Nursing Care of Women with Complications During Pregnancy
1 Define each key term listed.
2 Explain the use of fetal diagnostic tests in women with complicated pregnancies.
3 Describe antepartum complications, their treatment, and their nursing care.
4 Identify methods to reduce a woman’s risk for antepartum complications.
5 Discuss the management of concurrent medical conditions during pregnancy.
6 Describe environmental hazards that may adversely affect the outcome of pregnancy.
7 Describe how pregnancy affects care of the trauma victim.
8 Describe psychosocial nursing interventions for the woman who has a high-risk pregnancy and for her family.
 , p. 82)
, p. 82) , p. 91)
, p. 91) , p. 96)
, p. 96) , p. 97)
, p. 97) , p. 82)
, p. 82) , p. 96)
, p. 96) , p. 98)
, p. 98) , p. 91)
, p. 91) , p. 107)
, p. 107) http://evolve.elsevier.com/Leifer
http://evolve.elsevier.com/Leifer
Most women have uneventful pregnancies that are free of complications. Some, however, have complications that threaten their well-being and that of their babies. Many problems can be anticipated in the course of prenatal care and thus prevented or made less severe. Others occur without warning.
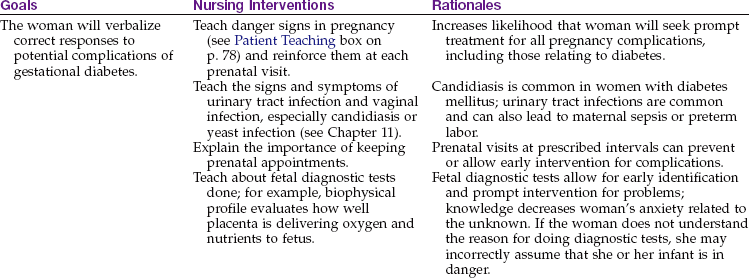
Women who have no prenatal care or begin care late in pregnancy may have complications that are severe because they were not identified early. Danger signs that should be taught to every pregnant woman and reinforced at each prenatal visit are listed in the Patient Teaching box. The woman should be taught to notify her health care provider if any of these danger signs occur. A high-risk pregnancy is defined as one in which the health of the mother or fetus is in jeopardy.
 Patient Teaching
Patient Teaching
Danger Signs in Pregnancy
The nurse should teach the woman to promptly report any danger signs that occur during pregnancy, including the following:
The causes of high-risk pregnancies usually have the following characteristics:
• Relate to the pregnancy itself
• Occur because the woman has a medical condition or injury that complicates the pregnancy
• Result from environmental hazards that affect the mother or her fetus
• Arise from maternal behaviors or lifestyles that have a negative effect on the mother or fetus
Early and consistent assessment for risk factors during prenatal visits is essential for a positive outcome for the mother and the fetus.
Assessment of Fetal Health
Extraordinary technical advances have enabled the management of high-risk pregnancies so that both the mother and the fetus have positive outcomes. Various tests can be used prenatally to assess the well-being of the fetus. Nursing responsibilities during the assessment of fetal health include preparing the patient properly, explaining the reason for the test, and clarifying and interpreting results in collaboration with other health care providers. The nurse can provide the psychosocial support that will allay or reduce parental anxiety. Figure 5-1 shows amniocentesis, and Table 5-1 reviews common diagnostic tests that assess the status of the fetus. Fetal assessment techniques used during labor are discussed in Chapter 6.
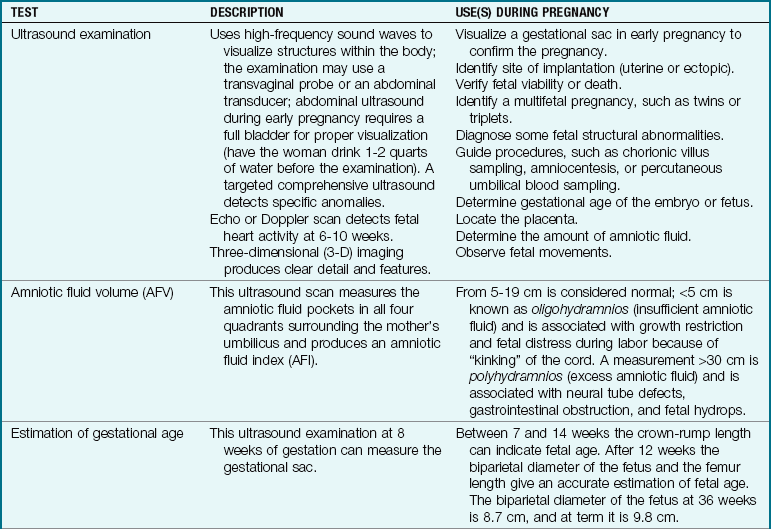
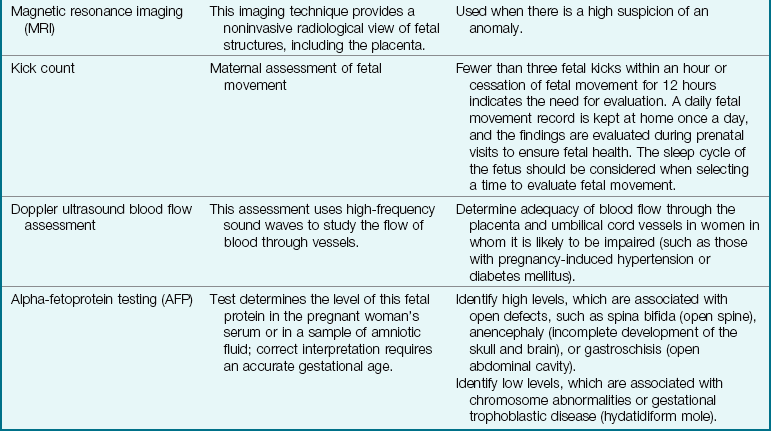
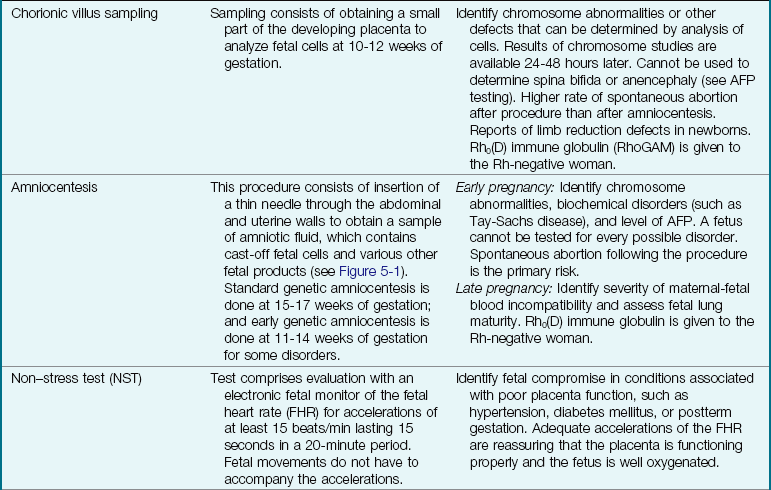
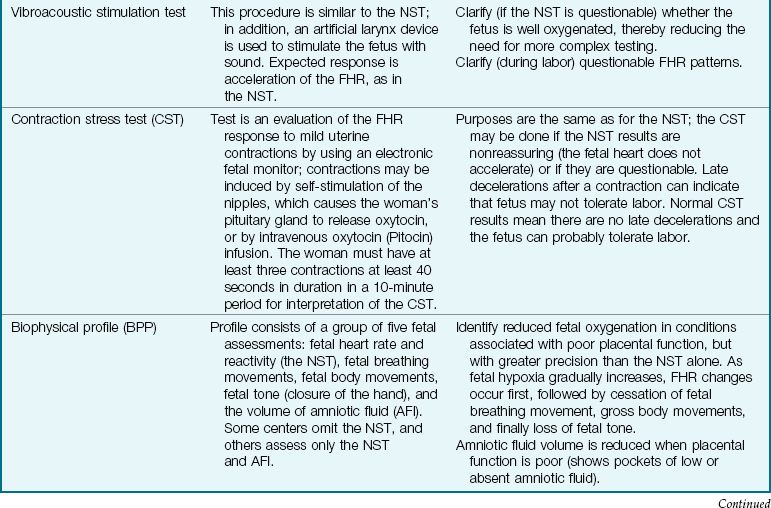
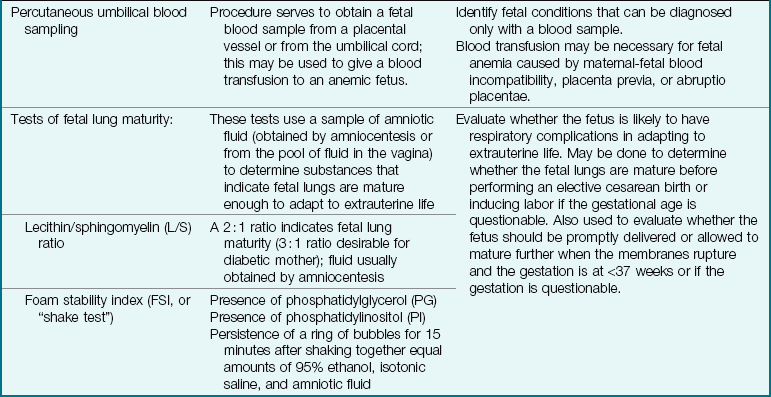
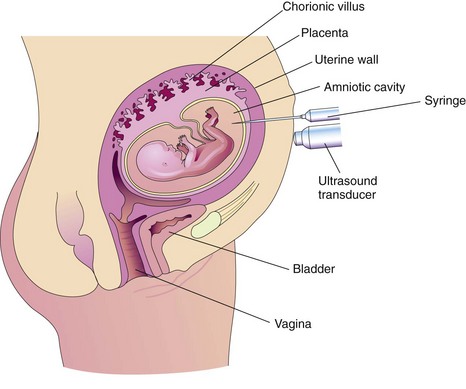
FIGURE 5-1 Amniocentesis. An ultrasound transducer on the abdomen ensures needle placement away from the body of the fetus and the placenta. A needle is inserted into the amniotic cavity, and a sample of amniotic fluid is collected for laboratory examination and fetal assessment.
The future of fetal assessment lies in the continued development of new ultrasound technologies and hand-held receivers. Ultrasound pictures taken by a portable instrument can be transmitted via the Internet to be interpreted by experts in medical centers. Telemedicine, a growing field, is a specialized technology in prenatal care.
Pregnancy-Related Complications
Mild nausea and vomiting are easily managed during pregnancy (see Chapter 4). In contrast, the woman with hyperemesis gravidarum has excessive nausea and vomiting that can significantly interfere with her food intake and fluid balance. Fetal growth may be restricted, resulting in a low-birth-weight infant. Dehydration impairs perfusion of the placenta, reducing the delivery of blood oxygen and nutrients to the fetus.
Manifestations: Hyperemesis gravidarum differs from “morning sickness” of pregnancy in one or more of the following ways:
• Persistent nausea and vomiting, often with complete inability to retain food and fluids
• Dehydration as evidenced by a dry tongue and mucous membranes, decreased turgor (elasticity) of the skin, scant and concentrated urine, and a high serum hematocrit level
• Electrolyte and acid-base imbalances
• Psychological factors such as unusual stress, emotional immaturity, passivity, or ambivalence about the pregnancy
Treatment: The health care provider will rule out other causes for the excessive nausea and vomiting, such as gastroenteritis or liver, gallbladder, or pancreatic disorders, before making this diagnosis. The medical treatment for hyperemesis gravidarum is to correct dehydration and electrolyte or acid-base imbalances with oral or intravenous fluids. Antiemetic drugs may be prescribed after the health care provider informs the woman about any potential risk to the developing fetus. Occasionally, severe cases necessitate total parenteral nutrition. The woman may need hospital admission to correct dehydration and inadequate nutrition if home measures are not successful. The condition is self-limiting in most women, although it is quite distressing to the woman and her family.
Nursing Care: Nursing care focuses on patient teaching, because most care occurs in the home. The woman should be taught how to reduce factors that trigger nausea and vomiting. She should avoid food odors, which may abound in meal preparation areas and tray carts if she is hospitalized. If she becomes nauseated when her food is served, the tray should be removed promptly and offered again later.
Accurate intake and output records are kept to assess fluid balance. Frequent, small amounts of food and fluid keep the stomach from becoming too full, which can trigger vomiting. Easily digested carbohydrates, such as crackers or baked potatoes, are tolerated best. Foods with strong odors should be eliminated from the diet. Taking liquids between solid meals helps to reduce gastric distention. Sitting upright after meals reduces gastric reflux (backflow) into the esophagus.
The emesis basin is kept out of sight so that it is not a visual reminder of vomiting. It should be emptied at once if the woman vomits and the amount documented on the intake and output record.
Stress may contribute to hyperemesis gravidarum; stress may also result from this complication. The nurse should provide support by listening to the woman’s feelings about pregnancy, child rearing, and living with constant nausea. Although psychological factors may play a role in some cases of hyperemesis gravidarum, the nurse should not assume that every woman with this complication is adjusting poorly to her pregnancy.
Bleeding Disorders of Early Pregnancy
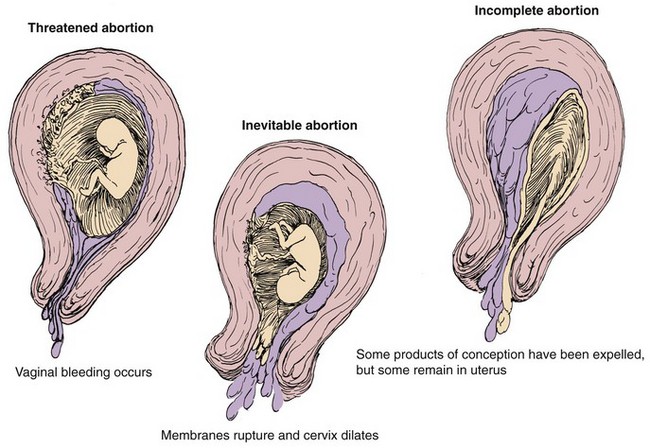
Several bleeding disorders can complicate early pregnancy, such as spontaneous abortion (miscarriage) (Figure 5-2), ectopic pregnancy (see Figure 5-3), or hydatidiform mole (see Figure 5-4). Maternal blood loss decreases the oxygen-carrying capacity of the blood, resulting in fetal hypoxia, and places the fetus at risk.
Abortion
Table 5-2 differentiates types of abortions.
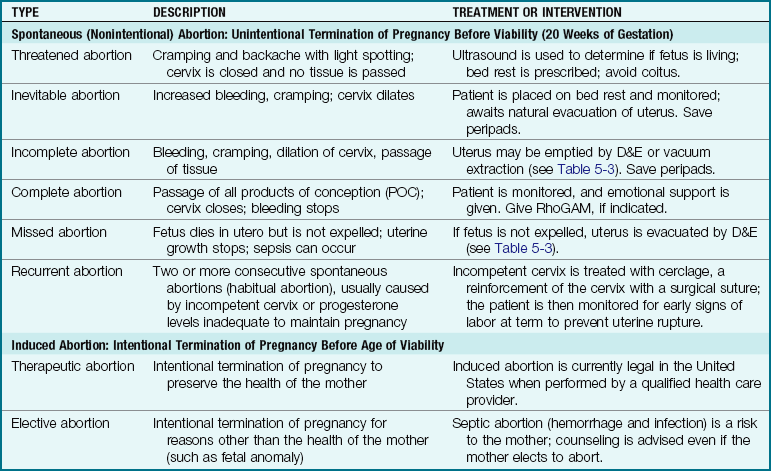
Treatment: Abortion is the spontaneous (miscarriage) or intentional termination of a pregnancy before the age of viability (20 weeks of gestation) (see Table 5-2). When a threatened abortion occurs, efforts are made to keep the fetus in utero until the age of viability. In recurrent pregnancy loss, causes are investigated that could include genetic, immunological, anatomical, endocrine, or infectious factors. Cerclage, or suturing an incompetent cervix that opens when the growing fetus presses against it, is successful in most cases. A low human chorionic gonadotropin (hCG) level or low fetal heart rate by 8 weeks of gestation may be an ominous sign.
