Neurological Care Plans
Alzheimer’s Disease/Dementia
 For additional care plans, go to http://evolve.elsevier.com/Gulanick/.
For additional care plans, go to http://evolve.elsevier.com/Gulanick/.
Multi-infarct Dementia (MID); Dementia of the Alzheimer Type (DAT)
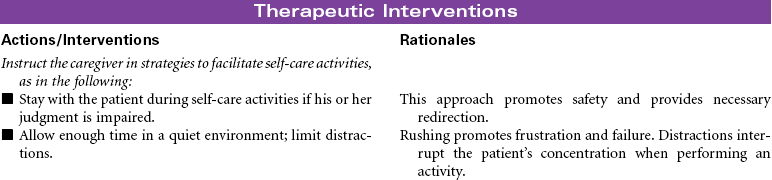
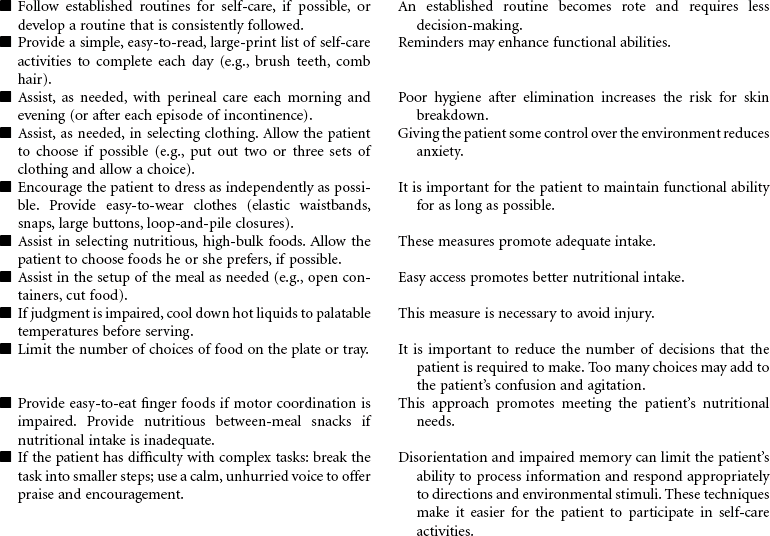
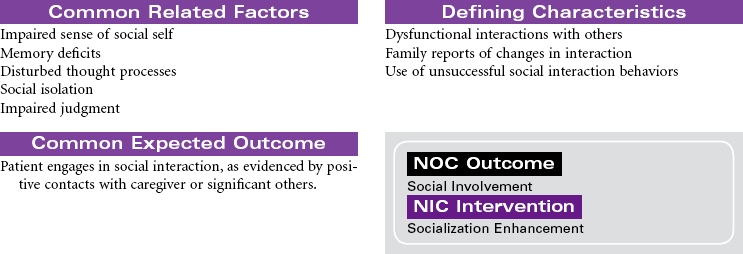
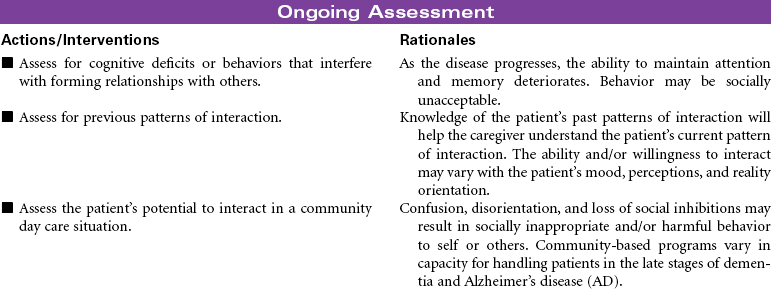
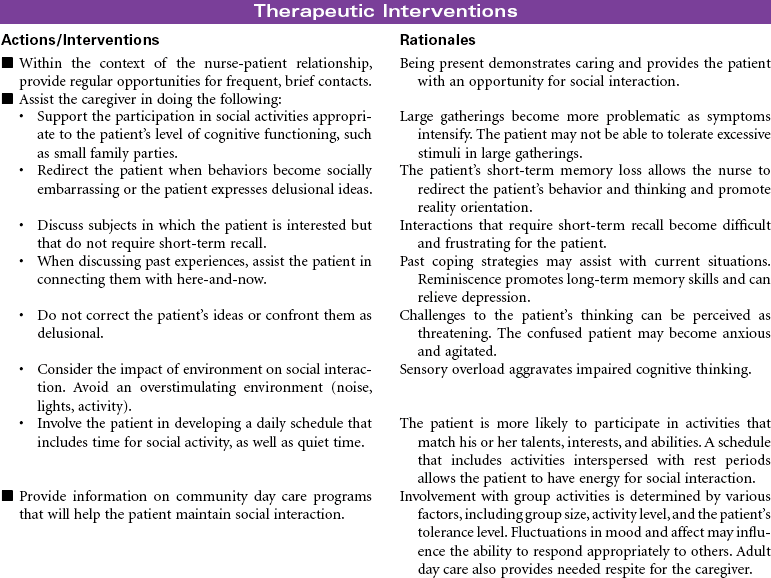
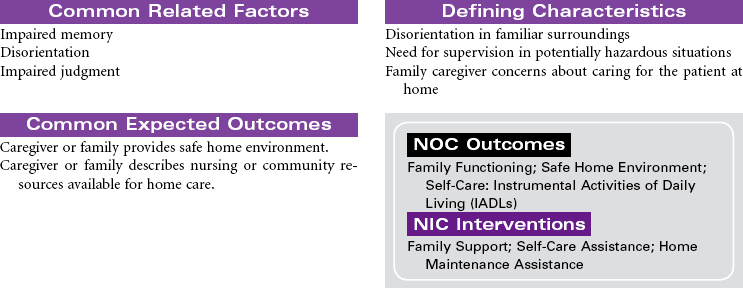
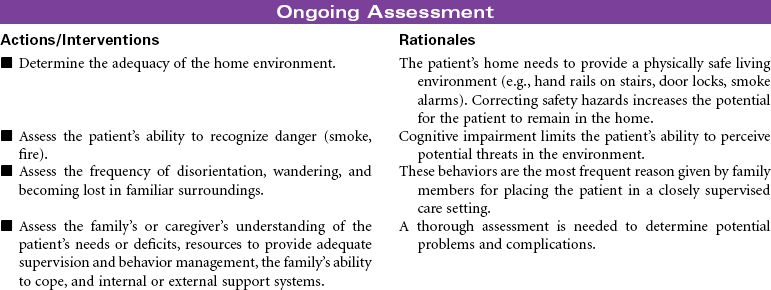
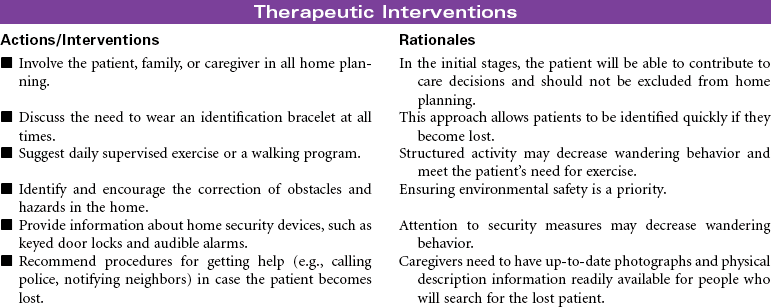
Dementia is characterized by a progressive impairment of cognitive function, personality, and behavior. The person with dementia experiences loss of memory, disorientation, impaired language skills, decreased concentration, and impaired judgment. In advanced stages, the person experiences behavior and personality changes such as aggressiveness, mood swings, wandering, and confusion. These changes interfere with the person’s ability to carry out role responsibilities and activities of daily living. The causes of dementia are numerous and include degenerative disorders of the nervous system, vascular disorders, autoimmune disorders, and traumatic brain injury such as concussions. Multi-infarct dementia develops in people who have sustained brain injury from multiple strokes. This type of irreversible dementia occurs more often in men than women. People in the later stages of acquired immunodeficiency syndrome (AIDS) may develop dementia. Alcoholism and Parkinson’s disease are known to contribute to dementia.
Alzheimer’s disease (AD) is an irreversible disease of the central nervous system that manifests as a cognitive disorder. Onset is usually between 50 and 60 years and is characterized by progressive deterioration of memory and cognitive function. Disease progression begins with memory impairment, speech and motor difficulties, disorientation of time and place, impaired judgment, memory loss, forgetfulness, and inappropriate affect, followed by loss of independence, complete disorientation, wandering, hoarding, communication difficulties, complete memory loss, and the final stage with blank expression, irritability, seizures, emaciation, and absolute dependence until death.
Although the cause is unknown, research has found specific genetic loci associated with the development of AD. Chronic inflammation, stroke, and cellular damage from free radicals have been identified as risk factors for AD. Drug therapy for AD includes cholinesterase inhibitors and n-methyl-d-aspartate (NMDA) antagonists. These drugs have been shown to delay the progression of cognitive impairment. Some patients may experience improved memory function with these drugs.
This care plan addresses needs for patients with a wide variety of dementia, of which Alzheimer’s is a type. Focus is on the home care setting.
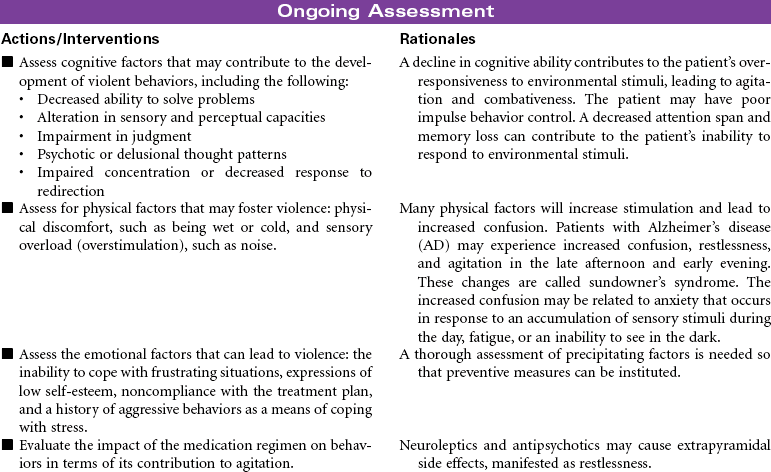
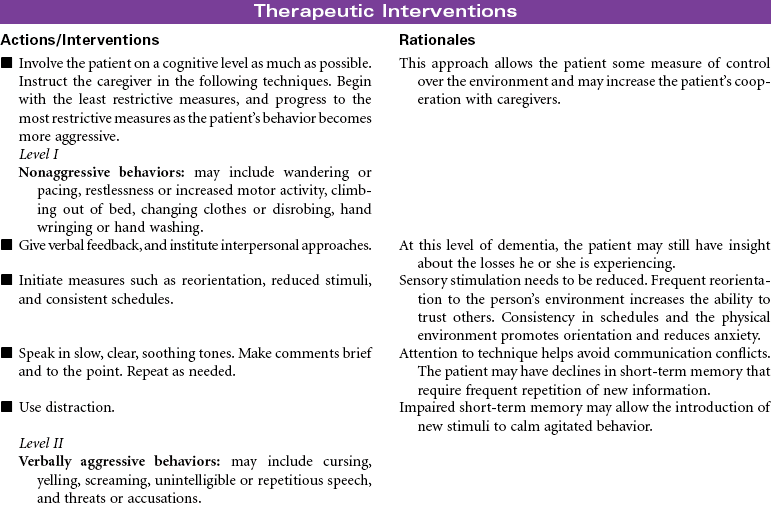
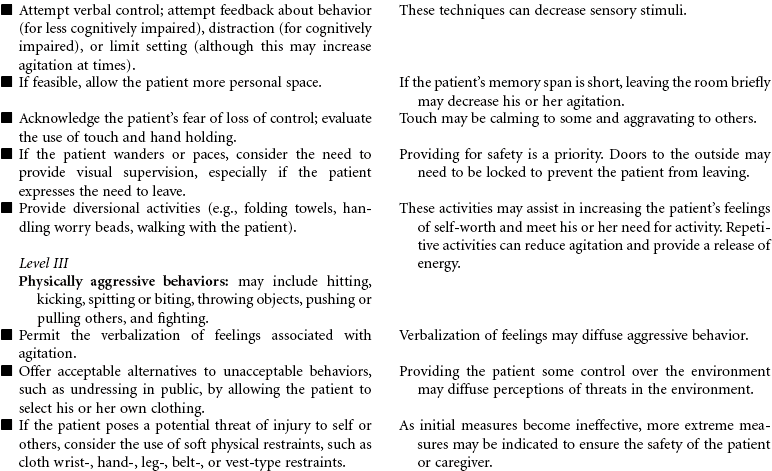
 Risk for Violence: Self-Directed or Other-Directed
Risk for Violence: Self-Directed or Other-Directed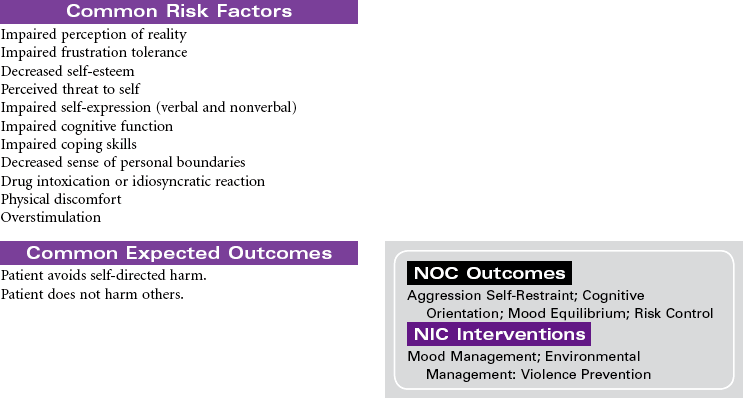


