurred acutely or it is a chronic problem. Acute diarrhoea is more likely to be infectious in nature, while chronic diarrhoea has a large number of causes.
Questions box 13.4
Questions to ask the patient presenting with diarrhoea
denotes symptoms for the possible diagnosis of an urgent or dangerous problem
1. How many stools per day do you pass now normally?
2. What do the stools look like (stool form e.g. loose and watery)?
3. Do you have to race to the bathroom to have a bowel movement? (Urgency in colonic disease)
4. Have you been woken from sleep during the night by diarrhoea? (Organic cause more likely)
5. Have you seen any bright-red blood in the stools, or mucus or pus? (Suggests colonic disease)
6. Are you passing large volumes of stool every day? (Suggests small bowel disease if non-bloody)
7. Are your stools pale, greasy, smelly and difficult to flush away (steatorrhoea)?
8. Have you seen oil droplets in the stool? (Chronic pancreatitis)
9. Have you had problems with leakage of stool (faecal incontinence)?
10. Have you lost weight? (e.g. cancer, malabsorption)
11. Have you had treatment with antibiotics recently? (Consider Clostridium difficile infection)
12. Have you had any recent travel? Where to? (Consider infections such as Giardia)
13. Have you a personal history of inflammatory bowel disease or prior gastrointestinal surgery?
14. Have you any history in the family of coeliac disease or inflammatory bowel disease?
15. Have you had any problems with arthritis? (e.g. inflammatory bowel disease, Whipple’s disease)
16. Have you had recent fever, rigors or chills (e.g. infection, lymphoma)?
17. Have you had frequent infections? (Immunoglobulin deficiency)
Clinically, diarrhoea can be divided into a number of different groups based on the likely disturbance of physiology.2
1. If the stools are watery and of high volume consider the following:
• Secretory diarrhoea when the diarrhoea is of high volume (commonly more than 1 litre per day) and persists when the patient fasts; there is no pus or blood, and the stools are not excessively fatty. Secretory diarrhoea occurs when net secretion in the colon or small bowel exceeds absorption; some of the causes include infections (e.g. E. coli, Staphylococcus aureus, Vibrio cholerae), hormonal conditions (e.g. vasoactive intestinal polypeptide-secreting tumour, Zollinger-Ellisonb syndrome, carcinoid syndrome) and villous adenoma.
• Osmotic diarrhoea when it disappears with fasting and there are large-volume stools related to the ingestion of food. Osmotic diarrhoea occurs due to excessive solute drag; causes include lactose intolerance (disaccharidase deficiency), magnesium antacids or gastric surgery.
• Abnormal intestinal motility if the patient has thyrotoxicosis or the irritable bowel syndrome.
2. If the stools contain blood consider the following:
• Exudative diarrhoea when there is inflammation in the colon. Typically the stools are of small volume but frequent, and there may be associated blood or mucus (e.g. inflammatory bowel disease, colon cancer).
3. If the stools are fatty consider the following:
• Malabsorption of nutrients and steatorrhoea. Here the stools are fatty, pale-coloured, extremely smelly, float in the toilet bowel and are difficult to flush away. Steatorrhoea is defined as the presence of more than 7 g of fat in a 24-hour stool collection. There are many causes of steatorrhoea (page 215).
CONSTIPATION
It is important to determine what patients mean if they say they are constipated.3 Constipation is a common symptom and can refer to the infrequent passage of stools (fewer than three times per week), hard stools or stools that are difficult to evacuate.
This symptom may occur acutely or may be a chronic problem (see Questions box 13.5). In many patients, chronic constipation arises because of habitual neglect of the impulse to defecate, leading to the accumulation of large, dry faecal masses. With constant rectal distension from faeces, the patient may grow less aware of rectal fullness, leading to chronic constipation.
