CHAPTER 19 Basic equine orthodontics and maxillofacial surgery
Basic equine orthodontics
Introduction
The prevention of and treatment for dental malocclusions is the field of dentistry known as orthodontics. Orthodontics, in its most basic form, is the controlled movement of teeth through alveolar bone. The purpose of equine orthodontics is to correct or prevent irregularities and malocclusions of the teeth and/or jaws through equilibration of dental crowns, application of dental appliances, exodontia, and/or surgery.
The orthodontic principles of tooth movement are at work on horses that develop abnormal wear patterns on exposed dental crowns. Dental elongations place stresses on the tooth that can result in abnormal movement. The general laws of biomechanics apply to movement of teeth. Alveolar bone is reabsorbed when the root and reserve crown maintain compressive force on the periodontal ligament. New alveolar bone is deposited when stretching forces act on bone. However, these laws are subject to numerous variations and exceptions when factors such as magnitude, direction, and duration of force are introduced.1 Dental cementum has the inherent tendency to resorb when pressure is applied to it but to a lesser degree than bone. Dental floating and equilibration are forms of orthodontic correction used in an attempt to reduce abnormal forces placed on teeth and thus improve occlusion. The application of orthodontic wire, springs, coils, arch bars, bands, brackets, incline planes, and elastics has been used in correcting common malocclusion problems of horses (Fig. 19.1).2–5

Fig. 19.1 (A) Orthodontic spring device used to spread 307 and 309 to allow room for an impacted 308 to erupt. (B) Intra-oral mirror used to visualize the orthodontic spring in the 308 position. (C) Lateral radiograph of impacted 308 with orthodontic spring in the dental space.
(Courtesy of B.W. Fletcher DVM.)
Extracting deciduous teeth to guide the eruption of the permanent teeth into a favorable occlusion has been referred to as preventative or interceptive orthodontics.6 Interceptive orthodontics, when wisely and judiciously applied to well-selected cases, can prevent dental malocclusions that cause functional problems with dental wear throughout the horse’s life (Fig. 19.2).

Fig. 19.2 Crowded lower incisor arch with retained deciduous teeth 701 and 801, causing displacement (labiocclusion) of permanent teeth 301 and 401. Following the principles of interceptive orthodontics, the deciduous teeth were removed, and the exposed mesial crown portions of 702 and 802 were filed, widening the space for 301 and 401 to migrate forward.
Many dental malocclusions involve an abnormal skeletal relationship between the upper and lower jaws. General form and capacity for growth of bone are inherited characteristics. A basic understanding of the growth of the upper and lower portions of the head is important in the diagnosis and treatment for many types of malocclusions7 (see Ch. 5).
Bone is plastic, and its form and capacity for growth are affected and modified by environmental forces and factors. A branch of orthodontic treatment, first referred to as biomechanical orthodontics, has developed over the past century. Applying the theories of bone plasticity traced back to Fouz and Wolff, several techniques have been used to correct dentofacial deformities and malocclusions in the horse using the principles of functional orthodontics.8 A more descriptive term, functional jaw orthopedics, was popularized by Karl Haupl, who refined the concepts and techniques used today in this branch of human dentistry.9 Pressure, whether functional or artificially created, affects bone growth. Cellular growth of bone is constant, occurring in the young horse from an increase in size and change in form or in the adult from the replacement of dead cells. Bone metabolism remains constant whether forces acting on the bone are normal or abnormal in direction or amount, but bone grows in the direction of least resistance. Forces of occlusion, when acting incorrectly, therefore, become factors of malocclusion.
Functional orthodontics is the use of appliances, devices, or techniques to modify the forces placed on the jaws of young, growing animals to encourage growth in a way that corrects or at least limits the extent of malocclusion when the animal reaches adulthood. Reduction of hooks and elongated teeth that interfere with normal jaw growth is the simplest application of functional orthodontics in horses. Both fixed and removable appliances have been used in foals, with mixed results, in an attempt to modify jaw growth and the spatial relationship between the dental arches (Figs 19.3 & 19.4).

Fig. 19.3 Removable functional orthodontic device in the mouth of a 5-month-old foal with a parrot-mouth deformity. This device is used to improve the dental alignment and encourage growth of the lower jaw. The device must be worn 16 hours daily and requires intensive nutritional management and husbandry of the foal for a successful outcome.

