4 PRINCIPLES OF OCCLUSION
Most restorative procedures affect the shape of the occlusal surfaces. Proper dental care ensures that functional contact relationships are restored in harmony with both dynamic and static conditions. Maxillary and mandibular teeth should contact to allow optimum function, minimize trauma to the supporting structures, and allow an even load distribution throughout the dentition. Positional stability of the teeth is crucial if arch integrity and proper function are to be maintained over time.
As an aid to the diagnosis of occlusal dysfunction, it is helpful to evaluate the condition of specific anatomic features and functional aspects of a patient’s occlusion with reference to a concept of “optimum” or “ideal” occlusion. Deviation from this concept can then be measured objectively and may prove to be a useful guide during treatment planning and active treatment phases.
Over time, many concepts of “ideal” occlusion have been proposed. In the literature, the concept of what is “ideal,” “acceptable,” and “harmful” continues to evolve.
This chapter reviews the anatomic structures important to the study of occlusion and includes a discussion of mandibular movement (movement of the lower jaw). The concepts of ideal versus pathologic occlusion are introduced, as is the history of occlusal theory. The chapter concludes with guidelines for the initial phase of occlusal treatment.
ANATOMY
Temporomandibular Joints
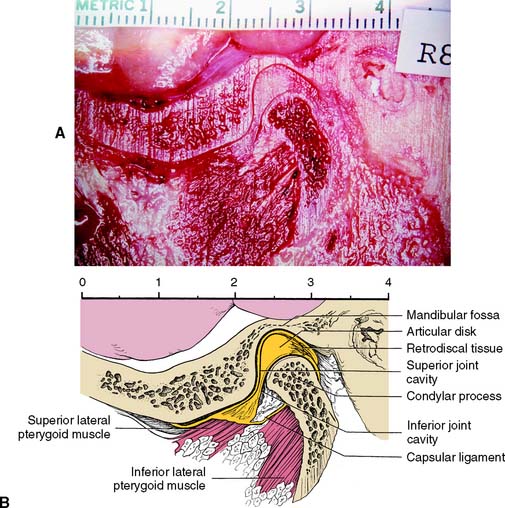
The major components of the temporomandibular joints (TMJs) are the cranial base, the mandible, and the muscles of mastication with their innervation and vascular supply. Each joint can be described as ginglymoarthrodial, which means that it is capable of both a hinging and a gliding articulation. An articular disk separates the mandibular fossa and articular tubercle of the temporal bone from the condylar process of the mandible.
The articulating surfaces of the condylar processes and fossae are covered with avascular fibrous tissue (in contrast to most other joints, which have hyaline cartilage). The articular disk consists of dense connective tissue; it also is avascular and devoid of nerves in the area where articulation normally occurs. Posteriorly, it is attached to loose highly vascularized and innervated connective tissue, the retrodiscal pad or bilaminar zone,* which connects to the posterior wall of the articular capsule surrounding the joint (Fig. 4-1). Medially and laterally, the disk is attached firmly to the poles of the condylar process. Anteriorly, it fuses with the capsule and with the superior lateral pterygoid muscle. Superior and inferior to the articular disk are two spaces: the superior and inferior synovial cavities. These are bordered peripherally by the capsule and the synovial membranes and are filled with synovial fluid. Because of its firm attachment to the poles of each condylar process, the disk follows condylar movement during both hinging and translation, which is made possible by the loose attachment of the posterior connective tissues.
Ligaments
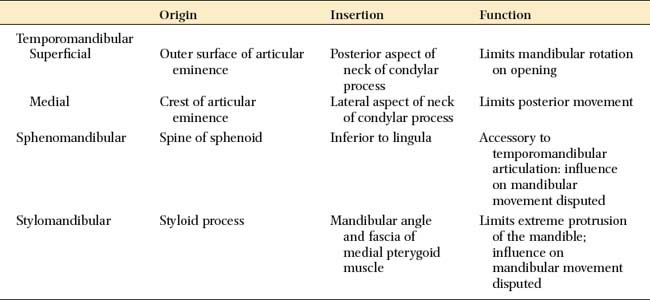
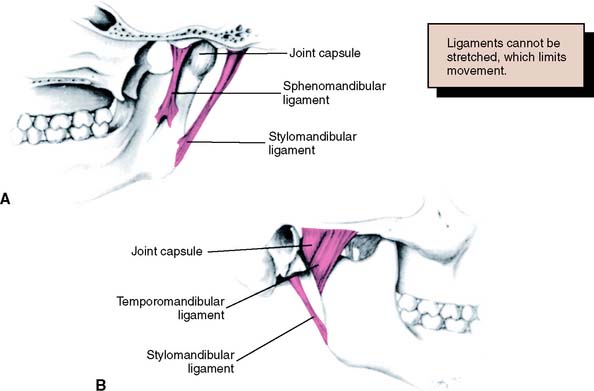
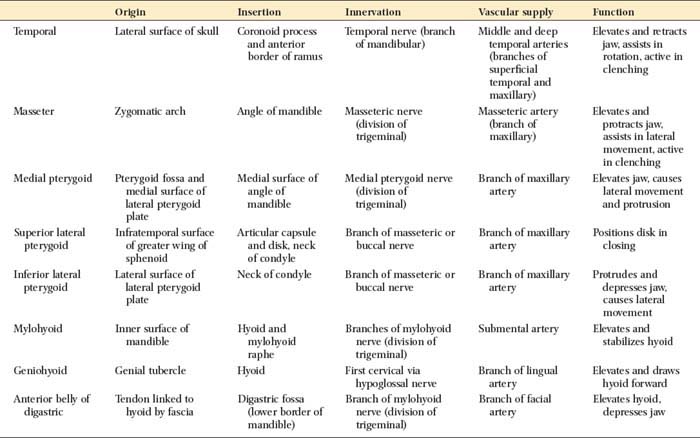
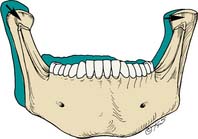
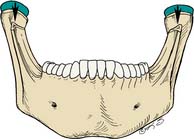
The body of the mandible is attached to the base of the skull by muscles and also by three paired ligaments (Table 4-1): the temporomandibular (also called the lateral), the sphenomandibular, and the stylomandibular. Ligaments cannot be stretched significantly, and so they limit the movement of joints. The temporomandibular ligaments limit the amount of rotation of the mandible and protect the structures of the joint, limiting border movements.1 The sphenomandibular and stylomandibular ligaments (Fig. 4-2) limit separation between the condylar process and the disk; the stylomandibular ligaments also limit protrusive movement of the mandible.
Musculature
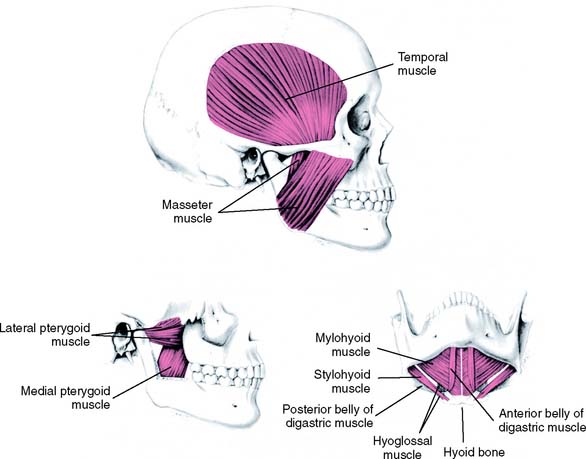
Several muscles are responsible for mandibular movements. These can be grouped into the muscles of mastication and the suprahyoid muscles (Fig. 4-3). The former include the temporal, the masseter, and the medial and lateral pterygoid muscles; the latter are the geniohyoid, the mylohyoid, and the digastric muscles. Their respective origins, insertions, and innervation and vascular supply are summarized in Table 4-2.
Muscular function
The functions of the mandibular muscles are well-coordinated, complex events.
The three paired muscles of mastication provide elevation and lateral movement of the mandible. These are the temporal, the masseter, and the medial pterygoid muscles. The lateral pterygoid muscles, each with two bellies (which probably should be considered as two separate muscles), function horizontally during opening and closing; the inferior belly (or inferior lateral pterygoid) is active during protrusion, depression, and lateral movement; the superior belly (or superior lateral pterygoid) is active during closure. The latter muscle is thought to assist in maintaining the integrity of the condyle-disk assembly by pulling the condylar process firmly against the disk, because the superior belly has been shown to attach to the disk and the neck of the condyle.
The muscles of the suprahyoid group have a dual function. They can elevate the hyoid bone or depress the mandible. The movement that results when they contract depends on the state of contraction of the other muscles of the neck and jaw region. When the muscles of mastication are in a state of contraction, the suprahyoid muscles elevate the hyoid bone. However, if the infrahyoid muscles (which anchor the hyoid bone to the sternum and clavicle) are contracted, the suprahyoid muscles depress and retract the mandible. The geniohyoid and mylohyoid initiate the opening movements, and the anterior belly of the digastric muscle completes mandibular depression. Although the stylohyoid muscle (which also belongs to the suprahyoid group) may contribute indirectly to mandibular movement through fixation of the hyoid bone, it does not play a significant role in mandibular movement.
Dentition
The relative positions of the maxillary and mandibular teeth influence mandibular movement. Many “ideal” occlusions have been described.2 In most of these, the maxillary and mandibular teeth contact simultaneously when the condylar processes are fully seated in the mandibular fossae and the teeth do not interfere with harmonious movement of the mandible during function. Ideally, in the fully bilateral seated position of the condyle-disk assemblies, the maxillary and mandibular teeth exhibit maximum intercuspation. This means that the maxillary lingual and mandibular buccal cusps of the posterior teeth are evenly distributed and in stable contact with the opposing occlusal fossae. These functional cusps can then act as stops for vertical closure without excessively loading any one tooth, while left and right TMJs are simultaneously in an unstrained position.
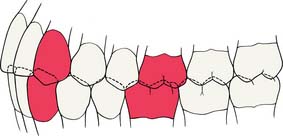
However, in many patients, maximal intercuspal contact occurs with the condyles in a slightly translated position. This position is referred to as maximum intercuspation which is defined as the complete intercuspation of the opposing teeth independent of condylar position, sometimes referred to as the best fit of the teeth regardless of the condylar position. If the mesiobuccal cusp of the maxillary first molar is aligned with the buccal groove of the mandibular first molar, an Angle Class I orthodontic relationship (Fig. 4-4) exists; this is considered normal (see glossary). In such a relationship, the anterior teeth overlap both horizontally and vertically. This position is defined as the dental relationship in which there is normal anteroposterior relationship of the jaws, as indicated by correct intercuspation of maxillary and mandibular molars, but, when a malocclusion is present, there are crowding and rotation of teeth elsewhere (i.e., a dental dysplasia or arch length deficiency). Orthodontic textbooks3 have traditionally described an arbitrary 2 mm for horizontal overlap and vertical overlap as being ideal. For most patients, however, greater vertical overlap of the anterior teeth is desirable, to prevent undesirable posterior tooth contact as a result of flexing of the mandible during mastication. Empirically, dentitions with greater vertical overlap of the anterior teeth appear to have a better long-term prognosis than do dentitions with minimal vertical overlap.
CENTRIC RELATION
Centric relation is defined as the maxillomandibular relationship in which the condyles articulate with the thinnest avascular portion of their respective disks with the complex in the anterosuperior position against the shapes of the articular eminences. This position is independent of tooth contact. It is also clinically discernible when the mandible is directed superior and anteriorly and is restricted to a purely rotary movement about the transverse horizontal axis.
Centric relation is considered a reliable and reproducible reference position. If maximum intercuspation coincides with the centric relation position, restorative treatment is often straightforward. When maximum intercuspation does not coincide with centric relation, it is necessary to determine whether corrective occlusal therapy is needed before restorative treatment.
MANDIBULAR MOVEMENT
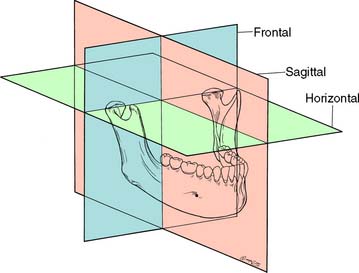
As for any other movement in space, complex three-dimensional mandibular movement can be broken down into two basic components: translation, when all points within a body have identical motion, and rotation, when the body is turning about an axis (Fig. 4-5). Every possible three-dimensional movement can be described in terms of these two components. It is easier to understand mandibular movement when the components are described as projections in three perpendicular planes: sagittal, horizontal, and frontal (Fig. 4-6).
