The endocrine examination
The thyroid gland is that which when enlarged by disease gives rise to ‘Derbyshire neck’ or ‘goitre’.
A formal examination of the whole endocrine system is not routine. Usually, there will be some clue from the history and general inspection to indicate what specific endocrine disease should be pursued.
The thyroid
THE THYROID GLAND
Examination anatomy
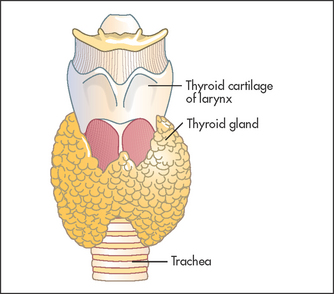
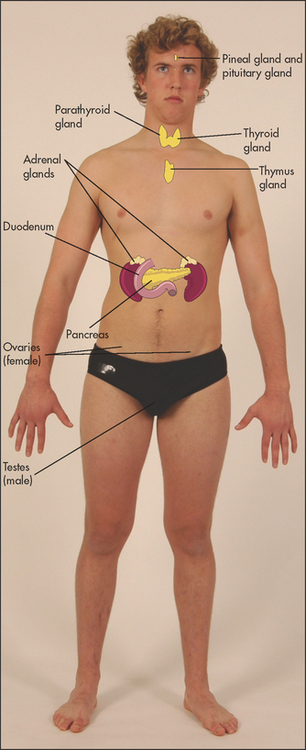
Even when it is not enlarged, the thyroida (see Figure 28.1) is the largest endocrine gland (see Figure 28.2). Enlargement is common, occurring in 10% of women and 2% of men and more commonly in iodine-deficient parts of the world. The normal gland lies anterior to the larynx and trachea and below the laryngeal prominence of the thyroid cartilage. It consists of a narrow isthmus in the middle line (anterior to the second to fourth tracheal rings and 1.5 centimetres in size) and two larger lateral lobes each about 4 centimetres long. Although the position of the larynx varies, the thyroid gland is almost always about 4 centimetres below the larynx.
Inspection
The normal thyroid may be just visible below the cricoid cartilage in a thin young person (see List 28.1).1,2 Usually only the isthmus is visible as a diffuse central swelling. Apparent enlargement (pseudogoitre) can occur as a result of the presence of a fat pad in the anterior and lateral part of the neck. This finding is more common in people who are overweight but can occur in those of normal weight. Enlargement of the gland, called a goitre,b should be apparent on inspection (see Good signs guide 28.1), especially if the patient extends the neck. Look at the front and sides of the neck and decide whether there is localised or general swelling of the gland. In healthy people the line between the cricoid cartilage and the suprasternal notch should be straight. An outward bulge suggests the presence of a goitre (see Figure 28.3). Remember that 80% of people with a goitre are biochemically euthyroid, 10% are hypothyroid and 10% are hyperthyroid.
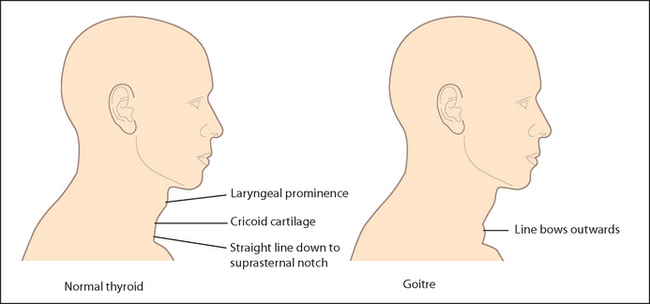
Figure 28.3 The thyroid and goitre (Adapted from McGee S. Evidence-based physical diagnosis, 2nd edition, St Louis, Saunders, 2007.)
The temptation to begin touching a swelling as soon as it has been detected should be resisted until a glass of water has been procured. The patient takes sips from this repeatedly so that swallowing is possible without discomfort. Ask the patient to swallow, and watch the neck swelling carefully.
Only a goitre or a thyroglossal cyst, because of attachment to the larynx, will rise during swallowing. The thyroid and trachea rise about 2 centimetres as the patient swallows; they pause for half a second and then descend. Some non-thyroid masses may rise slightly during swallowing but move up less than the trachea and fall again without pausing. A thyroid gland fixed by neoplastic infiltration may not rise on swallowing, but this is rare. Swallowing also allows the shape of the gland to be seen better.
Note whether an inferior border is visible as the gland rises. The thyroglossal cyst is a midline mass that can present at any age. It is an embryological remnant of the thyroglossal duct. Characteristically it rises when the patient protrudes the tongue.
