Correlation of physical signs and rheumatological disease
Rheumatoid arthritis
Rheumatoid arthritis is a chronic systemic inflammatory disease of unknown aetiology that characteristically involves the joints (see Figure 25.1). In the majority of cases, patients with rheumatoid arthritis have rheumatoid factor present in the serum (seropositive disease). These are heterogeneous antibodies directed against the Fc portion of immunoglobulin G (IgG), but are not specific for rheumatoid arthritis.
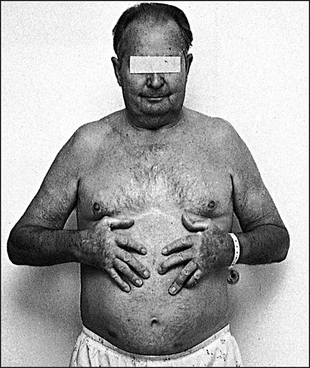

Figure 25.16 Giant cell arteritis (From Klippel JH, Dieppe PA (eds). Rheumatology, 2nd edn. Philadelphia: Mosby, 1997.)
To examine the patient with suspected rheumatoid arthritis (see Text box 25.1), sit him or her up in bed or on a chair.
GENERAL INSPECTION
Look to see whether the patient has a Cushingoid appearance due to steroid treatment (page 367), or whether there are signs of weight loss that may indicate active disease.
HANDS
Put the patient’s hands on a pillow. Look especially for symmetrical small joint synovitis (the distal interphalangeal joints are usually spared). The other common abnormalities are ulnar deviation, volar subluxation of the metacarpophalangeal joints, Z deformity of the thumb with swan necka and boutonnière deformity of the fingers. Examine the fingernails and periungual areas for splinter-like vasculitic changes and look for wasting of the small muscles of the hand. Look at the palms for palmar erythema. Feel the palms for palmar tendon crepitus while the patient extends and flexes the fingers. Look for signs of an ulnar nerve palsy (from ulnar nerve entrapment at the elbow) and a median nerve palsy (carpal tunnel).
ELBOWS
Look around the elbows for rheumatoid nodules, which suggest seropositive disease, and examine the elbow joint. Flexion contractures are common.
SHOULDERS AND AXILLAE
Examine for tenderness and limitation of movement. Also palpate the axillary nodes because enlarged nodes may indicate active disease of joints in the area that they drain.
EYES
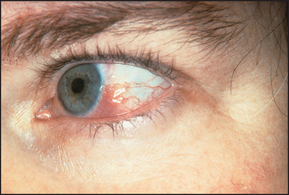
Look at the eyes for redness, which may indicate the dryness of Sjögren’s syndrome (see List 23.6), which occurs in 10%–15% of cases. Note also nodular scleritis—an elevated white or purple-red lesion, which is pathologically a rheumatoid nodule and usually appears surrounded by the intense redness of the injected sclera (see Figure 25.2). These nodules occur especially in the superior parts of the sclera and are often bilateral, but affect only 1% of patients. Iritis does not occur.
With severe scleritis, scleral thinning may occur, exposing the underlying choroid. This is called scleromalacia. Look for cataracts due to steroid treatment. Conjunctival pallor may be present, indicating anaemia due to iron deficiency. This can be a result of blood loss from non-steroidal anti-inflammatory drug use, folate deficiency from a poor diet, hypersplenism or chronic inflammation, or some combination of these.
MOUTH
Look for dryness of the mouth and dental caries (Sjögren’s syndrome), and ulcers related to drug treatment (e.g. methotrexate).
TEMPOROMANDIBULAR JOINTS
Feel the temporomandibular joints for crepitus as the patient opens and shuts the mouth.
NECK
Go on to examine the cervical spine for tenderness, muscle spasm and reduction of rotational movement. Examine for cervical lymphadenopathy.
CHEST
Now examine the lungs for signs of pleural effusions or pulmonary fibrosis. Caplan’sb syndrome is the presence of rheumatoid lung nodules in combination with pneumoconiosis.
HEART
Listen to the heart for a pericardial rub (relatively common) and for murmurs indicating valvular regurgitation (especially the aortic valve), which may occur due to nodular involvement of a heart valve.
ABDOMEN
Feel the abdomen for splenomegaly (this occurs in up to 10% of patients and suggests the possibility of Felty’s syndrome) and hepatomegaly. Feel the inguinal lymph nodes.