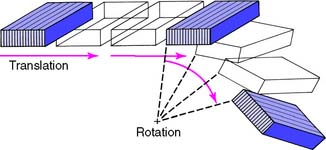
Fig. 4-5 Three-dimensional movement of a body can be defined by a combination of translation (all points within the body having identical movement) and rotation (all points turning around an axis).
Reference Planes
Sagittal plane
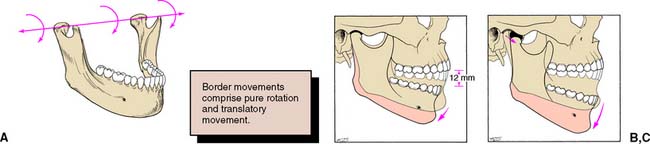
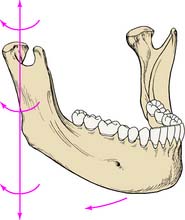
In the sagittal plane (Fig. 4-7), the mandible is capable of a purely rotational movement as well as translation. Rotation occurs around the terminal hinge axis, an imaginary horizontal line through the rotational centers of the left and right condylar processes. The rotational movement is limited to about 12 mm of incisor separation before the temporomandibular ligaments and structures anterior to the mastoid process force the mandible to translate. The initial rotation or hingeing motion is between the condyle and the articular disk. During translation, the lateral pterygoid muscle contracts and moves the condyle-disk assembly forward along the posterior incline of the tubercle. Condylar movement is similar during protrusive mandibular movement.
Horizontal plane
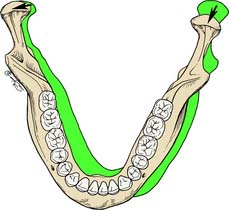
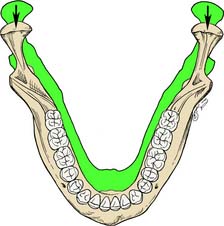
In the horizontal plane, the mandible is capable of rotation around several vertical axes. For example, lateral movement consists of rotation around an axis situated in the working (laterotrusive) condylar process (Fig. 4-8) with relatively little concurrent translation. A slight lateral translation of the condyle on the working side in the horizontal plane—known as laterotrusion, Bennett movement,4 or mandibular side shift (Fig. 4-9)—is frequently present. This may be slightly forward or slightly backward (lateroprotrusion or lateroretrusion). The orbiting (nonworking) condyle travels forward and medially as limited by the medial aspect of the mandibular fossa and the temporomandibular ligament. Finally, the mandible can make a straight protrusive (anterior) movement (Fig. 4-10).
Frontal plane
In a lateral movement in the frontal plane, the mediotrusive (or nonworking) condyle moves down and medially, whereas the laterotrusive (or working) condyle rotates around the sagittal axis perpendicular to this plane (Fig. 4-11). Again, as determined by the anatomy of the medial wall of the mandibular fossa on the mediotrusive side, transtrusion may be observed; as determined by the anatomy of the mandibular fossa on the laterotrusive side, this may be lateral and upward or lateral and downward (laterosurtrusion and laterodetrusion). A straight protrusive movement observed in the frontal plane, with both condylar processes moving downward as they slide along the tubercular eminences, is shown in Figure 4-12.
Border Movements
Mandibular movements are limited by the TMJs and ligaments, the neuromuscular system, and the teeth. Posselt5 was the first to describe mandibular movement at the limits dictated by anatomic structures, as viewed in a given plane which he called border movements (Fig. 4-13). His classic work is well worth reviewing in the attempt to understand how the determinants control the extent to which movement can occur.
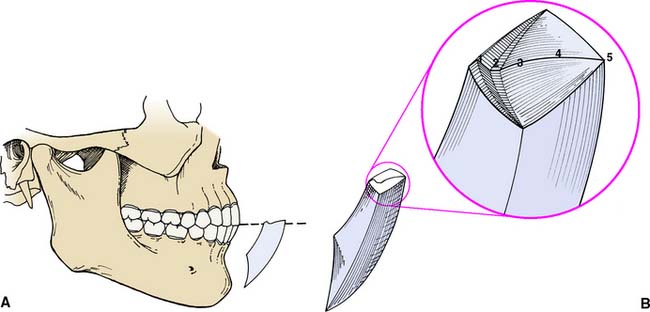
Fig. 4-13 A, Mandibular border movement in the sagittal plane. B, Posselt’s three-dimensional representation of the total envelope of mandibular movement. 1, Mandibular incisors track along the lingual concavity of the maxillary anterior teeth. 2, Edge-to-edge position. 3, Incisors move superiorly until posterior tooth contact recurs. 4, Protrusive path. 5, Most protrusive mandibular position.
Posselt used a three-dimensional representation of the extreme movements that the mandible is capable of (see Fig. 4-13B). All possible mandibular movements occur within its boundaries. At the top of both illustrations, a horizontal tracing represents the protrusive movement of the incisal edge of the mandibular incisors (solid numbered line in Fig. 4-13B).
Starting from the maximum intercuspation position, in the protrusive pathway, the lower incisors are initially guided by the lingual concavity of the maxillary anterior teeth. This leads to gradual loss of posterior tooth contact as the incisors reach the edge-to-edge position. This is represented in Posselt’s diagram by the initial downward slope. As the mandible moves farther protrusively, the incisors slide over a horizontal trajectory representing the edge-to-edge position (the flat portion in the diagram), after which the lower incisors move upward until new posterior tooth contact occurs. Further protrusive movement of the mandible typically takes place without significant tooth contact.
The border farthest to the right of Posselt’s solid (see Fig. 4-13B) represents the most protruded opening and closing stroke. The maximal open position of the mandible is represented by the lowest point in the diagram. The left border of the diagram represents the most retruded closing stroke. This movement occurs in two phases: The lower portion consists of a combined rotation and translation, until the condylar processes return to the fossae. The second portion of the most retruded closing stroke is represented by the top portion of the border that is farthest to the left in Posselt’s diagram. It is strictly rotational.
Posterior and anterior determinants of mandibular movement
These determinants (Table 4-3) are the anatomic structures that dictate or limit the movements of the mandible. The anterior determinant of mandibular movement is the dental articulation. The posterior determinants of mandibular movement are the temporomandibular articulations and their associated structures The posterior determinants (Fig. 4-14)—shape of the articular eminences, anatomy of the medial walls of the mandibular fossae, configuration of the mandibular condylar processes—cannot be controlled, and it is not possible to influence the neuromuscular responses of the patient unless it is done by indirect means (e.g., through changes in the configuration of the contacting teeth or by the provision of an occlusal appliance). If a patient has steeply sloped eminences, there is a large downward component of condylar movement during lateral and protrusive excursions. Similarly, the anatomy of the medial wall of each fossa normally allows the condyle to move slightly medially as it travels forward (mandibular side shift, or transtrusion). The side shift becomes greater as the extent of medial movement increases. However, the anatomy of the joint dictates the actual path and timing of condylar movement. Movement of the laterotrusive or working condylar process is influenced predominantly by the anatomy of the lateral wall of the mandibular fossa. The amount of the side shift is, of course, a function of the mediotrusive or nonworking condyle; on the working side, however, it is the anatomy of the lateral aspect of the fossa that guides the working condyle straight out or upward and downward. The amount of side shift does not appear to increase as the result of a loss of occlusion.6
Table 4-3 IMPACT OF SELECTED VARIABLES ON OCCLUSAL FORM OF RESTORATIONS
| Variation | Impact on Restoration | |
|---|---|---|
| POSTERIOR DETERMINANTS | ||
| Inclination of articular eminence | Steeper | Posterior cusps may be taller |
| Flatter | Posterior cusps must be shorter | |
| Medial wall of glenoid fossa | Allows more lateral translation | Posterior cusps must be shorter |
| Allows minimal lateral translation | Posterior cusps may be taller | |
| Intercondylar distance | Greater | Smaller angle between laterotrusive and mediotrusive movement |
| Lesser | Increased angle between laterotrusive and mediotrusive movement | |
| ANTERIOR DETERMINANTS | ||
| Horizontal overlap of anterior teeth | Increased | Posterior cusps must be shorter |
| Reduced | Posterior cusps may be taller | |
| Vertical overlap of anterior teeth | Increased | Posterior cusps may be taller |
| Reduced | Posterior cusps must be shorter | |
| OTHER | ||
| Occlusal plane | More parallel to condylar guidance | Posterior cusps must be shorter |
| Less parallel to condylar guidance | Posterior cusps may be longer | |
| Anteroposterior curve | More convex (shorter radius) | The most posterior cusps must be shorter |
| Less convex (larger radius) | The most posterior cusps may be longer |
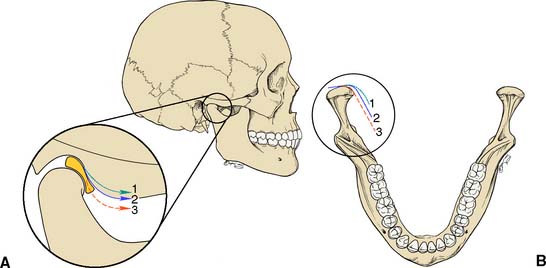
Fig. 4-14 Posterior determinants of occlusion. A, Angle of the articular eminence (condylar guidance angle). 1, Flat; 2, average; 3, steep. B, Anatomy of the medial walls of the mandibular fossae. 1, Greater than average; 2, average; 3, minimal side shift.
The anterior determinants (Fig. 4-15) are the vertical and horizontal overlaps and the maxillary lingual concavities of the anterior teeth. These can be altered by restorative and orthodontic treatment. A greater vertical overlap causes the direction of mandibular opening to be more vertical during the early phase of protrusive movement and creates a more vertical pathway at the end of the chewing stroke. Increased horizontal overlap allows a more horizontal jaw movement.
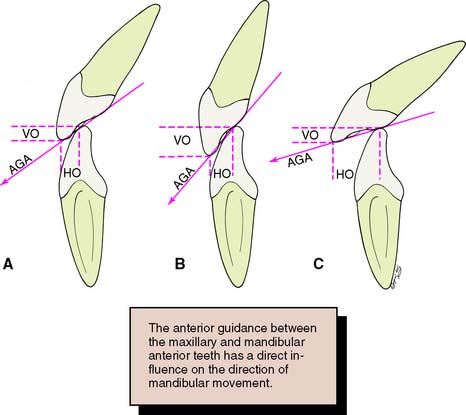
Fig. 4-15 Anterior determinants of occlusion. Different incisor relationships with differing horizontal and vertical overlaps (HO and VO) produce different anterior guidance angles (AGA). A, Class I. B, Class II, Division 2 (increased VO; steep AGA). C, Class II, Division 1 (increased HO; flat AGA).
Although the posterior and anterior determinants combine to affect mandibular movement, no correlation has been established7; that is, patients with steep anterior guidance angles do not necessarily have a steep posterior disclusion, and those with a steep posterior disclusion do not necessarily have steep guidance angles.
Functional Movements
Functional mandibular movement is defined as all normal, proper, or characteristic movements of the mandible made during speech, mastication, yawning, swallowing, and other associated movements. Most functional movement of the mandible (as occurs during mastication and speech) takes place inside the physiologic limits established by the teeth, the TMJs, and the muscles and ligaments of mastication; therefore, these movements are rarely coincident with border movements.