Inspect the skin of the neck for scars. A thyroidectomy scar forms a ring around the base of the neck in the position of a high necklace. Look for prominent veins. Dilated veins over the upper part of the chest wall, often accompanied by filling of the external jugular vein, suggest retrosternal extension of the goitre (thoracic inlet obstruction). Rarely, redness of the skin over the gland occurs in cases of suppurative thyroiditis.
Palpation
Palpation is best begun from behind (see Figure 28.4) but warn the patient first. Place both hands with the pulps of the fingers over the gland. The patient’s neck should be slightly flexed so as to relax the sternocleidomastoid muscles. Feel systematically both lobes of the gland and its isthmus. Feel one side at a time; use one hand to steady the gland and the other to palpate.

Figure 28.4 Palpating the thyroid from behind while the patient swallows sips of water (Courtesy of Glenn McCulloch)
• Size: only an approximate estimation is possible (see Figure 28.5). Feel particularly carefully for a lower border, because its absence suggests retrosternal extension.
• Shape: note whether the gland is uniformly enlarged or irregular and whether the isthmus is affected. If a nodule that feels distinct from the remaining thyroid tissue is palpable, determine its location, size, consistency, tenderness and mobility. Also decide whether the whole gland feels nodular (multinodular goitre).
• Consistency: this may vary in different parts of the gland. Soft (but firmer than a fat pad) is normal; the gland is often firm in simple goitre and typically rubbery hard in Hashimoto’s thyroiditis. A stony, hard node suggests carcinoma (see List 28.2), calcification in a cyst, fibrosis or Riedel’s thyroiditis.
• Tenderness: this may be a feature of thyroiditis (subacute or rarely suppurative), or less often of a bleed into a cyst or carcinoma.
• Mobility: carcinoma may tether the gland.
• A thrill: this may be palpable over the gland, as occurs when the gland is unusually metabolically active (e.g. in thyrotoxicosis).
Repeat the assessment while the patient swallows.
Palpate the cervical lymph nodes. These may be involved in carcinoma of the thyroid.
Move to the front. Palpate again. Localised swellings may be more easily defined here. Note the position of the trachea, which may be displaced by a retrosternal gland.
Percussion
The upper part of the manubrium can be percussed from one side to the other. A change from resonant to dull indicates a possible retrosternal goitre, but this is not a very reliable sign.
Auscultation
Listen over each lobe for a bruit (a swishing sound coinciding with systole). This is a sign of increased blood supply, which may occur in hyperthyroidism, or occasionally from the use of anti-thyroid drugs. The differential diagnosis also includes a carotid bruit (louder over the carotid itself) or a venous hum (obliterated by gentle pressure over the base of the neck). If there is a goitre, apply mild compression to the lateral lobes and listen again for stridor.
Pemberton’s sign
Ask the patient to lift both arms as high as possible. Wait a few moments, then search the face eagerly for signs of congestion (plethora) and cyanosis. Associated respiratory distress and inspiratory stridor may occur. Look at the neck veins for distension (venous congestion). Ask the patient to take a deep breath in through the mouth and listen for stridor. This is a test for thoracic inlet obstruction due to a retrosternal goitre or any retrosternal mass.3 (Lifting the arms up pulls the thoracic inlet upwards so that the goitre occupies more of this inflexible bony opening.) Examination of the thyroid should be part of every routine physical examination. Causes of a goitre are outlined in List 28.3.
HYPERTHYROIDISM (THYROTOXICOSIS)
Hyperthyroidism is a disease caused by excessive concentrations of thyroid hormones. The cause is usually overproduction by the gland but it may sometimes be due to accidental or deliberate use of thyroid hormone (thyroxine) tablets—thyrotoxicosis factitia. Thyroxine is sometimes taken by patients as a way of losing weight. The cause may be apparent in these cases if a careful history is taken (see Questions box 28.1). The antiarrhythmic drug amiodarone, which contains large quantities of iodine, can cause thyrotoxicosis in up to 12% of patients in low iodine-intake areas. Many of the clinical features of thyrotoxicosis are characterised by signs of sympathetic nervous system overactivity such as tremor, tachycardia and sweating. The explanation is not entirely clear. Catecholamine secretion is usually normal in hyperthyroidism; however, thyroid hormone potentiates the effects of catecholamines, possibly by increasing the number of adrenergic receptors in the tissues.
Questions box 28.1
Questions to ask the patient with suspected hyperthyroidism
 denotes symptoms for the possible diagnosis of an urgent or dangerous problem.
denotes symptoms for the possible diagnosis of an urgent or dangerous problem.
