Chapter 1 Clinical decision making and multiple problem spaces
In the second edition of this book we drew on our initial view of clinical reasoning as a process incorporating the elements of cognition, knowledge and metacognition, expanding this to place a greater emphasis on patient-centred care as the context for clinical reasoning. Practitioners were presented as interactional professionals (Higgs & Hunt 1999) whose effectiveness required interaction with their immediate and larger work environment, with the key players in that context, and with the situational elements pertinent to the patient and case under consideration. Health care was presented via a social ecology model as occurring within the wider sphere of social responsibility of professionals which requires practitioners to be proactive as well as responsive to changes in healthcare contexts (Higgs et al 1999).
In this opening chapter of the third edition we extend our previous examination of the nature of clinical reasoning and its context, drawing on our own research and that of colleagues and co-authors. We expand our interpretation of clinical reasoning from a process view, to explore clinical reasoning as a contextualized phenomenon (see also Chapters 2, 8). We extend consideration of the decision-making context from a focus on the immediate task environment of case management acting in the wider healthcare context to explore the multiple levels of the clinical decision-making space, or rather the multiple decision-making spaces, within which interactive reasoning and decision making occur (see Higgs 2006a, b).
In relation to clinical reasoning expertise, we extend the notion of an expert to encompasscapability, professional artistry and patient-centredness; expertise is a journey rather than a point of arrival (see also Chapters 11 and 16). In examining and making explicit these aspects of clinical reasoning our goal is to make clinical reasoning more accessible for novices to learn, for experienced practitioners to portray, for educators to teach, for clinicians to practise and for researchers to explore.
UNDERSTANDING CLINICAL REASONING
In the 10 years since we produced the first edition of this book, we have retained our view that clinical reasoning is both simple and complex. Simply, clinical reasoning is the sum of the thinking and decision-making processes associated with clinical practice; it is a critical skill in the health professions, central to the practice of professional autonomy, and it enables practitioners to take ‘wise’ action, meaning taking the best judged action in a specific context (Cervero 1988, Harris 1993). Despite being straightforward and ‘simple’ this view is very broad; clinical reasoning is seen as permeating throughout clinical practice and as being the core of practice. The importance of understanding the complex nature of clinical reasoning is emphasized in the goal of developing tolerance of ambiguity and a reflexive understanding of practice artistry during health sciences education, as suggested by Bleakley et al (2003).
The complex view of clinical reasoning is embedded in its simplicity and breadth (Higgs 2006b). By encompassing so much of what it means to be a professional (autonomy, responsibility, accountability and decision making in conditions of uncertainty), clinical reasoning gains an inherent mystique. This complexity lies in the very nature of the task or challenge, faced by novice and expert alike, which is to process multiple variables, contemplate the various priorities of competing healthcare needs, negotiate the interests of different participants in the decision-making process, inform all decisions and actions with advanced practice knowledge, and make all decisions and actions in the context of professional ethics and community expectations. The mystique is most evident in the skill of the expert diagnostician who makes difficult decisions with seeming effortlessness, and in the professional artistry of the experienced practitioner who produces an individually tailored health management plan that addresses complicated health needs with humanity and finesse. To address and achieve these professional attributes clinical reasoning is much more a lived phenomenon, an experience, a way of being and a chosen model of practising than it is simply a process. To this end we adopt the following definition of this complex phenomenon:
Clinical reasoning (or practice decision making) is a context-dependent way of thinking and decision making in professional practice to guide practice actions. It involves the construction of narratives to make sense of the multiple factors and interests pertaining to the current reasoning task. It occurs within a set of problem spaces informed by the practitioner’s unique frames of reference, workplace context and practice models, as well as by the patient’s or client’s contexts. It utilises core dimensions of practice knowledge, reasoning and metacognition and draws on these capacities in others. Decision making within clinical reasoning occurs at micro, macro and meta levels and may be individually or collaboratively conducted. It involves metaskills of critical conversations, knowledge generation, practice model authenticity and reflexivity. (Higgs 2006b)
Of note in this definition is the term ‘clinical’. For some health professionals their workplace is not ‘clinical’, their clients are not patients, the focus of their role may be on health rather than illness, and the term ‘consultant’ rather than ‘practitioner’ may be more appropriate. To avoid clumsy expression of these alternative terms we use the terms clinical reasoning and clinical decision making below.
CLINICAL REASONING AND METASKILLS
Our previous model of clinical reasoning (Higgs & Jones 2000) was presented as an upward and outward spiral, a cyclical and a developing process. Each loop of the spiral incorporated data input, data interpretation (or reinterpretation) and problem formulation (or reformulation) to achieve a progressively broader and deeper understanding of the clinical problem. Based on this deepeningunderstanding, decisions are made concerning intervention, and actions are taken. The process was described as including:
These additional dimensions were included in recognition of the growing expectation by and of consumers that they play an active role in their own health care. The image of compliant, dependent patients is replaced by one of informed healthcare consumers who expect their needs and preferences to be listened to, who increasingly want to participate in decision making about their health, and who expect to take action to enhance their health. Alongside this ‘health rather than illness’ focus on the part of the consumer, there are increasing expectations of service and of quality and ownership of health programmes, due to economic factors such as an increasing reliance on ‘user pays’ funding strategies, within which consumers are indeed purchasing health care. Similarly, caregivers need and wish to play a greater role in health management and decision making.