Termination of pregnancy after 20 weeks of gestation (age of viability) is called preterm labor and is discussed in Chapter 8. Table 5-3 describes procedures used in pregnancy termination. In all cases of pregnancy loss, counseling of the parent(s) is essential. Even when the mother elects to terminate pregnancy, there are emotional responses that should be recognized and addressed.
Table 5-3
Procedures Used in Pregnancy Termination
| PROCEDURE AND DESCRIPTION | COMMENTS |
| Vacuum aspiration (vacuum curettage): Cervical dilation with metal rods or laminaria (a substance that absorbs water and swells, thus enlarging the cervical opening) followed by controlled suction through a plastic cannula to remove all products of conception (POC) | Used for first-trimester abortions; also used to remove remaining POC after spontaneous abortion; may be followed by curettage (see Dilation and evacuation); paracervical block (local anesthesia of the cervix) or general anesthesia needed; conscious sedation with midazolam (Versed) may be used. |
| Dilation and evacuation (D&E): Dilation of the cervix as in vacuum curettage followed by gentle scraping of the uterine walls to remove POC | Used for first-trimester abortions and to remove all POC after a spontaneous abortion; greater risk of cervical or uterine trauma and excessive blood loss than with vacuum curettage; paracervical block or general anesthesia needed. |
| Mifepristone (RU486) | An oral medication that may be taken until up to 5 weeks of gestation; often used with a prostaglandin agent that causes bleeding and termination of pregnancy within 5 days. |
| Methotrexate | An oral or intramuscular medication given with misoprostol, a prostaglandin analog; applied intravaginally, causes termination of pregnancy within 1 or 2 days. |
| Prostaglandins | Available in gel form or intrauterine injection; can be used in the second trimester to terminate pregnancy; unpleasant side effects can occur. |
| Hypertonic uterine infusion | Causes uterine contractions to occur within 12-24 hours; in early second trimester, drugs such as misoprostol (Cytotec) and oxytocin expedite the process; complications include sepsis and bleeding. |
Oxytocin (Pitocin) controls blood loss before and after curettage, much as the drugs do after term birth. Rh0(D) immune globulin (RhoGAM [300 mcg] or the lower-dose MICRhoGAM [50 mcg]) is given to Rh-negative women after any abortion to prevent the development of antibodies that might harm the fetus during a subsequent pregnancy.
Physical care: The nurse documents the amount and character of bleeding and saves anything that looks like clots or tissue for evaluation by a pathologist. A pad count and an estimate of how saturated each is (e.g., 50%, 75%) documents blood loss most accurately. The woman with threatened abortion who remains at home is taught to report increased bleeding or passage of tissue.
The nurse should check the hospitalized woman’s bleeding and vital signs to identify hypovolemic shock resulting from blood loss. She should not eat (remain NPO) if she has active bleeding to prevent aspiration if anesthesia is required for dilation and evacuation (D&E) treatment. Laboratory tests, such as a hemoglobin level and hematocrit, are ordered.
After vacuum aspiration or curettage, the amount of vaginal bleeding is observed. The blood pressure, pulse, and respirations are checked every 15 minutes for 1 hour, then every 30 minutes until discharge from the postanesthesia care unit. The mother’s temperature is checked on admission to the recovery area and every 4 hours until discharge to monitor for infection.
Most women are discharged directly from the recovery unit to their home after curettage. Guidelines for self-care at home include the following:
• Report increased bleeding. Do not use tampons, which may cause infection.
• Take temperature every 8 hours for 3 days. Report signs of infection (temperature of 38° C [100.4° F] or higher; foul odor or brownish color of vaginal drainage).
• Take an oral iron supplement if prescribed.
• Resume sexual activity as recommended by the health care provider (usually after the bleeding has stopped).
• Return to the health care provider at the recommended time for a checkup and contraception information.
• Pregnancy can occur before the first menstrual period returns after the abortion procedure.
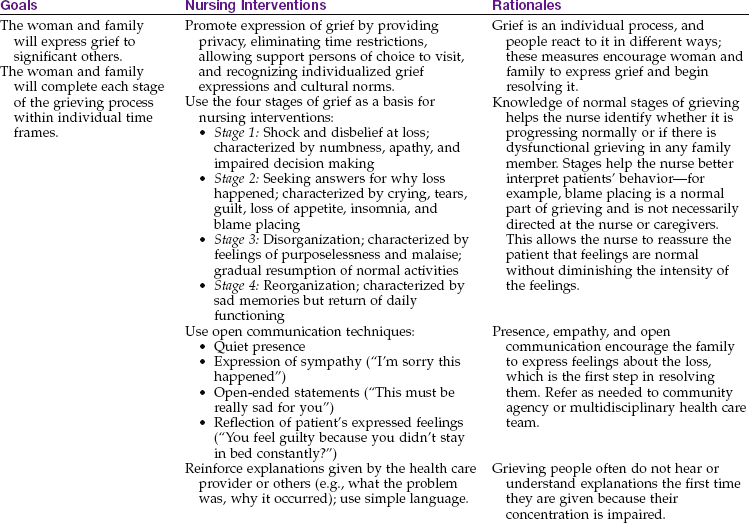
Emotional care: Society often underestimates the emotional distress spontaneous abortion causes the woman and her family. Even if the pregnancy was not planned or not suspected, they often grieve for what might have been. Their grief may last longer and be deeper than they or other people expect. The nurse listens to the woman and acknowledges the grief she and her partner feel. The Communication box gives examples of effective and ineffective techniques for communicating with the family experiencing pregnancy loss. Spiritual support of the family’s choice and community support groups may help the family work through the grief of any pregnancy loss. Nursing Care Plan 5-1 suggests interventions for families experiencing early pregnancy loss.
5-1  Nursing Care Plan
Nursing Care Plan
The Family Experiencing Early Pregnancy Loss
 Communication
Communication
The Family Experiencing Pregnancy Loss
Examples of Ineffective Communication Techniques
Do not give the woman or family any information.
Discourage expressions of sadness; for example, expect the father to be strong for the mother’s sake.
Avoid interacting with the family and talking about their loss.
Act uncomfortable with the family’s expressions of grief.
Minimize the importance of the pregnancy by comments such as “You’re young—you can always have more children”; “At least you didn’t lose a real baby”; “It was for the best; the baby was abnormal”; or “You have another healthy child at home.”
Say, “I know how you feel”; self-disclosure of your similar experience must be used carefully and only if it is likely to be therapeutic to the patient.
Examples of Effective Communication Techniques
Wait quietly with family: “Be there.”
Say, “I’m sorry” or “I’m here if you need to talk.”
Touch (may not be appreciated by some people or in some cultures).
Refer to spontaneous abortion as “miscarriage” rather than the harsher-sounding “abortion.”
Provide mementos as appropriate (lock of hair, photograph, footprint); save keepsakes for later retrieval if the family does not want them immediately.
Alert other hospital personnel to the family’s loss to prevent hurtful comments or questions.
Allow the family to see the fetus if they wish; prepare them for the appearance of the fetus.
Reduce the number of staff with whom the family must interact.
Ectopic Pregnancy
Ectopic pregnancy occurs when the fertilized ovum (zygote) is implanted outside the uterine cavity (Figure 5-3). Of all ectopic pregnancies, 95% occur in the fallopian tube (tubal pregnancy). An obstruction or other abnormality of the tube prevents the zygote from being transported into the uterus. Scarring or deformity of the fallopian tubes or inhibition of normal tubal motion to propel the zygote into the uterus may result from the following:
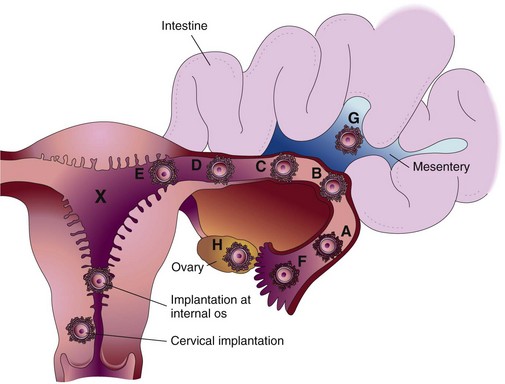
FIGURE 5-3 The uterus and fallopian tubes, illustrating various abnormal implantation sites. A to F are tubal pregnancies (the most common); G is an abdominal pregnancy; and X indicates the wall of the uterus where normal implantation should occur.
Use of an intrauterine device for contraception may contribute to ectopic pregnancy, because these devices promote inflammation within the uterus. A woman who has had a previous tubal pregnancy or a failed tubal ligation is also more likely to have an ectopic pregnancy.
A zygote that is implanted in a fallopian tube cannot survive for long because the blood supply and size of the tube are inadequate. The zygote or embryo may die and be resorbed by the woman’s body, or the tube may rupture with bleeding into the abdominal cavity, creating a surgical emergency.
Manifestations: The woman often complains of lower abdominal pain, sometimes accompanied by light vaginal bleeding. If the tube ruptures, she may have sudden severe lower abdominal pain, vaginal bleeding, and signs of hypovolemic shock (Box 5-1). The amount of vaginal bleeding may be minimal because most blood is lost into the abdomen rather than externally through the vagina. Shoulder pain is a symptom that often accompanies bleeding into the abdomen (referred pain).
Treatment: A sensitive pregnancy test for hCG is done to determine if the woman is pregnant. Trans-vaginal ultrasound examination determines whether the embryo is growing within the uterine cavity. Culdocentesis (puncture of the upper posterior vaginal wall with removal of peritoneal fluid) may occasionally be done to identify blood in the woman’s pelvis, which suggests tubal rupture. A laparoscopic examination may be done to view the damaged tube with an endoscope (lighted instrument for viewing internal organs).
The physician attempts to preserve the tube if the woman wants other children, but this is not always possible. The priority medical treatment is to control blood loss. Blood transfusion may be required for massive hemorrhage. One of the following three courses of treatment is chosen, depending on the gestation and the amount of damage to the fallopian tube:
1. No action is taken if the pregnancy is being resorbed by the woman’s body.
2. Medical therapy with methotrexate (if the tube is not ruptured) inhibits cell division in the embryo and allows it to be resorbed.
3. Surgery to remove the products of conception (POC) from the tube is performed if damage is minimal; severe damage requires removal of the entire tube and occasionally the uterus.
Nursing Care: Nursing care includes observing for hypovolemic shock as in spontaneous abortion. Vaginal bleeding is assessed, although most lost blood may remain in the abdomen. The nurse should report increasing pain, particularly shoulder pain, to the physician.
If the woman has surgery, preoperative and postoperative care is similar to that for other abdominal surgery, as follows:
• Measurement of vital signs to identify hypovolemic shock; of temperature to identify infection
• Assessment of lung and bowel sounds
• Intravenous fluid; blood replacement may be ordered if the loss was substantial
• Pain medication, often with patient-controlled analgesia (PCA) after surgery
• NPO status preoperatively; oral intake usually resumes after surgery, beginning with ice chips and then clear liquids, and it is advanced as bowel sounds resume
• Indwelling Foley catheter as ordered. Urine output is a significant indicator of fluid balance and will fall or stop if the woman hemorrhages; minimum acceptable urine output is 30 mL/hr
• Bed rest before surgery; progressive ambulation postoperatively; the nurse should have adequate assistance when the woman first ambulates because she is more likely to faint if she lost a significant amount of blood
In addition to physical preoperative and postoperative care, the nurse provides emotional support because the woman and her family may experience grieving similar to that accompanying spontaneous abortion. Loss of a fallopian tube threatens future fertility and is another source of grief.
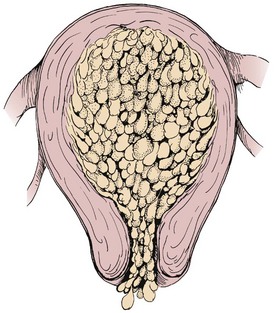
Hydatidiform Mole
Hydatidiform mole (gestational trophoblastic disease; also known as a molar pregnancy) occurs when the chorionic villi (fringelike structures that form the placenta) increase abnormally and develop vesicles (small sacs) that resemble tiny grapes (Figure 5-4). The mole may be complete, with no fetus present, or partial, in which only part of the placenta has the characteristic vesicles. Hydatidiform mole may cause hemorrhage, clotting abnormalities, hypertension, and later development of cancer (choriocarcinoma). Chromosome abnormalities are found in many cases of hydatidiform mole. It is more likely to occur in women at the age extremes of reproductive life, and a woman who has had one molar pregnancy has a 1% chance of another molar pregnancy in the future.
Manifestations: Signs associated with hydatidiform mole appear early in pregnancy and can include the following:
• Bleeding, which may range from spotting to profuse hemorrhage; cramping may be present
• Rapid uterine growth and a uterine size that is larger than expected for the gestation
• Failure to detect fetal heart activity
• Signs of hyperemesis gravidarum (see p. 79)
• Unusually early development of gestational hypertension (see p. 90)
• Higher than expected levels of hCG
• A distinctive “snowstorm” pattern on ultrasound but no evidence of a developing fetus in the uterus
Treatment: The uterus is evacuated by vacuum aspiration and D&E. The level of hCG is tested and retested until it is undetectable, and the levels are followed for at least 1 year. Persistent or rising levels suggest that vesicles remain or that malignant change has occurred. The woman should delay conceiving until follow-up care is complete because a new pregnancy would confuse tests for hCG. Rho(D) immune globulin is prescribed for the Rh-negative woman.
Nursing Care: The nurse observes for bleeding and shock; care is similar to that given in spontaneous abortion and ectopic pregnancy. If the woman also experiences hyperemesis or preeclampsia, the nurse incorporates care related to those conditions as well. The woman has also lost a pregnancy, so the nurse should provide care related to grieving, similar to that for a spontaneous abortion. The need to delay another pregnancy may be a concern if the woman is nearing the end of her reproductive life and wants a child; therefore the need for follow-up examinations is reinforced. The woman is encouraged and taught how to use contraception (see Chapter 11).
Bleeding Disorders of Late Pregnancy
Bleeding in late pregnancy is often caused by placenta previa or abruptio placentae (Table 5-4).
