The Child’s Experience of Hospitalization
1 Define each key term listed.
2 Identify various health care delivery settings.
3 Describe three phases of separation anxiety.
4 List two ways in which the nurse can lessen the stress of hospitalization for the child’s parents.
5 Discuss the management of pain in infants and children.
6 Describe two milestones in the psychosocial development of the preschool child that contribute either positively or negatively to the adjustment to hospitalization.
7 Contrast the problems of the preschool child and the school-age child facing hospitalization.
8 Identify two problems confronting the siblings of the hospitalized child.
9 List three strengths of the adolescent that the nurse might use when formulating nursing care plans.
10 Organize a nursing care plan for a hospitalized child.
11 Recognize the steps in discharge planning for infants, children, and adolescents.
 , p. 484)
, p. 484) , p. 484)
, p. 484) , p. 477)
, p. 477) , p. 475)
, p. 475) , p. 485)
, p. 485) , p. 472)
, p. 472) , p. 481)
, p. 481) http://evolve.elsevier.com/Leifer
http://evolve.elsevier.com/Leifer
Health Care Delivery Settings
Many hospitals today have well-organized outpatient facilities and satellite clinics for preventive medicine and care of the child who is ill. The advent of Medicaid and other such programs has made these services available to low-income families. Within clinics, there may be specialty areas (particularly at children’s facilities) such as well-child clinics, asthma clinics, cardiac clinics, and orthopedic clinics. In some institutions, information is distributed and brief classes are held for waiting parents.
In many private medical offices the pediatricians or their nurses are available at certain hours of each day to answer telephone inquiries. The pediatric nurse practitioner may visit patients in the home, give routine physical examinations at the clinic, and otherwise work with the physician so that a higher quality of individual care may be attained. The nurse practitioner is often the primary contact person for children in the health care system.
Types of Outpatient Clinics
Satellite clinics are convenient and offer families flexible coverage. Some are located in shopping malls. Parents may walk with children and be contacted by a beeper when it is their turn to see the health care provider. This eliminates confining children in a small area and is less frustrating to caregivers. In many cities, a group of pediatricians practice in an office removed from the hospital, which aids in the distribution of health services and provides evening and weekend health coverage.
Another area of outpatient care is the pediatric research center, such as the one at St. Jude’s Hospital in Memphis, Tennessee. This type of institution offers highly specialized care for patients with particular disorders, often at little or no expense to the patient. In the outpatient clinic, as in all other settings, documentation and record review are important parts of data collection.
For patients with uncomplicated conditions, elective surgery at an outpatient surgery clinic offers the advantage of lower cost, reduced incidence of health care–associated infection, and recuperation at home in familiar surroundings (e.g., herniorrhaphy or tonsillectomy). These outpatient clinics eliminate the need to separate the child from the family and reduce the extent of treatment and the emotional impact of the illness. Careful preparation must be given, and assurance must be obtained that the child’s home environment is adequate to meet recovery needs.
Promoting a Positive Experience
The attitude of nurses, receptionists, and other personnel in the clinic, office, or hospital unit is of the utmost importance. It can make the difference between an atmosphere that is warm and friendly and one in which the child is made to feel dehumanized. As more and more medical care is offered in outpatient clinics, there will be an even greater reduction in the number of children who require hospitalization. For many, the only exposure to medical personnel is through brief clinic appointments. Therefore it is very important that these encounters are positive ones for children and their families.
Preparing the Child for a Treatment or Procedure: Whenever possible the parent should be involved in the preparation for and initiation of a treatment or procedure, and the child should be prepared according to his or her developmental level (Box 21-1). For example, for infants, have a familiar object stay with the infant, restrain as needed, and cuddle and hug the infant following the procedure. For a toddler, model the behavior desired (i.e., opening the mouth), tell the child it is okay to yell if the treatment or procedure is uncomfortable, and use distractions. For a preschooler, explain the treatment or procedure in simple terms, allow the child to handle some of the equipment, and keep other equipment out of sight. For a school-age child, explain in advance what the treatment or procedure is and the reason it is needed, and allow the child responsibility for simple tasks, such as applying tape. For adolescents, explain the treatment or procedure in more detail, and encourage questioning. Involve them in decision making and planning, such as who should be in the room. Proper preparation decreases anxiety, increases cooperation, and assists the child in coping with the experience.
Home
Because hospitalization is now brief for most children, the choice is not either hospital or home care but a combination of the two. They are becoming interdependent. Dramatic technical improvements and research in specific disease entities are also helping to advance the movement to home care (e.g., cryoprecipitate for hemophiliacs, Broviac catheters for chemotherapy, heparin locks for intravenous access, glucometers for monitoring blood glucose). However, home care is broader than in years past. It is not merely a matter of supplying appliances and nursing care, but it also includes assessment of the total needs of children and their families. Families need to be linked to a wide variety of network services. This ideally involves a multidisciplinary approach spearheaded by the health care provider.
The hospice concept for children has received accolades from parents who have benefited from its service. Local and national support groups for specific problems afford opportunities for families to share and support one another and to learn from others’ successes and failures. Special groups and camps for children with chronic illnesses are also well established. Group therapy for children under stress is equally important in preventing mental health problems (e.g., groups for children whose parents are divorced, Alateen for children of alcoholics). These and other programs not only have the potential for improving life for the child and family but also may help to reduce the high cost of medical care. There have been dramatic changes in the delivery of health care to children and families. These changes affect the role and responsibilities of the nurse working both in wellness centers providing preventive care and in hospitals or homes treating illness.
Children’s Hospital Unit
The children’s hospital unit differs in many respects from adult divisions. The pediatric unit or hospital is designed to meet the needs of children and their parents. A cheerful, casual atmosphere helps to bridge the gap between home and hospital and is in keeping with the child’s emotional, developmental, and physical needs. Nurses wear colorful uniforms, and colored bedspreads and wagons or strollers for transportation provides a more homelike atmosphere.
The physical structure of the unit includes furniture of the proper height for the child, soundproof ceilings, and color schemes with eye appeal. There is a special treatment room for the health care provider to examine or treat the child. In this way the other children do not become disturbed by the proceedings. Some hospitals have a schoolroom. When this is not available, it is necessary for the home-school teacher to visit each school-age child individually. Today’s modern general hospitals have separate waiting rooms for children. This is more relaxing for parents, because they do not need to worry about whether their child is disturbing adult patients, and it is less frightening to the child.
Most pediatric departments include a playroom. It is generally large and light in color. Bulletin boards and whiteboards are within reach of the patients. Mobiles may be suspended from the ceiling. Some playrooms are equipped with an aquarium of fish because children love living things. Various toys suitable for different age-groups are available. This room may be under the supervision of a child life specialist or a play therapist. Parents usually enjoy taking their children to the playroom and observing the various activities. The playroom is considered an “ouch-free” area, or a safe haven from painful treatments.