1. Have you any history of thyroid problems?
2. Have you a family history of thyrotoxicosis? (There is a familial incidence of Graves’ disease and associated autoimmune conditions such as vitiligo, Addison’s disease, pernicious anaemia, type 1 diabetes, myasthenia gravis and premature ovarian failure)
3. Have you taken amiodarone or thyroxine?
4. Have you had recent exposure to iodine? (Iodinated X-ray contrast materials can precipitate thyrotoxicosis—usually in patients with an existing multinodular goitre)
5. Have you had palpitations? (Thyrotoxicosis can present with atrial fibrillation, which may precipitate heart failure)
6. Have you noticed insomnia, irritability or hyperactivity?
7. Have you had loss of weight, diarrhoea or increased stool frequency, increased sweating or heat intolerance?
8. Have you had muscle weakness? (Proximal muscle weakness is common and the patient may have noticed difficulty getting out of a chair)
9. Have you had eye problems such as double vision, grittiness, redness or pain behind the eyes?
The most common cause of thyrotoxicosis in young people is Graves’c disease, an autoimmune disease where circulating immunoglobulins stimulate thyroid-stimulating hormone (TSH) receptors on the surface of the thyroid follicular cells (see List 28.5 below).
Examine a suspected case of thyrotoxicosis as follows.
General inspection
Look for signs of weight loss, anxiety and the frightened facies of thyrotoxicosis.
Hands
Ask the patient to put out his or her arms and look for a fine tremor (due to sympathetic overactivity). Laying a sheet of paper over the patient’s fingers may more clearly demonstrate this tremor, to the amazement of less-experienced colleagues.
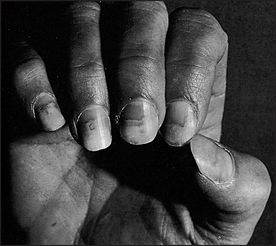
Look at the nails for onycholysis (Plummer’sd nails; see Figure 28.6). Onycholysis (where there is separation of the nail from its bed) is said to occur particularly on the ring finger, but can occur on all the fingernails and is apparently due to sympathetic overactivity. Inspect for thyroid acropathy (acropathy is another term for clubbing), seen rarely in Graves’ disease but not with other causes of thyrotoxicosis.
Inspect for palmar erythema and feel the palms for warmth and sweatiness (sympathetic overactivity).
Take the pulse. Note the presence of sinus tachycardia (sympathetic overdrive) or atrial fibrillation (due to a shortened refractory period of atrial cells related to sympathetic drive and hormone-induced changes). The pulse may also have a collapsing character due to a high cardiac output.
Arms
Ask the patient to raise the arms above the head and so test for proximal myopathy. Tap the arm reflexes for abnormal briskness, especially in the relaxation phase.
Eyes
Examine the patient’s eyes for exophthalmos, which is protrusion of the eyeball from the orbit (see Figure 28.7 and List 28.4). This may be very obvious, but if not, look carefully at the sclerae, which in exophthalmos are not covered by the lower eyelid. Next look from behind over the patient’s forehead for exophthalmos, where the eye will be visible anterior to the superior orbital margin. Now examine for the complications of proptosis, which include: (1) chemosis (oedema of the conjunctiva and injection of the sclera, particularly over the insertion of the lateral rectus); (2) conjunctivitis; (3) corneal ulceration (due to inability to close the eyelids); (4) optic atrophy (rare and possibly due to optic nerve stretching); and (5) ophthalmoplegia (the inferior rectus muscle power tends to be lost first, and later convergence is weakened).

The mechanism of exophthalmos is uncertain. It occurs only in Graves’ disease. It may precede the onset of thyrotoxicosis or may persist after the patient has become euthyroid. It is characterised by an inflammatory infiltrate of the orbital contents, but not of the globe itself. The orbital muscles are particularly affected, and an increase in their size accounts for most of the increased volume of the orbital contents and therefore for protrusion of the globe. It is probably due to an autoimmune abnormality.
Next examine for the components of thyroid ophthalmopathy, which are related to sympathetic overactivity and are not specific for Graves’ disease. Look for the thyroid stare (a frightened expression) and lid retraction (Dalrymple’se sign), where there is sclera visible above the iris. Test for lid lag (von Graefe’sf sign) by asking the patient to follow your finger as it descends at a moderate rate from the upper to the lower part of the visual field. Descent of the upper lid lags behind descent of the eyeball.
If ptosis is present, one should rule out myasthenia gravis, which can be associated with autoimmune disease.
