8 Head and Neck
Conceptual overview
GENERAL DESCRIPTION
The head and neck are anatomically complex areas of the body.
Head
Major compartments
The head is composed of a series of compartments, which are formed by bone and soft tissues. They are:
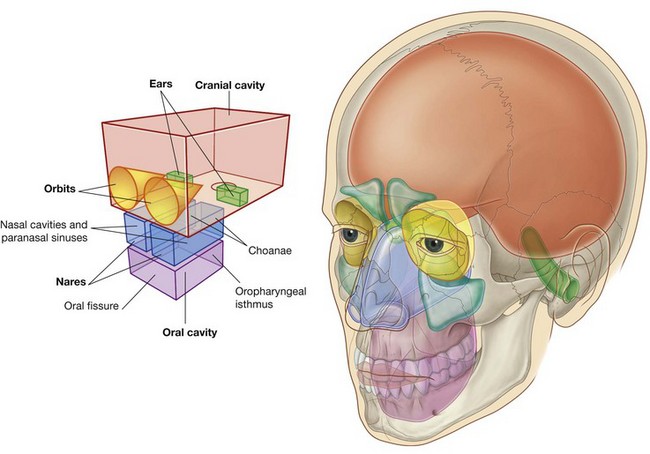
The cranial cavity is the largest compartment and contains the brain and associated membranes (meninges).
Most of the ear apparatus on each side is contained within one of the bones forming the floor of the cranial cavity. The external parts of the ears extend laterally from these regions.
The two orbits contain the eyes. They are cone-shaped chambers immediately inferior to the anterior aspect of the cranial cavity, and the apex of each cone is directed posteromedially. The walls of the orbits are bone, whereas the base of each conical chamber can be opened and closed by the eyelids.
The nasal cavities are the upper parts of the respiratory tract and are between the orbits. They have walls, floors, and ceilings, which are predominantly composed of bone and cartilage. The anterior openings to the nasal cavities are nares (nostrils), and the posterior openings are choanae (posterior nasal apertures).
Continuous with the nasal cavities are air-filled extensions (paranasal sinuses), which project laterally, superiorly, and posteriorly into surrounding bones. The largest, the maxillary sinuses, are inferior to the orbits.
The oral cavity is inferior to the nasal cavities, and separated from them by the hard and soft palates. The floor of the oral cavity is formed entirely of soft tissues.
The anterior opening to the oral cavity is the oral fissure (mouth), and the posterior opening is the oropharyngeal isthmus. Unlike the nares and choanae, which are continuously open, both the oral fissure and oropharyngeal isthmus can be opened and closed by surrounding soft tissues.
Other anatomically defined regions
In addition to the major compartments of the head, two other anatomically defined regions (infratemporal fossa and pteryatine fossa) of the head on each side are areas of transition from one compartment of the head to another (Fig. 8.2). The face and scalp also are anatomically defined areas of the head and are related to external surfaces.
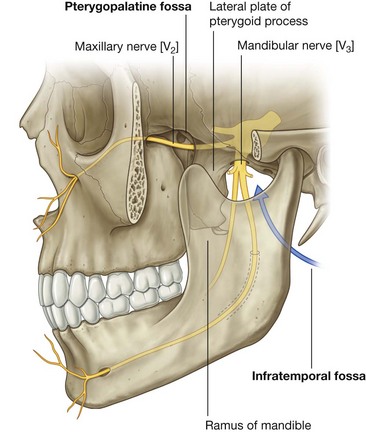
The infratemporal fossa is an area between the posterior aspect (ramus) of the mandible and a flat region of bone (lateral plate of the pterygoid process) just posterior to the upper jaw (maxilla). This fossa, bounded by bone and soft tissues, is a conduit for one of the major cranial nerves—the mandibular nerve (the mandibular division of the trigeminal nerve [V3]), which passes between the cranial and oral cavities.
The pteryatine fossa on each side is just posterior to the upper jaw. This small fossa communicates with the cranial cavity, the infratemporal fossa, the orbit, the nasal cavity, and the oral cavity. A major structure passing through the pteryatine fossa is the maxillary nerve (the maxillary division of the trigeminal nerve [V2]).
The face is the anterior aspect of the head and contains a unique group of muscles that move the skin relative to underlying bone and control the anterior openings to the orbits and oral cavity (Fig. 8.3).
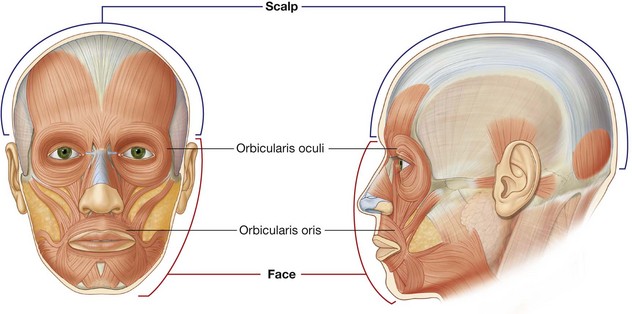
The scalp covers the superior, posterior, and lateral regions of the head (Fig. 8.3).
Neck
The neck extends from the head above to the shoulders and thorax below (Fig. 8.4). Its superior boundary is along the inferior margins of the mandible and bone features on the posterior aspect of the skull. The posterior neck is higher than the anterior neck to connect cervical viscera with the posterior openings of the nasal and oral cavities.
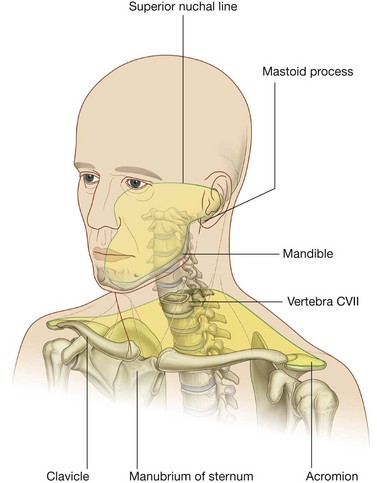
The inferior boundary of the neck extends from the top of the sternum, along the clavicle, and onto the adjacent acromion, a bony projection of the scapula. Posteriorly, the inferior limit of the neck is less well defined, but can be approximated by a line between the acromion and the spinous process of vertebra CVII, which is prominent and easily palpable. The inferior border of the neck encloses the base of the neck.
Compartments
The neck has four major compartments (Fig. 8.5), which are enclosed by an outer musculofascial collar:
 the visceral compartment contains important glands (thyroid, parathyroid, and thymus), and parts of the respiratory and digestive tracts that pass between the head and thorax; and
the visceral compartment contains important glands (thyroid, parathyroid, and thymus), and parts of the respiratory and digestive tracts that pass between the head and thorax; and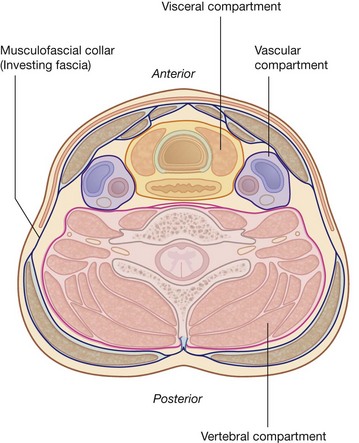
Larynx and pharynx
The neck contains two specialized structures associated with the digestive and respiratory tracts—the larynx and pharynx.
The larynx (Fig. 8.6) is the upper part of the lower airway and is attached below to the top of the trachea and above, by a flexible membrane, to the hyoid bone, which in turn is attached to the floor of the oral cavity. A number of cartilages form a supportive framework for the larynx, which has a hollow central channel. The dimensions of this central channel can be adjusted by soft tissue structures associated with the laryngeal wall. The most important of these are two lateral vocal folds, which project toward each other from adjacent sides of the laryngeal cavity. The upper opening of the larynx (laryngeal inlet) is tilted posteriorly, and is continuous with the pharynx.
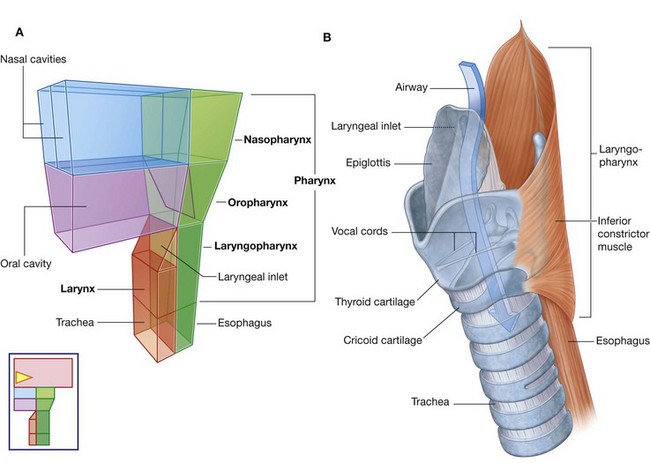
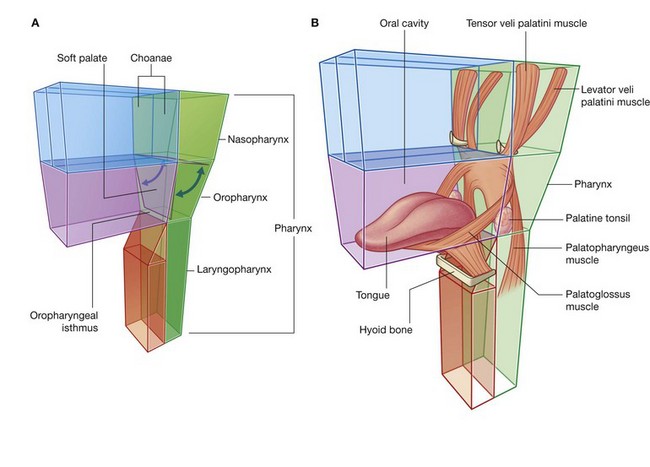
The pharynx (Fig. 8.6) is a chamber in the shape of a half-cylinder with walls formed by muscles and fascia. Above, the walls are attached to the base of the skull, and below to the margins of the esophagus. On each side, the walls are attached to the lateral margins of the nasal cavities, the oral cavity, and the larynx. The two nasal cavities, the oral cavity, and the larynx therefore open into the anterior aspect of the pharynx, and the esophagus opens inferiorly.
The part of the pharynx posterior to the nasal cavities is the nasopharynx. Those parts posterior to the oral cavity and larynx are the oropharynx and laryngopharynx, respectively.
FUNCTIONS
Protection
The head houses and protects the brain and all the receptor systems associated with the special senses—the nasal cavities associated with smell, the orbits with vision, the ears with hearing and balance, and the oral cavity with taste.
Contains upper parts of respiratory and digestive tracts
The head contains the upper parts of the respiratory and digestive systems—the nasal and oral cavities—which have structural features for modifying the air or food passing into each system.
Communication
The head and neck are involved in communication. Sounds produced by the larynx are modified in the pharynx and oral cavity to produce speech. In addition, the muscles of facial expression adjust the contours of the face to relay nonverbal signals.
Positioning the head
The neck supports and positions the head. Importantly, it enables an individual to position sensory systems in the head relative to environmental cues without moving the entire body.
Connects the upper and lower respiratory and digestive tracts
The neck contains specialized structures (pharynx and larynx) that connect the upper parts of the digestive and respiratory tracts (nasal and oral cavities) in the head, with the esophagus and trachea, which begin relatively low in the neck and pass into the thorax.
COMPONENT PARTS
Skull
The many bones of the head collectively form the skull (Fig. 8.7A). Most of these bones are interconnected by sutures, which are immovable fibrous joints (Fig. 8.7B).
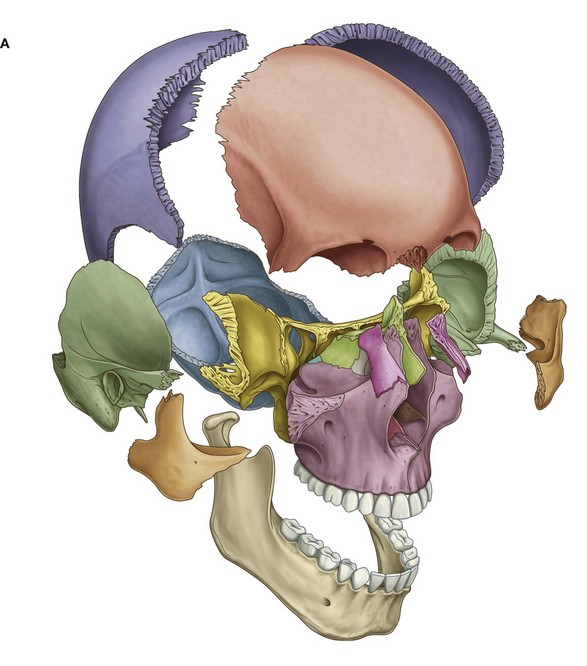
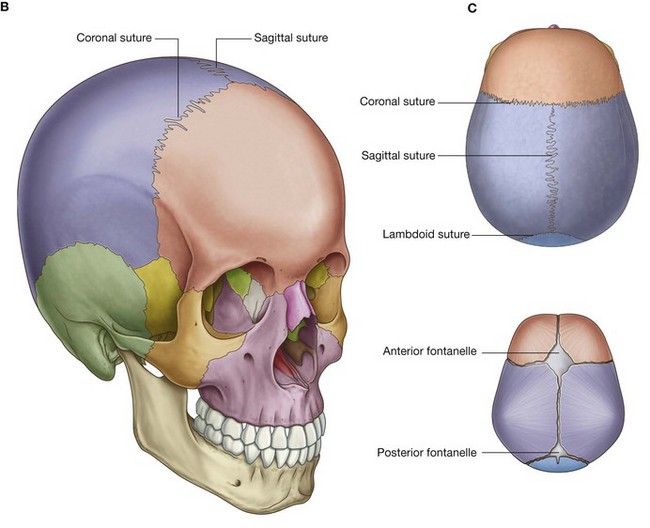
In the fetus and newborn, large membranous and unossified gaps (fontanelles) between the bones of the skull, particularly between the large flat bones that cover the top of the cranial cavity (Fig. 8.7C), allow:
Most of the fontanelles close during the first year of life. Full ossification of the thin connective tissue ligaments separating the bones at the suture lines begins in the late twenties, and is normally completed in the fifth decade of life.
