Cardiovascular Drugs
1 Identify several dental issues in the treatment of patients with cardiovascular disease.
2 Describe heart failure and identify drugs commonly used to treat it, including the mechanisms of action, pharmacologic effects, adverse reactions, and uses of each.
3 Define arrhythmia and dysrhythmia and describe how the heart maintains its normal rhythm.
4 Describe the mechanisms of action, pharmacologic effects, adverse reactions, and uses of antiarrhythmic agents and identify the issues to consider in dental treatment.
5 Define angina pectoris and describe the types of drugs used to treat it; identify the dental implications of these drugs.
6 Describe the various types of antihypertensive agents, including the mechanisms of action, pharmacologic effects, adverse reactions, and uses of each. Also identify potential drug interactions and the dental implications of these drugs.
7 Define hyperlipidemia and hyperlipoproteinemia and summarize the types of drugs used to restore cholesterol homeostasis in the body.
8 Describe the role of warfarin in blood coagulation and the potential adverse reactions and interactions associated with its use.
9 Identify several other drugs that affect blood coagulation.
The term cardiovascular disease refers to a variety of diseases of the heart and blood vessels. Examples of these diseases include hypertension, angina pectoris, coronary artery disease, cerebrovascular accident (CVA), and heart failure (HF). Although cardiovascular disease is the leading cause of death in the United States, patients with cardiovascular disease are now living longer, more productive lives because of cardiac care units, comprehensive drug therapy, and intensive screening procedures. This explains why cardiovascular disease affects such a large proportion of the dental patient population.
The dental health care worker first identifies the patient with cardiovascular disease while taking the medical or drug history. It is common for these patients to have several cardiovascular conditions such as HF, hypertension, and hypercholesterolemia. For each disease, a patient may take one or more medications. The importance of this group of drugs is demonstrated by the fact that about 25% of the top 200 drugs (see Appendix A) are from this group.
 of Top 200 are cardiovascular drugs.
of Top 200 are cardiovascular drugs.Because cardiovascular medications are often given for the patient’s lifetime, a knowledge of the actions, problems, and effects of these drugs on dental treatment is essential. Both the disease and the drugs used in their treatment can affect the management of a patient’s dental care.
Before each group of drugs is discussed, the disease for which the drugs are used is briefly described, beginning with general considerations concerning the dental treatment of patients with cardiovascular disease.
DENTAL IMPLICATIONS OF CARDIOVASCULAR DISEASE
Contraindications to Treatment
Although most patients with cardiovascular disease can be safely treated in the dental office, circumstances may arise in which dental treatment should be delayed until the patient’s disease is under better control.
Certain medical situations listed in Box 15-1 are absolute contraindications to dental treatment until a consultation with the patient’s provider has determined any special treatment alterations that might be warranted. These absolute contraindications apply only to uncontrolled or severe cardiovascular diseases. Examples of absolute contraindications to elective dental treatment include very high blood pressure and approximately 6 months after the patient has experienced a myocardial infarction (MI). Most patients with cardiovascular disease can be treated in the dental office. The type of procedure anticipated, the stress of the procedure, and the fact that many procedures are elective must be considered. By obtaining a thorough health history, a determination can be made about whether the patient’s provider should be consulted before beginning dental treatment. When the health care provider is contacted, it is important to explain the procedure(s) that is indicated for the patient.
Vasoconstrictor Limit
When a local anesthetic containing a vasoconstrictor is used in the treatment of patients with cardiovascular disease, the severity of the patient’s disease must be considered. The majority of cardiovascular patients should benefit from the use of epinephrine in the local anesthetic agent. The amount and effect of the epinephrine administered must be weighed against the fact that poor pain management can produce the release of endogenous epinephrine. Limiting the dose of epinephrine to the cardiac dose may be warranted in a few severely affected patients (see Chapter 9 for a detailed discussion of vasoconstrictor limits).
Using a slow rate of injection and appropriate aspiration techniques to avoid intravascular injection reduces the chance of vasoconstrictor adverse reactions. A “fight or flight” reaction related to the patient’s anxiety also results in the release of endogenous epinephrine indistinguishable in effect from that of the exogenous epinephrine. (So, being really scared feels exactly like epinephrine because one is making epinephrine.)
Infective Endocarditis
As stated in Chapter 7, the clear-cut uses of antibiotics for prophylaxis before a dental procedure (recommended by the American Heart Association [AHA] and the American Dental Association [ADA]) are a history of infective endocarditis, presence of a heart valve prosthesis, or congenital heart disease. The most current guidelines regarding antibiotic prophylaxis are discussed in detail in Chapter 7.
Cardiac Pacemakers
A cardiac pacemaker is an electrical device implanted in a patient’s chest to regulate the heart rhythm. If not appropriately shielded, some electrical devices commonly used in dentistry may interfere with proper pacemaker activity. Consultation with the patient’s provider may be appropriate before treating a patient with a pacemaker. These patients do not require antibiotic prophylaxis.
Periodontal Disease and Cardiovascular Disease
Research has discovered a relationship between periodontal disease and both cardiovascular disease and stroke. Persons with untreated cardiovascular disease are at increased risk for severe periodontal disease, insulin-dependent diabetes mellitus, atherosclerosis, and emboli production.
CARDIAC GLYCOSIDES
The heart functions as a pump, ensuring adequate circulation of the blood to meet the oxygen needs of all the body’s tissues. When oxygen needs are increased, as in exercise, the normal heart adjusts its output to meet the increased oxygen needs. If the heart is unable to keep up with the body’s needs, it becomes a “failing” heart and the pumping mechanism becomes inefficient. This occurs because the heart muscle has suffered an injury and cannot keep up its work. Some enlargement of the heart produces a more efficient heartbeat and cardiac output (Starling’s law). However, over time, additional cardiac enlargement occurs (cardiac muscle stretched past its maximum effectiveness by the presence of excess blood that it cannot pump out), and the patient becomes tachycardic. This inefficient pumping mechanism results in an inadequate cardiac output and unsatisfactory circulation. Various forms of injury to the heart, such as MI (heart attack), arrhythmias, and valvular abnormalities from rheumatic heart disease, can contribute to a failing heart.
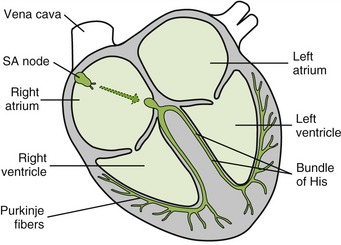
The heart has two sides: the right and left sides (Figure 15-1). In heart failure (HF), the heart does not provide adequate cardiac output to provide for the oxygen needs of the body. Over time, the blood accumulates in the failing ventricle(s). The ventricle(s) enlarges and finally becomes ineffective as a pump.
One or both sides of the heart can fail. Usually, the left side fails first. If the left side of the heart fails, the blood backs up into the pulmonary circulation (lungs). Pulmonary edema results, producing dyspnea and orthopnea. Dental patients with left failure may need to have dental treatment performed with the patient in the semireclined position. If the right side of the heart fails, then the right ventricle is unable to remove all the blood from that side of the heart. Right-sided heart failure causes systemic congestion. Symptoms include peripheral edema with fluid accumulation evidenced by pitting edema (pedal edema). Over time, many patients experience failure of both sides of the heart, which causes symptoms from failure of both sides.
Digitalis Glycosides
The most common type of drug used in the treatment of HF was first described by William Withering in 1785. At first, he thought that these drugs affected the kidneys because they produced diuresis. Later, these substances were referred to as cardiac or digitalis glycosides: cardiac because they affect the heart and glycoside because of their chemical structure. Digoxin (di-JOX-in) (Lanoxin) is the most commonly used cardiac glycoside.
 PHARMACOLOGIC EFFECTS
PHARMACOLOGIC EFFECTS
The major effect of digoxin on the failing heart is to increase the force and strength of contraction of the myocardium (positive inotropic effect). It allows the heart to do more work without increasing its oxygen use. When the contractile force of the heart is improved, the heart becomes a more efficient pump and the cardiac output increases. After the patient takes digoxin, the heart is reduced to a more efficient size and can function more effectively.
Digoxin affects the heart rate in several ways. It has little effect on the heart rate of normal patients, but in HF the heart rate is first increased. This occurs because of increased sympathetic action resulting from decreased cardiac output. As digoxin increases the cardiac output, the sympathetic tone is decreased, with a decrease in heart rate (bradycardia) as the end result. Digoxin also reduces the edema that occurs with HF. As a result of the improved pumping action, more blood circulates through the kidneys (increase in glomerular filtration rate), which mobilizes the edema from the tissues, producing diuresis. The diuresis is not a result of an effect on the kidneys; it is a result of digoxin’s indirect effect produced by the improving heart’s function. The size of the heart is reduced as the excess blood volume that has collected there is removed via the kidneys.
Digoxin can affect automaticity, conduction velocity, and refractory periods of different parts of the heart in different ways. It slows atrioventricular (AV) conduction, prolongs the refractory period of the AV node, and decreases the rate of the sinoatrial (SA) node. By prolonging the refractory period of the AV node, fewer impulses will be transmitted to the ventricle and the heart rate will fall. These effects are useful in the treatment of certain arrhythmias.
USES
The most common use of digoxin is in the treatment of HF. It is also used for atrial arrhythmias, including atrial fibrillation (AF) and paroxysmal atrial tachycardia (PAT). Patients with HF and normal sinus rhythm may not experience long-term benefit in reducing mortality from the use of digoxin. A recent large trial comparing the mortality of patients taking digoxin with placebo determined that digoxin did not reduce mortality. For this reason, the use of digoxin as first-line therapy is decreasing and other drugs such as angiotensin-converting enzyme inhibitors (ACEIs), angiotensin receptor blockers (ARBs), and β-adrenergic blockers are used more often. However, the results of a long-term clinical trial have found that addition of digoxin to other drugs decreases the rate of hospitalization, especially among sicker patients, but does not affect survival.
ADVERSE REACTIONS
Because of digoxin’s narrow therapeutic index (see Chapter 3), toxic effects are not uncommon. Even slight changes in dose, absorption, or metabolism can trigger toxic symptoms. In the elderly, toxicity is more likely to occur.
Gastrointestinal Effects.: Early signs of digoxin toxicity include anorexia, nausea and vomiting, and copious salivation. A reduction in the dosage of digoxin usually alleviates these adverse reactions.
Arrhythmias.: If a sufficient overdose is given, severe cardiac irregularities can develop. These arrhythmias can progress to ventricular fibrillation and death. Diuretics, often used in the treatment of HF, can produce hypokalemia, which can predispose a patient to serious arrhythmias. One should note that digitalis is used to treat arrhythmias and its toxicity can produce arrhythmias.
Neurologic Effects.: The neurologic signs of toxicity include headache, drowsiness, and visual disturbances (green and yellow vision, halo around lights). A pain in the lower face resembling that of trigeminal neuralgia has been reported as a neurologic symptom of digitalis toxicity. Weakness, faintness, and mental confusion have also been reported.
Oral Effects.: Increased salivation is associated with digoxin toxicity. Increase in gagging reflex has been produced, which may interfere with taking an impression.
Dental Drug Interactions.: With either increased or decreased blood levels, serious problems can occur when digoxin interacts with other drugs. One drug interaction between digoxin and the sympathomimetics may result in an increase in the chance of arrhythmias. Because both drugs can produce ectopic pacemaker activity, their concomitant administration can increase the chance of arrhythmias.
For this reason, the vasoconstrictors added to local anesthetics, which are sympathomimetics, should be used with caution. In patients with severe cardiac disease, the epinephrine dose may be limited to the cardiac dose (see Chapter 9). Erythromycin and tetracycline can increase the toxicity of digoxin in some patients.
MANAGEMENT OF THE DENTAL PATIENT TAKING DIGOXIN
Box 15-2 summarizes the management of the dental patient taking digoxin.
Gastrointestinal Effects.: If a patient complains of nausea or vomiting, special care must be taken to prevent emesis. These symptoms may be associated with digitalis toxicity, and the patient’s physician should be consulted if the nausea and vomiting have been protracted.
Epinephrine Administration.: Because digoxin toxicity can sensitize the myocardium to arrhythmias, epinephrine should be used cautiously or limited to the cardiac dose in patients taking digitalis. Patients taking digitalis should be questioned about toxic symptoms before epinephrine is administered. Hypokalemia from diuretics can exacerbate this arrhythmogenic potential.
OTHER DRUGS
Angiotensin-Converting Enzyme Inhibitors.: Current guidelines from the American College of Cardiology (ACC) and the AHA now recommend prescribing an ACEI for all patients with symptomatic (stage C) heart failure and asymptomatic patients with a decreased left ventricular ejection fraction (LVEF) or a history of MI. ACEIs improve symptoms in patients with heart failure within a period of 4 to 12 weeks, decrease the incidence of hospitalization and MI, and prolong survival. ACEIs are now considered first-line therapy and are the cornerstone of HF therapy.