When the child is not able to be taken to the playroom because of the diagnosis or physical condition, bedside play activities appropriate to the developmental level and diagnosis of the child should be provided. The daily routine of the pediatric unit emphasizes parent rooming-in, the provision of consistent caregivers, and flexible schedules designed to meet the needs of growing children.
The Child’s Reaction to Hospitalization
The child’s reaction to hospitalization depends on many factors such as age, amount of preparation given, security of home life, previous hospitalizations, support of family and medical personnel, and child’s emotional health. Many children cannot grasp what is going to happen to them even though they have been well prepared. At a time when children need their parents most, they may be separated from them, placed in the hands of strangers, and even fed different foods. Add to this a totally new environment and physical discomfort, and the result is one frightened and unhappy child.
Each child reacts differently to hospitalization. One may be demanding and exhibit temper tantrums, whereas another may become withdrawn. The “good” child on the unit may be going through greater torment than the one who cries and shows feelings outwardly. The best-prepared nurse cannot replace the child’s parents. However, hospitalization can be a period of growth rather than just an unpleasant interlude. Children may see the nurse as someone who cares for them physically, as their parents would, and as a source of security and comfort (Figure 21-1).

FIGURE 21-1 The nurse greets the child at eye level in a nonthreatening manner. This child views the nurse as a person who cares for her physically and is a source of security and comfort. (Courtesy Pat Spier, RN-C.)
The major causes of stress for children of all ages are separation, pain, and fear of body intrusion. This is influenced by the child’s developmental age, the maturity of the parents, cultural and economic factors, religious background, past experiences, family size, state of health on admission, and other factors.
 Nursing Tip
Nursing Tip
Familiar rituals and routines must be incorporated into the plan of care for a hospitalized child.
Separation Anxiety
Separation anxiety occurs in infants age 6 months and older and is most pronounced at the toddler age. There are three stages of separation anxiety: protest, despair, and denial or detachment. Unless infants are extremely ill, their sense of abandonment is expressed by a loud protest. Toddlers may watch and listen for their parents. Their cry is continuous until they fall asleep in exhaustion. Toddlers may call out, “Mommy,” repeatedly, and the approach of a stranger only causes increased screaming. The crying gradually stops, and the second stage of despair sets in. Children appear sad and depressed. They move about less and withdraw from strangers who approach. They do not play actively with toys. In the third stage, denial or detachment, children appear to deny their need for the parent and become detached or disinterested in their visits. They become more interested in their surroundings, their toys, and their playmates. On the surface, it appears the child has adjusted to the separation. However, it is important for the nurse to understand that the child is using a coping mechanism to detach and reduce the emotional pain.
If the detachment stage is prolonged, an irreversible disruption of parent-infant bonding may occur. Health care workers who do not understand the stages of separation anxiety may label the crying, protesting child as “bad,” the withdrawn depressed child in despair as “adjusting,” and the child who is in the detachment phase as a “well-adjusted” child. This misinterpretation can prevent health care workers from providing desperately needed assistance and guidance to the child and family.
The nurse must understand that the child who is in despair reverts back to the protest stage when the parent arrives for a visit. Rather than showing joy, the child cries loudly when the parent appears at the door. This is good! The child who has reached the detached phase appears unmoved and uninterested in the parent’s arrival. Nursing interventions are needed in this case to preserve and heal parent-child relationships. Optimally the nurse helps the parents to understand they should not deceive the child into believing they will stay and then “sneak out” while the child is distracted. This can tear the bond of trust.
Pain
The accepted definition of pain is that “pain is whatever the experiencing person says it is, existing whenever the experiencing person says it does” (American Academy of Pediatrics [AAP], 2001). This includes verbal and nonverbal expressions of pain. Freedom from pain is a basic need and right of the infant and child. To increase awareness of pain during patient assessment, pain has come to be considered a “fifth vital sign.” An assessment for pain is recorded with routine vital sign documentation.
The negative physical and psychological consequences of pain are well documented. Patients in pain secrete higher levels of cortisol, have compromised immune systems, experience more infections, and show delayed wound healing. Nurses must maintain a high level of suspicion for pain when caring for children. Infants cannot show the nurse where it hurts, and often a child’s report of pain is not given the credibility of an adult’s report. In addition, children may not realize they are supposed to report pain to the nurse.
The nurse should ask the child about pain using a pain rating scale. See Figure 21-2 for sample pain assessment tools. Children may sometimes refrain from complaining if they believe they will receive an injection to relieve the pain. In infants, pain may be assessed according to a behavior scale that includes tightly closed eyes, clenched fists, and a furrowed brow (see Figure 12-8). Pain assessment tools for preverbal children are discussed in Chapter 12. In toddlers, crying may be caused by anxiety and fear rather than by the degree of pain. On the other hand, chronically ill children may not grimace or cry when in pain, but withdraw from interacting with their surroundings.
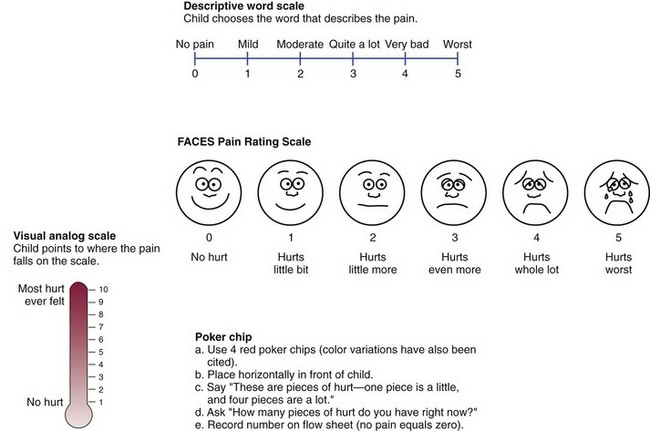
A pain indicator for communicatively impaired children (PICIC) has been developed and includes observations rated on a 4-point scale that includes the following:
The FLACC scale is a pain indicator that can be used with nonverbal children and is rated on a 0 to 2 scale for each observation with 10 being the highest level of pain; it includes the following:
All factors relating to pain assessment should be considered. Family members also experience emotional pain when they see their child in pain.
Nonpharmacological techniques such as drawing, distraction, imagery, relaxation, and cognitive strategies may enhance analgesia to provide necessary relief from pain symptoms. The child may draw “how the pain feels” and where it is located. Distractions such as storytelling, quiet conversation, and puppet play are effective. Imagery techniques, such as having children imagine themselves in a safe place, relieves anxiety. Slowing down breathing and listening to relaxation tapes is effective in reducing pain in adolescents. Cognitive (thinking) techniques such as “thought stopping” are also helpful in older patients. In this technique, the patient is instructed to repeat the word “stop” in response to negative thoughts and worries. A backrub or hand massage is also relaxing, depending on the child’s age and diagnosis. In newborns and infants undergoing brief painful procedures, oral sucrose may provide some analgesia. Pain medications should not be withheld from infants and children when needed.
