Chapter 6 Ethical issues in health promotion
Overview
Health promotion involves working to improve people’s health. This requires a series of value judgements: about what better health means for the individual and society; and about whether, when and how to make a health promotion intervention. This book has used the perspectives of social science to help you explore your role and aims in health promotion. In this chapter we consider some of the prevailing problems for a health promoter from a philosophical perspective:
In particular, the chapter focuses on the limits to individual freedoms and how these are balanced against the health of the community. The chapter outlines the key ethical principles of beneficence (doing good), non-maleficence (doing no harm), justice, telling the truth and respect for people and their autonomy.
The need for a philosophy of health promotion
Debate in health promotion has centred on discussion of practice and some attempts to develop a theoretical base. However, according to Seedhouse (1988), there has been little discussion concerning the philosophy of health and yet it is an essential part of the way in which we understand the world.
Health promotion involves decisions and choices that affect other people which require judgements to be made about whether particular courses of action are right or wrong. There are no definite ways to behave. Health promotion is, according to Seedhouse (1988), ‘a moral endeavour’. Philosophical debate helps to clarify what it is that one believes in most and how one wants to run one’s life. It can and does help practitioners to reflect on the principles of practice, and thus to make practical judgements about whether to intervene and which strategies to adopt.
Philosophy has three main branches:
Morals refer to those beliefs about how people ‘ought’ to behave. These debates about right and wrong, good and bad, and duty are part of everyday discourse. Is it wrong to tell a lie? Is it justified to kill another? Is it our duty to look after ageing parents? Judgement about the morality of these actions may derive from our personal values and moral beliefs which derive from: religion, culture, ideology, professional codes of practice or social etiquette, the law or our life experience. The function of ethical theory is not to provide answers but to inform these judgements and help people work out whether certain courses of action are right or wrong, and whether one ought to take a certain action.
Western philosophy has been shaped by two theories of ethics – deontology and consequentialism. Deontology comes from the Greek word deonto meaning duty. Deontologists hold that we have a duty to act in accordance with certain universal moral rules. Consequential ethics are based on the premise that whether an action is right or wrong depends on its end result.
Duty and codes of practice
Deontologists hold that there are universal moral rules that it is our duty to follow. Many of the philosophical discussions about the nature of duty are based on the theories of Immanuel Kant. The essence of Kant’s thinking is encapsulated in the categorical imperative which can help us to discover, through reason, if a rule or moral principle exists (Kant 1909).
The major features of Kant’s theory are:
Deontological theories make decision-making apparently easy because, as long as we obey the rules, then we must be doing the right thing, regardless of the consequences.
 BOX 6.1
BOX 6.1Screening for antenatal disorders
This screening programme is in place to reduce the birth prevalence of a chromosomal disorder. The assumption underlying screening for conditions such as Down’s syndrome is that parents with a positive result will decide to terminate the pregnancy. Some positive-testing parents who do not choose termination may indirectly benefit from the test because they will be better able to adjust to the condition of their baby.
The Kantian objection is that the screened population becomes a mere means to achieve the public health goal of reducing chromosomal disorders in the population.
The ethical dilemma is pointed up, as Holland (2007, p. 182) puts it: ‘how feasible it is to use antenatal and screening and termination to combat a disability on the one hand, whilst maintaining a positive societal attitude towards extant disabled people on the other’.
 BOX 6.2
BOX 6.2This example centres on the duty to respect life and highlights some of the difficulties that canarise from carrying out this duty.
There is in medical care a commonly accepted doctrine of ‘acts and omissions’ which states that if a person fails to perform an action that would prevent negative consequences he or she is morally less blameworthy than if he or she performed an action that resulted in the same consequence.
In 2005 Dr Michael Irwin accompanied a terminally ill widow, Mrs May Murphy to Switzerland. She took a lethal dose of barbiturates while he was in the room. Assisted suicide, defined as doctors giving patients the means to kill themselves, is legal in Switzerland.