Amyotrophic Lateral Sclerosis
Lou Gehrig’s Disease; Motor Neuron Disease; Progressive Bulbar Palsy; Progressive Muscular Atrophy
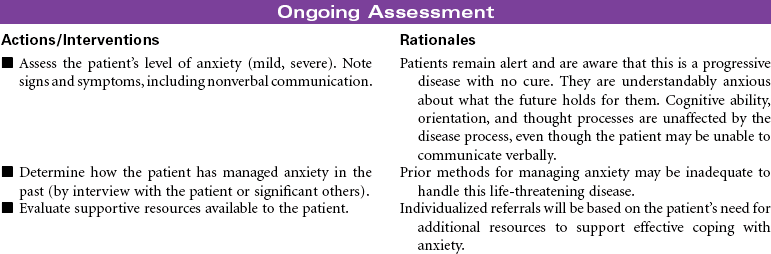
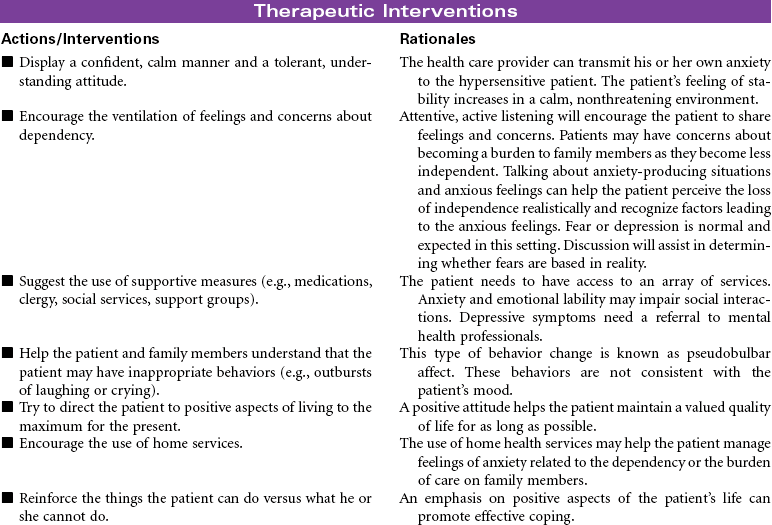
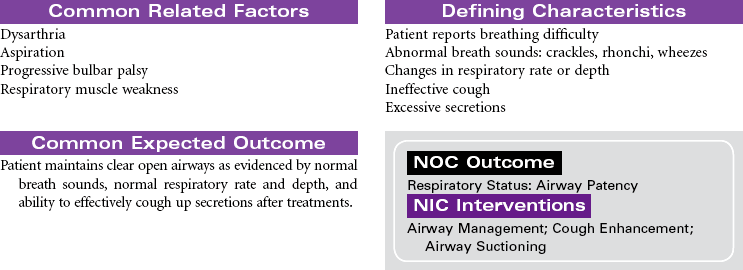
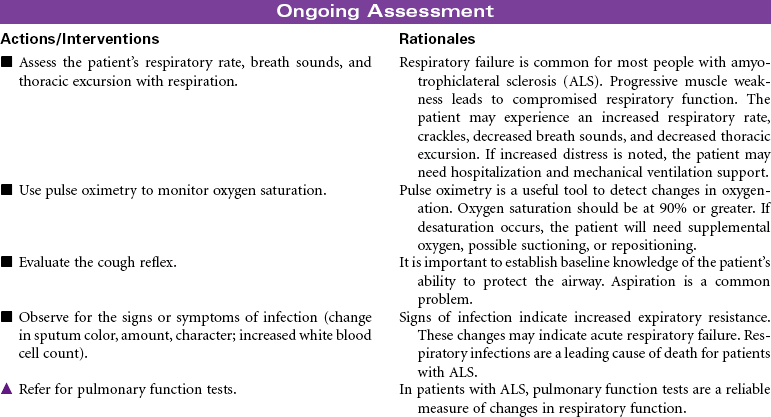
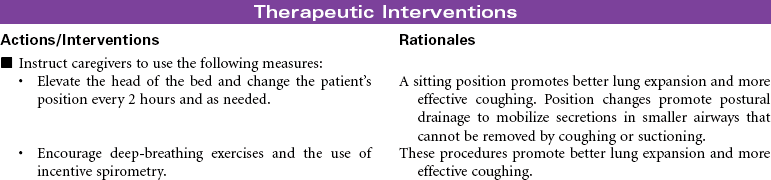
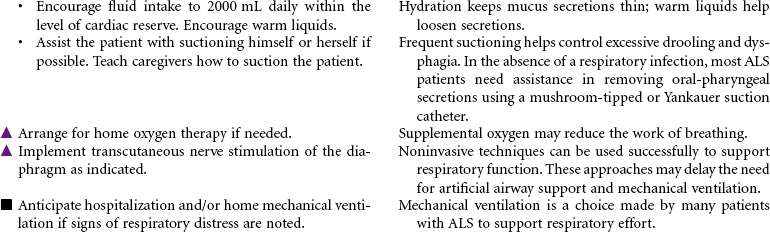
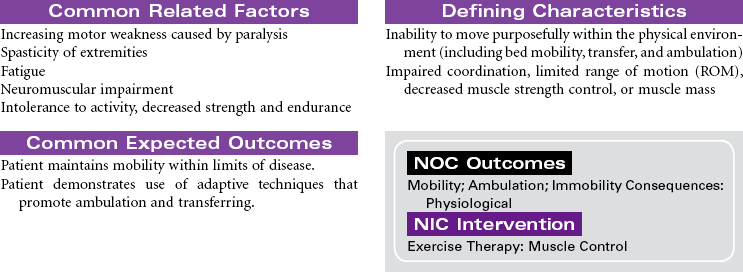
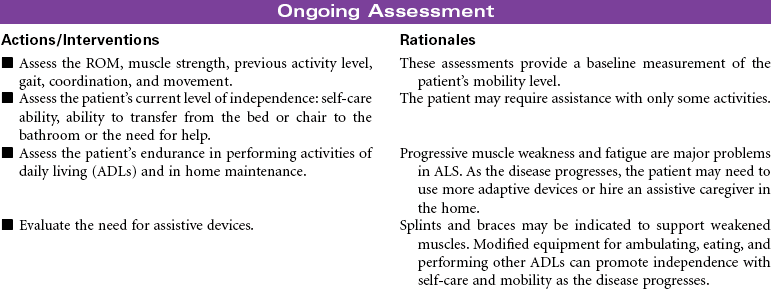
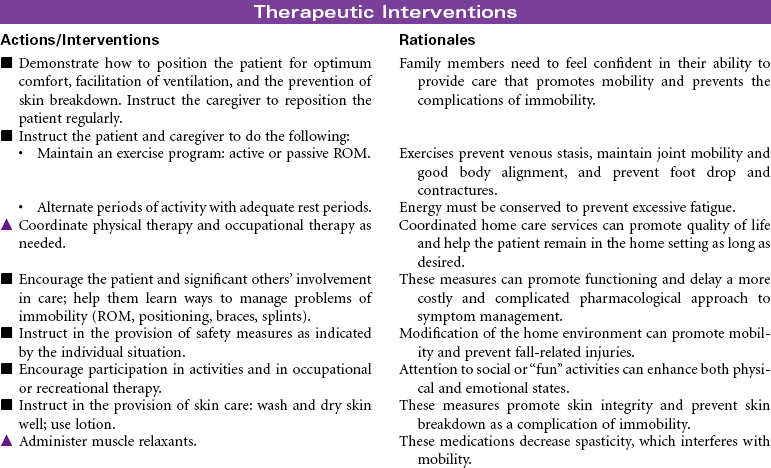
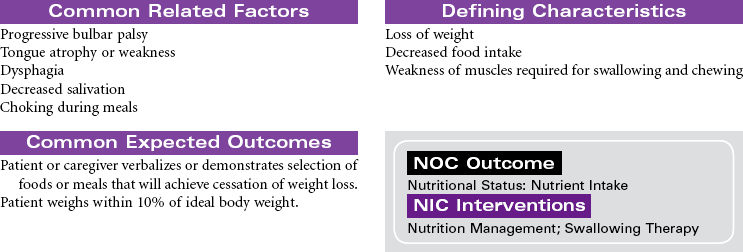
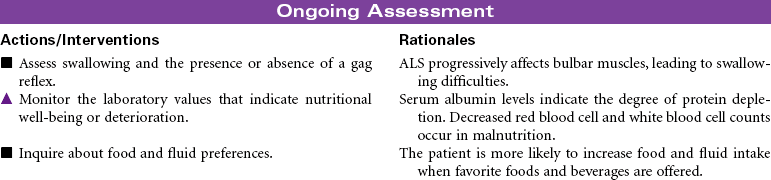
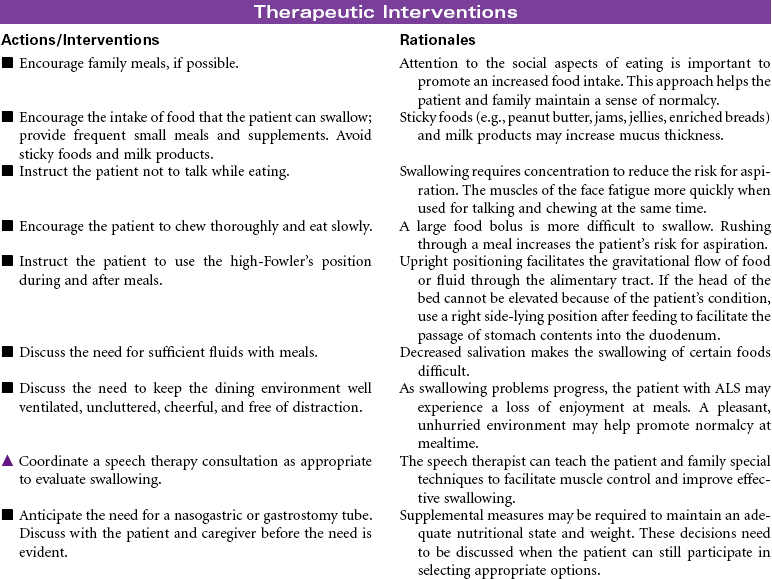
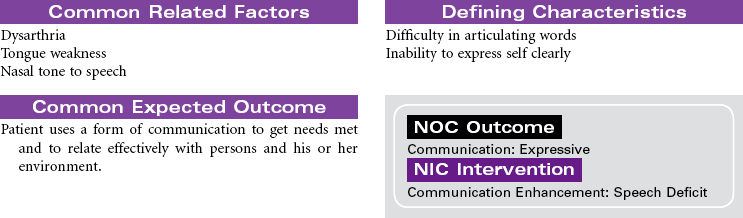
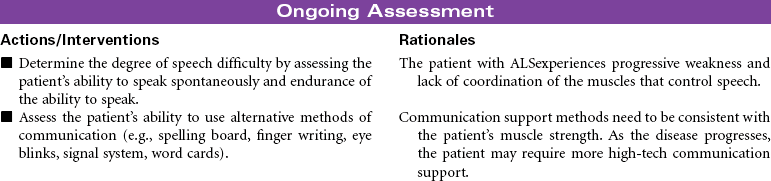
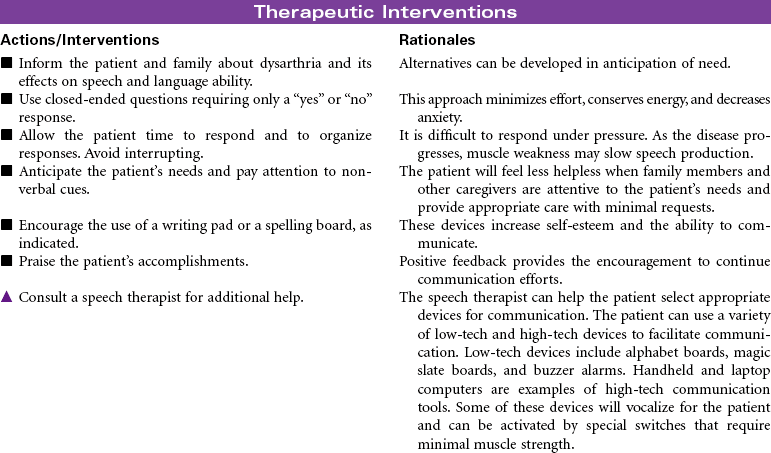
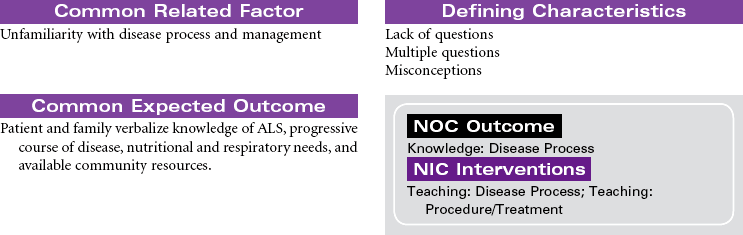
Amyotrophic lateral sclerosis (ALS), commonly called Lou Gehrig’s disease, is a rare progressive disease that attacks motor neurons, which control the movement of muscles through the anterior horns of the spinal cord and the motor nuclei of the lower brainstem. Onset is usually between 40 and 70 years of age, with men affected twice as often as women. Signs and symptoms of the disease begin with atrophic weakness of the hands and forearms in the early phase of the disease. As loss of motor neuron function progresses, the patient will develop mild lower extremity spasticity and diffuse hyperreflexia. Impaired respiratory function is present in the later phases of the disease, often requiring mechanical ventilatory support. Sensation and sphincter control are usually maintained. When the bulbar muscles are affected, dysarthria and dysphagia are seen with fasciculations in the tongue. The challenge for the patient with ALS is that awareness and cognitive function remain intact throughout the progression of the disease. There is usually progressive paralysis, with death occurring within 2 to 6 years. This care plan focuses on home care, where the patient usually remains until care needs are no longer manageable.

 = Independent
= Independent  = Collaborative
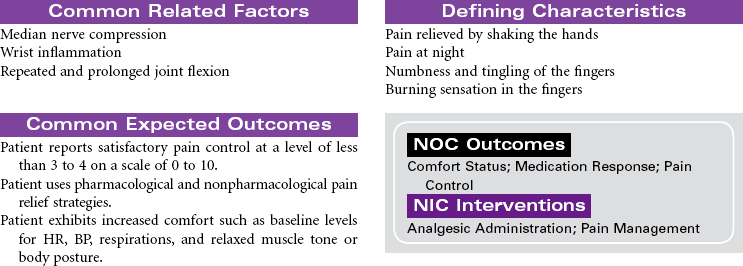
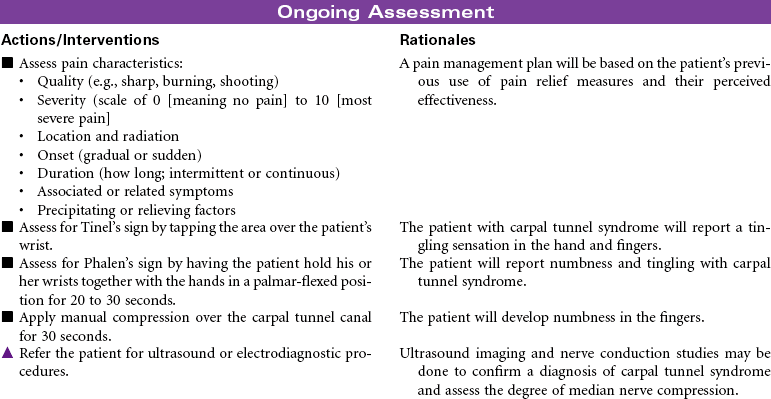
= CollaborativeCarpal Tunnel Syndrome
Repetitive Stress Injury; Median Nerve Compression
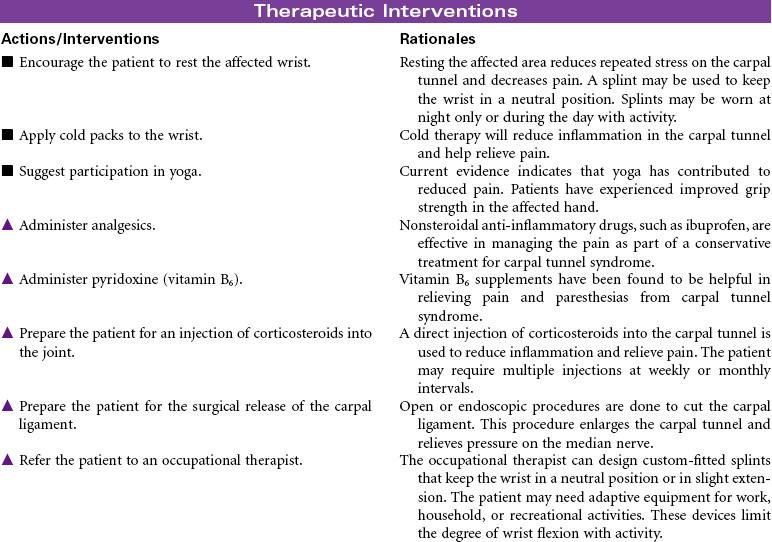
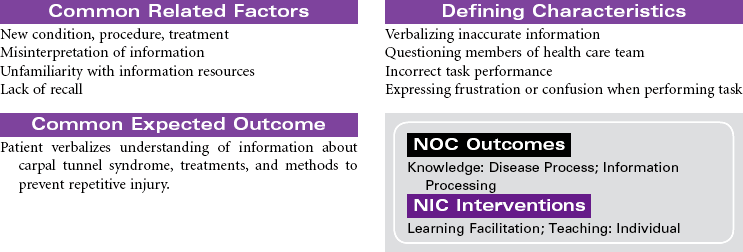
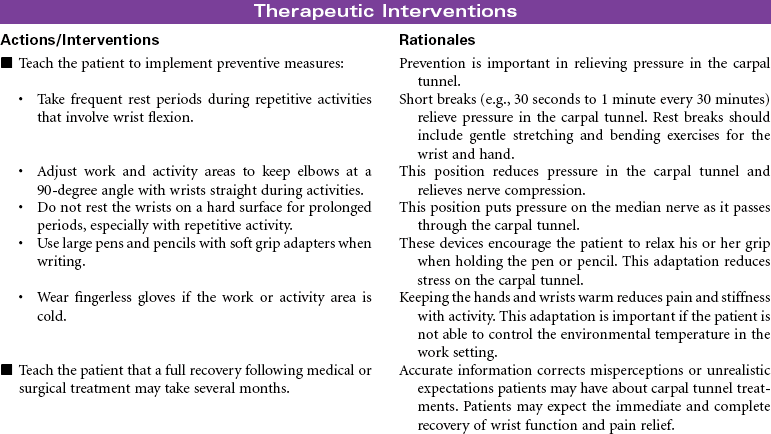
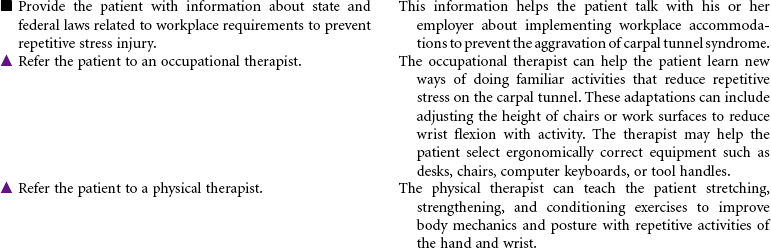
Carpal tunnel syndrome develops when the median nerve is compressed as it passes through the wrist to the hand. The carpal tunnel is an anatomical canal that is located between the bones of the hand and a band of fibrous tissue. This tissue protects the tendons of the wrist during movement of the joint. Inflammation of the synovium of the joint causes swelling, pain, and paresthesia. The swelling contributes to narrowing of the tunnel and compression of the median nerve. The pain and paresthesia occurs most often in the thumb, index finger, middle finger, and radial aspect of the ring finger. Chronic median nerve compression may lead to progressive weakness and loss of fine motor control in the hand. Muscle atrophy may develop over time. This disorder has a high prevalence among people in occupations that involve repeated and prolonged flexion of the wrist. Carpal tunnel syndrome is becoming a common occupational repetitive stress injury. Other situations that are known to contribute to carpal tunnel syndrome include burn injuries of the hand, wrist fractures, rheumatoid arthritis, and diabetes mellitus. Women are more likely to develop carpal tunnel syndrome than men. This gender difference is thought to be related to the smaller size of the carpal tunnel in women. Medical management of carpal tunnel syndrome includes splinting of the joint, drug therapy to reduce inflammation and pain, and modification of activities to restrict harmful movement. Surgery is done when prolonged nerve compression is severe and associated with muscle atrophy and progressive loss of motor and sensory function.

