Renal and Urinary Tract Care Plans
Acute Renal Failure
 = Independent
= Independent  = Collaborative
= Collaborative For additional care plans, go to http://evolve.elsevier.com/Gulanick/.
For additional care plans, go to http://evolve.elsevier.com/Gulanick/.
Acute Tubular Necrosis (ATN); Renal Insufficiency; Acute Kidney Injury
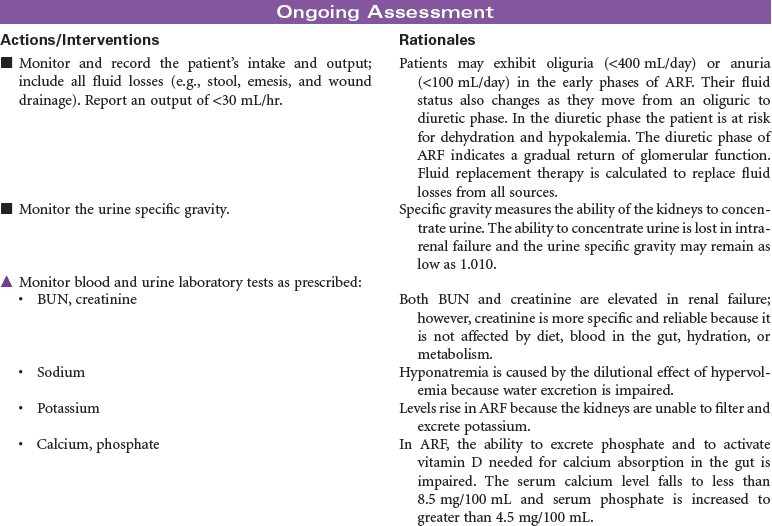
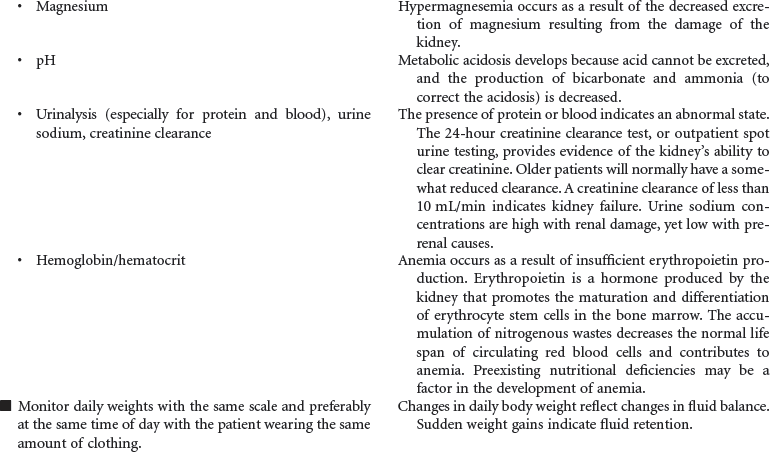
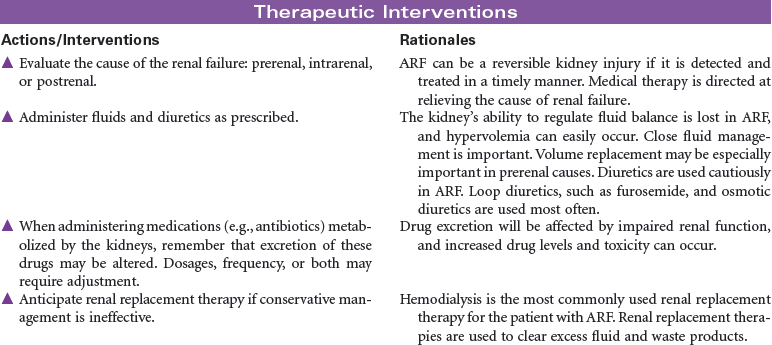
In acute renal failure (ARF), the kidneys are incapable of clearing the blood of the waste products of metabolism. ARF may occur as a single event, with return of normal renal function, or may progress to chronic kidney disease or kidney failure. The causes of acute renal failure can be divided into three major types: prerenal, resulting from a decrease in renal perfusion; intrarenal, caused by a direct injury to the nephrons from ischemia or renal toxins; and postrenal, as a result of urinary tract obstruction that leads to the backflow of urine into the kidney. Hospital-acquired renal failure is most likely a result of acute tubular necrosis (ATN), which results from the administration of nephrotoxins or an acute ischemic episode. Because of declines in renal function as part of the normal aging process, older patients are more at risk when receiving nephrotoxic agents such as IV contrast media or certain medications. During the period of loss of renal function, hemodialysis, peritoneal dialysis, or continuous renal replacement therapy may be required to clear the accumulated toxins from the blood. This care plan focuses on the patient with ARF during hospitalization.
 Impaired Renal Function
Impaired Renal Function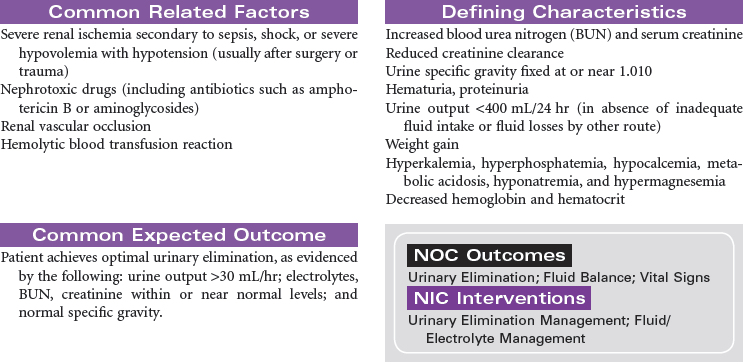
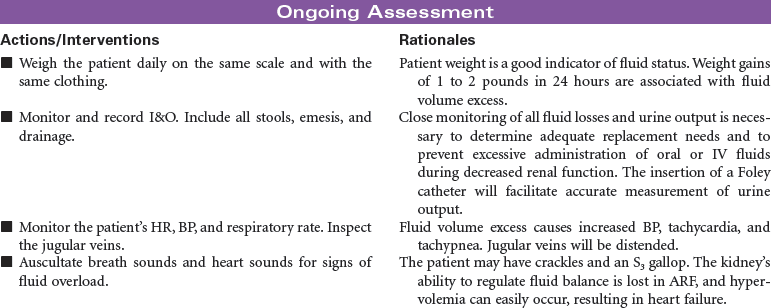
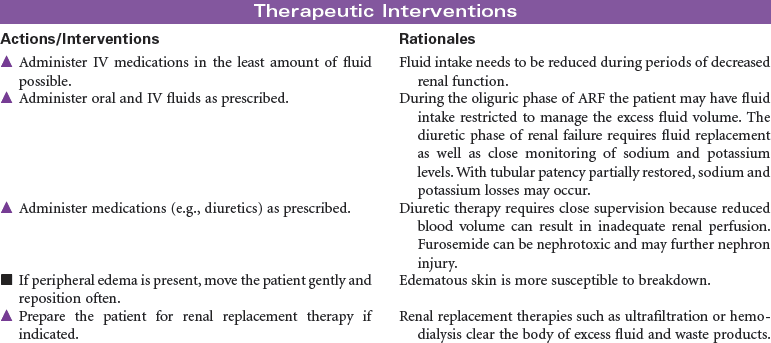
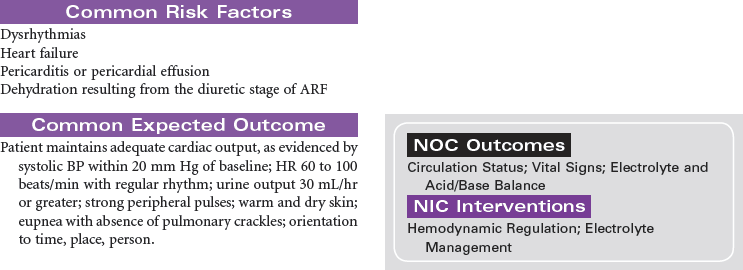
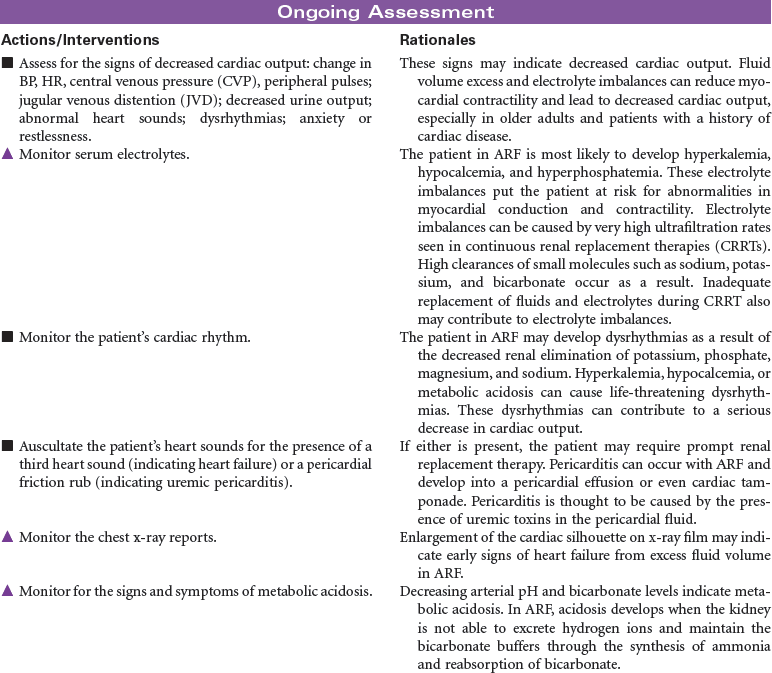
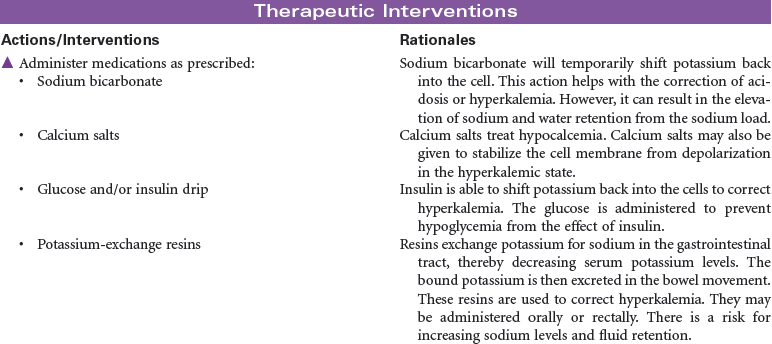
 Excess Fluid Volume
Excess Fluid Volume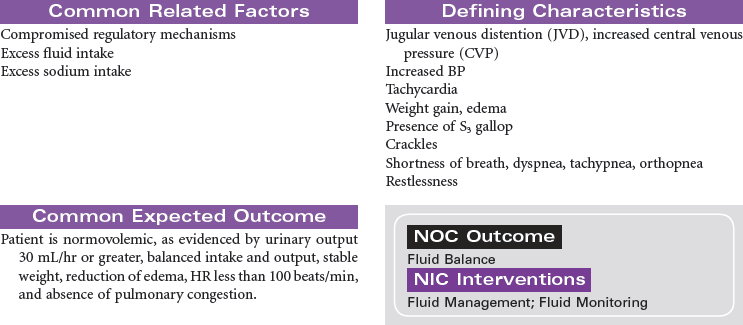

Hemodialysis
Internal Arteriovenous Fistula; Graft; Central Venous Catheter; Renal Replacement Therapy