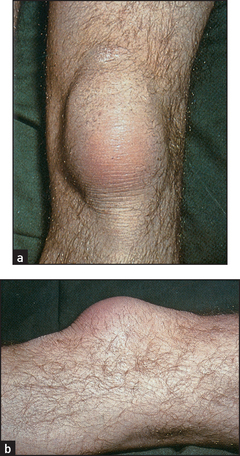
LOWER LIMBS
Examine the hips for limitation of joint movement. The knees, however, are more often affected and here one must note any quadriceps wasting (an important sign of knee arthritis), synovial effusions and flexion contractures. Valgus deformity (a result of lateral arthritic changes—osteoarthritis causes varus deformity) and ligamentous instability may occur as late complications. Look in the popliteal fossae for Baker’s cysts. Go on to look at the lower parts of the legs for ulceration; this can occur as a vasculitic complication of Felty’s syndrome. Examine for a stocking distribution peripheral neuropathy and for mononeuritis multiplex of the nerves of the lower limbs. There may also be signs of spinal cord compression due to anterior dislocation of the first cervical vertebra or vertical subluxation of the odontoid process.
ANKLES AND FEET
Now look for foot drop (peroneal nerve entrapment or vasculitis) and examine the ankle joint for limitation of movement. Look at the metatarsophalangeal joints for swelling and subluxation. There may also be lateral deviation and clawing of the toes. Remember that the interphalangeal joints are very rarely involved. Finally, feel the Achilles tendon for nodules—a sign of seropositive disease.
An assessment of the activity of the disease is an important way of assessing the adequacy of treatment and is used routinely by rheumatologists. This includes criteria such as the duration of morning stiffness, joint pain, fatigue, joint tenderness, soft-tissue swelling and the presence of extra-articular manifestations. These criteria can be found on the websites of the various rheumatological societies.
Seronegative spondyloarthritides
Four conditions are generally accepted as belonging to this group: ankylosing spondylitis, Reiter’s disease (reactive arthritis), psoriatic arthritis and enteropathic arthritis. These are called the seronegative spondyloarthritides because they were originally distinguished from rheumatoid arthritis by the absence of rheumatoid factor in the serum. However, up to 30% of patients with otherwise classical rheumatoid arthritis are rheumatoid factor negative. The seronegative spondyloarthropathies overlap clinically and pathologically, and have an association with HLA-B27.
ANKYLOSING SPONDYLITIS
The following areas should be examined.
Back and sacroiliac joints: may show loss of lumbar lordosis and thoracic kyphosis; severe flexion deformity of the lumbar spine (rare); tenderness of the lumbar vertebrae; reduction of movement of the lumbar spine in all directions; and tenderness of the sacroiliac joints. Measure the occiput to wall distance: serial measurements that show an increasing distance indicate worsening deformity. Perform Schober’s test and test for lateral movement of the spine by asking the patient to run a hand straight down the side of each leg in turn. This movement is often severely restricted.
Legs: Achilles tendinitis; plantar fasciitis; and signs of cauda equina compression (rare)—lower limb weakness, loss of sphincter control, saddle sensory loss.
Lungs: decreased chest expansion (less than 5 centimetres); signs of apical fibrosis.
Heart: signs of aortic regurgitation.
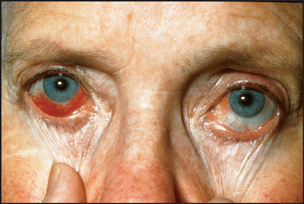
Eyes: acute iritis (tends to recur)—painful red eye (10%–15%) (see Figure 25.3).
Rectal and stool examination: signs of inflammatory bowel disease (either ulcerative colitis or Crohn’s disease). Note: signs of secondary amyloidosis—for example, hepatosplenomegaly, renal enlargement, proteinuria—may be present, although this is a very rare complication.
REACTIVE ARTHRITIS (REITER’S SYNDROME)
Classically this disease follows urethritis or diarrhoea, with conjunctivitis and arthritis (usually asymmetrical) of the large weight-bearing joints such as the hip, knee or ankle. The following areas should be examined.
Genital region: urethral discharge; circinate balanitis—scaly, superficial reddened erosions with well-demarcated borders on the glans penis (see Figure 25.4).

Eyes: conjunctivitis; iritis (rare).
Mouth: painless smooth mucosal lesions, especially of the tongue.
Back: sacroiliac joints (may be unilaterally involved).
Lower limbs (more commonly affected): knees, ankles; metatarsophalangeal joints and toes (‘sausage toes’); plantar fasciitis, Achilles tendinitis; keratoderma blennorrhagica on the sole (non-tender reddish-brown macules, which become scaling papules)—this is indistinguishable from pustular psoriasis; nails thickened, opaque and brittle.
Hands (less commonly involved): wrists; metacarpophalangeal joints, proximal interphalangeal joints, distal interphalangeal joints; keratoderma blennorrhagica on the palms; nail changes.