Angiotensin Receptor Blockers.: ARBs have also been shown to reduce mortality and symptoms. They are recommended for patients who cannot tolerate ACEIs and are also considered first-line therapy for HF. Candesartan and valsartan are the only ARBs currently approved by the Food and Drug Administration (FDA) for the treatment of heart failure.
β-Adrenergic Blockers.: The ACC/AHA guidelines now recommend β-blockers for patients with symptoms of HF and asymptomatic patients with decreased LVEF or a history of an MI. Although it has been customary to start a β-blocker after an ACEI, the results of several clinical trials suggest that starting with a β-blocker may be equally, if not possibly more, effective.
Vasodilators.: Hydralazine, an arterial vasodilator, reduces the peripheral resistance by arterial vasodilation. With a reduction in the afterload, the work of the heart is reduced. Isosorbide dinitrate, a venous dilator, reduces the preload, which reduces the work of the heart. With this combination, the heart is pumping against less resistance and is getting less blood returned to it (some blood remains in the venous circulation). The heart’s workload is reduced and symptoms of HF subside. The addition of hydralazine and isosorbide dinitrate to standard therapy in black patients with class III to IV heart failure significantly lowered mortality and the rate of hospitalization and improved quality-of-life scores. No data are available with this combination in addition to standard therapy in other populations.
Diuretics.: Most patients with HF have edema or fluid retention. Diuretics are used in these patients to relieve the symptoms of HF. In clinical trials, patients taking a combination of a diuretic and other drugs used to treat HF showed an increase in survival. Loop diuretics, such as furosemide, appear to be more effective than thiazide diuretics.
Aldosterone Antagonists.: In one clinical trial, the addition of spironolactone to standard therapy reduced the risk of mortality and hospitalization. In another clinical trial, the selective aldosterone antagonist eplerenone added to standard therapy reduced both all-cause and cardiovascular mortality in patients with an acute MI complicated by left ventricular systolic dysfunction and HF.
ANTIARRHYTHMIC AGENTS
The terms arrhythmia (ar, insensibility; rhythmos, rhythm) and dysrhythmia (dys, bad; rhythmos, rhythm) are used interchangeably to mean “abnormal rhythm.” Arrhythmias may result from abnormal impulse generation or abnormal impulse conduction. Cardiac diseases, such as myocardial anoxia, arteriosclerosis, and heart block, can produce arrhythmias. The antiarrhythmic agents are drugs that are used to prevent arrhythmias.
Automaticity
The cells of the cardiac muscles, unlike those of skeletal muscles, have an intrinsic rhythm called automaticity. “Pacemaker” cells spontaneously produce action potentials as they undergo slow spontaneous depolarization during diastole (as they rest, they leak ions). If any heart muscle cell is left undisturbed and isolated from the rest of the heart with appropriate nutrients and oxygen, each cell will beat spontaneously at its own rate. Each type of cardiac cell differs in its automaticity depending on the function of the particular cell. The cells that specialize in conduction functions have a faster rate of automaticity than other cardiac cells. This design ensures that the heart will beat in a coordinated manner.
The SA node has the fastest rate of depolarization and therefore directs all the other cells in the heart. It normally fires impulses approximately 80 times/min. The SA node is innervated by both the parasympathetic nervous system (PNS) and the sympathetic nervous system (SNS). The SA node sends a message (action potential) to the AV node via the atrial muscle. When the impulse arrives at the AV node there is a slight delay because the muscles beyond the AV node are thinner. The AV node sends the message via the bundle of His to the Purkinje fibers. The Purkinje fibers then send the message to the cardiac muscle cells, to the apex of the ventricles, directing them all to contract as they get the message. This system is repeated with each heartbeat.
In the normal patient, this system functions seamlessly. In the patient with cardiac arrhythmias, diseased parts of the heart can produce abnormal conduction pathways, which may result in arrhythmias.
Action Potential
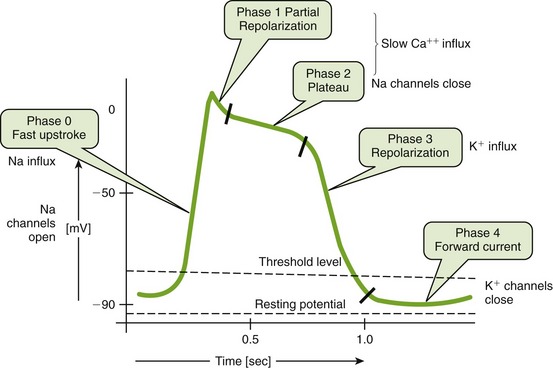
All action potentials have similar properties, but minor differences exist. During rest, the resting membrane potential varies but is −75 mV for some cardiac tissues. Electrical excitation from the nerve produces movement of ions across the membrane, generating an action potential (Figure 15-2). During each of these phases, there is a change in the ion flow that results in certain effects. These changes are seen in Figure 15-2.
Arrhythmias
There are many types of arrhythmias that produce various abnormalities of the heartbeat. These arrhythmias are usually divided into supraventricular (atrial) and ventricular types, depending on the location of the genesis of the arrhythmia. Abnormal arrhythmias may result in tachycardia or bradycardia of the supraventricular (atrial) or ventricular parts of the heart or from ectopic foci. The ectopic foci are “emergent leaders” that preempt the SA or AV nodal rate. The electrical impulses begin at the SA node and travel to the AV node. At the conduction level, different patterns of conduction include the normal pattern, bifurcation (conduction splits and goes two ways), reentry, unidirectional block (action potential is blocked from being stimulated from one side of the tissue but not from the other), and prolonged refractory period.
Several recent deaths of fit adolescents during athletic events have been linked to congenital presence of a prolonged QT interval (torsades de pointes, previously undiagnosed).
Antiarrhythmic Agents
Antiarrhythmic agents are placed in groups designated by Roman numerals I to IV. Subsets of these Roman numerals use capital letters (A, B, C). The specific actions of the antiarrhythmics are complicated. The antiarrhythmic agents work by depressing parts of the heart that are beating abnormally. For example, if the Speaker of the House (an ectopic foci) attempts to take over the office of President (SA node) and send additional messages to the other officers, then the antiarrhythmic agents can “quiet” these foci.
Antiarrhythmics may change the slope of depolarization, raise the threshold for depolarization, and alter the conduction velocity in different parts of the heart. For example, by decreasing the slope of depolarization, there would be a decrease in the frequency of discharge and the rate would slow. By raising the threshold for producing an action potential, extra beats may be suppressed. Examples of specific actions of these drugs include decrease in the velocity of depolarization, decrease in impulse propagation, and inhibition of aberrant impulse propagation. Tables 15-1 and 15-2 describe the classification and mechanism of action of the antiarrhythmics, the dental-related adverse reactions, and the dental implications of the antiarrhythmias.
TABLE 15-1
CLASSIFICATION AND MECHANISM OF ACTION OF THE ANTIARRHYTHMICS
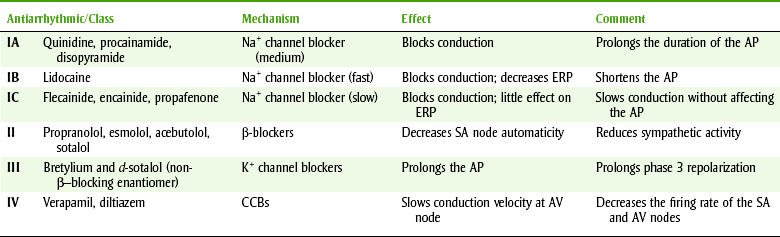
AP, action potential; AV, Atrioventricular; CCBs, calcium channel blockers; ERP, effective refractory period; K+, potassium; Na+, sodium; SA, sinoatrial.
TABLE 15-2
MANAGEMENT OF DENTAL PATIENTS TAKING ANTIARRHYTHMICS
| Antiarrhythmics | Implications |
| All | Check for abnormal or extra beats when taking patient’s blood pressure and pulse. Record the type of arrhythmia and the drug therapy. |
| Atrial fibrillation | Patient on warfarin—check INR. |
| Amiodarone | Liver toxicity, blue skin discoloration, photosensitivity—dental light |
| CCBs | Gingival enlargement (verapamil most reported) |
| Disopyramide | Anticholinergic xerostomia |
| Procainamide | Reversible lupus erythematosus–like syndrome, 25%-30%; CNS depression, xerostomia |
| Quinidine | Nausea, vomiting, diarrhea; cinchonism with large doses; atropine-like effect; xerostomia |
| Phenytoin | Gingival enlargement |
| β-Blockers, nonspecific | Drug interaction with epinephrine; limit to cardiac dose if patient’s condition warrants |
CCBs, Calcium channel blockers; CNS, central nervous system; INR, international normalized ratio.
Conclusions drawn from data must be carefully analyzed to arrive at appropriate conclusions that can be applied clinically. One study demonstrated that IC antiarrhythmics can prevent post-MI arrhythmics. Although it would seem that this action would be beneficial, with additional data it was determined that although these drugs prevented arrhythmias, patient mortality doubled or tripled. Before this study was completed, these deaths were thought to be a result of fatal arrhythmias unrelated to the drug. It pays to look at future outcomes (e.g., death) to determine whether a drug is “beneficial.”
DIGOXIN
Although digoxin is not included in the other groups of antiarrhythmics, it is used to treat some arrhythmias. It shortens the refractory period of atrial and ventricular tissues while prolonging the refractory period and diminishing conduction velocity in the Purkinje fibers. Toxic doses of digoxin can result in ventricular arrhythmias.
Adverse Reactions
Because of their narrow therapeutic index, antiarrhythmic agents are difficult to manage. Therefore they are only used in patients with arrhythmias that prevent the proper functioning of the heart.
Dental Implications
The dental implications of the antiarrhythmic agents are summarized in Table 15-2.
ANTIANGINAL DRUGS
Angina pectoris is a common cardiovascular disease characterized by pain or discomfort in the chest radiating to the left arm and shoulder. Pain can also be reported radiating to the neck, back, and lower jaw. The lower jaw pain can be of such intensity that it may be confused with a toothache. Angina occurs when the coronary arteries do not supply a sufficient amount of oxygen to the myocardium for its current work. Anginal pain can be precipitated by the stress (increased workload on the heart) induced by physical exercise or emotional states such as the anxiety and apprehension generated by a dental appointment.
At one time, the nitroglycerin (NTG)-like compounds (Table 15-3) were the only class of drugs that could effectively relieve the symptoms of angina. More recently, the β-adrenergic blocking agents and the calcium channel blocking drugs have added a new dimension to drug therapy for angina.
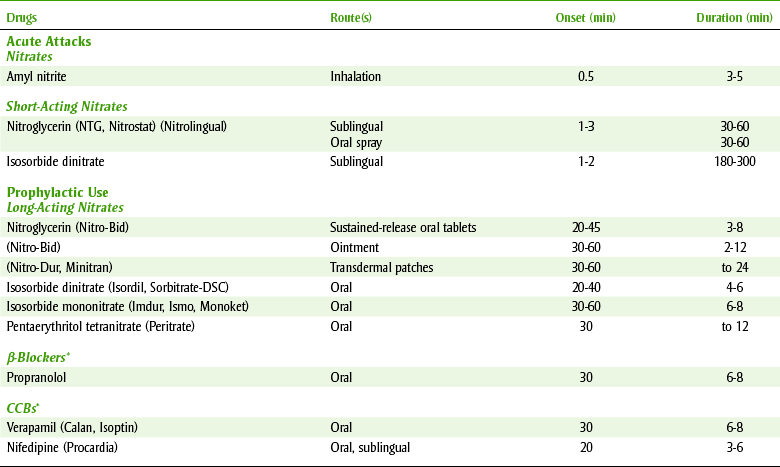
The basic pharmacologic effect of drugs used to manage angina is reduction of the workload of the heart by decreasing the cardiac output, the peripheral vascular resistance, or both. The oxygen requirement of the myocardium is in turn reduced, which relieves the painful symptoms of angina. It is important, however, to keep in mind that these drugs are not curative, and the dental team should be alert to the fact that an anginal episode could occur at any time. Appropriate emergency procedures to manage an acute anginal attack should be reviewed before treating a patient with angina (see Chapter 23). Table 15-3 lists the major antianginal drugs and some of their more pertinent characteristics.
Nitroglycerin-Like Compounds
Nitroglycerin (nye-troe-GLI-ser-in) (NTG) is by far the most often used nitrate for the management of acute anginal episodes. In addition to the long-acting nitrates, NTG is also used to prevent anginal attacks induced by stress or exercise. Box 15-3 provides guidelines for managing the patient taking NTG-like agents.
