3 (Part I) Quality and safety
Introduction
The dangers of essential oils have often been exaggerated, usually based on insufficient evidence and inappropriate comparisons. This chapter shows that these powerful substances, used knowledgeably and with due caution, pose no threat to health. The highest possible quality of medicament is always required in therapy, and this chapter shows that aromatherapy is no exception to the rule. The main chemical groups found in essential oils are outlined, along with an account of methods of testing for quality.
Background
It is remarkable that the safety record of essential oils is as good as it undoubtedly is, bearing in mind that:
• essential oils are powerful mixtures and have physiological, psychological and pharmacological effects, both desirable and undesirable, when applied to the body;
• in most countries, including the UK, these oils are freely available and there is no restriction on their sale and use;
• the majority of people who buy essential oils are members of the general public, who do not have expert knowledge of their nature and use.
Despite this good record, statements are sometimes made which sensationalize aromatherapy or exaggerate unwanted effects of the oils. More to the point would be to educate both the supplier and the general user in the appropriate and safe use of essential oils. That way lies a safe and sound future for the popular use of aromatherapy.
The food industry is the greatest user of essential oils, where they are used at low levels as flavourings and when used in this way there are none that could be expected to pose any significant risk to health (Adams & Taylor 2010). Chronic studies using animals, sponsored by the National Toxicity Program, have been performed on more than 30 major components of essential oils at much higher intake levels than the daily intake dose, and the majority showed no carcinogenic potential (Smith et al. 2005). Obviously, when consumed in higher quantities some plant extracts do exhibit toxicity, e.g. hemlock (used as a poison) and pennyroyal (toxic side effects), which underlines the need for adequate training.
Essential oil quality
Genuine aromatherapeutic essential oils
For therapeutic purposes the quality and wholeness of any essential oils used are of paramount importance, irrespective of cost, whereas when used in the flavour and fragrance industries the price, taste and aroma are the most important considerations; for them, standardized essential oils are necessary to ensure repeatability and a consistent quality.
Quality variation
Variation in the quality of an essential oil may be natural or due to human intervention. Wine is a commodity which is expected to have a different taste and character from year to year, although harvested, processed and bottled at the same vineyard and from the same vines. Plants are subject to varying amounts of sunshine, frost, rain, heat or cold each year, and it is these factors, plus the composition of the soil, which are responsible for the variations in quality and composition (and therefore the aroma) of the plant extracts, occurring naturally from year to year.
Synthetic materials, adulteration
Traders in essential oils may add cheaper oils or synthetics to the genuine oils, in order to maintain the same standard taste, aroma and price level for successive repeat deliveries to the same customer. The needs of the flavour and food industries are today so great that there are scarcely enough natural products in the world to meet the demand, and even where available some products are just too expensive for their purposes compared with synthetics. The aromatherapist, however, needs above all to acquire the natural physicochemical characteristics, whatever the variation from harvest to harvest.
Essential oils are made up of a vast array of natural chemicals, most of which are found in more than one oil. It is a fairly simple matter for the chemist to remove a desired constituent from a cheap oil and add it to an expensive oil, or to sell a modified ‘pure’ oil to an unsuspecting customer for a high price. Adulteration also takes place when a synthetic isolate is added, especially to one of the costly oils such as rose otto, when synthetic phenyl ethyl alcohol (occurring naturally in rose otto) is used as the adulterant. ‘Nature identical’ products are manufactured in a laboratory and are simply synthetic copies of ingredients found in nature. Alcohol, and occasionally a small amount of vegetable oil, which are both good solvents of essential oils, are used to adulterate, stretch or cut Nature’s gifts, and many descriptive words are used to justify the standardization sometimes necessary in the fragrance and food industries. ‘Certain suppliers with highly developed imagination will even use the term “ennobling” for the disfiguration of an essential oil’ (Arctander 1960). With some oils it is almost standard practice to adulterate, e.g. the use of PEG (polyethylene glycol) to extend lavender essential oil.
Imitations
Expensive essential oils such as Melissa officinalis [melissa] and Aloysia triphylla [lemon verbena] are often imitated by the perfume industry by using blends of cheaper oils to simulate the aroma; to the perfumer, the aroma is the most important asset of an ‘essential oil’, not whether it is natural, adulterated or synthetic. Tisserand and Balacs (1995 p. 177) say that Aloysia triphylla should not be used in therapy, but this advice is based on tests carried out at 12% using fragrance quality oils (Opdyke 1992). Most oils named lemon verbena are blends of lemon, citronella, lemongrass etc., as the genuine oil is expensive; these ‘made up’ verbena oils are likely to be phototoxic and also skin sensitizers because of the high citral content in the oils from which they have been constructed. However, the genuine oil, which has a similar concentration of citral to the above oils, does not irritate the skin (Schnaubelt 1998 p.117) – a good reason for not using industrial quality essential oils therapeutically!
Deterpenized oils
Essential oils used in the fragrance industry often have their terpenes partly or wholly removed on account of their insolubility in alcohol, which would result in cloudiness – a distinct commercial and aesthetic disadvantage in a perfume! The deterpenized oil is incomplete and contains in higher proportions the remaining constituents of the oil, for example the deterpenization of peppermint increases the content of the possibly hazardous ketone menthone. In aromatherapy there is no necessity for this and it is imperative not to interfere with the natural balance of the essential oil. Some therapists purchase bergapten-free bergamot oil, as this constituent (a furanocoumarin) can be responsible for phototoxicity of the skin in sunlight, but this is unnecessary (see Ch. 3 Part II).
Contaminants
The majority of essential oils are produced for use by the food and fragrance industries which, generally speaking, are not concerned whether or not fertilizers, pesticides or herbicides may be present in the oil. Stewart (2004 p.10) says that herbicides, fungicides and pesticides are intrinsically toxic and inevitably end up as contaminants in the oils, directly affecting their efficacy and safety.
Commercial grade oils can present toxic effects as a result of adulteration, folding, stretching etc. to which they are subjected in order to have:
• a standardized product which can be repeated at any time, which is impossible with naturally grown plants;
• a product at a price compatible with their marketing strategy (often meaning cheap).
