32 POSTOPERATIVE CARE
After placement and cementation of a fixed dental prosthesis (FDP), patient treatment continues with a carefully structured sequence of postoperative appointments designed to monitor the patient’s dental health (Fig. 32-1), stimulate meticulous plaque control habits, identify any incipient disease, and introduce whatever corrective treatment may be needed before irreversible damage occurs.

Fig. 32-1 Treatment after placement of multiple restorations. To ensure tissue health and long-term success, proper oral hygiene is mandatory.
Patients should be instructed in special plaque-control measures, especially around pontics and connectors, and the use of special oral hygiene aids such as floss threaders (Fig. 32-2). If the pontics are properly designed (see Chapter 20), floss can be looped through the embrasure spaces on each side, and the loop can be pulled tightly against the convex pontic tissue surface. A sliding motion is then used to remove dental plaque (Fig. 32-3). Flossing under pontics is essential for improving prosthesis longevity. When dental floss is used, the mucosa beneath pontics remains healthy; without it, mild or moderate inflammation results.1 Tissue response has been shown to be independent of the pontic material.2


Fig. 32-3 The patient should be instructed in the use of floss to clean partial fixed dental prostheses.
Recall examinations are especially important for patients with extensive restorations and should be carried out by the dentist. Responsibility for follow-up care should not be delegated to auxiliary personnel (although good cooperation with a dental hygienist will prove beneficial for success).
Detecting disease around an FDP can be extremely difficult at a stage when corrective treatment is still relatively simple. For instance, partial dissolution of the luting agent may be difficult to diagnose with a subgingival margin. Caries is often detected only after irreversible pulp involvement has resulted. Caries under a crown is more difficult to detect radiographically, although bitewing images provide some information interproximally. Follow-up studies on patients with FDPs reveal that identifying risk factors and predicting the development of caries in any particular patient are complicated. However, there is no indication that caries is more likely in association with prostheses than on unrestored teeth.3
If caries is overlooked, disease may rapidly progress to the point at which the fabrication of a new prosthesis becomes inevitable or, even worse, tooth loss results.
POSTCEMENTATION APPOINTMENTS
To enable the dentist to monitor the function and comfort of the prosthesis and to verify that proper plaque control has been mastered by the patient (Fig. 32-4), an appointment is generally scheduled within a week to 10 days after the cementation of an FDP. The dentist should check carefully that the gingival sulcus remains clear of any residual luting agent that may have been overlooked previously and that all aspects of the occlusion remain satisfactory.

Fig. 32-4 Postcementation monitoring of plaque control is necessary around recently cemented restorations. Poor oral hygiene has led to gingival inflammation (arrows).
Radiolucent cements should be avoided because detecting excess luting agent radiographically is impossible if that material is effectively radiolucent. As luting agent radiopacity increases, excess cement is spotted more easily on routine radiographs; therefore, the dentist should choose a luting agent that is as radiopaque as possible. In practice, luting agents are available in a wide range of radiopacities.4-6 Figure 32-5 summarizes data from these studies.
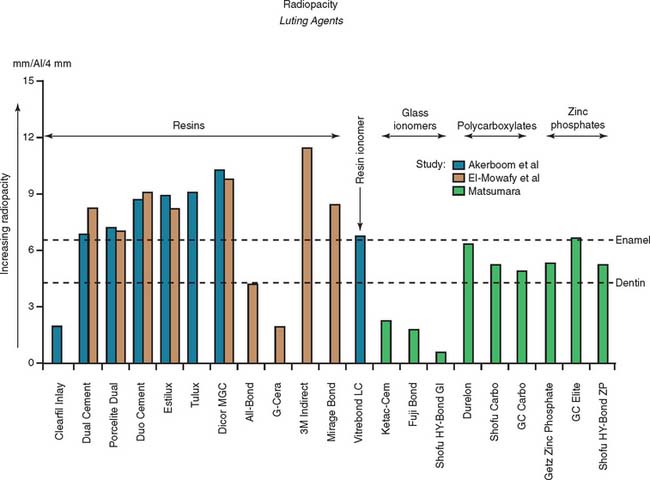
Fig. 32-5 Radiopacity of luting agents. In three in vitro studies,4-6 investigators compared the radiographic appearance of various luting agents to aluminum. The data were normalized to account for different specimen thicknesses used by the investigators. Excess luting agent is more difficult to detect if materials with lower values are chosen. In addition, margin gaps and recurrent caries are more difficult to diagnose.
The presence of fremitus (see Chapter 1) or “polished” facets on the occluding surfaces of cast restorations at the postcementation appointment should prompt a careful reassessment and correction of the occlusion. If any minor shift in tooth position has occurred, some occlusal adjustment may be necessary. If so, the patient is rescheduled to visit the following week to ensure that no further correction is needed.
PERIODIC RECALL
Patients with cast restorations should attend recall visits at least every 6 months. Less frequent recall may lead to oversight of recurrent caries or the development of periodontal disease. Patients who have been provided with extensive fixed prostheses (Fig. 32-6) need more frequent recall appointments, particularly when advanced periodontal disease was present. The appointments can be coordinated by the restorative dentist or the periodontist. To ensure treatment continuity, it is imperative to establish in advance who will assume primary responsibility for coordinating recall appointments.

Fig. 32-6 Patients who have received extensive treatment of this nature require more frequent follow-up care.
History and General Examination
The patient’s medical history should be reviewed and updated at least annually. The patient should be examined according to the principles introduced in Chapter 1. Particular attention is paid to the soft tissues, because early signs of oral cancer may be detected at a recall appointment.
Oral Hygiene, Diet, and Saliva
Patients tend to become somewhat less diligent in their plaque control efforts when the active phase of their treatment is completed. The dentist should look carefully for any signs of deterioration in oral hygiene and assess the general effectiveness of plaque control at every recall with an objective index (Fig. 32-7). Deficiencies must be identified early, and corrective therapy should be initiated. The dentist should ask about changes in diet, particularly increased sugar consumption or “fad” diets. Excessive weight loss or gain should also be investigated. For instance, a patient who has recently stopped smoking may start ingesting large amounts of candy, which can result in an increase in dental caries.

Fig. 32-7 A, Plaque control record filled out at the first appointment for teaching proper oral hygiene measures. B, Plaque control record after four sessions of instruction. This patient’s plaque level is such that definitive treatment can begin. This level of plaque control needs to be maintained during the postoperative phase of treatment.
(Modified from Goldman HM, Cohen DW: Periodontal Therapy, 5th ed. St. Louis, Mosby, 1973.)
Saliva plays an important role in caries development. Patients with xerostomia can rapidly develop extensive carious lesions.7 Diagnosing the cause of reduced saliva is imperative; the origin is often a drug side effect.8
Dental Caries
Dental caries (Fig. 32-8) is the most common cause of failure of a cast restoration.9-12 Detection can be very difficult,13 particularly where complete coverage is used. At each appointment, the teeth should be thoroughly dried and visually inspected (Fig. 32-9). The explorer must be used very carefully when early enamel lesions are assessed, because a heavy-handed examination may damage the fragile demineralized enamel matrix. An intact enamel matrix is essential for procedures that induce remineralization14 (e.g., improved plaque control, dietary changes, topical fluoride applications).

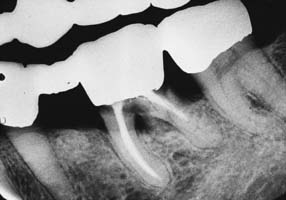
Fig. 32-8 Undetected caries beneath this partial fixed dental prosthesis resulted in serious complications.

Conservative treatment of caries at the cavosurface margin is especially problematic. The lesion can spread rapidly, particularly if the restoration has a less than optimal marginal fit. Correcting the problem with a small amalgam, composite resin, or glass ionomer restoration is sometimes possible (Fig. 32-10). If the cast restoration is supported by an amalgam or composite resin core, the extent of the caries may be difficult to determine. When there is doubt that all carious dentin has been removed, replacing the entire restoration is recommended.

