A system for the infectious diseases examination
We have selected two important presentations to be covered in this chapter to show how infectious diseases can be approached in a systematic manner.
Pyrexia of unknown origin
Pyrexia of unknown origin (PUO) is defined as documented fever (>38°C) of more than 3 weeks’ duration, where no cause is found despite basic investigations.1 The most frequent causes to consider are tuberculosis, occult abscess (usually intra-abdominal), osteomyelitis, infective endocarditis, lymphoma or leukaemia, systemic-onset juvenile rheumatoid arthritis, giant cell arteritis and drug fever (drug fever is responsible for 10% of fevers leading to hospital admission2). In studies of fever of unknown origin, infection is found to be the cause in 30%, neoplasia in 30%, connective tissue disease in 15% and miscellaneous causes in 15%; in 10% the aetiology remains unknown (see List 41.1). Remember, the longer the duration of the fever, the less likely there is an infectious aetiology. The majority of patients do not have a rare disease but rather a relatively common disease presenting in an unusual way.3
HISTORY
The history may give a number of clues in these puzzling cases. In some patients a careful history may give the diagnosis where expensive tests have failed. See Questions box 41.1.
Questions box 41.1
General questions to ask the patient with a fever
 denotes symptoms for the possible diagnosis of an urgent or dangerous problem.
denotes symptoms for the possible diagnosis of an urgent or dangerous problem.
1. How long have you had high temperatures?
2. Have you taken your own temperature? How high has it been?
3. Have you had shivers and shakes (rigors)? (Shaking chills suggest bacteraemia4)
4. Has anyone you know had a similar illness?
5. What medications are you taking?
6. Have you had any recent illnesses?
7. Have you had any recent operations or medical procedures?
8. Have you travelled recently? Where to?
9. Did you take antimalarial prophylaxis and have the recommended vaccinations for your trip?
The time course of the fever and any associated symptoms must be uncovered. Symptoms from the various body systems should be sought methodically. Examples include:
1. Gastrointestinal system—diarrhoea, abdominal pain, recent abdominal surgery (inflammatory bowel disease, diverticular disease, cholangitis).
2. Cardiovascular system—heart murmurs, dental procedures (infective endocarditis), chest pain (pericarditis).
3. Rheumatology—joint symptoms, rashes.
4. Neurology—headache (meningitis, cerebral abscess).
5. Genitourinary system—history of renal disease or infection, dysuria.
6. Respiratory system—old tuberculosis (TB) or recent TB contact, chest symptoms.
Details of any recent overseas travel are important. Find out also about hobbies and exposure to pets. Occupational exposure may be important. Take a drug history. Find out if the patient is involved in behaviour posing a risk of HIV infection. Patients who are already in hospital may have infected cannulas or old cannula sites.
Fever due to bacteraemia (the presence of viable bacteria in the bloodstream) is associated with a higher risk of mortality. Bacteraemia is present in up to 20% of hospital patients with acute fever.4,5
The systemic inflammatory response syndrome (SIRS) refers to two or more of the following four features: fever >38.3°C (or temperature <36°C), tachycardia (>90 beats/minute), tachypnoea (>20 breaths/minute) and an elevated white cell count (although it may be suppressed). SIRS may be due to acute infection but can also occur after burns or surgery or with other inflammatory diseases (e.g. thromboembolism, pancreatitis, vasculitis, autoimmune disease). Sepsis refers to the presence of infection in the setting of SIRS, so SIRS is sensitive but not specific for bacteraemia.4 Early identification of sepsis remains a clinical diagnosis, and immediate treatment with antibiotics saves lives.
EXAMINATION
General
Look at the temperature chart to see whether there is a pattern of fever that is identifiable. Inspect the patient and decide how seriously ill he or she appears. Search for the features of SIRS (fever, tachycardia, tachypnoea). Look for evidence of weight loss (indicating a chronic illness). Note any skin rash (see List 41.2). The details of the examination required will depend on the patient’s history.
