Anesthesia at High Altitude
Overview
In the course of common anesthetic practice, it is unusual to worry about alterations in total environmental pressure, because the majority of anesthetic procedures are conducted normally, within a limited pressure range. In fact, most organized hospital settings have developed in a narrow span of altitudes not far from sea level, although a significant portion of the world’s population continues to live at high altitude. In recent years, traditional surgical and anesthetic techniques have been expanded to countries in development, such as Nepal in Asia, the Andean Highlands of South America, and elevated African regions such as Zimbabwe. Utilization of gas-based anesthesia has increased at altitudes where total barometric pressure is reduced.
It is interesting to explore low barometric pressure at high altitudes with attention to the physiologic changes commonly associated with anesthesia, and the results provide principles and insights applicable to daily practice at “normal” environmental pressure. The first part of the chapter provides a description of the principal physiologic challenges introduced by low pressure; the second part summarizes anesthetic considerations at low barometric pressures.
Gases Around the Body
The pressure exerted by gas molecules on all surfaces of the body constitutes the environmental pressure. This pressure is the result of both the atmospheric gases prevailing at any one site and the composition of the gases in the column of air above the location. Total environmental pressure at sea level amounts to 760 mm Hg (14.7 lb/in2 atmospheric [psia]). This value undergoes frequent, often daily changes; at most, it ranges up and down by 10 to 15 mm Hg as a consequence of weather fluctuations. The composition of atmospheric air, on the other hand, is singularly constant in its original constituents and is summarized in Table 28-1.
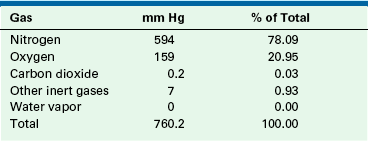
Only water vapor content varies significantly as a function of total humidity, and the partial pressure of the water molecules may contribute various amounts to the total pressure. Water vapor pressure ( ) depends on available water molecules in the atmosphere at a certain temperature. At 0° C, air that is fully saturated has a water vapor pressure of approximately 5 mm Hg, whereas at body temperature (37° C), the water vapor pressure is increased to 47 mm Hg. Whatever humidity and temperature prevail in the gas outside the body, as soon as air is inspired and equilibrated with moist tracheal gas, it is rapidly fully saturated and is heated or cooled to body temperature. Water vapor is added to gases in the airways by the moist linings of the respiratory tract.
) depends on available water molecules in the atmosphere at a certain temperature. At 0° C, air that is fully saturated has a water vapor pressure of approximately 5 mm Hg, whereas at body temperature (37° C), the water vapor pressure is increased to 47 mm Hg. Whatever humidity and temperature prevail in the gas outside the body, as soon as air is inspired and equilibrated with moist tracheal gas, it is rapidly fully saturated and is heated or cooled to body temperature. Water vapor is added to gases in the airways by the moist linings of the respiratory tract.
The addition of water vapor to atmospheric gases and the usual heating of the inspired gas to body temperature both induce substantial changes in the partial pressure of all gases and, in particular, to the partial pressure of oxygen (PaO2) (Table 28-2). Nitrogen and oxygen are the only gases present in substantial concentration in dry air. Moist, warm tracheal air contains significant amounts of water vapor.
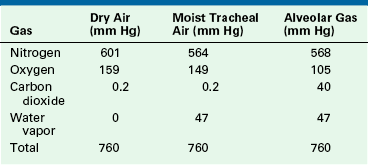
Because the total barometric pressure is unchanged in the trachea, water vapor displaces each of the other gases, thereby decreasing their partial pressures. Alveolar gas contains approximately 100 to 105 mm Hg of oxygen. Commonly, oxygen is taken up by the blood in the lungs, and carbon dioxide is released into the alveoli. During respiratory processes, the gases are primarily moved by convection from the atmosphere to the alveolar space and back to the exhaled gas outside the body. In the alveolar compartment, diffusion is the primary mechanism for oxygen and carbon dioxide exchange. Therefore changes in oxygen partial pressure in the inspired gas lead to proportional changes in the alveolar PaO2.
High-altitude environments are characterized by a decreased barometric pressure and a reduced partial pressure of inspired oxygen compared with sea level values. While breathing air, there is a large range of total atmospheric pressure changes still compatible with adequate gas exchange, from pressures on the highest mountains (about 300 mm Hg total pressure) to those at several hundred feet underwater (about 6 to 7 times 760 mm Hg). The limits can be extended, especially at altitude, by slow adaptive phenomena that require several days to weeks to unfold fully; these phenomena are in part under hereditary control.
Reduced Environmental Pressure
Acute awareness of the adverse effects of the low barometric pressure of high altitude is recorded in literature regarding the Spanish invasion of South America; these effects were commonly attributed to the “thinness of the air.” Acute mountain sickness at an elevation of about 10,000 feet was first described in 1671 by the physiologist Borelli.
Acute exposure to altitude can be achieved in a decompression chamber, by rapid ascent in an airplane, or by a brisk climb on a mountain. The decrease in total barometric pressure with altitude and the attendant reduction in inspired PaO2 are shown in Figure 28-1; Figure 28-2 illustrates the approximate values for PaO2 in inspired air, moist tracheal air, alveolar gas, and arterial and mixed venous blood. High altitude (HA) significantly affects the human body because of a decrease in the PaO2 in an environment of low ambient barometric pressure. A whole spectrum of disturbances and diseases was described for sojourners into HA. On one hand, the lack of oxygen generally triggers physiologic mechanisms and may result in a well-compensated state called acclimatization. The extent to which a person adapts to this depends on the rate and extent of the ascent and the baseline physiologic status of the individual. On the other hand, high-altitude illness (HAI) refers to the set of symptoms that range from mild to severe, sometimes even life-threatening consequences, such as cerebral and pulmonary edema.
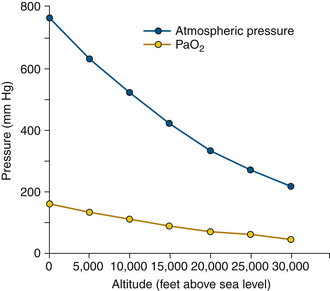
FIGURE 28-1 Effects of altitude on total barometric pressure and partial pressure of oxygen (PaO2). Note that PaO2 is a fixed proportion (20.95%) of total barometric pressure. At sea level, PaO2 is 159 mm Hg; this value is approximately halved at 18,000 feet.