PSORIATIC ARTHRITIS
Some 10% of patients with psoriasis have arthritis.
Examine as for rheumatoid arthritis, but include the spine and sacroiliac joints. There are five distinct groups of psoriatic arthritis, but overlap is common:
• Monoarticular and asymmetrical oligoarticular arthritis of the hands and feet and other joints (note sausage-shaped digits in Figure 24.39—see page 325). Most psoriatic arthritis is of this type.
• Symmetrical polyarthritis, similar to rheumatoid arthritis (but seronegative).
• Distal interphalangeal joint involvement with psoriatic nail changes (see Figure 24.6 on page 303).
• Arthritis mutilans (destructive polyarthritis).
• Sacroiliitis with or without peripheral joint involvement.
Gouty arthritis
Begin with the feet, as acute gouty arthritis affects the metatarsophalangeal joint of the great toe in 75% of cases (see Figure 25.5). Next examine the ankles and knees, which tend to be involved after recurrent attacks. The fingers, wrists and elbows are affected late (see Figure 25.6). Inspect and palpate for gouty tophic (these are urate deposits with inflammatory cells surrounding them). The presence of tophi indicates chronic recurrent gout. They tend to occur over the joint synovia, the olecranon bursa (see Figure 25.7), the extensor surface of the forearm, the helix of the ear (see Figure 25.8) and in the infrapatellar and Achilles tendons.

Figure 25.5 Acute gout of first metatarsophalangeal joint (Hochberg MC. Rheumatology, 5th edn. Mosby, 2010.)



Finally, examine for signs of the causes of secondary gout: increased purine turnover due to myeloproliferative disease (page 284), lymphoma (page 286) or leukaemia; and decreased renal urate excretion due to renal disease or hypothyroidism. Hypertension, diabetes mellitus and ischaemic heart disease are more common among sufferers of gout.
Calcium pyrophosphate arthritis (pseudogout)
This may present a similar picture to that described above for true gout, but usually large joints (especially the knees) and wrists are involved. In a minority of patients there will be signs of hyperparathyroidism, haemochromatosis or true gout.
Calcium hydroxyapatite arthritis
This causes large-joint arthritis (especially knee and shoulder) and is more common in elderly patients.
Systemic lupus erythematosus
Systemic lupus erythematosus (SLE) is a multisystemic chronic inflammatory disease of unknown origin, named because the erosive nature of the condition was likened to the damage caused by a hungry wolf.d
GENERAL INSPECTION
Look for weight loss (due to chronic inflammation) or a Cushingoid appearance (steroid treatment; see Text box 25.2). While taking the history note any abnormal mental state—psychosis may occur due to the lupus itself or to steroid therapy.
TEXT BOX 25.2 Examining for SLE

Proximal myopathy (active disease or steroids)
Alopecia, with or without scarring, lupus hairs
Eyes—scleritis, cytoid lesions, etc
Cardiovascular system—pericarditis
Respiratory system—pleural effusion, pleurisy, pulmonary fibrosis, collapse or infection
Feet—red soles, small-joint synovitis
HANDS
Note any vasculitic-appearing lesions around the nail bed, or telangiectasia and erythema of the skin of the nail base. A rash may occur—photosensitivity is common. The hand rash of lupus tends to occur over the phalanges, as opposed to that of dermatomyositis, which affects the knuckles.
Raynaud’s phenomenon may occur if the weather is cold (see List 23.5 on page 294).
Examine for arthritis: synovitis of the proximal and metacarpophalangeal joints. The arthritis of SLE is not erosive, but if severe may lead to reducible deformities due to damage to supporting structures.
FOREARMS
Livedo reticularis may occur here (see Figure 25.10); in Latin this describes skin discolouration in the form of a small net. This is formed by connected bluish-purple streaks without discrete borders. They occur usually on the limbs. Livedo can occur in vasculitis and in the antiphopholipid syndromee or from atheroembolism.1 Look also for purpura (due to vasculitis2 or autoimmune thrombocytopenia). Examine for a proximal myopathy (due to the disease itself or to steroid treatment). Subcutaneous nodules very rarely occur in SLE. The axillary nodes may be enlarged but will not be tender.

HEAD AND NECK
Alopecia (hair loss) is an important diagnostic clue that occurs in about two-thirds of patients and may be associated with scarring. Look especially for lupus hairs, which are short, broken hairs above the forehead. The hair as a whole may be coarse and dry, as in hypothyroidism.
