The Child with a Cardiovascular Disorder
1 Define each key term listed.
2 Distinguish the differences between the cardiovascular system of the infant and that of the adult.
3 List the general signs and symptoms of congenital heart disease.
4 Differentiate between patent ductus arteriosus, coarctation of the aorta, atrial septal defect, ventricular septal defect, and tetralogy of Fallot.
5 Discuss six nursing goals relevant to the child with acquired heart disease.
6 List the symptoms of rheumatic fever.
7 Discuss the prevention of rheumatic fever.
8 Discuss hypertension in childhood.
9 Differentiate between primary and secondary hypertension.
10 Identify factors that can prevent hypertension.
11 Recognize the manifestation of Kawasaki disease and the related nursing care.
12 Describe heart-healthy guidelines for children over the age of 2 years.
 , p. 620)
, p. 620) , p. 620)
, p. 620) , p. 612)
, p. 612) , p. 612)
, p. 612) , p. 615)
, p. 615) , p. 612)
, p. 612) http://evolve.elsevier.com/Leifer
http://evolve.elsevier.com/Leifer
The Cardiovascular System
The cardiovascular system consists of the heart, the blood, and the blood vessels. See Figure 3-7 for changes that occur in cardiovascular circulation at birth. As the heart beats, blood, oxygen, and nutrients are transported to all tissues of the body, and waste products are removed. Because of anatomical and physiological immaturity, the cardiovascular system of the child differs from that of the adult. Figure 26-1 summarizes some of these differences.
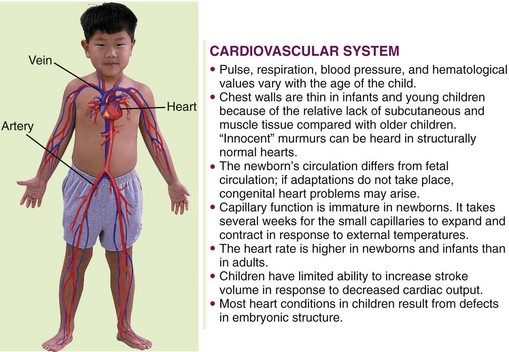
FIGURE 26-1 Summary of some cardiovascular system differences between the child and the adult. The cardiovascular system consists of the heart, blood, and blood vessels. As the heart beats, blood, oxygen, and nutrients are transported to all the tissues of the body, and waste products are removed.
The cardiovascular system develops between the third and the eighth week of gestation. It is the first system to function in intrauterine life. When cardiovascular development is incomplete, heart defects occur. Fetal circulation is designed to serve the metabolic needs during intrauterine life and also to permit safe transition to life outside the womb.
Signs Related to Suspected Cardiac Pathology
Although signs and symptoms of specific congenital heart defects relate to the specific pathology involved, several signs and symptoms are common to most infants with congenital cardiac problems. When the nurse assesses the child, the following observations should be reported:
Congenital Heart Defects
Congenital heart defects may be caused by genetic or maternal factors (e.g., drug intake or rubella illness) or environmental factors. Fetal echocardiography can detect cardiac malformations in high-risk cases. Acquired heart disease occurs after birth, as a result of a defect or illness.
Pathophysiology: Congenital heart defects are not a problem for the fetus because the fetal-maternal circulation compensates for all fetal oxygen needs. However, at birth, the infant’s circulatory system must take over and provide for the child’s own oxygen needs. Any heart defect or patent (open) fetal pathways in the cardiovascular system after birth produce signs and symptoms that indicate an anatomical heart defect. Congenital heart disease occurs in approximately 8 of 1000 births, and 50% of these infants evidence signs and symptoms before the first year of life. Some defects, such as mitral valve prolapse, may not be manifested until later in life.
Of the congenital anomalies, heart defects are the principal cause of death during the first year of life. Therefore nurses must stress the need for good prenatal care and impress on parents the value of regular checkups at well-baby clinics. Many organic heart murmurs have been detected early in infancy at periodic checkups.
Diagnosis and Treatment: The appearance of clinical symptoms and results of diagnostic tests aid in the diagnosis of congenital heart disease (Table 26-1). The treatment of most cardiac defects is surgical. A thoracotomy (chest incision) is performed, and the use of a cardiopulmonary bypass machine and hypothermia during the procedure minimize blood loss and enhance patient response. Hypothermia (hypo, “under,” and thermal, “heat”) reduces the temperature of body tissues, resulting in a decreased need for oxygen. The cardiopulmonary bypass machine provides oxygenation of the body tissues while the surgeon stops the heart to perform surgery. Heart transplants may be the treatment of choice in cases such as a three-chambered heart.