There are only three pairs of synovial joints on each side in the head. The largest are the temporomandibular joints between the lower jaw (mandible) and the temporal bone. The other two synovial joints are between the three tiny bones in the middle ear, the malleus, incus, and stapes.
Cervical vertebrae
The seven cervical vertebrae form the bony framework of the neck.
Cervical vertebrae (Fig. 8.8A) are characterized by:
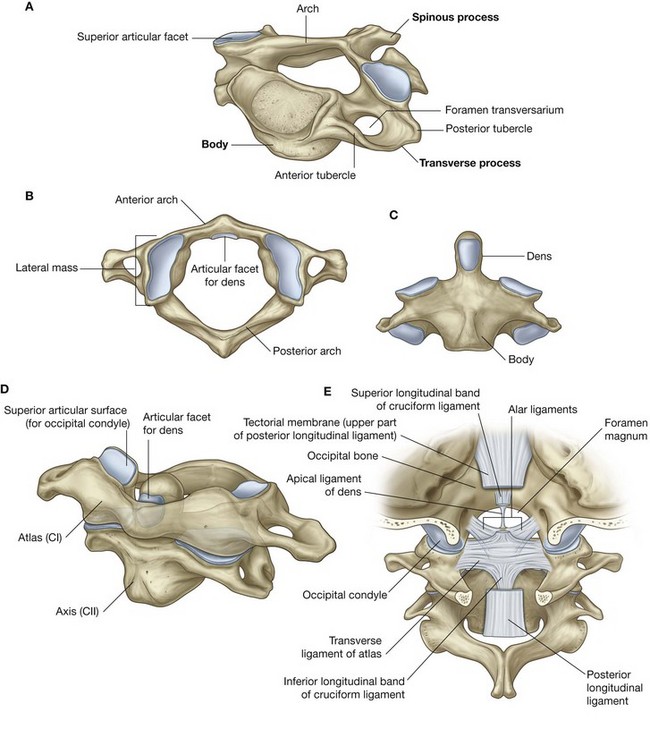
Fig. 8.8 Cervical vertebrae. A. Typical features. B. Atlas—vertebra CI (superior view). C. Axis—vertebra CII (anterior view). D. Atlas and axis (anterolateral view). E. Atlanto-occipital joint (posterior view).
Together the foramina transversarium form a longitudinal passage on each side of the cervical vertebral column for blood vessels (vertebral artery and veins) passing between the base of the neck and the cranial cavity.
The typical transverse process of a cervical vertebra also has anterior and posterior tubercles for muscle attachment. The anterior tubercles are derived from the same embryological elements that give rise to ribs in the thoracic region. Occasionally, cervical ribs develop from these elements, particularly in association with the lower cervical vertebrae.
The upper two cervical vertebrae (CI and CII) are modified for moving the head (Fig. 8.8B–8.8E) (see also Chapter 2).
Hyoid bone
The hyoid bone is a small U-shaped bone (Fig. 8.9A) oriented in the horizontal plane just superior to the larynx, where it can be palpated and moved from side to side.
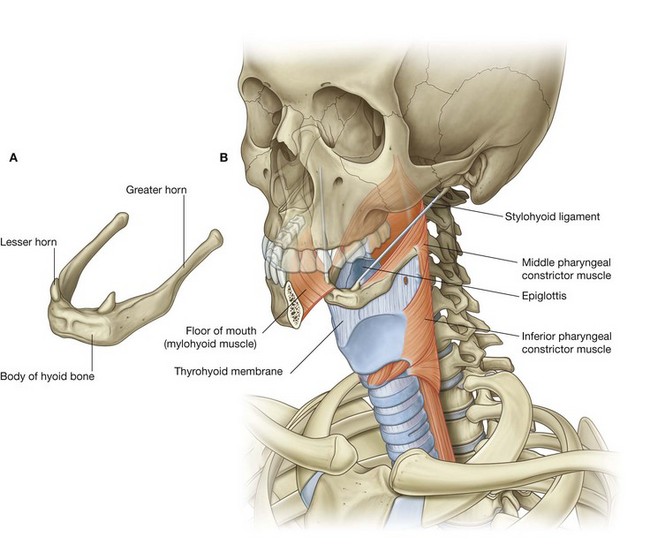
The hyoid bone does not articulate directly with any other skeletal elements in the head and neck.
The hyoid bone is a highly movable and strong bony anchor for a number of muscles and soft tissue structures in the head and neck. Significantly, it is at the interface between three dynamic compartments:
Soft palate
The soft palate is a soft tissue flap-like structure “hinged” to the back of the hard palate (Fig. 8.10A) with a free posterior margin. It can be elevated and depressed by muscles (Fig. 8.10B).
RELATIONSHIP TO OTHER REGIONS
Thorax
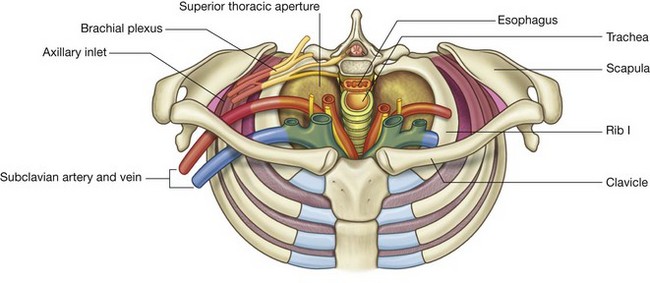
The superior thoracic aperture (thoracic inlet) opens directly into the base of the neck (Fig. 8.11). Structures passing between the head and thorax pass up and down through the superior thoracic aperture and the visceral compartment of the neck. At the base of the neck, the trachea is immediately anterior to the esophagus, which is directly anterior to the vertebral column. There are major veins, arteries, and nerves anterior and lateral to the trachea.
Upper limbs
There is an axillary inlet (gateway to the upper limb) on each side of the superior thoracic aperture at the base of the neck (Fig. 8.11):
KEY FEATURES
Vertebral levels CIII/IV and CV/VI
In the neck, the two important vertebral levels (Fig. 8.12) are:
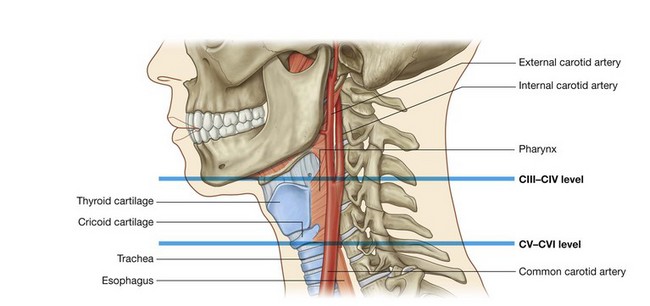
The internal carotid artery has no branches in the neck and ascends into the skull to supply much of the brain. It also supplies the eye and orbit. Other regions of the head and neck are supplied by branches of the external carotid artery.
Airway in the neck
The larynx (Fig. 8.13) and the trachea are anterior to the digestive tract in the neck, and can be accessed directly when upper parts of the system are blocked.
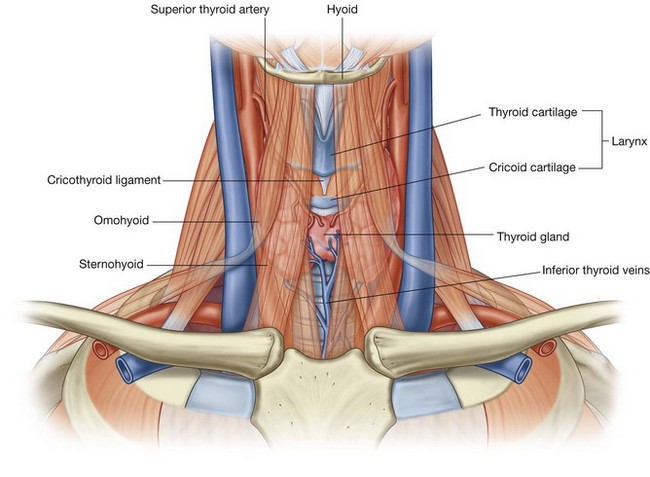
A cricothyrotomy makes use of the easiest route of access through the cricothyroid ligament (cricovocal membrane, cricothyroid membrane) between the cricoid and thyroid cartilages of the larynx. The ligament can be palpated in the midline, and usually there are only small blood vessels, connective tissue, and skin (though occasionally, a small lobe of the thyroid gland—pyramidal lobe) overlying it. At a lower level, the airway can be accessed surgically through the anterior wall of the trachea by tracheostomy. This route of entry is complicated because large veins and part of the thyroid gland overlie this region.
Cranial nerves
There are twelve pairs of cranial nerves and their defining feature is that they exit the cranial cavity through foramina or fissures.
All cranial nerves innervate structures in the head or neck. In addition, the vagus nerve [X] descends through the neck and into the thorax and abdomen where it innervates viscera.
Parasympathetic fibers in the head are carried out of the brain as part of four cranial nerves—the oculomotor nerve [III], the facial nerve [VII], the glossopharyngeal nerve [IX], and the vagus nerve [X] (Fig. 8.14). Parasympathetic fibers in the oculomotor nerve [III], the facial nerve [VII], and the glossopharyngeal nerve [IX] destined for target tissues in the head leave these nerves, and are distributed with branches of the trigeminal nerve [V].
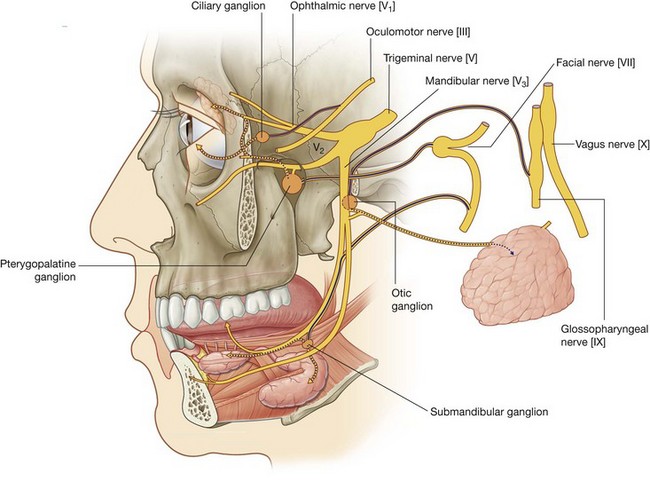
The vagus nerve [X] leaves the head and neck to deliver parasympathetic fibers to the thoracic and abdominal viscera.
Cervical nerves
There are eight cervical nerves (C1 to C8):
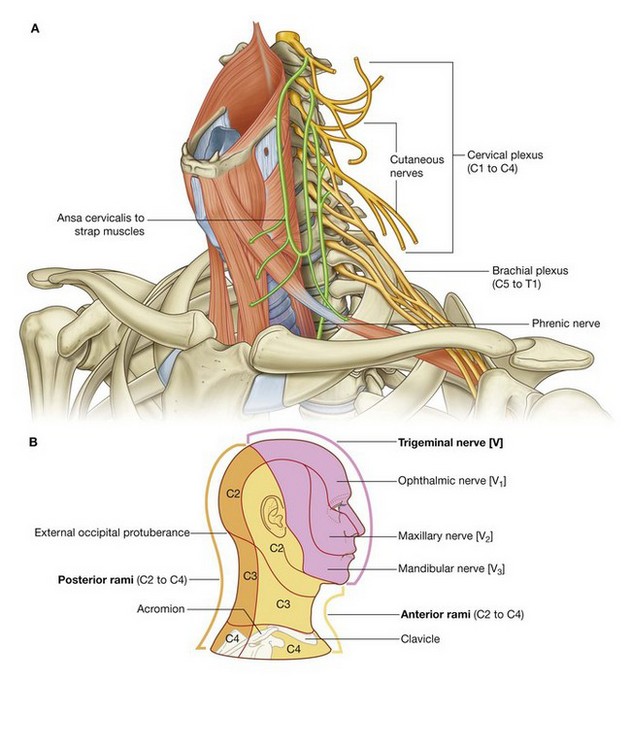
The anterior rami of C1 to C4 form the cervical plexus. The major branches from this plexus supply the strap muscles, the diaphragm (phrenic nerve), skin on the anterior and lateral parts of the neck, skin on the upper anterior thoracic wall, and skin on the inferior parts of the head (Fig. 8.15B).
The anterior rami of C5 to C8, together with a large component of the anterior ramus of T1, form the brachial plexus, which innervates the upper limb.
Functional separation of the digestive and respiratory passages
The pharynx is a common chamber for the digestive and respiratory tracts. Consequently, breathing can take place through the mouth as well as through the nose, and material from the oral cavity can potentially enter either the esophagus or the larynx. Importantly:
Normally, the soft palate, epiglottis, and soft tissue structures within the larynx act as valves to prevent food and liquid from entering lower parts of the respiratory tract (Fig. 8.16A).
