The Child with a Respiratory Disorder
1 Define each key term listed.
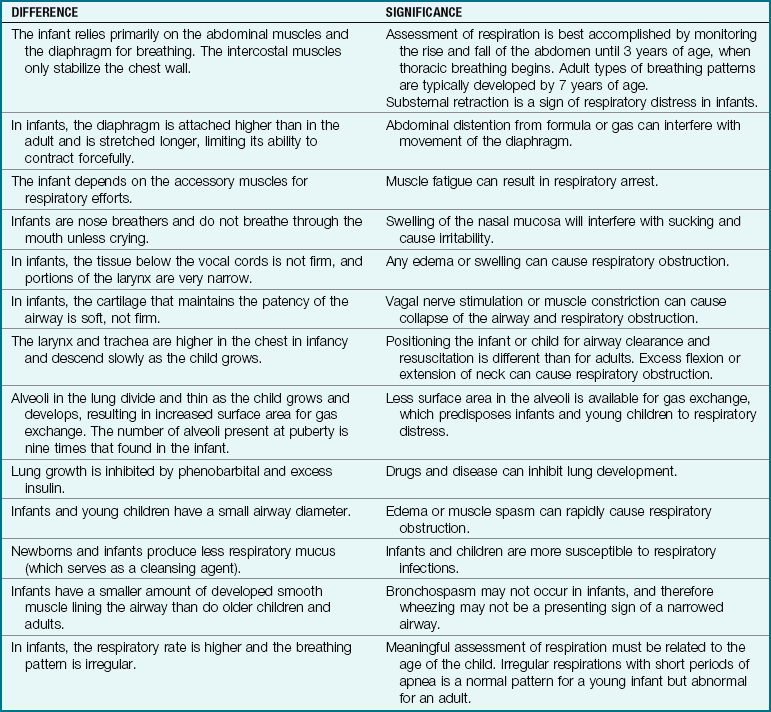
2 Distinguish the differences between the respiratory tract of the infant and that of the adult.
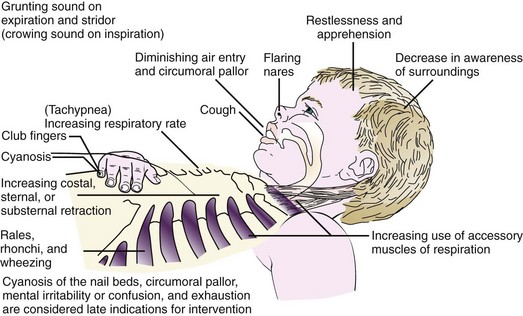
3 Review the signs and symptoms of respiratory distress in infants and children.
4 Discuss the nursing care of a child with croup, pneumonia, or respiratory syncytial virus.
5 Recognize the precautions involved in the care of a child diagnosed with epiglottitis.
6 Compare bed rest for a toddler with bed rest for an adult.
7 Describe smoke inhalation injury as it relates to delivery of nursing care.
8 Discuss the postoperative care of a 5-year-old who has had a tonsillectomy.
9 Recall the characteristic manifestations of allergic rhinitis.
10 Discuss how sinusitis in children is different from that in adults.
11 Assess the control of environmental exposure to allergens in the home of a child with asthma.
12 Express five goals of asthma therapy.
13 Interpret the role of sports and physical exercise for the asthmatic child.
14 Recall four nursing goals in the care of a child with cystic fibrosis.
15 Devise a nursing care plan for the child with cystic fibrosis, including family interventions.
 , p. 591)
, p. 591) , p. 602)
, p. 602) , p. 585)
, p. 585) , p. 586)
, p. 586) , p. 588)
, p. 588) , p. 587)
, p. 587) , p. 583)
, p. 583) , p. 590)
, p. 590) http://evolve.elsevier.com/Leifer
http://evolve.elsevier.com/Leifer
The Respiratory System
Development of the Respiratory Tract
Pulmonary structures differentiate in an orderly fashion during fetal life. This makes it possible to determine at what point a particular defect may have occurred. The laryngotracheal groove appears at 2 to 4 weeks of gestation. The trachea and the esophagus originate as one hollow tube; gradually, by 4 weeks of gestation, a septum forms to completely separate them. If the septum fails to form completely, a tracheoesophageal fistula occurs (see Chapter 28). By the seventh week of fetal life the diaphragm forms and separates the chest from the abdominal cavity. If the diaphragm fails to close completely, a diaphragmatic hernia allows the abdominal contents (intestines, spleen, and stomach) to enter the chest cavity and prevents the lungs from expanding fully. Alveoli and capillaries, which are necessary for gas exchange in the human body, are formed between 24 and 28 weeks of gestation.
At the twenty-fourth week the formed alveolar cells begin to produce surfactant. Surfactant is composed of lecithin and sphingomyelin and prevents the alveoli from collapsing during respirations after birth. A premature birth is accompanied by problems with respiratory gas exchange. During fetal life the lungs are filled with a fluid that has a low surface tension and viscosity; this is rapidly absorbed after birth. Spontaneous respiratory movements occur in the fetus, although gas exchange occurs via placental circulation. When surfactant is present in the lungs, the respiratory movements force some of the surfactant into the amniotic fluid. At about 35 weeks of gestation, the lecithin component is twice that of the sphingomyelin component. The analysis of the lecithin/sphingomyelin ratio (L/S ratio) by amniocentesis (see Table 5-1) is one method of determining fetal maturity and the ability of the fetus to survive outside the uterus.
Normal Respiration
The process of normal respiration is described in Figure 25-1.
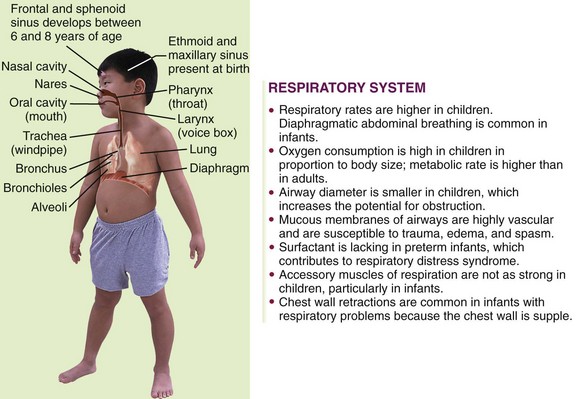
FIGURE 25-1 Summary of respiratory tract in children. The ribs and the diaphragm allow for inspiration of air. Air enters the body through the nares, or nostrils. The mucous membranes and cilia that line the respiratory tract warm, moisten, and filter the air as it passes to the pharynx. The pharynx contains the tonsils, which assist in infection control. The larynx at the upper end of the trachea contains the epiglottis, the glottis, and the vocal cords, which prevent food and fluids from entering the trachea and allow voice sounds. The trachea is encircled by smooth muscle and cartilage to maintain patency and carries the air to the bronchi and then to the smaller bronchioles. The bronchioles continue to divide and lead to small, thin air sacs (alveoli) that are kept open on inspiration by the air contained in them. During expiration when the air sacs collapse, surfactant prevents the walls from sticking together, allowing for reinflation. Gas exchange occurs in the alveoli by diffusion to the bloodstream. The volume of air inhaled with each breath is related to body size.
Ventilation
Ventilation, the process of breathing air into and out of the lungs, is affected by several elements and their interaction with each other:
• Intercostal muscles, diaphragm, ribs: These allow chest expansion and contraction. Expansion of the chest lowers pressure in the chest cavity, and air flows from the higher pressure of the atmosphere into the lower pressure of the chest cavity. The opposite occurs during expiration.
• Brain: The vagus nerve and the respiratory centers in the medulla of the brain regulate rhythmic respiratory movements. Signals sent to the respiratory center will increase or decrease respiratory rates.
• Chemoreceptors: These sensors respond to changes in the oxygen saturation of the blood by sending a signal to the pons in the brainstem, which is stimulated to increase respirations when the oxygen (O2) saturation is low.
Note: A high carbon dioxide (CO2) level in the blood and a low O2 saturation stimulate the brain to increase the respiratory rate. In chronic lung disease, however, the receptors become tolerant to the high CO2 and low O2 concentration in the blood. Administration of supplemental oxygen increases the O2 saturation level and may result in a decreased respiratory effort (carbon dioxide narcosis), leading to respiratory failure. The differences between the respiratory tracts of the growing infant and the adult are shown in Table 25-1.
Procedures that may be performed on the child with a respiratory condition include throat and nasopharyngeal cultures, bronchoscopy, lung biopsy, arterial blood gas (Pao2, Paco2) and pH analysis, pulse oximetry, and various pulmonary function tests (PFTs). Chest x-ray films, computed tomography, radioisotope scan, bronchogram, and angiography may prove useful, depending on symptoms. The inspection, percussion, and auscultation procedures performed by the nurse are of utmost value in data collection.
Disorders and Dysfunction of the Respiratory System
Pathophysiology: A cold, also known as acute coryza, is the most common infection of the respiratory tract. It can be caused by a number of viruses, principally the rhinoviruses, which are spread from one child to another by sneezing, coughing, or direct contact. The age, state of nutrition, and general health of the child contribute to the susceptibility level.
The rhinovirus is spread by contact with contaminated fingers that touch the conjunctiva of the eyes or the mucous membranes of the mouth. Routine handwashing practices, especially before rubbing the nose or sucking the fingers, can prevent the spread of the common cold.
The common cold differs from allergic rhinitis in that a child who has allergic rhinitis has no fever, no purulent nasal discharge, and no reddened mucous membranes. Sneezing, watery eyes, and itching of the skin are the primary manifestations of allergic rhinitis. In the older child or adolescent, persistent nasopharyngitis may be related to inhaled cocaine or other drug abuse.
Manifestations: The symptoms of a cold in an infant or small child are different from those in an adult. Children’s air passages are smaller and more easily obstructed. The virus causes inflammation and edema of the membranes of the upper respiratory tract, which damages cilia and prevents the drainage of mucus. Fever as high as 40° C (104° F) is not uncommon in children under 3 years of age. Nasal discharge, irritability, sore throat, cough, and general discomfort are present, and there may be vomiting and diarrhea. The diagnosis is complicated by the fact that many infectious diseases resemble the common cold during their onset. Complications of a cold include bronchitis, pneumonitis, and ear infections.
Treatment and Nursing Care: There is no cure for the common cold. Treatment should begin early, when a cold is suspected. The following treatment is designed to relieve symptoms:
• Rest: Fatigue should be prevented. Confinement to bed for a child does not always result in physical rest. In pediatrics, “bed rest” means providing play therapy that promotes minimal activity. The nurse should consider the age and developmental level of the child and the activity level involved in the play when designing appropriate activities and guiding parents in the home care of their child.
• Clear airways: Congested nasal passages cause discomfort and impede nursing or sucking of formula. Because fluid consumption is essential to prevent fever and dehydration, the airways must be cleared before feeding and before bedtime to provide a restful sleep. The nurse can teach the parents that instilling a few drops of saline solution into the nose and then suctioning with a bulb syringe (Skill 12-2) is the best way to clear the nostrils. Medicated nosedrops can be irritating to the mucosa of a young child’s nasal passages. Use of nosedrops with an oily base should be avoided because they are readily aspirated and can cause respiratory problems. Rebound congestion can be avoided by limiting the use of medicated nosedrops to no more than 3 days. Use of over-the-counter combination cold remedies should be avoided. Contents on the label should be checked for safe dosage.