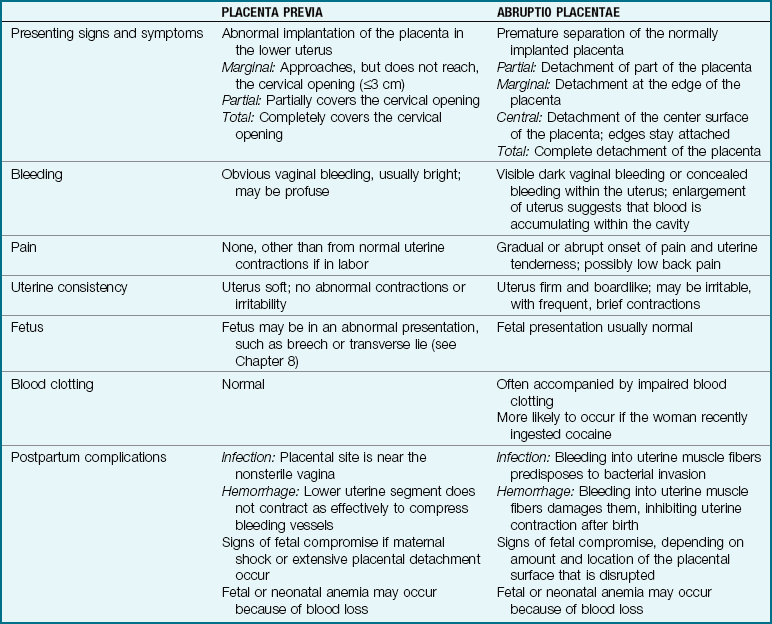
Placenta Previa
Placenta previa occurs when the placenta develops in the lower part of the uterus rather than the upper. There are three degrees of placenta previa, depending on the location of the placenta in relation to the cervix (Figure 5-5, A), as follows:
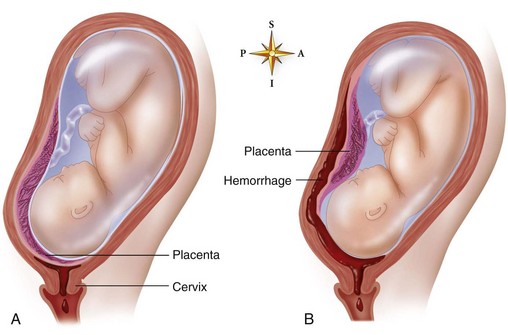
FIGURE 5-5 Placenta previa and abruptio placentae. A, Placenta previa. The placenta (purple in this illustration) is implanted low in the uterus. Detachment of the placenta from the uterine wall occurs as the cervix dilates, resulting in bleeding. B, Abruptio placentae. The placenta (purple) is implanted normally in the uterus but separates from the uterine wall. If the fetal head is engaged, bleeding (red in this illustration) may accumulate in the uterus instead of being expelled externally.
Marginal: Placenta reaches within 2 to 3 cm of the cervical opening
A low-lying placenta is implanted near the cervix but does not cover any of the opening. This variation is not a true placenta previa and may or may not be accompanied by bleeding. The low-lying placenta may be discovered during a routine ultrasound examination in early pregnancy. It also may be diagnosed during late pregnancy because the woman has signs similar to those of a true placenta previa.
Manifestations: Painless vaginal bleeding, usually bright red, is the main characteristic of placenta previa. The woman’s risk of hemorrhage increases as term approaches and the cervix begins to efface (thin) and dilate (open). These normal prelabor changes disrupt the placental attachment. The fetus is often in an abnormal presentation (e.g., breech or transverse lie) because the placenta occupies the lower uterus, which often prevents the fetus from assuming the normal head-down presentation.
The fetus or neonate may have anemia or hypovolemic shock because some of the blood lost may be fetal blood. Fetal hypoxia may occur if a large disruption of the placental surface reduces the transfer of oxygen and nutrients.
The woman with placenta previa is more likely than others to have an infection or hemorrhage after birth for the following reasons:
• Infection is more likely to occur because vaginal organisms can easily reach the placental site, which is a good growth medium for microorganisms.
• Postpartum hemorrhage may occur because the lower segment of the uterus, where the placenta was attached, has fewer muscle fibers than the upper uterus. The resulting weak contraction of the lower uterus does not compress the open blood vessels at the placental site as effectively as would the upper segment of the uterus.
Treatment: Medical care depends on the length of gestation and the amount of bleeding. The goal is to maintain the pregnancy until the fetal lungs are mature enough that respiratory distress is less likely (at about 34 weeks of gestation). Delivery will be done if bleeding is sufficient to jeopardize the mother or fetus, regardless of gestational age.
The woman should lie on her side or have a pillow under one hip to avoid supine hypotension. If bleeding is extensive or the gestation is near term, a cesarean section is performed for partial or total placenta previa. The woman with a low-lying placenta or marginal placenta previa may be able to deliver vaginally unless the blood loss is excessive.
Nursing Care: The priorities of nursing care include observation of vaginal blood loss and of signs and symptoms of shock. Vital signs are taken every 15 minutes if the woman is actively bleeding, and oxygen is often given to increase the amount delivered to the fetus. Vaginal examination is not done because it may precipitate bleeding if the placental attachment is disrupted. The fetal heart rate is monitored continuously. The nurse implements care for a cesarean delivery, as needed (see Chapter 8). The parents of the infant are often fearful for their child, particularly if a preterm delivery is required. Supportive care should be given.
Abruptio Placentae
Abruptio placentae is the premature separation of a placenta that is normally implanted. Predisposing factors include the following:
• Cigarette smoking and poor nutrition
• Blows to the abdomen, such as might occur in battering or accidental trauma
Abruptio placentae may be partial or total (see Figure 5-5, B); it may be marginal (separating at the edges) or central (separating in the middle). Bleeding may be visible or concealed behind the partially attached placenta.
 Nursing Tip
Nursing Tip
Pain is an important symptom that distinguishes abruptio placentae from placenta previa.
Manifestations: Bleeding accompanied by abdominal or low back pain is the typical characteristic of abruptio placentae. Unlike the bleeding in placenta previa, most or all of the bleeding may be concealed behind the placenta. Obvious dark-red vaginal bleeding occurs when blood leaks past the edge of the placenta. The woman’s uterus is tender and unusually firm (boardlike) because blood leaks into its muscle fibers. Frequent, cramplike uterine contractions often occur (uterine irritability).
The fetus may or may not have problems, depending on how much placental surface is disrupted. As in placenta previa, some of the blood lost may be fetal, and the fetus or neonate may have anemia or hypovolemic shock.
Disseminated intravascular coagulation (DIC) is a complex disorder that may complicate abruptio placentae. The large blood clot that forms behind the placenta consumes clotting factors, which leaves the rest of the mother’s body deficient in these factors. Clot formation and anticoagulation (destruction of clots) occur simultaneously throughout the body in the woman with DIC. She may bleed from her mouth, nose, incisions, or venipuncture sites because the clotting factors are depleted.
Postpartum hemorrhage may also occur because the injured uterine muscle does not contract effectively to control blood loss. Infection is more likely to occur because the damaged tissue is susceptible to microbial invasion.
Treatment: The treatment of choice, immediate cesarean delivery, is done because of the risk for maternal shock, clotting disorders, and fetal death. Blood and clotting factor replacement may be needed because of DIC. The mother’s clotting action quickly returns to normal after birth because the source of the abnormality is removed.
Nursing Care: Preparation for cesarean section and close monitoring of vital signs and fetal heart are essential. Signs of shock and bleeding from the nose, the gums, or other unexpected sites should be promptly reported. Rapid increase in the size of the uterus suggests that blood is accumulating within it. The uterus is usually very tender and hard. Nursing care after delivery is similar to that with placenta previa.
The fetus sometimes dies before delivery. See Nursing Care Plan 5-1 for nursing care related to fetal death (stillbirth) and support of the grieving family. Many therapeutic communication techniques outlined in the Communication box on p. 85 are appropriate. The care of a pregnant woman with excessive bleeding is summarized in Box 5-2.
Hypertension During Pregnancy
Hypertension may exist before pregnancy (chronic hypertension), but often it develops as a pregnancy complication (gestational hypertension [GH], formerly known as pregnancy-induced hypertension [PIH]). Table 5-5 compares the different types of hypertension during pregnancy. The term preeclampsia may be used when GH includes proteinuria. Preeclampsia progresses to eclampsia when convulsions occur. One sometimes hears the term toxemia, an old term for GH.
Table 5-5
Hypertensive Disorders of Pregnancy
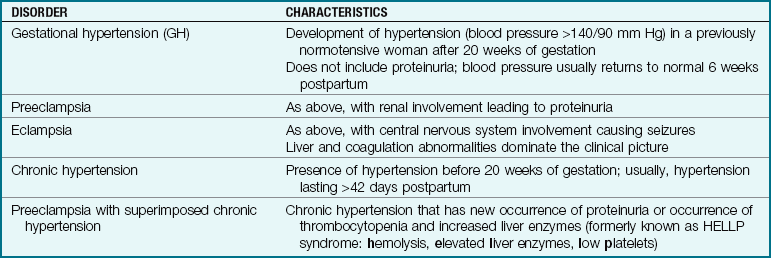
Modified from American College of Obstetricians and Gynecologists. (2006). Diagnosis and management of preeclampsia. ACOG Practice Bulletin #33, Washington, DC; and National Institutes of Health, 2001.
The cause of GH is unknown, but birth is its cure. It usually develops after the twentieth week of gestation. Vasospasm (spasm of the arteries) is the main characteristic of GH. Although the cause is unknown, any of several risk factors increases a woman’s chance of developing GH (Box 5-3).
There has been a gradual increase in the number of women delaying pregnancy until over age 30 years, and the chances of chronic hypertension complicating pregnancy has increased. Chronic hypertension is considered moderate if the systolic reading is between 140 and 160 mm Hg and the diastolic reading is below 110 mm Hg. However, an increase over baseline blood pressure of 30 mm Hg or more systolic and 15 mm Hg diastolic will place the woman in a high-risk category. Therefore a woman with a baseline blood pressure that is normally low, such as 90/60 mm Hg, may be at risk for GH if her blood pressure rises to 120/80 mm Hg (Creasy et al., 2009). Blood pressure normally decreases during the first two trimesters.
Hypertension is closely related to the development of complications, such as abruptio placentae, fetal growth restriction, preeclampsia, prematurity, and stillbirth, so special care of the pregnant woman with hypertension is essential. The approach to chronic hypertension during pregnancy is complex because many drugs used to treat hypertension, such as atenolol, cause a drop in mean arterial blood pressure and can result in restricted fetal growth and other problems. For this reason, antihypertensive medication is not given for mild to moderate levels of high blood pressure. Instead, frequent prenatal visits, urinalysis to detect proteinuria, and fetal assessments are the standards of care, and medication is started if the blood pressure exceeds the moderate range. Drugs of choice include methyldopa (Aldomet), alpha-adrenergic and beta-adrenergic blockers (labetalol), and calcium channel blockers (nifedipine) in some cases of hypertensive crisis.
Manifestations of Gestational Hypertension: Vasospasm impedes blood flow to the mother’s organs and placenta, resulting in one or more of these signs: (1) hypertension, (2) edema, and (3) proteinuria (protein in the urine). Severe GH can also affect the central nervous system, eyes, urinary tract, liver, gastrointestinal system, and blood clotting function. Table 5-6 summarizes laboratory tests that aid in diagnosis.
Table 5-6
Laboratory Tests for Patients with Gestational Hypertension
| TEST | RATIONALE |
| Hemoglobin and hematocrit | Detects hemoconcentration for indication of severity of gestational hypertension (GH) |
| Platelets | Thrombocytopenia suggests GH |
| Urine for protein | Proteinuria confirms GH when hypotension is present |
| Serum creatinine | Elevated creatinine and oliguria suggest GH |
| Serum uric acid | Elevated uric acid suggests GH |
| Serum transaminase | Elevated transaminase confirms liver involvement in GH |
Modified from National High Blood Pressure Education Program. (2001). Working group on high blood pressure in pregnancy. Contemporary Obstetrics and Gynecology, 46(2), 22.
Hypertension: Despite an increase in blood volume and cardiac output, most pregnant women do not experience a rise in blood pressure because they have a resistance to factors that cause vasoconstriction. In addition, the resistance to blood flow in their vessels (peripheral vascular resistance) decreases because of the effects of hormonal changes. A blood pressure of 140/90 mm Hg or above is considered to constitute hypertension in pregnancy.
Edema: Edema can occur because fluid leaves the blood vessels and enters the tissues. Although total body fluid is increased, the amount within the blood vessels is reduced (hypovolemia), further decreasing blood flow to the maternal organs and placenta. It is likely to be the first sign the woman notices but is not essential to the diagnosis.
Sudden excessive weight gain is the first sign of fluid retention. Visible edema follows the weight gain. Edema of the feet and legs is common during pregnancy, but edema above the waist suggests GH. The woman may notice facial swelling or may stop wearing rings because they are hard to remove. Edema is severe if a depression remains after the tissue is compressed briefly with the finger (“pitting”).
Edema resolves quickly after birth as excess tissue fluid returns to the circulation and is excreted in the urine. Urine output may reach 6 L/day and often exceeds fluid intake.
Other Manifestations of Preeclampsia: Other signs and symptoms occur with severe preeclampsia. All are related to decreased blood flow and edema of the organs involved.
Central nervous system: A severe, unrelenting headache may occur because of brain edema and small cerebral hemorrhages. The severe headache often precedes a convulsion. Deep tendon reflexes become hyperactive because of central nervous system irritability.
Eyes: Visual disturbances such as blurred or double vision or “spots before the eyes” occur because of arterial spasm and edema surrounding the retina. Visual disturbances often precede a convulsion.
Urinary tract: Decreased blood flow to the kidneys reduces urine production and worsens hypertension.
Gastrointestinal system and liver: Epigastric pain or nausea occurs because of liver edema, ischemia, and necrosis and often precedes a convulsion. Liver enzyme levels are elevated because of reduced circulation, edema, and small hemorrhages.
Blood clotting: HELLP syndrome is a variant of GH that involves hemolysis (breakage of erythrocytes), elevated liver enzymes, and low platelets. Hemolysis occurs as erythrocytes break up when passing through small blood vessels damaged by the hypertension. Obstruction of hepatic blood flow causes the liver enzyme levels to become elevated. Low platelet levels occur when the platelets gather at the site of blood vessel damage, reducing the number available in the general circulation. Low platelet levels cause abnormal blood clotting.
Eclampsia: Progression to eclampsia occurs when the woman has one or more generalized tonic-clonic seizures. Facial muscles twitch; this sign is followed by generalized contraction of all muscles (tonic phase), then alternate contraction and relaxation of the muscles (clonic phase). An eclamptic seizure may result in cerebral hemorrhage, abruptio placentae, fetal compromise, or death of the mother or fetus.
Effects on the Fetus: GH reduces maternal blood and nutrition flow through the placenta and decreases the oxygen available to the fetus. Fetal hypoxia may result in meconium (first stool) passage into the amniotic fluid or in fetal distress. The fetus may have intrauterine growth restriction and at birth may be long and thin with peeling skin if the reduced placental blood flow has been prolonged. Fetal death sometimes occurs.
Treatment: Medical care focuses on prevention and early detection of GH. Drugs are sometimes needed to prevent convulsions and to reduce a dangerously high blood pressure.
Prevention: Correction of some risk factors reduces the risk for GH. For example, improving the diet, particularly of the pregnant adolescent, may prevent GH and promote normal fetal growth. Other risk factors, such as family history, cannot be changed. Early and regular prenatal care allows GH to be diagnosed promptly so that it is more effectively managed.
Management: Treatment of GH depends on the severity of the hypertension and on the maturity of the fetus. Treatment focuses on (1) maintaining blood flow to the woman’s vital organs and the placenta, and (2) preventing convulsions. Birth is the cure for GH. If the fetus is mature, pregnancy is ended by labor induction or cesarean birth. If GH is severe, the fetus is often in greater danger from being in the uterus than from being born prematurely.
Some women with mild GH can be managed at home if they can comply with treatment and if home nursing visits are possible. If the woman has severe GH or cannot comply with treatment, or if home nursing visits are not available, she is usually admitted to the hospital. Conservative treatment, whether at home or in the hospital, includes the following:
• Activity restriction to allow blood that would be circulated to skeletal muscles to be conserved for circulation to the mother’s vital organs and the placenta. The woman should remain on bed rest on her side to improve blood flow to the placenta.