Fig. 19.4 Removable functional orthodontic mouthpiece on a 10-month-old gelding. This device incorporated a metal incline plane and a restrictive band labial to the upper incisors. This type of device works well, but owner compliance with long term care, is a problem.
Surgical correction of dental malocclusion and dentofacial deformities in the horse has had limited application. The most severe types of deformities, such as wry nose, have been corrected successfully in a small number of horses by following the principles of orthognathic surgery.10–13 Osteodistration surgical techniques have been employed to correct both wry nose and parrot mouth.14
Malocclusion can be categorized according to three etiological types:
Most horses with reasonable dentofacial alignment and occlusion and normal jaw function, should be considered to have normal occlusion. Although a very small abnormality in occlusal contact can affect dental wear, its impact on function cannot always be predicted by its morphology. Understanding the concepts of normal occlusion is fundamental to orthodontic diagnosis. (See Ch. 6, Dental physiology.)
The equine veterinary literature has given little attention to any type of dental malocclusion with the exception of parrot mouth. Although parrot mouth is probably the most common malocclusion of the incisors, many other types of dental malocclusions of the horse are more commonly encountered. Many types of malocclusion occur in horses.15 Colyer (1935) and Joest (1970) described many variations seen in equine teeth that lead to various types of dental malocclusion.16,17 Hypsodont teeth that are not properly aligned in the dental arcade suffer from severe abnormalities of wear. Abnormal wear has been shown to be the leading cause of dental disease and to adversely affect proper mastication.18
Surveys of equine dental patients have shown a high percentage of horses with significant dental malocclusions.15,19–22 Many of these malocclusions were severe enough to cause clinical problems, and a certain percentage of affected horses were classified as having a handicapping unsoundness.15 Treatment of horses with a dental malocclusion has been aimed at correcting dental overgrowth and managing periodontal disease.18,21,23,24 Orthodontic techniques have been introduced by equine practitioners to correct some of the more severe dental malocclusions.25,26 Dentofacial deformities, such as wry nose, parrot mouth, and monkey mouth, involve both the dental complex and the facial skeleton.
The genetic and functional environment work closely to determine the growth of all bones.27,28 The genetic factors that are at play and the veterinary literature pertaining to craniofacial deformity in domestic animals have been reviewed.29 The intrauterine environment has a known effect on facial growth and development. Intrauterine molding occurs when growth of the fetus is greater than that of the uterus, causing pressure from the uterus to distort the developing face. Intrauterine molding has been documented to occur in human beings and may be the cause of some facial and skeletal limb deformities seen in foals.30,31 Postnatal environmental factors affecting morphology include all non-genetic influences brought to bear on the developing individual. These include the environmental effects of muscle function and neuromuscular adaptation.32,33 Force placed on the teeth and jaws of the growing horse from abnormal wear of the exposed dental crowns is another factor to consider.
The scientific basis of environmental causes of malocclusion rests primarily on findings of experiments performed on animals.27 Under certain experimental conditions, growth can be extensively stimulated or stunted. The duration of pressure has a greater effect on growth than does the magnitude. Environmental factors that are recognized as leading to dentofacial abnormalities include:
• habits of long duration, such as sucking
• posture of the head, mandible, tongue, and lip because posture determines the resting pressure on soft-tissue
• eruption of the tooth and wear of the crown
• trauma, either osseous, soft tissue, articular, or dental.
The current theory for explaining growth of the craniofacial bones states that growth of the face occurs in response to functional needs and is mediated by the soft tissue in which the jaw is embedded.34 That is, the soft tissues grow, and both the bone and cartilage follow this growth.
Function plays an important role in normal growth of the jaw and is closely related to inherited patterns of growth. Perturbation of growth of the jaw can be induced by trauma to the soft tissues.27 In response to the disturbance of optimal occlusal relationships, growth of the jaw can be modified by a new functional environment. To modify inherited growth of the jaw of human beings, the functional disturbance must be of sufficient magnitude and duration (e.g., more than 6 hours per day for thumb-sucking by children).9 Deviation of the mandible to one side causing dental malocclusion is common in tethered pigs and is probably due to the pig pulling on its tether in one direction to reach food and water35 (Fig. 19.5).
