Chapter 22 Clinical reasoning in physiotherapy
INTRODUCTION
This chapter has undergone significant revision since the last edition of this book. We have retained the overview of clinical reasoning in physiotherapy being hypothesis-oriented and collaborative, along with discussion of key factors within the therapist influencing clinical reasoning. To this we have added discussion of the biopsychosocially oriented World Health Organization (WHO) framework of health and disability (WHO 2001) that depicts the scope of knowledge, skills and clinical reasoning focus physiotherapists must have. We present a biopsychosocial, collaborative hypothesis-oriented model of clinical reasoning in practice along with the notion of dialectical reasoning strategies, and a framework of different hypothesis categories that can operate within that model. We contend that these reasoning tools can assist therapists’ application of biopsychosocial theory to practise in the spirit of the WHO framework and provide quality patient-centred physiotherapy services.
SITUATING PHYSIOTHERAPISTS’ CLINICAL REASONING WITHIN A BROADER FRAMEWORK OF HEALTH AND DISABILITY
Whether working with patients having musculoskeletal/sports, neurological, oncological or cardiorespiratory problems from infants through to old age, or working in health promotion/injury prevention, physiotherapists must consider all factors potentially contributing to a person’s health. Although physiotherapists are often perceived as having a focus on the ‘physical’, contemporary biopsychosocial understanding of health and disability (Borrell-Carrió et al 2004) requires that any attention to a patient’s physical health include full consideration of environmental and psychosocial factors that may influence physical health, within the scope and limits of the therapists’ education. This requires a holistic philosophy of health and disability, assessment and management knowledge (including referral pathways) and skills for all potential contributing factors. In addition, clinical reasoning proficiency is required to recognize whether these potential contributing factors are relevant to the individual patient, in order to make appropriate clinical judgements that will contribute to the patient’s optimal health care.
The WHO has published a ‘family’ of international classifications to guide health services, such as the International Classification of Functioning, Disability and Health (ICF) (WHO 2001). The ICF provides a standardized language and framework to facilitate communication about health and health care across professional disciplines and sciences. The ICF is based on a WHO framework of health and disability (Figure 22.1) that portrays a person’s functioning and disability as outcomes of interactions between health conditions and contextual factors (both environmental and personal). ‘Functioning’ refers to all body functions, activities (a person’s executions of tasks) and participation (a person’s involvement in life situations such as work, family, leisure). ‘Disability’ is another umbrella term, referring to impairments in body function and structure, activity limitations and participation restrictions.
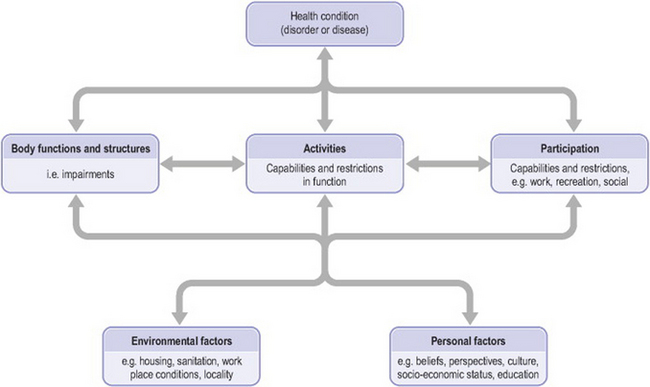
Figure 22.1 Framework of health and disability (adapted from ‘Interactions between the components of ICF’, World Health Organization 2001, p 18, with permission)
Thus patients’ health conditions can be seen to both influence and be influenced by their body functions and structures (or physical status), their capacity and performance of functional activities of life, and their subsequent ability to participate in their family, work and leisure roles. People’s physical status, activities, participation and health condition can be positively or negatively influenced by a variety of factors, including environmental factors (e.g. social attitudes, architectural characteristics, legal and social structures, climate, terrain) and personal factors (e.g. gender, age, psychological features such as thoughts/beliefs, feelings and coping styles, health and illness behaviours, social circumstances, education, past and current experiences). This framework provides an excellent contextualization for physiotherapy practice.