Chewing
When incising food, adults open their mouths a comfortable distance and move the mandible forward until they incise, with the anterior teeth meeting approximately edge to edge. The food bolus is then transported to the center of the mouth as the mandible returns to its starting position, with the incisal edges of the mandibular anterior teeth tracking along the lingual concavities of the maxillary anterior teeth (Fig. 4-16). The mouth then opens slightly, the tongue pushes the food onto the occlusal table, and, after moving sideways, the mandible closes into the food until the guiding teeth (typically the canines) contact.8 The cycle is completed as the mandible returns to its starting position.9 This pattern repeats itself until the food bolus has been reduced to particles that are small enough to be swallowed, at which point the process can start over. The direction of the mandibular path of closure is influenced by the inclination of the occlusal plane with the teeth apart and by the occlusal guidance as the jaw approaches maximum intercuspation.10
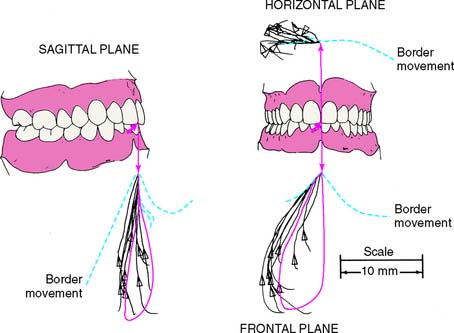
Fig. 4-16 Comparison of border and chewing movements for soft food at the central incisor. Sagittal, frontal, and horizontal views in an orthographic projection.
(From Gibbs CH, et al: Chewing movements in relation to border movements at the first molar. J Prosthet Dent 46:308, 1981.)
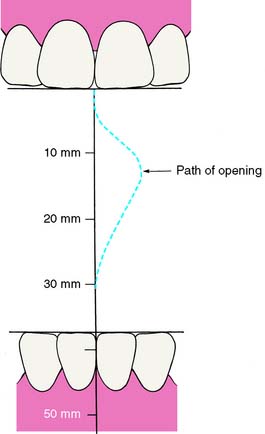
The chewing pattern observed in children differs from that found in adults. Until about age 10, children begin the chewing stroke with a lateral movement. After the age of 10, they start to chew increasingly like adults, with a more vertical stroke11 (Fig. 4-17). Stimuli from the pressoreceptors play an important role in the development of functional chewing cycles.12
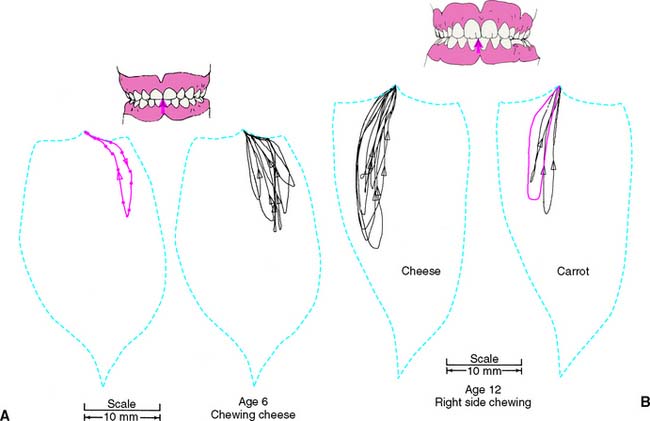
Fig. 4-17 Frontal views of chewing. The dashed lines are border movements. A, Chewing in a young person, characterized by a wide lateral movement on opening and decreased lateral movement on closing. B, In an older child, the chewing pattern resembles that of an adult.
(From Wickwire NA, et al: Chewing patterns in normal children. Angle Orthod 51:48, 1981.)
Mastication is a learned process. At birth, no occlusal plane exists, and only after the first teeth have erupted far enough to contact each other is a message sent from the receptors to the cerebral cortex, which controls the stimuli to the masticatory musculature. Stimuli from the tongue and cheeks, and perhaps from the musculature itself and from the periodontium, may influence this feedback pattern.
Speaking
The teeth, tongue, lips, floor of the mouth, and soft palate form the resonance chamber that affects pronunciation. During speech, the teeth are generally not in contact, although the anterior teeth may come very close together during soft “c,” “ch,” “s,” and “z” sounds, forming the “speaking space: the space that occurs between the incisal and/or occlusal surfaces of the maxillary and mandibular teeth during speech.”13 When pronouncing the fricative “f,” the inner vermilion border of the lower lip traps air against the incisal edges of the maxillary incisors. Phonetics is a useful diagnostic guide for correcting vertical dimension and tooth position during fixed and removable prosthodontic treatment.14-17
Parafunctional Movements
Parafunctional movements of the mandible may be described as sustained activities that occur beyond the normal functions of mastication, swallowing, and speech. There are many forms of parafunctional activities, including bruxism, clenching, nail biting, and pencil chewing, among others. Typically, parafunction is manifested by long periods of increased muscle contraction and hyperactivity. Concurrently, excessive occlusal pressure and prolonged tooth contact occur, which is inconsistent with the normal chewing cycle. Over a protracted period, this can result in excessive wear; widening of the periodontal ligament; and mobility, migration, or fracture of the teeth. Muscle dysfunction such as myospasms, myositis, myalgia, and referred pain (headaches) from trigger point tenderness may also occur. The degree of symptoms varies considerably among individuals. The two most common forms of parafunctional activities are bruxism and clenching. Increased radiographic bone density is often seen in patients with a history of sustained parafunctional activity.
Bruxism
Oral habits consisting of involuntary rhythmic or spasmodic nonfunctional gnashing, grinding, or clenching of teeth, in other than chewing movements of the mandible, that may lead to occlusal trauma is known as bruxism (Fig. 4-18). This activity may be diurnal, nocturnal, or both. Although bruxism is initiated on a subconscious level, nocturnal bruxism is potentially more harmful because the patient is not aware of it while sleeping. Therefore, it can be difficult to detect, but it should be suspected in any patient exhibiting abnormal tooth wear or pain. The prevalence of bruxism is about 10% and is less common with age.18 The etiology of bruxism is often unclear. Some theories relate bruxism to malocclusion, neuromuscular disturbances, responses to emotional distress, or a combination of these factors.19 A study on cohort twins has demonstrated substantial genetic effects20; the condition has been related to sleep disturbance21; and the symptoms of bruxism are three times more common in smokers.22 Altered mastication has been observed in subjects who brux23,24 and may result from an attempt to avoid premature occlusal contacts (occlusal interferences). There may also be a neuromuscular attempt to “rub out” an interfering cusp. The fulcrum effect of rubbing on posterior interferences creates a protrusive or laterotrusive movement that can cause overloading of the anterior teeth, with resultant excessive anterior wear. It is common for wear on anterior teeth to progress from initial faceting on the canines to the central and lateral incisors. Once vertical overlap diminishes as the result of wear, posterior wear facets are commonly observed. However, the chewing patterns of normal subjects can be quite varied, and the relationship, if any, between altered mastication and occlusal dysfunction is not clear.25
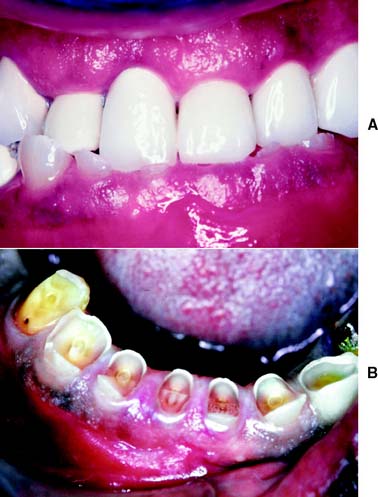
Fig. 4-18 Extensive abrasion (tooth wear) resulting from parafunctional grinding.
(Courtesy of Dr. M. Padilla.)
The causes of bruxism are difficult to determine. One theory26 states that bruxism is performed on a subconscious reflex-controlled level and is related to emotional responses and occlusal interferences. In certain malocclusions, the neuromuscular system exerts fine control during chewing to avoid particular occlusal interferences. As the degree of muscle activity necessary to avoid the interferences becomes greater, an increase in muscle tone may result, with subsequent pain in the hyperactive musculature, which in turn can lead to restricted movement. The relationship, if any, between bruxism and temporomandibular disorders is still unclear.27
Patients who brux can exert considerable forces on their teeth, and much of this may have a lateral component. Posterior teeth do not tolerate lateral forces as well as vertical forces in their long axes. Buccolingual forces, in particular, appear to cause rapid widening of the periodontal ligament space and increased mobility.
Clenching
Clenching is defined as the pressing and clamping of the jaws and teeth together frequently associated with acute nervous tension or physical effort. The pressure thus created can be maintained over a considerable time with short periods of relaxation in between. The etiology can be associated with stress, anger, physical exertion, or intense concentration on a given task, rather than an occlusal disorder. In contrast to bruxism, clenching does not necessarily result in damage to the teeth because the concentration of pressure is directed more or less through the long axes of the posterior teeth without the involvement of detrimental lateral forces. Abfractions—cervical defects at the cementoenamel junction—may result from sustained clenching.28,29 Also, the increased load may result in damage to the periodontium, TMJs, and muscles of mastication. Typically, the elevator muscles become overdeveloped. Muscle splinting, myospasm, and myositis may progress, causing the patient to seek treatment. As with bruxism, clenching can be difficult to diagnose and difficult if not impossible for the patient to voluntarily control.
HISTORY OF OCCLUSAL STUDIES
Historically, the study of occlusion and articulation has undergone an evolution of concepts. These can be broadly categorized as concepts of bilaterally balanced,30 unilaterally balanced, and mutually protected articulation. Current emphasis in teaching fixed prosthodontics and restorative dentistry has been on the concept of mutual protection (Fig. 4-19). However, because restorative treatment requirements vary, the clinician should understand possible combinations of occlusal schemes and their advantages, disadvantages, and indications.

Fig. 4-19 Canine-guided or mutually protected articulation. During lateral excursions, there are no contacts on the mediotrusive (nonworking) side; all contacts are between the laterotrusive (working side) canines.
In most patients, maximum tooth contact occurs anterior to the centric relation position of the mandible. Often, this maximum intercuspation position anterior to centric relation is referred to as centric occlusion, although the term is also used to refer to occlusal contact in centric relation. To avoid confusion, maximum intercuspation and centric relation are the terms used in this text.
Bilaterally Balanced Articulation
Early work in removable prosthodontics centered on the concept of a bilaterally balanced articulation. This requires having a maximum number of teeth in contact in maximum intercuspation and all excursive positions. In complete denture fabrication, this tooth arrangement helps maintain denture stability because the nonworking contact prevents the denture from being dislodged. However, as the principles of bilateral balance were applied to the natural dentition and in fixed prosthodontics, it proved to be extremely difficult to accomplish, even with great attention to detail and with the use of sophisticated articulators. In addition, high rates of failure resulted. An increased rate of occlusal wear, increased or accelerated periodontal breakdown, and neuromuscular disturbances were commonly observed. The last were often relieved when posterior contacts on the mediotrusive side were eliminated in an attempt to eliminate unfavorable loading. Thus, the concept of a unilaterally balanced occlusion (group function) evolved31 (Fig. 4-20).

Unilaterally Balanced Articulation (Group Function)
In a unilaterally balanced articulation, excursive contact occurs between all opposing posterior teeth on the laterotrusive (working) side only. On the mediotrusive (nonworking) side, no contact occurs until the mandible has reached centric relation. Thus, in this occlusal arrangement, the load is distributed among the periodontal support of all posterior teeth on the working side. This can be advantageous if, for instance, the periodontal support of the canine is compromised. While on the working side, occlusal load is distributed during excursive movement, and the posterior teeth on the nonworking side do not contact. In the protrusive movement, no posterior tooth contact occurs.
Long centric
As the concept of unilateral balance evolved, it was suggested that allowing some freedom of movement in an anteroposterior direction is advantageous. This concept is known as long centric. Schuyler32 was one of the first to advocate such an occlusal arrangement. He thought that it was important for the posterior teeth to be in harmonious gliding contact when the mandible translates from centric relation forward to make anterior tooth contact. Others33 have advocated long centric because centric relation only rarely coincides with the maximum intercuspation position in healthy natural dentitions. However, its length is arbitrary. At given vertical dimensions, long centric ranges from 0.5 to 1.5 mm in length have been advocated. This theory presupposes that the condyles can translate horizontally in the fossae over a commensurate trajectory before beginning to move downward. It also necessitates a greater horizontal space between the maxillary and mandibular anterior teeth (deeper lingual concavity), allowing horizontal movement before posterior disocclusion (separation of opposing teeth during eccentric movements of the mandible).
Mutually Protected Articulation
During the early 1960s, an occlusal scheme called mutually protected articulation was advocated by Stuart and Stallard,34 based on earlier work by D’Amico.35 In this arrangement, centric relation coincides with the maximum intercuspation position. The six anterior maxillary teeth, together with the six anterior mandibular teeth, guide excursive movements of the mandible, and no posterior occlusal contacts occur during any lateral or protrusive excursions.
