7 Aromas, mind and body
Introduction
Smell is the most mysterious and evocative of our senses: it is our chemical sense, informing us about the surrounding environment and giving information that is not tangible, visible or audible. This chapter explores the connections between a person’s thoughts, feelings and immune status, and suggests that the ability of essential oils to affect all these via the sense of smell makes aromatherapy a truly holistic therapy.
The impact of the mind and emotions on the body
Throughout the ages people concerned with healing have been aware that there is a connection between thoughts, emotions and the state of health of the physical body. The British Medical Journal in 1884 observed that ‘the depression of the spirits at these melancholy occasions (funerals) … disposes them to some of the worst effects of the chills’ (Wood 1990a). These effects can be real, and changes in blood chemistry have been recorded even when the emotions are conjured up artificially, as in the case of superstition. Three thousand years ago the impact and influence of the intangible human mind on the material body was recorded in the Old Testament: ‘A merry heart doeth good like a medicine; but a broken spirit drieth the bones’ (Proverbs 17: 22, King James version).
In modern times this has been recognized not only by psychotherapists and those in psychosomatic medicine, but also in general medicine.
Psychoneuroimmunology (PNI)
In the past the psyche, the nervous system and the immune system were studied more or less as independent systems functioning alongside each other, but without direct connections. The science of PNI attempts to understand how the brain and the immune system communicate with each other,
PNI is also referred to as psychoendoneuroimmunology (PENI).
The immune system
Neuropeptide messengers produced by the immune system, brain and nerve cells provide two-way communication between the emotional brain and bodily systems via hormonal feedback loops. The limbic system (hypothalamus and pituitary), the spleen, the adrenal and thymus glands all have nerve interconnections. Thus emotions are capable not only of directing the body but also of receiving and being modified by information feedback from cells in the body.
Adrenalin and cortisol are two of the many chemical messengers whose release can be triggered by negative emotion in sudden or long-term stress: these two hormones influence the immune system directly to switch it off (Borysenko 1988 p. 14). Adrenocorticotrophic hormone (ACTH) suppresses pituitary action by stimulating the adrenal gland to produce adrenaline (epinephrine), which is a stimulator of the autonomic nervous system (ANS). The idea has gradually gained ground that emotional states can translate into altered responses in the immune system: negative thoughts and sad emotions can sometimes temporarily lessen the effectiveness of the immune system. Hence the body puts non-material thoughts and emotions into physical effect, either to produce a beneficial healing effect or to inflict self-damage. This idea is echoed by many writers.
The effect of the emotions on health
It has not yet been possible for anyone to show a link between a particular emotion and any specific physical disease – ‘Pessimism is not linked to any particular disease’ (Wood 1990b) – although pessimism or depression amplify symptoms of pain. It can probably be said that the course of nearly all disease is affected by thoughts, feelings, emotions and attitudes, which are in turn influenced by personality.
Fight-or-flight response
In the distant past people developed a response to dangerous situations designed to protect the body, known as the automatic primary stress response; the arousal system is located in the brain stem. When a person is presented with a threatening set of circumstances, the median hemisphere of the hypothalamus instantly puts chemical messengers (catecholamines) into the bloodstream. In conjunction with the sympathetic nervous system, these trigger an array of interconnected reactions – the release of steroids, glycogen and adrenaline, faster breathing, increased heart rate, raised blood pressure, dilated pupils and so on – all designed to prepare the body for instant action resulting from the awareness of danger. Today, this ancient inbuilt fight-or-flight response is evoked many times, not only in response to short-term acute physical risk (e.g. war, traffic, mugging etc.) but also to threats such as job security, divorce and money problems. Long-term stress conditions like these make the traditional response unsuitable: not only it is ineffective, but it can harm the body it is supposed to protect. The high-pressure lifestyle lived by so many people is responsible for many health-threatening situations, both chronic and acute, and it is now generally recognized that some physical problems in our society have a non-physical component in their aetiology. ‘It is not a question of whether an illness is physical or emotional, but how much of each’ (Dunbar 1954).
Anticipation stress
Why stress should have the effect of reducing the body’s defences is not clear and is, as yet, unexplained, but it is known that students are prone to catch colds at examination times and that such times of stress reduce the efficiency of the immune system, as a result of lowered production of interferon leading to decreased function of natural killer cells. Some of the more ambitious students suffer a greater reduction in the immune system defences, perhaps because the examination represents a bigger threat to them (Borysenko 1988 pp. 12–16). The effects of stress of this kind are popularly recognized in the case of brides-to-be who may catch a ‘bride’s cold’.
Grief
Statistics exist for various stressful situations that make people more prone to accidents and poor health, e.g. divorce, marriage, holidays, death etc. Depression following the death of a spouse is likely to have an adverse effect on the protective immune system and the health of the survivor: there are 50% more deaths than would normally be expected in widowers during the first year after the loss.
Voluntary stress
Although repeated stressful situations may produce ill effects resulting in chronic illness, many people joyfully expose themselves to repeated stress with no apparent ill effect, e.g. mountaineering, car racing and skiing. It is when repeated stress is unwanted and creates unhappiness that it will have unwanted effects; on the other hand, if the repeated stressful situations are sought and enjoyed, they can bring beneficial effects. In sporting contexts the euphoria resulting from the release of endorphins is recognized, for instance ‘runner’s high’.
Thinking and healing
Using the mind to control pulse rate and breathing, and to bring about general relaxation of the body, has long been practised in different cultures. In the meditative state the brain waves drop from the β rhythm to the slower α rhythm; the blood circulation is diverted more to the brain and vital organs, with less going to the muscles, so that the heart rate is slower, blood pressure is lower and little oxygen is used.
Case study 7.1 Death and bereavement
Client assessment
B, a 61–year–old man, was battling severe pain from cancer of the lung and he and his wife were but slowly coming to terms with the fact that his life would not be prolonged.
Intervention
The essential oils used to assist and comfort were put into a 10 mL dropper bottle:
• 2 mL (40 drops) Boswellia carteri [frankincense] – analgesic (to mental pain and fear also), antidepressive, energizing, immunostimulant
• 2 mL Chamaemelum nobile [Roman chamomile] – calming and sedative (easing anxiety, tension, anger and fear)
• 10 drops Rosa damascena [rose otto] – general tonic, neurotonic, balancing and calming to the mind
A few drops of this was applied to the soles of his feet and put on tissue to inhale. 15 drops were put into almond oil for hand, foot and back massages.
The therapist worked closely with him and his family in the hospital setting, his wife carrying a tissue with a drop of rose oil – she claimed it helped her accept the inevitable.
Outcome
His feeling of relaxation and peace was evident and he claimed he also slept well for a couple of nights after a treatment.
After he passed away – peacefully – the following blend was provided to help the family cope with the bereavement, oils to relieve grief being analgesic, calming, healing and stimulating to the heart and mind:
• 1 drop Melissa officinalis [melissa] – calming, sedative, uplifting to the emotions, a good pick-me-up after shock
• 3 drops Origanum majorana [marjoram] – analgesic, calming, neurotonic, strengthening to the mind
• 1 drop Rosa damascena [rose otto] – cicatrizant, as well as having the properties above
This blend was used by the family for self-massage around the neck and shoulders every night and morning. B’s mother thanked the therapist, saying that she was sure it had helped her to accept and adjust.
All this is initiated by thought alone, effected via the hypothalamus. Hesse, experimenting on cats in the 1950s, found that when the hypothalamus was stimulated, increased activity or relaxation was produced (Hesse & Akerl 1955). Sometimes, in people suffering a terminal illness, this mind-to-body effect can make healing possible even though a cure is not.
It is now realized that for optimum healing the sufferer must be fully involved in all stages of the treatment, from diagnosis to final cure, and that all true healing comes from within. Healing is accomplished by mental and physical routes, with primary roles played by the patient, doctor and nurse, while family and friends take secondary supportive parts. As Plato wrote in the third century BC:
The curing of the part should not be attempted without treatment of the whole. No attempt should be made to cure the body without the soul and if the head and the body are to be healthy, you must begin by curing the mind. … For this is the great error of our day in the treatment of the human body, that physicians first separate the soul from the body.
Trust and placebo
Another well-known example of the effect of thought on the physical body is the placebo effect. This happens when the cure or amelioration of an illness is due to the patient’s trust and belief in a prescribed substance, to faith in the healer, or frequently a combination of both. Dummy painkillers are 56% as effective as morphine in the treatment of severe chronic pain (Chaitow 1991). This remarkable and much-used placebo effect is important in all healing: when people are made to feel better, positive healing thoughts, which encourage the healing process, are generated. If an aromatherapy treatment does no more than make people feel better in themselves, it puts the whole person into healing mode.
