Fetal Development
1 Define each key term listed.
2 Describe the process of gametogenesis in human reproduction.
3 Explain human fertilization and implantation.
4 Describe embryonic development.
5 Describe fetal development and the maturation of body systems.
6 Describe the development and functions of the placenta, the umbilical cord, and the amniotic fluid.
7 Compare fetal circulation to circulation after birth.
8 Explain the similarities and differences in the two types of twins.
 , p. 34)
, p. 34) , p. 34)
, p. 34) , p. 31)
, p. 31) , p. 41)
, p. 41) , p. 32)
, p. 32) , p. 31)
, p. 31) , p. 41)
, p. 41) , p. 31)
, p. 31) , p. 38)
, p. 38) , p. 31)
, p. 31) , p. 31)
, p. 31) http://evolve.elsevier.com/Leifer
http://evolve.elsevier.com/Leifer
The human body contains many millions of cells at birth, but life begins with a single cell created by the fusion of a sperm with an ovum. Deoxyribonucleic acid (DNA) programs a genetic code into the nucleus of the cell; the nucleus controls the development and function of the cell. Defects in the DNA code can result in inherited disorders. The genes and chromosomes contained within the DNA determine the uniqueness of the traits and features of the developing person.
Normal human chromosomes begin in pairs, one supplied by the mother and the other by the father. Each body cell contains 46 chromosomes, made up of 22 pairs of autosomes (body chromosomes) and 1 pair of sex chromosomes that determine the sex of the fetus. Each chromosome contains genes that involve heredity. Cell division then occurs, which is the basis of human growth and regeneration.
Biological development is not isolated. It is influenced by the external environment, such as maternal drug use (teratogens that cause damage to growing cells include some prescribed medications), maternal undernutrition, or smoking by the mother, and it is now known that sounds such as music are heard by the fetus and are recognized by the newborn. All these factors influence prenatal growth and development. Early prenatal care is essential to the optimum outcome of the pregnancy (see Chapter 4).
Cell Division and Gametogenesis
The division of a cell begins in its nucleus, which contains the gene-bearing chromosomes. The two types of cell division are mitosis and meiosis. Mitosis is a continuous process by which the body grows and develops and dead body cells are replaced. In this type of cell division, each daughter cell contains the same number of chromosomes as the parent cell. The 46 chromosomes in a body cell are called the diploid number of chromosomes. The process of mitosis in the sperm is called spermatogenesis, and in the ovum it is called oogenesis.
Meiosis is a different type of cell division in which the reproductive cells undergo two sequential divisions. During meiosis the number of chromosomes in each cell is reduced by half to 23 chromosomes per cell, each including only one sex chromosome. This is called the haploid number of chromosomes. This process is completed in the sperm before it travels toward the fallopian tube and in the ovum if it is fertilized after ovulation. At the moment of fertilization (when the sperm and the ovum unite), the new cell contains 23 chromosomes from the sperm and 23 chromosomes from the ovum, thus returning to the diploid number of chromosomes (46); traits are therefore inherited from both the mother and the father. The formation of gametes by this type of cell division is called gametogenesis (Figure 3-1).
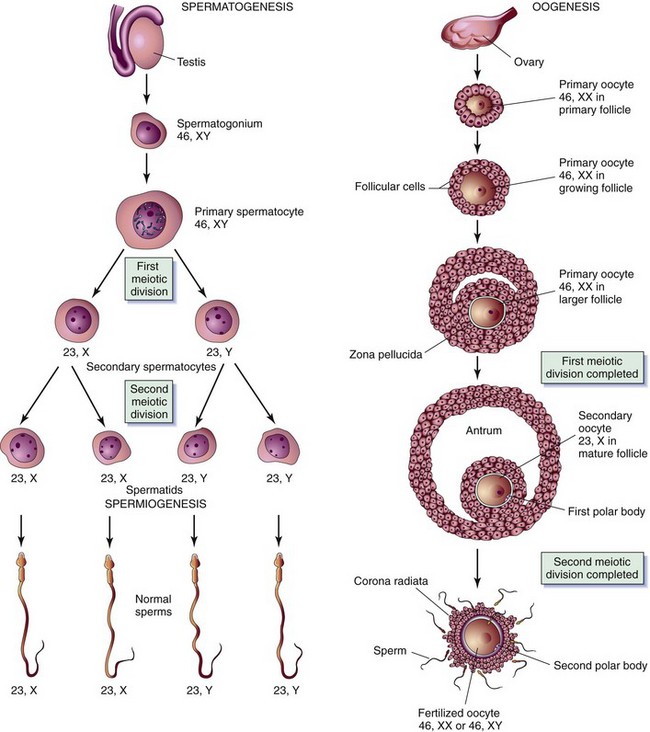
FIGURE 3-1 Normal gametogenesis. Four sperm develop from one spermatocyte, each with 23 chromosomes—including one sex chromosome, either an X or a Y. In oogenesis, one ovum develops with 23 chromosomes—including one sex chromosome, always an X. An XY combination produces a boy, and an XX combination produces a girl.