The relationship of the anterior teeth, or anterior guidance, is critical to the success of this occlusal scheme. In a mutually protected articulation, the posterior teeth come into contact only at the very end of each chewing stroke, minimizing horizontal loading on the teeth. Concurrently, the posterior teeth act as stops for vertical closure when the mandible returns to its maximum intercuspation position. Posterior cusps should be sharp and should pass each other closely without contacting to maximize occlusal function. Investigations of the neuromuscular physiology of the masticatory apparatus indicate advantages associated with a mutually protected occlusal scheme.8 However, in studies involving unrestored dentitions, relatively few occlusions can be classified as mutually protected.36
Optimum occlusion
In an ideal occlusal arrangement, the load exerted on the dentition should be distributed optimally. Occlusal contact has been shown37 to influence muscle activity during mastication. Any restorative procedures that adversely affect occlusal stability may affect the timing and intensity of elevator muscle activity. Horizontal forces on any teeth should be avoided or at least minimized, and loading should be predominantly parallel to the long axes of the teeth. This is facilitated when the tips of the functional cusps are located centrally over the roots and when loading of the teeth occurs in the fossae of the occlusal surfaces rather than on the marginal ridges. Horizontal forces are also minimized if posterior tooth contact during excursive movements is avoided. Nevertheless, to enhance masticatory efficiency, the cusps of the posterior teeth should have adequate height. Stabilizing contacts involves primarily the mandibular buccal cusps, and it has been suggested that maintenance or improvement of the number of such contacts should be among occlusal treatment objectives.38
The chewing and grinding action of the teeth is enhanced if opposing cusps on the laterotrusive side interdigitate at the end of the chewing stroke. The mutually protected occlusal scheme probably meets this criterion better than the other occlusal arrangements. The features of a mutually protected articulation are as follows39:
In achieving these criteria, it is assumed that (1) a full complement of teeth exists, (2) the supporting tissues are healthy, (3) there is no reverse articulation (crossbite) and (4) the occlusion is Angle Class I.
Rationale
At first glance, it might seem illogical to load the single-rooted anterior teeth as opposed to the multirooted posterior teeth during chewing. However, the canines and incisors have a distinct mechanical advantage over the posterior teeth40: The effectiveness of the force exerted by the muscles of mastication is notably less when the loading contact occurs farther anteriorly.
The mandible is a lever of the class III type (Fig. 4-21), which is the least efficient of lever systems. An example of another class III lever would be a fishing pole. The longer the pole, the more effort it takes to pull a fish out of the water. The same holds true for the muscles of mastication and the teeth: the farther anteriorly initial tooth-to-tooth contact occurs (i.e., the longer the lever arm), the less effective the forces exerted by the musculature are and the smaller the load to which the teeth are subjected is. The canine—with its long root, significant amount of periodontal surface area, and strategic position in the dental arch—is well adapted to guiding excursive movements. This function is governed by pressoreceptors in the periodontal ligament, receptors that are very sensitive to mechanical stimulation.41
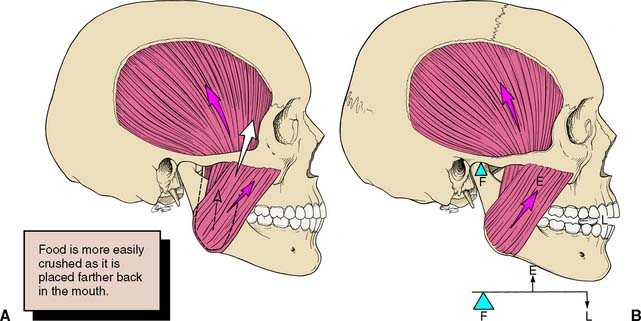
Fig. 4-21 Lever system of the mandible. A, The elevator muscles of the mandible insert anterior to the temporomandibular joints (TMJs) and posterior to the teeth, forming a class III lever system. B, The fulcrum (F) is the TMJ, the force or effort (E) is applied by the muscles of mastication, and the resistance or load (L) is food placed between the teeth. The load diminishes as the lever arm increases. Therefore, less load is placed on the anterior teeth than on the posterior teeth.
The elimination of posterior contacts during excursions reduces the amount of lateral force to which posterior teeth are subjected. Therefore, molars and premolars in group function are subjected to greater horizontal and potentially more pathologic force than the same teeth in a mutually protected articulation.
PATIENT ADAPTABILITY
There are significant differences in the adaptive response of patients to occlusal abnormalities. Some individuals are unable to tolerate seemingly trivial occlusal deficiencies, whereas others are able to tolerate distinct malocclusions without obvious symptoms (Fig. 4-22). Most patients seem able to adapt to small occlusal deficiencies without exhibiting acute symptoms.

Fig. 4-22 Patient adaptability: None of the four patients described here expressed any concern about their occlusion. A, Anterior esthetics motivated a 45-year-old woman to seek treatment, although loss of posterior occlusal contact probably contributed to the development of her anterior diastema. B, A 26-year-old woman had no complaints or neuromuscular symptoms, despite contacting only on her second and first molars. C, A patient with amelogenesis imperfecta sought care for esthetic reasons rather than functional complaints. D, A 21-year-old man with congenitally missing lateral incisors had neither functional nor pain complaints when he was referred for fixed prosthodontic care after orthodontic treatment.
Lowered Threshold
Patients with a low pain threshold generally do not present much difficulty in diagnosis. They readily identify every pain. A lowered threshold, however, is not to be confused with hypochondria; it is merely an indication of poor adaptability to occlusal discrepancies. The tolerance or adaptability of an individual patient is likely to vary: It is lower at times of emotional stress and general malaise, when clinical symptoms such as severe headaches, muscle spasm, and pain may surface.
Raised Threshold
Individuals who have adapted to existing malocclusions may report being quite comfortable with their dentition, although a number of signs are evident. Even in the absence of pain, however, occlusal treatment may be advised so as to prevent or minimize wear on the teeth and damage to the musculature or TMJs.
PATHOGENIC OCCLUSION
A pathogenic occlusion is defined as an occlusal relationship capable of producing pathologic changes in the stomatognathic system. In such occlusions, sufficient disharmony exists between the teeth and the TMJs to result in symptoms that necessitate intervention.
Signs and Symptoms
There are many indications that a pathogenic occlusion may be present. Diagnosis is often complicated because patients almost always have a combination of symptoms. Although it is often not possible to prove a direct correlation between specific symptoms and malocclusion, the following symptoms can help confirm this diagnosis.
Teeth
The teeth may exhibit hypermobility, open contacts, or abnormal wear. Hypermobility of an individual tooth or an opposing pair of teeth is often an indication of excessive occlusal force. This may result from premature contact in centric relation or during excursive movements. Such contacts frequently can be detected by placing the tip of the index finger on the crown portion of the mobile tooth and asking the patient to repeatedly tap the teeth together. Small amounts of movement (fremitus) that otherwise might not be readily seen can often be felt this way.
Open proximal contacts may be the result of tooth migration because of an unstable occlusion and should prompt further investigation (Fig. 4-23). Diagnostic casts made during previous treatment help assess any changes in the stability of the occlusion. Abnormal tooth wear, cusp fracture, or chipping of incisal edges may be signs of parafunctional activity.42,43 However, extensive tooth destruction is often caused by a combination of acid erosion and attrition.44-46 In these cases, the acid may be present in the diet (e.g., excessive citrus fruit consumption) or endogenous (caused by regurgitation or frequent vomiting).

Periodontium
There is no convincing evidence that chronic periodontal disease is caused directly by occlusal overload. However, a widened periodontal ligament space (detected radiographically) may indicate premature occlusal contact and is often associated with tooth mobility (Fig. 4-24). Similarly, isolated or circumferential periodontal defects are often associated with occlusal trauma. In patients with advanced periodontal disease who have extensive bone loss, rapid tooth migration may occur with even minor occlusal discrepancies. Tooth movement may make it difficult for these patients to institute proper oral hygiene measures, and the result may be a recurrence of periodontal disease. Precise adjustment of the occlusion is probably more crucial in patients with a compromised crown/root ratio than in those with better periodontal support (see Chapter 32).

Musculature
Acute or chronic muscular pain on palpation can indicate habits associated with tension such as bruxism or clenching. Chronic muscle fatigue can lead to muscle spasm and pain. In one study,47 subjects were instructed to grind their teeth for approximately 30 minutes. They experienced muscle pain that typically peaked 2 hours after parafunctioning and lasted as long as 7 days. Asymmetric muscle activity can be diagnosed by observing a patient’s opening and closing movements in the frontal plane. A deviation of a few millimeters is quite common, but any deviation larger than this may be a sign of dysfunction and mandates further examination (Fig. 4-25).48 Restricted opening, or trismus, may be a result of the fact that the mandibular elevator muscles are not relaxing.
Temporomandibular joints
Pain, clicking, or popping in the TMJs can indicate temporomandibular disorders. Clicking and popping may be present without the patient’s awareness. A stethoscope is a useful diagnostic aid; one study revealed that joint sounds are generally reliable indicators of temporomandibular disorders.49 The patient may complain of TMJ pain that is actually of muscular origin and is referred to the joints.
Clicking may also be associated with internal derangements of the joint. A patient with unilateral clicking when opening and closing (reciprocal click) in conjunction with a midline deviation may have a displaced disk. The midline deviation typically occurs toward the side of the affected joint because the displaced disk can prevent (or slow down) the normal anterior translatory movement of the condyle.
Myofascial pain dysfunction
The myofascial pain dysfunction (MPD) syndrome manifests as diffuse unilateral pain in the preauricular area, with muscle tenderness, clicking, or popping noises in the contralateral TMJ and limitation of jaw function. Often the muscles, and not the TMJ, are the primary site, but over time the functional problem may lead to organic changes in the joint. Three major theories about the cause of MPD are recognized: (1) According to the psychophysiologic theory,50 MPD results from bruxing and clenching, with chronic muscle fatigue leading to muscle spasm and altered mandibular movement. Tooth movement may follow, and the malocclusion becomes apparent when spasm is relieved. According to this theory, treatment should focus on emotional rather than physical therapy. (2) According to the muscle theory,51 continuous muscle hyperactivity is responsible for MPD, with pain referred to the TMJ and other areas of the head and neck region. (3) According to the mechanical displacement theory,52 malocclusion of the teeth displaces the condyles, and the feedback from the dentition is altered, which results in muscle spasm.
Correct diagnosis and management is often complicated by the concurrent presence of multiple etiologies. Patients with MPD may require multidisciplinary treatment involving occlusal therapy, medications, biofeedback, and physical therapy. Extensive fixed prosthodontic treatment should be postponed until the patient’s conditions have been stabilized at acceptable levels.
OCCLUSAL TREATMENT
When a patient exhibits signs and symptoms that appear correlated to occlusal interferences (see also p. 195), occlusal treatment should be considered.53 Such treatment can include tooth movement through orthodontics, elimination of deflective occlusal contacts through selective reshaping of the occlusal surfaces of teeth, or the restoration and replacement of missing teeth that result in more favorable distribution of occlusal force.
The objectives of occlusal treatment are as follows:
In the short term, these objectives can be accomplished with a removable occlusal device (Fig. 4-26) fabricated from clear acrylic resin that overlies the occlusal surfaces of one arch. On a more permanent basis, this can be accomplished through selective occlusal reshaping, tooth movement, the placement of restorations, or a combination of these. Definitive occlusal treatment involves accurate manipulation of the mandible, particularly in centric relation. Because the patient may resist such manipulation as a result of protective muscular reflexes, some type of deprogramming device may be needed (e.g., an occlusal device).