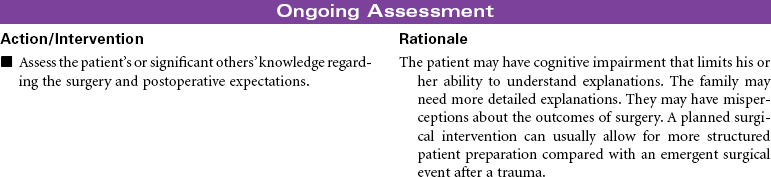
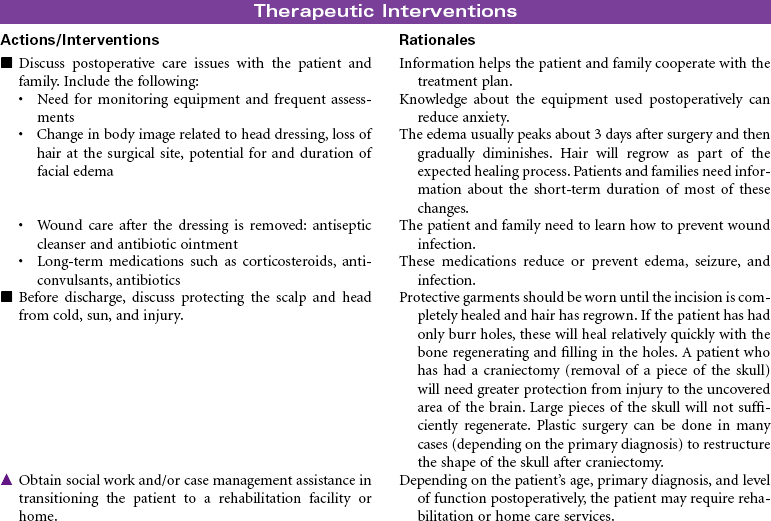
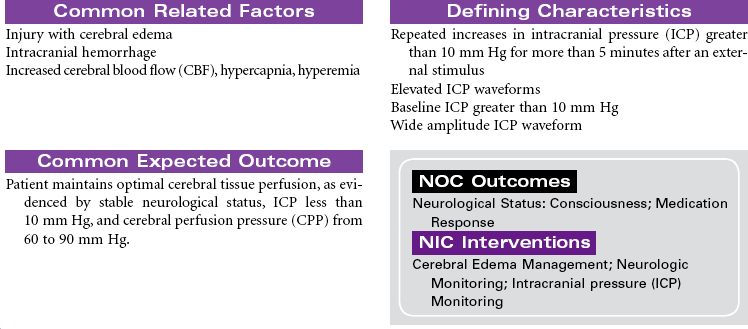
Craniotomy
Craniectomy; Burr Hole; Cranioplasty; Cranial Surgery
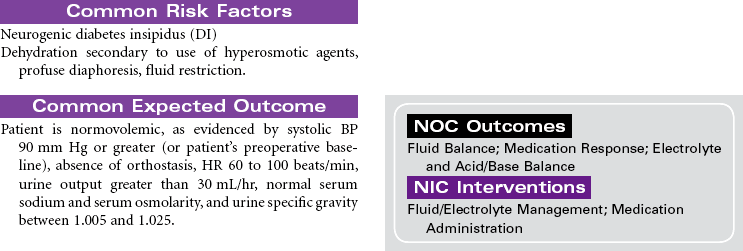
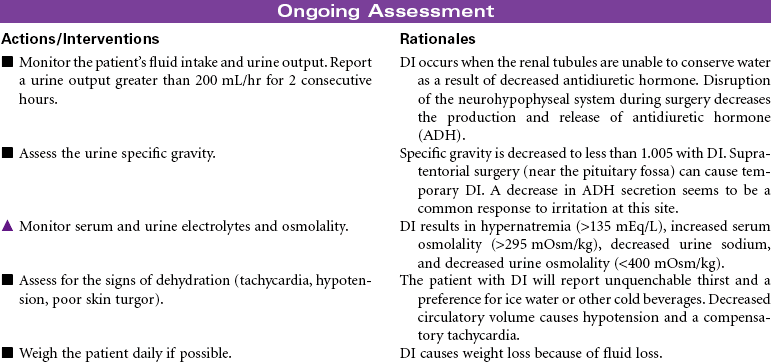
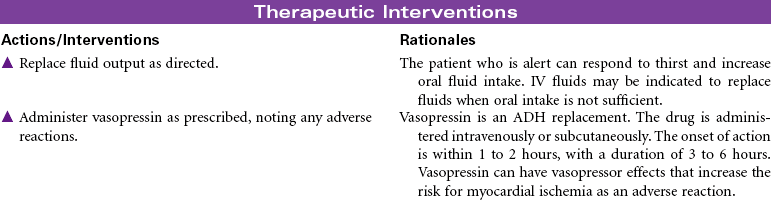
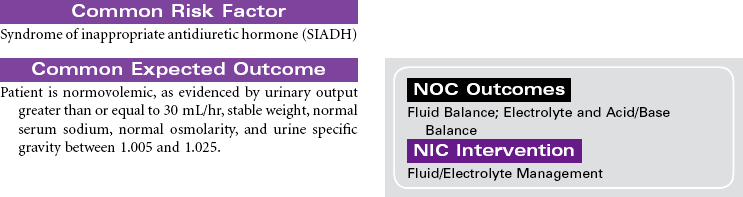
Craniotomy is the surgical opening of the cranium to gain access to disease or injury affecting the brain, ventricles, or intracranial blood vessels. Craniectomy involves removal of part of the cranium to treat compound fractures, infection, or decompression. Burr holes are drilled in the cranium and used for clot evacuation and decompression of fluid beneath the dura or in preparation for craniotomy. Cranioplasty is the application of artificial material to repair the skull to improve integrity and shape. Cranial surgery is either supratentorial (above the tentorium, involving the cerebrum) or infratentorial (below the tentorium, involving the brainstem or cerebellum).
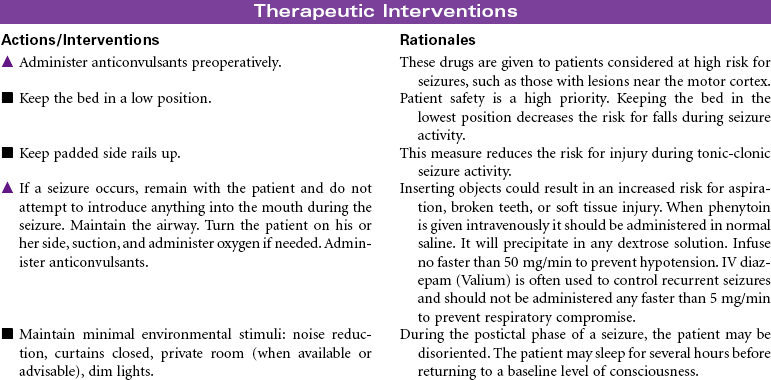
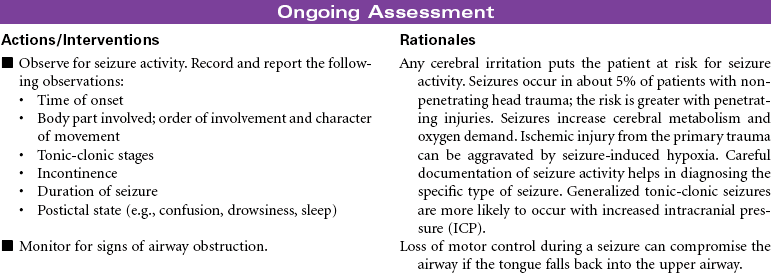
 Risk for Seizures
Risk for Seizures




Head Trauma
Traumatic Brain Injury; Closed Trauma; Skull Fracture; Subdural Hematoma; Concussion
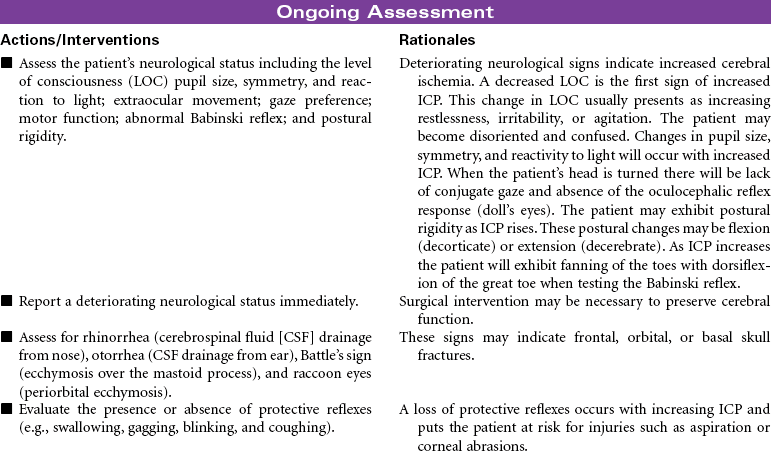
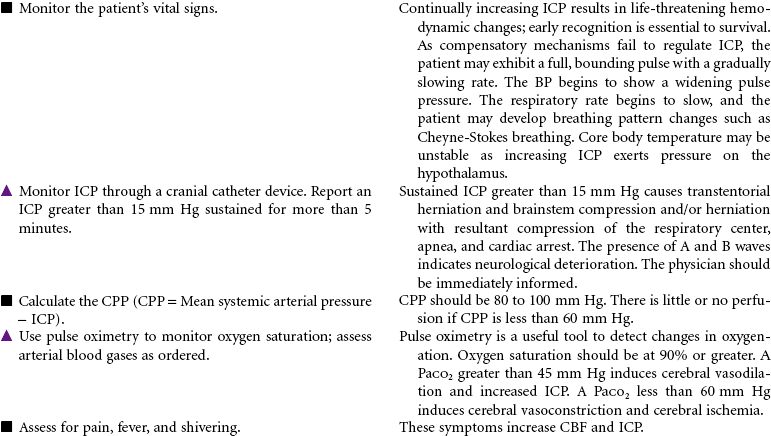
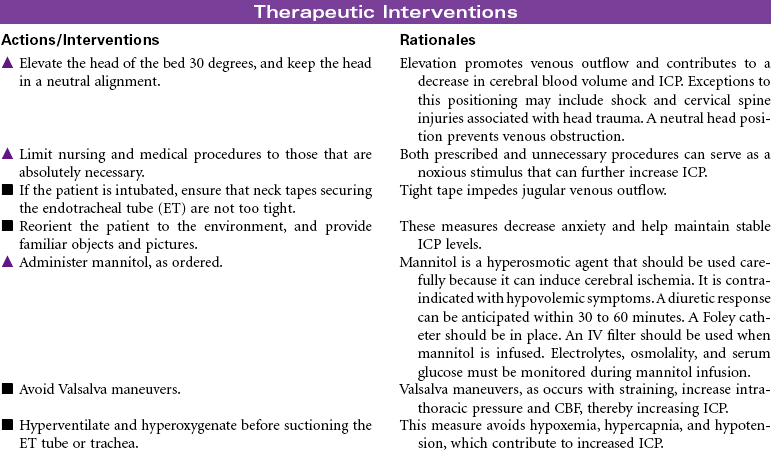
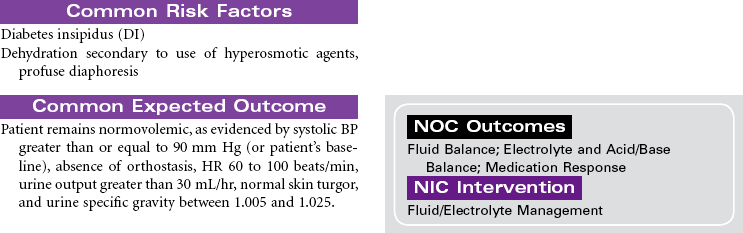
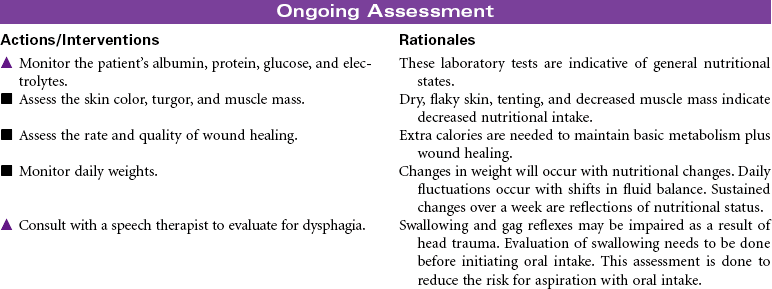
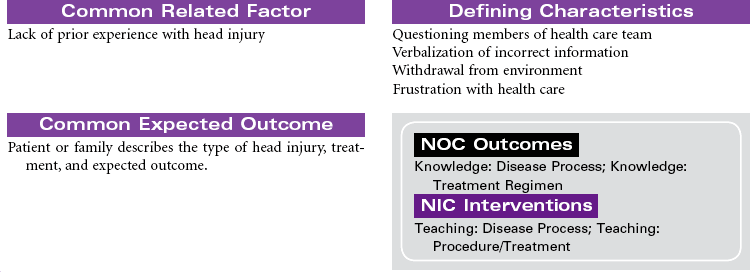
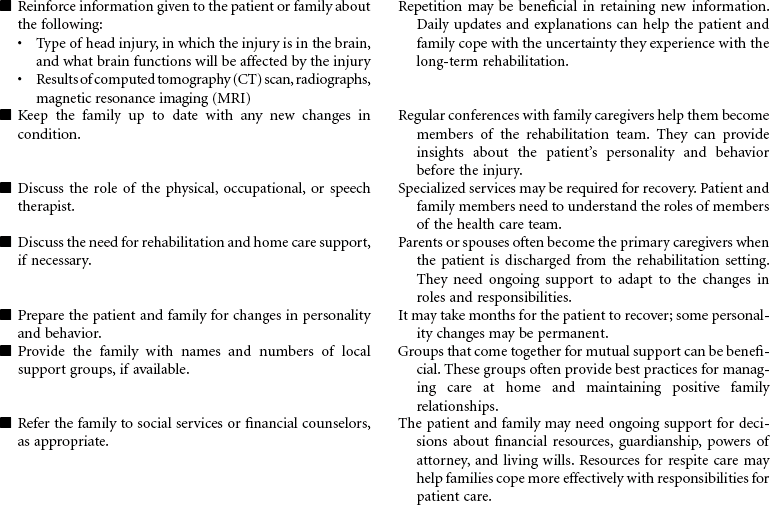
Head injury (craniocerebral trauma) is a leading cause of death in the United States for people 1 to 42 years of age. An estimated 3 million people suffer head injuries every year. About half of all severe head injuries result from accidents involving automobiles, motorcycles, bicycles, and pedestrians. People who do not use appropriate safety equipment (e.g., seat belts, helmets) have a significant increase in head injury with accidents. Approximately 20% of head injuries are associated with violence, such as blunt force trauma and firearms. Recent evidence identifies traumatic brain injury from concussions sustained by athletes playing contact sports and military personnel during combat. The severity of the head injury is defined by the traumatic coma data bank on the basis of the Glasgow Coma Scale (GCS): Severe head injury = GCS of 8 or less; moderate head injury = GCS of 9 to 12. Most head injuries are blunt (closed) trauma to the brain. Damage to the scalp, skull, meninges, and brain runs the gamut of skull fracture with loss of consciousness, concussion, and/or extracerebral or intracerebral pathological conditions. Patients with moderate to severe head trauma are usually observed in a critical care unit where immediate intervention can be achieved. Most deaths occur in the first few hours after head trauma as a result of internal bleeding or worsening cerebral edema. Patients with minor head trauma (scalp laceration or concussion) are most often treated and released to be observed at home with instructions to call or return if symptoms worsen. Older people are most often affected with postconcussion syndrome, characterized by decreased neurological function 2 weeks to 2 months after the initial injury and often caused by a slow subdural bleed. This care plan focuses on moderate-to-severe head trauma in the acute care setting.