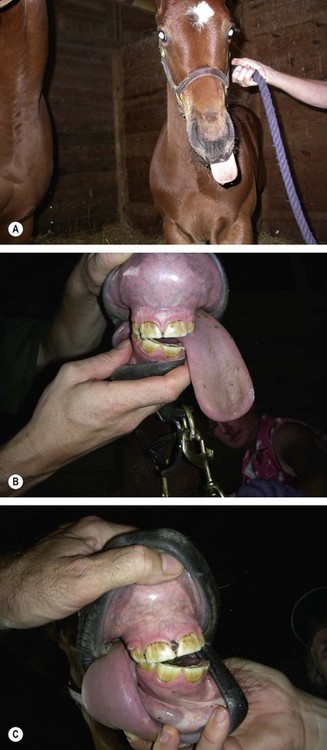
Fig. 19.5 (A) Foal developed unilateral hypoglossal nerve paralysis 24 hours after birth. The tongue can be seen protruding out of the left side of the mouth. (B) Same foal at 5 months of age. The tongue protrudes from the left side of the mouth except when it is stimulated. (C) The incisor teeth no longer meet on the left side due to ventral deviation of the rostral mandible from constant tongue pressure. This foal regained full function of the tongue by 10 months of age, but retained a diagonal incisor arcade.
Epidemiological studies are needed to establish breed or family predisposition to malocclusion. The classification system of malocclusion (i.e., modified angle) presently being used in human and small animal dentistry is not well adapted for use in the horse.6,36,37 Such a classification system of malocclusion does not exist for horses even though we use the MAL Class 1–3 system adapted by the AVDC.38 A well-designed system and its standardized use by a broad base of well-informed observers would be helpful in acquiring meaningful information about the effect of treatment in horses suffering from dental malocclusion. Additionally, cephalometric measurements and studies of jaw interrelation during craniofacial growth in the horse are essential for orthodontic therapy of horses to progress.
Sequelae of malocclusion
Malocclusion of the continually erupting and wearing hypsodont teeth of horses leads to abnormal wear patterns of the exposed dental crowns. Mechanical forces placed on teeth that are wearing abnormally can cause teeth to move within their alveolus. The teeth may tip, rotate, or shift, depending on the angle of force applied, leading to formation of diastemata (i.e., periodontal pocketing), the leading cause of periodontal disease.39,40 Most malocclusions cause teeth to wear in such a fashion that abnormal forces are applied to the teeth and jaws, exacerbating malocclusion. These abnormally worn teeth alter the masticatory pattern of some horses. They can also lead to secondary abnormalities of wear, such as alteration of the angle of the molar tables and inadequate wear of the buccal edges of the upper arcades and lingual edges of the lower arcades. The most severe form of this type of altered wear pattern is referred to as shear mouth.
Examples of altered wear causing tooth movement
Long enamel points and exaggerated transverse ridges may form due to malalignment of the upper and lower jaws. Exaggerated transverse ridges wedge between the teeth in the opposite arcade, forcing the teeth apart to create diastemata into which food becomes packed. Misplaced teeth develop abnormal wear of their occlusal surface with the unopposed portion of the crown becoming protuberant and developing an excessive angle. Mechanical forces placed on the protuberant crown force the tooth further out of alignment and can cause tipping or increased malalignment of the crown, which leads to periodontal packing of feed around the displaced crown. The tooth in the opposing arcade does not wear normally and may become protuberant or develop excessive enamel points or ridges that mirror the defect in the opposite arcade.
A missing or displaced tooth in one dental arcade leads to abnormal wear of the opposing teeth. The mesial and distal teeth in the same arcade tend to drift into the space that is unoccupied. This abnormal interproximal drifting can open spaces between adjacent teeth in the same dental arch, leading to formation of diastemata and periodontal pocketing between teeth and inspiring sequential drifting.41,42 This is not a consistent feature, and sometimes all the teeth in the dental arch move simultaneously to close the gap. This closure shortens the dental arcade and predisposes dentition to abnormal patterns of wear (e.g., hooks) on the ends of the opposite arcade. Some drifted teeth become angled medially or laterally so that the side of the crown develops occlusal wear. These angled teeth can have a smooth occlusal surface and excessive attrition of the crown, often associated with a step or wave in the opposing arcade.