• Adequate fluid intake: Anorexia is common in children with nasopharyngitis. Fluids should be encouraged to prevent dehydration. Cool, bland liquids are usually tolerated well in a child who has a sore throat.
• Prevention of fever: Ibuprofen (Motrin) or acetaminophen (Tylenol) can be administered when a high fever accompanies a cold.
• Skin care: A petroleum-based ointment can be applied to the nares and upper lip to prevent skin irritation from a nasal discharge.
 Medication Safety Alert!
Medication Safety Alert!
Parents should be cautioned to check the label of any medication for appropriate dosages. The safe dosage for acetaminophen (Tylenol) elixir differs from that of acetaminophen (Tylenol) drops.
Moist air soothes the inflamed nose and throat. An electric cold air humidifier is safe and convenient. It must be cleaned and disinfected daily. If a great deal of moisture is indicated (as in croup), the infant may be taken to a small room, such as the bathroom, and the hot water faucets or shower can be turned on to produce sufficient steam.
The older child is taught the proper way to remove nasal secretions from the nose. The mouth is opened slightly, and secretions are gently blown through both nostrils at the same time. This method prevents the infection from being forced into the eustachian tubes. Children must be taught to cover the mouth and nose when sneezing and to wash their hands afterward. Tissues must be properly discarded. Antibiotics are not effective against the common cold because it is viral in origin.
Otitis media is an inflammation of the middle ear. The middle ear is connected to the throat by the eustachian tube, which provides drainage of middle ear secretions into the nasopharynx and equalizes pressure between the middle ear and the outside atmosphere. When the lining of the eustachian tube becomes infected as a complication of nasopharyngitis, otitis media often develops, usually following an upper respiratory infection. Infants are more prone to middle ear infections because their eustachian tubes are shorter, straighter, and wider than those of older children or adults. For a detailed discussion of otitis media, see Chapter 23.
Acute Pharyngitis
Pathophysiology: Acute pharyngitis is an inflammation of the structures in the throat. This infection is common among children between 5 and 15 years of age. In 80% of cases the causative organism is a virus. Group A beta-hemolytic streptococcus (strep throat) occurs in 20% of the cases. The bacterium Haemophilus influenzae is common in children under 3 years of age.
Manifestations, Treatment, and Nursing Care: Symptoms include fever, malaise, dysphagia (dys, “difficult,” and phagia, “swallowing”), and anorexia. It is difficult to distinguish viral from bacterial types by symptoms only. Conjunctivitis, rhinitis, cough, and hoarseness with a gradual onset and persisting no longer than 5 days are characteristic of viral pharyngitis. In a child over 2 years of age, streptococcal pharyngitis characteristically includes high fever (40° C [104° F]) and difficulty in swallowing, and it may last longer than 1 week. A strep throat is determined by throat culture. When the culture is positive, antimicrobial therapy such as penicillin is administered orally for 10 days. Compliance may be a problem; therefore the nurse carefully explains to parents the need for the child to finish all of the medication. Erythromycin may be prescribed if the child is allergic to penicillin. Acetaminophen may be taken to relieve soreness of the throat. If the child is old enough to gargle, a solution of warm water and salt may be used.
Prompt treatment of strep throat is important to prevent serious complications such as rheumatic fever, glomerulonephritis, peritonsillar abscess, otitis media, mastoiditis, meningitis, osteomyelitis, or pneumonia. The persistence of a positive streptococcal culture after careful follow-up and therapy may indicate that the child is a group A beta-hemolytic streptococcus carrier. However, it may also mean that the child did not complete the 10-day course of medication or that a drug-resistant organism has evolved. The child with strep throat is no longer infectious to others once drug therapy has begun and fever has decreased.
Sinusitis in Children
The frontal sinuses are present at 8 years of age but may not be fully developed until age 18. Some ethmoid sinus cells are present at birth. The sphenoid sinus is present by 3 years of age and is fully developed by age 12. The maxillary sinuses are present at birth and develop as long as teeth are erupting. The proximity of this sinus to the tooth roots often results in tooth pain when the sinus is infected. The maxillary and ethmoid sinuses are most often involved in childhood sinusitis. Therefore the signs and symptoms of sinusitis in children are different from those in adults, depending on the age of the child and which sinus is fully developed. An acute sinusitis is suspected when an upper respiratory infection lasts longer than 10 days, with a daytime cough. Halitosis is often present. Untreated sinusitis can lead to periorbital cellulitis, because the infection spreads from the ethmoid sinus to the subperiosteal space around the eye. Treatment involves a 10- to 14-day course of antibiotic therapy.
Croup Syndromes
Pathophysiology: Croup is a general term applied to a number of conditions whose chief symptom is a “barking” (croupy) cough and varying degrees of inspiratory stridor (a harsh, high-pitched sound). When the larynx is involved, the clinical picture becomes more intense because of possible alterations in respiratory status, such as airway obstruction, acute respiratory failure, and hypoxia (Figure 25-2). Acute spasmodic laryngitis is the milder form of the syndrome. Acute laryngotracheobronchitis is the most common. It is also referred to as subglottic croup because edema occurs below the vocal cords. Croup can be benign or acute. Benign croup is frightening but rarely life threatening. Acute croup can develop into a respiratory emergency.
Congenital laryngeal stridor (laryngomalacia): Some infants are born with a weakness of the airway walls and a floppy epiglottis that causes a stridor on inspiration. There may be inspiratory retractions. The symptoms lessen when the infant is placed prone or propped in the side-lying position. Respiratory infection and crying may cause the symptoms to become frightening to the parents. The condition usually clears spontaneously as the child grows and the muscles strengthen. The nurse should provide reassurance and suggest slow, small feedings and a prone or side-lying position for the infant.
Spasmodic laryngitis (spasmodic croup): Spasmodic croup usually occurs in children between 1 to 3 years of age and can be caused by a virus, allergy, or psychological trigger. Very often, gastroesophageal reflux (GER) will trigger an attack. Spasmodic croup has a sudden onset, usually at night, and is characterized by a barking, brassy cough and respiratory distress. The child appears anxious, and the parents become frightened. The attack lasts a few hours, and by morning the child appears normal and is in no distress. Increasing humidity and providing fluids are helpful treatment measures.
Laryngotracheobronchitis: The viral condition laryngotracheobronchitis is manifested by edema, destruction of respiratory cilia, and exudate, resulting in respiratory obstruction. A mild upper respiratory infection usually precedes the development of a characteristic barking or brassy cough. Stridor develops, and classic symptoms of respiratory distress follow (see Figure 25-2). The infant prefers to be held upright or sit up in bed (orthopnea). Crying and agitation worsen the symptoms. Hypoxia can develop and be accompanied by tachycardia and diminished breath sounds.
Treatment and nursing care: When the child is treated at home, parents are often instructed to increase humidity levels around the child. This can be accomplished by using an electric cold water humidifier. The humidifier must be emptied, washed, and disinfected each day to prevent the growth of microorganisms that occur in stagnant tap water. The child can also be taken into the bathroom, where the hot water in the shower is turned on to increase humidity. The child inhales the moist air, which usually relieves the respiratory distress and laryngeal spasm (constriction of laryngeal muscles).
When continuing symptoms of respiratory distress necessitate hospitalization, the child may be given nebulizer therapy or placed in a mist tent, or croupette (see Figure 22-19). The cool air, well saturated in microdroplets that can enter the small airway of a child, causes mucosal cooling and vasoconstriction and relieves the respiratory obstruction and distress. However, the value of mist tent therapy in the acutely ill child is unproven. Intravenous (IV) fluids are prescribed to prevent dehydration and to decrease the risk of vomiting and aspiration that can occur after a coughing episode. Organization of care is essential to enable the child to have long periods of rest. The child is placed on a cardiorespiratory monitor (CRM), and the vital signs are observed closely. Oxygen is given to reduce hypoxia (see Chapter 22). Oxygen saturation is monitored, and saturation levels are maintained above 90% (see Skill 13-1 for sensor application).
Opiates are contraindicated because they depress respiration. Sedatives are contraindicated because increased restlessness is a primary sign of increased respiratory obstruction, and sedatives can mask signs of restlessness. Nebulized epinephrine may be used to relieve the symptoms of respiratory obstruction (Figure 25-3). Corticosteroids are often prescribed to reduce the edema caused by inflammation and to prevent further destruction of ciliated epithelium in children hospitalized with croup, providing there is no history of recent exposure to varicella (chickenpox) (Lenney et al., 2009).

Epiglottitis
Pathophysiology: Epiglottitis is a swelling of the tissues above the vocal cords, that is, supraglottic swelling. This results in narrowing of the airway inlet, with the possibility of total obstruction. It is caused by H. influenzae type B and most often occurs in children 3 to 6 years of age. It can occur in any season. The course is rapid and progressive. Epiglottitis is a life-threatening medical emergency. Blood gases fluctuate, and there is leukocytosis.
Manifestations: The onset of epiglottitis is abrupt, and the child presents with classic symptoms. The child insists on sitting up, leans forward with the mouth open, and drools saliva because of the difficulty in swallowing. The child appears wide-eyed, anxious, and restless, and he or she may emit a froglike croaking sound on inspiration. Cough is absent. Inspection of the throat shows an enlarged, reddened edematous epiglottis much like a “beefy-red thumb.” However, the examining tongue blade may trigger a laryngospasm and result in sudden respiratory arrest.
Bronchitis
Pathophysiology: A study of the respiratory system reveals that the air tubes leading to the lungs resemble an upside-down tree. The trachea is the main trunk, with the bronchi, bronchioles, and alveoli as branches. These passages proceed from large to small and are lined with a continuous membrane. If there is an infection of the bronchial tree, it is seldom confined to one area but more often involves other structures.
Acute bronchitis is an infection of the bronchi. It seldom occurs as a primary infection but is usually secondary to a cold or other communicable disease. It is caused by a variety of organisms. Poor nutrition, allergy, and chronic infection of the respiratory tract may precipitate this condition. Most patients are under 4 years of age.
Bronchiolitis
Pathophysiology: Acute bronchiolitis is a viral infection of the small airways (bronchioles) in the lower respiratory tract. It occurs in infants and children 6 months to 2 years of age, with a peak at 6 months of age. The small diameter of the bronchioles in the infant are susceptible to obstruction when inflammation results in edema and excess mucus. The obstruction often leads to atelectasis. The gas exchange in the lungs becomes impaired, and hypoxia can occur.
Manifestations: An upper respiratory infection or cold with a mild fever and serous (clear) nasal discharge is followed by the development of a wheezing cough and signs of respiratory distress. The increase in respiratory rate interferes with successful feeding, and the infant becomes irritable and dehydrated. The respiratory syncytial virus (RSV) is the causative organism in 50% of cases in infants. An apneic episode is usually the cause of hospitalization. Infants who have bronchiolitis may develop a hyperreactive airway or asthma later in life.
