Chapter 29 Clinical reasoning to facilitate cognitive–experiential change
HEALTHCARE PRACTITIONERS ARE TEACHERS
Healthcare practitioners across all disciplines, areas of practice and practice settings assess and collaboratively manage (independently and in conjunction with other health professionals) patients’ physical impairments, environment and psychosocial status. This holistic approach to understanding patients and their problems is consistent with the World Health Organization (WHO) model of health and disability (WHO 2001). Healthcare management regularly includes facilitating patients’ learning, including understanding of their health condition and factors either predisposing or contributing to the maintenance of their health problems, understanding management options and understanding prognosis. An example of learning commonly required within physiotherapy is patients’ awareness of habits in body posture and movement and alternative or more effective strategies, and their understanding and performance of general and specific exercises and self-management strategies. Ideally, clinicians’ approach to promoting patient learning is tailored to the individual patient (in terms of expectations and goals, clinical presentation, cognitive and physical capabilities) and to the nature of the learning desired (e.g. technicalities of a specific exercise versus construction of a revised health and disability belief). However, the skill and effectiveness of clinicians in this important aspect of management varies enormously (Payton et al 1998). Ineffectiveness in facilitating patient learning can stem from a multitude of clinician, patient/family/carer, resource and policy factors. Here we focus on factors relating to the clinician, particularly clinicians’ understanding and philosophy of health and disability and their approach to promoting patient learning, especially with respect to changing beliefs regarding health and disability.
PHILOSOPHY OF PRACTICE
Healthcare practitioners’ philosophy of practice and their world view in general influences their perceptions and their approach to practice (Cusick 2001, Higgs et al 1999, Hooper 1997, Jensen et al 2000, Unsworth 2004). For example, based on research into expert physical therapy practice, Jensen and colleagues’ model of expert practice in physical therapy has the therapist’s philosophy of practice as the core ingredient of expert practice that both influences and is influenced by four additional integrated dimensions of expert practice: a dynamic, multidimensional knowledge base; a clinical reasoning process embedded in a collaborative, problem-solving approach; a central focus on movement assessment linked to patient function; and consistent virtues seen in caring and commitment to patients. The patient-centred expert practice evident in the findings of this research (see Chapter 11 for further details) is consistent with the intent and requirements of practising within a biopsychosocial as opposed to biomedical philosophy of health care (Borrell-Carrió et al 2004; Engel 1977, 1978; Waddell 1987).
BIOPSYCHOSOCIAL MODEL
The biopyschosocial model as it was originally proposed ‘dispenses with the scientifically archaic principles of dualism and reductionism and replaces the simple cause-and-effect explanations of linear causality with reciprocal causal models’ (Engel 1978, p. 175).
The WHO model of health and disability (WHO 2001; see also Chapter 22) reflects this biopsychosocial perspective whereby patients’ clinical presentations (their body functions and structures or physical status; their capacity and performance of functional activities of life; and their subsequent ability to participate in their family, work and leisure roles) are portrayed as the result of influences (both positive and negative) of their health condition, environment and personal factors. Importantly, the contributions of the physical/biomedical, environmental and psychosocial influences to a particular patient are individual and complex. That is, the individual factors not only combine in determining a patient’s disability experience, they also directly influence each other (Borrell-Carrió et al 2004).
However, some clinicians’ personal and professional philosophies of practice are clearly more biomedically than biopsychosocially based, leading either to a lack of attention to these influences on patients’ presentations (for example the view that ‘psychological’ aspects of patients’ problems are separate from the physical and it is not the clinician’s role to manage psychological issues) or to an overly superficial and hence less effective assessment, reasoning and management of psychosocial barriers. This may also be associated with a view that psychosocial factors only become relevant when working with patients in chronic pain and disability and are not relevant to the more acute patient presentations. Further, while health professionals may claim to be biopsychosocially oriented in their assessment, reasoning and management, espoused philosophies of practice do not always reflect actual practice attitudes and behaviours (Argyris & Schön 1978, Jorgensen 2000, Mattingly & Hayes Fleming 1994). In a critical review of cognitive-behavioural theory and practice, Sharp (2001) argued that the cognitive dimension of cognitive-behavioural therapy for chronic pain as reported in the literature is inadequate and that behavioural management inappropriately dominates the cognitive-behavioural interventions. The conception of biopsychosocial for some remains dualistic, in that either (a) the patient’s presentation is viewed as a combination of biomedical and psychosocial problems, rather than construing biopsychosocial as a genuine integration of mind and body where each influences the other (Borrell-Carrió et al 2004, Duncan 2000, Engel 1978, Pincus 2004), or (b) appreciation and focus are given to psychological factors without appropriate recognition and attention to the social circumstances that have contributed to shaping those cognitions and that remain as barriers to change (Osborn & Smith 1998, Sim & Smith 2004).