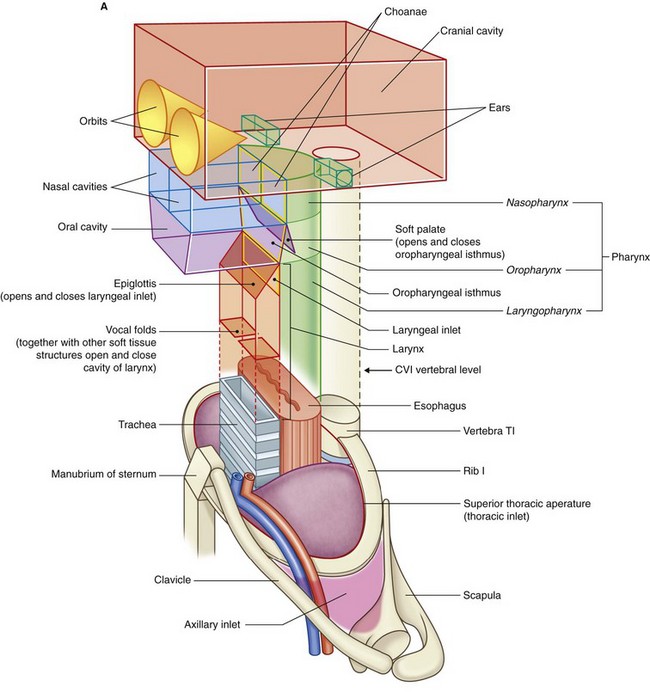
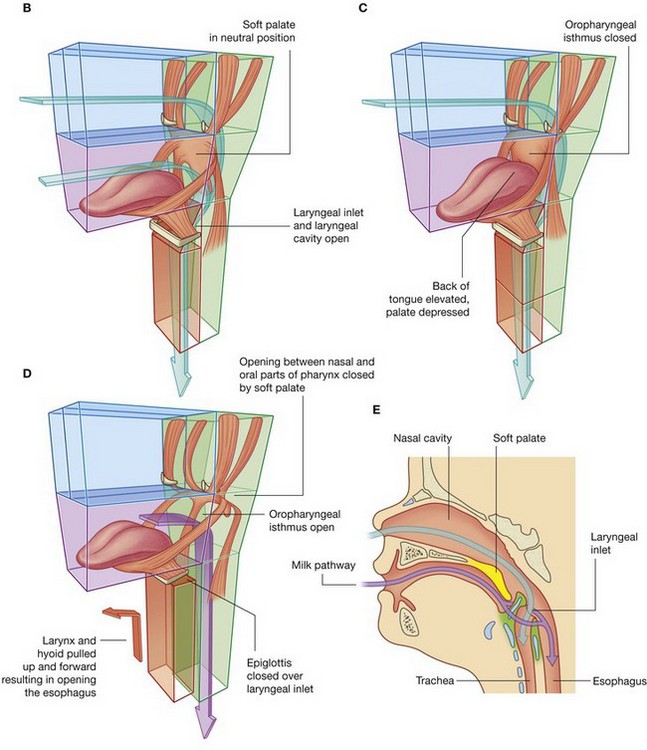
Fig. 8.16 Larynx, soft palate, epiglottis, and oropharyngeal isthmus. A. Overall design. B. Normal breathing. C. Breathing with food or liquid in the oral cavity. D. Swallowing. E. In a newborn child.
During normal breathing, the airway is open and air passes freely through the nasal cavities (or oral cavity), pharynx, larynx, and trachea (Fig. 8.16A). The lumen of the esophagus is normally closed because, unlike the airway, it has no skeletal support structures to hold it open.
When the oral cavity is full of liquid or food, the soft palate is swung down (depressed) to close the oropharyngeal isthmus, thereby allowing manipulation of food and fluid in the oral cavity while breathing (Fig. 8.16C).
When swallowing, the soft palate and parts of the larynx act as valves to ensure proper movement of food from the oral cavity into the esophagus (Fig. 8.16D).
The soft palate elevates to open the oropharyngeal isthmus while at the same time sealing off the nasal part of the pharynx from the oral part. This prevents food and fluid from moving upward into the nasopharynx and nasal cavities.
The epiglottis of the larynx closes the laryngeal inlet and much of the laryngeal cavity becomes occluded by opposition of the vocal folds and soft tissue folds superior to them. In addition, the larynx is pulled up and forward to facilitate the moving of food and fluid over and around the closed larynx and into the esophagus.
In newborns, the larynx is high in the neck and the epiglottis is above the level of the soft palate (Fig. 8.16E). Babies can therefore suckle and breathe at the same time. Liquid flows around the larynx without any danger of entering the airway. During the second year of life, the larynx descends into the low cervical position characteristic of adults.
Triangles of the neck
The two muscles (trapezius and sternocleidomastoid) that form part of the outer cervical collar divide the neck into anterior and posterior triangles on each side (Fig. 8.17).
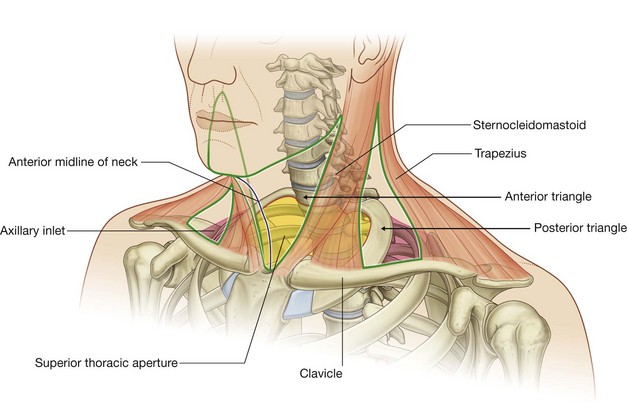
The boundaries of each anterior triangle are:
Regional anatomy
SKULL
The skull has 22 bones, excluding the ossicles of the ear. Except for the mandible, which forms the lower jaw, the bones of the skull are attached to each other by sutures, are immobile, and form the cranium.
The cranium can be subdivided into:
The bones forming the calvaria are mainly the paired temporal and parietal bones, and parts of the unpaired frontal, sphenoid, and occipital bones.
The bones forming the base of the cranium are mainly parts of the sphenoid, temporal, and occipital bones.
The bones forming the facial skeleton are the paired nasal bones, palatine bones, lacrimal bones, zygomatic bones, maxillae, inferior nasal conchae, and the unpaired vomer.
The mandible is not part of the cranium nor part of the facial skeleton.
Anterior view
The anterior view of the skull includes the forehead superiorly, and, inferiorly, the orbits, the nasal region, the part of the face between the orbit and the upper jaw, the upper jaw, and the lower jaw (Fig. 8.18).
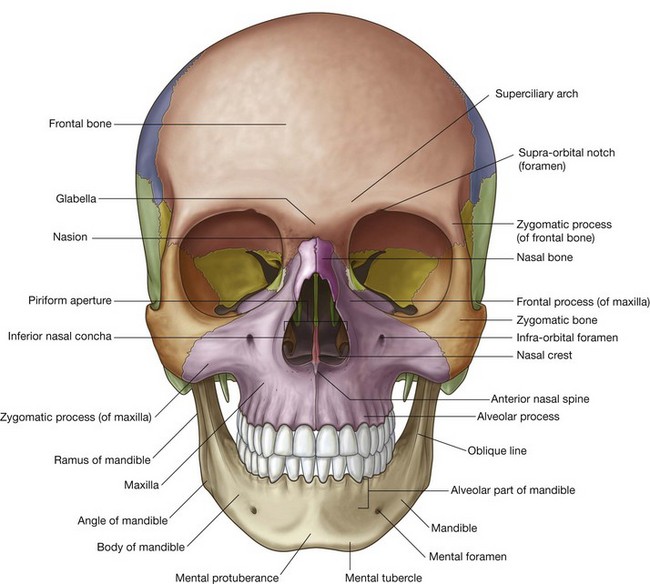
Frontal bone
The forehead consists of the frontal bone, which also forms the superior part of the rim of each orbit (Fig. 8.18).
Just superior to the rim of the orbit on each side are the raised superciliary arches. These are more pronounced in men than in women. Between these arches is a small depression (the glabella).
Clearly visible in the medial part of the superior rim of each orbit is the supra-orbital foramen (supra-orbital notch; Table 8.1).
Table 8.1 External foramina of the skull
| Foramen | Structures passing through foramen |
|---|---|
| Anterior view | |
| Supra-orbital foramen | Supra-orbital nerve and vessels |
| Infra-orbital foramen | Infra-orbital nerve and vessels |
| Mental foramen | Mental nerve and vessels |
| Lateral view | |
|---|---|
| Zygomaticofacial foramen | Zygomaticofacial nerve |
| Superior view | |
|---|---|
| Parietal foramen | Emissary veins |
| Inferior view | |
|---|---|
| Incisive foramina | Nasopalatine nerve; sphenopalatine vessels |
| Greater palatine foramen | Greater palatine nerve and vessels |
| Lesser palatine foramina | Lesser palatine nerves and vessels |
| Pterygoid canal | Pterygoid nerve and vessels |
| Foramen ovale | Mandibular nerve [V3]; lesser petrosal nerve |
| Foramen spinosum | Middle meningeal artery |
| Foramen lacerum | Filled with cartilage |
| Carotid canal | Internal carotid artery and nerve plexus |
| Foramen magnum | Continuation of brain and spinal cord; vertebral arteries and nerve plexuses; anterior spinal artery; posterior spinal arteries; roots of accessory nerve [XI]; meninges |
| Condylar canal | Emissary veins |
| Hypoglossal canal | Hypoglossal nerve [XII] and vessels |
| Jugular foramen | Internal jugular vein; inferior petrosal sinus; glossopharyngeal nerve [IX]; vagus nerve [X]; accessory nerve [XI] |
| Stylomastoid foramen | Facial nerve [VII] |
Medially, the frontal bone projects inferiorly forming a part of the medial rim of the orbit.
Laterally, the zygomatic process of the frontal bone projects inferiorly forming the upper lateral rim of the orbit. This process articulates with the frontal process of the zygomatic bone.
Zygomatic and nasal bones
The lower lateral rim of the orbit, as well as the lateral part of the inferior rim of the orbit is formed by the zygomatic bone (the cheekbone).
Superiorly, in the nasal region the paired nasal bones articulate with each other in the midline, and with the frontal bone superiorly. The center of the frontonasal suture formed by the articulation of the nasal bones and the frontal bone is the nasion.
Laterally, each nasal bone articulates with the frontal process of each maxilla.
Inferiorly, the piriform aperture is the large opening in the nasal region and the anterior opening of the nasal cavity. It is bounded superiorly by the nasal bones and laterally and inferiorly by each maxilla.
Visible through the piriform aperture are the fused nasal crests, forming the lower part of the bony nasal septum and ending anteriorly as the anterior nasal spine, and the paired inferior nasal conchae.
Maxillae
The part of the face between the orbit and the upper teeth and each upper jaw is formed by the paired maxillae.
Superiorly, each maxilla contributes to the inferior and medial rims of the orbit.
Laterally, the zygomatic process of each maxilla articulates with the zygomatic bone and medially, the frontal process of each maxilla articulates with the frontal bone.
Inferiorly, the part of each maxilla, lateral to the opening of the nasal cavity, is the body of maxilla.
On the anterior surface of the body of maxilla, just below the inferior rim of the orbit, is the infra-orbital foramen (Table 8.1).
Inferiorly, each maxilla ends as the alveolar process, which contains the teeth and forms the upper jaw.
Mandible
The lower jaw (mandible) is the most inferior structure in the anterior view of the skull. It consists of the body of mandible anteriorly and the ramus of mandible posteriorly. These meet posteriorly at the angle of mandible. All these parts of the mandible are visible, to some extent, in the anterior view.
The body of mandible is arbitrarily divided into two parts:
The base of mandible has a midline swelling (the mental protuberance) on its anterior surface where the two sides of the mandible come together. Just lateral to the mental protuberance, on either side, are slightly more pronounced bumps (mental tubercles).
Laterally, a mental foramen (Table 8.1) is visible halfway between the upper border of the alveolar part of mandible and the lower border of the base of mandible. Continuing past this foramen is a ridge (the oblique line) passing from the front of the ramus onto the body of mandible. The oblique line is a point of attachment for muscles that depress the lower lip.
Lateral view
The lateral view of the skull consists of the lateral wall of the cranium, which includes lateral portions of the calvaria and the facial skeleton, and half of the lower jaw (Fig. 8.19):
bones forming the lateral portion of the calvaria include the frontal, parietal, occipital, sphenoid, and temporal bones; bones forming the visible part of the facial skeleton include the nasal, maxilla, and zygomatic bones.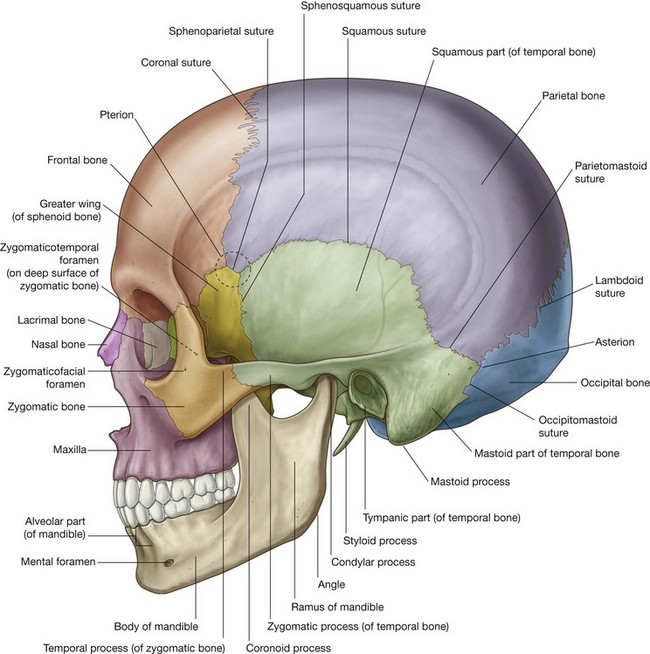
Lateral portion of the calvaria
The lateral portion of the calvaria begins anteriorly with the frontal bone. In upper regions, the frontal bone articulates with the parietal bone at the coronal suture. The parietal bone then articulates with the occipital bone at the lambdoid suture.
In lower parts of the lateral portion of the calvaria, the frontal bone articulates with the greater wing of sphenoid bone (Fig. 8.19), which then articulates with the parietal bone at the sphenoparietal suture, and with the anterior edge of the temporal bone at the sphenosquamous suture.
The junction where the frontal, parietal, sphenoid, and temporal bones are in close proximity is the pterion. The clinical consequences of a skull fracture in this area can be very serious. The bone in this area is particularly thin and overlies the anterior division of the middle meningeal artery, which can be torn by a skull fracture in this area, resulting in an extradural hematoma.
The final articulation across the lower part of the lateral portion of the calvaria is between the temporal bone and the occipital bone at the occipitomastoid suture.
Temporal bone
A major contributor to the lower portion of the lateral wall of the cranium is the temporal bone (Fig. 8.19), which consists of several parts:
the squamous part has the appearance of a large flat plate, forms the anterior and superior parts of the temporal bone, contributes to the lateral wall of the cranium, and articulates anteriorly with the greater wing of the sphenoid bone at the sphenosquamous suture, and with the parietal bone superiorly at the squamous suture; the zygomatic process is an anterior bony projection from the lower surface of the squamous part of the temporal bone that initially projects laterally and then curves anteriorly to articulate with the temporal process of the zygomatic bone to form the zygomatic arch; immediately below the origin of the zygomatic process from the squamous part of the temporal bone is the tympanic part of the temporal bone, and clearly visible on the surface of this part is the external acoustic opening leading to the external acoustic meatus (ear canal); the petromastoid part, which is usually separated into a petrous part and a mastoid part for descriptive purposes.The mastoid part is the most posterior part of the temporal bone, and is the only part of the petromastoid part of the temporal bone seen on a lateral view of the skull. It is continuous with the squamous part of the temporal bone anteriorly, and articulates with the parietal bone superiorly at the parietomastoid suture, and with the occipital bone posteriorly at the occipitomastoid suture. These two sutures are continuous with each other, and the parietomastoid suture is continuous with the squamous suture.