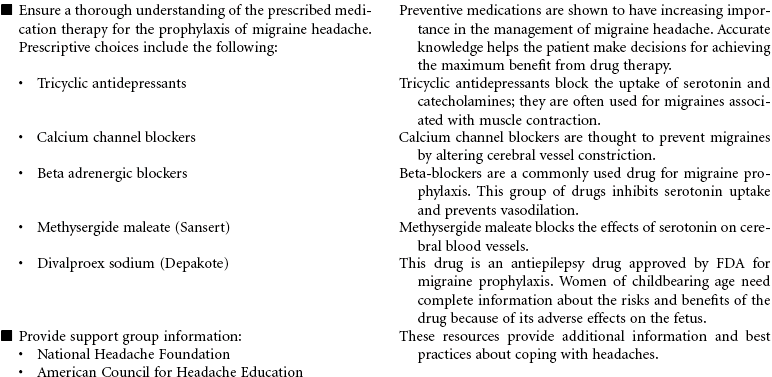
Headache: Migraine, Cluster, Tension
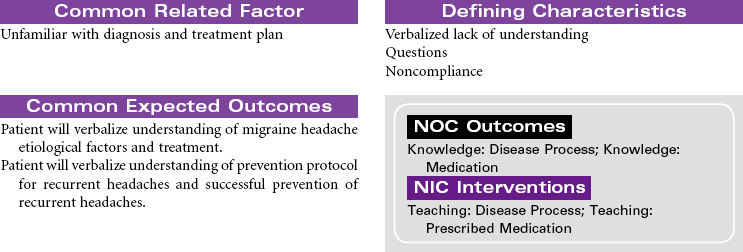
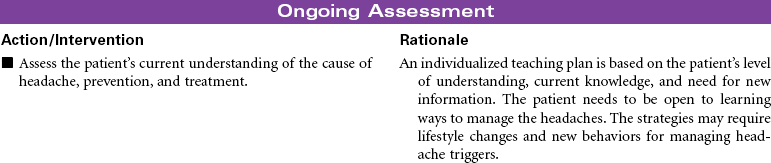
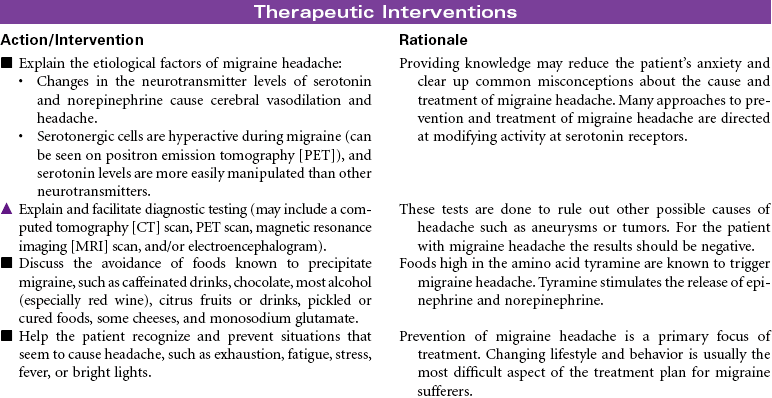
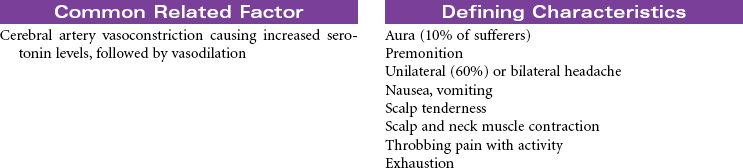
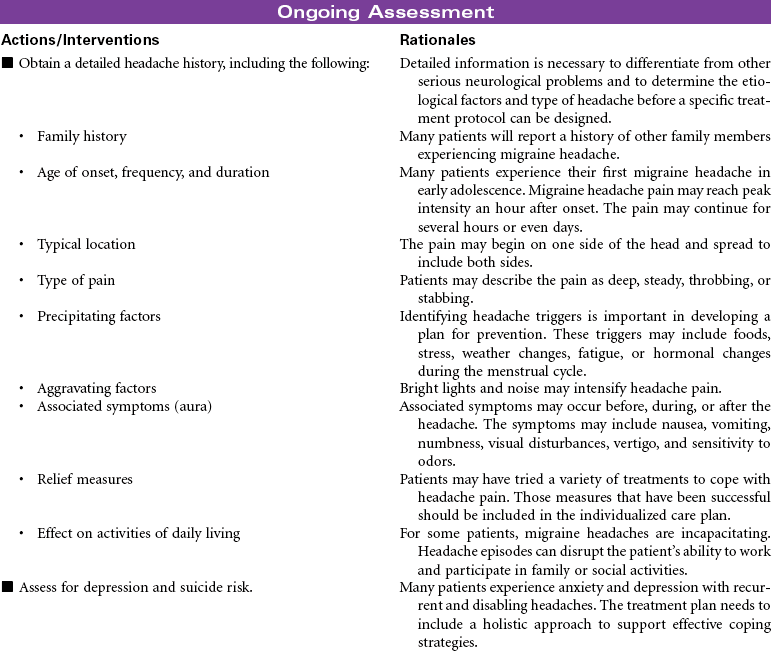
Headache is defined as pain in the head or face, classified as either “primary” or “secondary” in origin. Migraine, cluster, and tension headaches are classified as primary because the pain occurs without a known pathological cause. Secondary headaches are a result of a known pathology, such as cranial tumor or aneurysm. Migraine headache, a recurring unilateral or bilateral headache, is the most common type of vascular headache. Multiple theories have been proposed to explain the cause of migraine headache. Evidence suggests that muscle tension, changes in cerebrovascular tone, and biochemical factors are involved in producing the pain of a migraine headache. Women are affected three times more often than men. Migraines may begin in early childhood and adolescence, and 65% of patients with migraine headaches have a family history of migraine headache. Migraines may occur with an aura or without. The aura is a collection of neurological symptoms that precede the onset of pain by 10 to 30 minutes. These symptoms include changes in level of consciousness, vision, behavior, and motor or sensory function. Many patients develop a migraine headache without a precipitating event. For other patients a variety of precipitating events trigger migraine headaches, including stress, foods high in tyramine, hunger, sleep disturbances, and for women, alterations in reproductive hormone levels. Manifestations are associated with autonomic nervous system dysfunction.
Tension headaches are the most common form of headache, occurring in women more often than men. The usual age of onset is 20 to 25 years old. The pain is usually mild to moderate and described as a tightening or sensation of pressure around the head. This type of headache is believed to be related to muscle tension in the jaw and neck with hypersensitivity of pain fibers in the trigeminal nerve. The exact mechanisms for the pain are unknown. Many patients may experience both migraine and tension headaches.
Cluster headaches are defined as pain episodes that occur for several days or weeks at a time followed by long periods of remission. The person may experience several short headaches in one day. Men are affected more often than women, with the age of occurrence between 20 and 50 years old. The pain is described as severe, with tearing, burning, and reddening of the eye on one side of the face. The mechanisms of cluster headaches are thought to be similar to those causing migraine headaches. The exact mechanisms remain unknown but may include vascular and neurogenic alterations of the hypothalamus associated with changes in serotonin transmission.
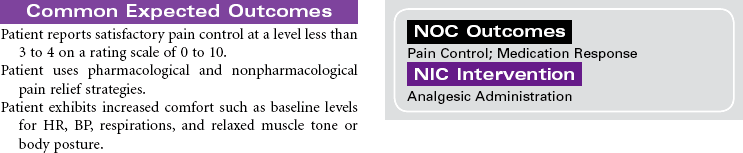
This care plan focuses on the classic migraine, which is believed to be a dysfunction of the hypothalamic and upper brainstem areas. Diagnosis, treatment, and follow-up care are usually accomplished in an outpatient setting.

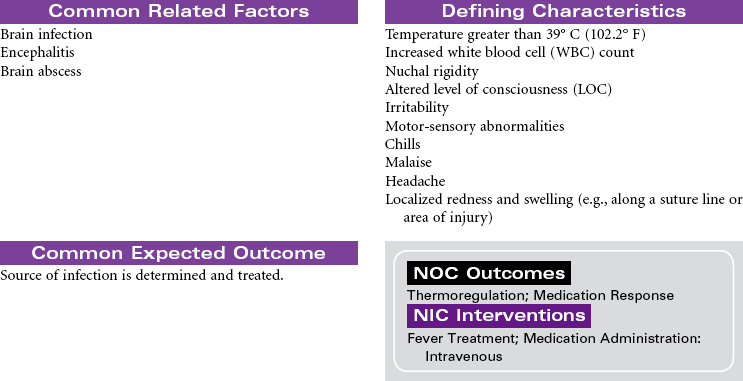
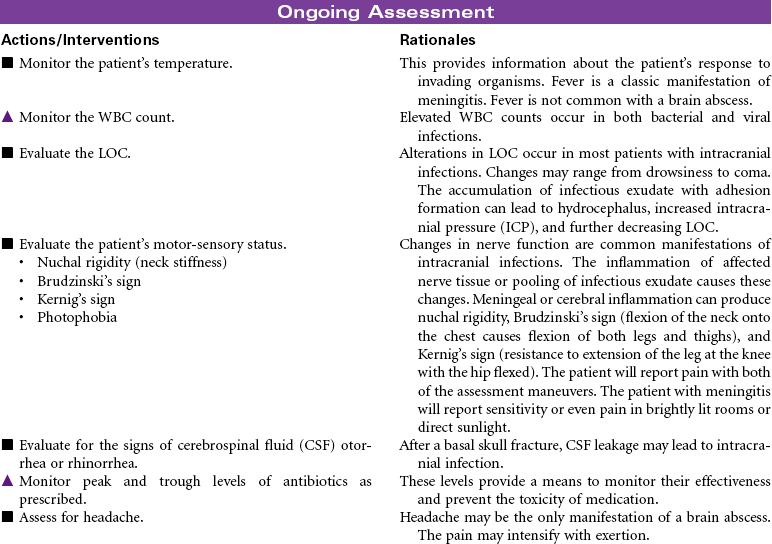
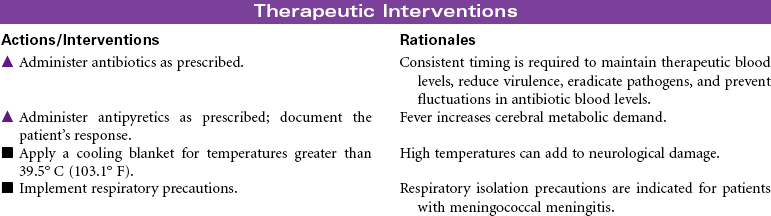
Intracranial Infection
Meningitis; Encephalitis; Brain Abscess,
Intracranial infection may be the result of meningitis, encephalitis, or brain abscess. The clinical manifestations of these intracranial infections are similar. Meningitis is an inflammation or infection of the membranes of the brain or spinal cord caused by bacteria, viruses, or other organisms. Bacterial meningitis is the most common form of the disorder. The infecting bacteria are often found in the nasopharynx and can be transmitted by sneezing or coughing. Pneumococcal meningitis is often secondary to pneumonia, sinusitis, alcoholism, and trauma (e.g., a basal skull fracture). The causative bacteria is Streptococcus pneumoniae. Meningococcal meningitis is caused by Neisseria meningitides. This form of meningitis is more common in children and young adults. Factors contributing to infection with meningitis include poor hygiene, high-density living arrangements, and inadequate nutrition. Meningitis may occur as a complication of infection with Haemophilis influenzae. Epidemics are seen in winter and spring months. Immunizations are available for both forms of meningitis. Antibiotic therapy is required. Viral illnesses are treated symptomatically. Viral meningitis is more likely to occur in summer months. Hydrocephalus often occurs secondary to viral meningitis.
Encephalitis is an inflammation or infection of the brain and meninges. The highest mortality rate is caused by herpes simplex virus (HSV), which is the most common form. An abscess is a localized purulent collection in the brain. Direct causes are a result of extension of infections from the ear, tooth, mastoid, or sinus. Indirect causes include bacterial endocarditis, skull fracture, or nonsterile procedures. Hospitalization is usually required for differential diagnosis, neurological monitoring, and treatment. When the infection does not respond to antibiotic therapy, the abscess may need surgical drainage.


Low Back Pain/Herniated Intervertebral Disk
Slipped Disk; Ruptured Disk; Sciatica; Laminectomy
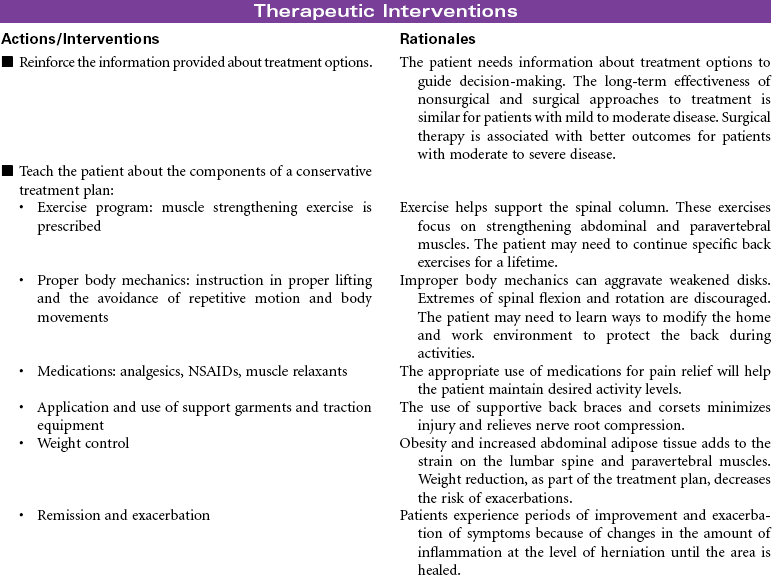
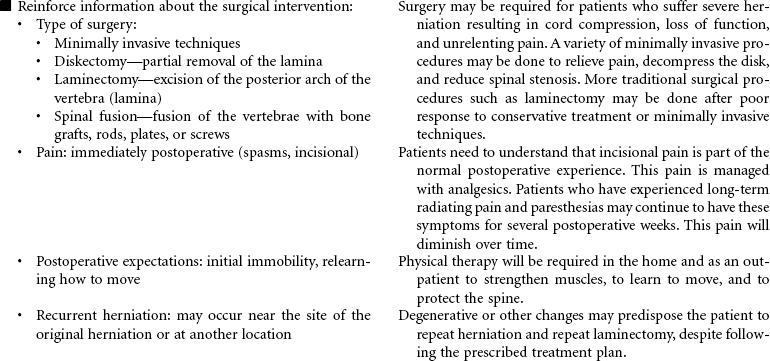
Herniated lumbar intervertebral disks are a common cause of severe back pain. Age of onset is typically between 30 and 50 years of age, with men affected more often than women. Etiological factors include trauma, degenerative diseases (e.g., osteoarthritis and ankylosing spondylitis), and congenital defects (e.g., scoliosis). Weak back and abdominal muscles combined with strenuous activity and heavy lifting is a common scenario for disk herniation in the lumbar spine. In many cases the disk is spontaneously reduced or reabsorbed without treatment, but more often the problem becomes chronic with pain and disability depending on the location and severity of the herniation. The amount of disk pulposus herniated into the spinal canal affects the narrowing of the space and the degree of compression on the lumbar or sacral spinal roots. A variety of surgical procedures may be done to reduce nerve compression and relieve lower back pain. Conservative management (rest, heat or ice, and nonsteroidal anti-inflammatory drugs [NSAIDs]) is usually accomplished in the ambulatory setting and is the focus of this care plan. Duration of treatment depends on location of herniation and symptoms. Hospitalization is necessary only if pain and sensorimotor deficits are incapacitating.



Lyme Disease
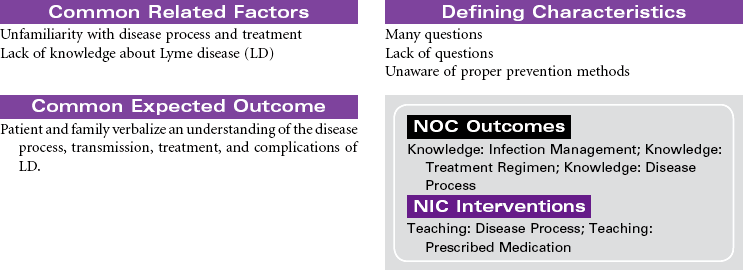
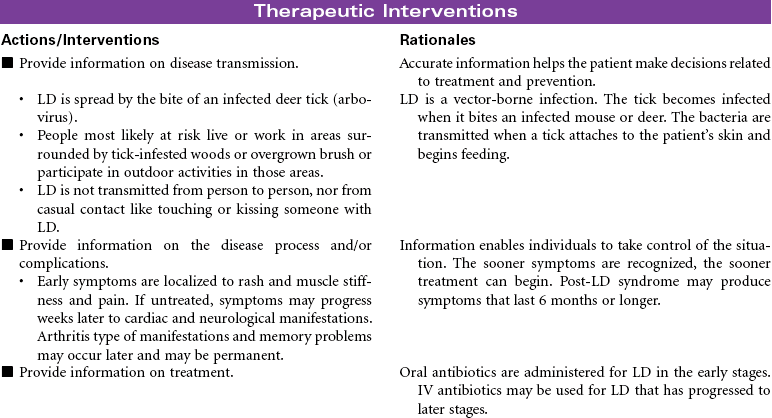
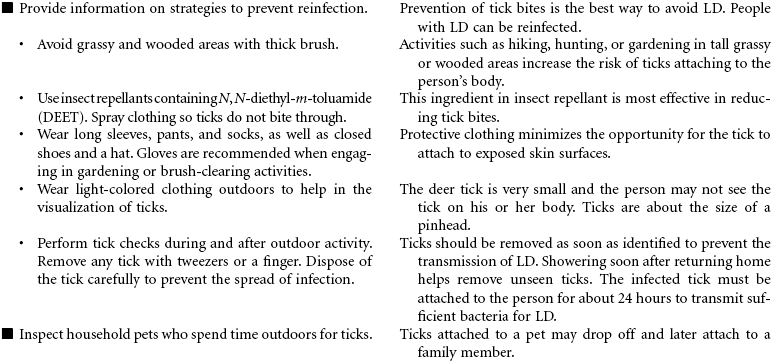
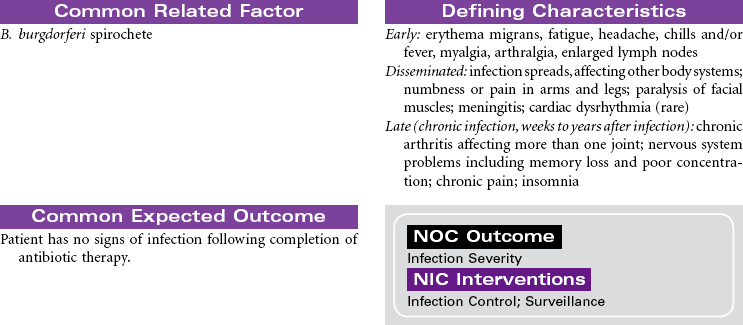
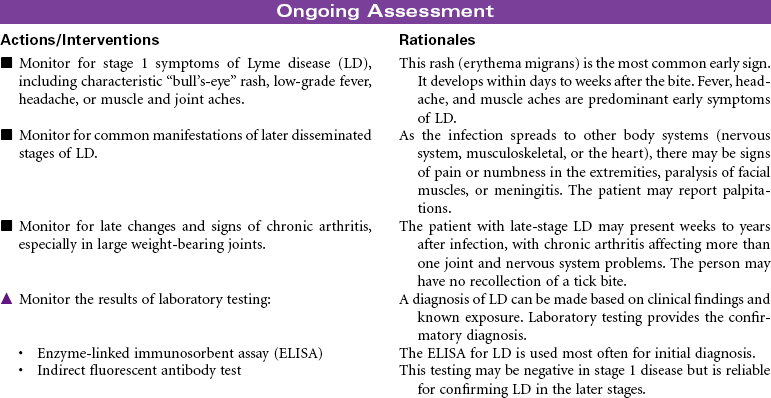
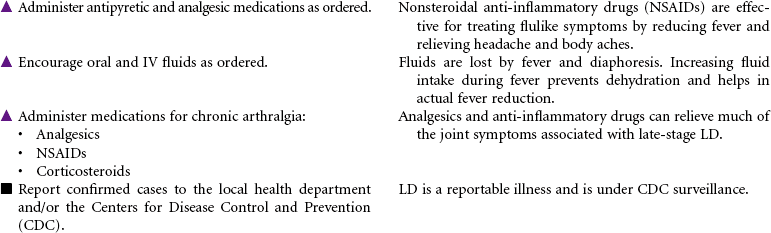
Lyme disease (LD) is primarily a vector-borne infection. In the United States, the majority of reported cases of LD are localized to states in the northeast, mid-Atlantic, upper north central regions, and several counties in northwest California. The peak incidence for the disease is in the summer months. The causative agent is Borrelia burgdorferi, a bacterium transmitted to humans by the bite of an infected deer tick. LD is the most common tick-borne infection in Canada and the United States. Diagnosis of LD is based primarily on clinical findings and is often treated based on early objective signs and a known exposure. Testing for LD via enzyme-linked immunosorbent assay (ELISA) should be performed to confirm diagnosis. Stage 1 of the infection often presents with a characteristic “bull’s-eye” rash (erythema migrans) in 60% to 80% of cases. It is often accompanied by nonspecific symptoms such as fever, malaise, fatigue, headache, muscle aches (myalgia), and joint pain (arthralgia). The period from infection to onset of symptoms is usually 7 to 14 days. Some individuals are asymptomatic or only manifest nonspecific symptoms such as fever, headache, or myalgia. These individuals may delay treatment until the disease becomes disseminated throughout the body. These later stages of LD may take weeks or months after the initial infection to produce clinical symptoms. The patient may experience cardiac dysrhythmias, severe muscle weakness, or even paralysis. Nearly all patients can be successfully treated with antibiotics. Oral amoxicillin or doxycycline is the preferred antibiotic for treatment. LD treated in the early, localized stage is generally curable. Patients whose diagnosis is made in the late stage of LD usually require longer therapy with oral or IV antibiotics. In these cases, the severity of LD symptoms may be reduced, but the disease remains indefinitely.