Cognitive-behavioural approach
The cognitive-behavioural approach situated in the biopsychosocial model is increasingly put forward as the preferred approach for the management of chronic pain and disability and associated psychosocial influences (e.g. Main et al 2000, Morley et al 1999, Turk & Flor 2006). The evolution of this approach is described elsewhere (Gamsa 1994a, 1994b), but in general it is based on the theory that patients’ thoughts, feelings and behaviours are interrelated in their pain or disability experience. Turk & Flor (2006, p. 340) explain that the cognitive-behavioural perspective is based on five central assumptions:
Based on individual patient assessment, cognitive-behavioural management then draws on a combination of explanation and education directed at facilitating restructuring of unhelpful or maladaptive thoughts and associated feelings, and operant behavioural techniques to strengthen patients’ constructive thoughts, self-efficacy and active coping behaviours while discouraging the reverse (Jones & Edwards 2006). The aim is to assist patients in gaining control over the effects of pain and disability while also modifying the actual affective, behavioural, cognitive and sensory aspects of the experience (Turk & Flor 2006).
PSYCHOSOCIAL FACTORS CONTRIBUTE TO THE DISABILITY EXPERIENCE
In the biopsychosocial and WHO models of health and disability, patients’ thoughts, feelings, self-efficacy and coping strategies contribute (positively and negatively) to their disability experiences (Craig 2006, Flor & Turk 2006, Gottlieb et al 2001, Jones & Edwards 2006, King et al 2002).
Psychosocial factors, of course, involve more than just the patient’s own thoughts and feelings; the expressed or perceived thoughts and feelings and the behaviour of others (healthcare practitioners, family, friends, acquaintances and service representatives such as insurers and resource providers) also influence an individual’s disability experience. For example, in a qualitative study investigating the personal experience and psychological processes involved in maintaining pain, distress and disability in subjects presenting with benign chronic low back pain, Osborn & Smith (1998) used an interpretative phenomenological analysis to identify four themes common to the participants: (a) searching for an explanation; (b) comparing this self with other selves; (c) not being believed; and (d) withdrawing from others. The frustrations regarding inadequate explanation from the medical system reported by these participants is well recognized as an iatrogenic contributing factor to maintained disability (e.g. Main et al 2000, Main & Watson 2002). The effect of these subjects’ self-image was evident in their continuing comparisons to others and to their memory of their past selves while also projecting who they were likely to be in the future (Osborn & Smith 1998, p. 72):
Their contemporary self-regard contrasted with a nostalgic recall of their past and those around them, and their comparisons served almost inevitably as an index of their sense of threat and loss. Attempts to buttress self-esteem by comparison with those more unfortunate often proved counterproductive and served only to remind participants of their own gloomy prognosis.
Sim & Smith (2004) noted that this loss of a former self is a common finding in people suffering with chronic disability and pain, and described the circumstances that leave these people with a fundamental choice of trying to maintain their former self in spite of the pain, to suspend the former self in the hope that it can be regained once the pain is gone, or to come to terms with a new painful self.
The third theme identified by Osborn & Smith (1998) of not being believed created for the participants a continual need to justify their pain, and the incongruity of being mobile or appearing healthy created a sense that they should appear ill in order to conform to the expectations of others. The participants’ tendency to withdraw from others was the final theme. The researchers related this to participants’ fear of misunderstanding and rejection, highlighting the various and complex forms which fear-avoidance may take (Phillips 1987). In other words, fear-avoidance may have a social basis and not just a biomedical one.