Hemodialysis is one of the renal replacement therapies that is necessary to sustain life in people with no or very little kidney function. In general, dialysis is the diffusion of solute molecules and fluids across a semipermeable membrane. Dialysis may be a short-term therapy in situations such as acute renal failure (ARF) or long-term therapy for the patient with chronic renal failure. Hemodialysis may be used to remove drugs from the circulatory system as part of the treatment for drug overdoses. The purpose of dialysis is to remove excess fluids, toxins, and metabolic wastes from the blood. The primary mechanisms of dialysis are diffusion, osmosis, and ultrafiltration. The composition of the dialysis solution establishes a concentration and/or osmotic gradient to promote diffusion and osmosis of urea, creatinine, and electrolytes from the blood to the dialysate. Ultrafiltration is used to remove excess fluid by adjusting pressures in the blood compartment and the dialysate compartment. Rapid changes in vascular volume and electrolyte concentrations during hemodialysis can result in complications such as hypotension, muscle cramping, and cerebral edema. Hemodialysis increases the patient’s risk for infection. The most common source for infection is through vascular access sites. The incidence of blood borne infections such as human immunodeficiency virus (HIV) infection and hepatitis B and C has decreased with improved screening of patients and use of dedicated equipment for patients with these infections.
Hemodialysis requires a vascular access. This can be accomplished by surgically creating an arteriovenous (AV) fistula or graft (synthetic material used to connect an artery and a vein); or by insertion of an external catheter into a large central vein. The internal AV fistula is made by surgically creating an anastomosis between an artery and a vein, thus allowing arterial blood to flow through the vein, causing engorgement and enlargement. Placement may be in either forearm, using the radial artery and cephalic vein or brachial artery and cephalic vein. The internal AV fistula is the preferred access for long-term hemodialysis and must heal and mature before it may be used for access in hemodialysis. The central venous catheter may be either single or double lumen. A single-lumen catheter serves as the arterial source, and the venous return is made through a peripheral vein or by the use of an alternating flow