To these dimensions we now add four meta-skills:
It is preferable to view clinical reasoning as a contextualized interactive phenomenon rather than a specific process. The practitioner responsible for making the decisions interacts both with the task and informational elements of decision making and with the human elements and interests of other participants in the decision making. Such interactions can be called critical creative conversations that involve interactions based on critical appraisal of circumstances and, where possible, critical interests in promoting emancipatory practice, and the creation and implementation of particularized, person-centred healthcare programmes (Higgs 2006a).
THE ADEQUACY OF DIFFERENT INTERPRETATIONS
There is no single model of clinical reasoning that adequately represents what clinical reasoning is in the context of different professions and different workplaces. The reason for this lies in several factors:
THE NATURE OF CLINICAL REASONING AS A PHENOMENON
Consider the real world of clinical decision making. Orasanu & Connolly (1993) have described the characteristics of decision making in dynamic settings as follows:
To work within this practice world we need an approach to clinical reasoning that accommodates these complexities. Higgs and colleagues (2006, p. l) described a number of key characteristics of clinical reasoning as follows:
DIFFERENT INTERPRETATIONS OF CLINICAL REASONING
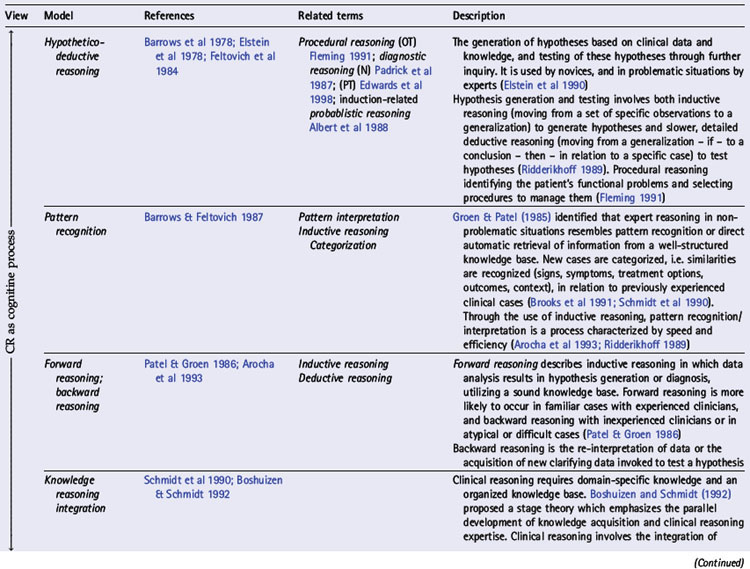
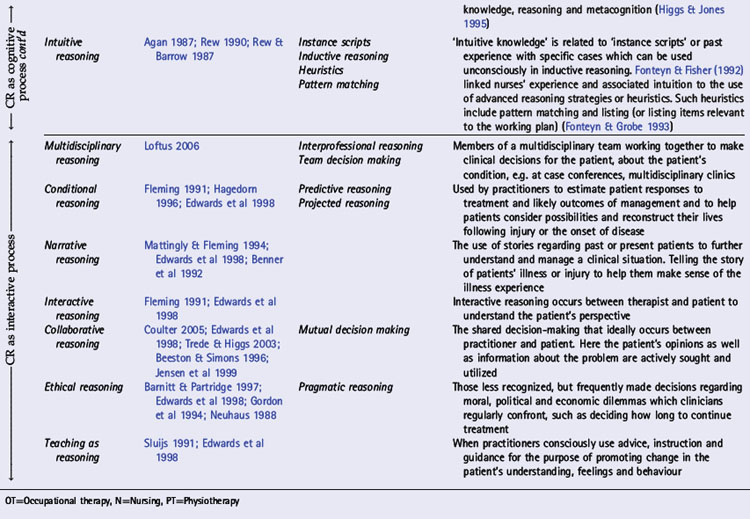
In various chapters of this book a number of interpretations of clinical reasoning are discussed from the perspective of different disciplines, the history of clinical reasoning research, and models of practice within which clinical reasoning occurs. In Table 1.1 we present an overview of key models,strategies and interpretations of clinical reasoning. These have been divided into two groups: cognitive and interactive models. This division reflects three trends: changes in the focus of research and theoretical understandings of clinical reasoning (see Chapters 18, 19); changes in society and expectations of health care (see Chapter 2); and a major shift in emphasis (as outlined above) from the second to the third edition of this book.
