Endocrine and Metabolic Care Plans
 For additional care plans, go to http://evolve.elsevier.com/Gulanick/.
For additional care plans, go to http://evolve.elsevier.com/Gulanick/.
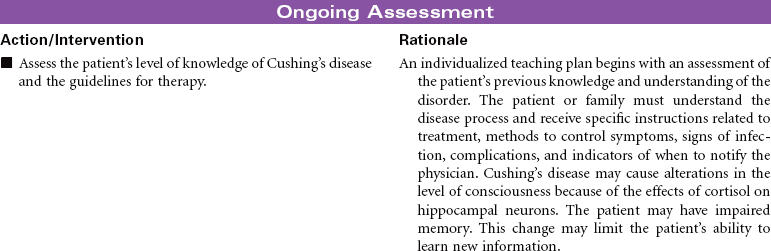
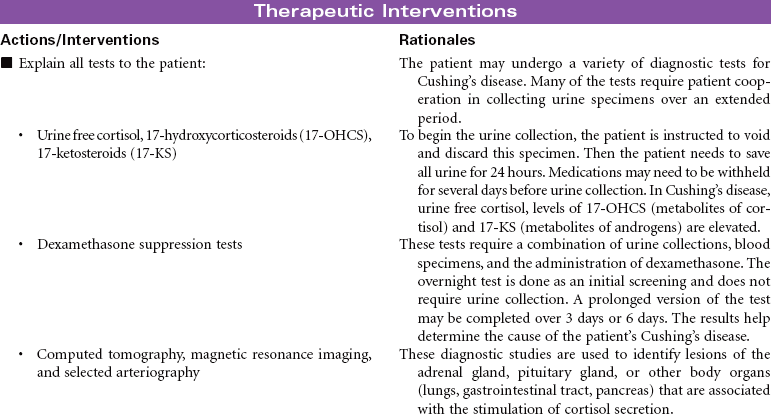
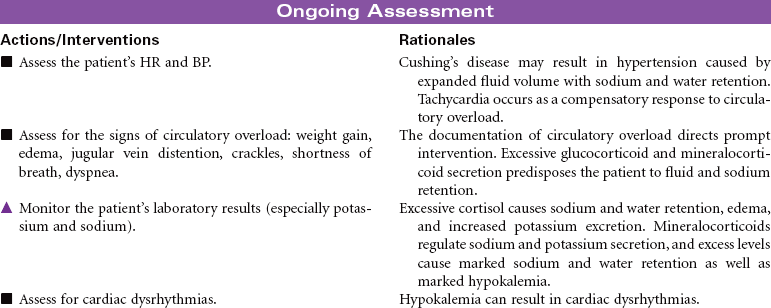
Cushing’s Disease
Hypercortisolism; Cushing’s Syndrome; Adrenocortical Hyperfunction
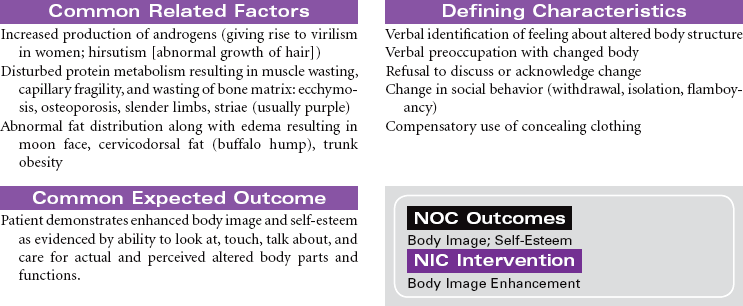
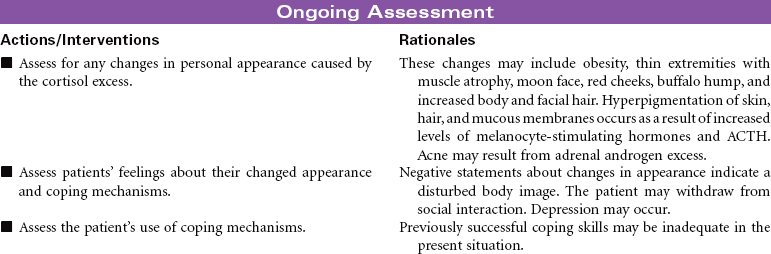
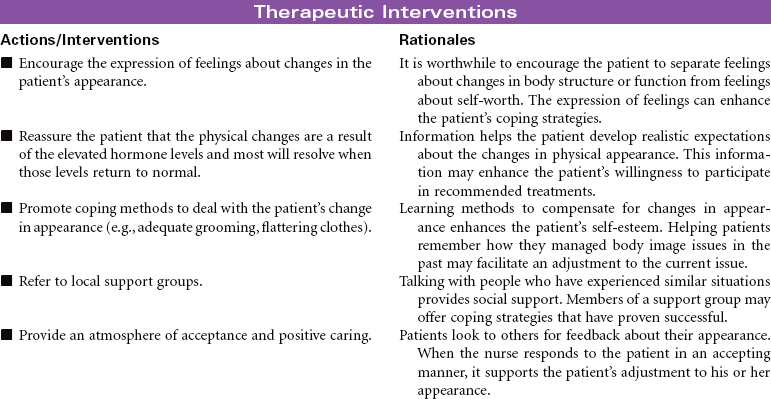
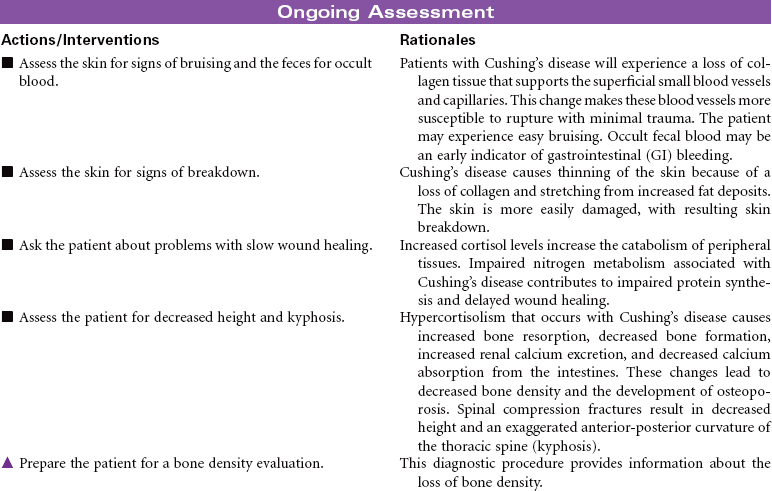
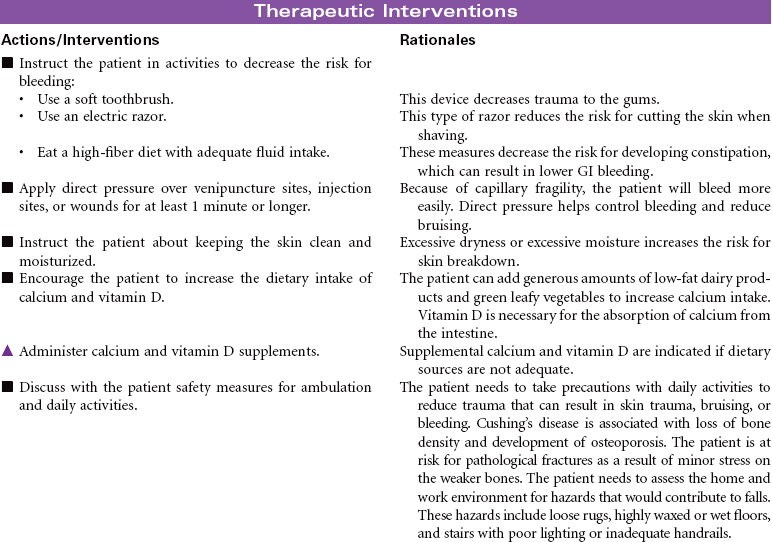
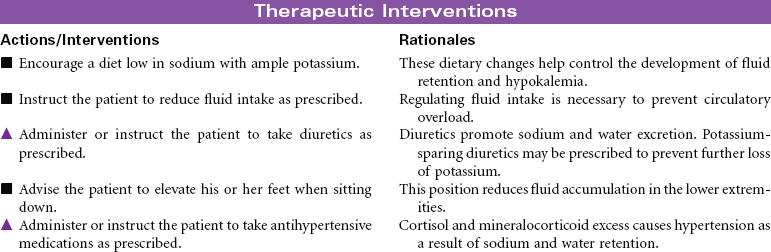
Cushing’s disease reflects an excess of cortisol. Depending on the cause of the disease, mineralocorticoids and androgens also may be secreted in increased amounts. The disorder may be primary (an intrinsic adrenocortical disorder [e.g., neoplasm]), secondary (from pituitary or hypothalamic dysfunction with increased adrenocorticotrophic hormone secretion resulting in glucocorticoid excess), or iatrogenic (from prolonged or excessive administration of corticosteroids). The disease results in fluid and electrolyte disturbances, suppressed immune response, altered fat distribution, and disturbances in protein metabolism. Changes in physical appearance that occur with Cushing’s disease can have significant influence on the patient’s body image and emotional well-being. The focus of this care plan is on the ambulatory patient with Cushing’s disease.
