Chapter 25 Infections of the central nervous and locomotor systems
Infections of the central nervous system
As the cerebrospinal fluid is devoid of effective antimicrobial defences, generalized infection rapidly sets in when pyogenic organisms enter the subarachnoid space and the cerebrospinal fluid. This may be caused by:
Meningitis
Inflammation of the meninges, the membranes that cover the brain and spinal cord, is classified according to the aetiological agent, as:
Bacterial meningitis
Bacterial meningitis is more severe than the viral type and remains a serious cause of morbidity and mortality despite antibiotic therapy. Prompt diagnosis is of the essence in preventing disabling sequelae of infection and death.
Clinical features
Symptoms include severe headache, fever, vomiting, photophobia and convulsions leading to drowsiness and unconsciousness. Signs are mainly those of meningeal irritation, i.e. neck and spinal stiffness, and Kernig’s sign (pain and resistance on extending the knee when the thigh is flexed). These cardinal signs and symptoms may be absent in neonatal meningitis and meningitis in the elderly and the immunocompromised. Sequelae include encephalopathy (altered cerebral function), cranial nerve palsies, cerebral abscess, obstructive hydrocephalus and subdural effusion of sterile or infected fluid.
Epidemiology, treatment and prevention
N. meningitidis (the meningococcus) is the main agent of meningitis in the UK and USA and most infections are caused by group B strains. The disease is common in children and young adults. Penicillin is the drug of choice: cefotaxime and chloramphenicol are alternatives. Haemophilus meningitis is mostly seen in children between 1 month and 4 years old and is treated with chloramphenicol or cefotaxime. Pneumococcal infection, common in older patients and those without a functioning spleen, is treated with penicillin. Tuberculous infection is managed by ‘triple therapy’, as described in Chapter 23.
Meningitis may spread quickly in close household contacts. Avoiding overcrowding in living and working conditions is helpful. Chemoprophylaxis with antibiotics (e.g. rifampicin) in meningococcal infection can eliminate the carrier state, which may develop in some.
Meningitis due to other organisms
Rarely, other organisms, such as Listeria monocytogenes, Leptospira interrogans and Cryptococcus neoformans (a fungus), may cause meningitis.
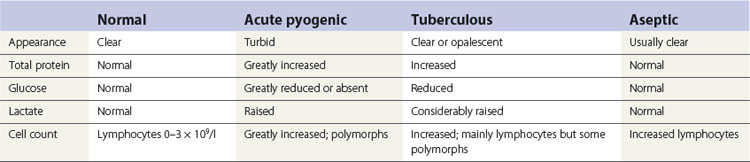
Laboratory diagnosis
Examination of the cerebrospinal fluid, usually obtained by a lumbar puncture, is essential. Changes that occur in the cerebrospinal fluid, depending on whether the aetiology is acute pyogenic, tuberculous or viral, dictate appropriate and timely therapy (Table 25.1). Cerebrospinal fluid should also be centrifuged and the deposit Gram-stained and cultured to isolate and identify the causative agent. Blood cultures are also useful in the diagnosis of bacterial meningitis.
Viral meningitis
Viral or aseptic meningitis can be caused by many agents, as shown in Table 25.2.
Table 25.2 Major causes of viral meningitis and/or encephalitis
Pathogenesis
The major routes of viral entry into the body are the respiratory and gastrointestinal tracts. From these portals, they spread to the central nervous system by direct migration via the olfactory nerves or indirectly via blood. Cells involved in viral spread include capillary endothelial cells, epithelial cells of the choroid plexus and infected leukocytes.
Encephalitis
Infection of the brain substance (as opposed to the meninges) is called encephalitis. This is a somewhat artificial division as patients often show signs and symptoms of meningitis and encephalitis at the same time.
Aetiology
The most frequently involved viruses are herpes simplex virus, mumps virus and arboviruses.
Poliomyelitis
Poliomyelitis is caused by poliovirus types 1–3, belonging to the Picornaviridae.
Pathogenesis
The portal of infection is the mouth, and the virus multiplies in the lymphoid tissue of the pharynx and the intestine. It then enters the blood stream and causes a viraemia, with resulting spread into the central nervous system, causing neurological disease. The disease is an influenza-like illness, with meningitis and encephalitis. In some, damage to the anterior horn cells of the spinal cord leads to respiratory failure (requiring artificial ventilation) or permanent lower motor neuron weakness and paralytic poliomyelitis.
Epidemiology and prevention
Although epidemics of poliomyelitis were common in the past, it is now rare in the West, owing to effective polio vaccine. However, the disease is still prevalent in developing countries, where universal vaccination programmes are difficult to implement, despite the goal of the World Health Organization to eradicate the disease by the year 2000. The polio vaccines are of two types: the killed (Salk) vaccine and the live attenuated (Sabin) vaccine (Chapter 37).
Cerebral abscess
Many bacteria may cause brain abscesses. These include streptococci (Streptococcus milleri and Streptococcus pneumoniae) enterococci (Enterococcus faecalis), staphylococci, anaerobic cocci and coliforms. The infections are mostly polymicrobial in nature (i.e. mixed infections).
Pathogenesis
The infective agent may reach the brain in the blood or by direct extension. In the latter case, a brain abscess may result as a direct extension of sinus infection caused by oral bacteria or, rarely, as a complication of acute or chronic dental infection. Infection may also follow traumatic injury to the maxillofacial region.