Treatment and Nursing Care: The treatment of an infant with bronchiolitis is symptomatic and similar to that of the child with croup. A semi- Fowler’s position with a slightly hyperextended neck facilitates respirations. Oral feedings are often supplemented by IV fluids. Intake and output are recorded. Bronchodilating aerosol therapy and high-humidity tents are prescribed. Frequent assessment of vital signs and monitoring of oxygen saturation levels are essential.
Respiratory Syncytial Virus
Respiratory syncytial virus (RSV) is responsible for 50% of cases of bronchiolitis in infants and young children and is the most common cause of viral pneumonia. RSV is the single most important respiratory pathogen in infancy. RSV occurs worldwide and causes annual epidemics during the winter months. Most children are infected with RSV before their second birthday, and reinfection is common, especially in children attending day care centers. Infants between 2 and 7 months of age can become seriously ill with this condition because their airways are so small and prone to obstruction by the thick mucus produced. Older children and adults are not as seriously ill and continue to go to work or school, becoming carriers and spreading the infection.
Transmission: RSV is spread by direct contact with respiratory secretions, usually by contaminated hands to the mucous membranes (eyes, mouth, nose). RSV survives for more than 6 hours on countertops, tissues, and soap bars. RSV is not spread via the airborne route. The incubation period is approximately 4 days.
Hospital-acquired infection can be a major problem because caregivers may be carrying the organism. For this reason, an infant diagnosed with RSV infection is placed on transmission-based contact isolation precautions to prevent the spread of RSV to other sick children.
RSV immunoglobulin may be used for preterm newborns with bronchopulmonary dysplasia who are at risk for infection.
Diagnosis: An examination of nasopharyngeal washings for RSV antigens can be done while the child waits in the admitting unit so that the diagnosis is established before the infant is admitted to the pediatric unit.
Prevention: Prevention of RSV is available via a monoclonal antibody, palivizumab (Synagis), given in monthly intramuscular injections. This medication is started at the onset of RSV season and terminated at the end of the season (usually November through March). The AAP practice guidelines state that candidates for preventive therapy include infants with bronchopulmonary dysplasia, severe immunodeficiencies, or significant congenital heart disease and those on continuous mechanical respiratory support (Meissner & Bocchini, 2009). The powder form of palivizumab should be administered within 6 hours of reconstitution because it is preservative free.
Treatment and Nursing Care: The care of infants with RSV infection should be assigned to personnel who are not caring for patients at high risk for adverse response to RSV. Infection prevention and control techniques (see Appendix A) are used to prevent the spread of infection to others on the unit. Contact isolation precautions are used to prevent fomite spread. Frequent handwashing is essential. Liquid soap dispensers should be available at the sink, because the organism survives for a long time on a dry bar of soap.
Support of the Infant and Family: Effective communication skills are necessary to provide support for parents of the infant who is seriously ill. The parent can be familiarized with the mist tent and encouraged to participate in the care and feeding of the infant. Adults who have RSV can shed the virus for 1 week after the infection, and precautions should be taken if that adult is caring for infants (see Appendix A for infection prevention and control precautions).
Symptomatic Care: An ineffective breathing pattern is the priority nursing diagnosis for an infant hospitalized with RSV infection. Reporting tachypnea (increased respiration) and tachycardia (increased heart rate) is essential because these vital sign changes may be indicative of hypoxemia. It is also important to auscultate breath sounds and report wheezing, rales, or rhonchi. A child who has been wheezing and suddenly has a “quiet chest” on auscultation may be at risk for respiratory arrest. The higher-pitched the wheeze, the more constricted the airway. Signs of respiratory distress should be assessed and reported. Oxygen saturation levels are monitored, and oxygen is administered at levels needed to maintain a minimum of 90% to 95% saturation. Suctioning of mucus may be necessary to maintain a patent airway. Monitoring IV fluids and recording intake and output are essential to prevent dehydration. Urine output should be a minimum of 1 to 2 mL/kg/hr for infants and children. Pedialyte or Ricelyte are examples of clear liquid electrolyte formulas prescribed for infants at risk of dehydration. The child should be weighed daily to detect early signs of dehydration. Inhaled bronchodilators or steroids are not helpful with RSV infections.
Antiviral Medication: Antiviral medication such as ribavirin (Virazole) may be prescribed for use with severely ill infants or infants who have heart or lung problems that place them at high risk for serious complications. The medication has been found to be effective in the treatment of RSV infection but is rarely used prophylactically because of its serious side effects. The medication is administered by fine-droplet aerosol mist while the infant is in a mist tent. It is administered 18 to 24 hours a day for a minimum of 3 days. If the infant is on a ventilator, the nurse must monitor the ventilator tubes, which may be warped by ribavirin. Caregivers and visitors who are of childbearing age, pregnant, or breastfeeding should not care for infants receiving ribavirin, because teratogenic effects have been reported. The ribavirin mist can cause precipitation on the surface of plastics, and caregivers with contact lenses may develop conjunctivitis because of the lens changes this causes. When providing care to an infant receiving ribavirin therapy, the nurse should turn off the nebulizer and allow the mist to settle before opening the mist tent and providing care. Linen removed from the bed should be slowly rolled and carefully folded to avoid releasing droplets of ribavirin into the air.
An IV immune globulin (RespiGam) may be prescribed for high-risk infants to prevent complications from RSV disease. RespiGam is administered intravenously and necessitates close observation for fluid volume overload. Routine immunizations may have to be postponed for 9 months if antiviral medication for RSV is prescribed. Intramuscular palivizumab can also be given to high-risk infants and does not interfere with mumps-measles-rubella (MMR) or varicella vaccines.
Complications: Infants who have a small airway size and are severely ill and hospitalized with RSV infection may be at risk for wheezing and reactive airway disease (RAD) later in life. Some studies (Kliegman et al., 2007) have shown that the inflammation caused by RSV injures the respiratory epithelial cells, resulting in exposed sensory nerve fibers that respond easily to environmental irritants.
Pneumonia
Pathophysiology: Pneumonia or pneumonitis is an inflammation of the lungs in which the alveoli (air sacs) become filled with exudate and surfactant may be reduced. The affected portion of the lung does not receive enough air. Breathing is shallow. As a result, the bloodstream is denied sufficient oxygen.
Pneumonia may occur as the initial or primary disease, or it may complicate another illness, in which case it is termed secondary pneumonia. There are many types of pneumonia. Classification may be by causative organism (i.e., bacterial or viral) or by the part of the respiratory system involved (i.e., lobar or bronchial). Group B streptococci are the most common cause of pneumonia in newborns, whereas Chlamydia are the most common cause of pneumonia in infants 3 weeks to 3 months of age. The incidence of H. influenzae type B infection has been decreasing with current immunization programs. RSV, rhinovirus, adenovirus, and pneumococcus are other organisms that are responsible for pneumonia in infants and children. Immunocompromised children may develop pneumonia caused by a gram-negative organism or a fungi such as Pneumocystis jiroveci (formerly known as Pneumocystis carinii).
 Nursing Tip
Nursing Tip
The heptavalent pneumococcal vaccine (Prevnar) is recommended for children under 2 years of age and is given at 2, 4, 6, 12, and 15 months of age. The polyvalent pneumococcal vaccine (PPV) provides protection for children over 2 years of age.
Toddlers often aspirate small objects such as peanuts or popcorn and develop pneumonia as a result; therefore such foods are to be discouraged for this age-group. Lipoid pneumonia occurs when the infant inhales an oil-based substance into the airways. It is less common today because children are seldom given cod liver oil or castor oil routinely, as they were in the past. Nosedrops with an oil base must not be used for children because the oil can be aspirated and cause lipoid pneumonia. A toddler who drinks kerosene may also develop a type of pneumonia. Hypostatic pneumonia may occur in patients who have poor circulation in their lungs and remain in one position too long. The child recovering from anesthesia must be turned frequently to stimulate circulation through the lungs. Early ambulation also accomplishes this.
Severe acute respiratory syndrome (SARS) is a severe type of pneumonia caused by the coronavirus (SARS-CoV). Symptoms are similar to pneumonia, but often the severity of the respiratory distress necessitates assisted ventilation and treatment in the intensive care unit (ICU). Nursing care and treatment involve supportive care. Airborne infection isolation precautions are recommended in the care and treatment of these patients (see Appendix A).
Manifestations: The symptoms of pneumonia vary with the patient’s age and the causative organism. They may develop suddenly or may be preceded by an upper respiratory tract infection. The cough is dry at first, but it gradually becomes productive. Fever rises as high as 39.5° to 40° C (103° to 104° F) and may fluctuate widely during a 24-hour period. The respiratory rate may increase (tachypnea) to 40 to 80 breaths/min in infants and to 30 to 50 breaths/min in older children. Respirations are shallow as the child attempts to reduce the amount of chest pain. The chest pain may be caused by a pleural irritation or a musculoskeletal irritation from frequent coughing. Sternal retractions may be seen when the accessory muscles of respiration are used. The nostrils may flare. The child is listless, has a poor appetite, and tends to lie on the affected side. X-ray films confirm the diagnosis and determine whether there are complications such as atelectasis. A differential white blood cell count is routinely performed. Blood specimens show a marked increase in the number of white blood cells (16,000 to 40,000/mm3). Culture specimens may be obtained from the nose, the throat, or sputum.
Treatment: Treatment depends on the causative organism. Antipyretics are given to reduce fever. Oxygen is administered for dyspnea or cyanosis. When this treatment is begun early, the child is less restless and does not require as many sedatives or drugs to relieve pain. Because drug therapy has become so effective, many uncomplicated cases can be treated at home. Fluid intake should be increased, particularly clear fluids and “flattened” soft drinks. Pediazole, (a combination of erythromycin ethylsuccinate and sulfisoxazole acetyl) may be prescribed for infants younger than 6 months of age, but amoxicillin is the drug of choice for children up to 5 years of age.
Rest, fluids, and a cough suppressant before bedtime are the basics of home care. Parent education concerning the need to complete all medication prescribed is essential. Tobacco use in the environment should be avoided, and the need for H. influenzae type B (Hib) immunizations is stressed. The proper use and disposal of tissues, covering the mouth during a cough, and the modeling of proper handwashing techniques are preventive measures the nurse should teach the family.