MECHANISM
NTG is a vasodilator. It releases free nitrite ion and nitric oxide (NO). NO, an even more potent vasodilator than nitrite, activates guanylyl cyclase and increases cyclic guanosine monophosphate (cGMP), producing relaxation of vascular smooth muscle throughout the body. Indirectly, there is a reduction in work of the heart produced by the effect on both the venous and the arterial sides of the circulation. The venous dilation reduces the amount of blood returning to the heart (preload) and thereby reduces the heart’s workload. The arterial dilation reduces the resistance against which the heart must pump (afterload). By reducing workload on the heart, NTG decreases the oxygen demand with relief or reduction of angina pain (Figure 15-3). Tolerance to these effects occurs, unless a nitrate-free period is observed daily.
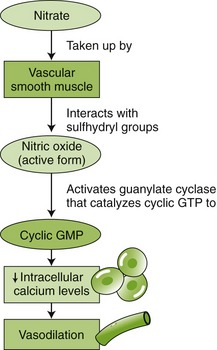
FIGURE 15-3 Pharmacologic action of nitrates. (From McKenry L, Tessier E, Hogman MA: Mosby’s pharmacology in nursing, ed 22, St Louis, 2006, Mosby.)
Amyl nitrite is the only NTG-like agent that is not a nitrate; it is a nitrite. It is a volatile agent in a closed container. It is administered by crushing the container and inhaling the volatile fumes in an emergency situation (similar to the aromatic ammonia spirit inhalant ampules sniffed when one faints). Because amyl nitrite has no advantage over sublingual (SL) NTG and it has unapproved recreational uses, it is not often used.
SL NTG is used to treat acute anginal attacks. It has a rapid onset (few minutes) by this route, and its effect can last up to 30 minutes. It is available as an SL tablet (Nitrostat) or spray used sublingually (Nitrolingual). SL isosorbide dinitrate is also effective for an acute anginal attack. The dental office emergency kit should contain one of these products to manage acute anginal attacks. Dental patients with a history of angina should be asked to bring their NTG to each dental appointment.
ADVERSE REACTIONS
Most adverse reactions associated with NTG occur because of its effect on vascular smooth muscle. Severe headaches are often reported (vasodilation) after the use of NTG. Flushing, hypotension, lightheadedness, and syncope (fainting) can also result. Hypotension is enhanced by alcohol and hot weather. SL NTG can produce a localized burning or tingling at the site of administration. The presence of stinging is not indicative of the potency of the NTG.
SIGNIFICANT DRUG INTERACTIONS AND CONTRAINDICATIONS
Phosphodiesterase 5 (PDE5) inhibitors are a class of drug used to treat erectile dysfunction. These drugs include sildenafil (Viagra), vardenafil (Levitra), and tadalafil (Cialis). The administration of any of these drugs with either daily or intermittent doses of any nitrate is contraindicated. The combination of PDE5 inhibitors with any type of nitrate can cause dangerously low blood pressure.
STORAGE
NTG is degraded by heat and moisture but not by light. NTG should be stored in its original brown glass container and tightly closed because it can be adsorbed by plastic. It should not be refrigerated because condensation of the moisture in the air produces moisture that can reduce its effectiveness.
If the original bottle is unopened, NTG is active until the expiration date printed on the bottle (assume average storage conditions). When the bottle is opened, the date opened should be written on the outside of the bottle. It should be discarded after 3 months or based on the expiration date printed on the bottle (whichever date is the earliest). The NTG spray is effective until its expiration date is reached because air does not enter the container with use.
Various long-acting NTG-like products (see Table 15-3), such as isosorbide dinitrate (eye-soe-SOR-bide dye-NYE-trate) and isosorbide mononitrate, are available for the long-term prophylaxis of anginal attacks. The dose forms available include tablets (swallowed) and topical (ointment and patch) products. With long-term, regular use, tolerance to this effect develops. In fact, no difference can be detected between a long-acting nitrate and placebo when taken without a daily “vacation.” To prevent tolerance, prophylactic nitrates should be given with at least an 8- to 12-hour “vacation” every day (often during sleeping, depending on symptom pattern). The mononitrate dose form requires a 7-hour “vacation” daily; the first dose is given in the morning and the second dose is given 7 hours later.
Calcium Channel Blocking Agents
Another group of drugs approved for use in angina pectoris is the calcium channel blockers (CCBs) (see discussion in the section on hypertension). A few examples are verapamil (ver-AP-a-mil) (Calan, Isoptin), diltiazem (dil-TYE-a-zem) (Cardizem), and nifedipine (nye-FED-i-peen) (Procardia, Adalat) (Table 15-4).
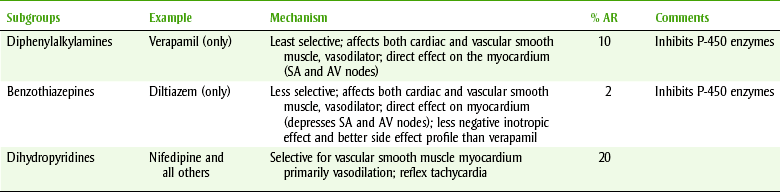
The mechanism of action of CCBs for the treatment of angina pectoris is related to the inhibition of movement of calcium during the contraction of cardiac and vascular smooth muscle. Vasodilation and a decrease in peripheral resistance result, thereby decreasing the work of the heart. Some CCBs decrease myocardial contractility (negative inotropic effect), resulting in reduced cardiac output. Others increase coronary vasodilation. The choice of the specific CCB depends on the patient’s cardiac disease.
In addition to their use in angina, these drugs are used in the treatment of cardiac arrhythmias and hypertension. Adverse effects include dizziness, weakness, constipation, and hypotension. Nifedipine has been associated with gingival enlargement and dysgeusia (altered sense of taste). The gingival enlargement is similar to that produced by phenytoin. Dental patients receiving these drugs should be given additional oral hygiene instructions, and frequent dental appointments should be planned.
β-Adrenergic Blocking Agents
β-Adrenergic blocking drugs such as propranolol (proe-PRAN-oh-lole) (Inderal), metoprolol (me-TOE-proe-lole) (Lopressor), and atenolol (a-TEN-oh-lole) (Tenormin), are used in the treatment of angina pectoris. These drugs block the β response to catecholamine stimulation, thereby reducing both the chronotropic and inotropic effects. The net result is a reduced myocardial oxygen demand. β-Adrenergic blockers are effective in reducing both exercise- and stress-induced anginal episodes. Adverse effects include bradycardia, HF, headache, dry mouth, blurred vision, and unpleasant dreams. β-Adrenergic blocking drugs are discussed in the section on hypertension and in Chapter 4 in the section on sympathetic blockers.
Ranolazine
In January 2006 the FDA announced the approval of ranolazine (Ranexa) for the treatment of chronic angina. In 2008 the FDA further approved the use of ranolazine for the treatment of chronic angina either alone or in combination with β-blockers, CCBs, and nitrates. It is a new molecular entity and is the first drug to be approved to treat chronic angina in more than 10 years. Although it has several pharmacologic activities, its exact mechanism of action is unknown. It does not significantly alter heart rate or blood pressure. It does prolong the QT interval, and caution should be used when it is used in combination with other drugs that increase the QT interval. Two major clinical trials found ranolazine to be more effective than placebo in treating chronic angina. In both studies, however, ranolazine appeared to be less effective in women than in men.
Dental Implications
TREATMENT OF AN ACUTE ANGINAL ATTACK
The dental team should be prepared to treat an acute anginal attack before treating the patient with a history of angina. Before administering NTG the dental team should make sure that the patient has not used a PDE5 inhibitor within the past 24 hours. If the patient has used one of these drugs, then NTG cannot be given. The best course of action is to immediately contact 911. The patient’s personal NTG tablets or spray should be available and placed on the bracket table in case of an acute attack. Long-acting nitrates and topical products are not useful for the treatment of an acute anginal attack. For acute emergencies, the dental office should have a supply of SL NTG (see discussion of storage). The patient should be in the seated position before ingesting the NTG. One tablet can be administered at once, followed in 5 minutes by another, and in another 5 minutes by a third tablet. If these tablets do not stop the anginal attack, the patient should be taken to the emergency room. If using the spray, one should make sure that the patient does not inhale while spraying.
PREVENTION OF ANGINAL ATTACK
Two methods to prevent an acute attack of angina include pretreatment with either an anxiolytic agent (e.g., benzodiazepine or nitrous oxide [N2O]) or SL NTG. One should make sure that the patient has not used a PDE5 inhibitor within the past 24 hours. If he or she has, then SL NTG cannot be used as prophylaxis for an acute attack.
Anxiolytics.: Because anxiety produces stress and causes the heart to work harder, an antianxiety agent, or anxiolytic (benzodiazepine), may be prescribed to allay anxiety and prevent an acute anginal attack. N2O-oxygen (N2O-O2) can also relax an anxious dental patient, and N2O itself produces vasodilation.
Nitroglycerin.: Premedicating an anxious dental patient with SL NTG before an anxiety-provoking procedure can reduce the chance of an attack. For example, the patient can be given SL NTG a few minutes before a local anesthetic injection.
Because of NTG’s instability, it must be properly stored in the dental office. One should check the expiration date on the office supply regularly.
MYOCARDIAL INFARCTION
A patient with symptoms of an anginal attack that is not relieved by three doses of SL NTG (0.04 mg) may be experiencing an MI. If the patient who has not been previously diagnosed as having angina experiences chest pain, he or she should be taken to an emergency room for diagnosis. Occasionally, an anginal attack can proceed to an acute MI. For this reason, the dental team should make sure any patient with an attack that is not relieved by NTG is accompanied by an employee to the hospital emergency room.
ANTIHYPERTENSIVE AGENTS
Hypertension is the most common cardiovascular disease, affecting some 50 million Americans (28.6%) and 1 billion individuals worldwide. The most recent National Health and Nutrition Examinations Survey (NHANES) for 1999-2002 reported that the prevalence of hypertension increases with age and is higher among women than men (29% versus 27.8%). The age-adjusted prevalence of hypertension was 40.5% among non-Hispanic blacks, 27.4% in non-Hispanics, and 25.1% for Mexican Americans. Data from the recent Framingham Heart Study suggested that individuals with normal blood pressure at the age of 55 have a 90% lifetime risk for developing hypertension. Statistically, it is likely that many dental patients will be suffering from hypertension.
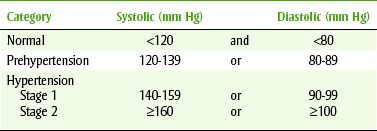
In 2003, the Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 7) presented a new set of clear and concise guidelines that simplified the classification of blood pressure that was based on many new hypertension observational studies and clinical trials. Normal blood pressure is defined as a systolic pressure of less than 120 mm Hg and a diastolic pressure of less than 80 mm Hg. A new category designated prehypertension (120 to 139 mm Hg or 80 to 89 mm Hg) has been added, and people in the range of 130/80 to 139/89 mm Hg are at twice the risk of developing hypertension compared with those with lower values. Stages 2 and 3 were combined to form a new stage 2. Newer information suggests that even the blood pressure within the formerly “normal” blood pressure range is associated with an increase in morbidity and mortality. Most commonly, there are no symptoms associated with hypertension, which is why hypertension is called the “silent killer.” Often, the use of the term hypertension gives patients the impression that it is related to stress or “tension.” Patients need to be aware that high blood pressure occurs without regard to stress or tension. Complications of hypertension affect organs such as the heart, kidney, brain, and retina. After some damage has occurred, symptoms of malfunction become noticeable.
Eventually, a sustained elevated blood pressure damages the body’s organs, so untreated hypertensive patients are more likely to have kidney and heart disease and cardiovascular problems (MI, CVA). These complications are greatly increased with concomitant smoking.
Fortunately, early detection and treatment with drug therapy (Box 15-4) reduces the possibility of damage to vital organs (reduced morbidity) and extends the patient’s lifetime (reduced mortality). Only about 50% of those with known hypertension are properly treated. If hypertensive patients are properly treated (blood pressure is normalized), their risk of complications is equal to that of the patient without hypertension.
Hypertension is generally divided into the following categories based on the cause or progression of the disease:
• Essential hypertension: Approximately 85% to 90% of patients diagnosed with hypertension have essential, idiopathic, or primary hypertension. These terms all stand for hypertension from an unknown cause. Antihypertensive agents are used to control the hypertension in this group of patients. Essential hypertension is divided into stages, depending on the severity of the elevation of the blood pressure (Table 15-5). This is the form usually seen in the dental office.
• Secondary hypertension (identifiable causes): In approximately 10% of hypertensive patients, the cause can be identified and associated with (secondary to) a specific disease process involving the endocrine or renal systems. For example, renal hypertension can result from a narrowed renal artery. Drug therapy, such as steroids, nonsteroidal antiinflammatory drugs (NSAIDs), birth control pills, decongestants, and tricyclic antidepressants, can also produce secondary hypertension. Secondary hypertension can be eliminated by removing the cause, that is, by surgically correcting the renal artery narrowing or discontinuing the offending drug.