• Maternal assessment of fetal activity (“kick counts”). She should report a decrease in movements or if none occur during a 4-hour period.
• Blood pressure monitoring two to four times per day in the same arm and in the same position. A family member must be taught the technique if the woman can safely remain at home.
• Daily weight measurement on the same scale, in the same type of clothing, and at the same time of day to observe for sudden weight gain.
• Checking urine for protein with a dipstick using a first-voided, clean-catch specimen.
 Home Care Considerations
Home Care Considerations
Hypertension in Pregnancy
Patient teaching for home care should include the following:
• Exercise may have to be curtailed
• Discontinue smoking and alcohol use
• Primary management is without drugs since blood pressure normally falls in the first two trimesters of pregnancy
• Daily blood pressure measurement
• Daily urine dipstick for protein
• Monitor fetal kicks and uterine activity
• Balanced diet with sufficient protein to replace loss
Diuretics and sodium restriction are not prescribed for GH. They are not effective for the treatment of GH and may aggravate it because they further deplete the woman’s blood volume. Aspirin therapy or dietary supplements such as calcium have not been shown to be helpful in managing GH. The intake of high-salt foods is discouraged. The woman’s diet should have adequate calories and protein (see Chapter 4 for prenatal dietary guidelines). See Table 5-1 for fetal assessment tests that may be done.
Drug therapy: Several drugs may also be used to treat GH, as described in the following sections. Magnesium sulfate is an anticonvulsant given to prevent seizures. It also may slightly reduce the blood pressure, but its main purpose is as an anticonvulsant. It is usually given by intravenous infusion (controlled with an infusion pump). Administration continues for at least 12 to 24 hours after birth because the woman remains at risk for seizures.
Magnesium is excreted by the kidneys. Poor urine output (less than 30 mL/hr) may allow serum levels of magnesium to reach toxic levels. Excess magnesium first causes loss of the deep tendon reflexes, which is followed by depression of respirations; if levels continue to rise, collapse and death can occur. Calcium gluconate reverses the effects of magnesium and should be available for immediate use when a woman receives magnesium sulfate.
The therapeutic serum level of magnesium is 4 to 8 mg/dL, which would be an abnormal level in a person not receiving this therapy. The woman with this serum level is slightly drowsy but retains all her reflexes and has normal respiratory function; the level is high enough to prevent convulsions.
Magnesium inhibits uterine contractions. Most women receiving the drug must also receive oxytocin to strengthen labor contractions (see Chapter 8). They are at increased risk for postpartum hemorrhage because the uterus does not contract firmly on bleeding vessels after birth. This contraction-inhibiting effect of magnesium makes it useful to stop preterm labor. The nurse should alert the newborn nursery staff when magnesium sulfate has been administered during labor, because if the newborn is treated with aminoglycosides (such as kanamycin [Kantrex] or neomycin), an interaction can occur and result in paralysis of the newborn.
Antihypertensive drugs are used to reduce blood pressure when it reaches a level that might cause intracranial bleeding, usually higher than 160/100 mm Hg. Severe hypertension can harm the fetus by causing abruptio placentae or placental infarcts (death of placental tissue). The goal of antihypertensive therapy is a gradual reduction of blood pressure to normal levels. The nurse should observe for untoward signs such as sudden hypotension. Hydralazine and labetalol are the drugs most often used. Nifedipine is not currently approved by the Food and Drug Administration (FDA) for hypertensive control. Sodium nitroprusside may be used in hypertensive crisis, but prolonged use can cause fetal complications.
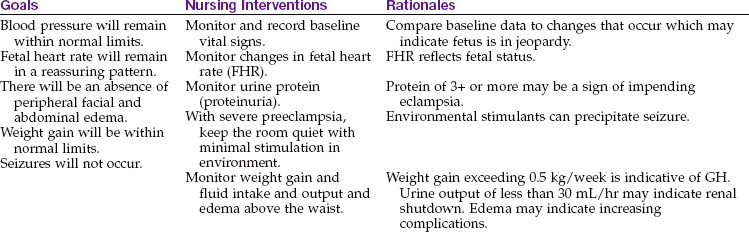
Nursing Care: Nursing care focuses on (1) assisting women to obtain prenatal care, (2) helping them cope with therapy, (3) caring for acutely ill women, and (4) administering medications. Nursing Care Plan 5-2 gives common interventions for women with GH.
5-2 Nursing Care Plan
The Woman with Gestational Hypertension
A woman is admitted with signs of mild gestational hypertension (GH), and plans are made for discharge to the home with careful follow-up. The woman asks what she can do to avoid further complications and problems.
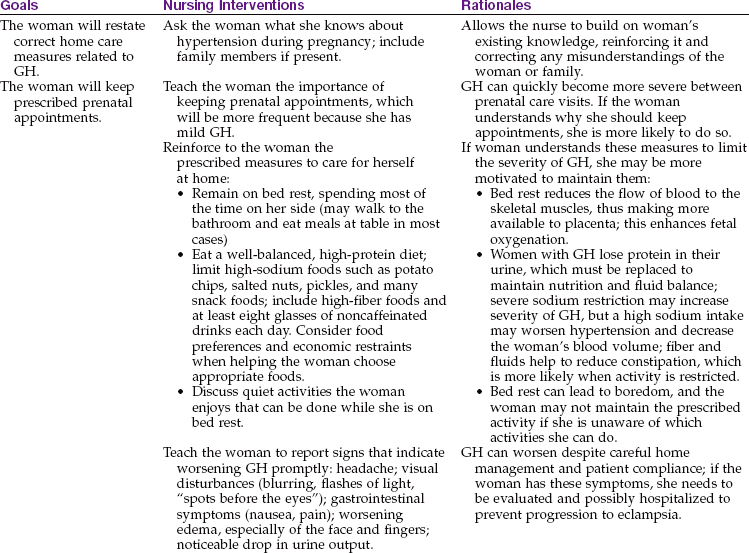
Effective therapeutic regimen management related to GH
1. A woman in the prenatal clinic states that high blood pressure runs in her family, and she has been taking medication for a slightly elevated blood pressure for many years. She states she has had most success with the medication she is currently taking (atenolol) and would like to continue this regimen during her pregnancy. What is the best response of the nurse?
2. In developing a teaching plan for a woman with GH, what factors must be considered and included in the plan?
Promoting prenatal care: Nurses can promote awareness of how prenatal care allows risk identification and early intervention if complications arise. Nurses can help the woman to feel like an individual—especially in busy clinics, which often seem impersonal—thus encouraging her to return regularly.
Helping to cope with therapy: Daily weight measurements identify sudden weight gain that precedes visible edema. The weight should be checked early in the morning and after urination, and with the woman wearing similar clothes each day. The nurse helps the woman to understand the importance of bed rest and to find ways to manage it. Activity diverts blood from the placenta, reducing the infant’s oxygen supply, so the nurse must impress upon the woman how important rest is to her child’s well-being. Positioning the patient on her side during bed rest helps to improve blood flow to the placenta and more effectively provides oxygen and nutrients to the fetus. See the discussion of preterm labor (Chapter 8) for more information about care related to bed rest.
Caring for the acutely ill woman: The acutely ill woman requires intensive nursing care directed by an experienced registered nurse. A quiet, low-light environment reduces the risk of seizures. The woman should remain on bed rest on her side, often the left side, to promote maximum fetal oxygenation. Side rails should be padded and raised to prevent injury if a convulsion occurs. Stimulation such as loud noises or bumping of the bed should be avoided. Visitors are limited, usually to one or two support persons. Suction equipment is available for immediate use.
If a seizure occurs, the nursing focus is to prevent injury and restore oxygenation to the mother and fetus. If the woman is not already on her side, the nurse should try to turn her before the seizure begins. The nurse does not forcibly hold the woman’s body but protects her from injury caused by striking hard surfaces.
Breathing can stop during a seizure. An oral airway, inserted after the seizure, facilitates breathing and suctioning of secretions. Aspiration of secretions can occur during a seizure, so the health care provider may order chest radiographs and arterial blood gas measurements. Oxygen by face mask improves fetal oxygenation. The woman is reoriented to the environment when she regains consciousness. Labor may progress rapidly after a seizure, often while the woman is still drowsy, and the fetus is monitored continuously (see Chapter 6 for signs of impending birth).
Administering medications: Magnesium sulfate is administered by an experienced registered nurse. A licensed practical nurse or licensed vocational nurse (LPN/LVN) may assist. Hospital protocols provide specific guidelines for care when magnesium sulfate is given. Common protocols include the following:
• Blood pressure, pulse, respirations recorded hourly
• Temperature recorded every 4 hours
• Deep tendon reflexes checked every 1 to 4 hours
• Intake and output recorded (often hourly); an indwelling Foley catheter may be ordered
• Urine protein checked with a reagent strip (dipstick) at each voiding
• Laboratory blood levels of magnesium ordered every 4 hours
Deterioration of the maternal or fetal condition is promptly reported. Signs and symptoms of deterioration include the following:
• Increasing hypertension, particularly if blood pressure is 160/100 mm Hg or higher
• Signs of central nervous system irritability, such as facial twitching or hyperactive deep tendon reflexes
• Decreased urine output, especially if less than 25 mL/hr
• Symptoms such as severe headache, visual disturbances, or epigastric pain, which often immediately precede a convulsion
The registered nurse reports the following signs of possible magnesium toxicity, or factors that may cause magnesium toxicity, to the physician and prepares calcium gluconate to reverse this toxicity:
Providing postpartum care: GH is of concern to the prenatal patient and the fetus and continues to be a threat in the postpartum period. Women with chronic hypertension are at risk for pulmonary edema, renal failure, and convulsions. Close monitoring for 48 hours after delivery is essential. Patients requiring antihypertensive drugs postpartum who are breastfeeding are usually given methyldopa or labetalol. Other antihypertensive drugs may have adverse effects on the breastfeeding infant. Diuretics decrease milk production and are generally not administered.
Blood Incompatibility Between the Pregnant Woman and the Fetus
The placenta allows maternal and fetal blood to be close enough to exchange oxygen and waste products without actually mixing (see Chapter 3). However, small leaks that allow fetal blood to enter the mother’s circulation may occur during pregnancy or when the placenta detaches at birth. No problem occurs if maternal and fetal blood types are compatible. However, if the maternal and fetal blood factors differ, the mother’s body will produce antibodies to destroy the foreign fetal red blood cells (RBCs, or erythrocytes). These antibodies will pass through the placenta to the fetus and destroy the Rh-positive blood cells in the fetus.
Rh and ABO Incompatibility
The Rh-negative blood type is an autosomal recessive trait, which means that a person must receive a gene for this characteristic from both parents. The Rh-positive blood type is a dominant trait. The Rh-positive person may have inherited two Rh-positive genes or may have one Rh-positive and one Rh-negative gene. This explains why two Rh-positive parents can conceive a child who is Rh-negative.
People either have the Rh blood factor on their erythrocytes or they do not. If they have the factor, they are Rh positive; if not, they are Rh negative. An Rh-positive person can receive Rh-negative blood with no untoward effects (if all other factors are compatible) because in Rh-negative blood this factor is absent. However, the reverse is not true—Rh incompatibility between the woman and fetus can occur only if the woman is Rh negative and the fetus is Rh positive.
A person with Rh-negative blood is not born with antibodies against the Rh factor. However, exposure to Rh-positive blood causes the person to make antibodies to destroy Rh-positive erythrocytes. The antibodies remain ready to destroy any future Rh-positive erythrocytes that enter the circulation (sensitization).
If fetal Rh-positive blood leaks into the Rh-negative mother’s circulation, her body may respond by making antibodies to destroy the Rh-positive erythrocytes. This process is called isoimmunization. Because this leakage usually occurs at birth, the first Rh-positive child is rarely seriously affected. However, the woman’s blood levels of antibodies increase rapidly each time she is exposed to more Rh-positive blood (in subsequent pregnancies with Rh-positive fetuses). Antibodies against Rh-positive blood cross the placenta and destroy the fetal Rh-positive erythrocytes before the infant is born. A similar response occurs with ABO incompatibility when the mother is type O and the infant’s blood type is type A or type B.
Manifestations: The woman has no obvious effects if her body produces anti-Rh antibodies. Increased levels of these antibodies in her blood are revealed by rising antibody titers in laboratory tests. Fetal Rh status can now also be determined by a newer, noninvasive DNA testing of maternal plasma (Moise, 2005a). When these maternal anti-Rh antibodies cross the placenta and destroy fetal erythrocytes, erythroblastosis fetalis results (Figure 5-6). The effect on the newborn is discussed in Chapter 14.
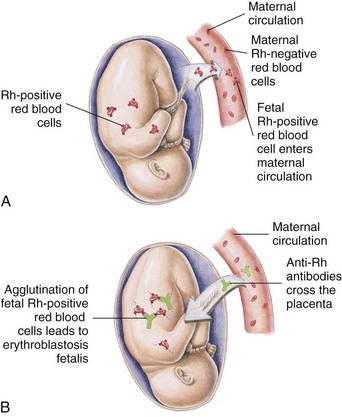
FIGURE 5-6 Erythroblastosis fetalis. A, A few fetal Rh-positive red blood cells enter the circulation of the Rh-negative mother during pregnancy or at birth, causing the mother to produce antibodies against Rh-positive blood cells. B, The Rh-positive antibodies from the maternal circulation cross the placenta, enter the fetal circulation, and destroy fetal Rh-positive blood cells.
Treatment and Nursing Care: The primary management is to prevent the manufacture of anti-Rh antibodies by giving Rho(D) immune globulin (RhoGAM) to the Rh-negative woman at 28 weeks of gestation and within 72 hours after birth of an Rh-positive infant or abortion (see Chapter 14). It is also given after amniocentesis and to women who experience bleeding during pregnancy, because fetal blood may leak into the mother’s circulation at these times. If the fetal blood type is unknown (as with abortion), Rho(D) immune globulin is given to the Rh-negative mother. Rho(D) immune globulin has greatly decreased the incidence of infants with Rh-incompatibility problems. However, some women are still sensitized, usually because they did not receive Rho(D) immune globulin after childbirth or abortion. Rho(D) immune globulin will not be effective if sensitization has already occurred.
Nursing Tip
Most cases of Rh incompatibility between an Rh-negative mother and an Rh-positive fetus can be prevented with the administration of Rh0(D) immune globulin (RhoGAM) in every case in which it is indicated.
The woman who is sensitized to destroy Rh-positive blood cells is carefully monitored during pregnancy to determine if too many fetal erythrocytes are being destroyed. Several fetal assessment tests may be used, including the Coombs’ test, amniocentesis, or percutaneous umbilical blood sampling (see Table 5-1).
An intrauterine transfusion may be done for the severely anemic fetus. The Rh factor should be documented on the chart and the health care provider notified if the woman is Rh negative. See Chapter 14 for the effect of Rh and ABO incompatibility on the newborn.
Pregnancy Complicated by Medical Conditions
Health problems that are present before pregnancy can influence the outcome of pregnancy and necessitate special management. Chronic health problems discussed in this section include diabetes mellitus, heart disease, anemia, and infections.
Diabetes Mellitus
Diabetes mellitus (DM) can be classified according to whether it preceded pregnancy or had its onset during pregnancy. Types of DM include the following:
• Type 1 diabetes mellitus: Usually caused by a pathological disorder of the pancreas resulting in an insulin deficiency
• Type 2 diabetes mellitus: Usually caused by insulin resistance; usually has a strong genetic predisposition
• Pregestational diabetes mellitus: Type 1 or 2 diabetes that existed before pregnancy occurred
• Gestational diabetes mellitus (GDM): glucose intolerance with onset during pregnancy. In true GDM, glucose usually returns to normal by 6 weeks postpartum.