Inferiorly, a large bony prominence (the mastoid process) projects from the inferior border of the mastoid part of the temporal bone. This is a point of attachment for several muscles.
Medial to the mastoid process, the styloid process projects from the lower border of the temporal bone.
Visible part of the facial skeleton
The bones of the viscerocranium visible in a lateral view of the skull include the nasal, maxilla, and zygomatic bones (Fig. 8.19) as follows:
the maxilla with its alveolar process containing teeth forming the upper jaw; anteriorly, it articulates with the nasal bone; superiorly, it contributes to the formation of the inferior and medial borders of the orbit; medially, its frontal process articulates with the frontal bone; laterally, its zygomatic process articulates with the zygomatic bone; the zygomatic bone, an irregularly shaped bone with a rounded lateral surface that forms the prominence of the cheek, is a visual centerpiece in this view—medially, it assists in the formation of the inferior rim of the orbit through its articulation with the zygomatic process of the maxilla; superiorly, its frontal process articulates with the zygomatic process of the frontal bone assisting in the formation of the lateral rim of the orbit; laterally, seen prominently in this view of the skull, the horizontal temporal process of the zygomatic bone projects backward to articulate with the zygomatic process of the temporal bone and so form the zygomatic arch.Usually a small foramen (the zygomaticofacial foramen; Table 8.1) is visible on the lateral surface of the zygomatic bone. A zygomaticotemporal foramen is present on the medial deep surface of the bone.
Mandible
The final bony structure visible in a lateral view of the skull is the mandible. Inferiorly in the anterior part of this view, it consists of the anterior body of mandible, a posterior ramus of mandible, and the angle of mandible where the inferior margin of the mandible meets the posterior margin of the ramus (Fig. 8.19).
The teeth are in the alveolar part of the body of mandible and the mental protuberance is visible in this view.
The mental foramen is on the lateral surface of the body and on the superior part of the ramus a condylar and coronoid process extend upward.
The condylar process is involved in articulation of the mandible with the temporal bone, and the coronoid process is the point of attachment for the temporalis muscle.
Posterior view
The occipital, parietal, and temporal bones are seen in the posterior view of the skull.
Occipital bone
Centrally the flat or squamous part of occipital bone is the main structure in this view of the skull (Fig. 8.20). It articulates superiorly with the paired parietal bones at the lambdoid suture and laterally with each temporal bone at the occipitomastoid sutures. Along the lambdoid suture small islands of bone (sutural bones or wormian bones) may be observed.
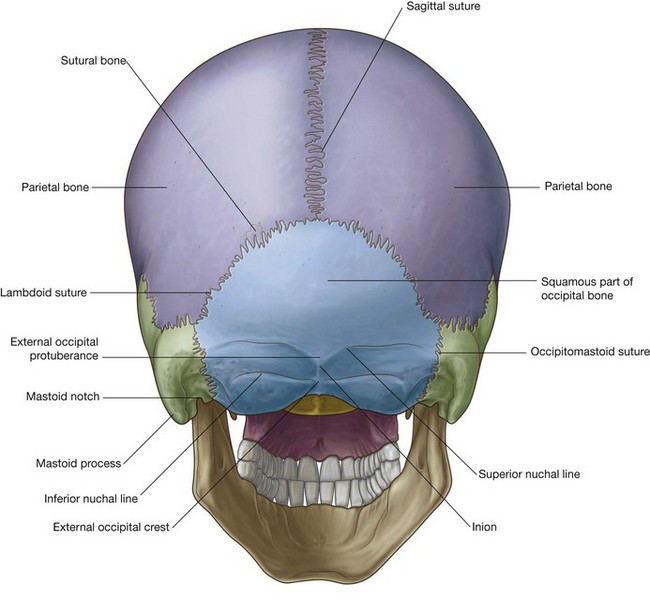
Several bony landmarks are visible on the occipital bone. There is a midline projection, (the external occipital protuberance) with curved lines extending laterally from it (superior nuchal lines). The most prominent point of the external occipital protuberance is the inion. About 1 inch (2.5 cm) below the superior nuchal lines two additional lines (the inferior nuchal lines) curve laterally. Extending downward from the external occipital protuberance is the external occipital crest.
Temporal bones
Laterally, the temporal bones are visible in the posterior view of the skull, with the mastoid processes being the prominent feature (Fig. 8.20). On the inferomedial border of each mastoid process is a notch (the mastoid notch), which is a point of attachment for the posterior belly of the digastric muscle.
Superior view
The frontal bone, parietal bones, and occipital bone are seen in a superior view of the skull (Fig. 8.21). These bones make up the superior part of the calvaria or the calva (skullcap).
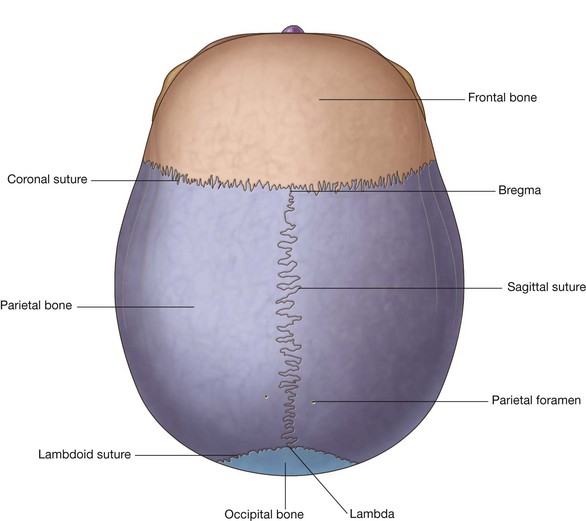
In an anterior to posterior direction:
The junction of the sagittal and coronal sutures is the bregma, and the junction of the sagittal and lambdoid sutures is the lambda.
The only foramen visible in this view of the skull may be the paired parietal foramina, posteriorly, one on each parietal bone just lateral to the sagittal suture (Fig. 8.21).
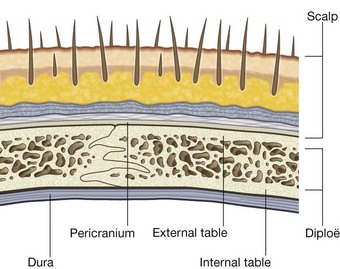
The bones making up the calvaria (Fig. 8.22) are unique in their structure, consisting of dense internal and external tables of compact bone separated by a layer of spongy bone (the diploë).
Inferior view
The base of the skull is seen in the inferior view and extends anteriorly from the middle incisor teeth posteriorly to the superior nuchal lines and laterally to the mastoid processes and zygomatic arches (Fig. 8.23).
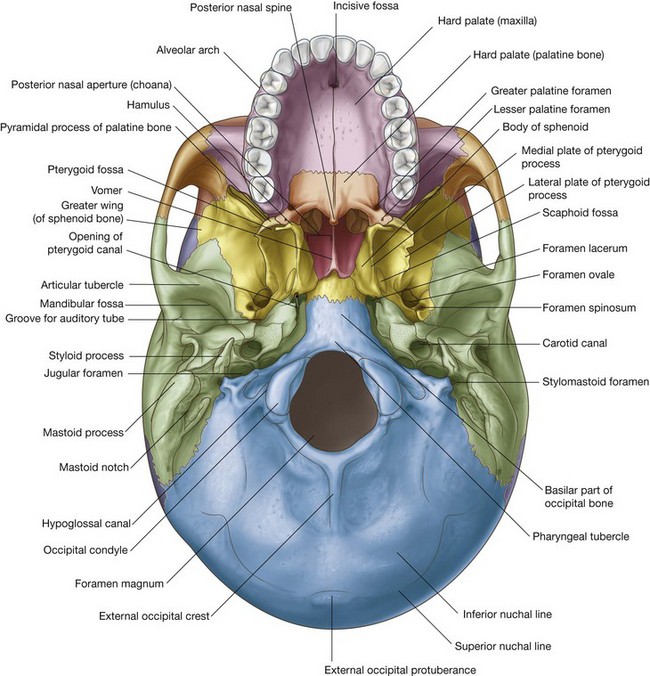
For descriptive purposes the base of the skull is often divided into:
a middle part, which extends from behind the hard palate to the anterior margin of the foramen magnum; and a posterior part, which extends from the anterior edge of the foramen magnum to the superior nuchal lines.Anterior part
The main features of the anterior part of the base of the skull are the teeth and the hard palate.
The teeth project from the alveolar processes of the two maxillae. These processes are together arranged in a U-shaped alveolar arch that borders the hard palate on three sides (Fig. 8.23).
The hard palate is composed of the palatine processes of each maxilla anteriorly and the horizontal plates of each palatine bone posteriorly.
The paired palatine processes of each maxilla meet in the midline at the intermaxillary suture, the paired maxilla and the paired palatine bones meet at the palatomaxillary suture, and the paired horizontal plates of each palatine bone meet in the midline at the interpalatine suture.
Several additional features are also visible when the hard palate is examined:
the incisive fossa in the anterior midline immediately posterior to the teeth, the walls of which contain incisive foramina (the openings of the incisive canals, which are passageways between the hard palate and nasal cavity); the greater palatine foramina near the posterolateral border of the hard palate on each side, which lead to greater palatine canals;Middle part
The middle part of the base of the skull is complex:
Anterior half
Vomer
Anteriorly, the small vomer is in the midline, resting on the sphenoid bone (Fig. 8.23). It contributes to the formation of the bony nasal septum separating the two choanae.
Sphenoid
Most of the anterior part of the middle part of the base of the skull consists of the sphenoid bone.
The sphenoid bone is made up of a centrally placed body, paired greater and lesser wings projecting laterally from the body, and two downward projecting pterygoid processes immediately lateral to each choana.
Three parts of the sphenoid bone, the body, greater wings, and pterygoid processes, are seen in the inferior view of the skull (Fig. 8.23). The lesser wing of the sphenoid is not seen in the inferior view.
Body
The body of the sphenoid is a centrally placed cube of bone containing two large air sinuses separated by a septum.
It articulates anteriorly with the vomer, ethmoid, and palatine bones, posterolaterally with the temporal bones, and posteriorly with the occipital bone.
Pterygoid processes
Extending downward from the junction of the body and the greater wings are the pterygoid processes (Fig. 8.23). Each of these processes consists of a narrow medial plate and broader lateral plate separated by the pterygoid fossa.
Each medial plate of the pterygoid process ends inferiorly with a hook-like projection, the pterygoid hamulus, and divides superiorly to form the small, shallow scaphoid fossa.
Just superior to the scaphoid fossa, at the root of the medial plate of the pterygoid process is the opening of the pterygoid canal, which passes forward from near the anterior margin of the foramen lacerum.
Greater wing
Lateral to the lateral plate of the pterygoid process is the greater wing of the sphenoid (Fig. 8.23), which not only forms a part of the base of the skull, but also continues laterally to form part of the lateral wall of the skull. It articulates laterally and posteriorly with parts of the temporal bone.
Important features visible on the surface of the greater wing in an inferior view of the skull are the foramen ovale and the foramen spinosum on the posterolateral border extending outward from the upper end of the lateral plate of the pterygoid process.
Posterior half
In the posterior half of the middle part of the base of the skull are the occipital bone and the paired temporal bones (Fig. 8.23).
Occipital bone
The occipital bone, or more specifically its basilar part, is in the midline immediately posterior to the body of the sphenoid. It extends posteriorly to the foramen magnum and is bounded laterally by the temporal bones.
Prominent on the basilar part of the occipital bone is the pharyngeal tubercle, a bony protuberance for the attachment of parts of the pharynx to the base of the skull (Fig. 8.23).
Temporal bone
Immediately lateral to the basilar part of the occipital bone is the petrous part of the petromastoid part of each temporal bone.
Wedge-shaped in its appearance, with its apex anteromedial, the petrous part of the temporal bone is between the greater wing of the sphenoid anteriorly and the basilar part of the occipital bone posteriorly. The apex forms one of the boundaries of the foramen lacerum, an irregular opening filled in life with cartilage (Fig. 8.23).
The other boundaries of the foramen lacerum are the basilar part of the occipital bone medially and the body of the sphenoid anteriorly.
Posterolateral from the foramen lacerum along the petrous part of the temporal bone is the large circular opening for the carotid canal.
Between the petrous part of the temporal bone and the greater wing of the sphenoid is a groove for the cartilaginous part of the pharyngotympanic tube (auditory tube). This groove continues posterolaterally into a bony canal in the petrous part of the temporal bone for the pharyngotympanic tube.
Just lateral to the greater wing of the sphenoid is the squamous part of the temporal bone, which participates in the temporomandibular joint. It contains the mandibular fossa, which is a concavity where the head of the mandible articulates with the base of the skull. An important feature of this articulation is the prominent articular tubercle, which is the downward projection of the anterior border of the mandibular fossa (Fig. 8.23).
Posterior part
The posterior part of the base of the skull extends from the anterior edge of the foramen magnum posteriorly to the superior nuchal lines (Fig. 8.23). It consists of parts of the occipital bone centrally and the temporal bones laterally.
Occipital bone
The occipital bone is the major bony element of this part of the base of the skull (Fig. 8.23). It has four parts organized around the foramen magnum, which is a prominent feature of this part of the base of the skull and through which the brain and spinal cord are continuous.
The parts of the occipital bone are the squamous part, which is posterior to the foramen magnum, the lateral parts, which are lateral to the foramen magnum, and the basilar part, which is anterior to the foramen magnum (Fig. 8.23).
The squamous and lateral parts are components of the posterior part of the base of the skull.
The most visible feature of the squamous part of the occipital bone when examining the inferior view of the skull is a ridge of bone (the external occipital crest), which extends downward from the external occipital protuberance toward the foramen magnum. The inferior nuchal lines arc laterally from the midpoint of the crest.