In 1992 medical staff stopped feeding Tony Bland, a young man crushed into a permanent vegetative state by the Hillsborough football disaster. This action was regarded as withholding life-saving treatment and morally acceptable.
Both acts had brought about the same consequence – the death of a patient. Is there a moral distinction, in your view, between killing and letting die? Must human life be preserved regardless of its quality?
Many health care workers have codes of practice which set out guidelines for the fulfilment of duties. For example, doctors take the Hippocratic oath which requires them as a first principle to avoid doing harm. The Nursing and Midwifery Council (2004) states the duty to respect life, the duty to care, and the duty to do no harm. Kant would have added ‘the duty to be truthful in all declarations is a sacred, unconditional command of reason, and not to be limited by any expediency’ (Kant 1909). The Society of Health Education and Promotion Specialists (SHEPS) includes these principles in its code of conduct:
But, as Sindall (2002) has argued, health promotion has not engaged in the kind of debate necessary to agree the principles, duties and obligations to which health promoters would need to agree to work in the field. Codes of conduct are simply devices offering a framework in which to practise. They do not help practitioners involved in the messy and complex everyday world of health care (Duncan 2008). For example, Article 3 of the nursing code (Nursing and Midwifery Council 2004) declares that the registered nurse, midwife or specialist community public health nurse must obtain consent before any treatment or care but the concept of informed consent is complex.
What do you understand by the concept of informed consent? What difficulties might there be in complying with this aspect of the code of practice?
Patients have different capacities to understand the nature of treatment or intervention. Patients may feel they will be judged or withheld from other interventions if they refuse. Consent is so obviously presumed in many cases, e.g. in the ‘invitation’ to screen or test, that refusal can seem impossible. Practitioners may also not communicate risk clearly such that patients are not fully informed when they consent.
Consequentialism and utilitarianism: the individual and the common good
The other classical school of ethics is known as consequentialism, of which utilitarianism is its best-known branch. Consequentialism differs from deontological theories because it is concerned with ends and not only means. The utilitarian principle is that a person should always act in such a way that will produce more good or benefits than disadvantages. Utilitarians such as John Stuart Mill and Jeremy Bentham aimed for the greatest good or pleasure for the greatest number of people. Utilitarians can thus respond to all moral dilemmas by reviewing the facts and weighing up the consequences of alternative courses of action. This can, of course, prove difficult. What exactly is a good end? How does one predict whether an outcome will be favourable? One of the main problems with utilitarianism is that, if the aim of all actions is to achieve the greatest good, does this justify harm or injustice to a few if society benefits? Smoking restrictions offer an example, where the health of society takes precedence over the right of the individual to smoke.
Health promotion raises many questions over its ends and means:
In Chapter 4 we saw that some writers have expressed concern over ‘social engineering’ in health promotion and think that government intervention has risked becoming government intrusion. Many interventions are justified as being in the interests of a ‘healthy society’, yet they may not have been requested or desired.
 BOX 6.4
BOX 6.4Some of these actions are intended to protect the population from possible harm. Others are promoting evidence-based health interventions, although their universal application can restrict the actions of others. For example, the use of public funds to support child care is not relevant for those without children.
Ethical principles
Ethical principles can help to clarify the decisions that have to be taken at work. Sometimes decisions may be guided by trying to do the best for the most number of people; at other times they may be guided by an overriding concern for people’s right to determine their own lives; and sometimes decisions may be guided by other ethical principles or a professional code of conduct.
There are four widely accepted ethical principles (Beauchamp & Childress 1995):
These principles provide a framework for consistent moral decision-making. However, situations rarely involve a single option, but can encapsulate increasingly complex and sometimes conflicting choices between these principles. Seedhouse (1988) has developed these principles into an ethical grid which helps provide health promoters with an easy-to-follow guide on which to ground their work on moral principles (Figure 6.1).