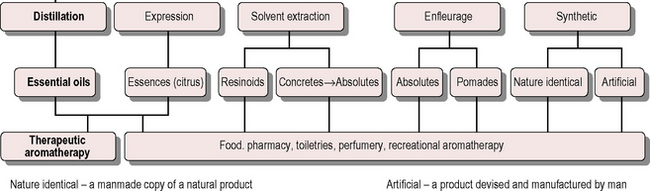
The various types of aromatic product available are shown in Figure 3.1. For therapeutic use aromatherapists use only distilled essential oils and expressed essences, although some occasionally make exception to the rule by using jasmine absolute or benzoin.
Procurement of genuine, authentic essential oils
Of the many factors involved in the safe use of therapeutic essential oils, not least is the specification of the oil itself. Knowledge of factors such as where it is grown, whether it is cloned by cuttings or grown from seed, the plant variety, how it is grown (wild, organic, or with chemicals), the part of the plant used and the chemotype is important for safe usage.
The need for the use of genuine essential oils in therapeutic treatments is illustrated perfectly by the following case cited by Valnet:
A patient being treated for a fistula of the anus by the instillation of pure and natural drops of lavender and who was beginning to recover, had to go on a journey. Having forgotten his essential oil, he purchased a further supply from a chemist. Unfortunately, this essence was neither pure nor natural; one single instillation resulted in such severe inflammation that the patient was unable to sit down for over two weeks.
The overriding consideration must be consumer safety and to this end genuine, authentic essential oils must be procured, genuine in this case meaning of known plant origin and authentic meaning not standardized: note that the word natural does not necessarily mean unadulterated or safe.
It is not easy to procure such oils, for many and varied reasons, some of which follow:
1. High quality at the time of harvesting can diminish due to distillation, rectification, fractionation, adulteration, transportation, storage and time.
2. The bulk of essential oils comes from faraway countries, only 3–5% coming from Europe.
3. Availability is influenced by various factors including war (vetiver, patchouli) and changing climate (ambrette seed).
4. The trade has very limited knowledge of scientific names and it is vital for aromatherapy to use the scientific name, because the use of local common names for the plants leads to confusion. More than one name may be given to the same plant, or the same common name can be given to different plants (such as marjoram, which might be Origanum majorana or Thymus mastichina).
Cedarwood oil may be any of the following, since all are traded simply as cedarwood: Cedrus atlantica [Atlas cedarwood], Cedrus deodora [deodar or Himalayan cedarwood], Cedrus libani [cedar of Lebanon], Chamaecyparis lawsoniana [western white cedar], Cryptomeria japonica [Japanese cedar], Juniperus procera [east African cedarwood], Juniperus mexicana [Texas cedarwood], Juniperus virginiana [red cedarwood], Thuja occidentalis [white cedar], Thuja plicata [western red cedar].
The common name oregano is applied to more than 43 different species and 18 hybrids belonging to five different families (Skoula & Harborne 2002).
5. A supply problem exists because the market for herbal medicines is increasing and more oils are being used in aromatherapy.
6. Wild plants are sometimes collected by an unsupervised, unskilled labour force paid by weight of plant collected, and who are not always able to identify the required plant, resulting in indiscriminate harvesting.
Accurate identification
The importance of knowing what material is being used in a treatment is obvious, therefore it is imperative that the oil is precisely identified. This fact escapes the attention of many people treating others, and even of some carrying out scientific trials. Before embarking on a trial using essential oils it is of primary importance that a specified oil from a known source is used, and to have as a minimum a GC (gas chromatography) analysis of the oil actually used in the test. The scientific botanical name of the plant should be used and oil from the same harvest batch should be used throughout the test(s).
In many cases it is not sufficient merely to specify the genus and species (and the variety if applicable): it is also necessary to designate the chemotype (explained in Ch. 1) and the part of the plant used for extraction. An example is the cinnamon tree, where the oil from the bark consists principally of an aldehyde, whereas the oil from the leaf is mainly a phenol, with different effects and uses. The oil from the thuja or white cedar tree, Thuja occidentalis (responsible for the restriction on cedarwood oils in France), is taken from the leaves, but other ‘cedarwoods’ are taken from the wood. In the Apiaceae family, the seed oils can be significantly different from oils extracted from other parts of the same plant, e.g. in the case of Angelica archangelica the root oil is phototoxic, whereas that from the seed is not. Therapists need to be aware of this; it is their responsibility to ensure that inappropriate treatment is not given.
Some oils that are sold do not exist, and Dürbeck (2003) calls them phantom oils); some examples are:
• Peru balsam from El Salvador and tolu balsam are both standardized or synthesized in Europe.
• Sandalwood from South India (Mysore) is not available yet continues to be sold.
• Rosewood oil from the Amazon is not available because the industry is now finished.
• The same situation exists with Copaiba balsam.
• Tea tree – there is three times more sold in the world than is produced in Australia; tea tree oil is a comparatively simple essential oil comprising only about 30 compounds (cf. ylang ylang, with about 1200) and so is easy to reconstruct; also the ‘natural’ oil is often ‘regulated’ at source.
• Sumatran Patchouli may be relabelled Malaysian Patchouli.
• Barrème lavender (a lavender high in linalyl acetate) has not been produced for many years but unbelievably still appears on some sales lists.
Pharmacopoeia
About 60 different standards exist for the chemical composition of essential oils, yet there are only 16 essential oils listed in the New European Pharmacopoeia (Dürbeck 2003). Current pharmaceutical formulae demonstrate that essential oils and oleoresins derived from spices and herbs are valued not only as flavouring agents but also for other properties they possess; for instance, they:
• stimulate the appetite by increasing salivation
• act as carminatives to relieve gastric discomfort and flatulence
• counteract the griping action of purgatives
• contribute as mild expectorants in cough mixtures and pastilles
• check profuse secretion and relieve congestion of the bronchioles when used in inhalants
• act as counterirritants and rubefacients, for the chest in bronchitis and pleurisy, and for the relief of rheumatic pain, when formulated as ointments, creams and liniments.