Immediately lateral to the foramen magnum are the lateral parts of the occipital bones, which contain numerous important structural features.
On each anterolateral border of the foramen magnum are the rounded occipital condyles (Fig. 8.23). These paired structures articulate with the atlas (vertebra CI). Posterior to each condyle is a depression (the condylar fossa) containing a condylar canal, and anterior and superior to each condyle is the large hypoglossal canal. Lateral to each hypoglossal canal is a large, irregular jugular foramen formed by opposition of the jugular notch of the occipital bone and jugular notch of the temporal bone.
Temporal bone
Laterally in the posterior part of the base of the skull is the temporal bone. The parts of the temporal bone seen in this location are the mastoid part of the petromastoid part and the styloid process (Fig. 8.23).
The lateral edge of the mastoid part is identified by the large cone-shaped mastoid process projecting from its inferior surface. This prominent bony structure is the point of attachment for several muscles. On the medial aspect of the mastoid process is the deep mastoid notch, which is also an attachment point for a muscle.
Anteromedial to the mastoid process is the needle-shaped styloid process projecting from the lower border of the temporal bone. The styloid process is also a point of attachment for numerous muscles and ligaments.
Finally, between the styloid process and the mastoid process is the stylomastoid foramen.
CRANIAL CAVITY
The cranial cavity is the space within the cranium that contains the brain, meninges, proximal parts of the cranial nerves, blood vessels, and cranial venous sinuses.
Roof
The calvaria is the dome-shaped roof that protects the superior aspect of the brain. It consists mainly of the frontal bone anteriorly, the paired parietal bones in the middle, and the occipital bone posteriorly (Fig. 8.24).
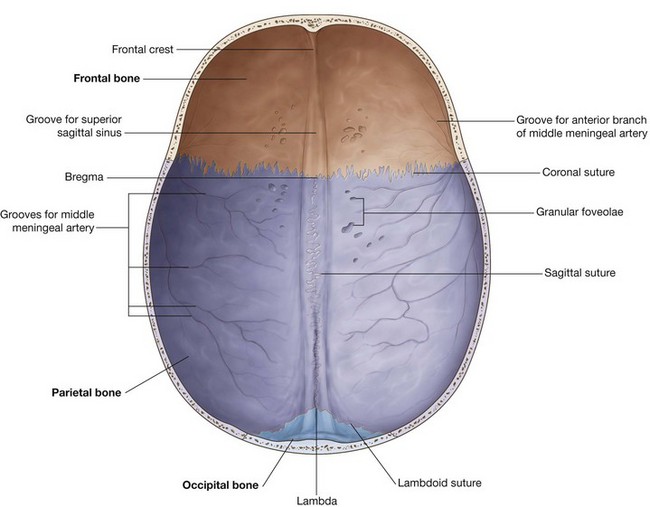
Sutures visible internally include:
Visible junctions of these sutures are the bregma, where the coronal and sagittal sutures meet, and the lambda, where the lambdoid and sagittal sutures meet.
Other markings on the internal surface of the calva include bony ridges, and numerous grooves and pits.
From anterior to posterior, features seen on the bony roof of the cranial cavity are:
a midline ridge of bone extending from the surface of the frontal bone (the frontal crest), which is a point of attachment for the falx cerebri (a specialization of the dura mater that partially separates the two cerebral hemispheres); at the superior point of the termination of the frontal crest the beginning of the groove for the superior sagittal sinus, which widens and deepens posteriorly and marks the position of the superior sagittal sinus (an intradural venous structure); on either side of the groove for the superior sagittal sinus throughout its course, a small number of depressions and pits (the granular foveolae), which mark the location of arachnoid granulations (prominent structures readily identifiable when a brain with its meningeal coverings is examined; the arachnoid granulations are involved in the reabsorption of cerebrospinal fluid); andFloor
The floor of the cranial cavity is divided into anterior, middle, and posterior cranial fossae.
Anterior cranial fossa
Parts of the frontal, ethmoid, and sphenoid bones form the anterior cranial fossa (Fig. 8.25). Its floor is composed of:
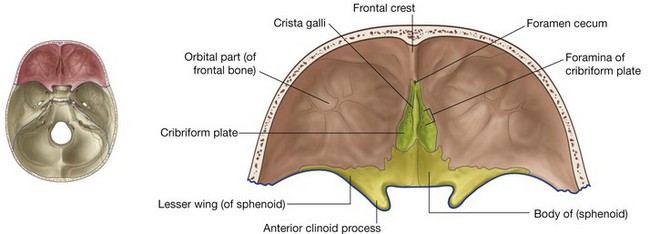
The anterior cranial fossa is above the nasal cavity and the orbits, and it is filled by the frontal lobes of the cerebral hemispheres.
Anteriorly, a small wedge-shaped midline crest of bone (the frontal crest) projects from the frontal bone. This is a point of attachment for the falx cerebri. Immediately posterior to the frontal crest is the foramen cecum (Table 8.2). This foramen between the frontal and ethmoid bones may transmit emissary veins connecting the nasal cavity with the superior sagittal sinus.
Table 8.2 Internal foramina of the skull
| Foramen | Structures passing through foramen |
|---|---|
| Anterior cranial fossa | |
| Foramen cecum | Emissary veins to nasal cavity |
| Olfactory foramina in cribriform plate | Olfactory nerves [I] |
| Optic canal | Optic nerve [II]; ophthalmic artery |
| Middle cranial fossa | |
|---|---|
| Superior orbital fissure | Oculomotor nerve [III]; trochlear nerve [IV]; ophthalmic division of the trigeminal nerve [V1]; abducent nerve [VI]; ophthalmic veins |
| Foramen rotundum | Maxillary division of the trigeminal nerve [V2] |
| Foramen ovale | Mandibular division of the trigeminal nerve [V3]; lesser petrosal nerve |
| Foramen spinosum | Middle meningeal artery |
| Hiatus for the greater petrosal nerve | Greater petrosal nerve |
| Hiatus for the lesser petrosal nerve | Lesser petrosal nerve |
| Posterior cranial fossa | |
|---|---|
| Foramen magnum | End of brainstem/beginning of spinal cord; vertebral arteries; spinal roots of the accessory nerve; meninges |
| Internal acoustic meatus | Facial nerve [VII]; vestibulocochlear nerve [VIII]; labyrinthine artery |
| Jugular foramen | Glossopharyngeal nerve [IX]; vagus nerve [X]; accessory nerve [XI]; inferior petrosal sinus, sigmoid sinus (forming internal jugular vein) |
| Hypoglossal canal | Hypoglossal nerve [XII]; meningeal branch of the ascending pharyngeal artery |
| Condylar canal | Emissary vein |
Posterior to the frontal crest is a prominent wedge of bone projecting superiorly from the ethmoid (the crista galli). This is another point of attachment for the falx cerebri, which is the vertical extension of dura mater partially separating the two cerebral hemispheres.
Lateral to the crista galli is the cribriform plate of the ethmoid bone (Fig. 8.25). This is a sieve-like structure, which allows small olfactory nerve fibers to pass through its foramina from the nasal mucosa to the olfactory bulb. The olfactory nerves are commonly referred to collectively as the olfactory nerve [I].
On each side of the ethmoid, the floor of the anterior cranial fossa is formed by relatively thin plates of frontal bone (the orbital part of the frontal bone), which also forms the roof of the orbit below. Posterior to both the frontal and ethmoid bones, the rest of the floor of the anterior cranial fossa is formed by the body and lesser wings of the sphenoid. In the midline, the body extends anteriorly between the orbital parts of the frontal bone to reach the ethmoid bone and posteriorly it extends into the middle cranial fossa.
The boundary between the anterior and middle cranial fossae in the midline is the anterior edge of the chiasmatic sulcus, a smooth groove stretching between the optic canals across the body of the sphenoid.
Lesser wings of the sphenoid
The two lesser wings of the sphenoid project laterally from the body of the sphenoid and form a distinct boundary between the lateral parts of the anterior and middle cranial fossae.
Overhanging the anterior part of the middle cranial fossae, each lesser wing ends laterally as a sharp point at the junction of the frontal bone and the greater wing of the sphenoid near the upper lateral edge of the superior orbital fissure that is formed between the greater and lesser wings.
Medially each lesser wing widens, curves posteriorly, and ends as a rounded anterior clinoid process (Fig. 8.25). These processes serve as the anterior point of attachment for the tentorium cerebelli, which is a sheet of dura that separates the posterior part of the cerebral hemispheres from the cerebellum. Just anterior to each anterior clinoid process is a circular opening in the lesser wing of the sphenoid (the optic canal), through which the ophthalmic artery and optic nerve [II] pass as they exit the cranial cavity to enter the orbit. The optic canals are usually included in the middle cranial fossa.
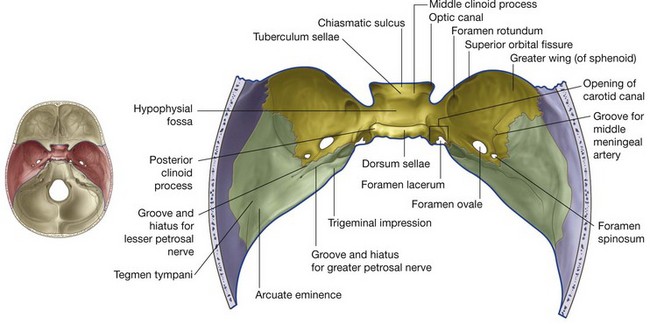
Middle cranial fossa
The middle cranial fossa consists of parts of the sphenoid and temporal bones (Fig. 8.26).
The boundary between the anterior and middle cranial fossae in the midline is the anterior edge of the chiasmatic sulcus, which is a smooth groove stretching between the optic canals across the body of the sphenoid.
The posterior boundaries of the middle cranial fossa are formed by the anterior surface, as high as the superior border, of the petrous part of the petromastoid part of the temporal bone.
Sphenoid
The floor in the midline of the middle cranial fossa is elevated and formed by the body of the sphenoid. Lateral to this are large depressions formed on either side by the greater wing of the sphenoid and the squamous part of the temporal bone. These depressions contain the temporal lobes of the brain.
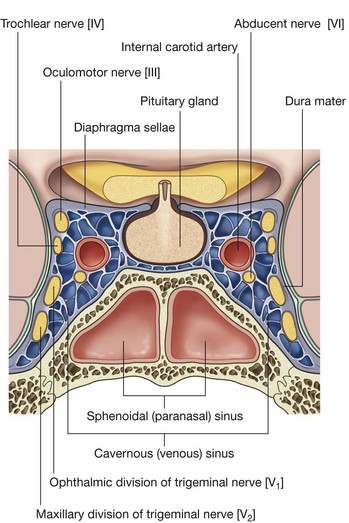
Sella turcica
Just posterior to the chiasmatic sulcus is the uniquely modified remainder of the body of the sphenoid (the sella turcica), which consists of a deep central area (the hypophysial fossa) containing the pituitary gland with anterior and posterior vertical walls of bone (Fig. 8.26).
The anterior wall of the sella is vertical in position with its superior extent visible as a slight elevation (the tuberculum sellae) at the posterior edge of the chiasmatic sulcus.
Lateral projections from the corners of the tuberculum sellae (the middle clinoid processes) are sometimes evident.
The posterior wall of the sella turcica is the dorsum sellae, a large ridge of bone projecting upward and forward. At the top of this bony ridge the lateral edges contain rounded projections (the posterior clinoid processes), which are points of attachment, like the anterior clinoid processes, for the tentorium cerebelli.
Fissures and foramina
Lateral to each side of the body of the sphenoid, the floor of the middle cranial fossa is formed on either side by the greater wing of the sphenoid (Fig. 8.26).
A diagonal gap, the superior orbital fissure, separates the greater wing of the sphenoid from the lesser wing and is a major passageway between the middle cranial fossa and the orbit. Passing through the fissure are the oculomotor nerve [III], the trochlear nerve [IV], the ophthalmic nerve [V1], the abducent nerve [VI], and ophthalmic veins.
Posterior to the medial end of the superior orbital fissure on the floor of the middle cranial fossa is a rounded foramen projecting in an anterior direction (the foramen rotundum), through which the maxillary nerve [V2] passes from the middle cranial fossa to the pteryatine fossa.
Posterolateral to the foramen rotundum is a large oval opening (the foramen ovale), which allows structures to pass between the extracranial infratemporal fossa and the middle cranial fossa. The mandibular nerve [V3], lesser petrosal nerve (carrying fibers from the tympanic plexus that originally came from the glossopharyngeal nerve [IX]) and, occasionally, a small vessel (the accessory middle meningeal artery), pass through this foramen.
Posterolateral from the foramen ovale is the small foramen spinosum (Fig. 8.26). This opening also connects the infratemporal fossa with the middle cranial fossa. The middle meningeal artery and its associated veins pass through this foramen and, once inside, the groove for the middle meningeal artery across the floor and lateral wall of the middle cranial fossa clearly marks their path.
Posteromedial to the foramen ovale is the rounded intracranial opening of the carotid canal. Directly inferior to this opening is an irregular foramen (the foramen lacerum) (Fig. 8.26). Clearly observed in the inferior view of the skull, the foramen lacerum is closed in life by a cartilaginous plug and no structures pass through it completely.
Temporal bone
The posterior boundary of the middle cranial fossa is formed by the anterior surface of the petrous part of the petromastoid part of the temporal bone.
Medially, there is a slight depression (trigeminal impression) in the anterior surface of the petrous part of the temporal bone (Fig. 8.26), which marks the location of the sensory ganglion for the trigeminal nerve [V].
Lateral to the trigeminal impression and on the anterior surface of the petrous part of the temporal bone is a small linear groove that passes in a superolateral direction, and ends in a foramen (the groove and hiatus for the greater petrosal nerve). The greater petrosal nerve is a branch of the facial nerve [VII].
Anterolateral to the groove for the greater petrosal nerve is a second, smaller groove and hiatus for the lesser petrosal nerve, a branch from the tympanic plexus carrying fibers that originally came from the glossopharyngeal nerve [IX] (Fig. 8.26).
Above and lateral to the small openings for the greater and lesser petrosal nerves, near the superior ridge of the petrous part of the temporal bone, is a rounded protrusion of bone (the arcuate eminence) produced by the underlying anterior semicircular canal of the inner ear.