• Malignant hypertension: In the third group of hypertensive patients, those with malignant hypertension, blood pressures are very high or rapidly rising and there is usually evidence of retinal and renal damage. The small number of patients in this group must be treated aggressively with antihypertensive agents. Malignant hypertension can develop in about 5% of patients with primary or secondary hypertension.
Patient Evaluation
The evaluation of patients with hypertension has three objectives. They are to assess lifestyle and identify other cardiovascular risk factors or concomitant disorders that may affect prognosis and treatment, to reveal identifiable causes of hypertension, and to assess for the presence or absence of target-organ damage or cardiovascular disease.
Treatment of Hypertension
Pharmacologic management of hypertension involves the algorithm in Figure 15-4, as diastolic pressures become greater than 80 mm Hg. The principle of hypertension treatment is to treat blood pressures less than 140/90 mm Hg or less than 130/80 mm Hg in patients with diabetes or chronic kidney disease:
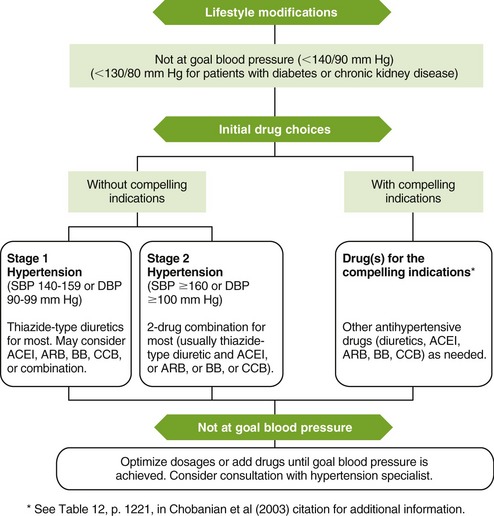
FIGURE 15-4 Algorithm for treatment of hypertension. ACEI, Angiotensin-converting enzyme inhibitor; ARB, angiotensin receptor blocker; BB, β-blocker; CCB, calcium channel blocker; DBP, diastolic blood pressure; SBP, systolic blood pressure. (From Chobanian AV, Bakris GL, Black HR, et al: Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure, Hypertension 42:1206-1252, 2003.)
• Lifestyle modifications are the mainstay of prehypertension therapy and instituted for both stage 1 and stage 2 hypertension. Lifestyle modifications are encouraged even if the patient’s blood pressure is normal. Lifestyle modifications include weight reduction; aerobic physical activity; a diet rich in fruits, vegetables, and low-fat dairy products with reduced content of saturated and total fats; dietary sodium restriction; moderate alcohol consumption; and smoking cessation. If patients with prehypertension present with compelling indications, these indications must be treated.
• Initial drug choices: Once the patient has been diagnosed with either stage 1 or stage 2 hypertension, he or she must be further evaluated for any compelling indications (Table 15-6). The choice of antihypertensive therapy is based on the stage of hypertension and the presence or absence of compelling indications (see Table 15-6 and Figure 15-4). Many people will require two drugs to control the blood pressure. By combining agents, the side effects of individual agents are less and the high blood pressure can be normalized. If compelling indications are present, the compelling indications must be treated and other antihypertensive drugs can be added as needed. Thiazide diuretics have been the basis of most antihypertensive clinical trials and have been virtually unsurpassed in preventing the cardiovascular complications of hypertension. Diuretics also enhance the antihypertensive efficacy of multidrug regimens, are useful in achieving blood pressure control, and are more affordable than other antihypertensive drugs.
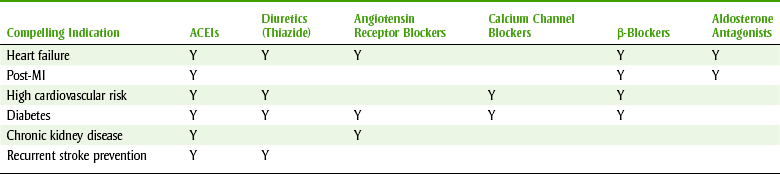
Table 15-7 lists some common antihypertensive agents and their mechanisms of action and side effects, while Figure 15-5 reviews sites and mechanisms of action. The groups recommended for initial use include diuretics, β-blockers, ACEIs, CCBs, and ARBs (Box 15-5). Antihypertensive products may contain one drug or be combinations of more than one drug (see Box 15-4). If the patient is not at blood pressure goal, current drug dosages can be optimized or additional drugs can be added until goal pressure is achieved.
TABLE 15-7
SELECTED ANTIHYPERTENSIVES, THEIR MECHANISMS, AND ADVERSE REACTIONS
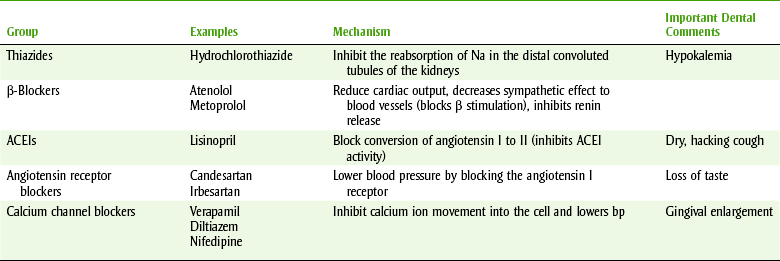
ACEIs, Angiotensin-converting enzyme inhibitors; bp, blood pressure.
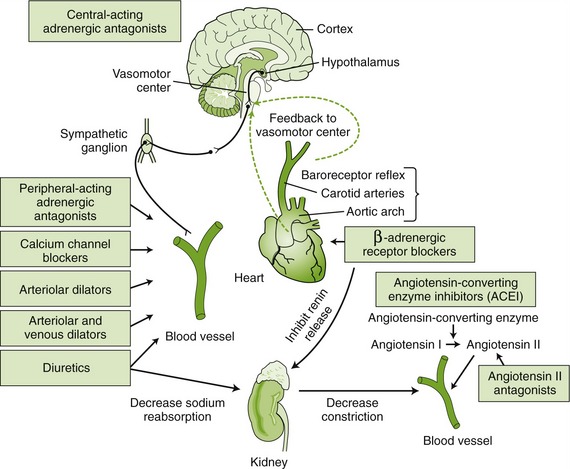
FIGURE 15-5 Site and method of action of various antihypertensive drugs. (Modified from Lewis SM, Heitkemper MM, Dirksen SR: Medical-surgical nursing: assessment and management of clinical problems, ed 7, St Louis, 2007, Mosby.)
The control of blood pressure is an interplay of many factors, and treatment of hypertension is directed at some of the forces that alter blood pressure. The cardiac output and peripheral resistance determine blood pressure. Other changes that affect blood pressure produce changes in these two factors. Because the SNS can affect peripheral resistance, agents that block the SNS reduce blood pressure through their effect on peripheral resistance. Mechanisms of action of the antihypertensive agents attempt to lower blood pressure by their action on either cardiac output or total peripheral resistance.
Regardless of medication use, the blood pressure of each hypertensive patient seen in the dental office should be measured and recorded. Only by recording successive blood pressures for an individual patient can the patient’s blood pressure control be evaluated and any abnormality for a particular patient noted. In addition, because control of blood pressure is so important to patient health, patients should be questioned about compliance with their antihypertensive medication. Abrupt discontinuation of some blood pressure medicines may result in rebound hypertension, which means that the blood pressure rises to a higher level than it was before treatment. Concern for patient total health is based on the fact that it is of little use for a patient to have clean and perfectly restored teeth if that patient has a fatal MI resulting from untreated hypertension.
Diuretic Agents
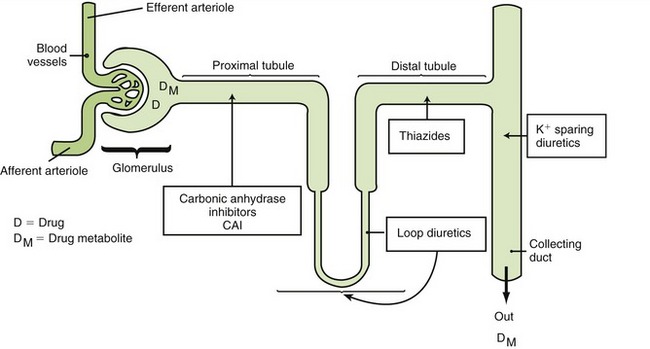
The three major types of diuretics are thiazides (-like), loop, and potassium (K) sparing (Figure 15-6).
THIAZIDE DIURETICS
The thiazide diuretics are among the most commonly used agents for the treatment of hypertension. Hydrochlorothiazide (hye-droe-klor-oh-THYE-a-zide) (HCTZ) is the most commonly used thiazide. Many patients with stage 1 hypertension are treated solely with HCTZ. When other antihypertensive drugs are used, they are often combined with thiazides. Although a large number of thiazide and thiazide-like diuretics are currently available, these agents all have essentially the same pharmacologic effects. Even thiazide-like agents, such as chlorthalidone (klor-THAL-i-doan) (Hygroton), act by a similar mechanism by interfering with the sodium reabsorption in the distal tubule.
Mechanism of Action.: The exact mechanism by which the thiazide diuretics lower blood pressure has not been determined (Table 15-8). The thiazides initially inhibit the reabsorption of sodium from the distal convoluted tubule and part of the ascending loop of Henle of the kidney. Water and chloride ions passively accompany the sodium, producing diuresis. Because more sodium is presented to the site of sodium-potassium exchange, there is also an increase in potassium excretion. If sodium intake is increased, the potassium loss is exacerbated.
TABLE 15-8
MECHANISM OF ACTION OF THE ANTIHYPERTENSIVE AGENTS
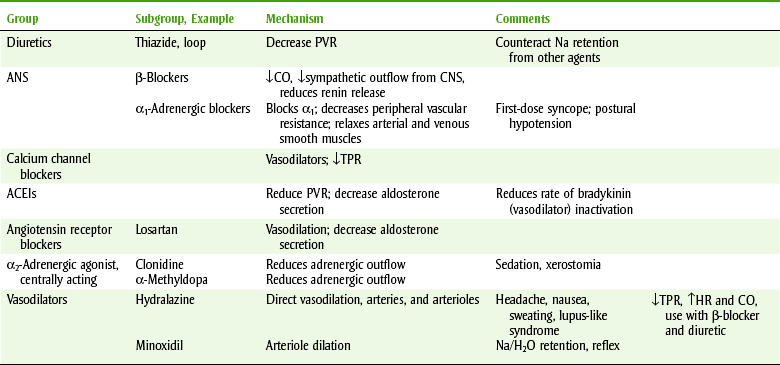
ACEIs, Angiotensin-converting enzyme inhibitors; ANS, autonomic nervous system; CNS, central nervous system; CO, cardiac output; H2O, water; HR, heart rate; NA, sodium; PVR, peripheral vascular resistance; TPR, total peripheral resistance.
The thiazides’ effect on blood pressure may occur because of the following. Initially, thiazide diuretics reduce the extracellular fluid volume because of their natriuretic action. This volume reduction returns to normal with continued therapy, but a slight decrease in interstitial volume may remain. Other effects of the thiazides that may contribute to their antihypertensive effects include changes in sodium and calcium concentrations or a reduced sensitivity to the sympathetic nervous system.
Adverse Reactions.: Common adverse reactions associated with thiazides (Table 15-9) include hypokalemia (secondary to sodium-potassium exchange) and hyperuricemia (inhibits uric acid secretion).
TABLE 15-9
ADVERSE REACTIONS OF THE THIAZIDES
| Problem with | Adverse Reaction | Define |
| Potentiate arrhythmias | Hypokalemia | ↓Potassium |
| Diabetes | Hyperglycemia | ↑Glucose |
| Hyperlipidemia | Hyperlipidemia | ↑Lipids |
| Gout | Hyperuricemia | ↑Uric acid, ↑calcium, ↓magnesium, ↑sodium |
Hyperglycemia, hyperlipidemia, hypercalcemia (promote calcium reabsorption), and anorexia are other side effects. Hyperuricemia is of special concern when the patient has a history of gout. In the patient with diabetes, hyperglycemia, or impaired glucose tolerance, must be managed by diet or insulin alterations. There is a small chance of cross-hypersensitivity (allergy) between the sulfonamide oral medicine (antimicrobial agents) and the thiazides because of the similarity in their structures. The most common oral adverse reaction is xerostomia.
The most important dental drug interaction with the thiazides is interaction with the NSAIDs. NSAIDs can reduce the antihypertensive effect of the thiazide diuretics. This interaction takes a few days to develop, and therefore a few doses of an NSAID can safely be used for acute pain control. A longer duration of use should be undertaken with blood pressure monitoring. Patients often have their own blood pressure monitoring systems at home. Patients are often taking thiazide diuretics for their blood pressure and NSAIDs for arthritis. With chronic use of both agents, their blood pressure medication is adjusted to account for the concurrent use of an NSAID.