As flavouring agents, essential oils are acceptable for repeated dosage, e.g. in tablets to be chewed and for repeated usage in such products as toothpaste. As perfumes they are present in a variety of cosmetics which are used daily over long periods of time.
Some essential oils listed in the British Pharmacopoeia (BP) are stocked in hospital pharmacies, but oils prepared to BP standards may not be suitable for use in aromatherapy. One reason for this is that many plants, for example thyme, Thymus vulgaris, exist in the wild as many different chemotypes, each chemotype producing quite a different essential oil in makeup and therapeutic action (see Ch. 1 p. 8) and such differences are not always reflected in the pharmacopoeia. Another reason is because the specification is either too broad or incomplete and does not reflect the natural materials currently available; some oils listed are folded, which alters their composition: such essences are not used in aromatherapy.
Storage and shelf life
Factors that affect the storage of aromatherapy products are:
• Air – oxidation can be a problem and essential oils keep best when bottles are full, with as little air as possible. Oxidation – the combining of free oxygen with compounds in the essential oils – affects some oils particularly, altering their therapeutic effects, e.g.
 oils with a significant monoterpenes content can lead to the formation of sensitizing hydroperoxides (e.g. turpentine) some oils high in the terpenes limonene and pinene may react with oxygen; the antibacterial activity of lemongrass oil is diminished when oxidized (Orafidiya 1993) once a bottle is opened, air enters to replace any essential oil used, which poses no problem if used within a reasonable time. The degradation process is accelerated by the other two factors, heat and light
oils with a significant monoterpenes content can lead to the formation of sensitizing hydroperoxides (e.g. turpentine) some oils high in the terpenes limonene and pinene may react with oxygen; the antibacterial activity of lemongrass oil is diminished when oxidized (Orafidiya 1993) once a bottle is opened, air enters to replace any essential oil used, which poses no problem if used within a reasonable time. The degradation process is accelerated by the other two factors, heat and light• Temperature – heat speeds up the oxidation process and a cool temperature is best for extending the shelf life, especially for blends of essential/carrier oils and carrier oils. Sudden changes in temperature appear to be more harmful than a slow seasonal change.
• Light – essential oils should be stored in dark- coloured glass bottles – dark amber, green or black for best results. Blue glass does not protect the oil from some harmful light rays and nor does clear glass.
If products are not stored under the best conditions possible there can be a change in molecular composition and therefore there may be different therapeutic effects, perhaps adding undesired effects such as skin irritation or even sensitization.
Essential oils
Distilled oils which have not been adulterated generally have a shelf-life of many years because the small molecules of which they are composed are relatively stable. Experience shows that, with few exceptions, most essential oils have a very long shelf-life under the right conditions. One writer (Stewart 2004 p. 446) states that the shelf-life is not known but that it is measured in millennia, not months; with personal experience the author is inclined to agree with this, and it is reasonable to expect a shelf- life of several years, but there are exceptions, as indicated above. Essential oils are flammable and must be protected from naked flame; some aroma ‘burners’ are not safe in some situations.
Expressed oils
It is often recommended that expressed citrus oils be stored under refrigeration, which extends their shelf- life by up to a year if the bottle is unopened. Once opened, half a year is a reasonable life to expect, assuming conditions are not extreme. These expressed oils under cool conditions will precipitate their natural waxes; this does not affect their therapeutic value and so the oil can be used as normal; the only drawback is that the wax may clog the dropper.
Blended oils
The shelf life of a blend of essential oils in a vegetable carrier oil is not as long as that of single or blended essential oils, depending as it does on the ratio of the mix – a 5% dilution will not last as long as a 50% dilution. The fatty oils contain unstable compounds (proteins, polypeptides, amino acids) which can break down. These blends go rancid because of the fatty acids, but storage in a fridge will slow down this effect, giving a shelf life of perhaps 2 years. There is an easy test to verify the blend: if it smells rancid it is unusable; if it smells good, then it is suitable for use.
Summing up, to maintain aromatherapy products in good condition:
Safety
Tradition and experience
Centuries of experience with many essential oils worldwide have shown them to be effective and safe:
• The Egyptians proved the antiseptic powers of aromatics in the mummification process.
• Hippocrates fought the plague in Athens by using aromatic essences for fumigation.
• St Hildegard of Bingen was using lavender oil in the 12th century.
• Hungary water (a lotion scented with rosemary) began its 600-year life in the 14th century.
• By the year 1500, oils of benzoin, calamus, cedarwood, cinnamon, frankincense, myrrh, rose, rosemary, sage, spikenard and turpentine were known to and used by pharmacists.
Essential oils were first mentioned in an official pharmacopoeia around the year 1600 in Germany (Price 2000 p. 6). Borneo camphor (an alcohol) was mentioned in Schröder’s pharmacopoeia of 1689 as a ‘prodigious alexipharmic’ or antidote to poison. For other oils there is little historical evidence, and for almost all essential oils, although there is ample proof of their antiseptic powers in vitro, clinical trials are lacking. While this may be due in part to shortage of research funds, it is also attributable to the difficulty (even impossibility) of conducting blind trials with aromatic substances.
Animal testing
Although toxicological tests have been performed on humans, aromatherapists should be aware that the majority have been carried out on animals – normally rabbits for dermal toxicity and rats for oral toxicity. However:
• Animal physiology cannot be compared with that of a human being: it is not possible to extrapolate the results of animal testing to human physiology: basil and tarragon oils may contain estragole (methyl chavicol) in high amounts and this compound has been implicated by research on animals as being a strong carcinogen. The carcinogenicity is due to the metabolite 1-hydroxyestragole, but estragole presents little hazard to humans at normal food usage levels of 1 μg/kg per day (Howes, Chan & Caldwell 1990).