THE CLINICAL REASONING PROCESS IN PHYSIOTHERAPY: HYPOTHESIS-ORIENTED AND COLLABORATIVE
Understanding the clinical reasoning underlying a physiotherapist’s assessment and management of a patient requires consideration of the thinking process of the therapist, the patient and the shared decision making between the two. Figure 22.2 presents a biopsychosocial model of clinical reasoning as a collaborative process between physiotherapists and patients (Edwards & Jones 1995). In all physiotherapy settings, the physiotherapist’s reasoning begins with the initial data/cues obtained (e.g. referral, observation of the patient). This preliminary information will evoke a range of impressions or working interpretations. While typically not thought of as such, they can be considered hypotheses in the sense that these initial interpretations are not fixed, final decisions. Instead, they are considered against subsequent information (data) obtained that may support or not support the initial impressions. Although this is similar to a process of hypothesis testing, depending on their education, not all therapists will be cognisant of this process, or indeed of their reasoning in general. Hypothesis generation involves a combination of specific data interpretations or inductions and the synthesis of multiple clues or deductions. In most settings the initial hypotheses are quite broad, for example in an outpatient setting: ‘looks like a back or hip problem’. Initial hypotheses may be physical, psychological or socially related, with or without a ‘diagnostic’ implication.
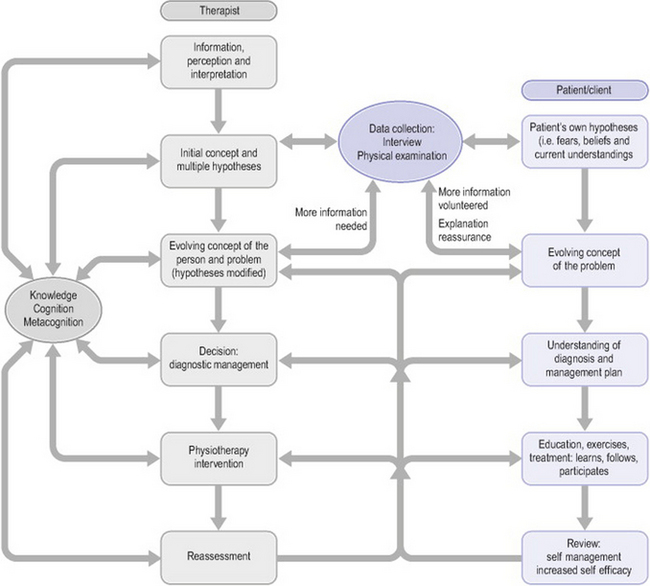
Figure 22.2 Biopsychosocial model of clinical reasoning as a collaborative process between physiotherapists and patients (adapted from Edwards & Jones 1995, with permission)
All physiotherapists have an element of routine to their examination. Through professional education and clinical experience, they will have identified the categories of information which they have found to be particularly useful for problem identification and management decisions (e.g. environmental information along with subjective and physical features of the patient’s physical impairments such as site, behaviour and history of symptoms, specific tests of function, structure and cognition). Beyond these routines, specific inquiries and tests are tailored to each patient’s unique presentation. Initial hypotheses lead to certain inquiries and tests specific to each patient. This cognitive activity of ‘hypothesis testing’ ideally includes the search for both supporting and negating evidence. The resulting data are then interpreted for their fit with previously obtained data and hypotheses considered. Even routine inquiries, tests and spontaneous information offered by the patient will be interpreted in the context of initial hypotheses. In this way the physiotherapist acquires an evolving understanding of the patient and the patient’s problem. Initial hypotheses will be modified and new hypotheses considered. This hypothesis generation and testing process continues until sufficient information is obtained to make a physiotherapy diagnosis regarding the physical and psychosocial presentation, appropriateness of physiotherapy and/or additional health professional referral, and the physiotherapy management that will be trialled.
The clinical reasoning process continues throughout ongoing patient management. Re-assessment either provides support for the hypotheses and chosen course of action or signals the need for hypothesis modification/generation or further data collection and problem clarification (e.g. additional physiotherapy examination or referral for other specialist consultation). Within a treatment session, therapists are constantly reading patient responses to guide their clinical decisions and reviewing treatment outcomes to test management hypotheses.