Response to Drugs
Infants and children respond to drugs differently than adults. Elimination of the drug from the body may be prolonged because of an immature liver enzyme system. However, the renal clearance of drugs may be greater in toddlers than in adults. A decreased protein-binding capacity in the blood of small newborns may allow a greater proportion of free unbound drug to remain in the body of the small infant. Dosages are influenced by weight and differences in expected absorption, metabolism, and clearance. Every medication must be calculated by the nurse to determine the safety of the dose before the medication is administered. See the dosage calculation technique in Chapter 22.
Drugs Used for Pain Relief in Infants and Children
Acetaminophen is commonly used for the relief of mild to moderate pain in infants and children. The maximum dose is 15 mg/kg/dose for infants and children, with a maximum of 5 doses in 24 hours. Toxicity involves liver failure.
Nonsteroidal antiinflammatory drugs (NSAIDs), such as ibuprofen (Motrin), are given in a maximum dosage of 8 to 10 mg/kg every 6 hours (q6h). Ketorolac is a parenterally administered NSAID given for a maximum of 5 days.
Opioids are used for moderate to severe pain such as postoperative pain, sickle-cell crises, and cancer and should be administered with stool softeners to prevent constipation. If used for long periods of time, tolerance to the pain-relieving effect as well as respiratory depression effects can develop. The right dose of an opioid drug is the amount that relieves pain with a margin of safety for the child. The dose should be repeated before the pain recurs. Addiction is rare in children and adults receiving opioids for pain (Kliegman et al., 2007). Providing adequate pain relief enables patients to focus on their surroundings and other activities, whereas inadequate pain relief causes the patient to focus on the pain and when more medication will be given to stop the pain.
Fentanyl is a potent analgesic given for short surgical procedures. It has a rapid onset with a short duration of action.
Naloxone should be available for use in case of opioid overdose. Flumazenil (Romazicon) should be on hand for a midazolam (Versed) or diazepam (Valium) overdose.
Local anesthetics are used with safety and effectiveness in children. Topical anesthetics are used for skin sutures, intravenous (IV) catheter placement, and lumbar punctures. EMLA cream is a mixture of lidocaine and prilocaine (eutectic mixture of local anesthetics) that is applied topically to the intact skin (Figure 21-3) and can be used with neonates. “Numby Stuff” uses a mild electrical current (iontophoresis) to push a topical preparation of Lidocaine and epinephrine into the skin providing local anesthesia within 10 minutes of the application of the patch. “LMX4” is a nonprescription topical anesthetic that is similar to EMLA. A vapocoolant spray can provide superficial skin anesthesia for short periods of time. Preoperative and postoperative care is discussed in Chapter 22.
FIGURE 21-3 EMLA cream, a topical anesthetic used before an invasive procedure to reduce pain involved in piercing the skin.
Patient-controlled analgesia (PCA) allows the patient to press a button attached to an IV analgesic infusion to self-administer a bolus of medication. Parents and children as young as 7 years of age can be taught to use PCA. A built-in lockout interval prevents accidental overdosing. Any child receiving opioid analgesic drugs should be observed closely for side effects, such as respiratory depression.
More effective pain relief at lower dosages may be achieved when a low-dose analgesic is administered around-the-clock on a regular schedule rather than as needed (PRN). However, “breakthrough pain” can occur, and additional doses of an analgesic may have to be given. This type of pain management is called preventive pain control.
Conscious Sedation
Conscious sedation is the administration of IV drugs to a patient to impair consciousness but retain protective reflexes, the ability to maintain a patent airway, and the ability to respond to physical and verbal stimuli. Conscious sedation is used to perform therapeutic or diagnostic procedures outside the traditional operating room setting. A skilled registered nurse is required to continuously monitor the patient in an area where emergency equipment and drugs are accessible for resuscitation.
A 1 : 1 nurse-patient ratio is continued until there are stable vital signs, age-appropriate motor and verbal abilities, adequate hydration, and a presedation level of responsiveness and orientation. Parents are instructed concerning diet, home care, and follow-up visits.
Fear
Intrusive procedures, such as placing IV lines and performing blood tests, are fear provoking. They disrupt the child’s trust level and threaten self-esteem and self-control. They may make it necessary to restrict activity. Care must be taken to respect the modesty, integrity, and privacy of each child. Hospital personnel can provide an environment that supports the child’s need for mastery and control. These interventions are discussed according to age in this chapter and throughout the text. Selected nursing diagnoses for the hospitalized child and family are presented in Nursing Care Plan 21-1.
 Nursing Care Plan
Nursing Care Plan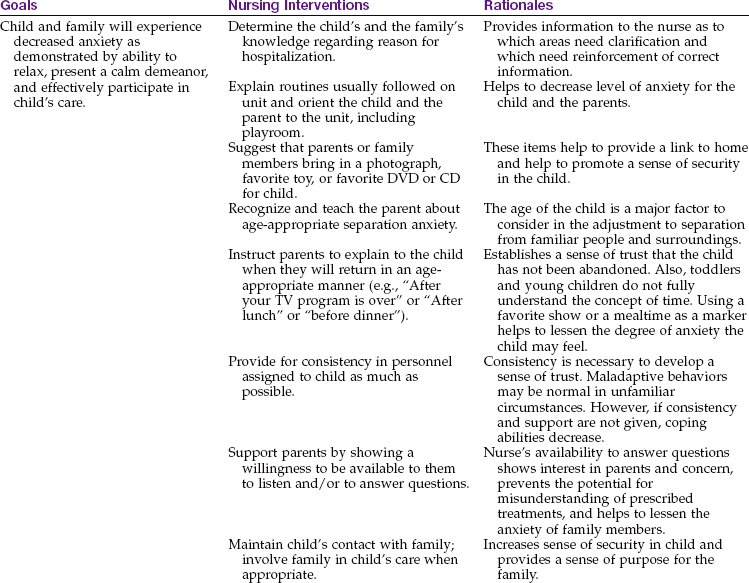
Regression
Regression of growth and development during hospitalization can be expected. Regression is the loss of an achieved level of functioning to a past level of behavior that was successful during earlier stages of development. Examples of regression include demanding a bottle in a child who usually drinks from a cup, refusal to use a potty chair in a child who has achieved bowel and bladder control, or demanding to be carried by a child who had been walking independently. Regression can be minimized by an accurate nursing assessment of the child’s abilities and the planning of care to support and maintain growth and development. However, regression should not be punished. Nurses can guide parents to praise appropriate behavior and ignore regressions. When the child is free of the stress that caused the regression, praise will motivate the achievement of appropriate behavior.