Questions box 13.5
Questions to ask a patient presenting with constipation
denotes symptoms for the possible diagnosis of an urgent or dangerous problem
1. How often do you have a bowel movement?
2. Are your stools hard or difficult to pass?
3. What do the stools look like (stool form, e.g. small pellets)?
4. Do you strain excessively on passing stool?
5. Do you feel there may be a blockage at the anus area when you try to pass stool?
6. Do you ever press your finger in around the anus (or vagina) to help stool pass?
7. Has your bowel habit changed recently?
8. Any recent change in your medication?
10. Any abdominal pain? Is pain made better by a bowel movement?
12. Do you ever have diarrhoea?
13. Do you have a history of colon polyps or cancer? Any family history of colon cancer?
Ask about medications and the past history. Constipation may arise from ingestion of drugs (e.g. codeine, antidepressants, or aluminium or calcium antacids) and with various metabolic or endocrine diseases (e.g. hypothyroidism, hypercalcaemia, diabetes mellitus, phaeochromocytoma, porphyria, hypokalaemia) and neurological disorders (e.g. aganglionosis, Hirschsprung’sc disease, autonomic neuropathy, spinal cord injury, multiple sclerosis). Constipation can also arise after partial colonic obstruction from carcinoma; it is therefore very important to determine whether there has been a recent change in bowel habit, as this may indicate development of a malignancy. Patients with very severe constipation in the absence of structural disease may be found on a transit study to have slow colonic transit; such slow-transit constipation is most common in young women.
Constipation is common in the later stages of pregnancy.
Ask about excessive straining or a feeling of stool being blocked during attempted bowel movements. Difficulty with evacuation of faeces may occur with disorders of the pelvic floor muscles or nerves, or anorectal disease (e.g. fissure or stricture). Patients with this problem may complain of straining, a feeling of anal blockage or even the need to self-digitate to perform manual evacuation of faeces.
A chronic but erratic disturbance in defecation (typically alternating constipation and diarrhoea) associated with abdominal pain, in the absence of any structural or biochemical abnormality, is very common; such patients are classified as having the irritable bowel syndrome.4 Patients who report abdominal pain plus two or more of the following symptoms—abdominal pain relieved by defecation, looser or more frequent stools with the onset of abdominal pain, passage of mucus per rectum, a feeling of incomplete emptying of the rectum following defecation and visible abdominal distension—are more likely to have the irritable bowel syndrome than organic disease.
Patients confined to bed in hospital or who have had abdominal operations are often constipated. Starvation and changes in diet can be other causes.
MUCUS
The passage of mucus (white slime) may occur because of a solitary rectal ulcer, fistula or villous adenoma, or in the irritable bowel syndrome.
BLEEDING
Patients may present with the problem of haematemesis (vomiting blood), melaena (passage of jet-black stools) or haematochezia (passage of bright-red blood per rectum). Sometimes patients may present because routine testing for occult blood in the stools is positive (page 214). It is important to ensure that if vomiting of blood is reported, this is not the result of bleeding from a tooth socket or the nose, or coughing up of blood.
Haematemesis indicates that the site of the bleeding is proximal to or at the duodenum (see Table 13.1). Ask about symptoms of peptic ulceration; haematemesis is commonly due to bleeding chronic peptic ulceration, particularly from a duodenal ulcer. Peptic ulcers often bleed without abdominal pain.
TABLE 13.1
Causes of acute gastrointestinal bleeding
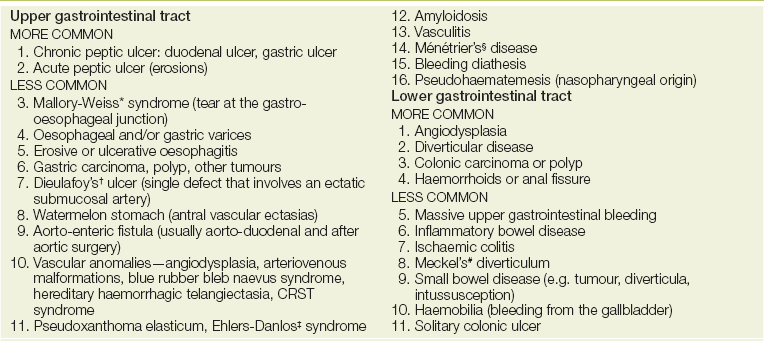
CRST = calcinosis, Raynaud’s phenomenon, sclerodactyly and telangiectasia.
*George Kenneth Mallory (1900-86), professor of pathology, Boston, and Soma Weiss (1898-1942), professor of medicine, Boston City Hospital, described this syndrome in 1929.
†Georges Dieulafoy (1839-1911), Paris physician.
‡Edvard Ehlers (1863-1937), German dermatologist, described the syndrome in 1901, and Henri Alexandre Danlos (1844-1912), French dermatologist, described the syndrome in 1908.
§Pierre Ménétrier (1859-1935), French physician.