Just anterior and lateral to the arcuate eminence the anterior surface of the petrous part of the temporal bone is slightly depressed. This region is the tegmen tympani, and marks the thin bony roof of the middle ear cavity.
Posterior cranial fossa
The posterior cranial fossa consists mostly of parts of the temporal and occipital bones with small contributions from the sphenoid and parietal bones (Fig. 8.27). It is the largest and deepest of the three cranial fossae and contains the brainstem (midbrain, pons, and medulla) and the cerebellum.
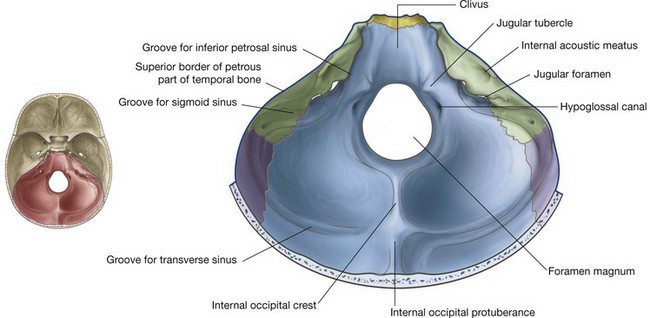
Boundaries
The anterior boundaries of the posterior cranial fossa in the midline are the dorsum sellae and the clivus (Fig. 8.27). The clivus is a slope of bone that extends upward from the foramen magnum. It is formed by contributions from the body of the sphenoid and from the basilar part of the occipital bone.
Laterally the anterior boundaries of the posterior cranial fossa are the superior border of the petrous part of the petromastoid part of the temporal bone.
Posteriorly the squamous part of the occipital bone to the level of the transverse groove is the major boundary, while laterally the petromastoid part of the temporal bone and small parts of the occipital and parietal bones border the fossa.
Foramen magnum
Centrally, in the deepest part of the posterior cranial fossa, is the largest foramen in the skull, the foramen magnum. It is surrounded by the basilar part of the occipital bone anteriorly, the lateral parts of the occipital bone on either side, and the squamous part of the occipital bone posteriorly.
The spinal cord passes superiorly through the foramen magnum to continue as the brainstem.
Also passing through the foramen magnum are the vertebral arteries, the meninges, and the spinal roots of the accessory nerve [XI].
Grooves and foramina
The clivus slopes upward from the foramen magnum. Lateral to the clivus is a groove for the inferior petrosal sinus between the basilar part of the occipital bone and the petrous part of the petromastoid part of the temporal bone (Fig. 8.27).
Laterally, across the upper half of the posterior surface of the petrous part of the temporal bone, is an oval foramen (the internal acoustic meatus). The facial [VII] and vestibulocochlear [VIII] nerves, and the labyrinthine artery pass through it.
Inferior to the internal acoustic meatus the temporal bone is separated from the occipital bone by the large jugular foramen (Fig. 8.27). Leading to this foramen from the medial side is the groove for the inferior petrosal sinus, and from the lateral side the groove for the sigmoid sinus.
The sigmoid sinus passes into the jugular foramen, and is continuous with the internal jugular vein, while the inferior petrosal sinus empties into the internal jugular vein in the area of the jugular foramen.
Also passing through the jugular foramen are the glossopharyngeal nerve [IX], the vagus nerve [X], and the accessory nerve [XI].
Medial to the jugular foramen is a large rounded mound of the occipital bone (the jugular tubercle). Just inferior to this, and superior to the foramen magnum, is the hypoglossal canal, through which the hypoglossal nerve [XII] leaves the posterior cranial fossa, and a meningeal branch of the ascending pharyngeal artery enters the posterior cranial fossa.
Just posterolateral to the hypoglossal canal is the small condylar canal that, when present, transmits an emissary vein.
Squamous part of the occipital bone
The squamous part of the occipital bone has several prominent features (Fig. 8.27):
on either side of the internal occipital crest, the floor of the posterior cranial fossa is concave to accommodate the cerebellar hemispheres; the internal occipital crest ends superiorly in a bony prominence (the internal occipital protuberance); extending laterally from the internal occipital protuberance are grooves produced by the transverse sinuses, which continue laterally, eventually joining a groove for each sigmoid sinus—each of these grooves then turns inferiorly toward the jugular foramina.The transverse and sigmoid sinuses are intradural venous sinuses.
In the clinic
Medical imaging of the head
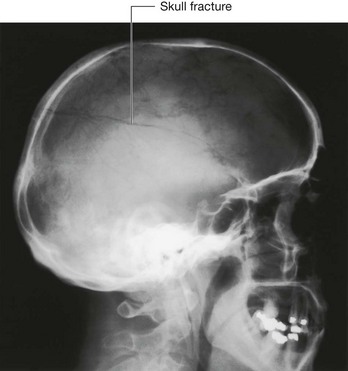
Until two decades ago the standard method of imaging the head was plain radiography. The radiographs are taken in three standard projections—namely the posteroanterior view, the lateral view, and the Towne’s view. Additional views are obtained to assess the foramina at the base of the skull and the facial bones. Currently, skull radiographs are used in cases of trauma, but such use is declining. Skull fractures are relatively easily detected (Fig. 8.28). The patient is assessed and treatment is based upon the underlying neurological or potential neurological complications.
Since the development of the first computed tomography (CT) scanner, cerebral CT has been the “workhorse” of neuroradiological examination. It is ideally used for head injury because the brain and its coverings can be easily and quickly examined and blood is easily detected. By altering the mathematical algorithm of the data set the bones can also be demonstrated.
With intravenous contrast, CT angiography can be used to demonstrate the position and the size of an intracerebral aneurysm before endovascular treatment.
Magnetic resonance imaging (MRI) is unsurpassed by other imaging techniques in its ability for contrast resolution. The brain and its coverings, cerebrospinal fluid (CSF), and the vertebral column can be easily and quickly examined. Newer imaging sequences permit CSF fluid suppression to define periventricular lesions.
Magnetic resonance angiography has been extremely useful in determining the completeness of the intracranial vasculature (circle of Willis), which is necessary in some surgical conditions.
MRI is also a powerful tool in the assessment of carotid stenosis.
Initial work using ultrasound to assess the brain appeared fruitless, but with increasing probe technology it is now possible to carry out intracranial Doppler studies, which enable a surgeon to detect whether a patient is experiencing cerebral embolization from a carotid plaque.
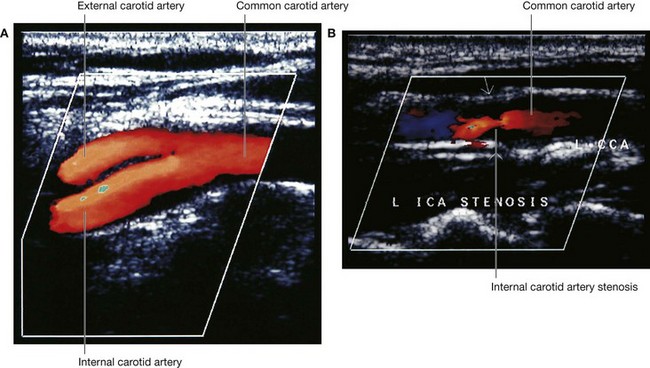
Extracranial ultrasound is extremely important in tumor staging and in assessing neck masses and the carotid bifurcation (Fig. 8.29).
Ultrasound is useful in children because they have an acoustic window through the fontanelles.
In the clinic
Fractures of the skull vault and extradural hematoma
The skull vault is a remarkably strong structure—and quite rightly, because it protects our most vital organ, the brain. The shape of the skull vault is of critical importance and its biomechanics prevent fracture. From a clinical standpoint skull fractures alert clinicians to the nature and force of an injury and potential complications. The fracture itself is usually of little consequence (unlike, say, a fracture of the tibia). Of key importance is the need to minimize the extent of primary brain injury and to treat potential secondary complications, rather than focusing on the skull fracture. Skull fractures that have particular significance include depressed skull fractures, compound fractures, and pterion fractures.
In a depressed skull fracture a bony fragment is depressed below the normal skull convexity. This may lead to secondary arterial and venous damage with hematoma formation. Furthermore, a primary brain injury can also result from this type of fracture.
In a compound fracture there is a fracture of the bone together with a breach of the skin, which may allow an infection to enter. Typically these fractures are associated with scalp lacerations and can usually be treated with antibiotics.
Important complications of compound fractures include meningitis, which may be fatal.
A more subtle type of compound fracture involves fractures across the sinuses. These may not be appreciated on first inspection, but are an important potential cause of morbidity and should be considered in patients who develop intracranial infections secondary to trauma.
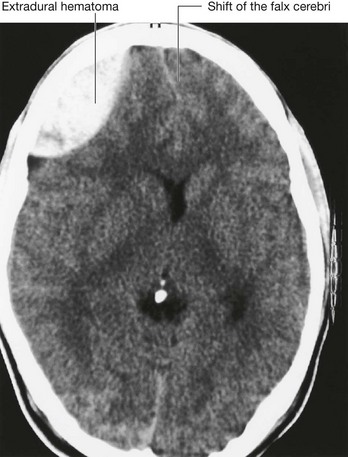
The pterion is an important clinical point on the lateral aspect of the skull. To find the precise point of the pterion, an imaginary line 1 inch (2.5 cm) above the zygomatic arch, and 1 inch (2.5 cm) posterior to the lateral orbital margin will approximate to this region. At the pterion the frontal, parietal, greater wing of the sphenoid, and temporal bones come together. Importantly, deep to this structure is the middle meningeal artery. An injury to this point of the skull is extremely serious because damage to this vessel may produce a significant extradural hematoma, which can be fatal.
MENINGES
The brain, as well as the spinal cord, is surrounded by three layers of membranes (the meninges, Fig. 8.30A)—a tough, outer layer (the dura mater), a delicate, middle layer (the arachnoid mater), and an inner layer firmly attached to the surface of the brain (the pia mater).
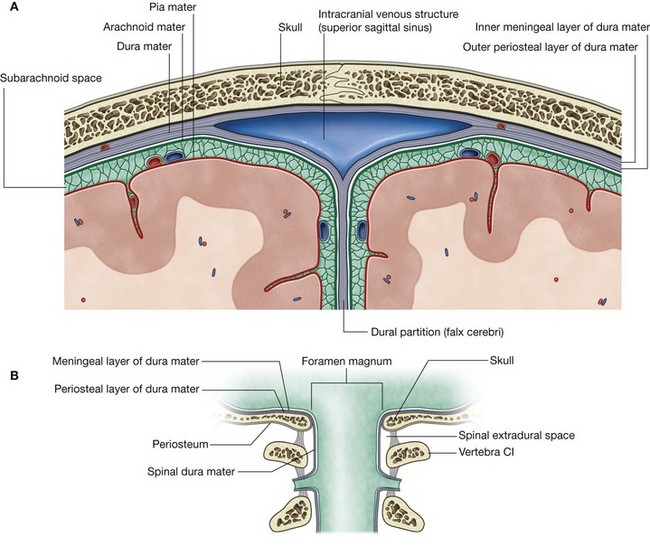
The cranial meninges are continuous with, and similar to, the spinal meninges through the foramen magnum, with one important distinction—the cranial dura mater consists of two layers, and only one of these is continuous through the foramen magnum (Fig. 8.30B).
Cranial dura mater
The cranial dura mater is a thick, tough, outer covering of the brain. It consists of an outer periosteal layer and an inner meningeal layer (Fig. 8.30A):
the outer periosteal layer is firmly attached to the skull, is the periosteum of the cranial cavity, contains the meningeal arteries, and is continuous with the periosteum on the outer surface of the skull at the foramen magnum and other intracranial foramina (Fig. 8.30B); the inner meningeal layer is in close contact with the arachnoid mater and is continuous with the spinal dura mater through the foramen magnum.The two layers of dura separate from each other at numerous locations to form two unique types of structures (Fig. 8.30A):
Dural partitions
The dural partitions project into the cranial cavity and partially subdivide the cranial cavity. They include the falx cerebri, tentorium cerebelli, falx cerebelli, and the diaphragma sellae.
Falx cerebri
The falx cerebri (Fig. 8.31) is a crescent-shaped downward projection of meningeal dura mater from the dura lining the calva that passes between the two cerebral hemispheres. It is attached anteriorly to the crista galli of the ethmoid bone and frontal crest of the frontal bone. Posteriorly it is attached to and blends with the tentorium cerebelli.
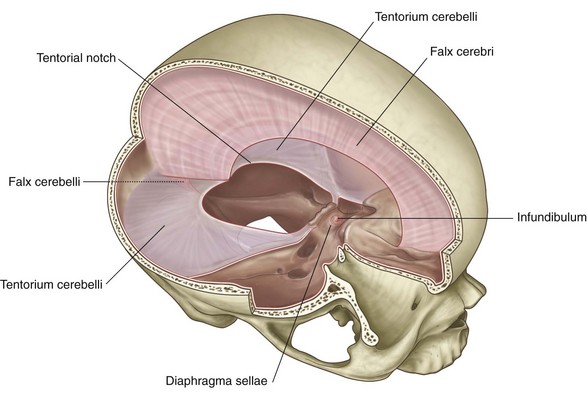
Tentorium cerebelli
The tentorium cerebelli (Fig. 8.31) is a horizontal projection of the meningeal dura mater that covers and separates the cerebellum in the posterior cranial fossa from the posterior parts of the cerebral hemispheres. It is attached posteriorly to the occipital bone along the grooves for the transverse sinuses. Laterally, it is attached to the superior border of the petrous part of the temporal bone, ending anteriorly at the anterior and posterior clinoid processes.
The anterior and medial borders of the tentorium cerebelli are free, forming an oval opening in the midline (the tentorial notch), through which the midbrain passes.
Falx cerebelli
The falx cerebelli (Fig. 8.31) is a small midline projection of meningeal dura mater in the posterior cranial fossa. It is attached posteriorly to the internal occipital crest of the occipital bone and superiorly to the tentorium cerebelli. Its anterior edge is free and is between the two cerebellar hemispheres.
Diaphragma sellae
The final dural projection is the diaphragma sellae (Fig. 8.31). This small horizontal shelf of meningeal dura mater covers the hypophysial fossa in the sella turcica of the sphenoid bone. There is an opening in the center of the diaphragma sellae through which passes the infundibulum, connecting the pituitary gland with the base of the brain, and any accompanying blood vessels.