Fig. 32-10 Occasionally, cervical glass ionomer or amalgam restorations (arrows) can extend the useful life of a previously placed cast restoration and postpone complicated replacement of the prosthesis.
Root caries
Caries of exposed root surfaces (Fig. 32-11) can be a severe problem in the age group commonly seeking fixed prosthodontic care.15-17 In the classic Vipeholm study,18 root caries accounted for more than 50% of new lesions in patients in the 50-year-old age group. Root caries incidence increased considerably with age.19 In the caries examination from phase 1 of the Third National Health and Nutrition Examination Survey, root caries affected 22.5% of the dentate population.20 Root surface caries seems to be associated with individual dental plaque scores and high counts of salivary Streptococcus mutans.21 Xerostomia that is age-related or caused by medication or radiation treatment has been implicated in the etiology of rampant caries.22-24 Other factors include the patient’s economic status, diet, oral hygiene, and ethnic background.25 Only a most vigorous effort on the part of the dentist and patient leads to resolution of the problem. Prevention is focused on diet counseling and fluoride treatment. Treatment often requires the placement of large cervical glass ionomer or amalgam restorations that wrap around the periphery of previously placed cast restorations. Such restorations are difficult to place. However, in view of the constraints, they are a preferred alternative to comprehensive re-treatment with elaborate fixed prostheses.
Periodontal Disease
Unfortunately, periodontal disease often occurs after placement of fixed prostheses,26 especially where the cavosurface margin has been placed subgingivally27-29 or the prosthesis is overcontoured.30 Inflammation is more severe with poorly fitting restorations31 (Fig. 32-12), but even “perfect” margins have been associated with periodontitis.32 At recall appointments, particular attention is given to sulcular hemorrhage, furcation involvement, and calculus formation as early signs of periodontal disease. Improperly contoured restorations should be recontoured or replaced.
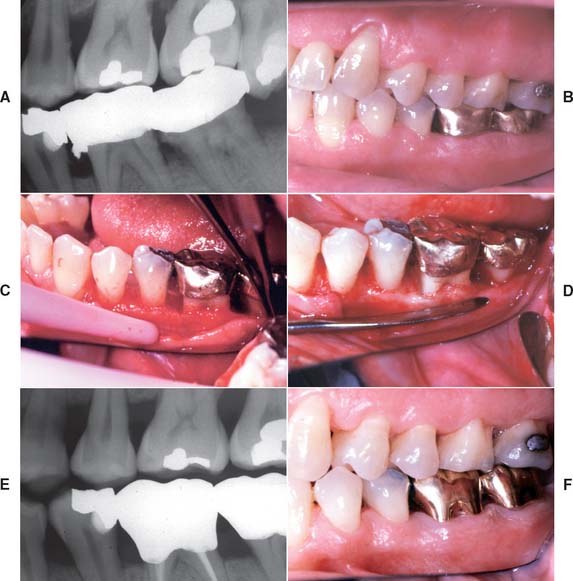
Fig. 32-12 Periodontal failure resulting from defective fixed prostheses. A, Inadequate margins and contour. B, Appearance before surgery. C, Flap reflected. D, Appearance after surgical recontouring. E, Radiograph of new cast restorations. F, Replacement restorations.
(Courtesy of Dr. C. L. Politis.)
Occlusal Dysfunction
The patient is examined for signs of occlusal dysfunction at each recall appointment. The patient should be asked about any noxious habits such as bruxism. An examination of the occlusal surfaces may reveal abnormal wear facets (Fig. 32-13). In particular, the canines should be inspected, because wear in this area soon leads to other excursive interferences. If a patient engages in parafunctional activity that causes tooth wear, the progression of facet formation often begins on the canines. In a slightly more advanced state of wear, additional facets can be observed on the incisor teeth, after which excursive interfering contacts result in wear facets on the posterior teeth. Abnormal tooth mobility is investigated, as is muscle and joint pain. A standardized muscle-and-joint palpation technique (see Chapter 1) is helpful. Articulated diagnostic casts should be periodically remade (Fig. 32-14) and compared with previous records so that any occlusal changes can be monitored and corrective treatment initiated.

Fig. 32-13 If a cast restoration is not designed according to neuromuscular and temporomandibular controls, extensive wear can result after a relatively short time.
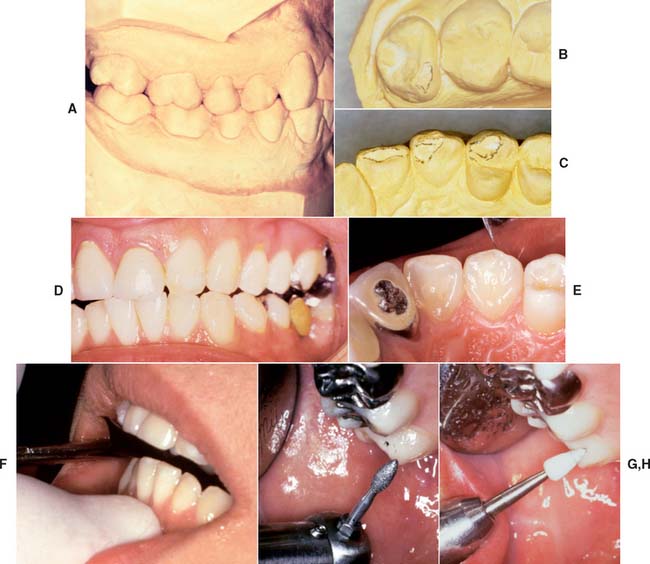
Fig. 32-14 Posttreatment occlusal analysis. A, Diagnostic casts should be articulated periodically. B and C, Non-working wear facets on the maxillary molar correspond with wear on the premolar, canine, and lateral incisor. D and E, Mandibular excursion corresponding to the observed wear patterns. F and G, After marking, the newly detected interferences can be easily removed. H, The adjusted surfaces are polished.
A small number of patients may not have responded well to previous occlusal treatment or may resume parafunctional activity some time after completion of the active phase of fixed prosthodontic treatment. Although resolving the underlying etiology is preferable, a nightguard can occasionally be prescribed (Fig. 32-15). Its design is identical to that of the occlusal device described in Chapter 4 for treating neuromuscular symptoms resulting from malocclusion. However, the device is worn only at night. If the patient primarily clenches, the dentist should consider a slightly flatter anterior ramp than is ordinarily incorporated in the conventional device.

Pulp and Periapical Health
At the recall appointment, the patient may describe one or more episodes of pain during the previous months. This could indicate the loss of vitality of an abutment tooth and should be investigated. Appropriate corrective measures can then be taken.
One advantage of partial-coverage restorations is that pulp health can be monitored with an electric pulp tester (Fig. 32-16), although the vitality of any tooth with a complete crown can still be assessed by thermal means. Correlating the histologic condition of a pulp directly with the patient’s response to pulp testing is difficult.33 Therefore, such results should be combined with other clinical data that result from careful patient history documentation and examination. Seeking the opinion of an endodontist is often advisable (Fig. 32-17). Radiographs provide useful information about the presence of periapical pathosis. Teeth with fixed restorations should be reviewed radiographically every few years. The use of a standardized technique enables the dentist to make an objective comparison with previous films. Although some studies have shown a high incidence of periapical disease associated with fixed prostheses,34,35 other studies have shown a low incidence of this complication.29,36,37


EMERGENCY APPOINTMENTS
On occasion, patients have an emergency between routine recall visits. With carefully planned and executed treatment, however, these should be rare (although problems can still develop even with the best treatment). Patients should be taught to notice small changes in their oral health and to report them without delay. For instance, the porcelain veneer of a metal-ceramic restoration may be shielded from further fracture when a small chip is promptly rounded off and the occlusion adjusted immediately after it is first noticed. Postponement of corrective treatment can be especially costly, necessitating a remake of a complex prosthesis that could have been saved with prompt attention.
Pain
A patient presenting with pain should be asked about its location, character, severity, timing, and onset. Factors that precipitate, relieve, or change the pain should be investigated, and appropriate treatment measures should be initiated (see Chapter 3).
Although most oral pain is of pulpal origin, such an origin should never be assumed. A detailed investigation is always recommended. In difficult or questionable situations, the diagnosis should be confirmed by an appropriate specialist.
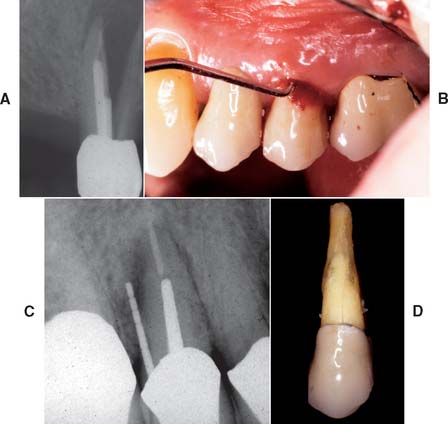
If the patient has several endodontically treated teeth that have been restored with posts and cores and with fixed prostheses, the possibility of root fracture should be considered, especially for teeth that were internally weakened as a result of endodontic treatment in conjunction with oversized posts of suboptimal length. If a fracture has occurred, the tooth is almost invariably lost, which can significantly complicate follow-up treatment, especially if it involves an abutment tooth for an FDP (Fig. 32-18).
Loose Abutment Retainer
A loose retainer (Fig. 32-19) may not be easily perceived by the patient, especially if it is part of a fixed prosthesis supported by several abutment teeth. The patient may have noticed a bad taste or smell rather than detecting movement.

Fig. 32-19 A, Severe tooth destruction may result when a loose retainer goes undetected. B, Looseness of one retainer can occasionally be observed directly (arrow) when force is exerted in an occlusal direction. C, Water is then applied to the cervical area, and the diagnosis is confirmed if bubbles appear when pressure is exerted (D).
Unless appropriate instrumentation is available, removing the prosthesis intact for recementation is often difficult or impossible. The more recently developed devices shown in Figures 32-20 to 32-22 have been successful, but they are expensive. The devices shown in Figure 32-23 are less reliable and can be quite intimidating and uncomfortable for the patient. On occasion, a direct pull with hemostat forceps succeeds. (Metal-ceramic crowns should first be coated with autopolymerizing acrylic resin to prevent chipping or cracking.) Applying the tip of an ultrasonic scaler to the restoration is recommended because prolonged ultrasonic vibration can decrease crown retention.38 A procedure for removing crowns and FDPs with a strongly adhesive resin39 has been used successfully in certain cases40 (Fig. 32-24). When trying to remove a permanently cemented prosthesis, the dentist must use great caution. Unless force is applied in the path of withdrawal, an abutment tooth may fracture, and tooth loss may result.
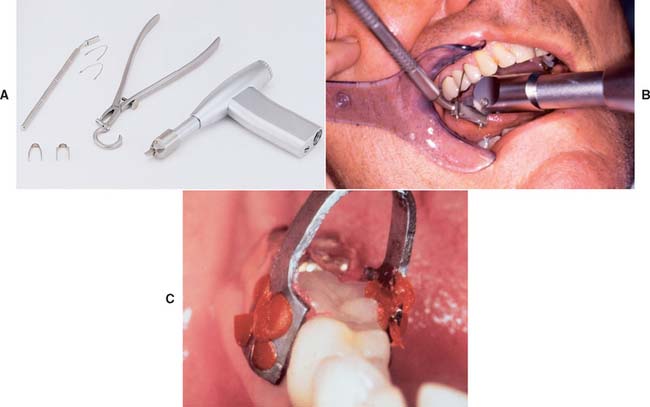
Fig. 32-20 CORONAflex crown remover. This is an air-driven device that connects to standard dental handpiece hoses via KaVo’s MULTIflex coupler. The crown remover delivers a controlled low-amplitude impact at its tip. The device works well on partial fixed dental prostheses (FDPs) and is well tolerated by patients. A, The kit includes loops to thread under FDP connectors that attach to a holder, calipers, and an adhesive clamp to obtain a purchase on single crowns. The goal is to deliver the impact in the long axis of the abutment tooth. B, The loop is threaded under the connector. The tip of the crown remover is placed on the bar, and the impact is activated by releasing the index finger from the air valve. C, The adhesive clamp is attached with autopolymerizing resin used to remove a single crown.
(A and C, Courtesy of KaVo Dental Corporation, Lake Zurich, Illinois.)

Fig. 32-21 The Metalift Crown and Bridge Removal System (Classic Practice Resources, Baton Rouge, Louisiana). A, Five-unit partial fixed dental prosthesis (FDP) supporting a partial removable dental prosthesis. The anterior abutment (right mandibular central incisor) is loose; the posterior abutments (both right mandibular premolars) are firmly cemented. B, Access to the metal on each abutment is provided by preparing through the porcelain with a diamond. C, The metal is penetrated with a No. 1 round bur to create a pilot channel in each abutment. D, The pilot hole is followed by the special drill. E, The holes should just penetrate the metal, as indicated by the visible cement. F, The Metalift instrument is threaded into both crowns, breaking the cement seal. G, The partial FDP is removed, and if the abutments are satisfactory as seen here (H), it can be recemented for further service. The manufacturer supplies threaded keys that can be used to seal the occlusal holes. To facilitate recovery, they can also be incorporated in crowns before cementation.
(Courtesy of Dr. R. D. Westerman.)

Fig. 32-22 Removal devices. A, K.Y. Pliers. This device has specially rasped finish with small sharp pins and is designed to grip a crown or partial fixed dental prosthesis and to deliver a removal force along the long axis. Grip can be enhanced with emery powder. B, Easy Pneumatic C&B Remover II. This device uses compressed air to deliver a controlled, adjustable force to remove the restoration.
(A, Courtesy of GC America, Alsip, Illinois. B, Courtesy of Dent Corp Research and Development, White Plains, New York.)

Fig. 32-23 Crown removers. A, Back-action. B, Spring-activated.
(A, Courtesy of Henry Schein Inc., Melville, New York. B, Courtesy of Peerless International Inc., North Easton, Massachusetts.)

Fig. 32-24 Richwil Crown and Bridge Remover (Almore International, Inc., Portland, Oregon). This adhesive resin tablet is softened in warm water for 1 to 2 minutes, and the patient is instructed to occlude into it (A) (the manufacturer recommends tying a length of floss to the tablet to prevent aspiration). The resin is cooled with water. A sharp opening action should remove the crown (B). Care is needed to avoid removing a restoration in the opposing jaw.
A loose retainer usually indicates inadequate tooth preparation, poor cementation technique, or caries. In this case, the tooth requires repreparation and a new prosthesis. Sectioning the prosthesis rather than attempting to remove it intact is often the best policy (Fig. 32-25).
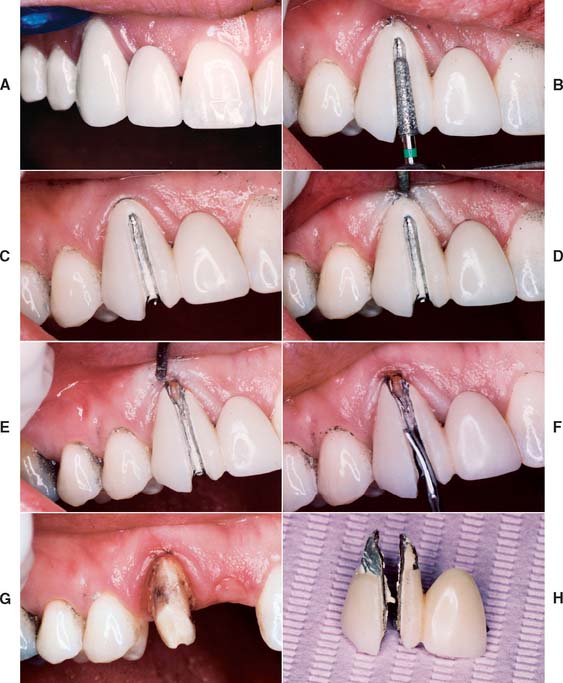
Fig. 32-25 Removal of an existing crown by sectioning. A, This cantilevered partial fixed dental prosthesis required replacement for esthetic and periodontal reasons. B, The restoration is carefully sectioned, with the initial cut through the ceramic just to the metal. It is easiest to do this on the facial and incisal surfaces. C, The goal is to cut through the metal just to the cement and follow the cement toward the gingival margin. D, The gingiva is displaced with an instrument and the crown carefully sectioned to the gingival margin (E). F, A suitable instrument (e.g., a cement spatula or sterilized screwdriver) is placed in the cut and gently rotated to force the halves of the crown apart. It may be necessary to section part of the lingual surface to facilitate this step. G, The abutment. Additional incisal reduction was necessary; the notch in the incisal edge is of no concern. H, Removed prosthesis.
(Courtesy of Dr. D. H. Ward.)
Fractured Connector
An improperly fabricated connector may fracture under functional loading (Fig. 32-26). Depending on the design and location of the FDP, the patient may complain of varying degrees of pain. Extra force is typically transmitted to the abutment teeth, and discomfort from overloading the periodontal ligament may draw attention away from the location of the actual problem. If the abutment teeth have good bone support and minimal mobility, fractured connectors can be very difficult to detect clinically. Wedges can sometimes be positioned to separate the individual FDP components enough to confirm the correct diagnosis.

Fractured Porcelain Veneer
Mechanical failure of a metal-ceramic restoration (Fig. 32-27) is not uncommon. It is usually related to faults in framework design, improper laboratory procedures, excessive occlusal function, or trauma (e.g., an automobile or sports accident).

If the porcelain has fractured on an otherwise satisfactory multiunit prosthesis, an attempt at repair rather than a remake may be justified to save the patient additional discomfort, time, and expense. When the fractured porcelain is not missing and there is little or no functional loading on the fracture site, it can sometimes be bonded in place with a porcelain repair system (Fig. 32-28) with the use of silane coupling agents or 4-methacryloxyethyl-trimellitic anhydride (4-META) to promote bonding with acrylic or composite resin.41-44 Unfortunately, the strength of joints made this way seems to diminish with changes in temperature45 and with prolonged water storage.46 Benefits from such repair are considered temporary, but it may be preferable to dismantling and remaking a complex FDP. In other circumstances, the fractured area may be repaired with composite resin retained by means of mechanical undercuts in the metal framework.47 The use of a silane coupling agent is also recommended for these repairs.

Fig. 32-28 On occasion, repairing a fractured metal-ceramic veneer rather than replacing the entire fixed dental prosthesis is advantageous. In this example, the porcelain surface has been etched; a resin repair system has been used.
A more permanent repair can sometimes be effected by making a metal-ceramic restoration to fit over the fractured original. This technique is appropriate when the pontic rather than an abutment retainer has fractured. A little ingenuity is needed to produce a suitable design.48,49 The most common difficulty encountered when such a repair is attempted is weakening of the connectors during the preparation, with the associated risk of subsequent prosthesis fracture (Fig. 32-29).
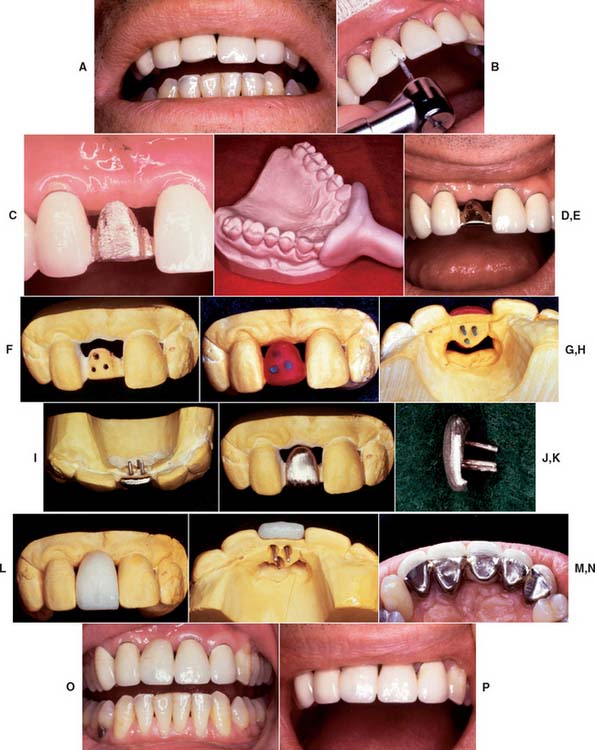
Fig. 32-29 Repair of a fractured metal-ceramic pontic. A, Pretreatment appearance. B, The ceramic veneer is removed with diamond rotary instruments. C, Appearance after porcelain removal. D, Special impression tray. E, Pinholes are placed in the substructure. F, Cast of the substructure. G and H, Waxed overlay. Note the plastic pins used (H). I, Cast overlay. J, Facial aspect. K, Proximal aspect. L, Facial aspect after the porcelain application. M, Lingual aspect after firing (cast relieved). N, Appearance after cementation. O and P, The finished repair.
(Courtesy of Dr. A. G. Gegauff.)
RE-TREATMENT
Fixed prostheses do not last forever; however, with good plaque removal, patient motivation, and average or above-average resistance to disease, a well-designed and well-fabricated restoration can provide many years of service. With poor care and neglect, even the “perfect” prosthesis or restoration can fail rapidly (Fig. 32-30). Because of exceptional host resistance, long-term success is sometimes possible with obviously defective restorations (Fig. 32-31).

Fig. 32-30 Osseous defects (arrows) within 2 years of the placement of this partial fixed dental prosthesis.
(Courtesy of Dr. J. Keene.)

Fig. 32-31 A “saddle” pontic should not be fabricated, because it makes plaque control impossible. A, However, this particular partial fixed dental prosthesis was replaced after 35 years of service. B, Despite poor pontic design, there are no significant signs of ulceration. This example illustrates the variability of tissue response as a result of differences in host resistance.
Nevertheless, at some stage, the decision about re-treatment must be made. Much depends on whether the re-treatment is part of an ongoing program of comprehensive care or whether the existing prosthesis has been subjected to years of neglect.
Planned Re-treatment
At the original treatment planning stage, re-treatment should be considered. This consideration may need to be general rather than specific because of difficulties in accurately predicting the pattern of future dental disease. On occasion, however, a prosthesis is designed to accommodate the eventual failure of a doubtful abutment (Fig. 32-32). With a little foresight, survey contours can already be incorporated in the retainers of an FDP to accommodate a future partial removable dental prosthesis in the event of a terminal abutment loss. Similarly, accommodations can be made for future occlusal rests by deliberately increasing occlusal reduction during tooth preparation and using metal occlusal surfaces. Furthermore, proximal boxes can be incorporated if it is anticipated that a nonrigid (dovetail) rest could simplify future re-treatment (see Fig. 32-32).
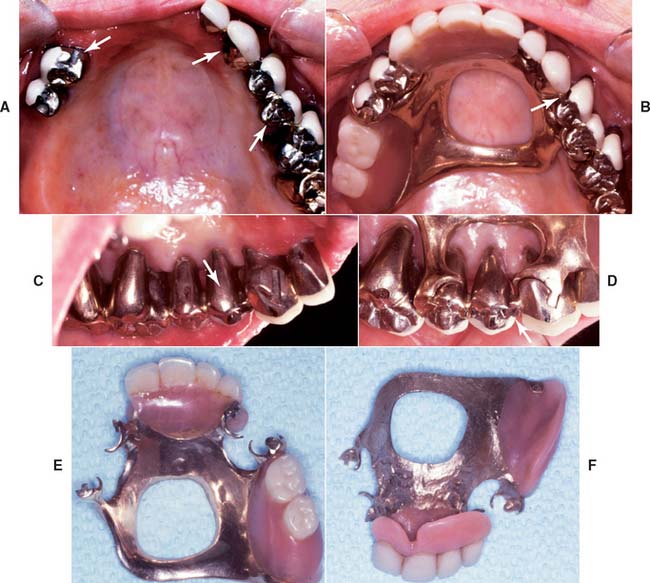
Fig. 32-32 Anticipation of future needs. A, Appearance 4 years after the restoration of an arch with periodontally compromised teeth. Three intracoronal rests (arrows) were fabricated to support a partial removable dental prosthesis (RDP). B, An additional rest (arrow) was included as a nonrigid connector for splinting the prostheses in the maxillary left quadrant. This rest is parallel to the others, and so it is available (if needed) for future support of a modified or new RDP. C, The lingual aspect of the premolar incorporates the appropriate survey contour (arrow) to accommodate such a prosthesis. D, The RDP in place. Note the third intracoronal rest (arrow). E and F, External and internal aspects of the RDP. This was cast in type IV gold, which allows the relatively easy addition of a new minor connector with conventional soldering techniques.
When tooth preparations are conservative, when margins are supragingival, and when complicated FDP designs are avoided, replacement dentistry can be performed in an orderly manner, as long as plaque control and follow-up care are maintained.
The key to successful fixed prosthodontic treatment planning lies in anticipating potential areas of future failure. Ideally, the design of a prosthesis should incorporate an escape mechanism to allow simple and convenient alteration to accommodate future treatment needs.
Neglect
An extensive fixed prosthesis that has been neglected is much more difficult to treat. Considerable expertise is needed to successfully perform the lengthy and demanding procedures. Specialized treatment is almost always necessary and usually includes controlling mobility of the abutment teeth, improving support for removable appliances in the edentulous area, and creating a more favorable load distribution.
TREATMENT PRESENTATIONS
Several treatment results are presented, including follow-up documentation as appropriate, in some cases over many years. The treatments demonstrate successful treatment approaches that are consistent with the principles discussed throughout this text.

Fig. 32-33 Simple cast restorations (Treatment I). A complete cast crown and inlay used to restore the first molars. A, Wax patterns. B, Castings seated and adjusted for clinical evaluation. C, Cemented restorations. D, This two-surface intracoronal cast restoration served for 66 years.

Fig. 32-34 Single cast restorations reestablish canine guidance and functional occlusion (Treatment II). A, Extensive anterior wear caused by prolonged parafunctional activity that resulted from malocclusion. B, Anterior pinledges are waxed concurrently with the molar castings. C, Anterior guidance and posterior occlusion are reestablished. D and E, Castings seated and adjusted and at clinical evaluation. F, A normal canine-to-canine relationship has been reestablished. G, Working-side excursion.

Fig. 32-35 Simple partial fixed dental prostheses (FDPs) (Treatment III). Long-term follow-up: These small FDPs remain serviceable after 7 and 13 years. A and B, Seven-year follow-up. C and D, Thirteen-year follow-up.
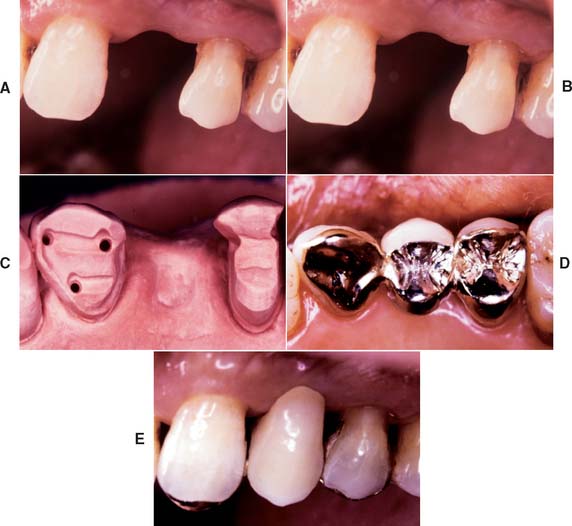
Fig. 32-36 Partial-coverage retainers used to support a partial fixed dental prosthesis (FDP) replacing the maxillary premolar (Treatment IV). A and B, Tooth preparations. C, Preparations on definitive cast. D and E, Occlusal and buccal views of cemented FDP.

Fig. 32-37 Pinledge splint (Treatment V). A and B, Periodontally involved anterior teeth prepared for pinledges. C and D, Completed restorations. Some metal is displayed as a result of the long clinical crown length and opened embrasures resulting from periodontal surgery. However, this treatment approach is preferred because it is much more conservative of tooth structure than is splinting with metal-ceramic crowns.
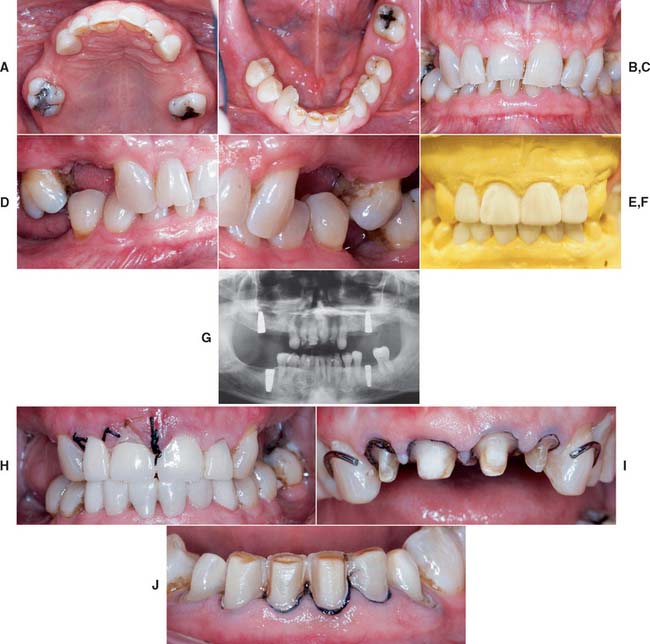

Fig. 32-38 Full-mouth rehabilitation with fixed, implant-supported, and removable partial prosthodontics (Treatment VI). Before treatment: Note the reverse smile line and discrepancy in the maxillary central incisor gingival tissue levels. The maxillary first molars had furcation involvement and poor prognosis as a result of periodontal bone loss. A and B, Occlusal views. C, Frontal view. D and E, Right and left views in maximum intercuspation. F, Diagnostic waxing. G, Dental implants were placed to restore the mandibular arch and provide retention and support for a maxillary partial removable dental prosthesis (RDP). H, The gingival tissue levels were corrected with periodontal surgery. I and J, Anterior teeth prepared for fixed restorations. After treatment: K and L, Occlusal views of maxillary arch with and without partial RDP. M, Occlusal view of restored mandibular arch. N and O, Right and left mirror views in maximum intercuspation. P, Frontal view.
(Courtesy of Dr. B. A. Purcell.)
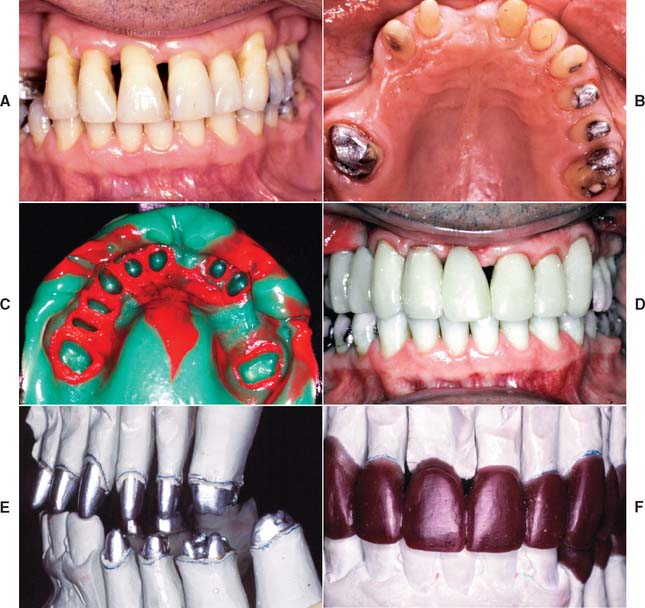
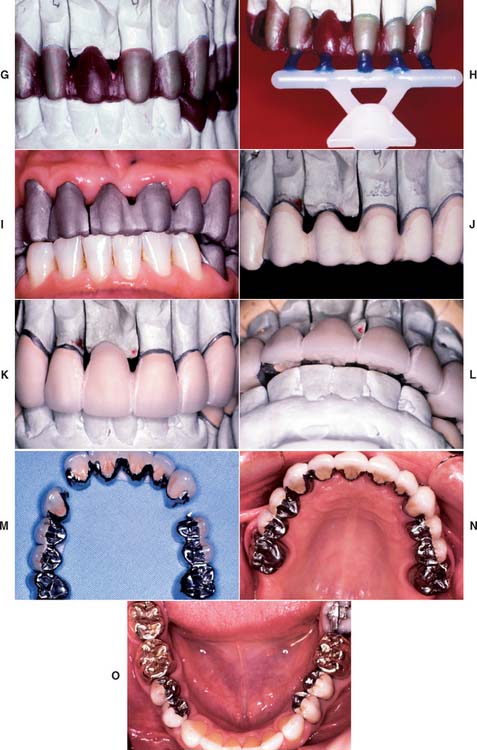
Fig. 32-39 Extensive fixed prosthodontics (Treatment VII). Teeth with advanced periodontal disease restored with fixed prosthodontics. A, Initial presentation. The patient required extraction of the right maxillary incisor and surgical correction of the periodontal defects. B, Maxillary teeth prepared for metal-ceramic restorations. C, Reversible hydrocolloid impression. D, Interim restorations. E, Definitive casts. F, Anatomic contour wax patterns. G, Patterns cut back for porcelain application. H, Sprued patterns. I, Metal framework evaluation. J, Opaque porcelain applied. K, Bisque porcelain. L, Centric contacts are on metal. M, Finished restorations before cementation. The extensive prosthesis is segmented with intracoronal rests. N and O, Cemented prostheses.
(Courtesy of Dr. M. T. Padilla.)
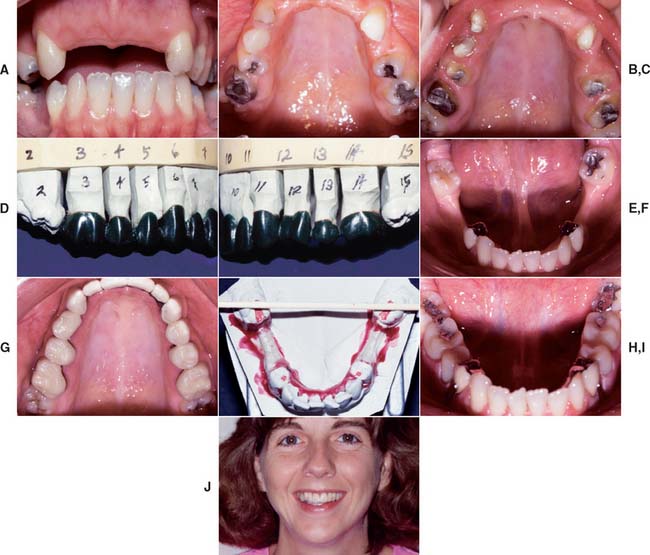
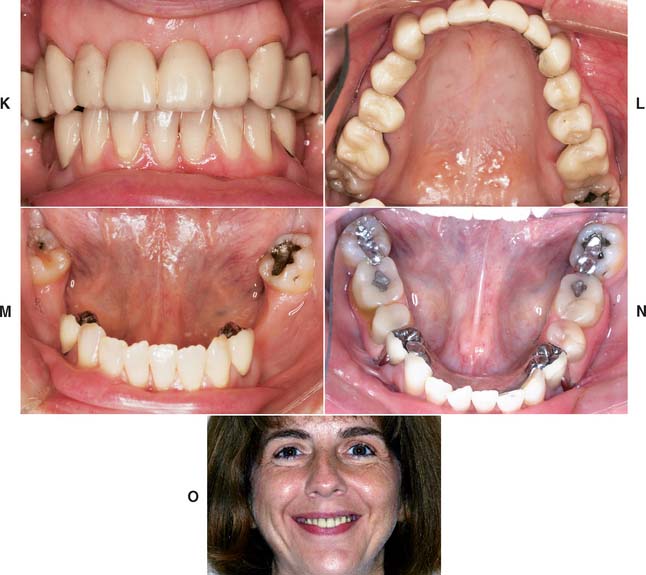
Fig. 32-40 Extensive fixed and removable prostheses (Treatment VIII). A and B, The patient presented with missing maxillary anterior teeth and mandibular posterior teeth. There was a significant slide from centric relation to maximum intercuspation. The patient was treated with a combination of fixed and removable prostheses. C, Maxillary teeth prepared and foundation restorations placed. D and E, Maxillary teeth waxed to anatomic contour. F and G, Completed fixed restorations. H, Definitive cast for mandibular partial removable dental prosthesis (RDP) framework before duplication. A rotational path of placement was used to engage mesial undercuts in second molars. I, Completed mandibular RDP. Amalgam stops were placed in the first molars to prevent premature wear of the denture teeth. J, Completed treatment. K to O, Appearance 13 years after treatment.
(Courtesy of Dr. J. A. Holloway.)

Fig. 32-41 Anticipation of future needs (Treatment IX). A and B, Pretreatment photographs. C to E, Buccal/labial view of bisque bake. F and G, Occlusal view before and at clinical evaluation. Note the location of the occlusal rests to anticipate various future partial removable dental prosthesis designs. An intracoronal rest (dovetail) was incorporated in the left lateral incisor. It is filled with composite resin, which is easily removed if the need arises. H, Completed treatment.


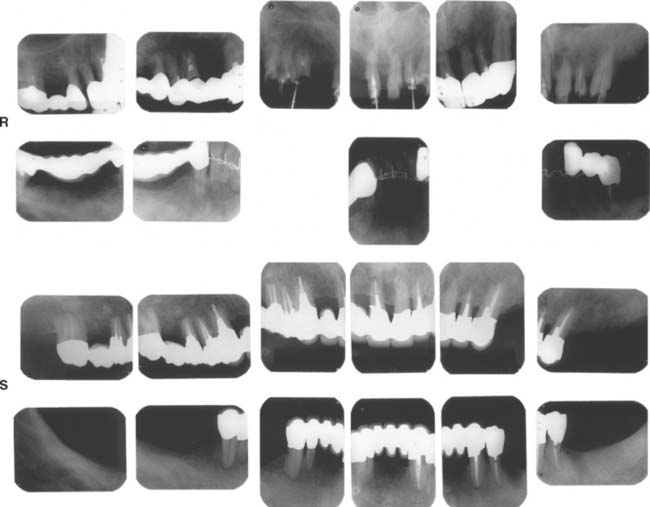
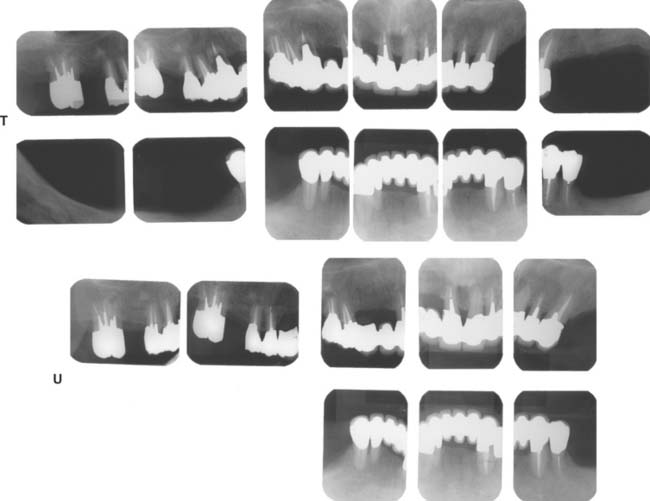
Fig. 32-42 This patient presented with multiple failing restorations and severely compromised function (Treatment X). A to E, Preoperative photographs. F to J, Posttreatment photographs. Where possible, I-bars were used to minimize clasp visibility. Also note the extensive use of metal occlusal surfaces. When prostheses are designed for dentitions with compromised crown/root ratios, precise adjustment of the occlusion and anterior guidance components is critical. K to Q, Seventeen-year follow-up photographs. Note that the maxillary canine was lost and the existing retainer was modified into a pontic through the addition of composite resin. Additional endodontic treatment was needed as time passed. R, Preoperative radiographs. S, Postoperative radiographs. T, Eight-year postoperative radiographs. U, Seventeen-year postoperative radiographs. A fixed dental prosthesis (FDP) was fabricated, replacing the missing tooth #3 with teeth #5, #4, and #2 as abutments. The teeth were prepared with minimal taper, and the castings exhibited good retention. After 10 years, the FDP failed when tooth #2 became dislodged, possibly as a result of the additional loading by the removable dental prosthesis (RDP). Tooth #2 and the pontic were removed, endodontic treatment was performed, a new crown was fabricated, and the #3 pontic was incorporated in a new RDP. Tooth #6 was lost as a result of internal resorption and caries. Initially, the tooth was discolored, but the lesion was inactive, and the attempt to save it failed after 8 years. Its guarded prognosis was discussed as a significant risk factor before treatment initiation. This suggests that teeth with a guarded prognosis can be maintained if attention is paid to the principles of casting adaptation and occlusion.

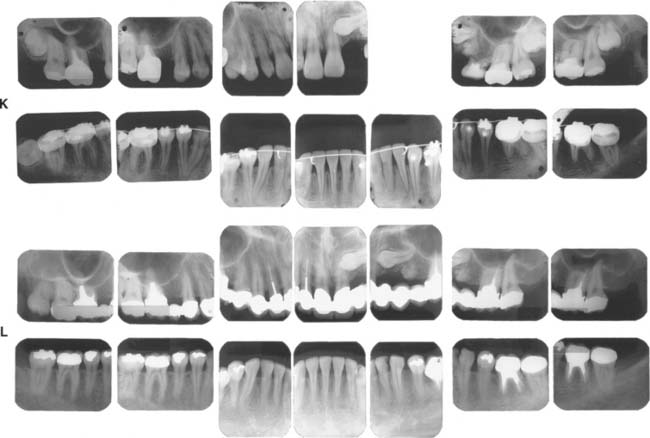
Fig. 32-43 Long-term follow-up after comprehensive treatment with fixed prostheses of the patient in Fig. 32-41 (Treatment XI). A to E, Preoperative photographs. F to J, Postoperative photographs. K, Preoperative radiographs. L, Fourteen-year postoperative radiographs. If the fixed prostheses have been designed carefully and the patient is cooperative and maintains excellent plaque control, fixed dental prostheses can withstand the test of time. Today, these prostheses continue to provide excellent esthetics and function after more than 16 years of service. Note that no intervention was done for the impacted canine. Initially, this patient presented with only posterior guidance on the left and right first molars. A gingival graft was performed on the left side before the fixed prosthodontic treatment. Fourteen years later, all teeth are stable without any clinically significant mobility, and the anterior guidance components exhibit no visible faceting. No significant change has occurred in bone levels, whereas apparent radiographic bone densities appear slightly increased. Meticulous attention to precise adjustment of the occlusion, especially the anterior guidance component, contributed to the long-term success of this treatment. On the 14-year postoperative radiographs, no signs of occlusal trauma are seen. Also, note that three endodontically treated molars have very large access cavities. Such teeth have a guarded prognosis and are prone to fracture, but no fractures have occurred. Again, this suggests the importance of precise and optimal load distribution at the time of initial treatment and during periodic follow-up appointments. This patient was recalled every 6 months.

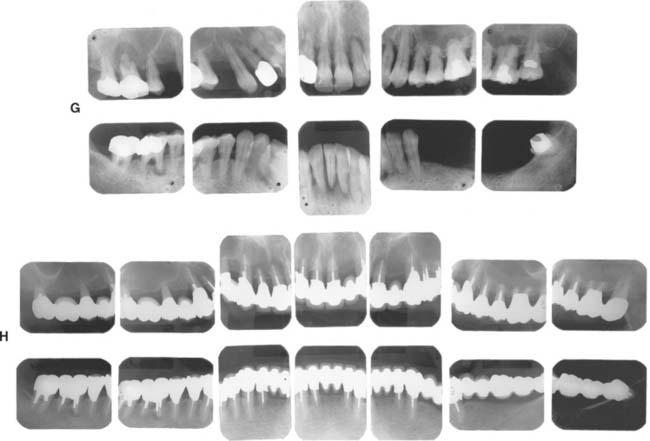
Fig. 32-44 Treatment of a severely periodontally compromised dentition (Treatment XII). A to C, Preoperative photographs. D to F, Fourteen-year postoperative photographs. In the initial discussion of an extensive treatment plan with a patient with a severely compromised dentition, the many risks and possibilities of failure must be fully understood by all parties. This extremely complex rehabilitation continues to serve well today. A meticulous design and frequent recall appointments, combined with outstanding home care, enables this patient to enjoy improved function 14 years later. Throughout the follow-up, the patient was seen at 1-month and periodic 3-month recall appointments, depending on pocket charting and patient motivation. Today, tooth #4 has no attached gingiva and little bone support, but no pocket formation. Initially, it was expected that this tooth would be the first to be lost. In conjunction with loss of tooth #1, this would have necessitated a partial removable dental prosthesis or implant-supported fixed dental prosthesis. Occlusal rests, undercuts, and guide planes had been incorporated in the initial prosthesis to anticipate such failure. After more than 14 years, the prostheses continue to serve satisfactorily. The anterior guidance component is starting to show some wear. Throughout the recall, wherever posterior tooth contact was observed in excursive movements, they were eliminated as part of ongoing occlusal adjustment. Meticulous management of load distribution has contributed to the long-term success of this very complex rehabilitation. G, Preoperative radiographs. H, Fourteen-year postoperative radiographs. This patient was referred initially for complete maxillary and mandibular denture fabrication. Before prosthodontic treatment, the periodontal condition was treated. Treatment included a modified Widman flap, performed throughout both arches. A root resection was done for tooth #14, and tooth #30 was hemisected, which resulted in two premolar-like restorations. Use of the severely tilted tooth #17 as a single abutment to support a very long span posed a substantial risk to the long-term success of this treatment, and the tooth’s future loss was anticipated in the design of the prostheses. Another risk was posed by the root structure of tooth #1, with a small, fused root. This tooth was lost after 14 years as a result of a periodontal defect that progressed along a vertical groove in the fused root.

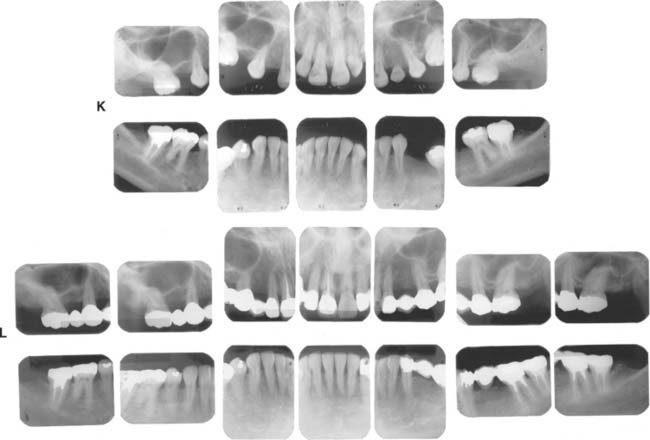
Fig. 32-45 Long-term evaluation (Treatment XIII). A to E, Preoperative photographs. F to J, Eighteen-year posttreatment photographs. Three simple fixed dental prostheses combining conventional and metal-ceramic prostheses with postsoldered connectors continue to serve 18 years after initial placement. Complications over the years included the reshaping of some restorations to correct occlusal discrepancies and the endodontic treatment of tooth #19 through the prosthesis (the access cavity was restored with amalgam). This patient presented with congenitally missing teeth #4 and #12. The maxillary canine was left in the premolar position for use as an abutment with posterior disocclusion resulting from guidance on the canine-shaped pontic. This is not ideal from the perspective of force distribution; however, the canine root successfully withstood the loading over time. Risk factors initially discussed with the patient included uncertainty regarding the effect of the crown/root ratios on the long-term prognosis. At the time of prosthetic treatment, more than 25 years ago, osseous integration was not the reliable treatment modality that it is today. The young woman declined a removable prosthesis as an alternative to fixed dental prostheses. A pinledge retainer was used on the small lateral incisor. Over time, not only was this esthetically effective, but it contributed to long-term maintenance of its periodontal health. Similarly, a pinledge was used on the left mandibular canine, a far more conservative option than a metal-ceramic restoration. If instead metal-ceramic retainers had been used, by now this likely would have resulted in additional treatment needs and possibly the loss of the lateral incisor. Teeth #18, #19, and #3 were treated endodontically; cast posts and cores were used. Also, note that tooth #8 has served well over time. The conservative access cavity was restored, and the favorable position in the arch results in favorable loading. Recall appointments for this patient were scheduled at 6-month intervals throughout the evaluation period. K, Preoperative radiographs. L, Eighteen-year postoperative radiographs.
SUMMARY
Well-organized and efficient postoperative care is the chief mechanism for ensuring optimal longevity and success in fixed prosthodontics. A restoration that is cemented, forgotten, and ignored is likely to fail, regardless of how skillfully it was designed and executed. Restored teeth require more assiduous plaque removal and maintenance than do healthy unrestored teeth, and, similarly, an FDP requires additional care and attention.
Common complications after completion of the active phase of treatment include caries, periodontal failure, endodontic failure, loose retainers, porcelain fracture, and root fracture.50,51 If possible, the dentist should anticipate the long-term prognosis and treatment needs of the patient and attempt to design the treatment plan accordingly. On occasion, FDPs can be designed so that future re-treatment can be anticipated and simplified. However, it is impossible, even for the most experienced and talented clinicians, to anticipate every contingency and complication. The patient must understand the limitations of fixed prosthodontics before treatment begins.
 GLOSSARY*
GLOSSARY*
adhesive failure \ăd-hē′siv,-ziv fāl′yur\ (1998): bond failure at an interface between two materials due to a tensile or shearing force—see COHESIVE FAILURE
car·ies n singular: a dental disease causing the destruction of enamel, dentin and/or cementum. The etiology is generally ascribed to acid-producing bacteria
occlusal adjustment \a-klōō′zal, -sal a-jŭst′mant\ 1: any change in the occlusion intended to alter the occluding relation 2: any alteration of the occluding surfaces of the teeth or restorations—see also OCCLUSAL RESHAPING
occlusal trauma \a-klōō′zal, -sal trou′ma, trô′-\: trauma to the periodontium from functional or parafunctional forces causing damage to the attachment apparatus of the periodontium by exceeding its adaptive and reparative capacities. It may be self-limiting or progressive—see PRIMARY O.T., SECONDARY O.T.
occlusion analysis \a-klōō′shun a-năl′ -ss\ obs: a systematic examination of the masticatory system with special consideration to the effect of tooth occlusion on the teeth and their related structures (GPT-4)
-ss\ obs: a systematic examination of the masticatory system with special consideration to the effect of tooth occlusion on the teeth and their related structures (GPT-4)
o·ver·clo·sure \ō′var-klō′zhar\ n: an occluding vertical dimension at a reduced interarch distance; an occluding vertical dimension that results in excessive interocclusal distance when the mandible is in the rest position; it results in a reduced interridge distance when the teeth are in contact
o·ver·den·ture \ō′var-d n′chur\ n: any removable dental prosthesis that covers and rests on one or more remaining natural teeth, the roots of natural teeth, and/or dental implants; a dental prosthesis that covers and is partially supported by natural teeth, natural tooth roots, and/or dental implants—called also overlay denture, overlay prosthesis, superimposed prosthesis
n′chur\ n: any removable dental prosthesis that covers and rests on one or more remaining natural teeth, the roots of natural teeth, and/or dental implants; a dental prosthesis that covers and is partially supported by natural teeth, natural tooth roots, and/or dental implants—called also overlay denture, overlay prosthesis, superimposed prosthesis
root \rōōt, r t\ n (bef. 12c): the portion of the tooth apical to the cementoenamel junction that is normally covered by cementum and is attached to the periodontal ligament and hence to the supporting bone
t\ n (bef. 12c): the portion of the tooth apical to the cementoenamel junction that is normally covered by cementum and is attached to the periodontal ligament and hence to the supporting bone
STUDY QUESTIONS
1 Tolboe H, et al. Influence of oral hygiene on the mucosal conditions beneath bridge pontics. Scand J Dent Res. 1987;95:475.
2 Tolboe H, et al. Influence of pontic material on alveolar mucosal conditions. Scand J Dent Res. 1988;96:442.
3 Ericson G, et al. Cross-sectional study of patients fitted with fixed partial dentures with special reference to the caries situation. Scand J Dent Res. 1990;98:8.
4 Akerboom HB, et al. Radiopacity of posterior composite resins, composite resin luting cements, and glass ionomer lining cements. J Prosthet Dent. 1993;70:351.
5 Matsumura H, et al. Radiopacity of dental cements. Am J Dent. 1993;6:43.
6 el-Mowafy OM, Benmergui C. Radiopacity of resin-based inlay luting cements. Oper Dent. 1994;19:11.
7 Gibson G. Identifying and treating xerostomia in restorative patients. J Esthet Dent. 1998;10:253.
8 Keene JJJr, et al. Antidepressant use in psychiatry and medicine: importance in dental practice. J Am Dent Assoc. 2003;134:71.
9 Walton JN, et al. A survey of crown and fixed partial denture failures: length of service and reasons for replacement. J Prosthet Dent. 1986;56:416.
10 Libby G, et al. Longevity of fixed partial dentures. J Prosthet Dent. 1997;78:127.
11 Sundh B, Odman P. A study of fixed prosthodontics performed at a university clinic 18 years after insertion. Int J Prosthodont. 1997;10:513.
12 Priest GF. Failure rates of restorations for single-tooth replacement. Int J Prosthodont. 1996;9:38.
13 Bauer JG, et al. The reliability of diagnosing root caries using oral examinations. J Dent Educ. 1988;52:622.
14 Silverstone LM. Remineralization phenomena. Caries Res. 1977;11(suppl 1):59.
15 Gordon SR. Older adults: demographics and need for quality care. J Prosthet Dent. 1989;61:737.
16 Hellyer PH, et al. Root caries in older people attending a general dental practice in East Sussex. Br Dent J. 1990;169:201.
17 Guivante-Nabet C, et al. Active and inactive caries lesions in a selected elderly institutionalised French population. Int Dent J. 1998;48:111.
18 Gustafsson BE, et al. The Vipeholm dental caries study: the effect of different levels of carbohydrate intake on caries activity in 436 individuals observed for 5 years. Acta Odontol Scand. 1954;11:232.
19 Fure S. Five-year incidence of caries, salivary and microbial conditions in 60-, 70- and 80-year-old Swedish individuals. Caries Res. 1998;32:166.
20 Winn DM, et al. Coronal and root caries in the dentition of adults in the United States, 1988-1991. J Dent Res. 1996;75(Spec. No.):642.
21 Reiker J, et al. A cross-sectional study into the prevalence of root caries in periodontal maintenance patients. J Clin Periodont. 1999;26:26.
22 Younger H, et al. Relationship among stimulated whole, glandular salivary flow rates, and root caries prevalence in an elderly population: a preliminary study. Spec Care Dentist. 1998;18:156.
23 Powell LV, et al. Factors associated with caries incidence in an elderly population. Community Dent Oral Epidemiol. 1998;26:170.
24 Sorensen JA. A rationale for comparison of plaque-retaining properties of crown systems. J Prosthet Dent. 1989;62:264.
25 Alexander AG. Periodontal aspects of conservative dentistry. Br Dent J. 1968;125:111.
26 Valderhaug J. Gingival reaction to fixed prostheses. J Dent Res. 1971;50:74.
27 Reichen-Graden S, Lang NP. Periodontal and pulpal conditions of abutment teeth. Status after four to eight years following the incorporation of fixed reconstructions. Schweiz Monatsschr Zahnmed. 1989;99:1381.
28 Wagman SS. The role of coronal contour in gingival health. J Prosthet Dent. 1977;37:280.
29 Mojon P, et al. Relationship between prosthodontic status, caries, and periodontal disease in a geriatric population. Int J Prosthodont. 1995;8:564.
30 Rantanen T. A control study of crowns and bridges on root canal filled teeth. Suom Hammaslaak Toim. 1970;66:275.
31 Abou-Rass M. The stressed pulp condition: an endodontic-restorative diagnostic concept. J Prosthet Dent. 1982;48:264.
32 Saunders WP, Saunders EM. Prevalence of periradicular periodontitis associated with crowned teeth in an adult Scottish subpopulation. Br Dent J. 1998;185:137.
33 Karlsson S. A clinical evaluation of fixed bridges, 10 years following insertion. J Oral Rehabil. 1986;13:423.
34 Eckerbom M, et al. Prevalence of apical periodontitis, crowned teeth and teeth with posts in a Swedish population. Endod Dent Traumatol. 1991;7:214.
35 Valderhaug J, et al. Assessment of the periapical and clinical status of crowned teeth over 25 years. J Dent. 1997;25:97.
36 Olin PS. Effect of prolonged ultrasonic instrumentation on the retention of cemented cast crowns. J Prosthet Dent. 1990;64:563.
37 Oliva RA. Clinical evaluation of a new crown and fixed partial denture remover. J Prosthet Dent. 1980;44:267.
38 Parreira FR, et al. Cast prosthesis removal using ultrasonics and a thermoplastic resin adhesive. J Endod. 1994;20:141.
39 Robbins JW. Intraoral repair of the fractured porcelain restoration. Oper Dent. 1998;23:203.
40 Chung KH, Hwang YC. Bonding strengths of porcelain repair systems with various surface treatments. J Prosthet Dent. 1997;78:267.
41 Kupiec KA, et al. Evaluation of porcelain surface treatments and agents for composite-to-porcelain repair. J Prosthet Dent. 1996;76:119.
42 Pameijer CH, et al. Repairing fractured porcelain: how surface preparation affects shear force resistance. J Am Dent Assoc. 1996;127:203.
43 Nowlin TP, et al. Evaluation of the bonding of three porcelain repair systems. J Prosthet Dent. 1981;46:516.
44 Gregory WA, et al. Composite resin repair of porcelain using different bonding materials. Oper Dent. 1988;13:114.
45 Barreto MT, Bottaro BF. A practical approach to porcelain repair. J Prosthet Dent. 1982;48:349.
46 Welsh SL, Schwab JT. Repair technique for porcelain-fused-to-metal restorations. J Prosthet Dent. 1977;38:61.
47 Miller TH, Thayer KE. Intraoral repair of fixed partial dentures. J Prosthet Dent. 1971;25:382.
48 Cardoso AC, Spinelli Filho P. Clinical and laboratory techniques for repair of fractured porcelain in fixed prostheses: a case report. Quintessence Int. 1994;25:835.
49 Westerman RD. A new paradigm for the construction and service of fixed prosthodontics. Dent Today. 1999;18:62.
50 Goodacre CJ, et al. Clinical complications in fixed prosthodontics. J Prosthet Dent. 2003;90:31.
51 Goodacre CJ, et al. Clinical complications with implants and implant prostheses. J Prosthet Dent. 2003;90:121.