• Absorption is usually higher through animal skin than human skin (Hotchkiss 1994) but for the aromatic amines the reverse is true: 13% of MDA (methylenedioxy-amphetamine) permeated the skin in rats compared to 33% in human skin, while for MbOCA (methylene bis[orthochloroaniline]) the figures were 2% and 6%, respectively; for (+)- limonene the figures are 6% (rat) and 3% (human) (Hotchkiss 1994).
• Many tests were carried out using isolated components, which is not relevant to whole oils as used in aromatherapy.
• RIFM administered relatively massive overdoses to determine lethal toxicity.
Huge sums are spent on research, clinical trials and licensing for each orthodox medicine, pill or tablet which appears on the market to help alleviate suffering and disease, but despite all the care and time spent on research there are still many serious side effects. Essential oils have not been clinically tested in this way because it would cost billions, not millions, of pounds to test each oil and synergistic mix for each therapeutic effect of which it is capable. In the absence of scientific proof, orthodoxy finds it difficult to accept aromatherapy, which is still more art than science; yet in the recent past clinical tests on animals have allowed the creation of drugs that have had disastrous effects on humans, e.g. thalidomide, opren. There is room for more than one approach in the healing arena and natural ways need to be included too.
The book Essential Oil Safety (Tisserand & Balacs 1995) is not universally accepted because most of the information is based on tests carried out using perfume grade oils.
This book is not recommended for use by people who use good quality therapeutic grade oils because it does not contain any information relevant to such oils …it is a book on commercial grade oils. …If you are using cheap perfume grade oils, such as those in most retail stores, then you may need to read and heed this book (Stewart 2004 p. 21). Such commercial quality oils are used in candles, soaps, shampoos, toothpaste, fragrancers etc. and this is recreational aromatherapy, not therapeutic aromatherapy.
The book is an excellent guide in itself, although the authors themselves say that ‘this text is largely an extrapolation of toxicological reports from the Research Institute for Fragrant Materials’ (RIFM). In the absence of specific information on therapeutic oils, there is a useful body of knowledge on fragrance materials as used on the skin by the perfume industry, thanks to impressive work carried out by RIFM (established in 1966). RIFM has published over 1000 monographs on fragrance materials, almost 200 of these concerning aromatic materials derived from plants, including essential oils, absolutes and resins. The International Fragrance Association (IFRA) makes recommendations to the perfume industry for the safe use of such materials based on the published findings of RIFM, and these may be useful guides to aromatherapists when applying essential oils to the skin.
Isomers and safety
The activity of an essential oil molecule depends on its shape, and it is necessary to be aware of the existence of isomers, where one name (e.g. thujone) can apply to different molecular shapes each having different activities. Thujone is a ketone and should not to be treated lightly whenever and wherever it occurs. The thujone molecule has four possible shapes, and it is not known whether they all have the same toxic potential or whether they ought to be avoided. Tyman (1990) suggested that there are probably differences in effect between α- and β-thujone, and others have suggested that the same is true for cis- and trans-anethole isomers. The thujone in the whole essential oil of Thuja occidentalis (up to around 80%) is definitely toxic. One frequently repeated statement is that all forms of ketone are neurotoxic, but this is not so: some are neurotoxic but not all; the author has found the intelligent use of sage oil (Salvia officinalis) containing the ketone thujone to be problem free.
There is a variation of opinion on the safety of carvone isomers, viz. the (+)-carvone molecule in caraway oil and the (−)-carvone in spearmint oil. Carum carvi [caraway] is considered to be a safe oil in all respects by Tisserand and Balacs (1995 p. 204) ( despite noting it as a mucous membrane irritant), but Winter (1999 p. 113) states that both (+)-carvone and the (−)-carvone have no known toxicity. The seed oil of Anethum graveolens [dill] contains 40–60% of ketones including (+)-carvone and is considered neurotoxic by Franchomme and Pénoël (2001 p. 351). There are many anomalies to be found in aromatherapy books and training courses. In some circumstances the so called ‘toxic’ molecules are the very ones that are needed for beneficial results, such as the phenol thymol in Thymus vulgaris ct. thymol, an extremely effective antiseptic and antifungal agent (Mills 1991).
Toxicity depends not only on the nature of the main component, but also on the relationships and synergy (see below) between it and some of the smaller (perhaps as yet unidentified) constituents, which are known to lessen or nullify undesirable effects in some cases. This may illustrate why certain oils high in ketones are not considered toxic, and why a few oils considered toxic by some people do not appear to be so (see Synergism below). It should be remembered that a great deal of good has been effected by qualified aromatherapists in the UK since the 1960s, and no serious harm has so far been recorded.
Synergism
Essential oils are complex substances, and there is no simple direct relationship between the effects of any single component of an essential oil and the effects of the complete natural essential oil – essential oils are synergistic mixes.
Single oils
A whole essential oil has a natural synergistic power where the combined action of disparate individual molecules within an essential oil has a total effect greater than the sum of their individual effects. The word is derived from the Greek syn = together, ergon = work.
As discussed in Ch. 2, essential oils are complex mixtures, some containing from a few dozen to several hundreds of different molecules which act in synergy to produce their healing effect, but if the composition is altered then the natural synergy of the remaining constituents is diminished or destroyed. An isolated component generally needs much greater care in use as unwanted side effects may be produced. When that same constituent is present in the whole oil, other constituents act as ‘quenchers’ of these unwanted effects (see Quenching, below), enabling the oil to be used without harmful effect. Complete essential oils have been found in practice to be more effective than their isolated principal constituent(s) and without side effects on account of this synergistic effect (Hall 1904).
Very rarely an oil consists largely of only one component and then the effects of the oil may be closely correlated with that component, so that the effect of the oil and that of the main component are the same (wintergreen oil is almost wholly methyl salicylate, 98% or 99%). Usually, however, the essential oil consists of many components creating a synergy, and so it is not possible to ascribe the effects of the whole oil to one particular component, even a major one. Constituents present in very small amounts (e.g. furanocoumarins) are often found to be as active as, or even more active than, the principal constituent.