device. A double-lumen catheter is used for both the arterial source and the venous return. Because of their location and low durability, femoral catheters are usually used only with inpatients on a short-term basis. Central venous catheters are considered a temporary access device but may be used for weeks or even months on an outpatient basis. The settings for hemodialysis include inpatient dialysis units in hospitals, outpatient dialysis centers, and the patient’s home.

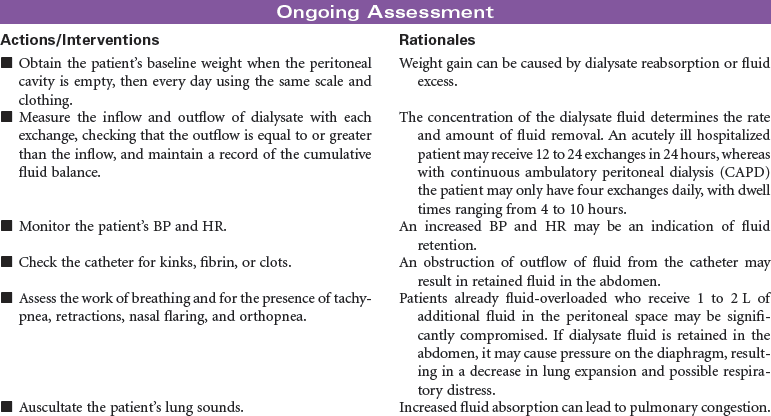
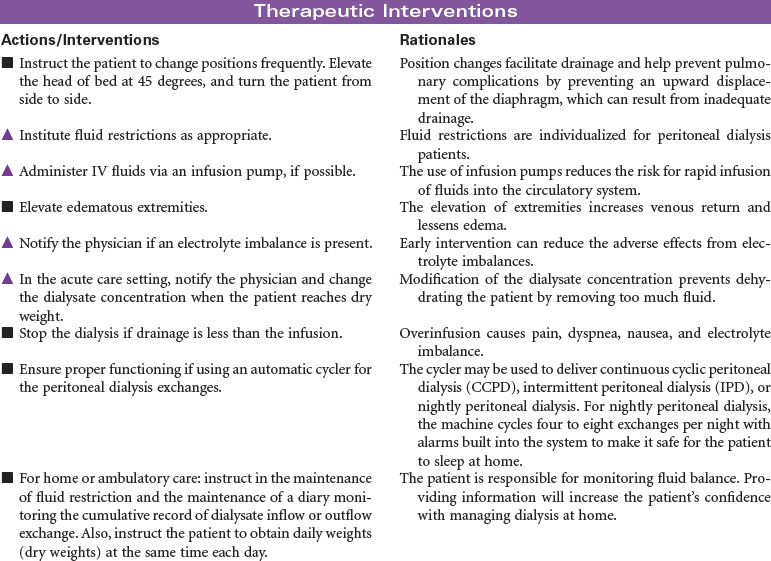
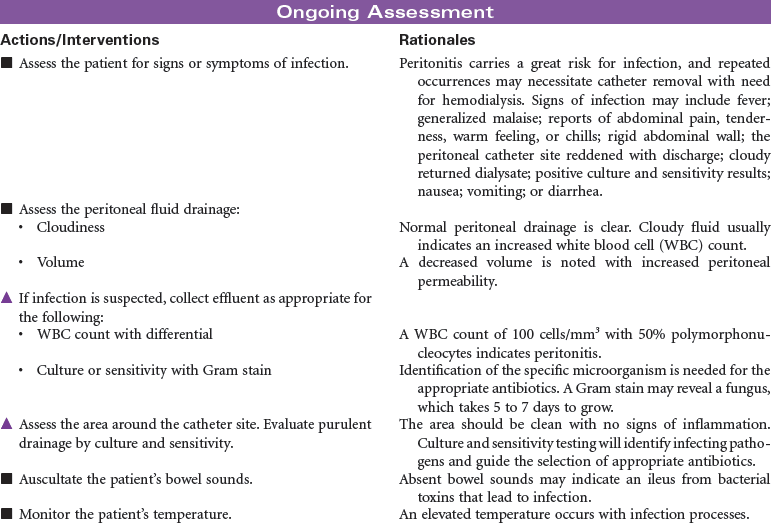
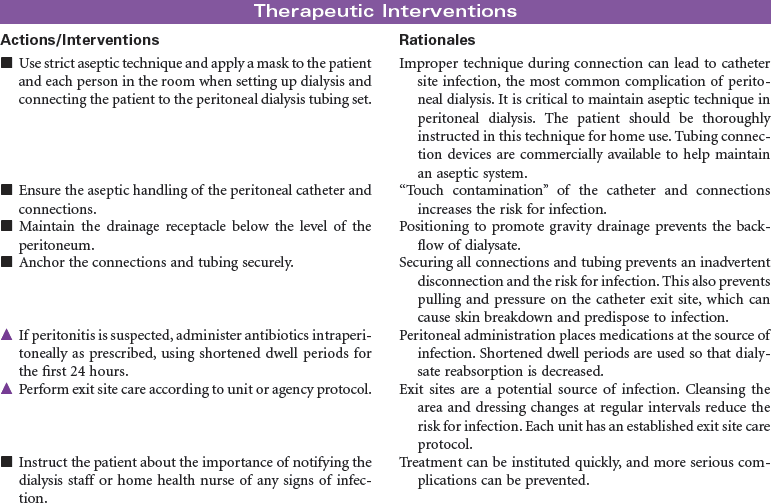
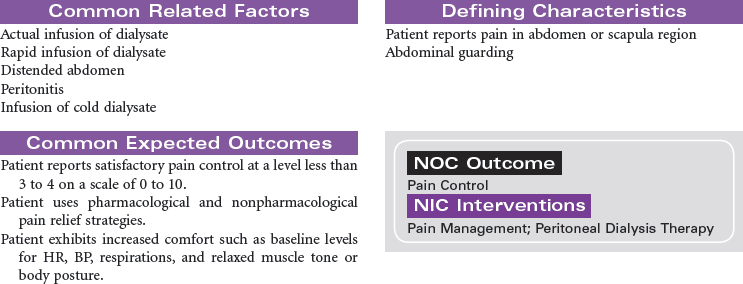
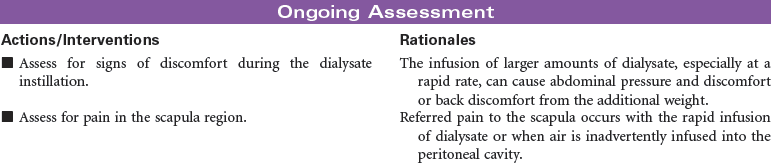
Peritoneal Dialysis
Intermittent Peritoneal Dialysis; Continuous Ambulatory Peritoneal Dialysis; Continuous Cyclic Peritoneal Dialysis; Renal Replacement Therapy
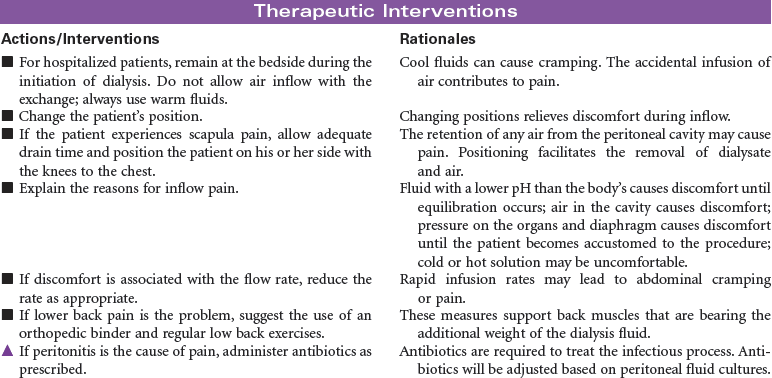
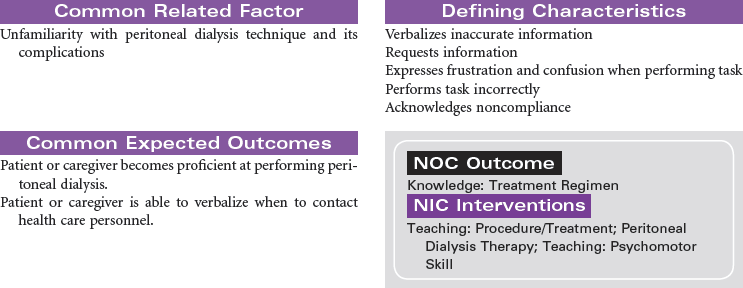
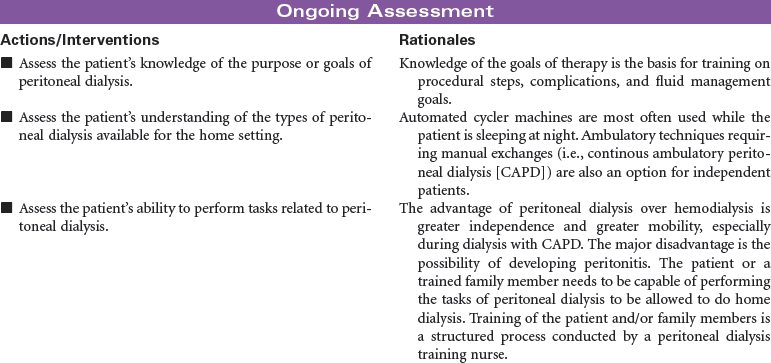
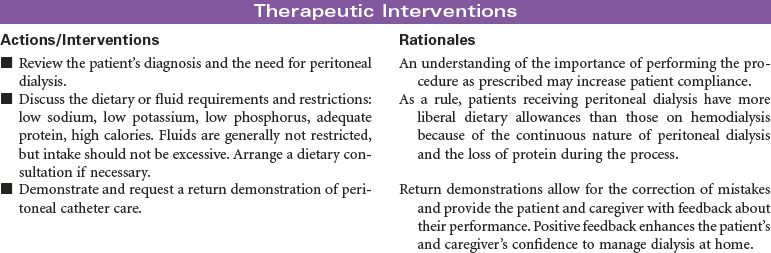
Peritoneal dialysis is indicated for patients with kidney failure who have vascular access problems, who cannot tolerate the hemodynamic alterations of hemodialysis, or who prefer the independence of managing their own therapy in their home environment. A peritoneal catheter is placed through the anterior abdominal wall to achieve access into the peritoneum. During peritoneal dialysis, the peritoneum functions as the semi-permeable membrane by which molecules flow from the side of higher concentration to the side of lower concentration. This procedure removes excess fluid and waste products from the body. Peritoneal dialysis may be performed as intermittent peritoneal dialysis, continuous ambulatory peritoneal dialysis, or continuous cyclic peritoneal dialysis. Peritoneal dialysis provides more gradual physiological changes than hemodialysis and is appropriate for the older adult patient with diabetes and cardiovascular disease. It is contraindicated in patients with peritonitis, recent abdominal surgery, or respiratory insufficiency because the fluid in the peritoneum decreases lung volume. This care plan focuses on peritoneal dialysis in the acute care setting with teaching for the ambulatory and home care setting.