Equally important to the therapist’s thinking are patients’ thoughts about their problems, as reflected in the boxes on the right side of Figure 22.2. That is, patients begin their encounter with a physiotherapist with their own ideas of the nature of their problem, as shaped by personal experience and advice from medical practitioners, family and friends. Patients’ understanding of their clinical problem has been shown to impact on their levels of pain tolerance, disability and eventual outcome (Flor & Turk 2006, Jones & Edwards 2006). Patients’ beliefs and feelings which are counterproductive to their management and recovery can contribute to lack of involvement in the management process, poor self-efficacy and, ultimately, to a poor outcome. Conversely, patients who have been given an opportunity to share in the decision making have been shown to take greater responsibility for their own management and to have a greater likelihood of achieving better outcomes (Edwards et al 2004b). Patients’ self-efficacy and the responsibility they take for their management can be maximized through a collaborative reasoning process with their therapists.
Through a process of evaluating patients’ understanding of and feelings about their problems, through explanation, reassurance and shared decision making, patient and therapist jointly develop an evolving understanding of the problem and its management. Responsibility is shared between patient and therapist, with the patient taking an active role in the management.
Patient learning (i.e. altered understanding and improved health behaviour) is a primary outcome sought in the collaborative reasoning approach. When the patient is recognized as a source of knowledge for the therapist, reflective therapists will also learn from the collaborative experience. That is, when patients are given the opportunity to tell their story rather than simply answer questions, reflective therapists, who attend to individual patient presentations noting features that appear to be linked (such as increased stress affecting one patient’s symptoms but not another’s), will learn the variety of ways in which patients’ health, cognition, behaviour, movement and pain can interact. And just as patients can be taught to problem-solve to recognize various physical and psychological stressors, therapists must continually reflect on their working hypotheses and the effects of their interventions to ‘validate’ their clinical patterns and procedural knowledge.
KEY FACTORS INFLUENCING CLINICAL REASONING
Clinical reasoning is influenced by factors relating to the specific task, the setting, the patient or client and the decision maker. For purposes of this discussion, we highlight certain critical aspects of those factors pertaining to the decision maker. The box to the left in Figure 22.2 highlights the strong relationship of the clinician’s knowledge, cognition and metacognition within the process of clinical reasoning. Double-headed arrows are used to convey that these factors influence all aspects of the clinical reasoning process and in turn are strengthened by clinical reasoning experience, particularly when clinicians think or reflect about what they do during and after a clinical encounter.
KNOWLEDGE
Clinical reasoning requires rich organization of a wide range of knowledge including scientific and professional theory, procedural know-how and personal philosophy of practice, values and ethics. The importance of knowledge to physiotherapists’ clinical reasoning is highlighted in Jensen’s expertise research, in which expert physiotherapists were seen to possess a broad, multidimensional knowledge base acquired through professional education and reflective practice where both patients and colleagues were valued as sources of learning (Jensen et al 2000). Physiotherapists utilize various forms of knowledge in their clinical reasoning including propositional (‘knowing that’) and non-propositional (‘knowing how’) knowledge (see Higgs & Titchen 2000, and Chapter 11). Identifying the use of these different types of knowledge in clinical practice reflects the tension between clinical reasoning that is focused on the clinical aspect of patient care and that kind of decision making that is identified in the current imperative for practitioners to serve as moral agents in assisting patients to negotiate the demands of increasingly complex healthcare systems (Nelson 2005).
COGNITIVE AND METACOGNITIVE SKILLS
Along with the different forms of knowledge associated with decision making, cognitive skills (e.g. data analysis and synthesis and inquiry strategies) and metacognitive skills (self-awareness and reflection) are key factors influencing physiotherapists’ clinical reasoning. Physiotherapists must be able to identify and solve problems in ambiguous or uncertain situations.
Therapists’ analysis of patients’ presentations occurs at varying levels of complexity. Single bits of information that are perceived as potentially relevant (e.g. patients’ description of symptoms, activity or participation restrictions, or understanding and expectations) must be understood in their own right, often requiring further clarification and ‘validation’ with the patient. Then, at a higher level of complexity, separate bits of information must be synthesized into a larger analysis of their meaning. In this way the addition of new information often alters a previous working interpretation. For example, on its own, tenderness to palpation and pain with physical testing may implicate specific somatic tissues. However, when these findings are considered alongside a long history of impairments and disability with what appear to be significant influences from psychosocial factors, the same physical signs may warrant an alternative interpretation such as central sensitization-induced mechanical hyperalgesia (Meyer et al 2006).