Formation of a hook on the rostral aspect of the first cheek tooth (Triadan 06) or caudal aspect of the last cheek tooth (Triadan 11) places force on the crown of the tooth with the protuberance, forcing that tooth away from the rest of the arcade, resulting in a diastema. Packing of feed into the diastema leads to periodontal disease, which if left uncontrolled, may lead to formation of an abscess, loosening of the tooth, and eventually expulsion of the tooth (Fig. 19.6). A rostral or caudal hook can also result in mechanical forces applied to the jaw that affect growth, mastication, shedding of deciduous teeth, head carriage, and function of the temporomandibular joint. As the protuberant portion of the crown at the end of the dental arcade becomes more prominent, it tends to limit rostrocaudal motion of the jaw and place mechanical forces on both the upper and lower jaws. A hook on the first upper or lower cheek tooth of the growing foal works mechanically to restrict the growth of the shorter jaw. In the adolescent horse with mixed dentition, mechanical forces placed on the jaws and teeth from hooks inhibit growth of the shorter jaw and compress the crowns of the deciduous teeth, limiting the space for the deciduous teeth to shed and predisposing erupting permanent teeth to impaction. In the adult horse, hook formation can lead to several pathological processes depending on the size, shape and position of the hook and the demands for performance placed on the horse.

Fig. 19.6 Prominent hooks on 106 and 206 due to malocclusion of the upper and lower dental arcades. The rostral pressure placed on the 106 has moved it forward causing a space or diastema between 106 and 107 (arrow). This condition can lead to severe periodontal disease and eventual tooth loss.
The position of the jaw changes slightly as the horse moves its head up and down. With the head elevated, the lower jaw retracts caudally in relation to the upper jaw. This can be demonstrated by elevating the head high in the air and noticing the occlusion of the incisor teeth. The cheek tooth arcades also shift with head position. Some clinicians speculate that this positional shifting is the reason that horses that eat from an elevated hay rack or net have a higher incidence of hooks on the rostral aspect of the 06s than do horses that eat in the normal position off the ground.
As a horse flexes its neck, the lower jaw tends to move forward in relation to the upper jaw.43 This becomes important when dealing with horses that are asked to perform with the neck flexed in collection, such as dressage horses, gaited horses, or harness horses worked in an overcheck with their necks forced into flexion. Hooks on the rostral aspect of the upper 06s or caudal aspect of the lower 11s inhibit the rostral motion of the lower jaw when the horse’s mouth is closed. Some horses tend to open their mouths when collected, but often, trainers use various types of nosebands to force the mouth closed, thus preventing relief from the forces placed on the jaws and limiting the amount of flexion the horse can exhibit. Secondary problems, such as soreness in one or both temporomandibular regions or in the muscles of the neck or back, can be associated with the horse’s inability to freely move its jaw rostrally and caudally.
Documentation of malocclusion and craniofacial deformities
The clinician should document the history and clinical findings of all horses that may require any type of orthodontic treatment. A complete history, including the horse’s pedigree and an oral examination of its parents, is helpful in counseling the client about the heritability of the malocclusion. Historical information also allows the clinician to determine whether the condition was noticed at birth or soon after and if it is becoming progressively worse as the horse grows. The proposed use of the horse and knowledge of the rules of its breed’s registry are necessary to make ethical decisions regarding treatment of the horse when the deformity may have a hereditary component.
The clinical assessment should begin with a general physical examination of the horse and a complete, detailed, oral examination. Photographs and skull measurements are useful in monitoring clinical progress. Radiographic evaluation of the skull sometimes allows for more precise assessment of the problem and is another source of permanent, measurable documentation for monitoring improvement. Dental impressions and stone castings are helpful in the documentation of deformities as well as in planning treatment. Stone castings can also be used in the fabrication and fitting of removable or fixed dental appliances (see Ch. 21). Bite impressions using a sheet of base plate wax allow for proper alignment of upper and lower stone models and for following progress of treatment.6
Parrot mouth
An overjet of the incisor teeth is seen in most mammals, including man. This condition is abnormal in the horse and commonly referred to as parrot mouth, brachygnathism, overshot maxilla, or buck tooth, but officially is classified as a type 2 malocclusion (MAL2). When this malocclusion is slight, the labial aspect of the lower incisors rests on the lingual aspect of the uppers. When the condition is more severe, the incisors are completely out of occlusion, and the premaxillae tend to be deviated downward causing the lower incisors to rest on the hard palate caudal to the upper incisors. The parrot mouth syndrome in horses can involve the incisor portion of the dentition alone, or it can occur in combination with varying degrees of malocclusion of the upper and lower cheek teeth. The mismatch in length of the upper and lower jaws can be either from brachygnathism of the mandible or from prognathism of the maxillae and premaxillae.17
Mandibular brachygnathism has been reported to occur with other types of congenital deformity involving the musculoskeletal system.44,45 Without cephalometric norms, determining whether an affected horse has a short lower jaw or a long upper jaw is impossible. Some observations of horses with parrot mouth show that the lower jaw is shorter (by 1.5–9.3 %), while others show that the upper jaw is longer (by 11.15–18.1 %).17 Some observers conclude that the lower jaw of some horses with parrot mouth is underdeveloped.16,46 It is not unusual for the upper canines of adult male horses affected with severe parrot mouth to be positioned rostral to the lower canines.