Thiazides can cause hypokalemia and can therefore sensitize the myocardium to developing arrhythmias. The potential for arrhythmias is exacerbated in patients taking digoxin, especially if digitalis toxicity is present. Epinephrine, as contained in local anesthetic mixtures, also has arrhythmogenic potential. Therefore in a dental situation in which a patient is taking thiazide diuretics and digitalis toxicity may be present, the epinephrine dose should be limited to the cardiac dose (see Chapter 9). The thiazide diuretics potentiate the action of the other antihypertensives, increasing the potential for hypotension. This drug interaction is used to therapeutic advantage so that lower doses of each drug are needed to control the patient’s blood pressure.
LOOP DIURETICS
Loop diuretics can be considered the “strong cousins” of the thiazides. Furosemide (fur-OH-se-mide) (Lasix), the most commonly used loop diuretic, is the prototype drug. Furosemide acts on the ascending limb of the loop of Henle and has some effect on the distal tubule. Like thiazides, loop diuretics inhibit the reabsorption of sodium with a concurrent loss of fluids. Furosemide’s side effects are similar to those of the thiazides and include hypokalemia and hyperuricemia. However, there is a higher risk of adverse reactions with furosemide because it is much more potent than the thiazide diuretics. Furosemide is used in management of hypertensive patients with HF. Loop diuretics can be used when rapid diuresis is required. As occurs with thiazides, NSAIDs can interfere with furosemide’s antihypertensive action (see comments on HCTZ).
POTASSIUM-SPARING DIURETICS
Potassium-sparing diuretics are “puny” diuretics with “potassium-catching” ability. Individual members of this group have different mechanisms of action, but all have weak diuretic action.
Spironolactone.: Spironolactone (speer-on-oh-LAK-tone) (Aldactone) is chemically similar to aldosterone but competitively antagonizes its action (aldosterone antagonist). The result is sodium excretion through diuresis and loss of fluid volume. However, potassium ion is conserved because some of the potassium is reabsorbed at the expense of sodium in the sodium-potassium exchange system in the distal tubule.
Triamterene.: Triamterene (trye-AM-ter-een) (Dyrenium), also a potassium-sparing diuretic, interferes with potassium-sodium exchange (active transport) in the distal and cortical collecting tubules and the collecting duct by inhibiting sodium-potassium-adenosine triphosphatase (Na-K+-ATPase). The diuresis and potassium conservation that occurs resembles that of spironolactone.
The potassium-sparing diuretics act at different sites in the kidney than do the thiazide diuretics. These two types of diuretics have the opposite effect on potassium loss. A combination product is designed to reduce the amount of potassium loss and prevent hypokalemia. The combination of triamterene and HCTZ (Dyazide, Maxzide) is one of the most often used preparations.
POTASSIUM SALTS
Although the potassium salts are not cardiac drugs, lack of potassium caused by the diuretics must be managed, often with potassium supplementation. Potassium is involved in many important physiologic processes such as nerve impulses; contraction of smooth, cardiac, and skeletal muscles; and maintenance of normal renal function. It is indicated in the treatment of hypokalemia produced by diuretics. It is relatively contraindicated in patients with severe renal impairment or those receiving potassium-sparing diuretics (a few exceptions to this statement exist). The most common adverse reaction of potassium relates to the gastrointestinal tract and includes nausea and abdominal discomfort caused by gastrointestinal irritation. Patients taking potassium supplements should be questioned about their use of diuretics, and the possibility of cardiovascular disease should be explored when a drug history is taken. ACEIs should not be given to persons taking potassium supplements because hyperkalemia occurs with ACEIs. Examples of potassium supplements are K-Dur, K-Tab, Micro-K, K-Lyte, K-Lor, and Klor-Con (K, the element symbol for potassium, is used in their names).
β-Adrenergic Blocking Agents
β-Adrenergic blockers, one group of adrenergic blocking agents, are used often to treat hypertension.
The adrenergic β-receptors are subtyped into β1- and β2-receptors (there also may be a β3-receptor). They have been shown in clinical trials to decrease both the morbidity and mortality related to hypertension.
β1-Receptor stimulation is associated with an increase in heart rate, cardiac contractility, and AV conduction. Stimulation of β2-receptors produces vasodilation in skeletal muscles and bronchodilation in the pulmonary tissues. These receptors are initially described in Chapter 4, which discusses the autonomic nervous system drugs.
Many β-adrenergic blocking drugs are approved for use in the management of hypertension (see Box 15-4). Nonselective or nonspecific β-adrenergic receptor blocking drugs, such as propranolol (proe-PRAN-oh-lole), the prototype, block both β1- and β2-receptors. In usual doses, the selective, or specific, β-adrenergic receptor blocking drugs, such as metoprolol (me-toe-PROE-lole), block the β1-receptors more than the β2-receptors (β1 > β2). At larger doses, receptor selectivity disappears. Pindolol (PIN-doe-lole) and acebutolol (a-se-BYOO-toe-lole) have partial agonist activity and cause some β-stimulation while blocking catecholamine action. The selective β-blockers (β1 > β2) have some advantages in patients who may have preexisting bronchospastic disease, such as asthma, because they do not block the airway’s bronchodilating action (not as likely to result in bronchoconstriction). They are less likely to produce a drug interaction with epinephrine.
β-Adrenergic blockers lower blood pressure primarily by decreasing cardiac output. Other effects that may contribute to their antihypertensive effect include a lowering of plasma renin levels, a reduction in plasma volume and venous return, a decrease in sympathetic outflow from the central nervous system (CNS), and a reduction in peripheral resistance. These drugs are often used as step 2 drugs, either as a single drug or in combination with other antihypertensive drugs.
The side effects of the β-blocking agents include bradycardia, mental depression, and decreased sexual ability. HF and CNS effects, such as confusion, hallucinations, dizziness, and fatigue, have been reported. Gastrointestinal tract effects include diarrhea, nausea, and vomiting. β-Blockers can produce xerostomia (very mild) or worsen a patient’s lipid profile. Exacerbations of asthma, angina, and peripheral vascular disease have been seen.
DENTAL DRUG INTERACTIONS
Nonselective β-blockers can have a drug interaction with epinephrine. Patients pretreated with a nonspecific β-blocker, such as propranolol, and given epinephrine may have a twofold to fourfold increase in vasopressor response (blood pressure goes up more in patients pretreated with β-blockers than in untreated patients), resulting in hypertension. The increased blood pressure triggers, via the vagus nerve, a reflex bradycardia.
The amount of caution required with this drug interaction depends on the patient’s underlying cardiovascular disease, if any increase in blood pressure, and the dose of the β-blocker the patient is taking. In patients with cardiovascular disease or higher blood pressure, the amount of epinephrine given to patients taking nonspecific β-blockers should be limited to the cardiac dose unless careful blood pressure monitoring accompanies the use of larger doses. Neither gingival retraction cord containing epinephrine nor 1 : 50,000 epinephrine should be used. Usual dental doses of epinephrine can be given to patients who are taking β-blockers provided that their blood pressure is under control. Box 15-4 separates the β-blockers into those without intrinsic sympathetic activity and those with intrinsic sympathetic intrinsic activity.
α- AND β-ADRENERGIC BLOCKING DRUG
Labetalol (la-BET-a-lole) (Trandate, Normodyne) is a β-adrenergic receptor blocking drug that also has α-receptor blocking activity. In addition to the typical β-adrenoceptor blocking effects, labetalol also reduces peripheral resistance through its α-blocking action. Labetalol is used either alone or in combination with the diuretics. Side effects and drug interactions are similar to the α- and β-adrenergic blockers.
Calcium Channel Blocking Agents
The common CCBs include the drugs verapamil (ver-AP-a-mil) (Isoptin, Calan), nifedipine (nye-fed-i-peen) (Procardia, Adalat), and diltiazem (dil-TYE-a-zem) (Cardizem). Many CCBs (see Box 15-4) end in the suffix -dipine. These agents are used to treat hypertension and other cardiac conditions such as arrhythmias and angina.
MECHANISM
CCBs inhibit the movement of extracellular calcium ions into cells, including those of the vascular smooth muscle and cardiac cells. The inhibition of calcium ion influx produces vasodilation, which produces coronary vasodilation and reverses vasospasms. By producing systemic vasodilation, the CCBs reduce the afterload on the heart (reduce the total peripheral resistance). These effects are useful in the treatment of both angina pectoris and hypertension.
Today, only long-acting CCBs are used. The short-acting channel blockers were associated with a higher risk of MIs and fatalities, when take at higher doses. This may have been a result of the short-acting CCBs’ ability to suddenly and powerfully lower blood pressure. The heart would overcompensate for this sudden drop by dramatically increasing blood pressure. Long-acting CCBs have a gradual onset of action, which may allow time for the heart to adjust to the drop in blood pressure.
PHARMACOLOGIC EFFECTS
Smooth Muscle Effects.: Vascular smooth muscle is relaxed, and dilation of coronary and peripheral arteries and arterioles occur, reducing preload. Other smooth muscle is relaxed but to a lesser extent. Orthostatic hypotension is uncommon. Some CCBs, such as nifedipine and its relatives, are more specific for this effect.
ADVERSE REACTIONS
Most side effects associated with the CCBs are merely extensions of their pharmacologic effects.
Central Nervous System Effects.: CCBs can produce excessive hypotension, which can cause dizziness and lightheadedness. Dental patients should be warned to rise from the dental chair slowly. Headache can occur in up to 10% to 20% of patients taking CCBs.
Gastrointestinal Effects.: Gastrointestinal side effects include nausea, vomiting, and constipation. Individual CCBs differ in the incidence of these various side effects.
ORAL MANIFESTATIONS
The oral manifestations of the CCBs include xerostomia, dysgeusia, and gingival enlargement (formerly called gingival hyperplasia). Gingival enlargement has been reported most often with nifedipine, but diltiazem, verapamil, and other CCBs have been implicated.
Nifedipine’s manufacturer originally reported the incidence of gingival enlargement as less than 0.5%. Manufacturers of both diltiazem and verapamil have mentioned gingival enlargement as an infrequently reported postmarketing event. Other studies have found the incidence for nifedipine to be 15% to 80%, depending on the criteria used. In one study, diltiazem’s incidence was determined to be 74%. These greatly varying rates of gingival enlargement may be the result of vastly differing criteria used in the studies (e.g., self-report by patients without prompting versus measuring gum changes in all patients). Studies with the highest rates evaluated the incidence of gingival enlargement versus a control group, prospectively.
The gingival enlargement can begin one to several months after starting therapy with a CCB. Some authors have found no relationship between the dose of the drug and the likelihood of a reaction occurring, whereas others indicate that higher doses produce more severe reactions. Like phenytoin enlargement, nifedipine enlargement begins as nodular and firm tissue that bleeds easily on probing. The enlargement begins in the anterior labial dental papillae and can proceed eventually to include the lingual and palatal gingiva. The hyperplastic interdental papillae can eventually extend onto crown surfaces, interfering with the ability to chew.
Detailed oral hygiene instructions and more frequent recall appointments to reduce plaque load have been said to reduce this enlargement, but no well-controlled studies have confirmed this suspicion. The patient may be told to maintain scrupulous oral hygiene until more information is available.
On discontinuation of the CCB or switching to a drug outside the CCB group, the gingival enlargement usually reverts to normal tissue and does not reappear. This may take weeks to months. If drug therapy cannot be discontinued because of the severity of the patient’s cardiac condition, a gingivectomy or gingivoplasty may be required. Changing to another CCB does not appear to result in reversal of the enlargement.
DENTAL DRUG INTERACTIONS
The CCBs are one of the few antihypertensive groups whose effect is not reduced by the NSAIDs. Both nausea and constipation, side effects of the CCBs, could be additive with the side effects produced by NSAIDs (e.g., ibuprofen) (nausea) and the opioids (e.g., codeine) (constipation).
Angiotensin-Related Agents
ANGIOTENSIN-CONVERTING ENZYME INHIBITORS
ACEIs prevent the conversion of angiotensin I to angiotensin II. ACEI drugs are commonly used as antihypertensives. Examples include captopril (KAP-toe-pril) (Capoten), enalapril (e-NAL-a-pril) (Vasotec), and lisinopril (lyse-IN-oh-pril) (Prinivil, Zestril). Many ACEIs (see Box 15-4) end in the suffix -pril.