Expertise and clinical reasoning
In a review of clinical reasoning literature in medicine, Norman (2005) suggested that there may not be a single representation of clinical reasoning expertise or a single correct way to solve a problem. He noted that ‘the more one studies the clinical expert, the more one marvels at the complex and multidimensional components of knowledge and skill that she or he brings to bear on the problem, and the amazing adaptability she must possess to achieve the goal of effective care’ (p. 426).
Clinical reasoning and clinical practice expertise is a journey, an aspiration and a commitment to achieving the best practice that one can provide. Rather than being a point of arrival, complacency and lack of questioning by self or others, expertise requires both the capacity to recognize one’s limitations and practice capabilities and the ability to pursue professional development in a spirit of self-critique. And it is – or at least we should expect it to be – not only a self-referenced level of capability or mode of practice, but also a search for understanding of and realization of the standards and expectations set by the community being served and the profession and service organization being represented. Box 1.1 presents these characteristics and expectations of experts.
Box 1.1 Characteristics and expectations of expert practitioners
a) General characteristics of experts (Glaser & Chi 1988)
b) Particular characteristics and expectations of health professional experts (Higgs & Jones 2000)
We have deliberately added the idea of expectations to this discussion to emphasize that any human construct is sociohistorically situated. Beyond the research-driven science view of technical expertise there is a need for any professional – but particularly experts, with their claim to superior service and performance – to address the needs of society. Today there is a growing expectation of patient-centred humanization (including cultural competence, information sharing, collaborative decision making, virtuous practice) of expert practice that turns health professional expertise into a collaborative professional relationship rather than an expert-empowered, technically superior, practitioner-centred approach. As highlighted in the research findings of Jensen et al (2006), this patient-centred approach is grounded in a strong moral commitment to beneficence or doing what is in the patient’s best interest. This manifests in therapists’ non-judgemental attitude and strong emphasis on patient education, with expert therapists being willing to serve as patient advocate or moral agent in helping them be successful.
Box 1.1 demonstrates an evolution in thinking about expertise, beginning with the classic research by Glaser & Chi (1988) into expert attributes (a). In 2000 we added to this view ideas of patient-centredness, collaboration, metacognition, mentoring, effective communication and cultural competence (Higgs & Jones 2000) (b). We have added the third group (c) to reflect ideas highlighted in this book.
We propose that clinical expertise, of which clinical reasoning is a critical component, be viewed as a continuum along multiple dimensions. These dimensions include clinical outcomes, personal attributes such as professional judgement, technical clinical skills, communication and interpersonal skills (to involve the client and others in decision making and to consider the client’s perspectives), a sound knowledge base, an informed and chosen practice model and philosophy of practice, as well as cognitive and metacognitive proficiency.
A concept related to expertise is professional artistry, which ‘reflects both high quality of professional practice and the qualities inherent in such artistic or flexible, person-centred, highly reflexive practice’ (Paterson & Higgs 2001, p. 2). Professional artistry refers to ‘practical knowledge, skilful performance or knowing as doing’ (Fish 1998, p. 87) that is developed through the acquisition of a deep and relevant knowledge base and extensive experience (Beeston & Higgs 2001). Professional artistry reflects a uniquely individual view within a shared tradition involving a blend of practitioner qualities, practice skills and creative imagination processes (Higgs & Titchen 2001). Rogers (1983, p. 601) spoke of the artistry of clinical reasoning that is ‘exhibited in the craftsmanship with which the therapist executes the series of steps that culminate in a clinical decision’. The concept of professional practice judgement artistry is discussed in Chapter 16.
ERRORS AND QUALITY: COGNITIVE DIMENSIONS
Errors in clinical reasoning are frequently linked to errors in cognition (Kempainen et al 2003, Rivett & Jones 2004, Scott 2000). Examples of such errors include over-emphasis on findings that support an existing hypothesis, misinterpretation of non-contributory information as confirming an existing hypothesis, rejection of findings which do not support a favoured hypothesis and incorrect interpretation related to inappropriately applied inductive and deductive logic (Elstein et al 1978, Kempainen et al 2003). These errors are commonly associated with habits of thinking and practice which themselves are a potential risk of pattern recognition. That is, in adopting a pattern recognition approach the novice or unreflective practitioner might focus too much on looking for the presence or absence of specific patterns and overlook other potentially important information, or might find it difficult to see anything outside the most familiar patterns (De Bono 1977). Patterns can become rigid, making it difficult to recognize variations. This excessive focus on favourite patterns also leads to patterns being identified on the basis of insufficient information, where one or several key features in a presentation are prematurely judged to represent a particular pattern. Metacognitive skills are the key to protecting against errors associated with pattern recognition.