Table 26-1
Diagnostic Tests Used in Congenital Heart Defects
| TEST | DEFINITION | VALUE |
| Angiocardiography (selective) | Serial x-ray films of the heart and great vessels after injection of an opaque substance; a radiopaque catheter is moved into the heart chambers, and contrast medium is injected in specific areas | Abnormal communications in the heart can be observed; the course of the blood through the heart and great vessels can be traced |
| Aortography | X-ray films of the aorta after the injection of an opaque material | Useful in revealing patent ductus arteriosus |
| Radionuclide angiocardiography | Noninvasive nuclear procedure that permits visualization of the course of blood through the heart | May be used as a precardiac catheterization screening study; provides assessment of congenital and acquired cardiovascular lesions and monitors the effects of therapy; an intravenous (IV) device is necessary to permit injection of the radionuclide |
| Barium swallow | Barium given by mouth | Shows indentation of the esophagus by the aorta or other vessels |
| Cardiac catheterization | A radiopaque catheter is passed through the femoral artery directly into the heart and large vessels | Reveals blood pressure within the heart; physician can examine the heart closely with the tip of the catheter to detect abnormalities; blood samples can be obtained to determine oxygen content |
| Chest x-ray film | A radiographic image of a body structure | Provides a permanent record; shows abnormalities in the shape and position of heart |
| Cineangiocardiography | Motion pictures of images recorded by fluoroscopy | Useful recording and monitoring device |
| Echocardiography | The use of ultrasound to produce an image of sound waves of the heart; transducer placed directly on chest; sounds are analyzed | Noninvasive procedure; localizes murmurs; determines if heart is structurally normal |
| Electrocardiogram | Tracing of heart action by electrocardiography | Detects variations in heart action and shows the condition of the heart muscle; may also be used as a monitoring device during cardiac catheterization |
| Magnetic resonance imaging (three-dimensional [3-D] imaging) | Noninvasive imaging technique that uses low-energy radio waves in combination with a magnetic field to generate signals that produce tomographic images | Very useful in diagnosing coarctation of the aorta |
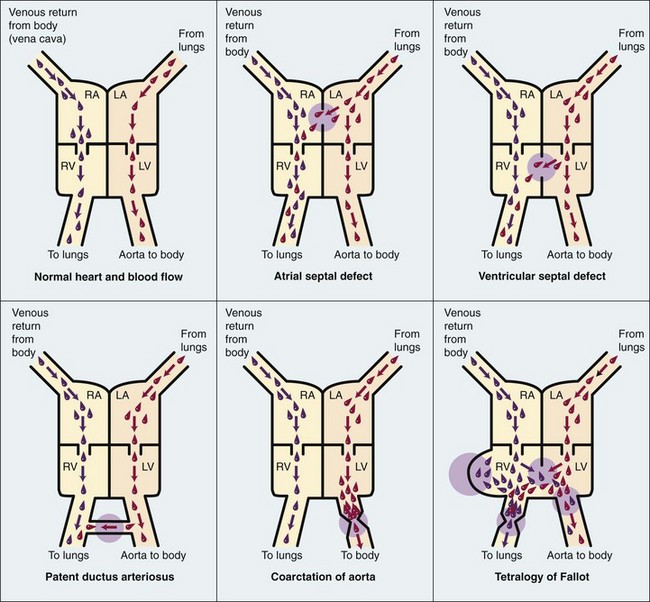
Classification: Congenital heart defects can be divided into two categories: cyanotic and acyanotic. A more accurate classification is based on the effect of the defect on blood circulation. The study of blood circulation is termed hemodynamics (hemo, “blood,” and dynamics, “power”). Blood always flows from an area of high pressure to an area of low pressure and takes the path of least resistance. Physiologically, defects can be organized into (1) lesions that increase pulmonary blood flow, (2) lesions that restrict blood flow, and (3) lesions that decrease pulmonary blood flow. There are also mixed lesions. A shunt refers to the flow of blood through an abnormal opening between two vessels of the heart. Figure 26-2 compares the normal heart and the heart with various congenital defects.
Defects That Increase Pulmonary Blood Flow
Congenital heart defects that cause the blood to return to the right ventricle and recirculate through the lungs before exiting the left ventricle through the aorta are known as defects that increase pulmonary blood flow. For example, the defect in the atrial septum in the fetus allows blood to flow from the right atrium through the defect into the left atrium, providing a bypass of the lungs. After birth, the pressure is higher in the left atrium; if the atrial opening persists, the blood flows back into the right atrium (left-to-right shunt) and then recirculates to the lungs, causing increased pulmonary flow. Some defects that increase pulmonary flow are atrial septal defect, ventricular septal defect, and patent ductus arteriosus (see Figure 26-2). In heart defects that result in increased pulmonary flow because of a left-to-right shunt, the oxygenated blood recirculates to the lungs, and cyanosis is rare.
Atrial Septal Defect: Atrial septal defect (ASD) involves an abnormal opening between the right and left atria. Blood that already contains oxygen is forced from the left atrium back to the right atrium. Most patients do not have symptoms. The defect may be recognized when a murmur is heard during a routine health examination. Cardiac catheterization, electrocardiogram, and echocardiography may be performed to help to confirm the diagnosis. The surgical repair involves application of a surgical Dacron patch or repair with open cardiac surgery. Nonsurgical closure during cardiac catheterization can sometimes be accomplished. Continued cardiology follow-up is necessary. Low-dose aspirin therapy is usually prescribed for 6 months after repair. Prognosis is excellent.
Ventricular Septal Defect: Ventricular septal defect (VSD) is the most common heart anomaly. As the name suggests, there is an opening between the right and left ventricles of the heart. Increased pressure within the left ventricle forces blood back into the right ventricle (left-to-right shunt). A loud, harsh murmur combined with a systolic thrill is characteristic of this defect. The condition may be mild or severe. It is often associated with other defects. Many children with small defects may experience spontaneous closure during the first year of life as a result of growth. Small defects may be closed during cardiac catheterization (Kliegman et al., 2007).
Early surgical intervention has a low risk for most infants, and the prognosis is excellent. Normal growth and development are usually achieved within 1 or 2 years after surgery.
Open heart surgery is performed under hypothermia. With the use of the heart-lung bypass machine the condition can be corrected in a fairly dry or bloodless field. The hole is ligated (closed) with sutures or a synthetic patch.
Patent Ductus Arteriosus: The circulation of the fetus differs from that of the newborn in that most of the fetal blood bypasses the lungs. The ductus arteriosus is the passageway (shunt) through which the blood crosses from the pulmonary artery to the aorta and avoids the deflated lungs. This vessel closes shortly after birth; when it does not close, blood continues to pass from the aorta, where the pressure is higher, into the pulmonary artery. This causes oxygenated blood to recycle through the lungs, overburdening the pulmonary circulation and making the heart pump harder.
The symptoms of patent ductus arteriosus (PDA) may go unnoticed during infancy. As the child grows, dyspnea is experienced, the radial pulse becomes full and bounding on exertion, and there is an unusually wide range between systolic and diastolic blood pressures. This is referred to as the pulse pressure. A characteristic machinery type of murmur may be heard. A two-dimensional echocardiogram is useful in visualizing and determining blood flow across the PDA.
PDA is one of the more common cardiac anomalies. It occurs twice as frequently in girls as in boys. Premature infants with hypoxia often respond to indomethacin drug therapy that results in closure of the PDA. Heart surgery is performed on all full-term newborns diagnosed with PDA to prevent congestive heart failure (CHF), embolus formation, and other complications. The ductus may be ligated via thoracotomy (incision into the chest) or via the visually assisted thoracoscopic surgery (VATS) technique that eliminates the need for a large chest incision. Nonsurgical options include the insertion of coils to occlude the PDA, which is done in a cardiac catheterization lab. The prognosis is excellent.