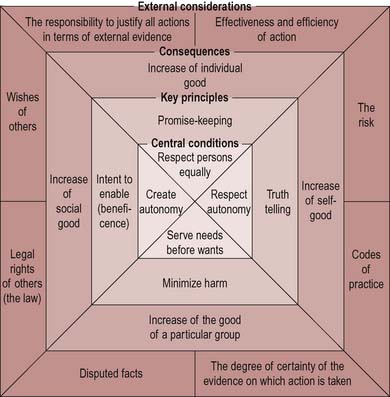
Figure 6.1 The ethical grid. The limit to the use of the grid is that it should be used honestly to seek to enable the enhancing potentials of people. From Seedhouse (1988).
The ethical grid
This provides a tool for practitioners, helping them to question basic principles and values, and be clear about what they mean and intend to do. The grid suggests ways in which practitioners can work through proposed actions. In any situation we should be asking ourselves:
Health promotion involves working to improve people’s health. This requires a series of value judgements about what health means for the individual and society and about whether, when and how to intervene.
In the USA a charity has offered young women addicted to heroin or crack cocaine and who have frequent pregnancies resulting in abortions, stillbirths or addicted babies a sum of money to be sterilized.
Use Seedhouse’s ethical grid illustrated in figure 6.1 to consider whether or not such action is morally justified.
You probably concluded that offering money as an inducement for sterilization is a coercive measure that does not respect the autonomy of the individual. Although it may give women greater control over their reproduction, having more money may result in increased drug use. Sterilization is an irreversible procedure about which women need to be fully and freely informed. This action is not, then, one which increases morality. It is a quick-fix solution which fails to deal with the root causes of drug addiction.
In the following scenarios, decide what ethical issues are involved and what action you would take and why.
Autonomy
Autonomy derives from the Greek word autonomous meaning self-rule. It refers to people’s capacity to choose freely for themselves and be able to direct their own life. Since people do not exist in isolation from each other, there will be restrictions on individual autonomy and autonomous people have a sense of responsibility: they cannot do entirely as they like. Thus, people do not have complete freedom of choice. The limits to an individual’s autonomy are when that individual’s action affects others in a negative way. Beyond this, traditional notions of liberal individualism see autonomy as essential to all human beings. It is only constrained by:
In addition, a person needs to be free from pressures such as fear and want, and have the personal and social circumstances to make any chosen action possible.
Autonomy must, therefore, be thought of not as an absolute but as attainable, to a greater or lesser extent. Not everyone has autonomy. When people’s capacity for rationality is affected in some way, decisions are often taken on their behalf on the basis that ‘they do not know what’s best for them’. Thus people with a learning disability or mental illness, young children and older people with mental confusion are often assumed to be unable to make a rational choice. It was not until the 20th century that women were deemed able to make a rational choice in a democratic vote. The Children Act of 1989 first recognized the rights and capacity of children to have a say in their care.
The rights of young people with severe learning disabilities to determine their sexual health is a contested area:
In recent years, the courts have ruled that a young woman with a learning disability should be sterilized to avoid the possible trauma of pregnancy and childbirth or abortion, for which it was considered she would not be prepared. It was also deemed in the best interests of a possible child who would not be able to be brought up by the young woman.
In these situations, what do we mean by autonomy? In part, we must mean respecting our clients as persons and helping them to cope with the consequences of their choices. Seedhouse (1988) makes a distinction between creating autonomy and respecting autonomy, which he regards as the central conditions when working for health.
Creating autonomy is making an effort to improve the quality of a person’s autonomy by trying to enhance what that person is able to do. In health promotion work, this is often called empowerment. It may involve information to enable clients to make choices or developing the clients’ skills in analysing situations and making decisions through increasing self-awareness and assertiveness. As we have stated elsewhere in this book, it is of prime importance in health promotion practice to recognize the limits to individual autonomy, and that social and economic circumstances can constrain individual health choices. Health promoters may claim they are creating autonomy by explaining the health hazards of smoking and thereby enabling individuals to make an informed choice to quit. Yet the autonomy of smokers may be compromised by addiction; their social circumstances in which cigarettes may serve as a ‘drug of solace’; as well as advertising, peer pressure and so on.