ERRORS AND QUALITY: INTERACTIVE DIMENSIONS
Within the changing face of health care and the trend towards interactive reasoning there is a need not only to look beyond the cognitive processes of reasoning but also to see matters of quality and errors beyond simply cognitive abilities. Practitioners who wish to adopt a patient-centred approach or a team approach may make errors related to inauthentic implementation of espoused models of practice, lack of valuing or inclusion of the knowledge and reasoning input of team members or patients, and limitations in interpersonal communication, including cultural incompetence. The matter of ethical reasoning also becomes more prominent in interactive reasoning, in terms of choosing to share decision-making responsibilities while yet retaining individual responsibility for one’s actions. Also, in determining to share decision making with patients the practitioner faces the dilemma of dealing with patient’s wishes, informed position and power, which may be in conflict with what the practitioner considers to be in the patient’s best interests.
A MODEL OF INTERACTIVE REASONING AND THE PROBLEM SPACE
Health care is not a decontextualized implementation of protocols, scientific evidence or intellectual information processing. Instead, whether at the level of individual patient or system, health care and decision making operate in context. This is true not only of decision making but also of the store of practice wisdom that the practitioner draws upon as the professional frame of reference for decision making. Practice experiences are gained in context; they are stored in the context of the settings and happenings which they comprise, and they are recalled for future application and contemplation as contextualized meaning chunks (see e.g. Boshuizen & Schmidt 2000, Gordon 1988, Schön 1983).
One of the greatest challenges of clinical reasoning is to harmonize generally accepted healthcare practices and evidence for practice with person-centred practice. This means that best practice should be particularized, not generic. Many people today are recognizing the importance of firmly embedding thinking and reasoning in context (Whiteford & Wright-St Clair 2005). In recent significant research on the impact of context on clinical decision making, Smith (2006) identified that clinical decision making in actual practice is a context-dependent process that is socially and culturally determined. Smith developed a model of factors influencing clinical decision making (see also Chapter 8) in which three levels of context impact on clinical decision making: the immediate patient care context, the practitioner context and the workplace context.
According to Schön (1983), clinical reasoning involves the naming and framing of problems based on a personal understanding of the client’s situation. Two forms of scientific reasoning identified by researchers in occupational therapy are diagnostic reasoning (Rogers & Holm 1991) and procedural reasoning (Mattingly & Fleming 1994). These processes involve a progression from problem sensing to problem definition and problem resolution. These tasks give rise to the idea of the problem space. The notion of the problem space in clinical reasoning has been used by a number of authors. Elstein et al (1978), for example, considered the size of the problem space in relation to the number of hypotheses generated by students and physicians. They found that early in the patient encounter students and physicians generated a limited number of hypotheses (three to five) from limited patient data, and that these guided subsequent data collection. The authors postulated that this was a way of coping with the problem of information overload by reducing the size of the problem space that must be searched for a solution to the problem. Patel & Arocha (2000) examinedthe theory of protocol analysis that is based on the idea that verbalizations in problem solving are interpreted as a search through a problem space of hypotheses and data.
We use the term problem space in a broader way than described above, to reflect the multiple contexts of clinical reasoning. Problem spaces comprise the immediate clinical problem and task environment of clinical decision making embedded in the interests and frames of references of the practitioner(s) and the patient/client. These problem spaces, in turn, are located in the broader clinical reasoning context that encompasses the many local, organizational, sociocultural, global factors that influence clinical decision making (see Figure 1.1).

THE CLIENT’S PROBLEM SPACE
The role for the healthcare consumer is radically different in many respects from the dependent patient role of traditional medicine, where ‘autonomy’ of health professionals was defined as complete control over clinical decision making and clinical intervention. Consumers of health care are becoming increasingly well informed about their health and about healthcare services. Terms such as self-help and holistic health care are becoming more central to health care, and the goal of achieving effective participation by consumers in their health care is widespread, requiring health professionals to involve their clients actively in clinical decision making wherever possible. Increasingly, clients’ choices, rights and responsibilities in relation to their health are changing. Payton et al (1990) advocated client involvement in decision making about the management of their health and well-being. They argued that this process of client participation is based on the ‘recognition of the values of self-determination and the worth of the individual’ (p. ix). Using understanding of their clients’ rights and responsibilities, clinicians need to develop their own approaches to involving the client in reasoning and decision making. Mutual decision making requires not only a sharing of ownership of decisions but also the development of skills in negotiation and explaining, to facilitate effective two-way communication. Professional autonomy becomes redefined as independence in function (within a teamwork context) combined with responsibility and accountability for one’s actions (including the sharing of decision making).
The problem space of clients plays an important role in the process of clinical reasoning since it impacts on framing, naming and dealing with their healthcare needs and concerns; it comprises:
An important aspect of involving patients or clients in clinical decision making is determining and facilitating an appropriate level of participation and responsibility. A level of participation in clinical reasoning appropriate for the individual has been demonstrated to contribute to the patient’s sense of control; in this process it is important to ensure that the patient’s input is voluntary and the patient is informed of the inherent uncertainties of clinical decision making (Coulter 2002).