Fertilization
Fertilization occurs when a sperm penetrates an ovum and unites with it, restoring the total number of chromosomes to 46. It normally occurs in the outer third of the fallopian tube, near the ovary (Figure 3-2). The sperm pass through the cervix and the uterus and into the fallopian tubes by means of the flagellar (whiplike) activity of their tails and can reach the fallopian tubes within 5 minutes after coitus. As soon as fertilization occurs, a chemical change in the membrane around the fertilized ovum prevents penetration by another sperm.
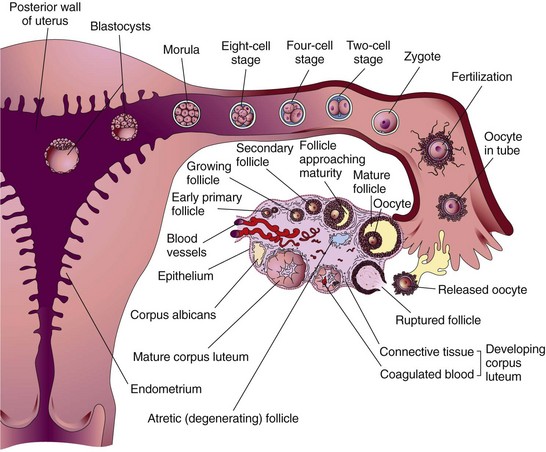
FIGURE 3-2 Ovulation and fertilization. Ovulation occurs; the egg is caught by the fimbriae (fingerlike projections of the fallopian tube) and is guided into the fallopian tube, where fertilization occurs. The zygote continues to multiply (but not grow in size) as it passes through the fallopian tube and implants into the posterior wall of the uterus.
The time during which fertilization can occur is brief because of the short life span of mature gametes. The ovum is estimated to survive for up to 24 hours after ovulation. The sperm remains capable of fertilizing the ovum for up to 5 days after being ejaculated into the area of the cervix.
 Nursing Tip
Nursing Tip
During sexual counseling the nurse should emphasize that the survival time of sperm ejaculated into the area of the cervix may be up to 5 days and that pregnancy can occur with intercourse as long as 5 days before ovulation.
Sex Determination
The sex of human offspring is determined at fertilization. The ovum always contributes an X chromosome (gamete), whereas the sperm can carry an X or a Y chromosome (gamete). When a sperm carrying the X chromosome fertilizes the X-bearing ovum, a female child (XX) results. When a Y-bearing sperm fertilizes the ovum, a male child (XY) is produced (Figure 3-3).
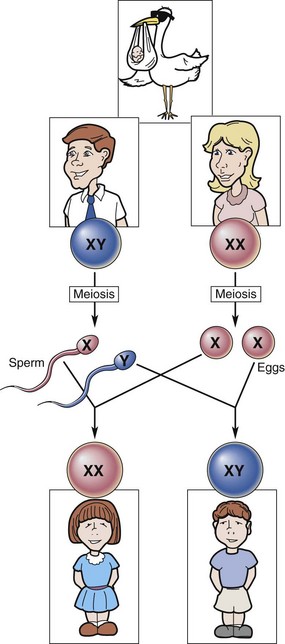
FIGURE 3-3 Sex determination. If an X chromosome from the male unites with an X chromosome from the female, the child will be a female (XX). If a Y chromosome from the male unites with an X chromosome from the female, the child will be a male (XY).
Because sperm can carry either an X or a Y chromosome, the male partner determines the sex of the child. However, the pH of the female reproductive tract and the estrogen levels of the woman’s body affect the survival rate of the X- and Y-bearing sperm as well as the speed of their movement through the cervix and the fallopian tubes. Thus the female has some influence on which sperm fertilizes the mature ovum.
Inheritance
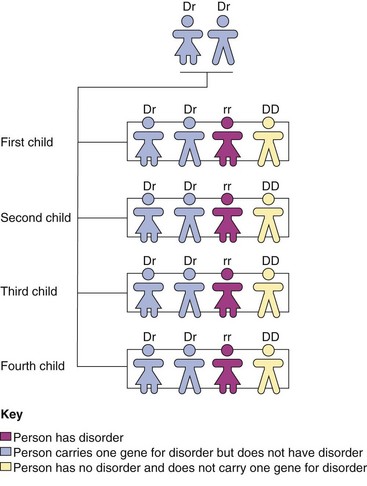
Each gene (a segment of the DNA chain) is coded for inheritance. The coded information carried by the DNA in the gene is responsible for individual traits, such as eye and hair color, facial features, and body shape. Genes carry instructions for dominant and recessive traits. Dominant traits usually overpower recessive traits and are passed on to the offspring. If only one parent carries a dominant trait, an average of 50% of the offspring will have (and thus display) that dominant trait. If each parent carries a recessive trait, there is a higher chance that one of the offspring will display that trait (Figure 3-4).