 Deficient Knowledge
Deficient Knowledge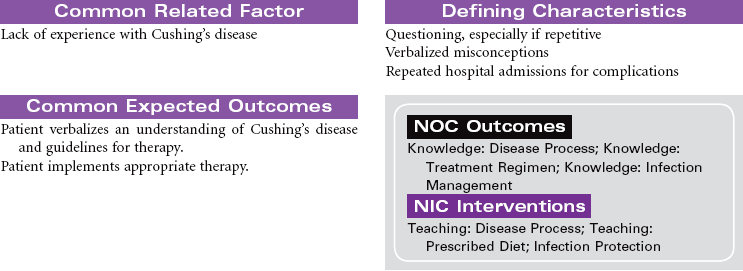
Diabetes Mellitus
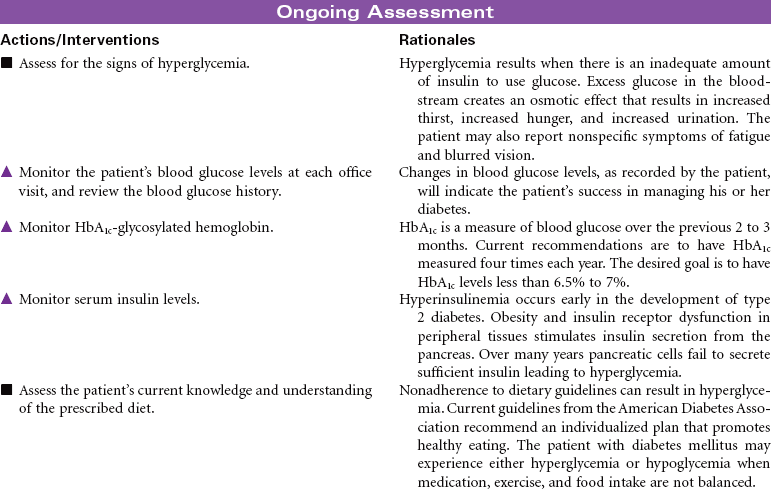
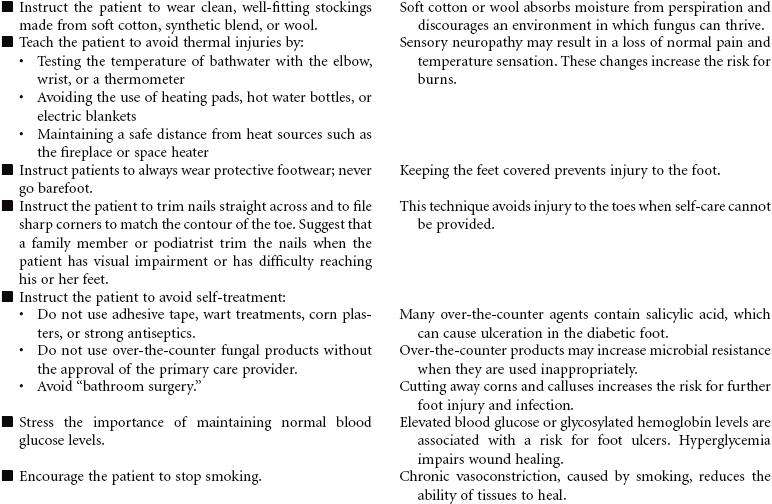
Diabetes mellitus is a disorder of metabolism in which carbohydrates, fats, and proteins cannot be used for energy. Insulin, a hormone secreted by islet cells of the pancreas, is required to facilitate movement of glucose across cell membranes. Once inside the cell, glucose is the primary metabolic fuel. Type 1 diabetes occurs when the pancreas is no longer able to secrete insulin. This condition occurs as a result of an autoimmune process with destruction of pancreatic beta cells and has its onset between ages 1 and 24 years. The autoimmune process is triggered by a combination of genetic predisposition and environmental stimuli such as a virus. The result of the insulin deficiency is hyperglycemia. It represents 5% to 10% of the cases of diabetes. Type 2 diabetes results because of resistance of peripheral tissue receptors to the effects of insulin. This type of diabetes also has a genetic predisposition for insulin resistance in skeletal muscles, fat cells, and liver cells. Type 2 diabetes is characterized by hyperinsulinemia and hyperglycemia. Over time the beta cells of the pancreas fail to produce sufficient insulin. Its onset is slow and gradual, with many individuals having had the disease 10 years before diagnosis. It represents 90% to 95% of the cases of diabetes. This is usually a condition of middle-aged to older individuals, although a recent increase in the incidence of type 2 diabetes has occurred in children. Obesity is a major factor in the development of type 2 diabetes in both children and adults. Current studies relate waist circumference of 40 inches for men and 35 inches for women to increased risk for this form of diabetes.
Diabetes is a major public health problem; more than 16 million individuals, or 6.5% of the population, have the disease. Diabetes causes significant morbidity and mortality. Seventy percent of diabetes-related deaths are from cardiovascular disease. The severity of dyslipidemia and hypertension is higher in the person with type 2 diabetes. Diabetes is the most common single cause of end-stage renal disease in the United States. Diabetic retinopathy is the most frequent cause of new cases of blindness among adults 20 to 74 years of age. Diabetes is the leading cause of nontraumatic lower extremity amputations in the United States. This care plan concentrates on the care of individuals with type 2 diabetes.
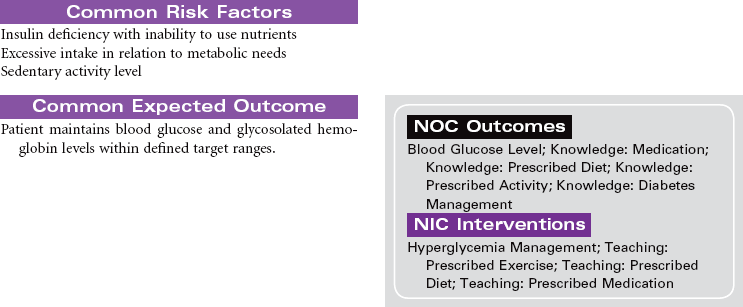
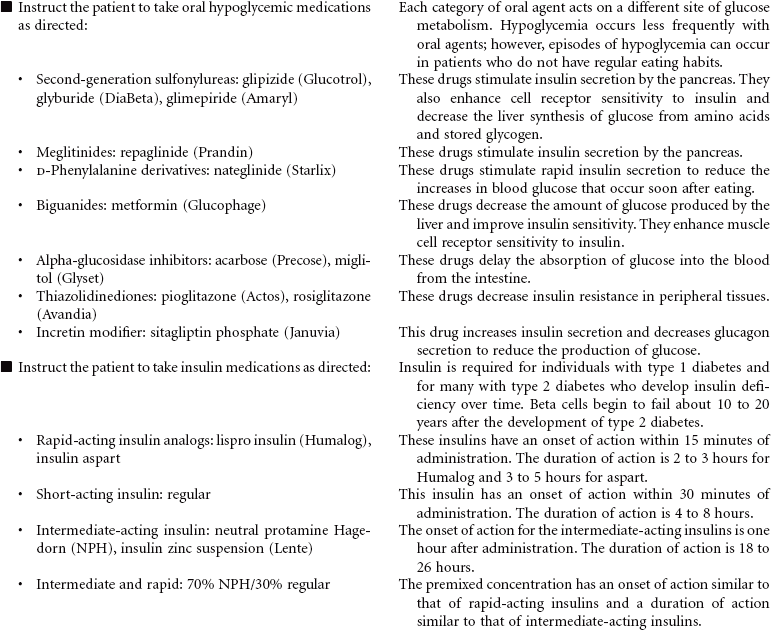
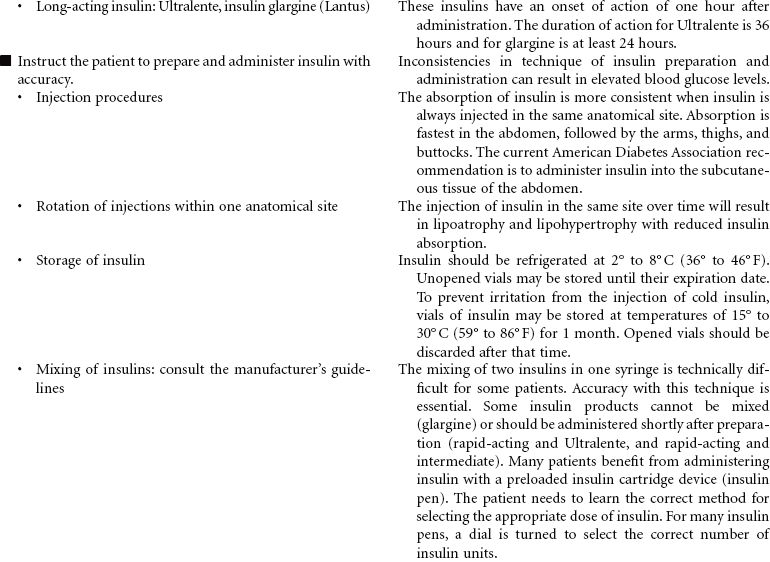
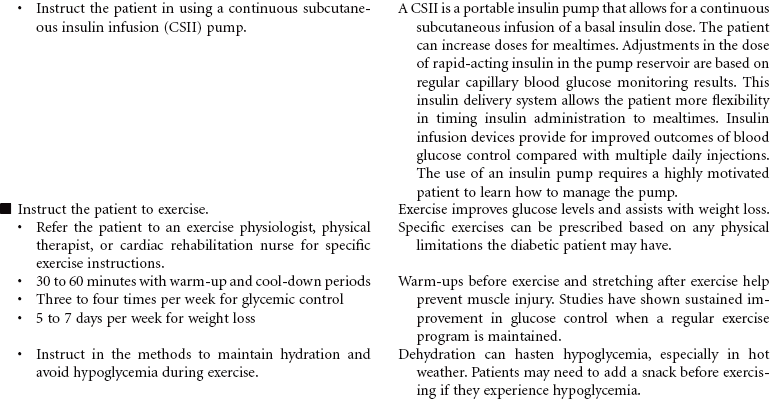
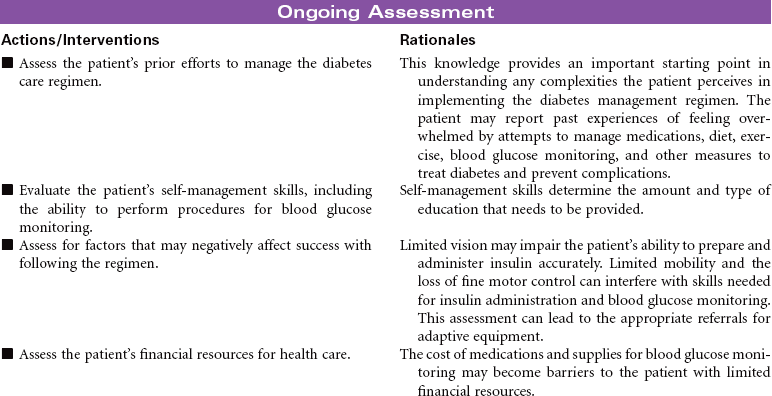
 Risk for Ineffective Therapeutic Regimen Management
Risk for Ineffective Therapeutic Regimen Management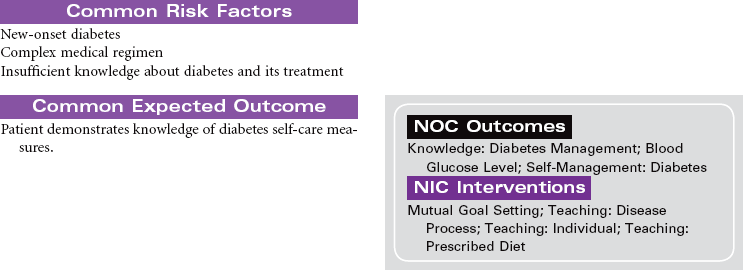

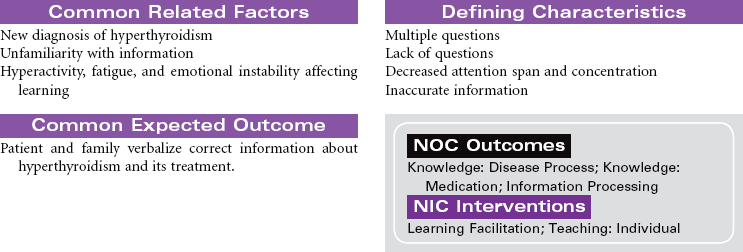
Hyperthyroidism
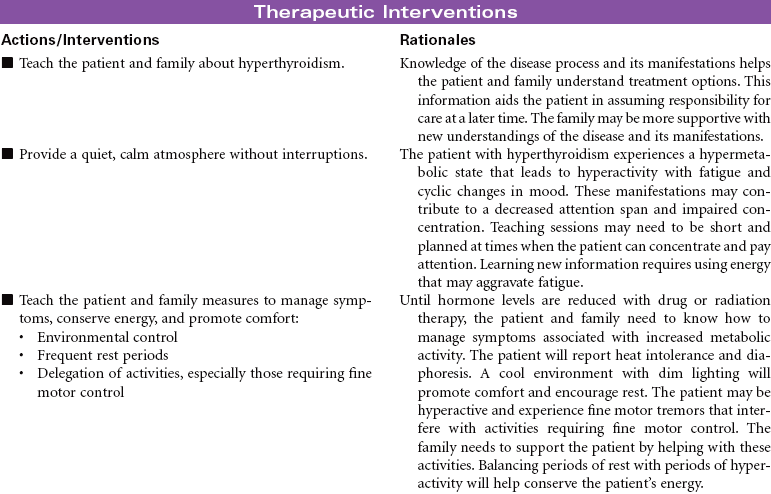
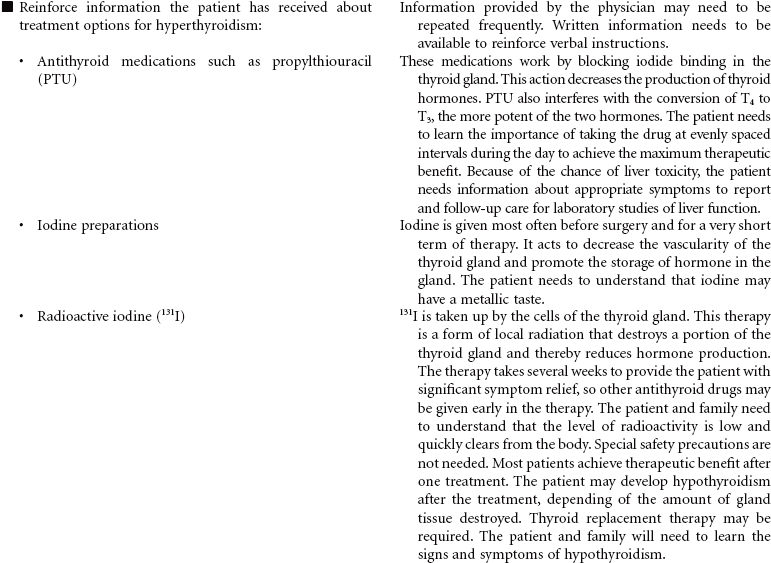
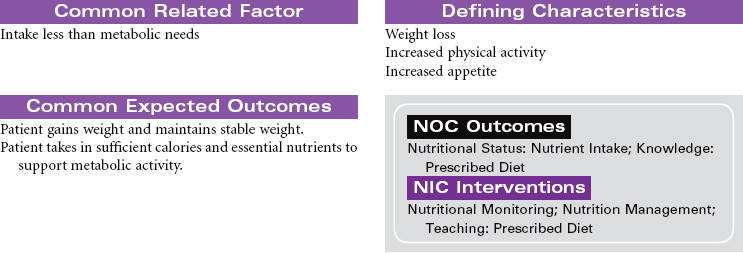
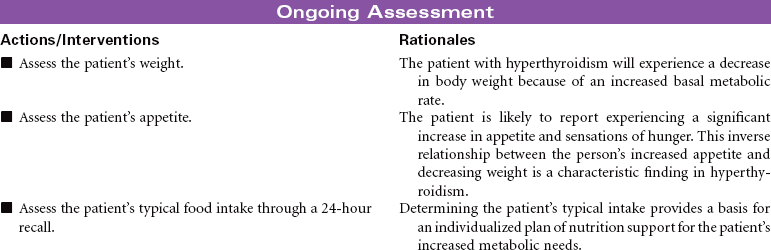
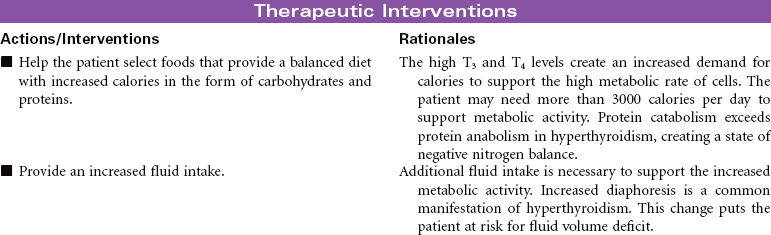
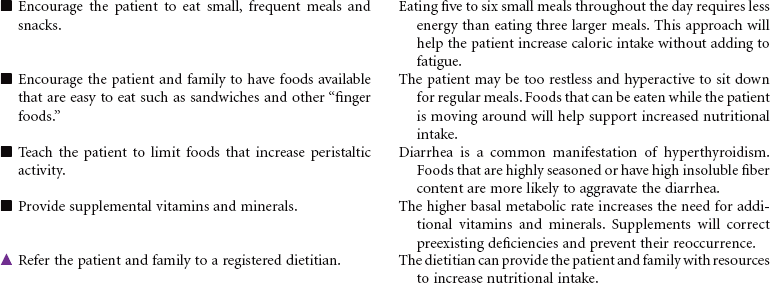
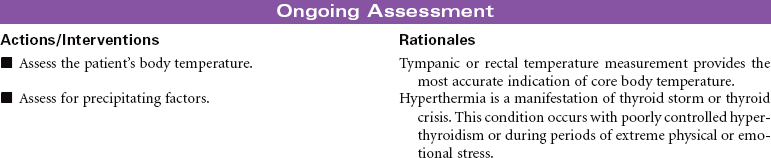
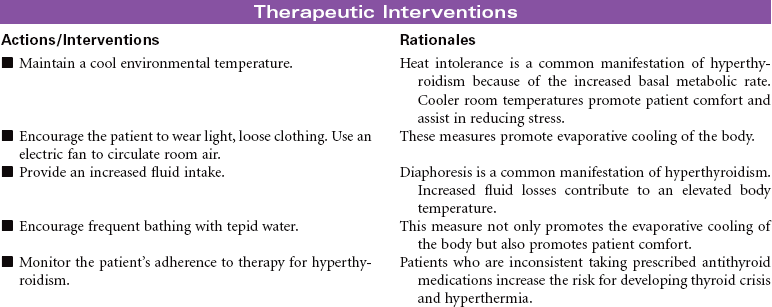
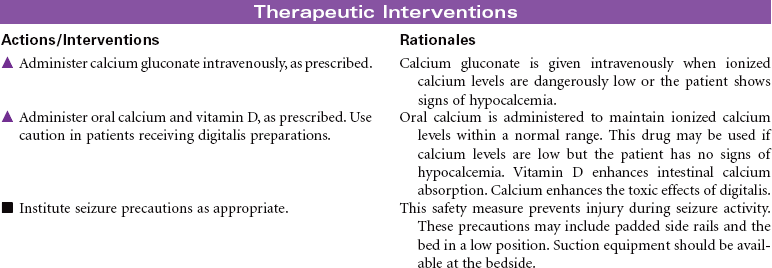
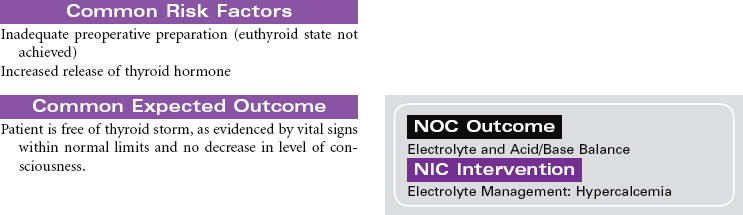
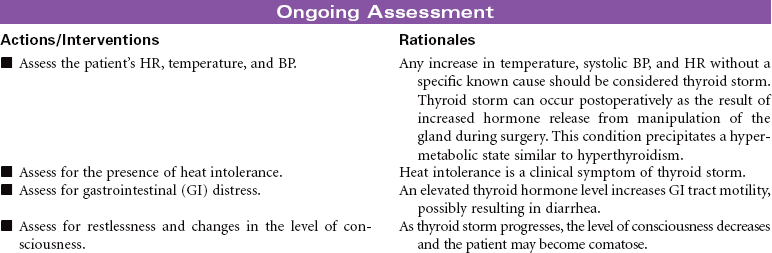
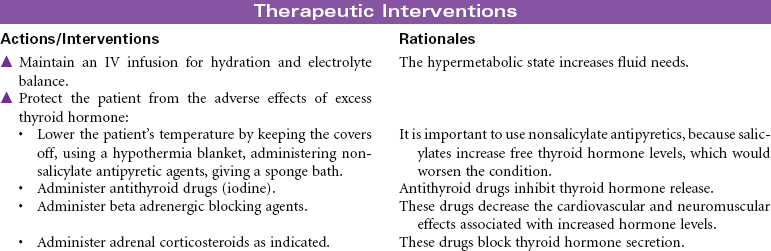
Hyperthyroidism occurs as a result of increased circulating levels of thyroid hormones. Women are affected more often than men. The peak age for diagnosis of the disorder is 20 to 40 years. The most common cause is Graves’ disease. This form of hyperthyroidism is an autoimmune disorder that contributes to a failure of the normal regulation of thyroid hormone secretion. Other causes of hyperthyroidism include toxic multinodular goiter, thyroid gland tumors, and pituitary gland tumors. The clinical manifestations of hyperthyroidism develop as a result of the hypermetabolic effects of increased thyroid hormones on all body systems. These manifestations include heat intolerance, irritability, restlessness, goiter, tachycardia, palpitations, increased blood pressure, diaphoresis, weight loss, increased appetite, diarrhea, visual changes, menstrual irregularities, and changes in libido. Thyrotoxic crisis or thyroid storm is a rare but severe form of hyperthyroidism that develops suddenly in response to excessive stress or poorly controlled hormone levels. The management of hyperthyroidism includes drug therapy, radioactive iodine therapy, and surgical removal of all or part of the thyroid gland.


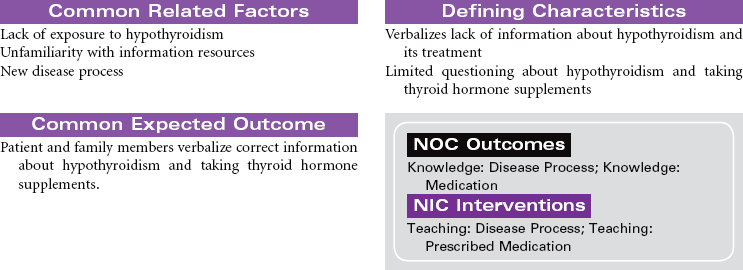
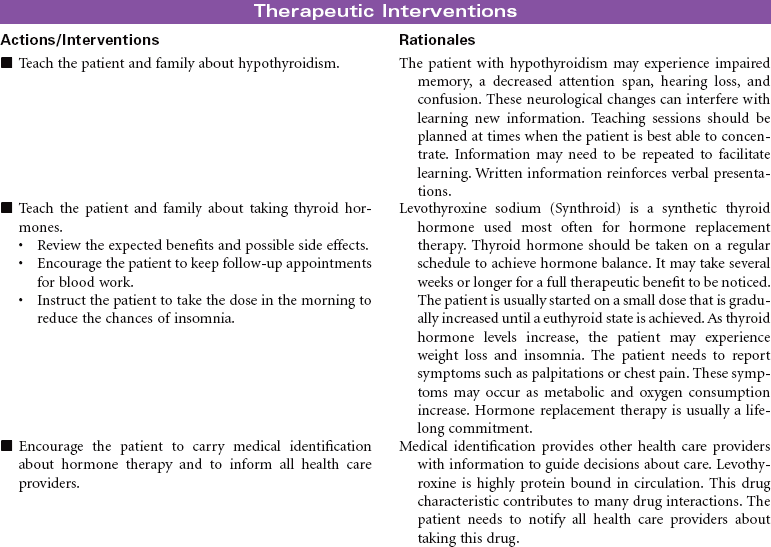
Hypothyroidism
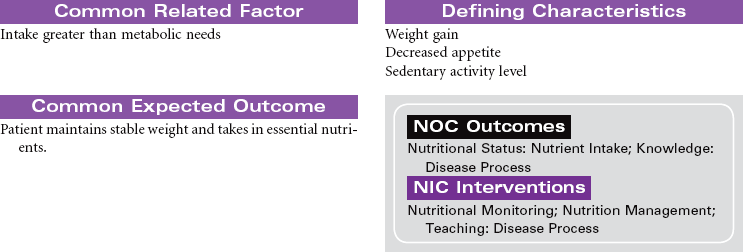
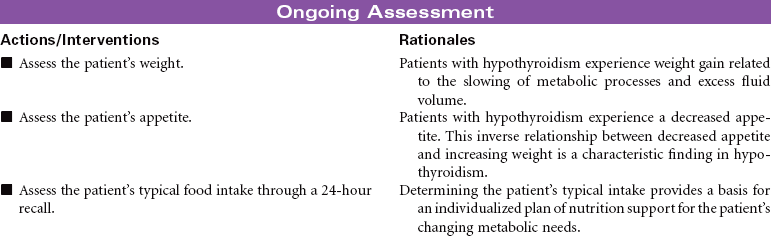
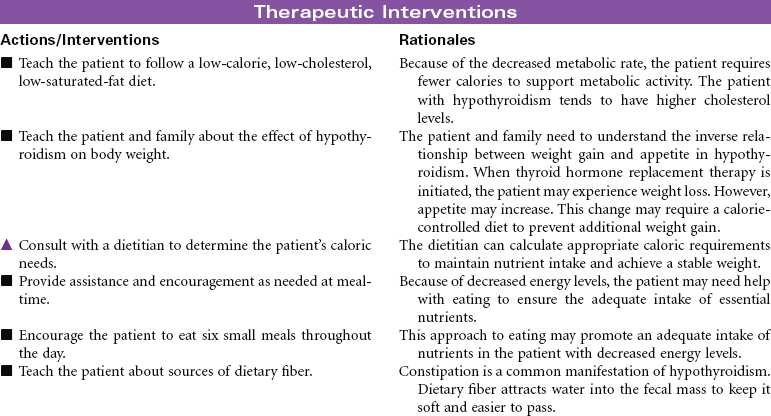
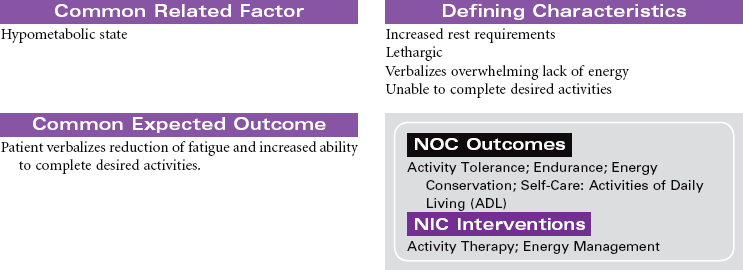
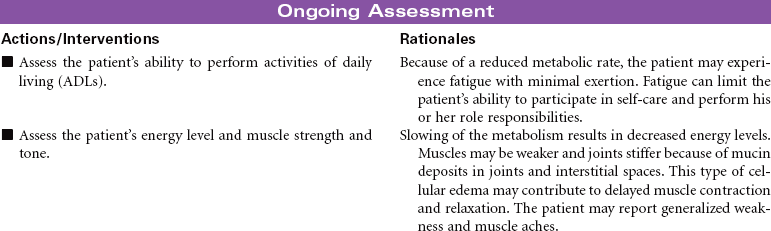
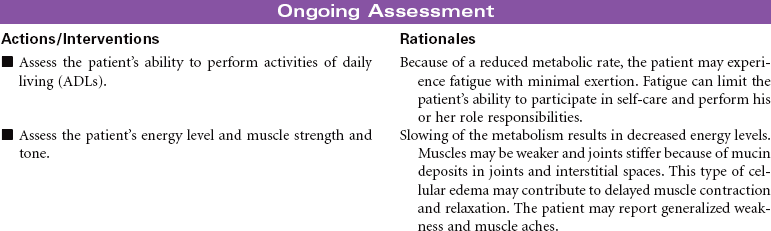
Hypothyroidism occurs because of a deficiency in thyroid hormone. Almost every system in the body is affected through a general slowing of metabolic processes. The disorder is common, especially among women older than 30 years of age. In the older adult, hypothyroidism may be overlooked because many of the manifestations are similar to changes associated with the normal aging process (constipation, intolerance to cold, decreased activity tolerance, weight gain, lethargy, decreased short-term