Chapter 14 Knowledge generation and clinical reasoning in practice
Health professionals have a responsibility to contribute to the development of their profession’s knowledge base and to continually expand and critique the knowledge used in practice (Higgs & Titchen 2000). Practitioners need to be able to critically appreciate knowledge, generate knowledge from practice and recognize the practice epistemology that underpins their practice.
To commence our own critical appreciation of knowledge, we define it as follows:
Knowledge is a dynamic and context-bound phenomenon that utilizes language to construct meaning. Language serves as a tool for thinking, learning and making meaning (Vygotsky 1986, Wittgenstein 1958) (see Chapter 31). Knowledge is constructed in the framework of sociopolitical, cultural and historical contexts. Practice knowledge evolves within a dynamic ‘history of ideas’ (see Berlin 1979, Lovejoy 1940) contained in the particular practice domain and within the history of how ideas born in that practice domain have shaped and been shaped by that practice (Higgs et al 2001).
Each of these dimensions and contexts of knowledge has particular relevance to how we use knowledge in reasoning and generate knowledge from within reasoning. During professional socialization, practitioners learn the ways of being, acting, thinking and communicating that characterize their profession.
PRACTICE EPISTEMOLOGY
In Chapter 3 the importance of practitioners knowing and choosing their practice models was argued. In this chapter we extend this argument to the understanding and adoption of a position relating to practice epistemology. To say that ‘this is the epistemological position that underpins my practice’ is to recognize that my practice is carried out within the context of a certain discursive tradition (a scientific and professional community in this case) of knowledge generation. This tradition, with its rules and norms of practice, determines what constitutes knowledge and what strategies of knowledge generation are valid. Within the biomedical practice framework (or model), for example, with its inherent physical sciences epistemological stance, knowledge is seen as an objective, predictive, empirical, generalizable, explanatory phenomenon that arises from the use of the natural scientific method and theorization in a world of external objective reality. In humanistic, psychosocial practice models, located in the human and social sciences and the arts, knowledge is seen as being interpretive, theoretical, and constructed in social worlds that recognize and seek to interpret multiple constructed realities. In emancipatory practice models, located in the critical social sciences, knowledge is recognized as being historically and culturally constructed, and historical reality is something that, once understood more deeply, can be changed in order to seek positive changes in practice.
We begin our reflections on this topic in acknowledgement of the position that knowledge and practice are inseparable (see Fish & Coles 1998, Higgs et al 2001, Ryle 1949). Indeed professional practice, with clinical reasoning at its core, could be viewed as knowing in practice. And professional knowledge should be considered not as a repository of knowledge of the discipline combined with the individual practitioner’s store of knowledge, but rather as a practice of knowing within the broader field of professional practice. Thus the knowing and the doing of practice are concurrent, intertwined journeys of being and becoming in practice.
APPRECIATING PRACTICE AND PRACTICE KNOWLEDGE
To appreciate something involves sensing, becoming aware of, understanding and valuing it. Critical appreciation is a process of examining and seeking to understand an activity or an object by as many means and from as many points of view as possible. This incorporates:
This process can lead the ‘appreciator’ away from the specific activity or object under review, towards a view of the bigger picture surrounding it (Fish 2001).
Critical appreciation and professional judgement have much in common. Professional judgement can focus on the product of clinical reasoning, that is, the decisions or judgements made in clinical practice; this is comparable to the evaluation made by connoisseurs (Eisner 1985) who use critical appreciation to make judgements about their field of expertise (e.g. art). The processes of clinical reasoning and critical appreciation both involve using discretionary judgement and self-evaluation (Freidson 1994, 2001). This process of self-critique also applies to the continual refinement and updating of practitioners’ knowledge bases. They are expected to seek out the best and most salient knowledge available to deal with practice tasks and problems and to recognize when their knowledge is deficient, redundant or irrelevant. In such cases they need to pursue further learning, reflect on practice to generate experience-based knowledge, and seek out other people’s knowledge (including that of their clients) as input to professional decision making.