This synthesis of patient information is a form of pattern recognition. In both everyday life and in physiotherapy practice, knowledge is stored in our memory in chunks or patterns that facilitate more efficient communication and thinking (Anderson 1990, Rumelhart & Ortony 1977, Schön 1983). These patterns are prototypes in memory of frequently experienced situations that individuals use to recognize and interpret other situations. In physiotherapy, patterns exist not only in classic diagnostic syndromes and associated management strategies, but also in the pathobiological mechanisms associated with those syndromes and the multitude of environmental, physical, psychological, social and cultural factors that contribute to the development and maintenance of patients’ problems. Physiotherapists must be able to recognize patterns of biomedical factors that contraindicate physiotherapy as clinical ‘red flags’ suggesting the presence of potentially serious organic pathology (Roberts 2000) and a range of psychosocial factors (conceptualized by the notion of yellow, blue and black flags (Kendall et al 1997, Main & Burton 2000, Main et al 2000)) that may predispose to chronic pain, prolonged loss of work and serve as potential obstacles to recovery.
Pattern recognition is required to generate hypotheses, and hypothesis testing provides the means by which those patterns are refined, proved reliable and new patterns are learned (Barrows & Feltovich 1987). Although expert therapists are able to function largely via pattern recognition, novices who lack sufficient knowledge and experience to recognize clinical patterns will rely on the slower hypothesis-testing approach to work through a problem. However, when confronted with a complex, unfamiliar problem, experts, like novices, will rely more on the hypothesis-oriented method of clinical reasoning (Barrows & Feltovich 1987, Patel & Groen 1991).
Physiotherapists are constantly faced with alternative choices of assessment, interpretation, and management action, the decisions about which may relate to their ability to synthesize the multitude of information obtained about a patient’s presentation and the weighting they have given (consciously or unconsciously) to the various findings. Since therapists’ cognition (perceptions, interpretations, synthesis and weighting of information) is directly related to their knowledge, faulty knowledge or personal biases and habits of practice can lead to errors in reasoning. Similarly, despite pattern recognition being a mode of thinking used by experts in all professions of life (Schön 1983), it also represents perhaps the greatest source of errors in our thinking (see Chapter 1).
METACOGNITION
Learning and being able to recognize common clinical patterns and their variations while minimizing the risks and limitations of pattern recognition requires metacognition. Metacognition, or reflective self-awareness, allows clinicians to monitor their data collection, clinical reasoning and clinical performance, also taking into account any knowledge limitations including their broader societal and cultural beliefs and values that, along with propositional and craft knowledge, underpin their practice.
Clinical reasoning models such as the one described here need further investigation to establish their validity in relation to actual practice, and to identify how clinical reasoning differs between expert (highly effective and efficient managers of patient problems) and non-expert clinicians. Although this biopsychosocial, collaborative, hypothesis-oriented model of clinical reasoning has not been formally evaluated, research in physiotherapy expertise does support key features of this model.
Key attributes of expert physiotherapists as identified by Jensen and colleagues (1992, 1999, 2000, 2006) and Resnik & Jensen (2003) that support explicit or implicit features of our model include the following:
FACILITATING THE APPLICATION OF BIOPSYCHOSOCIAL PRACTICE
Although many therapists will be familiar with our biopsychosocial model as illustrated in Figure 22.1, they may still struggle to apply this model in practice. Familiarity with the different clinical reasoning strategies and categories of decisions required may assist therapists in their application of the biopsychosocial model.
CLINICAL REASONING STRATEGIES IN PHYSIOTHERAPY
In a qualitative research study of clinical reasoning in physiotherapy, Edwards and colleagues (Edwards 2001, Edwards et al 2004a) identified patterns of clinical reasoning in expert physiotherapists in three different fields of physiotherapy (musculoskeletal, neurological and domiciliary care). They found that individual expert therapists in all three fields employed a similar range of clinical reasoning strategies, despite the differing emphases of their diagnostic and management strategies across the three settings. These clinical reasoning strategies were associated with a range of diverse clinical actions. They corresponded with various conceptions of clinical reasoning that have been identified by research, by theoretical proposition or by an exposition of the relevant skills in the literature of medicine, nursing, occupational therapy and physiotherapy.