memory, depression). The most common cause of hypothyroidism is an autoimmune inflammation (Hashimoto’s thyroiditis) of the thyroid gland with resulting atrophy of glandular tissue. Hypothyroidism may also develop after a thyroidectomy. Myxedema occurs in hypothyroidism as a result of hyaluronic acid accumulation in tissues. Fluid binds to the hyaluronic acid, producing skin puffiness most noticeable around and below the eyes. Myxedema also causes enlargement of the tongue, which contributes to the impaired speech patterns of the patient with hypothyroidism. When hypothyroidism goes undiagnosed or undertreated, the patient may develop myocardial hypotonic function and ventricular dilation. The patient is at risk for developing decreased cardiac output and systemic tissue and organ hypoxia. This situation is a rare occurrence called myxedema coma and is considered life threatening. Goiter, enlargement of the thyroid gland, may occur when hypothyroidism is the result of decreased hormone synthesis. When hormone production is reduced, thyroid-secreting hormone (TSH) secretion increases owing to lack of negative feedback. The size of the thyroid gland increases as a result of TSH stimulation.

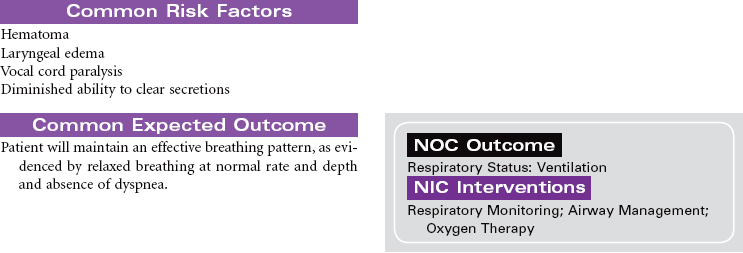
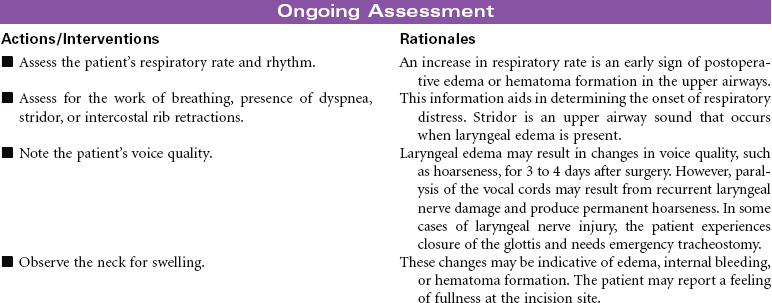
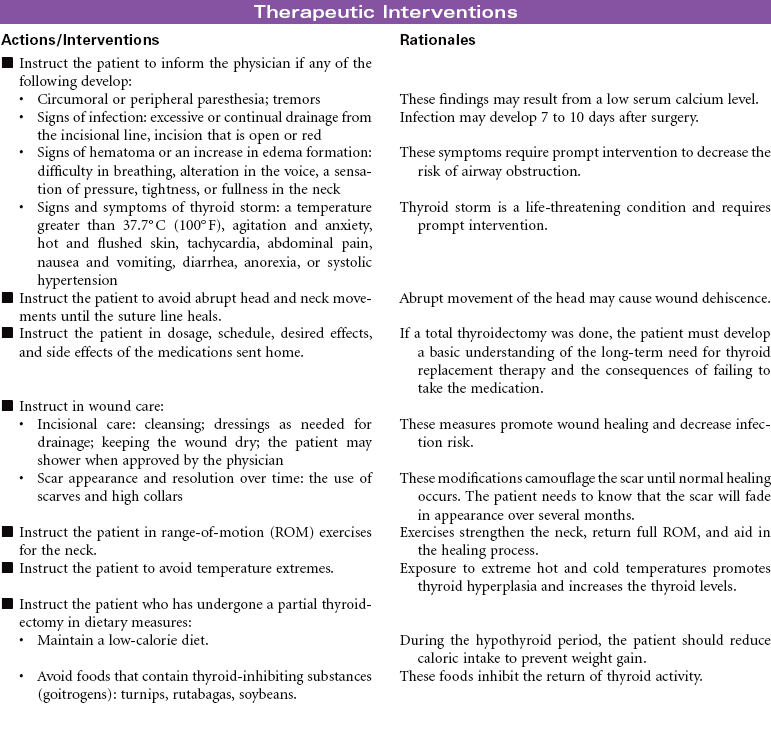
Thyroidectomy
Hyperthyroidism; Thyrotoxicosis; Thyroid Storm
Thyroidectomy is the surgical removal of the thyroid gland performed for benign or malignant tumor, hyperthyroidism, thyrotoxicosis, or thyroiditis in patients with very large goiters, or for patients unable to be treated with radioiodine or thioamides. The surgical procedure may be a total thyroidectomy or subtotal, which is partial removal of the thyroid gland. This care plan focuses on the postoperative management of a patient undergoing a thyroidectomy.