Respecting autonomy is respecting a person’s chosen direction, whether or not it is approved – for example, respecting a pregnant woman’s autonomy to smoke. Creating and respecting autonomy are closely related. People cannot express a free wish if they are not aware of the possibilities open to them and thus it may, in some circumstances, be ethically justifiable not to respond to a client’s expressed wishes but to attempt to open up other options.
Respecting clients’ autonomy can be difficult for health promoters. There is often a tendency to give advice, to exert pressure on them to make the ‘right’ decision or to persuade clients to change their behaviour. The challenge is to accept a role of partner and enabler rather than expert and controller. Ewles & Simnett (2003) identify three common ways in which health promoters hinder rather than respect their clients’ autonomy:
Think of some examples from your work when you have attempted to create autonomy in your clients so that they are able to express their wishes and wants.
At what point did you decide that the client is autonomous and to respect his or her wishes?
Chapter 10 explores a community development way of working which aims to empower people with regard to their own health agenda. It explores this dilemma of control and autonomy, and to what extent community development workers impose, collaborate with or genuinely facilitate local or community health needs. Chapter 9 looks at ways practitioners support individuals to change and whether such approaches are intent on empowering individuals or merely getting them to change.
Perhaps the starkest example of the ethical problems associated with respecting autonomy is that which confronts the health worker when a patient or client chooses not to follow advice or treatment which is known to be beneficial. It would seem straightforward that this is the client’s right and the health worker should respect the client’s autonomy in choosing such a decision, if the client is properly informed and understands any risks involved. However, the health worker is committed to ‘doing good’ and may feel it is his or her duty to persuade the client. This is particularly so if the client’s decision has implications for other people. Certainly this is paternalistic and putting the health worker’s need to do good above the client’s wish for autonomy. Yet, by not seeking to persuade or motivate the client, the practitioner may, by omission, be doing harm.
Respecting autonomy involves respecting another person’s rights and dignity such that a person reaches a maximum level of fulfilment as a human being. In the context of health promotion and health care this means that the relationship with patients or clients is based on a respect for them as people, and with individual rights. It follows that we must then see them as ‘whole people’ – with physical, social, emotional and spiritual needs – as fundamentally equal and also as unique individuals.
A patient who has undergone heart bypass surgery continues to smoke after the operation.
This extract suggests the following:
a doctor who takes seriously his self-imposed and professional obligation to benefit his patient ought to treat the patient if that is what the patient on reflection wants him to do, if some treatment is available which will provide net benefit to the patient … Of course that in no way prevents the doctor from advising that the most effective way of regaining and maintaining health is to alter one’s lifestyle in the relevant way. But coercion will generally be contraindicated by the requirement to respect people’s autonomy, and withdrawal of care from those who reject one’s advice will generally be contraindicated by a doctor’s personally and professionally undertaken duty of care, or obligation of beneficence (Gillon 1990, p. 34).
Rights in relation to health care are usually taken to include:
Health workers are often placed in the position of deciding whether to inform patients or relatives of an adverse prognosis. Although the patient’s right to information is usually considered paramount, there are occasions when the health worker’s duty of beneficence – to do good and avoid harm – may outweigh this right.
Beneficence and non-maleficence
Frankena (1963) suggests that beneficence means doing or promoting good as well as preventing, removing and avoiding evil or harm. The common good is often put before individual good. Wearing a seat belt may halve the risk of death to the driver but the odds that a particular individual will ever benefit are not great, as few people will be killed on the roads. Rose (1981) termed this the ‘prevention paradox’, according to which a measure that brings large benefits to the community offers little to each participating individual. The alternative to a mass approach is to focus on risk groups but this may stigmatize certain groups (Naidoo & Wills 2005).
In the UK the safety of the measles, mumps and rubella vaccine was questioned due to a putative link with autism and Crohn’s disease. It was followed by reports of a rise in measles cases because of the large numbers dissenting from the mass immunization programme.