These approaches are: diagnostic or procedural reasoning (Elstein et al 1978, Fleming 1991); interactive reasoning (Fleming 1991); conditional or predictive reasoning (Fleming 1991, Hagedorn 1996); narrative reasoning (Benner et al 1992, Mattingly 1991); ethical reasoning (Barnitt & Partridge 1997, Gordon et al 1994, Neuhaus 1988); teaching as reasoning (Sluijs 1991); and collaborative decision making (Beeston & Simons 1996, Jensen et al 1999, Mattingly & Hayes Fleming 1994).
DIAGNOSIS AND MANAGEMENT
Clinical reasoning strategies can be grouped broadly under ‘diagnosis’ and ‘management’.
Diagnosis
Management
Edwards et al (2004a) found that expert physiotherapists used different processes of clinical reasoning, albeit in an often tacit manner, within each of the reasoning strategies. These processes express different forms of decision making and clinical action. Adopting the terminology of Mezirow’s transformative learning theory (1991), Edwards et al (2004b) termed these different clinical reasoning and decision-making processes ‘instrumental’ and ‘communicative’ (see also Edwards et al 2004a, 2006). These terms also refer to the actions that result from two key forms of decision making: narrative and hypothetico-deductive reasoning.
These two forms of decision making and action are underpinned by different assumptions about knowledge and reality. Table 22.1 illustrates how these different assumptions are related in broad terms to quantitative and qualitative paradigms of research. The assumptions underlying quantitative research are also those underlying diagnostic (hypothetico-deductive) reasoning which are also those underlying the biomedical model of health care. Consider the diagnostic process in medicine where phenomena such as body temperature, blood pressure and blood counts are measured and the results analysed as deviations from an expected or normal value. As part of their physical examination, physiotherapists also quantify, measure and grade against normal values such aspects as muscle strength, ligament laxity or integrity and joint range of movement. Physiotherapists also compare the extent of any deviation between the affected and unaffected sides of the body.
Table 22.1 Assumptions underlying research paradigms, reasoning processes and decision making
| Knowledge generation | Quantitative | Qualitative |
|---|---|---|
| Research paradigm | Scientific/experimental | Interpretive |
| Positivist | ||
| Underlying assumptions about truth/reality | Objective | Context-dependent |
| Measurable | Socially constructed | |
| Predictable | Multiple realities | |
| Generalizable | ||
| Reasoning processes | Hypothetico-deductive or diagnostic | Narrative |
| Forms of decision making and management | Instrumental | Communicative |
The assumptions underlying diagnostic reasoning – namely that reality, truth and/or knowledge are best understood in an objective, measurable, generalizable and predictable framework – are very suited to the assessment and analysis of physical impairments. However, involving the language of ‘normality’ and ‘abnormality’ as they do, these assumptions are less suited to reasoning focused on understanding the interpretation of illness or disability experience (Mattingly 1991) and the influence of those interpretations on such biological phenomena as movement (Edwards et al 2006). In the literature concerned with disability there is an emphasis on the social construction of disability (e.g. Imrie 2004, Johnson 1993, Werner 1998). That is, the ‘construction’ of disability has its genesis as much in the disabling effects of attitudes towards and beliefs about disabled persons, which exclude and marginalize them from participation in mainstream activities and roles in societies, as in the cumulative functional effects of their physical impairment(s). Hence, in Table 22.1, it can be seen that two of the important underlying assumptions of narrative reasoning (and the interpretive paradigm) are that reality is socially constructed and context-dependent (Higgs & Titchen 2000).
We contend that in every action of clinical practice physiotherapists can reason, make decisions and choose management strategies, using these two fundamentally different processes (with their contrasting underlying assumptions) in an intentional manner. With the increasing incidence of chronic conditions, it is becoming more imperative that physiotherapists are able to reason clinically in a manner that reflects understanding of both ‘impairment’ and ‘disability’ (WHO 2001) and the complexity of mind–body interaction (Edwards et al 2006). The two forms of reasoning and action are therefore intrinsically linked and should not be dichotomized or separated. The relationship between two fundamentally different forms of reasoning is also termed a dialectical model of reasoning and is further described in Edwards & Jones (2007).
HYPOTHESIS CATEGORIES
If clinical reasoning strategies can help in the organization of clinical reasoning for the various tasks in clinical practice, it is also important to consider how the clinical knowledge generated in and belonging to each of these settings is organized and thus made more explicit and accessible. There are implications for the teaching of students and inexperienced practitioners alike in each setting. Identification and organization of such knowledge would provide a framework through which experts in each field can share their clinical knowledge and insights, clinical patterns can be questioned and new patterns can be learned.