 = Independent
= Independent  = Collaborative
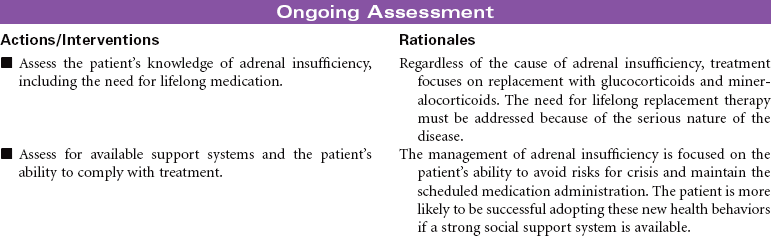
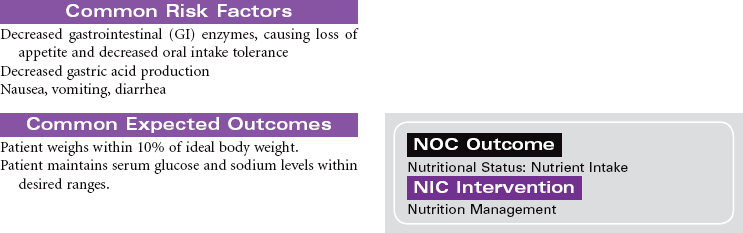
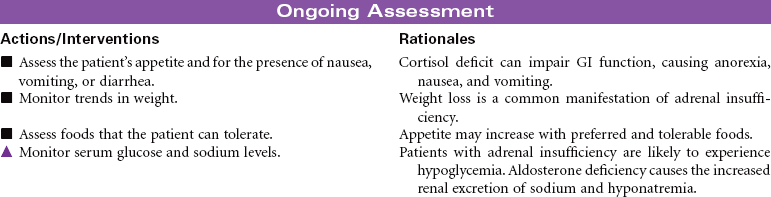
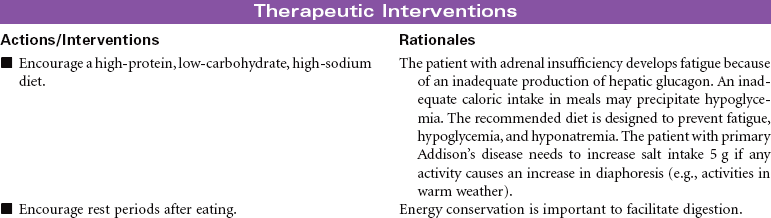
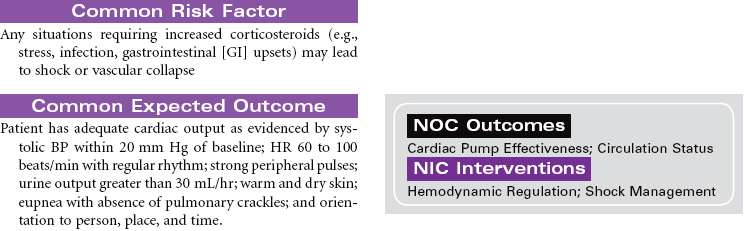
= CollaborativeAdrenal Insufficiency (Addison’s Disease)
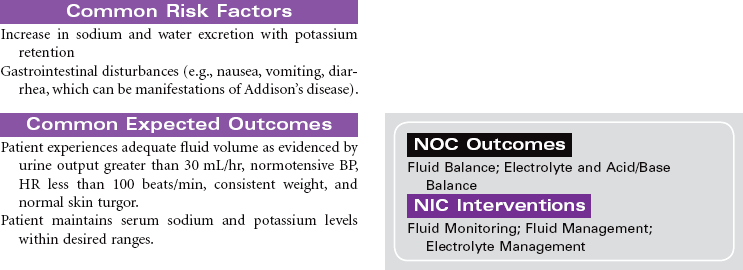
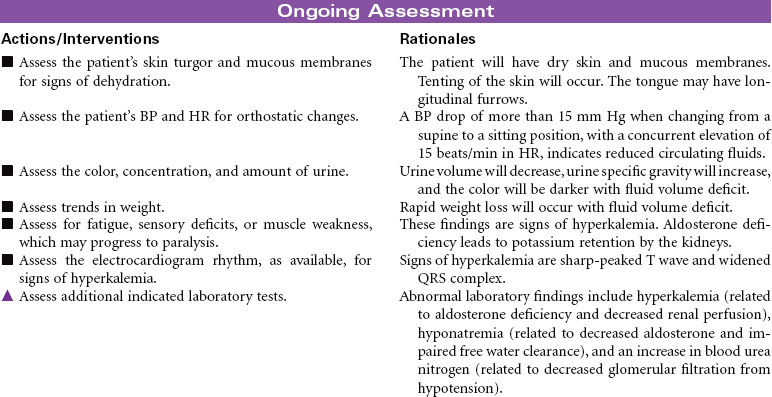
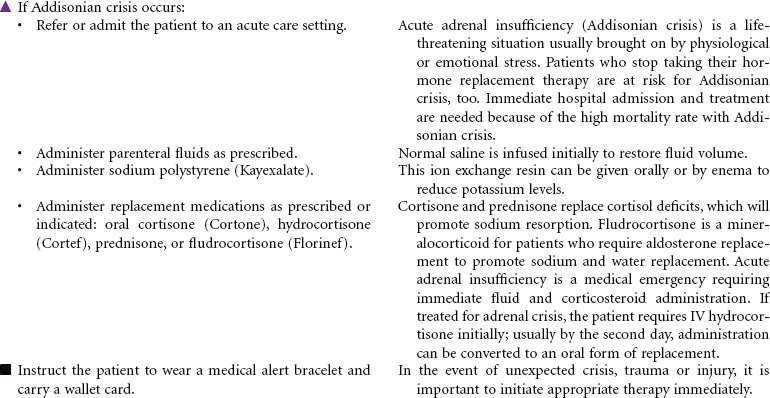
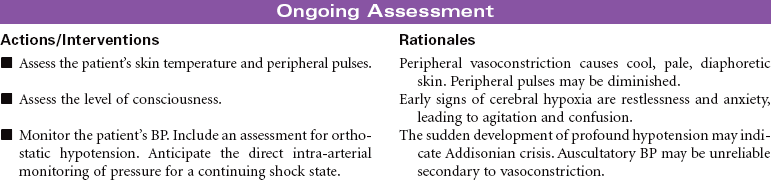
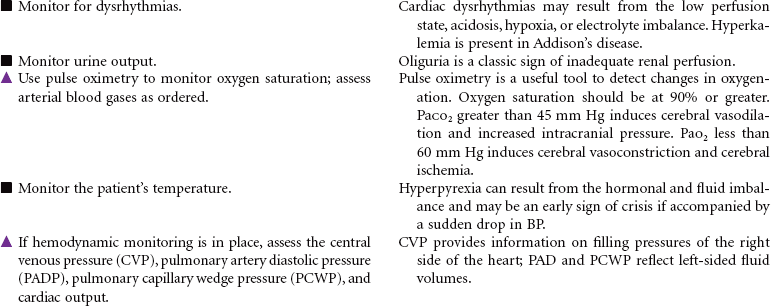
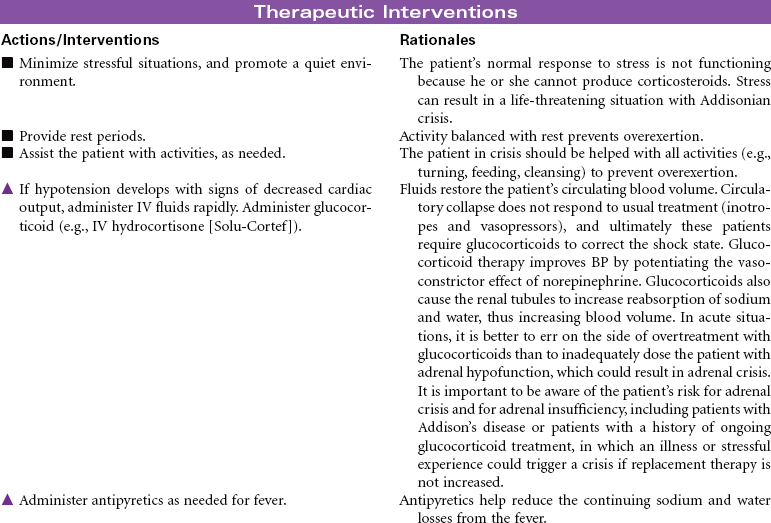
Adrenal insufficiency, or Addison’s disease, is an abnormality of the adrenal glands associated with the destruction of the adrenal cortex and impairment of glucocorticoid and mineralocorticoid production. Causes of this disorder include autoimmune mechanisms, tuberculosis, fungal infection, acquired immunodeficiency syndrome (AIDS), metastatic cancer, hemorrhage, infarction of the adrenal cortex, or surgical removal of the adrenal glands. A secondary form of the disorder may occur from anterior pituitary suppression, causing decreased levels of adrenocorticotrophic hormone, with aldosterone secretion remaining normal. Patients using long-term glucocorticoid therapy may also manifest adrenocortical insufficiency if there is abrupt cessation of the drug. Because of widespread steroid use for multiple diseases, secondary adrenocortical insufficiency occurs more often than the primary form. Addisonian crisis is the most dangerous component of adrenal insufficiency. It is a life-threatening emergency with severe hypotension that may occur during stress, sudden withdrawal of replacement therapy, adrenal surgery, or sudden pituitary gland destruction. This care plan addresses chronic care in an outpatient setting, as well as acute care of Addisonian crisis.