Hands
Look for the stigmata of infective endocarditis or vasculitic changes. Note whether there is clubbing. The presence of arthropathy or Raynaud’s phenomenon may point to a connective tissue disease.
Arms
Inspect for drug injection sites suggesting intravenous drug abuse (see Figure 7.2 on page 97). Feel for the epitrochlear and axillary nodes (e.g. lymphoma, other malignancy, sarcoidosis, focal infections).
Head and neck
Feel the temporal arteries (over the temples). In temporal arteritis these may be tender and thickened.
Examine the eyes for iritis or conjunctivitis (connective tissue disease—e.g. Reiter’s syndrome) or jaundice (e.g. ascending cholangitis, blackwater fever in malaria). Look in the fundi for choroidal tubercles in miliary tuberculosis, Roth’s spots in infective endocarditis and retinal haemorrhages or the infiltrates of leukaemia or lymphoma.
Inspect the face for a butterfly rash (systemic lupus erythematosus, see Figure 25.11 on page 333) or seborrhoeic dermatitis, which is common in patients with HIV infection.
Examine the mouth for ulcers, gum disease or candidiasis, and the teeth and tonsils for infection (e.g. abscess). Look in the ears for otitis media. Feel the parotid glands for evidence of infection.
Palpate the cervical lymph nodes. Examine for thyroid enlargement and tenderness (subacute thyroiditis).
Chest
Examine the chest. Palpate for bony tenderness. Carefully examine the respiratory system (e.g. for signs of pneumonia, tuberculosis, empyema, carcinoma) and the heart for murmurs (e.g. infective endocarditis, atrial myxoma) or rubs (e.g. pericarditis).
Abdomen
Examine the abdomen. Inspect for rashes, including rose-coloured spots (in typhoid fever—2- to 4-millimetre flat red spots, which blanch on pressure and occur on the upper abdomen and lower chest). Examine for evidence of hepatomegaly and ascites (e.g. spontaneous bacterial peritonitis, hepatic carcinoma, metastatic deposits), splenomegaly (e.g. haemopoietic malignancy, infective endocarditis, malaria), renal enlargement (e.g. renal cell carcinoma) or localised tenderness (e.g. collection of pus). Palpate for testicular enlargement (e.g. seminoma, tuberculosis). Feel for inguinal lymphadenopathy.
Perform a rectal examination, feeling for a mass or tenderness in the rectum or pelvis (e.g. abscess, carcinoma, prostatitis). Perform a vaginal examination to detect collections of pelvic pus or evidence of pelvic inflammatory disease. Look at the penis and scrotum for a discharge or rash.
HIV infection and AIDS
The acquired immunodeficiency syndrome (AIDS), first described in 1981, is caused by the human immunodeficiency virus (HIV).6,7 This is a T-cell lymphotrophic virus, which results in T4-cell destruction and therefore susceptibility to opportunistic infections and the development of tumours, notably Kaposi’sa sarcoma and nonHodgkin’s lymphoma.
HISTORY
HIV infection should be suspected particularly if the patient falls into a high-risk group (e.g. male homosexual, intravenous drug abuser, sexual tourist, sexual partner of HIV-infected person, haemophiliac, blood transfusion or blood product recipient, prostitute or sexual contact with one of these).
The patient may have had a seroconversion illness (50% of cases). Any combination of fever, lymphadenopathy, maculopapular rash, arthralgia, pharyngitis, nausea and vomiting, headache, weight loss and oral candidiasis is possible.
Careful questioning (see Questions box 41.2) about the mode of infection is important but should be left to a subsequent consultation if the patient seems reluctant to discuss this. Patients may be unwilling to inform their sexual partners that they are infected. This puts these people at risk of infection and there is a duty on the treating clinician’s part to ensure that they are informed, tested and protected (e.g. by condom use).
HIV infection is often present in combination with other sexually transmitted infections such as syphilis and gonorrhoea and with the hepatic viruses B and C. The incidence varies in different countries but hepatitis C is uncommon in Australian HIV patients.