Defects That Restrict Ventricular Blood Flow
Some congenital cardiac defects can restrict blood flow from the ventricles because of a stenosis (narrowing) of a vessel.
Coarctation of the Aorta: The word coarctation means “a tightening.” In coarctation of the aorta, there is a constriction or narrowing of the aortic arch or of the descending aorta (i.e., the blood meets an obstruction) (see Figure 26-2). Hemodynamics consists of increased pressure proximal to the defect and decreased pressure distally. The characteristic symptoms are a marked difference in the blood pressure and pulses of the upper and lower extremities. The patient may not develop symptoms until late childhood. X-ray examination may reveal cardiac enlargement and “notching” of the ribs caused by vessels developed as collateral circulation. Pulses and blood pressure will differ in the upper and lower extremities. Two-dimensional echocardiography can aid in the diagnosis. If the condition is untreated, hypertension, CHF, and infective endocarditis may develop. Treatment depends on the type and severity of the defect. Infants who have associated CHF are treated medically until the optimal time for surgery.
Percutaneous balloon angioplasty is the treatment of choice for older children, and stents can be inserted to maintain patency. The surgeon resects the narrowed portion of the aorta and joins its ends. The joining is called an anastomosis. If the section removed is large, an end-to-end graft using tubes of synthetic polyester (Dacron) or similar material may be necessary. Some children complain of leg pain after exercise. As in PDA, closed heart surgery is performed because the structures are outside the heart. The prognosis is good if there are no other defects and the child’s physical condition is favorable at the time of surgery. If restenosis occurs after surgery for coarctation, a balloon angioplasty can relieve the obstruction. The nurse should observe the child after coarctation surgery for the development of hypertension and abdominal pain associated with nausea and vomiting, leukocytosis, and gastrointestinal bleeding or obstruction. Antihypertensive drugs, steroids, and nasogastric tube decompression are the priority treatment of these postsurgical complications.
Defects That Decrease Pulmonary Blood Flow
A decrease in pulmonary blood flow occurs when a congenital heart anomaly allows blood that has not passed through the lungs (unoxygenated blood) to enter the aorta and the general circulation. Cyanosis caused by the presence of unoxygenated blood in the circulation is a characteristic feature of this type of congenital heart anomaly.
Tetralogy of Fallot: Tetra means “four.” In tetralogy of Fallot there are four defects:
1. Stenosis or narrowing of the pulmonary artery, which decreases the blood flow to the lungs
2. Hypertrophy of the right ventricle, which enlarges because it must work harder to pump blood through the narrow pulmonary artery
3. Dextroposition (dextro, “right,” and position) of the aorta, in which the aorta is displaced to the right and blood from both ventricles enters it
4. VSD (see Figure 26-2)
When venous blood enters the aorta, the infant displays symptoms of cardiac problems. Cyanosis increases with age, and clubbing of the fingers and toes is seen (see Figure 25-10). The child rests in a “squatting” position to breathe more easily. This position alters systemic venous return. Feeding problems, growth retardation, frequent respiratory infections, and severe dyspnea on exertion are prevalent. The red blood cells (RBCs) of the body increase, causing polycythemia (poly, “many,” cyt, “cells,” and hema, “blood”) to compensate for the lack of oxygen.
Narrowing of the pulmonary artery causes CHF as a result of the increased muscular force necessary to propel blood through the narrowed orifice. When unoxygenated blood enters the general circulation, hypoxia occurs and may be manifested by cyanosis.
Failure to thrive results from decreasing energy and ability to eat and increased oxygen consumption. Multiple hospitalizations, cyanotic skin, and limited energy can impede growth and development both physically and socially.
Paroxysmal hypercyanotic episodes, or “tet” spells, occur during the first 2 years of life. Spontaneous cyanosis, respiratory distress, weakness, and syncope occur. They can last a few minutes to a few hours and are followed by lethargy and sleep. Parents and day care personnel must be instructed to place the child in a knee-chest position when a tet spell occurs (Figure 26-3). Often the child will pause and voluntarily squat in position until the attack abates. Recovery from the tet spell is usually rapid.
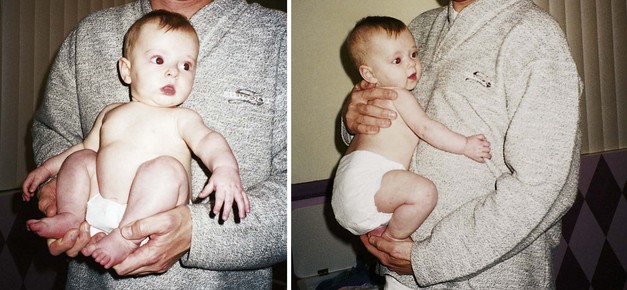
FIGURE 26-3 Tet position. Infants and children with tetralogy of Fallot can have paroxysmal hypercyanosis or “tet” spells. Placing the child in the tet position (a knee-chest position) will relieve these symptoms. Older children will spontaneously squat when a tet spell occurs.
Diagnosis of tetralogy of Fallot is confirmed by chest x-ray study that shows a typical boot-shaped heart. An electrocardiogram, three-dimensional echocardiography, and cardiac catheterization aid in confirming the diagnosis.
Complications such as cerebral thrombosis caused by polycythemia (thickened blood as a result of increased RBCs) are a problem, especially if dehydration occurs. Iron deficiency anemia develops because of decreased appetite and increased energy required to suck or eat. Bacterial endocarditis can occur and is prevented with prophylactic antibiotic therapy.
Treatment is designed to increase pulmonary blood flow to relieve hypoxia. A Blalock-Taussig surgical procedure can be performed successfully on newborns or premature infants. Open heart surgery using cardiopulmonary bypass provides total correction of all defects and is usually done on the older, stable child with excellent results. Postoperatively the nurse should be observant for signs of congestive heart failure and an irregular heartbeat.
 Nursing Tip
Nursing TipDefects That Cause Mixed Pathology
Hypoplastic Left Heart Syndrome: In hypoplastic left heart syndrome there is an underdevelopment of the left side of the heart, usually resulting in an absent or nonfunctional left ventricle and hypoplasia of the ascending aorta. This condition can be diagnosed before birth and the infant placed on a transplant list early so surgery can be performed soon after birth. The initial survival of the infant depends on a patent foramen ovale and ductus arteriosus to provide a pathway for oxygenated blood to the general body system. Other serious congenital anomalies may be present, and the infant should be carefully assessed.