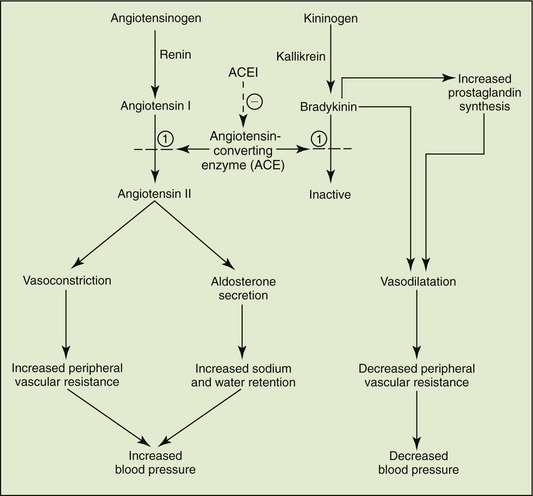
Mechanism.: A complex but important homeostatic mechanism involved in maintaining blood pressure is the renin-angiotensin-aldosterone system. This system adjusts the quantity of sodium and water retained (circulatory volume) and the peripheral resistance (blood vessels). When the kidney senses a decrease in blood pressure or flow, it releases renin, which catalyzes the conversion of angiotensinogen (inactive precursor) to angiotensin I. A second enzyme, ACE, converts angiotensin I to angiotensin II. This is the enzyme that is blocked by ACEIs (Figure 15-7). Angiotensin II produces vasoconstriction (increasing peripheral vascular resistance) and stimulates the adrenal cortex to release aldosterone, facilitating water retention. By blocking these events, the blood pressure is lowered. Cardiac output and heart rate are relatively unaffected. ACEIs retard the progression of diabetic nephropathy whether hypertension is present or not.
Adverse Reactions.: The two most common kinds of adverse reactions associated with the ACEIs are those related to the cardiovascular system and CNS (Box 15-6).
Cardiovascular Effects.: Hypotension has produced dizziness, lightheadedness, and fainting. Tachycardia and chest pain have been noted.
Central Nervous System Effects.: CNS side effects may include dizziness, insomnia, fatigue, and headache.
Respiratory Effects.: An increase in upper respiratory symptoms, including a dry, hacking cough can occur. ACEIs can produce a dry cough, in up to 10% of patients, and this cough can occur within the first week of therapy and disappears after withdrawal of the drug. The cough begins as a tickle in the throat, leading to a dry, nonproductive, and persistent cough that may be worse at night or in the supine position. It occurs because the ACE also inactivates bradykinin, a potent stimulator of allergic reactions, including cough. The blood levels of bradykinin rise because the ACEIs are blocking the enzyme that normally destroys bradykinin.
Hyperkalemia.: ACEIs can cause hyperkalemia, and potassium supplements and potassium-sparing diuretics should not be used with these drugs.
Other Effects:: ACEIs should not be given to women who could be pregnant or become pregnant because of the risk of teratogenicity. Rarely, pancreatitis, with symptoms of abdominal pain, and abdominal distention have occurred. Proteinuria is more common in patients taking higher doses or who have renal impairment.
Oral Adverse Reactions.: Dysgeusia, an altered sense of taste, is most commonly reported in patients taking captopril (6%). The loss of taste is usually reversible after a few months, even with continued drug treatment.
Autoimmune oral lesions, such as lichenoid or pemphigoid reactions, may produce oral manifestations. This reaction may have a photosensitivity factor.
Dental Drug Interactions.: The antihypertensive effectiveness of ACEIs is reduced by administration of the NSAIDs. A few doses of an NSAID are of little concern, but chronic administration for several days might result in an increase in the patient’s blood pressure. The ACEIs may be used alone or in combination with a β-blocker, thiazide diuretic, or CCB. These drugs are commonly prescribed, and the dental team will treat many patients taking one or more of these agents.
ANGIOTENSIN RECEPTOR BLOCKERS
The ARBs act by attaching to the angiotensin II receptor and blocking the effect of angiotensin II. ARBs end with the suffix –artan. Losartan (loe-SAR-tan) (Cozaar), is the prototype. Losartan has a high affinity and selectivity for the type 1 angiotensin II receptor. It blocks the vasoconstrictor and aldosterone-secreting effects of angiotensin II. An increase in plasma renin level follows, thus causing vasodilation, decreased sodium and water retention, and reduction in blood pressure.
Adverse Reactions.: Because ARBs work by blocking angiotensin II at its receptor, they are more specific than ACEIs and may be expected to have fewer adverse reactions.
Central Nervous System Effects.: CNS effects can include dizziness, fatigue, insomnia, and headache.
Renin Inhibitors
Aliskiren (Tekturna) is the first of a new class of drugs approved by the FDA for the treatment of hypertension. It is indicated for oral use as either monotherapy or in combination with other antihypertensive drugs. Aliskiren is a renin inhibitor that works by binding to renin which then reduces the levels of angiotensin I, angiotensin I, and aldosterone. Unlike ACEIs and ARBs, aliskiren does not appear to increase plasma renin activity. The most commonly reported adverse reactions include headache, dizziness, fatigue, cough, and upper respiratory tract infections. There have been reports of angioedema of the head and neck and hypotension.
α1-Adrenergic Blocking Agents
The adrenergic blockers include the α-blockers and β-blockers, which were discussed earlier. Two α-receptor subtypes, α1 and α2, have been identified (see Box 15-4). Doxazosin (doks-AYE-zoe-sin) (Cardura) and terazosin (ter-AY-zoe-sin) (Hytrin) are examples of selective α1-adrenergic blocking drugs.
MECHANISM
The α1-receptors, located on postsynaptic receptor tissues, produce vasoconstriction and increase peripheral resistance when stimulated. The α1-blocking agents produce peripheral vasodilation in the arterioles and venules that decreases peripheral vascular resistance. They have little effect on cardiac output or renal blood flow. They are more effective when combined with diuretics or β-blockers.
α1-Adrenergic blockers result in a reduction in urethral resistance and pressure, bladder outlet resistance, and urinary symptoms. This effect accounts for their use in management of older males who have an enlarged prostate gland. Surgery can often be avoided in those patients who are managed by drug therapy. If a man has both hypertension and benign prostatic hypertrophy (BPH), then one can “kill two birds with one stone.”
ADVERSE REACTIONS
Orthostatic Hypotension.: Orthostatic hypotension can result in dizziness or syncope. A “first-dose orthostatic hypotensive reaction” sometimes occurs with the initial dose or with changes in the dose of doxazosin. Syncope is more likely to occur when the patient is volume depleted or sodium restricted. Both exercise and alcohol may exaggerate the effect.
DENTAL DRUG INTERACTIONS
Nonsteroidal Antiinflammatory Drugs.: NSAIDs, especially indomethacin, can reduce the antihypertensive effect of the α1-blockers (Box 15-7). They produce this effect by inhibiting renal prostaglandin synthesis or causing sodium and fluid retention.
Epinephrine.: The sympathomimetics can increase the antihypertensive effects of doxazosin. The α1-blockers prevent the α1-agonist effects (vasoconstriction) of epinephrine, leaving the β1- and β2-agonist effects (vasodilation) to predominate. The combined vasodilation can result in severe hypotension and reflex tachycardia.
Other Antihypertensive Agents
These other antihypertensive agents are used less than those previously described because they generally have more or less tolerated adverse reactions. Clonidine is used in some patients in whom the previously discussed antihypertensives are ineffective.
CLONIDINE
Clonidine (KLON-i-deen) (Catapres) is a CNS-mediated (centrally acting) antihypertensive drug. Clonidine reduces peripheral resistance through a CNS-mediated action on the α-receptor. Stimulation of presynaptic central α2-adrenergic receptors results in decreased sympathetic outflow. Thus clonidine reduces heart rate, cardiac output, and total peripheral resistance. It is indicated for the management of essential hypertension and can be administered orally or by a transdermal patch (Catapres-TTS).
Adverse Reactions.: Adverse effects include a high incidence of sedation and dizziness. Rapid elevation of blood pressure has occurred with abrupt discontinuation. CNS depressants used in dental conscious-sedation techniques may contribute to postural hypotension when used in a patient taking clonidine.
OTHER CENTRALLY ACTING ANTIHYPERTENSIVE AGENTS
Two other centrally acting antihypertensive drugs, methyldopa (meth-ill-DOE-pa) (Aldomet) and guanabenz (GWAHN-a-benz) (Wytensin), are also available. Adverse effects and indications for use are similar to those of clonidine. The centrally acting antihypertensive drugs may be combined with diuretics in essential hypertension management.
GUANETHIDINE
Guanethidine’s (gwahn-ETH-i-deen) (Ismelin) severe adverse reactions severely limit its use. It acts by blocking the release of norepinephrine from the sympathetic nerve endings. It also depletes the amount of norepinephrine stored in synaptic vesicles. Both actions decrease the amount of norepinephrine that can be released with sympathetic stimulation, thereby reducing SNS tone and decreasing blood pressure (see Figure 15-5). Guanethidine has a delayed onset of action, and its effects can persist for at least 2 weeks after it is discontinued.
Guanethidine causes severe postural and exertional hypotension, which is exacerbated by anything that causes vasodilation, such as warm weather, ingestion of alcohol, or exercise. Hypotension is most severe after the patient has spent several hours in a supine position, such as in the dental chair. Other adverse reactions include diarrhea, interference with ejaculation, and cardiac problems. Muscle weakness has also been reported.
RESERPINE
Originally used as a tranquilizer, reserpine (re-SER-peen) is currently used in low doses as an antihypertensive agent. Like guanethidine, reserpine depletes norepinephrine from the sympathetic nerve endings and can accumulate in the body. Adverse reactions include diarrhea, bad dreams, sedation, and even psychic depression leading to suicide. Reserpine increases the production of stomach acid and aggravates peptic ulcers. It can also produce galactorrhea, breast engorgement, and gynecomastia.
HYDRALAZINE
Hydralazine (hye-DRAL-a-zeen) (Apresoline) exerts its antihypertensive effect by acting directly on the arterioles to reduce peripheral resistance (vasodilation). At the same time, a rise in heart rate and output occurs. Propranolol is often administered concurrently to reduce the reflex tachycardia and increase cardiac output. Hydralazine is often used in combination with the thiazides or other antihypertensive agents. Both diastolic and systolic blood pressures are reduced proportionately, and there is little orthostatic hypotension. The most commonly reported side effects associated with hydralazine are cardiac arrhythmias, angina, headache, and dizziness. A serious toxic reaction produces symptoms like those of systemic lupus erythematosus (lupus-like reaction).
Management of the Dental Patient Taking Antihypertensive Agents
Although the antihypertensive drugs cause a variety of adverse reactions, many of them exert similar actions that can alter dental treatment (Box 15-8). Because the hypertension of patients taking antihypertensive medications may or may not be controlled, the blood pressure of each patient should be measured on each visit to the dental office. Not uncommonly, a patient whose blood pressure is “normal” on one visit might be found to be hypotensive or hypertensive on a subsequent visit.
ADVERSE REACTIONS
Xerostomia.: Dry mouth is an adverse reaction associated with several of the antihypertensives. If the dental health care worker notices this effect, it is imperative to discuss with the patient methods used to alleviate this discomfort.
Dysgeusia.: With some antihypertensives, an altered sense of taste may occur, which may be related to xerostomia.
Gingival Enlargement.: CCBs have the ability to produce gingival enlargement. Meticulous oral hygiene and frequent recall appointments may minimize this effect.
Orthostatic Hypotension.: When a patient has been in a supine position and suddenly rises to an upright position, a sudden fall in blood pressure may occur. This side effect is called orthostatic hypotension. Patients taking antihypertensive agents who have been supine for some time should be slowly raised from that position. They should dangle their legs over the side of the chair or bed and wiggle them before rising to the standing position. The patient should be supported for a few steps to prevent syncope. Guanethidine causes this problem often; other agents produce variable amounts of orthostatic hypotension.
Constipation.: Some antihypertensive agents (verapamil) can cause constipation, which could be additive with the constipation produced by the opioids. An increase in dietary fiber, a bulk laxative, or a stool softener may be considered if an opioid is prescribed for a patient receiving a constipation-producing antihypertensive medication.
ANTIHYPERLIPIDEMIC AGENTS
Hyperlipidemia and hyperlipoproteinemia are elevations of plasma lipid concentrations above accepted normal values. These metabolic disorders include elevations in cholesterol and/or triglycerides and are associated with the development of arteriosclerosis, although the exact correlation is unknown. There are many different types of hyperlipoproteinemias that result in elevations of chylomicrons, very-low-density lipoproteins (VLDLs), low-density lipoproteins (LDLs), or combinations of these.
Foam cells in the actual blood vessel, which are more prevalent in uncontrolled diabetes, become filled with cholesterol esters. Accumulation of these esters leads to deposition of lipids in the arteries. Collagen and fibrin also accumulate, occluding the vessels. Atherosclerosis can lead to coronary artery disease, MI, and cerebral arterial disease. The endothelium over the plaques activates platelets, leading to the formation of thrombi and clinical symptoms. Additional risk factors for development of complications include untreated hypertension, smoking, obesity, and alcohol use.