HIV should be strongly suspected in patients who present with TB and TB should be suspected in HIV patients with a chronic respiratory illness. HIV infection has replaced TB as the great imitator of other illnesses. HIV testing should be routine in any unexplained infectious illness.
EXAMINATION
Examine the patient as follows.
General inspection
Take the patient’s temperature. The patient may appear ill and wasted due to chronic ill-health or chronic opportunistic infection. Mycobacterium avium complex (MAC) presents with fever and weight loss.
• The maculopapular rash of acute HIV infection (5- to 10-millimetre maculopapular lesions on the face and trunk and rarely on the palms and soles).
• Herpes zoster (shingles, which may involve more than one dermatome in this disease and is more commonly seen in early rather than advanced HIV infection).
• Oral herpes simplex (cold sores) or genital herpes.
• Oral and flexural candidiasis (once the CD4 level is below 200/mm3).
• Molluscum contagiosum, impetigo, seborrhoea or other nonspecific exanthems.
• Kaposi’s sarcoma: red-purple vascular non-tender tumours. These present typically on the skin but can occur anywhere.
• Skin lesions resembling Kaposi’s sarcoma may also be seen. These are called bacillary angiomatosis and are caused by Bartonella henselae and Bartonella quintana (see Figures 41.1 and 41.2).


Severe psoriasis is common in HIV patients.
Adverse drug reactions are more common in patients with HIV infection and may be the cause of a rash. Look for hyperpigmentation. Patients taking the drug clofazimine for MAC infection usually become deeply pigmented. Areas of peripheral fat atrophy—lipodystrophy—on limbs, cheeks and buttocks may be seen in 20–30% of patients treated with the protease inhibitor drugs. Some of these patients have fat redistribution with central obesity.
Hands and arms
Look for nail changes including onycholysis. Feel for the epitrochlear nodes; a node 0.5 centimetres or larger may be characteristic.8 Note any injection marks.
Face
• candidal plaques (see Figure 41.4)
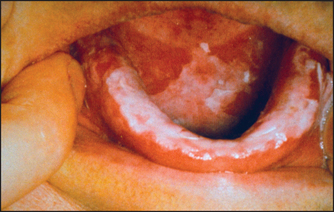
Figure 41.4 Oral candidiasis (From McDonald FS, ed. Mayo Clinic images in internal medicine, with permission. © Mayo Clinic Scientific Press and CRC Press.)
• tongue ulceration (e.g. herpes simplex, cytomegalovirus or candidal infections) or gingivitis9
Kaposi’s sarcoma (see Figure 41.3) may also occur on the hard or soft palate (in which case associated lesions are almost always present elsewhere in the gastrointestinal tract). Oral squamous cell carcinoma and non-Hodgkin’s lymphoma are more common in AIDS.

Figure 41.3 (a) Kaposi’s sarcoma in the mouth (b) Kaposi’s sarcoma on the foot ((a) From McDonald FS, ed. Mayo Clinic images in internal medicine, with permission. © Mayo Clinic Scientific Press and CRC Press; (b) Dr A Watson, Infectious Diseases Department, The Canberra Hospital.)
Parotidomegaly is sometimes seen as a result of HIV-associated Sjögren’s syndrome. These patients may have dry eyes and mouth for this reason.
Hairy leucoplakia is a unique raised or flat white, painless and often hairy-looking lesion typically present on the lateral surface of the tongue; it is caused by Epstein-Barr virus (EBV) infection in HIV-infected people and is almost diagnostic of HIV infection.
Palpate over the sinuses for tenderness (sinusitis). Examine the cervical and axillary nodes. There may be generalised lymphadenopathy, and all lymph node groups should be examined.
Chest
Note any tachypnoea or dry cough. Note chronic cough, either dry or productive of purulent sputum. On auscultation crackles may be present at the bases due to bronchiolitis obliterans. There are often, however, no chest signs despite the presence of pulmonary infiltrates on chest X-ray due to Pneumocystis jiroveci (formerly carinii) or other opportunistic infections.