THE PRACTITIONER’S PROBLEM SPACE
Practitioners bring their personal and professional selves to the task of clinical decision making; these selves frame their problem space. As well as functioning within their personal frames of reference, clinicians operate within their professional frameworks (e.g. the ethical and competency standards/requirements of the profession) and within a broader context of professionalism. The term health professional implies a qualified healthcare provider who demonstrates professional autonomy, competence and accountability (Higgs 1993). Professional status incorporates the responsibility to make unsupervised and accountable clinical decisions and to implement ethical, competent and person-centred practice. This requires health professionals to consider the patient’s problem space, as described above, and to make decisions about the patient’s level of involvement. Dealing with ill-structured healthcare problems requires high-level clinical reasoning abilities, increasingly refined and elaborated medical knowledge (Schmidt et al 1990) and judgement (Round 2001). In relation to ethical issues, practitioners need the ability to deal with these matters in person-centred, professional ways. In addition, practitioners’ problem spaces include their choice of practice model (see Chapter 3), their clinical reasoning capability, and clinical reasoning expertise (see Chapter 11).
THE COLLABORATIVE PROBLEM SPACE OF THE TEAM
Most health professionals work in collaboration with other team members, either directly or indirectly via referral. This includes work across mainstream and complementary and alternative medicine. Byrne (1999) suggested that a coordinated and integrated approach to care is particularly important in the management of chronic and complex health problems. Similarly, Grace et al (2006) identified an increasing preference in patients with chronic health problems, particularly those dissatisfied with mainstream medicine, for practices that directly integrate complementary and alternative medicine with general practice; such models worked best for the patients when both practitioners worked in collaboration. Another area where multidisciplinary health care has been found to be beneficial and widespread is chronic pain management (Loftus & Higgs 2006).
The level of collaboration in clinical decision making in these settings varies considerably. Practitioners may make decisions separately and report decisions to others (e.g. via patient records); they may refer patients to others to take over patient care or to receive advice; they may operate as a decision-making team, making decisions on behalf of their patients (see Chapter 26); or they may work with patients as members of the decision-making team (see Chapters 4 and 34).
THE PROBLEM SPACE OF THE WORKPLACE AND THE LOCAL SYSTEM
Clinicians frequently face ill-defined problems, goals that are complex and outcomes that are difficult to predict clearly. Many aspects of the workplace (see Chapter 9) influence clinical decision making, particularly levels of available human, material and economic resources. Many factors in the workplace frame our approaches to our practice of clinical reasoning. Funding pressures create ‘clinical practices whose explicit demands are heavily weighted toward management and productivity rather than diagnosis and understanding’ (Duffy 1998, p. 96). Such practices are not conducive to reflecting on our understanding of practice. Further, misinterpretations of what evidence-based practice really requires (see Reilly et al 2004), means that some clinicians do not use clinical reasoning critically and wisely to assess evidence for its applicability to individual patients (Jones et al 2006a, b).
One way of thinking about healthcare systems is to conceptualize them as ‘soft systems’, a term introduced by Checkland (1981) to refer to systems in which goals may be unrecognizable and outcomes ambiguous. Professional judgement and decision making within the ambiguous or uncertain situations of health care is an inexact science (Kennedy 1987) which requires reflective practice and excellent skills in clinical reasoning (Cervero 1988, Schön 1983). These skills reflect the importance of individual perspectives rather than a priori criteria (Jungermann 1986). Skills of professional judgement and critical self-evaluation are needed to cope with information processing constraints or ‘bounded rationality’ (Newell & Simon 1972) which result in limitations on the individual’s ability to access knowledge and solve problems (Bransford et al 1986, Feltovich 1983, Hassebrock & Johnson 1986). One way to interpret the way in which professionals cope with the uncertainties and challenges of clinical reasoning is to look beyond science. Harris (1993), for instance, presents the concept of professional practice as comprising a blend of art, craft and technology.
THE PROBLEM SPACE OF THE GLOBAL SYSTEM WITH ITS HEALTHCARE DISCOURSE, KNOWLEDGE AND TECHNOLOGY
Many factors of the wider healthcare environment need to be taken into consideration in clinical reasoning. Health professionals need to develop a broad understanding of the environment in which they work, including knowledge of the factors influencing health (e.g. the environment, socioeconomic conditions, cultural beliefs and human behaviour). In addition, they need to understand how the information age and the technological revolution impact on healthcare demands, provision and expectation. They need to be able to work confidently and effectively with an increasing body of scientific, technical and professional knowledge. Developing a sound individual understanding of clinical reasoning and a capacity to reason effectively will facilitate the clinician’s ability to manage complex and changing information.
CONCLUSION
Whether understanding clinical reasoning is for knowledge generation or research (what is it like?), education (how can it be learned?), or practice (how can we use it? how can we do it well?), the central need is to understand what it is and how it can be developed. In this chapter we have portrayed clinical reasoning as a complex set of processes occurring within multiple and multidimensional problem spaces.