Occlusal Device Therapy
Occlusal devices (sometimes referred to as occlusal splints, occlusal appliances, or orthotics) are used extensively in the management of temporomandibular disorders and bruxism.54 In controlled clinical trials, they have effectively controlled myofascial pain (i.e., the patient perceives positive changes as a result of the device therapy). However, no clear hypothesis about the mechanism of action has been proved, and none of the various hypotheses (repositioning of condyle and/or the articular disk, reduction in masticatory muscle activity, modification of “harmful” oral behavior, and changes in the patient’s occlusion) has been consistently supported by scientific studies.55 Occlusal devices are particularly helpful in determining whether a proposed change in a patient’s occlusal scheme will be tolerated. The proposed scheme is created in an acrylic resin over-lay, which allows testing of the scheme through reversible means, although at a slightly increased vertical dimension. If a patient responds favorably to an occlusal device, the response to restorative treatment should be positive as well. Thus, occlusal device therapy can serve as an important diagnostic procedure before initiation of fixed prosthodontic treatment. The device can be made for either maxillary or mandibular teeth. Some clinicians express a preference for one or the other and cite advantages; however, both maxillary and mandibular devices have proved satisfactory.
Fabrication of Device
There are several satisfactory methods for making an occlusal device.45 One made from heat-polymerized acrylic resin has the advantage of durability, but autopolymerizing resin used alone or in conjunction with a vacuum-formed matrix can serve equally well. Box 4-1 compares the indirect and direct techniques.
Box 4-1 Comparison of Occlusal Devices
Courtesy of Dr. J. E. Petrie.
Direct procedure with a vacuum-formed matrix
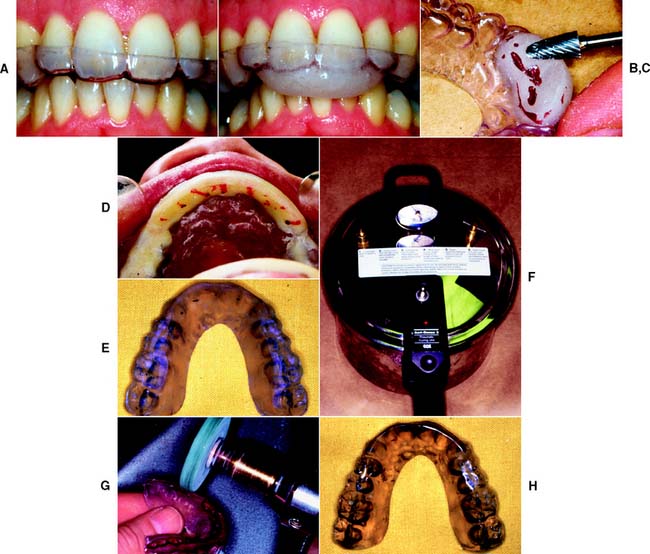
Indirect procedure with autopolymerizing acrylic resin
Accurately mounted diagnostic casts are essential for this procedure. A relatively small mounting error can lead to considerable loss of time at try-in. Particular attention must be given to occlusal defects or interfering soft tissue projections on the casts, which could cause errors during mounting.
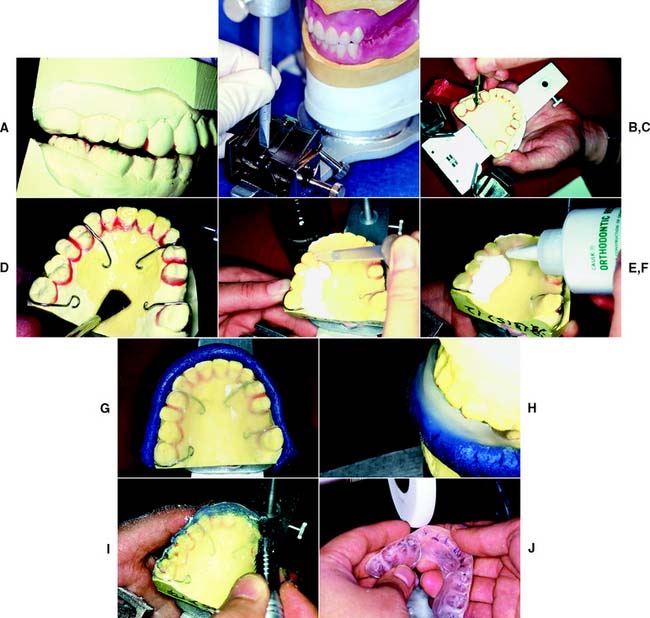
Indirect procedure with autopolymerizing resin (alternative technique)

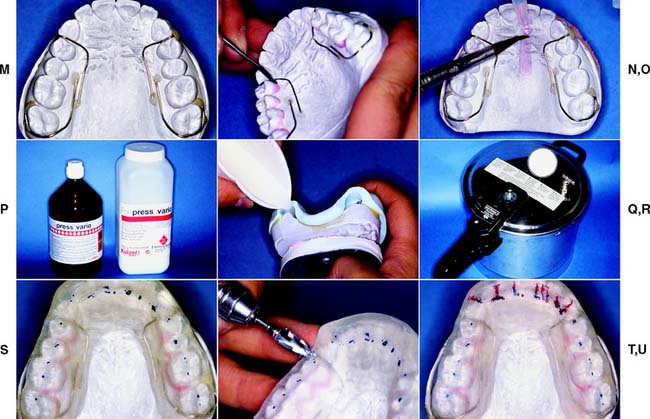
Indirect procedure with heat-polymerized acrylic resin
A more durable device can be made with heat-polymerized acrylic resin. The desired occlusal surface is shaped in wax on articulated diagnostic casts, or the direct device made with a vacuum-formed matrix can be used as a pattern. This is flasked and processed in a manner similar to that for a complete denture. Because of processing errors, it is important to remount the cast and make necessary adjustments before finishing and polishing are completed.
Attention to detail
Regardless of the device chosen, success depends very much on meticulous attention to detail during the fabrication. When making a direct device, a well-adapted and stable vacuum-formed base should be used and the procedure followed exactly. For example, the clinician must be sure that the anterior guidance is properly established and that the patient’s jaw can be easily manipulated before adding resin to the posterior region. When the indirect procedure is used, the casts must articulate to an accurate centric relation record made at the correct occlusal vertical dimension. Inaccurate mounting is probably the most common cause for frustration and results in excessive adjustments at delivery.
Follow-Up
After delivery to the patient, the occlusion must be verified and corrected as necessary. The patient is instructed to wear the device 24 hours a day, removing it only for oral hygiene, and to return at regular weekly and biweekly intervals (or sooner if a problem is anticipated) for modification. A reduction in discomfort suggests that definitive occlusal adjustment (see Chapter 6) or restorative dentistry, or both, will probably be successful. If device therapy fails to relieve the discomfort, further evaluation and diagnosis of the etiology and parameters of the chief complaint should be pursued.
SUMMARY
Mandibular movement depends on certain anatomic limitations. The extremes, called border movements, are subject to restriction by the TMJs and ligaments and the teeth. Speech and mastication are examples of functional movements. Bruxism and clenching are examples of parafunctional movements. These accomplish no purposeful objective and are potentially harmful.
A balanced occlusion provides complete denture patients with stability, because there is even contact between all the teeth in each excursion. This is potentially destructive in dentate patients and is not indicated for fixed prosthodontic treatment. In a unilaterally balanced occlusion (group function), eccentric occlusal contact occurs only between posterior teeth on the laterotrusive (working) side. This may be indicated when it is important to distribute the occlusal load over multiple teeth. Mutually protected articulation offers the most desirable distribution of occlusal load. Centric relation coincides with the maximum intercuspation position, and the relationship of the maxillary and mandibular anterior teeth (the anterior guidance) is instrumental to its success.
In the presence of pathology that is potentially related to malocclusion, occlusal therapy may be indicated. Occlusal devices can serve as useful diagnostic and therapeutic adjuncts to treatment. For such patients, occlusal therapy should be initiated and completed before any substantial restorative care is undertaken.
 GLOSSARY*
GLOSSARY*
ab·duct \ăb dŭkt’\ vt (1834): to draw away from the median plane—comp ADDUCT
abrade \uh-brād’\vt (1677): to rub away the external covering or layer of a part—comp ATTRITION, EROSION
abra·sion \ă-brā’ shun\ n (1656): 1: the wearing away of a substance or structure (such as the skin or the teeth) through some unusual or abnormal mechanical process 2: an abnormal wearing away of the tooth substance by causes other than mastication—comp ATTRITION, EROSION
acquired eccentric relation \a-kwīrd’  k-s
k-s n’trk r-lā’shun\: any eccentric relationship position of the mandible relative to the maxilla, whether conditioned or learned by habit, which will bring the teeth into contact
n’trk r-lā’shun\: any eccentric relationship position of the mandible relative to the maxilla, whether conditioned or learned by habit, which will bring the teeth into contact
adaptation \ăd’ăp-tā’shun\ n (1610): 1: the act or process of adapting; the state of being adapted 2: the act of purposefully adapting two surfaces to provide intimate contact 3: the progressive adjustive changes in sensitivity that regularly accompany continuous sensory stimulation or lack of stimulation 4: in dentistry, (a) the degree of fit between a prosthesis and supporting structures, (b) the degree of proximity of a restorative material to a tooth preparation, (c) the adjustment of orthodontic bands to teeth
ad·duct \a-dŭkt’,-ă-\ vt (1836): to draw toward the median plane or toward the axial line—comp ABDUCT
ag·o·nist \ăg’a-nst\ n (ca. 1626): 1: in physiology, a muscle that is controlled by the action of an antagonist with which it is paired 2: in anatomy, a prime mover 3: in pharmacology, a drug that has an affinity for and stimulates physiologic activity in cell receptors normally stimulated by naturally occurring substances
Angle’s classification of occlusion \ăng’gulz klăs’a-f-kā’shun ŭv a-klōō’shun\ [Edward Harley Angle, American orthodontist, 1855–1930]: eponym for a classification system of occlusion based on the interdigitation of the first molar teeth originally described by Angle as four major groups depending on the anteroposterior jaw relationship. Class IV is no longer used. Class I (normal occlusion or neutroocclusion): the dental relationship in which there is normal anteroposterior relationship of the jaws, as indicated by correct interdigitation of maxillary and mandibular molars, but with crowding and rotation of teeth elsewhere, i.e., a dental dysplasia or arch length deficiency. Class II (distocclusion): the dental relationship in which the mandibular dental arch is posterior to the maxillary dental arch in one or both lateral segments; the mandibular first molar is distal to the maxillary first molar. Class II can be further subdivided into two divisions. Division 1: bilateral distal retrusion with a narrow maxillary arch and protruding maxillary incisors. Subdivisions include right or left (unilaterally distal with other characteristics being the same). Division 2: bilateral distal with a normal or square-shaped maxillary arch, retruded maxillary central incisors, labially malposed maxillary lateral incisors, and an excessive vertical overlap. Subdivisions include right or left (unilaterally distal with other characteristics the same). Class III (mesioocclusion): the dental relationship in which the mandibular arch is anterior to the maxillary arch in one or both lateral segments; the mandibular first molar is mesial to the maxillary first molar. The mandibular incisors are usually in anterior cross bite. Subdivisions include right or left (unilaterally mesial with other characteristics the same). Class IV: the dental relationship in which the occlusal relations of the dental arches present the peculiar condition of being in distal occlusion in one lateral half and in mesial occlusion in the other (no longer used).