Symptoms include a grayish blue color of the skin and mucous membranes and signs of CHF, including dyspnea, weak pulses, and a cardiac murmur. Survival beyond the first few months of life without intervention is rare. A multistage shunting procedure can be done as a temporary holding measure until a new heart is available. With the advent of successful heart transplants, however, the prognosis of these infants is much brighter, and emphasis is placed on maintaining life and hope until an appropriate heart is available for transplant. After a transplant, immunosuppressive therapy to prevent organ rejection is required.
General Treatment and Nursing Care of Children with Congenital Heart Defects
Recent technological advances have enabled therapeutic catheterization procedures for valvuloplasty, angioplasty, and other corrections of pediatric heart pathologies as an alternative to open heart surgery. After the procedure the nursing care involves monitoring vital signs, observing for thrombosis formation, and performing neurovascular checks of the limb, including pedal pulses. Emotional support of the family and education concerning what to do and expect during and after therapy is a nursing responsibility. In most cases, hospitalization after cardiac catheterization is limited to 2 or 3 days. Parents must be guided to understand that the child should not be overprotected or restricted from normal activities related to optimum growth and development. Fear and anxiety can be transferred from the parents to the child. Education concerning general health, hygiene, dental care, balanced diet, and routine immunizations should be emphasized. Immunizations after cardiac transplantation must be placed on hold.
Immunizations are not recommended before cardiac surgery, because immunosuppressants are used to prevent rejection of the transplanted heart, and the child’s ability to manufacture antibodies in response to routine immunizations will be impaired. Dental health care in children with heart disease is important to prevent bacteremia, which can cause bacterial endocarditis. Antibiotics are usually required before dental care. Competitive sports are avoided for children with congenital heart disease, because the pressure for a team win can interfere with the child’s need to stop activity if specific symptoms arise. Some children benefit from being transported to school so that energy can be consumed during school activities rather than by walking to school.
Nutritional guidance is aimed at preventing anemia and promoting optimal growth and development. Parents should be instructed in the techniques of preventing dehydration in children with polycythemia. Family trips or vacations during the hot summer months require attention to the child’s fluid needs to replace fluid loss from sweating. Vacations to high altitudes or very cold environments may cause adverse responses in a child who is already hypoxic or has cardiac problems.
Cardiac surgery—if needed to repair a defect that causes heart failure—is generally performed at a regional medical center where the necessary costly equipment is available. Chest tubes may be used postoperatively to remove secretions and air from the pleural cavity and to allow reexpansion of the lungs. These are attached to underwater-seal drainage systems or a commercially manufactured disposable system such as Pleur-evac. Units for infants and older children are available. This system must be airtight to prevent collapse of the lung. Drainage systems are always kept below the level of the chest to prevent the backflow of secretions. This is especially important during transportation. Two rubber-shod Kelly clamps must be available at all times for emergency clamping of tubes. These are applied to the tubes as close as possible to the child’s chest if a break in the system occurs.
Postoperative cardiac care usually takes place in an intensive care unit (ICU), where high-technology monitoring minimizes complications. The licensed vocational nurse will have contact with the child who is returning for postoperative checkups or is on a home care program after discharge. Providing routine supportive care, encouraging appropriate medical follow-up, and designing activities that promote optimal growth and development are primary goals of care.
Acquired Heart Diseases
Acquired heart disease is a cardiac problem that occurs after birth. It may be a complication of a congenital heart disease or a response to respiratory infection, sepsis, hypertension, or severe anemia. Heart failure is defined as cardiac output inadequate to meet the metabolic needs of the body.
Congestive Heart Failure
Manifestations: Manifestations of congestive heart failure (CHF) depend on the side of the heart affected. The right side of the heart moves unoxygenated blood to the pulmonary circulation. A failure results in the backup of blood in the systemic venous system. The left side of the heart moves oxygenated blood from the pulmonary circulation to the systemic circulation. A failure results in backup into the lung. When the body tries to compensate for the problems, peripheral vasoconstriction occurs and results in cold and/or blue hands and feet, tachycardia, and tachypnea. Although heart failure may start as a right- or left-sided failure, eventually both sides become involved.
Signs and symptoms may differ somewhat and are more subtle in infants. Some of these signs are cyanosis, pallor, rapid respiration, rapid pulse, feeding difficulties, fatigue, a weak cry, excessive perspiration (especially on the forehead), failure to gain weight, edema, and frequent respiratory infections.
Cyanosis: When observing color, the nurse notes whether the cyanosis is general or localized. If it is localized, the exact location is recorded in the nurse’s notes, for example, hands, feet, lips, or around the mouth. Is the cyanosis deep or light? Is it constant or transient? Sometimes color improves during crying, and sometimes it gets worse; this is significant. If overt cyanosis is not apparent in the African American infant, the palms of the hands and bottoms of the feet are observed. Clubbing of the fingers and toes (see Figure 25-10) may be evident as a result of blood pooling in the capillaries of the extremities in children with chronic hypoxia. The skin may be very pale or mottled. Sweating, particularly of the head, may be seen.
Rapid respiration: Rapid respiration is called tachypnea. A rate of over 60 breaths/min in a newborn at rest indicates distress. The amount of dyspnea, or shortness of breath, varies. In more acute cases, dyspnea is accompanied by flaring of the nostrils, mouth breathing, grunting, and sternal retractions. The infant has more trouble breathing when flat in bed than when held upright. Air hunger is evidenced if the child is irritable and restless. The cry is weak and hoarse.
Rapid pulse: A rapid pulse is termed tachycardia. An increase in pulse rate is one of the first signs of CHF. The heart is pumping harder in an effort to increase its output and provide sufficient oxygen to all the tissues of the body. Cardiac output can be increased by one of two mechanisms: tachycardia or increased stroke volume. Stroke volume is the amount of blood ejected during one contraction. Because infants and small children have a limited ability to increase stroke volume, their heart rate must increase to meet the demand.
Feeding difficulties: When the nurse feeds these infants, they tire easily and may stop after sucking a few ounces. When placed in the crib, they cry and appear hungry. They may choke and gag during feedings; the pleasure of sucking is spoiled by their inability to breathe.