Multiple Sclerosis
Disseminated Sclerosis; Demyelinating Disease
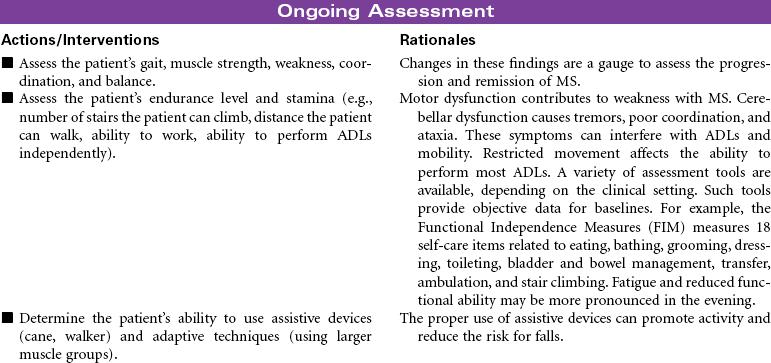
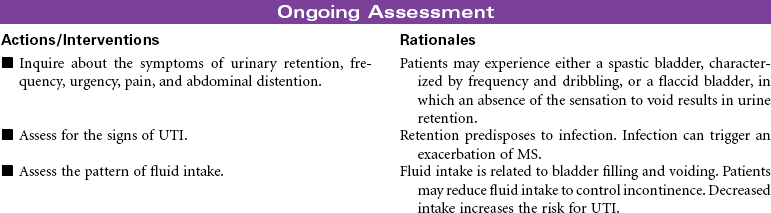
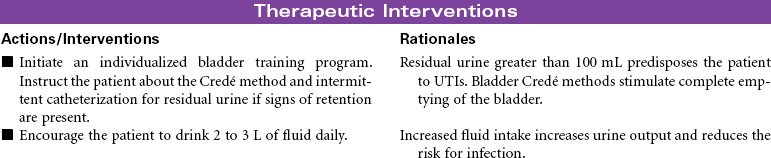
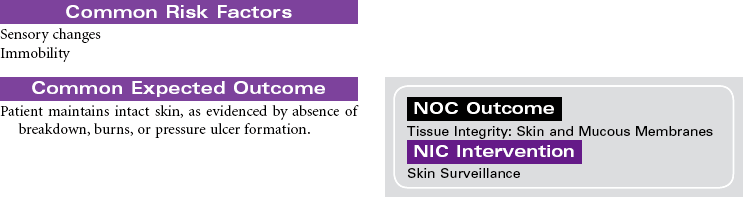
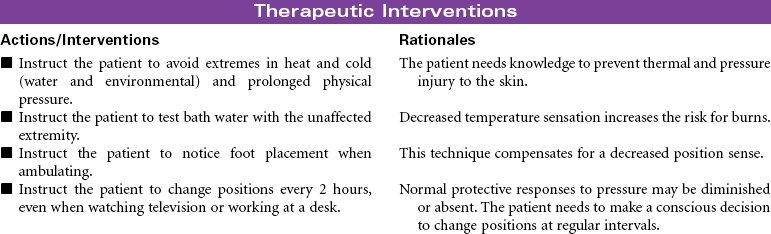
Multiple sclerosis (MS) is a chronic progressive and degenerative nervous system disease characterized by scattered patches of demyelination and glial tissue overgrowth in the white matter of the brain and spinal cord. These structural changes in nerve tissue lead to decreased nerve conduction. As the inflammation or edema diminishes, some remyelination may occur and nerve conduction returns. Over time the growth of glial tissue in the areas of repeated inflammation and demyelination leads to scarring (plaque) of the white matter and loss of nerve conduction. Among the clinical symptoms associated with MS are extremity weakness, visual disturbances, ataxia, tremor, incoordination, sphincter impairment, and impaired position sense. The clinical manifestations occur randomly with no predictable pattern of progression. Remissions and exacerbations are associated with the disease. Although the specific cause is unknown, etiological hypotheses include environmental, viral, and genetic factors. Infection with the Epstein-Barr virus in genetically susceptible individuals is thought to trigger an immune response that begins the inflammatory process causing demyelination. Loss of myelin disrupts nerve conduction. MS lesions are found in the cerebral white matter, optic nerves, brainstem, cerebellum, and cervical spinal cord. MS is considered the disease of young adults. Onset is typically between 15 and 50 years of age. Women are affected more often than men. This care plan focuses on maintenance care in the ambulatory care setting.




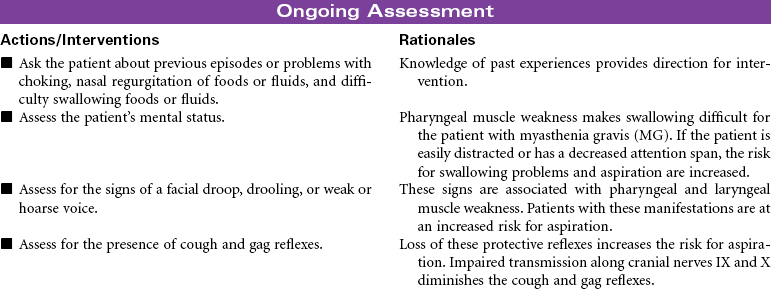
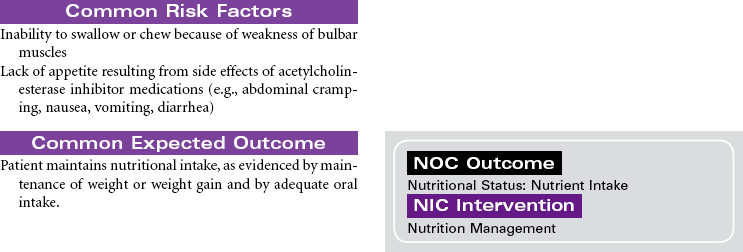
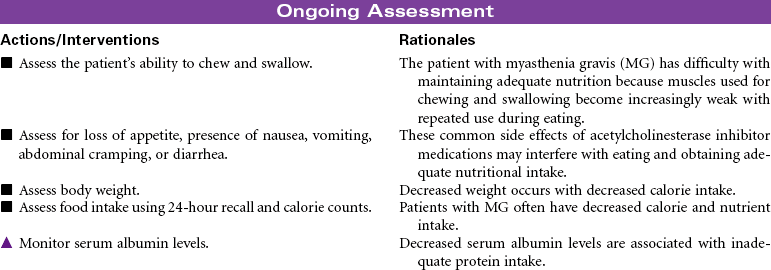
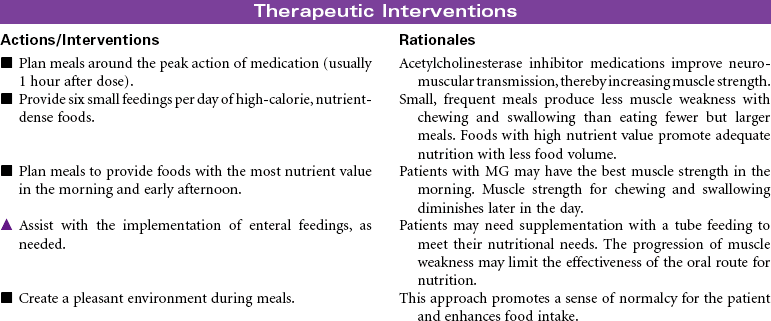
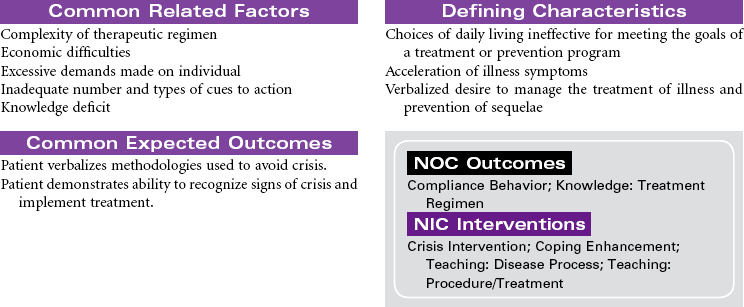
Myasthenia Gravis
Myasthenic Crisis; Cholinergic Crisis
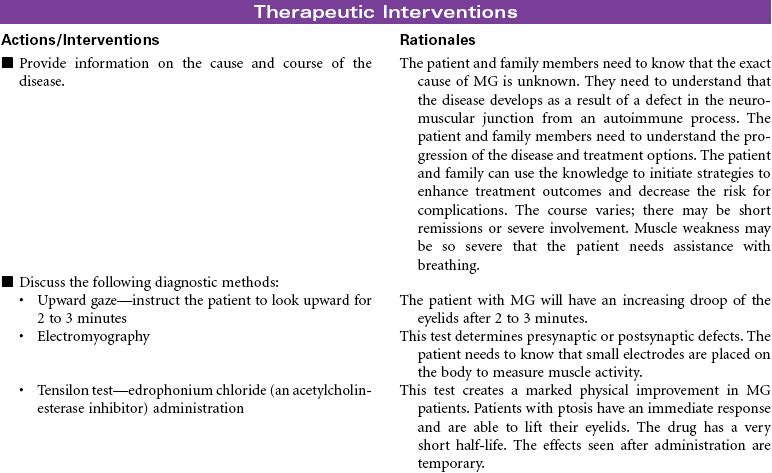
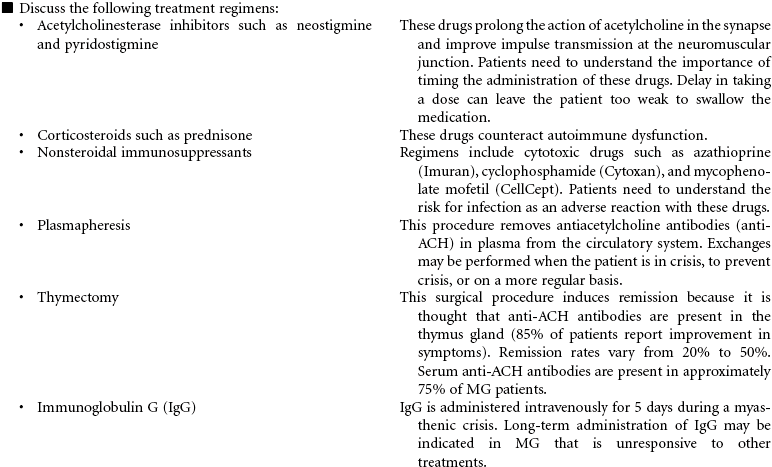
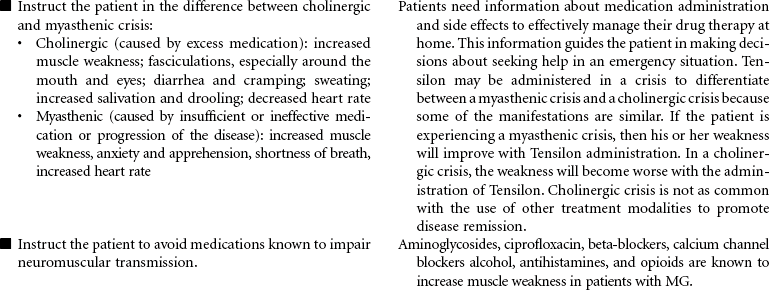
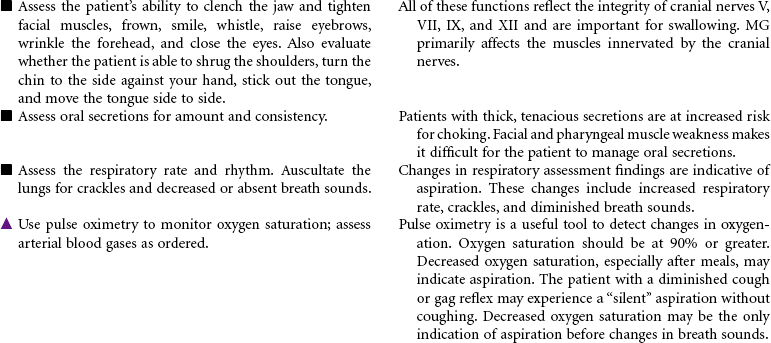
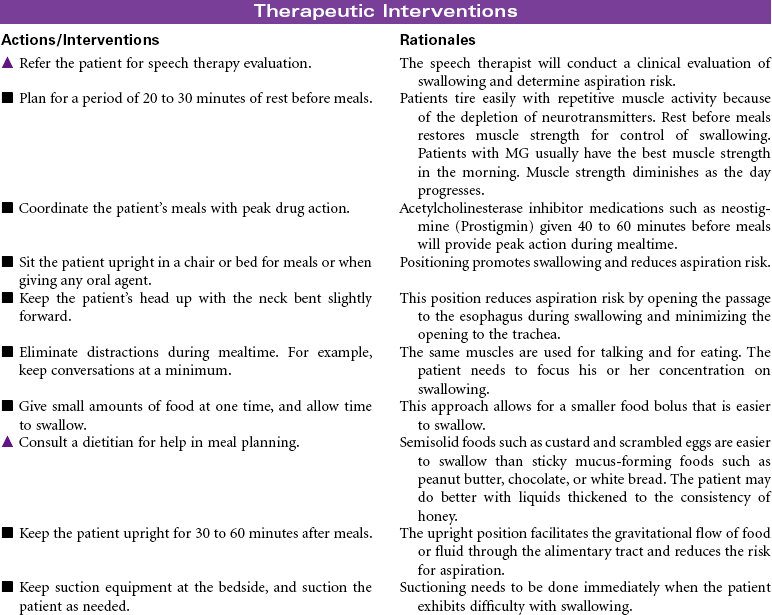
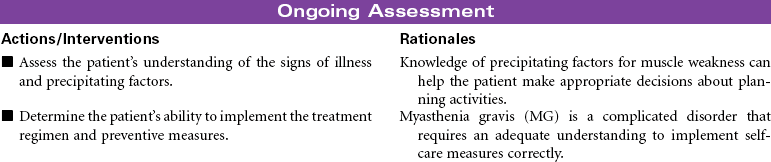
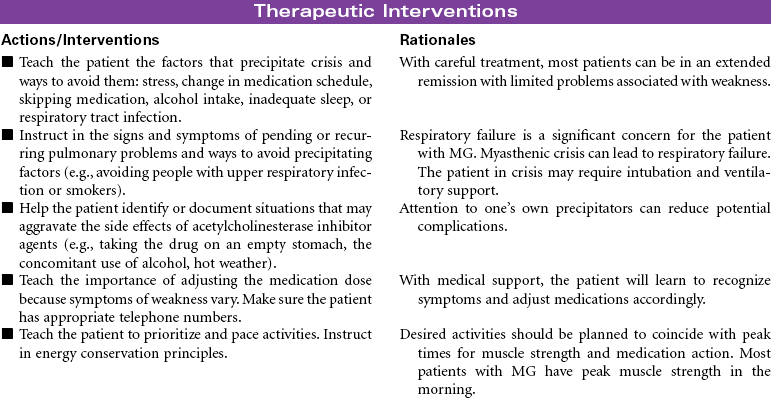
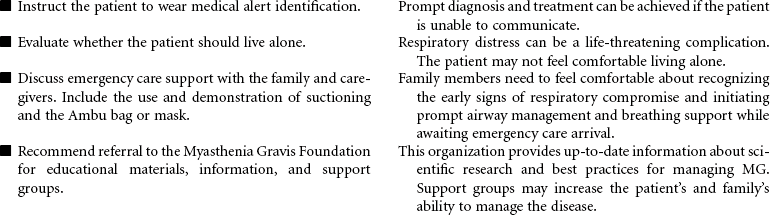
Myasthenia gravis (MG) is a chronic autoimmune disease of the neuromuscular junction. The exact mechanism that initiates the autoimmune process is unknown. The primary defect in MG is a decrease in the number of acetylcholine receptors in the post-synaptic neuromuscular junction. Antibodies attach to acetylcholine receptors, leading to their destruction. Nerve impulses are not transmitted to the skeletal muscles at the end plate of the neuromuscular junction. MG is characterized by motor muscle weakness that is aggravated by repetitive activity and is improved with rest and administration of acetylcholinesterase inhibitor agents. The muscles most often affected are the oculomotor (affecting eye movements and lid elevation), facial, pharyngeal and laryngeal, and muscles of the neck, shoulders, and limbs. Although symptoms may vary in severity from person to person, disruptions can occur in vision, facial appearance, walking, talking, and swallowing. Hospitalization and monitoring are required for the patient in crisis, because of risk for respiratory failure. Myasthenic crisis may be the result of progression of the disease. Cholinergic crisis is associated with excess acetylcholinesterase inhibitor medication. MG is more common in women of childbearing age and in men after the age of 50. The goal of treatment is to induce remission if possible and to control the muscle weakness with acetylcholinesterase inhibitor agents. Thymectomy may be performed early in the disease to eliminate the possibility that antiacetylcholine antibodies will be produced in the thymus gland. Approximately 80% of individuals with the disease have thymic hyperplasia; many have thymic tumors. Chemical immunosuppression (prednisone, azathioprine [Imuran], cyclophosphamide) to decrease antibody binding to acetylcholine receptor sites at the muscular end plate is also used.