Cultural Response
Showing culturally sensitive attitudes toward families with hospitalized children decreases anxiety. Flexibility and careful listening are necessary to understand cultural needs. Studies of children in many different societies show that the childhood environment typical in American culture is different from environments deriving from other traditions. Nurses must also be aware of their own cultural biases and how these might affect their assessments. In some cases a translator may be required.
The nurse must create a bridge between the health care system of the United States and the diverse people that system serves. Effective utilization of health care service and compliance with treatment plans is enhanced when the nurse’s approach is compatible with cultural needs and beliefs. Teaching will be effective only if the parents or child understand the language used. Interpreters should be used as needed. Nonverbal cues and body language are important in intercultural communication. Nurses should take the time to learn what their gestures and movements mean to the family from another culture.
In some developing countries the energies of parents are focused on survival rather than on promoting growth and development or intellectual skills. These practices become ingrained in the childrearing practices handed down from generation to generation. For example, within these cultures, parents may believe that an ill infant must be near the caregiver’s body at all times. Therefore, in the Western hospital, the nurse may find it a challenge to coax parents to allow the infant to remain in the crib, enveloped by an oxygen tent, and separated from them.
Crying may be interpreted by some cultures as a signal of an organic upset or illness. Because diarrhea is a common cause of infant death in developing countries, frequent feeding in response to crying is a survival response. When families from developing countries that use these survival practices move to the United States (where survival threats decrease), it may take generations to change the child care practices and focus on promoting optimum growth and development.
One cultural group may prize autonomy and initiative in their children, whereas another may tolerate only complete obedience. Protective amulets or charms placed on the wrists or clothing of infants must be respected. In the gypsy culture, the color red and the number three are positive symbols. Therefore a red-colored medicine to be given 3 times a day will receive more compliance than a white-colored medication prescribed 2 times a day. Respecting cultural and religious beliefs will enhance compliance.
The nurse must be careful to separate survival practices from cultural beliefs. It may be advantageous to change care practices based on survival when the threat to survival is no longer present. If the practice is based on cultural belief, however, the practice must be respected and no attempt should be made to change it. The nurse must assess the family through the eyes of its culture to avoid labeling a family who is different as dysfunctional.
Intercultural Communication: Responses to Hospitalization
Personal space is defined as an imaginary circle that surrounds us. The size of that space and how securely it is guarded is largely determined by culture. We can observe the space by watching two friends of the same culture talk to each other. Some people stand close to each other. Nurses, who often must invade that personal space in carrying out their duties, can be perceived as “pushy” or suspect, and the parent who retreats to protect it can be thought of by the nurse as “cold.”
Smiling
A smiling nurse may not be received in all cultures as a “friendly” nurse. In Russia a smile indicates happiness and is inappropriate in a serious or sad situation. Nurses may interpret a nonsmiling Russian as “unfriendly” if they are unaware of this cultural difference. Members of some cultures, however, smile in all circumstances. Their smile is a show of respect. When they are reprimanded, they smile to show they did not mind being reprimanded.
Eye Contact
In the United States, establishing eye-to-eye contact with the person with whom one is communicating is considered a show of respect and attention. In some Asian cultures, however, eye-to-eye-contact is seen as disrespectful. Native Americans consider it rude to stare at a speaker. Eye contact is acceptable for short periods only. The cultural term evil eye originates from cultures that interpret eye-to-eye contact as disrespectful.
Touch
In the United States, touch is often considered a gesture of friendliness. However, touch can give misleading messages. A pat on the head may imply superiority of the person touching the head. In the Vietnamese culture, touching the head is thought to rob those being touched of their souls.
Focus
Some cultures are receptive to communication or teaching if the focus is on the problem. Some cultures deal with the problem by focusing on its future impact on the family or the life of the child. Teaching strategies must be designed to approach the topic from the perspective appropriate to that culture.
When teaching infant and child care, the nurse must always determine the values of the cultural practice of the family before imposing a standardized process. Avoiding cultural conflict is essential to the successful outcome of parent and child teaching. Culture evolves and is not static. However, most families from varying cultures strive to maintain their cultural identities while adapting to Western practices. The nurse should support maintaining the individual cultural identity of that family. Culturally sensitive health care is also discussed in Chapter 15.
The Parents’ Reactions to the Child’s Hospitalization
When children are hospitalized, the entire family is affected. The parents of the hospitalized youngster need others to show interest in their physical and emotional needs. If they are frightened and tense, the child soon senses it.
Parents may believe they are to blame for the child’s illness; they may believe they should have recognized the symptoms earlier or could have prevented an accident by closer supervision. Immunizations and other types of preventive care may also have been neglected. These feelings can cause a sense of guilt, helplessness, and anxiety.
Parents seldom are the direct cause for hospital admission of a child. Even in cases of child abuse or neglect, nothing is gained by blaming the parents. The nurse must remain objective and empathic. The nurse listens carefully to parental concerns and acknowledges the legitimacy of their feelings, for example, “It is understandable that you feel this way; everything happened so fast.” Parents also commonly express feelings of helplessness at the loss of the parental role as protector. The nurse encourages and supports parents and other family members, stresses their importance to the child’s recovery, and encourages their participation in the care of the child. The admission of a child to the hospital is anxiety producing. The uncertainty of the situation can become overwhelming, causing feelings of panic. However, these feelings are usually temporary. The nurse should remain relaxed, reassure the parents, and reinforce positive parenting. Information about the child’s condition and treatment plan is given. Needs are assessed, and interventions are planned to meet specific needs.
Nursing Tip
Many hospitals allow parents to be with their child during painful or stressful procedures and during the recovery phase postoperatively.
Poor communication results in unnecessary fears. The nurse should explain in simple terms some of the equipment being used and facilities available on the unit. The nurse listens attentively and tries to clear up misconceptions. Rooming-in may alleviate some anxieties of parents. However, the nurse must continue to promptly and cheerfully tend to the needs of the child to indicate to the parents that their child is in good hands. Parental involvement in a child’s care offers the nurse the opportunity to assess the relationship and to provide guidance and teaching as needed.
Parents may need to take time from work, especially if treatment involves travel to special centers. Ronald McDonald homes offer lodging and other homelike amenities for parents of patients with life-threatening illness. The availability of these facilities is explored with the family. The social service worker may be of help in such instances. The care and welfare of other children at home while one parent is at work and the other is rooming-in with the ill child should be discussed. Parents should be advised that pain-control techniques are available and will be used to minimize painful experiences for the ill child.