This raises numerous issues central to the ethics of immunization:
Although it could be argued that people have a duty not to infect others and not to simply reap benefits of herd immunity, the risks of vaccination are contestable. Coercion therefore seems unjustified (Holland 2007).
In such circumstances the duty to care has to be extended to include the concept of informed consent. The individual must be informed, and understand the information and implications of any action which is taken to be beneficial. In this way the health worker can be said to be avoiding harm.
In the field of drug education, harm reduction has been adopted as a way of working. This is perhaps more realistic than the encompassing principle of doing no harm. The health care worker recognizes that clients may not wish to change their behaviour, and therefore seeks to encourage a safer way of life and reduce its harm. Drug workers may give clients clean needles and condoms, and provide information about emergency first aid to reduce the risks of HIV infection or accidents.
Should condoms be provided in prisons?
In England and Wales condoms can be prescribed by the prison medical officer where there is risk of HIV transmission. Condoms are not available in the prisons of Northern Island.
The example of screening illustrates the complexities of ethical decision-making and how attempting to follow the key ethical principles of doing good and avoiding harm is not a simple process. Most preventive services are offered with an explicit promise that they will do some good and an implicit understanding that they will do no harm. Yet what is the nature of that good? Screening, for example, only tells people that they are healthy at the present time. A negative result does not mean that illness will not develop the following year. Screening cannot promise a good outcome. Early detection can mean more effective or less radical treatment in some cases, but there may be no medical benefit and no treatment available. This used to be the case with HIV infection. However, anti retroviral drug therapies may prevent or delay illness in some people with HIV.
Consider these points in relation to a screening process with which you are familiar. Do you conclude that screening is of benefit, avoids harm and respects all persons equally?
Ethically, screening represents the tension between beneficence and non-maleficence. Poorly conducted screening can cause psychological harm from, for example, receiving false-positive results. Unfortunately, the pressure to ensure adequate take-up and to demonstrate success of a service means screening is often ‘sold’ to the public and consent is often presumed, making refusal seem possible.
Justice
Philosophers suggest three versions of justice:
Thus, justice requires that people are treated equally. But what is meant by equal? Does it mean according to equal need? Or according to merit? Or according to equal contribution? Or ensuring non-discriminatory practices?
For example, the equal distribution of resources can mean different things. It could mean that resources should be distributed equally in mathematical terms. Or should they be distributed according to how much was contributed – thus those that have and can put in most get out most? Or should we apply the Marxist adage ‘From each according to his ability, to each according to his needs’?
The National Health Service was established on the basis of free medical care to all those who need it. In an era of scarce resources, demand far exceeds supply. Need is an obvious criterion for distributing care but it is not sufficient. Tudor Hart, whose inverse-care law was described in Chapter 2, observed that those who needed health care most received least (Tudor Hart 1971). As we shall see in Chapter 18, although we may use some objective measurement for the assessment of individual health needs, such as the ability to self-care or to perform certain tasks, this does not overcome the subjective value judgement that is involved in making these decisions. In recent years, health economists have tried to establish some other sort of objective and measurable criteria to compare competing claims – possibly the relative financial costs of treatment or an assessment made on quality-adjusted life years (QALYs), which are described in Chapter 3.
Issues of social justice are glaringly evident in health promotion. We read earlier the evidence of wide differences in health status between different groups in society. Whilst health promoters may be unable to alter society’s inequities they may, nevertheless, be able to work on programmes which acknowledge that people’s abilities to achieve health differ, which avoid victim-blaming and which tackle discriminatory practices.
Being fair to everyone might seem to suggest adopting public health measures which iron out differences in resources, health care or environmental quality. Yet any kind of state intervention means addressing the issue of individual rights versus the common good. For instance, would it be just that top wage earners should pay 50% income tax to finance public spending on health and welfare? Chapter 7 examines different political perspectives on health promotion, and the fundamental differences between right and left of the political spectrum towards health and welfare.