Neck
Examine for thyroid enlargement, which is usually detectable (60–90% of patients). In Graves’ disease the gland is classically diffusely enlarged and is smooth and firm. An associated thrill is usually present, but this finding is not specific for thyrotoxicosis caused by Graves’ disease. Absence of thyroid enlargement makes Graves’ disease unlikely, but does not exclude it. Possible thyroid abnormalities in patients who are thyrotoxic but do not have Graves’ disease include a toxic multinodular goitre, a solitary nodule (toxic adenoma) and painless, postpartum or subacute (de Quervain’sg) thyroiditis. Patients with de Quervain’s thyroiditis typically have a moderately enlarged firm and tender gland. Thyrotoxicosis may occur without any goitre, particularly in elderly patients. Alternatively, in hyperthyroidism due to a rare abnormality of trophoblastic tissue (a hydatidiform mole or choriocarcinoma of the testis or uterus), or excessive thyroid hormone replacement, the thyroid gland will not usually be palpable.
If a thyroidectomy scar is present, assess for hypoparathyroidism (Chvostek’sh or Trousseau’si signs; page 372). These signs are most often present in the first few days after the operation.
Chest
Gynaecomastia (page 376) occurs occasionally. Examine the heart for systolic flow murmurs (due to increased cardiac output) and signs of congestive cardiac failure, which may be precipitated by thyrotoxicosis in older people.
Legs
Look first for pretibial myxoedema. This takes the form of bilateral firm, elevated dermal nodules and plaques, which can be pink, brown or skin-coloured. They are caused by mucopolysaccharide accumulation. Despite the name, this occurs only in Graves’ disease and not in hypothyroidism. Test now for proximal myopathy and hyperreflexia in the legs, which is present in only about 25% of cases.
HYPOTHYROIDISM (MYXOEDEMA)
Hypothyroidism (deficiency of thyroid hormone) is due to primary disease of the thyroid or, less commonly, is secondary to pituitary or hypothalamic failure (see List 28.5). Myxoedema implies a more severe form of hypothyroidism. In myxoedema, for unknown reasons, hydrophilic mucopolysaccharides accumulate in the ground substance of tissues including the skin. This results in excessive interstitial fluid, which is relatively immobile, causing skin thickening and a doughy induration.
The symptoms of hypothyroidism are insidious but patients or their relatives may have noticed cold intolerance, muscle pains, oedema, constipation, a hoarse voice, dry skin, memory loss, depression or weight gain (see Questions box 28.2).
Examine the patient with suspected hypothyroidism as follows (see Good signs guide 28.2).
General inspection
Look for signs of obvious mental and physical sluggishness, or evidence of the very rare myxoedema madness. Hypothyroid speech is a feature in about one-third of patients. This is characteristically slow, nasal and deep in pitch. Obesity is no more common than in euthyroid people.
Hands
Note peripheral cyanosis (due to reduced cardiac output) and swelling of the skin, which may appear cool and dry. The yellow discolouration of hypercarotenaemia (there is slowing down of hepatic metabolism of carotene) may be seen on the palms. Look for palmar crease pallor—anaemia may be due to: (1) chronic disease; (2) folate deficiency secondary to bacterial overgrowth, or vitamin B12 deficiency due to associated pernicious anaemia; or (3) iron deficiency due to menorrhagia.
Take the pulse, which may be of small volume and slow. Test for sensory loss, as the carpal tunnel is thickened in myxoedema.
Arms
Test for proximal myopathy (rare) and a ‘hung-up’ biceps or Achilles tendon reflex (see below).
Face
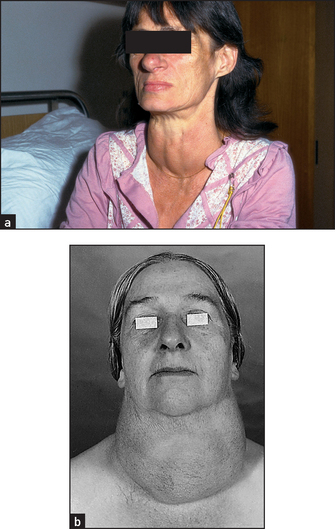
Inspect the patient’s face (see Figure 28.8). The skin, but not the sclerae, may appear yellow due to hypercarotenaemia. The skin may be generally thickened, and alopecia may be present, as may vitiligo (an associated autoimmune disease).

Inspect the eyes for periorbital oedema. Loss or thinning of the outer third of the eyebrows can occur in myxoedema but is also common in healthy people. Look for xanthelasmata (due to associated hypercholesterolaemia). Palpate for coolness and dryness of the skin and hair. There may be thinning of the scalp hair.
Look at the tongue for swelling. Ask the patient to speak, and listen for coarse, croaking, slow speech. Bilateral nerve deafness may occur with endemic or congenital hypothyroidism.
Thyroid gland
A primary decrease in thyroid hormone results in a compensatory oversecretion of TSH. A goitre will result if there is viable thyroid tissue.
Many cases of hypothyroidism are not associated with an enlarged gland as there is little thyroid tissue. The exceptions include severe iodine deficiency, enzyme deficiency (inborn errors of metabolism), late Hashimoto’s disease or treated (with radioactive iodine) thyrotoxicosis (see List 28.5).