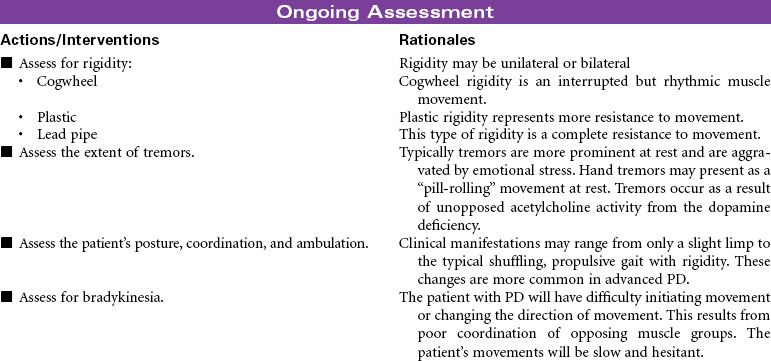
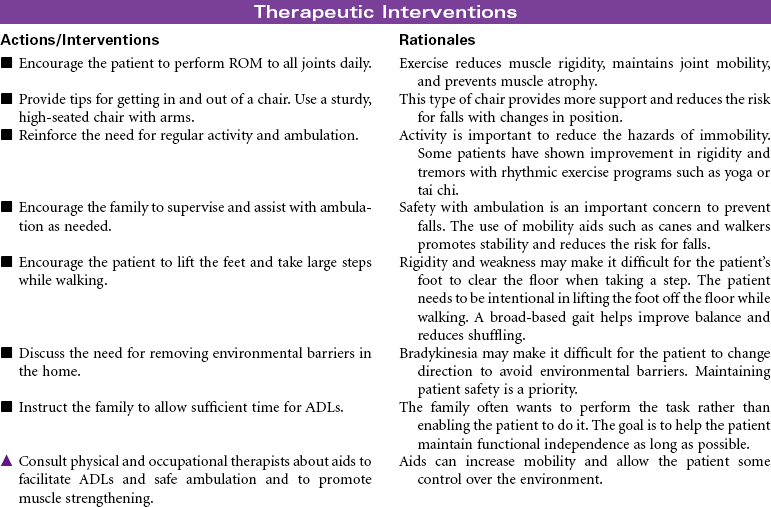
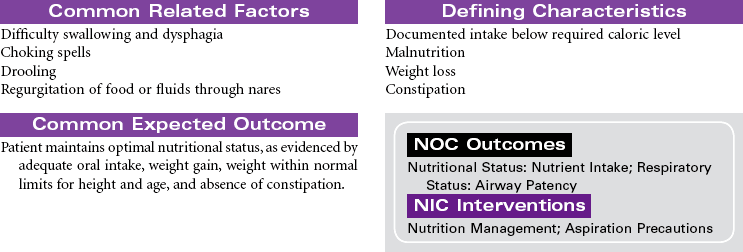
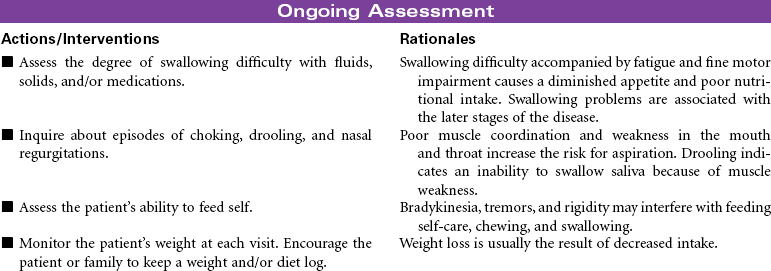
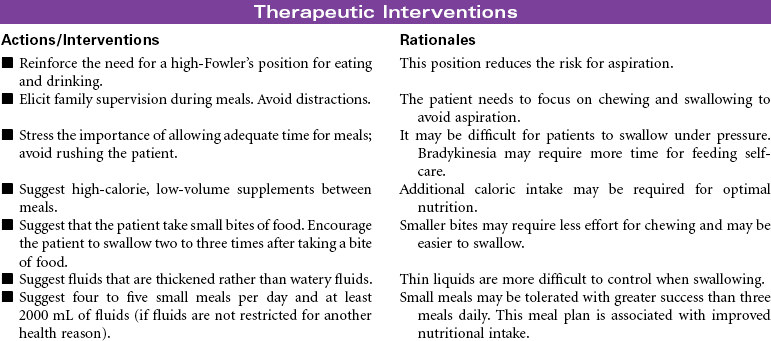
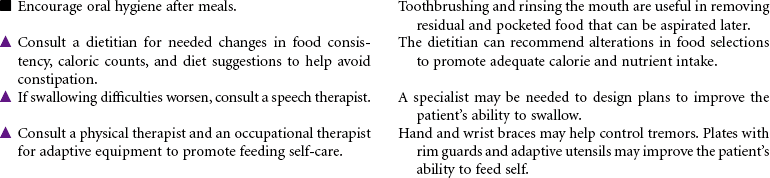
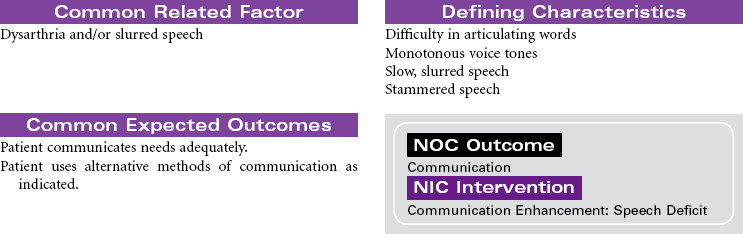
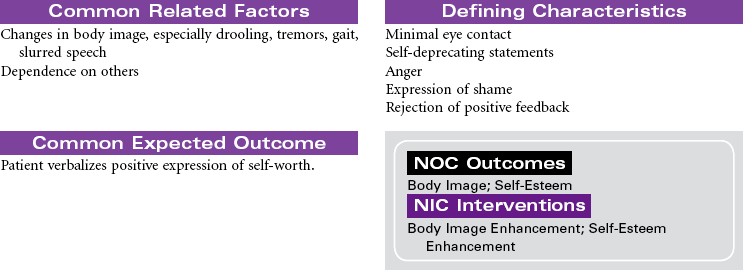
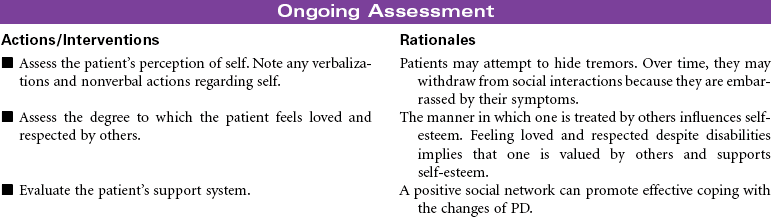
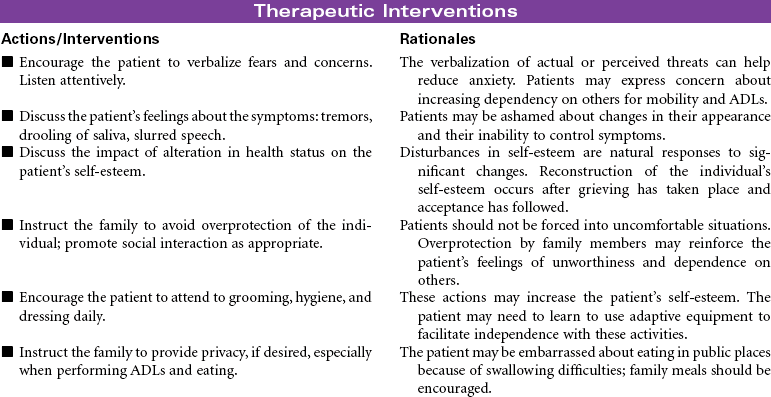
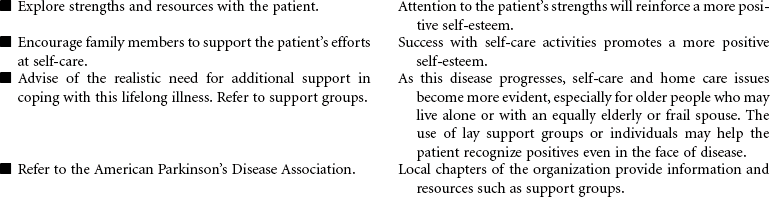
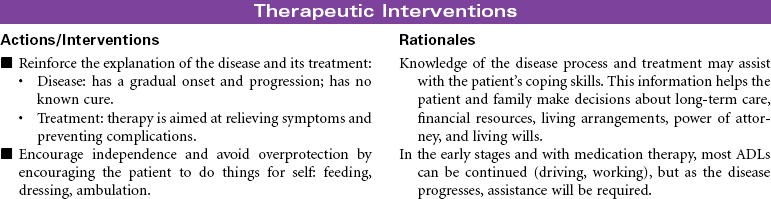
Parkinson’s Disease
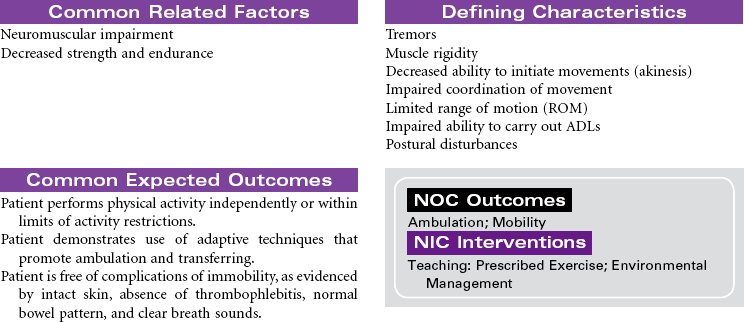
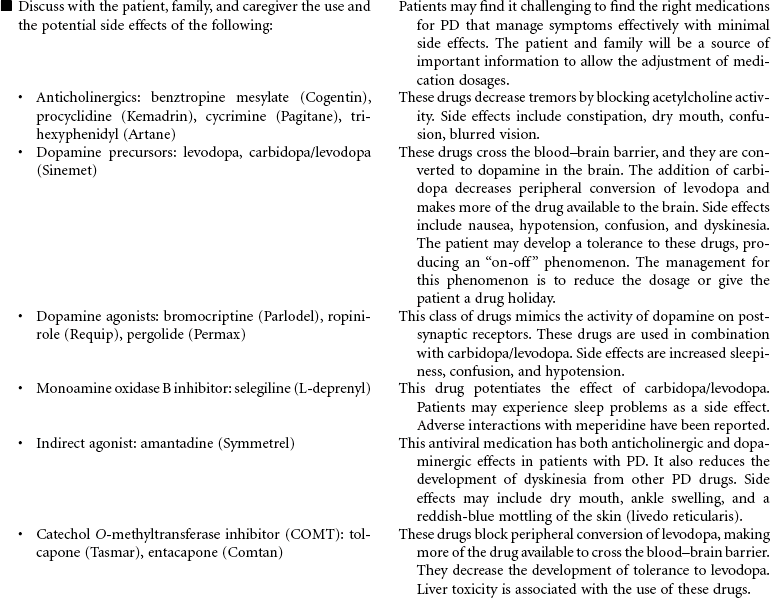
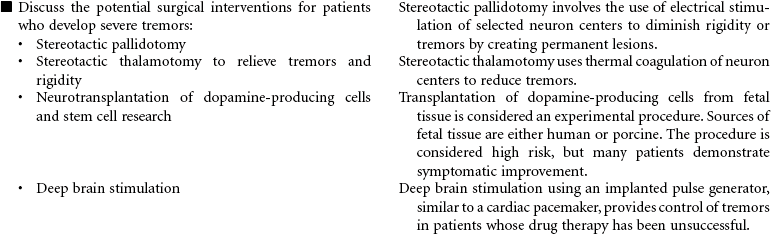
Parkinson’s disease (PD) is a movement disorder associated with dopamine deficiency in the brain. As a result, the patient develops a neurotransmitter imbalance between dopamine and acetylcholine. This imbalance affects the extrapyramidal system of the brain responsible for control and regulation of movement. There is no specific diagnostic test. A diagnosis of PD is based on thorough evaluation of presenting clinical manifestations. The four characteristic signs are tremor at rest, rigidity, postural instability, and slowness of movement. Other clinical manifestations include shuffling gait, masklike facial expressions, and muscle weakness affecting writing, speaking, eating, chewing, and swallowing. Onset is usually around 60 years of age; however, a significant number of young adults have PD. Etiological hypotheses include exposure to environmental toxins and age-related degeneration of brain neurons. Some theories suggest gene mutation may play a role in the development of PD. Free radical formation has also been considered as a contributing factor. Secondary Parkinsonism is associated with traumatic brain injury and side effects of the phenothiazine drug group. There is no cure for PD. Treatment is focused on slowing disease progression and symptom management. Drug therapy is the primary treatment for PD. As the disease progresses and tremors become more severe, surgical therapy may be used. Patient care is usually managed in the outpatient setting.


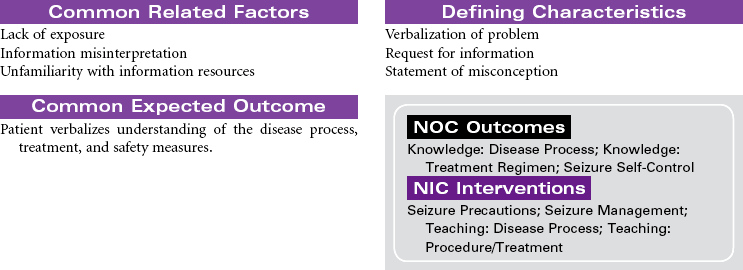
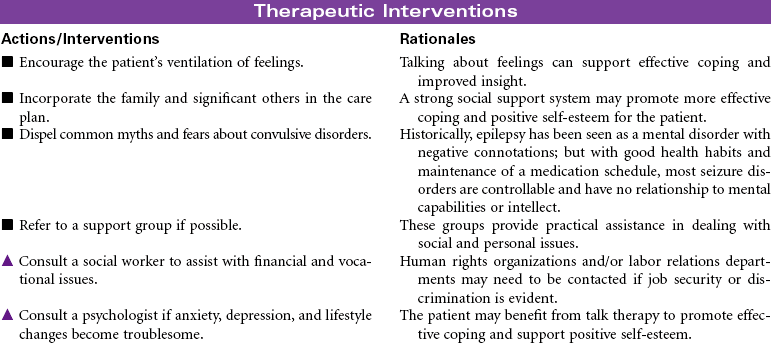
Seizure Activity
Convulsion; Epilepsy; Seizure Disorder
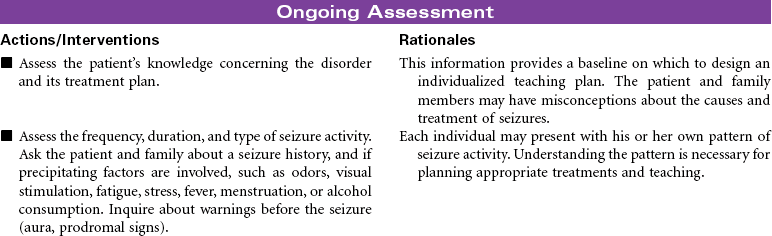
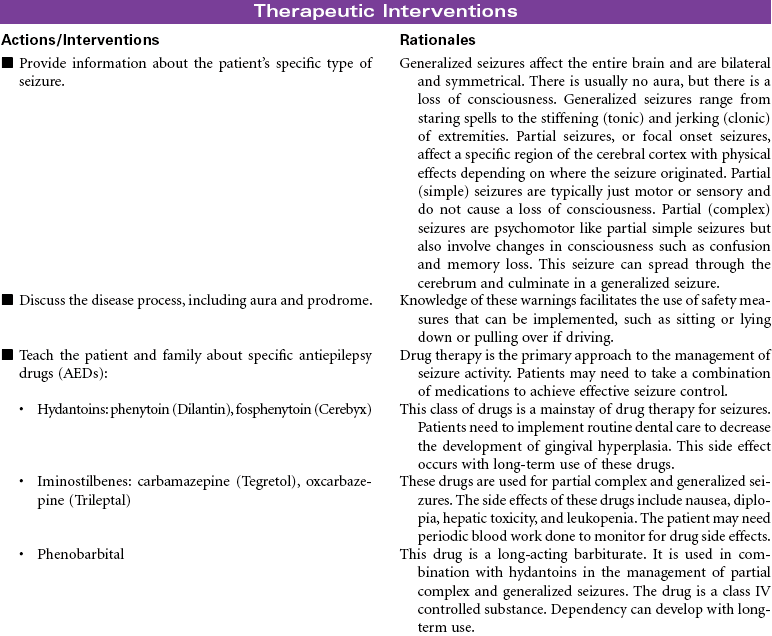
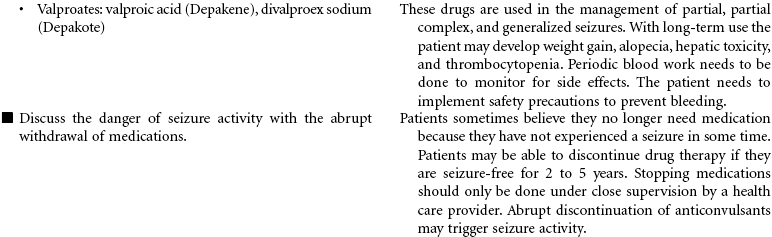
A seizure is an occasional, excessive disorderly discharge of neuronal activity from the cerebral cortex causing behavioral and physical disturbances. Recurrent seizures (epilepsy) may be classified as partial, generalized, or partial complex. Onset is usually before 20 years of age, and there seems to be a genetic predisposition to idiopathic epilepsy. Patients with new onset of seizure activity after age 20 may have a history of brain injury or disease such as closed head trauma, brain tumor, or stroke. Fever, low blood glucose level, drug and alcohol abuse, acid-base imbalances, electrolyte imbalances, and medication side effects may also contribute to the onset of seizures. Seizure activity has three distinct phases. The preictal phase is that time before the actual seizure. The patient may experience symptoms that warn of an impending seizure. This is called an aura. During the ictal phase, the patient experiences a progression of neuromuscular changes as a result of the disorganized neuron activity. The postictal phase is the period immediately following seizure activity. This phase represents brain recovery and return to baseline status. A patient with new onset of seizures may require hospitalization for diagnosis and initiation of treatment. Follow-up care is in the outpatient setting. This care plan focuses on self-care in the ambulatory setting.