Agan R. Intuitive knowing as a dimension of nursing. Advances in Nursing Science. 1987;10:63-70.
Albert AD, Munson R, Resnik MD, editors. Reasoning in medicine: an introduction to clinical inference. Baltimore: Johns Hopkins University Press. 1988.
Arocha JF, Patel VL, Patel YC. Hypothesis generation and the coordination of theory and evidence in novice diagnostic reasoning. Medical Decision Making. 1993;13:198-211.
Barnitt R, Partridge C. Ethical reasoning in physical therapy and occupational therapy. Physiotherapy Research International. 1997;2:178-194.
Barrows HS, Feltovich PJ. The clinical reasoning process. Medical Education. 1987;21:86-91.
Barrows HS, Feightner JW, Neufield VR, et al. An analysis of the clinical methods of medical students and physicians. In Report to the Province of Ontario Department of Health. Hamilton, Ontario: McMaster University; 1978.
Beeston S, Higgs J. Professional practice: artistry and connoisseurship. In: Higgs J, Titchen A, editors. Practice knowledge and expertise in the health professions. Oxford: Butterworth-Heinemann; 2001:108-117.
Beeston S, Simons H. Physiotherapy practice: practitioners’ perspectives. Physiotherapy Theory and Practice. 1996;12:231-242.
Benner P, Tanner C, Chesla C. From beginner to expert: gaining a differentiated clinical world in critical care nursing. Advances in Nursing Science. 1992;14:13-28.
Bleakley A, Farrow R, Gould D, et al. Making sense of clinical reasoning: judgement and the evidence of the senses. Medical Education. 2003;37(6):544-552.
Boshuizen HPA, Schmidt HG. On the role of biomedical knowledge in clinical reasoning by experts, intermediates and novices. Cognitive Science. 1992;16:153-184.
Boshuizen HPA, Schmidt HG. The development of clinical reasoning expertise. In: Higgs J, Jones M, editors. Clinical reasoning in the health professions. 2nd edn. Oxford: Butterworth-Heinemann; 2000:15-22.
Bransford J, Sherwood R, Vye N, et al. Teaching thinking and problem solving: research foundations. American Psychologist. 1986;41:1078-1089.
Brooks LR, Norman GR, Allen SW. Role of specific similarity in a medical diagnostic task. Journal of Experimental Psychology: General. 1991;120(3):278-287.
Byrne C. Interdisciplinary education in undergraduate health sciences. Pedagogue (Perspectives on Health Sciences Education). 1999;3:1-8.
Cervero RM. Effective continuing education for professionals. San Francisco: Jossey-Bass, 1988.
Checkland PB. Systems thinking: systems practice. New York: John Wiley, 1981.
Coulter A. The autonomous patient: ending paternalism in medical care. London: Nuffield Trust, 2002.
Coulter A. Shared decision-making: the debate continues. Health Expectations. 2005;8:95-96.
De Bono E. Lateral thinking. London: Penguin, 1977.
Duffy J. Stroke with dysarthria: evaluate and treat; garden variety or down the garden path. Seminars in Speech and Language. 1998;19:93-98.
Edwards IC, Jones MA, Carr J, et al. Clinical reasoning in three different fields of physiotherapy – a qualitative study. Proceedings of the Fifth International Congress of the Australian Physiotherapy Association, Melbourne. 1998:298-300.
Elstein AS, Shulman LS, Sprafka SA. Medical problem solving: an analysis of clinical reasoning. Cambridge, MA: Harvard University Press, 1978.
Elstein AS, Shulman LS, Sprafka SA. Medical problem solving: a ten year retrospective. Evaluation and the Health Professions. 1990;13:5-36.
Feltovich PJ. Expertise: reorganizing and refining knowledge for use. Professions Education Researcher Notes. 1983;4:5-9.
Feltovich PJ, Johnson PE, Moller JH, et al. LCS: the role and development of medical knowledge in diagnostic expertise. In: Clancey WJ, Shortliffe EH, editors. Readings in medical artificial intelligence: the first decade. Reading, MA: Addison-Wesley; 1984:275-319.
Fish D. Appreciating practice in the caring professions: refocusing professional development and practitioner research. Oxford: Butterworth-Heinemann, 1998.
Fleming MH. The therapist with the three track mind. American Journal of Occupational Therapy. 1991;45:1007-1014.
Fonteyn M, Fisher S. The study of expert nurses in practice. Paper presented at: Transformation through unity: decision-making and informatics in nursing, 17 October. Portland, OR:University of Oregon Health Science Centre. 1992.
Fonteyn M, Grobe S. Expert critical care nurses’ clinical reasoning under uncertainty: representation, structure and process. In: Frisse M, editor. Sixteenth annual symposium on computer applications in medical care. New York: McGraw-Hill; 1993:405-409.