Tubal Transport of the Zygote
The zygote is the cell formed by the union of the sperm and the ovum, and it is transported through the fallopian tube and into the uterus. Fertilization normally occurs in the outer third of the fallopian tube. During transport through the fallopian tube, the zygote undergoes rapid mitotic division, or cleavage. Cleavage begins with two cells, which subdivide into four and then eight cells to form the blastomere. The size of the zygote does not increase; rather, the individual cells become smaller as they divide and eventually form a solid ball called the morula (see Figure 3-2).
The morula enters the uterus on the third day and floats there for another 2 to 4 days. The cells form a cavity, and two distinct layers evolve. The inner layer is a solid mass of cells called the blastocyst (see Figure 3-2), which develops into the embryo and the embryonic membranes. The outer layer of cells, called the trophoblast, develops into an embryonic membrane, the chorion. Occasionally the zygote does not move through the fallopian tube and instead becomes implanted in the lining of the tube, resulting in a tubal ectopic pregnancy (see Chapter 5).
Implantation of the Zygote
The zygote usually implants in the upper section of the posterior uterine wall. The cells burrow into the prepared lining of the uterus, called the endometrium. The endometrium is now called the decidua; the area under the blastocyst is called the decidua basalis and gives rise to the maternal part of the placenta (Figure 3-5).
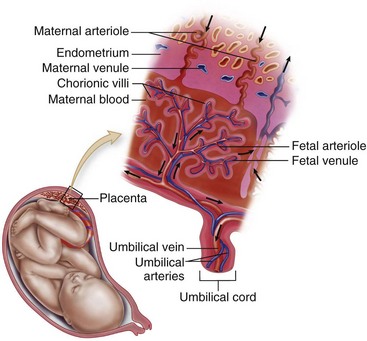
FIGURE 3-5 Maternal-fetal circulation showing the relationship of the fetus and the placenta in the uterus. Close placement of the fetal blood supply to the maternal blood in the placenta is shown. The maternal blood in the lacuna permits the diffusion of nutrients and other substances; some harmful substances are prevented from passing through by a thin placental barrier. No mixing of fetal or maternal blood occurs.
Development
During the week between fertilization and implantation, the cells within a zygote are identical to one another. After implantation the cells begin to differentiate and develop special functions. The chorion, the amnion, the yolk sac, and the primary germ layers appear.
Chorion
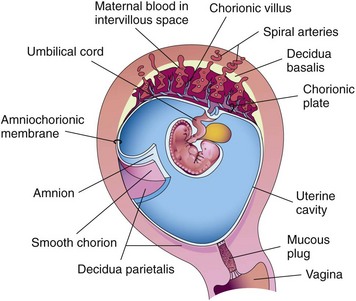
The chorion develops from the trophoblast (outer layer of embryonic cells) and envelops the amnion, embryo, and yolk sac. It is a thick membrane with fingerlike projections called villi on its outermost surface. The villi immediately below the embryo extend into the decidua basalis on the uterine wall and form the embryonic or fetal portion of the placenta (Figure 3-6).
Amnion
The amnion is the second membrane; it is a thin structure that envelops and protects the embryo. It forms the boundaries of the amniotic cavity, and its outer aspect meets the inner aspect of the chorion.
The chorion and the amnion together form an amniotic sac filled with fluid (bag of waters) that permits the embryo to float freely. Amniotic fluid is clear, has a mild odor, and often contains bits of vernix (fetal skin covering) or lanugo (fetal hair on the skin). The volume of amniotic fluid steadily increases from about 30 mL at 10 weeks of pregnancy to 350 mL at 20 weeks. The volume of fluid is about 1000 mL at 37 weeks. In the latter part of pregnancy the fetus may swallow up to 400 mL of amniotic fluid per day and normally excretes urine into the fluid. The following are functions of amniotic fluid:
Yolk Sac
On the ninth day after fertilization a cavity called the yolk sac forms in the blastocyst. It functions only during embryonic life and initiates the production of red blood cells. This function continues for about 6 weeks, until the embryonic liver takes over. The umbilical cord then encompasses the yolk sac, and the yolk sac degenerates.
Germ Layers
After implantation the zygote in the blastocyst stage transforms its embryonic disc into three primary germ layers known as ectoderm, mesoderm, and endoderm. Each germ layer develops into a different part of the growing embryo. The specific body parts that develop from each layer are listed in Box 3-1.
Prenatal Developmental Milestones
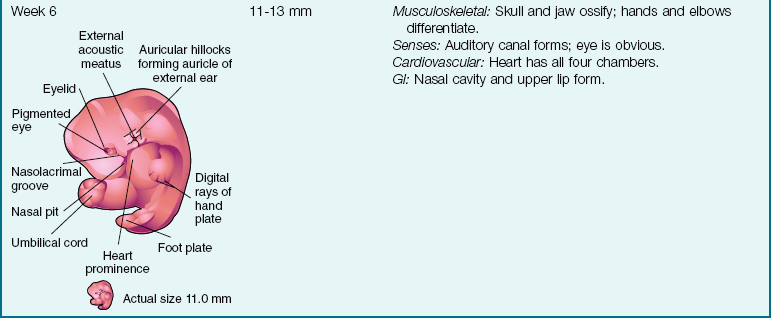
Table 3-1 follows the developmental milestones during intrauterine development. Developmental milestones exist in fetal growth and development, as they do in growth and development after birth. Three basic stages characterize prenatal development: zygote, embryo, and fetus. The zygote continues to grow and develop as it passes through the fallopian tube and implants into the wall of the uterus. The second to the eighth week of development is known as the embryonic stage; the developing infant is called an embryo. From the ninth week of development until birth the developing infant is called a fetus. By the second week after fertilization the ectoderm, the endoderm, and the amnion begin to develop.
Table 3-1
Embryonic and Fetal Development
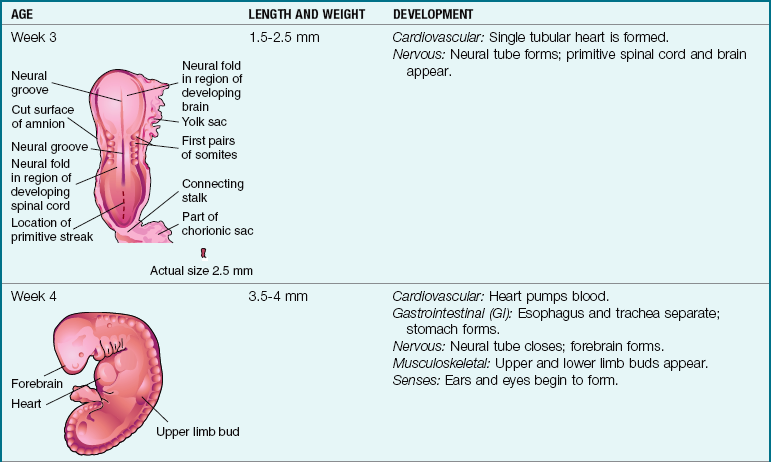
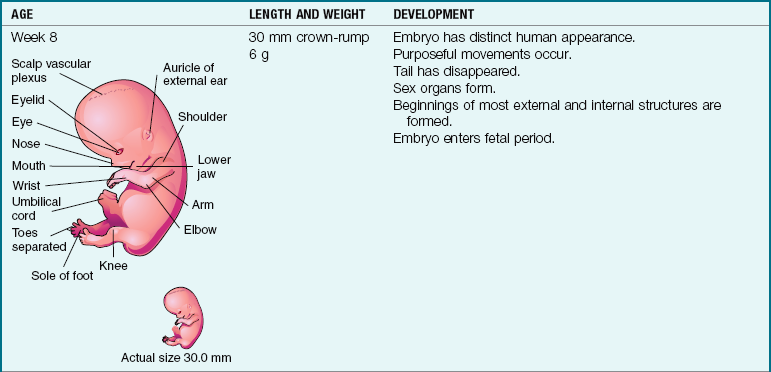
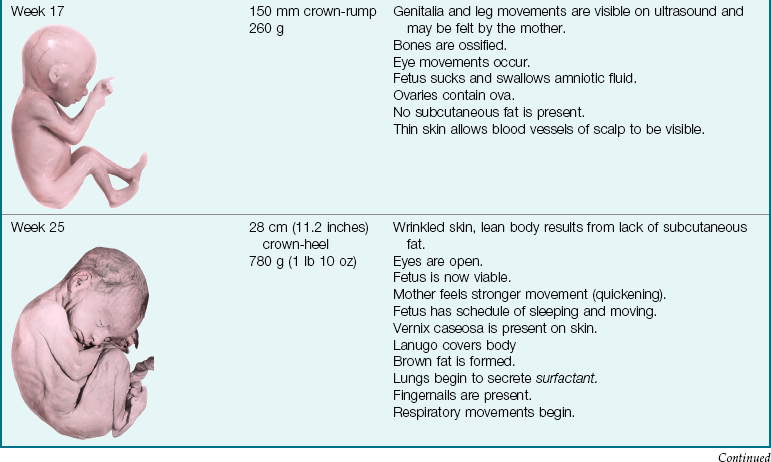
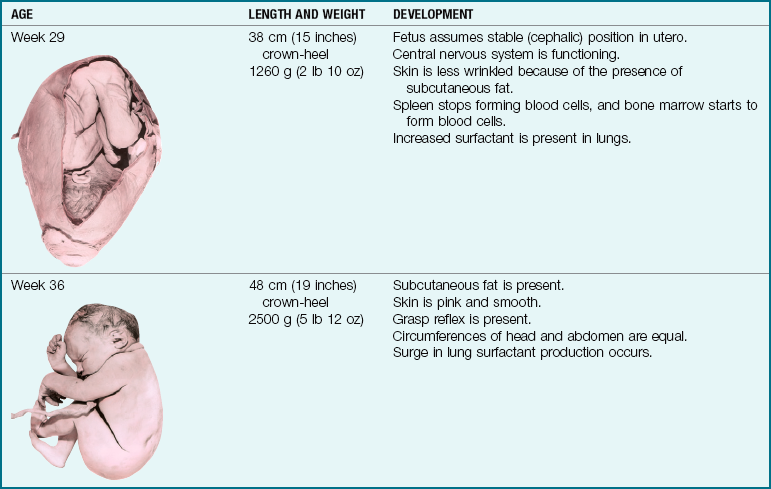
Note: Full term is considered 38 to 40 weeks of gestation. The crown-heel length is 48 to 52 cm (18 to 21 inches), and the weight is 3000 to 3600 g (6 lb 1 oz to 7 lb 15 oz).
By the third week the mesoderm and neural tube form, and the primitive heart begins to pump. It is at this time that some mothers first realize they have “missed” their menstrual period and suspect they are pregnant (therefore the fetus is affected by maternal influences even before the pregnancy becomes known).
 Nutrition Considerations
Nutrition Considerations
Folic Acid and Neural Tube Defects
It is now known that folic acid supplements can prevent most neural tube defects such as spina bifida. However, in an unplanned pregnancy, it is possible for a neural tube defect to occur before the mother confirms her pregnancy state. Early prenatal care with good nutrition and folic acid supplements are desirable so the embryo is protected in the very first days and weeks of development.
By 8 weeks of gestation the ovaries or testes are present, the beginnings of all systems have developed, and there is movement in the extremities. The fetal period begins at the ninth week, and by the tenth week the external genitalia are visible to ultrasound examination. At the fourteenth week the fetus moves in response to external stimuli. By 20 weeks of gestation the lungs have matured functionally enough for the fetus to survive outside the uterus (age of viability), but special care in the neonatal intensive care unit (NICU) would be required. The status of the fetus in utero can be monitored by fetal movements (kick counts). By 28 weeks the eyes open and the fetal position in the uterus becomes more stable. The fetus is considered to be full term at 38 to 40 weeks of gestation.
Infant survival and development at birth depends not only on the infant’s biological development but also on the response of the parent (see Table 15-5). The preparation of the parents during pregnancy is vital to the development of a positive, nurturing relationship between the parents and infant. The development of the fetus (see Table 3-1) can be correlated with the psychological and physical changes in the mother that occur prenatally (see Table 4-6).
Accessory Structures of Pregnancy
The placenta, the umbilical cord, and the fetal circulation support the fetus as it completes prenatal life and prepares for birth.
Placenta
The placenta (afterbirth) is a temporary organ for fetal respiration, nutrition, and excretion. It also functions as an endocrine gland. The placenta forms when the chorionic villi of the embryo extend into the blood-filled spaces of the mother’s decidua basalis. The maternal part of the placenta arises from the decidua basalis and has a beefy, red appearance. The fetal side of the placenta develops from the chorionic villi and the chorionic blood vessels. The amnion covers the fetal side and the umbilical cord and gives them a grayish, shiny appearance at term.
Nursing Tip
The placenta is much larger than the developing infant during early pregnancy, but the fetus grows faster. At term, the placenta weighs about one sixth the weight of the infant.
Placental Transfer
A thin membrane separates the maternal and fetal blood, and the two blood supplies do not normally mix (see Figure 3-5). However, separation of the placenta at birth may allow some fetal blood to enter the maternal circulation, which can cause problems with fetuses in subsequent pregnancies if the blood types are not compatible (see Chapter 5).
Fetal deoxygenated blood and waste products leave the fetus through the two umbilical arteries and enter the placenta through the branch of a main stem villus, which extends into the intervillus space (lacuna). Oxygenated, nutrient-rich blood from the mother spurts into the intervillus space from the spiral arteries in the decidua (see Figures 3-5 and 3-6). The fetal blood releases carbon dioxide and waste products and takes in oxygen and nutrients before returning to the fetus through the umbilical vein.
The thin placental membrane provides some protection but is not a barrier to most substances ingested by the mother. Many harmful substances such as drugs (therapeutic and abused), nicotine, and viral infectious agents are transferred to the fetus and may cause fetal drug addiction, congenital anomalies, and fetal infection.
Placental Hormones
Four hormones are produced by the placenta: progesterone, estrogen, human chorionic gonadotropin (hCG), and human placental lactogen (hPL).
Progesterone: Progesterone is first produced by the corpus luteum and later by the placenta. It has the following functions during pregnancy:
Estrogen: Estrogen has three important functions during pregnancy:
2. Increases the blood flow to uterine vessels
3. Stimulates development of the breast ducts to prepare for lactation
The effects of estrogen not directly related to pregnancy include the following:
Human Chorionic Gonadotropin: hCG is the hormone “signal” sent to the corpus luteum that conception has occurred. The hCG causes the corpus luteum to persist and to continue the production of estrogen and progesterone to sustain pregnancy. hCG is detectable in maternal blood as soon as implantation occurs—usually 7 to 9 days after fertilization—and is the basis for most pregnancy tests.
Umbilical Cord
The umbilical cord develops with the placenta and fetal blood vessels and is the lifeline between mother and fetus. Two arteries carry blood away from the fetus, and one vein returns blood to the fetus. Wharton’s jelly covers and cushions the cord vessels and keeps the three vessels separated. The vessels are coiled within the cord to allow movement and stretching without restricting circulation. The normal length of the cord is about 55 cm (22 inches). The umbilical cord usually protrudes from the center of the placenta.
 Memory Jogger
Memory JoggerFetal Circulation
After the fourth week of gestation, circulation of blood through the placenta to the fetus is well-established (see Figure 3-5). Because the fetus does not breathe and the liver does not have to process most waste products, several physiological diversions in the prebirth circulatory route are needed. There are three fetal circulatory shunts:
1. Ductus venosus: diverts some blood away from the liver as it returns from the placenta
2. Foramen ovale: diverts most blood from the right atrium directly to the left atrium, rather than circulating it to the lungs
3. Ductus arteriosus: diverts most blood from the pulmonary artery into the aorta
Circulation Before Birth
Oxygenated blood enters the fetal body through the umbilical vein. About half of the blood goes to the liver through the portal sinus, with the remainder entering the inferior vena cava through the ductus venosus. Blood in the inferior vena cava enters the right atrium, where most passes directly into the left atrium through the foramen ovale. A small amount of blood is pumped to the lungs by the right ventricle. The rest of the blood from the right ventricle joins that from the left ventricle through the ductus arteriosus. After circulating through the fetal body, blood containing waste products is returned to the placenta through the umbilical arteries.
Circulation After Birth
Fetal shunts are not needed after birth once the infant breathes and blood is circulated to the lungs. The foramen ovale closes because pressure in the right side of the heart falls as the lungs become fully inflated and there is now little resistance to blood flow. The infant’s blood oxygen level rises, causing the ductus arteriosus to constrict. The ductus venosus closes when the flow from the umbilical cord stops (Figure 3-7).
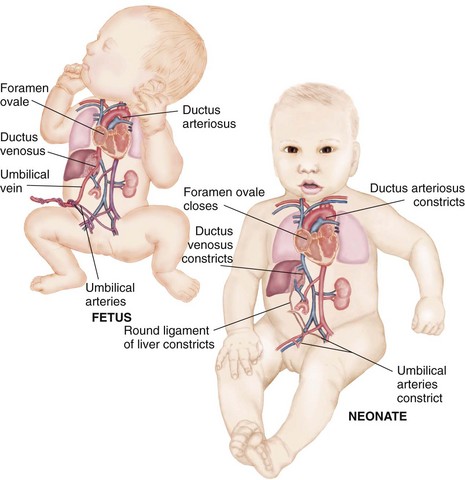
FIGURE 3-7 Changes in fetal-newborn circulation at birth. The changes in the circulation of the fetus and the neonate are shown. The ductus arteriosus, the ductus venosus, and the foramen ovale are shunts that close because of the expansion of the lungs and pressure changes within the heart.