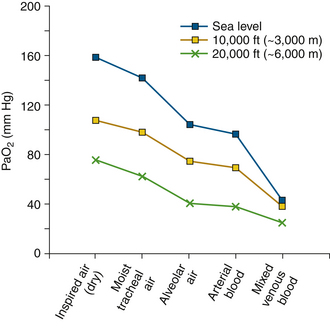
FIGURE 28-2 Effect of altitude on partial pressure of oxygen (PaO2) in the respiratory and blood compartments. Average values are shown at sea level, 10,000 feet, and 20,000 feet. Although changes in the gas phase and in arterial blood are reduced in physical proportion, mixed venous PaO2 changes that occur with altitude are reduced by adaptive responses, mainly an increase in cardiac output. Thus mixed venous blood and tissue values reflect much smaller changes in PaO2 than does arterial blood.
Acclimatization
Acclimatization is a physiologic state that tends to improve oxygen transport and utilization at HA. An essential adaptation to acute HA hypoxia is hyperventilation. In the range of altitude from 10,000 to 15,000 feet, the increase in altitude causes an increase in ventilation proportional to the decrease in density of the air. Thus the increase in ventilation approximates the amount required to produce equivalent delivery of oxygen to the alveolar spaces. This is achieved by an increase in respiratory rate and tidal volume.1 The arterial hypoxia results in stimulation of peripheral chemoreceptors, which causes an increase in alveolar ventilation. Carbon dioxide is washed out of the alveoli at an increased rate, and the arterial partial pressure of carbon dioxide (PaCO2) is decreased. The reduction of PaCO2 leads to a respiratory alkalosis with an associated increase of arterial pH, and these changes stimulate the excretion of bicarbonate from the blood and the kidneys. This increase in ventilation is generally sustained for several days, and it may not reach a plateau until several days at altitude. As a consequence, during the following days, the blood bicarbonate is reduced, and a new level appropriate for the level of hyperventilation is established, with a near normal pH. Thus the respiratory alkalosis is compensated.
The respiratory adaptations and the bicarbonate excretion affect the electrolyte status of spinal fluid and alter subsequent ventilatory responses. As the bicarbonate is excreted from the blood, bicarbonate is also lost from cerebrospinal fluid (CSF). In view of this decreased buffer capacity, changes in carbon dioxide in the CSF result in faster changes in hydrogen ion concentration and lead to an increased sensitivity to carbon dioxide. At this point in adaptation, ventilatory sensitivity to carbon dioxide is enhanced. Gradually, the respiratory system adapts (respiratory acclimatization) to hypoxia, resulting in an increase in the hypoxic ventilatory response. A resetting of the arterial PaCO2 set point also occurs. These processes result in restoration of normoxia with persistent hyperventilation and hypocapnia.2 Overall, the hypocapnia is beneficial for oxygen transport, because it shifts the dissociation curve to the left with increased affinity of hemoglobin (Hb) for oxygen; this enhances the oxygenation of blood at the lung. Extreme altitude results in an arterial PaO2 in the range of 20 mm Hg, a profound depression of the central nervous system (CNS) is unmasked, and ventilatory drive is depressed.
Other Effects
Additional effects on lung function have been demonstrated with exposure to altitude, including an increase in pulmonary diffusing capacity, an increase in pulmonary blood flow to the apical lung regions, larger lung volumes with increased vital and total lung capacity, hypoxic pulmonary vasoconstriction, and an increase in pulmonary vascular pressures. Hypoxic pulmonary vasoconstriction is a vasomotor response of small, muscular pulmonary arteries that tends to increase resistance to flow in areas of alveolar hypoxia, thereby improving ventilation/perfusion (V/Q) match and reducing the shunt fraction. As a result, prolonged arterial hypoxia increases right-ventricular pressure for extended periods of time and induces right ventricular hypertrophy, with predictable electrocardiographic (ECG) changes of right-axis deviation and right ventricular strain.
Hemoglobin concentration increases rapidly at altitude, within hours; this is because of rapidly rising hemoconcentration. Eventually, however, a real increase in erythropoiesis and a true increase in red cell mass ensues that may not be fully realized for several weeks. As the red cell mass and hemoglobin concentration rise, the erythropoietin level decreases. Because of the sigmoid shape of the oxygen dissociation curve, up to 3000 m (9843 feet) of elevation, oxygen saturation is maintained; beyond 3000 m (9843 feet), the arterial PaO2 falls steeply, resulting in lower oxygen saturation. Soon after the development of the hypoxic state, production of 2,3 diphosphoglycerate (2,3-DPG) increases, which shifts the hemoglobin dissociation curve to the right and allows for more effective extraction in the capillaries.
Cardiac output is characteristically increased as a result of an increase in the heart rate in response to hypoxia. This response adapts during continuing exposure as cardiac output decreases as a result of diuresis and a lower plasma volume. Tissue blood flow tends to increase as a result of increased nitric oxide (NO) concentration in the plasma, which causes vasodilation.3 A corresponding increase in organ blood flow occurs that includes pulmonary, cardiac, and cerebral blood flow. Increased pulmonary blood flow leads to failure of red blood corpuscles to fully equilibrate with the alveolar gas, which augments any existing hypoxia. HA may induce a hypercoagulable state as a result of polycythemia and platelet activation, which increases the risk of thromboembolic events.4
In acclimatization, a state of improved oxygen transport and utilization combats the HA hypoxia; molecular responses involved include activation of gene coding for proteins involved in oxygen transport (hypoxia inducible factor 1 [HIF-1])5 and growth of blood vessels (vascular endothelial growth factor [VEGFA])6 in the heart.
Despite these adaptive responses to altitude, no significant change occurs in either resting oxygen consumption or in the ability to perform high levels of exercise at moderate altitude. At altitudes in excess of 10,000 feet, exercise tolerance is limited with acute exposure, and other symptoms of acute hypoxia manifest themselves by interference with several organ systems.