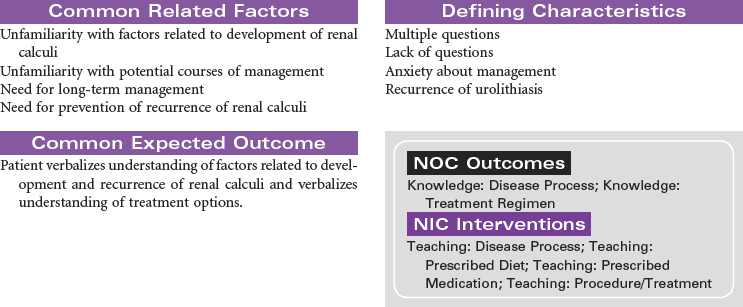
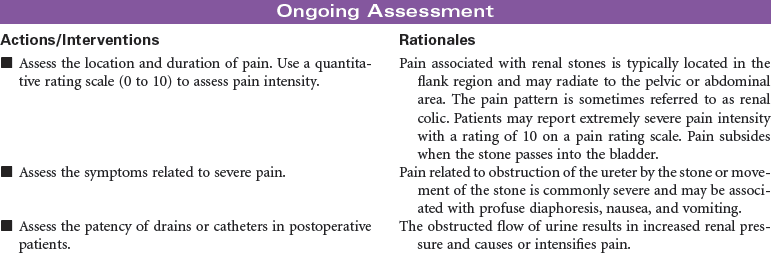
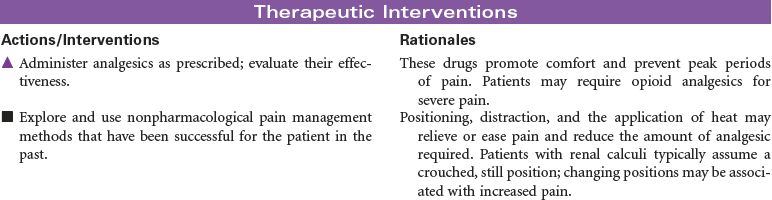
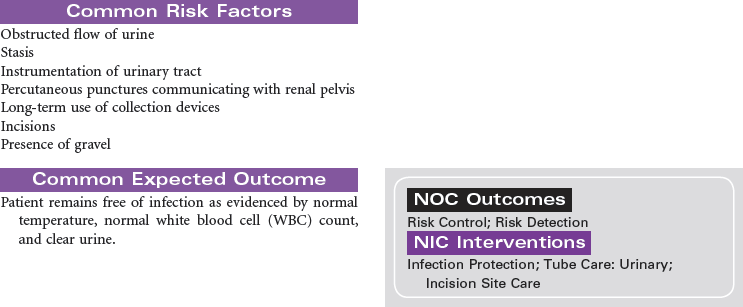
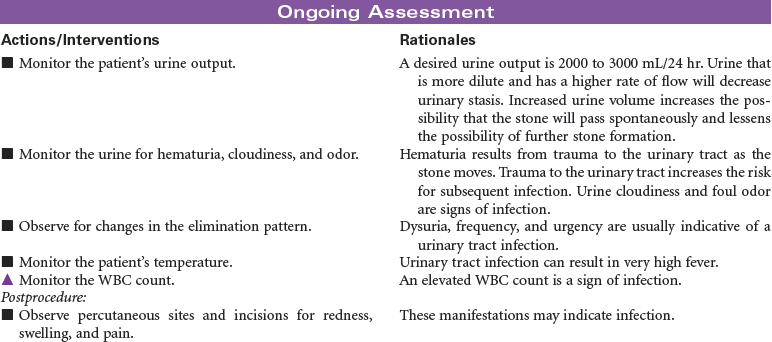
Renal Calculi
Kidney Stones; Urolithiasis; Nephrolithiasis; Staghorn Calculi
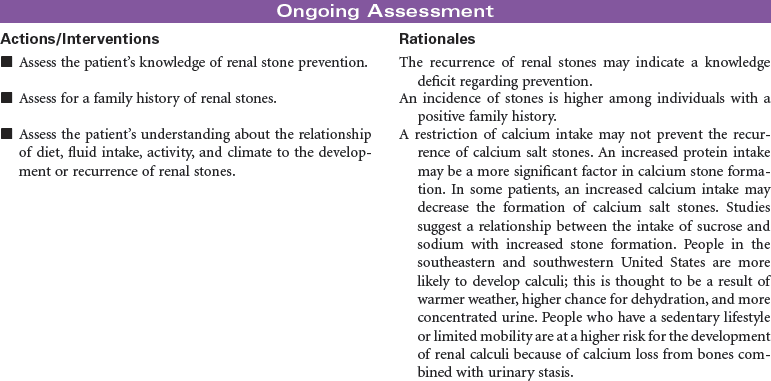
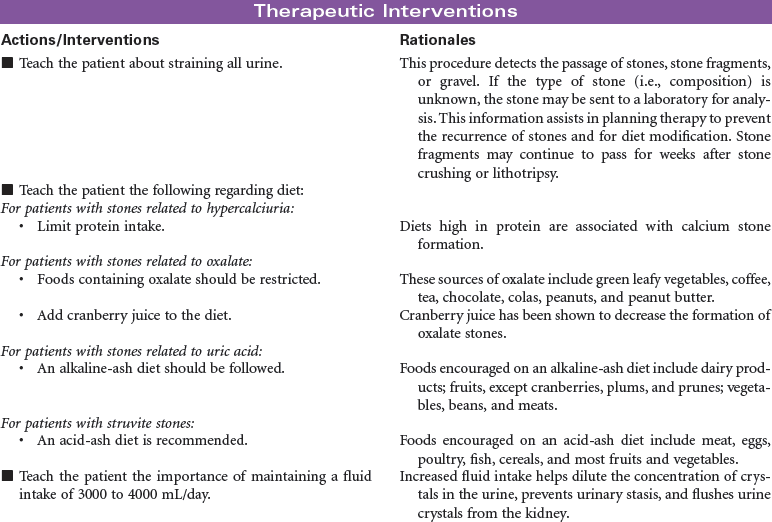
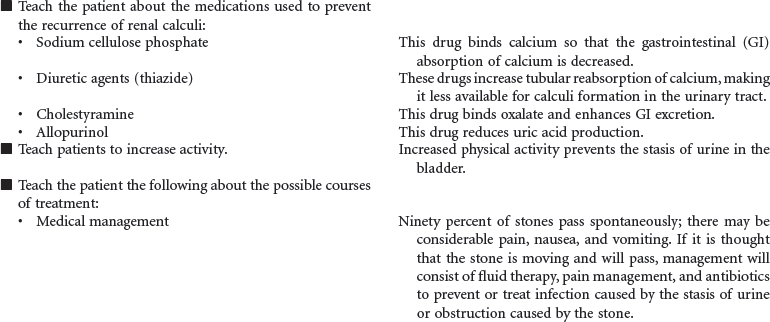
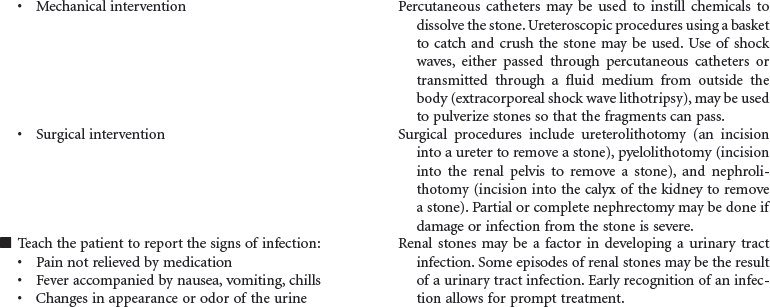
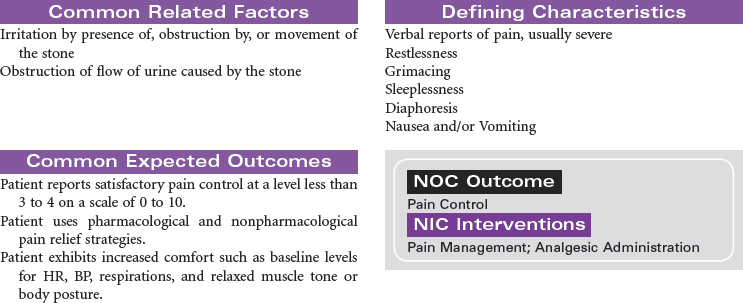
Renal stones are a common problem, affecting men more frequently than women, and Caucasians more commonly than African Americans. People in warmer climates are more commonly affected, probably indicating that dehydration is a factor. Stones may form anywhere in the urinary tract but most often form in the kidney; they commonly move to other parts of the urinary tract, causing pain, infection, and obstruction. Approximately 90% of stones pass spontaneously. Stones may be treated medically, mechanically (by nephroscopic technique or by lithotripsy [use of shock waves to crush the stones]), or surgically (by pyelolithotomy or nephrolithotomy). Renal stones may be made up of calcium phosphate, calcium oxalate, uric acid, cystine, magnesium ammonium phosphate (so-called struvite stones), or combinations of these substances. Calculi develop in situations associated with decreased urine flow, urinary tract injury, and metabolic disorders that alter calcium balance. Changes in urine pH and side effects of some drugs also may contribute to stone formation. Staghorn calculi are large stones that fill and obstruct the renal pelvis. The process of stone formation begins with supersaturation of the urine by one or more salts. As the concentration of salts in the urine increases, the salts precipitate into a solid state. These solid-state salts form crystals that grow into a stone. This growth process is influenced by the pH of the urine, the patient’s hydration status, the presence of other crystals and biological material in the kidney, structural changes in the urinary tract, and crystal growth–inhibiting substances. This care plan addresses management of the patient hospitalized with kidney stones; it also addresses postoperative and postlithotripsy care.