With recognition that the thoughts, feelings and behaviours of patients and others influence disability, healthcare practitioners clearly need strategies and skills in assessing and managing these influences within the limits of their professional training. The level of education health practitioners receive in this area varies enormously, both across and within professions. Although it is not realistic to refer all patients to healthcare practitioners with more extensive education in psychosocial assessment and management (e.g. psychologists), superficial assessments leading to superficial judgements and inappropriate management are equally inappropriate. All healthcare professions have their own body of literature to assist their members’ understanding and application in this important area. For example, there is now very helpful physiotherapy literature providing suggestions on assessment and management strategies specifically targeting patients’ unhelpful thoughts, feelings and behaviours (e.g. Harding 1998, Johnson & Moores 2006, Keefe et al 2006, Kendall & Watson 2000, Main & Watson 2002, Muncey 2002, Strong & Unruh 2002). However, as discussed above, many clinicians either have not incorporated this approach into their philosophy and application of practice or have acknowledged its importance but take a superficial approach to psychosocial assessment and management.
It is not uncommon to find recommended management strategies that selectively ignore patients’ maladaptive coping behaviours while reinforcing their adaptive responses without providing practitioners with explanation as to how judgements of adaptive versus maladaptive should be made. It is as though there is an assumption that maladaptive thoughts, statements and behaviours can be defined out of context and some sort of universal truth exists that defines for everyone what is normal versus abnormal. For example, praying is classically given as an example of a passive coping behaviour that should be challenged and ideally replaced with something more active. However, judgements such as this simply cannot be made out of context. Whereas for one person praying may well be a passive coping behaviour linked to an excessively negative perspective, for another it may function as an active coping mechanism with links to positive thoughts, providing a source of strength and conviction to fight on. We certainly take issue with such a positivist position regarding judgements about normality and motivation. Any assessment of a patient’s beliefs, emotions and behaviours cannot be made without a deeper understanding of the person (including personal perceptions and social influences) and the basis for their perspectives. Kleinman et al (1992, p. 6) highlight the challenge this creates to the epistemological premise that underpins traditional biomedical theory and research, ‘namely that there is objective knowledge, knowledge apart from subjective experience’. Although it may not be the intent of those promoting cognitive-behavioural therapy, it is very common to see such superficial judgements being made in practice.
SCHEMATA UNDERLYING PATIENTS’ COGNITIVE/AFFECTIVE STATUS
Because disability is influenced by patients’ past and present psychosocial circumstances, even with the same medical condition (e.g. low back pain, cardiorespiratory or neurological disorder), no two patients will have the same disability experience. Understanding what patients think and feel about their disability is an important first step in determining how their cognitive/affective status may be positively or negatively affecting them and their recovery. However, when patients with the same or similar medical conditions are viewed by the clinician as homogeneous, or when patients’ disability experiences are superficially explored (either through questionnaires alone or through shallow questioning) without attending to the basis of their expressed thoughts and feelings, the result is incomplete understanding and either failure to address important cognitive/affective factors or superficial attention to these factors with less than optimal results.
A construct we find promising for encouraging clinicians to seek a fuller understanding of patients’ disability experiences, so that patients’ thoughts are not oversimplified as simply internal behaviours that can be managed solely through operant behavioural strategies, is the notion of illness, pain and self schemata and how they are influenced by a person’s disability experience. Pincus & Morley (2001) reviewed the literature on selective information processing bias in chronic pain patients and, based on conflicting research findings related to attention, interpretation and memory bias, proposed that patients’ cognitive/affective status can be portrayed as schemata comprising personal perspectives (conscious and unconscious) linked with internal (e.g. sensory) and external (e.g. past and present life and disability-specific experiences) stimuli that contribute to determining patients’ attention, interpretations, behaviours and coping.
Illness schemata
Research in medical anthropology, medical sociology and cognitive psychology has contributed to the understanding of illness representations or schemata. In what is recognized as a seminal article, Leventhal et al (1980) put forward the notion that patients’ mental representations of health threats determine how they respond to those threats. Illness schemata are defined as individuals’ ‘implicit theories of illness’ that they use in order to interpret and respond to health threats. These illness representations are like imprints, or patterns of interconnected features, learned through social and personal experiences. Skelton & Croyle (1991, p. 4) reported on illness cognition research supporting the thesis that lay illness schemata comprise the following elements:
Pincus & Morley (2001) added to these elements evaluative dimensions relating to the disability, autonomous functioning, quality of life and emotional expectations. For example, Bishop (1991) identified a number of dimensions that people use in evaluating a medical condition, including such things as seriousness, social desirability, personal responsibility, controllability and changeability. Thus it is not only people’s existing beliefs and assumptions that make up their illness schema and contribute to determining their coping but also their appraisal of the threat posed by their medical condition.