Consult a medical-surgical nursing text for a more detailed discussion of diabetes mellitus in the nonpregnant person.
Pathophysiology
Diabetes mellitus is a disorder in which there is inadequate insulin to move glucose from the blood into body cells. It occurs because the pancreas produces no insulin or insufficient insulin, or because cells resist the effects of insulin. Essentially, cells starve because they cannot obtain glucose. To compensate, the body metabolizes protein and fat for energy, which causes ketones and acids to accumulate (ketoacidosis). The person loses weight despite eating large amounts of food (polyphagia). Fatigue and lethargy accompany cell starvation. To dilute excess glucose in the blood, thirst increases (polydipsia), and fluid moves from the tissues into the blood. This results in tissue dehydration and the excretion of large amounts (polyuria) of glucose-bearing urine (glycosuria).
Effect of Pregnancy on Glucose Metabolism
Pregnancy affects a woman’s metabolism (whether or not she has DM) to make ample glucose available to the growing fetus. Hormones (estrogen and progesterone), an enzyme (insulinase) produced by the placenta, and increased prolactin levels have two effects:
Most women respond to these changes by secreting extra insulin to maintain normal carbohydrate metabolism while still providing plenty of glucose for the fetus. If the woman cannot increase her insulin production, she will have periods of hyperglycemia (increased blood glucose levels) as glucose accumulates in the blood. Because the fetus continuously draws glucose from the mother, maternal hypoglycemia (low blood glucose) can occur between meals and during the night. There is also a normally increased tissue resistance to maternal insulin action in the second and third trimesters, and the fetus is then at risk for organ damage resulting from hyperglycemia.
Preexisting Diabetes Mellitus
Women who are diabetic before pregnancy must alter the management of their condition. The time of major risk for congenital anomalies to occur from maternal hyperglycemia is during the embryonic period of development, in the first trimester. Therefore, women who are diabetic before pregnancy have a greater risk of having a newborn with a congenital anomaly than a woman who develops gestational diabetes, which is usually manifested after the first trimester. With careful management, most diabetic women can have successful pregnancies and healthy babies. Nevertheless, there are many potential complications of diabetes (Box 5-4).
Gestational Diabetes Mellitus
Gestational diabetes mellitus (GDM) is common and resolves quickly after birth; however, some women who experience GDM develop overt diabetes later in life. The following factors in a woman’s history are linked to gestational diabetes (ACOG, 2006b):
• Maternal obesity (>90 kg or 198 lb)
• Large infant (>4000 g or about 9 lb [Figure 5-7], macrosomia)
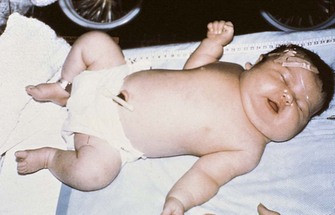
FIGURE 5-7 Macrosomic infant. A newborn with macrosomia caused by maternal diabetes mellitus during pregnancy. This infant weighed 5 kg (11 lb) at birth. Newborns with macrosomia often have respiratory and other problems.
• Maternal age older than 25 years
• Previous unexplained stillbirth or infant having congenital abnormalities
• History of GDM in a previous pregnancy
• Fasting glucose over 126 mg/dL or postmeal glucose over 200 mg/dL
Nursing Care Plan 5-3 lists specific interventions for the pregnant woman with GDM.
5-3 Nursing Care Plan
The Pregnant Woman with Gestational Diabetes Mellitus
A woman, para 0, gravida 1, is diagnosed with gestational diabetes mellitus (GDM). She states that she has no diabetes in her family history and has never been on any type of restricted diet. She is discharged to receive home care and close follow-up.
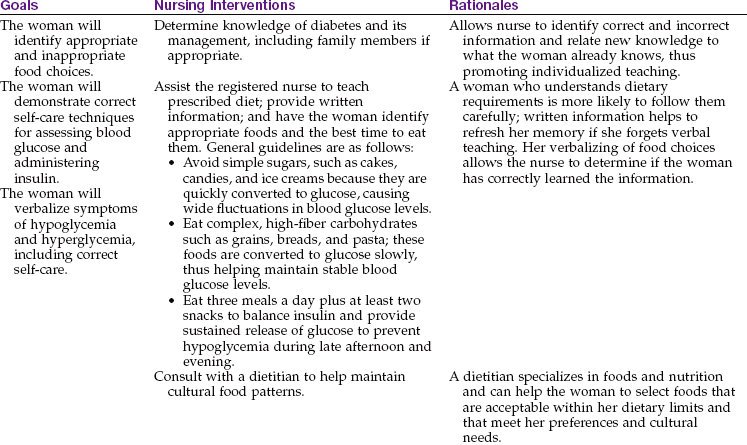
Deficient knowledge related to complications of diabetes during pregnancy
1. A 25-year-old primigravida has been diagnosed with gestational diabetes mellitus at 25 weeks of gestation and has been managing her condition at home with diet, exercise, and insulin. During a clinic visit early in her third trimester, she states that her mother had large infants and “everything was just fine,” and she does not feel any extra tests or monitoring or changes in her insulin regimen is necessary. What would be the best response of the nurse to ensure patient compliance with the prescribed regimen?
2. A woman with GDM seeks care for complaints of dysuria and pruritus in the perineal area and difficulty in controlling her blood sugar over the past few weeks. What questions should the nurse ask, and what actions should be anticipated?
Treatment: The nonpregnant woman with diabetes is treated with a balance of insulin or an oral hypoglycemic drug (agent that reduces blood glucose level), diet, and exercise. Some people with mild diabetes do not need drugs and control their condition by diet and exercise alone. Medical therapy during pregnancy includes identification of gestational diabetes, diet modifications, monitoring of blood glucose levels, insulin, exercise, and selected fetal assessments.
Identification of GDM: If the woman does not have preexisting diabetes, a prenatal screening test to identify GDM is routinely done between 24 and 28 weeks of gestation. The woman drinks 50 g of an oral glucose solution (fasting is not necessary), and a blood sample is taken 1 hour later and is analyzed for glucose. If the blood glucose level is 140 mg/dL or higher, a more complex, 3-hour glucose tolerance test is done.
Diet modifications: The woman is counseled to avoid single large meals with high amounts of simple carbohydrates. A balanced food intake is divided among three meals and at least two snacks throughout the day to maintain stable blood glucose levels. The timing and content of meals and snacks may require adjustment to prevent early-morning hypoglycemia. Foods that release glucose slowly are preferred to avoid rapid changes in blood glucose.
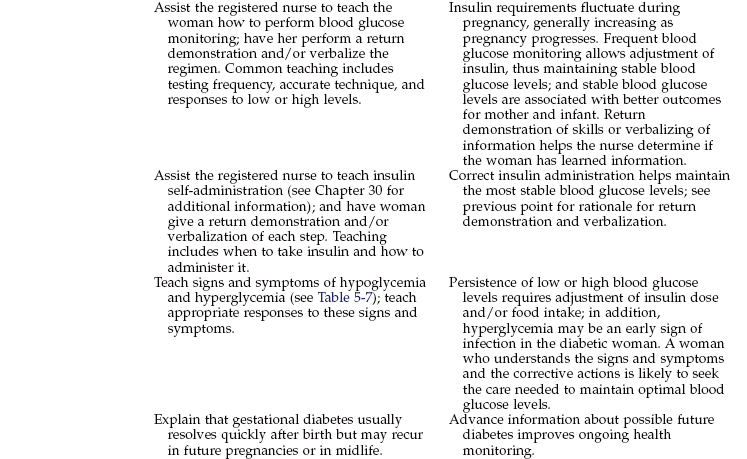
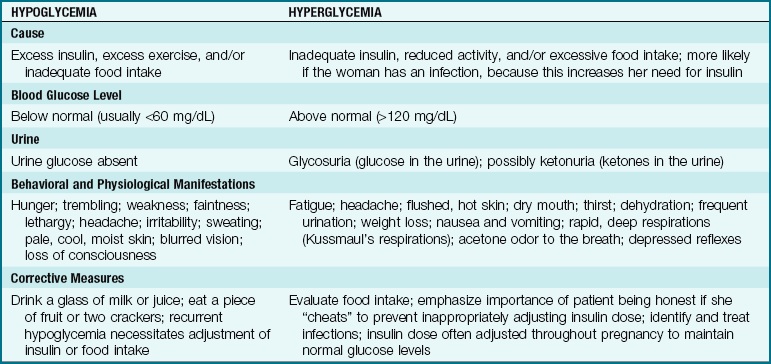
Monitoring of blood glucose levels: To ensure a successful pregnancy the woman must keep her blood glucose levels as close to normal as possible and be taught the signs and symptoms of both hypoglycemia and hyperglycemia (Table 5-7). The pregnant diabetic woman monitors her blood glucose levels several times a day as directed by the health care provider. Blood glucose self-monitoring is discussed in Chapter 31. Glycosylated hemoglobin (HgbA1C) is performed every 3 months to provide an indication of long-term (4- to 6-week) glucose control, and lower values can indicate successful glucose management of the pregnant diabetic. However, HgbA1C monitoring cannot be used as a guide to adjust daily insulin needs during pregnancy.
Monitoring of ketones: Urine ketones may be checked to identify the need for more carbohydrates. If the woman’s carbohydrate intake is insufficient, she may metabolize fat and protein to produce glucose, resulting in ketonuria. However, ketonuria that is accompanied by hyperglycemia requires prompt evaluation for diabetic ketoacidosis. Ketoacidosis can be rapidly fatal to the fetus. It is more likely to occur if the woman has preexisting diabetes or if she has an infection.
Insulin administration: Most oral hypoglycemic agents are not used during pregnancy because they can cross the placenta, possibly resulting in fetal birth defects or neonatal hypoglycemia. Glyburide is the only oral hypoglycemic agent that can be considered for use after the first trimester, when the benefits outweigh the risks for the mother and fetus. Insulin is the preferred drug to lower blood glucose levels during pregnancy because it does not cross the placenta. GDM may be controlled by diet and exercise alone, or the woman may require insulin injections. The dose and frequency of insulin injections are tailored to a woman’s individual needs. Insulin is often given on a sliding scale, in which the woman varies her dose of insulin based on each blood glucose level.
The insulin regimen of a diabetic woman is different during pregnancy than in the nonpregnant state. Typically, insulin dosage may have to be reduced to avoid hypoglycemia in the first trimester, when nausea decreases appetite and physical activity may be reduced. In the second trimester, increasing placental hormones increases insulin resistance (see Chapter 4), and the dosage of insulin may have to be increased. Insulin requirements may drop again at 38 weeks of gestation. GDM resolves promptly after birth, when the insulin-antagonistic (diabetogenic) effects of pregnancy cease.
Neutral protamine Hagedorn (NPH) or Lente insulin is not given at dinnertime because hypoglycemia during the night can occur. Humalog or insulin lispro is a fast-acting insulin that is highly effective if given before meals. The use of an insulin pump has proved to be of great value for glucose control in pregnant and nonpregnant patients with DM. (See Chapter 31 for the discussion of insulin administration and insulin pumps.)
Exercise: A pregnant woman with preexisting diabetes may have vascular damage, and exercise may then result in ischemia (decreased circulation) to the placenta and hypoxia (decreased oxygen) to the fetus. The level of exercise should be prescribed by the health care provider and blood glucose levels monitored closely. In GDM, however, exercise can help control blood glucose levels, and diet and exercise can minimize the need for insulin. The woman with GDM should be counseled that exercise after meals is preferred because glucose levels are high. Hypoglycemia can occur if the woman exercises when the effects of the last insulin dose are at peak. Hyperglycemia can occur if the woman exercises when the effects of the last dose of insulin have decreased. Therefore blood glucose levels should be monitored before, during, and after exercise (see Table 5-7).
Fetal assessments: Assessments (see Table 5-1) may be done to identify fetal growth and the placenta’s ability to provide oxygen and nutrients. Ultrasound examinations are used to identify intrauterine growth restriction, macrosomia, excess amniotic fluid (polyhydramnios) in the woman with poorly controlled diabetes, or decreased amniotic fluid (oligohydramnios) in placental failure.
Diabetes can affect the blood vessels that supply the placenta, impairing the transport of oxygen and nutrients to the fetus and the removal of fetal wastes. The non–stress test, the contraction stress test, and the biophysical profile provide information about how the placenta is functioning. Tests of fetal lung maturity are common if early delivery is considered.
Care during labor: Labor is work (exercise) that affects the amount of insulin and glucose needed. Some women receive an intravenous infusion of a dextrose solution plus regular insulin as needed. Regular insulin is the only type given intravenously. Blood glucose levels are assessed hourly, and the insulin dose is adjusted accordingly. Because macrosomia (large fetal size) is a common complication of GDM, close monitoring of the fetus during labor is essential, and cesarean delivery may be indicated. (See Chapter 8 for care of a woman requiring cesarean section.)
Care of the neonate: Infant complications after birth may include hypoglycemia, respiratory distress, and injury caused by macrosomia. Some infants have growth restriction because the placenta functions poorly. Neonatal nurses and a neonatologist (a physician specializing in care of newborns) are often present at the birth. (See Chapter 14 for a discussion of these neonatal problems.)
Nursing Care: Nursing care of the pregnant woman with diabetes mellitus involves helping her to learn to care for herself and providing emotional care to meet the demands imposed by this complication. Care during labor primarily involves careful monitoring for signs of fetal distress.
Teaching self-care: Most women with preexisting diabetes already know how to check their blood glucose level and administer insulin. They should be taught why diabetes management changes during pregnancy. The woman with newly diagnosed GDM must be taught these self-care skills.
The woman is taught how to select appropriate foods for the prescribed diet. She is more likely to maintain the diet if her caregivers are sensitive to her food preferences and cultural needs. A dietitian can determine foods to meet her needs and help find solutions to problems in adhering to the diet.
The woman who takes insulin may experience episodes of hypoglycemia (low blood glucose) or hyperglycemia (high blood glucose) (see Table 5-7). The woman is taught to recognize and respond to each condition, and family members are included in the teaching. Maintaining glycemic control during pregnancy is essential to prevent later complications such as macrosomia.
Providing emotional support: Pregnant women with diabetes often find that living with the glucose monitoring, diet control, and frequent insulin administration is bothersome. The expectant mother may be anxious about the outcome for herself and her child. Therapeutic communication helps her to express her frustrations and fears. For example, to elicit her feelings about her condition the nurse might say, “Many women find that all the changes they have to make are demanding. How has it been for you?” It may help to emphasize that the close management is usually temporary, especially if she has GDM.
A woman who is actively involved in her care is more likely to maintain the prescribed therapy. Referral to a diabetes management center is often helpful. As she learns to manage her care, liberal praise motivates the woman to maintain her therapy.
Encouraging breastfeeding: Studies have shown that newborns who have been exclusively breastfed have a lower incidence of developing diabetes later in life. Breastfeeding should be encouraged if the newborn does not have perinatal complications related to maternal diabetes, such as macrosomia, respiratory problems, or anomalies. Blood glucose levels of newborns are monitored closely in the first 24 hours of life. Breastfeeding uses glucose reserves in the mother, and glucose monitoring of the mother after breastfeeding is important. Fluids or food intake during breastfeeding may be desirable.