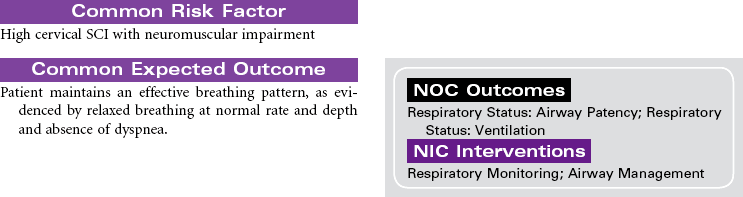
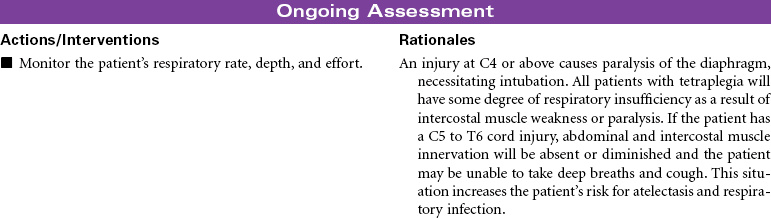
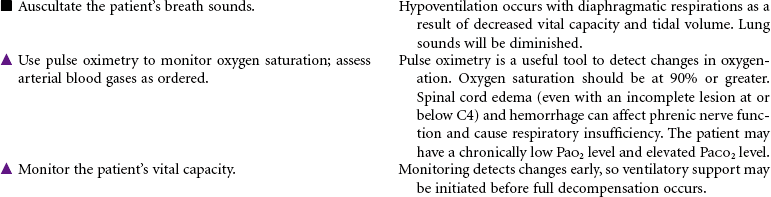
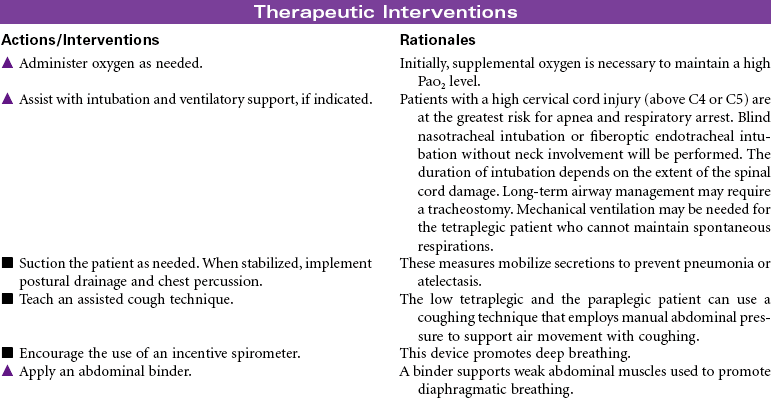
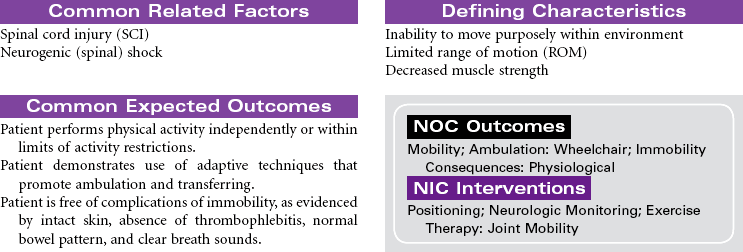
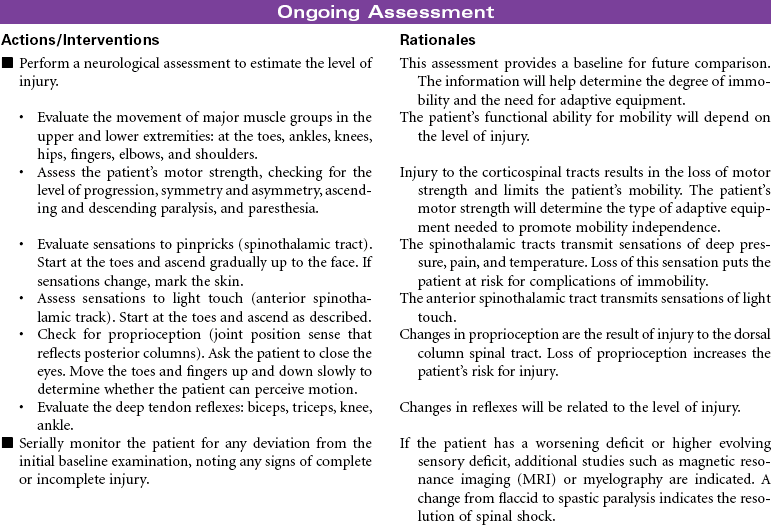
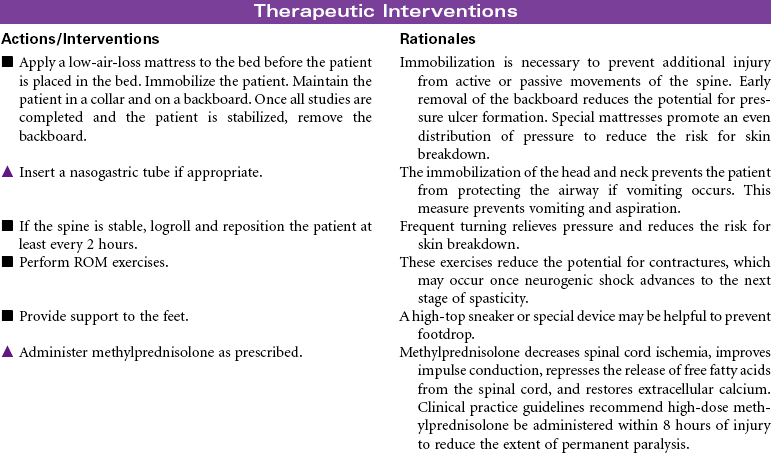
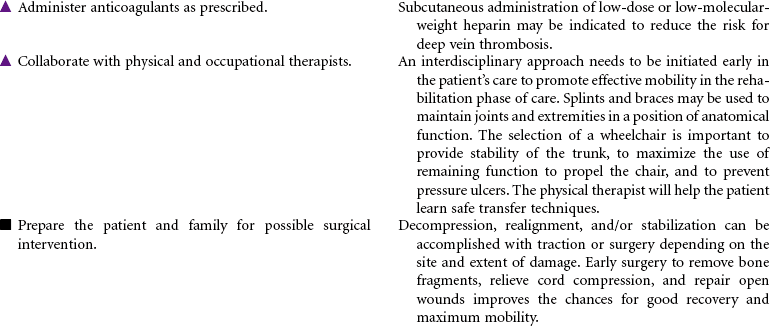
Spinal Cord Injury
Quadriplegia; Tetraplegia; Paraplegia; Neurogenic Shock; Spinal Shock
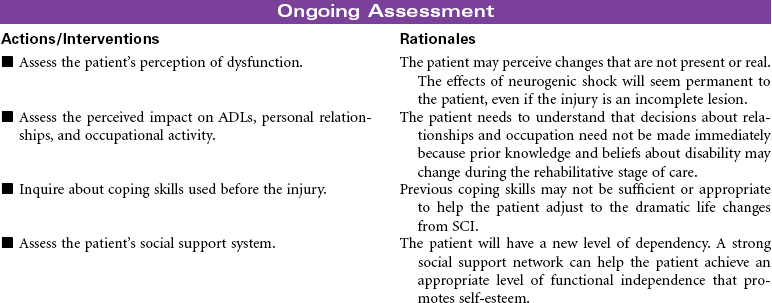
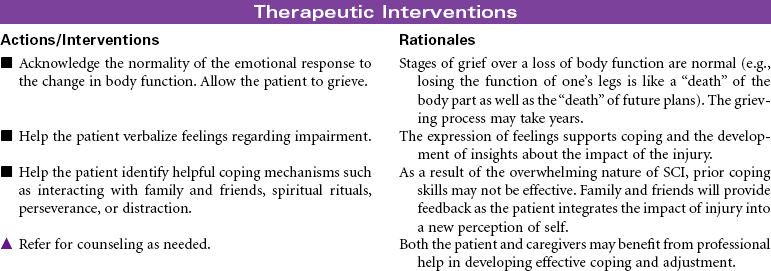
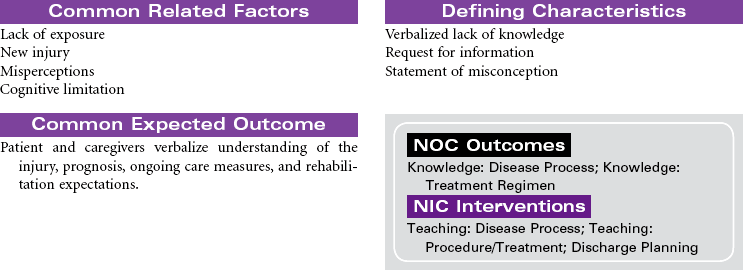
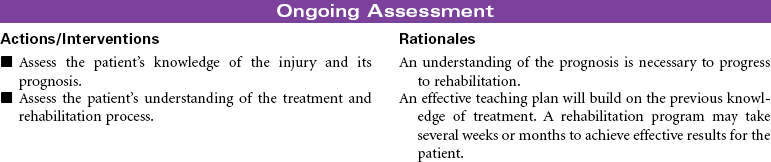
Spinal cord injury (SCI) is damage to the spinal cord at any level from C1 to L1 or L2, where the spinal cord ends. Primary causes of SCI are motor vehicle accidents, followed by sporting accidents, falls, and penetrating injuries (gunshot or knife wounds). Motor vehicle accidents are the leading cause among people younger than age 65. Among people older than 65 years, falls is the leading cause of SCI. Approximately 50% of people who sustain SCI are men between 15 and 29 years of age. Injury may result in a complete cord lesion with no preservation of motor and sensory function below the level of injury. An incomplete lesion results in residual and mixed motor and sensory function below level of injury and some potential for improvement in function. Complete cord injury above C7 results in tetraplegia (formerly called quadriplegia); injury from C7 to L1 causes paraplegia.
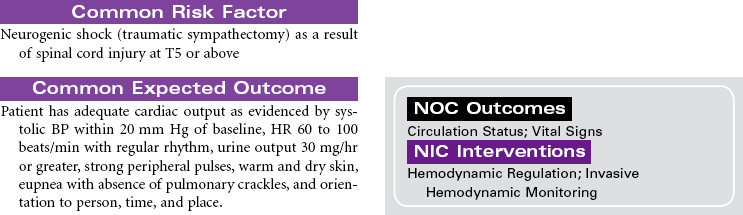
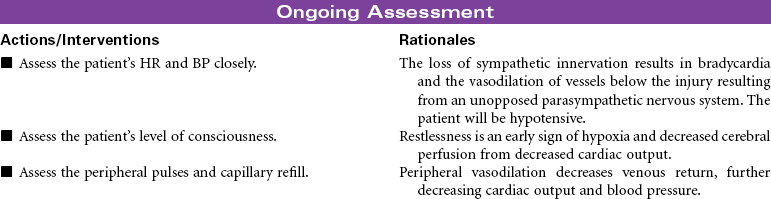
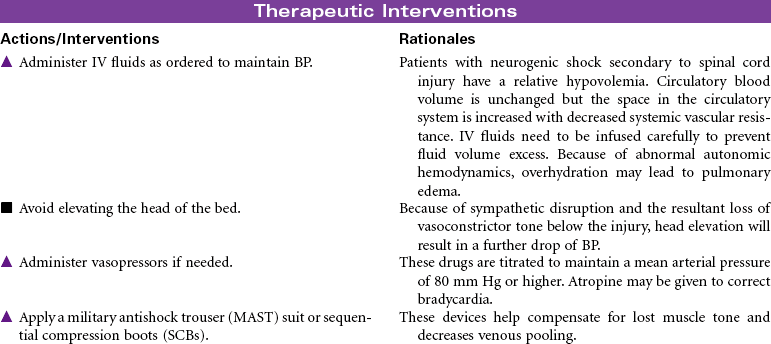
Neurogenic (or spinal) shock often follows cervical and high thoracic SCI. Spinal shock can last from 7 to 10 days to weeks or months after injury. It temporarily results in: (1) total loss of all motor and sensory function below the injury; (2) sympathetic disruption, resulting in loss of vasoconstriction and leaving parasympathetics unopposed, leading to bradycardia and hypotension; (3) loss of all reflexes below the injury; (4) inability to control body temperature, secondary to the inability to sweat, shiver, or vasoconstrict below the level of injury; (5) ileus; and (6) urinary retention. When neurogenic shock resolves, it is followed by a stage of spasticity.
This care plan focuses on the acute care of a patient with SCI.