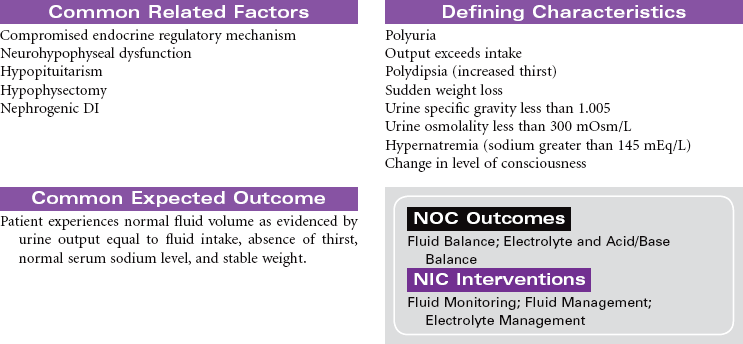
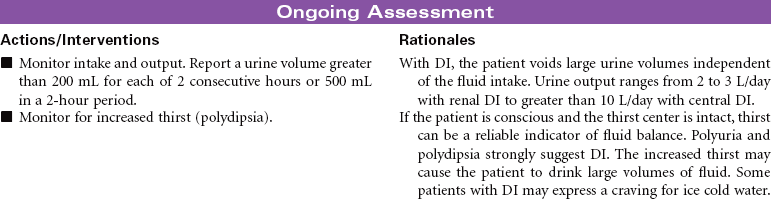
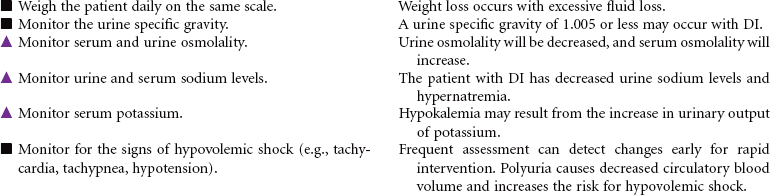
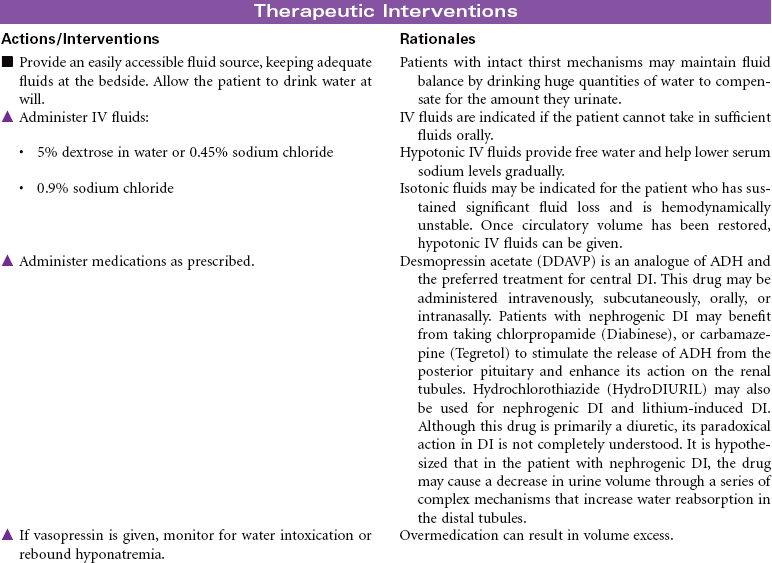
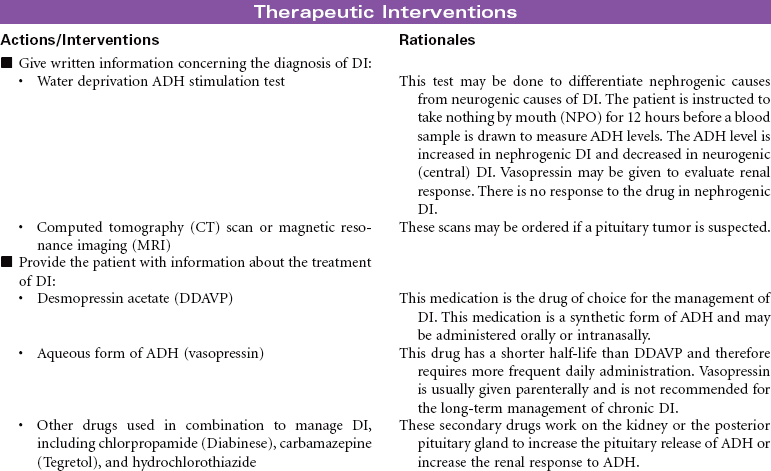
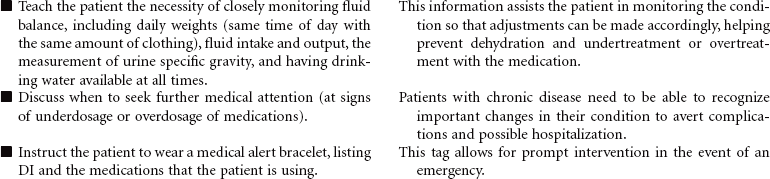
Diabetes Insipidus
Diabetes insipidus (DI) is a disturbance of water metabolism caused by a failure of antidiuretic hormone (ADH) synthesis or release from the posterior pituitary gland. The decrease in ADH secretion leads to excretion of a large amount of dilute urine. DI may have a nephrogenic or neurogenic cause. It may be a permanent disease state or a transient syndrome associated with other illness or trauma. Central (neurogenic) DI is caused by a change that disrupts production or release of ADH. Common causes include head trauma, cerebral edema, and tumors of the hypothalamus or pituitary. Renal (nephrogenic) DI is usually less severe than central DI. Causes include renal failure, some medications, and inherited familial defects in the renal tubules and collecting ducts causing an abnormal response to ADH. Patients taking lithium carbonate are at risk for developing DI. Lithium blocks renal response to ADH. Idiopathic DI has no identifiable cause but develops in people with a genetic predisposition for DI. This care plan focuses on the acute care management of DI and home care teaching instructions.