Telling the truth
The process of health education and information-giving in health promotion also involves complex ethical decisions. Seedhouse (1988) identifies truth-telling and promise-keeping as principles which the health promoter should hold on to when deliberating a course of action. As we saw earlier, the individual’s right to information and the health promoter’s duty to tell the truth may conflict with the duty of beneficence.
Practitioners want people to make healthy choices. When convinced of the ‘good’ of an action, practitioners may seek to persuade, perhaps through raising clients’ anxiety or selecting the information or evidence. Yet ethical health promotion also includes a commitment to enhancing autonomy. As we saw in Chapter 4, the essential nature of health promotion is that it is based on a principle of voluntarism. It should not seek to coerce or persuade, but rather to facilitate an informed choice.
Is it ethical to carry out opportunistic health education in primary health care? Consider the example of a patient who goes to her GP with back pain. The doctor takes the opportunity for some health education, and takes the patient’s blood pressure and family history. The patient had neither sought this nor was she made aware beforehand of the implications if her blood pressure is found to be raised. The patient has not freely chosen to have her blood pressure checked in this way. Although she gave her consent, it might not be regarded as fully informed.
Campbell (1990) suggests that persuasion is acceptable only if a true picture of various aspects is presented. All education, he argues, involves some persuasion, and it is too simplistic to suggest that a desire to empower and create autonomy rules out persuasion. This means, however, that the health promoter must ensure that clients seek advice and help, and are not persuaded against their will. Yet many health promoters would argue that the only way to balance this need to empower people and facilitate healthier choices is to make this easier through policy decisions and frameworks (see Chapter 11). This takes us back to the argument that developing healthy public policy prioritizes the public good over individual freedom of choice and may not even be mandated by public opinion.
There may also be debate about the point at which enough information has been collected to justify legislative or coercive means of health promotion. Government bans on beef on the bone and unpasteurized green-top milk are examples where government action has been criticized for removing choice and leading to negative effects on employment and economic activity. Yet government inaction in the field of regulation and labelling of food has also been criticized for removing people’s right to make decisions based on information.
In the following chapter we will explore how information about what is deemed ‘healthy’ is often influenced by political decisions and vested interests.
There is also an increasing trend towards sponsorship for health promotion activities. This ranges from health research sponsored by a tobacco company trust to the sponsorship of health information by drug companies, sanitary wear manufacturers or a local health food shop.
Sponsorship may be acceptable when it comes from enterprises compatible with health promotion principles and practices, and when the acceptance of income does not divert the practitioners from meeting more demonstrable health needs.
Because the knowledge base of health promotion is changing, there are few areas where recommendations can be made on a factual basis. It is possible to think of numerous examples in recent years where information on the risks or benefits of certain behaviours has changed:
Conclusion
Do practitioners whose work involves decisions affecting the lives of others engage in a moral deliberation about the best course of action? In general, most combine features of utility and deontology. They respect autonomy, try to be honest and fair and avoid victim-blaming. At the same time they try to achieve the best overall solution to any given situation. Yet situations can involve complex layers of decision-making generating many ethical dilemmas. Screening, for example, a frequently unchallenged linchpin of preventive health promotion, raises key issues about its benefits for an individual versus the increase of the social good, as well as questions about the extent to which screening is honestly presented. Before we can make any sort of ethical judgement we need to be clear about the values and principles which underpin our actions. If we return to the questions asked earlier in this chapter, what do we mean by doing good and avoiding harm? At what point should we switch from creating autonomy to respecting autonomy? What do justice and equity mean in health promotion practice?
Tools to enable clear thinking around ethical issues, such as codes of practice or Seedhouse’s (1988) ethical grid, provide a way to clarify decision-making and make the process more transparent. But dilemmas remain, and following different principles (each of which is sound and desirable) may lead to contradictory courses of action. Whilst there may never be absolute answers in ethical decision-making, a way forward is to be clear about which principles and duties you value most, and to encourage an open debate about ethical principles and how these translate into health promotion practice.