Angle EM. Classification of malocclusion. Dental Cosmos 1899; 41:248–64, 350–7.
an·tag·on·ist \ăn-tăg’a-nst\ n (1599): 1: a tooth in one jaw that articulates with a tooth in the other jaw—called also dental antagonist 2: a substance that tends to nullify the actions of another, as a drug that binds to cell receptors without eliciting a biologic response 3: a muscle whose action is the direct opposite of another muscle
anterior guidance \ăn-tîr’ē-or gīd’ns\: 1: the influence of the contacting surfaces of anterior teeth on tooth limiting mandibular movements 2: the influence of the contacting surfaces of the guide pin and anterior guide table on articulator movements—usage see ANTERIOR GUIDE TABLE 3: the fabrication of a relationship of the anterior teeth preventing posterior tooth contact in all eccentric mandibular movements—see ANTERIOR PROTECTED ARTICULATION, GROUP FUNCTION, MUTUALLY PROTECTED ARTICULATION
anterior open occlusal relationship \ăn-tîr’ē-or ō’pen a-klōō’zal r-lā’shen-shp’\: the lack of anterior tooth contact in any occluding position of the posterior teeth
arc of closure \ărk ŭv klō’zhur\: the circular or elliptic arc created by closure of the mandible, most often viewed in the mid-sagittal plane, using a reference point on the mandible (frequently either mandibular central incisors’ mesial incisal edge)
arthrodial joint \är-thrō’dē al joint\: a joint that allows gliding motion of the surfaces
ar·tic·u·lar \är tk’ya-ler\ adj (15c): of or relating to a joint
articular capsule \är tk’ya-ler kăp’sel\: the fibrous ligament that encloses a joint and limits its motion. It is lined with the synovial membrane
articular cartilage \är tk’ya-ler kär’tl-j\: a thin layer of hyaline cartilage located on the joint surfaces of some bones not found on the articular surfaces of the temporomandibular joints which is covered with an avascular fibrous tissue
attrition \a-trsh’un\ n (14c): 1: the act of wearing or grinding down by friction 2: the mechanical wear resulting from mastication or parafunction, limited to contacting surfaces of the teeth—comp ABRASION, EROSION
balanced articulation \băl ansd är-tk’ya-lā’shun\: the bilateral, simultaneous, anterior, and posterior occlusal contact of teeth in centric and eccentric positions—see CROSS ARCH B.A., CROSS TOOTH B.A.
balancing interference \băl’ans ng n’ter-fear’ans\: undesirable contact(s) of opposing occlusal surfaces on the nonworking side
Bennett angle \Bn’t ăng’gal\ obs: the angle formed between the sagittal plane and the average path of the advancing condyle as viewed in the horizontal plane during lateral mandibular movements (GPT-4)
Bennett’s movement [Sir Norman Godfrey Bennett, British dental surgeon, 1870–1947]: see LATEROTRUSION
Bennett NG. A contribution to the study of the movements of the mandible. Proc Roy Soc Med (Lond) 1908;1:79–88 (Odont Section)
bilateral balanced articulation: also termed balanced articulation, the bilateral, simultaneous anterior and posterior occlusal contact of teeth in centric and excentric positions
bo·lus \bō’lus\ n (1562): a rounded mass, as a large pill or soft mass of chewed food
border movement \bôr’der mōōv’ment\: mandibular movement at the limits dictated by anatomic structures, as viewed in a given plane
brux·ism \brŭk-sz’em\ n (ca. 1940): 1: the parafunctional grinding of teeth 2: an oral habit consisting of involuntary rhythmic or spasmodic nonfunctional gnashing, grinding, or clenching of teeth, in other than chewing movements of the mandible, which may lead to occlusal trauma—called also tooth grinding, occlusal neurosis
canine protected articulation \kā’nīn pra-tk’tid är-tk’ya-lā’shun\: a form of mutually protected articulation in which the vertical and horizontal overlap of the canine teeth disengage the posterior teeth in the excursive movements of the mandible—comp ANTERIOR PROTECTED ARTICULATION
cap·su·lar \kăp’su-ler\ adj (ca. 1730): pertaining to a capsule
capsular fibrosis \kăp’su-ler fī-brō’ss\: fibrotic contracture of the capsular ligament of the temporomandibular joint
capsular ligament \kăp’su-ler lg’a-ment\: as it relates to the temporomandibular joint, a fibrous structure that separately encapsulates the superior and inferior synovial cavities of the temporomandibular articulation
cap·sule \kăp’sal,-sōōl\ n (1693): a fibrous sac or ligament that encloses a joint and limits its motion. It is lined with synovial membrane
centric relation \sn’trk r-lā’shun\: 1: the maxillomandibular relationship in which the condyles articulate with the thinnest avascular portion of their respective disks with the complex in the anterior-superior position against the shapes of the articular eminencies. This position is independent of tooth contact. This position is clinically discernible when the mandible is directed superior and anteriorly. It is restricted to a purely rotary movement about the transverse horizontal axis (GPT-5) 2: the most retruded physiologic relation of the mandible to the maxillae to and from which the individual can make lateral movements. It is a condition that can exist at various degrees of jaw separation. It occurs around the terminal hinge axis (GPT-3) 3: the most retruded relation of the mandible to the maxillae when the condyles are in the most posterior unstrained position in the glenoid fossae from which lateral movement can be made at any given degree of jaw separation (GPT-1) 4: The most posterior relation of the lower to the upper jaw from which lateral movements can be made at a given vertical dimension (Boucher) 5: a maxilla to mandible relationship in which the condyles and disks are thought to be in the midmost, uppermost position. The position has been difficult to define anatomically but is determined clinically by assessing when the jaw can hinge on a fixed terminal axis (up to 25 mm). It is a clinically determined relationship of the mandible to the maxilla when the condyle disk assemblies are positioned in their most superior position in the mandibular fossae and against the distal slope of the articular eminence (Ash) 6: the relation of the mandible to the maxillae when the condyles are in the uppermost and rearmost position in the glenoid fossae. This position may not be able to be recorded in the presence of dysfunction of the masticatory system 7: a clinically determined position of the mandible placing both condyles into their anterior uppermost position. This can be determined in patients without pain or derangement in the TMJ (Ramsfjord)
Christensen’s phenomenon \Krs’chen-senz f-n m’a-nn’, -nen\ [Carl Christensen, Danish dentist and educator]: eponym for the space that occurs between opposing occlusal surfaces during mandibular protrusion
m’a-nn’, -nen\ [Carl Christensen, Danish dentist and educator]: eponym for the space that occurs between opposing occlusal surfaces during mandibular protrusion
Christensen C. The problem of the bite. D Cosmos 1905;47:1184–95.
clench·ing \kln’chng\ vt (13c): the pressing and clamping of the jaws and teeth together frequently associated with acute nervous tension or physical effort
click·ing \kl’kng\ n (611): a series of clicks, such as the snapping, cracking, or noise evident on excursions of the mandible; a distinct snapping sound or sensation, usually audible (or by stethoscope) or on palpation, which emanates from the temporomandibular joint(s) during jaw movement. It may or may not be associated with internal derangements of the temporomandibular joint
condylar path \kn’da-lar păth\: that path traveled by the mandibular condyle in the temporomandibular joint during various mandibular movements
condylar path element \kn’da-lar păth l’a-ment\: the member of a dental articulator that controls the direction of condylar movement
coronoid process \kôr’a-noid’, kr’- pro-ss\: the thin triangular rounded eminence originating from the anterosuperior surface of the ramus of the mandible—see HYPERPLASIA OF THE C.P.
defective occlusal contact \d-fk’tv a-klōō’sal kn’tăkt’\ obs: contact that is capable of guiding the mandible from its original path of action into a different path of motion or capable of disturbing the relation between a denture base and its supporting tissues (GPT-1)
delayed disclusion \d-lād’ ds-klōō’shun\: deferred separation of the posterior teeth due to the anterior guidance
dental articulation \dn’tl är-tk’ya-lā’shun\: the contact relationships of maxillary and mandibular teeth as they move against each other—usage: this is a dynamic process
determinants of mandibular movement \d-tûr’ma-nent\: those anatomic structures that dictate or limit the movements of the mandible. The anterior determinant of mandibular movement is the dental articulation. The posterior determinants of mandibular movement are the temporomandibular articulations and their associated structures
de·tru·sion \dē-trōō’shun\ n: downward movement of the mandibular condyle
de·vi·a·tion \dē’vē-ā’shun\ n (15c): with respect to movement of the mandible, a discursive movement that ends in the centered position and is indicative of interference during movement
disk-condyle complex \dsk-kn’dīl, -dl km’plks’\: the condyle and its disk articulation that functions as a simple hinge joint
disk \dsk\ n (1664): with respect to the temporomandibular joint, the avascular intraarticular tissue—spelled also disc
dis·oc·clu·sion \ds′a-kiōō′zhen\ vb: separation of opposing teeth during eccentric movemets of the mandible—see DELAYED D., IMMEDIATE D.
dynamic relations \dī-năm’k r-lā’shunz\ obs: relations of two objects involving the element of relative movement of one object to another, as the relationship of the mandible to the maxillae (GPT-4)
dys·func·tion \ds-fŭngk’shun\ n (ca. 1916): the presence of functional disharmony between the morphologic form (teeth, occlusion, bones, joints) and function (muscles, nerves) that may result in pathologic changes in the tissues or produce a functional disturbance
eccentric \k-sn’trk\ adj (14c): 1: not having the same center 2: deviating from a circular path 3: located elsewhere than at the geometric center 4: any position of the mandible other than that which is its normal position
edge to edge articulation \j tōō j är-tk’ya-lā’shun\: articulation in which the opposing anterior teeth meet along their incisal edges when the teeth are in maximum intercuspation
elevator muscle \l’a-vā’ter mŭs’el\: one of the muscles that, on contracting, elevates or closes the mandible
envelope of function \n’va-lōp ŭv fŭngk’shun\: the three-dimensional space contained within the envelope of motion that defines mandibular movement during masticatory function and/or phonation
envelope of motion \n’va-lōp ŭv mō’shun\: the three-dimensional space circumscribed by mandibular border movements within which all unstrained mandibular movement occurs
e·ro·sion \-rō’zhun\ n (1541): 1: an eating away; a type of ulceration 2: in dentistry, the progressive loss of tooth substance by chemical processes that do not involve bacterial action producing defects that are sharply defined, wedge-shaped depressions often in facial and cervical areas—comp ABFRACTION, ABRASION, ATTRITION
ex·cur·sion \k-skûr’shun\ n (1577): 1: a movement outward and back or from a mean position or axis; also, the distance traversed 2: in dentistry, the movement occurring when the mandible moves away from maximum intercuspation
excursive movement \k-skûr’sv mōōv’ment\: movement occurring when the mandible moves away from maximum intercuspation
excursive movement \k-skûr’sv mōōv’ment\: movement occurring when the mandible moves away from maximum intercuspation
FGP: acronym for Functionally Generated Path
frontal plane \frŭn’tl\: any plane parallel with the long axis of the body and at right angles to the median plane, thus dividing the body into front and back parts. So called because this plane roughly parallels the frontal suture of the skull
functional mandibular movements’ \fŭngk’sha-nal măn-db’ū-lar mōōv’ments\: all normal, proper, or characteristic movements of the mandible made during speech, mastication, yawning, swallowing, and other associated movements
gnath·ol·o·gy \năth’l-a-gē\ n: the science that treats the biology of the masticatory mechanism as a whole: that is, the morphology, anatomy, histology, physiology, pathology, and the therapeutics of the jaws or masticatory system and the teeth as they relate to the health of the whole body, including applicable diagnostic, therapeutic, and rehabilitation procedures
group function \grōōp fŭngk’shun\: multiple contact relations between the maxillary and mandibular teeth in lateral movements on the working side whereby simultaneous contact of several teeth acts as a group to distribute occlusal forces
Hanau’s Quint [Rudolph L. Hanau, (1881–1930) Buffalo, New York, U.S. engineer, born Capetown, South Africa]: rules for balanced denture articulation including incisal guidance, condylar guidance, cusp length, the plane of occlusion, and the compensating curve described by Rudolph Hanau in 1926
Hanau R. Articulation defined, analyzed, and formulated. J Am Dent Assoc 1926;13:1694–709.