Cattle inspected for breeding soundness show an incidence of parrot mouth ranging from 2–13 %. This percentage is similar to the 2–5 % incidence of parrot mouth reported in several equine studies.15,47 The degree to which this condition is expressed at birth, and the progression of the condition throughout growth and development of the horse have not been scientifically documented. The parrot mouth condition can be acquired by avulsion injury to the incisor teeth or premaxillae, compression fracture of the mandible, or illness immediately prior to a growth spurt.48,49
Equine parrot mouth is most often a result of breeding two horses with normal dental occlusion but extremely different head types. The degree of malocclusion seems to depend on many factors. Some horses are only affected in the region of the cheek teeth, some are affected only in the region of the incisors, and some are affected in both areas. Because horses have hypsodont teeth that depend on normal occlusal contact for wear, horses suffering from parrot mouth are more seriously affected by the condition at all stages in life than are similarly affected members of other species with brachydont teeth.
Few foals are born with the full expression of parrot mouth (Fig. 19.7). Foals born with a slight incisor overjet (i.e., upper incisor arcade labial to the lower incisor arcade) soon develop an overbite (i.e., the occlusal surface of the upper incisor arcade is dropped ventral to the occlusal surface of the lower incisor arcade). As the upper incisors elongate, the palate and incisive bones are pulled downward by gravity, causing the lower incisors to become trapped as they begin to contact the palate behind the upper incisors (Fig. 19.8). This places caudal pressure on the mandible, inhibiting its growth and creating a cascade of events that worsen the deformity. As the growth of the lower jaw is stunted, the cheek teeth malocclusion worsens, causing hooks to form on the rostral aspect of the upper first cheek teeth (Triadan 506 and 606). The unopposed incisor teeth continue to erupt and elongate. The elongated, unopposed lower incisors trapped between the wider, upper incisor arcade interfere with the normal masticatory cycle and limit free lateral motion of the jaw, leading to more abnormal wear of the cheek teeth.
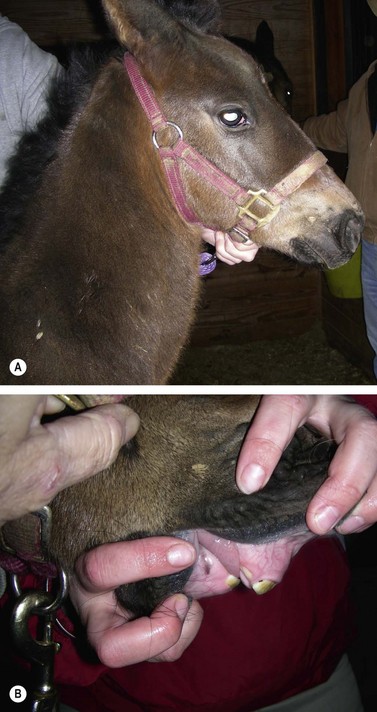
Fig. 19.7 (A) Lateral view of newborn foal with an incisor overjet (parrot mouth). (B) Intra-oral view of foal showing incisor overjet. Only the central deciduous incisors have erupted.
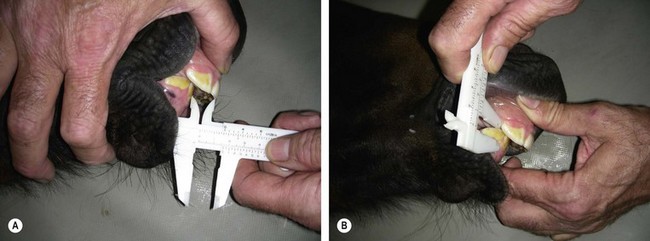
Fig. 19.8 (A) Measuring a parrot-mouth foal’s overjet in millimeters. (B) Measuring the overbite in millimeters.