#Johann Friedrich Meckel the younger (1781-1833), Professor of Surgery and Anatomy at Halle. His father and grandfather were also professors of anatomy.
Ask if the blood came up with the first vomit or not (see Questions box 13.6). A Mallory-Weiss tear usually occurs with repeated vomiting; typically the patient reports first the vomiting of clear gastric contents and then the vomiting of blood.
Questions box 13.6
Questions to ask the patient who presents with vomiting blood (haematemesis)
denotes symptoms for the possible diagnosis of an urgent or dangerous problem
1. Was there fresh blood in the vomitus? Or was the vomitus coffee-grain stained?
2. Have you passed any black stools or blood in the stools?
3. Before any blood was seen in the vomitus, did you experience intense retching or vomiting? (Mallory-Weiss tear)
4. Have you been taking aspirin, non-steroidal anti-inflammatory drugs or steroids?
5. Do you drink alcohol? Do you have liver disease?
Ask if there is blood in the stool, and whether it is on top or mixed in. Haemorrhoids and local anorectal diseases such as fissures will commonly present with passing small amounts of bright-red blood per rectum. The blood is normally not mixed in the stools but is on the toilet paper, on top of the stools or in the toilet bowl.
Melaena (black tarry stools) usually results from bleeding from the upper gastrointestinal tract, although right-sided colonic and small bowel lesions can occasionally be responsible. Massive rectal bleeding can occur from the distal colon or rectum, or from a major bleeding site higher in the gastrointestinal tract. With substantial lower gastrointestinal tract bleeding, it is important to consider the presence of angiodysplasia or diverticular disease (where bleeding more often occurs from the right rather than the left colon, even though diverticula are more common in the left colon).
Spontaneous bleeding into the skin, or from the nose or mouth, can be a problem for patients with coagulopathy resulting from liver disease.
JAUNDICE
Usually the relatives notice a yellow discolouration of the sclerae or skin before the patient does. Jaundice is due to the presence of excess bilirubin being deposited in the conjunctivae and skin. The causes of jaundice are described on page 217. If there is jaundice, ask about the colour of the urine and stools; pale stools and dark urine occur with obstructive or cholestatic jaundice because urobilinogen is unable to reach the intestine. Also ask about abdominal pain; gallstones, for example, can cause biliary pain and jaundice.5 (See Questions box 13.7.)
Questions box 13.7
Questions to ask the patient presenting with jaundice
denotes symptoms for the possible diagnosis of an urgent or dangerous problem
1. Is your urine dark? Are your stools pale? (Obstructive jaundice)
2. Do you have any skin itching (pruritus)?
3. Have you had any fever? (Cholangitis)
4. Have you had a change in your appetite or weight? (Malignancy)
5. Have you had any abdominal pain or change in bowel habit?
6. Have you had any vomiting of blood or passage of dark stools?
7. Do you drink alcohol? How much? How long? (CAGE questions, page 12)
8. Have you ever used intravenous drugs?
10. Have you ever had a blood transfusion?
11. Have you started any new medications recently?
12. Have you had any recent contact with patients with jaundice or liver problems?
13. Have you any history of recent high-risk sexual behaviours?
14. Have you travelled overseas to areas where hepatitis A is endemic?
15. Have you been immunised against hepatitis B?
16. Have you any history of inflammatory bowel disease? (Primary sclerosing cholangitis)
17. Have you had any surgeries (e.g. pancreatic or biliary)?
PRURITUS
This symptom means itching of the skin, and may be either generalised or localised. Cholestatic liver disease can cause pruritus that tends to be worse over the extremities. Other causes of pruritus are discussed on pages 186 and 539.
ABDOMINAL BLOATING AND SWELLING
A feeling of swelling (bloating) may be a result of excess gas or a hypersensitive intestinal tract (as occurs in the irritable bowel syndrome). Persistent swelling can be due to ascitic fluid accumulation; this is discussed on page 205. It may be associated with ankle oedema.
LETHARGY
Tiredness and easy fatigability are common symptoms for patients with acute or chronic liver disease, but the mechanism is not known. This can also occur because of anaemia due to gastrointestinal or chronic inflammatory disease. Lethargy is very common in the general population and is not a specific symptom.