Arterial supply
The arterial supply to the dura mater (Fig. 8.32) travels in the outer periosteal layer of the dura and consists of:
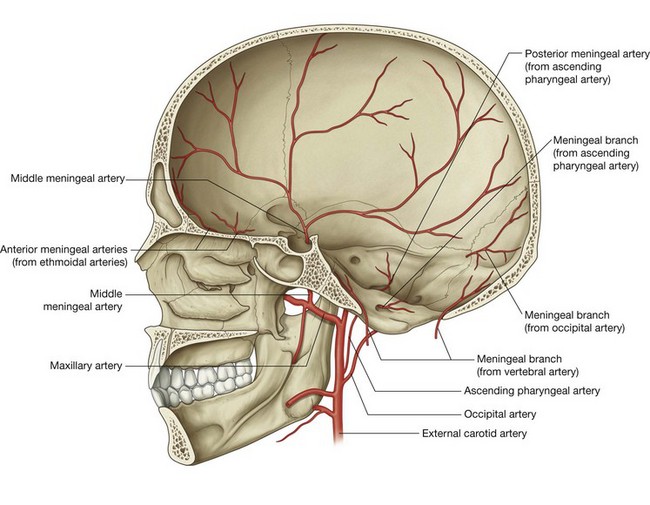
All are small arteries except for the middle meningeal artery, which is much larger and supplies the greatest part of the dura.
The anterior meningeal arteries are branches of the ethmoidal arteries.
The middle meningeal artery is a branch of the maxillary artery. It enters the middle cranial fossa through the foramen spinosum and divides into anterior and posterior branches:
the anterior branch passes in an almost vertical direction to reach the vertex of the skull, crossing the pterion during its course; the posterior branch passes in a posterosuperior direction, supplying this region of the middle cranial fossa.The accessory meningeal artery is usually a small branch of the maxillary artery that enters the middle cranial fossa through the foramen ovale and supplies areas medial to this foramen.
The posterior meningeal artery and other meningeal branches supplying the dura mater in the posterior cranial fossa come from several sources (Fig. 8.32):
the posterior meningeal artery, the terminal branch of the ascending pharyngeal artery, enters the posterior cranial fossa through the jugular foramen; a meningeal branch from the ascending pharyngeal artery enters the posterior cranial fossa through the hypoglossal canal;Innervation
Innervation of the dura mater (Fig. 8.33) is by small meningeal branches of all three divisions of the trigeminal nerve [V1, V2, and V3], the vagus nerve [X], and the first, second, and sometimes, third cervical nerves. (Possible involvement of the glossopharyngeal [IX] and hypoglossal nerves [XII] in the posterior cranial fossa has also been reported.)
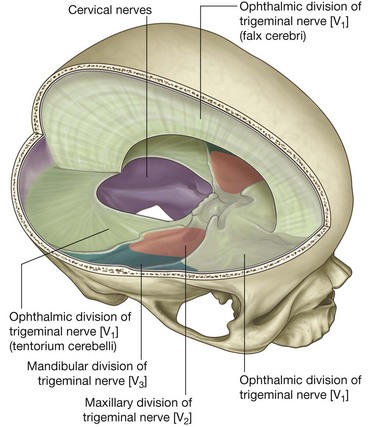
In the anterior cranial fossa meningeal branches from the ethmoidal nerves, which are branches of the ophthalmic nerve [V1], supply the floor and the anterior part of the falx cerebri.
Additionally, a meningeal branch of the ophthalmic nerve [V1] turns and runs posteriorly, supplying the tentorium cerebelli and the posterior part of the falx cerebri.
The middle cranial fossa is supplied medially by meningeal branches from the maxillary nerve [V2] and laterally, along the distribution of the middle meningeal artery, by meningeal branches from the mandibular nerve [V3].
The posterior cranial fossa is supplied by meningeal branches from the first, second, and sometimes, the third cervical nerves, which enter the fossa through the foramen magnum, the hypoglossal canal, and the jugular foramen. Meningeal branches of the vagus nerve [X] have also been described. (Possible contributions from the glossopharyngeal [IX] and hypoglossal [XII] nerves have also been reported.)
Arachnoid mater
The arachnoid mater is a thin, avascular membrane that lines, but is not adherent to, the inner surface of the dura mater (Fig. 8.34). From its inner surface thin processes or trabeculae extend downward, cross the subarachnoid space, and become continuous with the pia mater.
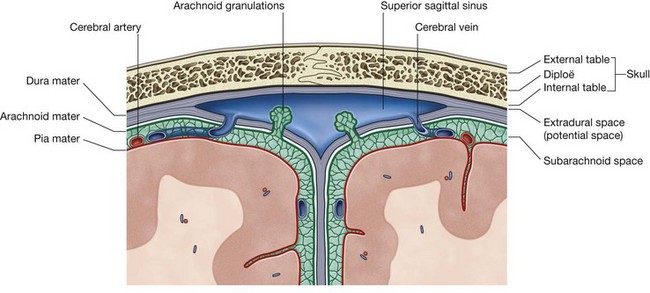
Unlike the pia, the arachnoid does not enter the grooves or fissures of the brain, except for the longitudinal fissure between the two cerebral hemispheres.
Pia mater
The pia mater is a thin, delicate membrane that closely invests the surface of the brain (Fig. 8.34). It follows the contours of the brain, entering the grooves and fissures on its surface, and is closely applied to the roots of the cranial nerves at their origins.
Arrangement of meninges and spaces
There is a unique arrangement of meninges, coupled with real and potential spaces within the cranial cavity (Fig. 8.34).
A potential space is related to the dura mater, while a real space exists between the arachnoid mater and the pia mater.
Extradural space
The potential space between dura mater and bone is the extradural space. Normally, the outer or periosteal layer of dura mater is firmly attached to the bones surrounding the cranial cavity.
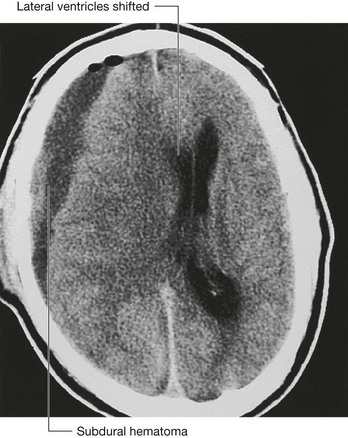
This potential space between dura and bone can become a fluid-filled actual space when a traumatic event results in a vascular hemorrhage. Bleeding into the extradural space due to rupture of a meningeal artery or a torn dural venous sinus results in an extradural hematoma. Bleeding due to the tearing of a vein as it enters a dural venous sinus can result in a subdural hematoma.
Subarachnoid space
Deep to the arachnoid mater is the only normally occurring fluid-filled space associated with the meninges. It occurs because the arachnoid mater clings to the inner surface of the dura mater and does not follow the contour of the brain, while the pia mater, being against the surface of the brain, closely follows the grooves and fissures on the surface of the brain. A narrow space (the subarachnoid space) is therefore created between these two membranes (Fig. 8.34).
The subarachnoid space surrounds the brain and spinal cord and in certain locations it enlarges into expanded areas (subarachnoid cisterns). It contains cerebrospinal fluid (CSF) and blood vessels.
Cerebrospinal fluid is produced by the choroid plexus, primarily in the ventricles of the brain. It is a clear, colorless, cell-free fluid that circulates through the subarachnoid space surrounding the brain and spinal cord.
The CSF returns to the venous system through arachnoid villi. These project as clumps (arachnoid granulations) into the superior sagittal sinus, which is a dural venous sinus, and its lateral extensions, the lateral lacunae.
In the clinic
Hydrocephalus
Hydrocephalus is a dilatation of the cerebral ventricular system, which is due to either an obstruction to the flow of CSF, overproduction of CSF, or a failure of reabsorption of CSF.
Cerebrospinal fluid is secreted by the epithelial cells of the choroid plexus within the lateral, third, and fourth ventricles of the brain. As it is produced it passes from the lateral ventricles through the interventricular foramina (the foramina of Monro) to enter the third ventricle. From the third ventricle it passes through the cerebral aqueduct (aqueduct of Sylvius) into the fourth ventricle, and from here it passes into the subarachnoid space via the midline foramen or the two lateral foramina (foramen of Magendie and foramina of Luschka).
The CSF passes around the spinal cord inferiorly, envelops the brain superiorly, and is absorbed through the arachnoid granulations in the walls of the dural venous sinuses. In adults almost half a liter of CSF is produced a day.
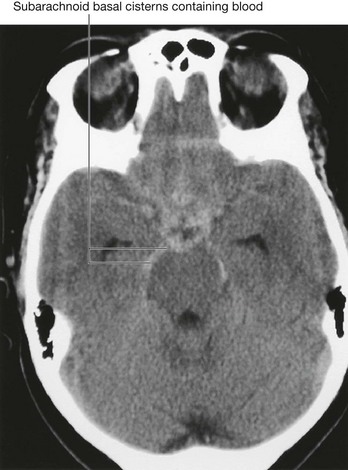
In adults the commonest cause of hydrocephalus is an interruption of the normal CSF absorption through the arachnoid granulations. This occurs when blood enters the subarachnoid space after subarachnoid hemorrhage, passes over the brain, and interferes with normal CSF absorption. To prevent severe hydrocephalus it may be necessary to place a small catheter through the brain into the ventricular system to relieve the pressure.
Other causes of hydrocephalus include congenital obstruction of the aqueduct of Sylvius and a variety of tumors (e.g., a midbrain tumor), where the mass obstructs the aqueduct. Rare causes include choroid plexus tumors that secrete CSF.
In children, hydrocephalus is always dramatic in its later stages. The hydrocephalus increases the size and dimensions of the ventricle, and as a result the brain enlarges. Because the skull sutures are not fused, the head expands. Cranial enlargement in utero may make a vaginal delivery impossible, and delivery then has to be by caesarean section.
Both CT and MRI enable a radiologist to determine the site of obstruction, and in most cases the cause of the obstruction. A distinction must be made between ventricular enlargement due to hydrocephalus and that due to a variety of other causes (e.g., cerebral atrophy).
In the clinic
Meningitis
Meningitis is a rare infection of the leptomeninges (the leptomeninges are a combination of the arachnoid mater and the pia mater). Infection of the meninges typically occurs via a bloodborne route, though in some cases it may be by direct spread (e.g., trauma) or from the nasal cavities through the cribriform plate in the ethmoid bone.
Certain types of bacterial inflammation of the meninges are so virulent that overwhelming inflammation and sepsis with cerebral irritation can cause the patient to rapidly pass into a coma and die.
Meningitis is usually treatable with simple antibiotics.
Certain types of bacteria that produce meningitis produce other effects; for example, subcutaneous hemorrhage (ecchymoses) is a feature of meningococcal meningitis.
The typical history of meningitis is nonspecific at first. The patient may have mild headache, fever, drowsiness, and nausea. As the infection progresses, photophobia (light intolerance) and ecchymosis may ensue. Straight leg raising causes marked neck pain and discomfort (Kernig’s sign) and an emergency hospital admission is warranted.
Immediate treatment consists of very-high-dose intravenous antibiotics and supportive management.
In the clinic
Brain tumors
Determination of the anatomical structure from which a tumor arises is of the utmost importance, no more so than when it arises within the cranial vault. Misinterpretation of the location of a lesion and its site of origin may have devastating consequences for the patient.
When assessing any lesion in the brain, it is important to define whether it is intra-axial (within the brain) or extra-axial (outside the brain).
Typical extra-axial tumors include meningiomas (tumors of the meninges) and acoustic neuromas. Meningiomas typically arise from the meninges with preferred sites including regions at and around the falx cerebri, the free edge of the tentorium cerebelli, and the anterior margin of the middle cranial fossa. Acoustic neuromas are typically at and around the vestibulocochlear nerve [VIII] and in the cerebellopontine angle.
Intra-axial lesions are either primary or secondary. By far the commonest type are the secondary brain lesions, which in most cases are metastatic tumor deposits, though metastatic infection also accounts for a number of these.
Metastatic tumor lesions are typically found in patients with either breast carcinoma or lung carcinoma, though many other malignancies can give rise to cerebral metastases.
Primary brain lesions are rare and range from benign tumors to extremely aggressive lesions with a poor prognosis. These tumors arise from the different cell lines and include gliomas, oligodendrocytomas, and choroid plexus tumors. Primary brain tumors may occur at any age, though there is a small peak incidence in the first few years of life followed by a later peak in early to middle age.
BRAIN AND ITS BLOOD SUPPLY
Brain
The brain is a component of the central nervous system.
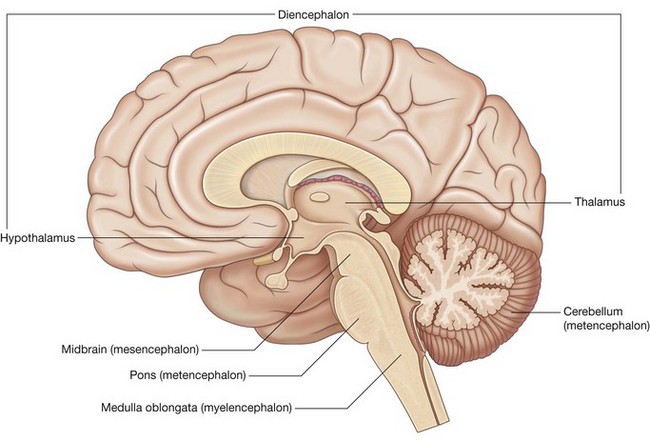
During development the brain can be divided into five continuous parts (Figs. 8.35 and 8.36). From rostral (or cranial) to caudal they are:
the telencephalon (cerebrum), which becomes the large cerebral hemispheres, the surface of which consists of elevations (gyri) and depressions (sulci) and is partially separated by a deep longitudinal fissure, and which fill the area of the skull above the tentorium cerebelli and are subdivided into lobes based on their position. the diencephalon, which is hidden from view in the adult brain by the cerebral hemispheres, consists of the thalamus, hypothalamus, and other related structures, and classically is considered to be the most rostral part of the brainstem. (However, in common usage today, the term brainstem usually refers to the midbrain, pons, and medulla); the mesencephalon (midbrain), which is the first part of the brainstem seen when an intact adult brain is examined, and is at the junction between and in both the middle and posterior cranial fossae; the metencephalon, which gives rise to the cerebellum (consisting of two lateral hemispheres and a midline part in the posterior cranial fossa below the tentorium cerebelli) and the pons (anterior to the cerebellum, a bulging part of the brainstem in the most anterior part of the posterior cranial fossa against the clivus and dorsum sellae); and
Blood supply
The brain receives its arterial supply from two pairs of vessels, the vertebral and internal carotid arteries (Fig. 8.37), which are interconnected in the cranial cavity to produce a cerebral arterial circle (of Willis).