Parents may ventilate their feelings and stresses through anger, crying, or body language. Behavior is not only a response to the current situation but often involves attitudes resulting from early childhood experiences. The nurse must not pass judgment on individuals whose behavior may seem demanding or unreasonable. An understanding and acceptance of people and their problems is essential for the successful pediatric nurse.
Siblings are also affected when a brother or sister is hospitalized. They may be afraid or feel left out, guilty, or resentful of the attention focused on the ill child. Suitable interventions by the nurse include directing some attention to the siblings, supporting their efforts to comfort the family member, and engaging them in play or drawing pictures, such as “How it feels to have an ill brother or sister.” They may also make cards and pictures for the patient.
The Nurse’s Role in the Child’s Hospitalization
Nurses are responsible for admitting new patients to the hospital unit. Besides performing the procedure skillfully, they must be prepared to meet the emotional needs of those involved. The impression the nurse gives, whether good or bad, definitely affects the child’s adjustment. Empathy in responding to the fears of the child and family members makes the admission procedure stimulating and educational—a positive experience for all.
A child should be prepared for hospitalization when possible. Ideally, the child and parents should tour the pediatric unit before admission. This enables the parents to meet some of the people who will care for their child. Children and their families may be overwhelmed by the size of the institution and the fear of becoming lost.
Between 1 and 3 years of age, children are worried about being separated from their parents. After 3 years of age, children may become more fearful about what is going to happen to them. Parents should try to be as matter-of-fact as possible about this new experience. Unless they have been hospitalized before, children can only try to imagine what will happen to them. It is not necessary to go into much detail; the child’s imagination is great, and giving information that is beyond comprehension may create unnecessary fears. It is logical to dwell on the more pleasant aspects, but not to the extent of saying that hospitalization involves no discomforts. For example, one might mention that meals will be served on a tray, that baths will be taken from a basin at the bedside, and that the child will be with other children. The fact that there is a buzzer for calling the nurse may add to the child’s sense of security. The parents may plan with the child what favorite toy or book to bring.
Perhaps more important than explaining certain occurrences is listening to how the child feels and encouraging questions. Parents should prepare them a few days, but not weeks, in advance. Parents should never lure children to the hospital by pretending that it is some other place. In emergency situations, there is little time for preparation. In such cases the entire medical team must try to give added emotional support to the child. The initial greeting should show warmth and friendliness—smile and introduce yourself.
Some hospitals allow the patient to be taken to the playroom for a short time before going to the room. When the parent tells the nurse the child’s name, associating it with a familiar person who has the same name will help the nurse to remember it. It creates a much warmer feeling to speak of “John” or “Suzy” than “your little boy” or “your daughter.”
The parent is encouraged to do as much for the child as possible, for example, remove clothes. The nurse tries not to appear rushed. A matter-of-fact attitude must be maintained regardless of the patient’s condition. A soft voice and quiet approach are less frightening to the child. A nurse who looks anxious causes unnecessary worry for everyone concerned. A troubled look may have nothing to do with the child. Taking one step at a time is advised. Calmness is catching. The nurse remains available to answer questions that might arise. When there is a good relationship between the parent and nurse, the child benefits from higher quality care.
When children are hospitalized, the nurse should be aware of the developmental history as well as the medical history. A developmental history includes the following:
• Family relationships and support systems
• Cultural needs that may affect care and hospital routine
• Nicknames, rituals, routines
• Developmental level and abilities
• Personality, adaptability, coping skills
• Past experiences, divorce, new siblings, extended family
• Previous separation experiences—vacations or hospitalizations
• Impact of current health problem on growth and development
Developing a Pediatric Nursing Care Plan
Developing the pediatric nursing care plan is similar to developing an adult care plan. The care plan is the result of the nursing process. It states specifically what is to be done for each child and keeps the focus on the child—not on the condition or the therapy. An established list of accepted nursing diagnoses is available and in use. These serve as a standard for organizing data collection. They also serve as a vehicle by which one nurse can communicate with another. A nursing diagnosis for a pediatric patient may require some modification. A survey of the child includes knowledge of growth and developmental processes. It also includes evaluating the primary caregiver, who has a direct role in the safety and maintenance of the child’s health. Nursing care plans are guides, and continual evaluation and reevaluation are called for to determine whether the goals for the individual child are being met. A Kardex system consisting of an 8- × 10-inch card summarizing pertinent medical and nursing orders, formerly used by many hospitals, has been replaced by electronic (paperless) charting. Figure 21-4 shows a nurse entering data for later retrieval into the unit computer.

Clinical Pathways
Clinical pathways are used in acute care settings as well as in alternate care settings. The clinical pathway is an interdisciplinary plan of care that displays the progress of the entire treatment plan for the patient. The main difference between a clinical pathway and a nursing care plan is that the nursing care plan focuses on the nurse’s role in the care of the patient, whereas the clinical pathway focuses on the broader view of the entire multidisciplinary health care team and general outcome goals of care with specific timelines. Understanding the nursing process and the nursing care plan is essential to understanding the nurse’s role in the clinical pathway. See Chapter 1 for further details concerning the clinical pathway.
Clinical pathways for children with specific conditions are presented in various chapters of this text. Pictorial pathways (Figure 21-5) have been used and are especially valuable in patient education and anticipatory guidance.

Meeting the Needs of the Hospitalized Child
Hospitalization is frustrating for infants. During infancy, rapid physical and emotional development takes place. Infants are used to getting what they want when they want it, and they show their displeasure quickly when illness restricts the satisfaction of their desires. Infants who were breastfed at home may be unable to continue this regimen. They miss the continuous affection of their parents. Their daily schedule is upset. The infant who drinks well from a cup at home may refuse it entirely at the hospital.
Nursing personnel must try to meet the needs of these patients by protecting them from excess frustration. It is not wise to expect them to develop new habits when they need energy to cope with their illness and the strange environment. One of the nurse’s major goals during this period is to assist with the parent-infant attachment process and to promote sensorimotor activities. This can be fostered by providing means for the infant and significant caregiver to interact and by attempting to ease the tension of the parents. The nurse can serve as a role model by performing activities with the infant, such as cuddling, rocking, talking, and singing. A swing, a bath with squeeze toys, a pacifier, and a hanging mobile are also appropriate as the infant’s condition permits.
Because the infant cannot understand explanations, the nurse administers uncomfortable procedures as gently as possible and returns the infant to the parents for consolation. Liberal visiting hours are essential (Figure 21-6). When parents are not available, soothing support and gentle touch are provided; otherwise the infant may learn to associate only pain with nursing care. Consistency in caregivers is also important at this stage of development.