Cholesterol and other plasma lipids are transported in the blood in the form of protein complexes (lipoproteins) to make them more soluble in plasma. LDLs are referred to as “bad cholesterol” because they deposit excess cholesterol in artery walls and are considered to be the most dangerous. High-density lipoproteins (HDLs) are referred to as “good cholesterol” because they have the lowest cholesterol content and are considered to be beneficial (they carry cholesterol away from the blood vessels).
The first line of treatment of hyperlipoproteinemia is increasing exercise and decreasing saturated fat and cholesterol from the diet. Depending on the severity of the condition and the success of the patient in making permanent lifestyle changes, drug therapy may be considered.
Therapy of hyperlipoproteinemia is directed at lowering the level of LDL-cholesterol (LDL-C). Drugs are available that reduce hyperlipoproteinemias: some more specific for cholesterol and some more specific for the triglycerides. Antihyperlipidemic drugs include the bile acid–binding resins, niacin, gemfibrozil, and 3-hydroxy-3-methylglutaryl coenzyme A (HMG Co-A) reductase inhibitors (Table 15-10). The HMG Co-A reductase inhibitors are the most commonly used antihyperlipidemics.
TABLE 15-10
EFFECT OF ANTIHYPERLIPIDEMIC AGENTS ON SERUM LIPIDS
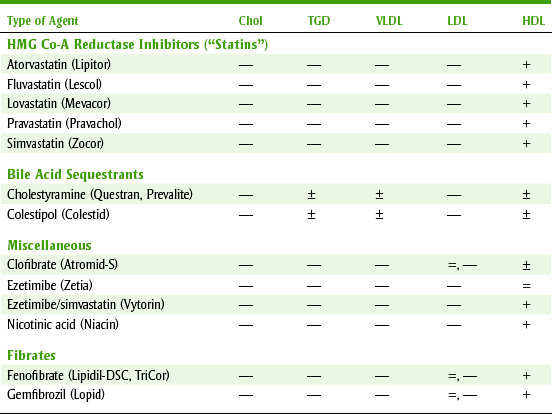
Chol, Cholesterol; HDL, high-density lipoproteins; HMG Co-A, 3-hydroxy-3-methylglutaryl coenzyme A; LDL, low-density lipoproteins; TGD, triglycerides; VLDL, very-low-density lipoproteins.
3-Hydroxy-3-Methylglutaryl Coenzyme A Reductase Inhibitors
The HMG Co-A reductase inhibitors are often referred to as the “statins” because their generic names end in that suffix. Their side effect profile is more desirable than any of the other drugs used to treat hyperlipidemias. However, their use is contraindicated in women who are pregnant or nursing. They have a Pregnancy Risk Factor of X.
Lovastatin (LOE-va-sta-tin) (Mevacor) was the first of the statins. The statins lower cholesterol levels by inhibiting HMG-CoA reductase, the rate-limiting enzyme in cholesterol synthesis. They may work because they are structural analogs of HMG Co-A reductase and thereby inhibit that enzyme. Another possible mechanism of the HMG Co-A reductase inhibitors may relate to the increase in the number of LDL receptors that occurs. The effectiveness of the HMG Co-A reductase inhibitors should be monitored by a lipid panel repeated once or twice a year.
ADVERSE EFFECTS
Adverse effects of HMG Co-A reductase inhibitors include gastrointestinal complaints such as stomachache, constipation, diarrhea, and gas. Other side effects are myositis, skin rash, impotence, hepatotoxicity, blurred vision, and lens (in the eye) opacities. Myositis results in complaints of muscle pain. Liver function tests should be performed because of the small potential for hepatotoxicity. These agents can increase the anticoagulant effect of warfarin.
INHIBITORS OF INTESTINAL ABSORPTION OF CHOLESTEROL
Ezetimibe (Zetia) was most recently approved to treat elevated cholesterol levels and low HDL-cholesterol (HDL-C) levels. This drug works by inhibiting the intestinal absorption of cholesterol. This drug can be used alone or in combination with an HMG-CoA reductase inhibitor. It currently comes in combination with simvastatin (HMG-CoA reductase inhibitor) to treat cholesterol from two different mechanisms of action. This drug decreases total cholesterol, LDL-C, and increases HDL-C levels. Side effects include fatigue, abdominal pain, and diarrhea.
Most recently, the ENHANCE trial has shown that there is little difference in the cholesterol lowering abilities of Vytorin (ezetimibe/simvastatin) and simvastatin alone. Vytorin was found to lower LDL-C, but it had little effect on plaque buildup in the arteries. The researchers went on to recommend that Vytorin and Zetia should only be used if a person fails to achieve adequate cholesterol control with a statin or cannot tolerate the adverse reactions of statins.
Niacin
Niacin (NYE-a-sin) (nicotinic acid) is a B vitamin (see Chapter 12). In larger doses, niacin produces a therapeutic effect. It lowers cholesterol levels by inhibiting the secretion of VLDLs without accumulation of triglycerides in the liver. This reduces LDL synthesis. At these larger doses, niacin commonly produces cutaneous flushing (especially the face and neck) and a sensation of warmth after each dose. The prostaglandin-mediated flushing is blocked by pretreatment with 0.3 gm of aspirin taken one-half hour before taking niacin or by taking one tablet of ibuprofen daily. This side effect can be minimized by beginning with low doses of niacin and slowly increasing the dose over a period of weeks. Increasing the dose of niacin enough to produce a decrease in lipids without having intolerable adverse effects is challenging. Hyperuricemia can occur and can be treated with allopurinol. Allergic reactions, cholestasis, and hepatotoxicity have been reported.
Cholestyramine
The bile acid–binding resins, cholestyramine (koe-less-TIR-a-meen) (Questran) and colestipol (koe-LES-ti-pole) (Colestid), lower cholesterol concentrations because cholesterol is a precursor that is required for the synthesis of the new bile acids. When the resins bind with the bile acids, they produce an insoluble product that is lost through the gastrointestinal tract. The bile acids, which must be replaced, use up cholesterol, thereby reducing cholesterol levels. Adverse reactions relate to the gastrointestinal tract and include constipation and bloating, but serious side effects are infrequent. These drugs are poorly tolerated because of their effects on the gastrointestinal tract and poor taste. Patients often abandon their use.
Gemfibrozil
Gemfibrozil (gem-FI-broe-zil) (Lopid) is used to treat hyperlipidemias, especially when triglycerides are elevated. It works by increasing lipolysis of triglycerides, decreasing lipolysis in adipose tissue, and inhibiting secretion of VLDLs from the liver. This drug causes fewer gastrointestinal complaints than the bile acid–binding drugs, but it can promote gallstone formation (cholelithiasis). An altered sense of taste and hyperglycemia have been reported. Hematologic and liver function should be monitored routinely. This drug should not be given with statins because of the increased risk for muscle cramping, myopathy, and rhabdomyolysis.
Dental Implications
Patients who take antihyperlipidemic agents are at a higher risk for developing hypertension and coronary artery disease. These patients are at increased risk for MIs and cardiac arrest. Dental health care workers should be prepared to handle such emergencies. The patient’s blood pressure and pulse rate should be taken before each appointment and recorded in the dental chart. If an emergency occurs, it is important to know the pre-emergency blood pressure and heart rate so that these can be compared with the current measurements. Because gastrointestinal and liver abnormalities are side effects associated with many of these drugs, their tolerance to the agents taken should be determined before dental drugs are prescribed or suggested. The small possibility of liver abnormalities requires laboratory testing for abnormal liver function.
DRUGS THAT AFFECT BLOOD COAGULATION
Anticoagulants are drugs that in some way interfere with coagulation. The first anticoagulant was discovered when cows that ingested spoiled sweet clover silage became hemorrhagic. The toxic agent in the clover was found to be dicumarol, and warfarin is a close relative. Warfarin has been used as a rodenticide. When the rats eat the warfarin, they begin to bleed and eventually die. Therapeutically, anticoagulants are administered in an attempt to prevent clotting. Examples of indications for warfarin are after an MI, thrombophlebitis, or to prevent a stroke. Warfarin (Coumadin) is the most important oral anticoagulant and is the one used almost exclusively in therapy.
HEMOSTASIS
Hemostasis is a normal mechanism in the body that is designed to prevent the loss of blood after injury to a blood vessel. The leaking vessel is plugged by a complicated process of clot formation. In the presence of a vascular injury, the entire clotting mechanism is initiated. Thromboplastin; factors V, VII, and X; and calcium ions form prothrombin, thrombin, and finally fibrinogen and fibrin (Figure 15-8). The fibrin, along with vascular spasms, platelets, and red blood cells, quickly forms the clot.
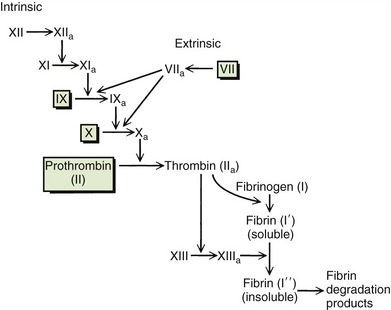
FIGURE 15-8 Intrinsic and extrinsic systems of blood coagulation. The boxed clotting factors (II [prothrombin], VII [extrinsic], IX [intrinsic], and X) depend on vitamin K for their synthesis. Warfarin inhibits these four clotting factors.
If the blood vessel’s interior remains smooth, circulating blood does not clot. However, if internal injury to the vessel occurs and a roughened surface develops, intravascular clotting will take place. This process involves an intrinsic prothrombin activator that includes a platelet factor, factor V, factors VIII through XII, and calcium ions. The prothrombin activator, which was formerly called thromboplastin, converts prothrombin to thrombin. Thrombin then converts fibrinogen to fibrin, and clot formation occurs.
Many of the factors required in the clotting process are synthesized in the liver. Prothrombin (II) and factors VII, IX, and X require vitamin K for synthesis. Because warfarin antagonizes vitamin K, it interferes with the synthesis of four clotting factors to produce an anticoagulant effect.
In certain diseases, intravascular clots can form. These clots, or thrombi, may break off, forming emboli that lodge in the smaller vessels of major organs, such as the heart, brain, and lungs, producing severe and even fatal thromboembolic disease. Anticoagulant therapy attempts to reduce intravascular clotting and prevent life-threatening situations. Each person’s anticoagulant therapy must be adjusted to suit his or her needs. If the dose of the anticoagulant is too large, hemorrhage may occur. If the dose is too small, the danger of embolism remains.
WARFARIN
Warfarin (WAR-far-in) (Coumadin) is an oral anticoagulant (interferes with coagulation). It blocks γ-carboxylation of glutamate residues in the synthesis of factors VII, IX, and X; prothrombin (II); and endogenous anticoagulant protein C. Instead of forming the factors, incomplete and inactive molecules are formed that do not function properly. Warfarin also prevents the metabolism of the inactive vitamin K epoxide back to its active form.
Warfarin’s pharmacologic effect is delayed when therapy begins and ends. This latent period in the onset of action of warfarin occurs for the following two reasons:
1. The blood level of the warfarin accumulates over time until it plateaus or reaches steady state. The maximum effect for one dose occurs after five half-lives = 5 = 42 hours = 210 hours (9 days).
2. Endogenous clotting factors II, VII, IX, and X have half-lives that are 60, 6, 24, and 40 hours, respectively. They must become depleted before the anticoagulant effect is maximized.
When reducing the dose of warfarin or discontinuing it, there will be a delay in the change in the effect because the drug must be metabolized to inactivate it and the clotting factors must be synthesized again.
Monitoring.: Warfarin’s effect is monitored using the international normalized ratio (INR). The INR is a function of the prothrombin time (PT) of the patient, PT of control, and the international sensitivity index (ISI). The ISI is a number that is a function of the potency of the specific (human or rabbit) thromboplastin used in the particular laboratory. The advantage of the INR over the PT ratio is that the INR value from any laboratory in the world can be compared, whereas the PT ratio varies among laboratories. The formula for the INR is seen in Figure 15-9.

The therapeutic target INR (number at which the provider is trying to keep the patient’s INR) for most indications, such as thrombophlebitis or AF, is between 2 and 3. For patients with a prosthetic heart valve, the target INR is between 2.5 and 3.5. The INR can range from 1 (INR without drug effect) to 4, although with overdose it can reach higher levels.
In the past, the laboratory test that was used to monitor warfarin was the PT ratio. The prothrombin time ratio (PTr) is the ratio of the PTpatient/PTcontrol. Some laboratories are still reporting the PTr. PTr ranges from 1 (PTr without drug) to 2.5 or higher. The target numbers for the PTr and the INR are not interchangeable.