Heart Disease
Heart disease affects a small percentage of pregnant women. During a normal pregnancy, an increase in heart rate, blood volume, and cardiac output places a physiological strain on the heart that may not be tolerated in a woman with preexisting heart disease. Cardiac failure can occur prenatally, during labor, or in the postpartum period.
Manifestations: Increased levels of clotting factors predispose a woman to thrombosis (formation of clots in the veins). If her heart cannot meet these increased demands of pregnancy, congestive heart failure (CHF) results and the fetus suffers from reduced placental blood flow. Box 5-5 lists signs and symptoms of CHF.
During labor, each contraction temporarily shifts 300 to 500 mL of blood from the uterus and placenta into the woman’s circulation, possibly overloading her weakened heart. Excess interstitial fluid rapidly returns to the circulation after birth, predisposing the woman to circulatory overload during the postpartum period. She remains at an increased risk for CHF after birth until her circulating blood volume returns to normal levels in the postpartum period.
Treatment: The pregnant woman with heart disease is usually under the care of both a cardiologist and an obstetrician. She needs more frequent antepartum visits to determine how her heart is coping with the increased demands of pregnancy. Excessive weight gain must be avoided because it adds to the demands on her heart. Preventing anemia with adequate diet and supplemental iron prevents a compensatory rise in the heart rate, which would add to the strain on the woman’s heart. The priority of care is limiting physical activity to decrease the demands made on the heart. The limitation of activity can range from frequent rest periods to strict bed rest, depending on the degree of heart impairment. A woman on prolonged bed rest for any reason has a greater risk for forming venous thrombi (blood clots).
Drug therapy may include heparin to prevent clot formation. Anticoagulants such as warfarin (Coumadin) may cause birth defects and are not given during pregnancy. Beta-adrenergic blocking drugs used to treat hypertension and dysrhythmias can cause fetal bradycardia (slow heartbeat), respiratory depression, and hypoglycemia. Thiazide diuretics can cause harmful effects on the fetus, especially if given in the third trimester. Angiotensin-converting enzyme (ACE) inhibitors are contraindicated for use during pregnancy.
A vaginal birth is preferred over cesarean delivery because it carries less risk for infection or respiratory complications that would further tax the impaired heart. Forceps or a vacuum extractor may be used to decrease the need for maternal pushing (see Chapter 8).
Nursing Care: A woman with heart disease may already be familiar with its management. She should be taught about any necessary changes, such as the change from warfarin anticoagulants to subcutaneous heparin, and should be instructed in how to inject the drug. Laboratory tests include partial thromboplastin time (PTT), activated partial thromboplastin time (aPTT), and platelet counts. She should promptly report signs of excess anticoagulation, such as bruising without reason, petechiae (tiny red spots on the skin), nosebleeds, or bleeding from the gums when brushing her teeth.
The woman is taught signs that may indicate CHF so she can promptly report them. The nurse helps her to identify how she can obtain rest to minimize the demands on her heart. She should avoid exercise in temperature extremes. She should be taught to stop an activity if she experiences dyspnea, chest pain, or tachycardia.
The woman may need help to plan her diet so that she has enough calories to meet her needs during pregnancy while not gaining too much weight. She should be taught about foods that are high in iron and folic acid to prevent anemia. She should avoid foods high in sodium, such as smoked meats and potato chips. Foods high in vitamin K should be avoided in patients receiving heparin therapy.
Stress can also increase demands on the heart. The nurse should discuss stressors in the woman’s life and help her to identify ways to reduce them. During hospitalization the health care provider should be notified if the pulse exceeds 100 beats/min or respirations are greater than 25 breaths/min at rest. Signs of dyspnea (difficulty in breathing), coughing, and abnormal breath sounds should be recorded and reported. Postpartum bradycardia (slowed heart rate) should be reported to the health care provider because the heart may fail as a result of the increased blood volume that occurs after delivery.
Anemia
Anemia is the reduced ability of the blood to carry oxygen to the cells. Hemoglobin levels lower than 10.5 g/dL in the second trimester and below 11 g/dL in the first and third trimesters indicate anemia during pregnancy (Creasy et al., 2009). Four anemias are significant during pregnancy: two nutritional anemias (iron-deficiency anemia and folic acid–deficiency anemia), and two anemias resulting from genetic disorders (sickle cell disease and thalassemia).
Nutritional Anemias
Most women with anemia have vague symptoms, if any. The anemic woman may fatigue easily and have little energy. Her skin and mucous membranes are pale. Shortness of breath, a pounding heart, and a rapid pulse may occur with severe anemia. The woman who develops anemia gradually has fewer symptoms than the woman who becomes anemic abruptly, such as through blood loss.
Iron-Deficiency Anemia: Pregnant women need additional iron for their own increased blood volume, for transfer to the fetus, and for a cushion against the blood loss expected at birth. The RBCs are small (microcytic) and pale (hypochromic) in iron-deficiency anemia. The tannic acid in tea and bran may decrease absorption of iron from foods eaten at the same meal.
Folic Acid–Deficiency Anemia: Folic acid (also called folate or folacin) deficiency is characterized by large, immature RBCs (megaloblastic anemia). Iron-deficiency anemia is often present at the same time. Anticonvulsants, oral contraceptives, sulfa drugs, and alcohol can decrease the absorption of folate from food.
Genetic Anemias
Sickle Cell Disease: Unlike those with nutritional anemias, people with sickle cell disease have abnormal hemoglobin that causes their erythrocytes to become distorted into a sickle (crescent) shape during episodes of hypoxia or acidosis. It is an autosomal recessive disorder, meaning that the affected person receives an abnormal gene from each parent. The abnormally shaped blood cells do not flow smoothly, and they clog small blood vessels. The sickle cells are destroyed more rapidly, resulting in chronic anemia. Approximately 1 of 12 African-Americans has the trait (HgbAS). (See Chapter 27 for further discussion of sickle cell disease.)
Pregnancy may cause a sickle cell crisis, with massive erythrocyte destruction and occlusion of blood vessels. The main risk to the fetus is occlusion of vessels that supply the placenta, leading to preterm birth, growth restriction, and fetal death.
The woman should have frequent evaluation and treatment for anemia during prenatal care. Fetal evaluations concentrate on fetal growth and placental function. Oxygen and fluids are given continuously during labor to prevent sickle cell crisis. Genetic counseling should be offered.
Thalassemia: Thalassemia is a genetic trait that causes an abnormality in one of two chains of hemoglobin, the alpha (α) or beta (β) chain. The β chain variety is most often encountered in the United States. The person can inherit an abnormal gene from each parent, causing β-thalassemia major, or Cooley’s anemia. If only one abnormal gene is inherited, the person will have β-thalassemia minor.
The woman with β-thalassemia minor usually has few problems other than mild anemia, and the fetus does not appear to be affected. However, administration of iron supplements may cause iron overload in a woman with β-thalassemia because the body absorbs and stores iron in higher-than-usual amounts.
Nursing Care for Anemias During Pregnancy
The woman is taught which foods are high in iron and folic acid to help her prevent or treat anemia. She is taught how to take the supplements so that they are optimally effective. For example, the nurse explains that although milk is good to drink during pregnancy, it should not be taken at the same time as the iron supplement or the iron will not be absorbed as easily. Foods high in vitamin C may enhance absorption.
 Nutrition Considerations
Nutrition ConsiderationsTo prevent or correct nutritional anemias, such as iron and folic acid deficiencies, the nurse should teach all women appropriate food sources of those nutrients.
The woman is taught that when she takes iron, her stools will be dark green to black and that mild gastrointestinal discomfort may occur. She should contact her physician or nurse-midwife if these side effects trouble her; another iron preparation may be better tolerated. She should not take antacids with iron.
The woman with sickle cell disease requires close medical and nursing care. She should be taught to prevent dehydration and activities that cause hypoxia. The woman with β-thalassemia is taught to avoid situations in which exposure to infection is more likely (e.g., avoid crowds during flu season) and to report any symptoms of infection promptly. (See Chapter 27 for a discussion of sickle cell anemia and thalassemia.)
Infections
The acronym TORCH has been used to describe infections that can be devastating for the fetus or newborn. The letters stand for the first letters of these four infections or infectious agents: toxoplasmosis, rubella, cytomegalovirus, and herpes simplex virus; the o is sometimes used to designate “other” infections. However, there are many more infections that may be devastating for the mother, fetus, or newborn. Some of these are damaging any time they are acquired, whereas others are relatively harmless except when acquired during pregnancy. See Chapter 4, Table 4-1, for routine prenatal laboratory testing.
Viral Infections
Viral infections often have no effective therapy and may cause serious problems in the mother and/or the fetus or newborn. However, immunizations can prevent some of these infections. An infant born to a mother with an active viral infection, such as rubeola or varicella, must be placed on airborne and contact isolation. Refer to Appendix A for isolation precautions.
Cytomegalovirus: Cytomegalovirus (CMV) infection is widespread and commonly occurs during the childbearing years. The infection is often asymptomatic in the mother. However, an infected infant may have some of the following serious problems:
Rubella: Rubella is a mild viral disease with a low fever and rash. However, its effects on the developing fetus can be destructive. Rubella occurring in very early pregnancy can disrupt the formation of major body systems, whereas rubella acquired later is more likely to damage organs that are already formed. Some effects of rubella on the embryo or fetus include the following:
Treatment and nursing care: Immunization against rubella infection has been available for some time, but some women of childbearing age are still susceptible. When a woman of childbearing age is immunized, she should not get pregnant for at least 1 month after the immunization. The vaccine is offered during the postpartum period to nonimmune women. It is not given during pregnancy because it is a live attenuated (weakened) form of the virus.
Herpesvirus: There are two types of herpes viruses. Type 1 is more likely to cause fever blisters or cold sores. Type 2 is more likely to cause genital herpes. After the primary infection the virus becomes dormant in the nerves and may be reactivated later as a recurrent (secondary) infection. Initial infection during the first half of pregnancy may cause spontaneous abortion, IUGR, and preterm labor. Most pregnancies are affected by recurrent infections rather than primary infections. The infant is infected one of the following ways:
• The virus ascends into the uterus after the membranes rupture.
• The infant has direct contact with infectious lesions during vaginal delivery.
Neonatal herpes infection can be either localized or disseminated (widespread). Disseminated neonatal infection has a high mortality rate, and survivors may have neurological complications.
Treatment and nursing care: Neonatal herpes infection can be prevented by avoiding contact with the lesions. If the woman has active genital herpes lesions when the membranes rupture or labor begins, a cesarean delivery may be required to prevent fetal contact during birth or the development of an ascending infection. Cesarean birth is not necessary if there are no active genital lesions. The mother and infant do not need to be isolated as long as direct contact with lesions is prevented (see Appendix A). Breastfeeding is safe if there are no lesions on the breasts.
Hepatitis B: The virus that causes hepatitis B infection can be transmitted by blood, saliva, vaginal secretions, semen, and breast milk; it can also cross the placenta. The woman may be asymptomatic or acutely ill with chronic low-grade fever, anorexia, nausea, and vomiting. Some become chronic carriers of the virus. The fetus may be infected transplacentally or by contact at birth with blood or vaginal secretions. The infant may become a chronic carrier and a continuing source of infection. Box 5-6 lists those who are at greater risk of having hepatitis B infection.
Treatment and nursing care: All women should be screened for hepatitis B during the course of prenatal care, and the screening should be repeated during the third trimester for women in high-risk groups. Infants born to women who are positive for hepatitis B should receive a single dose of hepatitis B immune globulin (for temporary immunity right after birth) followed by hepatitis B vaccine (for long-term immunity). The Centers for Disease Control and Prevention (CDC) recommends routine immunization with hepatitis B vaccine for all newborns (those born to carrier mothers and to noncarrier mothers) at birth and at ages 1 to 2 months and 6 to 18 months (CDC, 2008). Immunization during pregnancy is not contraindicated. If possible, injections should be delayed until after the infant’s first bath, so that blood and other potentially infectious secretions are removed to avoid introducing them under the skin. Because they have occupational exposure to blood and other infectious secretions, health care staff should be immunized against hepatitis B.
Human Immunodeficiency Virus: Human immunodeficiency virus (HIV) is the causative organism of acquired immunodeficiency syndrome (AIDS). The virus eventually cripples the immune system, making the person susceptible to infections that eventually can result in death. There is no known immunization or curative treatment. See Chapter 11 and a medical-surgical text for further discussion of HIV, infections associated with the syndrome, and treatment.
Although first identified in homosexual males, the incidence of HIV infection and AIDS continues to rise in women. HIV infection is acquired one of the following four ways:
1. Unprotected (through condom nonuse, breakage, or slippage) sexual contact (anal, vaginal, or oral) with an infected person
2. Sharing a needle with an infected person
The infant may be infected in one of the following three ways:
The infected woman has a 20% to 40% chance of transmitting the virus to her fetus perinatally. Infants born to HIV-positive women will be HIV positive at birth because maternal antibodies to the virus pass through the placenta to the infant. From 3 to 6 months are needed to identify the infants who are truly infected.
Nursing care: Counseling should be provided to all women concerning behaviors that place them at risk for contracting HIV (Box 5-7). HIV testing is recommended for all prenatal patients. HIV-positive women should be educated that the transmission of HIV infection to the newborn can be greatly reduced by appropriate drug therapy. Pregnant women with AIDS are more susceptible to infection, and the fetus may develop an impaired immune system that increases the risk of opportunistic infections after birth. Breastfeeding is contraindicated for mothers who are HIV positive.
The fetus and the woman are monitored closely during the antepartum period. All infants born to HIV-positive women are presumed to be HIV positive and standard precautions (see Appendix A) are initiated for both mother and infant. The infant may receive drug therapy during the first 6 weeks of life. The nurse should anticipate and help the mother cope with the anxiety that is almost certain to occur about whether the neonate is infected. Social services can help the family with the care of the child at home. Women should be taught about the risks of sharing needles, the importance of using condoms, and the need to avoid oral sex.
Nonviral Infections
Toxoplasmosis: Toxoplasmosis is caused by Toxoplasma gondii, a parasite that may be acquired by contact with cat feces or raw meat and transmitted through the placenta. The woman usually has mild symptoms. Congenital toxoplasmosis includes the following possible signs in the newborn:
Treatment and nursing care: Specific treatment for toxoplasmosis is controversial. Therapeutic abortion may be offered to the woman who contracts the infection during the first half of pregnancy. Nurses can teach women the following measures to reduce the likelihood of acquiring the infection:
• Wash hands and all kitchen surfaces after handling raw meat.
• Avoid touching the mucous membranes of the eyes or mouth while handling raw meat.
• Avoid uncooked eggs and unpasteurized milk.
• Wash fresh fruits and vegetables well.
• Avoid materials contaminated with cat feces, such as litter boxes, sand boxes, and garden soil.
Group B Streptococcus Infection: Group B streptococcus (GBS) is a leading cause of perinatal infections that have a high neonatal mortality rate. The organism can be found in the woman’s rectum, vagina, cervix, throat, or skin. Although she is colonized with the organism, the woman is usually asymptomatic, but the infant may be infected through contact at birth with vaginal secretions. The risk is greater if the woman has a long labor or premature rupture of membranes. GBS is a significant cause of maternal postpartum infection (endometritis, or infection of the uterine interior), especially after cesarean birth. Symptoms include an elevated temperature within 12 hours after delivery, rapid heart rate (tachycardia), and abdominal distention. Diagnosis of GBS is confirmed by vaginal or rectal culture.
GBS infection can be deadly for the infant. A newborn may have either early-onset (before 7 days) or late-onset (after 7 days) GBS infection.