Pain schema
Pincus & Morley (2001) portrayed the pain schema as comprising the immediate sensory-intensity, spatial and temporal features of pain, along with the initial affective responses and self-protective behaviours that ensue.
Self schema
The self schema is a complex multifaceted construct that relates to who you are with reference to who you used to be (prior to your perceived change in self) and who you would like to be in the future. It includes an evaluative dimension that contributes to an individual’s sense of self-worth. Disability has the potential to disrupt aspects of the self such that repeated failures to function ‘normally’, and the negative emotions that result, can lead to changes in a person’s self-image (Osborne & Smith 1998, Sim & Smith 2004).
SCHEMA ENMESHMENT
Schemata evolve over time, and the repeated simultaneous activation of aspects from different schemata is thought to be a mechanism of learning that results in a blurring of representations such that elements from one schema become incorporated in another. This enmeshment of schemata is believed to be one explanation for the observation that events leading to activation of one schema with relatively benign consequences can develop into a schema evoking more significant effects (Pincus & Morley 2001). For example, enmeshment of the pain schema and the self schema could result in a patient’s aggravation of pain, not simply evoking specific pain behaviours (e.g. grimaces or cessation of activity), but also activating the patient’s negative self schema such that the pain provocation evokes negative thoughts and self-statements.
Pincus & Morley (2001) put forward examples of possible interrelationships that can exist between a person’s pain, illness and self schemata (Figure 29.1). Figure 29.1A portrays the relationship in a healthy person, where there is only partial overlap. The extent of overlap in acute pain is reported to depend on the context, and the authors provide the example of pain occurring with needle puncture during blood donation having no significance to general physical well-being and little relevance to the sense of self other than perhaps strengthening the person’s sense of altruism. In contrast, the same needle puncture pain occurring with a blood test for a potentially fatal disease would clearly activate both pain and illness schemata but also contemplation of the self and what the future may hold. Figure 29.1B is suggested as an enmeshment that might be found with a chronic pain patient who is adaptively coping with the condition and whose ‘self’ is largely unchanged and self-worth is retained. Figure 29.1C portrays a situation where the pain and self schemata are enmeshed without change to the illness schema. Here Pincus & Morley offered the example of the athlete whose pain following a traumatic injury has impacted on self-identity but without any significant activation of illness scenarios. Lastly, in Figure 29.1D all three schemata are enmeshed, as might occur in the chronic pain patient who is not coping and where the threats associated with the pain/illness experience have led to serious changes in the patient’s concepts of self and self-worth.
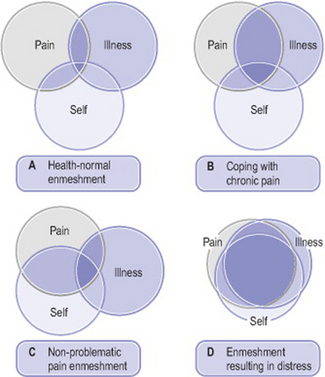
Figure 29.1 Variations in the overlap of pain, illness, and self schemata.
From Pincus & Morley 2001. Copyright © 2001 by the American Psychological Association. Reprinted with permission
We present this schema theory not to suggest that new discrete psychological categorizations are needed. Rather, we put this theory forward as we feel it highlights that patients are clearly not homogeneous in their psychosocial presentations while illustrating examples of factors (schemata) and combinations of factors (schema enmeshment) that may contribute to a patient’s disability experience. It is hoped that this deeper view of patients’ thoughts and feelings will discourage clinicians from limiting themselves to superficial assessments and superficial judgements regarding patients’ cognitions, emotions and disability behaviours.