Glaser R, Chi MTH. Overview. In: Chi MTH, Glaser R, Farr MJ, editors. The nature of expertise. Hillsdale, NJ: Lawrence Erlbaum; 1988:xv-xxviii.
Gordon D. Clinical science and clinical expertise: changing boundaries between art and science in medicine. In: Lock M, Gordon DR, editors. Biomedicine examined. Dordrecht: Kluwer Academic; 1988:257-295.
Gordon M, Murphy CP, Candee D, et al. Clinical judgement: an integrated model. Advances in Nursing Science. 1994;16:55-70.
Grace S, Higgs J, Horsfall D. Integrating mainstream and complementary and alternative medicine: investing in prevention. Proceedings of the University of Sydney From Cell to Society 5 conference, 9–10 November. 2006:18-25.
Groen GJ, Patel VL. Medical problem-solving: some questionable assumptions. Medical Education. 1985;19(2):95-100.
Hagedorn R. Clinical decision making in familiar cases: a model of the process and implications for practice. British Journal of Occupational Therapy. 1996;59:217-222.
Harris IB. New expectations for professional competence. In: Curry L, Wergin JF, editors. Educating professionals: responding to new expectations for competence and accountability. San Francisco: Jossey-Bass; 1993:17-52. and Associates
Hassebrock F, Johnson PE. Medical knowledge and cognitive effort in diagnostic reasoning. Paper presented at the annual meeting of the American Educational Research Association. 1986. San Francisco
Higgs J. Physiotherapy, professionalism and self-directed learning. Journal of the Singapore Physiotherapy Association. 1993;14:8-11.
Higgs J. Realising hermeneutic dialogues: creating spaces for critical, creative conversations in learning, research, clinical decision making and practice advancement. In CPEA Occasional Paper no. 5. Collaborations in Practice and Education Advancement. Australia: University of Sydney; 2006.
Higgs J. The complexity of clinical reasoning: exploring the dimensions of clinical reasoning expertise as a situated, lived phenomenon. Seminar presentation at the Faculty of Health Sciences, 5 May. Australia: University of Sydney. 2006.
Higgs J, Hunt A. Rethinking the beginning practitioner: introducing the ‘interactional professional’. In: Higgs J, Edwards H, editors. Educating beginning practitioners: challenges for health professional education. Oxford: Butterworth-Heinemann; 1999:10-18.
Higgs J, Jones M. Clinical reasoning. In: Higgs J, Jones M, editors. Clinical reasoning in the health professions. Oxford: Butterworth-Heinemann; 1995:3-23.
Higgs J, Jones M. Clinical reasoning in the health professions. In: Higgs J, Jones M, editors. Clinical reasoning in the health professions. 2nd edn. Oxford: Butterworth-Heinemann; 2000:3-14.
Higgs J, Titchen A. Towards professional artistry and creativity in practice. In: Higgs J, Titchen A, editors. Professional practice in health, education and the creative arts. Oxford: Blackwell Science; 2001:273-290.
Higgs C, Neubauer D, Higgs J. The changing health care context: globalization and social ecology. In: Higgs J, Edwards H, editors. Educating beginning practitioners: challenges for health professional education. Oxford: Butterworth-Heinemann; 1999:30-37.
Higgs J, Trede F, Loftus S, et al. Advancing clinical reasoning: interpretive research perspectives grounded in professional practice. In CPEA Occasional Paper no. 4. Collaborations in Practice and Education Advancement. Australia: University of Sydney; 2006.
Jensen GM, Gwyer J, Hack LM, et al. Expertise in physical therapy practice. Boston: Butterworth-Heinemann, 1999.
Jensen GM, Gwyer J, Hack LM, et al. Expertise in physical therapy practice, 2nd edn. St Louis: Saunders-Elsevier, 2006.
Jones M, Grimmer K, Edwards I, et al. Challenges in applying best evidence to physiotherapy. Internet Journal of Allied Health Sciences and Practice. 4(3), 2006. Online. Available: http://ijahsp.nova.edu/ 18 June 2007
Jones M, Grimmer K, Edwards I, et al. Challenges in applying best evidence to physiotherapy practice: part 2 – reasoning and practice challenges. Internet Journal of Allied Health Sciences and Practice. 4(4), 2006. Online. Available: http://ijahsp.nova.edu/ 18 June 2007
Jungermann H. The two camps on rationality. In: Arkes HR, Hammond KR, editors. Judgment and decision making: an interdisciplinary reader. New York: Cambridge University Press; 1986:627-641.
Kassirer JP, Kopelman RI. Learning clinical reasoning. Baltimore: Williams and Wilkins, 1991.
Kempainen RR, Migeon MB, Wolf FM. Understanding our mistakes: a primer on errors in clinical reasoning. Medical Teacher. 2003;25(2):177-181.