Treatment: A culture of the woman’s rectum and vagina for the presence of GBS should be taken at 35 to 37 weeks of gestation. All positive cultures require penicillin treatment during labor. High-risk factors such as previous history of GBS infection, prolonged rupture of the membranes, or fever above 37.7° C (100° F) during labor necessitate penicillin treatment to prevent GBS infection. Any GBS-positive urine culture is considered a cause for antibiotic treatment during pregnancy, and the newborn is treated with antibiotics at birth.
Tuberculosis: The incidence of tuberculosis is rising in the United States, and drug-resistant strains of the bacterium are emerging. Pregnant women are screened for pulmonary tuberculosis by either a tuberculin skin test or a serum QuantiFERON-TB Gold test (QFT-G), like any other patient (refer to a medical-surgical nursing text). If the screening test is positive, the woman should have a chest radiograph (x-ray film) with the pregnant abdomen shielded by a lead apron. If required, sputum cultures that are positive for the bacterium confirm the diagnosis.
The adult with tuberculosis experiences fatigue, weakness, loss of appetite and weight, fever, and night sweats. The newborn may acquire the disease by contact with an untreated mother after birth.
Treatment and nursing care: The local public health department is notified of positive cultures and/or chest radiograph results, and isoniazid and rifampin are usually prescribed for 9 months. Pregnant women who are taking isoniazid should also take pyridoxine to reduce the risk of peripheral neuritis. Ethambutol may be given if drug-resistant tuberculosis is suspected. If the mother has active pulmonary tuberculosis, the infant must be kept in a separate area away from the mother. The local health department must be notified, and the discharge plan of the mother and infant must be approved before they are allowed to leave the hospital. The infant may have preventive therapy with isoniazid for 3 months after birth. The health care staff, including nurses, must teach the family how the organism is transmitted and the importance of continuing the antitubercular drugs consistently for the full course of therapy. Incompletely treated tuberculosis is a significant cause of drug-resistant organisms. Modern antitubercular drugs usually render the sputum culture negative within 2 weeks; thus home care is the protocol, with health department follow-up.
Sexually Transmitted Infections
Sexually transmitted infections (STIs), formerly known as sexually transmitted diseases (STDs), are those for which a common mode of transmission is sexual intercourse, although several can also be transmitted in other ways. Herpesvirus and HIV infections have been discussed. Other infections that are typically transmitted sexually are syphilis, gonorrhea, chlamydia, trichomoniasis, and condylomata acuminata (genital warts).
Changes in the vaginal secretions that occur during pregnancy can increase the risk of developing a vaginal infection. The high estrogen levels present during pregnancy thicken the vaginal mucosa and increase secretions that have a high glycogen content. This makes the woman susceptible to yeast infections and other microorganisms. Later in pregnancy the pH of the vagina decreases, resulting in a protective effect.
All sexual contacts of persons infected with a disease that can be sexually transmitted should be informed and treated; otherwise the cycle of infection and reinfection will continue. Consistent use of a latex condom, including the female condom, helps to reduce the sexual spread of STIs. STIs and vaginal infections are discussed in detail in Chapter 11.
Urinary Tract Infections
Urinary tract infections (UTIs) are common in females because of the short urethra and the ease of contamination of the urethra from the rectum, and of contamination from the vagina during sexual activity.
The urinary tract is normally self-cleaning because acidic urine inhibits the growth of microorganisms and flushes them out of the body with each voiding. Pregnancy alters this self-cleaning action because pressure on urinary structures keeps the bladder from emptying completely and because the ureters dilate and lose motility under the relaxing effects of the hormone progesterone. Urine that is retained in the bladder becomes more alkaline, providing a favorable environment for the growth of microorganisms.
Some women have excessive microorganisms in their urine but no symptoms (asymptomatic bacteruria). The asymptomatic infection may eventually cause cystitis (bladder infection) or pyelonephritis (kidney infection). The woman with cystitis has these signs and symptoms:
If not treated, cystitis can ascend in the urinary tract and cause pyelonephritis. Pyelonephritis is a particularly serious infection in pregnancy and is accompanied by these signs and symptoms:
Maternal hypertension, chronic renal disease, and preterm birth may occur with pyelonephritis during pregnancy. The high maternal fever is dangerous for the fetus because it increases the fetal metabolic rate, which in turn increases fetal oxygen needs to levels that the mother cannot readily supply.
Treatment: UTIs are treated with antibiotics, often ampicillin. Asymptomatic bacteruria is treated with oral antibiotics for 10 days, cystitis for 1 to 2 weeks. Pyelonephritis is treated with multiple antibiotics, initially administered intravenously. Cystitis in pregnant women is treated with a full 7 days of antibiotic therapy.
Nursing Care: All females should be taught how to reduce the introduction of rectal microorganisms into the bladder. For example, a front-to-back direction should be used when wiping after urination or a bowel movement, when doing perineal cleansing, or when applying and removing perineal pads. The nurse can begin teaching during the woman’s prenatal visits and reinforce it during the postpartum stay. The mother should be taught how to clean and diaper an infant girl to avoid fecal contamination of her urethra.
Adequate fluid intake promotes frequent voiding. Drinking at least eight glasses of liquid per day and excluding caffeine-containing beverages, helps to flush urine through the urinary tract regularly. Cranberry juice may make the urine more acidic and therefore less conducive to the growth of infectious organisms.
Sexual intercourse mildly irritates the bladder and urethra, which can promote a UTI. Urinating before intercourse reduces irritation; urinating afterward flushes urine from the bladder. Using water-soluble lubricant during intercourse can also reduce periurethral irritation.
Pregnant women should be taught the signs and symptoms of cystitis and pyelonephritis so that they will know to seek treatment at once.
Environmental Hazards During Pregnancy
A teratogen is a substance that causes an adverse effect on the developing embryo or fetus. Some birth defects are caused by a combination of genetic and environmental factors. The specific anomaly that develops depends on the time of exposure to the environmental teratogen in relation to the stage of development of the embryo. In the first weeks of life the vital organs are developing, and exposure to an environmental teratogen may cause miscarriage. Exposure to a teratogen in later pregnancy might result in growth restriction. The four main teratogens of concern during pregnancy are drugs, chemicals, infectious agents, and radiation.
Bioterrorism and the Pregnant Patient
The concepts learned in a microbiology class come to life when nurses discuss the current threat of bioterrorism. In general, there are three basic categories of biological agents:
• Category A: Easily transmitted from person to person (such as smallpox, anthrax, or tularemia)
• Category B: Spread via food and water (such as Q fever, brucellosis, and Staphylococcus enterotoxin B [SEB])
• Category C: Spread via manufactured weapons designed to spread disease (such as hantavirus and tick-borne encephalitis)
Even diseases not normally transmitted by airborne means can be altered to make them transmissible by air. Therefore routine knowledge of an illness related to bioterrorist attacks does not always indicate all possible methods of transmission.
The obstetrical nurse must be observant for unusual symptoms present in large numbers of young, healthy pregnant patients who come to the clinic or emergency department. Such an unusual increase should trigger suspicion of a bioterrorism-related illness and be reported to the charge nurse or unit manager. These suspicions should then be promptly reported to the infection control department of the facility, which will then contact the local health department and the CDC to ensure that appropriate protocols are activated. A laboratory test, rapid antigen detection for influenza, can be performed on these patients. A positive result on this test rules out symptoms that mimic influenza but may be an early sign of a bioterrorism-related infection.
The approach to the care of a pregnant patient who is a victim of a bioterrorist attack may follow protocols similar to those presented in this section of general trauma during pregnancy. Other general protocols relate to the use of standard precautions (see Appendix A), the maintenance of a safe food and water supply to ensure adequate nutrition and hydration, and the maintenance of a safe air supply to prevent further transmission of disease (Table 5-8). The use of available vaccines for the pregnant patient can adversely affect the fetus and must be carefully evaluated, and informed consent must be obtained. Administration of the measles, mumps, and rubella (MMR) vaccine is contraindicated, but most other vaccines may be given if the risk of the disease is truly significant (CDC, 2008). Whenever possible the choice of antimicrobial treatment must also be weighed according to the risks to the fetus and the mother.
Table 5-8
Precautions Required for Common Bioterrorism Agents
| AGENT | PRECAUTION |
| Botulism, anthrax, tularemia | Standard precautions |
| Smallpox | Airborne and contact precautions |
| Pneumonic plague | Droplet precautions |
| Hemorrhagic fever | Airborne, droplet, and contact precautions |
Nurses should participate in community emergency preparedness programs that set up response protocols for patients of all ages and provide shelters, supportive services, intensive care units, emergency supplies, and communication services. The Association for Women’s Health and Neonatal Nurses (AWHONN) recommends that an emergency birth kit that includes ready-to-feed formula and a basic disaster supply kit be kept on hand by families who are pregnant. Advice concerning suggested contents can be accessed at www.AWHONN.org. Continuing education units (CEUs) are now available to help the nurse stay current in this area of nursing. Morbidity and Mortality Weekly Report (MMWR), published by the CDC, is available to health care professionals via the Internet and reports on any unusual biological or chemical outbreaks across the nation and worldwide (www.cdc.gov/mmwr).
Substance Abuse
The use of illicit or recreational drugs during pregnancy has an adverse effect on both the mother and the fetus. Often multiple drugs are used, and lifestyle factors such as malnutrition, poor prenatal care, and STIs may also exist concurrently. Prescribed drugs are assigned a “pregnancy risk category” by the U.S. Food and Drug Administration (FDA) that are published in most drug reference books. Classifications range from A (no risk) to D (positive evidence of risk) and X (contraindicated for use in pregnancy). See Chapter 4 for a detailed review of the drug classifications.
It is well established that several legal and illicit substances are harmful to the developing fetus (Figure 5-8). The fetus of the woman who takes drugs (legal or illicit) or drinks alcohol is exposed to higher levels of the substance for a longer time, because the substances become concentrated in the amniotic fluid and the fetus ingests the fluid. Many environmental substances are most harmful to the fetus early in pregnancy, perhaps before the woman realizes she is pregnant. Table 5-9 reviews some substances that are harmful to the fetus.
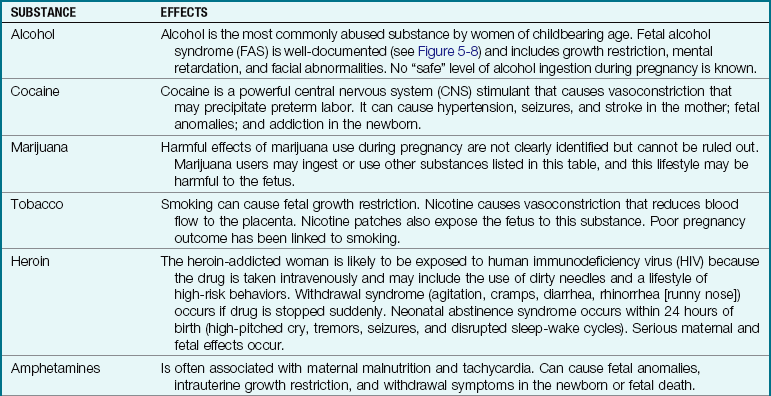
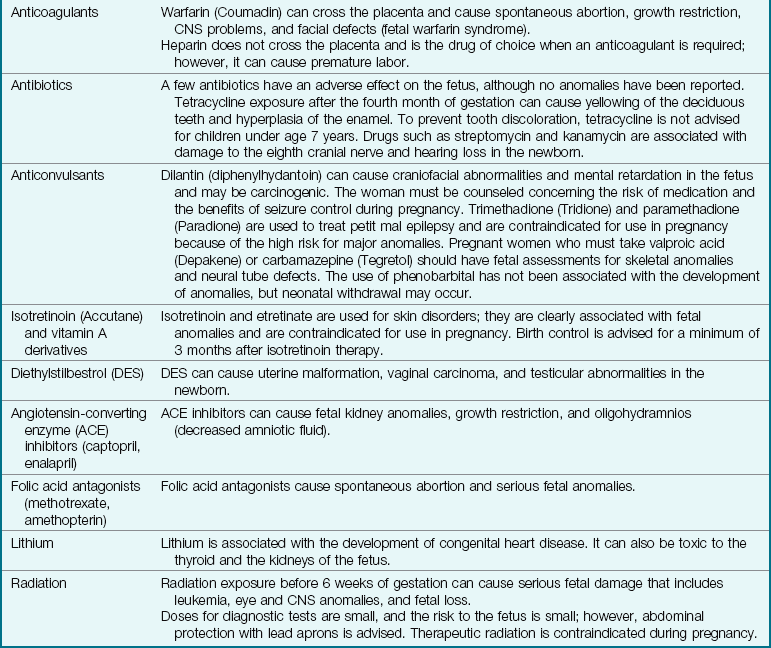
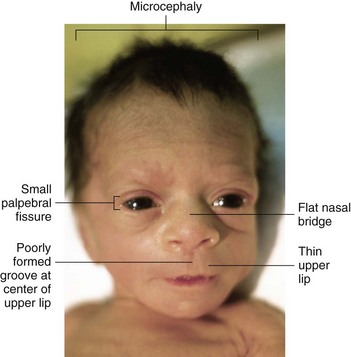
FIGURE 5-8 Fetal alcohol syndrome (FAS). The facial features of an infant with FAS include short palpebral (eye) fissures; a flat nasal bridge; a thin, flat upper lip; a poorly formed groove at the center of the upper lip; and a small head (microcephaly).
Nursing Tip
When asking questions about substance use during pregnancy, the nurse should focus on how the information will help nurses and physicians provide the safest and most appropriate care to the pregnant woman and her infant.
Treatment and Nursing Care: Care focuses on identifying the substance-abusing woman early in pregnancy, educating her about the effects of substance abuse, and encouraging her to reduce or eliminate use. Appropriate referrals should be made.
Nursing Tip
A single episode of consuming two alcoholic drinks during pregnancy can lead to the loss of some fetal brain cells. One drink is defined as 12 oz of beer, 5 oz of wine, or 1.5 oz of hard liquor (Wittendorf & Muenke, 2005).
A partnership should be created with the woman, and a plan for compromises and treatment should be developed. Dietary support, monitoring of the woman’s weight gain, and fetal assessment promote better pregnancy outcomes.
In the case of therapeutic drugs, the woman’s need for the drug is weighed against the potential for fetal harm it may cause and the fetal or maternal harm that may occur if the woman is not treated. In general, the health care provider will choose the least teratogenic drug that is effective and prescribe it in the lowest effective dose.
Educating females about the effect of drugs on a developing fetus is best done before pregnancy. Because drug use is prevalent in schools, preadolescence is not too soon to begin this education. Women should be taught to eliminate the use of any unnecessary substance before becoming pregnant. A woman is encouraged to tell her health care provider if she thinks she is pregnant (or is trying to conceive) before having a nonemergency radiograph, being prescribed a drug, or taking herbal or food supplements.
A trusting, therapeutic nurse-patient relationship makes it more likely that a woman will be truthful about the use of substances, both legal and illicit. The nurse who collects data must use a nonjudgmental approach and treat the issue as a health problem rather than a moral problem. The nurse should support the woman who is trying to reduce her drug use. The nurse should praise her efforts to improve her overall health and to have a successful pregnancy.
A multidisciplinary approach is needed to plan for the care of a mother and newborn that includes referral to community agencies after discharge or child protective services if needed. Drugs that are contraindicated for use in women who are breastfeeding are identified in various drug references. These references should be used as a guide in counseling mothers concerning breastfeeding. See Chapter 14 for discussion of neonatal abstinence syndrome.