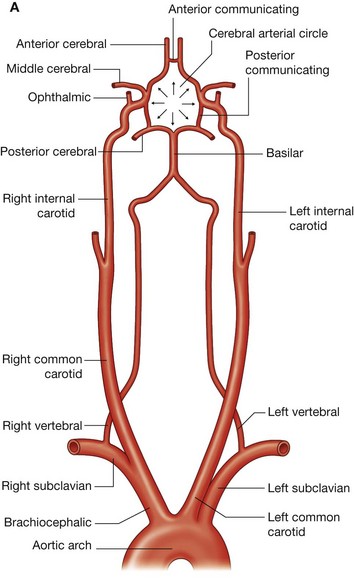
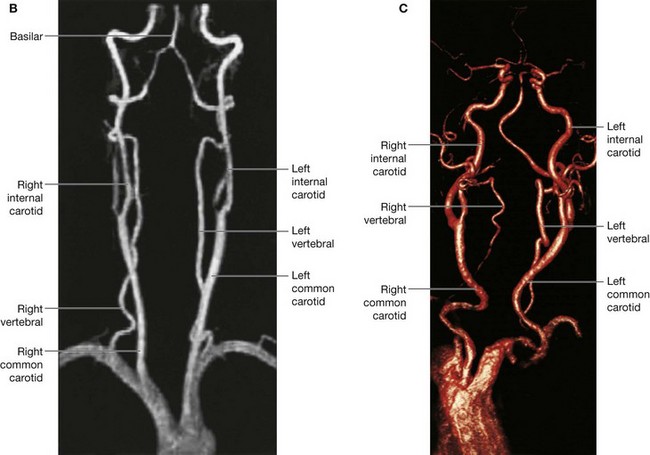
Fig. 8.37 Arterial supply to the brain. A. Diagram.
Arterial supply to the brain. B. Magnetic resonance angiogram showing normal carotid and vertebral arteries. C. Enhanced CT scan of carotid vessels.
The two vertebral arteries enter the cranial cavity through the foramen magnum and just inferior to the pons fuse to form the basilar artery.
The two internal carotid arteries enter the cranial cavity through the carotid canals on either side.
Vertebral arteries
Each vertebral artery arises from the first part of each subclavian artery in the lower part of the neck, and passes superiorly through the transverse foramina of the upper six cervical vertebrae. On entering the cranial cavity through the foramen magnum each vertebral artery gives off a small meningeal branch.
Continuing forward, the vertebral artery gives rise to three additional branches before joining with its companion vessel to form the basilar artery (Fig. 8.38):
one branch joins with its companion from the other side to form the single anterior spinal artery, which then descends in the anterior median fissure of the spinal cord; a second branch is the posterior spinal artery, which passes posteriorly around the medulla then descends on the posterior surface of the spinal cord in the area of the attachment of the posterior roots—there are two posterior spinal arteries, one on each side (although the posterior spinal arteries can originate directly from the vertebral arteries, they more commonly branch from the posterior inferior cerebellar arteries);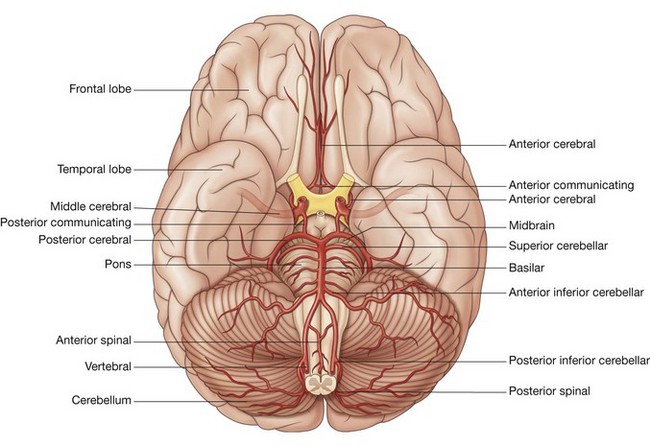
The basilar artery travels in a rostral direction along the anterior aspect of the pons (Fig. 8.38). Its branches in a caudal to rostral direction include the anterior inferior cerebellar arteries, several small pontine arteries, and the superior cerebellar arteries. The basilar artery ends as a bifurcation, giving rise to two posterior cerebral arteries.
Internal carotid arteries
The two internal carotid arteries arise as one of the two terminal branches of the common carotid arteries (Fig. 8.37). They proceed superiorly to the base of the skull where they enter the carotid canal.
Entering the cranial cavity each internal carotid artery gives off the ophthalmic artery, the posterior communicating artery, the middle cerebral artery, and the anterior cerebral artery (Fig. 8.38).
Cerebral arterial circle
The cerebral arterial circle (of Willis) is formed at the base of the brain by the interconnecting vertebrobasilar and internal carotid systems of vessels (Fig. 8.37). This anastomotic interconnection is accomplished by:
an anterior communicating artery connecting the left and right anterior cerebral arteries to each other; two posterior communicating arteries, one on each side, connecting the internal carotid artery with the posterior cerebral artery (Figs. 8.37 and 8.38).In the clinic
Stroke
A stroke is the acute development of a focal neurological deficit as a result of localized or diffuse cerebral hypoperfusion.
The causes of stroke include cerebral thrombosis, cerebral hemorrhage, subarachnoid hemorrhage, and, most commonly, cerebral embolus. In the case of most strokes, small vessel cerebrovascular obstruction is caused by emboli from an atherosclerotic plaque within more proximal vessels in the neck and thorax.
In most patients an atherosclerotic plaque is demonstrated at or around the bifurcation of the common carotid artery into internal and external carotid arteries. Over time the carotid plaque increases in size and eventually produces a marked stenosis. As the stenosis increases, local eddy currents provide the abnormal flow from which platelet and atherosclerotic emboli develop, pass into an intracranial vessel, and obstruct flow. Within five minutes the tissue in the region of the obstruction is dead (cerebral infarction; Fig. 8.39).

Less severe strokes—transient ischemic attacks (TIAs)—are caused in the same way as strokes, but recovery is usually complete within 24 hours. They serve as a warning that treatment may be necessary.
Intervention to prevent further strokes initially comprises a general alteration in lifestyle, control of hypertension (if present), and drug treatment to inhibit platelet aggregation (e.g., aspirin), to decrease the chance of clots forming and embolizing into the cerebral circulation.
In patients with severe stenoses surgery is indicated to remove the clot and atherosclerotic plaque at the carotid bifurcation and to reconstruct this region.
In the clinic
Intracerebral aneurysms
Cerebral aneurysms arise from the vessels in and around the cerebral arterial circle (of Willis). They typically occur in and around the anterior communicating artery, the posterior communicating artery, the branches of the middle cerebral artery, the distal end of the basilar artery (Fig. 8.40), and the posterior inferior cerebellar artery.
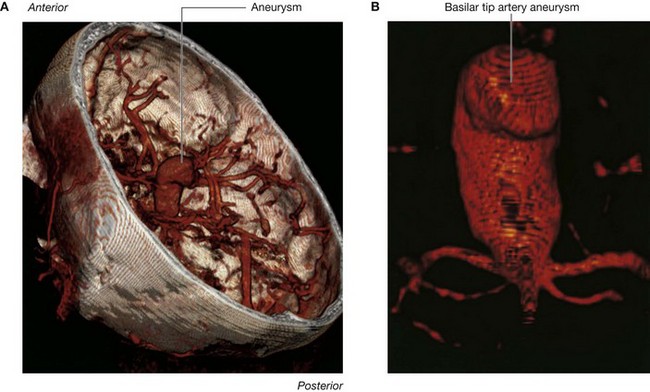
Fig. 8.40 Basilar tip aneurysm. A. Three-dimensional cranial cutaway CT scan. B. Magnified view of aneurysm.
As the aneurysms enlarge, they have a significant risk of rupture. Typically patients have no idea that there is anything wrong. No prodromal signs or symptoms are demonstrable. As the aneurysm ruptures, the patient complains of a sudden-onset “thunderclap” headache that produces neck stiffness and may induce vomiting. In a number of patients death ensues, but many patients reach the hospital, where the diagnosis is established. An initial CT scan demonstrates blood within the subarachnoid space, and this may be associated with an intracerebral bleed. Further management usually includes cerebral angiography, which enables the radiologist to determine the site, size, and origin of the aneurysm.
Usually patients undergo complex surgery to ligate the neck of the aneurysm. More recently radiological intervention has superseded the management of some aneurysms in specific sites. This treatment involves cannulation of the femoral artery, and placement of a long catheter through the aorta into the carotid circulation and thence into the cerebral circulation. The tip of the catheter is placed within the aneurysm and is packed with fine microcoils (Fig. 8.41), which seals the rupture.
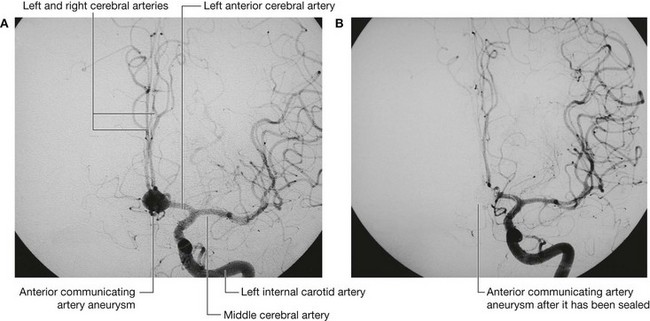
Venous drainage
Venous drainage of the brain begins internally as networks of small venous channels lead to larger cerebral veins, cerebellar veins, and veins draining the brainstem, which eventually empty into dural venous sinuses. The dural venous sinuses are endothelial-lined spaces between the outer periosteal and the inner meningeal layers of the dura mater, and eventually lead to the internal jugular veins.
Also emptying into the dural venous sinuses are diploic veins, which run between the internal and external tables of compact bone in the roof of the cranial cavity, and emissary veins, which pass from outside the cranial cavity to the dural venous sinuses (Fig. 8.42).
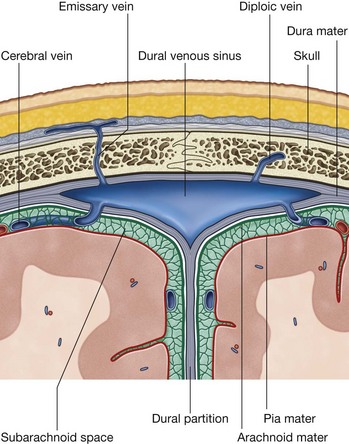
The emissary veins are important clinically because they can be a conduit through which infections can enter the cranial cavity because they have no valves.
Dural venous sinuses
The dural venous sinuses include the superior sagittal, inferior sagittal, straight, transverse, sigmoid, and occipital sinuses, the confluence of sinuses, and the cavernous, sphenoparietal, superior petrosal, inferior petrosal, and basilar sinuses (Fig. 8.43, Table 8.3).
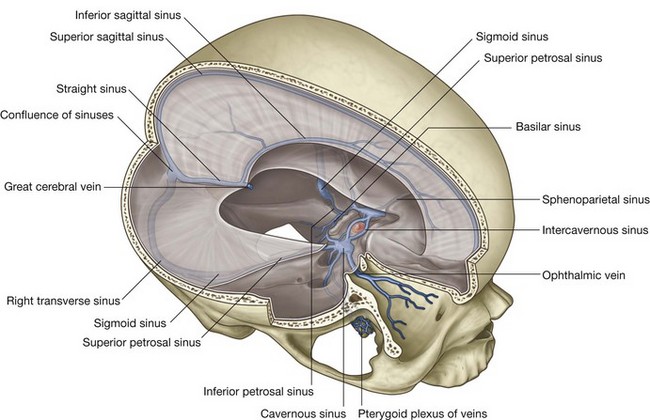
Table 8.3 Dural venous sinuses
| Dural sinus | Location | Receives |
|---|---|---|
| Superior sagittal | Superior border of falx cerebri | Superior cerebral, diploic, and emissary veins and CSF |
| Inferior sagittal | Inferior margin of falx cerebri | A few cerebral veins and veins from the falx cerebri |
| Straight | Junction of falx cerebri and tentorium cerebelli | Inferior sagittal sinus, great cerebral vein, posterior cerebral veins, superior cerebellar veins, and veins from the falx cerebri |
| Occipital | In falx cerebelli against occipital bone | Communicates inferiorly with vertebral plexus of veins |
| Confluence of sinuses | Dilated space at the internal occipital protuberance | Superior sagittal, straight, and occipital sinuses |
| Transverse (right and left) | Horizontal extensions from the confluence of sinuses along the posterior and lateral attachments of the tentorium cerebelli | Drainage from confluence of sinuses (right—transverse and usually superior sagittal sinuses; left—transverse and usually straight sinuses); also superior petrosal sinus, and inferior cerebral, cerebellar, diploic, and emissary veins |
| Sigmoid (right and left) | Continuation of transverse sinuses to internal jugular vein; groove of parietal, temporal, and occipital bones | Transverse sinuses, and cerebral, cerebellar, diploic, and emissary veins |
| Cavernous (paired) | Lateral aspect of body of sphenoid | Cerebral and ophthalmic veins, sphenoparietal sinuses, and emissary veins from pterygoid plexus of veins |
| Intercavernous | Crossing sella turcica | Interconnect cavernous sinuses |
| Sphenoparietal (paired) | Inferior surface of lesser wings of sphenoid | Diploic and meningeal veins |
| Superior petrosal (paired) | Superior margin of petrous part of temporal bone | Cavernous sinus, and cerebral and cerebellar veins |
| Inferior petrosal (paired) | Groove between petrous part of temporal bone and occipital bone ending in internal jugular vein | Cavernous sinus, cerebellar veins, and veins from the internal ear and brainstem |
| Basilar | Clivus, just posterior to sella turcica of sphenoid | Connect bilateral inferior petrosal sinuses and communicate with vertebral plexus of veins |