Poor weight gain: The child fails to gain weight. A sudden increase in weight may indicate edema and the beginning of heart failure.
Edema: Blood flow to the kidneys is decreased, and the glomerular filtration rate slows. This causes both fluid and sodium to be retained. The nurse watches for puffiness about the eyes and, occasionally, in the legs, feet, and abdomen. Urine output may decrease.
Frequent respiratory tract infections: Resistance is very low. Slight infections can be highly dangerous because the heart and lungs are already compromised. Immunizations are reviewed and updated as needed. The nurse prevents exposure to other children who have upper respiratory tract infections and other illnesses.
Treatment and Nursing Care: The nursing goals significant to the care of children with heart failure are the following:
The nurse must organize care so the infant is not unnecessarily disturbed. A complete bath and linen change for an infant with a serious heart defect may not be a priority. The infant is fed early if crying and late if asleep. The physician orders the position in which the infant is placed. In some cases the knee-chest position facilitates breathing; in other cases, a position with the head elevated (Fowler’s position) may be helpful. Older infants may be placed in infant seats.
Feedings are small and frequent. A soft nipple with holes large enough to prevent the infant from tiring is provided. Often, formulas with increased caloric density are used. In some cases, nasogastric tube feedings are advantageous because they are less tiring for the child. Oxygen is administered to relieve dyspnea. As breathing becomes easier, the infant begins to relax. A soft voice and gentle care are soothing. Whenever possible, the infant is held and comforted during feedings.
Digitoxin and digoxin (Lanoxin) are common oral digitalis preparations. In pediatric patients, Lanoxin is preferred because of its rapid action and shorter half-life. These agents slow and strengthen the heartbeat. The nurse counts the patient’s pulse for 1 full minute before administering them. A resting apical pulse is most accurate. As a rule, if the pulse rate of an infant or child is below 100 beats/min the medication is withheld and the physician is notified. In older children the pulse rate should be above 70 beats/min. Because the pulse rate varies with the age of the child, it is ideal for the physician to specify in the written drug order at what heart rate the nurse should withhold the drug. When this is not done, the nurse obtains clarification. The physician is notified when the drug is withheld.
The physician is contacted if the patient vomits. Digitalis administration is not repeated until the physician confirms it is safe to do so. Tachycardia and irregularities in the rhythm of the pulse are significant and should be reported. Symptoms of toxicity include nausea, vomiting, anorexia, irregularity in rate and rhythm of the pulse, and a sudden change in pulse. If the infant is discharged while still receiving medication, the parents are taught how to take the pulse and what signs to be alert for when administering the drug.
A group of drugs called angiotensin converting enzyme inhibitors (ACE-Is) are prescribed. Captopril, vasotec, and lisinopril are examples of these drugs. The nurse should observe for signs of hypotension, cough, renal dysfunction and hyperkalemia. Serum potassium should be carefully monitored.
 Medication Safety Alert!
Medication Safety Alert!
Dosage of drugs such as digoxin should be checked by two nurses. A single dose larger than 0.05 mg, or 50 mcg, should be reconfirmed with the health care provider.
Diuretics such as furosemide (Lasix) or chlorothiazide (Diuril) are useful in reducing edema. Careful monitoring of serum electrolyte levels prevents electrolyte imbalance, particularly potassium depletion. Parents of older patients are taught to recognize foods high in potassium, such as bananas, oranges, milk, potatoes, and prune juice. Diapers are weighed to determine urine output. Daily weighing of the infant also helps the physician determine the effectiveness of the diuresis.
An accurate record of intake and output is essential. Signs of dehydration such as thirst, fever, poor skin turgor, apathy, sunken eyes or fontanelle, dry skin, dry tongue, dry mucous membranes, and decreased urination should be brought to the immediate attention of the nurse in charge. Pneumonia can occur rapidly. Fever, irritability, and an increase in respiratory distress may indicate this condition. The child’s position is changed regularly to help prevent hypostatic pneumonia.
The nurse working in a cardiac unit assesses the child frequently for complications of cardiac and respiratory failure and should be competent in cardiopulmonary resuscitation techniques and the necessary modifications required for pediatric patients (Pediatric Advanced Life Support [PALS] certification).
The parents of the child need support and understanding over a long period. Because the heart is the body’s major vital organ, this type of diagnosis causes much apprehension. The physician must reassure the parents without minimizing the danger involved.
The patterns formed during infancy can build the framework of a healthy personality for the patient. Children who have heart conditions but who are well integrated into family life have a decided advantage over children who are made to think they are invalids. Routine naps and early bedtime provide adequate rest for most children.
As children grow, they usually set their own limits on the amount of activity they can handle. Prompt treatment of infections is important. A suitable diet with adequate fluids is necessary. Eating iron-rich foods is encouraged. Dental care should be regular. All-day attendance in school may be too tiring for the child; therefore special arrangements may be necessary. The child needs careful evaluation before any type of minor surgery is performed.
Detailed discharge planning and coordination of community services are of value to the family.
Rheumatic Fever
Pathophysiology: Rheumatic fever (RF) is a systemic disease involving the joints, heart, central nervous system (CNS), skin, and subcutaneous tissues. It belongs to a group of disorders known as collagen diseases. Their common feature is the destruction of connective tissue. RF is particularly detrimental to the heart, causing scarring of the mitral valves. Its peak incidence is between 5 and 15 years of age. RF is common worldwide in lower-income groups and where overcrowded conditions exist. It is more prevalent during winter and spring, and carrier rates among school-age children are believed to be higher during these seasons. Genetic factors have implicated an abnormal immune response.
RF is an autoimmune disease that occurs as a complication of untreated group A beta-hemolytic streptococcus infection of the throat. The disease almost disappeared during the 1960s and 1970s; since the late 1980s, however, a resurgence has occurred in the United States. This has highlighted the need for more aggressive diagnosis and treatment of streptococcal pharyngitis.
