What If …
This appendix addresses a number of patient-related questions that are among the most common the dental practitioner will encounter in daily practice. The “decision trees” help guide the practitioner through the steps involved in assessing clinical situations quickly and making related treatment decisions.
Topics covered in “What If” include drugs safe to use in pregnancy, allergy management, infective endocarditis prophylaxis, and a summary of the relationship between dental treatment, warfarin, and the international normalized ratio.
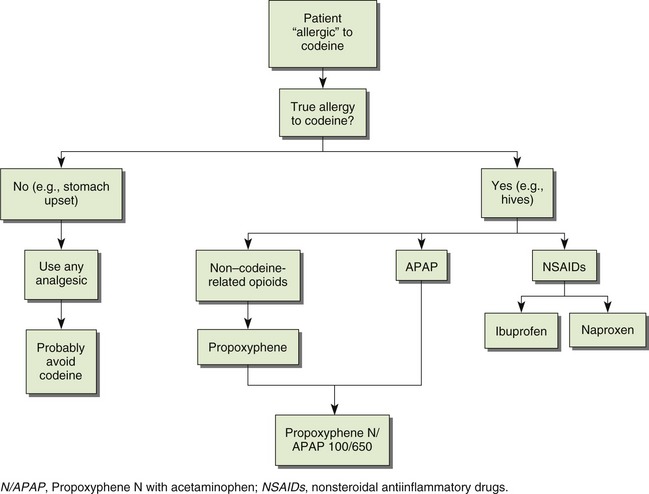
Allergies discussed include codeine, aspirin, penicillin, sulfites, and latex.
WHAT IF … THE PATIENT IS PREGNANT?*
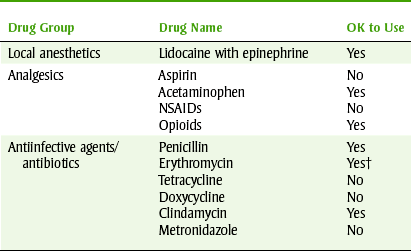
NSAIDs, Nonsteroidal antiinflammatory drugs.
*For more details see Chapter 24.
†Avoid erythromycin estolate in pregnancy.
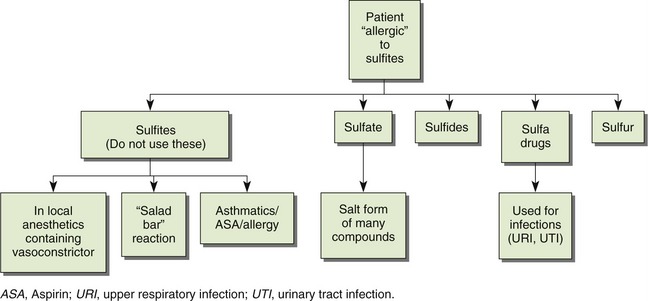
WHAT IF … THE PATIENT IS ALLERGIC TO SULFITES?
There is a lack of cross-hypersensitivity among the following: “sulfa” drugs, sulfites, sulfur, sulfate, and sulfide. “Sulfa drugs” are used to treat urinary tract infections, and their allergic reaction is usually a rash. Dental patients allergic to “sulfa” drugs may safely be given local anesthetics or a vasoconstrictor that contains sulfites.
WHAT IF … THE PATIENT IS ALLERGIC TO LATEX?
The increased use of latex-containing products has exposed more people with increasing frequency to latex allergens. Latex comes from the rubber tree and contains natural latex. Patients who are frequently exposed to latex-containing products (e.g., patients with spina bifida) and health care workers who use latex products (e.g., dental professionals) have a greater likelihood of developing allergies.
The extent of the reactions to latex ranges from contact dermatitis to severe anaphylactic reaction with death within a few minutes. If a dental practitioner uses any latex materials in his or her office, then parenteral epinephrine should be readily available.
There is also a cross-hypersensitivity between the foods listed in Box D-1 and latex allergy. If a patient is allergic to the listed fruits, then the dental health care worker should carefully question the patient regarding any reactions to latex-containing products (e.g., balloons, condoms). The patient should also be informed about cross-hypersensitivity that may occur between these fruits and latex. When powdered gloves are used, the latex can be absorbed into the powder and circulated around the room. This airborne latex can float around rooms and can even be stirred up with cleaning. Airborne latex can produce respiratory reactions such as asthma and anaphylaxis.
If a patient has an allergy to latex, he or she should be given the first appointment so that the latex particles have not contaminated the operatory air. The ventilation should be checked and measured for turnovers to make sure that the particles are removed overnight. One should be aware of the occupants of the building because use of latex in another office could inject latex particles into the central heating or cooling.
Manufactured latex products may contain a small amount of natural latex proteins, a very large amount, or somewhere in between. Asking for more information on the latex gloves used in the dental office may reduce the exposure to allergenic proteins.
When treating a latex-allergic patient, nonlatex equipment should be substituted for any products that contain latex (Box D-2). Newer catalogues contain a wide range of dental-related products (e.g., nonlatex bite blocks, dams, and adhesives for bandages). Books that contain additional information about latex allergy may include infection-control topics.
WHAT IF … THE PATIENT IS TAKING WARFARIN (COUMADIN)? (See Chapter 15)
| Dental Procedure | OK to Treat if INR < |
| Periodontal probing | <4 |
| Restorative, simple scaling/root planning endodontics | 3.5 |
| Extraction, simple | 2.5-3.5 |
| Extraction, multiple | 2-3.5 |
| Periodontal surgery | 2.5 |