Legs
There may be non-pitting oedema. Ask the patient to kneel on a chair with the ankles exposed. Tap the Achilles tendon with a reflex hammer. There is apparently normal (in fact, slightly slowed) contraction followed by delayed relaxation of the foot in hypothyroidism (the ‘hung-up’ reflex; see Figure 28.11). Examine for signs of peripheral neuropathy and for other uncommon neurological abnormalities associated with hypothyroidism (see List 28.6).

Figure 28.11 Testing ankle jerks (second method see also page 453) This method best demonstrates the ‘hung-up’ reflexes of hypothyroidism. Look for rapid dorsiflexion followed by slow plantar flexion after the tendon is tapped. (Courtesy of Glenn McCulloch)
The pituitary
Pituitary tumours can present as a result of: (1) local effects such as headaches, visual field loss and loss of acuity; and (2) changes in pituitary hormone secretion. (See Questions box 28.3.) These changes include: (1) excess growth hormone, causing acromegaly; (2) excess adrenocorticotrophic hormone (ACTH), causing Cushing’s syndrome; (3) excess prolactin, causing galactorrhoea, secondary amenorrhoea or male infertility or deficiency (hypopituitarism); and (4) excess TSH, causing hyperthyroidism.
PANHYPOPITUITARISM
Panhypopituitarism is a deficiency of most or all of the pituitary hormones and is usually due to a space-occupying lesion or destruction of the pituitary gland (see List 28.7). Hormone production is often lost in the following order: (1) growth hormone (dwarfism in children, insulin sensitivity in adults); (2) prolactin (failure of lactation after delivery); (3) gonadotrophins (loss of secondary sexual characteristics, secondary amenorrhoea in women, loss of libido and infertility in men); (4) TSH (hypothyroidism); and (5) ACTH (hypoadrenalism, with loss of secondary sexual hair due to decreased adrenal androgen production).
However, isolated single hormonal deficiencies or multiple deficiencies may occur in any combination.
General inspection
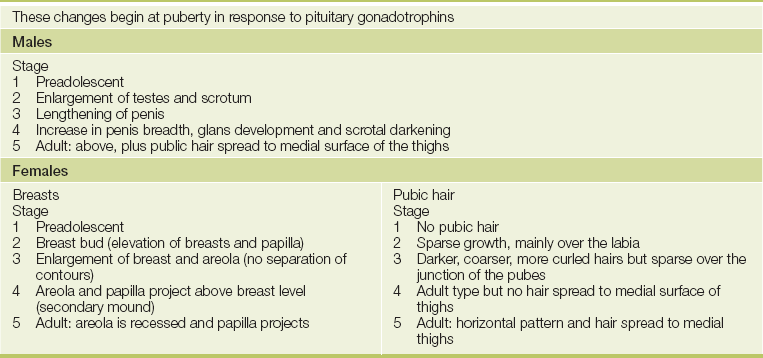
The patient may be of short stature (failure of growth hormone secretion before growth is complete). Look for pallor of the skin (due to anaemia or occasionally ACTH deficiency because of the loss of its melanocyte-stimulating activity), fine-wrinkled skin and lack of body hair (due to gonadotrophin deficiency). There may be complete absence of the secondary sexual characteristics (see Table 28.1) if gonadotrophin failure occurred before puberty.
Face
Look at the face more closely. Multiple skin wrinkles around the eyes are characteristic of gonadotrophin deficiency. Inspect the forehead carefully for hypophysectomy scars—transfrontal scars will be apparent (see Figure 28.9) but not transsphenoidal ones, as this operation is performed through the base of the nose, via an incision under the upper lip.
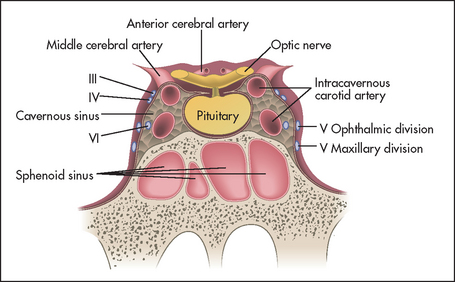
Examine the eyes (see Chapter 32). The visual fields must be assessed for any defects, especially bitemporal hemianopia (an enlarging pituitary tumour may compress the optic chiasm), and the fundi examined for optic atrophy (optic nerve compression from a pituitary tumour). Assess the third, fourth, sixth and first divisions of the fifth cranial nerves, as these may be affected by extrapituitary tumour expansion into the cavernous sinus (see Figure 28.10).
Feel the facial hair over the bearded area in men for normal beard growth (which is lost with gonadotrophin deficiency).