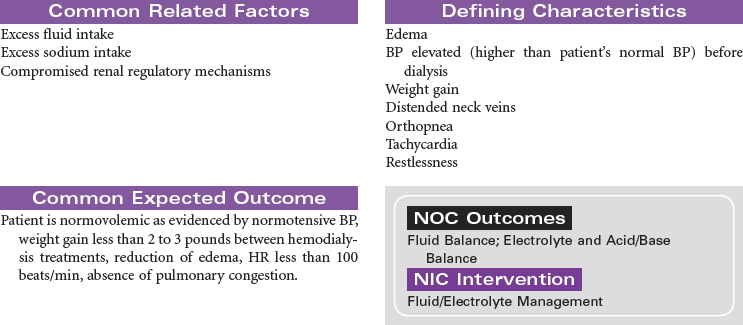
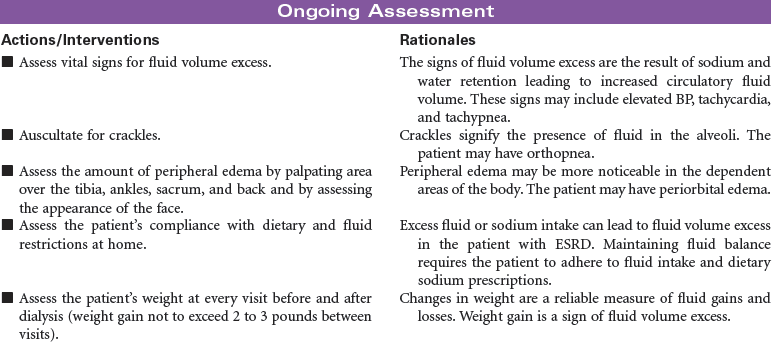
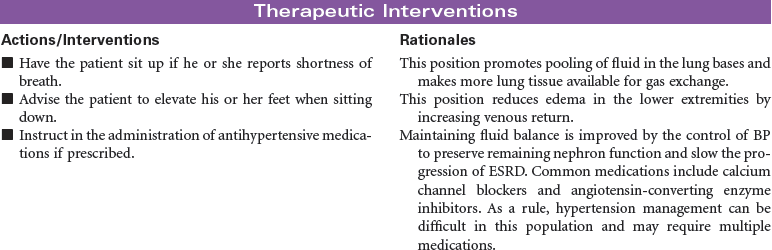
Renal Failure, Chronic/End-Stage Renal Disease
Uremia, Chronic Kidney Disease (CKD)
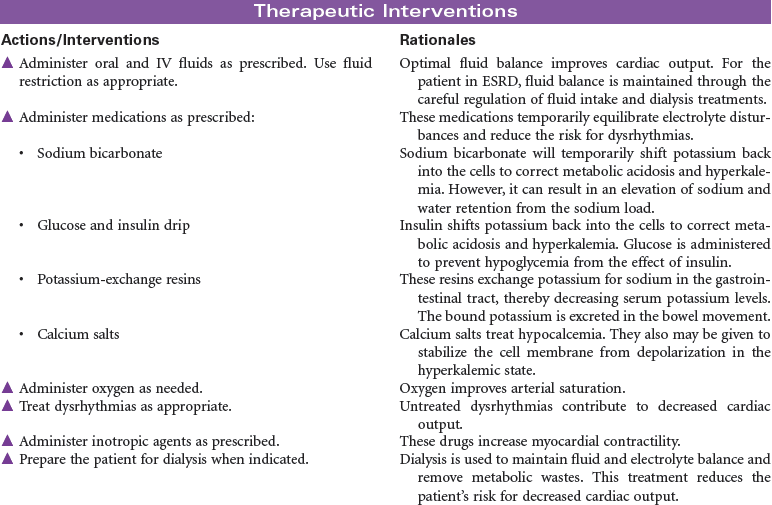
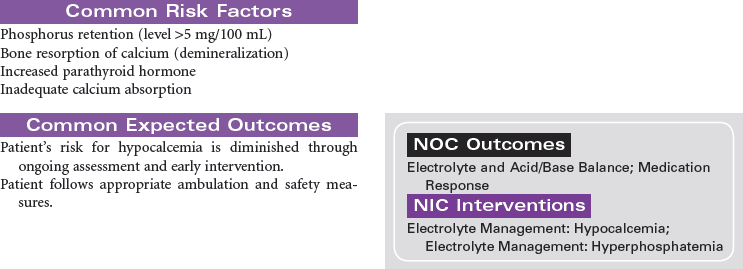
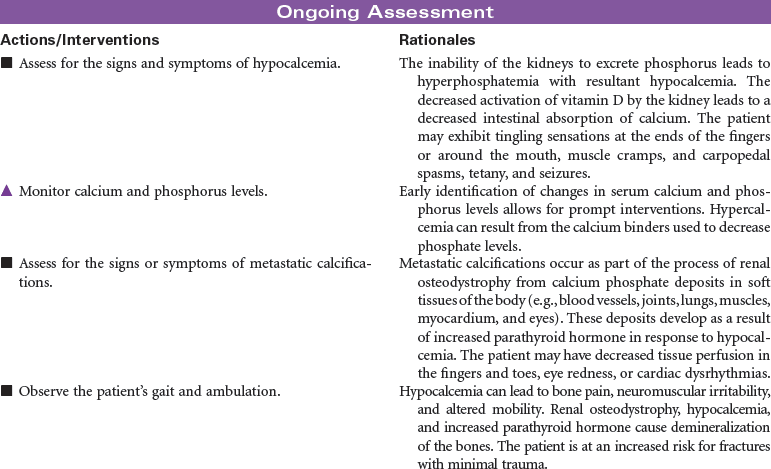
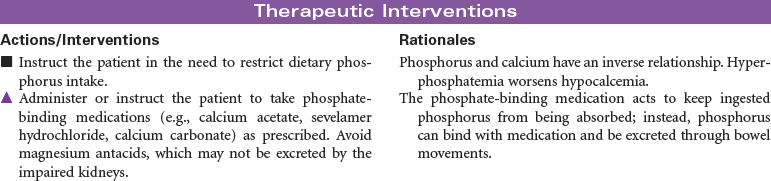
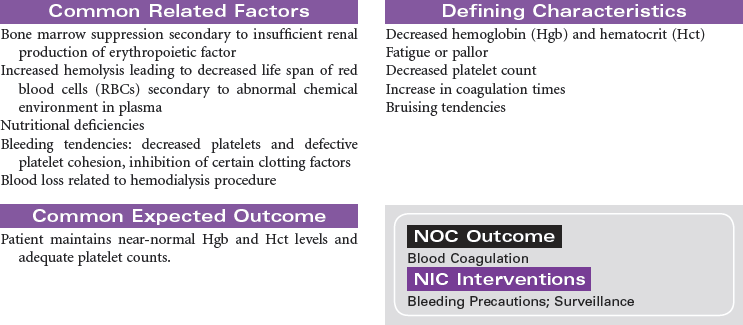
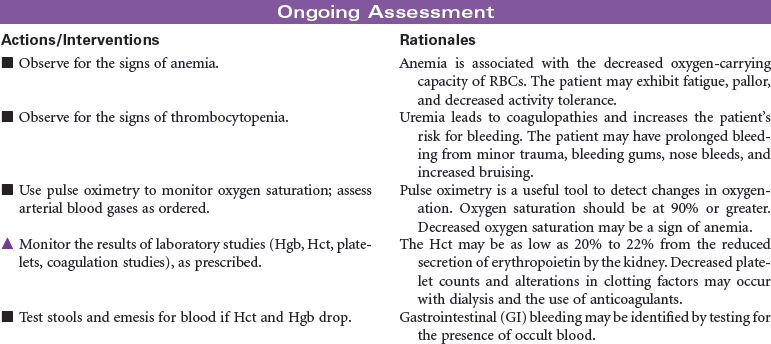
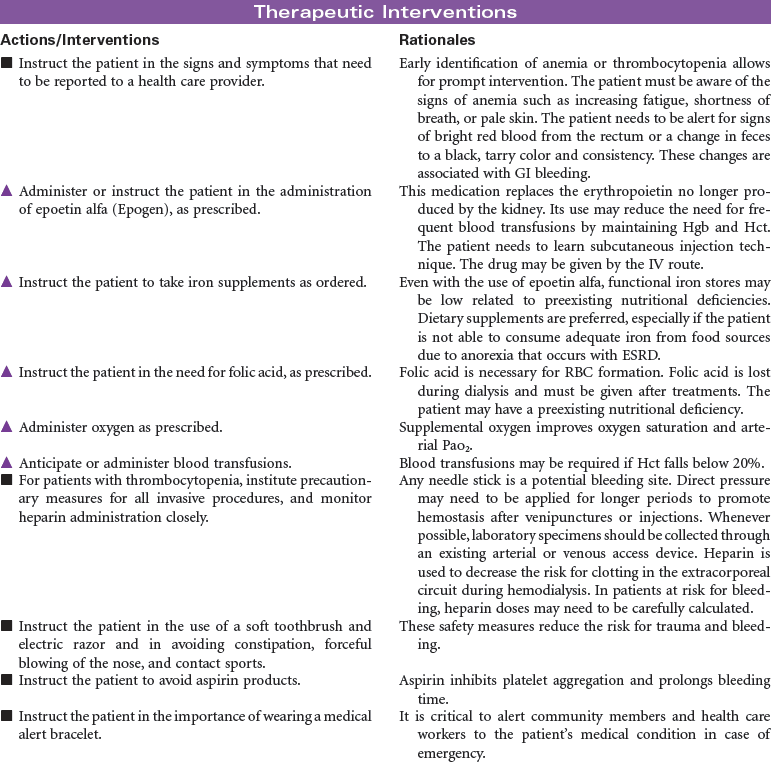
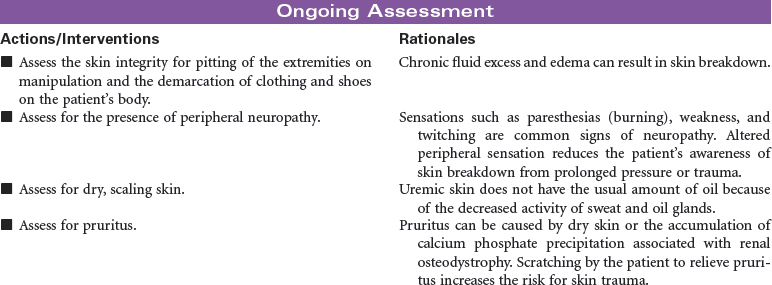
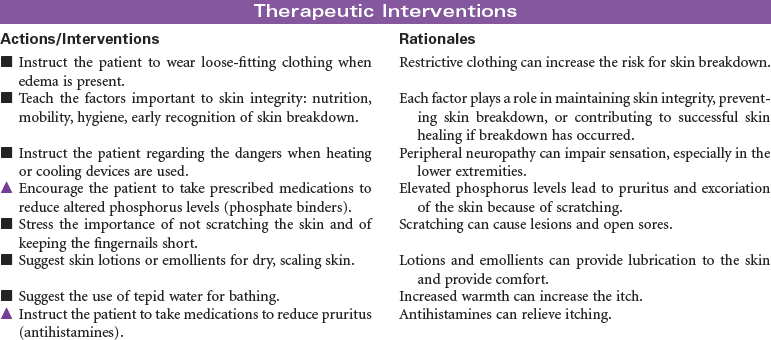
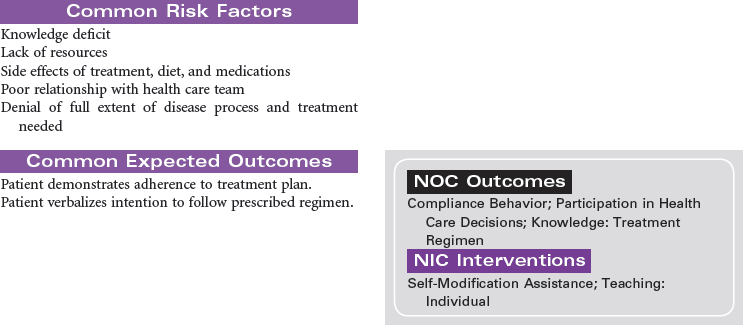
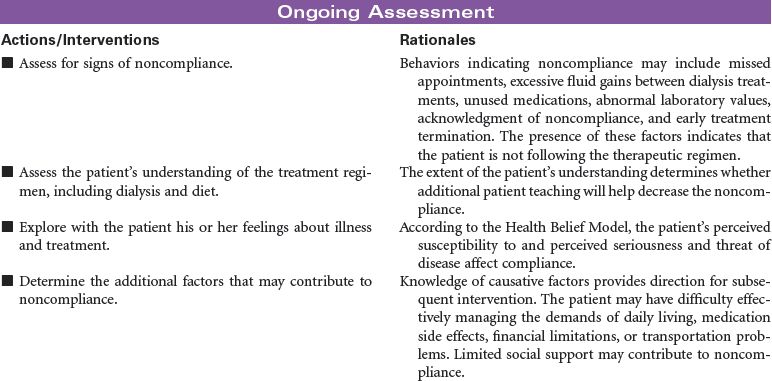
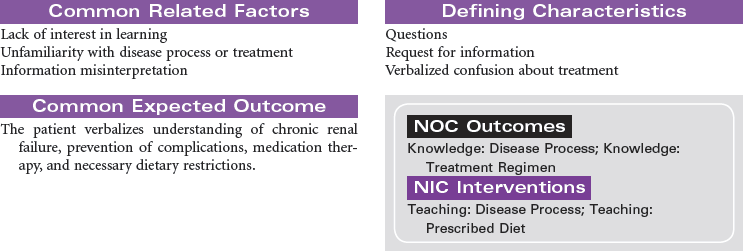
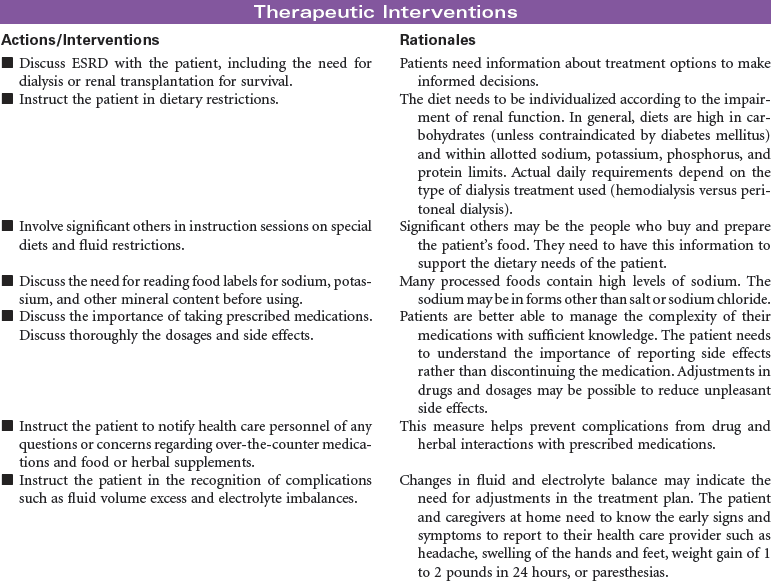
End-stage renal disease (ESRD) is defined as irreversible kidney disease, causing chronic abnormalities in the body’s homeostasis and necessitating treatment with dialysis or renal transplantation for survival. The patient with chronic renal failure may lose up to 80% of nephron function and exhibit few signs of renal failure other than increasing blood urea nitrogen and serum creatinine levels. In ESRD, also called stage 5 chronic kidney disease, the glomerular filtration rate (GFR) has decreased to less than 15 mL/min/1.73 m2. African Americans have a higher incidence of ESRD than Caucasian. Diabetes and hypertension are the most common causes. Uremia, or uremic syndrome, consists of the signs, symptoms, and physiological changes that occur in renal failure. These changes involve all body systems and are related to fluid and electrolyte abnormalities, accumulation of uremic toxins that cause physiological changes and altered function of various organs, and regulatory function disorders (e.g., hypertension, renal osteodystrophy, anemia, and metastatic calcifications). Patients with ESRD may be limited in their ability to carry out normal activities. This care plan may be used for the patient with ESRD in inpatient, outpatient, or at-home settings.