The Hospitalized Toddler
The toddler’s world revolves around the parents, particularly the mother (or significant caregiver). Hospitalization is a painful experience for toddlers. They cannot understand why they are separated from their mothers, and they become very distressed. Toddlers who have a continuous, secure relationship with their mothers react more violently to separation because they have more to lose. Nursing goals in the care of the hospitalized toddler are presented in Box 21-2.
Separation anxiety is at its peak in the toddler (see Chapter 17). The nurse who comprehends the various separation stages sees parental visits as necessary, even though the process of separation and reunion is painful. A cohesive staff is essential to meet the needs of the children and their parents. Education of the parents helps to promote their continued visits and to decrease feelings of inadequacy. Ritualistic patterns of care create a sense of structure and are appropriate for children in this age-group.
Repetitive games that deal with disappearance and return are helpful. Peek-a-boo and hide-and-seek serve such a purpose. The use of a transitional object, such as a blanket or a favorite toy from home, promotes security. Pictures of the family and tape recordings of favorite stories are other tools that help the child remain connected with the family. When the nurse or parent leaves, he or she explains when he or she will return in terms of the toddler’s experience (e.g., after naptime or lunch) and then returns promptly at that time. A loving hug, good-bye, and prompt exit are then necessary. The continued reappearance of the parents as promised is of value in reducing the child’s anxiety and reestablishing his or her sense of trust. The parent should not wait until a child falls asleep to depart. This prevents confrontation but disturbs the child’s sense of trust. The nurse assures the parents that he or she will remain with the child for comfort.
Rooming-in is highly desirable. When rooming-in is impossible, consistent caregivers should be assigned to care for the child and the parent. The nurse indicates by his or her approach that he or she considers the parent’s contributions extremely important to the child’s well-being. The nurse interprets the stages of separation anxiety to the parent (Figure 21-7). The nurse must also realize that parents are under stress and should not be asked to assume responsibilities beyond their capabilities. The nurse observes parents for signs of fatigue and suggests appropriate interventions.
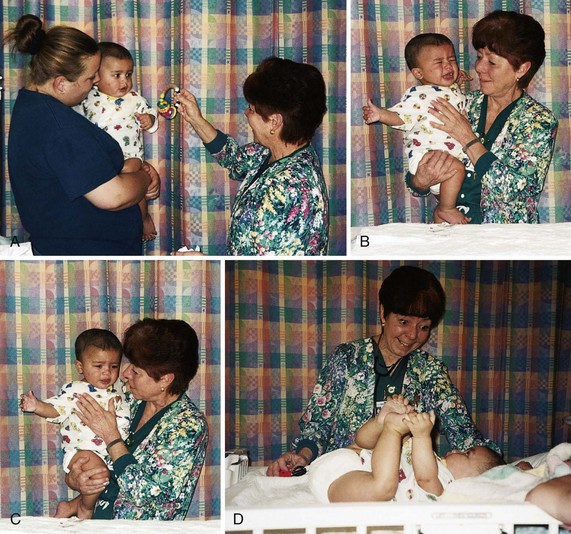
FIGURE 21-7 A, The clinical nurse specialist (CNS) approaches the small child calmly, slowly, at eye level, and with the parent present. B, The infant shows apprehension and anxiety when carried by the CNS. C, Beginning trust is established. D, After trust is established, general assessment can begin. (Courtesy Pat Spier, RN-C.)
Occasionally parents do not choose to care for their child; for example, “We feel that since we are paying for this, we should just be able to entertain him.” In such instances, the parents’ wishes are respected. Referral to the clinical nurse specialist might also be appropriate to facilitate communication and to better understand the underlying dynamics of the situation.
The home habits of the toddler are recorded and used as a basis for everyday routine. A potty chair is provided if the child is trained. Some regression in behavior is to be expected. If the toddler still prefers bottles to cups, there should be no attempt to change this in the hospital. Familiar toys and books are important. A steady, calm voice communicates safety. Toddlers are in the stage of autonomy. Loss of a small amount of the self-control they have achieved usually results in resistance and negativism.
Children are forewarned about any unpleasant or new experience that they may need to undergo while in the hospital. This is done in keeping with their level of understanding. Being truthful about things that may hurt prevents the child from feeling betrayed. Preparation and explanation are done immediately before a procedure so that the child does not worry needlessly for an extended time. Crying and protesting when told about certain procedures are healthy expressions of feelings and relieve tension. Distractions such as blowing bubbles, looking through a kaleidoscope, and playing with pop-up toys may help to reduce anxiety and pain.
Supervised playroom activity contributes to intellectual, social, and motor development. Treatments in the playroom are avoided. Toddlers are encouraged to play with safe equipment used in their care, such as bandages, tongue blades, and stethoscopes. Whenever possible, they are allowed out of their cribs because confinement is frustrating for little ones who have just begun to enjoy walking. Playtime establishes rapport and is an important part of the nursing care of children.
There are indications that restricting the child’s mobility for surgical and medical procedures involving splints, IV therapy, burn dressings, and so on may contribute to the development of emotional or personality problems or to speech and learning difficulties (Kliegman et al., 2007). Therefore, when restraint is required, it must be accompanied by increased emotional support such as rooming-in, additional attention from nurses, and suitable diversion.
It is common for children to experience changes in behavior on their return home. They may be demanding and may cling to the parent every minute. “He just won’t let me out of his sight” is a common description. The parent should give the toddler extra attention and reassurance until trust is regained.
The Hospitalized Preschooler
The experience of hospitalization may be easier for preschool children who have had outside contact (e.g., nursery school and kindergarten) than for those who have never been separated from their parents. Because children of this age operate with concrete thinking, they can understand more and they can be better prepared for hospitalization. Explanations must be made in realistic terms, because preschool children cannot understand abstract explanations. When explaining procedures the nurse should be careful to use nonthreatening words (Table 21-1). They are made to realize that hospitalization is not a punishment for something they have done wrong. Children may feel guilty, particularly if an accident happens because of some mischief on their part, such as in the case of burns or falls.
Table 21-1
Words to Avoid and Words to Use
| AVOID | USE INSTEAD |
| Shot | Medicine under the skin |
| Incision | Special opening |
| Put to sleep, anesthesia | Special sleep |
| Electrodes | Stickers |
| X-ray | Special picture |
| Stretcher, gurney | Rolling bed |
| Catheter | Tube |
| Take “your temperature” | Check “your temperature” |
Preschool children are distressed when their parents prepare to leave them but, unlike the toddler, they can understand time relationships through activities—at breakfast, after lunch, and the like. The nurse and parents must not tell the child that they will return unless they intend to do so.