High-Altitude Illness
HAI is composed of a group of syndromes that develop as a result of continuous exposure to hypoxia, and it is generally divided into four categories: 1) acute mountain sickness, 2) high-altitude cerebral edema, 3) high-altitude pulmonary edema, and 4) chronic mountain sickness. The risk of HAI is directly proportional to the rate of ascent and the altitude reached; therefore a gradual ascent to promote acclimatization may be the best strategy to prevent HAI. Guidelines suggest that above an altitude of 2500 m (8200 feet), the altitude at which a person sleeps should not be increased by more than 600 meters (1970 feet) per day7 (Table 28-3).4,8
TABLE 28-3
High-Altitude Illness and Various Clinical Syndromes
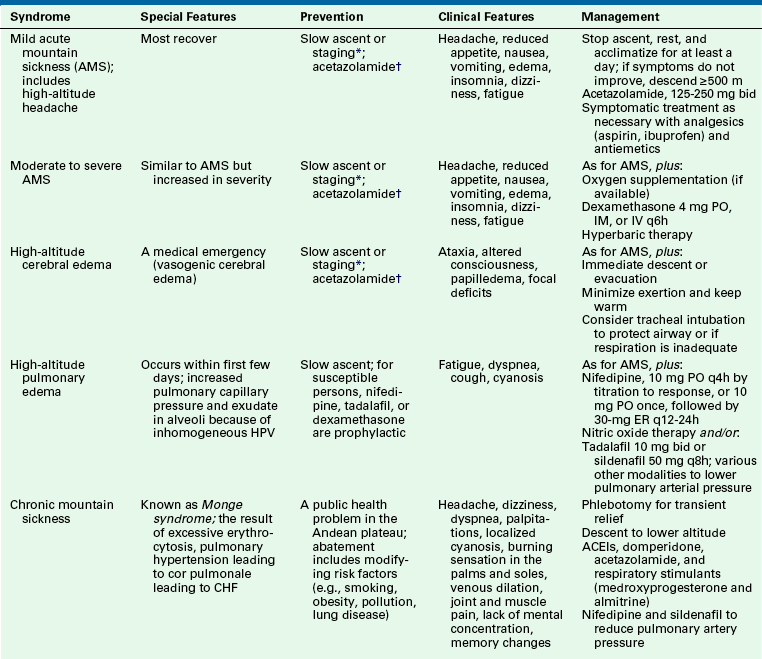
ACEI, angiotensin-converting enzyme inhibitor; bid, twice per day; CHF, congestive heart failure; ER, extended-release; HPV, hypoxic pulmonary vasoconstriction; IM, intramuscular; IV, intravenous; PO, by mouth.
∗Several days are spent at an intermediate altitude of 200 m.
†Produces a state of bicarbonate diuresis and thereby augments the ventilatory response to hypoxia; may also produce tissue respiratory acidosis and diuresis and inhibits carotid body response to carbon dioxide.
Modified from Leissner KB, Mahmood FU: Physiology and pathophysiology at high altitude: considerations for the anesthesiologist, J Anesth 23:543-553, 2009; and Moon RE, Camporesi EM: Clinical care in extreme environments: at high and low pressure and in space. In Miller R, Eriksson L, Fleisher LA, Wiener-Kronish J, editors: Miller’s anesthesia, ed 7, Philadelphia, 2010, Elsevier.
Gamow Bag
The Gamow bag is a rescue product for high-altitude climbers and trekkers that can be used for the treatment of moderate to extreme altitude sickness.9 A Gamow bag is an inflatable pressure bag large enough to fit a person inside. By inflating the bag with a foot pump, the effective altitude can be decreased by as much as 7000 feet, thus relieving the symptoms of acute mountain sickness (AMS). The Gamow bag is also used for treatment of life-threatening high-altitude pulmonary edema (HAPE) and high-altitude cerebral edema (HACE). Gamow bags are constructed of durable nylon and are reinforced with circular nylon straps. A lengthwise zipper allows patients access into the bag, and the four clear windows allow visual contact during treatment. The bag is pressurized with ambient air to 2 psi by use of a foot pump powered by healthy partners standing outside the bag (Fig. 28-3).

Gamow bag treatments for altitude sicknesses are used to provide temporary relief in the hope that it will give the patient enough time and strength to descend to a lower altitude, alleviating the need for a full-blown lifesaving rescue effort by everyone on the mountain. Descent to a lower altitude is generally recommended in most cases.
Pregnancy and Altitude
Because the fetus in utero does not derive oxygen directly from the low barometric pressure at HA, it seems to be little affected by acute exposure to altitudes up to 2500 to 3000 m and suffers no adverse effects. Adaptation to chronic exposure to HA includes a decrease in villous membrane thickness and an increase in placental capillary volume. Infants born at HA are suddenly exposed to the hypoxic environment, whereas the transition to adult circulation occurs more gradually,10 with a higher incidence of patent foramen ovale (PFO) and patent ductus arteriosus. Increased incidence of acute respiratory distress syndrome (ARDS) and pulmonary arterial hypertension that requires oxygen and/or mechanical ventilation is also seen.
Anesthetic Problems and Altitude
Two main problems can be identified in the administration of anesthetics at altitude: the relative hypoxic background of air at lower ambient pressure, especially before and after anesthetic administration, and the prevailing technical problems associated with delivery of anesthetic vapors from vaporizers when the total ambient pressure is reduced. Significant alterations in the effectiveness of intravenous (IV) agents and of regional anesthetic techniques have not been reported, and these agents and techniques may still be used with the some precautions as at sea level.
Pressure Considerations
The effective anesthetic power of nitrous oxide is also reduced as total barometric pressure decreases. It has been shown that analgesia induced by 50% N2O is reduced by nearly 50% at 5000 feet, and it becomes insignificant at 10,000 feet.11,12 Therefore nitrous oxide is not a useful anesthetic gas at altitude. In fact, Safar and Tenicela13 and James and White14 condemned the use of nitrous oxide for anesthesia at altitude.
Although total IV anesthesia (TIVA) seems to be safer than inhalational anesthetics, at HA all anesthetics and opiates still potentially depress the respiratory drive. In addition, the regular dose of these drugs may show increased respiratory depression in unacclimatized individuals. Thus the anesthetic technique least likely to suppress ventilation should be applied, especially in the field, where monitoring facilities and supplemental O2 may not be readily available.
Regional anesthesia seems to be a safe option when applicable, but regional anesthesia can compromise respiratory function when it affects the phrenic nerve. Because of this, caution must be exercised during the performance of brachial plexus and stellate ganglion block. Increased incidence of postdural puncture headache with subarachnoid block has been reported, possibly owing to hypovolemia, along with increased and altered sensitivity to CSF pressure; otherwise, effects are similar to those seen when such procedures are performed at sea level.
At an altitude approximating 5000 feet, the partial pressure of oxygen in air is reduced from the sea-level value of approximately 160 mm Hg to about 125 mm Hg. While room air is breathed at altitude, arterial PaO2 is consequently lowered to approximately 80 mm Hg in normal individuals. Powell and Gingrich11 recommended administering a gas mixture that contains no less than 40% oxygen during anesthesia at an altitude of 1 mile (approximately 5000 feet) to compensate for the reduced arterial PaO2 commonly observed during anesthesia. When this altitude is doubled to about 10,000 feet, the inspired PaO2 is reduced to 110 mm Hg, and PaO2 is reduced to 65 mm Hg in air. At this hypoxic level, alveolar ventilation increases, and PaCO2 is steadily reduced (34 mm Hg at rest).