Chest
Go on to the chest. Look for skin pallor and for a decrease in nipple pigmentation. In men, decreased body hair (axillary and chest) may be present. In women, secondary breast atrophy may be found.
Genital region
Loss of pubic hair occurs in both sexes. In men, testicular atrophy may be present. Atrophied testes are characteristically small and firm. The normal-sized testis is about 15–25 mL in volume.
Ankle reflexes
Test for ‘hung-up’ jerks (see Figure 28.11). These are an important sign of pituitary hypothyroidism. Occasionally, pituitary hypothyroid patients may be slightly overweight, but the classical myxoedematous appearance is usually absent.
ACROMEGALY
Acromegalyj is excessive secretion of growth hormone, typically due to an eosinophilic pituitary adenoma. Growth hormone stimulates the liver and other tissues to produce somatomedins, which in turn promote growth. Growth hormone is also a protein anabolic hormone exerting its effects at the ribosomal level, and it is diabetogenic as it exerts an anti-insulin effect in muscle and increases hepatic glucose release. The disease has a very gradual onset and patients may not have noticed symptoms. Most patients, however, have headache caused by stretching of the dura by the enlarging pituitary tumour.
Gigantism is the result of growth hormone hypersecretion occurring before puberty and fusion of the epiphyses. It results in massive skeletal as well as soft-tissue growth. Acromegaly occurs when the growth plates have fused, so that only soft-tissue and flat-bone enlargement are possible.

Hands
Sit the patient on the side of the bed or in a chair and look at his or her hands. Notice a wide spade-like shape (due to soft-tissue and bony enlargement). Increased sweating and warmth of the palms may be noted. This is due to an increased metabolic rate. The skin may appear thickened. Changes of osteoarthritis in the hands are common and are due to skeletal overgrowth. Examine for median nerve entrapment, which can occur because of soft-tissue overgrowth in the carpal tunnel area.
Arms
Proximal myopathy may be present. Palpate behind the medial epicondyle (the ‘funny bone’) for ulnar nerve thickening.
Axillae
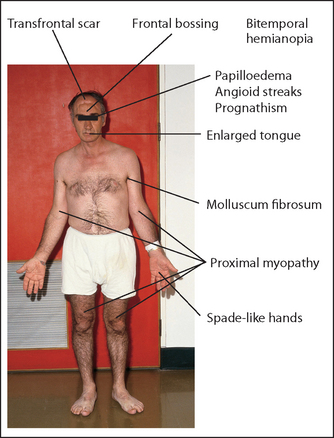
Carefully inspect the axillae for skin tags (called molluscum fibrosum, which are non-tender skin-coloured protrusions; see Figure 28.12(b)). Summon up courage and feel for greasy skin. Look for acanthosis nigricans.
Face
Look for a large supraorbital ridge, which causes frontal bossing (this may also occur occasionally in Paget’s disease, rickets, achondroplasia or hydrocephalus). The lips may be thickened.
Examine the eyes for visual field defects; classically there may be bitemporal hemianopia if the pituitary tumour is large. Look in the fundi for optic atrophy (due to nerve compression) and papilloedema (due to raised intracranial pressure with an extensive tumour). The presence of angioid streaks (red, brown or grey streaks that are three to five times the diameter of a retinal vein and appear to emanate from the optic disc) should also be sought: these are due to degeneration and fibrosis of Bruch’s membrane. Also note hypertensive changes or diabetic changes in the fundus. Ocular palsies may occur with an extensive pituitary tumour.
Look in the mouth for an enlarged tongue that may not fit neatly between the teeth. The teeth themselves may be splayed and separated, with malocclusion as the jaw enlarges. The lower jaw may look square and firm (as it does on some American actors). When the jaw protrudes it is called prognathism.k
Neck
The thyroid may be diffusely enlarged or multinodular (all the internal organs may enlarge under the influence of growth hormone). Listen to the voice for hoarseness.
Chest
Look for coarse body hair and gynaecomastia. Examine the heart for signs of arrhythmias, cardiomegaly and congestive cardiac failure, which may be due to ischaemic heart disease, hypertension or cardiomyopathy (all more common in acromegaly).
Abdomen
Examine for hepatic, splenic and renal enlargement, and look for testicular atrophy (the latter indicating gonadotrophin deficiency secondary to an enlarging pituitary tumour). Acromegaly may be associated with a mixed pituitary tumour, and resultant hyperprolactinaemia can also cause testicular atrophy.
Lower limbs
Look for signs of osteoarthritis in the hips especially, and knees (Chapter 24), and for pseudogout. Foot drop may be present because of common peroneal nerve entrapment (page 458).