‘Immunity is to some degree under mental control’ (Wood 1990a). Just as positive healing thoughts induce healing reactions in the body, the efficiency of the immune system is reduced by negative beliefs and thoughts. Immunity from disease appears to be enhanced or diminished by beliefs, and by the environment in so far as it affects our emotions. Fortunately, the human race is intrinsically optimistic, with a will to survive.
Where does aromatherapy fit in?
How can aromatherapy play an effective and worthwhile part in the mental–physical sphere of healing? It is established beyond doubt that essential oils can have physical impact in that they are bactericidal, anti-inflammatory, antifungal, appetite stimulating, hyperaemic, expectorant etc. (see Ch. 4 and Table 7.1). They possess properties which can affect the mind and emotions to sedate, calm and uplift; they also have effects on bodily systems, they evoke memories, change perception, calm agitation, relieve stress, activate cognitive responses and affect intercommunication (Cook 2008, Ouldred & Bryant 2008). They are therefore ideal tools for tackling not only physical problems but at the same time mental and emotional states, working via the sense of smell.
Table 7.1 Effects of essential oils used internally and externally (from Schilcher 1984)
| External application | Internal application |
|---|---|
| Hyperaemic | Expectorant |
| Anti-inflammatory | Appetite stimulating |
| Antiseptic/disinfectant | Choleric, cholekinetic |
| Granulation stimulating | Carminative |
| Deodorizing | Antiseptic/disinfectant |
| Insecticide/insect repellent | Sedative |
| Circulation stimulating |
The placebo effect (expectations effect) is another factor that may influence the effect of an aroma on human behaviour, mood and health:
People’s beliefs that odours can influence their mood or health may lead them to perceive such consequences when they are exposed to an odorant and may even help trigger actual effects. The potential for placebo effects is high in an area such as aromatherapy where various essential oils are promoted as having specific beneficial mood and health effects and the individuals using the odorants desire such outcomes.
Relaxation response
When safe and calm, people experience the opposite of the stress response, in that tension, blood pressure, oxygen use and so on are reduced. This has been termed the ‘relaxation response’ (Benson 1975). It can be brought about by many means, including reading, listening to favourite music, contemplating nature – and aromatherapy.
When, during a massage, the touch of the therapist is combined with the mental and physical effects of the essential oils, the client is helped to achieve a temporary separation from worldly worries, somewhat akin to a meditative state. The massage itself induces the relaxation response, which activates the body’s healing mode, and this, in conjunction with the essential oils, is outstanding for the relief of tension and anxiety, both physical and mental.
Whatever the method of application, the authors feel that in many cases most of the healing effect of essential oils is primarily through inhalation (see Ch. 6) via the mind and emotional pathways, and that a lesser part takes place via the physical body. There is no doubt that smelling plant volatile oils can affect the mood and general feeling of wellbeing in the individual. This is especially true when the essential oils are applied with whole-body massage: the physical and mental relaxation achieved during a massage session has to be experienced to be appreciated. To select essential oils to address the mental, emotional and physical needs of the client, the cause(s) of the health
Case study 7.2 Panic attacks and vertigo
Client assessment
A is in his mid-60s, referred for aromatherapy by a community psychiatric nurse as he had developed panic attacks and vertigo. She felt that aromatherapy would help in relieving his stress and therefore aid relaxation. His problems had arisen as a result of the long-term caring, full time, of a relative with Parkinson’s disease.
A was physically and mentally tired and not sleeping well. He described himself as having a ‘thickness of the head’ and ‘solid headaches’. Emotionally he was low – and tearful as he expressed his frustration at his condition. His arms and legs had large areas of ‘shark’s skin’ – psoriasis and warts – and he complained of coldness and aching in his knees.
Intervention
This was aimed at easing anxiety and depression, promoting sleep, relieving headaches, and at the same time providing warmth and acceptable physical contact.
A was given six massage sessions, once a fortnight, remedial massage techniques being used around the patella where there were granular deposits, and around the scapula where there was much tension.
The oils chosen were one drop each of:
• Citrus aurantium var. sinensis [sweet orange] – antidepressant, calming, mildly sedative; also recommended for vertigo
• Boswellia carteri [frankincense] – analgesic, antidepressant, energizing, immunostimulant
• Origanum majorana (sweet marjoram) – analgesic, calming, nervous system regulator, neurotonic; also recommended for vertigo
• 10 mL sweet almond oil – emollient, helps relieve psoriasis
For use in between treatments, A was given a 50 mL lotion containing:
• 10 drops Citrus limon [lemon] – anticoagulant, calming, immunostimulant
• 5 drops Boswellia carteri [frankincense] – analgesic, antidepressant, energizing, immunostimulant
• 5 drops Chamaemelum nobile [Roman chamomile] – anti-inflammatory, antispasmodic, calming and sedative, stimulant
This was to be applied twice daily to his shoulders, knees and psoriatic areas.
Outcome
After the first session A was more relaxed, although he still had some tension in the shoulder region. He appreciated the treatments, which relaxed and rejuvenated him.
By the third treatment the discomfort in his head had cleared and he began to feel brighter and more able to cope.
After his sixth and final session he no longer experienced vertigo, the headaches had gone, his skin was much improved and he felt less tense in his shoulders. Emotionally, he was better able to relax at home and felt more positive about the future.
Patient assessment
J attended the antenatal clinic at the Southern General Hospital in the early weeks of pregnancy and was extremely anxious and agitated. She was suffering from phobias, unable to enter a lift at any time and preferring very light rooms having windows with an open aspect. It became extremely difficult for J to attend the clinic because of her anxiety state, and her consultant suggested using aromatherapy.
Intervention
The first consultation took place in the antenatal clinic in a quiet bright room where, after an initial chat, J relaxed slightly and began to relate to – and trust – the aromatherapist.
She was offered a hand massage first, which was thought to be less threatening at the outset, allowing her to feel more confident with the therapist. She relaxed very well, so a shoulder and back massage was suggested, with J sitting astride a chair, her arms on a pillow placed on the chair back. The oils were chosen for their emotional effect, being confirmed in Price (2000) – Aromatherapy and your Emotions:
• 3 drops Lavandula angustifolia [lavender] – antispasmodic, cardiotonic, calming and sedative, tonic
• 2 drops Chamaemelum nobile [Roman chamomile] – antispasmodic, calming and sedative, stimulant
• 1 drop Citrus aurantium var. amara [neroli] – antidepressive, neurotonic
After this first treatment she felt much more able to discuss her fears and worries and counselling was able to take place, after which ways were discussed as to how her partner could help her cope with her fears.
She was given a tape of simple relaxation techniques, such as breathing and visualization, to use daily, together with a blend of the oils above (9, 6, 3 drops in 50 mL peach oil), for her husband to massage into her shoulders every night.
It was decided that it would help allay J’s fears to continue her aromatherapy treatments in a labour room, which enabled her to become familiar with both her surroundings and the midwives before she eventually arrived in labour.
In the early stages J was referred to a psychiatrist, but as she did not wish to take the medication prescribed at that point it was decided to continue with aromatherapy treatments, and her pregnancy progressed well.
When she was admitted to the labour suite, back and leg massages were given, using the blend above but with Myristica fragrans [nutmeg] instead of neroli. Salvia sclarea [clary] and lavender were given to her on a ball of cotton wool to inhale whenever necessary. She progressed well and surprised everyone – including herself – by remaining very calm throughout.
problem must be identified. All essential oils have an effect on both mind and body, although much research needs to be done in this respect.
Pregnancy and children
The influence of odours on humans begins even before birth; the odour of anise was presented to 24 neonates and it was shown that babies born to mothers who consumed anise during their pregnancy showed a stable preference for the smell, whereas babies born to non-anise consuming mothers showed aversive or neutral responses (Schaal et al. 2000).
A report by Nordin et al. (2004) showed that abnormal taste and smell was reported by 76% of 187 pregnant women tested, typically believed to be caused by their pregnancy. Increased smell sensitivity was common during the early stages of pregnancy (67%), occasionally accompanied by qualitative smell distortions (17%) and phantom smells (14%). Smell abnormalities occurred less in later periods of pregnancy and were virtually absent after delivery. Abnormal taste sensitivity was fairly commonly reported (26%), often described as an increase in bitter and a decrease in salt taste. Pregnancy smell and taste disorders relate to fetal protection mechanisms to avoid poisons and increase salt levels for the expanded fluid levels.
Anecdotal evidence indicates that during pregnancy olfactory sensitivity is increased, and the lack of scientific evidence to back this up was investigated (Cameron 2007). One hundred women who did not smoke were tested and the overall conclusion was that the effect of pregnancy was small and inconsistent, but interestingly the women felt that they had heightened awareness of smells during their pregnancy.
Adding the aroma of lemon to a classroom helps to involve all the senses in the learning experience, and Chu (2008) says that low-achieving school-children experienced success in a written task in the presence of an ambient odour (herbal tea), and when they experienced this same odour in a later task they were shown to be significantly better than a relevant control group. Chu claims that this is the first study to show a classic conditioning effect to influence human behaviour (but see Aromas, Memory and Mood, below).
The sense of smell is important in children with severe learning difficulties (see Ch. 13) who may have diminished hearing and sight, and essential oils can be used to make their life easier and more friendly. Fragrances have been used on wristbands to identify carers, each with their own aroma, to identify the child’s possessions and to locate areas, rooms and facilities (Sanderson, Harrison & Price 1991). This technique can also be used to make a baby sitter acceptable to the child.
The elderly
Aromas are well accepted in homes for the elderly, where they can create a pleasant atmosphere, either stimulating or relaxing, and some aromas may create an ambience which will bring back memories, possibly sparking off nostalgic conversation between the residents, with obvious benefits (see Ch. 14).
Gender differences
There appears to be a gender difference in the impact on the mind of inhaled essential oils, as it seems that women are the more likely to derive beneficial results. One study indicating this was the use of Citrus sinensis [sweet orange] diffused into the waiting room of a dental practice, where the results of a questionnaire filled in by patients of both genders showed that sweet orange oil had a relaxant effect compared to non-odour controls. Compared to men, women had a lower anxiety state, a more positive mood and higher level of calmness. The typical smell of dental premises, eugenol, was associated with anxiety and fear, although this was masked for women by the orange aroma, lowering their anxiety; for men this was only minor (Lehrner et al. 2000).
Another study set out to demonstrate the gender effect of odour on pain perception: 20 men and 20 women were exposed to pain by holding a hand in hot water while smelling previously selected odours. Separate analyses for men and women revealed a significant effect of odour on pain perception for women but not for men, and when the odour was found to be pleasant women demonstrated a significant reduction in pain perception (Marchand & Arsenault 2002). The gender difference was shown in a different light when subjects proofread pages of text containing misspelt words: all participants performed significantly better when aroma was present in the room; lavender produced the greatest effect on women, whereas peppermint had the greatest effect on men (Kliauga, Hubert & Cenci 1996).
Miyazaki, Motohashi & Kobashaya (1992a) investigated the effects on females of inhalation of orange oil (unspecified), Chamaecyparis taiwanensis lig. [hinoki] and menthol, and found an increase in speed performing a mental task and a decrease in the number of mistakes for all three aromas. Profiles of mood state (POMS) scores indicated that depression/dejection, anger/hostility and tension/anxiety decreased after inhalation of the oils, whereas fatigue scores tended to increase.
A similar study explored the effects of inhalation of orange oil (unspecified), Chamaecyparis taiwanensis lig. [hinoki] and eugenol on the mood of six male individuals, and POMS were monitored: blood pressure showed a decrease after inhalation of hinoki or orange oils, but an increased heart rate with eugenol. Eugenol was deemed to be unpleasant and scores indicated increases in fatigue, depression/dejection, confusion and anger/hostility and a decrease in vigour, whereas inhalation of hinoki oil had the opposite effect (Miyazaki, Motohashi & Kobashaya 1992b).
Pleasant smells give pleasure and feelings of self-esteem (Baron 1990, Nezlak & Shean 1990) and the effect on women may be greater because, according to Herz and Cupchik (1992), women have more intense odour memories than men.
Although it is understood that personality can bias sensory perception, Chen and Dalton (2005) say that the emotional state of a person has a similar effect. Subjects were exposed via video clips to prime happiness, sadness, negative/hostility and neutral feelings. The time taken to detect odours (suprathreshold odours of pleasant, unpleasant and neutral) and the intensity of the odours was recorded. It was found that females reacted faster to smells with emotional links than to neutral smells. Emotional states augmented the intensity of odours for males.
The skin of women is more permeable than that of men to toxic chemical molecules having a similar size to those of essential oil compounds, and they can retain more fat-soluble compounds in their body and so are affected more (Eisberg 1983).
It is interesting to note that almost all practising aromatherapists and users of aromatherapy products are women, only about 2% of men being involved: this is perhaps because the overall effects of essential oils on women are more significant than on men.
Anosmia – absence of the sense of smell
If a person has poor vision, it is obvious by the wearing of spectacles or using a white stick, but there is no easy means of recognizing a person’s inability to smell. Aromas are made up of individual chemicals and each cilium is equipped with uniquely contoured depressions into which a single aroma molecule can fit, somewhat like a jigsaw puzzle. If the appropriate ‘dock’ for the molecule being inhaled is absent, that smell will not be registered.
Total, specific and temporary anosmia
Anosmia can be total (where nothing is smelt at all), specific (an inability to register certain smells) or temporary. Almost everyone suffers temporary anosmia at some time, and probably each person has about five specific anosmias. About 5% of people are insensitive to the sweaty smell notes, and whereas about 50% of people are anosmic to androsterone, musk is almost universally noticed. Some aromas have exceptionally low detection thresholds, for example grapefruit and green pepper. Individuals vary in their perception of aromas, even among young adults, who constitute the most consistent age group (Doty 1991), but these differences are due to more than genetic anosmias, as shown by experiments revealing that repeated exposures can alter detection thresholds (Wysocki, Dorries & Beauchamp 1989).
Case study 7.4 Prolonged temporary anosmia
Client assessment
Mr P had suffered from severe chronic sinusitis for several years, his sense of smell diminishing over the years. After an operation there was no improvement, and not being able to smell was upsetting him. His wife was an excellent cook and he was unable either to smell – or to taste – her cooking. His wife, having heard the therapist on the radio, persuaded him to travel the 60 miles to her clinic, to see if aromatherapy could help him.
Intervention
It was decided to carry out a treatment ‘sandwich’ once a week: massage of his face, including pressure points, a Swiss reflex treatment on the sinus reflexes of his feet (see Ch. 8), finishing with a repeat of the facial treatment.
Two of the essential oils in the selected blend have extremely strong aromas, yet Mr P was unable to smell them:
• 2 drops Eucalyptus globulus [blue gum] – anticatarrhal, anti-infectious, anti-inflammatory, expectorant
• 3 drops Lavandula angustifolia [lavender] – anti-inflammatory, antiseptic, calming
• 2 drops Mentha x piperita [peppermint] – anti-infectious, anti-inflammatory, soothing
After each treatment two spills, with eucalyptus and peppermint respectively, were held to his nose in the hope of a reaction.
He was also given 20 drops each of the same oils in 50 mL carrier lotion, to apply on his face every morning after shaving, instead of his usual astringent.
Outcome
At the third visit, when the peppermint spill was led to his nose, Mr P let out a delighted yell:‘I can smell mint – it’s faint, but it’s definitely mint!’
After the next visit, Mr P showed enough improvement for him to visit the clinic only once a fortnight, still using his lotion at home very day.
After 3 months, the visits were altered to once a fortnight – and after 6 months from the commencement of treatment he had recovered his sense of smell sufficiently to appreciate some of the aromas from his wife’s cooking – a happy result for her too!
Temporary anosmia may be caused by colds, rhinitis and sinusitis, and results in a loss of taste. There are four types of taste cells (salt, bitter, sour and sweet) although appreciation of food flavours does not depend solely on these but also on texture, acidity/alkalinity, hot/cold, the trigeminal nerve – and smell.
If a person is incapable of smelling an aroma, does this mean that aromatherapy will not be effective? Many aromatherapists believe that prolonged use of essential oils will restore the sense of smell in some cases.
The authors treated a case of chronic sinusitis (suffered for 17 years), when even after an operation the client was unable to smell his wife’s cooking – his main cause for concern! After three treatments he was able to detect Mentha x piperita [peppermint], one of the essential oils in the mix used (which also included Eucalyptus globulus [Tasmanian blue gum] and Ocimum basilicum [European basil]). After 6 months of weekly treatments and daily self-care he had recovered his sense of smell sufficiently to recognize some of the gastronomic aromas greeting him on his return from work. This is in line with some surprising findings which indicate that in both humans and animals possessing specific anosmia, the sensitivity to some odours can be restored by repeated exposure to those odours (Holley 1993, Van Toller & Dodd 1992). There was an increase of cerebral blood flow in humans following inhalation of 1,8-cineole (found in eucalyptus and rosemary essential oils) and a similar result was obtained with an anosmic person (Nasel et al. 1994).
Fuji et al. (2002) claim that laryngectomy results in severe hyposmia (lowered smell ability) or anosmia. They tested olfactory acuity preoperatively and 3, 6, and 12 months postoperatively, and reported that olfactory acuity initially worsens but then improves to almost preoperative levels.
Polluted city air adversely affects the sense of smell: dwellers in Mexico City were found to have less olfactory ability than residents of Tlaxcala, where there is no pollution (Hudson et al. 2006). A later test showed that air pollution impairs olfactory and intranasal trigeminal sensitivity even in otherwise healthy young adults (Guarneros et al. 2009).
Does anosmia, sleep or unawareness negate aromatherapy?
• Effect of aroma during sleep: Aromas of essential oils have measurable physiological effects on humans during sleep. Ten participants were monitored to see whether any physiological changes occurred when they were subjected to 3-minute periods either of air alone or of peppermint aroma during stage two sleep. The results revealed conclusively that humans do react behaviourally, autonomically and centrally to the aroma of essential oil of peppermint administered while sleeping. Significant differences were found in responsiveness to periods with and without aroma for EEG, EMG and heart rate as well as behavioural changes (Badia et al. 1990).
• Awareness: Odour conditioning and physiological responses can occur even when people are not consciously aware of the odour (Lorig 1989, Lorig et al. 1988). Kirk-Smith and Booth (1990) used a fragrance at such a low level as to be imperceptible to the subjects, and found specific mood changes in both men and women compared to a non-odorous situation. In another study, half the subjects were exposed to a fragrance and the other half to no fragrance while working on stressful tasks. Days later all were exposed to the fragrance previously used, and those women previously exposed to the fragrance reported more anxiety, even though they were not consciously aware of an aroma on either day (Kirk-Smith et al. 1983). Degel and Köster (1999) revealed that unnoticed aromas can have an effect, showing that in certain circumstances odorants may influence attention performance in people who are not aware of their presence. A later investigation found that the unnoticed presence of odorants may affect everyday behaviour and cognitive functions (Holland et al. 2005).
From the results obtained in the above-mentioned tests, everything points to the fact that inhaled fragrances do have effects on humans even if:
• the aroma is at an imperceptible level and not noticeable
• the subject is anosmic or not
Thus everyone, anosmic or not, conscious of the aroma or not, awake or not, is likely to benefit from aromatherapeutic treatment. See also Box 7.1 Smell adaptation.
It is a common assumption that the sense of smell is affected by adaptation as a result of continued exposure to a stimulus. An example of smell adaptation is that on entering a room there may be a noticeable aroma, but which is no longer apparent shortly afterwards. Presumably the aroma quickly disappears because receptors fatigue in the continuing presence of odorous molecules in the mucus (Engen 1982). The question arises whether, in these circumstances, aromas can bring about changes in the client. Engen goes on to say that, although olfactory adaptation is apparently commonly experienced, its effect has been exaggerated. He points out that animals using olfactory cues to find a mate would be frustrated if the cue should disappear halfway there.
A study investigating whether or not people with a professional interest in smell exhibited higher olfactory sensitivity showed that people working in an odorous environment showed no inferiority in terms of smelling ability. Working in an odorous environment for a full day had no major effect on general olfactory abilities, as indicated by measures performed at the beginning and end of a working day. Results do not support the idea that odorous environments are deleterious to general olfactory function (Hummel, Guel & Delank 2004).
Broad experience in the field of aromatherapy massage says that the aromas are indeed effective throughout the treatment, even though the quality of perception at the end of the treatment may well be different from that at the beginning.
Trials
When aromas are used therapeutically in clinical contexts they may be working in different ways at the same time. For example, lavender oil may:
• act pharmacologically as a light sedative
• be alerting, simply by being there as a stimulus
• create positive feelings because it is pleasant
• aid recall of past personal situations, positive or negative
• have social connotations of health or cleanliness (Kirk-Smith 1995).
The placebo effect must be taken into account when conducting trials using aromas, because the memory, attitude and expectations of the subject may modify the outcome, in addition to any effects of the aroma employed.
The use of olfaction in aromatherapy will increase and it is imperative that aromatherapy is put on a surer footing than at present; this can be achieved by the thousands of therapists currently in practice, who should not be deterred from embarking on clinical trials. With a little expert help in setting up a simple trial, much useful information could be gained in a relatively short time. Kirk-Smith (1995), in his review of therapeutic processes involving olfaction, agrees that further clinical evaluation of olfaction in therapy is needed, but trials involve many skills (therapeutic and scientific) and expectations or perceptions about the odour, as well as pleasantness, must be taken into account when predicting effects. It is not a simple matter to ascribe any reported benefits from the use of an aroma directly to that aroma. As mentioned above, it is imperative that the aromatic materials used in any future trials be precisely identified, otherwise the value of the tests will be diminished or negated.
Olfaction
Changes in thinking about odour reception have occurred following the identification of a very large family of genes responsible for coding olfactory receptors (Buck & Axel 1991).
People may have a sensitive sense of smell yet have poor perception and have difficulty in describing a smell; this is because olfactory input is widely distributed in the amygdala and the phylogenetically primitive cortex, without direct projections to the neocortex (Klemm et al. 1992).
The nose has two distinct functions:
An average human breathes in about 8 L of air each minute and more than a million molecules are taken in with each breath, yet even a remarkably small number of odorous molecules mixed in the air intake can be detected by humans (Engen 1987).
Inhalation
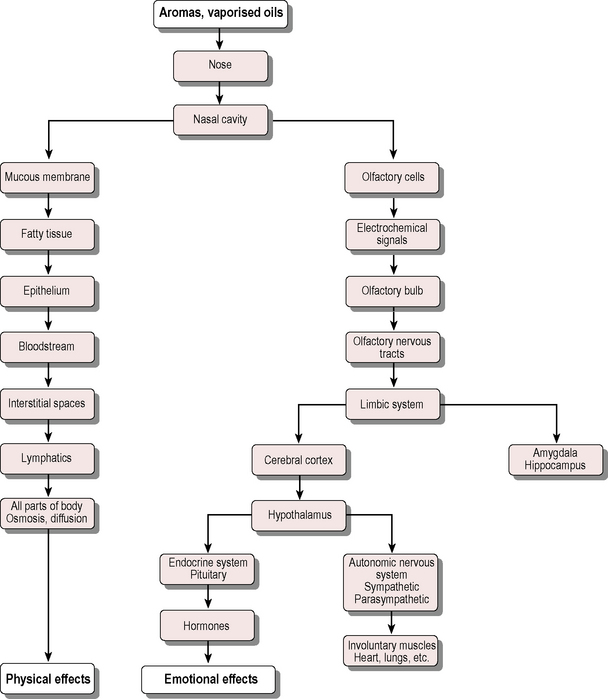
When essential oils are inhaled, the volatile molecules are carried by eddy currents to the roof of the nose, where delicate cilia protrude from the receptor cells into the nose itself. When the molecules lock on to these ‘hairs’ an electrochemical message is transmitted via the olfactory bulb and olfactory tract to the limbic system (amygdala and hippocampus). This may trigger memory and emotional responses, which can cause messages to be sent via the hypothalamus to other parts of the brain and the rest of the body (Fig. 7.1). Mainland and Sobel (2006) say that sniffing is necessary for olfactory perception and that a typical human sniff has a duration of 1.6 seconds, an average inhalation velocity of 27 L/min and a volume of 500 cm3. Sniffs are not merely a stimulus but are rather a central component of the olfactory perception, they also
• affect odour intensity perception and identity perception
• drive activity in the olfactory cortex
• are rapidly modulated by an olfactomotor system
• are sufficient to generate an olfactory perception even in the absence of an odour.
Humans recognize fewer molecules than other mammals, but can discriminate among 10,000 different odours (Menini et al 2004). The received messages are converted into action, resulting in the release of euphoric, relaxing, sedative or stimulating neurochemicals.
The limbic system, which developed 70 million years ago and used to be called the rhinencephalon (from the Greek rhis = nose, enkephalon = brain), is heavily implicated in the expression of emotion, although whether it generates emotions or merely integrates them is not clear (Stoddart 1990). The body can replace olfactory nerve cells, an unusual feature of human nerve tissue, which serves to emphasize their importance.
Fibres from the olfactory nerve carry impulses to two small but significant parts of the brain, the locus ceruleus (where noradrenaline (norepinephrine) is concentrated) and the raphe nucleus (serotonin) (Godfrey-Hardinge 1993 personal communication). It is suggested that sedative aromas such as Origanum majorana [sweet marjoram], Lavandula angustifolia [lavender], Chamaemelum nobile [Roman chamomile], Matricaria recutita [German chamomile] and Citrus aurantium (flos) [neroli] cause stimulation of the raphe nucleus, which then releases the neurochemical serotonin, whereas stimulating aromas such as Rosmarinus officinalis [rosemary], Citrus limon (per.) [lemon], Ocimum basilicum [basil] and Mentha x piperita [peppermint] will affect the locus ceruleus, which then releases noradrenaline.
The use of essential oil aromas in aromatherapy treatments is not too far removed from intranasal drug delivery in common use today, e.g. steroid inhalers for allergies, peptides and anaesthetics (Chen, Su & Chang 1989). Lavender, which has been used in the treatment of insomnia (Hardy, Kirk-Smith & Stretch 1995), consists largely of oxygenated terpenes, which interact with cell membranes to suppress cell action potentials (Teuscher et al. 1990) and might account for a sedative effect. Animal tests using 42 essential oils and their components showed linalyl acetate and linalool from lavender oil to have the most sedative consequences (Buchbauer et al. 1993): a serum level in line with intravenous injection was produced, possibly owing to ready absorption by nasal and lung mucosa (Buchbauer et al. 1991). The use of an essential oil for such a purpose has advantages, as lavender oil
• does not have unwanted side effects
• can be used to vary long-term treatment, giving relief from powerful drugs and their side effects
Warren et al. (1987) patented the use of a stress-reducing fragrance which included nutmeg oil. Subjects were stressed, and with nutmeg oil present systolic blood pressure was reduced and subjects rated themselves as being calmer and less anxious. Nutmeg oil contains the phenolic ethers myristicin and elemicin, which convert to the hallucinogens TMA (trimethoxyamphetamine) and MMDA (methoxymethylene-dioxyamphetamine).
In their paper on the use of fragrances and essential oils as medicaments, Buchbauer and Jirovetz (1994) drew the conclusion that interaction between fragrance molecules and receptors in the central nervous system (in combination with reflectoric effects) is responsible for the sedation caused by the inhalation of fragrances or essential oils.
Many odorants stimulate not only the olfactory system via the first cranial nerve but also the trigeminal system via the fifth cranial nerve, which enervates the nasal mucosa. The trigeminal system is part of the body’s somatosensory system and mediates sensations such as itching, burning or warmth and cooling: potent trigeminal stimulants such as ammonia and menthol have been used as smelling salts to arouse those who have fainted (Heuberger 2010).
Aromas affect emotions
Aromas are important in everyday life, though notoriously difficult to describe. We are surrounded by aromas, some natural but many synthetic. There are many natural aromatic messages, e.g. babies are able to recognize their own mother by her individual odour; also, synchronous menstruation occurs in groups of women living in close proximity, e.g. nuns.
Fragrances are added to almost everything from floor polishes to foods in order to
• manipulate the working environment, or in shops and hotels
• invoke a ‘feel-good’ factor in customers in shops or hotels
• reduce apprehension in airports and dentists’ waiting rooms
These aromas are inflicted on us regardless of our wishes and feelings – like background music – and the short- and long-term effects on people are not always known, since the emotions produced can be strong and unforgettable. The psychosomatic effect of smell is experienced by most people: for example the unfamiliar mixture of odours encountered in hospitals can produce a feeling of dread, accompanied by physical manifestations such as sweating, nausea and fainting (in visitors as well as patients), and the memory of the smell of some school meals can affect the appetite throughout life.
Essential oils consist of natural molecules and at the very least are to be welcomed as a means of introducing a natural product into the synthetic hospital environment. The use of carefully selected essential oils makes good sense both therapeutically and financially, for they are simple and inexpensive to use and no costly equipment is required. (see Table 7.2)
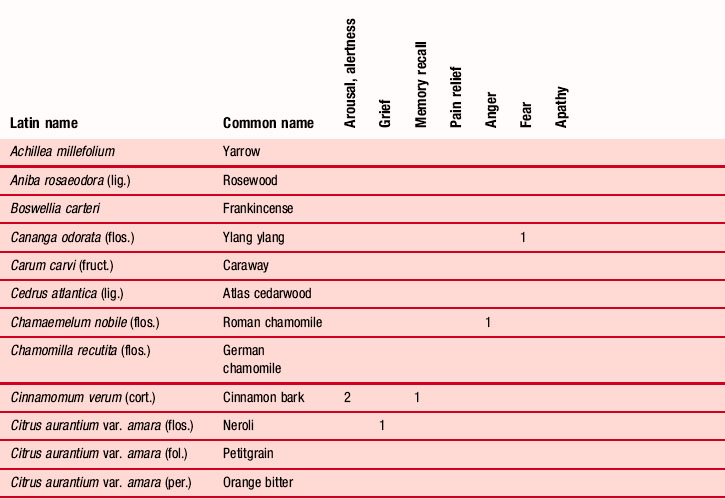
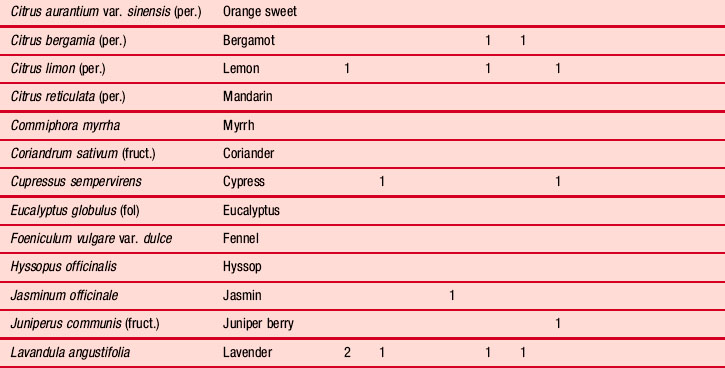
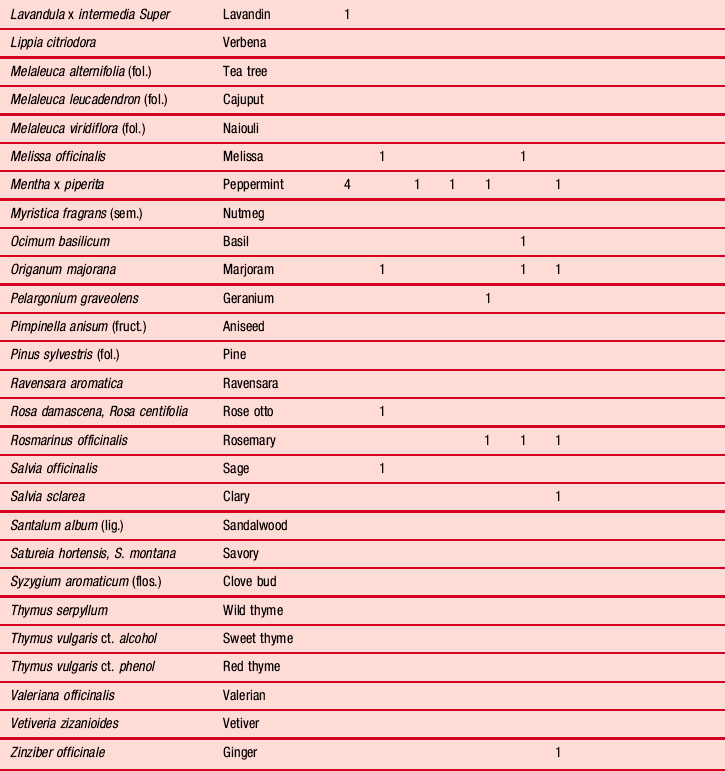
Table 7.2 Effects on the emotions mentioned by various authors. The figures indicate the number of times each is mentioned
The emotional and content qualities of autobiographical memories evoked by three memory-cue items (campfire, fresh-cut grass and popcorn) were presented in an olfactory, visual and auditory form by Herz (2004). The results showed that memories recalled by odours showed significantly more emotional and evocative content than those recalled by the visual or auditory forms. Herz argued that the data presented in his paper contributed to the growing body of evidence indicating a privileged relationship between olfaction and emotion during recollection.
Conditioning, pairing
Classic conditioning using a visual or an auditory stimulus requires many pairings, but in the case of olfaction sometimes only one pairing is needed, e.g. conditioning the body’s production of natural killer (NK) cells, fever and cytotoxic T-lymphocytes (CTL) to camphor (see below). The connection between the olfactory and immune systems is important for species survival (Hiramoto et al. 1993). Taste and odour pair easily with illness, which is useful in some cases, but an odour may become associated with an unwanted state or an illness. Aversive conditioning using an odour has been used to control overeating and resulted in a significant loss of weight compared with a control group (Foreyt & Kennedy 1971).
• Schiffman and Siebert (1991) found that an apricot fragrance paired with a relaxed state later triggered the relaxed state; this conditioning was particularly useful in the treatment of lower back pain.
• Betts (1994) used olfaction to control arousal symptoms in epileptic seizures, not only in those who experience olfactory auras but in any patient having an aura long enough to give time to apply a countermeasure before the major seizure starts. Essential oils employed included lavender, chamomile, ylang ylang and lemongrass; rosemary oil was avoided (see observations under Rosemary inAppendix A on the CD-ROM). Betts says that using the autohypnotic technique it is possible to train the patient to associate intense relaxation with the smell of the oil, so that the remembered aroma alone is sufficient to act as a countermeasure.
• Olness and Ader (1992) paired taste and aroma with an anticancer drug in the treatment of an 11-year-old girl who had a severe autoimmune disease. As a result of this pairing, the anticancer drug was needed in only six out of 12 treatments.
A neutral odour can be paired with an emotional state in a single session, so that it will evoke the same emotional state in different circumstances later. This effect is quite strong and it is not even necessary for the aroma to be perceived either during the pairing or when evoking the state; this is likely to be due to olfaction’s relative lack of representation in the neocortex (Kirk-Smith, Van Toller & Dodd 1983). King (1988) has similarly paired a ‘sea fragrance’ with relaxation training, measuring the effects of fragrance alone with forehead EMG (electromyography). Rose and Behm (1994) found that inhalation of the vapour from an extract of black pepper served to reduce the withdrawal symptoms experienced on cessation of tobacco smoking; essential oils containing citral are also said to have this effect.
Sedative/stimulant influence of odours
It has long been known that aromas have an effect on the psyche; incense was used first as a calming agent to induce a state of contentment (Lee & Lee 1992) and there are many examples: in ancient Greece, the physician Galen recommended the use of aromatic herbs against hysterical convulsions; burning bay leaves were inhaled by the Oracle at Delphi to induce a trance-like state to enable communication with the gods. Later, aromatic woods were burned to drive out ‘evil spirits’.
Almost a century ago a series of experiments on rats provided confirmation of the anecdotal sedative effects of some oils: when relaxing oils were dispersed in the air the rats took longer to perform tasks (Macht & Ting 1921): oils used included lavender, rose and valerian (common names only given). This method is effective because of the large area in the lungs available for the absorption of airborne oils into the bloodstream (Jirovetz et al. 1992).
Gatti and Cayola looked at the action of essences on the nervous system (1923a), the therapeutic effects of essential oils (1923b) and the use of valerian oil as a cure for nervous complaints (1929). They noted that the physical effects of the sedative/stimulant action of the oils were achieved more quickly by inhalation than by ingestion, and that opposite reactions could be obtained depending on whether the dose was small or large.
Since these early days more experiments have been carried out and knowledge of the psychotherapeutic effects of essential oils has grown, but nevertheless more research is needed; aromatherapy works, but it is necessary to find out how. Some interesting studies illustrating calming, stimulating and other effects are given below.
Many patients undergoing magnetic resonance imaging (MRI) body scans find them distressing and claustrophobic; this expensive procedure can be aborted by a stressed patient pressing the panic button, wasting both time and money. At the Memorial Sloan-Kettering Hospital in New York, a fragrance (constituents unknown) is used to calm patients receiving whole-body scans. Redd et al. (1994) administered bursts of heliotropine (a vanilla-like scent) to patients undergoing this procedure which reduced recalled anxiety by 63% in those who liked the smell. The calming brought about was thought to be attributable to the pleasing effect of the aroma, as pleasant conditions make stress more bearable.
According to Dember and Warm (New Scientist 1991), people do much better in a task that requires sustained attention if they receive regular puffs of an aroma. The test of concentration involved staring for 40 minutes at a pattern on a computer screen and hitting a key whenever the pattern changed very slightly. People generally did well to begin with, but performance eventually fell off and the fragrance effect was likened to a mild dose of caffeine. Peppermint was found to be stimulating and lily of the valley relaxing.
A traditional use of peppermint oil in aromatherapy was confirmed by Parasuraman (1991) when it was shown that peppermint aroma enhanced the sensory pathway for visual detection, allowing more control over attention; also rosemary (39% 1,8-cineole) was shown to be refreshing and to improve locomotor activity in mice (Buchbauer 1988).
The aroma of jasmine has been shown to stimulate mental function (Sugano 1989) and to shorten pentobarbital-induced sleeping time in mice (Kikuchi et al. 1989); cis- and trans-phytol were considered the stimulant-like compounds in a solvent-extracted oil. The sedative influence of lavender and the excitatory effect of jasmine in humans were confirmed by (Karamat et al. 1992). Sugano (1989) also showed that inhalation of lavender and the compound α-pinene had a sedative effect.
Aromas, memory and mood
Aromas can be employed easily and safely by using diffusers in rooms and cars, placing on tissues etc., and used in these simple ways they can improve sleep quality, change mood positively, alleviate stress and improve alertness. Aromas are able to remind people of past experiences, even from childhood, and when experienced during a learning process can aid recall of the information – this is sometimes known as ‘context-dependent learning’. Much of this has been known anecdotally for some time, but there are now numerous studies showing that aromas do affect human conditions. In 1989, Rottman found that the aroma of jasmine in a room improved performance in problem-solving tests, and Schab (1990) found that the presence of an ambient aroma during a learning process brought about 50% better recall than when no aroma was present; Smith, Standing and Deman (1992) had a similar result. The effects of Rosmarinus officinalis [rosemary] and Lavandula angustifolia [lavender] were tested on 140 subjects divided into three groups, one being a control group. Either the lavender or the rosemary was diffused into a test cubicle prior to the test:
• Lavender produced a significant decrease in working memory and impaired reaction times for both memory- and attention-based tasks
• Rosemary significantly enhanced the quality of memory and alertness compared to the lavender and control groups.
The effects of aromatherapy on relaxation, alertness, mood, anxiety and EEG (electroencephalogram) were investigated in 40 subjects using lavender (unspecified) or rosemary (unspecified) essential oil diluted 10% in grapeseed oil and inhaled from a cotton swab. The rosemary group had increased alertness (decreased frontal α and β power) and were faster but not more accurate in mathematical computations. The lavender group performed the mathematics more quickly and more accurately, and the EEG recordings showed a stronger β power, suggesting increased drowsiness; both groups felt more relaxed, and it was concluded that aromas do affect psychological and physiological states (Diego et al. 1998).
Skamoto et al. (2005) investigated the effect of exposure to lavender aroma during rest periods at work. The workers carrying out a computer task requiring concentration (60 minutes’ work interspersed with 30 minutes’ rest) were divided into three groups:
The afternoon sessions when concentration was lowest showed a positive effect for lavender over the control and jasmine groups. This finding is interesting because although lavender is usually thought of as having a sedative effect (perhaps the lavender allowed for a more efficient rest period), it is known that it is amphoteric and can also have an arousing effect.
Moss et al. (2003) concluded that the aroma of essential oils produced objective effects on cognitive performance and subjective effects on mood: Zoladz and Raudenbush (2005) showed that cinnamon and peppermint aromas improved subjects’ ability to pay attention, their recognition and working memory, visuomotor response speed, mood and energy. In a study to assess whether peppermint could increase the alertness of clerical workers in an office environment, typing accuracy, speed, increased performance and ability to alphabetize improved significantly (Barker et al. 2003).
Another study showed that aromas can influence the way people think and behave (Baron 1990). Subjects were put in a room that was intermittently fragranced with air freshener; under these conditions they set themselves higher goals, were more inclined to negotiate in a friendly manner and were able to resolve conflicts more successfully.
A study was carried out by Raudenbush, Corley and Eppich (2001) to determine whether physical tasks would be enhanced by the inhalation of peppermint aroma; athletes performed four tasks:
Participants performed the protocol twice under different odour conditions, first with a peppermint-odorized adhesive strip under the nose, and second with an odourless adhesive strip. The peppermint aroma resulted in increases in running speed, hand grip strength and number of push-ups, but had no effect on the skill-related basketball free-throw shots.
In a different study athletes performed a 15-minute treadmill stress test and at 3-minute intervals 50 mL of beverage (water with peppermint aroma added, unadulterated water, or a commercial sports drink) were consumed: in the control condition no beverage was consumed. Both the peppermint drink and the sports drink led to greater ratings of personal performance and increased mood (Schuler, Rawson & Raudenbush 2004).
Matricaria recutita [German chamomile] oil has been used to study the effects of olfaction on mood and imaging. When subjects were asked to visualize positive or negative phrases following exposure to either chamomile oil vapour or placebo, the oil significantly increased the time it took for images to be produced, suggesting either that enhanced neural processing was taking place or that the oil was sedative; it also shifted mood rating in a positive direction (Roberts & Williams 1992).
Psychophysiological effect of aroma
There can be no doubt that changes in physiological and psychological parameters can be caused by essential oil inhalation, and Miyazaki et al. (1991) reported that changes in mood due to inhalation could be measured using the light reflex of the pupil; they also found that orange oil (unspecified) increased the activity of the parasympathetic nervous system. Using encephalography (EEG) and psychological scoring to examine the effects of inhalation of various oils, it was found that bitter orange oil increased sleeping time significantly under conditions of mental stress. In psychophysiological studies of fragrance by Sugano and Sato (1991) it was concluded that lavender, orange and rose would elevate work efficiency and counter the effects of a stressful life; chamomile, jasmine and musk increased β-band microvibrations, suggesting mental stimulation.
These studies demonstrated that psychological and physiological parameters can be changed by the inhalation of essential oils, but the oils used in most of the tests cited in this section were not properly identified. Lavender was found to be unpleasant in some tests (Klemm et al. 1992, Lorig & Roberts 1990) but pleasant in others (Torii et al. 1988); there are similar findings with jasmine. It is hard to imagine that Lavandula angustifolia could consistently be rated as unpleasant, whereas it is entirely possible that L. latifolia or L. stoechas (among others) could merit this description: the ester content of lavenders grown in different regions can vary from 8% to 50%, altering the aroma considerably; jasmine oil is not distilled and contains traces of chemical solvent. It is astonishing that time and money can be spent in research without ascertaining what materials are being tested and studied, but this has happened, which tends to detract from the value of the whole exercise.
Klemm et al. (1992) studied the physiological responses of 16 young women to aromas from seven essential oils (birch tar, galbanum, heliotropine, jasmine, lavender, lemon and peppermint) assessed by EEG recordings from 19 locations on their scalps. Subjective responses to the odours differed, but the most consistently arousing and strong odours included galbanum, lavender, lemon and peppermint. The most pleasant were lemon and peppermint, whereas birch tar, galbanum and lavender were consistently unpleasant. All aromas affected the EEG in at least some subjects, and all subjects responded to some.
It is not clear from studies carried out whether or not personal like or dislike of the odour has a real bearing on the effects of essential oil inhalation. Bulgarian rose, lavender and geranium oils were tested on 48 medical students by spraying a 1% solution into the room; there was an increase in concentration, attention span, work rhythm and a shortening of reflex times; these effects were independent of personal like/dislike of the aroma (Tasev, Toleva & Balabanova 1969). On the other hand, the study by Marchand and Arsenault (2002) came to the conclusion that if the aroma was found to be pleasant then mood perception was significantly increased, whereas unpleasant aromas significantly reduced mood perception. Practical experience shows that essential oils work in an aromatherapy treatment even if the aroma is not liked, although the client tends to be more relaxed and more ready to accept treatment with a positive outlook if the aroma is perceived as pleasant.
Summary
Great advances have been made in our knowledge of the interactions of the mind, emotions and nervous and immune systems, and there is growing recognition of their combined impact on general health. Essential oils have an effect on everyone and have an important role to play in bringing about a state of relaxation, thereby favouring healing – aromas are effective even during sleep or unawareness of their presence. Everyone is capable of deriving benefit from aromatherapy.
Badia P., Wesensten N., Lammers W., Culpepper J., Harsh J. Responsiveness to olfactory stimuli presented in sleep. Physiol. Behav.. 1990;48(1):87-90.
Barker S., Grayhem P., Koon J., Perkins J., Whalen A., Raudenbush B. Improved performance on clerical tasks associated with administration of peppermint odor. Percept. Mot. Skills. 2003;97:1007-1010.
Baron R.A. Environmentally induced positive affect: its impact on self efficacy, task performance, negotiation and conflict. Journal of Applied Social Psychology. 1990;20:368-384.
Benson H. The relaxation response. New York: Morrow; 1975.
Betts T. Sniffing the breeze. Aromatherapy Quarterly. 1994;40(Spring):19-22.
Borysenko J. Mending the mind, mending the body. Toronto: Bantam; 1988.
Buchbauer G. Aromatherapy: do essential oils have therapeutic properties?. Proceedings of the Beijing International Conference on Essential Oils, Flavours, Fragrances and Cosmetics. London: International Federation of Essential Oils and Aroma Trades; 1988.
Buchbauer G., Jirovetz L. Aromatherapy – use of fragrances and essential oils as medicaments. Flavour & Fragrance Journal. 1994;9:217-222.
Buchbauer G., Jirovetz L., Jäger W., Dietrich H., Plank C., Karamat E. Aromatherapy: evidence for sedative effects of the essential oil of lavender after inhalation. Z. Naturforsch.. 1991;46c:1067-1072.
Buchbauer G., Jirovetz L., Jäger W., Plank C., Dietrich H. Fragrance compounds and essential oils with sedative effects upon inhalation. J. Pharm. Sci.. 1993;82(6):660-664.
Buck L., Axel R. A novel multigene family may encode odorant receptors: a molecular basis for odour recognition. Cell. 1991;65:175-187.
Cameron E.L. Measures of human olfactory perception during pregnancy. Chem. Senses. 2007;32:775-782.
Chaitow L. Mind your immunity. Here’s Health. 1991(October):19-20.
Chen D., Dalton P. The effect of emotion and personality on olfactory perception. Chem. Senses. 2005;30:345-351.
Chen Y.W., Su K.S.E., Chang S. Nasal systemic drug delivery. New York: Dekker; 1989.
Chu S. Olfactory conditioning of positive performance in humans. Chem. Senses. 2008;33:65-71.
Cook N. Aromatherapy: reviewing evidence for its mechanisms of action and CNS effects. Br. J. Neurosci. Nurs.. 2008;4(12):595-601.
Degel J., Köster E.P. Odors: implicit memory and performance effects. Chem. Senses. 1999;24(3):317-325.
Diego M.A., Jones N.A., Field T., et al. Aromatherapy positively affects mood, EEG patterns of alertness and math computations. Int. J. Neurosci.. 1998;96(3–4):217-224.
Doty R.L. Olfactory system. In: Gerchell T.V., et al, editors. Smell and taste in health and disease. New York: Raven Press; 1991:175-203.
Dunbar H.F. Emotions and bodily changes, fourth ed. New York: Columbia University Press; 1954.
Eisberg S. Male chauvinism in toxicity testing? Manufacturing Chemist. 1983;3(July):3.
Engen T. The perception of odours. New York: Academic Press; 1982.
Engen T. Remembering odours and their names. Am. Sci.. 1987;75:497-502.
Foreyt J.P., Kennedy W.A. Treatment of overweight by aversion therapy. Behav. Res. Ther.. 1971;9:29-34.
Fuji M., et al. Olfactory acuity after total laryngectomy. Chem. Senses. 2002;27:117-121.
Gatti G., Cayola R. L’azione delle essenze sul sistema nervoso. Rivista Italiana delle Essenze e Profumi. 1923;5(12):133-135.
Gatti G., Cayola R. Azione terapeutica degli olii essenziali. Rivista Italiana delle Essenze e Profumi. 1923;5:30-33.
Gatti G., Cayola R. L’essenza di valeriana nella cura delle malattie nervose. Rivista Italiana delle Essenze e Profumi. 1929;2:260-262.
Guarneros M., et al. Mexico City air pollution adversely affects olfactory function and intranasal trigeminal sensitivity. Chem. Senses. 2009;34:819-826.
Hardy M., Kirk–Smith M., Stretch D. Replacement of chronic drug treatment of insomnia in psychogeriatric patients by ambient odour. Lancet. 1995;346:701.
Herz R.S. A naturalistic analysis of autobiographical memories triggered by olfactory visual and auditory stimuli. Chem. Senses. 2004;29:217-224.
Herz R.S., Cupchik G.C. An experimental characterisation of odour evoked memories in humans. Chem. Senses. 1992;17(5):519-528.
Hesse W.R., Akerl K. Experimental data on the role of the hypothalamus in mechanisms of emotional behaviour. AMA Arch. Neurol. Psychiatry. 1955;73:127-129.
Heuberger E. Effects of essential oils on the central nervous system. In: Başer K.H.C., Buchbauer G., editors. Handbook of essential oils: science, technology and applications. Boca Raton: CRC Press; 2010:283.
Hiramoto R.N., Hsueh C.M., Rogers C.F., Demissie S., Hiramoto N.S., Soong S.J., et al. Conditioning of the allogenic cytotoxic lymphocyteresponse. Pharmacol. Biochem. Behav.. 1993;44(2):275-280.
Holland R.W., Hendriks M., Aarts H. Smells like clean spirit. Nonconscious effects of scent on cognition and behaviour. Psychol. Sci.. 2005;16(9):689-693.
Holley A. Actualité du mécanisme de l’olfaction. In: 12èmes Journées Internationales Huiles Essentielles. Milano: Istituto Tetrahedron; 1993:21-27.
Hudson R., et al. Effect of air pollution in residents of Mexico City. Chem. Senses. 2006;31:79-85.
Hummel T., Guel H., Delank W. Olfactory sensitivity of subjects working in odorous environments. Chem. Senses. 2004;29(6):533-536.
Jirovetz L., Buchbauer G., Jäger W., Woidich A., Nikiforov A. Analysis of fragrance compounds in blood samples of mice by gas chromatography, mass spectrometry, GC/FTIR and GC/AES after inhalation of sandalwood oil. Biomed. Chromatogr.. 1992;6(3):133-134.
Karamat E., Ilmberger J., Buchbauer G., Roblhuber K., Rupp C. Excitatory and sedative effects of essential oils on human reaction time performance. Chem. Senses. 1992;17:847.