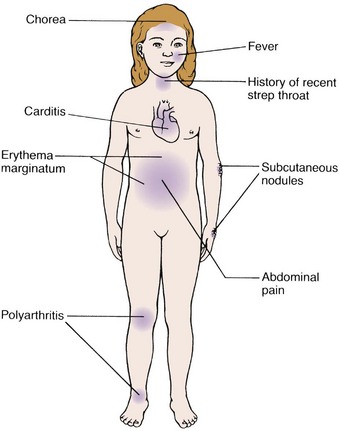
Manifestations: Symptoms of RF range from mild to severe and may not occur for 1 to 6 weeks after a strep throat infection (Figure 26-4). The classic symptoms are migratory polyarthritis (wandering joint pains), skin eruptions, chorea (a nervous disorder), and inflammation of the heart. Subcutaneous nodules may appear beneath the skin but are less common in children. Abdominal pain, often mistaken for appendicitis, sometimes occurs. Fever varies from slight to very high. Pallor, fatigue, anorexia, and unexplained nosebleeds may be seen. An elevated antistreptolysin O titer (ASO) is a standard diagnostic test for RF. Rheumatic fever tends to recur, and each attack carries the threat of further damage to the heart. The recurrences are most frequent during the first 5 years after the initial attack, and they decline rapidly thereafter.
Migratory polyarthritis: The polyarthritis (poly, “many,” arthr, “joint,” and itis, “inflammation of”) seen in RF is distinctive in that it does not result in permanent deformity to the joint. It involves mainly the larger joints: knees, elbows, ankles, wrists, and shoulders. The joints become painful and tender and are difficult to move. The symptoms last for a few days, disappear without treatment, and frequently return in another joint. This pattern may continue for a few weeks. The symptoms tend to be more severe in older children. The joint may be visibly swollen and inflamed. On diagnosis, salicylates are administered to relieve the pain.
Skin eruptions: Erythema marginatum, the rash seen in RF, consists of small red circles with red-colored margins, a pale center, and wavy lines appearing on the trunk and abdomen. They appear and disappear rapidly and are significant in diagnosing the disease.
Sydenham’s chorea: Chorea is a disorder of the CNS characterized by involuntary, purposeless movements of the muscles. It may occur as an acute rheumatic involvement of the brain. Sydenham’s chorea is primarily seen in prepubertal girls.
Attacks of chorea, which begin slowly, may be preceded by increased tension and behavioral problems. The child becomes “clumsy,” may stumble and spill things, and may have difficulty buttoning clothes and writing. When the facial muscles are involved, grimaces occur. The child may laugh and cry inappropriately. In severe cases the patient may become completely incapacitated, and deterioration in speech may be noticeable. Treatment of Sydenham’s chorea is directed toward the relief of symptoms. The condition usually disappears spontaneously within weeks to months. Medication may also be required. The presence of Sydenham’s chorea alone can support the diagnosis of RF.
Rheumatic carditis: Carditis, an inflammation of the heart, is a manifestation of RF that can be fatal. It occurs more often in the young child. The tissues that cover the heart and the heart valves are affected. The heart muscle (myocardium) may be involved, as may the pericardium and the endocardium. The mitral valve, which is located between the left atrium and the left ventricle, is often involved. Vegetations form that interfere with the proper closing of the valve and disturb its normal function. When this valve becomes narrowed, the condition is called mitral stenosis. Myocardial lesions called Aschoff’s bodies are also characteristic of the disease. The burden on the heart is great, because it must pump harder to circulate the blood. As a result, it may become enlarged. Symptoms of poor circulation and heart failure may appear.
The child has an irregular, low-grade fever; is pale and listless; and has a poor appetite. Moderate anemia and weight loss are apparent. The child may experience dyspnea on exertion. The pulse and respiration rates are out of proportion to the body temperature. The physician may detect a soft murmur over the apex of the heart.
Diagnosis: The diagnosis of RF is difficult to make, and for this reason the Jones criteria have been developed and modified over the years (Box 26-1). The presence of two major criteria or one major and two minor criteria, supported by evidence of recent streptococcal infection, indicates a high probability of rheumatic fever. A careful physical examination is done, and a complete history of the patient is obtained. Certain blood tests are helpful. The erythrocyte sedimentation rate (ESR) is elevated. Abnormal proteins, such as C-reactive protein, may also be evident in the blood serum. Leukocytosis may occur but is not regularly present. Antibodies against the streptococci (measured by ASO titer) may also be detected. Additional studies may include chest x-rays, throat culture, and pulmonary function tests. The electrocardiogram, a graphic record of the electrical changes caused by the beating of the heart, is very useful. Changes in conductivity, particularly a prolonged PR interval (first-degree heart block), may indicate carditis. These tests are repeated throughout the course of the disease so the physician may determine when the active stage has subsided.
Treatment and Nursing Care: Treatment is aimed at preventing permanent damage to the heart. This is accomplished by antibacterial therapy, physical and mental rest, relief of pain and fever, and management of cardiac failure should it occur. Initial antibacterial therapy is directed toward eliminating the streptococcal infection. Penicillin is the drug of choice (given for a 10-day period) unless the patient is sensitive to it, in which case erythromycin is substituted.
Elimination of infection through medication is followed by long-term chemoprophylaxis (prevention of disease by drugs); intramuscular benzathine penicillin G is given monthly to children with a history of RF or evidence of rheumatic heart disease for a minimum of a 5-year period or until an age of 18 years is attained. Oral administration is considered for patients with minimal involvement whose reliability about taking medications can be confirmed. Erythromycin is recommended for long-term therapy for children who cannot tolerate penicillin. Financial assistance may be available to patients and their families. Local heart associations, rehabilitation services, and state and municipal health departments are sources of such aid.
Antiinflammatory drugs are used to decrease fever and pain. Aspirin is the drug of choice for joint disease without evidence of carditis. The use of steroids is reserved for severe cardiac symptoms or when aspirin does not relieve cardiac pain. Concerns during therapy include aspirin toxicity and the effects of aspirin on blood clotting. Mild signs of Cushing’s disease, such as moon face, acne, and hirsutism (increased hairiness), should be anticipated with the use of steroids. More severe reactions such as gastric ulcer, hypertension, overwhelming infection, and toxic psychosis may occur. Phenobarbital is effective in reducing chorea. Padded side rails are used to protect the patient who experiences spasms. If CHF occurs, symptomatic treatment is given.