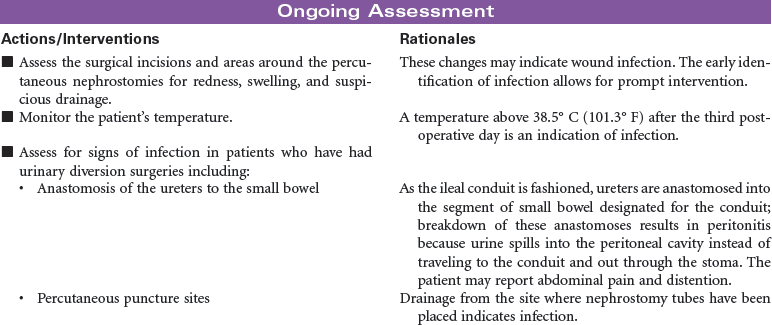
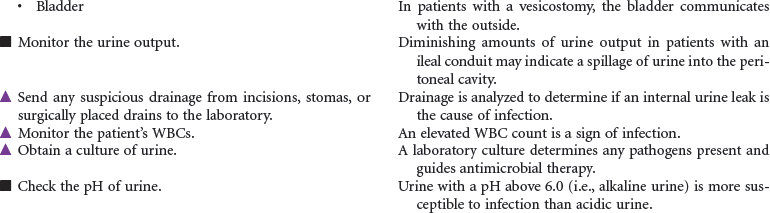
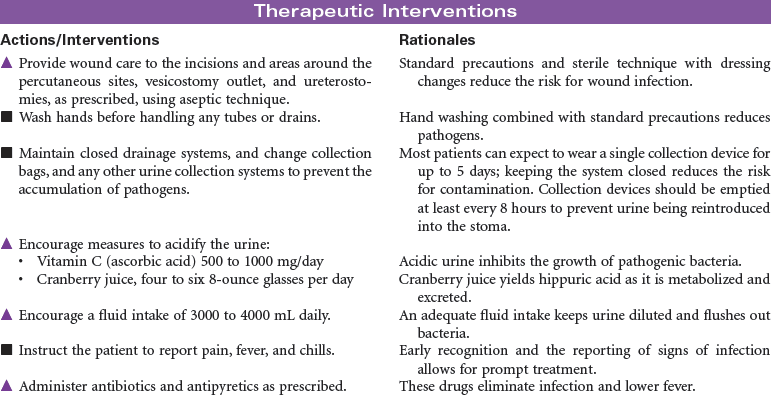
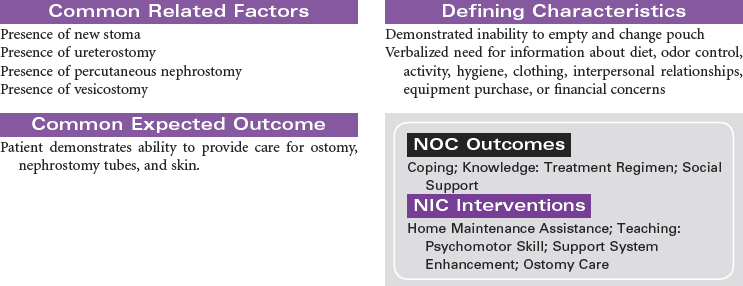
Urinary Diversion
Bladder Cancer; Ileal Conduit; Koch Pouch; Nephrostomy; Sigmoidostomy; Ureterostomy; Vesicostomy
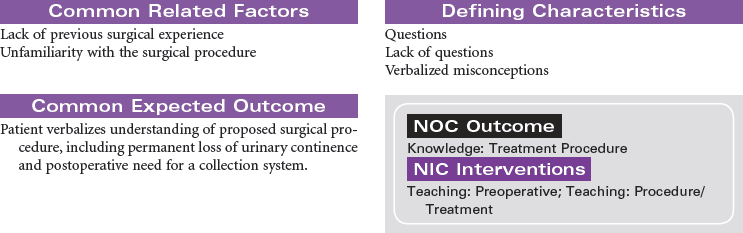
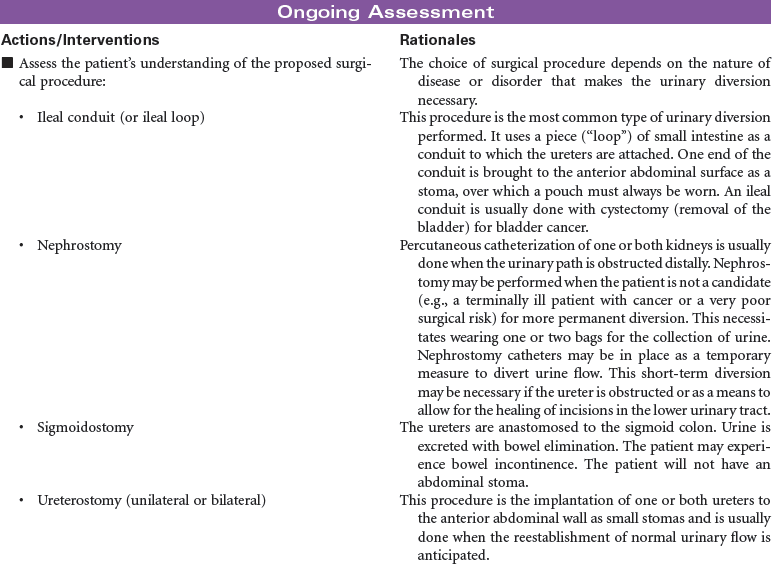
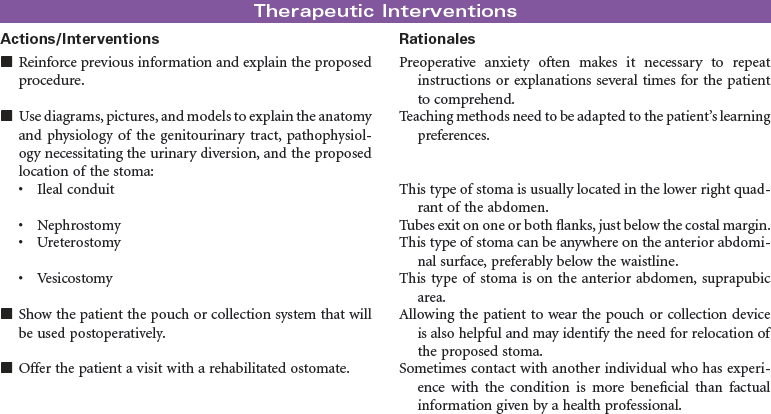
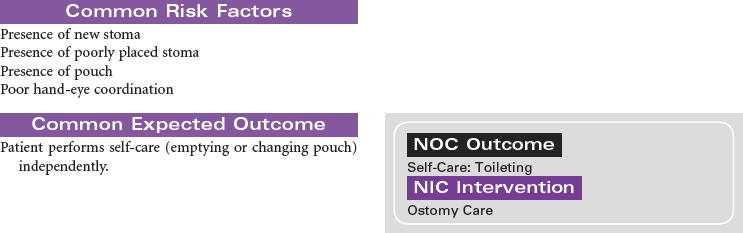
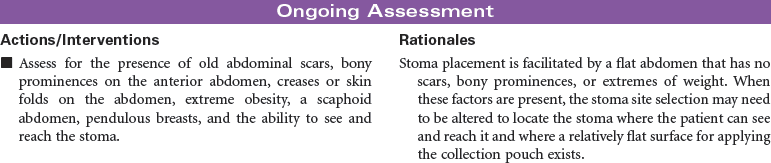
Urinary diversion is the surgical diversion of urinary flow from its usual path through the urinary tract. Urinary diversion procedures may be performed as a result of obstruction of the urinary tract; destruction of normal urinary structures by trauma; neurogenic bladder caused by disease or injury; and cancer, usually of the bladder. Urinary diversion may be temporary or permanent depending on the underlying problem. Bladder cancer occurs more often in older men than in women. When the tumors are superficial in the bladder wall, a variety of surgical procedures can be performed to remove the tumor and maintain normal urinary tract function. These procedures include transurethral resection, laser photocoagulation, and segmental cystectomy. If the bladder tumor is invasive and involves the trigone area, the preferred treatment is total cystectomy with a urinary diversion to maintain outflow of urine. Some procedures result in incontinence and necessitate the wearing of a collection system or pouch. Other procedures reroute the urinary flow to another structure (e.g., a surgically created internal reservoir, colon) from which the urine is eventually excreted (often called continent procedures). Nephrostomy may be performed under fluoroscopic control as an outpatient procedure. Other diversions require open abdominal surgery, and the patient is typically hospitalized for 4 to 7 days. This care plan addresses nursing care for new postoperative patients, as well as for individuals who have undergone urinary diversion at some point in the past.