Urinalysis and blood pressure
Test the urine for glucose, as excess growth hormone is diabetogenic in 25% of cases. Take the blood pressure to test for hypertension.
Finally, decide if the disease is active or not. Signs of active disease include: (1) large numbers of skin tags (skin tags can occur commonly in healthy people); (2) excessive sweating; (3) the presence of glycosuria; (4) increasing visual field loss; (5) enlarging goitre; and (6) hypertension. Note: Headache also suggests disease activity.
OTHER PITUITARY SYNDROMES
Cushing’s syndrome can occur as a result of excess pituitary ACTH secretion but has other causes as well. Hyperthyroidism can occur as a result of excess pituitary TSH production. Prolactinomas of the pituitary can cause galactorrhoea (production of milk) in both women and men.
The adrenals
CUSHING’S SYNDROME
Cushing’s syndrome is due to a chronic excess of glucocorticoids. Steroids have multiple effects on the body, due to stimulation of the DNA-dependent synthesis of select messenger ribonucleic acids (RNAs). This leads to the formation of enzymes, which alter cell function and result in increased protein catabolism and gluconeogenesis. Remember that Cushing’s disease is specifically pituitary ACTH overproduction, while Cushing’s syndrome is due to excessive steroid hormone production from any cause (see List 28.8, Good signs guide 28.3 and Questions box 28.4).
Questions box 28.4
Questions to ask the patient with suspected Cushing’s syndrome
denotes symptoms for the possible diagnosis of an urgent or dangerous problem.
1. Have you gained a lot of weight recently? How much?
4. Have you had problems with acne?
5. Have you felt agitated and been unable to sleep?
6. Have you had problems with weakness of your muscles or difficulty getting up out of chairs? (Proximal myopathy)
7. Have you had problems maintaining erections (men) or had amenorrhoea (women)?
Hands
Skinfold thickness is best assessed on the backs of the hands and may be reliable only as a sign of Cushing’s in young women. The skinfold should be thicker than 1.8 millimetres.
Standing
Have the patient undress to the underpants and, if possible, stand up. Look from the front, back and sides. Note moonlike facies and central obesity (see Figures 28.13 and 28.14). The limbs appear thin despite sometimes very gross truncal (mostly intra-abdominal rather than subcutaneous fat) obesity.l This is the characteristic fat distribution that occurs with steroid excess. Bruising may be present (due to loss of perivascular supporting tissue–protein catabolism). Look for excessive pigmentation on the extensor surfaces (because of melanocyte-stimulating-hormone [MSH]-like activity in the ACTH molecule). Ask the patient to squat at this point to test for proximal myopathy, due to mobilisation of muscle tissue or excessive urinary potassium loss. Look at the back for the buffalo hump, which is due to fat deposition over the interscapular area. Palpate for bony tenderness of the vertebral bodies due to crush fractures from osteoporosis (a steroid anti-vitamin D effect and increased urinary calcium excretion may be responsible in part for disruption of the bone matrix).

Sitting
Ask the patient to sit on the side of the bed, but remember that he or she may be suffering from steroid psychosis and refuse to do anything you ask.
Face and neck
Look for plethora (this occurs in the absence of polycythaemia which, however, may also be present). The face may have a typical moon shape due to fat deposition in the upper part. Inspect for acne and hirsutism (if adrenal androgen secretion is also increased). Telangiectasias may also be present.
Examine the visual fields for signs of a pituitary tumour, and the fundi for optic atrophy, papilloedema and hypertensive or diabetic changes. Look for supraclavicular fat pads.
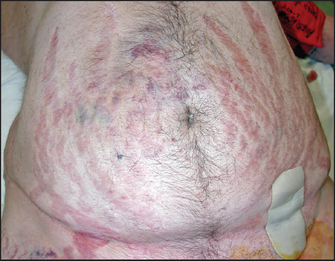
Abdomen
Lay the patient in bed on one pillow. Examine the abdomen for purple striae, which are due to weakening and disruption of collagen fibres in the dermis, leading to exposure of vascular subcutaneous tissues (see Figure 28.14). In patients with Cushing’s syndrome these are wider (1 centimetre) than those seen in people who have gained weight rapidly for other reasons. They may also be present near the axillae on the upper arms or on the inside of the thighs. Palpate for adrenal masses (rarely a large adrenal carcinoma will be palpable over the renal area). Palpate for hepatomegaly due to fat deposition or, rarely, to adrenal carcinoma deposits.
Legs
Palpate for oedema (due to salt and water retention). Look for bruising and poor wound healing.
Urinalysis and blood pressure
Test the urine for sugar (as steroids are diabetogenic; this is due to an increase in hepatic gluconeogenesis and an anti-insulin effect on peripheral tissues). Hypertension is common due to salt and water retention (an aldosterone effect) and possibly to increased angiotensin secretion or a direct effect on blood vessels.