Bed rest during the initial attack is recommended until the ESR returns to normal levels. The amount of work the heart must do must be limited by resting the entire body. In this way the circulation of the heart is slower, and the heart does not need to work as fast or as hard as when a child is active. The nurse should teach parents and children about the need for rest and the types of play activity appropriate during home care.
Nursing activities should be organized to ensure as few interruptions as possible to prevent tiring the patient. A bed cradle can be used to prevent pressure on painful extremities. Care includes special attention to the skin, especially over bony prominences; back care; good oral hygiene; and small, frequent feedings of nourishing foods. Maintaining healthy teeth and preventing cavities is of special importance. The patient with RF is particularly susceptible to subacute bacterial endocarditis, which can occur as a complication of dental or other procedures likely to cause bleeding or infection. Prophylactic antibiotic treatment is required before any dental procedure. Nutrition consists of small servings from the basic food groups. These are increased as the child’s appetite improves. A record of fluid intake and output is kept, because overhydration may tax the heart. All efforts are made to provide emotional support for the child and family. Provision should be made for the child to continue school studies.
Prevention: Prevention of infection and prompt treatment of group A beta-hemolytic streptococcal infections can prevent the occurrence of RF. All throat infections should be cultured. Once a diagnosis of strep throat is established, the nurse stresses the need to complete antibiotic therapy even if symptoms disappear and the child “feels better.” Close medical supervision and follow-up care are essential. The prognosis is favorable.
Systemic Hypertension
Pathophysiology: Hypertension, or high blood pressure, is being seen more often during childhood and adolescence. Blood pressure is a product of peripheral vascular resistance and cardiac output. An increase in cardiac output or peripheral resistance results in an increase in blood pressure. Systemic blood pressure increases with age and is correlated with height and weight throughout childhood and adolescence. (See Appendixes H and I for blood pressure measurements in infants and children.) Significant hypertension is considered when measurements are persistently at or above the 95th percentile for the patient’s age and sex. Hypertension is referred to as secondary when the increased pressure can be explained by a disease process. Renal, congenital, vascular, and endocrine disorders represent the majority of illnesses that account for secondary hypertension. Primary, or essential, hypertension implies that no known underlying disease is present. Nevertheless, heredity, obesity, stress, and a poor diet and exercise pattern can contribute to any type of hypertension.
There is increasing evidence that essential hypertension, although not generally seen until adolescence or adulthood, may have its roots in childhood. Prevention is thus significant in reducing the incidence of stroke or myocardial infarction as a person ages. The assessment of blood pressure levels should be part of every physical examination during childhood. Hypertension is more prevalent in children whose parents have high blood pressure. High blood pressure in children is usually discovered during a routine physical examination. Measuring blood pressure in young children requires careful attention to cuff size (see Chapter 22).
Treatment and Nursing Care: Treatment and nursing care involve nutritional counseling, weight reduction, and an age-appropriate program of aerobic exercise. Adolescents should be counseled concerning the adverse effects of drugs, alcohol, and tobacco on blood pressure. Drug therapy to reduce high blood pressure may not be effective in adolescents, who often are noncompliant with long-term regimens. The focus of treatment for secondary hypertension is the underlying disease causing the high blood pressure.
Prevention: The main focus of a hypertensive prevention program is patient education. The nurse can work with school personnel to promote awareness of the problem at parent-teacher association (PTA) meetings. Community health fairs should offer opportunities for blood pressure screening. Blood pressure measurement must be part of every routine physical examination. Risk factors such as obesity, elevated serum cholesterol levels, sedentary lifestyle, and drug, alcohol, or tobacco use should be discussed.
Hyperlipidemia
Hyperlipidemia refers to excessive lipids (fat and fatlike substances) in the blood. Lipoproteins contain lipids and proteins and include the following:
• Low-density lipoproteins (LDL), which contain a low amount of triglycerides, high level of cholesterol, and some protein. LDL carries cholesterol to the cells, which aids in cellular metabolism and steroid production.
• High-density lipoproteins (HDL) contain low amounts of triglycerides, little cholesterol, and high levels of protein. HDL carries cholesterol to the liver for excretion.
Children with a parental history of cholesterol levels exceeding 240 mg/dL or a family history of early cardiac death (under age 55 years) should have their cholesterol levels tested. Children with two consecutive blood levels of cholesterol exceeding 170 mg/dL should be followed closely and offered nutritional guidance.
However, screening only those children who are identified as high risk may not identify all children who need follow-up care. Because there is evidence that the factors responsible for degenerative vascular disease may begin in childhood and may be somewhat controllable, considerable interest has developed in screening children for risk factors and in attempting to change these risks (Table 26-2).

An active prevention program for all children and adolescents is essential. Lifelong healthy eating habits should be nurtured early and practiced by the entire family. The Step I dietary program advocated by the National Cholesterol Education Program involves no more than 300 mg of cholesterol per day and no more than 30% of total dietary calories from fat. Children under 2 years of age should not have a fat-restricted diet, because calories and fats are necessary for CNS growth and development. The American Academy of Pediatrics (AAP) recommendations for heart-healthy guidelines are presented below.
 Health Promotion
Health Promotion
Heart-Healthy Guidelines for Children
Provide breast milk or formula for 1 year.
Provide rice or other single-grain cereal from 4 to 6 months.
Provide a balanced mixture of cereal, vegetables, fruits, and meats for the second 6 months of life.
Baby foods are labeled regarding calories and nutrient composition; avoid foods with added sugar or salt. Most baby foods, with the exception of combined foods and desserts, do not have these additives.
Infants do not need desserts to grow; infant fruits are more nutritious.
Avoid excessive fats, salt, and refined sugars.
Avoid salty snacks and sweet desserts.
Offer heart-healthy snacks of vegetables, fruits, and finger foods.
Offer a variety of foods from the basic food groups.
Discourage the consumption of large amounts of milk, which can lead to nutritional imbalances.
Provide heart-healthy school lunches.
Role-model good daily exercise.
Screen children with family history of congenital heart disease (cholesterol, triglycerides, blood pressure).*
Emphasize the importance of heart-healthy foods to improve endurance and good body image.
Discourage the excessive intake of dietary saturated fat, sodium, sugar, and excess calories.
Be a nonsmoking parent as a model for the adolescent.
Assess stress management capabilities; counsel accordingly.