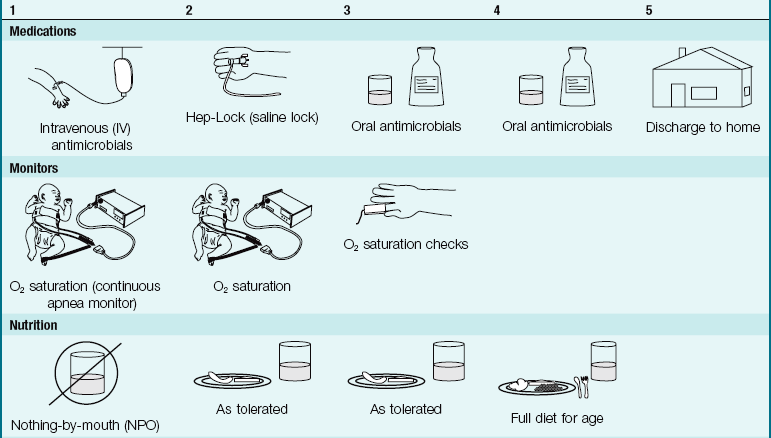
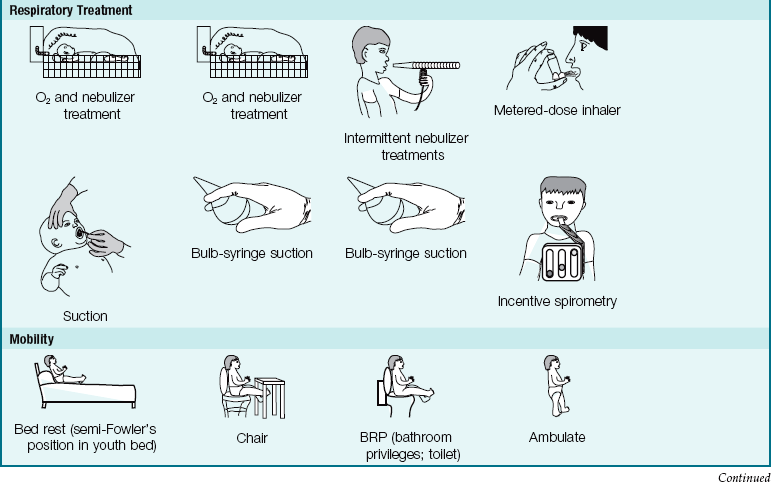
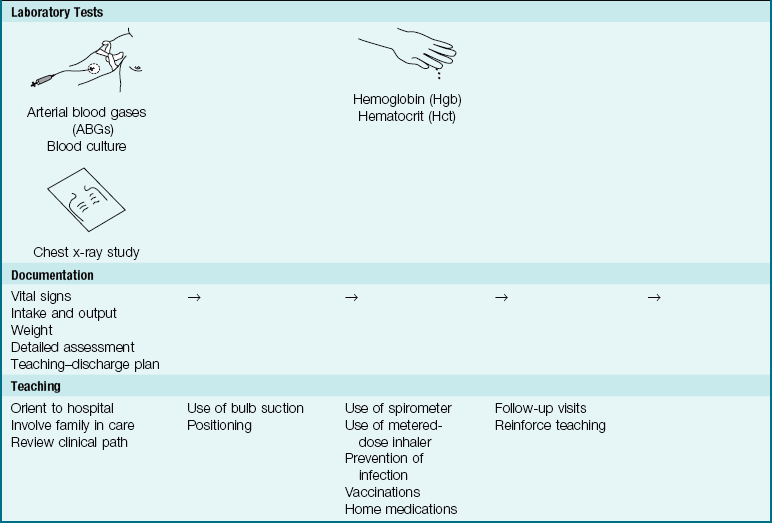
Nursing Care: Nursing care in all types of pneumonia is basically the same. The age of the patient determines the nurse’s approach and the type of equipment used. (The newborn receives oxygen in the Isolette, whereas the older child requires a croupette or a larger tent.) Rest is an important part of the treatment. The nurse must organize care so that the child is not disturbed unnecessarily. Planned, quiet activities for the child are recommended (Pictorial Pathway 25-1).

The nurse checks the vital signs at regular intervals. When a child is flushed with fever, heavy clothing and blankets should be removed. The nurse encourages the child to take fluids, flavored ice pops, or small sips of water frequently. If vomiting persists, parenteral fluids are given.
Smoke Inhalation Injury
Smoke inhalation injury may cause carbon monoxide poisoning. Poisonous substances inhaled from burning material may also cause pathological disturbance. There are three stages of inhalation injury:
1. Pulmonary insufficiency in the first 6 hours
2. Pulmonary edema from 6 to 72 hours
3. Bronchopneumonia after 72 hours, which may cause atelectasis
When the child is injured by fire and burns are evident around the face or mouth, heat injury to the upper airway should be suspected. Burned materials can be carried deep into the respiratory tract in the form of insoluble gases and may cause chemical injury. Smoke from burning synthetic materials and plastic are especially toxic to the airways. Severe exposure to these chemicals can inhibit secretion of surfactant and cause a hyaline membrane to form, resulting in adult respiratory disease syndrome (ARDS). Carbon monoxide is not toxic to the lungs but, by combining with hemoglobin to form carboxyhemoglobin (COHb), prevents oxygen from binding to hemoglobin and thus inhibits cellular respiration.
Safety Alert!
Pulse oximetry readings are of little value in carbon monoxide poisoning because pulse oximetry does not detect COHb and readings may appear normal.
Treatment is often symptomatic and includes oxygen administration, careful monitoring of intake and output, and frequent assessments of arterial blood gas reports. In severe carbon monoxide poisoning hyperbaric oxygenation (see Chapter 34) may be the treatment of choice. See Chapter 32 for agents used in bioterrorism attacks.
Tonsillitis and Adenoiditis
Pathophysiology: The tonsils and adenoids, located in the pharynx (throat), are made of lymph tissue and are part of the body’s defense mechanism against infection. The symptoms of tonsillitis include difficulty in swallowing and breathing. Enlarged adenoids block the nasal passage, resulting in mouth breathing. Other symptoms are similar to those of nasopharyngitis. Nursing care involves providing a cool mist vaporizer to keep the mucous membranes moist; salt water gargles; throat lozenges (if age-appropriate); a cool, liquid diet; and acetaminophen to promote comfort. Antibiotics are not usually prescribed unless a throat culture is positive for the streptococcal organism.
Treatment: The removal of the tonsils and adenoids, referred to as a “T&A,” is usually not recommended for children under 3 years of age. It is thought that the condition may correct itself if surgery is postponed, because the tissues become smaller as the child grows. A tonsillectomy (removal of the palatine tonsils) is indicated only if persistent airway obstruction or difficulty in breathing occurs. The surgery is not performed during an acute infectious episode because inflamed tissue responds poorly to surgery.
Children are prepared for the surgery with age-appropriate explanations. Wording should be carefully selected, because young children may associate being “put to sleep” for the operation with their sick pet being “put to sleep” and never heard from again. Same-day surgery is the usual setting for a tonsillectomy, with the child returning home after a few hours. The presence of loose teeth should be reported to the anesthesiologist, because there may be a danger of aspiration during the surgical procedure. Identification bands are applied, and routine preoperative care is initiated and documented.
Postoperative Care: To facilitate drainage immediately after surgery, the child is placed partly on the side and partly on the abdomen, with the knee of the uppermost leg flexed to hold the position. The child is watched carefully for evidence of bleeding, such as an increase in pulse rate and respirations, restlessness, frequent swallowing (which may be from blood trickling down the back of the child’s throat), or vomiting of bright red blood. An ice collar may be applied for comfort. The child’s face and hands are wiped with a warm washcloth, and the hospital gown and linen are changed whenever necessary. Small amounts of clear liquids are given as tolerated. Red- or brown-colored juices are avoided, because they make it difficult to evaluate the content of emesis and the presence of blood. A Popsicle may appeal to the child. If these are well tolerated, progression to a soft diet is begun. The child is kept quiet for the remainder of the day. A small child may nestle on a parent’s lap. Coughing, clearing the throat, and blowing the nose are avoided to decrease the risk of precipitating bleeding at the operative site. Appropriate pain relief is important and will minimize crying, which may further irritate the throat. Hemorrhage is the most common postoperative complication. The nurse should not assume that because the surgery is minor it does not involve certain risks.
Written instructions are given to the parents when the child is discharged. The child should be kept quiet for a few days and should receive nourishing fluids and soft foods. After this, the child may continue to take a nap or to have a rest period so that he or she has sufficient convalescent time. Acetaminophen may be given to reduce throat discomfort. The child must be protected from exposure to infections. Gargling and highly seasoned food should be avoided during the first postoperative week.
Allergic Rhinitis
Allergic rhinitis is an inflammation of the nasal mucosa caused by an allergic response. It often occurs during specific seasons and is referred to as hay fever. Allergic rhinitis is not a life-threatening condition and does not necessitate hospitalization, but it occurs in 10% of children and accounts for many school absences.
Pathophysiology: The mast cells in the nasal mucosa respond to an antigen by releasing mediators such as histamine, which cause edema and increased mucous secretion. A generalized parasympathetic response can follow. The child may have a genetic predisposition to develop the allergy, and exposure to the allergen triggers the response.
Manifestations: The characteristic signs of allergic rhinitis include nasal congestion, a clear, watery nasal discharge, sneezing, and itching of the eyes (Figure 25-4).
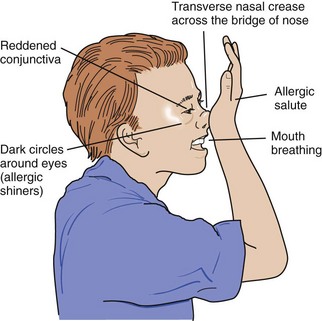
FIGURE 25-4 The allergic salute. Signs of allergic rhinitis include a typical rubbing of the nose in response to nasal discharge (allergic salute), darkened circles under the eyes (allergic shiners) caused by an obstruction of lymphatic and vein flow, and a transverse crease across the bridge of the nose resulting from the allergic salutes.
Diagnosis: Laboratory tests of the mucous membranes of the nose reveal the presence of eosinophils, and skin sensitization testing may be positive for specific allergens. The history shows seasonal occurrence, family history of allergy or asthma, typical appearance, and absence of fever or purulent drainage.
Treatment: Symptomatic treatment revolves around the use of antihistamine (nonsedating) medications and decongestants to reduce edema of the nasal mucous membranes without creating sedation, which can interfere with learning. Topical medications should not be used because of a “rebound effect” that occurs with long-term use. Prophylactic therapy with cromolyn inhalants or glucocorticoid nasal sprays may be prescribed if antihistamines are not effective, but this type of medication requires daily administration and parent and child compliance. Immunotherapy for identified allergens may be prescribed.
The main goals of the nurse are to help the parent identify the difference between the allergy and a cold and to provide a referral for medical care and support during the long-term allergy testing and immunotherapy process. Teaching the family about controlling the environmental exposure to allergens is very important. Dust control, prevention of contact with animal dander, the use of air-conditioners and high-efficiency particulate air (HEPA) filters in the home, and the planning of vacation locales that do not present pollen challenges are some of the vital issues to discuss with the family. Leukotriene antagonist drugs have also been effective in the treatment of allergic rhinitis (Kliegman et al., 2007).