‘ … minor components of essential oils can modify the activity of main components, reaffirming the importance of chemically characterizing essential oils in order to understand the overall bioactivity’
Similarly, in herbal medicine research has been done on isolated chemical constituents of Echinacea in an attempt to determine the active principle within the plant. This has proved illusive, and the conclusion drawn is that the medicinal effect is most likely to be as a result of the unique interplay of the naturally occurring substances within the living plant (Raynor 1999).
The synergism of many commercial essentials oils is destroyed during the production process, e.g. rectification and fractionation, as illustrated by the case of eucalyptus. Most eucalyptus products generally found commercially have routinely been redistilled, rectified and refined, which means that some molecules have been left behind in the redistillation process following the rectification of the crude oil, e.g. the rare phenol australol (Pénoël 1993, personal communication).
Antimicrobial synergy
Tests carried out on individual components from Eucalyptus citriodora revealed that they were relatively inactive; however, a combination of the three isolated major components in the same ratio as found in the natural oil produced a fourfold increase in antimicrobial activity against Staphylococcus aureus (Low, Rawal & Griffin 1974).
Antioxidant synergy
In tests to measure the antioxidant activity of essential oils, nutmeg, pepper and thyme oils, among others, were found to be effective and to have beneficial effects on lipid metabolism (Simpson 1994). Thyme oils are known to be biologically active in the antibacterial, antifungal and antioxidant areas. Nine of the constituent components of thyme oil were shown to have antioxidant properties (linalool, thujone, camphene, thymol, carvacrol, γ-terpinene, β-caryophyllene, borneol and myrcene, listed in descending order of activity), but it was noted that antioxidant activity for the whole oil was greater than that of the most active single component linalool (Deans et al. 1993).
Enhanced synergistic effect of blends
Apart from the synergy produced by the components of a single oil, there is also an enhancement of effect when two or more whole oils are mixed together. For example, the combined bactericidal effect of several oils together is greater than the effect of any of the individual oils, which is why the authors have always recommended using a blend of two or three oils in a treatment.
Quenching
Quenching is an important aspect of synergism, and essential oils display a quenching effect whereby the potential unwanted side effects of one component are nullified by the presence of other component(s). This quenching effect is well known in the perfumery industry, where it is turned to advantage by adding quenching components to its perfumes to prevent skin irritation. This feature can also be made use of when mixing oils. The peel oils from Citrus paradisi [grapefruit] or Citrus sinensis [sweet orange], when added to Cymbopogon citratus in a 50:50 mix, successfully quench the irritant properties of the latter (Witty 1992, personal communication). Comparing two eucalyptus oils, Eucalyptus globulus [Tasmanian blue gum] and E. smithii [gully gum], each contains around 65% of 1,8-cineole (an oxide which is a skin irritant), yet the former is contraindicated for use on young children and the latter is not (Pénoël 1992/93).
Isolates
Isolates are sometimes used in pharmaceutical preparations but they are not advised for use in aromatherapy. Citral on its own is a severe skin irritant, but whole lemon oil, which contains citral, is not, thanks to the presence of (+)-limonene and its synergistic quenching effect. Although citral produces sensitization reactions in humans when applied alone, it produces no such reactions when applied as a mixture with other compounds (Opdyke 1976b).
Phenol is a well known antiseptic which used to be used in hospitals, but the phenol in Thymus vulgaris ct. thymol, although it is 20 times more effective and exhibits the mucosal irritating properties of the group far less (Mills 1991 p. 282). Schnaubelt (1998 p. 25) echoes this when he says that pure phenol is toxic, but natural plant phenols, such as thymol, ‘have additional side chains that transform them into non-toxic, effective antiseptics’.
Tests carried out with the isolates phenyl acetaldehyde, citral and cinnamic aldehyde – found in Citrus aurantium (flos) [neroli bigarade], Cymbopogon citratus, C. flexuosus [lemongrass] and Cinnamomum verum (cort.) [cinnamon bark] oils, respectively – showed them to be skin sensitizers. The whole essential oils in which the aldehydes are present (at up to 85%) were found not to provoke sensitizing reactions. It appeared that some other component(s) of the natural oil inhibited the induction or expression of sensitization (Opdyke 1976b). To test this, several terpenes and alcohols found along with the particular aldehyde in the natural composition were combined with each of the aldehydes in question. It appears to be a consistent finding that each of these aldehydes, although producing sensitization reactions when applied alone, produces no sensitization reactions in selected simple mixtures with other compounds (Opdyke 1979) (Table 3.1). The irritant quality of oils with a high citral content (even 70%) can be quenched by adding an oil containing an equal amount of (+)-limonene, a terpene present in some citrus oils to around 80–90%.
Table 3.1 Results of quenching tests on mixtures of cinnamic aldehyde with other essential oil components
| Second test material | Relative proportions* | Results of sensitization test |
|---|---|---|
| Dipropylene glycol | 1: 1 | + |
| Phenylethyl alcohol | 1: 1 | + |
| Eugenol | 1: 1 | – |
| Eugenol | 1: 1† | – |
| Eugenol | 2.5: 1† | + |
| Cinnamic alcohol | 1: 1 | + |
| Benzyl salicylate | 1: 1 | + |
| (+)-limonene | 1: 1 | – |
* Ratio (w/w) of cinnamic aldehyde to second test material. Each mixture was tested at an overall concentration of 6% in petrolatum by the maximization procedure (Kligman 1966, Kligman & Epstein 1975).
Reprinted from Opdyke 1979 p. 255, with kind permission from Elsevier Ltd.
These findings point to the difference between using a single compound and the use of a natural synergistic mix with inbuilt quenching action. The above-mentioned tests contrast with two earlier tests carried out by Kligman in 1971 and 1972 on 25 volunteers using cinnamon bark oil at 8% concentration and producing 18 and 20 sensitization reactions, respectively (Kligman & Epstein 1975). Cinnamal is not the only component in C. verum (cort.) [cinnamon bark] oil that acts as a sensitizer, so perhaps this may be a case of synergy enhancing the unwanted effect. IFRA recommend that this oil is used at a maximum 1% concentration in a fragrance compound (IFRA 1992), equivalent to 0.2% in an aromatherapy massage oil (i.e. one drop in 25 mL carrier oil), although a lower level of use of 0.1% for the skin has been recommended (Tisserand & Balacs 1995 p. 130).