Synthesis of signs
Certain signs are of some aetiological value in Cushing’s syndrome.
• Signs which suggest that adrenal carcinoma may be the underlying cause: (1) a palpable abdominal mass; (2) signs of virilisation in the female; (3) gynaecomastia in the male.
• Signs which suggest that ectopic ACTH production may be the cause: (1) absence of the Cushingoid body habitus unless the responsible tumour has been slow growing and allowed time for Cushingoid features to develop; (2) more prominent oedema and hypertension; (3) marked muscle weakness. Note: When Cushing’s is due to ectopic ACTH production from a small cell carcinoma, the patient is much more likely to be male (LR+ 13)4 and the history to be of more rapid onset of the symptoms and signs (18 months: LR+ 15).4
• Significance of hyperpigmentation: this suggests an extra-adrenal tumour, or enlargement of an ACTH-secreting pituitary adenoma following adrenalectomy (Nelson’sm syndrome).
ADDISON’S DISEASE
Addison’s diseasen is adrenocortical hypofunction with reduction in the secretion of glucocorticoids and mineral ocorticoids. It is most often due to autoimmune disease of the adrenal glands. Other causes are outlined in List 28.9.
If this disease is suspected, look for cachexia. Then, with the patient undressed, look for pigmentation in the palmar creases (see Figure 28.15), elbows, gums and buccal mucosa and genital area and in scars. This occurs because of compensatory ACTH hypersecretion in primary hypoadrenalism (when there is adrenal disease), as ACTH has melanocyte-stimulating activity. Also inspect for vitiligo (localised hypomelanosis; see Figure 28.16), an autoimmune disease that is commonly associated with autoimmune adrenal failure.


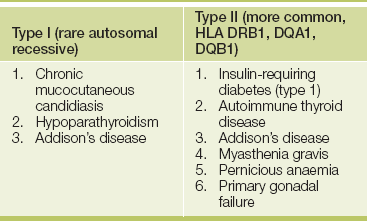
Take the blood pressure and test for postural hypotension. Remember that the rest of the autoimmune disease cluster may be associated with autoimmune adrenal failure (see Table 28.2).
TABLE 28.2
A classification of conditions found in various combinations in autoimmune polyglandular syndromes
References
1. Alvi, A, Johnson, JT. The neck mass. A challenging differential diagnosis. Postgrad Med. 1995; 97:87–90. [93–94. Reviews how the history and examination narrow the differential diagnosis.].
2. Siminoski, K. Does this patient have a goiter. JAMA. 1995; 273:813–817. [A guide to examining the thyroid.].
3. Wallace, C, Siminoski, K. The Pemberton sign. Ann Intern Med. 1996; 125:568–569. [Describes the sign, due to a retrosternal goitre compressing cephalic venous inflow (and in some tracheal airflow).].
4. McGee, S. Evidence-based physical diagnosis, 3rd edn. St Louis: Saunders, 2012.
aThe first person to distinguish an enlarged thyroid from cervical lymphadenopathy was the Roman medical writer Aulus Aurelius Cornelius Celsus (approx. 53 BC–7 AD). He is more famous for describing the four cardinal signs of inflammation: redness, swelling, heat and tenderness.
bFrom the Latin guttur, meaning ‘throat’.
cRobert Graves (1796–1853), Dublin physician.
dHenry Plummer (1874–1936), physician at the Mayo Clinic in the United States.
eJohn Dalrymple (1803–52), British ophthalmic surgeon.
fFriedrich von Graefe (1828–70), professor of ophthalmology in Berlin, described this in 1864. He was one of the most famous ophthalmologists of the 19th century; Horner was one of his pupils. He died of tuberculosis at the age of 42.
gFritz de Quervain (1868–1940), professor of surgery, Berne, Switzerland.
hFranz Chvostek (1835–84), Viennese physician.
iArmand Trousseau (1801–1867), Parisian physician.
jAcromegaly was first described by Pierre Marie in 1886 and was first called hyperpituitarism by Harvey Cushing in 1909. The acral parts are the hands and feet.
kFrom the Greek pro meaning ‘forwards’ and gnathos meaning ‘jaw’.
lThe enthusiastic student can calculate the central obesity index. This is the sum of three truncal circumferences (neck, chest and waist) divided by six peripheral ones (arms, thighs and legs on both sides). A normal index is less than 1.
mWarren Nelson (1906–64), American endocrinologist.
nThomas Addison (1793–1860) described the disease in 1849. Addison, Bright and Hodgkin made up the famous trio of physicians at Guy’s Hospital, London.