Asthma
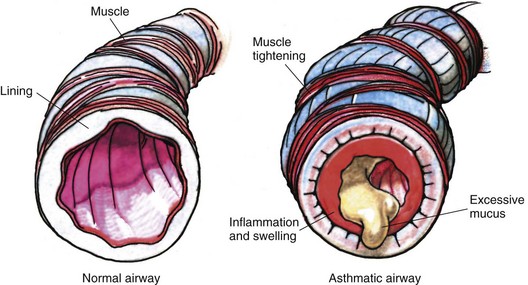
Pathophysiology: Asthma is a syndrome caused by increased responsiveness of the tracheobronchial tree to various stimuli that results in reversible, paroxysmal (intermittent) constriction of the airways (Figure 25-5). The term asthma is a Greek word for panting or breathlessness. Asthma is the principal cause of chronic illness in children. It is the leading cause of school absenteeism, emergency department visits, and hospitalization. Although it may occur at any age, about 80% of asthma sufferers have their first symptoms before 5 years of age. Before puberty, about twice as many boys as girls are affected; thereafter the sex incidence is equal.
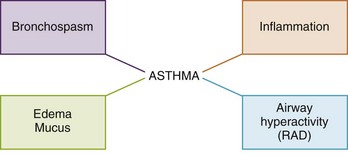
FIGURE 25-5 There are four main components of asthma, and the medication prescribed by the physician is specifically designed to deal with the component manifested by the individual child. Inhaled corticosteroids may be prescribed for children with reactive airway disease (RAD), whereas an inhaled bronchodilator is the treatment of choice for bronchospasm. A child with asthma can manifest one or more of the components of the asthma syndrome.
Asthma is a recurrent and reversible obstruction of the airways in which bronchospasm, mucosal edema, and secretion of and plugging by mucus contribute to significant narrowing of the airways and subsequently impaired gas exchange (Figure 25-6). Both large and small airways may be involved. The onset of asthma may be triggered by house dust, animal dander, wool, feathers, pollen, mold, passive smoking, strong odors (as from wet paint, wood stoves, or fireplaces), and certain foods. Vigorous physical activity (especially in cold weather) and rapid changes in temperature and humidity may precipitate an attack. Viral infections are also responsible. Emotional upsets, which affect smooth muscle and vasomotor tone (vas, “vessel,” and motor, “mover”), are closely intertwined with the condition. Whatever the precipitating cause, the response of the airways is similar. As the attack worsens, arterial blood gases change. Paco2 rises and the blood pH falls, increasing respiratory acidosis and producing a strain on the heart. Children who are prone to allergies often develop asthma. Some children who suffer from infantile eczema (see Chapter 30) develop asthma as they grow older. A family history of allergies is often seen.
Diagnosis: A history, physical examination, and response to bronchodilator therapy are the first diagnostic tools. An elevated level of eosinophils in the blood is typical. Eosinophils in the sputum are also diagnostic. Allergy skin testing and a radioallergosorbent test (RAST) are measures that can identify a sensitivity to allergens. Exercise testing and pulmonary function tests help to diagnose asthma and assess the progress of the syndrome.
Asthma is rarely diagnosed in infancy; the increased susceptibility of infants to respiratory obstruction and dyspnea in response to many different illnesses has many causes:
• Decreased smooth muscle of an infant’s airway
• Presence of increased mucous glands in the bronchi
• Normally narrow lumen of the normal airway
• Lack of muscle elasticity in the airway
• Fatigue-prone and overworked diaphragmatic muscle on which infant respiration depends
The symptom of wheezing in infancy can be caused by gastroesophageal reflux, cystic fibrosis, or the chronic aspiration often seen in developmentally delayed infants, or it may be a manifestation of a milk or food allergy.
Manifestations: The symptoms of asthma may begin slowly or abruptly. They may be mild, moderate, or severe. Obstruction is most severe during expiration because the airways become smaller during this phase of respiration. The trapped air in the lung causes hyperinflation and results in an increase in the effort needed for breathing. This increased work of breathing can eventually put a strain on the heart. The hypoxia and resulting acidosis can then cause general pulmonary vasoconstriction that damages alveoli, decreases surfactant, and causes a chronic respiratory problem.
In acute episodes the patient coughs, wheezes, and has difficulty breathing, particularly during expiration. The child may complain that his or her chin, neck, or chest itches. Signs of air hunger, such as flaring of the nostrils, and the use of the accessory muscles of respiration (chest and abdominal muscles) may be evident. Orthopnea appears. The child is restless, perspires, and sometimes complains of abdominal pain; participation in activities decreases. Pulse and respirations are increased, and rales (abnormal respiratory sounds) may be heard in the chest. Inflammation of the nose and sinuses may accompany asthma.
Asthma attacks often happen during the night and are frightening for both the child and the parents. Repeated attacks over a long period may lead to emphysema. Chronic asthma is manifested by discoloration beneath the eyes (allergic shiners), slight eyelid eczema, and mouth breathing.
Laboratory studies may reveal eosinophilia (increased blood eosinophils). Pulmonary function tests assess the degree of respiratory obstruction. Exercise testing may reveal bronchoconstriction with prolonged physical exercise.
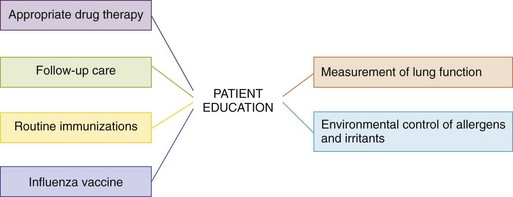
Treatment and Long-Term Management: The main goals of asthma therapy are as follows (Figure 25-7):
Medications: Medications used for outpatient treatment of asthma are for quick relief (“rescue”) in case of return of acute symptoms and for long-term control. An asthma specialist is usually responsible for the follow-up care of the child with asthma (Kliegman et al., 2007).
Bronchodilators: Albuterol (Ventolin, Proventil), metaproterenol (Alupent), and terbutaline (Brethaire) are examples of bronchodilators used for the long-term management of asthma in children. Salmeterol (Serevent) is a long-acting bronchodilator used to prevent nighttime symptoms and for exercise-induced asthma. The drug is inhaled with the aid of a metered-dose inhaler (MDI). If a child has difficulty coordinating the mechanism or inhaling the dose, a spacer device can be added. The nurse should teach the family how to use the devices and the precautions concerning frequency of doses.
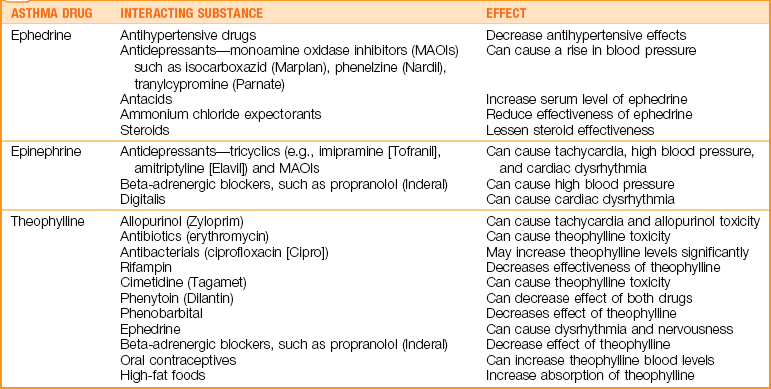
Theophylline is given orally, usually at night, in a liquid, tablet, or powder form that is sprinkled on a teaspoon of applesauce. The nurse should observe for signs of theophylline toxicity, which include restlessness, tremor, headache, tachycardia, abdominal pain, hypotension, and diuresis; the nurse should also instruct the patient and family about drug-drug interactions (Table 25-2). Periodic serum levels must be taken to ensure safety. Toxicity can lead to convulsions and death. Theophylline is rarely used today in routine management of pediatric asthma because of the potential for serious side effects. However, intravenous theophylline is used in acute, life-threatening situations. The family must be taught to tell the health care provider when the last dose of theophylline was given when seeking medical care for asthma problems.
Antiinflammatory drugs: Cromolyn sodium (Intal) is a nonsteroidal antiinflammatory drug (NSAID) that is inhaled using a Spinhaler, a device that delivers the drug. Its use is as a prophylactic, or preventive medication. It cannot be used as a therapeutic drug for the emergency care of respiratory distress. Cromolyn sodium is prescribed before exercise if a child has exercise-induced asthma to enable the child to participate in the activity. Daily doses are prescribed to ensure an adequate blood level. Nedocromil (Tilade), another antiinflammatory, may be prescribed. Corticosteroids are steroid medications that decrease inflammation. Inhaled preparations have fewer side effects than oral preparations and are used when bronchodilators are not effective. An increased appetite and euphoria are side effects of most steroids.
Slow inhalation of an inhaled drug enables the drug to reach the lower airway. Rapid inhalation causes some of the dose to be lost by being deposited on the sides of the pharynx. Nebulized inhalation therapy (often referred to as med-nebs) is administered by the respiratory therapist in the hospital, and home care units are also available.
Leukotriene modifiers: The leukotriene modifiers block inflammation and cause bronchodilation. Drugs such as zafirlukast (Accolate), zileuton (Zyflo), and montelukast (Singulair) are used in older children with other medications for long-term asthma control. Omalizumab (Xolair) is used for adolescents with allergic asthma and is given by monthly subcutaneous injection (Rosenwasser, 2003).
Nursing Care: The necessary general control of the environment is explained to the child and family. Avoiding pet dander, mold, smoking, and dust is essential. Stuffed toys are not desirable. Humidity in living areas of the house should be controlled between 25% and 50%, because excess humidity (above 50%) promotes mold growth. Dust collectors such as carpets, upholstery, or drapes should not be in the bedroom of an asthmatic child. Mattress covers, foam rubber pillows, and cotton blankets are preferred. Wool, down, and feather-stuffed items should be avoided. Upholstery, drapes, and carpets can be sprayed every 3 months with benzyl benzoate (Acarosan) to kill dust mites, followed by cleaning and vacuuming. The use of HEPA air-filtering devices in the bedroom and HEPA filters in the vacuum is advisable. Children can be taught to monitor their own lung function with the use of a peak flow meter at home (Skill 25-1). Involvement in self-care aids in compliance and results in better control of asthmatic symptoms.
Skill 25-1 Using the Peak Flow Meter








1. Be sure the arrow points to 0 or is at the bottom of the numbered scale.
2. Instruct the child to close his or her mouth over the mouthpiece.
3. Instruct the child to take a deep breath and blow as hard as possible into the peak flow meter.
4. Observe and record the score or measurement on the peak flow meter.
5. Repeat three times and report the highest of the three readings.
6. Compare the score with previous scores and correlate with the plan of care.

Very often the parents and teachers exclude the child from physical activity in school because of the fear of triggering an asthmatic attack. School personnel must be taught by the school nurse the types of activities that are best tolerated by the asthmatic child. Swimming is best tolerated, probably because of the high humidity in the air inhaled, and the exhaling of air underwater is similar to “pursed-lip” exhaling. Sports such as baseball, short sprints, and gymnastics are well tolerated, because the activity is intense but short. Prolonged intense activity, such as jogging, lap running, race running, or basketball, is less tolerated by individuals with asthma. Preexercise puffs of a prescribed inhaler and a warm-up before vigorous exercise can enable the child to participate more fully in age-appropriate school physical exercise. Many Olympic athletes have successfully managed their asthma symptoms. The promotion of normal growth and development is a basic goal in asthma care, and participation with peers is important.