COGNITIVE-EXPERIENTIAL MANAGEMENT FOR FACILITATING PATIENT LEARNING
The interactions of patients’ cognitions and emotions with their pain or disability experiences are well documented (e.g. Craig 2006, Flor & Turk 2006), and Turk & Flor (2006) have highlighted the growing body of evidence supporting the cognitive-behavioural approach in the management of a wide range of pain syndromes. However, we propose that a reconceptualization from cognitive-behavioural to cognitive-experiential may assist in discouraging superficial approaches to psychosocial assessment and cognitive-behavioural management. A cognitive-experiential approach requires a different focus of assessment than that traditionally used for determination of a physical diagnosis and requires management reasoning and action directed toward understanding and promoting change (i.e. learning) in patients’ pain and disability experiences.
Clinical reasoning and the interpretation of experience
‘Believing … that man is an animal suspended in webs of significance he himself has spun, I take culture to be those webs, and the analysis of it to be therefore not an experimental science in search of law but an interpretive one in search of meaning’ (Geertz 1973, p. 5).
In endeavouring to understand the decisions and actions that may arise from patients’ interpretations of experience, models of reasoning which can embrace different paradigms of inquiry (as suggested by Geertz) are called for. We propose such a model of reasoning in this chapter (see also Chapter 22). Firstly, it is useful to reconceptualize one of the roles of clinical reasoning in clinical practice. Clinical reasoning is not only concerned with how clinicians interpret a broad range of data in the conduct of practice and then learn from their reasoning, through the ‘outcomes’ or consequences of their decision making; it is also concerned with fostering a process of adult learning in and together with patients regarding what can be learned to assist them to move from one place of understanding of their health to another place of understanding and therefore decision making. In the clinical practice context this will usually involve both an instrumental and a communicative form of learning. These two forms of learning are the products of different reasoning processes.
Instrumental learning arises from reasoning using assumptions that knowledge is objective, measurable, predictive and generalizable (Edwards et al 2006, Mezirow 1991). Some of the excellent behavioural strategies used in cognitive-behavioural therapy may fall within the process of instrumental learning, where patients are taught particular ways of responding to and coping with pain; ways which might be useful for many other patients in a similar situation. The evaluation of such learning is amenable to an empirical evaluation in terms of performance or non-performance of particular tasks.
Unhelpful schema enmeshment is proposed to be a product of learning related to patients’ pain and disability experiences (Pincus & Morley 2001). Understanding the interpretation of experience requires a communicative form of learning (Edwards et al 2006) arising from a narrative reasoning approach which utilizes assumptions about knowledge, including that knowledge is context-dependent, socially constructed, has multiple realities and is also irrevocably linked to historical, cultural and structural factors (Germov 2005). In other words, with respect to the latter factors, neither knowledge nor data can be understood apart from such contexts. For example, an understanding of the aetiology of the ongoing poor health of indigenous people in Australia cannot be separated from an understanding of their stories (narratives) and the history of Aboriginal people since European settlement began in 1788 (Gray & Saggers 2005).
Working with patients for better health, when framed in adult learning terms, involves another kind of skill building in addition to teaching behavioural strategies, relevant and constructive though they undoubtedly can be. It also involves patients learning how to reflect critically on their situations using both forms of learning - instrumental and communicative - and the understanding of knowledge associated with each. The term ‘critical’ in critical reflection does not mean necessarily reflecting more profoundly but reflecting with a critical examination of the assumptions underlying a presently held set of values and conclusions (or interpretations) from one’s experiences (Brookfield 2000).
The adult learning process described here has been termed ‘transformatory learning’ (Mezirow 1991). In this chapter we also describe it as a cognitive-experiential approach to learning for better health. In using this term we wish to highlight what we consider an important element not necessarily captured in cognitive-behavioural approaches toward better health. The adult learning process of cognitive-experiential learning does not focus primarily on identifying, addressing and then modifying or changing identified activities and visible behaviours. Certainly, the aim or end result of such cognitive-experiential learning may well see the patient change unhelpful behaviours. Also, such identified data form an essential part of most health practitioners’ assessment practices and help direct goal setting and collaborative processes. Notwithstanding, a cognitive-experiential learning process also focuses on how patients’ interpretations of experience (pain, illness and/or disability) have created meanings which then inform their beliefs and, importantly, their decision making regarding their health. Using the quoted assertions of Geertz (1973), part of our inquiry, as a basis for further learning, is to understand ‘the webs of significance’ which patients have created for and about themselves. In certain circumstances such a web may be supportive, whereas in others it may enmesh patients, leaving them less able to function and participate in roles and activities than they would otherwise wish.