This question of the way in which specialty knowledge is organized has been addressed in the area of manual physiotherapy, where a set of hypothesis categories was introduced by Jones in 1987 (Jones 1987). Since that time the specific categories considered important and the terminology used to describe them have continued to evolve (Jones & Rivett 2004) to the most recent form (Box 22.1).
Box 22.1 Hypothesis categories
Proposed categories of physiotherapists’ judgments to assist their understanding and decision making regarding the patient as a person and their problem(s):
Some evidence is available to support these categories, demonstrating that therapists generate and test diagnostic and management hypotheses throughout their encounters with patients (Doody & McAteer 2002, Rivett & Higgs 1997). Also, anecdotal evidence from experienced physiotherapists and clinical educators has supported the relevance and use of these particular hypothesis categories across all areas of physiotherapy practice, with some variation in emphasis between therapists working in neurological, paediatric and domiciliary care settings compared to outpatient musculoskeletal and sports physiotherapy. We are not recommending these particular hypothesis categories for universal use, rather they are proposed as a useful means of assisting therapists to consider their clinical decisions. Whatever categories are used should be continually reviewed to ensure that they reflect contemporary practice.
Clinical reasoning and decision making across the different hypothesis categories occur simultaneously or with varying emphasis, depending on the context and nature of the clinical situation and problems encountered. That is, therapists recognize patient cues which in turn elicit hypotheses in one or more categories. Clinical patterns exist within all the hypothesis categories. As patient cues emerge and specific hypotheses are considered, the hypotheses should be tested for the remaining features of the pattern through further patient inquiry, physical tests and ultimately with the physiotherapy intervention.
We recommend that these categories be considered within broader conceptualizations of health and disability such as the WHO model (see Figure 22.1). In this way such hypothesis categories can assist therapists to relate the various components of the WHO model to the particular clinical decisions required in practice.
CONCLUSION
As experienced clinical educators of undergraduate and postgraduate physiotherapy students and practising clinicians, we have observed that understanding of clinical reasoning and conceptual models encourages therapists’ conscious reflection about health, disability and the focus of reasoning and decision making that can be taken. In particular, we have found it beneficial to use and teach clinical reasoning in the context of the WHO framework described above, our biopsychosocial, collaborative reasoning model, the notion of dialectical reasoning strategies, and the framework of different hypothesis categories. Collectively, these reflections and improved understandings should assist therapists’ understanding of their patients and their patients’ problems so that the most effective course of management can be pursued.
Regardless of any theoretical or working conceptual models which may be elaborated to explain or teach clinical reasoning, clinical reasoning without self-monitoring and reflection on the part of the therapist is sterile. That is, assessment and treatment ‘rules’ and procedures may be followed correctly but remain unfruitful. This impasse is especially likely to occur in complex or ambiguous patient presentations that comprise ‘the swampy lowland … (where) confusing problems defy technical solution’ which Schön (1987, p. 3) described. These are precisely the indeterminate situations in which the experience and insights of experienced, senior and expert clinicians are often called upon.
To grow in expertise, professionals need self-monitoring skills in order to plan, control and evaluate problem-solving knowledge and methods (Hassebrock et al 1993), while reflection is critical if practitioners are to learn from experience. Whereas some clinicians learn little or nothing from their experience, instead relying on literature and continuing education to acquire new information, others continually revise and expand their clinical knowledge through their reflective approach to patient care.
In this chapter we have presented the WHO (2001) framework of health and disability as a means of highlighting the scope of knowledge, the skills and the clinical reasoning focus that physiotherapists must have in order to apply biopsychosocial theory to practice. This is particularly important in a profession such as physiotherapy, where clinicians are personally (physically, professionally, emotionally and socially) involved in the treatment of their patients. Therapists must attend to and search for cues, both diagnostic (suggesting source and cause of the patient’s impairment and disability) and non-diagnostic (suggesting psychological, social and cultural aspects of the patient’s problem), in order to arrive at management decisions that address holistically all relevant aspects of the individual’s health and, as far as possible, the context in which that health or illness is experienced. Physiotherapists’ clinical reasoning is portrayed as hypothesis-oriented and collaborative, requiring diverse and well-organized knowledge with good cognitive and metacognitive skills to facilitate the application and continual critique and revision of all forms of knowledge. Clinical reasoning strategies and hypothesis categories have been presented as valuable tools and approaches that can assist physiotherapists’ application of biopsychosocial theory to practice. Although awareness and understanding of one’s clinical reasoning is not essential to clinical practice, it is our view that by promoting awareness, reflection and critical appraisal, clinical reasoning can be enhanced.