The child is hospitalized for more severe asthma attacks. The nurse limits conversation with the child during the emergency period to questions that can be answered “yes” or “no.” Oxygen reduces hypoxia and improves the patient’s color. It is administered by nasal prongs, hood, or facial mask.
If the child is in respiratory distress on admission, oxygen is administered per the physician’s protocol, and the child is positioned comfortably. One method is to place a pillow on the overbed table and have the child extend the arms over it, elbows bent. This is comfortable and allows maximum use of the accessory muscles of breathing. Lung sounds are assessed for rhonchi, wheezing, or rales. Arterial blood gases and vital signs are monitored. The child is evaluated for clinical improvement (quieter, slower respirations, relaxed facial expressions, cessation of retractions). Oral fluids are encouraged because they help to liquefy secretions and are needed to compensate for fluid loss from dyspnea and diaphoresis. Carbonated beverages, such as ginger ale and colas, are avoided when the child is wheezing. Beverages are served at room temperature because cold liquids can trigger reflex bronchospasm. Milk products are avoided because they tend to increase the production of mucus. Intake and output should be recorded. The patient is observed for cracked lips, the absence of tears, poor skin turgor, and a decrease in urine output, all of which signal dehydration.
A well-balanced diet and adequate fluids are necessary for general health. Ample time is allowed for meals, because respiratory distress may interfere with eating. The nurse organizes tasks so that the child obtains sufficient rest. The child is assisted with the use of the nebulizer.
Medication Safety Alert!
Oxygen is a drug, and administration should be correlated with monitoring of oxygen saturation levels. Too little oxygen can result in hypoxia; too much oxygen can result in lung damage.
Self-care: The child is gradually taught self-care. The importance of exercise to strengthen vulnerable lungs is emphasized. Pursed-lip breathing (blowing out as if blowing a kiss) and biofeedback are also helpful. The child is taught to observe “personal triggers” that are forewarnings of an attack. He or she is taught how to use the peak flow meter. Other aspects of care include how to administer MDIs and understanding medications and their possible side effects. Specific information about how often and when to use inhalers is paramount. The child is encouraged to discuss daily school routines. The health care provider is seen regularly to evaluate progress and readjust the medications as needed. The nurse reviews the signs of respiratory infection with the child and where, when, and whom to call for help. Early attention to symptoms may prevent escalation of the disease.
Metered-dose inhalers: Routine monitoring of airway obstruction should be part of comprehensive asthma management. A child of age 6 years can self-test with adult supervision. A diary of peak flow readings (PFRs) should be brought to the physician at each follow-up visit (Figure 25-8). The nurse should be alert to the fact that compliance may be a problem with older children and adolescents, who may cause false results by manipulating the unit.
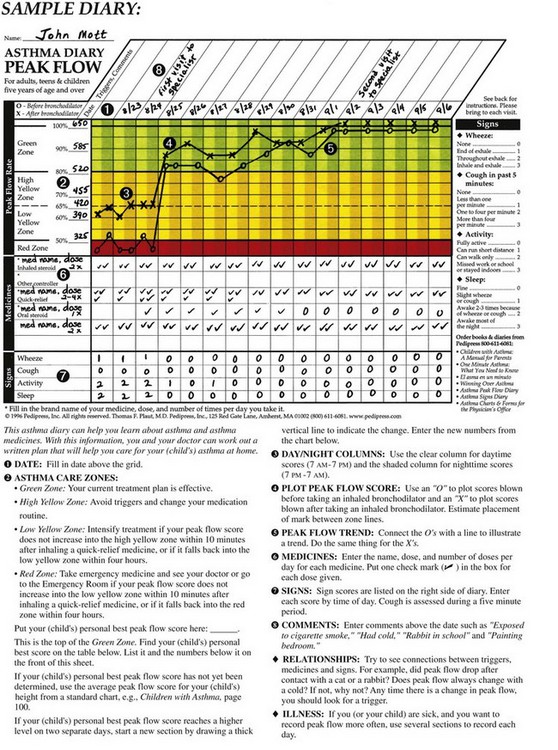
FIGURE 25-8 The asthma diary. The clear column is for daytime peak flow reading (PFR) score, and the shaded column is for nighttime peak flow scores. An X indicates PFR following inhaler therapy. An O indicates PFR without inhaler therapy. A check mark indicates medication taken. Asthma triggers and comments are recorded. The diary is brought to each follow-up clinic visit.
An MDI consists of a pump that is a mouthpiece and an actuator (or holder) into which a medicine canister is inserted. Pushing down on the actuator releases a dose of medication (puff), which is inhaled through the mouthpiece. This delivers the medicine directly to the lungs without systemic side effects. The use of a spacer slows the movement of the medicine, allowing more time to inhale the medicine. Some spacers reduce the need for hand-press-breath coordination during inhalation. Aerochambers with masks are available for infants. Practice to acquaint the infant to the treatment is helpful, since crying reduces delivery of medication to the lungs. Parents should be taught to use distractions such as books, music, or toys to minimize crying. Dry powder inhalers are becoming popular since more medications are coming in powder form. The child should be taught to rinse the mouth after steroid inhalation to prevent the development of candidiasis. Activators should be cleaned regularly.
Most near-empty inhaler canisters will float in a bowl of water. Measuring the canister content level enables the child to request a refill and avoid missing medication doses. Inhalers are designed to be used with an open-mouth technique or a closed-mouth technique (Skill 25-2). A nebulizer machine can be used in the home when inhalers are not appropriate for the individual child.
Skill 25-2 Using a Metered-Dose Inhaler
1. Insert the metered-dose inhaler (MDI) canister into the holder.
3. Instruct the child to exhale a normal breath.
4. Instruct the child to close mouth around the mouthpiece (or hold 2 to 4 cm [0.8 to 1.6 inches] from the open mouth).
5. Push down on the canister for one puff.
6. Instruct the child to inhale deeply and slowly for 3 to 5 seconds.
The nurse should help the child see connections between triggers, medicines, and signs of respiratory distress. For example, did the peak flow drop after contact with a cat or rabbit? Does the peak flow always change with a cold? Any time there is a change in peak flow, the child should know to look for what triggered it.
During every clinic visit, the nurse should have the child demonstrate the use of the inhaler or spacer and reinforce the principles involved.
Status Asthmaticus
Status asthmaticus is continued severe respiratory distress that is not responsive to drugs, including epinephrine and aminophylline. This is a medical emergency. The child requires immediate admission to the ICU. Oxygen is administered via nasal cannula because mist in a mist tent can cause coughing or wheezing. Vital signs and the flow of IV medications are carefully monitored. Complying with the prescribed medical regimen, promptly seeking medical care when indicated, minimizing exposure to known allergens, wearing medical identification bracelets, and having a written plan for crisis management can minimize the life-threatening occurrence of status asthmaticus.
Cystic Fibrosis
Pathophysiology: Cystic fibrosis (CF) is a major worldwide cause of serious chronic lung disease in children. It occurs in approximately 1 in 3000 live births of Caucasian infants and 1 in 17,000 births of African American infants in the United States (National Center for Health Statistics, 2006). It is most prevalent in persons of northern and central European descent. It is an inherited recessive trait, with both parents carrying a gene for the disease. There is a defect in chromosome number 7 that is thought to have developed many years ago as a protective response of the human body against cholera. As the chromosomes mutated to develop the body’s resistance to cholera, the change in the gene resulted in another defect that caused CF. The Centers for Disease Control and Prevention (CDC) highly recommends screening of all newborns for CF by use of a measure of immunoreactive trypsinogen level, which is elevated in cystic fibrosis. The screening will enable early detection and treatment (Neff, 2005).
The basic defect in CF is an exocrine gland dysfunction that includes (1) increased viscosity (thickness) of mucous gland secretions, and (2) a loss of electrolytes in sweat because of an abnormal chloride movement. CF is considered a multisystem disease because of the following effects of the thick, viscid secretions:
• Respiratory system: Small and large airways are obstructed by the thick secretions, resulting in difficulty breathing. The accumulation and stasis of the thick secretions create a medium for growth of organisms that cause repeated respiratory infections. The thick secretions in the lungs and response of tissues to infections cause hypoxia that can result in heart failure. Emphysema, wheezes, and respiratory distress are common.
• Digestive system: The thickened secretions prevent the digestive enzymes from flowing to the gastrointestinal tract, resulting in poor absorption of food and general growth failure. Bulky, foul-smelling stools that are frothy because of the undigested fat content are characteristic. Thick, impacted feces can cause rectal prolapse. Pancreatic, liver, and biliary obstruction occur.
• Skin: Loss of electrolytes (sodium and chloride) in the sweat causes a “salty” skin surface. Loss of electrolytes via the skin predisposes the child to electrolyte imbalances during hot weather.
• Reproductive system: Thick secretions can decrease sperm motility. Thick cervical mucus can inhibit sperm from reaching the fallopian tubes.
Manifestations: The manifestations of CF are illustrated in Figure 25-9.
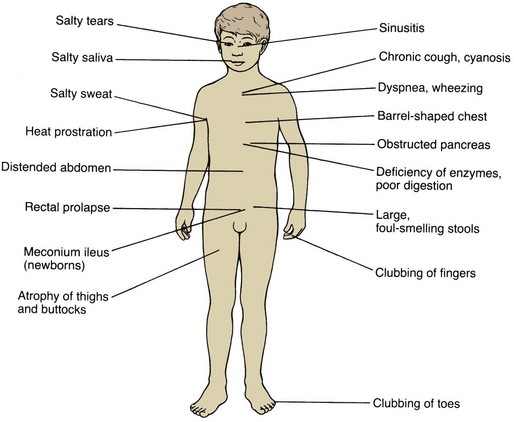
Lung Involvement: The air passages of the lungs become clogged with mucus. There is widespread obstruction of the bronchioles. It is difficult for the child to breathe; expiration is especially difficult. More and more air becomes trapped in the lungs (obstructive emphysema), and small areas of collapse (atelectasis) may occur. Eventually the chest assumes a barrel shape, with increased diameter across the front and back. The right ventricle of the heart, which supplies the lungs, may become strained and enlarged. Clubbing of the fingers and toes (Figure 25-10), a compensatory response indicating a chronic lack of oxygen, may be present. Staphylococcus and Pseudomonas infections can easily occur in the lungs, which provide a suitable medium for the organisms’ growth. This causes more thickening of the abnormal secretions, irritates and damages lung tissues, and further increases lung obstruction.

Dyspnea, wheezing, and cyanosis may occur. The child is irritable and tires easily. Gradually, there is a change in physical appearance. Evidence of obstructive emphysema, atelectasis, and fibrosis of lung tissue may also be present. The prognosis for survival depends on the extent of lung damage. However, this is only part of the picture, because CF also affects the pancreas and sweat glands.
Pancreatic Involvement: The pancreas lies behind the stomach. Some of its cells secrete pancreatic enzymes that drain from the pancreatic duct into the duodenum in the same area in which bile enters. Changes occurring in the pancreas result from obstruction by thickened secretions that block the flow of pancreatic digestive enzymes. As a result, foodstuffs, particularly fats and proteins, are not properly digested and used by the body.