Kennedy M. Inexact sciences: professional education and the development of expertise. Review of Research in Education. 1987;14:133-168.
Lawson AE, McElrath CB, Burton MS, et al. Hypothetico-deductive reasoning skill and concept acquisition: testing a constructivist hypothesis. Journal of Research in Science Teaching. 1991;28:953-970.
Loftus S. Language in clinical reasoning: learning and using the language of collective clinical decision making. In Unpublished doctoral thesis. Australia: University of Sydney; 2006. Online. Available: http://ses.library.usyd.edu.au/handle/2123/1165
Loftus S, Higgs J. Clinical decision-making in multidisciplinary clinics. In: Flor H, Kalso E, Dostrovsky JO, editors. Proceedings of the 11th World Congress on Pain. Seattle: International Association for the Study of Pain, IASP Press; 2006:755-760.
Mattingly C, Fleming MH. Clinical reasoning: forms of inquiry in a therapeutic practice. Philadelphia: F A Davis, 1994.
Neuhaus BE. Ethical considerations in clinical reasoning: the impact of technology and cost containment. American Journal of Occupational Therapy. 1988;42:288-294.
Newell A, Simon HA. Human problem solving. Englewood Cliffs, NJ: Prentice-Hall, 1972.
Norman G. Research in clinical reasoning: past history and current trends. Medical Education. 2005;39:418-427.
Orasanu J, Connolly T. The reinvention of decision making. In: Klein GA, Orasanu J, Calderwood R, et al, editors. Decision making in action: models and methods. Norwood, NJ: Ablex; 1993:3-20.
Padrick K, Tanner C, Putzier D, et al. Hypothesis evaluation: a component of diagnostic reasoning. In: McClane A, editor. Classification of nursing diagnosis: proceedings of the seventh conference. Toronto: CV Mosby; 1987:299-305.
Patel VL, Arocha JF. Methods in the study of clinical reasoning. In: Higgs J, Jones M, editors. Clinical reasoning in the health professions. 2nd edn. Oxford: Butterworth-Heinemann; 2000:78-91.
Patel VL, Groen GJ. Knowledge-based solution strategies in medical reasoning. Cognitive Science. 1986;10:91-116.
Paterson M, Higgs J. Professional practice judgement artistry. In CPEA Occasional Paper no. 3. Centre for Professional Education Advancement. Australia: University of Sydney; 2001.
Payton OD, Nelson CE, Ozer MN. Patient participation in program planning: a manual for therapists. Philadelphia: FA Davis, 1990.
Reilly S, Douglas J, Oates J. Evidence-based practice in speech pathology. London: Whurr, 2004.
Rew L. Intuition in critical care nursing practice. Dimensions of Critical Care Nursing. 1990;9:30-37.
Rew L, Barrow E. Intuition: a neglected hallmark of nursing knowledge. Advances in Nursing Science. 1987;10:49-62.
Ridderikhoff J. Methods in medicine: a descriptive study of physicians’ behaviour. Dordrecht: Kluwer Academic, 1989.
Rivett DA, Jones MA. Improving clinical reasoning in manual therapy. In: Jones MA, Rivett DA, editors. Clinical reasoning in manual therapy. Edinburgh: Butterworth-Heinemann; 2004:403-431.
Rogers JC. Clinical reasoning: the ethics, science, and art. Eleanor Clarke Slagle Lecture, American Journal of Occupational Therapy. 1983;37:601-616.
Rogers JC, Holm M. Occupational therapy diagnostic reasoning: a component of clinical reasoning. American Journal of Occupational Therapy. 1991;45:1045-1053.
Round AP. Introduction to clinical reasoning. Journal of Evaluation in Clinical Practice. 2001;7:109-117.
Schmidt HG, Norman GR, Boshuizen HPA. A cognitive perspective on medical expertise: theory and implications. Academic Medicine. 1990;65:611-621.
Schön DA. The reflective practitioner: how professionals think in action. London: Temple Smith, 1983.
Scott I. Teaching clinical reasoning: a case-based approach. In: Higgs J, Jones M, editors. Clinical reasoning in the health professions. 2nd edn. Oxford: Butterworth-Heinemann; 2000:290-297.
Sluijs EM. Patient education in physiotherapy: towards a planned approach. Physiotherapy. 1991;77:503-508.
Smith MCL. Clinical decision making in acute care cardiopulmonary physiotherapy. In Unpublished doctoral thesis. Sydney: University of Sydney; 2006.
Titchen A. Professional craft knowledge in patient centred nursing and the facilitation of its development. Oxford: Ashdale Press, 2000.
Trede F, Higgs J. Re-framing the clinician’s role in collaborative clinical decision making: re-thinking practice knowledge and the notion of clinician–patient relationships. Learning in Health and Social Care. 2003;2(2):66-73.
Whiteford G, Wright-St Clair V, editors. Occupation and practice in context. Sydney: Elsevier. 2005.