Interaction takes place between the constituents within a single oil and also between two or more essential oils, hence potentially toxic elements may be altered, enhanced or counteracted by other constituents present.
Safe quantities
Essential oils may be applied to the body in a variety of ways, and these are discussed in Ch. 6, but usually their use involves inhalation, application to the skin or ingestion. Essential oils are powerful, otherwise they would be of no use therapeutically, and inappropriate use in whatever way can bring about undesired effects. Dosage, in terms of both quantity and duration, is all important, as too little may mean little or no result, and too much may either have a beneficial effect or create a serious problem. The majority of essential oils may be considered less toxic than the over-the-counter medicines aspirin and paracetamol. Aromatherapy is safe and there need be no hesitation in introducing these natural aromatic products into a hospital environment. Many substances in common use are toxic in overdose, e.g. carrots are beneficial in moderation but a surfeit will produce illness, and this is true of many everyday foods such as tomatoes, saffron or mustard. Many essential oils contain constituents which when isolated are found to be toxic, but many items normally regarded as quite safe also contain substances which, when isolated, could be shown to be toxic – e.g. tea, almonds, apples, pears, radishes, mustard, sage, hops etc. (Griggs 1977).
Valnet (1980 p. 11) cites headaches and the loss of eyebrows in workers handling vanilla, but vanilla ice-cream is eaten and enjoyed without ill effect. An essential oil may be both safe and toxic depending on the dosage – it all depends on the knowledge, skill and experience of the therapist: for example, lavender is sedative in low dose but a high dose can cause insomnia (amphoteric effect).
Ingestion of essential oils
Only therapeutic essential oils should be employed for internal use, although it is not easy to guarantee the purity of an essential oil. Essential oils are absorbed into the blood stream and are metabolized into water- soluble products, allowing for renal elimination. The ingestion of essential oils should be left in the hands of a competent aromatologist (e.g. a licentiate of the Institute of Aromatic Medicine), or an aromatherapist working under the direction of a doctor. Legal requirements and rules of the hospital management board have to be observed, as well as the ethical considerations of any professional body to which the aromatherapist belongs. Nevertheless, some conditions such as enteritis, irritable bowel syndrome and diverticulitis can scarcely be treated in any other way than by ingestion.
Essential oils should always be correctly diluted for internal use; the best medium, if a dispersant is not readily available, is a fixed oil because the essential oils will dissolve easily and completely in it. Runny honey is also a good diluent, with the addition of a little water. Ingestion of essential oils is not advised for pregnant women and very young children.
Ingestion/overdose
When it comes to testing the toxic effects of swallowing essential oils, all studies have been carried out on animals as testing on humans is considered too hazardous. Occasionally some knowledge is derived from an accident involving a child or a deliberate overdose by an adult. Therefore, many of the opinions offered on this subject in the aromatherapy literature must be regarded as speculative.
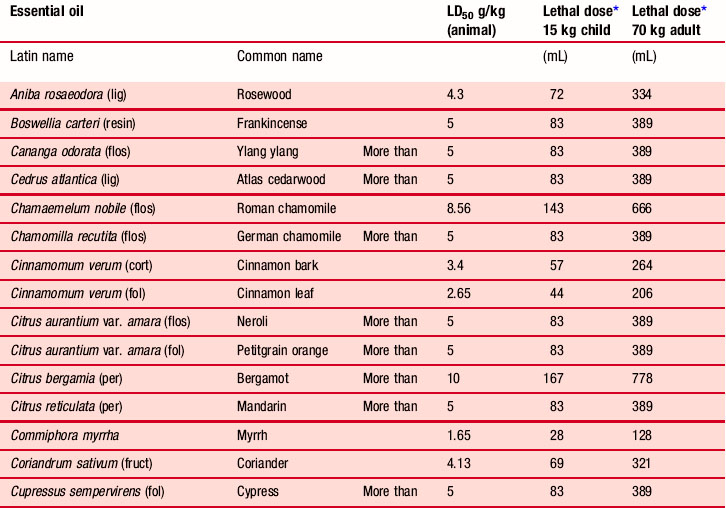
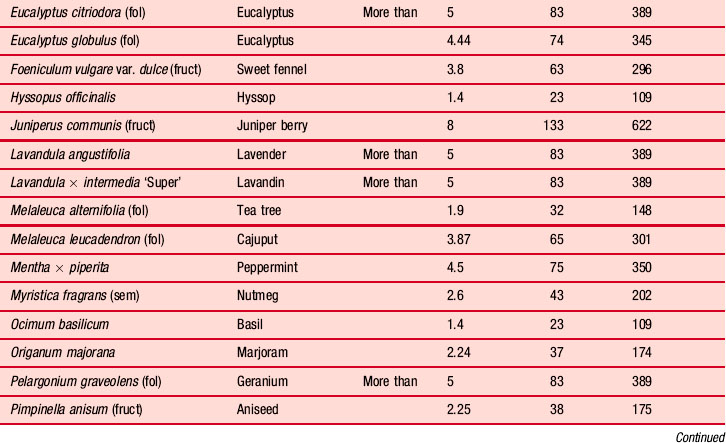
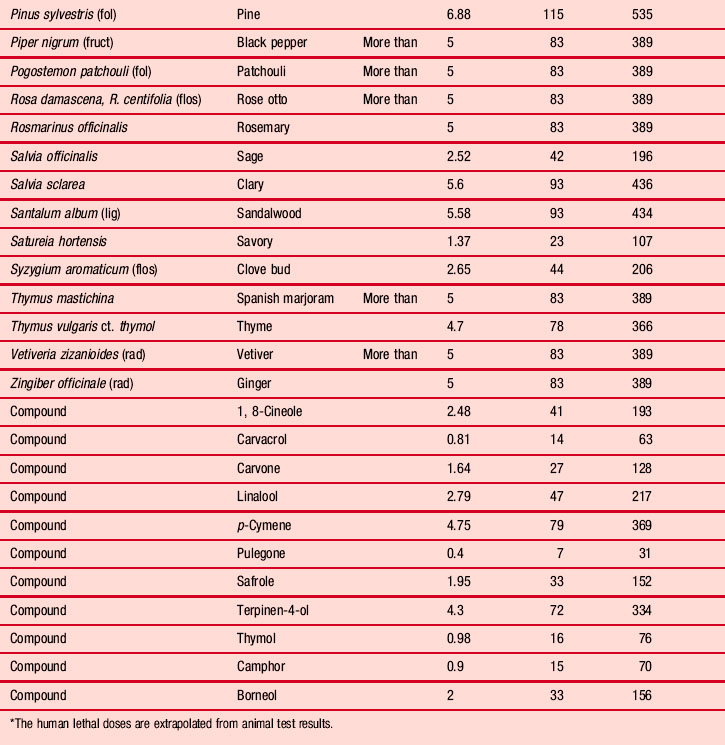
The ingestion of a large quantity of neat essential oil is unlikely as it would produce a burning sensation in the mouth and throat, and in some serious cases cause nausea, vomiting and diarrhoea. If the overdose is extreme there may follow lethargy, ataxia and coma, or perhaps irritability and convulsions (e.g. pennyroyal). The pupils may be dilated (e.g. camphor) or constricted (e.g. eucalyptus). Table 3.2 shows the lethal dose (LD50 is the dose at which 50% of the test subjects die) of some representative oils for a typical adult and a small child. These figures have been extrapolated from figures derived from animal testing and, as previously stated, metabolization in humans is not always the same as in animals so their accuracy cannot be guaranteed. In the absence of other information we must rely on these data as a guide.