Examine the eyes for scleritis and episcleritis (more common as a manifestation of rheumatoid arthritis than SLE). The eyes may be red and dry (Sjögren’s syndrome). Pallor of the conjunctivae occurs with anaemia, usually due to chronic disease. Occasionally, jaundice due to autoimmune haemolytic anaemia may be found. Perform a fundoscopy for cytoid bodies, which are hard exudates (white spots) due to aggregates of swollen nerve fibres and are secondary to vasculitis.
A facial rash may be diagnostic (see Figure 25.11). The classical rash is an erythematous ‘butterfly rash’ over the cheeks and bridge of the nose and must be distinguished from rosacea. Mouth ulcers on the soft or hard palate may occur and the mouth may be dry (Sjögren’s syndrome).

The rash of discoid lupus may be found in the same area or affect different parts of the body. Lesions begin as spreading red plaques that have a central area of hyperkeratosis and follicular plugging. An active lesion has an oedematous edge. The appearance may suggest psoriasis. A healed lesion may have marginal hyperpigmentation with central atrophy and depigmentation. The scalp, external ear and face are most commonly affected, but in some patients lesions may occur all over the arms and chest. Extensive annular or psoriaform lesions may indicate the presence of subacute cutaneous lupus.
After examining the face, feel for cervical lymphadenopathy, which is usually non-tender.
CHEST
Signs of a pericardial rub (from pericarditis) may be found. In the respiratory examination a pleural rub (pleuritis) or signs suggesting the presence of a pleural effusion, pulmonary fibrosis, pulmonary collapse or pulmonary hypertension may be detected. Chest disease is probably most often secondary to an interstitial pneumonitis rather than to vasculitis of the lungs.
ABDOMEN
Splenomegaly, usually mild, can be detected in 10% of cases. Hepatomegaly (mild) may occur in uncomplicated cases. Chronic liver disease due to chronic hepatitis (‘lupoid hepatitis’) is a separate autoimmune disease rather than a variant of SLE.
HIPS
Examine the hip joint movements: in aseptic (avascular) necrosis there is pain on movement, with preservation of hip extension but loss of the other movements. This is due to ischaemia of the femoral head and may be related to steroid use or to the SLE itself.
LEGS
Examine for proximal myopathy and peripheral neuropathy (mainly sensory).
Rarely there may be signs of hemiplegia, cerebellar ataxia or chorea.
Leg ulceration over the malleoli, due to vasculitis or the antiphospholipid syndrome,1 is important. Very occasionally the toes may be gangrenous. There may be ankle oedema from the nephrotic syndrome or fluid retention from steroids. Livedo reticularis may be present on the legs.
Systemic sclerosis (scleroderma)
This is a disorder of connective tissue with variable cutaneous fibrosis and with abnormalities of the microvasculature of the fingers, gut, lungs, heart and kidneys. In diffuse systemic sclerosis there is more prominent skin sclerosis and these patients may have pulmonary fibrosis. In limited systemic sclerosis (CREST syndrome: Calcinosis, Raynaud’s phenomenon, o Esophageal motility disturbance, Sclerodactyly and Telangiectasia), diffuse skin sclerosis and severe interstitial lung disease do not occur but patients are at risk of developing pulmonary hypertension.
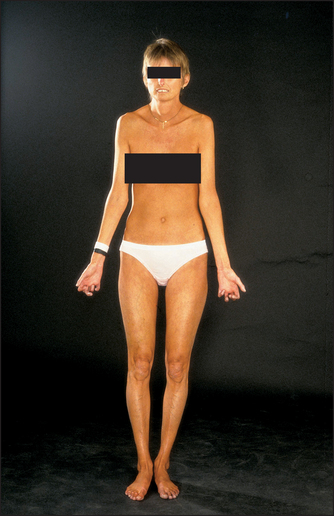
GENERAL INSPECTION
Look for cachexia due to dysphagia (from an oesophageal motility disturbance) or malabsorption (due to bacterial overgrowth; see Text box 25.3).
Skin changes in systemic sclerosis vary. There may be an early oedematous phase with non-tender pitting oedema of the hands, which appear tightly swollen. In patients with progressive disease the oedematous skin is replaced by indurated skin that appears thickened, hard and tight. This phase usually begins in the fingers (see List 25.1).
HANDS
Examine the hands. Note particularly calcinosis (palpable nodules due to calcific deposits in the subcutaneous tissue of the fingers), Raynaud’s phenomenon sometimes causing atrophy of the finger pulps (due to ischaemia; see Figure 25.13), sclerodactyly (tightening of the skin of the fingers leading to tapering) and multiple large telangiectasia on the fingers (see Figure 25.14).


Look for contraction deformity of the fingers, which is relatively common (see Figure 25.15), and for synovitis, although this is uncommon. The nails can be affected by Raynaud’s. It can be useful to inspect the nail folds using a hand-held magnifying glass: in scleroderma you may see dilated capillary loops but this is not diagnostic. These are best viewed on the fourth digit. Tendon friction rubs may be present in patients with diffuse disease and suggest an adverse prognosis. Assessing hand function is important in this disease.

ARMS
Determine the extent of skin tethering in the arms. If the skin thickening extends above the wrists to the arms, legs or trunk, the diagnosis is diffuse scleroderma rather than CREST. If the skin thickening extends only to the elbows and face, this is called limited scleroderma. Assess for proximal myopathy due to myositis.
FACE
The skin of the face is involved in progressive disease. There is loss of normal wrinkles and skin folds as well as loss of the eyebrows. The face appears pinched and expressionless (‘bird-like’ facies). Inspect for malar telangiectasia and look for salt-and-pepper pigmentation. Ask the patient to close the eyes—skin tethering may make this incomplete. The eyes may be dry (Sjögren’s syndrome), although this is uncommon, and the conjunctivae pale (there are a number of reasons for anaemia, including the presence of chronic disease, bleeding from oesophagitis, watermelon stomach and microangiopathic haemolytic anaemia).
Ask the patient to open the mouth fully. It may appear puckered and narrow. Inability to open the mouth so that there is more than 3 centimetres of clearance between the incisors indicates abnormal restriction.
Chest
Inspect the skin of the chest wall, which may have acquired a tight, thickened appearance, like ancient Roman breastplate armour.
Examine the lungs for pulmonary fibrosis, evidence of reflux pneumonitis or (rarely) a pleural effusion or alveolar cell carcinoma.
Examine the heart for cor pulmonale secondary to pulmonary fibrosis or for pericarditis. Left ventricular failure may also occur due to myocardial involvement.
URINALYSIS AND BLOOD PRESSURE
These are very important because renal involvement is common in scleroderma and is often associated with severe hypertension. Renal disease is one of the most common causes of death in scleroderma.
The stool
Look for evidence of steatorrhoea (due to malabsorption from bacterial overgrowth). A summary of the physical signs that can be found in scleroderma is presented in Text box 25.3.
Rheumatic fever
Rheumatic fever is an inflammatory disease that is a delayed sequel to infection with group A beta-haemolytic Streptococcus; it is uncommon in Western nations today. It is diagnosed by finding two major or one major and two minor criteria, plus evidence of recent streptococcal infection.
– Carditis (causing tachycardia, murmurs, cardiac failure, pericarditis)
– Chorea (page 478)
EXAMINING THE PATIENT WITH SUSPECTED RHEUMATIC FEVER
First examine the large joints of the limbs for effusions and synovitis. Two or more joints must be involved (classically there is a transient migratory polyarthritis). Feel for subcutaneous nodules over bony prominences. Look for a rash. Erythema marginatum is a slightly raised pink or red rash that blanches with pressure. The red rings have a clear centre and round margins, and occur on the trunk and proximal limbs; the rash is not found on the face. Look for choreiform movements. Their onset is usually delayed until about 3 months after the throat infection.
Now examine the cardiovascular system for any signs of pancarditis: (1) a pericardial rub due to pericarditis; (2) congestive cardiac failure due to myocarditis; (3) mitral or aortic regurgitation due to acute endocarditis.
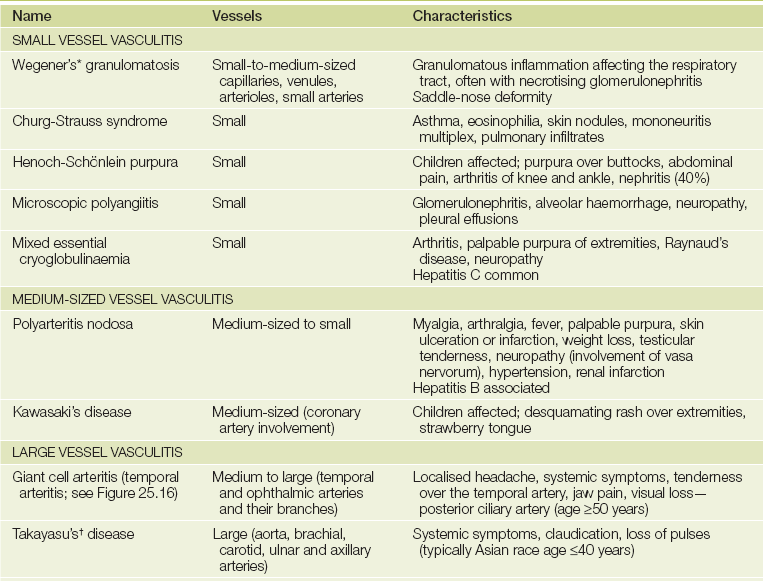
The vasculitides
This is a heterogeneous group of disorders characterised by inflammation and damage to blood vessels.2 The clinical features and major vessels involved are shown inTable 25.1.
Soft-tissue rheumatism
This includes a number of common, painful conditions that arise in soft tissue, often around a joint. The problem may be general (e.g. fibromyalgia) or restricted to a single anatomical region (e.g. tendon, tenosynovium, enthesis or bursa). There are a large number of these conditions; the more common ones are described here.
FIBROMYALGIA SYNDROME
This syndrome is a common, frequently overlooked condition that mostly affects women in their 40s and 50s. It presents with a variable group of symptoms including widespread musculoskeletal aches and pains, and usually with symptoms of chronic fatigue. The musculoskeletal pain is mostly axial (neck and back) and diffuse. It is made worse by stress or cold. Pain may be felt ‘all over’ and is unresponsive to anti-inflammatory drug treatment. The combination of pain and fatigue may cause the patient severe disability. There is usually a poor sleep pattern. The patient wakes up not feeling refreshed and more tired in the morning than later in the day. Note that no abnormal pathology has been found in the joints, muscles or tendons of these patients.
Examination
Test for the characteristic multiple hyperalgesic tender points (see Figure 25.17). These areas may be tender to finger pressure in normal people but in affected patients there is marked tenderness and a definite withdrawal response. This response should be obtained in at least 11 of 18 sites in the upper and lower limbs and on both sides (i.e. it is widespread and symmetrical). Next examine for hyperalgesia at control sites such as the forehead or distal forearm, where it should be absent.
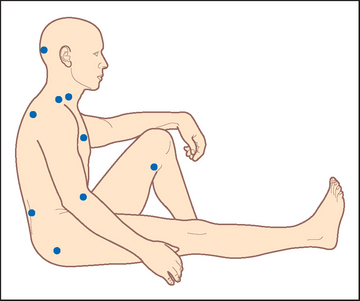
Figure 25.17 Frequent sites of localised tenderness in fibromyalgia 18 tender point sites (test bilaterally) are:
1. Insertion of suboccipital muscle
2. Under lower sternocleidomastoid muscle
3. Insertion of supraspinatus muscle
4. Trapezius muscle (mid upper)
5. Near second costochondral junction
6. 2 centimetres distal to lateral epicondyle
7. At prominence of greater trochanter
The diagnosis is based on the presence of typical symptoms and multiple hyperalgesic tender sites (with negative control sites). Inflammatory and endocrine disease must be excluded.
SHOULDER SYNDROMES
Soft-tissue disorders of the shoulder are common and have certain particular clinical features.
Rotator cuff syndrome
Supraspinatus tendinitis is the most common form of rotator cuff syndrome. It is associated with degeneration and subsequent inflammation in the supraspinatus tendon as it is compressed between the acromion and humeral head when the arm is raised. It mostly affects 40- to 50-year-olds. Symptoms may begin following unaccustomed physical activities such as gardening.
Examination
Examine the shoulder joint. Note pain on abduction of the arm (see Figure 25.18), with a painful arc of movement between 60 and 120° of abduction. Involvement of other rotator cuff tendons causes similar painful movement. Biceps tendinitis is present in the majority of patients with a rotator cuff syndrome. Yergason’sf sign for biceps tendinitis is helpful (LR+ 2.8).3 The patient flexes the elbow to 90° and pronates the wrist. Hold the patient’s wrists and try to prevent the patient’s attempts to supinate the forearm. Inflammation of the head of the biceps causes pain in the shoulder since this muscle is the main supinator of the forearm.
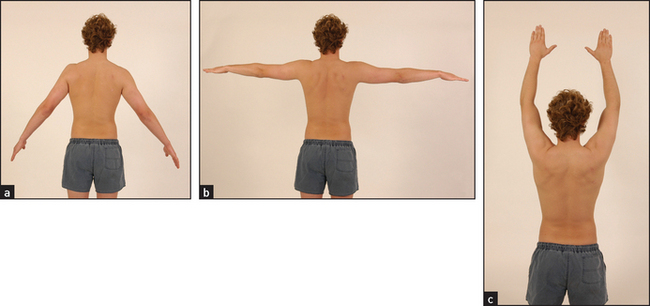
Figure 25.18 Inflammation of the rotator cuff tendons may cause a ‘painful arc’ during abduction of the arm The initial movement (a) is painless but the next 90° of movement (b) causes pain. When the arm reaches full abduction (c) the pain eases as the pressure is taken off the rotator cuff apparatus. (Courtesy of Glenn McCulloch)
Frozen shoulder
Capsulitis of the shoulder, or frozen shoulder, is associated with limitation of active and passive arm movements in all directions. It may follow immobilisation of the arm after a stroke. There is typically a sudden onset of shoulder pain, which is worse at night and radiates to the base of the neck and down the arm. Pain is made worse by shoulder movement and may be bilateral. Pain and stiffness usually subside over a period of months. Complete movement may not be regained.
ELBOW EPICONDYLITIS (TENNIS AND GOLFER’S ELBOW)
Many contact and non-contact sports can cause physical injury, although serious injuries are rather uncommon with certain sports (e.g. synchronised swimming). There may be pain over the epicondyles of the elbow. The lateral epicondyle is the most often affected and is called ‘tennis elbow’. Pain arises from the site of insertion of the extensor muscle tendons into the lateral epicondyle (enthesis). Involvement of the medial epicondyle at the site of insertion of the flexor tendons of the forearm causes medial epicondylitis—‘golfer’s elbow’. These conditions are also common in manual workers such as painters.
Examination
Examine for local tenderness over the lateral (see Figure 25.19) or medial epicondyle (see Figure 25.20). Ask the patient to extend the fingers against resistance (see Figure 25.21). This will make the pain of lateral epicondylitis worse. Ask the patient to flex the fingers against resistance. This will exacerbate the pain of medial epicondylitis.

Figure 25.19 Examination of the elbow Looking for signs of lateral epicondylitis. Palpation over the forearm extensor muscle origin elicits pain. Straining the muscles by resisted extension of the wrist exacerbates the symptoms. (Courtesy of Glenn McCulloch)


TENOSYNOVITIS OF THE WRIST
Inflammation of the synovial tubes in which tendons run can occur in patients with rheumatoid arthritis but also in otherwise healthy people. The cause is often unaccustomed repetitive movement. A common site for tenosynovitis is at the wrist, where it involves the long extensor and abductor tendons of the thumb (de Quervain’s tenosynovitis; see Figure 25.22).

Figure 25.22 A patient with de Quervain’s tenosynovitis There is characteristic swelling of the tendon sheath of the abductor pollicis brevis over the styloid process of the radius.
Examination
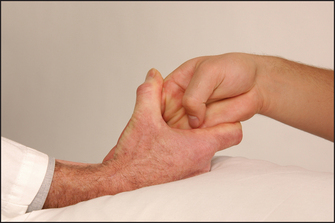
This reveals tenderness and swelling on the radial side of the wrist (radial styloid). There is pain on active or passive movement of the thumb. Confirm the diagnosis by performing Finkelstein’sg test. Hold the patient’s hand with the thumb tucked into the palm and then quickly turn the wrist into full ulnar deviation (see Figure 25.23). An alternative approach that is reported to produce fewer false-positives involves gripping the patient’s thumb rather than tucking the thumb into the palm.4 Sharp pain will occur in the tendon sheath when the test is positive. Also examine the other common sites of tendon involvement: the flexor tendons of the fingers and the Achilles tendon.
BURSITIS
Bursae are found in areas exposed to mechanical strain or trauma, either at the site where muscle or tendon glides over bone or muscle, or superficially where bony prominences are exposed to mechanical stress. Bursitis usually occurs as a local soft-tissue inflammatory reaction to unusual mechanical pressure. It may be associated with rheumatoid arthritis, gout or sepsis. Common sites include the prepatellar area (housemaid’s knee; see Figure 25.24), over the olecranon (olecranon bursitis) and over the greater trochanter (trochanteric bursitis; often actually a tendinitis).
Nerve entrapment syndromes
Nerve entrapment syndromes are caused by compression of peripheral nerves at vulnerable sites and are associated with pain, paraesthesias and numbness in a particular nerve distribution.
CARPAL TUNNEL SYNDROME
Compression of the median nerve at the wrist is the most frequent form. This seems hardly surprising when one remembers that the carpal tunnel, sandwiched between the carpal bones and the carpal ligament, contains 9 flexor tendons as well as the median nerve. These patients complain of numbness, pain and paraesthesias in the median nerve distribution (the 3 radial fingers and the radial side of the ring finger). It can be a sign of early rheumatoid arthritis. Symptoms often wake patients from sleep and may radiate up the forearm (one-third of cases) and involve the fourth and fifth fingers and wrist but not the palm or dorsum of the hand—classic pattern. If the palms are involved the pattern is called probable. The most common cause is an overuse tenosynovitis of the flexor tendon sheaths at the wrist. Fluid retention during pregnancy or from use of the oral contraceptive pill can also produce carpal tunnel symptoms. In addition, median nerve compression can occur in rheumatoid arthritis, hypothyroidism, acromegaly and amyloidosis.