In infants the stools may be loose. Because of impaired digestion and food absorption, the feces of the child become large, fatty, and foul-smelling. They are usually light in color. The child does not gain weight despite a good appetite and may look undernourished. The abdomen becomes distended, and the buttocks and thighs atrophy (waste away) as fat disappears from the main deposit sites.
A condition known as meconium ileus exists when the intestine of the newborn becomes obstructed with abnormally thick meconium while in utero. This condition is caused by the absence of pancreatic enzymes that normally digest proteins in the meconium. The abnormal, puttylike stool sticks to the walls of the intestine, causing blockage. The presenting symptoms develop within hours after birth. The absence of stools and the presence of vomiting and of abdominal distention lead to suspicion of intestinal obstruction. X-ray films confirm the diagnosis.
Sweat Glands: The sweat, tears, and saliva of the patient with CF become abnormally salty because of an increase in sodium chloride levels. Up to about 20 years of age, more than 60 mEq/L of sodium chloride in sweat is diagnostic of CF (Neff, 2005). Levels of 40 to 60 mEq/L are highly suggestive. The analysis of sweat is a major aid in diagnosing the condition. The sweat test is the best diagnostic study. Because these children lose large amounts of salt through perspiration, they must be watched for heat prostration. Liberal amounts of salt should be given with food, and extra fluids and salt should be provided during the hot weather.
Complications: CF is often responsible for rectal prolapse in infants and children partly because of poor muscle tone in the rectal area and because of the excessive leanness of the buttocks of the patient.
As the disease progresses, the liver may become hard, nodular, and enlarged. Cor pulmonale (cor, “heart,” and pulmon, “lung”), heart strain caused by improper lung function, is often a cause of death. There is a deficiency of vitamin A because the child is unable to absorb fats from which this vitamin is obtained. Sexual development may be delayed in these patients. Males are generally sterile, but sexual function is unimpaired. Adolescent girls may experience secondary amenorrhea during exacerbations.
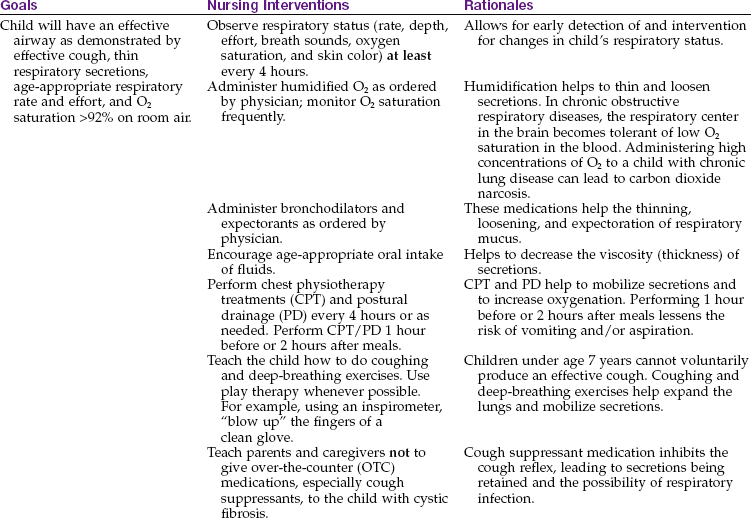
Respiratory relief: See Chapter 22 for a discussion of oxygen therapy. Antibiotics may be given as a preventive measure against respiratory infection; however, this treatment is controversial. Nursing Care Plan 25-1 summarizes interventions for the CF patient. Intermittent aerosol therapy is administered to provide medication to the lower respiratory tract and to promote the evacuation of secretions. An inhaler that acts as a mucus clearance device can be used in the home care of these children. Bronchodilators are used to increase the width of the bronchi, allowing free passage of air into the lungs. Human recombinant dornase alfa (Pulmozyme) in a single daily aerosol dose is effective in decreasing thickness of secretions, thereby improving pulmonary function.
25-1  Nursing Care Plan
Nursing Care Plan
The Pediatric Patient with Cystic Fibrosis
A 5-year-old child diagnosed with cystic fibrosis is admitted to the unit. The child has loose, foul-smelling stools, a persistent cough with some nasal flaring, and chest retractions.
Ineffective airway clearance related to inability to clear mucus from respiratory tract secondary to cystic fibrosis as evidenced by thick mucus production, unproductive or minimal cough, and adventitious breath sounds (wheezes, crackles, dyspnea, tachypnea, cyanosis)
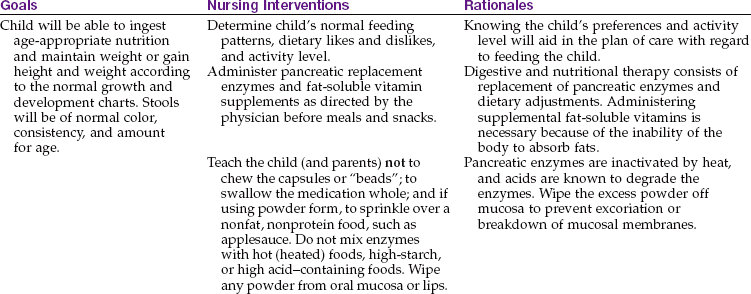
Imbalanced nutrition: less than body requirements related to decrease in the availability of pancreatic enzymes; poor intestinal absorption of nutritional intake; anorexia secondary to cystic fibrosis as evidenced by decreased oral intake, weight loss or failure to thrive, diarrhea, steatorrhea, or constipation

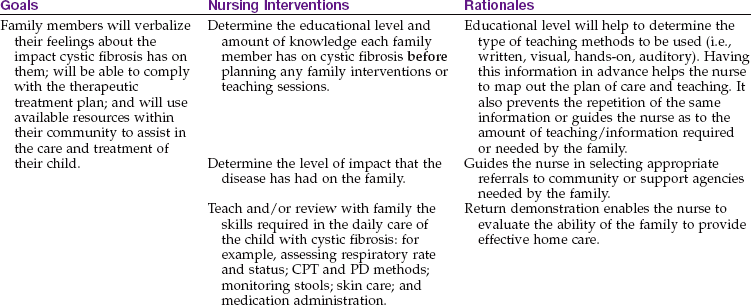
Interrupted family processes related to chronicity of disease, need for outside support, the risk of life-threatening complications as evidenced by frequent physician office visits or hospitalizations, a diminished focus on other siblings in home, and the need for therapeutic interventions and compliance with home care routines
Postural drainage and chest-clapping therapy are also of value (Figure 25-11). These are performed by the physical or respiratory therapist during hospitalization. When postural drainage and chest clapping are done properly, the secretions in the chest are moved up and out. This should be explained to the parents so they will continue this valuable procedure when the child comes home. Instructions may need to be repeated frequently to encourage full cooperation of the parents and child. These procedures are done after nebulization and at least 2 hours after eating. General exercise is good for the patient because it stimulates coughing. Play activities such as somersaults and headstands within the child’s endurance limits are therapeutic.
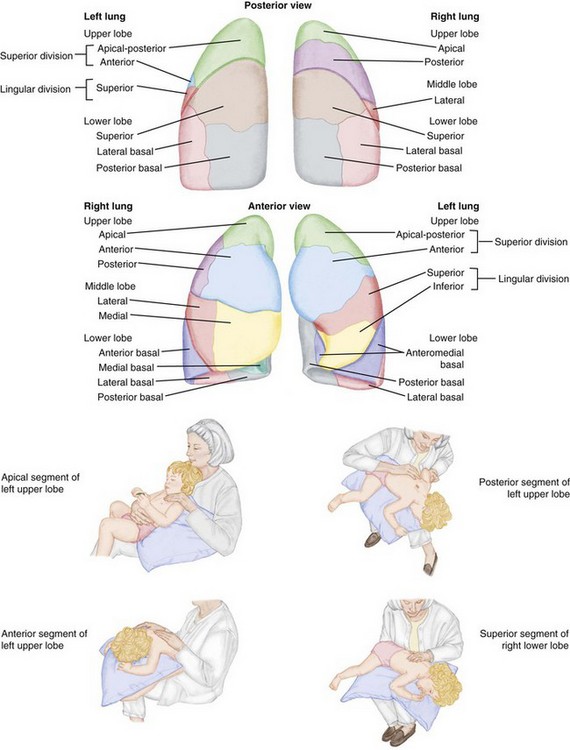
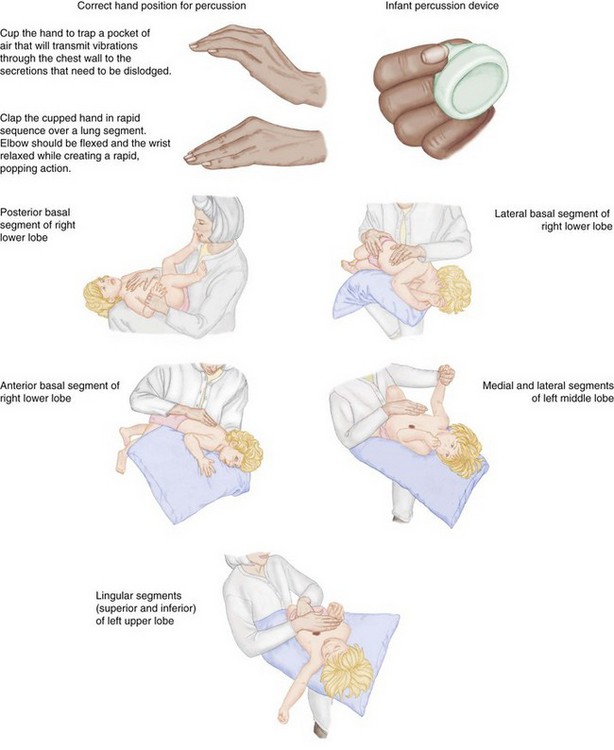
FIGURE 25-11 Postural drainage. The positions for postural drainage are correlated with the segment being drained.
Breathing exercises may also be recommended for the older child. Pursed-lip breathing is one technique that is simple and effective. The patient is instructed to inhale through the nose, then to exhale through the mouth with the lips pursed as if whistling. Exhalation should be at least twice as long as inhalation. (If it takes 3 seconds to breathe in, 6 seconds are taken to allow all the air to escape.) The child is taught not to force the air out but to let it escape naturally.
Prevention of respiratory infections is essential. The child is isolated from patients and personnel who may harbor infections. The period of hospitalization is kept brief, if possible, to avoid cross-infection. This child must be given the necessary immunizations against childhood diseases (see Chapter 32).
An oral pancreatic preparation, such as pancrelipase (Pancrease), is given to the child with each meal and snack to replace the pancreatic enzymes the child’s body cannot produce. This medication is considered specific for the disease because it helps the child to digest and absorb food, thus improving the condition of the stools. If the child is ill and not eating, the medication is withheld. When meals are erratic, such as during vacations, medication is given when the largest amount of food will be consumed. High doses have been associated with the development of gastrointestinal strictures, and the child should be monitored. Vitamins A, D, E, and K, iron, and zinc supplements are also prescribed.