Trauma During Pregnancy
There is a high incidence of trauma during the childbearing years. The incidence of trauma during pregnancy may continue to rise, because women are increasingly employed during their pregnancy and there is a trend toward a more violent society. Automobile accidents, homicide, and suicide are the three leading causes of traumatic death (CDC, 2009). Although pregnant women usually are more careful to protect themselves from harm, increased stress from pregnancy may lead to injury both in and out of the home. Falls are not uncommon because of the woman’s altered sense of balance. The pregnant woman also needs to be especially careful when stepping in and out of the bathtub or when using a ladder or stepstool.
The automobile is another hazard. The woman needs to wear a seat belt every time she is in a car, both as a driver and as a passenger. The lap portion of the belt is placed low, just below her protruding abdomen. The pregnant woman and her fetus are more likely to suffer severe injury or death because of not being restrained during a crash than they are to be injured by the restraint itself. Air bags are a supplemental restraint and are intended for use in addition to seat belts. No one should ride with anyone who has been drinking alcohol or whose judgment is impaired for other reasons.
Terrorist acts that involve bombs or blasts usually cause significant bodily injury in gas-filled parts of the body, such as the lungs, gastrointestinal tract, and middle ear. Symptoms of “blast lung” can develop as late as 48 hours after the blast and include bradycardia, low blood pressure, dyspnea, cough, and bloody sputum (hemoptysis). Bomb fragments can contain contaminated or infectious materials and can penetrate the skin, which may necessitate special isolation precautions (see Appendix A). In addition to a routine comprehensive assessment, the pregnant woman should have fetal monitoring for 4 to 6 hours after any trauma. The nurse should understand the changes in anatomy and physiology that normally occur during pregnancy and should ensure that the pregnant woman is not positioned on her back to prevent supine hypotensive syndrome (see Chapter 4). Modifications in the technique of performing cardiopulmonary resuscitation (CPR) on a pregnant woman is described in Box 5-8.
Physical trauma is usually blunt trauma (falls or blows to the body) but may be penetrating trauma (knife or gunshot wounds). Physical abuse against women (battering) is a significant cause of trauma, and violence often escalates during pregnancy. Battering occurs in all ethnic groups and all social strata. It often begins or becomes worse during pregnancy. The abuser is usually her male partner, but he may be another male, such as the father of a pregnant adolescent. Men who abuse women are also likely to abuse children in the relationship.
Women abused during pregnancy are more likely to have miscarriages, stillbirths, and low-birth-weight babies. They often enter prenatal care late, if at all. The risk of homicide escalates during pregnancy.
Abuse during pregnancy, as at other times, may take many forms. It is not always physical abuse; many women are abused emotionally. Emotional abuse makes leaving the relationship especially difficult because it lowers the woman’s self-esteem and isolates her from sources of help. The time of greatest danger to the abused woman occurs when she leaves her abuser.
Manifestations of Battering: In addition to having late or erratic prenatal care, the battered woman may have bruises or lacerations in various stages of healing. A radiograph may reveal old fractures. The woman tends to minimize injury or “forget” its severity. She may assume responsibility for the trauma, as evidenced by remarks such as, “If I had only kept the children quiet, he wouldn’t have gotten so mad.” Her abuser is often particularly attentive after the battering episode.
Treatment and Nursing Care of the Pregnant Woman Experiencing Trauma: Nurses must be aware that any woman may be in an abusive relationship. Therapeutic, nonjudgmental communication helps establish a trusting nurse-patient relationship. Nonabused women, including nurses, often cannot understand why a woman would stay in a harmful relationship. The abuser has usually isolated the woman by controlling whom she sees, where she goes, and how she spends money. Emotional abuse often supplements physical abuse, making the woman feel that she is “stupid” or “no good” and that she is “lucky that he loves her because no one else would ever love her.” She usually feels that she has no choice but to stay in the abusive relationship. She may assume part of the blame, believing that her abuser will stop hurting her if she tries harder.
The woman being assessed for abuse is taken to a private area. The nurse determines whether there are factors that increase the risk for severe injuries or homicide, such as drug use by the abuser, a gun in the house, prior use of a weapon, or violent behavior by the abuser outside the home. The nurse also determines whether the children are being hurt. It is vital that the abuser not find out that the woman has reported the abuse or that she intends to leave.
 Safety Alert!
Safety Alert!
If a woman confides that she is being abused during pregnancy, this information must be kept absolutely confidential. Her life may be in danger if her abuser learns that she has told anyone. She should be referred to local shelters, but the decision to leave her abuser is hers alone.
Nurses can refer women to shelters and other services if they wish to leave the abuser. However, the decision about whether to end the relationship rests with the woman. Abuse of children must be reported to appropriate authorities.
Nursing care for the acutely injured pregnant woman supplements medical management: the focus is on stabilizing the mother’s condition when life-threatening injuries occur. Placing a small pillow under one hip tilts the heavy uterus off the inferior vena cava to improve blood flow throughout the woman’s body and to the placenta. An assessment of vital signs and urine output reflects blood circulation to the kidneys. Urine output should average at least 30 mL/hr. Bloody urine may indicate damage to the kidneys or the bladder.
The nurse assesses for uterine contractions or tenderness, which may indicate onset of labor or abruptio placentae. Continuous electronic fetal monitoring (see Chapter 6) is usually instituted if the fetus is viable and near maturity.
In cases of severe trauma and blood loss, the nurse must relate the increased blood volume of pregnancy to the probable need for increased fluid and blood intake to stabilize the pregnant trauma patient. Peripheral vasoconstriction that normally occurs as a response to shock will cause a decreased flow of oxygen to the fetus. Placing a pillow under one hip to prevent pressure of the uterus on the vena cava is essential. Because of the increased coagulability of the pregnant woman, the aftermath of trauma can result in a high risk for blood-clotting problems such as thrombophlebitis. Values of fibrinogen of 200 to 400 mg/100 mL may be normal for a nonpregnant patient but are indicative of the development of DIC in the pregnant woman, who normally has a fibrinogen level of 400 to 650 mg/100 mL. A fractured pelvis may result in cephalopelvic disproportion (CPD) and necessitate cesarean delivery. Dopamine, a drug routinely used to achieve hemodynamic stability in trauma patients, causes uteroplacental vasoconstriction and may lead to fetal death.
The use of tocolytics to delay labor may be contraindicated in some types of trauma, such as burns. Magnesium sulfate is a vasodilator and also may be contraindicated for use in some types of trauma and shock. Electrical shock injuries can be more serious to the fetus even though the mother does not seem to be seriously injured, because amniotic fluid offers low resistance to the passage of the electrical current to the fetus. In general, it is important for the nurse to understand and correlate the physiology of pregnancy to help the mother and fetus who are victims of trauma. See Box 5-8 for CPR modification during pregnancy.
Effects of a High-Risk Pregnancy on the Family
Normal pregnancy can be a crisis because it is a time of significant change and growth. The woman with a complicated pregnancy has stressors even beyond those of the normal pregnancy. Her family is also affected by the pregnancy and the impending birth.
Disruption of Usual Roles
The woman who has a difficult pregnancy must often remain on bed rest at home or in the hospital, sometimes for several weeks. Others must assume her usual roles in the family, in addition to their own obligations. Finding caregivers for young children in the family may be difficult if extended family lives far away. Placing the children in day care may not be an option if financial problems exist.
Nurses can help families adjust to these disruptions by identifying sources of support to help maintain reasonably normal household function.
Financial Difficulties
Many women work outside the home, and their salary may stop if they cannot work for an extended period. At the same time, their medical costs are rising. Social service referrals may help the family cope with their expenses.
Delayed Attachment to the Infant
Pregnancy normally involves gradual acceptance of and emotional attachment to the fetus, especially after the woman feels fetal movement. Fathers feel a similar attachment, although at a slower pace. The woman who has a high-risk pregnancy often halts planning for the child and may withdraw emotionally to protect herself from pain and loss if the outcome is poor.
Loss of Expected Birth Experience
Couples rarely anticipate problems when they begin a pregnancy. Most have specific expectations about how their pregnancy, particularly the birth, will proceed. A high-risk pregnancy may result in the loss of their expected experience. If the loss is during early pregnancy, they may be unable to attend childbirth preparation classes or to have a vaginal birth. Perinatal loss shatters the hopes of human life and severs a unique attachment between mother and fetus (Figure 5-9). Parents exhibit mourning behaviors associated with the various stages of the grieving process. Health care providers must address these aspects of the grieving process as they work with the parents through interventions including the following:

FIGURE 5-9 Memory kit. This “memory kit” includes pictures of the newborn, clothing, death certificate, footprints, ID band, fetal monitor printout, and ultrasound picture.
• Allowing parents to remain together in privacy
• Accepting behaviors related to grieving
• Developing a plan of care to provide support to the family
• Offering a memento such as a footprint, ID band, lock of hair, and so forth (see Figure 5-9)
• Offering parents an opportunity to hold the infant, if they choose
• Preparing parents for the appearance of the infant
• Providing parents with educational materials and referrals to support groups
• Discussing wishes concerning religious and cultural rituals
Many new noninvasive technologies are on the horizon to detect problem pregnancies and enable early diagnosis and treatment, which may help to prevent perinatal loss (Table 5-10).
Table 5-10
Noninvasive Technologies in Prenatal Care
| TECHNIQUE | OUTCOME |
| AmniSure | Identifies a placental protein that is present in amniotic fluid to help diagnose premature rupture of the membranes. |
| Three-dimensional (3-D) ultrasound | Enables clear in utero identification of malformations, such as cleft lip or palate, abdominal wall defects, and spinal anomalies. Early tests can measure gestational sac and cervical volume to enable early treatment of incompetent cervix and intrauterine growth restriction (IUGR). |
| Fetal DNA | Free fetal DNA in maternal blood circulation is normal, but high levels may be an early indicator of preeclampsia. |
| Fetal trophoblast cells | Cells isolated from the maternal external cervical opening at 12-15 weeks of gestation can provide identification of genetic disorders. The test is safer than amniocentesis for this purpose. |
| Proteomic technology | Amniotic fluid protein studied by proteomic technology, referred to as SELDI-TOF-MS, enables identification of intrauterine inflammation that may lead to preterm birth or fetal injury. Early diagnosis and treatment can prevent premature birth. |
Data from Park, J., & Norwitz, E. (2005). Technical innovations in clinical obstetrics. Contemporary Obstetrics and Gynecology, 50 (Supp), Sept 2005, 6-17; Cousins, L., Smok, D., Lovett, S., & Poeltler, D. (2005). AmniSure placental alpha microglobulin-1 rapid immunoassay versus standard diagnostic methods for detection of ruptured membranes. American Journal of Perinatalogy, 22, 317-320; Amiel, A., et al. (2005). “Genetic pap” at 5-12 gestational weeks: A new screening method for Down syndrome. Journal of the Society for Gynecological Investigation, 12S, 290, abstract 644; Buhimschi, I., Cristner, B., & Buhimschi, C. (2005). Proteomic biomarker analysis of amniotic fluid for identification of intraamniotic inflammation. British Journal of Obstetrics and Gyaenecology, 112, 173-181.
Get Ready for the NCLEX® Examination!
Key Points
• Hyperemesis gravidarum is persistent nausea and vomiting of pregnancy and often interferes with nutrition and fluid balance.
• The most common reason for early spontaneous abortion is abnormality of the developing fetus or the placenta.
• If a woman has a tubal rupture from an ectopic pregnancy, the nurse should observe for shock.
• Because of hemorrhage into the abdomen in the case of a tubal rupture, vaginal blood loss may be minimal, even though intraabdominal blood loss can be massive.
• The woman who has gestational trophoblastic disease (hydatidiform mole) should have follow-up medical care for 1 year to detect the possible development of choriocarcinoma. She should not get pregnant during this time.
• Placenta previa is the abnormal implantation of the placenta in the lower part of the uterus.
• Abruptio placentae is the premature separation of the placenta that is normally implanted.
• The three main manifestations of preeclampsia are hypertension, edema, and proteinuria.
• Eclampsia occurs when the woman has a seizure.
• A positive non–stress test (NST) indicates heart accelerations and is reassuring of fetal health.
• A negative contraction stress test (CST) indicates there are no late decelerations after a uterine contraction and denotes fetal health.
• An abortion is the termination of pregnancy before the fetus is viable.
• Positioning the mother on her left side during bed rest helps improve blood flow to the placenta and prevent pressure on the vena cava.
• A blood pressure of 140/90 mm Hg or above is considered hypertension in the pregnant patient.
• A routine, noninvasive ultrasound examination can confirm pregnancy, detect some anomalies, and reveal the sex of the fetus.
• Rho(D) immune globulin (RhoGAM) can be given to an Rh-negative mother to prevent blood incompatibilities between the mother and an Rh-positive fetus (erythroblastosis fetalis).
• GDM first occurs during pregnancy and resolves after pregnancy. The newborn may be excessively large (macrosomia), and the mother may develop DM later in life. Control of blood glucose level is essential to protect the fetus.
• TORCH diseases of pregnancy include toxoplasmosis, rubella, cytomegalovirus, and herpes, with the o also denoting others.
• The nurse must consider the physiological changes that occur during pregnancy to understand and care for the pregnant trauma victim. Both the mother and the fetus must be monitored closely.
• Urinary tract infections are more common during pregnancy because compression and dilation of the ureters results in urine stasis. Preterm labor is more likely to occur if a woman has pyelonephritis.
• The fetus of the woman who takes drugs (legal or illicit) or drinks alcohol is exposed to higher levels of the substance for a longer time, because the substances become concentrated in the amniotic fluid and the fetus ingests the fluid.
• Drugs and alcohol consumed by the mother can cross the placenta and adversely affect the developing fetus.
Additional Learning Resources
 Go to your Study Guide for additional learning activities to help you master this chapter content.
Go to your Study Guide for additional learning activities to help you master this chapter content.
Go to your Evolve website (http://evolve.elsevier.com/Leifer) for the following FREE learning resources:
• Answer Guidelines for Critical Thinking Questions
• Answers and Rationales for Review Questions for the NCLEX® Examination
• Glossary with English and Spanish pronunciations
• Interactive Review Questions for the NCLEX® Examination
• Patient Teaching Plans in English and Spanish
 Online Resources
Online Resources• Office on Violence Against Women: www.ovw.usdoj.gov
• Pregnancy and exercise: www.familydoctor.org/handouts/305.html
Review Questions for the NCLEX® Examination
1. A woman has an incomplete abortion followed by vacuum aspiration. She is now in the recovery room with her husband and is crying softly. Select the most appropriate nursing action.
1. Leave the couple alone, except for necessary recovery room care.
2. Tell the couple that most abortions are for the best because the infant would have been abnormal.
3. Tell the couple that spontaneous abortion is very common and does not mean they cannot have other children.
4. Express your regret at their loss and remain nearby if they want to talk about it.
2. A woman is admitted with a diagnosis of “possible ectopic pregnancy.” Select the nursing assessment that should be promptly reported.
1. Absence of vaginal bleeding
3. Stable pulse and respiratory rate; rise in blood pressure more than 10 mm Hg systolic
3. It is important to emphasize that a woman who has gestational trophoblastic disease (hydatidiform mole) should continue to have follow-up medical care after initial treatment because:
1. choriocarcinoma sometimes occurs after the initial treatment.
2. she has lower levels of immune factors and is vulnerable to infection.
3. anemia complicates most cases of hydatidiform mole.
4. permanent elevation of her blood pressure is more likely.
4. Select the primary difference between the symptoms of placenta previa and abruptio placentae.
5. During the prenatal clinic visit, your intervention with an abused woman is successful if you have assessed the status of the woman and: