2 DIAGNOSTIC CASTS AND RELATED PROCEDURES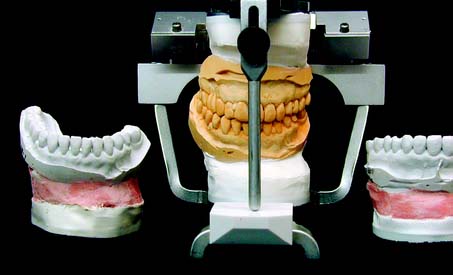
Accurate diagnostic casts (Fig. 2-1) transferred to a semiadjustable articulator are essential in planning fixed prosthodontic treatment. This enables static and dynamic relationships of the teeth to be examined without interference from protective neuromuscular reflexes, and unencumbered views from all directions reveal aspects of the occlusion not always easily detectable intraorally (e.g., the relationship of the lingual cusps in the occluded position). If the maxillary cast has been transferred with a facebow, a centric relation (CR) interocclusal record has been used for articulation of the mandibular cast, and the condylar elements have been appropriately set (such as with protrusive and/or excursive interocclusal records), reproducing the patient’s movements with reasonable accuracy is possible. If the casts have been articulated in CR, assessing both the CR and the maximum intercuspation (MI) position is possible, because any slide can then be reproduced. Other critical information not immediately apparent during the clinical examination includes the occlusocervical dimension of edentulous spaces. On an articulator, these are readily assessed in the occluded position and throughout the entire range of mandibular movement. Relative alignment and angulation of proposed abutment teeth are easier to evaluate on casts than intraorally, as are many other subtle changes in individual tooth position. Articulated diagnostic casts permit a detailed analysis of the occlusal plane and the occlusion, and diagnostic procedures can be performed for a better diagnosis and treatment plan; tooth preparations can be “rehearsed” on the casts, and diagnostic waxing procedures allow evaluation of the eventual outcome of proposed treatment.

Fig. 2-1 Diagnostic casts mounted on a Whip Mix articulator.
(Courtesy of Whip Mix Corporation, Louisville, Kentucky.)
IMPRESSION MAKING FOR DIAGNOSTIC CASTS
Accurate impressions of both dental arches are required. Flaws in the impressions result in inaccuracies in the casts that easily compound. For instance, a small void in the impression caused by the trapping of an air bubble on one of the occlusal surfaces results in a nodule on the occlusal table. If it is not recognized and carefully removed, it leads to an inaccurate articulator mounting, and the diagnostic data are incorrect.
As long as the impression extends several millimeters beyond the cervical line of the teeth, the borders of diagnostic impressions are usually not of great concern for fixed prosthodontic purposes, unless a removable prosthesis is also to be fabricated. Properly manipulated irreversible hydrocolloid (alginate) is sufficiently accurate and offers adequate surface detail for planning purposes. However, the material does not reproduce sufficient surface detail for suitable definitive casts and dies on which actual fixed prostheses are fabricated (see Chapter 17).
Irreversible Hydrocolloid
The irreversible hydrocolloids, or alginates, are essentially sodium or potassium salts of alginic acid and are therefore water soluble. They react chemically with calcium sulfate to produce insoluble calcium alginate. These materials contain other ingredients, chiefly diatomaceous earth (for strength and body), trisodium phosphate (Na3PO4), and similar compounds to control the setting rate as they react preferentially with calcium sulfate. When this reaction is complete and the retarder is consumed, gel formation begins. The clinician can control the reaction rate by varying the temperature of the mixing water. Because irreversible hydrocolloid is largely water, it readily absorbs (by imbibition) as well as gives off (by syneresis) liquid to the atmosphere, causing distortion of the impression. Alginate impressions must therefore be poured immediately.
Diagnostic Impression Technique
Tray selection
All impression materials require retention in the impression tray. This can be provided for irreversible hydrocolloid by using an adhesive or by making perforations or undercuts around the rim of the tray. All types of trays are capable of producing impressions with clinically acceptable accuracy.1 For irreversible hydrocolloids, the largest tray that will fit comfortably in the patient’s mouth should be selected. A greater bulk of material produces a more accurate impression (i.e., a bulky impression has a more favorable surface area/volume ratio and is less susceptible to water loss or gain and therefore unwanted dimensional change). In contrast, elastomeric impression materials work well with a relatively tightly fitting custom impression tray in which a uniform thin layer of material is used. This produces the most accurate impression (see Chapter 14).
Distortion of irreversible hydrocolloid can occur if any part of the impression is unsupported by the tray or if there is movement of the tray during setting. For these reasons, the tray may need to be extended and its perimeter modified with modeling compound (Fig. 2-2).

Fig. 2-2 Stock impression trays can be readily modified with modeling compound to provide better support for the alginate. The posterior border typically needs extension. If the patient has a high palate, the alginate should be supported here, too, although the compound should not block out the retentive area of the tray.
Impression making
For optimum results, the teeth should be cleaned and the mouth thoroughly rinsed. Some drying is necessary, but excessively dried tooth surfaces cause the irreversible hydrocolloid impression material to adhere. The material is mixed to a homogenous consistency and loaded into the tray, and its surface is smoothed with a moistened gloved finger.2 Concurrently, a small amount of material is wiped into the crevices of the occlusal surfaces (Fig. 2-3A,B) before the tray is seated (Fig. 2-3C). Also, a small amount can be applied by wiping it into the mucobuccal fold. As the tray is inserted into the patient’s mouth and seated, the patient is reminded to relax the cheek muscles. If a patient continues to stretch wide open while the tray is being fully seated, impression material is often squeezed out of the mucobuccal fold or from underneath the upper lip.
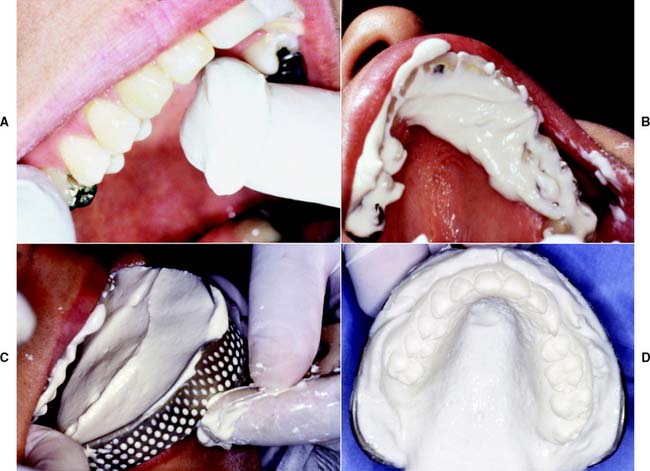
A loss of tackiness of the material (gelation) implies initial set. The tray should be removed quickly 2 to 3 minutes after gelation. Teasing or wiggling the set impression from the mouth causes excessive distortion as a result of viscous flow. Also, certain irreversible hydrocolloid materials become distorted if held in the mouth more than 2 or 3 minutes after gelation.3 After removal (Fig. 2-3D), the impression should be rinsed and disinfected, dried slightly with a gentle air stream, and poured immediately. For disinfection, spraying with a suitable glutaraldehyde and placement in a self-sealing plastic bag for approximately 10 minutes is recommended, after which it can be poured. Alternatively, the impression can be immersed in iodophor or glutaraldehyde disinfectant. The disinfection protocol is an essential precaution for preventing cross-infection and protecting laboratory personnel (see Chapter 14). It should be noted that irreversible hydrocolloid impressions carry significantly higher numbers of bacteria than do elastomeric materials.4 No significant loss of accuracy or surface detail is caused by the disinfection procedure.5,6 To ensure accuracy, pouring should be completed within 15 minutes after the impression is removed from the mouth. Keeping an impression in a moist towel is no substitute for pouring within the specified time. Trimming off gross excess impression material before setting the tray down on the bench top is helpful. A vacuum-mixed ADA type IV or type V stone is recommended. The choice of the brand of stone is important because of the harmful surface interactions between specific irreversible hydrocolloid materials and gypsum products.7
After mixing, a small amount of stone is added in one location (e.g., the posterior aspect of one of the molars). Adding small amounts consistently in the same location helps minimize bubble formation (see the section on pouring stone dies in Chapter 17). If air is trapped, bubbles can be eliminated by poking at them with a small instrument (e.g., a periodontal probe or a wax spatula). While setting, the poured impressions must be stored tray side down, not inverted. Inverting freshly poured impressions results in a cast with a rough and grainy surface.8 Stone is added to create a sufficient base that provides adequate retention for mounting on the articulator. To achieve maximum strength and surface detail, the poured impression should be covered with wet paper and stored in a humidor for 1 hour. This minimizes distortion of the irreversible hydrocolloid during the setting period. The setting gypsum cast should never be immersed in water. If this is done, setting expansion of plaster, stone, or die stone doubles or even triples through the phenomenon of hygroscopic expansion (see Chapter 22). For best results, the cast should be separated 1 hour after pouring.
Evaluation
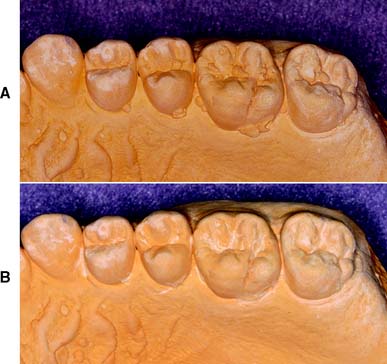
Although it is apparently a simple procedure, diagnostic cast fabrication is often mishandled. Seemingly minor inaccuracies can lead to serious diagnostic errors. Questionable impressions and casts should be discarded and the process repeated (Fig. 2-4). Voids in the impression create nodules on the poured cast. These can prevent proper articulation and effectively render useless a subsequent occlusal analysis or other diagnostic procedure.
Articulator selection
Handheld casts can provide information concerning alignment of the individual arches but do not enable analysis of functional relationships. For an analysis, the diagnostic casts need to be attached to an articulator, a mechanical device that simulates mandibular movement. Articulators can simulate the movement of the condyles in their corresponding fossae. They are classified according to how closely they can reproduce mandibular border movements. Because the movements are governed by the bones and ligaments of the temporomandibular joints, they are relatively constant and reproducible. With most articulators, mechanically adjustable posterior controls are used to simulate these movements; in some, plastic premilled or customized fossa analogs are used. If an articulator closely reproduces the actual border movements of a given patient, chair time is significantly reduced because the dental laboratory can then design the prosthesis to be in functional harmony with the patient’s movements. In addition, less time is needed for adjustments at delivery.
On some instruments, the upper and lower members are permanently attached to each other, whereas on others they can be readily separated. The latter instruments may have a latch or clamplike feature that locks the two components together in the hinge position. Instrument selection depends on the type and complexity of treatment needs, the demands for procedural accuracy, and general expediency. For instance, when a fixed dental prosthesis is waxed, it is advantageous to be able to separate the instrument into two more easily handled parts. Use of the proper instrument for a given procedure can translate into significant time saving during subsequent stages of treatment.
Small Nonadjustable Articulators
Many cast restorations are made on small nonadjustable articulators (Fig. 2-5). Their use often leads to restorations with occlusal discrepancies, because these instruments do not have the capacity to reproduce the full range of mandibular movement. Some discrepancies can be corrected intraorally, but this is often time consuming and leads to increased inaccuracy. If discrepancies are left uncorrected, occlusal interferences and associated neuromuscular disorders may result.

Of practical significance are differences between the hinge closure of a small articulator and that of the patient. The distance between the hinge and the tooth to be restored is significantly less on most nonadjustable articulators than in the patient. This can lead to restorations with premature tooth contacts because cusp position is affected. This type of arcing motion on the nonadjustable articulator results in steeper travel than occurs clinically, which subsequently results in premature contacts on fabricated restorations between the distal mandibular inclines and the mesial maxillary inclines of posterior teeth (Fig. 2-6).
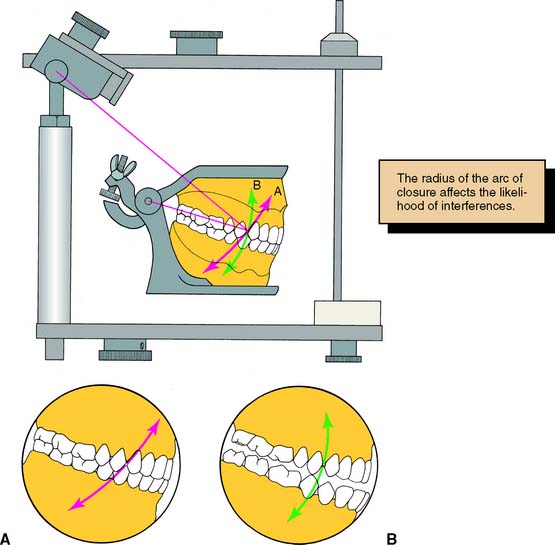
Fig. 2-6 Discrepancies in the path of closure when using a small nonadjustable articulator can lead to restorations with premature occlusal contacts. A, Path of closure of an anatomically accurate articulator. B, The small nonadjustable instrument has a smaller radius closure path, which results in premature contact at the clinical try-in between the premolars during hinge closure.
Depending on the specific design of the articulator, ridge and groove direction may be affected in accordance with the same principle. This is important to note, because resulting prematurities are likely on the nonworking side (see Chapters 1, 4, and 6).
Semiadjustable Articulators
For most routine fixed prostheses, the use of a semiadjustable articulator (Fig. 2-7) is a practical approach to providing the necessary diagnostic information while minimizing the need for clinical adjustment during treatment. The use of semiadjustable instruments does not require an inordinate amount of time or expertise. They are about the same size as the anatomic structures they represent. Therefore, the articulated casts can be positioned with sufficient accuracy so that arcing errors are minimal and usually of minimal clinical significance (i.e., minimal time should be required for chairside adjustments of fabricated prostheses).
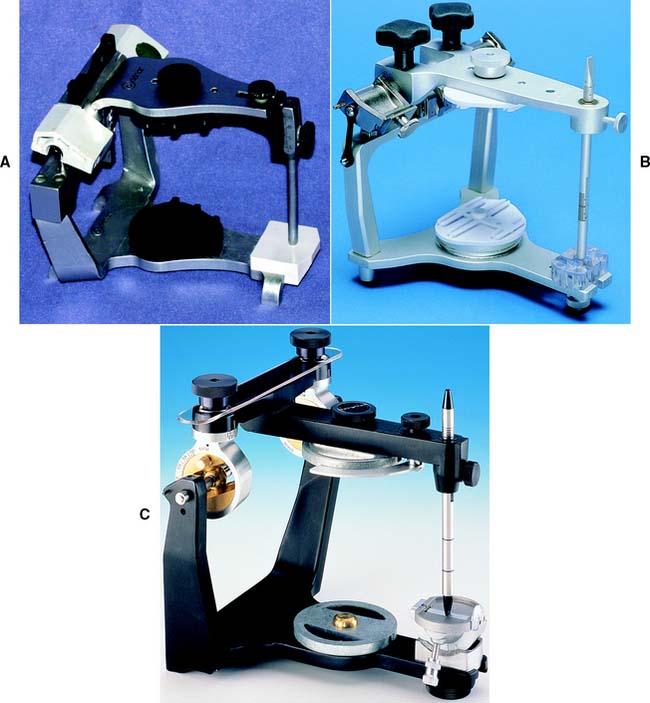
Fig. 2-7 Semiadjustable arcon articulators. A, The Denar Anamark. B, The Whip Mix model 2240. C, The Hanau Wide-Vue.
(A and C, Courtesy of Waterpik Technologies, Inc., Fort Collins, Colorado. B, Courtesy of Whip Mix Corporation, Louisville, Kentucky.)
There are two basic designs of the semiadjustable articulator: the arcon (for articulator and condyle) (Fig. 2-8A,C) and the nonarcon (Fig. 2-8B,D). Nonarcon instruments gained considerable popularity in complete denture prosthodontics because the upper and lower members are rigidly attached, enabling easier control when artificial teeth are positioned. As a consequence of their design, however, certain inaccuracies occur in cast restorations, which led to the development of the arcon-type instrument.
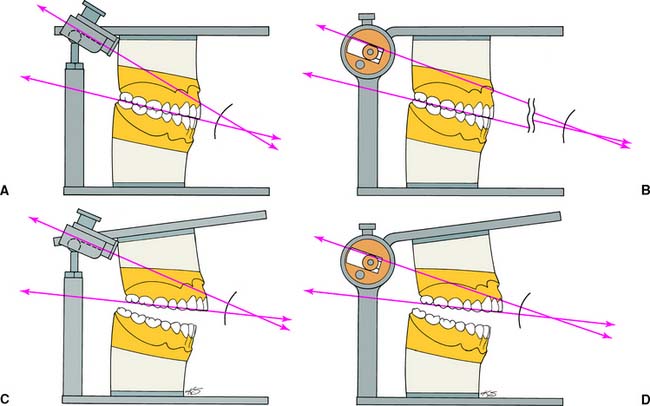
Fig. 2-8 Articulators. A and C show an arcon articulator; B and D show a nonarcon articulator. An advantage of the arcon design is that the condylar inclination of the mechanical fossae is at a fixed angle to the maxillary occlusal plane. With the nonarcon design, the angle changes as the articulator is opened, which can lead to errors when a protrusive record is being used to program the articulator.
(Redrawn from Shillingburg HT, et al: Fundamentals of Fixed Prosthodontics, 2nd ed. Chicago, Quintessence Publishing, 1981.)
In an arcon articulator, the condylar spheres are attached to the lower component of the articulator, and the mechanical fossae are attached to the upper member of the instrument. Thus, the arcon articulator is anatomically “correct,” which makes understanding of mandibular movements easier, as opposed to the nonarcon articulator (whose movements are confusingly “backwards”). The angulation of the mechanical fossae of an arcon instrument is fixed in relation to the occlusal plane of the maxillary cast; in the nonarcon design, it is fixed in relation to the occlusal plane of the mandibular cast.
Most semiadjustable articulators permit adjustments to the condylar inclination and progressive and/or immediate side shift. Some have straight condylar inclined paths, although more recent instruments have curved condylar housings, which are more anatomically correct.
The mechanical fossae on semiadjustable articulators can be adjusted to mimic the movements of the patient through the use of interocclusal records. These consist of several thicknesses of wax or another suitable material in which the patient has closed into. Because these records can be several millimeters thick, an error is introduced when nonarcon articulators are set with protrusive wax records, because the condylar path is not fixed in relation to the maxillary occlusal plane. As the protrusive record used to adjust the instrument is removed from the arcon articulator, the maxillary occlusal plane and the condylar inclination become more parallel, which leads to reduced cuspal heights in subsequently fabricated prostheses (see Table 4-3).
Fully Adjustable Articulators
A fully (or highly) adjustable articulator (Fig. 2-9) has a wide range of positions and can be set to follow a patient’s border movements. The accuracy of reproduction of movement depends on the care and skill of the operator, the errors inherent in the articulator and recording device, and any malalignments resulting from slight flexing of the mandible and the nonrigid nature of the temporomandibular joints.
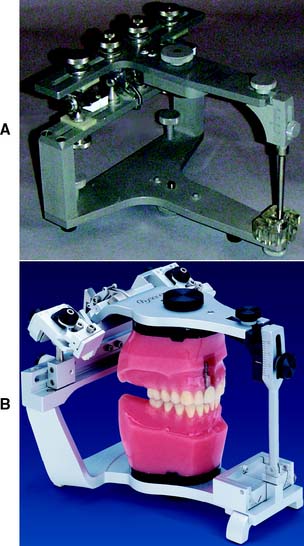
Fig. 2-9 Fully adjustable articulators. A, The Stuart. B, The Denar D5A.
(B, Courtesy of Waterpik Technologies, Inc., Fort Collins, Colorado.)
Rather than relying on wax records to adjust the instrument, special pantographic tracings are used to record the patient’s border movements in a series of tracings. The armamentarium used to generate these tracings is then transferred to the articulator, and the instrument is adjusted so that the articulator replicates the tracings, essentially reproducing the border movements of the patient. The ability of fully adjustable instruments to track irregular pathways of movement throughout entire trajectories enables the fabrication of complex prostheses, which require minimal adjustment at the evaluation and delivery appointment.
Fully adjustable articulators are not often required in general practice. Using and adjusting them can be time consuming and require a high level of skill and understanding of the dentist and the technician. Once this skill has been acquired, however, the detailed information they convey can save considerable chairside time. They can be very useful as treatment complexity increases (e.g., when all four posterior quadrants are to be restored simultaneously or when it is necessary to restore an entire dentition, especially in the presence of atypical mandibular movement).
FACEBOWS
Transverse Horizontal Axis
The mandibular hinging movement around the transverse horizontal axis is repeatable. Therefore, this imaginary hinge axis around which the mandible may rotate in the sagittal plane is of considerable importance when fixed prostheses are fabricated. Facebows are used to record the anteroposterior and mediolateral spatial position of the maxillary occlusal surfaces in relation to this transverse opening and closing axis of the patient’s mandible. The facebow is then attached to the articulator to transfer the recorded relationship of the maxilla by ensuring that the corresponding cast is attached in the correct position in relation to the hinge axis of the instrument. After the maxillary cast has been attached to the articulator with mounting stone or plaster, the mandibular cast is subsequently related to the maxillary cast with an interocclusal record. If the patient’s casts are accurately transferred to an instrument, considerable time is saved in the fabrication and delivery of high-quality prostheses.
Most facebows are rigid, caliper-like devices that allow some adjustments. Two types of facebows are recognized: arbitrary and kinematic. Arbitrary facebows are less accurate than the kinematic type, but they suffice for most routine dental procedures. Kinematic facebows are indicated when it is crucial to precisely reproduce the exact opening and closing movements of the patient on the articulator. For instance, when a decision to alter the occlusal vertical dimension is to be made in the dental laboratory during the fabrication of fixed prostheses, the use of a kinematic facebow transfer in conjunction with an accurate CR interocclusal record is indicated.
Kinematic Hinge Axis Facebow
Hinge axis recording
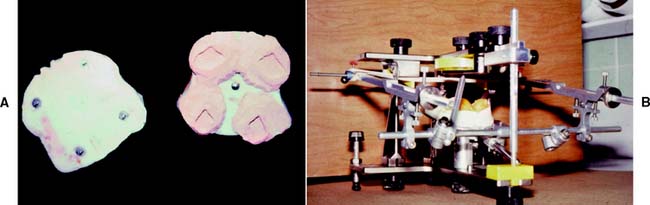
The hinge axis of the mandible can be determined to within 1 mm by observing the movement of kinematic facebow styli positioned immediately lateral to the temporomandibular joint close to the skin. A clutch, which is essentially a segmented impression-traylike device, is attached to the mandibular teeth with a suitable rigid material such as impression plaster. The kinematic facebow consists of three components: a transverse component and two adjustable side arms. The transverse rod is attached to the portion of the clutch that protrudes from the patient’s mouth. The side arms are then attached to the transverse member and adjusted so that the styli are as close to the joint area as possible. The mandible is then manipulated to produce a terminal hinge movement, and the stylus locations are adjusted with thumbscrews (superiorly and inferiorly, anteriorly and posteriorly) until they make a purely rotational movement (Fig. 2-10). Because the entire assembly is rigidly attached to the mandible, a strictly rotational movement signifies that stylus position coincides with the hinge axis. When this purely rotational movement is verified, the position of the hinge axis is marked with a dot on the patient’s skin, or it may be permanently tattooed if future use is anticipated or required.
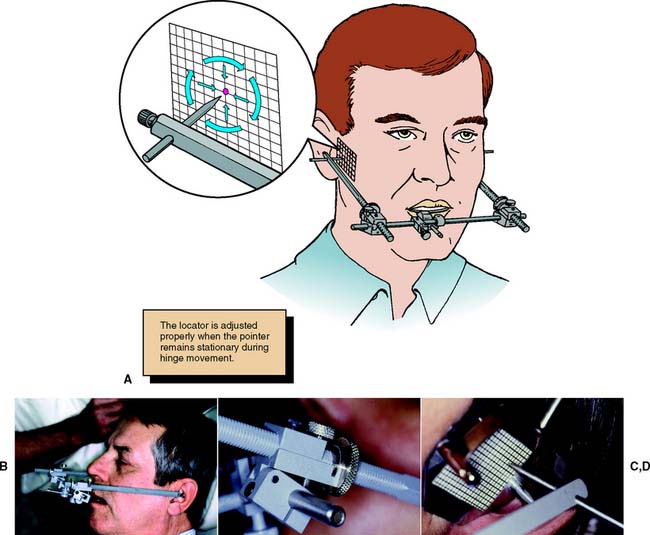
Fig. 2-10 Hinge axis recording. A, Left and right styli are attached via a facebow to a clutch affixed to the mandibular teeth. When the mandible makes a strictly rotational movement, the stylus remains stationary if aligned with the actual axis of rotation. If the stylus is positioned forward or backward, above or below the actual axis, it travels one of the arcs indicated by the arrows when the mandible makes a rotational movement. Thus, the arc indicates in what direction an adjustment should be made to the stylus position. B, Hinge axis locator positioned. C, Set screws allow side arm adjustment. D, Adjustment continues until no arcing of the pointer is seen.
Kinematic facebow transfer
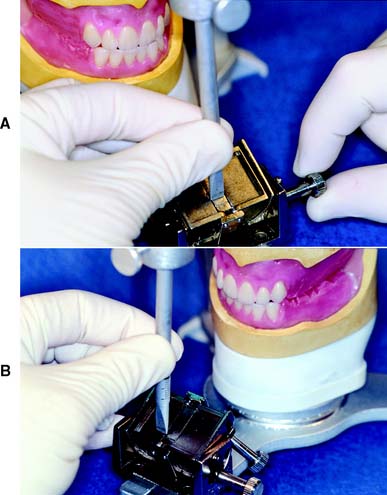
An impression of the maxillary cusp tips is obtained in a suitable recording medium on a facebow fork (Fig. 2-11). The facebow is attached to the protruding arm of the fork. The side arms are adjusted until the styli are aligned with the hinge axis marks on the patient’s skin. The patient must be in the same position that was used when the axis was marked to prevent skin movement from introducing any inaccuracy. A pointer device is usually attached to the bow and adjusted to a repeatable reference point selected by the clinician. The reference point is used later for reproducibility. The kinematic facebow recording is then transferred to the articulator, and the maxillary cast is attached.
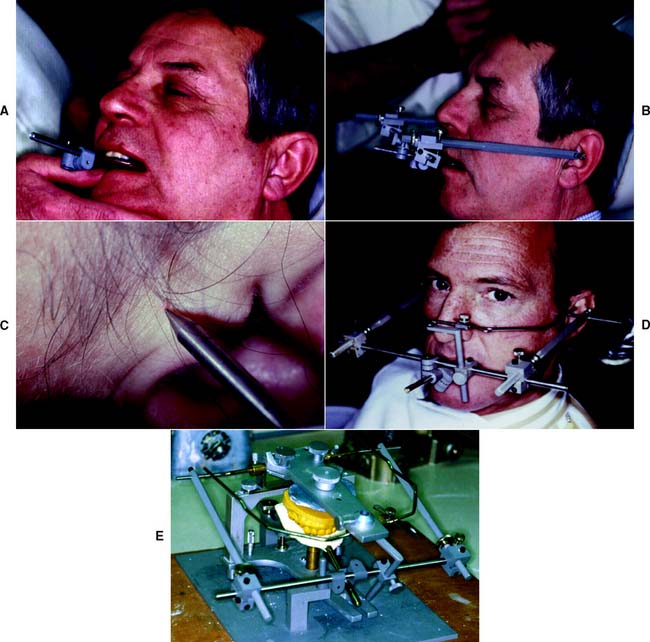
Fig. 2-11 Kinematic hinge axis facebow. A, Clutch seated on the mandibular teeth. The clutch separates for removal into two components by loosening the screws on left and right sides. B, Kinematic facebow assembly positioned. C, Pointers aligned with the previously marked hinge axis location. D, Assembled kinematic facebow. E, Kinematic facebow aligned on the articulator.
The kinematic facebow technique is time consuming, so it is generally limited to extensive prosthodontics, particularly when a change in the occlusal vertical dimension is to be made. A less precisely derived transfer would then lead to unacceptable errors and a compromised result.
Arbitrary Hinge Axis Facebow
Arbitrary hinge axis facebows (Fig. 2-12) approximate the horizontal transverse axis and rely on anatomic average values. Manufacturers design these facebows so the relationship to the true axis falls within an acceptable degree of error. Typically, an easily identifiable landmark such as the external acoustic meatus is used to stabilize the bow, which is aligned with earpieces similar to those on a stethoscope. Such facebows can be used single-handedly because they are self-centering and do not require complicated assembly. They give a sufficiently accurate relationship for most diagnostic and restorative procedures. However, regardless of which arbitrary position is chosen, a minimum error of 5 mm from the axis can be expected,9 as can errors in the steepness of the occlusal plane.10 When coupled with the use of a thick interocclusal record made at an increased vertical dimension, this error can lead to considerable inaccuracy.
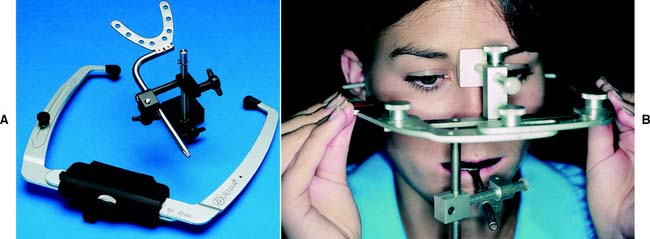
Fig. 2-12 Arbitrary hinge axis facebows. A, The Denar Slidematic. B, Whip Mix Quick Mount. Note the nasion relator as the anterior reference point.
(A, Courtesy of Waterpik Technologies, Inc., Fort Collins, Colorado.)
Anterior reference point
The use of an anterior reference point (Fig. 2-13) enables the clinician to duplicate the recorded position on the articulator at future appointments. This saves time, because previously recorded articulator settings can be used again. An anterior reference point, such as the inner canthus of the eye or a freckle or mole on the skin, is selected. After this has been marked, it is used, along with the two points of the hinge axis, to define the position of the maxillary cast in space. This procedure has the following advantages:

Fig. 2-13 Anterior reference point. The Denar Slidematic facebow uses a mark 43 mm superior to the incisal edge of the maxillary central incisor as an anterior reference point. Other systems use the infraorbital foramen or nasion. The mark serves as a reference to average anatomic values. It also allows subsequent casts to be mounted without a repeat recording.
(Courtesy of Waterpik Technologies, Inc., Fort Collins, Colorado.)
Facebow transfer
Step-by-step procedure
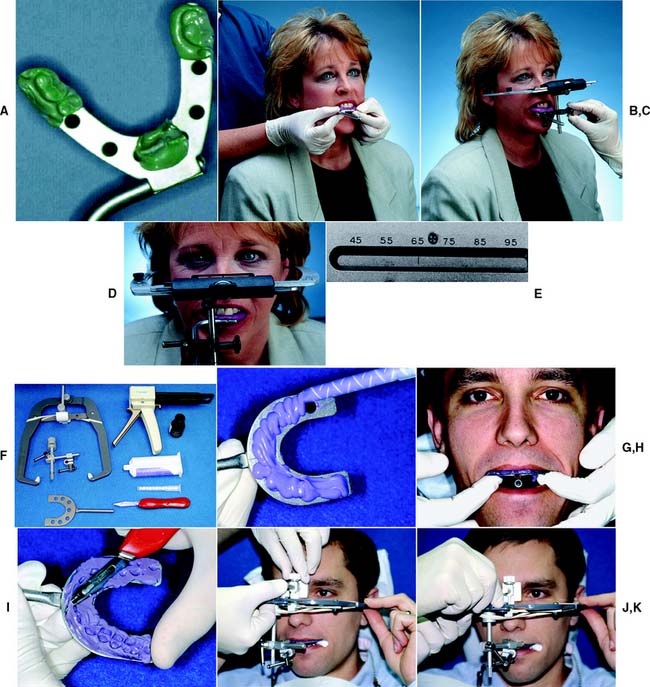
Fig. 2-14 Facebow technique. A to E, Denar Slidematic Facecow Technique. A, Indentations obtained in compound. B, Facebow fork positioned. C, Facebow attached to facebow fork, toggles tightened. D, Transfer complete. E, Width measurement is read from the top of the facebow. F to K, Whip Mix Quick Mount Facebow Technique. F, Armamentarium. G, Automixed elastomer is applied to the transfer fork. H, Adapting the facebow fork to the maxillary teeth. I, The obtained record is trimmed with a sharp blade to facilitate seating. J, Nasion relator being positioned. K, Knobs and toggles are tightened.
(B to D, Courtesy of Waterpik Technologies, Inc., Fort Collins, Colorado. F, H to K, Courtesy of Whip Mix Corporation, Louisville, Kentucky.)
The technique is slightly different with other arbitrary facebows (Fig. 2-14F to K).
Centric relation record
A centric relation record (Fig. 2-15) provides the orientation of mandibular to maxillary teeth in CR in the terminal hinge position, in which opening and closing are purely rotational movements. Centric relation is defined as the maxillomandibular relationship in which the condyles articulate with the thinnest avascular portion of their respective disks with the condyle-disk complex in the anterosuperior position against the articular eminences. This position is independent of tooth contact.
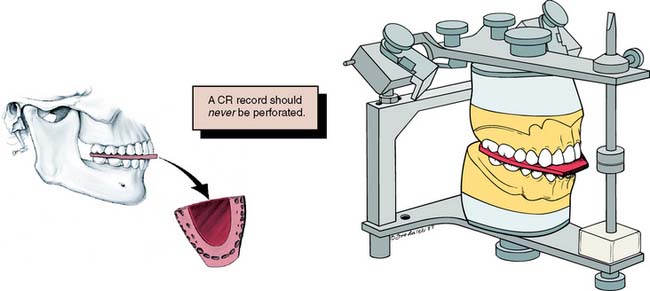
Fig. 2-15 A centric relation (CR) record transfers the tooth relationships at CR from the patient to the articulator.
MI may or may not be coincident with the CR position. The CR record is transferred to the maxillary cast on the articulator and is used to relate the mandibular cast to the maxillary cast. Once the mandibular cast is attached to the articulator with mounting stone, the record is removed. The casts then occlude in precisely the CR position as long as the maxillary cast is correctly related to the hinge axis with a facebow (see Fig. 2-14). When the articulator controls are set properly, through the use of appropriate excursive records, translated mandibular positions can be reproduced from CR. A CR/MI slide is readily reproducible on casts that have been articulated in CR. Thus, premature tooth contacts (deflective contacts) can be observed, and it can be determined whether an occlusal correction is necessary or appropriate before fixed prosthodontic treatment. Casts articulated in the MI position do not enable the evaluation of CR and retruded contact relationships. Therefore, the articulation of diagnostic casts in CR is of greater diagnostic value.
In theory, when a kinematic facebow is used, the thickness of a terminal hinge record is unimportant; a thicker record merely increases the amount of rotation. When an arbitrary facebow is used, any arcing movement results in some degree of inaccuracy. Both techniques are subject to small errors, which can be minimized by keeping the record thin.11,12 However, it is essential that the teeth not perforate the record. Any tooth contact during record fabrication can cause mandibular translation because of neuromuscular protective reflexes governed by mechanoreceptors in the periodontium, rendering the resulting articulation useless.
Jaw manipulation
Accurate mounting of casts depends on precise manipulation of the patient’s mandible by the dentist. The condyles should remain in the same place throughout the opening-closing arc. Trying to force the mandible backwards leads to downward translation of the condyles, and restorations made to such a mandibular position are in supraclusion at the evaluation stage (Fig. 2-16).
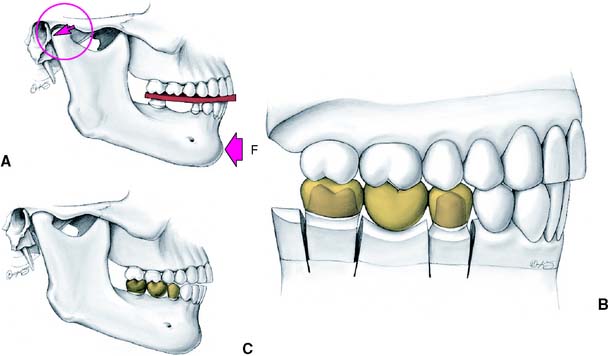
Fig. 2-16 Incorrect centric relation recording. A, If the mandible is forced backward (F), the condyles are not in their most superior position but are moved backward and downward (arrow). B, Any restorations made on casts related with this CR record are in supraclusion when tried in the mouth. C, Note the relationship of the anterior teeth.
The load-bearing surfaces of the condylar processes, which face anteriorly, should be manipulated into apposition with the mandibular fossae of the temporal bones, with the disk properly interposed. The ease with which this can be accomplished depends on the degree of the patient’s neuromuscular relaxation and on sound technique. The latter, in turn, depends on the patient’s permitting the dentist to control the mandible. Attempts to force or shake the mandible lead to a protective muscle response by the patient.
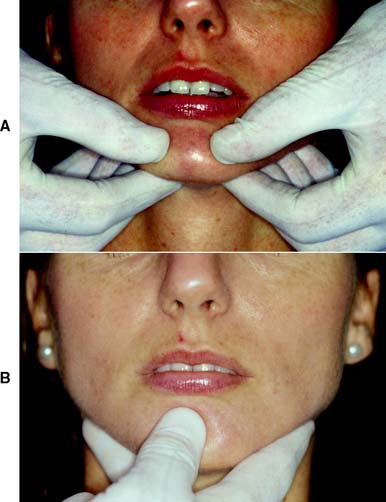
The bimanual manipulation technique described by Dawson13 is recommended as a reproducible technique14 that can be reliably learned.15 In this technique, the dental chair is reclined and the patient’s head is cradled by the dentist. With both thumbs on the chin and the fingers resting firmly on the inferior border of the mandible (Fig. 2-17A), the dentist exerts gentle downward pressure on the thumbs and upward pressure on the fingers, manipulating the condyle-disk assemblies into their fully seated positions in the mandibular fossae. Next, the mandible is carefully hinged along the arc of terminal hinge closure. Note: It is more difficult to ensure that the condyles are properly located when the single-handed approach (Fig 2-17B) is used with the fingers exerting upward pressure, although this technique does allow the other hand to hold the record.
Anterior programming device (Fig. 2-18)
In some patients in whom CR does not coincide with MI, resistance may be encountered when hingeing the mandible. Because of well-established protective reflexes that are reinforced every time the teeth come together, such patients do not allow their mandibles to be manipulated and hinged easily. If tooth contact can be prevented, they “forget” these reflexes, and manipulation becomes easier. The teeth can be kept apart with cotton rolls, a plastic leaf gauge, or a small anterior programming device made of autopolymerizing acrylic resin (also known as a Lucia jig).16
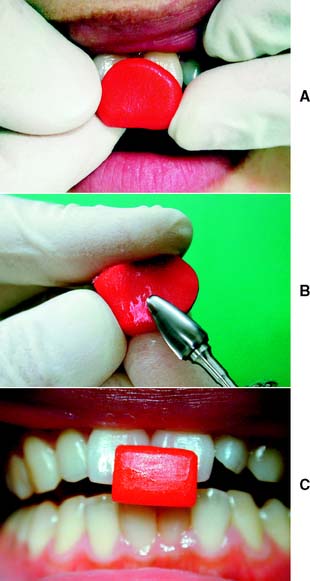
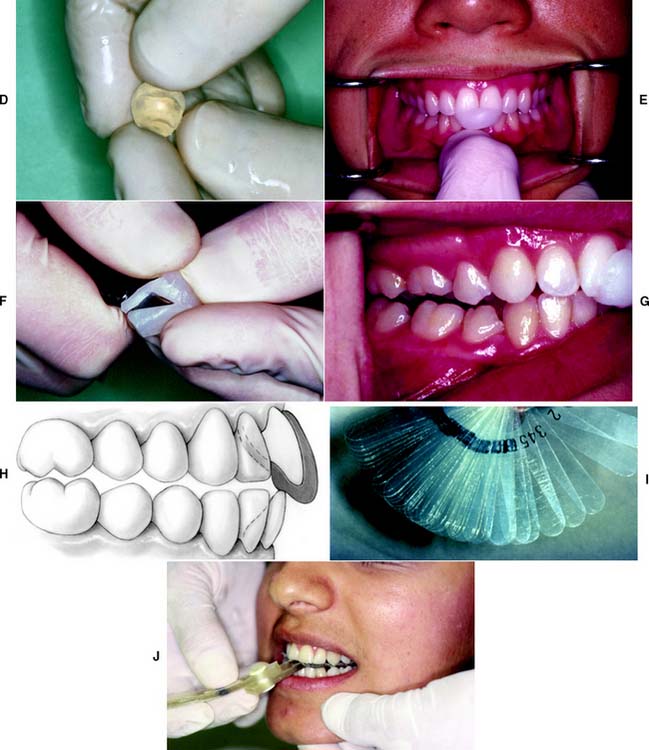
Fig. 2-18 An anterior programming device is used to facilitate centric relation recording. A, Autopolymerizing resin is mixed and adapted to the maxillary central incisors. The patient’s mouth is guided into closure and stopped when the posterior teeth are about 1 mm apart. B, The indentations are used as a guide during trimming of the device. The completed device (C) should allow the patient to make smooth lateral and protrusive movements. An inclined contact area must be avoided, because it will tend to cause the mandible to retrude excessively. D, Alternatively, a thermoplastic material can be used. E, After softening and positioning, the mandible is guided into centric relation closure. F, The device is trimmed with a scalpel. G, Again, posterior disclusion is verified. H, Cross-section through device. I and J, Use of a plastic leaf gauge to prevent habitual closure into maximal intercuspation.
If the mandible cannot be manipulated satisfactorily after an anterior programming device has been in place for 30 minutes, marked neuromuscular dysfunction is likely. Normally, this is relieved by providing an occlusal device (whose fabrication and adjustment are described in Chapter 4).
Centric relation recording technique
Different techniques can be used to make a CR record. The choice of recording medium is, to some degree, a function of the casts to be articulated. For instance, very accurate casts made from elastomeric impression materials can be articulated with a high-accuracy interocclusal record material such as polyvinyl siloxane. However, less accurate diagnostic casts poured from irreversible hydrocolloid are better articulated with the use of a more “forgiving” material such as interocclusal wax, provided that the record is properly reinforced. Most studies have shown considerable variability among various registration materials and techniques,17 and so particular care is needed with this procedure.
Reinforced Aluwax record
The reinforced Aluwax record is a “forgiving” method for recording the CR position. It is a reliable technique, originally described by Wirth18 and Wirth and Aplin,19 and has provided consistent results.20,21
Armamentarium (Fig. 2-19A)

Fig. 2-19 Centric relation (CR) recording technique. The reproducibility of the CR position is verified because CR has to be reproduced several times while the record is made. A, Armamentarium. B, A sheet of soft Aluwax is adapted to the maxillary arch. C, A piece of hard pink wax is added to the lower anterior portion of the wafer. D, Some Ash’s Metal #7 is folded around the posterior border and luted to the wafer with sticky wax to increase rigidity. E, The reinforced sheet is repositioned and the mandible is guided into CR until the pink wax provides a stop for vertical closure. F, Note that the maxillary indentations capture only the cusp tips. Some Aluwax is added to the lower incisor indentations. The record is repositioned and the CR closure repeated. G, The incisor indentations are reproduced in the Aluwax. H, After additional wax is added to the area of the first molars, hinge closure is repeated (I). J, The molar indentations are clearly visible. The incisor indentations should have been reproduced. Any “double” indentation indicates inaccuracy. K, The CR closure is repeated one more time after additional Aluwax is added to the premolar regions. L, The completed CR record.
(Courtesy of Dr. J. N. Nelson.)
Step-by-step procedure
The advantage of this sequential technique is that the CR position is reproduced multiple times as the record is generated. The heat-retaining Aluwax is soft and distorts easily. Therefore, if the patient’s mouth is not guided into exactly the same position, this problem becomes readily apparent. Once the completed record has been obtained with adequate but fairly shallow indentations for all cusps (Fig. 2-19K,L), the same arcing motion has been reproduced four times, confirming that the CR position has been accurately captured.
Anterior programming device with elastomeric or ZOE record
Step-by-step procedure
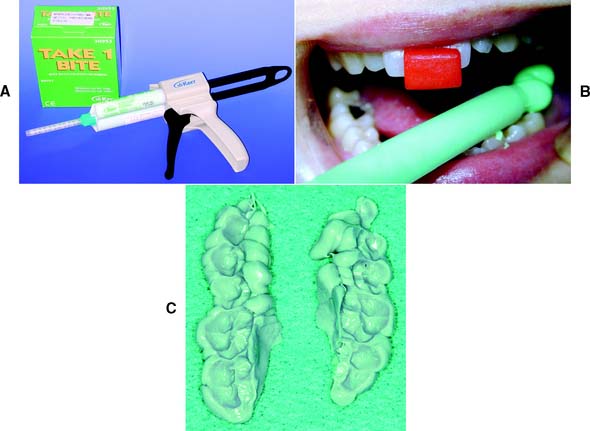
Fig. 2-20 Centric relation (CR) recording. A, Elastomeric material for CR recording. B, Mandibular quadrants coated, the dentist is using an anterior resin jig (see Fig. 2-18) to ensure a reproducible recording position is obtained. The patient’s mouth remains occluded until the material has set. C, The record before trimming.
As an alternative to the use of elastomeric material, a gauze mesh with zinc oxide–eugenol occlusal registration paste can be used (Fig. 2-21). The step-by-step procedure follows the one described for the elastomeric technique. However, rather than using a syringe to apply the material onto the mandibular arch, the practitioner should coat the interocclusal cloth forms outside the mouth and interpose them, after which the patient’s mouth can be guided into CR. Care must be taken, however, to position the frame that holds the cloth form so that it does not interfere with the closure movement.

Fig. 2-21 Gauze mesh cloth forms with plastic holders, and ZOE paste can be used instead of elastomeric paste.
Other alternative techniques include using impression plaster or autopolymerizing resin as the recording medium. In all these techniques, accuracy depends on complete seating of the casts into the recording medium. Seating is often prevented by better detail reproduction in the record than in the casts, especially around the fossa. This additional detail needs to be carefully trimmed until the cast is completely seated in the record.
Recording jaw relationships in partially edentulous dentitions
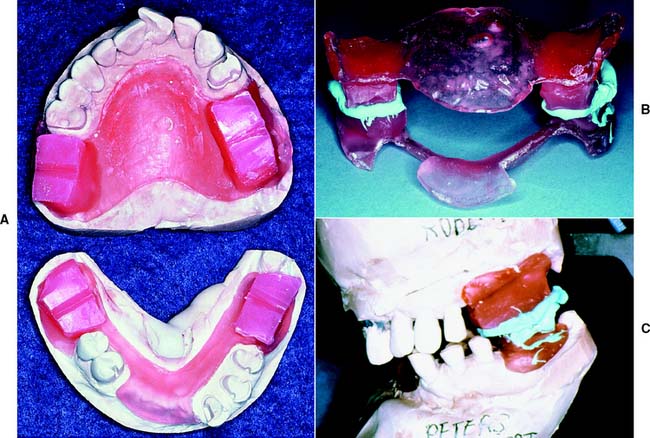
When there are insufficient teeth to provide bilateral stability, obtaining a CR record as described may not be possible. As a result, acrylic resin record bases must be fabricated (Fig. 2-22). To avoid errors caused by soft tissue displacement, which prevents accurate transfer of rigid materials from one set of casts to another, these bases should be made on the casts that are to be articulated. If breakage of the casts is a concern, it may be advisable to make record bases on an accurate duplicate cast made with reversible agar hydrocolloid impression material in a flask designed for that purpose.
Articulating the diagnostic casts
Maxillary cast
The maxillary cast (Fig. 2-23) is seated in the indentations on the facebow fork after the facebow is attached to the articulator. Wedges or specially designed braces can be used to support the weight of the cast and to prevent the fork from flexing or moving. After it has been scored and wetted, the cast is attached to the mounting ring of the articulator with a low-expansion, fast-setting mounting stone or plaster.
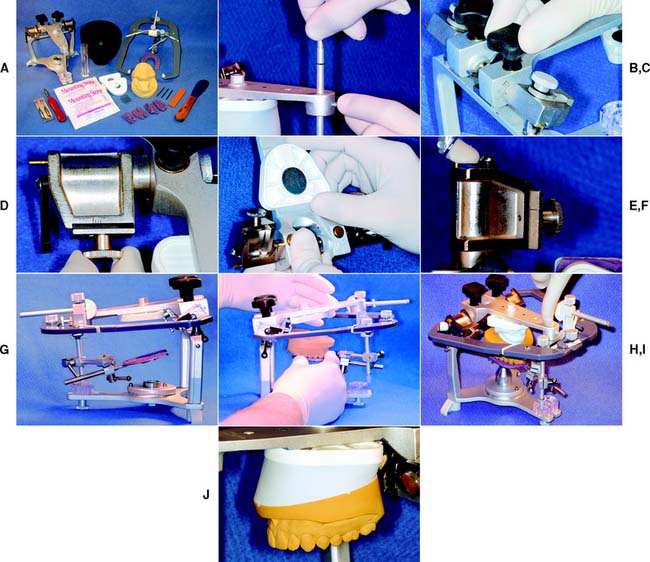
Fig. 2-23 Mounting the maxillary cast on a Whip Mix articulator. A, Armamentarium. B, The incisal pin is removed. C, The condylar inclination is adjusted to the facebow setting. D, The side shift is set to zero. E, A mounting plate is attached. F, The facebow earpieces are attached to the condylar elements. G, Facebow is attached to the articulator. H, The scored maxillary cast is positioned on the facebow fork, and the cast is prewetted. I, Mounting stone is applied to the cast and the mounting plate. The upper member of the articulator is closed until it contacts the crossbar of the facebow. J, Additional stone is added as needed.
(Courtesy of Whip Mix Corporation, Louisville, Kentucky.)
Mandibular cast
To relate the mandibular cast properly to the maxillary cast, the incisal guide pin should be lowered sufficiently to compensate for the thickness of the CR record. The articulator is inverted, and the record is seated on the maxillary cast. The mandibular cast (Fig. 2-24) is then carefully seated in the record, and each cast is checked for stability. The maxillary and mandibular casts can be luted together with metal rods, or pieces of wooden tongue blade, and sticky wax. The mandibular member of the articulator is closed into mounting stone; the condylar balls should be fully seated in the corresponding fossae. If the articulator has a centric latch, this step is simplified. Otherwise, the articulator should be held until the stone has reached its initial set. No attempt should be made to smooth the stone until it has fully set.
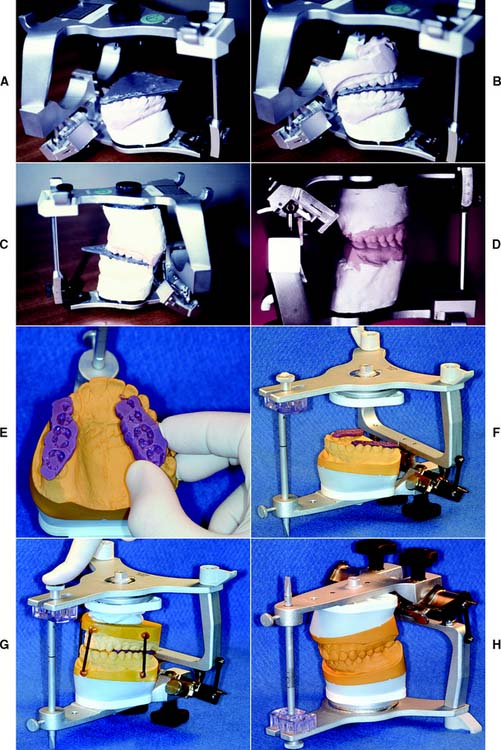
Fig. 2-24 Mounting the mandibular cast. A to D, Denar articulator. A, The centric relation (CR) record is positioned on the inverted maxillary cast. B, The incisal guide pin is adjusted, and the mandibular cast is oriented in the record. C, The cast is attached with mounting stone. D, When the pin is raised, the casts contact in CR closure. E to H: Whip Mix articulator. E, Trimmed elastomeric CR records. F, CR records positioned on the inverted articulator. G, The incisal guide pin is adjusted, the cast is stabilized, and plaster is applied to the prewetted cast and the mandibular mounting plate before the articulator is closed. H, Completed mounting.
(E to H, Courtesy of Whip Mix Corporation, Louisville, Kentucky.)
Evaluation
Accuracy is crucial in both CR and maximum intercuspation. Before the articulator controls are adjusted, the accuracy of CR must be confirmed by comparing the tooth contacts on the casts with those in the mouth (Fig. 2-25). During the clinical examination, the position of tooth contacts in CR can be marked with thin articulating film. Normally, the markings are on the mesial inclines of maxillary cusps and the distal inclines of mandibular cusps. Their exact location can be transferred by having the patient close through thin occlusal indicator wax. The articulated casts are closed, and the retruded tooth contacts marked with articulating film. When the indicator wax is transferred to the casts, the perforations should correspond exactly to these marks.
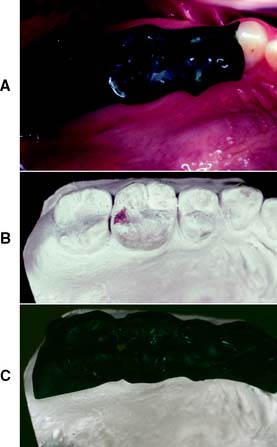
Fig. 2-25 Verifying mounting accuracy. A, Occlusal indicator wax is adapted to the maxillary teeth, and the patient’s mouth is guided into centric relation closure. B, The cast contacts are marked with thin articulating film. C, If the mounting is accurate, the markings correspond to perforations in the wax.
For additional verification, maximum intercuspation of the articulated casts should be examined. MI is usually a translated mandibular position that may not be reproducible with absolute accuracy on a semiadjustable articulator. However, any substantive discrepancy invariably indicates an incorrect mounting. If further confirmation of mounting accuracy is required (as may be the case when definitive casts are being articulated), additional CR records can be made and compared with a split-cast mounting system or a measuring device such as the Denar Centri-Check marking system† (Fig. 2-26).

Fig. 2-26 The Denar Centri-Check marking system. The casts are positioned in the same relationship as on the articulator, but the condylar elements are replaced by styli. Each stylus marks graph paper attached to the maxillary half of the articulator. Successive centric relation records can be compared by examining these marks.
(Courtesy of Waterpik Technologies, Inc., Fort Collins, Colorado.)
Posterior articulator controls
The advantages and disadvantages of the different articulators are summarized in Table 2-1. The more sophisticated (fully adjustable) articulators have a large range of adjustments that can be programmed to follow the condylar paths precisely. Their posterior controls are designed to enable simulation of movement of the condylar processes, duplicating protrusive and lateral tooth contacts. The semiadjustable instruments can be adjusted to a lesser extent. Their posterior controls are designed to replicate the most clinically significant features of mandibular movement (e.g., condylar inclination and mandibular side shift). These instruments can be programmed from eccentric interocclusal records or a simplified pantograph. An alternative technique is to use average values for the control settings. It is important to note that no method used to program an articulator to reproduce eccentric jaw movements is without error.23
Table 2-1 ARTICULATOR SELECTION FOR FIXED PROSTHODONTICS
ROOT SURFACE AREA OF ABUTMENT
Arbitrary values
On the basis of clinical investigations, certain generally applicable average anatomic values have evolved for condylar inclination, both immediate and progressive side shift. These values have been described relative to the Frankfort horizontal plane and the midsagittal plane. For instance, an average value of 1.0 mm has been reported24 for immediate side shift.
When arbitrary values are used to adjust posterior articulator controls, the actual instrument settings vary from one manufacturer to another. However, depending on the degree of adjustability of the articulator, using arbitrary values does not necessarily lead to less accuracy than do alternative techniques (e.g., eccentric interocclusal records to program a semiadjustable articulator, particularly when the instrument can execute only a straight protrusive path).
Eccentric interocclusal recordings
Eccentric interocclusal records (check bites) have been recommended25 for setting the posterior controls of a semiadjustable articulator. These consist of wax or another recording material interposed between the maxillary and mandibular arches; they record the position of the condyles in eccentric mandibular positions. Static positional records are made in translated jaw positions: a protrusive record and two lateral records. The protrusive record can be used to adjust both condylar inclinations on the articulator, and the lateral records are used to adjust the side shift on semiadjustable articulators.
An articulator set by an eccentric record is accurate in only two positions: at CR and at the position recorded by the record (Fig. 2-27). This occurs because the path taken between these may differ significantly on the articulator from what is actually performed by the mandible. A semiadjustable instrument may have a protrusive and a side shift path that are straight lines, whereas the true paths are invariably curved. In an attempt to minimize errors, many contemporary semiadjustable articulators come with curved fossae.
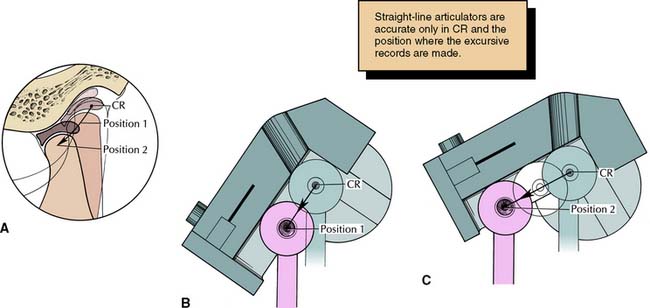
Fig. 2-27 A, The typical condylar path is curved, with its steepest inclination near centric relation (CR). If a semiadjustable articulator with a straight condylar path is programmed from an eccentric record, very different values will be obtained (depending on where the record is made) from what is actually performed by the mandible. B, Record made at position 1. C, Record made at position 2.
Step-by-step technique
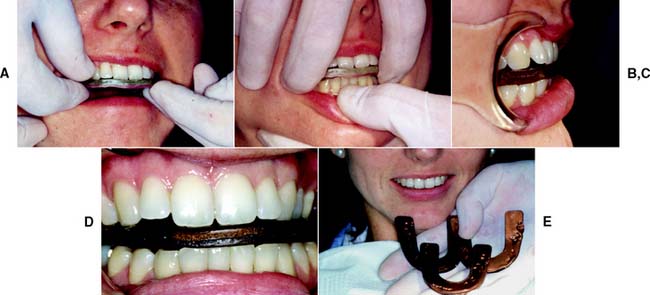
Fig. 2-28 Eccentric interocclusal records. A, Adaptation of wax to the maxillary arch. B, Protrusive record. C and D, The patient’s mandible is guided into left and right lateral excursive movements. Records are made in the left and right canine edge-to-edge positions. E, The completed records.
Simplified pantographs
A simplified pantograph (Fig. 2-29) measures only certain components of mandibular movement thought to be of greatest clinical significance, usually the condylar inclinations and mandibular side shift. This device can be quickly assembled. Numerical values are measured directly from the recording and are used to set a semiadjustable articulator to provide useful diagnostic information.

Fig. 2-29 A, The Panadent Axi-Path Recorder. B and C, An axis stylus traces the condylar path and measures the amount of Bennett movement (B≤ and B′) while the patient’s mouth is guided into an eccentric border movement.
(A to C, Courtesy of Panadent Corporation, Grand Terrace, California.)
Simplified pantographs may reveal an excessively shallow condylar inclination or an exaggerated mandibular side shift. If either of these conditions is identified, restoration of the posterior teeth is likely to be complex, and the use of a fully adjustable articulator is recommended. Some manufacturers offer inserts of standard “fossae” of varying configuration, whose selection depends on the measurements obtained with a simplified pantograph (Fig. 2-30).
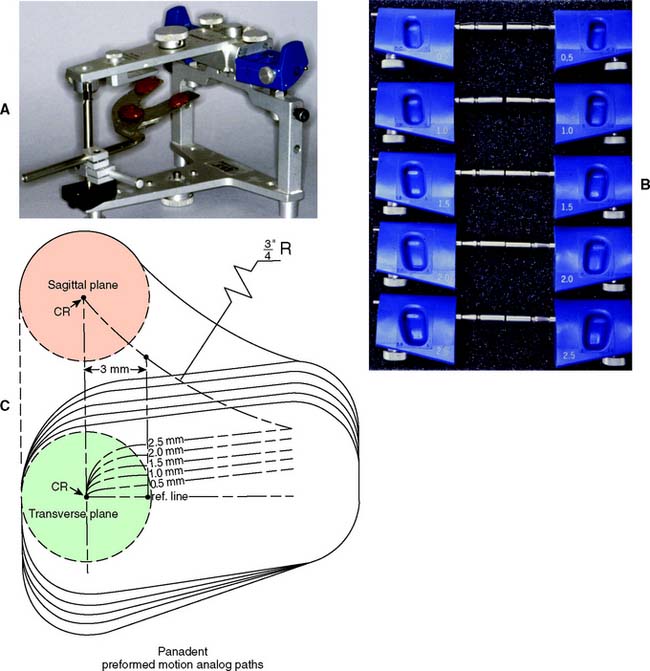
Fig. 2-30 A, The Panadent PCH Articulator with support legs. B, Fossa blocks (motion analogs) with different amounts of Bennett movement are selected from the simplified recorder or lateral interocclusal records. The blocks are rotated to the correct condylar inclination. C, Schematic showing the sagittal and transverse planes of the available motion analog blocks. CR, centric relation; ¾″R, ¾-inch radius of fossa curvature.
(A to C, Courtesy of Panadent Corporation, Grand Terrace, California.)
Pantographic recordings
Fully adjustable articulators are usually programmed on the basis of a pantographic recording (Fig. 2-31). Jaw movements are registered by directional tracings on recording plates. The plates are rigidly attached to one jaw, and the recording styli are attached to the other. A total of six plates are needed to achieve a precise movement record of the mandible. Left and right lateral border and protrusive tracings are made on each plate. The pantograph is then attached to the articulator, and the controls are adjusted and modified until the instrument can faithfully reproduce the movements of the styli on the tracings (Fig. 2-32). A simpler, although less accurate, procedure is to measure the tracings directly and adjust the condylar controls without transferring the recordings.
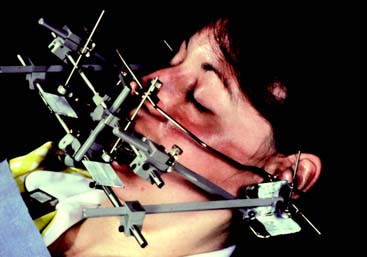
Fig. 2-31 Pantographic recording with the Stuart instrument.
(Courtesy of Drs. R. Giering and J. Petrie.)
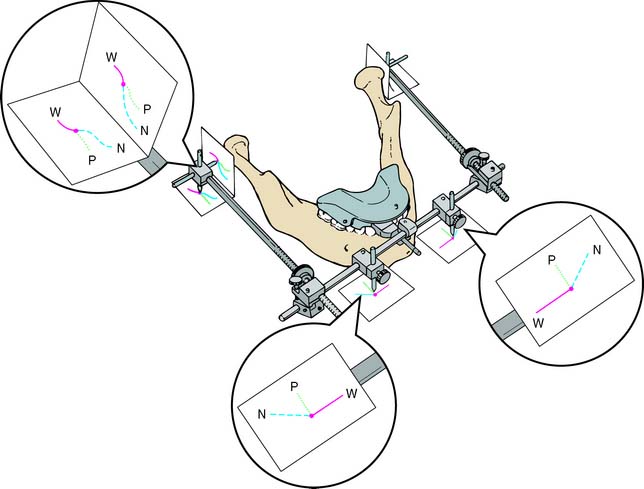
Fig. 2-32 Pantographic tracings represent information that could only be obtained with an infinite number of excursive records: This simplified schematic shows the relative orientation of six recording plates (attached to the maxillary bow, omitted for clarity) to the scribing styli, attached to the mandibular bow. N, nonworking or balancing movement; P, protrusive movement; W, working movement. The centric relation position is represented by the intersection of the paths marked by the dot.
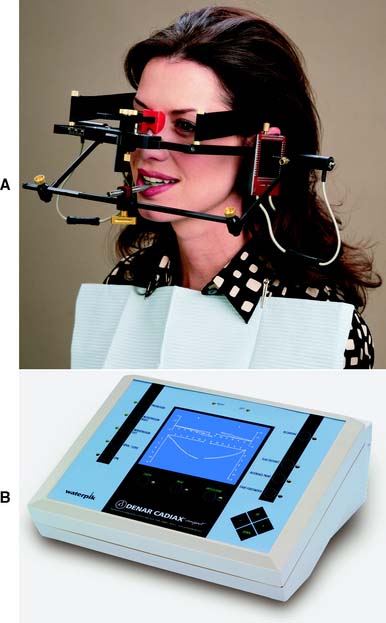
Electronic pantograph (the Denar Cadiax Compact*)
The Electronic Pantograph (the Denar Cadiax Compact) is designed to record and measure functional and border movements (Fig. 2-33). It consists of upper and lower bows that record and measure mandibular movements and has been shown to provide valid and reliable measures of condylar determinants.27
Stereograms
Another approach to reproducing posterior condylar controls is to cut or mold a three-dimensional recording of the jaw movements. This “stereogram” (Fig. 2-34) is then used to form custom-shaped fossae for the condylar heads.
Anterior guidance
Border movements of the mandible are governed by tooth contacts and by the shape of the left and right temporomandibular joints. In patients with normal jaw relationships, the vertical and horizontal overlap of anterior teeth and the lingual concavities of the maxillary incisors are highly significant during protrusive movements. In lateral excursions, the tooth contacts normally existing between the canines are usually dominant, although the posterior teeth may also be involved (see Chapter 4). Restorative procedures that change the shape of the anterior teeth can have a profound effect on excursive tooth contacts. For this reason, when preparation of anterior teeth is contemplated, the exact nature of the anterior contacts should be transferred to the articulator, where it can be studied and stored before these teeth are prepared.
Mechanical anterior guide table
Most articulator manufacturers supply a mechani-cal anterior guide (incisal guidance) table (Fig. 2-35). Such tables can be pivoted anteriorly and posteriorly to simulate protrusive guidance, and they have lateral wings that can be adjusted to approximate lateral guidance. However, the sensitivity of these adjustments is insufficient for successfully transferring the existing lingual contours of natural teeth to newly fabricated restorations. Therefore, the principal use for these mechanical tables is in the fabrication of complete dentures and occlusal devices (see Chapter 4).
Custom acrylic anterior guide table
This simple device is used for accurately transferring to an articulator the contacts of anterior teeth when determining their influence on border movements of the mandible. Acrylic resin is used to record and preserve this information, even after the natural lingual contours of the teeth have been altered during preparation for complete coverage restorations. The technique is similar to that for stereographic recording used in setting the posterior controls of some articulators.
Custom guide table fabrication
Armamentarium (Fig. 2-36A)
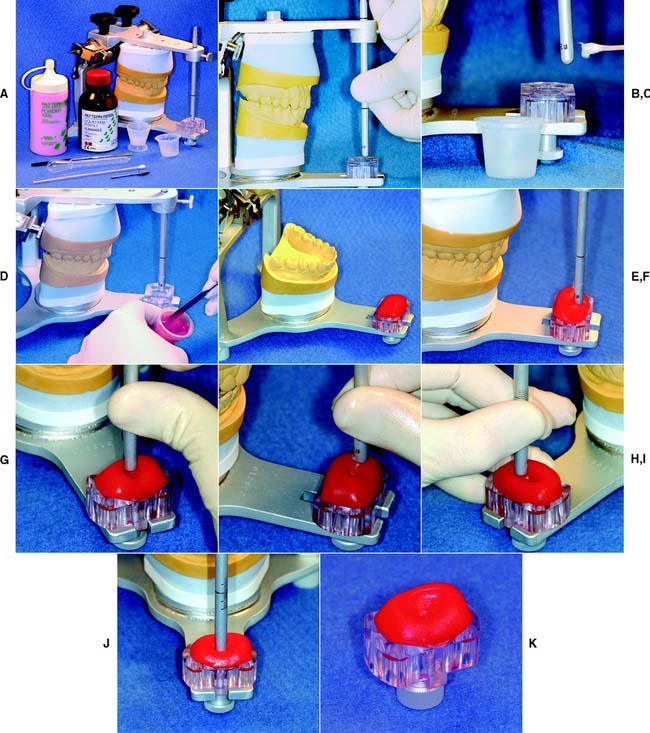
Fig. 2-36 Fabrication of a custom anterior guide table. A, Armamentarium. B, Incisal pin is raised 1 or 2 mm. C, The tip of the pin is lubricated. D, Resin is dispensed and mixed. E, Resin is applied to acrylic table. F, Pin is inserted when resin is at the doughy stage. G, The protrusive path is tracked. H, Right working movement and all intermediate laterotrusive paths. I, Left working movement and all intermediate laterotrusive paths. J, Resin is allowed to set. K, Excess resin still needs to be removed.
(Courtesy of Whip Mix Corporation, Louisville, Kentucky.)
Step-by-step procedure
Evaluation
When the custom anterior guide table has been completed, the incisal pin should contact the table in all excursive movements. This can be checked with thin Mylar strips (shim stock). If contact is deficient, a small mix of new resin is added and the process repeated. If too much resin has been used, the table may interfere with the hinge opening-closing arc of the articulator (Fig. 2-37). Excess can be easily trimmed away.

Diagnostic cast modification
One advantage of having accurately articulated diagnostic casts is that proposed treatment procedures can be rehearsed on the stone cast before any irreversible changes are made in the patient’s mouth. These diagnostic procedures are essential when the dentist attempts to solve complicated problems. Even the most experienced clinician may have difficulty deciding between different treatment plans. Even in apparently simple situations, time that the practitioner spends rehearsing diagnostic procedures on the casts is usually well rewarded.
Diagnostic cast modifications include the following:
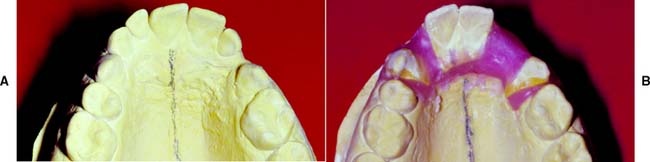

Fig. 2-39 Diagnostic waxing procedure. Diagnostic tooth preparation and waxing help simplify complex prosthodontic treatment planning for predictable results. A and B, Cross-mounted diagnostic casts. A record base is used to articulate the partially edentulous mandibular cast. C and D, Diagnostic tooth preparations determine the correct reduction for esthetics and function. E to H, Diagnostic waxing, done in conjunction with diagnostic denture tooth arrangement.
(Courtesy of Dr. J. Bailey.)
On many occasions, it is necessary to combine two or more of these options. In fact, most treatment planning decisions (e.g., preparation design, choice of abutment teeth, selection of an optimum path of placement of a fixed dental prosthesis, or deciding to treat a patient with a fixed or removable dental prosthesis) can be simplified by adhering to these diagnostic techniques.
SUMMARY
Diagnostic casts provide valuable preliminary information and a comprehensive overview of the patient’s needs that are often not apparent during the clinical examination. They are obtained from accurate irreversible hydrocolloid impressions and should be transferred to a semiadjustable articulator by using a facebow transfer and interocclusal record. For most routine fixed prosthodontic diagnostic purposes, the use of an arbitrary hinge axis facebow is sufficient. If special concerns apply, such as a change in vertical dimension, a kinematic facebow transfer is needed. Two types of articulators are recognized: arcon and nonarcon. For highly complex treatment needs, a fully adjustable articulator may be indicated. Such articulators are adjusted by using a pantographic tracing.
Diagnostic casts should be articulated in CR to enable observation of deflective tooth contact and to assess any slide that may be present from CR to MI. Centric relation is defined as the maxillomandibular relationship in which the condyles articulate with the thinnest avascular portion of their respective disks with the complex in the anterosuperior position against the shapes of the articular eminences. This position is independent of tooth contact. It is recorded with a suitable medium interposed between the maxillary and mandibular teeth and by guiding the patient into the CR position. This can be accomplished through bimanual manipulation. If many teeth are absent, record bases with wax rims may need to be fabricated to obtain a CR record.
If it is difficult to manipulate a patient’s mandible into a reproducible hinge movement, a deprogramming device is helpful. These can be used to help minimize “muscle memory,” resulting in easier replication of the rotational hinge movement of the mandible.
Posterior articulator controls can be adjusted on the basis of arbitrary values according to anatomic averages, by means of eccentric records, simplified pantographs, pantographs, or stereographs.
Anterior guidance can be approximated on articulators with a mechanical guide table. As an alternative, a custom acrylic guide table can be generated from the diagnostic casts. The latter is useful when anterior teeth are to be restored.
Diagnostic procedures such as diagnostic waxing, tooth preparation, and diagnostic cast modification can greatly enhance diagnosis and treatment planning.
 GLOSSARY*
GLOSSARY*
acquired eccentric relation \a-kwīrd′  k-
k- n′trk r-lā′shun\: any eccentric relationship position of the mandible relative to the maxilla, whether conditioned or learned by habit, which will bring the teeth into contact
n′trk r-lā′shun\: any eccentric relationship position of the mandible relative to the maxilla, whether conditioned or learned by habit, which will bring the teeth into contact
acrylic resin base \a-krl′k rz′n bās\: a denture base made of acrylic resin
adjustable anterior guidance \a-jŭst′a′bul ăn-tîr′ē-or gīd′ns\: an anterior guide on an articulator whose surface may be altered to provide desired guidance of the articulator’s movement mechanism; the guide may be programmed (calibrated) to accept eccentric interocclusal records
adjustable articulator \a-jŭst′a′bul är-tk′ya-lā′tor\: an articulator that allows some limited adjustment in the sagittal and horizontal planes to replicate recorded mandibular movements—see ARTICULATOR
ala-tragus line \a′lah tră′gŭs līn\: a line running from the inferior border of the ala of the nose to some defined point on the tragus of the ear, usually considered to be the tip of the tragus. It is frequently used, with a third point on the opposing tragus, for the purpose of establishing the ala tragus plane. Ideally the ala-tragus plane is considered to be parallel to the occlusal plane. The occlusal plane is at an angle of approximately 10 degrees relative to the Frankfort horizontal plane, when viewed in the mid-sagittal plane—see CAMPER’s LINE
anterior guidance \ăn-tîr′ē-or gīd′ns\: 1: the influence of the contacting surfaces of anterior teeth on tooth limiting mandibular movements 2: the influence of the contacting surfaces of the guide pin and anterior guide table on articulator movements—usage see ANTERIOR GUIDE TABLE 3: the fabrication of a relationship of the anterior teeth preventing posterior tooth contact in all eccentric mandibular movements—see ANTERIOR PROTECTED ARTICULATION, GROUP FUNCTION, MUTUALLY PROTECTED ARTICULATION
anterior guide : see ANTERIOR GUIDE TABLE
anterior guide pin \ăn-tîr′ē-or gīd pn\: that component of an articulator, generally a rigid rod attached to one member, contacting the anterior guide table on the opposing member. It is used for the purpose of maintaining the established vertical separation. The anterior guide pin and table, together with the condylar elements, direct the movements of the articulators’ separate members
anterior guide table \ăn-tîr′ē-or gīd tā′bl\: that component of an articulator on which the anterior guide pin rests to maintain the occlusal vertical dimension and influence articulator movements. The guide table influences the degree of separation of the casts in all relationships—see also ANTERIOR PROGRAMMING DEVICE
anterior programming device \ăn-tîr′ē-or prō′grăm’ng d-vīs′\: an individually fabricated anterior guide table that allows mandibular motion without the influence of tooth contacts and facilitates the recording of maxillomandibular relationships; also used for deprogramming—see also deprogrammer
anterior reference point \ăn-tîr′ē-or rf′er-ens, rf′rens point\: any point located on the midface that, together with two posterior reference points, establishes a reference plane
ar·con \ar′kon\ n: a contraction of the words “ARTICULATOR” and “CONDYLE,” used to describe an articulator containing the condylar path elements within its upper member and the condylar elements within the lower member
arcon articulator \ar’kon är-tk′ya-lā′tor\: an articulator that applies the arcon design; this instrument maintains anatomic guidelines by the use of condylar analogs in the mandibular element and fossae assemblies within the maxillary element
arrow point tracer \ăr′ō point trā′ser\: 1: a mechanical device used to trace a pattern of mandibular movement in a selected plane—usually parallel to the occlusal plane 2: a mechanical device with a marking point attached to one jaw and a graph plate or tracing plane attached to the other jaw. It is used to record the direction and range of movements of the mandible—see GOTHIC ARCH TRACER
articulating paper \är-tk′ya-lāt′ing pā′per\: ink-coated paper strips used to locate and mark occlusal contacts
ar·tic·u·la·tor \är-tk′ya-lā′tor\ n: a mechanical instrument that represents the temporomandibular joints and jaws, to which maxillary and mandibular casts may be attached to simulate some or all mandibular movements—usage: articulators are divisible into four classes Class I articulator: a simple holding instrument capable of accepting a single static registration; vertical motion is possible—see NONADJUSTABLE A. Class II articulator: an instrument that permits horizontal as well as vertical motion but does not orient the motion to the temporomandibular joints. Class III articulator: an instrument that simulates condylar pathways by using averages or mechanical equivalents for all or part of the motion; these instruments allow for orientation of the casts relative to the joints and may be arcon or nonarcon instruments—see SEMI-ADJUSTABLE A. Class IV articulator: an instrument that will accept three dimensional dynamic registrations; these instruments allow for orientation of the casts to the temporomandibular joints and simulation of mandibular movements—see FULLY ADJUSTABLE A., FULLY ADJUSTABLE GNATHOLOGIC A.
average axis facebow \ăv′er-j, ăv′rj ăk′ss fās bō\: a device used to relate the maxillary cast to the condylar elements of an articulator using average anatomic landmarks to estimate the position of the transverse horizontal axis on the face.
average value articulator \ăv′rj văl′yōō är-tk′ya-lā′ter\: an articulator that is fabricated to permit motion based on mean mandibular movements—called also Class III articulator
base material \bās mă-tîr′ē-al\ obs: any substance of which a denture base may be made, such as acrylic resin, vulcanite, polystyrene, or metal (GPT-4)
cen·tric \n′trk\ adj (1590): 1: located in or at a center; central 2: concentrated about or directed toward a center
centric occlusion \n′trk a-klōō′zhen\: the occlusion of opposing teeth when the mandible is in centric relation. This may or may not coincide with the maximal intercuspal position—comp MAXIMAL INTERCUSPAL POSITION
centric relation \n′trk r-lā′shun\: 1: the maxillomandibular relationship in which the condyles articulate with the thinnest avascular portion of their respective disks with the complex in the anterior-superior position against the shapes of the articular eminencies. This position is independent of tooth contact. This position is clinically discernible when the mandible is directed superior and anteriorly. It is restricted to a purely rotary movement about the transverse horizontal axis (GPT-5) 2: the most retruded physiologic relation of the mandible to the maxillae to and from which the individual can make lateral movements. It is a condition that can exist at various degrees of jaw separation. It occurs around the terminal hinge axis (GPT-3) 3: the most retruded relation of the mandible to the maxillae when the condyles are in the most posterior unstrained position in the glenoid fossae from which lateral movement can be made at any given degree of jaw separation (GPT-1) 4: The most posterior relation of the lower to the upper jaw from which lateral movements can be made at a given vertical dimension (Boucher) 5: a maxilla to mandible relationship in which the condyles and disks are thought to be in the midmost, uppermost position. The position has been difficult to define anatomically but is determined clinically by assessing when the jaw can hinge on a fixed terminal axis (up to 25 mm). It is a clinically determined relationship of the mandible to the maxilla when the condyle disk assemblies are positioned in their most superior position in the mandibular fossae and against the distal slope of the articular eminence (Ash) 6: the relation of the mandible to the maxillae when the condyles are in the uppermost and rearmost position in the glenoid fossae. This position may not be able to be recorded in the presence of dysfunction of the masticatory system 7: a clinically determined position of the mandible placing both condyles into their anterior uppermost position. This can be determined in patients without pain or derangement in the TMJ (Ramsfjord)
Boucher CO. Occlusion in prosthodontics. J PROSTHET DENT 1953; 3:633-56.
Ash MM. Personal communication, July 1993.
Lang BR, Kelsey CC. International prosthodontic workshop on complete denture occlusion. Ann Arbor: The University of Michigan School of Dentistry, 1973.
Ramsfjord SP. Personal communication, July 1993.
centric relation record \sn′trk r-lā′shun r-kōrd\: a registration of the relationship of the maxilla to the mandible when the mandible is in centric relation. The registration may be obtained either intraorally or extraorally
clutch \klŭch\ coll n: a device placed in both the maxillary and mandibular arches for the purpose of supporting components used to record mandibular movement
1condylar guidance \k n′da-lar gīd′ns\ vt: mandibular guidance generated by the condyle and articular disc traversing the contour of the glenoid fossae
n′da-lar gīd′ns\ vt: mandibular guidance generated by the condyle and articular disc traversing the contour of the glenoid fossae
2condylar guidance \kn′da-lar gīd′ns\ n: the mechanical form located in the upper posterior region of an articulator that controls movement of its mobile member
condylar guide assembly \kn′da-lar gīd a-m′blē\: the components of an articulator that guide movement of the condylar analogues
condylar hinge position \kn′da-lar hnj pa-zsh′an\ obs: the position of the condyles of the mandible in the glenoid fossae at which hinge axis movement is possible (GPT-4)
de·pro·gram·mer \dē-prō′grăm′er\ n: various types of devices or materials used to alter the proprioceptive mechanism during mandibular closure
diagnostic cast \dī′ag-ns′tik kăst\: a life-size reproduction of a part or parts of the oral cavity and/or facial structures for the purpose of study and treatment planning
diagnostic waxing : waxing of intended restorative contours on dental casts for the purpose of evaluation and planning restorations
earbow \îr-bō\ n (20c): an instrument similar to a facebow that indexes to the external auditory meatus and registers the relation of the maxillary dental arch to the external auditory meatus and a horizontal reference plane. This instrument is used to transfer the maxillary cast to the articulator. The earbow provides an average anatomic dimension between the external auditory meatus and the horizontal axis of the mandible—see FACEBOW
eccentric \k-n′trk\ adj (14c): 1: not having the same center 2: deviating from a circular path 3: located elsewhere than at the geometric center 4: any position of the mandible other than that which is its normal position
eccentric interocclusal record \k-n′trk n′ter-a-klōō′sal rk′erd\: a registration of any maxillomandibular position other than centric relationship
eccentric relation \k-n′trik r-lā′shun\: any relationship of the mandible to the maxilla other than centric relation—see ACQUIRED E.R.
facebow \fās bō\: a caliper-like instrument used to record the spatial relationship of the maxillary arch to some anatomic reference point or points and then transfer this relationship to an articulator; it orients the dental cast in the same relationship to the opening axis of the articulator. Customarily the anatomic references are the mandibular condyles transverse horizontal axis and one other selected anterior point; called also hinge bow—see EARBOW, KINEMATIC F.
facebow fork \fās bō fork\: that component of the facebow used to attach the occlusion rim to the facebow
facebow record \fās bō rk′erd\: the registration obtained by means of a facebow
Fischer’s angle [Rudolf Fischer, Swiss dentist, Zurich, Switzerland]: eponym for the angle formed by the intersection of the protrusive and nonworking side condylar paths as viewed in the sagittal plane
Fischer R. Beziehungen zwischen den Kieferbewegungen und der Kauflachenform der Zuhne. Schweizerische Monataschrift fur Zahnheilkunde Zurich 1926;74.
Fischer R. Die Offnungsbewegungen des Unterkiefers und ibre Wiedergabe am Artikulator. Schweizerische Monateschrift fur Zahnheilkunde 1935;45:867-99.
Frankfort horizontal plane \Frăngk′fort hôr′-zn′tl plān\: 1: eponym for a plane established by the lowest point on the margin of the right or left bony orbit and the highest point on the margin of the right or left bony auditory meatus 2: a horizontal plane represented in profile by a line between the lowest point on the margin of the orbit to the highest point on the margin of the auditory meatus; adopted at the 13th General Congress of German Anthropologists (the “Frankfort Agreement”) at Frankfort am Main, 1882, and finally by the International Agreement for the Unification of Craniometric and Cephalometric Measurements in Monaco in 1906; called also auriculo-orbital plane, eye-ear plane, Frankfort horizontal (FH), Frankfort horizontal line
fully adjustable articulator \f
l′ē a-jŭst-a′bal är-tk′ya-lā′tor\: an articulator that allows replication of three dimensional movement of recorded mandibular motion—called also Class IV articulator
fully adjustable gnathologic articulator \f
l′ē a-jŭst-a′bal năth′ō-lj′ik är-tk′ya-lā′tor\: an articulator that allows replication of three dimensional movement plus timing of recorded mandibular motion—called also Class IV articulator
guide pin \gīd pn\: the component of a dental implant system that is placed within the surgically prepared osseous site for an endosteal implant. It assists in determination of location and angulation of the site relative to other soft tissue or bony landmarks
hinge axis : see TRANSVERSE HORIZONTAL AXIS
hinge position \hnj pa-zsh′an\ obs: the orientation of parts in a manner permitting hinge movement between them (GPT-4)
horizontal plane of reference \hôr′-zn-tl, hr′- plān ŭv rf′er-ans, rf′rans\: a horizontal plane established on the face of the patient by one anterior reference point and two posterior reference points from which measurements of the posterior anatomic determinants of occlusion and mandibular motion are made
hydrocolloid \hī′dra-kl′oid\ n (1916): a colloid system in which water is the dispersion medium; those materials described as a colloid sol with water that are used in dentistry as elastic impression materials—see IRREVERSIBLE H., REVERSIBLE H.
incisal guidance \n-s′zal gīd′ans\: 1: the influence of the contacting surfaces of the mandibular and maxillary anterior teeth on mandibular movements 2: the influence of the contacting surfaces of the guide pin and guide table on articulator movements
instantaneous axis of rotation \n′stan-tā′nē-as ăk′ss ŭv rō-tā′shun\: the hypothetical center of rotation of a moving body, viewed in a given plane, at any point in time; for any body that has planar motion, there exists, at any instant, some points that have zero velocity and will be fixed at a given instant. The line joining these points is the instantaneous axis of rotation. The intersection of this line with the plane of motion is called the instantaneous center of rotation
in·ter·cus·pa·tion \n′ter-kŭs-pā′shun\ n, obs: the interdigitation of cusps of opposing teeth (GPT-4)
interocclusal record \n′ter-a-klōō′sal rk′ard\: a registration of the positional relationship of the opposing teeth or arches; a record of the positional relationship of the teeth or jaws to each other
irreversible hydrocolloid \r′-vûr′sa-bal hī′dra-kl′oid′\: a hydrocolloid consisting of a sol of alginic acid having a physical state that is changed by an irreversible chemical reaction forming insoluble calcium alginate—called also alginate, dental alginate
kinematic axis \kn′a-măt′k ăk′ss\: the transverse horizontal axis connecting the rotational centers of the right and left condyles
kinematic facebow \kn′a-măt′k fās-bō\: a facebow with adjustable caliper ends used to locate the transverse horizontal axis of the mandible
lateral interocclusal record \lăt′ar-al n′ter-a-klōō′sal rk′ard′\: a registration of the positional relationship of opposing teeth or arches made in either a right or left lateral position of the mandible
leaf gauge \lēf gāj\: a set of blades or leaves of increasing thickness used to measure the distance between two points or to provide metered separation
Lucia jig [Victor O. Lucia, U.S. prosthodontist]: eponym—see ANTERIOR PROGRAMMING DEVICE
Lucia VO. Treatment of the edentulous patient. Chicago: Quintessence, 1986.
lu·mi·nance \lōō′ma-nans\ n (1880): the intensity of light per unit area
man·di·ble \măn′da-bal\ n (15c): the lower jawbone
man·dib·u·lar \măn-db′ya-lar\ adj: of or pertaining to the mandible
mandibular axis : see SAGITTAL AXIS, TRANSVERSE HORIZONTAL AXIS, VERTICAL AXIS
mandibular condyle : the articular process of the mandible, called also the head of the mandible—see also CONDYLE
mandibular relationship record \măn-db′ya-lar r-lā′shun-shp\: any registration of the relationship of the mandible to the maxillae
me·a·tus \mē-ā′tus\ n, pl me·a·tus·es or me·a·ti (1665): a natural body passage; a general term for any opening or passageway in the body
1mount·ing \moun′tng\ v: the laboratory procedure of attaching a cast to an articulator or cast relater
2mount·ing \moun′tng\ n: the relationship of dental casts to each other and the instrument to which they are attached; see also—SPLIT-CAST M.
mounting plate \moun′tng plāt\: removable metal or resin devices that attach to the superior and inferior members of an articulator, which are used to attach casts to the articulator
muscle spasm \mŭs′al spăz′am\: a sudden involuntary contraction of a muscle or group of muscles attended by pain and interference with function. It differs from muscle splinting in that the contraction is sustained even when the muscle is at rest and the pain/dysfunction is present with passive and active movements of the affected part—called also myospasm
NA : acronym for NAsion; a cephalometric landmark located where the intranasal and nasofrontal sutures meet
nano·me·ter \năn′a-mē′tar\ n (1963): unit of length to measure the wavelength of light. It is equivalent to 1 ¥ 10−9 M or 10 angstroms. 1 nm = 1/1,000,000 mm
nas·ion \nā′zhun\ n: a bony cephalometric landmark at which the nasofrontal suture is bisected by the midsagittal plane
nonadjustable articulator \nn-a-jŭst′ă-bal är-tk′ya-lā′tor\: an articulator that does not allow adjustment to replicate mandibular movements—see also CAST RELATOR
nonarcon articulator : 1: any articulator which broadly replicates the three dimensional motions of the left and right condylar compartments 2: any articulator design in which the condylar element (analog) is not part of the lower member of the articulator and may be used to simulate the three dimensional motions of the left and right condylar compartments
oc·clude \a-klōōd′\ vb oc·clud·ed; oc·clud·ing vt (1597): 1: to bring together; to shut 2: to bring or close the mandibular teeth into contact with the maxillary teeth
occluding centric relation record \a-klōōd′ng n′trk r-lā′shun rk′ard\ obs: a registration of centric relation made at the established occlusal vertical dimension (GPT-4)
oc·clu·sal \a-klōō′zal, -sal\ adj (1897): pertaining to the masticatory surfaces of the posterior teeth, prostheses, or occlusion rims
occlusal device \a-klōō′zal, -sal d-vīs′\: any removable artificial occlusal surface used for diagnosis or therapy affecting the relationship of the mandible to the maxillae. It may be used for occlusal stabilization, for treatment of temporomandibular disorders, or to prevent wear of the dentition
occlusal disharmony \a-klōō′zal, -sal ds-hăr′ma-nē\: a phenomenon in which contacts of opposing occlusal surfaces are not in harmony with other tooth contacts and/or the anatomic and physiologic components of the craniomandibular complex
occlusion record \a-klōō′shun rk′ard\ obs: a registration of opposing occluding surfaces made at any maxillomandibular relationship (GPT-4)
occlusion rim \a-klōō′shun rm\: occluding surfaces fabricated on interim or final denture bases for the purpose of making maxillomandibular relation records and arranging teeth—called also record rim
pan·to·graph \păn′ta-gräf′\ n (1723): 1: an instrument used for copying a planar figure to any desired scale 2: in dentistry, an instrument used to graphically record in, one or more planes, paths of mandibular movement and to provide information for the programming of an articulator
pantographic tracing \păn′ta-gräf′k trā′sng\: a graphic record of mandibular movement usually recorded in the horizontal, sagittal and frontal planes as registered by styli on the recording tables of a pantograph or by means of electronic sensors
preliminary cast \pr-lm′a-nr′ē\: a cast formed from a preliminary impression for use in diagnosis or the fabrication of an impression tray
preliminary impression \pr-lm′a-nr′ē m-prsh′an\: a negative likeness made for the purpose of diagnosis, treatment planning, or the fabrication of a tray
preoperative record \prē-p′ar-a-tv, -p′ra-, -p′a-rā- rk′ard\ obs: any record made for the purpose of study or treatment planning (GPT-4)
preoperative wax-up : a dental diagnostic procedure in which planned restorations are developed in wax on a diagnostic cast to determine optimal clinical and laboratory procedures necessary to achieve the desired esthetics and function—called also diagnostic wax-up, preoperative waxing
pretreatment records \prē-trēt′mant rk′ardz\: any records made for the purpose of diagnosis, recording of the patient history, or treatment planning in advance of therapy
pro·file \prō′fīl′\ n (ca. 1656): an outline or contour, especially one representing a side view of a human head
protrusive interocclusal record \prō-trōō′sv n′tar-a-klōō′zal rk′ard\: a registration of the mandible in relation to the maxillae when both condyles are advanced in the temporal fossa
reciprocal click \r-sp′ra-kal klk\: clicks emanating from the temporomandibular joint, one of which occurs during opening movement and the other during closing movement
1re·cord \r-kōrd\ vb (14c): 1: to register data relating to specific conditions that exist currently or previously 2: to register permanently by mechanical means, i.e., jaw relationships—see CENTRIC RELATION R., ECCENTRIC INTEROCCLUSAL R., INTEROCCLUSAL R., OCCLUDING JAW R., TERMINAL JAW RELATION R.
2re·cord \r-kōrd\ n (14c): 1: an official document 2: a body of known or recorded facts about someone or something
record base \rk′ard bās\: an interim denture base used to support the record rim material for recording maxillomandibular records
reg·is·tra·tion \rj′-strā′shun\ n (1566): 1: the making of a record of the jaw relationships present, or those desired, thus allowing their transfer to an articulator to assist in proper fabrication of a dental prosthesis 2: a record made of the desired maxillomandibular relationship and used to relate casts to an articulator—see MAXILLOMANDIBULAR RELATIONSHIP RECORD
semi-adjustable articulator \m′ē-a-jŭst′a-bal är-tk′ya-lā-tor\: an articulator that allows adjustment to replicate average mandibular movements—called also Class III articulator
1spat·u·late \spăch′a-lt\ adj (1760): shaped like a spatula
2spat·u·late \spăch′a-lt\ vt -ed /-ing /-s: to work or treat with a spatula
split-cast method \splt-kăst mth′ad\ obs: 1: a procedure for placing indexed casts on an articulator to facilitate their removal and replacement on the instrument 2: the procedure of checking the ability of an articulator to receive or be adjusted to a maxillomandibular relation record (GPT-4)
split-cast mounting \splt-kăst moun′tng\: a method of mounting casts wherein the dental cast’s base is sharply grooved and keyed to the mounting ring’s base. The procedure allows verifying the accuracy of the mounting, ease of removal and replacement of the casts
stereographic record \str′ē-a-grăf′k\: an intra or extraoral recording of mandibular movement as viewed in three planes in which the registrations are obtained by engraving, milling, or burnishing the recording medium by means of studs, rotary instruments, styli, teeth, or abrasive rims
transverse horizontal axis \trăns-vûrs′, trănz-, trăns′vûrs′, trănz′-\: an imaginary line around which the mandible may rotate within the sagittal plane
STUDY QUESTIONS
1 Mendez AJ. The influence of impression trays on the accuracy of stone casts poured from irreversible hydrocolloid impressions. J Prosthet Dent. 1985;54:383.
2 Lim PF, et al. Adaptation of finger-smoothed irreversible hydrocolloid to impression surfaces. Int J Prosthodont. 1995;8:117.
3 Khaknegar B, Ettinger RL. Removal time: a factor in the accuracy of irreversible hydrocolloid impressions. J Oral Rehabil. 1977;4:369.
4 al-Omari WM, et al. A microbiological investigation following the disinfection of alginate and addition cured silicone rubber impression materials. Eur J Prosthodont Restor Dent. 1998;6:97.
5 Hall BD, et al. Effects of a chemical disinfectant on the physical properties of dental stones. Int J Prosthodont. 2004;17:65.
6 Johnson GH, et al. Dimensional stability and detail reproduction of irreversible hydrocolloid and elastomeric impressions disinfected by immersion. J Prosthet Dent. 1998;79:446.
7 Reisbick MH, et al. Irreversible hydrocolloid and gypsum interactions. Int J Prosthodont. 1997;10:7.
8 Young JM. Surface characteristics of dental stone: impression orientation. J Prosthet Dent. 1975;33:336.
9 Palik JF, et al. Accuracy of an earpiece face-bow. J Prosthet Dent. 1985;53:800.
10 O’Malley AM, Milosevic A. Comparison of three facebow/semi-adjustable articulator systems for planning orthognathic surgery. Br J Oral Maxillofac Surg. 2000;38:185.
11 Piehslinger E, et al. Computer simulation of occlusal discrepancies resulting from different mounting techniques. J Prosthet Dent. 1995;74:279.
12 Adrien P, Schouver J. Methods for minimizing the errors in mandibular model mounting on an articulator. J Oral Rehabil. 1997;24:929.
13 Dawson PE. Temporomandibular joint pain-dysfunction problems can be solved. J Prosthet Dent. 1973;29:100.
14 Tarantola GJ, et al. The reproducibility of centric relation: a clinical approach. J Am Dent Assoc. 1997;128:1245.
15 McKee JR. Comparing condylar position repeatability for standardized versus nonstandardized methods of achieving centric relation. J Prosthet Dent. 1997;77:280.
16 Lucia VO. A technique for recording centric relation. J Prosthet Dent. 1964;14:492.
17 Gross M, et al. The effect of three different recording materials on the reproducibility of condylar guidance registrations in three semi-adjustable articulators. J Oral Rehabil. 1998;25:204.
18 Wirth CG. Interocclusal centric relation records for articulator mounted casts. Dent Clin North Am. 1971;15:627.
19 Wirth CG, Aplin AW. An improved interocclusal record of centric relation. J Prosthet Dent. 1971;25:279.
20 Lundeen HC. Centric relation records: the effect of muscle action. J Prosthet Dent. 1974;31:244.
21 Kepron D. Variations in condylar position relative to central mandibular recordings. In: Lefkowitz W, editor. Proceedings of the Second International Prosthodontic Congress. St. Louis: Mosby; 1979:210.
22 Teo CS, Wise MD. Comparison of retruded axis articular mountings with and without applied muscular force. J Oral Rehabil. 1981;8:363.
23 Tamaki K, et al. Reproduction of excursive tooth contact in an articulator with computerized axiography data. J Prosthet Dent. 1997;78:373.
24 Lundeen HC, Wirth CG. Condylar movement patterns engraved in plastic blocks. J Prosthet Dent. 1973;30:866.
25 Bell LJ, Matich JA. A study of the acceptability of lateral records by the Whip-Mix articulator. J Prosthet Dent. 1977;38:22.
26 Celar AG, et al. Guided versus unguided mandibular movement for duplicating intraoral eccentric tooth contacts in the articulator. J Prosthet Dent. 1999;81:14.
27 Chang WSW, et al. An in vitro evaluation of the reliability and validity of an electronic pantograph by testing with five different articulators. J Prosthet Dent. 2004;92:83.