Diet: The maintenance of adequate nutrition is essential. The diet is high in protein and calories. Supplemental enzymes are given with the food to aid in digestion, and fat-soluble vitamins may be prescribed. The child should be weighed daily. Intake and output are recorded. Children should have free access to salt, although a regimented salt supplementation is no longer recommended. Infants can breastfeed with added enzyme intake. Formula fed infants do best with a higher calorie-per-ounce formula, such as Pregestimil or Alimentum. Parenteral alimentation (total parenteral nutrition [TPN]) may be indicated in some cases.
General hygiene: The nurse must pay special attention to the skin of the child with CF. The diaper area is cleansed after each bowel movement. An ointment to protect the skin is advisable because the character of the stool subjects the diaper area to irritation. The buttocks are exposed to air when a rash occurs. Because the child has little fat and muscle, the position must be changed frequently, especially if the child is weak and cannot get out of bed. Frequent changes of position also prevent the development of pneumonia.
The child wears light clothing to avoid becoming overheated; it should be loose to allow freedom of movement. Good oral hygiene is necessary, because the teeth may be in poor condition because of dietary deficiencies. Mouth care is given after postural drainage because foul mucus may be raised, leaving an unpleasant taste in the patient’s mouth.
Long-term care: The goals of care include minimizing pulmonary complications, ensuring adequate nutrition, promoting growth and development, and assisting the family to adjust to the chronic care required at home. This is extremely taxing financially, physically, and emotionally. The parents must distribute their time and energy within the family yet give careful attention to their sick child or, sometimes, children. How do they keep from spoiling the child? Do they limit the normal activities of the remaining children to spare the sick one? What about birthday parties, camping, scouts, pets, and epidemics at school? What does a trip to the shore or mountains entail? When do the parents find time for themselves? Coping techniques must be developed and used.
Parents need explicit instructions regarding diet, medication, postural drainage, prevention of infection, rest, and continued medical supervision. Many families require the assistance of a social worker to secure funds for equipment and drugs. Genetic counseling is also advised.
Emotional support: The child who is chronically ill finds it hard to accept restricted activity. The amount and types of diversion required vary in CF because the disease affects children of all ages and varies in severity.
It is thought that children benefit from simple, straightforward answers to questions about their illness. An uncomplicated diagram might be helpful. They should know why they must take medications with each meal, use the nebulizer, and have postural drainage. They should see and handle the unfamiliar equipment necessary for care.
The young child finds it more difficult to be separated from parents during hospitalization. Even when the prognosis is grave, a child’s courage is sustained if parents are there. Rooming-in is encouraged whenever possible. Close contact by mail, telephone, or e-mail with school, church, and clubs is important for the school-age child. It is helpful for patients to develop an activity that they enjoy, such as piano or art. This increases feelings of worth and provides outlets for feelings. Consideration must be given to ways of fostering love, acceptance, trust, fair play, security, freedom of choice, creativity, and maintenance of self-identity.
Bronchopulmonary Dysplasia
Pathophysiology: Bronchopulmonary dysplasia (BPD) is a fibrosis, or thickening, of the alveolar walls and the bronchiolar epithelium caused by oxygen concentrations above 40% or by the mechanical pressure ventilation given to newborns for a prolonged time. Swelling of the tissues causes edema, and the respiratory cilia are paralyzed by the high oxygen concentrations and lose their ability to clear mucus from the airways. Respiratory obstruction, mucus plugs, and atelectasis follow.
Prevention: Respiratory distress in the newborn is the major reason why oxygen and ventilators are used for prolonged periods. The main cause of respiratory distress in the newborn is prematurity. Therefore the prevention of preterm births is the best way to prevent BPD. The goal of treatment for respiratory distress in the newborn should be to administer only the amount of oxygen required to prevent hypoxia, at the minimum necessary ventilator pressures, so as to prevent tissue trauma. The use of antenatal steroids to hasten lung development during preterm labor and the administration of surfactant within 15 minutes after delivery in a very premature infant may prevent respiratory distress that would necessitate oxygen and prolonged ventilation treatment.
Treatment: Once BPD has developed, the goal of therapy is to reduce inflammation of the airway and to wean the infant from the mechanical ventilator. The infant may become oxygen dependent and develop reactive airway bronchoconstriction. Noninvasive ventilation techniques have been developed, such as synchronous intermittent mandatory ventilation (SIMV) via nasal cannula prongs, continuous positive airway pressure (CPAP), high-flow blended nasal cannulas, and high-flow humidified oxygen, which are safer and may minimize the development of BPD. Right-sided heart failure may also develop. Fluid restriction, bronchodilators, and diuretics may be prescribed. A tracheostomy may be also needed. Nasogastric tube feedings may be required to conserve energy while maintaining adequate nutrition. Infants with BPD often develop respiratory stridor and retractions with even minor respiratory infections that result in repeated hospitalizations. Ongoing home care is required, and respiratory problems persist through adulthood. Maintaining optimum growth and development is a challenge. Education and support of the family for a technology-dependent child at home are essential, and a multidisciplinary health care team approach is essential.
Sudden Infant Death Syndrome
Sudden infant death syndrome (SIDS) is clinically defined as the sudden, unexpected death of an apparently healthy infant between 2 weeks and 1 year of age, for which a routine autopsy fails to identify the cause. It is also referred to as “crib death.” The peak incidence is between 2 and 4 months of age. The clinical features of the disease remain constant:
It has occurred even when the parents were sleeping in the same room. The occurrence of SIDS has decreased by 38% between 1992 and 1996 when the “back to sleep” program was first implemented. Approximately 2230 infants died of SIDS in the United States in 2005 (CDC, 2009).
SIDS is thought to be caused by a brainstem abnormality of cardiorespiratory control. Overheating, irregular respiratory patterns, and decreased arousal responses are contributing factors. Increased risk factors for SIDS may include maternal smoking or cocaine use that causes hypoxia of the fetus, preterm birth, and poor postneonatal care. A face-down sleeping position may cause rebreathing of expired air or airway occlusion. Wrapping the infant who is placed face down may increase the risk for SIDS by preventing the infant from lifting and turning the face to the side.
Prevention: For high-risk infants, home apnea monitors have been used to warn parents of an impending problem and enable them to try to resuscitate the infant manually. All parents should have cardiopulmonary resuscitation education. However, frustration with frequent alarm malfunctions and noncompliance have made this intervention less effective. The AAP recommends that all healthy infants be placed in the supine (back-lying) position on firm mattresses to prevent SIDS. The use of soft pillows or fluffy blankets for the infant to lie on is discouraged because it can prevent the infant from raising and turning his or her head. A national educational media campaign for this recommended positioning of infants has decreased the occurrence of SIDS.
Nursing Care: In talking with grieving parents after the death of their infant, the nurse must convey some important facts: that the infant died of a disease entity called sudden infant death syndrome, that currently the disease cannot be predicted or prevented, and that they are not responsible for the child’s death. Grieving parents need time to say good-bye to their child. They are encouraged to hold and rock the infant, shed tears, and assist in burial preparations. This process is conducive to the resolution of grief.
Parents experience much guilt and are catapulted into a totally unexpected bereavement that creates the need for numerous explanations to relatives and friends. Often needless blame has been placed on one parent by the other or by relatives. The family baby-sitter and physician may also be targets of attack. Emergency department personnel must be especially sensitive and supportive during this crisis. There have been crib deaths for which parents have been mistakenly charged with child abuse.
Get Ready for the NCLEX® Examination!
Key Points
• Routine handwashing practices can prevent the spread of the common cold.
• Quiet play may be more restful than confinement to bed for toddlers and young children.
• Use of nosedrops with an oil base should be avoided.
• Laryngomalacia and acute spasmodic laryngitis are benign forms of croup.
• Laryngotracheobronchitis and epiglottitis are acute types of croup.
• A croupette, or mist tent, provides moist air supersaturated with microdroplets that can enter the small airway of a child and relieve respiratory distress.
• A tongue blade examination of the throat can cause sudden respiratory arrest in a child with epiglottitis.
• Frequent swallowing while the child is sleeping is an early sign of bleeding immediately after a tonsillectomy.
• Coughing, clearing the throat, and blowing the nose should be avoided in the immediate postoperative period after a tonsillectomy.
• Swimming and sports activities that involve intermittent activity are well tolerated by asthmatic children.
• Cystic fibrosis is a multisystem disease characterized by an increased viscosity of mucous gland secretions.
• Bulky, frothy, foul-smelling stools are characteristic of cystic fibrosis.
• The maxillary and ethmoid sinuses are most often involved in childhood sinusitis.
• Periorbital cellulitis is a complication of childhood sinusitis.
• Pulse oximetry readings are of little value in carbon monoxide poisoning.
• An intubation tray should be readily available at the bedside in infants with carbon monoxide poisoning.
Additional Learning Resources
 Go to your Study Guide for additional learning activities to help you master this chapter content.
Go to your Study Guide for additional learning activities to help you master this chapter content.
 Go to your Evolve website (http://evolve.elsevier.com/Leifer) for the following FREE learning resources:
Go to your Evolve website (http://evolve.elsevier.com/Leifer) for the following FREE learning resources:
• Answer Guidelines for Critical Thinking Questions
• Answers and Rationales for Review Questions for the NCLEX® Examination
• Glossary with English and Spanish pronunciations
• Interactive Review Questions for the NCLEX® Examination
• Patient Teaching Plans in English and Spanish
 Online Resources
Online Resources• Guidelines for the Diagnosis and Management of Asthma: www.nhlbi.nih.gov/guidelines/asthma/asthgdln.pdf
• National Asthma Control Initiative (NACI): http://rover.nhlbi.nih.gov/health/prof/lung/asthma/naci
• Respiratory syncytial virus: www.cdc.gov/rsv
Review Questions for the NCLEX® Examination
1. Which is a priority nursing diagnosis in a child admitted with acute asthma?
2. Which sign or symptom observed in a sleeping 2-year-old child immediately after a tonsillectomy necessitates reporting and follow-up care?
3. The nurse is reinforcing teaching concerning the use of a cromolyn sodium inhaler for a 10-year-old with asthma. Which would be an accurate concept to emphasize?
1. You should use the inhaler whenever you feel some difficulty in breathing.
2. You should use the inhaler between meals.
3. You should use the inhaler regularly every day even if you are symptom free.
4. You can discontinue using the inhaler when you are feeling stronger.
4. A health care provider is preparing to examine the throat of a child diagnosed with acute epiglottitis. A priority nursing responsibility would be to:
5. An infant is admitted with a diagnosis of respiratory syncytial virus (RSV) infection. The type of transmission-based isolation precaution the nurse would set up would be:
Critical Thinking Question
1. The father of a child diagnosed with cystic fibrosis visits his child in the hospital. He states that he thinks the hospital food does not agree with his child because he notices the child has a loose stool with a very bad odor. None of his other children have that type of stool. He brought some loperamide (Imodium) pills from the drugstore to give to the child. What is the best response of the nurse?