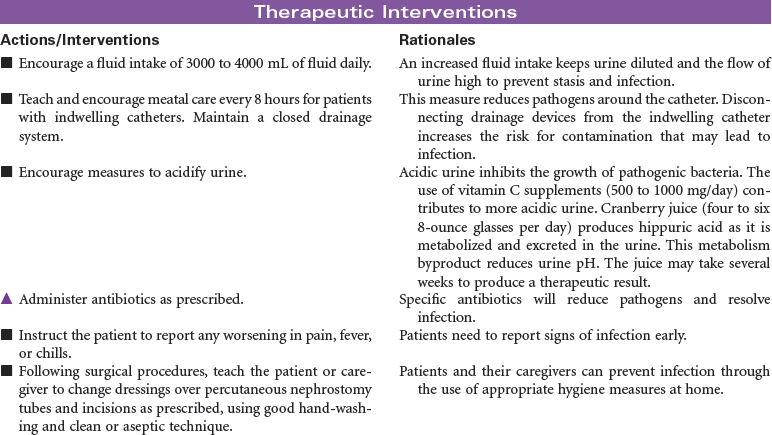
Urinary Tract Infection
UTI; Pyelonephritis; Cystitis; Urethritis; Nephritis
Urinary tract infection (UTI) is an invasion of all or part of the urinary tract (kidneys, bladder, urethra) by pathogens. UTIs are usually caused by bacteria, most typically Escherichia coli, although viral and fungal organisms also may cause UTI. UTIs may begin as pathogens from the perineum and ascend through the urethra to the urinary bladder. UTIs are common nosocomial infections and often result following instrumentation (e.g., catheterization or diagnostic procedures of the genitourinary tract). The Centers for Disease Control and Prevention (CDC) has prepared guidelines for prevention of catheter-associated urinary tract infection (CAUTI). These guidelines include recommendations for appropriate use of urinary catheters in hospital and long-term care settings, and alternatives to indwelling urinary catheters for management of patient problems with urination. UTIs are more common in women than men, particularly in sexually active, younger women. UTIs, which can be chronic and recurring, can lead to systemic infection such as urosepsis, which can be life-threatening. In older patients, diagnosis and treatment of UTIs may be delayed because patients are often asymptomatic or demonstrate only subtle cognitive changes and urinary incontinence rather than the typical complaints of urgency, frequency, burning, and pain on urination. If infections of the urinary tract are not treated effectively, renal damage and loss of renal function can occur. The focus of this care plan is care of any individual with a UTI in any setting.




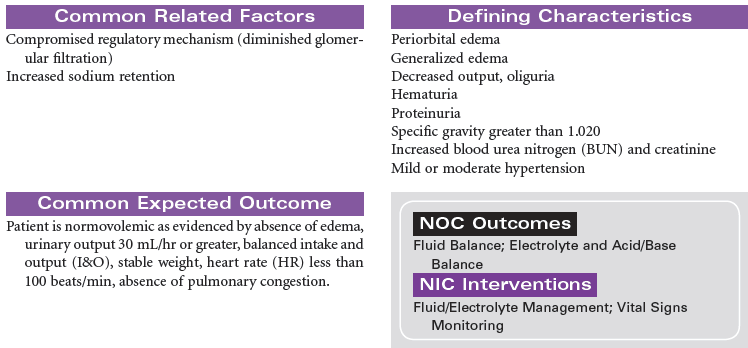
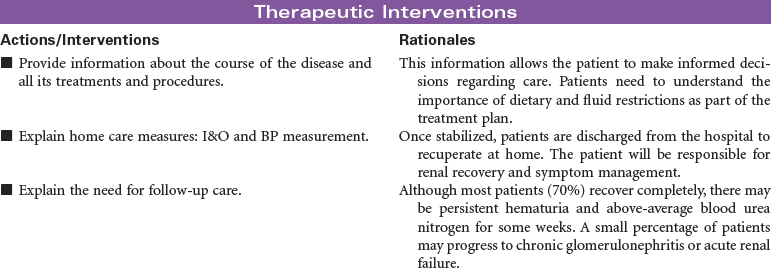
Glomerulonephritis
Acute Poststreptococcal Glomerulonephritis; Acute Glomerulonephritis; Rapidly Progressive Glomerulonephritis; Chronic Glomerulonephritis
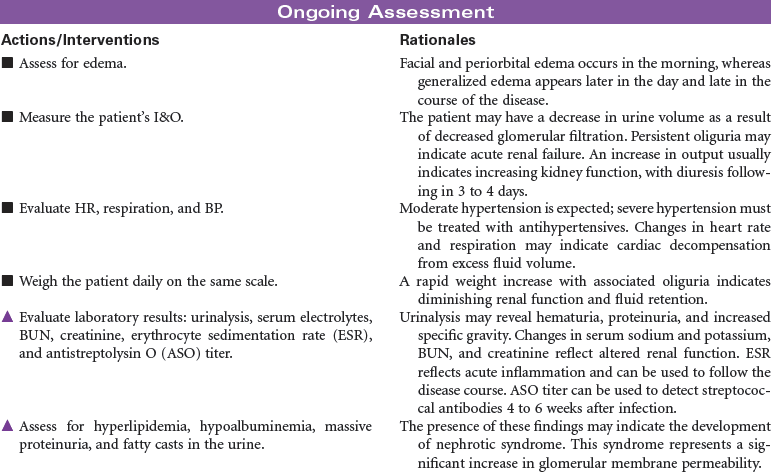
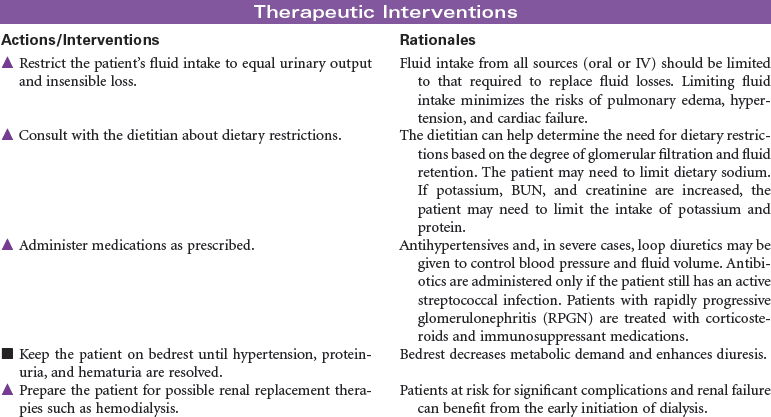
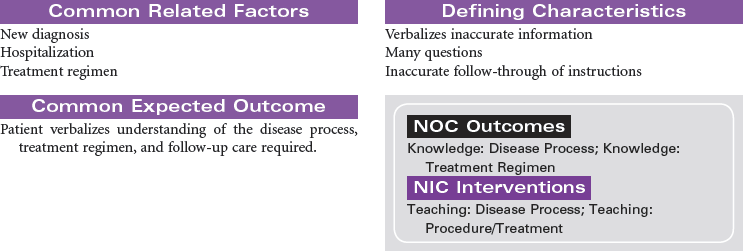
Glomerulonephritis is caused by an immune response that produces inflammation in the glomerulus and related renal tissues. The stimulus for this immune response may include bacterial or viral infection, drugs or other nephrotoxic chemicals, and diseases such as systemic lupus erythematosus and scleroderma. Antigen–antibody complexes accumulate in the glomerulus. An inflammatory response occurs, resulting in decreased glomerular filtration and increased membrane permeability to red blood cells and large protein molecules. The inflammatory process may include tubular, interstitial, and vascular tissues. An acute form of glomerulonephrites occurs in the patient after recovery from a streptococcal infection. This form of the disease is more common in children and young adults. Rapidly progressive glomerulonephritis (RPGN) is another form of the disease precipitated by a variety of causes such as infection and nephrotoxic drugs. Acute glomerulonephritis and RPGN may progress to chronic glomerulonephritis. The patient with chronic glomerulonephritis is often asymptomatic, and the disease goes undetected. All forms of glomerulonephritis may cause acute or chronic renal failure. The treatment of glomerulonephritis depends on the underlying cause and the extent of impaired glomerular filtration. Symptom management is the primary focus of care. In severe forms of the disease, the patient may require renal replacement therapy such as dialysis or kidney transplantation.