Tetanus
Tetanus is caused by infection with Clostridium tetani (drumstick bacillus).
Clinical features
After an incubation period of 5–15 days, the exotoxins produced by the organisms precipitate severe and painful muscle spasms:
Pathogenesis
Contamination of wounds with tetanus spores derived from dust, manured soil or rusty objects results in spore germination and release of the powerful exotoxins tetanospasmin and tetanolysin (see Chapters 5 and 13). Although the bacteria remain localized at the site of infection, the exotoxins are absorbed at the motor nerve endings and diffuse centripetally towards the anterior horn cells of the spinal cord, blocking the normal inhibitory impulses that control motor nerve function, with resultant sustained contraction of the muscles. Wounds of the face, neck and upper extremities are more dangerous than those of the lower extremities as they have a shorter incubation period and result in more severe disease.
Epidemiology
The main source of spores is animal faeces. The incidence is higher in the developing world because of lack of immunization and poor standards of wound care. Although tetanus is commonly associated with deep penetrating wounds, it can often result from superficial abrasions (e.g. thorn pricks). Neonatal tetanus due to infection of the umbilical stump is common in rural areas of developing countries.
Diagnosis
Diagnosis is mainly clinical as bacteriological confirmation frequently fails. Swab or exudate from the wound typically shows ‘drumstick bacilli’; biochemical identification and confirmation by mouse pathogenicity are described in Chapter 13.
Prophylaxis of wounded patients
Penicillin may be given as prophylaxis, not only to prevent tetanus but also to avoid pyogenic infection.
Booster doses of toxoid 10 years after the primary course and again 10 years later maintain a satisfactory level of protection. Any adult who has received five doses is likely to have lifelong immunity.
Infections of the locomotor system
The two major infections associated with the locomotor system (i.e. bones and joints) are acute septic arthritis and osteomyelitis.
Natural defences in the locomotor system include:
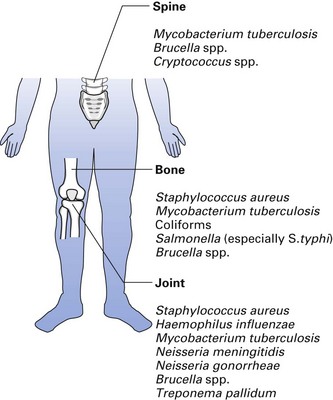
Important pathogens are listed in Figure 25.1.
Acute septic arthritis
Aetiology
Commonly associated bacteria are Staphylococcus aureus, H. influenzae, Streptococcus pneumoniae and other streptococci, Neisseria gonorrhoeae and non-sporing anaerobes such as Bacteroides spp. Other infrequent but notable agents are M. tuberculosis, Salmonella spp. and Brucella spp.
Clinical features
Limitation of movement with swelling, redness and severe pain are the cardinal symptoms; usually, only a single joint is involved. Crippling and permanent joint damage may result despite antibiotic therapy.
Epidemiology
Acute septic arthritis occurs most commonly in children. Sources of infection are many and include sepsis of the skin, nasopharynx, sinuses, lungs, peritoneum and genital tract. The source of infection of artificial joints could be the patient, the operating team or the theatre air.
Reactive arthritis
Reactive arthritis is the term given to acute arthritis affecting one or more joints; it develops 1–4 weeks after infection of the genital (post-sexual reactive arthritis) or gastrointestinal tract (post-dysenteric reactive arthritis). The causative agent in post-sexual reactive arthritis is Chlamydia trachomatis; almost all patients are men. Post-dysenteric reactive arthritis may follow infections with Salmonella, Shigella, Yersinia or Campylobacter.
Reactive arthritis should be differentiated from septic arthritis as it is not due to joint infection. It is thought to be mediated by immunological mechanisms, and there is an apparent genetic predisposition to the disease.
Osteomyelitis
Osteomyelitis can be divided into acute and chronic forms. Acute infection usually occurs in children under 10 years old, whereas the chronic variety is more common in adults.
Aetiology
Pathogenesis
Any septic lesion can be the source of the organism (e.g. a boil or pustule); spread to bone is usually haematogenous. Infection at all ages may be a result of major trauma (e.g. compound fracture) that exposes bone tissue to the environment.
Laboratory diagnosis
Diagnosis is by blood culture (a number of cultures may be required to isolate the infective agent(s), which circulate in the blood in very small numbers); culture of pus from the bony focus – pus may be obtained by needle aspiration or by open surgery; and by specimens from the related infective focus, e.g. ‘cold abscess’ pus in tuberculosis.
Treatment
Antibiotics alone are helpful if started early in the disease, by the parenteral route first and the oral route later. Penicillinase-resistant penicillin (such as flucloxacillin) should be given first if culture results are not available as Staphylococcus aureus is the predominant agent. Drugs that penetrate bone well (such as fusidic acid and clindamycin) are alternatives. Erythromycin is an alternative in patients who are hypersensitive to penicillin.
Surgery may be needed to drain pus and remove sequestra, if any.
Osteomyelitis of the jaws
Osteomyelitis of the jaws (see also Chapter 34) is uncommon owing to the relatively high vascularity of the jaws, especially the maxilla; therefore, the mandible is more commonly affected than the maxilla. The following predisposing conditions are noteworthy:
Key facts
Review questions (answers on p. 354)
Please indicate which answers are true, and which are false.