The quantities used in aromatherapy are very small, so there is normally an extremely high safety factor when comparing the lethal dose with the effective dose. The effective dose (ED50) is the term used when some sort of response is being monitored in the experimental animal other than the death of the animal. The median effective dose is the dose at which 50% of the test subjects achieve the desired benefit.
Toxicity figures given in aromatherapy literature do not always make it clear that these doses are per kilogram of body weight, which could lead to the misunderstanding that the figures given are the effective or lethal doses for a person. They are not: they are dependent on the person’s weight. For example, the LD50 value for the oil from Salvia officinalis [sage] is 2.6 g/kg, which equates to a fatal dose of approximately 170 mL for a 60 kg person; the equivalent figure for Chamaemelum nobile [Roman chamomile] is 570 mL for a 60 kg person. The quantities involved are so great that anyone in their right mind would jib at taking them; however, illness may be caused at a much lower dose.
The following should never be administered internally:
• Oils obtained from gums (other than by distillation)
• Resins (because of the solvent residue)
• Absolutes (because of the solvent residue)
• Commercial quality oils (i.e. standardized) used by the perfume, food and pharmaceutical industries.
Ingestion of eucalyptus essential oil
Eucalyptus oil poisoning
There have been many cases of eucalyptus oil poisoning and it is puzzling why eucalyptus oil is so frequently taken by mouth, especially in Australia. A difficulty arises because there are very many kinds of eucalyptus oil of varying composition, and in none of the incidents referred to below is the botanical source specified; this may explain the sometimes conflicting recommendations for treatment given below. Ingesting up to 25 mL of eucalyptus oil led to coma in about 50% of 34 cases examined by Gurr and Scroggie (1965), which lasted from 30 minutes to 8 hours, usually with complete recovery after 24 hours: recovery has been noted even after ingestion of 60 mL. Another case of complete recovery was that of a 3-year-old boy who ingested 10 mL of eucalyptus oil and was soon deeply comatose with shallow, irregular respiration. Gastric lavage was given; he regained consciousness after 5 hours and was normal after 24 hours (Patel & Wiggins 1980). Spoerke et al. (1989) reviewed 14 cases of accidental exposure to eucalyptus oil, of which nine were ingestion. They concluded that small amounts seemed to be comparatively harmless and for larger amounts gastrointestinal symptoms were the most common, followed by central nervous system depression; amounts ingested ranged from 5 to 30 mL and patient age varied from 7 months to 20 plus years. Inhalation and skin exposure produced no or minimal symptoms.
A review of 41 child cases of eucalyptus poisoning in South East Queensland showed that 80% were completely asymptomatic, including four children who had swallowed more than 30 mL (maximum 45 mL). Two children were dizzy or ataxic, four had mildly depressed conscious levels, one child had an itchy rash and another had pruritus. A 4-month-old baby who had ingested 30 mL was the only one to display meiosis, hypertonia and hyperreflexia. The presence and severity of symptoms was not related to the amounts ingested (Webb & Pitt 1993); it was suggested that children should not undergo gastrointestinal decontamination unless symptomatic on arrival at hospital. Tibbals (1995) looked at 109 cases of child eucalyptus oil poisoning and recommended that children should receive medical attention regardless of the amount ingested.
Action to be taken
Traditional treatment in the event of an overdose is quite rigorous, involving gastric lavage or emesis and dilution with milk or fixed oil. Temple et al. (1991) re-evaluated this protocol after reviewing five cases of child poisoning following ingestion of citronella essential oil. One of these included a 16-month-old child who had ingested 25 mL of the oil, but in all five cases there was little medical intervention and all patients recovered with no ill effects. They concluded that advice given in standard texts based on cases managed with outmoded techniques should be evaluated, as the risks of evacuative and pharmacological interventions were considered greater than the risk of severe poisoning.
An example not to be followed
A nurse practising aromatherapy in a hospice some years ago was concerned to prove the safety of the oils she was administering to patients and took 5 mL of each of about 40 essential oils by mouth (one per week). In a personal communication she stated that she suffered no ill effects apart from sometimes dreaming more vividly than usual. The 40 oils included some that are potentially hazardous, and this extreme example must not be followed. Individuals vary greatly in their reaction to different substances and such actions may produce a disastrous result. There is a large safety factor when using the oils in normal aromatherapy quantities, i.e. two or three drops compared to approximately 100 drops that a 5 mL teaspoon would hold.