At this age the child is afraid of bodily harm, particularly invasive procedures. The surgical patient must be shown the part of the body that requires surgery. The nurse can sketch a body outline and draw a circle around the operative site, giving simple information about the system that will be affected. It is stressed that only this area of the body will be involved. Children in this age-group engage in magical thinking and fantasy. Fantasizing the unknown can be frightening to a young child. The preschooler needs clear, understandable, and truthful explanations. Children who ask questions should be complimented and listened to; any misinterpretations should be corrected. The child is helped to increase self-esteem through praise. The child relieves tension through role playing. Tongue depressors, adhesive bandages, and other materials related to everyday hospital life are relished by the sick child.
Parents are faced with a disrupted home life throughout the child’s hospitalization. Parents cannot cope with everyday tasks when they are lonely for and worried about their child. The frequent trips to the hospital interfere with the daily routine, and other children in the family may resent them. Contact with the physician is needed. Parents have a legal and ethical right to be informed of the benefits and risks of therapy and to be included in the decision making process. When the child is finally discharged, he or she may be demanding and irritable. Parents need the kind support of hospital personnel to enable them to make informed decisions and deal with these added strains.
The Hospitalized School-Age Child
Children of school age can endure separation from their parents if it is not prolonged. Children who have been cherished from birth can tolerate brief interruptions in their lives more easily than can those who have been denied a secure environment. The school-age child is in a stage of industry and independence. Forced dependency in the hospital (such as immobilization) can result in a feeling of loss of control and loss of security. School-age children need to feel “grown up.” They can participate in their care and be offered simple choices to foster their feeling of independence. They can choose their menus within appropriate restrictions, “help the nurse” in various activities, and keep busy with age-appropriate toys.
Knowledge of growth and development in the school-age child helps the nurse provide anticipatory guidance. Nurses can also enlist parents to determine what, if any, successful approaches they use in guiding the child. Behavioral problems may be addressed by a team conference. Nurses who work with children should keep abreast of current trends and guidance approaches. Positive direction and consistency are tools of particular importance to the pediatric nurse.
The education of the school-age child must continue throughout any illness. This gives the child a sense of continuity with the outside world, provides periods of socialization, reinforces weak academic areas, and reassures the child that he or she can return to his or her peers after discharge. The parents may act as liaisons between school and hospital. The teacher must be informed of the child’s physical and emotional health to be effective. The nurse provides children with opportunities to study undisturbed so that they will be prepared for classes. Diagnostic tests and treatments should be scheduled around established school routines whenever possible. Many school districts have individual tutors for homebound or hospitalized school-age children.
It is common for school-age children to be “brave” and to show little, if any, fear in situations that actually upset them a good deal. Observation of body language may provide some clues to emotional states. The nurse’s presence during unfamiliar procedures is comforting. Following treatments the nurse should encourage children to draw and talk about their drawings or to act out their feelings through puppet play.
 Safety Alert!
Safety Alert!The Hospitalized Adolescent
Adolescents, in particular, experience feelings of loss of control during hospitalization. Daily routines are disrupted, and dependence-independence issues come to the foreground. When feelings of independence, self-assertion, and identity are threatened, the adolescent may respond by withdrawal, noncompliance, or anger. Care plans must be designed to incorporate choice, privacy, and understanding.
Early Adolescence: Nursing care plans must be oriented to the adolescent’s age. Illness during early adolescence, approximately 10 to 13 years of age, is seen mainly as a threat to body image. There is a narcissistic concern about height, weight, and sexual development. Patients are aware of heightened body sensations and often have numerous physical complaints. Intense relationships with members of one’s own sex are prevalent; they precede heterosexual involvement. Patients in this age-group are anxious about how the illness will affect their physical appearance, functioning, and mobility; however, they are not usually overwhelmed by forced dependence. Self-portrait drawings are effective at this time. Maintaining privacy and same-sex room assignments are essential.
Middle Adolescence: During middle adolescence (approximately 14 to 16 years of age), adolescents are anxious about their ability to appeal to the opposite sex and to meet gender role expectations. Physical growth is practically complete. The peer group assumes greater importance in determining acceptability and behavior. During middle adolescence the struggle for emancipation from the family, although erratic, is at its peak. It is disturbing not only to the adolescent but also to parents, who must relinquish much of their control to hospital personnel. Incorporating choice, privacy, appropriate hair and cosmetic appearance, and the opportunity for peer visitors is important during hospitalization.
Late Adolescence: Late adolescents, approximately 17 to 21 years of age, are mainly concerned with the tasks of education, career, marriage, children, community, and style of life. The dating partner becomes the person of primary importance. Hospitalization may pose the threat of postponement of career and future plans. Contact with school personnel, counselors, and teachers is important to prevent long-term impact on the education and development of the adolescent.
Adjustment to Illness: The adolescent has many intellectual strengths including the ability to think abstractly and to solve problems. Adolescents can understand the implications of their disease both in the present and in the future, and they are capable of participating in decisions related to treatment and care. The nurse who recognizes these skills and encourages their practice helps patients gain confidence in their intellectual abilities, thus increasing their sense of independence and self-esteem.
Roommate Selection: Roommate selection, although often overlooked, is extremely important for this age-group. Adolescents usually do better with one or more roommates than in a single room. Because few community hospitals have adolescent wings, it is helpful if the patients participate in the decision regarding whether the adolescent is admitted to the pediatric or the adult unit. A few adjoining rooms at the ends of these units will suffice. Placing the teenager next to a senile, dying, or severely debilitated patient in the adult unit or an infant in the pediatric unit should be avoided.
Confidentiality and Legality
Respecting the confidentiality of children is important to establishing trust. In general, information should not be divulged or shared without consent. Many problems can be avoided if the confidentiality of the relationship is clearly defined during initial meetings. Patient records must be carefully monitored to prevent loss or observation by unauthorized personnel. The nurse must avoid giving private information about any patient to telephone callers or visitors. Appointment books and computer screens in an office are concealed rather than kept open to view on the desk.
The term emancipated minor generally refers to an adolescent younger than 18 years of age who is no longer under the parent’s authority. Married minors or minors in the military are automatically considered emancipated and may give consent for medical treatment for themselves and their children.
In some parts of the United States the young adolescent may receive medical assistance without parental awareness for certain conditions, such as sexually transmitted infections, contraception, pregnancy, abortion, and drug abuse. These laws are designed to afford the young person immediate medical help without fear of reprisal. However, some laws are being challenged in the courts. In a medical emergency a minor can be treated without the consent of parents if the situation is life-threatening.
Because laws vary from state to state, nurses must keep abreast of policies and legislation within their practice. Such information is available from the local medical or state nursing licensing boards.
Discharge Planning
Preparation for the patient’s discharge ideally begins on admission, because the goal of hospitalization is to return a healthier and happier child to the parents. An approach directed only toward good physical care of the patient’s disease is not sufficient. The nurse must also consider the emotional growth of the child and the education of the patient and family. This will provide a positive learning experience for all involved.