Kikuchi A., Tsuchiya T., Tanida M., Uenoyama S., Nakayama Y. Stimulant like ingredients in absolute jasmine. Chem. Senses. 1989;14(2):304.
King J.R. Anxiety reduction using fragrances. In: Van Toller S., Dodd G.H., editors. Perfumery: the psychology and biology of fragrance. London: Chapman & Hall; 1988:147-165.
Kirk-Smith M.D. Possible psychological and physiological processes in aromatherapy. Aroma 95 One body-one mind conference proceedings. 1995.
Kirk-Smith M.D., Booth D.A. The effect of five odorants on mood and the judgement of others. In: MacDonald D.W., Muller-Schwarze D., Natynezuk S.E., editors. Chemical signals in vertebrates. Oxford: Oxford University Press; 1990:48-54.
Kirk-Smith M.D., Van Toller C., Dodd G.H. Unconscious odour conditioning in human subjects. Biol. Psychol.. 1983;17:221-231.
Klemm W.R., Lutes S.D., Hendrix D.V., Warrenburg S. Topographical EEG maps of human responses to odors. Chem. Senses. 1992;17(3):347-361.
Kliauga M., Hubert K., Cenci T. Consumer panel study on the effect of peppermint and lavender fragrances on proof reading efficiency. In: Gilbert A., editor. Compendium of olfactory research. Dubuque IA: Kendall/Hunt; 1996:131-135.
Knasko S.C. Ambient odour: effects on human behaviour. Int. J. Aromather.. 1997;8(3):32.
Lee W.H., Lee L. The book of practical aromatherapy. New Canaan CT: Keats; 1992:125.
Lehrner J., Eckersberger C., Walla P., Potsch G., Deecke L. Ambient odour of orange in a dental office reduces anxiety and improves mood in female patients. Physiol. Behav.. 2000;71:83-86.
Lorig T.S. Human EEG and odour response. Prog. Neurobiol.. 1989;33:387-398.
Lorig T.S., Roberts M. Odour and cognitive alteration of the contingent negative variation. Chem. Senses. 1990;15:537-545.
Macht D.I., Ting G.C. Experimental inquiry into the sedative properties of some aromatic drugs and fumes. J. Pharmacol. Exp. Ther.. 1921;18:361-372.
Mainland J., Sobel N. The sniff is part of the olfactory perception. Chem. Senses. 2006;31:181-196.
Marchand S., Arsenault P. Odours modulate pain perception: a gender specific effect. Physiol. Behav.. 2002;76:251-256.
Menini A., Lagostena L., Boccaccio A. Olfaction: from odorant molecules to the olfactory cortex. News Physiol. Sci.. 2004;19(3):101-104.
Miyazaki Y., Motohashi Y., Kobashaya S. Changes in mood by inhalation of essential oils in humans I. Mokuzai Gakkaishi. 1992;38(10):903-908.
Miyazaki Y., Motohashi Y., Kobashaya S. Changes in mood by inhalation of essential oils in humans II. Mokuzai Gakkaishi. 1992;38(10):909-913.
Moss M., Cook J., Wesnes K., Duckett P. Aromas of rosemary and lavender essential oils differentially affect cognition and mood in healthy adults. Int. J. Neurosci.. 2003;113(1):15-38.
Nasel B., Nasel C.h., Samec P., Schindler E., Buchbauer G. Functional imaging of effects of fragrances on the human brain after prolonged inhalation. Chem. Senses. 1994;19(4):359-364.
Nezlak J.B., Shean G.D. Social interaction and personal fragrance use. Perfumer & Flavorist. 1990;15:43-45.
New Scientist. On the scent of a better day at work. 1991:18. 2 March
Nordin S., et al. A longitudinal descriptive study of self-reported abnormal smell and taste perception in pregnant women. Chem. Senses. 2004;29:391-402.
Olness K., Ader R. Conditioning as an adjunct in the pharmacotherapy of Lupus erythematosus: a case report. J. Dev. Behav. Pediatr.. 1992;13:124-125.
Ouldred E., Bryant C. Dementia Care Pt 2: understanding and managing behavioural challenges. Br. J. Nurs.. 2008;17(4):242-247.
Parasuraman R. Effects of fragrances on behaviour, mood and physiology. 1991. Paper presented at the annual meeting of the American Association for the Advancement of Science, Washington DC
Plato, 3rd century BC. The Republic (D. Lee, Trans.). Penguin, Harmondsworth.
Price S. Aromatherapy and your emotions. London: Thorsons; 2000.
Raudenbush B., Corley N., Eppich W. Enhancing athletic performance through the administration of peppermint odour. Journal of Sport and Exercise Psychology. 2001;23:156-160.
Redd W.H., Manne S.L., Peters B., Jacobsen P.B., Schmidt H. Fragrance administration to reduce patient anxiety in MRI. J. Magn. Reson. Imaging. 1994;4(4):623-626.
Roberts A., Williams J.M.G. The effect of olfactory stimulation on fluency, vividness of imagery and associated mood: a preliminary study. Br. J. Med. Psychol.. 1992;65:197-199.
Rose J.E., Behm F.M. Inhalation of vapour from black pepper reduces smoking withdrawal symptoms. Drug Alcohol Depend.. 1994;34:225-229.
Rottman T.R. The effects of ambient odour on the cognitive performance, mood and activation of low and high impulsive individuals in a naturally arousing situation. 1989. Doctoral Dissertation
Sanderson H., Harrison J., Price S. Massage and aromatherapy for people with learning difficulties. Birmingham: Hands On Publications; 1991.
Schaal B., et al. Human fetuses learn odours from their pregnant mother’s diet. Chem. Senses. 2000;25:729-737.
Schab F.R. Odours and remembrance of things past. J. Exp. Psychol. Learn. Mem. Cogn.. 1990;16:648-655.
Schiffman S.S., Siebert J.M. New frontiers in fragrance use. Cosmetics and Toiletries. 1991;106(6):39-45.
Schilcher H. Ätherische Öle–Wirkungen und Nebenwirkungen. Dtsch. Apoth. Ztg.. 1984;124:1433-1443.
Schuler A., Rawson A., Raudenbush. Effects of beverage flavour on athletic performance, mood, and workload. Journal of Sport and Exercise Psychology. 26(Suppl.), 2004.
Skamoto R., Minoura K., et al. Effectiveness of aroma on work efficiency: lavender aroma during recesses prevents deterioration of work performance. Chem. Senses. 2005;30:683-691.
Smith D.G., Standing L., Deman A. Verbal memory elicited by ambient odour. Percept. Mot. Skills. 1992;74(2):339-343.
Stoddart D.M. The scented ape. Cambridge: Cambridge University Press; 1990:132.
Sugano H. Effects of odours on mental function. Chem. Senses. 1989;14(2):303.
Sugano H., Sato N. Psychophysiological studies of fragrance. Chem. Senses. 1991;16:183-184.
Tasev T., Toleva P., Balabanova V. The neuropsychic effect of Bulgarian rose, lavender and geranium. Folia. Med.. 1969;11(5):307-317.
Teuscher E., Melzig M., Villmann E., Moritz K.U. Untersuchungen zum Wirkungsmechanismus Ätherischer Öle. Zeitschrift für Phytotherapie. 1990;11:87-92.
Torii S., Fukuda H., Kanemoto H., Miyauchi R., Hamauzu Y., Kawasaki M. Contingent negative variation and the psychological effects of odour. In: Van Toller S., Dodd G.H., editors. 1988 Perfumery. The psychology and biology of fragrance. London: Chapman & Hall; 1988:107-120.
Van Toller S., Dodd G., editors, Fragrance: the psychology and biology of perfume. Barking: Elsevier; 1992:99-101.
Warren C.B., Munteanu M.A., Schwartz G.E., et al. Method of causing the reduction of physiological and/or subjective reactivity to stress in humans being subjected to stress conditions. 1987.
Wood C. Sad cells. J. Altern. Complement. Med.. 1990(October):15.
Wysocki C.J., Dorries K., Beauchamp G.K. Ability to perceive androsterone can be acquired by ostensibly anosmic people. Proc. Natl. Acad. Sci. USA. 1989;86:7976-7978.
Zoladz P.R., Raudenbush B. Cognitive enhancement through stimulation of the chemical senses. North American Journal of Psychology. 2005. March 01
Kirk-Smith M.D. Possible psychological and physiological processes in aromatherapy. In: Aroma 95 One body–one mind conference proceedings. Brighton: Aromatherapy Publications; 1995:92-103.
Schiffman S.S., Siebert J.M. New frontiers in fragrance use. Cosmetics and Toiletries. 1991;106(6):39-45.
Stevenson C.J. The psychophysiological effects of aromatherapy massage following cardiac surgery. Complement. Ther. Med.. 1994;2:27-35.