One of the most debilitating experiences of patients with chronic pain, as one increasingly common example of ill health, has been the so-called irrational and recalcitrant behaviour of such pain. In so-called ‘central pain states’, pain is no longer modulated by the same linear or cause-and-effect neurophysiological processes found in acute pain. Instead the pattern and behaviour of pain is less predictable, with secondary hyperalgesia creating false positive findings to traditional physical assessments that are often misinterpreted as indicative of local impairment and pathology (Fields et al 2006, Gifford et al 2006). Traditionally, such pain was difficult to validate on clinical examination, leading to a range of behavioural diagnoses based on an instrumental or biomedical form of reasoning (Gifford et al 2006, Main and Watson 2002, Waddell 2004). However, current pain research has provided patients with a plausible account of the ‘irrationality’ of chronic pain (Edwards et al 2006, Fields et al 2006, Gifford et al 2006). This research has been important because no longer are patients themselves held to be the primary source of irrationality in the situation (Steen & Haugli 2000). Instead of feeling compelled to act out particular social roles (such as the sick role) either successfully or unsuccessfully, as discussed earlier (Osborn & Smith 1998, Steen & Haugli 2000), patients are enabled to participate in more constructive learning processes. For example, patients are enabled to begin to identify the effects of the problem (e.g. pain) on their lives rather than viewing themselves and their pain as inextricable entities (Orchison 1997, White & Epston 1990). We see this as part of ‘un-enmeshing’ the enmeshed schemata discussed above.
CONCLUSION
The increasing body of evidence demonstrating significant influences of psychosocial factors on patients’ pain and disability experiences has resulted in greater use of cognitive-behavioural approaches, particularly in therapies involved in the management of chronic pain and disability. However, the cognitive-behavioural approach has been criticized for its excessive focus on behavioural management, with a tendency for all patients with apparent psychosocial contributing factors to be treated as a single homogeneous group as though their cognitions, feelings and behaviours all had a similar basis that would be responsive to some generic application of cognitive-behavioural principles. Schemata and health representation theory provide some insight into how people structure their understanding of health, disability and pain which should discourage superficial approaches to the assessment and management of psychosocial factors. Cognitive-experiential learning represents a form of learning which utilizes reasoning processes from different paradigms of knowledge generation. To this extent we believe that it is a form of learning which expresses the underlying diverse scope of factors which influence and even ‘construct’ disability and which are, in turn, expressed in the WHO ICF model (2001) and the biopyschosocial model underpinning that (Imrie 2004). Cognitive-experiential learning has received more attention in terms of research in the field of adult learning than in health (Mezirow 2000). Our view expressed in this chapter is that cognitive-experiential learning holds significant promise in the area of persons learning to make constructive decisions regarding their health, particularly in situations of existing illness and the kinds of disability associated with chronic conditions. We have touched on chronic pain as one example of this. The measurement of outcomes from this type of learning related to patient decision making in health and disability remains a challenge for further research.
Argyris C, Schön D. Organizational learning: a theory in action perspective. Reading: Addison-Wesley, 1978.
Bishop GD. Understanding the understanding of illness: lay disease representations. In: Skelton JA, Croyle RT, editors. Mental representation in health and illness. New York: Springer-Verlag; 1991:32-59.
Borrell-Carrió F, Suchman AL, Epstein RM. The biopsychosocial model 25 years later: principles, practice, and scientific inquiry. Annals of Family Medicine. 2004;2(6):576-582.
Brookfield S. Clinical reasoning and generic thinking skills. In: Higgs J, Jones M, editors. Clinical reasoning in the health professions. 2nd edn. Oxford: Butterworth-Heinemann; 2000:62-67.
Craig KD. Emotions and psychobiology. In: McMahon S, Koltzenburg M, editors. Wall and Melzack’s textbook of pain. 5th edn. Philadelphia: Elsevier; 2006:231-239.
Cusick A. Personal frames of reference in professional practice. In: Higgs J, Titchen A, editors. Practice knowledge and expertise in the health professions. Oxford: Butterworth-Heinemann; 2001:91-95.