Closure of Fetal Circulatory Shunts
The foramen ovale closes functionally (temporarily) within 2 hours after birth and permanently by age 3 months. The ductus arteriosus closes functionally within 15 hours and permanently in about 3 weeks. The ductus venosus closes functionally when the cord is cut and permanently in about 1 week. After permanent closure, the ductus arteriosus and the ductus venosus become ligaments.
Because the foramen ovale and ductus arteriosus are initially closed functionally, some conditions may cause one or the other to reopen after birth. A condition that impedes full lung expansion (e.g., respiratory distress syndrome) can increase resistance to blood flow from the heart to the lungs, causing the foramen ovale to reopen. Similar conditions often reduce the blood oxygen levels and can cause the ductus arteriosus to remain open. See Chapter 26 for further discussion of newborn congenital cardiac problems.
Impaired Prenatal Development and Subsequent Illness
Research has shown that undernutrition in utero can result in permanent changes in fetal structure, physiology, and metabolism and can influence the development of conditions such as heart disease and stroke in adult life (see Health Promotion box). Other factors that influence health in later life can be exposure to toxins in utero or factors that occur in the first 3 years of growth and development.
 Health Promotion
Health Promotion
Healthy People 2020: Fetal Nutrition and Development
The growth of the fetus is limited by the nutrients and oxygen received from the mother. A mother’s ability to nourish her fetus is established in her own fetal life and by her adult nutritional experience. Therefore, to prevent illness in the next generation, there must be a focus on the health practices of this generation. A healthy mother can produce a healthy child who is less prone to develop illness. Part of the goal of Healthy People 2020 is to develop a healthy lifestyle in all people so that as parents they can nourish and parent healthy children for the next generation.
During the first 3 months of fetal life the fetus is most susceptible to external influences such as undernutrition. However, different organs and tissues undergo rapid development at specific times during gestational life and are therefore sensitive to undernourishment or viral and/or toxic influences during these periods.
Infants with intrauterine growth restriction may have a reduced number of cells in their organs and can therefore be predisposed to the development of specific diseases later in life. For example, a reduced number of pancreatic beta cells can impair insulin secretion and result in a health problem in the adult. Obesity, inactivity, and other factors during the life span influence the timing and severity of disease in the adult.
It is also possible that in utero changes in vascular or renal structures or in hormonal systems resulting from in utero malnourishment can influence the development of hypertension later in life. Studies have also shown that impaired fetal liver growth in late gestation can permanently impair lipid metabolism and predispose to increased cholesterol levels in adult life. A reduced liver size can be identified by measuring abdominal circumference at birth. The best assessment of fetal growth takes weight, length of gestation, placental size, and newborn head and abdominal circumference into consideration.
Multifetal Pregnancy
Twins occur once in every 90 pregnancies in North America. When hormones are given to assist with ovulation, twinning and other multifetal births (triplets, quadruplets, and quintuplets) are more likely to occur. The first set of septuplets (seven fetuses) to survive was born in the United States in 1997. In 2009, the first set of octuplets was born, all of whom survived.
Monozygotic (MZ) twins (Figure 3-8, A), often called identical twins, are genetically identical, are of the same sex, and look alike, because they develop from a single fertilized ovum. Physical differences between monozygotic twins are caused by prenatal environmental factors involving variations in the blood supply from the placenta. Most monozygotic twins begin to develop at the end of the first week after fertilization. The result is two identical embryos, each with its own amnion but with a common chorion and placenta and some common placental vessels. If the embryonic disc does not divide completely, various types of conjoined (formerly called Siamese) twins may form. They are named according to the regions that are joined (e.g., thoracopagus indicates an anterior connection of the thoracic regions). Conjoined twins have a single amnion.
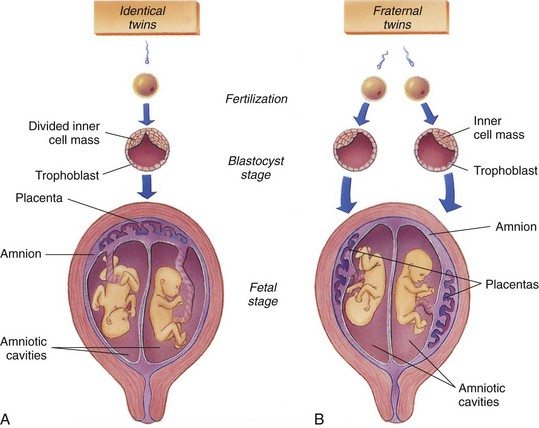
FIGURE 3-8 Multiple births. A, Identical (monozygotic) twins develop when the embryonic tissue from a single egg splits to form two individuals. The placenta is shared by the twins. B, Fraternal (dizygotic) twins develop when two different ova are fertilized at the same time by two different sperm, producing separate zygotes. Each twin has its own placenta, amnion, and chorion.