If a patient requires specific home treatment, such as hyperalimentation, colostomy care, crutches, special diet, or insulin therapy, instructions are given to the parents gradually throughout their child’s hospitalization. The instructions are written so they can be referred to as needed. If the older child is to administer any self-treatment, careful explanations and supervision are required until both patient and parents are confident they can carry out the procedure safely at home. This may require the participation of home health services.
Parents also must be prepared for behavioral problems that may arise after hospitalization. Severe stress may be obvious during the patient’s stay. The services of a children’s counselor are helpful if nightmares and regression occur. Guidance includes the following suggestions:
• Anticipate behaviors such as clinging, regression in bowel and bladder control, aggression, manipulation, and nightmares
• Allow the child to become a participating family member as soon as possible
• Take the focus off the illness; praise accomplishments unrelated to it
• Be kind, firm, and consistent with misbehavior
• Build trust by being truthful
• Provide suitable play materials such as clay, paints, and doctor and nurse kits
• Listen to and clarify misconceptions about the illness
• Prevent long periods of separation until a sense of security is regained
• Allow the child to visit hospital staff during routine clinic visits if desired
Whenever possible, parents are given at least 1 day’s notice of their child’s discharge from the hospital so they can make the necessary arrangements. This is particularly important if both parents work, or if transportation is a problem. The physician writes the discharge order. The approximate hour of dismissal is relayed to the parents. The child is weighed and dressed, and all personal belongings are collected. Parents are given a written return clinic appointment card when indicated.
Parents sign a release form and visit the hospital business office according to hospital procedure. The nurse may accompany the child and parents to the hospital exit to say good-bye. According to condition, the child is placed in a hospital wagon, wheelchair, or stretcher for transport. The nurse assists in securing the child into the vehicle. Documentation includes when and with whom the child departed, patient’s behavior (smiling, alert, crying, and so on), method of transportation from the facility, patient’s weight at the time of discharge, and any instructions or medications given to the child or the parents.
 Legal and Ethical Considerations
Legal and Ethical Considerations
Discharge Documentation
Discharge documentation should include who accompanied the child (and identification given), time of discharge, behavior and condition of the child, method of transportation, vital signs and weight, medications, and instructions given to parents or caregiver.
Home Care
Many children with acute and chronic conditions are cared for in the home. Home health care and other community agencies work together to provide holistic care (Jackson et al., 2009). Respite care provides trained workers who come into the home for brief periods to relieve parents of the responsibility of caring for the child. This enables the parents to shop, do business transactions, or simply take time for much-needed self-care. The school system also shares in the responsibility for care, which is crucial if a family is to be successful in home care. The health care worker assisting in the home should do the following:
• Observe how the parents interact with the child.
• Observe facial expressions and body language.
• Post signs above the bed denoting special considerations, such as “Never position on left side” and “Do not feed with plastic spoon.”
• Listen to the parents and observe how they attend to the physical needs of the youngster.
• Ask questions or discuss apprehensions the parents may have about their ability to care for the child.
• Be attuned to the needs of other children in the home.
• Be creative in exploring avenues for socialization, because these children are seldom invited to birthday or slumber parties.
• Explore community facilities or support groups that might benefit the family.
Get Ready for the NCLEX® Examination!
Key Points
• The care of sick children can take place in a variety of settings.
• Play is an important part of a nursing care plan for children.
• Nursing care plans for hospitalized children should include measures to minimize negative impact on growth and development.
• There are various pain scales available to help the nurse determine the pain level in a nonverbal child.
• Pain is the fifth vital sign and should be assessed and treated in infants and children.
• Three major causes of stress for children of all ages are separation, pain, and fear of bodily harm.
• Separation anxiety is most pronounced in the toddler.
• The three stages of separation anxiety are protest, despair, and detachment.
• When a school-age child requires hospitalization, a school, home, or hospital teacher can be requested by the nurse to prevent loss of grade status.
• Nurses caring for children must maintain a high level of suspicion for pain, because children are often unable to verbalize discomfort.
• Techniques such as drawing, distraction, imagery, and relaxation; cognitive strategies; and analgesia provide relief from pain.
• A culturally sensitive attitude toward families with hospitalized children decreases anxiety.
• Treatments should not be performed in the playroom.
• The surgical patient should be shown the part of the body that will be operated on. Children are assured that this is the only area of the body that will be involved.
• Respecting the confidentiality of the adolescent is important to establishing trust.
• The pediatric nursing care plan is a product of the nursing process as applied to the child.
• Clinical pathways are a multidisciplinary plan of care with outcome goals that involve timelines.
• The developmental level of the child influences specific needs during the hospitalization experience.
• The child’s age, sex, developmental level, and diagnosis are factors that influence placement on a unit.
Additional Learning Resources
 Go to your Study Guide for additional learning activities to help you master this chapter content.
Go to your Study Guide for additional learning activities to help you master this chapter content.
 Go to your Evolve website (http://evolve.elsevier.com/Leifer) for the following FREE learning resources:
Go to your Evolve website (http://evolve.elsevier.com/Leifer) for the following FREE learning resources:
• Answer Guidelines for Critical Thinking Questions
• Answers and Rationales for Review Questions for the NCLEX® Examination
• Glossary with English and Spanish pronunciations
• Interactive Review Questions for the NCLEX® Examination
• Patient Teaching Plans in English and Spanish
 Online Resource
Online Resource• City of Hope Pain & Palliative Care Resource Center—City of Hope: http://prc.coh.org
Review Questions for the NCLEX® Examination
1. What are the stages of separation anxiety in the toddler?
1. Protest, despair, and denial
2. Denial, dependence, and submission
2. Assessment of pain is considered a fifth vital sign to be documented by the nurse. The nurse understands that pain in infants:
1. cannot be reliably assessed.
2. will not be remembered by the infant.
3. The best way to minimize separation anxiety in a hospitalized infant is to:
1. explain routines carefully.
2. encourage parent to room-in.
4. Which statement by the parent of a hospitalized 4-year-old child indicates an understanding of the child’s needs?
1. “I am going to buy him a box of new toys to keep him busy while in the hospital.”
2. “I am going to bring some of his favorite toys from home for him to play with while in the hospital.”
3. “I’m glad there is a television in the room for him to watch all day.”
4. “I will stay every day until he falls asleep and then I will go home.”
5. A 4-year-old hospitalized child wets his bed. The parents tell the nurse that the child was completely toilet trained. What should the nurse understand?
Critical Thinking Question
1. A 5-year-old child has been hospitalized for 2 days. She is watching the television mounted above her bed. She is expressionless but does not cry or appear to be in distress. Her mother calls on the telephone and states that since her child seems to be adjusted, she may not come in today to visit because she does not want to “upset her.” How should the nurse interpret the child’s behavior? How should the nurse respond to the mother?