Duncan G. Mind-body dualism and the biopsychosocial model of pain: what did Descartes really say? Journal of Medicine and Philosophy. 2000;25:485-513.
Edwards I, Jones MA, Hillier S. The interpretation of experience and its relationship to body movement: a clinical reasoning perspective. Manual Therapy. 2006;11:2-10.
Engel GL. The need for a new medical model: a challenge for biomedicine. Science. 1977;196:129-136.
Engel G. The biopsychosocial model and the education of health professionals. Annals New York Academy of Sciences. 1978;310:535-544.
Fields HL, Basbaum AI, Heinricher MM. Central nervous system mechanisms of pain modulation. In: McMahon S, Koltzenburg M, editors. Wall and Melzack’s textbook of pain. 5th edn. Philadelphia: Elsevier; 2006:125-142.
Flor H, Turk DC. Cognitive and learning aspects. In: McMahon S, Koltzenburg M, editors. Wall and Melzack’s textbook of pain. 5th edn. Philadelphia: Elsevier; 2006:241-258.
Gamsa A. The role of psychological factors in chronic pain. I. A half century of study. Pain. 1994;57:5-15.
Gamsa A. The role of psychological factors in chronic pain. II. A critical appraisal. Pain. 1994;57:17-29.
Geertz C. The interpretation of cultures. New York: Basic Books, 1973.
Germov J. Imagining health problems as social issues. In: Germov J, editor. Second opinion - an introduction to health sociology. 3rd edn. Oxford: Oxford University Press; 2005:3-27.
Gifford L, Thacker M, Jones MA. Physiotherapy and pain. In: McMahon S, Koltzenburg M, editors. Wall and Melzack’s textbook of pain. 5th edn. Philadelphia: Elsevier; 2006:603-617.
Gottlieb A, Golander H, Bar-Tal Y, et al. The influence of social support and perceived control on handicap and quality of life after stroke. Aging Clinical Experimental Research. 2001;13:11-15.
Gray D, Saggers S. Indigenous health: the perpetuation of inequality. In: Germov J, editor. Second opinion - an introduction to health sociology. 3rd edn. Oxford: Oxford University Press; 2005:111-128.
Harding V. Cognitive-behavioural approach to fear and avoidance. In: Gifford L, editor. Topical issues in pain 1. Falmouth: CNS Press; 1998:173-191.
Higgs C, Neubauer D, Higgs J. The changing health care context: globalization and social ecology. In: Higgs J, Edwards H, editors. Educating beginning practitioners: challenges for health professional education. Oxford: Butterworth-Heinemann; 1999:30-37.
Hooper B. The relationship between pretheoretical assumptions and clinical reasoning. American Journal of Occupational Therapy. 1997;51(5):328-338.
Imrie R. Demystifying disability: a review of the International Classification of Functioning, Disability and Health. Sociology of Health and Illness. 2004;26(3):287-305.
Jensen GM, Gwyer J, Shepard KF, et al. Expert practice in physical therapy. Physical Therapy. 2000;80(1):28-43.
Johnson R, Moores L. Pain management: integrating physiotherapy and clinical psychology. In: Gifford L, editor. Topical issues in pain 5. Falmouth: CNS Press; 2006:311-319.
Jones MA, Edwards I. Learning to facilitate change in cognition and behaviour. In: Gifford L, editor. Topical issues in pain 5. Falmouth: CNS Press; 2006:273-310.
Jorgensen P. Concepts of body and health in physiotherapy: the meaning of the social/cultural aspects of life. Physiotherapy Theory and Practice. 2000;16(2):105-115.
Keefe F, Scipio C, Perri L. Psychosocial approaches to managing pain: current status and future directions. In: Gifford L, editor. Topical issues in pain 5. Falmouth: CNS Press; 2006:241-256.
Kendall N, Watson P. Identifying psychosocial yellow flags and modifying management. In: Gifford L, editor. Topical issues of pain 2. Falmouth: CNS Press; 2000:131-139.
King G, Tucker MA, Baldwin P, et al. A life needs model of pediatric service delivery: services to support community participation and quality of life for children and youth with disabilities. Physical and Occupational Therapy in Pediatrics. 2002;22(2):53-77.