Anderson JR. Cognitive psychology and its implications, 3rd edn. New York: Freeman, 1990.
Barnitt R, Partridge C. Ethical reasoning in physical therapy and occupational therapy. Physiotherapy Research International. 1997;2:178-194.
Barrows HS, Feltovich PJ. The clinical reasoning process. Medical Education. 1987;21:86-91.
Beeston S, Simons H. Physiotherapy practice: practitioners’ perspectives. Physiotherapy Theory and Practice. 1996;12:231-242.
Benner P, Tanner C, Chesla C. From beginner to expert: gaining a differentiated clinical world in critical care nursing. Advances in Nursing Science. 1992;14:13-28.
Borrell-Carrió F, Suchman AL, Epstein RM. The biopsychosocial model 25 years later: principles, practice, and scientific inquiry. Annals of Family Medicine. 2004;2(6):576-582.
Doody C, McAteer M. Clinical reasoning of expert and novice physiotherapists in an outpatient orthopaedic setting. Physiotherapy. 2002;88(5):258-268.
Edwards I. Clinical reasoning in three different fields of physiotherapy: a qualitative study. Australian Digitized Theses Program, 2001. Online. Available www.library.unisa.edu.au/adt-root/ 18 Nov 2005
Edwards IC, Jones MA. Collaborative reasoning. In: Unpublished paper submitted in partial fulfilment of the Graduate Diploma in Orthopaedics. Adelaide: University of South Australia; 1995.
Edwards I, Jones M. Clinical reasoning and expertise. In: Jensen GM, Gwyer J, Hack LM, Shepard KF, editors. Expertise in physical therapy practice. 2nd edn. Boston: Elsevier; 2007:192-213.
Edwards I, Jones M, Carr J, et al. Clinical reasoning strategies in physical therapy. Physical Therapy. 2004;84(4):312-335.
Edwards I, Jones MA, Higgs J, et al. What is collaborative reasoning? Advances in Physical Therapy. 2004;6:70-83.
Edwards I, Jones MA, Hillier S. The interpretation of experience and its relationship to body movement: a clinical reasoning perspective. Manual Therapy. 2006;11:2-10.
Elstein AS, Shulman LS, Sprafka SA. Medical problem solving: an analysis of clinical reasoning. Cambridge, MA: Harvard University Press, 1978.
Fleming MH. The therapist with the three track mind. American Journal of Occupational Therapy. 1991;45:1007-1014.
Flor H, Turk DC. Cognitive and learning aspects. In: McMahon S, Koltzenburg M, editors. Wall and Melzack’s textbook of pain. 5th edn. Philadelphia: Elsevier; 2006:241-258.
Gordon M, Murphy CP, Candee D, et al. Clinical judgement: an integrated model. Advances in Nursing Science. 1994;16:55-70.
Hagedorn R. Clinical decision making in familiar cases: a model of the process and implications for practice. British Journal of Occupational Therapy. 1996;59:217-222.
Hassebrock F, Johnson PE, Bullemer P, et al. When less is more: representation and selective memory in expert problem solving. American Journal of Psychology. 1993;106:155-189.
Higgs J, Titchen A. Knowledge and reasoning. In: Higgs J, Jones M, editors. Clinical reasoning in the health professions. 2nd edn. Oxford: Butterworth-Heinemann; 2000:23-32.
Imrie R. Demystifying disability: a review of the International Classification of Functioning, Disability and Health. Sociology of Health and Illness. 2004;26(3):287-305.
Jensen GM, Shepard KF, Hack LM. Attribute dimensions that distinguish master and novice physical therapy clinicians in orthopedic settings. Physical Therapy. 1992;72:711-722.
Jensen GM, Gwyer J, Hack LM, et al. Expertise in physical therapy practice. Boston: Butterworth-Heinemann, 1999.
Jensen GM, Gwyer J, Shepard KF, et al. Expert practice in physical therapy. Physical Therapy. 2000;80(1):28-43.