When advising an owner about managing a horse with parrot mouth, one should keep in mind that the mode of inheritance of malocclusion is not clear. Parrot mouth is a complex conformational trait and is the outcome of multiple genes (polygenetic). Each breeding horse has a different propensity to pass the deformity on to its offspring. Breeding a horse that has a congenital defect, or breeding a horse that has previously produced offspring with a congenital defect is risky. The breeder’s long-term goals and philosophy should dictate breeding decisions. One should consider the horse’s good traits and the seriousness of the defect. Breeding horses with any type of congenital defect probably increases the incidence of that defect in the breeding population and may eventually lead to an intolerable concentration of affected horses in the gene pool. An extreme approach would be to neuter horses with congenital defects and to remove their sires and dams from the breeding population. Although this would prevent horses with a congenital defect from passing it on, it would also prevent them from reproducing their good conformational and behavioral traits, and ability to perform. One good strategy would be to not re-mate two horses that have previously produced defective offspring. Another approach would be to re-mate these horses but to retain in the breeding program only offspring that do not exhibit the defect. A good breeding practice is to mate horses with similar virtues but different faults.
Orthodontic management of a horse with parrot mouth should follow four basic principles:
1. abnormal wear of the teeth should be prevented or reduced
2. downward, gravitational drift of the premaxillae and upper incisor teeth should be prevented or corrected
3. rostral growth of the maxillae and premaxillae should be inhibited, and
The most important management tool used to correct parrot mouth is to reduce or prevent abnormal dental wear because abnormal dental wear patterns inhibit rostral and lateral movement and growth of the mandible. Rostral hooks on the upper 06s and caudal ramps or hooks on the last lower cheek teeth (08s, 09, 10s, or 11s, depending on the horse’s age) should be reduced. Excessive transverse ridges and enamel points on the cheek teeth should be reduced, and vaulted ceiling of occlusion corrected. Incisors excessively long from lack of wear should be reduced to bring the lower incisors out of contact with the soft tissues of the palate and to allow free lateral motion of the mandible. Care must be taken to not expose pulp chambers or to damage teeth when reducing crowns.
Foals with minor overjet (i.e., less than 5 mm) and with no overbite or malocclusion of the cheek teeth benefit from wiring of the upper teeth.25,26 This technique is used to inhibit rostral growth of the upper jaw from the second cheek tooth rostrally while allowing the growth of the mandible to proceed unimpeded. This wiring technique used alone is biomechanically unsound for use in horses with overbite or malocclusion of the cheek teeth.
Horses with a more severe malocclusion of the incisors (i.e., overbite) have been improved or corrected by applying a functional, orthodontic device early in their life, when they are in a rapid stage of growth.4 Orthognathic surgery and osteodistraction of a few foals has been attempted.14 Foals born with no contact between the upper and lower incisor teeth have an incisor overjet but no overbite, but within 3–6 months, gravity and soft-tissue tension on the upper lip cause the premaxillae and incisive bones to tip downward. This downward curve is evident during oral examination as a bow in the palate midway between the cheek teeth and the incisors. This downward movement of the upper incisors, in combination with lack of attrition or wear, leads to an overbite. Removable or fixed, functional, orthodontic devices combined with retention wires can be used to correct the overbite and allow free movement and rostral growth of the mandible.
Tension band wires have been used to inhibit rostral growth of the upper jaw of foals less than 6 months old that have sufficient potential for growth of the lower jaw to correct the deformity. Stainless steel wire (18- to 20-gauge, AISI 316L) can be used as a tension band device. A wire placed caudal to each second upper cheek tooth and brought rostrally around the upper incisors inhibits growth of this portion of the upper jaw. The lower jaw continues to grow normally, correcting the overjet.
If no portion of the upper and lower incisor arcades is in contact, a combination of tension band wires and a functional orthodontic device is used. Such a device in the most simple form consists of a removable plate, attached to a bit, that extends rostrally between the incisor arcades. When the mouth is closed, the plate places upward pressure on the upper incisors discouraging their ventral drift. A removable orthodontic device can be applied with the foal standing and unsedated. Because the device must be worn 16 hours per day to be effective, owner compliance is the most common problem associated with the use of the removable appliance, and compliance of the foal is the second limiting factor. Without an educated, enthusiastic, and committed owner and/or groom, the use of a removable appliance is doomed to failure.