horizontal plane \hôr’-zn’tl, hr- plān\: any plane passing through the body at right angles to both the median and frontal planes, thus dividing the body into upper and lower parts; in dentistry, the plane passing through a tooth at right angles to its long axis
horizontal overlap \hôr’-zn-tl, hr’- ō’ver-lăp’\: the projection of teeth beyond their antagonists in the horizontal plane
immediate mandibular lateral translation \-mē’dē-t măn-db’ya-lar lăt’ar-al trăns-lā’shun\: the translatory portion of lateral movement in which the nonworking side condyle moves essentially straight and medially as it leaves the centric relation position—see also EARLY MANDIBULAR LATERAL TRANSLATION; PROGRESSIVE MANDIBULAR LATERAL TRANSLATION
incisal guidance \n-s’zal gīd’ans\: 1: the influence of the contacting surfaces of the mandibular and maxillary anterior teeth on mandibular movements 2: the influence of the contacting surfaces of the guide pin and guide table on articulator movements
incisal guide angle \n-s’zal gīd ăng’gal\: 1: anatomically, the angle formed by the intersection of the plane of occlusion and a line within the sagittal plane determined by the incisal edges of the maxillary and mandibular central incisors when the teeth are in maximum intercuspation 2: on an articulator, that angle formed, in the sagittal plane, between the plane of reference and the slope of the anterior guide table, as viewed in the sagittal plane
instantaneous axis of rotation \n’stan-tā’nē-as ăk’ss ŭv rō-tā’shun\: the hypothetical center of rotation of a moving body, viewed in a given plane, at any point in time; for any body that has planar motion, there exists, at any instant, some points that have zero velocity and will be fixed at a given instant. The line joining these points is the instantaneous axis of rotation. The intersection of this line with the plane of motion is called the instantaneous center of rotation
intercondylar distance \n’ter-kn’da-lar ds’tans\: the distance between the occluding surfaces of the maxillary and mandibular teeth when the mandible is in a specific position
in·ter·fer·ence \n’ter-fîr’ans\ n (1783): in dentistry, any tooth contacts that interfere with or hinder harmonious mandibular movement
isometric contraction \ī’sa-mt’rk kon-trăk’shun\: muscular contraction in which there is no change in the length of the muscle during contraction
lateral condylar path \lăt’ar-al kn’da-lar păth\: the path of movement of the condyle-disk assembly in the joint cavity when a lateral mandibular movement is made
lateral mandibular relation \lăt’ar-al măn-db’ya-lar r-lā’shun\: the relationship of the mandible to the maxillae in a position to the left or right of the midsagittal plane
lateral movement \lăt’ar-al mōōv’ment\ obs: a movement from either right or left of the midsagittal plane (GPT-4)
lat·ero·de·tru·sion \lăt’ar-ō-de-trōō’zhun\ n: lateral and downward movement of the condyle on the working side—see LATEROTRUSION
lat·ero·pro·tru·sion \lăt’ar-al-prō-trōō’zhun\ n: a protrusive movement of the mandibular condyle in which there is a lateral component
lat·ero·re·tru·sion \lăt-ar-ō-r-trōō’shun\ n: lateral and backward movement of the condyle on the working side
lat·ero·sur·tru·sion \lăt-ar-ō-sûr-trōō’shun\ n: lateral and upward movement of the condyle on the working side—see LATEROTRUSION
lat·ero·tru·sion \lăt-ar-ō-trōō’shun\ n: condylar movement on the working side in the horizontal plane. This term may be used in combination with terms describing condylar movement in other planes, for example, laterodetrusion, lateroprotrusion, lateroretrusion, and laterosurtrusion
mal·oc·clu·sion \măl’a-klōō’shun\ n (1888): 1: any deviation from a physiologically acceptable contact between the opposing dental arches 2: any deviation from a normal occlusion—see ANGLE’s CLASSIFICATION OF OCCLUSION
man·di·ble \măn’da-bal\ n (15c): the lower jawbone
mandibular condyle: the articular process of the mandible, called also the head of the mandible—see also CONDYLE
mandibular hinge position \măn-db’ya-lar hnj pa-zish’an\ obs: the position of the mandible in relation to the maxilla at which opening and closing movements can be made on the hinge axis (GPT-4)
mandibular movement \măn-db’ya-lar mōōv’ment\: any movement of the lower jaw
mandibular side shift: see MANDIBULAR TRANSLATION
mandibular translation \măn-db’ya-lar trăns-lā’shun\: the translatory (medio-lateral) movement of the mandible when viewed in the frontal plane. While this has not been demonstrated to occur as an immediate horizontal movement when viewed in the frontal plane, it could theoretically occur in an essentially pure translatory form in the early part of the motion or in combination with rotation in the latter part of the motion or both—see also EARLY MANDIBULAR LATERAL TRANSLATION, IMMEDIATE MANDIBULAR LATERAL TRANSLATION, PROGRESSIVE MANDIBULAR LATERAL TRANSLATION
mas·ti·ca·tion \măs’t-kā’shun\ n (1649): the process of chewing food for swallowing and digestion
masticatory cycle \măs’t-ka-tôr’ē, -tōr’ē sī’kal\: a three dimensional representation of mandibular movement produced during the chewing of food
masticatory performance \măs’t-ka-tôr’ē par-fôr’mans\: a measure of the comminution of food attainable under standardized testing conditions
maximal intercuspal contacts \măk’sa-mal n’ter-kŭs’pal’ kn’tăkts’\: tooth contact in the maximum intercuspal position
maximal intercuspal position \măk’sa-mal n’ter-kŭs’pal’ pa-zsh’an\: the complete intercuspation of the opposing teeth independent of condylar position, sometimes referred to as the best fit of the teeth regardless of the condylar position—called also maximal intercuspation—comp CENTRIC OCCLUSION
median line \mē’dē-an līn\: the centerline dividing a body into the right and left
me·di·o·tru·sion \mē’dē-ō-trōō’shun\ n: a movement of the condyle medially—see NONWORKING SIDE
me·nis·cus \ma-ns’kas\ n, pl me·nis·ci \ma-ns’ī\: see DISK
mus·cle \mŭs’al\ n (14c): an organ that by contraction produces movements of an animal; a tissue composed of contractile cells or fibers that effect movement of an organ or part of the body
muscle hyperalgesia \mŭs’al hī’par-ăl-gē’sha\: increased sensitivity to pain in a muscle evoked by stimulation at the site of pain in the muscle
muscle marking: see BORDER MOLDING
muscular splinting \mŭs-kya’lar splnt’ng\: contraction of a muscle or group of muscles attended by interference with function and producing involuntary movement and distortion; differs from muscle spasm in that the contraction is not sustained when the muscle is at rest
musculoskeletal pain \mŭs’kya-lō-skl’-tl pān\: deep, somatic pain that originates in skeletal muscles, facial sheaths, and tendons (myogenous pain), bone and periosteum (osseous pain), joint, joint capsules, and ligaments (arthralgic pain), and in soft connective tissues
mutually protected articulation \myōō’chōō-al-lē pra-tk’td är-tk’ya-lā’shun\: an occlusal scheme in which the posterior teeth prevent excessive contact of the anterior teeth in maximum intercuspation, and the anterior teeth disengage the posterior teeth in all mandibular excursive movements. Alternatively, an occlusal scheme in which the anterior teeth disengage the posterior teeth in all mandibular excursive movements, and the posterior teeth prevent excessive contact of the anterior teeth in maximum intercuspation
mutually protected occlusion: see MUTUALLY PROTECTED ARTICULATION
my·al·gia \mī-ăl’jē-a\ n (1860): pain in a muscle or muscles
mylohyoid concavity \mī’la-hoid kn-kăv’-tē\: the fossa in the mandible below the mylohyoid line in the molar region
my·o·cen·tric \mī’a-sn’trk\ adj: that terminal point in space in which, with the mandible in rest position, subsequent colonic muscle contraction will raise the mandible through the interocclusal space along the myocentric (muscle balanced) trajectory. Also described as the initial occlusal contact along the myocentric trajectory (isotonic closure of the mandible from rest position)
myogenous pain \mī’a-jēn’ŭs\: deep somatic musculoskeletal pain originating in skeletal muscles, fascial sheaths, or tendons
neck of the condylar process \nk ŭv tha kn’dah lr pr ss\: the constricted inferior portion of the mandibular condylar process that is continuous with the ramus of the mandible; that portion of the condylar process that connects the mandibular ramus to the condyle
nonworking side \nn-wûr’kng sīd\: that side of the mandible that moves toward the median line in a lateral excursion. The condyle on that side is referred to as the nonworking side condyle
nonworking side condyle \nn-wûr’kng sīd kn’dl\: the condyle on the nonworking side
nonworking side interference \nn-wûr’kng sīd n’tar-fîr’ans\: undesirable contacts of the opposing occlusal surfaces on the nonworking side
noxious stimulus \nk’shas stm’ya-las\: a tissue damaging stimulus
oc·clu·sal \a-klōō’zal, -sal\ adj (1897): pertaining to the masticatory surfaces of the posterior teeth, prostheses, or occlusion rims
occlusal balance \a-klōō’zal, -sal băl’ans\: a condition in which there are simultaneous contacts of opposing teeth or tooth analogues (i.e., occlusion rims) on both sides of the opposing dental arches during eccentric movements within the functional range
occlusal contact \a-klōō’zal, -sal kn’tăkt’\: 1: the touching of opposing teeth on elevation of the mandible 2: any contact relation of opposing teeth—see DEFLECTIVE O.C, INITIAL O.C
occlusal device \a-klōō’zal, -sal d-vīs’\: any removable artificial occlusal surface used for diagnosis or therapy affecting the relationship of the mandible to the maxillae. It may be used for occlusal stabilization, for treatment of temporomandibular disorders, or to prevent wear of the dentition
occlusal disharmony \a-klōō’zal, -sal ds-hăr’ma-nē\: a phenomenon in which contacts of opposing occlusal surfaces are not in harmony with other tooth contacts and/or the anatomic and physiologic components of the craniomandibular complex
occlusal wear \a-klōō’zal, -sal wâr\: loss of substance on opposing occlusal units or surfaces as the result of attrition or abrasion
occlusion \a-klōō’shun\ n (1645): 1: the act or process of closure or of being closed or shut off 2: the static relationship between the incising or masticating surfaces of the maxillary or mandibular teeth or tooth analogues—see CENTRIC O., COMPONENTS OF O., ECCENTRIC O., LINE OF O., LINEAR O., MONOPLANE O., PATHOGENIC O., SPHERICAL FORM OF O.—comp ARTICULATION
open occlusal relationship \ō’pan a-klōō’zal, -sal r-lā’shun-shp’\: the lack of tooth contact in an occluding position—see ANTERIOR O.O.R., POSTERIOR O.O.R.
opening movement \ō’pa-nng\ obs: movement of the mandible executed during jaw separation; movement executed during jaw separation (GPT-1)—see ENVELOPE OF MOTION
para·func·tion \păr’a-fŭngk’shun\ adj: disordered or perverted function
pathogenic occlusion \păth’a-jn’k\: an occlusal relationship capable of producing pathologic changes in the stomatognathic system
posterior \p-stîr’ē-ar, pō-\ adj (1534): 1: situated behind or in back of; caudal 2: in human anatomy, dorsal
posterior border movement \p-stîr’ē-ar, pō- bôr’dar mōōv’mant\: movements of the mandible along the posterior limit of the envelope of motion
posterior determinants of mandibular movement \p-stîr’ē-ar, pō- d-tûr’ma-nant ŭv măn’db-ū-lar mōōv’mant\: the temporomandibular articulations and associated structures—see DETERMINANTS OF MANDIBULAR MOVEMENT
posterior determinants of occlusion: see DETERMINANTS OF MANDIBULAR MOVEMENT
progressive mandibular lateral translation \pra-grs’v măn-db’ya-lar lăt’ar-al trăns-lā’shun\: 1: the translatory portion of mandibular movement when viewed in a specified body plane 2: the translatory portion of mandibular movement as viewed in a specific body plane that occurs at a rate or amount that is directly proportional to the forward movement of the nonworking condyle—see MANDIBULAR TRANSLATION
proprioception \prō’prē-ō-sp’shun\ n (1906): the reception of stimulation of sensory nerve terminals within the tissues of the body that give information concerning movements and the position of the body; perception mediated by proprioceptors
pro·tru·sion \prō-trōō’zhan\ n (1646): a position of the mandible anterior to centric relation—see LATEROPROTRUSION
protrusive condyle path \prō-trōō’sv kn’dīl’, -dl păth\: the path the condyle travels when the mandible is moved forward from its initial position
pterygoid plates \tr’-goid’ plātz\: broad, thin, wing-shaped processes of the spheroid bone separated by the pterygoid fossa. The inferior end of the medial plate terminates in a long curved process or hook for the tendon of the tensor veli palatini muscle. The lateral plate gives attachment to the medial and lateral pterygoid muscles
retrodiscal tissue \rt’rō-ds’kal tsh’ōō\: a mass of loose, highly vascular and highly innervated, connective tissue attached to the posterior edge of the articular disk and extending to and filling the loose folds of the posterior capsule of the temporomandibular joint—called also bilaminar zone
retruded contact position \r-trōō’dd kn’tăkt pa-zsh’an\: that guided occlusal relationship occurring at the most retruded position of the condyles in the joint cavities. A position that may be more retruded than the centric relation position
re·tru·sion \r-trōō’shun\ vb: movement toward the posterior
re·tru·sive \r-trōō’sv\ adj: denotes a posterior location
ro·ta·tion \rō-tā’shun\ n (1555): 1: the action or process of rotating on or as if on an axis or center 2: the movement of a rigid body in which the parts move in circular paths with their centers on a fixed line called the axis of rotation. The plane of the circle in which the body moves is perpendicular to the axis of rotation
sag·it·tal \săj’-tl\ adj (1541): situated in the plane of the cranial sagittal suture or parallel to that plane—usage: see SAGITTAL PLANE
sagittal plane \săj’-tl plān\: any vertical plane or section parallel to the median plane of the body that divides a body into right and left portions
silent period \sī’lant pr’ē-ad\: a momentary electormyographic decrease in elevator muscle activity on initial tooth contact presumably due to the inhibitory effect of stimulated periodontal membrane receptors
speaking space \spē’kng spās\: the space that occurs between the incisal or/and occlusal surfaces of the maxillary and mandibular teeth during speech
1splint \splnt\ n (14c): 1: a rigid or flexible device that maintains in position a displaced or movable part; also used to keep in place and protect an injured part 2: a rigid or flexible material used to protect, immobilize, or restrict motion in a part—see ANDERSON S., CAP S., ESSIG S., FUNCTIONAL OCCLUSAL S., GUNNING’s S., INTERDENTAL S., KINGSLEY S., LABIAL S., LINGUAL S., PROVISIONAL S., RESIN-BONDED S., SOFT S., SURGICAL S., WIRE S.