It is important to remember that long-term adapted residents are more tolerant to hypoxemia and have increased hematocrit, pulmonary hypertension, and low PaCO2 and biocarbonate (HCO3) concentrations. These values are the baseline and should be maintained throughout the procedure.
Machine Considerations
Vapors and Vaporizers at Altitude
The saturated vapor pressure (SVP) of a volatile anesthetic agent depends only on temperature15 and is practically independent of total environmental pressure. Consequently, for a given vaporizer temperature, the concentration of a given mass of vapor increases as the barometric pressure is reduced, because the same mass of volatile agent is vaporized in a less and less dense carrier gas. However, the partial pressure of the agent (expressed in millimeters of mercury) remains unchanged, and so does its biologic effect on the neural tissue where the anesthetic effect is produced (see also Chapter 3).
With modern vaporizers, the partial pressure of the vapor should remain unaltered by barometric pressure changes. In fact, McDowall16 showed that the output of the FluoTec Mark 2 (Cyprane, Keighley, United Kingdom) vaporizer differed by only a small amount from the theoretical prediction, and those changes could be attributed to the slight change in the density of the carrier gas. However, Safar and Tenicela13 studied the Foregger vaporizer (Foregger Company, Roslyn Heights, NY) at 10,000 feet and showed, contrary to the theory, that a higher partial pressure of gas was produced at increased altitude. Twenty years later, James and White14 studied this with a more precise analytical technique, using the Engström EMMA vapor analyzer, whose principle of operation is a vibrating lipophilic-coated piezoelectric crystal. They studied the accuracies of a FluoTec Mark 2 vaporizer and a Dräger Vapor halothane vaporizer (Dräger Medical, Telford, PA) inside a pressure chamber simulating altitude but were unable to show differences in halothane partial pressure with decreased environmental pressure. These authors concluded that, because the reading of the vapor analyzer remained constant, the last two types of vaporizers produced a relatively constant partial pressure of halothane even at reduced environmental pressure (see also Chapter 3).
Concentration-calibrated variable bypass vaporizers—such as the Datex-Ohmeda Tec series (Tec 4, 5, and 7; GE Healthcare, Waukesha, WI) and the Dräger Vapor 19.n and 2000 series—set to deliver a given concentration in volumes percent at 1 atm pressure at an altitude where ambient pressure is less than 1 atm (<760 mm Hg) will deliver a higher concentration in volumes percent than that set on the dial. However, when that concentration (vol%) is converted to agent partial pressure, which determines effect or potency, the increase is proportionately smaller than the increase in volumes percent. For example, when gas flows from the anesthesia machine’s flowmeters into a variable-bypass vaporizer set to deliver 1% isoflurane at 20° C and 760 mm Hg ambient pressure, that gas flow is split in the ratio of 46:1 for bypass–to–vaporizing chamber flow (see Chapter 3 for derivation of split ratios). It will be assumed that the split ratio remains unchanged with changes in altitude. The SVP of isoflurane at 20° C is 240 mm Hg, and atmospheric pressure is 760 mm Hg; therefore the concentration of isoflurane that emerges from the vaporizing chamber is 32% (240/760). When atmospheric pressure is 500 mm Hg (~⅔ atm), the concentration of isoflurane that emerges from the vaporizing chamber would be 48% (240/500). Because the bypass flow remains constant (same split ratio), the concentration of isoflurane that emerges from the vaporizer would be approximately 2% by volume, almost double the dial setting. However, consider the partial pressures of isoflurane, because it is this value in the CNS that determines anesthetic depth or potency. At 1 atm, 1% partial pressure of isoflurane is 1% × 760, or 7.6 mm Hg. At ⅔ atm, the partial pressure of isoflurane would be 2% of 500, or 10 mm Hg—1.3 times that at 1 atm. This effect on agent concentration occurs because isoflurane vapor is added after the vaporizer’s incoming gas flow has been split.
The Tec 6 and Dräger D-Vapor vaporizers are different from the traditional variable-bypass vaporizers described above in that these vaporizers always deliver the dialed-in concentration in volumes percent regardless of ambient pressure. At altitude, therefore, the percent desflurane (Pdes) delivered will be less. Thus 10% desflurane at 1 atm represents a Pdes of 10% × 760, or 76 mm Hg. At ⅔ atm, 10% desflurane has a Pdes of 10% of 500, or 50 mm Hg. Thus to obtain the same Pdes (potency) as at 1 atm, the vaporizer dial setting must be increased to 15% because 15% × 500 is 75 mm Hg.
Gas Analyzers
Most of the gas analyzers used by anesthesiologists are based on one of the various physical properties of the agent being measured. Most analyzers respond to the number and activity of molecules of the agent present, independently of the presence of additional gas molecules. Such instruments, therefore, measure partial pressure, not concentration of agents. Most often, however, such devices are traditionally calibrated in percentages. This calibration scale might introduce important errors that must be prevented when specialized equipment will be used at increasing altitudes (see Chapter 8).
Oxygen Analyzers
All oxygen analyzers in current use—paramagnetic, fuel cell, and oxygen electrode devices—respond to partial pressure of oxygen alone and produce alterations of the total measurement output as barometric pressure changes. An oxygen analyzer calibrated at sea level to measure 21% oxygen in air gives a reading of 17.4% oxygen when reading air at 5000 feet. Of course, the analyzer must be recalibrated at altitude to read 21% when air is injected. If the oxygen activity were to be presented as partial pressure (e.g., mm Hg of oxygen), the device would indeed reflect oxygen availability to the patient’s lungs and blood at any pressure. As noted above, the key issue is that air at an altitude above 5000 feet is relatively hypoxic, and it approaches a clinically significant hypoxic level at 10,000 feet. The same principle applies in hyperbaric conditions: compressed air at 5 atm contains 21% oxygen, but total oxygen exerts a partial pressure of approximately 800 mm Hg (21% × 5 × 760, or 798 mm Hg).
Carbon Dioxide Analyzers
Carbon dioxide analyzers most frequently operate on the principle of infrared absorption. As indicated above, most analyzers have scales that read in percentages, although the sensitive element is responding to the increasing partial pressure of carbon dioxide. By the use of precise gas mixtures, it is possible to calibrate these analyzers to read exact percentages at a fixed altitude. If, however, the analyzer is calibrated at sea level, and the same gas containing a fixed percentage of carbon dioxide is injected into the analyzer at a different altitude, the reading of the analyzer decreases in the percentage scale in proportion to the total barometric pressure.