Screen periodically for serum cholesterol elevations and blood pressure measurements.
Provide serial monitoring of adolescents deemed to be at high risk (sustained high blood pressure readings on at least three separate occasions).
*Children over 2 years of age with a family history of hyperlipidemia or early atherosclerotic heart disease should undergo routine screening for hyperlipidemia.
Kawasaki Disease
Kawasaki disease (KD) (mucocutaneous lymph node syndrome) occurs worldwide and is the leading cause of acquired cardiovascular disease in the United States. It usually affects children under age 5 years. Studies have shown that KD may be a reaction to toxins produced by a previous infection with an organism such as the staphylococci. KD is not spread from person to person. The diagnosis is made by clinical signs and symptoms, because specific laboratory findings are not diagnostic. KD causes inflammation of the vessels in the cardiovascular system. The inflammation weakens the walls of the vessels and often results in an aneurysm (an abnormal dilation of the wall of a blood vessel). Aneurysms can cause thrombi (blood clots) to form, resulting in serious complications. Approximately 40% of untreated children develop aneurysms of the coronary vessels, which can be life threatening.
Manifestations: The onset is abrupt with a sustained fever, sometimes above 40° C (104° F), which does not respond to antipyretics or antibiotics. The fever lasts for more than 5 days. Conjunctivitis without discharge, fissured lips, a “strawberry tongue” (enlarged reddened papilla on the tongue), inflamed mouth and pharyngeal membranes, and enlarged nontender lymph nodes are seen. An erythematous skin rash develops, with swollen hands and desquamation (peeling) of the palms and soles (Figure 26-5). The child is very irritable and may develop signs of cardiac problems.

Treatment and Nursing Care: Intravenous (IV) gamma globulin given early in the illness can prevent the development of coronary artery pathology. Salicylate therapy (aspirin) is prescribed for its antithrombus properties. Warfarin (Coumadin) therapy may be prescribed if aneurysms are detected to prevent clot formation.
Nursing care is symptomatic and supportive. Parent teaching should be reinforced concerning the need to postpone active routine immunizations for eleven months after the administration of immune globulin, which is an immunosuppressant.
Long-term, low-dose aspirin therapy may be prescribed to prevent clot formation. Compliance may be a problem for any long-term regimen in which medication must be taken when the child feels “well.” The nurse should reinforce parent teaching concerning the recognition of cardiac problems and updating their CPR skills.
Get Ready for the NCLEX® Examination!
Key Points
• Signs and symptoms of congenital heart abnormalities in infants include dyspnea, difficulty with feedings, choking spells, recurrent respiratory infections, cyanosis, poor weight gain, clubbing of the fingers and toes, and heart murmurs.
• The nursing goals significant to the care of children with heart failure are to (1) reduce the work of the heart, (2) improve respiration, (3) maintain proper nutrition, (4) prevent infection, (5) reduce the anxiety of the parent, and (6) support growth and development.
• Congenital heart defects may be caused by genetic factors, maternal factors such as drug use or illness, or environmental factors. Acquired heart disease occurs after birth as a response to a defect or illness.
• Congenital heart defects that result in a recirculation of blood to the lungs do not usually produce cyanosis as a clinical sign.
• A congenital heart defect can cause an increase in pulmonary blood flow, a decrease in pulmonary blood flow, or an obstruction of blood flow.
• A difference in the blood pressure between the arms and the legs is characteristic of coarctation of the aorta.
• The defects in tetralogy of Fallot include pulmonary artery stenosis, hypertrophy of the right ventricle, dextroposition of the aorta, and a ventricular septal defect.
• Hypercyanotic “tet” spells are relieved by placing the child in a knee-chest position.
• Signs of congestive heart failure in infants include tachycardia, at-rest fatigue during feedings, and perspiration around the forehead.
• The dose of digoxin should be checked by two nurses before administration. A dose exceeding 0.05 mg should be reconfirmed with the health care provider.
• The major Jones criteria diagnostic of rheumatic fever include polyarthritis, erythema marginatum, Sydenham’s chorea, and rheumatic carditis.
• Chest tube drainage systems must always be kept below the level of the chest.
• A child under age 2 years should not have a fat-restricted diet.
Additional Learning Resources
 Go to your Study Guide for additional learning activities to help you master this chapter content.
Go to your Study Guide for additional learning activities to help you master this chapter content.
Go to your Evolve website (http://evolve.elsevier.com/Leifer) for the following FREE learning resources:
• Answer Guidelines for Critical Thinking Questions
• Answers and Rationales for Review Questions for the NCLEX® Examination
• Glossary with English and Spanish pronunciations
• Interactive Review Questions for the NCLEX® Examination
• Patient Teaching Plans in English and Spanish
 Online Resources
Online Resources• American Heart Association: www.americanheart.org/presenter.jhtml?identifier=4498
• Kawasaki’s disease: www.mayoclinic.com/health/kawasaki-disease/DS00576
• Tetralogy of Fallot: www.nhlbi.nih.gov/health/dci/Diseases/tof/tof_what.html; www.Cincinnatichildrens.org/health/heart
Review Questions for the NCLEX® Examination
1. When administering digoxin (Lanoxin) to an infant, the medication should be withheld and the physician notified if the:
2. An infant with tetralogy of Fallot is experiencing a tet attack involving cyanosis and dyspnea. Which position should the infant be placed in?
3. Prevention of rheumatic fever can best be accomplished by:
1. keeping children with fever home.
2. sending children with sore throats home from school.
4. The nurse is assessing a child admitted with possible Kawasaki’s disease. A characteristic sign or symptom that the nurse should observe and document would be:
5. A child who has had heart surgery returns to the pediatric unit with a chest tube and drainage bottles in place. What is a priority nursing responsibility when caring for a child with chest tubes?
Critical Thinking Questions
1. A child who was diagnosed with Kawasaki’s disease is discharged home with directions to take a low-dose aspirin tablet once a day. The parent states that she heard that aspirin is contraindicated for use in children and asks if she can substitute Tylenol instead. What is the best response of the nurse?
2. A parent states that her 4-month-old infant is scheduled for heart transplant surgery in 2 weeks. She states that the infant is now due for her second immunization series and asks if the child will be better protected if she has the immunizations now before she has the surgery. What is the best response of the nurse?