Part of appreciating practice knowledge is recognizing that what counts as knowledge is a matter of perspective. The dominant view of knowledge in Western society and in the health professions is the largely unquestioned view of knowledge from the physical sciences or empirico-analytical paradigm. This is the ‘hypothetico-deductive’ approach, in which knowledge generation is viewed not as a process of creation of knowledge but as a process of discovery of empirical ‘facts’ about the (physical) world/universe. Knowledge in this view is an account or a theory of what is ‘out there’; it represents or mirrors aspects of the natural world. This is the epistemology of representationalism, the notion that theories (and language) represent nature rather than the notion developed here, that theories are created in the context of human activity. In critique of this positivist epistemology (the idea that scientific propositions are given to the senses by nature itself), the British philosopher Karl Popper (1959, 1970) argued that the discovery of scientific fact begins by a process of theoretical conjecture, not, as the positivists would argue, through objective or empirical observation. From this conjunction arise testable or ‘falsifiable’ hypotheses. Thus in epistemological terms, science follows a process or method involving disproof, not proof. One cannot speak about truth in the traditional sense, that a hypothesis matches reality precisely or perfectly, but rather that empirical research has not yet proved the hypothesis incorrect. Theories that have withstood the strictures of empirical testing or experimentation give scientists a degree of certainty and confidence about them. While seeking the truth, such research actually generates knowledge or a truth that is currently undisproved by testing through observation or experimentation.
As scholars, educational practitioners and researchers we support a constructionist interpretation of knowledge according to which all knowledge is a construction of human beings (individuals or groups) who are striving to know about nature and experience. This view of knowledge involves an appreciation of knowledge as a sociohistorical political construct and recognition of the value of different forms of knowledge for different communities and contexts. We are socialized (in life, education and work) to value different forms of knowledge, often unquestioningly accepting the values and expectations of these social groups. Vygotsky (1978) referred to this process of acquiring knowledge as ‘internalization of activity’, and Rogoff (1995) used the term ‘participatory appropriation’ to emphasize the dynamic, relational and mutual nature of learning. This differs from a perspective of learning that implies pieces of knowledge being transferred from the outside to the inside of the individual.
New knowledge can be challenging in that it requires appreciation (evaluating, critique and valuing). This process of appreciation requires us to question previous values and entails a new thematic understanding of previously implicit ways of seeing and understanding. It is a dynamic process, where individuals are placed in the position of critics who do not blindly accept what their professional leaders or experts espouse, but actively question and interpret it in light of their own previous and current experience. They may in fact reject the new or emerging knowledge and suggest alternatives. Given the dynamic nature of contexts, not only can the circumstances that surround knowledge use, creation and acknowledgement change, but the knower’s frame of reference (including knowledge needs, values and knowledge abilities) might also change. All these changes impact on professional practice and must be internalized by both new learners and skilled practitioners. Much of this change may well occur around us, even in some instances without our initial explicit awareness, but it can also arise from continuous reflection on our practice.
EMPLOYING, CREATING AND MODIFYING KNOWLEDGE IN PRACTICE
In this section our goal is to explore strategies through which knowledge can come to be appreciated, generated, validated and valued. Employing existing or learned knowledge in practice is not simply a matter of transferring this knowledge to a new setting. This process customarily requires modification, particularly because knowledge generated through research or by theorists is inevitably generalized, and does not always meet the needs of the particular practice in the field. The knowledge generated by others does not always fit the perceived needs of a particular practitioner who may seek to deconstruct and reconstruct formal theory in terms that make it more intelligible and user-friendly. In practice, not only are propositional and non-propositional knowledge modified for and through practice, but they are also combined, extended, converted from one form to another and, most importantly, particularized (see Fish & de Cossart 2007, Montgomery 2006). For example, in designing a healthcare plan for a particular patient the practitioner adapts general research knowledge to suit that patient’s unique combination of life and health circumstances, drawing on experience-based knowledge from working with other similar situations.
The practice setting is a vital arena for the construction of new knowledge by practitioners themselves. First, professional judgement is utilized by practitioners in the selection of knowledge to be used and the kind of use to which that knowledge is put in the practice setting. Here, practitioners consider what is appropriate knowledge, how it might be used and whether it should be modified to suit the particular case. That modification is itself a version of creating knowledge in practice. Second, new knowledge may be created in the practice setting, when practitioners identify the need to develop new procedures or when they face new challenges. Evidence-based practice can exist only insofar as relevant evidence exists and is known by practitioners (Beeston & Simons 1996, Ford & Walsh 1994, Grahame-Smith 1995, Jones & Higgs 2000, White 1997). Further, it is important to recognize that for practitioners to use evidence in their practice it needs to be appropriated internally by them, an internalization that occurs when the evidence is seen to have relevance for their practice. In practical settings, professionals are continually adapting both formal public knowledge and their own informal knowledge to particular cases, or they are extending existing knowledge in response to the current case. Third, and perhaps most significantly, knowledge is created by practitioners in the practice setting when they theorize about their practice and make explicit and refine the tacit knowledge that lies embedded within and beneath their actions, activities and know-how.
In Figure 14.1 we attempt to illustrate a loosely sequenced series of activities which can be included in the process of making sense of the world of practice in order to produce knowledge. This is not intended to represent an empirical observation or generalization of knowledge generation in a prescriptive or predictive sense; neither is it a set of rules for generating knowledge. Rather, we propose that these interactive, reflexive, cognitive and communicative processes and actions can usefully contribute to knowledge development. The sequence commences with the formulation of ideas and proceeds through a deepening understanding of the phenomenon or reality that the thinker is seeking to appreciate. The next phase involves evaluative and critiquing processes which can result in a level of certainty that can be called conviction or validation of the truth, at which point the notion is judged to reflect reality satisfactorily. This allows or prompts the knower to release this knowledge claim for public critique. The cycle then progresses through critique by others and by the field, so that the knowledge claims become part of the accepted knowledge base of the group/profession/society. These phases are detailed below.
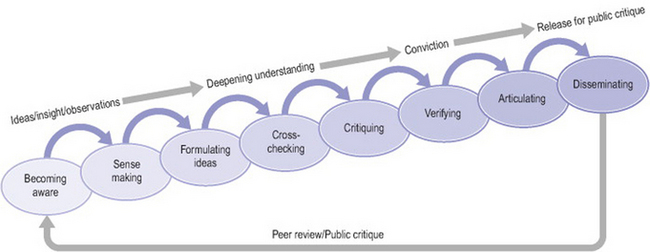
Figure 14.1 Appreciating practice knowledge
from Higgs et al 2004, with permission of Butterworth-Heinemann
FORMULATING IDEAS
Healthcare practitioners are expected to notice things; to become aware of their patients’ needs and responses. They are expected to critically appraise their own performance, role and actions. In so doing they can become aware of patterns of behaviour and outcomes in their clinical interventions. For example, they can reflect on the relative effectiveness and patient preference for different modes of treatment and the circumstances surrounding these findings. Fish (1998) has argued that this processing of noticing with heightened awareness and a learned habit requires the development of a ‘discerning eye’. For many practitioners, this awareness may be channelled directly into their clinical role, almost without conscious recognition. That is, they may acquire a large store of mainly tacit knowledge and experience.
Tacit knowledge plays an important role in practice. According to Heidegger (1926/1990), craft activity (involving a form of tacit knowledge) must remain tacit to work well and is brought to awareness only when the practitioner makes a mistake. This mistake then focuses the practitioner’s attention; the activity becomes explicit; the correction is made consciously (or thematically, to use Heidegger’s term) and practice knowledge is realized. Heidegger would argue that craft work must operate on a tacit basis, otherwise it ceases to become craft work and is articulated into a set of guidelines.
However, we argue that tacit knowledge can also be made explicit by practitioners deliberately reflecting upon the underlying elements of their practice in order to understand it, communicate it to other practitioners and teach it to students. In the context of healthcare practice, which blends science, art and craft, the wholeness and at times the essence of the artistry or craft of practice cannot be articulated. However, there is much about practice that needs to be further explored and can be made explicit. In particular, experience-based knowledge gained by one practitioner could greatly enhance the practice of others if it were presented to, validated and adopted by the profession. This requires articulation. Thus we distinguish between ‘unspeakable’ tacit knowledge, which is deeply embedded in the actions of practice, and the vast amount of procedural knowledge that awaits exploration. This exploration can occur when an appropriate exploration tool is identified, when an opportunity or stimulus (such as a critical incident) occurs to prompt reflection, or when health professionals take the time to explore and critique their practice. In their recent book Developing the Wise Doctor, Fish & de Cossart (2007) introduce the term ‘the invisibles of practice’ to refer to key elements of practice which are tacit (but can be made explicit) or are implicit (lying just beneath the surface of human endeavour, but can be easily made explicit when prompted). Their book offers a range of resources for developing clinicians’ understanding of these invisible dimensions of practice.
The act of noticing in practice is the first step to making practice epistemology an ingrained practice of practitioners as well as of researchers. The goal is to make paying attention to how knowledge is used in practice and created through practice a living part of practice. Noticing, however, as with the other knowledge generation actions discussed below, should not be just the actions of the isolated practitioner. Each of these actions should become part of professional education and socialization; they are part of working and being in a learning community and of a profession with both a tradition of knowledge-making and a future of knowledge evolution.
Practitioners often explore their existing knowledge base when seeking to make sense of a new idea, an insight, an observed pattern or inconsistency. They look at the compatibility of the new idea with existing knowledge, the value of the new idea, patterns emerging across a number of cases or situations, and whether the new idea is unique to the particular situation. And they challenge their existing knowledge to see what needs to be replaced or updated. Self-questioning and reflection play a major role here in appreciating the subtleties of a situation and developing understandings and explanations.
CROSS-CHECKING AND CRITIQUING
New ideas, variations, techniques and strategies are often explored and tested out in practice. Such active experimentation is part of creating new knowledge and cross-checking emerging knowledge. Checking may also take the form of self-debate, with the new idea or potential intervention strategy being analysed, deconstructed, examined from multiple perspectives to further the process of refining and testing it in terms of credibility, coherence, relevance, etc. The issue of the compatibility of new knowledge with practitioners’ existing knowledge is a critical factor in clinical effectiveness and the development of practitioners’ knowledge bases. In clinical reasoning, practitioners often need to deal with and make sense of differences between new knowledge and existing propositional and experience-based knowledge. Conflicts between such forms of knowledge could be due to the presence of existing knowledge that is obsolete, inadequate, incomplete, erroneous or irrelevant to the given situation, or there could be a problem with the new knowledge (e.g. lack of relevance or validity). There can also be some aspects of health care that remain irreconcilable, and practitioners need to be able to make professional judgements to deal with such situations rather than developing a clear knowledge position.
In critiquing emerging knowledge claims, practitioners need to address the relevance, credibility and currency of this potential knowledge for their practice. They can perform this critique against internal yardsticks, that is, their existing knowledge base and their capacity to scrutinize knowledge claims against first principles (using scientific knowledge and theory). They can also compare emerging knowledge against the knowledge of their field through literature reviews, systematic reviews and so on. And they can trial the knowledge claims during clinical reasoning in relation to real and hypothetical cases.
In relation to practical knowledge practitioners could ask, for example: Can my knowledge of biomechanics, anatomy or physiology help to explain why a newly invented treatment technique or variation should work? What could be the possible consequences of taking this course of action? How does this new approach sit with the professional knowledge base and the literature pertaining to evidence-based practice? If I use this knowledge or technique in my practice, do my self-knowledge and my knowledge of ethics, culture and professional standards create ease of use or difficulties?
Beyond the immediate questioning of emerging knowledge claims, this process of generating knowledge from practice addresses further questions. On one hand there is a seeking after some truth (or matching with reality), but there is also a critique of the rightness, justification and compatibility with self and others in the use of this knowledge in practice. To critique includes dealing with issues of relevance and appropriateness for the setting (e.g. individual client, culture, professional role). In addition, at a ‘meta’ level, we advocate an exploration of the nature of knowledge and its generation in the context of the particular practice arena, that is, practice epistemology. Is this knowledge or just an idea or observation? Can I verify it? Does this knowledge claim stand the test of scrutiny against my own and my profession’s way of being in our practice world and our way of knowing about this world?
VERIFYING
Verification of claims to knowledge requires rigour and conviction. Rigour in knowledge generation is both an intention (to seek truth or a truth) and an approach (including providing transparency of method to facilitate critique, being systematic and thorough in testing truth with open-mindedness in the pursuit of clarity and truthfulness). Yet the nature of the rigour is also dependent upon the knowledge tradition being utilized. In the positivist tradition, the requirement for rigour arises from the goal of the research, to generalize from its findings. Here, rigour is manifest in strict adherence to rules of the scientific method (e.g. objectivity, reliability and validity) and to the protocols of experimental research (e.g. random allocation of subjects, use of blind trials, measurement of statistical significance).
In keeping with the aim of the professional artist to generate meaning, confer significance or offer insight rather than to develop propositional knowledge, the major means of collecting evidence in the connoisseurship model is the practitioner through whom the meaning is developed and expressed (see Eisner 1981). And, just as the piece of art itself is the place from which art critics draw their evidence, so the arena in which practitioners seek evidence is the practice arena. Eisner also emphasized the importance of the connoisseur approach as a way of communicating meaning in a manner that is understandable to the relevant community. If no one but the connoisseur can recognize the description, it will not be regarded as a competent interpretation.
Rigour associated with the expertise of critical appreciation (the processes, language and form) develops within the context of a critical community, as argued by Schön (1983), who proposed that the professional knowledge by which practitioners ‘make sense of practice situations, formulate goals and directions for action, and determine what constitutes acceptable professional conduct’ is ‘embedded within the socially and institutionally constructed context shared by a community of practitioners’ (p. 33). Beyond individual critique and metacognitive scrutiny, rigour is achieved by peer critique through validating knowledge by exposing it to the professional community (as discussed below).
To be convinced that a claim to knowledge has been verified, knowers need to have reached a point where they believe that the evidence accumulated is sufficient to judge the claim to be acceptable or true. Thus conviction is a decision and a judgement rather than a point of absolute certainty. Ayer (1956 p. 222) argued that when seeking to verify knowledge claims we should take scepticism of these claims seriously. Such scepticism will enable us to learn ‘to distinguish the different levels at which our claims to knowledge stand’. Thus, knowing is a continual process of generating, refining and understanding knowledge.
ARTICULATING
One of the most difficult challenges in knowledge generation is to articulate knowledge clearly, in a form and language meaningful to the people (within and outside the health professions) who use that knowledge. In health care this is likely to include professional practitioners and their clients, and thus different forms of expression are needed to take account of different levels of medical knowledge and different language and cultural backgrounds.
Articulation (oral and written) of new practice knowledge can include definitions, explanations, illustrations, examples and arguments. Writing and dialogue play major roles in shaping, refining and communicating new knowledge. Such processes place the knowledge in the context of the practice community, hold the emerging ideas up against the challenge of existing knowledge and look at the resonance of the language and ideas with existing discourse. Writing is a process of making meaning as well as presenting meaning. Meaning emerges from the writing just as an artefact emerges from the work of the artist. The process of writing (or making meaning) takes the originator beyond what was planned and what was known at the beginning. Writing enables writers to discover what they really think, understand and want to say. And because the evolution of new knowledge emerges through a series of drafts, which seek to capture complex ideas in order to refine them, the oral tradition does not provide a sufficient basis for developing professional practice (see Fish 1998).
DISSEMINATING AND PEER REVIEWING
Practice knowledge varies across different health professions and within individual professions as they work with specific client groups or within specific contexts of care (Beeston & Higgs 2001). In this way knowledge and practice norms and traditions are social entities which emerge from practice and are shared by communities of practitioners. Krefting (1991) argued that the rigour of peer review by professional communities is concerned with credibility and transferability rather than with validity. The credibility of practice knowledge ‘requires that others in the community of practice find the meaning that is expressed to be credible in terms of the traditions of practice, and that they find it can be transferred to their own practice and applied in other contexts’ (Beeston & Higgs 2001, p. 114).
Many strategies are used to disseminate knowledge in professional communities, including conference presentations, journal articles and other publications, educational programmes and informal communications. As part of presenting the new knowledge to the field to allow for wider consideration and investigation, articulation of the knowledge should also include description of how it was generated and in what context, so that the knowledge claim can be critiqued.
ONGOING DEVELOPMENT
Ongoing development of knowledge is part of the search for truth in a changing world, recognizing that it is a dynamic phenomenon. Kleinig (1982, p. 152), for instance, argued that ‘the knowing subject must continually reflect on and test what [knowledge] is presented’. Practitioners need to develop an appreciation of the credibility of their knowledge, to be able to defend their knowledge, but at the same time to acknowledge that much of the range and depth of their knowledge has conditional certainty in terms of contextual relevance and durability.
Thus, knowledge claims developed by individuals or groups need to be critiqued and validated in the field in practice settings. At the simplest level this involves identifying whether the knowledge informs practice and is compatible with practice demands and tasks. However, the empirical improvement in patient outcomes as a result of utilizing this new knowledge is only part of the equation. Another important element of the validation of the new knowledge in the practice setting involves a critical appreciation of the professional practice within which the new knowledge is being activated. Appreciating practice (see Fish 1998, pp. 205–206) involves:
Understanding and developing practice, from the practitioners’ perspective, is a matter not of looking at practice via theory, but of working from within practice itself to enquire into practice (Eraut 1994, Fish 1998, Fish & Coles 1998). This allows new knowledge to be used, critiqued and refined in the practice context and may result in the identification of deeper understanding of professional practice itself.
Generating experience-based knowledge is one way of creating knowledge out of practice. Research is another. We are not talking here of research done out of the context of practice, but rather research that begins with an insight or observation arising from practice, or research that is conducted as part of practice or within the practice setting and, above all, research that serves the goal of enhancing practice.
The starting point of practice-based research can be a recognition that experience-based knowledge does indeed count as knowledge, that it arises from observation and awareness of experience (including professional practice) and that it undergoes a process of testing and verification, as discussed above, that can be just as rigorous as other research (experimental, phenomenological and critical). The second valuable realization is that this knowledge is different in source and process of generation and is different in kind (non-propositional) from research-generated (propositional) knowledge. Thirdly, it is valuable to recognize that both these forms of knowledge can often benefit from translation into the other form. For instance, the starting point of research could be professional craft knowledge of effective treatments; post-research this becomes empirically tested, generalized knowledge with claims of population applicability. Conversely, generalized knowledge for a broad and criterion-referenced population can be translated through the practice application and testing of skilled practitioners to become particularized, context-rich professional craft knowledge suitable for unique individuals or within population complex subgroups.
There is a particular need, whether by generating experience-based knowledge in practice or by researching practice wisdom, to take the professional craft knowledge of experienced practitioners, particularly their implicit and tacit knowledge, and seek to understand, test and share this knowledge for the enhancement of practice, education and patient outcomes. After the identification of dimensions of practice, particularly of expert practice, empirical research may then be used to test the efficacy of that knowledge more broadly across a range of practitioners and settings. Through this testing process, the professional craft knowledge of individuals can be transformed into propositional knowledge of the profession. It is then ready to be reconsidered by practitioners themselves. In this way the ongoing spiral of the development and use of knowledge in professional practice continues.
CONCLUSION
Practitioners who explore their own practice are an important starting point in the generation of new practice knowledge. They are a vital and primary source of evidence about clinical knowing and thinking, and they provide the key means of sharing and refining new visions of practice. For this reason the professional development of practitioners is vital to the welfare of patients and the progress of the profession. Being part of a professional group requires this attention to expanding one’s own as well as the profession’s knowledge base.
Ayer AJ. The problem of knowledge. London: Penguin, 1956.
Beeston S, Higgs J. Professional practice: artistry and connoisseurship. In: Higgs J, Titchen A, editors. Practice knowledge and expertise in the health professions. Oxford: Butterworth-Heinemann; 2001:108-117.
Beeston S, Simons H. Physiotherapy practice: practitioners’ perspectives. Physiotherapy Theory and Practice. 1996;12:231-242.
Berlin I, editor. Against the current: essays in the history of ideas. London: Hogarth Press. 1979.
Eisner E. On the differences between scientific and artistic approaches to qualitative research. Educational Reader. 1981;April:5-9.
Eisner EW. The art of educational evaluation: a personal view. London: Falmer Press, 1985.
Eraut M. Developing professional knowledge and competence. London: Falmer Press, 1994.
Fish D. Appreciating practice in the caring professions: refocusing professional development and practitioner research. Oxford: Butterworth-Heinemann, 1998.
Fish D. Mentoring and the artistry of professional practice. Mentoring in the new millennium: a selection of papers from the Second British Council Regional Mentor Conference, April 2000. Cluj-Napocca, Romania, Editura Napocca Star. 2001:11-26.
Fish D, Coles C, editors. Developing professional judgement in health care: learning through the critical appreciation of practice. Oxford: Butterworth-Heinemann. 1998.
Fish D, de Cossart L. Developing the wise doctor. London: Royal Society of Medicine Press, 2007.
Ford P, Walsh M. New rituals for old: nursing through the looking glass. Oxford: Butterworth-Heinemann, 1994.
Freidson E. Professionalism reborn: theory, prophesy and policy. Cambridge: Polity Press, 1994.
Freidson E. Professionalism: the third logic. Cambridge: Polity Press, 2001.
Grahame-Smith D. Evidence-based medicine: Socratic dissent. British Medical Journal. 1995;310:1126-1127.
Heidegger M. Macquarie J, Robinson E, editors. Being and time. Oxford: Basil Blackwell. 1926/1990.
Higgs J, Titchen A. Knowledge and reasoning. In: Higgs J, Jones M, editors. Clinical reasoning in the health professions. 2nd edn. Oxford: Butterworth-Heinemann; 2000:23-32.
Higgs J, Titchen A, Neville V. Professional practice and knowledge. In: Higgs J, Titchen A, editors. Practice knowledge and expertise in the health professions. Oxford: Butterworth-Heinemann; 2001:3-9.
Higgs J, Fish D, Rothwell R. Practice knowledge – critical appreciation. In: Higgs J, Richardson B, Abrandt Dahlgren M, editors. Developing practice knowledge for health professionals. Oxford: Butterworth-Heinemann; 2004:89-105.
Jones M, Higgs J. Will evidence-based practice take the reasoning out of practice? In: Higgs J, Jones M, editors. Clinical reasoning in the health professions. 2nd edn. Oxford: Butterworth-Heinemann; 2000:307-315.
Kleinig J. Philosophical issues in education. London: Routledge, 1982.
Krefting L. The culture concept in the everyday practice of occupational and physical therapy. Physical and Occupational Therapy in Pediatrics. 1991;11(4):1-16.
Lovejoy AO. Reflections on the history of ideas. Journal of the History of Ideas. 1940;1(1):3-23.
Montgomery K. How doctors think: clinical judgement and the practice of medicine. Oxford: Oxford University Press, 2006.
Popper K. The logic of scientific discovery. Cambridge: Cambridge University Press, 1959.
Popper KR. Normal science and its dangers. In: Lakatos I, Musgrave A, editors. Criticism and the growth of knowledge. New York: Cambridge University Press; 1970:51-58.
Rogoff B. Observing socio-cultural activity on three planes: participatory appropriation, guided participation, and apprenticeship. In: Wertsch JV, editor. Socio-cultural studies of mind. Cambridge: Cambridge University Press; 1995:139-164.
Ryle G. The concept of mind. Harmondsworth: Penguin, 1949.
Schön DA. The reflective practitioner: how professionals think in action. New York: Basic Books, 1983.
Vygotsky LS. Mind in society: the development of higher psychological processes. Cambridge, MA: Harvard University Press, 1978.
Vygotsky LS. Kozulin A, editor. Thought and language. Cambridge, MA: MIT Press. 1986. [originally published 1962]
White S. Evidence-based practice and nursing: The new panacea? British Journal of Nursing. 1997;6:175-178.
Wittgenstein L. 3rd edn. Anscombe GEM, editor. Philosophical investigations. Upper Saddle River, NJ: Prentice Hall. 1958. [originally published 1953]