Treatment
The treatment history is very important. Traditional non-steroidal anti-inflammatory drugs (NSAIDs), including aspirin, can induce bleeding from acute or chronic damage to the gastrointestinal tract. As described above, many drugs can result in disturbed defecation. A large number of drugs are also known to affect the liver. For example, acute hepatitis can occur with halothane, phenytoin or chlorothiazide. Cholestasis may occur from a hypersensitivity reaction to chlorpromazine or other phenothiazines, sulfonamides, sulfonylureas, phenylbutazone, rifampicin or nitrofurantoin. Anabolic steroids and the contraceptive pill can cause dose-related cholestasis. Fatty liver can occur with alcohol use, tetracycline, valproic acid or amiodarone. Large blood-filled cavities in the liver called peliosis hepatis can occur with anabolic steroid use or the contraceptive pill. Acute liver cell necrosis can occur if an overdose of paracetamol (acetaminophen) is taken.
Past history
Surgical procedures can result in jaundice from the anaesthesia (e.g. multiple uses of halothane), hypoxaemia of liver cells (hypotension during the operative or postoperative period) or direct damage to the bile duct during abdominal surgery. A history of relapsing and remitting epigastric pain in a patient who presents with severe abdominal pain may indicate that a peptic ulcer has perforated. A past history of inflammatory bowel disease (either ulcerative colitis or Crohn’s disease) is important as these are chronic diseases that tend to flare up.
Social history
The patient’s occupation may be relevant (e.g. healthcare workers may be exposed to hepatitis). Toxin exposure can also be important in chronic liver disease (e.g. carbon tetrachloride, vinyl chloride). If a patient has symptoms suggestive of liver disease, ask about recent travel to countries where hepatitis is endemic.
The alcohol history is very important, particularly as alcoholics often deny or understate the amount they consume (see List 1.3, page 12). Contact with anybody who has been jaundiced should always be noted.
The sexual history should be obtained. A history of any injections (e.g. intravenous drugs, plasma transfusions, dental treatment or tattooing) in a patient who presents with symptoms of liver disease is important, particularly as hepatitis B or C may be transferred in this way. Risk factors for viral hepatitis include sex (e.g. between men), intravenous drug use, blood transfusion and tattoos.
FAMILY HISTORY
A family history of colon cancer, especially of familial polyps, or inflammatory bowel disease is important. Ask about coeliac disease in the family. A positive family history of jaundice, anaemia, splenectomy or cholecystectomy may occur in patients with haemolytic anaemia (due to haemoglobin abnormalities or autoimmune disease) or congenital or familial hyperbilirubinaemia.
References
1. Hendrix, TR. Art and science of history taking in the patient with difficulty swallowing. Dysphagia. 1993; 8:69–73. [A very good review of the key historical features that must be obtained when a patient presents with trouble swallowing.].
2. Talley, NJ. Chronic unexplained diarrhea: what to do when the initial workup is negative. Rev Gastroenterol Disord. 2008; 8(3):178–185.
3. Talley, NJ, Lasch, KL, Baum, CL. A gap in our understanding: chronic constipation and its comorbid conditions. Clin Gastroenterol Hepatol. 2009; 7(1):9–19.
4. Ford, AC, Talley, NJ, Veldhuyzen van Zanten, SJ, Vakil, NB, Simel, DL, Moayyedi, P. Will the history and physical examination help establish that irritable bowel syndrome is causing this patient’s lower gastrointestinal tract symptoms. JAMA. 2008; 300(15):1793–1805.
5. Theodossi, A, Knill-Jones, RP, Skene, A. Interobserver variation of symptoms and signs in jaundice. Liver. 1981; 1:21–32. [The history and examination permitted a correct clinical diagnosis in jaundiced patients two-thirds of the time.].
aThe word nauseous can mean either nauseated (i.e. feeling like vomiting) or repulsive (i.e. likely to make other people vomit). It is probably best to use the word nauseated to describe a patient who feels like vomiting in order to avoid this unfortunate ambiguity. (The Latin word has only the second meaning.)
bRobert Milton Zollinger (1903–92), American surgeon, and Edwin H Ellison (1918–70), American physician. This syndrome is characterised by gastric acid hypersecretion, peptic ulceration and in 40% of cases diarrhoea, due to a gastrinoma (gastrin-secreting tumour). It was described in 1955.
cHarold Hirschsprung (1830–1916), physician, Queen Louise Hospital for Children, Copenhagen, described this disease in 1888. It had previously been described by Caleb Parry, English physician, in 1825.