static relation \stăt’k r-lā’shun\: the relationship between two parts that are not in motion
stomatognathic system \stō-măt’a-nā’thk ss’tum\: the combination of structures involved in speech, receiving, mastication, and deglutition as well as parafunctional actions
synovial fluid \s-nō’vē-al flōō’d\: a viscid fluid contained in joint cavities and secreted by the synovial membrane
temporomandibular disorders \tm’pa-rō’măn-db’ya-lar ds-ôr’derz\: 1: conditions producing abnormal, incomplete, or impaired function of the temporomandibular joint(s) 2: (obs) a collection of symptoms frequently observed in various combinations first described by Costen (1934, 1937), which he claimed to be reflexes due to irritation of the auriculotemporal and/or chorda tympanic nerves as they emerged from the tympanic plate caused by altered anatomic relations and derangements of the temporomandibular joint associated with loss of occlusal vertical dimension, loss of posterior tooth support, and/or other malocclusions. The symptoms can include headache about the vertex and occiput, tinnitus, pain about the ear, impaired hearing and pain about the tongue—acronym TMD
temporomandibular joint \tm’pa-rō’măn-db’ya-lar joint\: 1. the articulation between the temporal bone and the mandible. It is a bilateral diarthrodial, bilateral ginglymoid joint 2: the articulation of the condylar process of the mandible and the intraarticular disk with the mandibular fossa of the squamous portion of the temporal bone; a diarthrodial, sliding hinge (ginglymus) joint. Movement in the upper joint compartment is mostly translational, whereas that in the lower joint compartment is mostly rotational. The joint connects the mandibular condyle to the articular fossa of the temporal bone with the temporomandibular disk interposed
terminal hinge axis: see TRANSVERSE HORIZONTAL AXIS
TMD: acronym for TemporoMandibular Disorders—see TEMPOROMANDIBULAR DISORDERS
trans·la·tion \trăn-zsh’an, -ssh’-\ n (14c): that motion of a rigid body in which a straight line passing through any two points always remains parallel to its initial position. The motion may be described as a sliding or gliding motion
translatory movement \trăns-lă’tōr-ē\ obs: the motion of a body at any instant when all points within the body are moving at the same velocity and in the same direction (GPT-1)
transverse horizontal axis \trăns-vûrs’, trănz-, trăns’vûrs’, trănz’-\: an imaginary line around which the mandible may rotate within the sagittal plane
traumatogenic occlusion \trou’ma-ta-jn’k a-klōō’zhun\ obs: an occluding of the teeth that is capable of producing injury to oral structures (GPT-4)
vertical axis of the mandible \vûr’t-kul ăk’ss ŭv tha măn’d-bal\: an imaginary line around which the mandible may rotate through the horizontal plane
vertical overlap \vûr’t-kal ō’var-lăp\: 1: the distance teeth lap over their antagonists as measured vertically; especially the distance the maxillary incisal edges extend below those of the mandibular teeth. It may also be used to describe the vertical relations of opposing cusps 2: the vertical relationship of the incisal edges of the maxillary incisors to the mandibular incisors when the teeth are in maximum intercuspation
wear facet \wâr făs’t\: any wear line or plane on a tooth surface caused by attrition
working side \wûr’kng sīd\: the side toward which the mandible moves in a lateral excursion
working side contacts \wûr’kng sīd kn’tăkts\: contacts of teeth made on the side of the articulation toward which the mandible is moved during working movements
STUDY QUESTIONS
1 Okeson JP. Management of Temporomandibular Disorders and Occlusion, 5th ed. St. Louis: Mosby, 2003.
2 Schweitzer JM. Concepts of occlusion: a discussion. Dent Clin North Am. 1963;7:649.
3 Proffit WR, Fields HWJr. Contemporary Orthodontics, 3rd ed. St. Louis: Mosby, 1999.
4 Bennett NG. A contribution to the study of the movements of the mandible. Odontol Sec R Soc Med Trans. 1908;1:79. (Reprinted in J Prosthet Dent 8:41, 1958.)
5 Posselt U. Movement areas of the mandible. J Prosthet Dent. 1957;7:375.
6 Goldenberg BS, et al. The loss of occlusion and its effect on mandibular immediate side shift. J Prosthet Dent. 1990;63:163.
7 Pelletier LB, Campbell SD. Evaluation of the relationship between anterior and posterior functionally disclusive angles. II. Study of a population. J Prosthet Dent. 1990;63:536.
8 Hayasaki H, et al. A calculation method for the range of occluding phase at the lower incisal point during chewing movements using the curved mesh diagram of mandibular excursion (CMDME). J Oral Rehabil. 1999;26:236.
9 Lundeen HC, Gibbs CH. Advances in Occlusion. Boston: John Wright PSG, 1982.
10 Ogawa T, et al. Inclination of the occlusal plane and occlusal guidance as contributing factors in mastication. J Dent. 1998;26:641.
11 Wickwire NA, et al. Chewing patterns in normal children. Angle Orthod. 1981;51:48.
12 Lavigne G, et al. Evidence that periodontal pressoreceptors provide positive feedback to jaw closing muscles during mastication. J Neurophysiol. 1987;58:342.
13 Burnett CA, Clifford TJ. Closest speaking space during the production of sibilant sounds and its value in establishing the vertical dimension of occlusion. J Dent Res. 1993;72:964.
14 Pound E. The mandibular movements of speech and their seven related values. J Prosthet Dent. 1966;16:835.
15 Pound E. Let /S/ be your guide. J Prosthet Dent. 1977;38:482.
16 Howell PG. Incisal relationships during speech. J Prosthet Dent. 1986;56:93.
17 Rivera-Morales WC, Mohl ND. Variability of closest speaking space compared with interocclusal distance in dentulous subjects. J Prosthet Dent. 1991;65:228.
18 Duckro PN, et al. Prevalence of temporomandibular symptoms in a large United States metropolitan area. Cranio. 1990;8:131.
19 Hathaway KM. Bruxism. Definition, measurement, and treatment. In: Fricton JR, Dubner RB, editors. Orofacial Pain and Temporomandibular Disorders. New York: Raven Press, 1995.
20 Hublin C, et al. Sleep bruxism based on self-report in a nationwide twin cohort. J Sleep Res. 1998;7:61.
21 Macaluso GM, et al. Sleep bruxism is a disorder related to periodic arousals during sleep. J Dent Res. 1998;77:565.
22 Madrid G, et al. Cigarette smoking and bruxism. Percept Mot Skills. 1998;87:898.
23 Mongini F, Tempia-Valenta G. A graphic and statistical analysis of the chewing movements in function and dysfunction. J Craniomandib Pract. 1984;2:125.
24 Faulkner KD. Preliminary studies of some masticatory characteristics of bruxism. J Oral Rehabil. 1989;16:221.
25 Mohl ND, et al. Devices for the diagnosis and treatment of temporomandibular disorders. Part I: introduction, scientific evidence, and jaw tracking. J Prosthet Dent. 1990;63:198.
26 Rugh JD, Solberg WK. Electromyographic studies of bruxist behavior before and during treatment. J Calif Dent Assoc. 1975;3(9):56.
27 Lobbezoo F, Lavigne GJ. Do bruxism and temporomandibular disorders have a cause-and-effect relationship? J Orofac Pain. 1997;11:15.
28 Grippo JO. Abfractions: a new classification of hard tissue lesions of teeth. J Esthet Dent. 1991;3:14.
29 Owens BM, Gallien GS. Noncarious dental “abfraction” lesions in an aging population. Compend Contin Educ Dent. 1995;16:552.
30 Sears VH. Balanced occlusions. J Am Dent Assoc. 1925;12:1448.
31 Schuyler CH. Considerations of occlusion in fixed partial dentures. Dent Clin North Am. 1959;3:175.
32 Schuyler CH. An evaluation of incisal guidance and its influence in restorative dentistry. J Prosthet Dent. 1959;9:374.
33 Mann AW, Pankey LD. Concepts of occlusion: the P.M. philosophy of occlusal rehabilitation. Dent Clin North Am. 1963;7:621.
34 Stuart C, Stallard H. Concepts of occlusion. Dent Clin North Am. 1963;7:591.
35 D’Amico A. Functional occlusion of the natural teeth of man. J Prosthet Dent. 1961;11:899.
36 Ogawa T, et al. Pattern of occlusal contacts in lateral positions: canine protection and group function validity in classifying guidance patterns. J Prosthet Dent. 1998;80:67.
37 Bakke M, et al. Occlusal control of mandibular elevator muscles. Scand J Dent Res. 1992;100:284.
38 McDevitt WE, Warreth AA. Occlusal contacts in maximum intercuspation in normal dentitions. J Oral Rehab. 1997;24:725.
39 Dawson PE. Evaluation, Diagnosis, and Treatment of Occlusal Problems, 2nd ed. St. Louis: Mosby, 1989.
40 Stuart CE, Stallard H. Diagnosis and treatment of occlusal relations of the teeth. Texas Dent J. 1957;75:430.
41 Ramfjord S, Ash MM. Occlusion, 4th ed. Philadelphia: WB Saunders, 1994.
42 Ekfeldt A. Incisal and occlusal tooth wear and wear of some prosthodontic materials: an epidemiological and clinical study. Swed Dent J Suppl. 1989;65:1.
43 Imfeld T. Dental erosion. Definition, classification and links. Eur J Oral Sci. 1996;104:151.
44 Lewis KJ, Smith BGN. The relationship of erosion and attrition in extensive tooth loss. Case reports. Br Dent J. 1973;135:400.
45 Rytomaa I, et al. Bulimia and tooth erosion. Acta Odontol Scand. 1998;56:36.
46 Simmons JJ3rd, Hirsh M. Role of chemical erosion in generalized attrition. Quintessence Int. 1998;29:793.
47 Christensen LV. Facial pain and internal pressure of masseter muscle in experimental bruxism in man. Arch Oral Biol. 1971;16:1021.
48 Ishigaki S, et al. Clinical classification of maximal opening and closing movements. Int J Prosthod. 1989;2:148.
49 Leader JK, et al. The influence of mandibular movements on joint sounds in patients with temporomandibular disorders. J Prosthet Dent. 1999;81:186.
50 Mikami DB. A review of psychogenic aspects and treatment of bruxism. J Prosthet Dent. 1977;37:411.
51 Schwartz LL. A temporomandibular joint pain-dysfunction syndrome. J Chron Dis. 1956;3:284.
52 Gelb H. An orthopedic approach to occlusal imbalance and temporomandibular dysfunction. Dent Clin North Am. 1979;23:181.
53 Dawson PE. Position paper regarding diagnosis, management, and treatment of temporomandibular disorders. J Prosthet Dent. 1999;81:174.
54 Okeson JP. Management of Temporomandibular Disorders and Occlusion, 5th ed. St. Louis: Mosby, 1998. chap 15.
55 Dao TT, Lavigne GJ. Oral splints: the crutches for temporomandibular disorders and bruxism? Crit Rev Oral Biol Med. 1998;9:345.