A more sophisticated, fixed acrylic appliance can be fashioned to fit in the roof of the mouth. Acrylic is molded on a plaster model of the upper jaw or fashioned on the anesthetized foal in dorsal recumbency. A metal inclined plane can be incorporated in this device to place rostral force on the lower jaw when the mouth is closed. Application of these devices cannot be ‘cook-booked’ because each case presents a slightly different set of anatomical and biomechanical situations that requires detailed evaluation and careful planning.5
The primary advantage of a fixed dental appliance is that it can be permanently attached in the mouth, making compliance by the owner and by the foal less of a factor in success of treatment. To apply a fixed appliance, however, the foal must be anesthetized, and special equipment is required. Because foals grow rapidly, and because they tend to put their mouths in and on things that can damage fixed devices, repair and reapplication of the appliance are all too frequent occurrences. Fixed acrylic appliances that incorporate an aluminum or stainless steel incline plate can be attached to orthodontic retention wires.
The earlier correction is initiated, the better the results. Treatment is best initiated when the intermediate upper incisors (Triadan 502 and 602) are in wear (i.e., when the foal is 6–12 weeks old) so that interference with the eruption of these teeth is avoided. Prior to orthodontic correction, a full set of skull radiographs and occlusive measurements should be obtained. The cheek teeth should be floated to reduce tall transverse ridges and rostral or caudal hooks. The incisor plate opens the bite, thus separating the occlusal contact between the upper and lower cheek teeth. ‘Overfloating’ of the occlusal surface, therefore, is discouraged because it results in loss of contact between the upper and lower arcades during mastication when the incline plate is in place. Primiparous mares and dams with small nipples on the udder can present a problem for foals attempting to nurse after surgery. Foals should be fed a diet consisting of a pelleted complete foal ration before and after surgery.
Preoperatively, the foal receives antimicrobial and non-steroidal anti-inflammatory drugs, and the mouth is rinsed completely with a dilute chlorhexidine solution. General anesthesia is induced with xylazine and ketamine and maintained with a triple drip (i.e., a combination of xylazine, ketamine, and guaifenesin). The foal is positioned in lateral recumbency, and an oxygen tube is inserted nasally. Oxygen is delivered at 10 l/min during the procedure. Using a rasp or power grinder, the exposed crowns of the upper and lower incisors are reduced and leveled almost to the gingival margin, taking care not to expose the pulp (Fig. 19.9).

A small area just ventral to the facial crest is clipped and prepared for surgery. With one hand in the mouth, the junction between upper 3rd and 4th premolars (Triadan 07 and 08) on the arcade is identified as an indentation in the hard palate. A small, longitudinal, skin incision is made below the facial crest at a level just opposite this junction, avoiding branches of the facial nerve, maxillary artery, and salivary duct. A  -inch diameter Steinmann pin is introduced through the skin incision and directed between the reserve crowns of upper 3rd and 4th premolars just above the buccal gingival margin so that the pin emerges in the mouth
-inch diameter Steinmann pin is introduced through the skin incision and directed between the reserve crowns of upper 3rd and 4th premolars just above the buccal gingival margin so that the pin emerges in the mouth  –
– inch above the palatal gingival margin. Care should be taken to avoid the palatine artery. Intra-operative radiographs and/or fluoroscopy are helpful and sometimes necessary to properly position the pin between the teeth without damaging dental roots. The pin is removed, and a 14-gauge, 1.5-inch hypodermic needle is carefully placed in the hole created by the pin to act as a wire guide. A section of 18-gauge, stainless steel, orthopedic wire is cut to a length at least three times the distance from 4th premolar to the central incisors. One end of the wire is inserted into the dorsal aspect of the oral cavity through the needle, and the needle is removed over the other end of the wire, which is then doubled back and passed through the buccal incision into the buccal space of the oral cavity (Fig. 19.10). Care should be taken not to catch soft tissue with the wire or to damage a branch of the facial nerve during this process. The end of the wire in the buccal space is grasped with forceps inserted into the mouth, and it and the palatal portion of the wire are pulled rostrally to form a loop around the distal aspect of the reserve crowns of the upper 2nd and 3rd premolars. Kinks should be avoided because they hasten stress fatigue of the wires. The small skin incision is left open to heal by second intention. The foal is repositioned in lateral recumbency on the opposite side, and the procedure is repeated.