Gas Density and Flow
Alteration of total barometric pressure induces a proportional change in gas density. In fact, density reflects closely the number of molecules per unit volume. Gas flowmeters and variable-flow resistors used to produce oxygen-enriched mixtures represent critical devices that use indicators that depend on gas density. Some ventilators deliver tidal volumes that are lower than set volumes during volume-control ventilation because of decreased gas density and viscosity at HA.
Flowmeters
The action of most flowmeters is due to the decrease in pressure that occurs when a gas passes through a fixed resistance, an indication of total gas flow. If this fixed resistance is represented by an orifice, resistance depends primarily on gas density. However, if the fixed resistance is of a laminar nature, viscosity becomes the prime determinant of the magnitude of the pressure reduction provided by the flow. Most flowmeters currently in use utilize a floating bobbin supported by a stream of gas inside a tube with a tapered diameter.
The density of a gas changes in proportion to the change in total barometric pressure, but viscosity changes relatively little, or not at all, because viscosity depends mostly on temperature. In a tapered tube at low levels of flow, the movement of the bobbin primarily depends on laminar flow. As the float moves up the tube, the resistance makes it behave progressively more like an orifice. In practice, only minor errors, usually 1% per every 1000 feet of altitude, have been reported for most gas flowmeters, such that minor corrections to the total flow can be easily applied.17 However, if total environmental pressure changes by more than 1 atm, Halsey and White18 recommended a complete recalibration, because a single correction factor will be significantly in error. The following equation can be used to derive an approximate correction factor, both at altitude and at increased pressure:

In this expression, F1 is flow at the present ambient pressure, F0 indicates flow on the scale calibrated at sea level, d0 is density of gas at sea level, and d1 is density of gas at the present pressure. The correction factor may be significant at increased pressure but seldom exceeds 10% at altitudes up to 5000 feet.
James and White14 tested oxygen and nitrous oxide flow indicators (despite the warning not to use N2O at altitude) and measured the percentage error at flowmeter settings that ranged from 1 to 8 L/min. They demonstrated that errors were larger at higher flow settings and ranged from 3% to 8% at 5000 feet but from 5% to 20% at 10,000 feet. This is an issue when oxygen and nitrous oxide are used together at high flows, because flowmeters tend to underread the actual flow rate. The result is a hypoxic mixture that results from the mix of a flow of oxygen with a higher flow of nitrous oxide.14 An oxygen analyzer calibrated at HA can be used to monitor the final output.
High-Flow Oxygen Enrichment and Other Devices
Fixed-orifice Venturi devices are commonly used to provide an enriched gas mixture with elevated oxygen content. Fixed settings—usually 28%, 35%, or 40%—are produced by variable orifices, which produce different amounts of entrainment of air into an oxygen stream. Most of these devices “run rich” at altitude, because the total gas density decreases.14 Therefore the Venturi-type mask might be used safely at altitude, provided the flowmeter used to quantitate total oxygen flow is properly calibrated for the altitude at which it is being used.
During the rewarming phase of cardiopulmonary bypass, the low barometric pressure becomes a critical factor for adequate oxygenation. The reduction in the ambient PaO2 has a significant deleterious effect on the performance of the oxygenator used, although this can be overcome by having a low priming volume, low pressure drop, and sufficient gas transfer to provide safe oxygenation at HA in the oxygenator.
According to Boyle’s law, pressure is inversely proportional to volume, and as a result of a decrease in pressure at HA, up to a 30% increase in volume of air is seen in the tracheal tube cuff and within a laryngeal mask airway (LMA). During rapid ascent to altitudes commonly experienced during aeromedical transport, this may cause ischemic injury to the tracheal or pharyngeal mucosa. Removal of air from the cuff or filling the cuff with water may be indicated.
Recommendations for Anesthesia at Altitude
It is important to use anesthetics, analgesics, and tranquilizers judiciously, because they have the potential to decrease the ventilatory drive. They should be carefully titrated to effect. Ketamine seems to be a good anesthetic option, because it produces a dissociative state of anesthesia with minimal respiratory depression and does not interfere with the pharyngeal or laryngeal reflexes. Although oxygen desaturation and central apnea have been reported, supplemental oxgyen and respiratory monitoring can be implemented. There is a theoretical risk of worsening pulmonary vascular resistance; however, propofol, the most popular induction agent, seems to be safe, although there is a need for a higher dose than usual.19
The major risk of anesthesia at HA is that anesthetized patients can become hypoxic despite the fact that adequate oxygen concentrations are being administered. The effectiveness of nitrous oxide is so reduced by the decrease in partial pressure at altitude that no significant contribution by nitrous oxide to the anesthetic mixture is of clinical use. In addition, it is important to maintain a higher concentration of oxygen both during and after administration of the anesthetic to support adequate oxygenation. It is suggested that 30% oxygen be the minimum at 5000 feet, and that 40% oxygen be the minimum at 10,000 feet, for both intraoperative anesthetic management and postoperative recovery.
The problem may be compounded by inaccuracies in flow measurement, because the only way to obtain accurate flow rates at fixed altitude is to use flowmeters appropriately calibrated at altitude. Sea level–calibrated equipment may produce small errors at 5000 feet, but it certainly will deviate significantly, up to 20% at 10,000 feet. Finally, it is important to think of oxygenation and anesthetic vapor activity in terms of partial pressures of oxygen and partial pressures of anesthetic agent, rather than as volumetric percentages.
Gastric emptying is significantly delayed at HA and increases the risk for aspiration. Rapid-sequence induction and full-stomach precautions should be considered. Temperature homeostasis should be maintained at HA, because hypothermia-related causes of coagulopathy and hypothermia-induced vasoconstriction can mask hypovolemia. In addition, hypovolemia may be present because of insufficient water intake, a dry environment, increased surgical blood loss as a result of capillary ooze attributed to higher venous pressure, vasodilation and dense capillaries, increased set point of the plasma osmolality/plasma vasopressin relationship, and decreased aldosterone secretion mediated through the release of atrial natriuretic factor (ANF).
IV lines should be completely cleared of air bubbles, because right-to-left shunts develop frequently through a PFO in the setting of pulmonary vasoconstriction. Antithrombotic prophylaxis should be strongly considered for postsurgical patients because of the risks of hypercoagulability produced as a result of acclimatization to HA. Substrate metabolism at HA favors carbohydrate oxidation, thus the body depends more on blood glucose levels, because carbohydrate oxidation generates more adenosine triphosphate (ATP) per molecule of oxygen than fat utilization.4 Glucose levels should be checked, because HA may increase glucose consumption.