Abdomen
Examine for hepatosplenomegaly (e.g. infection, lymphoma). Perform a rectal examination (e.g. perianal ulceration from herpes simplex) and a sigmoidoscopy looking for Kaposi’s sarcoma or proctitis (e.g. cytomegalovirus, herpes simplex, amoebic dysentery or pseudomembranous colitis from antibiotic use). Examine the genitals for herpes simplex, warts, discharge or chancre.
Nervous system
Look for signs of meningism (e.g. cryptococcal meningitis). There may be focal signs due to a space-occupying intracranial lesion (e.g. toxoplasmosis, non-Hodgkin’s lymphoma).
A syndrome similar to Guillain-Barré and a pure sensory neuropathy can occur. HIV infection itself, opportunistic infection or the drugs used in treatment can be responsible for peripheral sensorimotor neuropathy, polymyositis, radiculopathy, mononeuritis multiplex or a myelopathy.
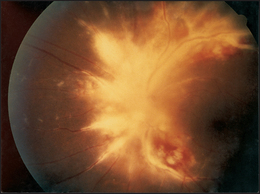
Look in the fundi for soft exudates (common in AIDS patients), scars (e.g. toxoplasmosis—see Figure 41.5) or retinitis (e.g. cytomegalovirus-induced retinitis with perivascular haemorrhages and fluffy exudates, which can cause blindness of rapid onset—see Figure 41.6).10 There may be signs of dementia (AIDS encephalopathy).
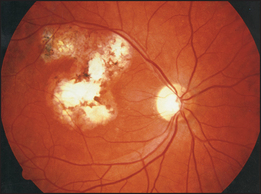
Figure 41.5 Retinal toxoplasmosis—old chorioretinal scar (Courtesy of Dr Chris Kennedy & Professor Ian Constable, Lions Eye Institute)
References
1. Hayakawa, K, Ramasamy, B, Chandrasekar, PH. Fever of unknown origin: an evidence-based review. Am J Med Sci. 2012; 344(4):307–316. [The modern approach to diagnosis still relies on the history and physical examination initially.].
2. Arbo, M, et al. Fever of nosocomial origin: etiology, risk factors and outcomes. Am J Med. 1993; 95:505–515.
3. Mourad, O, Palda, V, Detsky, AS. A comprehensive evidence-based approach to fever of unknown origin. Arch Intern Med. 2003; 163:545.
4. Coburn, B, Morris, AM, Tomlinson, G, Detsky, AS. Does this adult patient with suspected bacteremia require blood cultures. JAMA. 2012; 308(5):502–511. [Shaking chills but not fever alone suggests bacteraemia.].
5. Bates, DW, Cook, EF, Goldman, L, et al. Predicting bacteremia in hospitalized patients: a prospectively validated model. Ann Intern Med. 1990; 113:495–500.
6. American College of Physicians and Infectious Diseases Society of America. Human immunodeficiency virus (HIV) infection. Ann Intern Med. 1994; 120:310–319.
7. Nandwani, R. Human immunodeficiency virus medicine for the MRCP short cases. Br J Hosp Med. 1994; 51:353–356.
8. Malin, A, Ternouth, I, Sarbah, S. Epitrochlear nodes as marker of HIV disease in sub-Saharan Africa. BMJ. 1994; 309:1550–1551.
9. Weinert, ML, Grimes, RM, Lynch, DP. Oral manifestations of HIV infection. Ann Intern Med. 1996; 125:485–496. [Details the 16 leading oral complications, based on an extensive literature review.].
10. De Smet, MD, Nessenbatt, RB. Ocular manifestations of AIDS. JAMA. 1991; 266:3019–3022. [Provides a very good review of eye changes.].
aMoritz Kohn Kaposi (1837–1902), professor of dermatology, Vienna, described the sarcoma in 1892.