Oils in the eye
Undiluted essential oils are never placed in the ear nor on anogenital mucous surfaces and especially not in the eye, even diluted. If by accident essential oil does get into the eye then the advice given as to what to do varies slightly. One course of action is first to flush the eye under a running tap to expel most of the oil, and then to apply a fixed vegetable oil (Baudoux 2000 p. 35). Zhiri (2002 p. 21) agrees that neat essential oils should never be applied to the eyes, ears and anogenital mucosa, and also adds the nose; in case of accidental instillation or ingestion, either ingest or apply as appropriate a vegetable oil (e.g. olive, sunflower) to dissolve the essential oil, then seek medical aid. The authors have had experience of cases of mal use of essential oils in the eyes and on genital areas and have found the vegetable oil method to be effective, with minimum discomfort; essential oils are immediately soluble in vegetable oils, which give a dissolving/flushing action. For the eyes, the vegetable oil may be flooded in, and for the genital area a piece of cloth soaked in a vegetable oil immediately reduces the painful sensation, and usually there are no after effects.
Health professionals working in hospitals and similar establishments should secure the approval of a consultant or other suitably qualified and responsible person before giving oils by mouth (including gargles) or by the rectal and vaginal routes into the body. It is important to preserve procedural safety: the prescriber, dispenser and administrator should be separate persons to guard against error.
Undesired effects
A synthetic modern drug can have a positive effect on a diseased organ or part of the body but it can also have an adverse effect on a healthy part of the body, resulting in a second drug having to be administered. This in turn can give another adverse side effect, which will call for the administration of yet another drug. This cumulative effect of unwanted effects eventually killed the author’s mother, who, at the time of her death, was taking 22 different tablets a day, only one pertaining to her original problem.
In aromatherapy a different mindset is required, as essential oils bring many beneficial effects as well as a very occasional unwanted effect. As can be seen from the list of properties given for lavender oil, most of the side effects of essential oils are desirable. For example, lavender oil may be used as part of a treatment for depression and if, as a result, there are other beneficial results such as the alleviation of insomnia and relief from rheumatic pain, this is to be welcomed.
Undesired side effects occur usually as a result of the misuse of the oils, e.g. in the attempt to produce an abortion, or by accidental overdose – typically a toddler swallowing essential oils from a bottle. If essential oils are sold only in bottles with integral droppers and sensible precautions are taken to prevent access to them by children, this can be considered an extremely low risk therapy.
In normal aromatherapy the dose is usually very low but, as with any form of treatment, idiosyncratic reactions are a rare possibility. Such a case was reported by Vilaplana, Romaguera and Grimalt (1991) of a middle-aged woman who developed itching after using a cologne which was found to contain Bulgarian rose oil and geraniol. This was the first time in 326 cases of dermatitis that a person had tested positive to Bulgarian rose oil, and there were no other reported cases of dermatitis to the damask rose family, which prompts a question about the quality of this particular rose oil.
Hazardous oils
Some oils are rarely or never used in aromatherapy because of possible harmful effects (see Appendix B.4 on the CD-ROM). Some examples are Juniperus sabina [savin], Gaultheria procumbens [wintergreen], Peumus boldus [boldo leaf], Sassafras officinale [sassafras] and Thuja occidentalis [thuja]. Some other essential oils have a general prohibition on their use but without just cause. Mentha pulegium [pennyroyal] is alleged to be an abortifacient, but it may be used on men and those who are not pregnant, albeit with care because of its high content of the ketone pulegone.
Hyssopus officinalis [hyssop] is an excellent oil for respiratory disorders (used regularly over 30 years by the author) but is generally listed as toxic, as are Pimpinella anisum [aniseed] and several more. Salvia officinalis [sage] contains the ketone thujone (around 50%), and although nothing has been proven against the ketone molecule in sage oil, it is prudent to use it with care. Oils such as these may not be suitable for all health problems and may have contraindications, making their use not suitable for certain people in certain circumstances, but for the well trained therapist it is possible to use effectively the so-called hazardous or ‘toxic’ oils to the greater advantage of their clients. Confusion is aggravated by some authors and aromatherapy companies giving different warnings for different oils.
Epilepsy
It is widely taught that Hyssopus officinalis used on a person will provoke an epileptic fit, and this teaching is supposed to be based on a statement by Valnet (1980 p. 11), but what he actually wrote is ‘Even in weak doses the essences of sage, rosemary and hyssop can produce a tendency to epilepsy under certain conditions and in persons whose resistance is low’ (author’s italics). Cases of poisoning by sage and hyssop oils in the south of France have been investigated and the sage culprit has been identified as Salvia lavandulaefolia, which is rich in camphor. The epileptogenic effects of these two oils were extrapolated from animal tests, and for humans the sub clinical doses for Hyssopus officinalis and sage were found to be up to 0.1 mL/kg and 0.4 mL/kg, whereas lethal doses were more than 1.6 mL/kg and 4.0 mL/kg, respectively; the greatest toxicity was due to a combination of pinocamphone and isopinocamphone (Steinmetz et al. 1980). According to Renzini et al. (1999) Hyssopus officinalis begins to exhibit cytotoxicity at a concentration of 100 μg/mL and is due mainly to the component linalool, which is present in many essential oils. Millet et al. (1979) investigated – in animals – the convulsant activity of Hyssopus officinalis and Salvia lavandulaefolia and found the sub clinical dose for hyssop to be less than 0.08 g/kg; above 0.13 g/kg convulsions appeared and were lethal at 1.25 g/kg; this effect they also found to be due to the presence of pinocamphone and isopinocamphone.
Summary
Although some essential oils do present hazards, which frighten the inadequately trained, the properly trained therapist will recognize the hazard and take account of it to minimize or obviate any risk. This will be done by assessing the situation, applying the training received to the best advantage, and using common sense. These powerful oils should not be available to the general public, who may know nothing about their chemistry and effects.