The ambient temperature of the operating room must be raised, and it should be warm upon arrival of the patient. IV fluids should be warmed, warm-water baths should be prepared for areas of frostbite, and warming blankets should be applied. Humidification of inspired gases reduces evaporative heat loss and helps to warm the patient. Furthermore, heated peritoneal, bladder, or colonic lavage and extracorporeal circulatory rewarming may be used. Patients need to be monitored carefully during rewarming because of potential cardiac arrhythmia as a result of cold blood returning to the heart and peripheral vasodilation leading to hypotension and shock.
Common Medical Problems and Commercial Flights
The number of people traveling by air has increased to reach close to 2 billion annually in recent years20 with a corresponding increase in the frequency of in-flight emergencies. The exact figures are not known, but the reported incidences of in-flight emergencies vary from 1 to 75 reported events per 1 million passengers21 to 1 per 39,600 passengers.22 Common in-flight emergencies include syncope, trauma as a result of turbulence and objects falling from the overhead bin, nausea, vomiting, hyperventilation, and dizziness.
Most events are minor, but a few—myocardial infarction, respiratory failure secondary to exacerbation of reactive airway disease, and pulmonary embolism—can be life threatening. From 0.01 to 0.8 deaths per million passengers have been reported,8 but the actual figure may be even more staggering, because there is no mandatory reporting of all the emergencies and their outcomes. Contributory factors may be that older and sicker people are traveling in increased numbers. Many sick passengers are certified by physicians for air travel per the comprehensive medical guidelines set by the Aerospace Medical Association.23 The right of a person to fly cannot be denied unless that person is deemed a hazard to the safety of other passengers, and it is more common than before to see people who have obstructive and restrictive lung diseases with supplemental oxygen and passengers with obstructive sleep apnea on noninvasive ventilator support on board an aircraft.24 For passengers at risk of hypoxemia who intend to use pulse oximetry during the flight, recommendations are that they have a prior medical evaluation and a plan of management.25
In-Flight Environment and Its Clinical Implications
The scope of an anesthesiologist has expanded from the operating room to various other locations, and anesthesiologists have established themselves as perioperative physicians and trauma specialists. With the knowledge of physiology combined with the skill of airway management and routine handling of emergencies, an anesthesiologist is in a unique position to handle an emergency in the vicinity, and one such vicinity is inside an aircraft. Therefore the anesthesiologist must be aware of the challenges that can arise here, in case there is an emergency.
Most flights ascend to an altitude between 7300 and 13,000 meters, and the internal environment is regulated to keep the barometric pressure consistent with an altitude of 2400 m (8000 feet) and the temperature equivalent to that of sea level, which is well tolerated by most individuals. At 2400 m, the barometric pressure is 565 mm Hg, and there is some amount of hypoxia—partial pressure of alveolar oxygen (PAO2) is 118 mm Hg, PaO2 is 60 mm Hg, and the arterial oxygen saturation (SaO2) is 89%.
Patients with baseline hypoxemia as a result of lung or heart diseases may experience significant hypoxemia. The arterial PaO2 falls onto the steep portion of the hemoglobin dissociation curve, toward the left, and such patients should be considered for in-flight O2 administration.
The air in the cabin of an aircraft has decreased relative humidity (<10%). This dry air can exacerbate reactive airway diseases such as asthma and can also augment dehydration secondary to insensible water loss. As cabin pressure decreases, gas contained within closed spaces expands during flight. Because of this air expansion in the middle ear and sinus spaces, symptoms such as transient decrease in hearing acuity or minor ear and sinus pain are experienced by a few people. Spontaneous rupture of bronchogenic cysts, pulmonary bullae,26 and wound dehiscence have been reported. Medical devices that contain air spaces, such as tracheal tube cuffs and feeding tubes, will expand as cabin pressure decreases.
Spreading of communicable diseases, especially upper respiratory tract infections, is common during commercial flight. This is mainly due to the number of people in close proximity within a confined environment, because the air inside the cabin is relatively free of contaminants.27 During long-distance flights, deep venous thrombosis (DVT) is a potential risk because of venous stasis secondary to immobility and hyperviscosity secondary to dehydration. But its relation to air travel is doubtful, because its incidence is not greater in air travelers than in the general population.28 Yet it seems prudent to advise susceptible passengers to walk around during long flights, exercise the calf muscles while seated, prevent dehydration, and consider the use of compressive stockings. Early signs of a dislodged thrombus into the pulmonary circulation may be breathlessness, and a person must have a high index of suspicion for this, especially if is associated with acute pleuritic chest pain in a susceptible individual. It is interesting to note that the incidence of children becoming ill is much less when compared with adults.29
In-Flight Emergency Management
Flight crews are well trained in handling in-flight emergencies. Indeed, the safety of all passengers on board the flight is the responsibility of the flight crew. The routine management of an ill passenger during flight consists of obtaining the patient’s history, assessing his or her status, and making provisions for the patient’s comfort. Meanwhile, immediate availability to the patient of oxygen and medical equipment on board should be ensured, and flight personnel should delegate responsibility, request medical assistance when appropriate, and suggest diversion of the flight if it will be of benefit to the patient.
Aircraft are required to carry emergency medical kits, basic first aid kits, automated external defibrillators (AEDs), and supplemental oxygen as per the Federal Aviation Administration (FAA) minimum standards. To provide a PaO2 equivalent to sea level at an altitude of 2400 meters (8000 feet), the FiO2 should be 28%, which is achieved by a flow rate of 2 L/min. It must be remembered that the emergency equipment on board is limited in scope and variable in nature to manage the emergencies encountered.
If a physician must volunteer during an in-flight emergency, proof of identity must be provided, and treatment must be administered in concordance with ground medical personnel in liaison with the cabin crew members. The goal of in-flight medical assistance is to stabilize the patient and advise the flight crew as to a diagnosis and necessary treatment. In addition, when appropriate, the volunteer should seek consultation from ground-based medical support personnel and suggest diversion of the aircraft.24 It is very important that the volunteer physician clearly document the event and patient history for the continuum of care. The crew must cater to the needs of other passengers in addition to caring for the sick; they must also comply with the regulations governing aviation and with the laws of the aircraft’s country of registration, and they must act in accordance with physicians on the ground. The law does protect a physician acting as a Good Samaritan when there is no monetary benefit involved, but the quality of care should not have been compromised.29
Most airlines function on the basis of contacting their ground base first, which is a medical consulting service that consists of physicians trained in aerospace and emergency medicine; they must also request assistance from volunteering physicians on board if advised to do so by their ground-based medical personnel. If a flight must be diverted to a nearby airport in an emergency, the crew will contact the ground-based medical personnel, and ultimately the captain of the aircraft makes the decision for the flight diversion based on the airline policy and FAA regulations. The legislation governing these aspects and the responsibility of the medical consultants on the ground is complex and unclear.