Dizygotic (DZ) twins (see Figure 3-8, B), also called fraternal twins, may or may not be of the same sex and develop from two separate ova fertilized by two separate sperm. Dizygotic twins always have two amnions, two chorions, and two placentas, although their chorions and placentas sometimes fuse. Dizygotic twin pregnancies tend to repeat in families, and the incidence increases with maternal age. The twins are about as much alike as any siblings.
Many twin or higher multiples are born prematurely because the uterus becomes overly distended. The placenta may not be able to supply sufficient nutrition to both fetuses, with the result that one or both twins is smaller than average.
Get Ready for the NCLEX® Examination!
Key Points
• The uniqueness of each individual results from the blending of genes on the 46 chromosomes contained in each body cell and the environment of the embryo and fetus during development.
• Gametogenesis in the male is called spermatogenesis. Each mature sperm has 22 autosomes, plus either an X or a Y sex chromosome, for a total of 23. Gametogenesis in the female is called oogenesis. It begins at ovulation and is not completed until fertilization occurs. The mature ovum has 22 autosomes plus the X sex chromosome, for a total of 23. At conception the total number of chromosomes is restored to 46.
• When the ovum is fertilized by an X-bearing sperm, a female offspring results; when it is fertilized by a Y-bearing sperm, the child will be male.
• After fertilization in the fallopian tube, the zygote enters the uterus, where implantation is complete by 7 days after fertilization. If the zygote fails to move through the tube, implantation occurs there and a tubal ectopic pregnancy results.
• When implantation occurs in the uterine lining, the cells of the zygote differentiate and develop into the following structures: chorion, amnion, yolk sac, and primary germ layers. The chorion develops into the embryonic or fetal portion of the placenta; the amnion encloses the embryo and the amniotic fluid; the primary germ layers develop into different parts of the growing fetus; and the yolk sac, which functions only during embryonic life, begins to form red blood cells.
• The three germ layers of the embryo are the ectoderm, the mesoderm, and the endoderm. All structures of the individual develop from these layers.
• All body systems are formed and functioning in a simple way by the end of the eighth week.
• The accessory structures of pregnancy are the placenta, the umbilical cord, and the fetal circulation.
• These structures continuously support the fetus throughout prenatal life in preparation for birth.
• The placenta is an organ for fetal respiration, nutrition, and excretion. It is also a temporary endocrine gland that produces progesterone, estrogen, human chorionic gonadotropin (hCG), and human placental lactogen (hPL).
• Fetal circulation transports oxygen and nutrients to the fetus and disposes of carbon dioxide and other waste products from the fetus. The temporary fetal circulatory structures are the foramen ovale, the ductus arteriosus, and the ductus venosus. They divert most blood from the fetal liver and lungs because these organs do not fully function during prenatal life.
Additional Learning Resources
 Go to your Study Guide for additional learning activities to help you master this chapter content.
Go to your Study Guide for additional learning activities to help you master this chapter content.
Go to your Evolve website (http://evolve.elsevier.com/Leifer) for the following FREE learning resources:
• Answer Guidelines for Critical Thinking Questions
• Answers and Rationales for Review Questions for the NCLEX® Examination
• Glossary with English and Spanish pronunciations
• Interactive Review Questions for the NCLEX® Examination
• Patient Teaching Plans in English and Spanish
 Online Resources
Online Resources• Female reproductive system: www.nlm.nih.gov/medlineplus/femalereproductivesystem.html
• Fetal Diagnostic Centers: www.fetal.com
• Intrauterine growth restriction: http://familydoctor.org/online/famdocen/home/women/pregnancy/fetal/313.html
• Male reproductive system: www.nlm.nih.gov/medlineplus/malereproductivesystem.html
Review Questions for the NCLEX® Examination
1. The child’s sex is determined by the:
1. dominance of either the X or the Y chromosome.
2. number of X chromosomes in the ovum.
2. A woman who wants to become pregnant should avoid all medications unless they are prescribed by a physician who knows she is pregnant, because:
1. the placenta allows most medications to cross into the fetus.
2. medications often have adverse effects when taken during pregnancy.
3. fetal growth is likely to be slowed by many medications.
4. the pregnancy is likely to be prolonged by some medications.
3. The umbilical cord normally contains:
Critical Thinking Questions
1. A patient discusses her family planning decisions. She states that she will come to the clinic for prenatal care and will begin to take prenatal vitamins as soon as she knows she is pregnant. What would be the best response from the nurse?
2. A patient in the thirty-second week of gestation states she wants to deliver her infant now because she feels so “big and uncomfortable.” She states that she knows the infant has been fully formed since the first trimester and does not mind if it is a little small at birth. What would be the best response from the nurse?