Because warfarin is orally effective and less expensive than heparin, it is used in long-term treatment of thromboembolic diseases such as thrombophlebitis and MI.
Adverse Reactions.: The most common adverse effects associated with the oral anticoagulants are various forms of bleeding, including hemorrhage. Because of its narrow therapeutic index and because of numerous drug interactions, serious reactions can easily occur. One should look for petechial hemorrhages in the oral cavity. Ecchymoses can occur, even without concomitant trauma. With mild trauma, these effects may be seen in the oral cavity. Studies compared effects of lower and higher doses of warfarin in clot prevention. They found no advantage in use of higher doses but found an increase in adverse reactions. Dosing of warfarin is now titrated to a lower INR than in the past.
Aspirin.: The most serious drug interaction of warfarin is with aspirin (Table 15-11). Patients taking warfarin should not be given aspirin or aspirin-containing products (“cold preparations”) because bleeding episodes or fatal hemorrhages can result. Aspirin interacts with warfarin in several ways. First, aspirin causes hypoprothrombinemia and alters platelet adhesiveness (see Chapter 5). These effects in themselves reduce clotting ability. Aspirin can also irritate the gastrointestinal tract, which might bleed more in a patient taking warfarin.
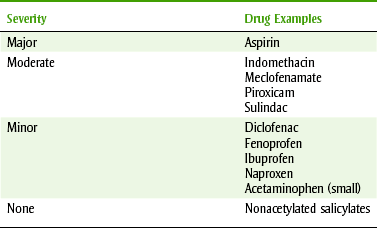
Another factor in the aspirin-warfarin interaction is related to protein binding of drugs. Warfarin is more than 99% bound to plasma proteins and about 1% free drug. Only the free drug (<1%) exerts the pharmacologic effect of decreased clotting. Because warfarin and aspirin compete for the same plasma protein–binding site, aspirin displaces the bound warfarin, thereby increasing the proportion of free (unbound) warfarin and hence potentiating its activity. Only the free drug in the blood exerts a pharmacologic effect. The bound drug is merely a reservoir for the drug. Even a small increase in free warfarin can lead to a large increase in effect, leading to dire consequences, including hemorrhage. If an NSAID is to be used in a patient taking warfarin, ibuprofen or naproxen should be prescribed. These agents have only a minor interaction with warfarin, and a few doses can be given in the patient with an INR within the therapeutic target.
Acetaminophen.: Acetaminophen and its effect on warfarin were prospectively analyzed. Hylek and colleagues studied patients taking warfarin in an attempt to identify factors that were associated with an INR above 6 (therapeutic INR = 2 to 3.5). A statistically significant association was found between acetaminophen use and the abnormal elevation of the INR. With higher doses of acetaminophen (9 gm/wk) there was a tenfold increase in the likelihood of presenting with an abnormal INR. Whether there is a causal relationship between acetaminophen use and warfarin, toxicity has not been proved. Managing patients taking warfarin who need analgesics may require more frequent monitoring of the INR, especially with intermittent use.
Antibiotics.: Antibiotics can also potentiate the effect of warfarin. Antibiotics reduce the bacterial flora in the gastrointestinal tract that normally synthesize vitamin K. This results in a decrease in vitamin K absorbed. Because warfarin also inhibits vitamin K–dependent factors, there is an added anticoagulant effect. If an antibiotic is to be used with warfarin (Table 15-12), clindamycin has no effect; doxycycline, tetracycline, and amoxicillin have small effect; and erythromycin and metronidazole have the greatest effect on altering warfarin’s anticoagulant action. If the antibiotic is used for prophylaxis before a dental procedure (one dose), the interaction would not have a chance to develop.
TABLE 15-12
WARFARIN AND ANTIINFECTIVE DRUG INTERACTIONS
| Most | Some | Least |
| Metronidazole | Tetracycline | Clindamycin |
| Erythromycin | Doxycycline | |
| Ketoconazole (-azole antifungals) | Penicillin, ampicillin, amoxicillin, dicloxacillin | |
| Cephalosporins | Quinolones |
Induction of the microsomal enzymes increases warfarin’s metabolism and reduces its effect. Phenobarbital induces the liver microsomal enzymes that would normally destroy the anticoagulant. Alcohol’s effect on warfarin depends on the pattern of alcohol use. With chronic alcohol ingestion, the metabolism of warfarin is stimulated. Acute alcohol intoxication inhibits the metabolism of warfarin. Other agents that inhibit the metabolism of warfarin include cimetidine, disulfiram, and metronidazole.
Management of the Dental Patient Taking Warfarin.: Box 15-9 summarizes the management of dental patients taking warfarin.
Bleeding.: Before any dental procedure is begun, the patient should be interviewed to determine whether any symptoms relating to bleeding have been noted. Many surgical procedures can be carried out on a patient receiving therapeutic doses of anticoagulants (Table 15-13). One should check with the prescribing physician to obtain the patient’s INR or PTr and the date the blood for the test was drawn. A higher INR can be tolerated if local measures are added. When a decision is made to change the dose of warfarin, the risk of lowering the dose of warfarin must be weighed against the benefit of lowering the dose of warfarin (Box 15-10). Discontinuing warfarin for a few days without knowledge of the patient’s INR could expose the patient to an increased risk of clotting. If the patient does not need the anticoagulant, then it can be permanently discontinued. If the patient needs anticoagulation, then the risk of intravascular clotting in these patients should not be underestimated.

TABLE 15-13 SAFETY OF OUTPATIENT DENTAL TREATMENT FOR PATIENTS RECEIVING WARFARIN (COUMADIN) ANTICOAGULANT THERAPY Rights were not granted to include this table in electronic media. Please refer to the printed book. From Hermann WW, Konzelman JL Jr, Sutley SH: Current perspectives on dental patients receiving coumarin anticoagulant therapy, J Am Dent Assoc 128(3):327, 1997. Copyright © 1997 American Dental Association. All rights reserved. Adapted 2009 with permission. American Dental Association
Analgesics.: Aspirin and aspirin-containing products are absolutely contraindicated in patients taking warfarin unless the patient is taking one aspirin tablet daily for its anticoagulant effect. In this case, the monitoring of warfarin effect is done while the patient is taking aspirin. Acetaminophen or any opioid alone or together may be substituted if analgesia is desired. A few doses of ibuprofen or naproxen may be safely used if there is no other contraindication to their use.
HEPARIN
Heparin (HEP-a-rin) is one of the most commonly used anticoagulant agents in hospitalized patients. Because it must be given by injection and cannot be used orally, its outpatient use is essentially nonexistent. Newer heparins, termed low-molecular-weight heparins, are being used, but until an oral dose form is developed, use of these heparins will be limited. Because its effect begins quickly, heparin is the first anticoagulant given to hospitalized patients with excessive clotting. Patients who might receive heparin are those with MI, stroke (embolism), or thrombophlebitis. When the heparin is started (as soon as possible), warfarin is also begun. Because warfarin’s effect has a latent period, the heparin can provide immediate anticoagulant effect while the warfarin is building up. The effect of an overdose of heparin is antagonized by protamine sulfate, which immediately reverses its anticoagulant effects.
CLOPIDOGREL
The drug clopidogrel (Plavix) is an inhibitor of adenosine diphosphate (ADP)–induced platelet aggregation, which results in prolonged bleeding time. Clopidogrel is indicated for patients with recent history of MI or stroke, established peripheral arterial disease, and for those patients with acute coronary artery syndrome. Its major side effects include thrombotic thrombocytopenic purpura (TTP) and increased bleeding. TTP can occur within as little as 2 weeks of beginning therapy. TTP is characterized by thrombocytopenia seen on peripheral smear, neurologic findings, renal dysfunction, and fever. It does not alter PT or INR values.
Clopidogrel can be taken with or without food. Patients taking this drug should be carefully managed in the dental office because of the risk for increased bleeding. NSAIDs should be avoided because of the risk for gastrointestinal bleeding. Aspirin use should also be avoided. Patients may be taking a combination of clopidogrel and aspirin to treat acute coronary syndrome. This should only be done under a doctor’s supervision. NSAID use should especially be avoided in these patients.
TICLOPIDINE
The drug ticlopidine (tye-KLOE-pi-deen) (Ticlid) is an irreversible inhibitor of ADP-induced platelet aggregation, which results in prolonged bleeding time. Ticlopidine is indicated to decrease thrombotic stroke in patients with previous stroke. It is used in patients who are intolerant of aspirin. Its major side effect, neutropenia, is monitored by appropriate blood tests. An increase in infections could signal neutropenia. It does not alter the PT or INR.
Ticlopidine is taken with food because it can produce diarrhea, nausea, and vomiting. Patients taking ticlopidine have increased bleeding after trauma or surgery. It takes 10 to 14 days to eliminate the bleeding effect. Bleeding can lead to ecchymoses, epistaxis, and perioperative bleed. For emergency surgery, injectable methylprednisolone can reverse the prolonged bleeding to normal in a few hours. NSAIDs should be avoided because gastrointestinal bleeding can result. Patients taking this drug should be carefully managed in the dental office, but no laboratory tests are used to monitor ticlopidine.
STREPTOKINASE AND ALTEPLASE
Enzymes, called clot busters, such as streptokinase (strep-toe-KYE-nase) (Streptase, Kabikinase) and the recombinant tissue-type plasminogen activator alteplase (AL-ti-plase) (tPA, Activase), are sometimes used in the therapy of deep vein thrombosis, arterial thrombosis, pulmonary embolism, and acute coronary artery thrombosis associated with MI. These may appropriately be termed thrombolytic drugs because they promote the conversion of plasminogen to plasmin, the natural clot-resolving enzyme. They are usually administered by direct vessel perfusion to the clot site. Considerable technical skill and immediate treatment of the thrombus is required for satisfactory results, within 3 hours of the onset of symptoms. Because streptokinase is a foreign protein, allergic reactions can occur. Hemorrhage may result from the use of any of these drugs and they are contraindicated in patients at risk for hemorrhage.
DIPYRIDAMOLE
The drug dipyridamole (dye-peer-ID-a-mole) (Persantine) is used to prolong the life of platelets in patients with prosthetic heart valves. The artificial valves cause premature death of the platelets because of their mechanical effect (trauma) on the blood cells passing through the valves. Dipyridamole does not add any additional anticlotting benefit over the use of aspirin and/or warfarin. It does not affect bleeding related to dental treatment.
PENTOXIFYLLINE
Pentoxifylline (pen-tox-IF-i-lin) (Trental) is a dimethylxanthine that improves blood flow by its hemorheologic effects, which include lowering blood viscosity and improving the flexibility of red blood cells. It is indicated for intermittent claudication produced by chronic occlusive artery disease of the limbs. Side effects associated with pentoxifylline include cardiovascular and gastric symptoms. Dry mouth, bad taste, excessive salivation, and swollen neck glands have infrequently been reported. Pentoxifylline does not alter blood clotting.
Drugs That Increase Blood Clotting
HEMOSTATIC AGENTS (FIBRINOLYTIC INHIBITORS)
Aminocaproic acid (EACA) and its analog, tranexamic acid (Cyklokapron), are similar to the amino acid lysine, and they inhibit plasminogen activation (synthetic inhibitor of fibrinolysis).
Aminocaproic acid and tranexamic acid are used intravenously, orally, or topically. Adverse effects include intravascular thrombosis, hypotension, and abdominal discomfort. Some literature recommends the use of topical tranexamic acid before dental procedures in patients taking warfarin who are at risk of bleeding. It is indicated in the treatment of hemorrhage after dental surgery.
CLINICAL SKILLS ASSESSMENT
1. What is angina and what are some of its causes?
2. What is the mechanism of action of nitroglycerin in treating angina and what are its adverse reactions?
3. Describe the role of nitrates in the treatment of angina.
4. Describe the interaction between nitrates and drugs used to treat erectile dysfunction.
5. What is hypertension and what is its prevalence in the United States?
6. Explain the pharmacologic effects of ACEIs for the treatment of hypertension.
7. Describe the current algorithm for treating hypertension. State the individual drug classes for treating compelling indications in patients with hypertension.
8. State the individual drug classes for treating hypertension and include pharmacologic effects, adverse effects, and any dental concerns.
9. What is the role of aspirin in anticoagulation therapy? List the other classes of anticoagulant drugs and include mechanism of action, adverse effects, and dental concerns.
10. What is the relationship between elevated cholesterol levels and heart disease?
11. Compare and contrast the classes of medication used to treat elevated cholesterol levels and include adverse effects and dental concerns.
12. Compare and contrast the classes of medication used to treat arrhythmias.
13. Compare and contrast the classes of medications used to treat HF and include adverse effects and dental concerns.
 Please visit http://evolve.elsevier.com/Haveles/pharmacology for review questions and additional practice and reference materials.
Please visit http://evolve.elsevier.com/Haveles/pharmacology for review questions and additional practice and reference materials.