Kleinman A, Brodwin PE, Good BJ, et al. Pain as human experience: an introduction. In: Good MJD, Brodwin PE, Good BJ, Kleinman A, editors. Pain as human experience: an anthropological perspective. Berkeley: University of California Press; 1992:1-28.
Leventhal H, Meyer D, Nerenz D. The common sense representation of illness danger. Rachman S, editor. Contributions to medical psychology,, vol 2. New York: Pergamon Press. 1980:7-30.
Main C, Watson P. The distressed and angry low back pain patient. In: Gifford L, editor. Topical issues in pain 3. Falmouth: CNS Press; 2002:175-192.
Main CJ, Spanswick CC, Watson P. The nature of disability. In: Main CJ, Spanswick CC, editors. Pain management: an interdisciplinary approach. Edinburgh: Churchill Livingstone; 2000:89-106.
Mattingly C, Fleming MH. Clinical reasoning: forms of inquiry in a therapeutic practice. Philadelphia: F A Davis, 1994.
Mezirow J. Transformative dimensions of adult learning. San Francisco: Jossey-Bass, 1991.
Mezirow J. Learning to think like an adult: core concepts of transformation theory. In: Mezirow J, editor. Learning as transformation: critical perspectives on a theory in progress. San Francisco: Jossey-Bass; 2000:3-33.
Morley S, Eccleston C, Williams A. Systematic review and meta-analysis of randomized controlled trials of cognitive behaviour therapy and behaviour therapy for chronic pain in adults, excluding headache. Pain. 1999;80:1-13.
Muncey H. Explaining pain to patients. In: Gifford LS, editor. Topical issues in pain 4. Falmouth: CNS Press; 2002:157-166.
Orchison R. From pain-full narratives to pain-less lives., 4. Adelaide: Dulwich Centre Newsletter. 1997:31-35.
Osborn M, Smith JA. The personal experience of chronic benign lower back pain: an interpretative phenomenological analysis. British Journal of Health Psychology. 1998;3:65-83.
Payton OD, Nelson CE, Hobbs MSC. Physical therapy patients’ perceptions of their relationships with health care professionals. Physiotherapy Theory and Practice. 1998;14:211-221.
Phillips HC. Avoidance behaviour and its role in sustaining chronic pain. Behaviour Research and Therapy. 1987;25:273-279.
Pincus T. The psychology of pain. In: French S, Sim J, editors. Physiotherapy: a psychosocial approach. Edinburgh: Elsevier; 2004:95-115.
Pincus T, Morley S. Cognitive-processing bias in chronic pain: a review and integration. Psychological Bulletin. 2001;127:599-617.
Sharp TJ. Chronic pain: a reformulation of the cognitive-behavioural model. Behaviour Research and Therapy. 2001;39:787-800.
Sim J, Smith MV. The sociology of pain. In: French S, Sim J, editors. Physiotherapy: a psychosocial approach. Edinburgh: Elsevier; 2004:117-139.
Skelton JA, Croyle RT. Mental representation, health, and illness: an introduction. In: Skelton JA, Croyle RT, editors. Mental representation in health and illness. New York: Springer-Verlag; 1991:1-9.
Steen E, Haugli L. Generalised chronic musculoskeletal pain as a rational reaction to a life situation? Theoretical Medicine. 2000;21:581-599.
Strong J, Unruh AM. Psychologically based pain management strategies. In: Strong J, Unruh AM, Wright A, Baxter GD, editors. Pain: a textbook for therapists. Edinburgh: Churchill Livingstone; 2002:169-185.
Turk D, Flor H. The cognitive-behavioural approach to pain management. In: McMahon S, Koltzenburg M, editors. Wall and Melzack’s textbook of pain. 5th edn. Philadelphia: Elsevier; 2006:339-348.
Unsworth CA. Clinical reasoning: how do pragmatic reasoning, worldview and client-centredness fit? British Journal of Occupational Therapy. 2004;67(1):10-19.
Waddell G. A new clinical model for the treatment of low back pain. Spine. 1987;12:632-644.
Waddell G. The back pain revolution, 2nd edn. Edinburgh: Churchill Livingstone, 2004.
White M, Epston D. Narrative means to therapeutic ends. New York: W W Norton, 1990.
World Health Organization. International classification of functioning, disability and health. Geneva: World Health Organization, 2001.