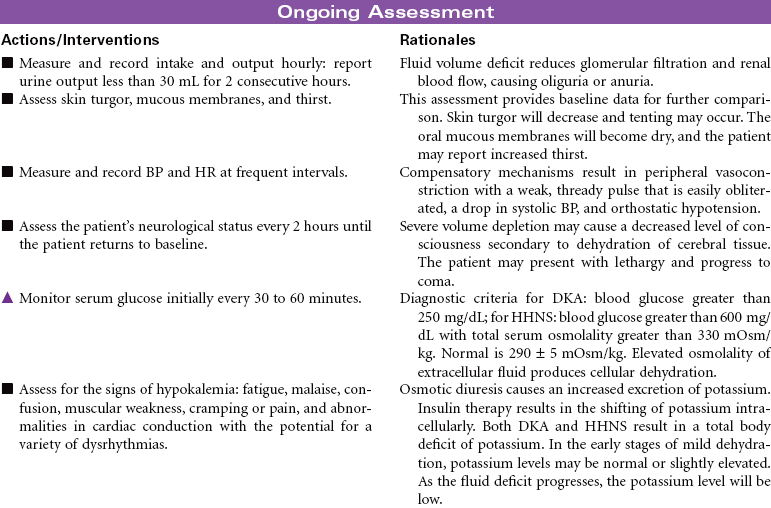
Diabetic Ketoacidosis and Hyperglycemic Hyperosmolar Nonketotic Syndrome
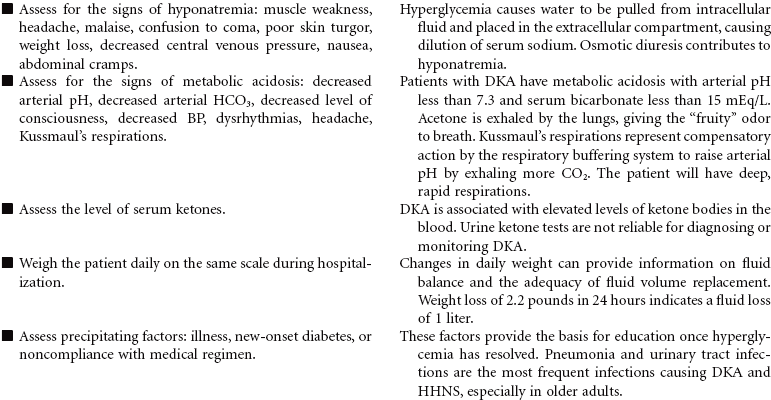
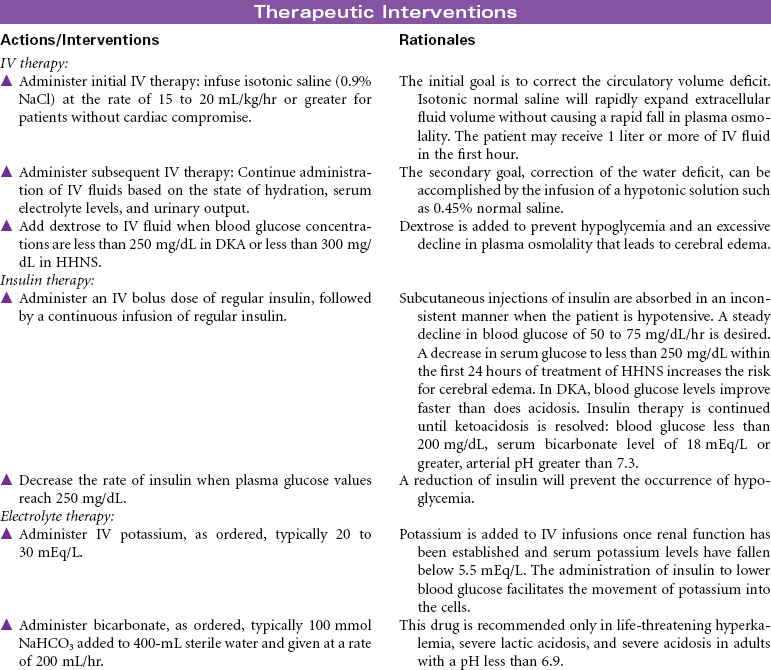
Insulin deficiency causes two conditions of hyperglycemia. Both diabetic ketoacidosis (DKA) and hyperglycemic hyperosmolar nonketotic syndrome (HHNS) are emergency situations and require hospitalization. In DKA, catecholamines, cortisol, and growth hormone are released to meet the cellular demand for glucose. These hormones trigger glycogenolysis and gluconeogenesis from protein catabolism. The insulin deficiency also stimulates breakdown of fats into fatty acids and ketones. The hyperglycemia causes an osmotic diuresis that results in fluid volume deficit. The patient develops hyponatremia, hypocalcemia, hypokalemia, and decreased levels of magnesium and phosphate. In type 1 diabetes, the onset of DKA can be abrupt and frequently occurs as the result of an infection. DKA occurs less often in type 2 diabetes when an acute illness or injury increases the demand for insulin. Careful assessment is required to determine the cause of DKA. Nondiabetic ketoacidosis can occur in alcohol intoxication, severe starvation ketosis, and with the use of drugs such as cocaine.
HHNS is characterized by the presence of severe hyperglycemia, dehydration, and hyperosmolarity. It is usually seen in elderly individuals who develop an infection and are unable to maintain oral intake sufficient to prevent dehydration. They produce enough insulin to minimize ketosis but not to control hyperglycemia. Diagnosis is sometimes made difficult by the limited symptoms that are present in the early stages. The patient may have extremely elevated blood glucose before clinical manifestations are evident. The patient with HHNS may present with neurological symptoms of stroke such as hemiparesis, seizures, and coma. These symptoms are related to cerebral dehydration. The major nursing diagnosis for both conditions involves fluid volume deficits. Specific nursing actions are dictated by the degree of fluid volume deficit and resultant fluid and electrolyte disorders.
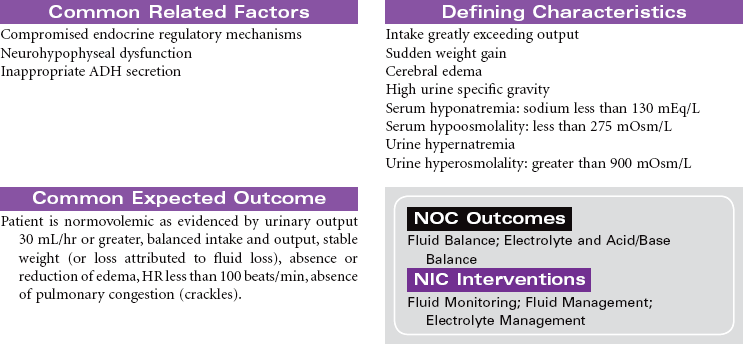
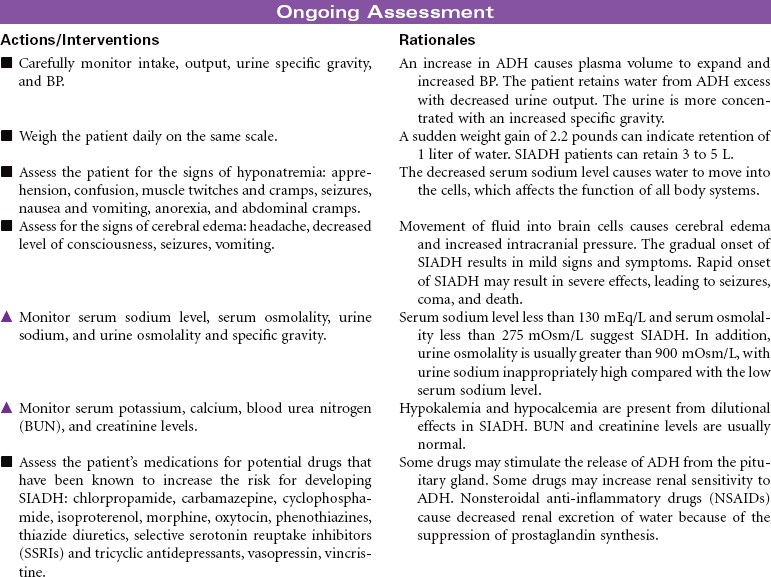
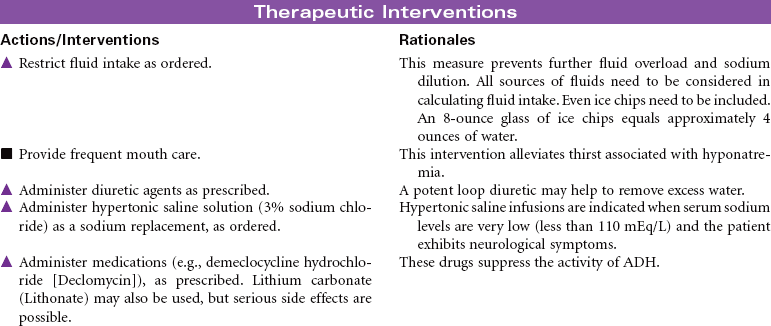
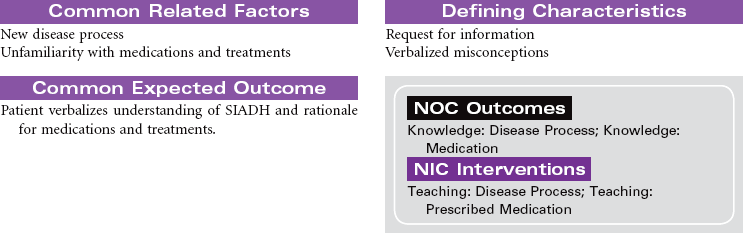
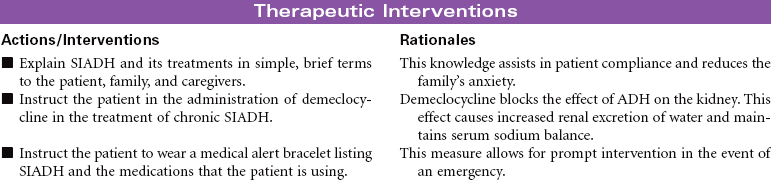
Syndrome of Inappropriate Antidiuretic Hormone (SIADH)
This syndrome develops as a result of the continued synthesis and release of antidiuretic hormone (ADH) unrelated to plasma osmolarity. The excess ADH causes increased permeability in the distal tubule and collecting duct of the nephron. As a result the patient will have water retention and dilutional hyponatremia. The patient will have decreased volume of highly concentrated urine. Potential causes of SIADH include head trauma, brain tumor, and subarachnoid hemorrhage. Systemic cancers (leukemias, lymphomas, pancreatic cancer) and bronchogenic cancer (particularly small cell carcinoma of the lung) are also potential causes. It is thought that normal pulmonary tissue can produce and secrete ADH but does not normally do so unless it is damaged, as in the case of cancer. Other causes of pulmonary-induced ADH production include bacterial and viral pneumonias, tuberculosis, fungal pneumonias, pulmonary contusion, and barotrauma. SIADH is an adverse reaction of many drugs, including thiazide diuretics, selective serotonin reuptake inhibitor antidepressants, and antineoplastic agents. This care plan focuses on the acute and chronic care management of SIADH.