Examination
Symptoms can be reproduced by gentle percussion over the carpal tunnel (which begins at the distal wrist crease) while the wrist is held in extension (Tinel’s sign—LR+ 1.8; LR– 0.8). This sign is negative in up to 30% of patients with electrophysiologically proven median nerve compression. Prolonged (60 seconds) passive wrist flexion (Phalen’s test) has a lower false-negative rate (LR+ 1.3, LR– 0.7).3 Ask the patient: ‘What do you do with your hands when the feeling is there?’ The flick sign is positive when the patient demonstrates a flicking movement with the wrist as if shaking a non-electronic thermometer (LR+ 29; LR– 0.1—but only in one study5). Look for wasting in the median nerve distribution and loss of motor (thenar muscle strength: weak thumb abduction) and sensory function (sensation over the thenar eminence, however, is usually preserved). These signs occur only in advanced cases.
MERALGIAh PARAESTHETICA
Compression of the lateral cutaneous nerve of the thigh causes paraesthesias and sensory loss over the lateral side of the thigh. This entirely sensory nerve passes through the lateral part of the inguinal ligament only just medial to the anterior superior iliac spine. Here it is subject to compression in patients who are obese, wear tight or heavy belts or spend long periods sitting. Diabetes, pregnancy and trauma can also be causes of problems with the nerve.
TARSAL TUNNEL SYNDROME
This may be caused by compression of the posterior tibial nerve in its fibro-osseous canal formed by the flexor retinaculum and the tarsal bones. Symptoms include burning pain and paraesthesias in the toe, sole and heel. Patients are often woken with pain at night and, as with the carpal tunnel syndrome, this may radiate upwards. Walking may improve the symptoms. Causes include diabetes, synovitis from rheumatoid arthritis, bony deformity and flexor tenosynovitis. Hypertrophy of the abductor hallucis muscle, which occurs in intemperate runners, is an occasional cause.
MORTON’S ‘NEUROMA’
This is caused by compression of one or more of the interdigital plantar nerves by the transverse metatarsal ligament. Patients complain of a burning pain or ache that extends distally from the affected web space to the toes (most often the third and fourth).
Metatarsalgia is a non-localised ache that spreads across the forefoot involving the area of some or all of the metatarsal heads. It can occur in normal feet after prolonged standing but also occurs in a number of other foot conditions (see List 25.2), and is often associated with poor-fitting shoes. Morton’s metatarsalgia is interdigital nerve entrapment (usually between the third and fourth metatarsal bones). Patients describe burning pain between the metatarsal bones and may have numbness on the adjacent toes. They get relief by removing their shoes and massaging their foot.
References
1. Grob, JJ, Bonerandi, JJ. Cutaneous manifestations associated with the presence of the lupus-anticoagulant. J Am Acad Dermatol. 1986; 15:211–219. [Antiphospholipid antibody syndrome can be associated with leg ulcers (that resemble pyoderma gangrenosum), livedo reticularis and fingertip ischaemia.].
2. Stevens, GL, Adelman, HM, Wallach, PM. Palpable purpura: an algorithmic approach. Am Fam Phys. 1995; 52:1355–1362.
3. McGee, S. Evidence-based clinical diagnosis, 3rd edn. Philadelphia: Saunders, 2012.
4. Elliott, BG. Finkelstein’s test: a descriptive error that can produce a false-positive. J Hand Surg Br. 1992; 17:481–482. [Careful explanation of the performance of this test (which is often misunderstood) appears in this article. Movement with the thumb folded into the hand can produce a false-positive result.].
5. Pryse-Phillips, WE. Validation of a diagnostic sign in the diagnosis of carpal tunnel syndrome signs. J Neurol Neurosurg Psychiatry. 1984; 47(8):870–872.
aThe appearance resembles a swan dipping its head into the water.
bAnthony Caplan, Welsh physician, described this in 1953.
cFrom the Latin tophus, which means ‘chalk stone’.
dFrom the Latin lupus, which means ‘wolf’. Lupus has been used as a name for any erosive disease of the skin; for example, lupus vulgaris is tuberculosis of the skin.
eAntiphospholipid syndrome refers to venous or arterial thrombosis or spontaneous miscarriages in the presence of antiphospholipid antibodies (lupus anticoagulant, anticardiolipin) on testing; half have SLE.
fRobert Mosely Yergason (1885–1949), American surgeon, described this sign in 1931.
gHarry Finkelstein (1865–1939), surgeon, Hospital for Joint Diseases, New York.
hThe Greek word meros means ‘thigh’ and algia means ‘painful’.