Jensen GM, Gwyer J, Hack LM, et al. Expertise in physical therapy practice, 2nd edn. St Louis: Saunders-Elsevier, 2006.
Johnson R. ‘Attitudes just don’t hang in the air…’: disabled people’s perceptions of physiotherapists. Physiotherapy. 1993;79:619-626.
Jones MA. The clinical reasoning process in manipulative therapy. In: Dalziel BA, Snowsill JC, editors. Proceedings of the Fifth Biennial Conference of the Manipulative Therapists Association of Australia. Melbourne: Manipulative Therapists Association of Australia; 1987:62-69.
Jones MA, Edwards I. Learning to facilitate change in cognition and behaviour. In: Gifford L, editor. Topical issues in pain 5. Falmouth: CNS Press; 2006:273-310.
Jones MA, Rivett DA. Introduction to clinical reasoning. In: Jones MA, Rivett DA, editors. Clinical reasoning for manual therapists. Edinburgh: Butterworth Heinemann; 2004:3-24.
Kendall NAS, Linton SJ, Main CJ. Guide to assessing psychosocial yellow flags in acute low back pain: risk factors for long term disability and work loss. New Zealand: Accident Rehabilitation and Compensation Insurance Corporation of New Zealand and the National Health Committee, Wellington, 1997.
Main CJ, Burton AK. Economic and occupational influences on pain and disability. In: Main CJ, Spanswick CC, editors. Pain management: an interdisciplinary approach. Edinburgh: Churchill Livingstone; 2000:63-87.
Main CJ, Spanswick CC, Watson P. The nature of disability. In: Main CJ, Spanswick CC, editors. Pain management: an interdisciplinary approach. Edinburgh: Churchill Livingstone; 2000:89-106.
Mattingly C. The narrative nature of clinical reasoning. American Journal of Occupational Therapy. 1991;45:998-1005.
Mattingly C, Fleming M Hayes. Clinical reasoning: forms of inquiry in a therapeutic practice. Philadelphia: F A Davis, 1994.
Meyer RA, Ringkamp M, Campbell JN, et al. Peripheral mechanisms of cutaneous nociception. In: McMahon S, Koltzenburg M, editors. Wall and Melzack’s textbook of pain. 5th edn. Philadelphia: Elsevier; 2006:3-34.
Mezirow J. Transformative dimensions of adult learning. San Francisco: Jossey-Bass, 1991.
Nelson L. Professional responsibility and advocacy for access: a case study in lymphedema services in Vermont. In: Purtilo R, Jensen GM, Brasic Royeen C, editors. Educating for moral action: a sourcebook in health and rehabilitation ethics. Philadelphia: F A Davis; 2005:107-120.
Neuhaus BE. Ethical considerations in clinical reasoning: the impact of technology and cost containment. American Journal of Occupational Therapy. 1988;42:288-294.
Patel VL, Groen GJ. The general and specific nature of medical expertise: a critical look. In: Ericsson A, Smith J, editors. Toward a general theory of expertise: prospects and limits. New York: Cambridge University Press; 1991:93-125.
Resnik L, Jensen GM. Using clinical outcomes to explore the theory of expert practice in physical therapy. Physical Therapy. 2003;83(12):1090-1106.
Rivett D, Higgs J. Hypothesis generation in the clinical reasoning behavior of manual therapists. Journal of Physical Therapy Education. 1997;11(1):40-45.
Roberts L. Flagging the danger signs of low back pain. In: Gifford L, editor. Topical issues of pain 2. Falmouth: CNS Press; 2000:69-83.
Rumelhart D, Ortony E. The representation of knowledge in memory. In: Anderson RC, Spiro RJ, Montague WE, editors. Schooling and the acquisition of knowledge. Hillsdale N J: Lawrence Erlbaum; 1977:99-135.
Schön DA. The reflective practitioner: how professionals think in action. London: Temple Smith, 1983.
Schön DA. Educating the reflective practitioner. San Francisco: Jossey-Bass, 1987.
Sluijs EM. Patient education in physiotherapy: towards a planned approach. Physiotherapy. 1991;77:503-508.
Werner D. Disabled persons as leaders in the problem solving process. In: In: Nothing about us without us: developing innovative technologies for, by and with disabled persons. Palo Alto, CA: Health Wrights; 1998.
World Health Organization. International classification of functioning, disability and health. Geneva: World Health Organization, 2001.