Flying During Pregnancy
Flying is not contraindicated in an uncomplicated pregnancy, but there are some precautions that a pregnant traveler should consider. Excessive flying should be avoided, and a pregnant traveler should rest as much as possible while in the air; in addition, it is important to make comfortable arrangements: get a seat with more leg room, wear support hose and shoes with adjustable straps in case the feet swell, plan to walk in the aisles, take frequent bathroom breaks, and drink adequate water. Travelers should be wary of dehydration on airplanes, which can be worse during pregnancy. Certain conditions in pregnancy—such as severe anemia, sickle cell disease, clotting disorders, and placental insufficiency—can increase the risk of problems.
According to the American College of Obstetricians and Gynecologists, air travel is safest for pregnant women during the second trimester. It is best not to travel before 12 weeks’ gestation because of morning sickness and possible increased risk of miscarriage, although many pregnant women have no trouble flying in the first trimester. After 28 weeks, when the risk of going into labor increases, most airlines require a letter from a doctor stating the patient’s fitness for air travel while pregnant and confirming the estimated due date. If more than 36 weeks’ pregnant, many airlines will not let pregnant patients fly because of the increased risk of delivering on board.
Spaceflight
Spaceflight involves the launch of a space vehicle, after which it accelerates to orbital speed and for a period of time stays in space in an environment known as microgravity, where there is an absence of gravitational forces. The International Space Station is a research lab set up in space, and experiments have been continuously conducted in the microgravity environment there since November 2000 by crewmembers who are replaced at regular intervals. Here, we will cover the physiologic changes that occur during spaceflight and its anesthetic implications, should a crewmember require medical treatment that involves anesthesiologists; these implications may be applicable to the astronauts for a long time after their return to earth.
The space station and space shuttle often operate in microgravity, and pressure is maintained close to the atmospheric pressure at sea level, which is about 760 mm Hg. The pressure in a space suit, however, is 222 mm Hg, which places the wearer at potential risk of decompression sickness as a result of the pressure change. Astronauts use space suits during extravehicular activity, and they breathe 100% oxygen to combat hypoxia (Fig. 28-4).

In the microgravity environment, central redistribution of blood occurs with reduced venous pressure and an increase in left-ventricular end-diastolic volume. In addition, facial edema occurs along with a diuresis that depletes up to 20% or more of plasma volume.30 Most astronauts experience transient nausea, vomiting, dizziness, and drowsiness shortly after reaching space. Skeletal muscle atrophy can occur after short missions, and cardiac muscle atrophy31 occurs after several days in space. Both renal stones from hypercalciuria and osteoporosis as a result of a loss of significant amounts of calcium from bones may occur during long spaceflights as an effect of lack of weight bearing.
Sudden exposure to zero atmospheric pressure, which could occur as a result of a tear in the space suit, causes ebullism and generalized bubble formation.8 If an unprotected human were to slip into the cold and airless void of space, using our knowledge of outer space, data from experiments, and extrapolations from accidents over the years, scientists were able to make some reasonable conclusions about what would happen.
A number of injuries would begin to occur immediately; although relatively minor at first, they would accumulate rapidly into a life-threatening combination. Expansion of gases within the lungs and digestive tract would be the first effect. Because water is converted into vapor immediately in the absence of atmospheric pressure, moisture in the mouth and eyes would quickly boil away. Water in the muscle and soft tissue would evaporate also, causing some parts of the body to swell to twice their usual size after a few moments. Within seconds the reduced pressure would cause the nitrogen dissolved in the blood to form gaseous bubbles, a painful condition known to divers as “the bends.” The first few seconds may not be life threatening, and “useful consciousness” would gradually fade as the effects of brain hypoxia set in. The gas exchange that normally takes place in the lungs would work in reverse, evolving oxygen out of the blood and into the alveoli as a result of the low atmospheric pressure. After about 10 seconds, loss of vision and impaired judgment occur, and the cooling effect of evaporation will lower the temperature of the mouth and nose to near freezing. Unconsciousness and convulsions would follow a few seconds later, followed by cyanosis, stupor, and unresponsiveness. Without intervention, the blood pressure would fall, the blood itself would begin to boil, and the heart would stop beating. There are no reports of successful resuscitation beyond that threshold.
Emergency care in space involves numerous challenges. First off, it is difficult to confine fluids; as a result, conventional vaporizers would have to be redesigned for use under conditions of microgravity. In addition, the risk of aspiration is increased, because acid reflux is more common in microgravity under general anesthesia. Also, the air-fluid interface generates bubbles, and IV fluids must have the air bubbles removed during administration, or fluids must be degassed before the flight. Hypotension may not be adequately treatable because of limited supplies, preexisting hypovolemia, and increased G-forces on reentry. Securing an airway may be difficult or unsuccessful because of facial edema and the insecure position of both the patient and the intubator. Scavenging the anesthetic gases and oxygen in space is another issue.
After landing, nausea and vomiting recur, and some degree of orthostatic intolerance is experienced by most astronauts.32 Such orthostasis may be due to hypovolemia, enhanced endothelial nitric oxide synthase expression, and downregulation of α-adrenergic receptors. In addition, some loss of pressor response to phenylephrine has been observed.33 Cardiovascular deconditioning, ventricular atrophy, and changes in arterial stiffness may also play a role. Although the physiologic response of anesthesia in space is not exactly known, the immediate postflight hemodynamic response to general or neuraxial anesthesia may include variable degrees of resistant hypotension.
The atrophy that occurs because of the effect of loss of gravity, immobilization, and disuse of the skeletal muscles result in proliferation of extrajunctional acetylcholine receptors. As a result astronauts may be sensitive to succinylcholine with an exaggerated hyperkalemia response and a risk of cardiac arrest. They may also be resistant to nondepolarizing neuromuscular blocking drugs. The most common electrolyte abnormalities reported after spaceflight are hypokalemia and hypomagnesemia.34
Thus the environment of space, limited in terms of area and resources available, makes any kind of medical treatment a logistical challenge. The anesthesiologist at present seems to be just an emergency care provider, should a need arise. Any further role in routine anesthetic management in space has a long way to go, along with developments in the active fields of robotics, surgery, and on-board diagnostics. It is important to realize the fact that even during a short spaceflight, astronauts have altered physiology that continues beyond their return to earth. Therefore it is best to avoid administration of elective anesthesia to astronauts after their return and to provide time for the altered physiology to normalize.