Stroke
Brain Attack; Cerebrovascular Accident (CVA); Thrombotic Stroke; Embolic Stroke; Hemorrhagic Stroke; Ischemic Stroke
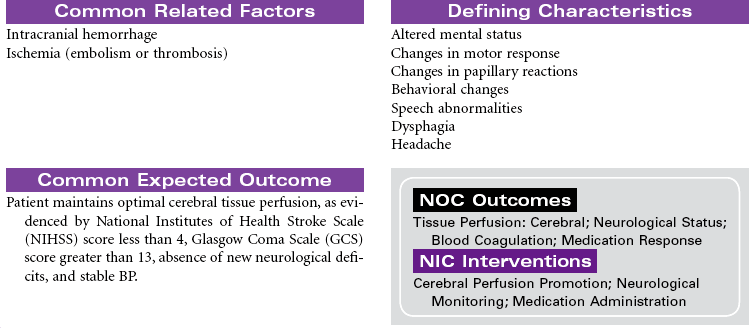
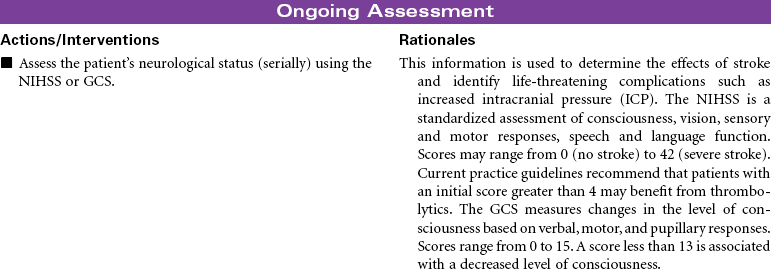
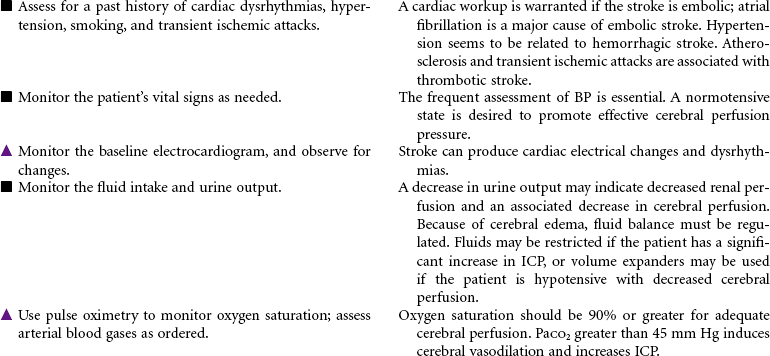
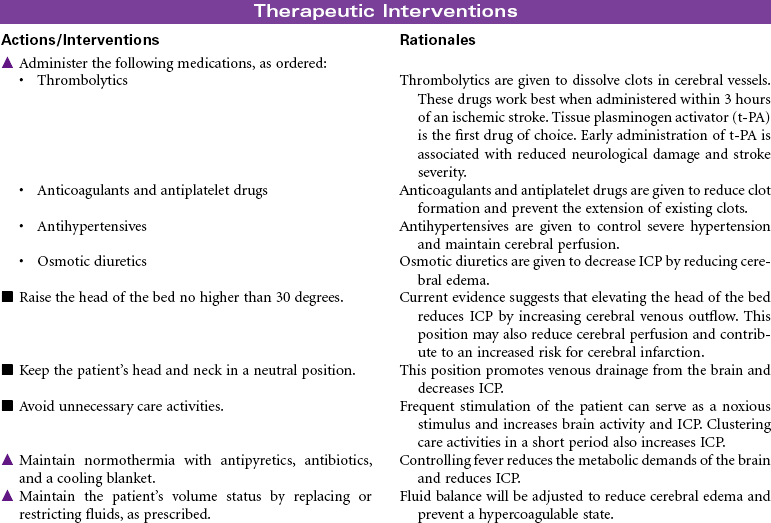
Stroke is a disease that affects the arteries leading to and within the brain. Strokes are classified as either ischemic (as a result of a cerebral thrombus or an embolus) or hemorrhagic (as a result of a rupture of a cerebral blood vessel). Stroke is the leading cause of serious, long-term disability in the United States and Canada. It is the third leading cause of death in the United States. A significant majority of those affected by strokes are older than 65 years of age. African Americans have a higher incidence of stroke than Caucasians or Hispanics. Risk factors for stroke include poorly controlled hypertension, diabetes mellitus, high cholesterol levels, smoking, cocaine use, alcohol abuse, obesity, high-dose estrogen drug therapy, and cerebral aneurysm. Acute ischemic stroke is a medical emergency requiring prompt treatment with thrombolytic therapy within 3 hours after symptom recognition (“time is brain”). Hemorrhagic stroke needs to be ruled out before treatment with thrombolytics. Stroke severity is determined using the National Institutes of Health Stroke Scale (NIHSS). Much attention is directed to providing safe, efficient and quality care to patients with stroke. National guidelines by the American Stroke Association and the Brain Attack Coalition provide direction for stroke care provided by hospitals. The Get With the Guidelines—Stroke continuous quality improvement program provides a mechanism for physicians and hospital staff to monitor their performance. The Joint Commission provides certification for Primary Stroke Centers.
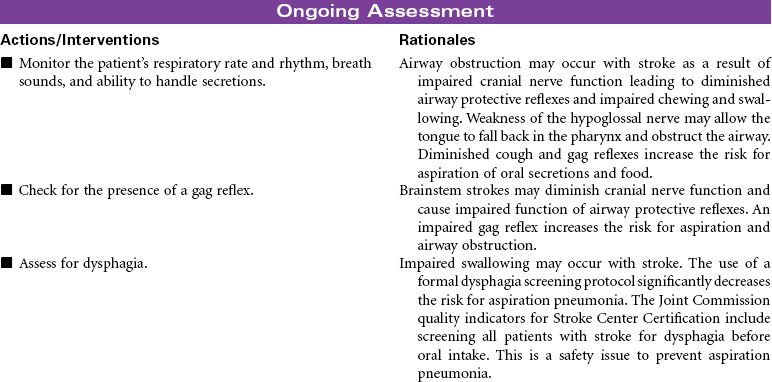
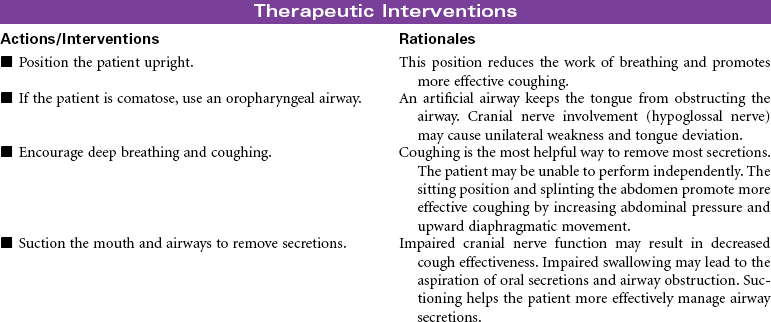
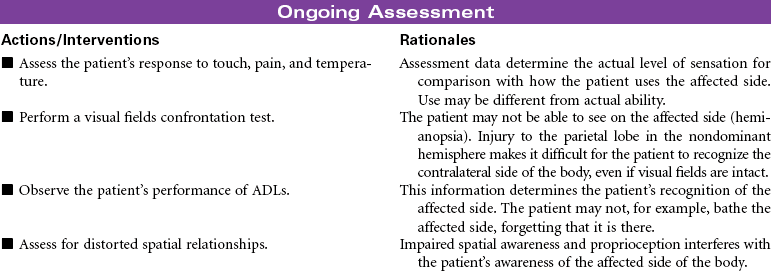
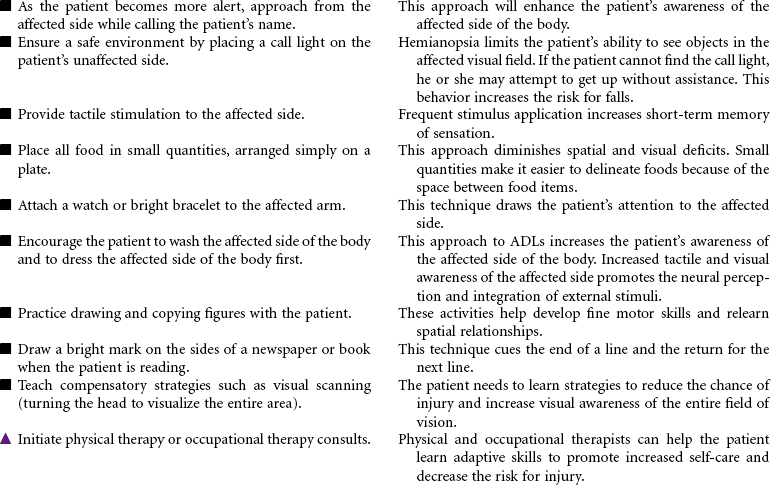
The clinical manifestations of stroke and outcomes for the patient vary, depending on the area of the brain affected. The area of the brain supplied by the middle cerebral artery is the most common site for stroke. A stroke in the nondominant hemisphere often causes spatial-perceptual deficits, changes in judgment and behavior, and unilateral neglect. A stroke in the dominant right hemisphere typically causes dysphasia, dysarthria, left-sided sensory loss and homonymous hemianopsia, a decreased awareness of the left side of the body, left-sided paralysis and/or paresis, apraxia, impaired judgment, increased emotional lability, and deficits in handling new spatial information. A stroke in the dominant left hemisphere can cause repetitive or expressive dysphasia, dysarthria, right-sided sensory loss and homonymous hemianopsia, right-sided paralysis and/or paresis, increased emotional lability, and a deficit in handling new language information. In this type of stroke there is typically intact judgment, infrequent apraxia, and usually a normal awareness of both sides of the body. This care plan focuses on acute care management of ischemic stroke in the hospital.




Transient Ischemic Attack
Transient Ischemic Attack (TIA); Carotid Endarterectomy; Carotid Artery Stent
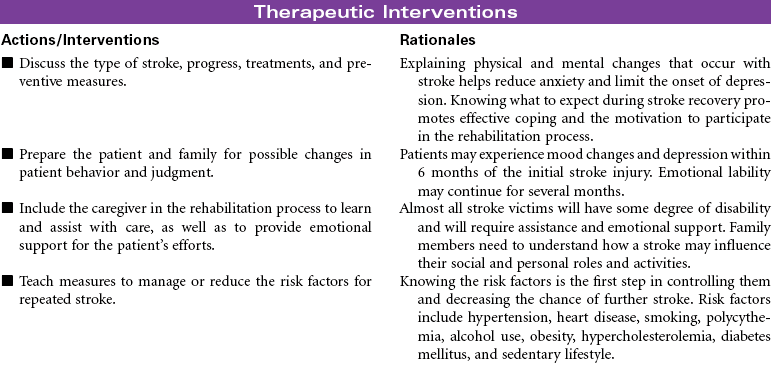
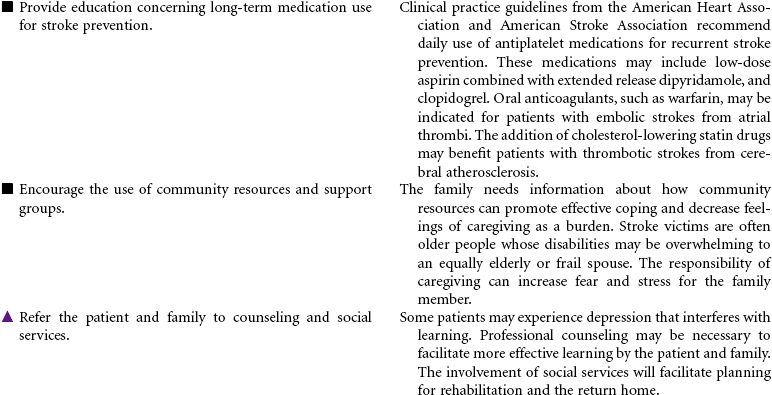
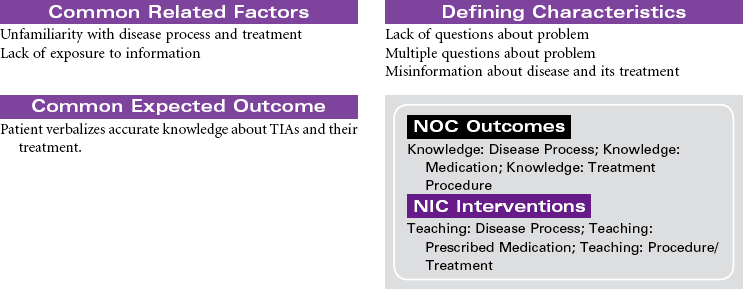
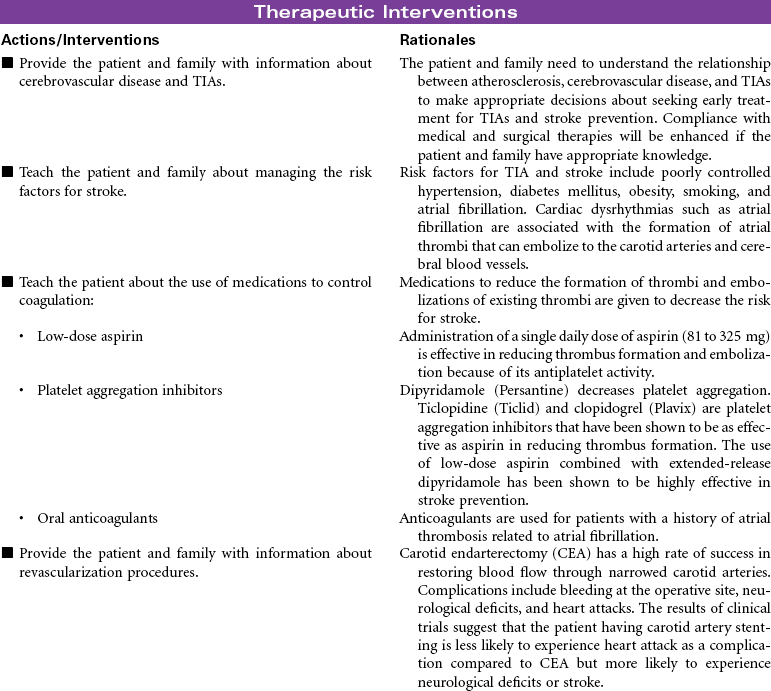
A transient ischemic attack (TIA) is a cerebrovascular disorder that produces temporary neurological deficits. Atherosclerosis in the cerebral vessels is the primary cause of TIA. Emboli that originate in blood vessels outside the cerebral circulation also contribute to the occurrence of TIAs. A TIA is considered an early warning of the risk for an impending stroke. The patient who experiences a TIA is nine times more likely to have a stroke than a patient without a TIA. Clinical manifestations of a TIA depend on the location of the ischemia in the brain. Symptoms usually last no longer than 5 to 20 minutes and resolve within 24 hours of onset. The patient will not have any residual neurological deficits. Treatment of TIA includes measures to promote cerebral blood flow and manage risk factors for stroke. Long-term drug therapy to control coagulation is an important part of the treatment. Surgical interventions are used to improve carotid artery blood flow in patients at high risk for stroke. A carotid endarterectomy (CEA) is done to remove atherosclerotic plaques in the carotid arteries and improve blood flow to the brain. Carotid artery stenting (CAS) is a newer and less invasive procedure that is done to improve blood flow. A stent is threaded into the carotid artery. Once in place the stent is expanded to widen the area of blockage and capture any dislodged plaque. Clinical trials comparing CEA to CAS found that both procedures are safe and offer equal benefits for a diverse population of patients. This care plan focuses on the patient undergoing pharmacological and surgical interventions for stroke prevention.

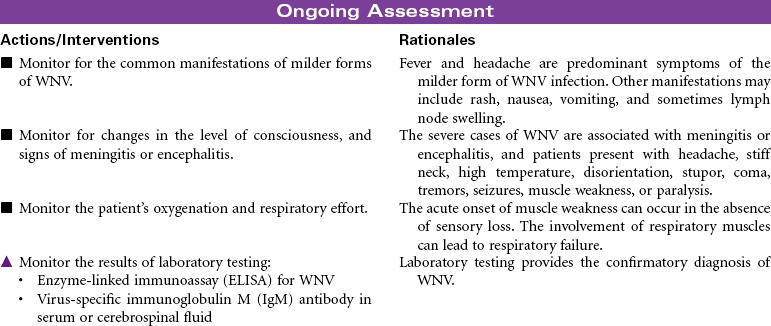
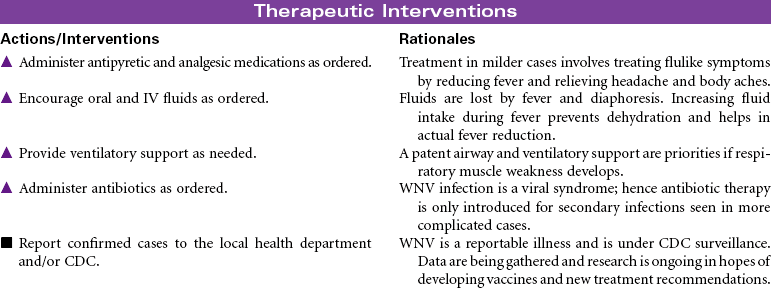
West Nile Virus
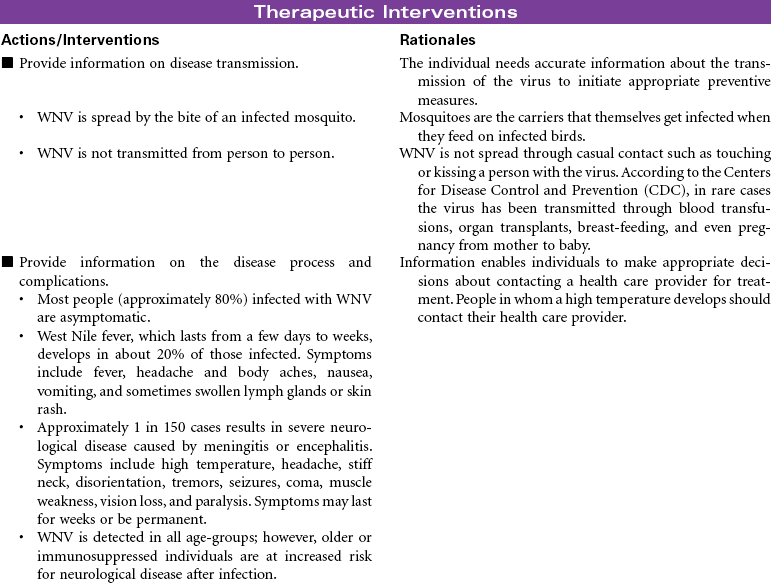
West Nile virus (WNV) is an infection that is spread to humans through infected mosquitoes and birds. The causative agent in WNV infection is a single-stranded RNA virus from the group flavivirus. Wild birds are the reservoir, and the mosquito is the vector. Other arthropods, such as sand flies and ticks, may serve as vectors. Transmission of the virus occurs when a mosquito bites an infected bird and then bites a human. Before 1999, WNV existed only in the Eastern hemisphere, with wide distribution in Africa, Asia, the Middle East, and Europe. Human infection was rare in the United States. Since 1999, cases of WNV, including WNV encephalitis, have been identified in 45 states in the United States. WNV is now recognized as seasonal infectious epidemic in the summer and fall months in North America. Most states have a system for testing dead birds for the presence of the virus.
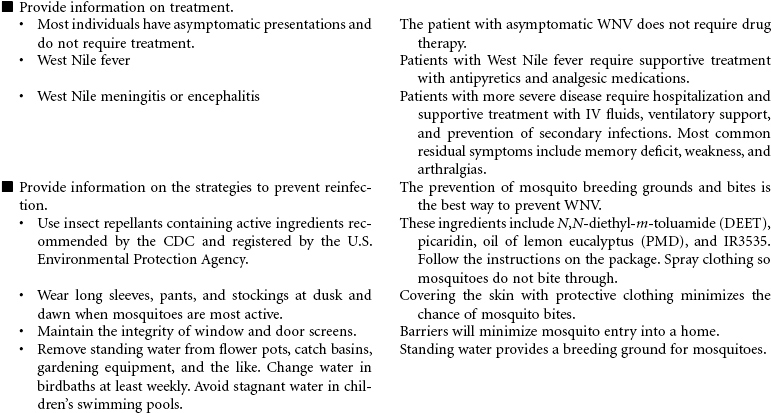
WNV is a potentially serious illness that affects the central nervous system. Diagnosis relies on the identification of viral antibodies in the serum or cerebrospinal fluid. Symptoms vary, with the majority of infected persons exhibiting no symptoms, and about 20% exhibiting mild flulike symptoms. Symptoms can last 3 to 6 days and are treated with supportive therapy for pain and fever. Less than 1% of cases result in severe neurological disease presenting as meningitis or encephalitis. Older adults have the highest risk for developing severe neurological disease from WNV infection. Although there is no specific treatment for WNV infection, persons with the more severe disease require hospitalization and supportive care with IV fluids, airway management, ventilatory support, and prevention of secondary infection.