References
1. Basu C.K., Selvamurthy W., Bhaumick G., Gautam R.K., Sawhney R.C. Respiratory changes during initial days of acclimatization to increasing altitudes. Aviat Space Environ Med. 1996;67:40–45.
2. Hupperets M.D., Hopkins S.R., Pronk M.G., et al. Increased hypoxic ventilatory response during 8 weeks at 3800 m altitude. Respir Physiol Neurobiol. 2004;142:145–152.
3. Erzurum S.C., Ghosh S., Janocha A.J., et al. Higher blood flow and circulating NO products offset high altitude hypoxia among Tibetans. Proc Natl Acad Sci U S A. 2007;104(17):593–598.
4. Leissner K.B., Mahmood F.U. Physiology and pathophysiology at high altitude: considerations for the anesthesiologist. J Anesth. 2009;23:543–553.
5. Fukuda R., Zhang H., Kim J.W., et al. HIF-1 regulates cytochrome oxidase subunits to optimize efficiency of respiration in hypoxic cells. Cell. 2007;129:111–122.
6. Forsythe J.S., Hang B.H., Iyer N.V., et al. Activation of vascular endothelial growth factor gene transcription by hypoxia-inducible factor 1. Mol Cell Biol. 1999;16:4604–4613.
7. Hackett P.H., Roach R.C. High-altitude illness. N Engl J Med. 2001;345:107–114.
8. Moon R.E., Camporesi E.M. Clinical care in extreme environments: at high and low pressure and in space. In Miller R., Eriksson L., Fleisher L.A., Wiener-Kronish J., eds.: Miller’s anesthesia, ed 7, Philadelphia: Churchill Livingstone, 2010.
9. Cymerman A, Rock PB: Medical problems in high mountain environments: a handbook for medical officers. USARIEM-TN94-2. U.S. Army Research Institute, Department of Environmental Medicine, Thermal and Mountain Medicine Division Technical Report. Available at archive.rubicon-foundation.org/7976.
10. Niermeyer S. Cardiopulmonary transition in the high altitude infant. High Alt Med Biol. 2003;4(2):225–239.
11. Powell J.N., Gingrich T.F. Some aspects of nitrous oxide anesthesia at an altitude of one mile. Anesth Analg. 1969;48:680–685.
12. James M.F.M., Manson E.D.M., Dennett J.E. Nitrous oxide analgesia and altitude. Anaesthesia. 1982;37:285–288.
13. Safar P., Tenicela R. High altitude physiology in relation to anesthesia and inhalation therapy. Anesthesiology. 1964;25:515–531.
14. James M.F.M., White J.F. Anesthetic considerations at moderate altitude. Anesth Analg. 1984;63:1097–1105.
15. Hill D.W. Physics applied to anesthesia, ed 4. Boston: Butterworths; 1980. 336–337
16. McDowall D.G. Anaesthesia in a pressure chamber. Anaesthesia. 1964;19:321–336.
17. Friedman M.D., Lightstone P.J. The effect of high altitude on flowmeter performance [abstract]. Anesthesiology. 1981;55:A117.
18. Halsey M.J., White D.C. Gas and vapour supply. In: Gray T.C., Nunn J.F., Utting J.E., eds. General anaesthesia. ed 4. London: Butterworths; 1980:953–961.
19. Puri G.D., Jayant A., Dorje M., Tashi M. Propofol-fentanyl anaesthesia at high altitude: anaesthetic requirements and haemodynamic variations when compared with anaesthesia at low altitude. Acta Anaesthesiol Scand. 2008;52:427–431.
20. IATA Annual Report. Available at http://www.iata.org/pressroom/documents/annual-report-2011.pdf.
21. Delaune E.F., 3rd., Lucas R.H., Illig P. In-flight medical events and aircraft diversions: one airline’s experience. Aviat Space Environ Med. 2003;74:62–68.
22. Cummins R.O., Schubach J.A. Frequency and types of medical emergencies among commercial air travelers. JAMA. 1989;261:1295–1299.
23. Aerospace Medical Association. Air Transport Medicine Committee: Medical guidelines for airline travel, ed 2. Alexandria, VA: Aerospace Medical Association; 2003.
24. Ruskin K.J., Hernandez A.K., Barash P.G. Management of in-flight medical emergencies. Anesthesiology. 2008;108:749–755.
25. Dillard T.A., Bansal A.K. Commentary: pulse oximetry during airline travel. Aviat Space Environ Med. 2007;78:143–144.
26. Closon M., Vivier E., Breynaert C., et al. Air embolism during an aircraft flight in a passenger with a pulmonary cyst: a favorable outcome with hyperbaric therapy. Anesthesiology. 2004;101:539–542.
27. Zitter J.N., Mazonson P.D., Miller D.P., Hulley S.B., Balmes J.R. Aircraft cabin air recirculation and symptoms of the common cold. JAMA. 2002;288:483–486.
28. Adi Y., Bayliss S., Rouse A., Taylor R.S. The association between air travel and deep vein thrombosis: systematic review and meta-analysis. BMC Cardiovasc Disord. 2004;4:7.
29. 105th Congress, public law 170, Avaiation Medical Assistance Act of 1998. Available at http://www.gpo.gov/fdsys/pkg/PLAW-105publ170/html/PLAW-105publ170.htm.
30. Leach C.S., Alfrey C.P., Suki W.N., et al. Regulation of body fluid compartments during short-term space flight. J Appl Physiol. 1996;81:105–116.
31. Tuday E.C., Berkowitz D.E. Microgravity and cardiac atrophy; no sex discrimination. J Appl Physiol. 2007;103:1–2.
32. Buckey J.C., Jr., Lane L.D., Levine B.D., et al. Orthostatic intolerance after spaceflight. J Appl Physiol. 1996;81:7–18.
33. Meck J.V., Waters W.W., Zeigler M.G., et al. Mechanisms of post-spaceflight orthostatic hypotension: low alpha1-adrenergic receptor responses before flight and central autonomic dysregualtion post flight. Am J Physiol Heart Circ Physiol. 2004;286:H1486–H1495.
34. Leach C.S., Alexander W.C., Johnson P.C. Endocrine, electrolyte, and fluid volume changes associated with Apollo missions. In: Johnston R.S., Dietlein L.F., Berry C.A., eds. Biomedical results of Apollo. Washington, DC: Biotechnology; 1975:163–184.