inch above the palatal gingival margin. Care should be taken to avoid the palatine artery. Intra-operative radiographs and/or fluoroscopy are helpful and sometimes necessary to properly position the pin between the teeth without damaging dental roots. The pin is removed, and a 14-gauge, 1.5-inch hypodermic needle is carefully placed in the hole created by the pin to act as a wire guide. A section of 18-gauge, stainless steel, orthopedic wire is cut to a length at least three times the distance from 4th premolar to the central incisors. One end of the wire is inserted into the dorsal aspect of the oral cavity through the needle, and the needle is removed over the other end of the wire, which is then doubled back and passed through the buccal incision into the buccal space of the oral cavity (Fig. 19.10). Care should be taken not to catch soft tissue with the wire or to damage a branch of the facial nerve during this process. The end of the wire in the buccal space is grasped with forceps inserted into the mouth, and it and the palatal portion of the wire are pulled rostrally to form a loop around the distal aspect of the reserve crowns of the upper 2nd and 3rd premolars. Kinks should be avoided because they hasten stress fatigue of the wires. The small skin incision is left open to heal by second intention. The foal is repositioned in lateral recumbency on the opposite side, and the procedure is repeated.

Fig. 19.10 Parrot-mouthed foal in lateral recumbency for placement of orthodontic wires. A Steinmann pin is used to make a hole between the reserve crowns of 607 and 608, and a 14-gauge needle is placed in the hole and used as a guide for the 18-gauge, orthopedic retention wire. The needle is pulled over the free end of the wire. A longer free end of the wire is placed back through the same skin incision just below the facial crest, pushed through the mucosa into the buccal recess and brought rostrally.
With both wire loops extending out of the oral cavity, the foal is placed in dorsal recumbency with a pad placed caudal to the poll to hyperextend the neck so that the roof of the mouth lies parallel to the ground. The loop wire around the first two cheek teeth is pulled tight and twisted several times on itself in the interdental space. Including the occlusal surface of the upper 2nd premolar in the twists is avoided by keeping the wire close to the hard palate and pulling downward on the buccal wire and upward on the palatal wire while twisting. The twisted strands from both sides are pulled rostrally and brought around the labial edge of the upper incisor arcade and twisted together. The wires should lie across the labial surface of the incisors at the gingival margin. The ends of the wires are cut and tucked between two incisors. An  -inch-thick plate of aluminum with several 3.5 mm perforations is sized so that it fits over the occlusal surface of the upper incisors and extends caudally over the hard palate
-inch-thick plate of aluminum with several 3.5 mm perforations is sized so that it fits over the occlusal surface of the upper incisors and extends caudally over the hard palate  inch caudal to the point at which the lower incisors contact the hard palate (Fig. 19.11A). Paraffin rope is placed around the gingival margin of the upper incisors, pulled under the wires on each side, and extended several centimeters caudally on the hard palate to form a dental dam to contain the unset acrylic (Fig. 19.11B). Hard-setting dental acrylic is mixed and formed into the roof of the mouth, within the confines of the paraffin rope, incorporating the wires and labial surface of the upper incisors. The acrylic should cover the knot in the wire on the labial aspect of the upper incisors to prevent the knot from irritating soft tissue. Splinting of the upper incisor arcade with acrylic stabilizes the teeth and prevents the force of the orthodontic wires from spreading or twisting the incisors. The acrylic band wrapping around the labial surface of the upper incisors and the orthodontic wires hold the acrylic firmly in the roof of the mouth. The acrylic is formed with the curved, rostral edge of the metal plate resting on the occlusal surface of the upper incisors and the caudal, straight edge of the plate level or slightly more ventral in the mouth than its rostral edge. This creates a flat or inclined surface for the lower incisors to contact (Fig. 19.11C). This inclined plate frees the mandible from caudal force imposed on it by the upper incisors and creates a slight rostral pull on the mandible as the lower incisors slide over the plate during chewing. As the foal chews, upward pressure is applied to the upper incisors and premaxillae, forcing them into a more normal position (Fig.19.12).
inch caudal to the point at which the lower incisors contact the hard palate (Fig. 19.11A). Paraffin rope is placed around the gingival margin of the upper incisors, pulled under the wires on each side, and extended several centimeters caudally on the hard palate to form a dental dam to contain the unset acrylic (Fig. 19.11B). Hard-setting dental acrylic is mixed and formed into the roof of the mouth, within the confines of the paraffin rope, incorporating the wires and labial surface of the upper incisors. The acrylic should cover the knot in the wire on the labial aspect of the upper incisors to prevent the knot from irritating soft tissue. Splinting of the upper incisor arcade with acrylic stabilizes the teeth and prevents the force of the orthodontic wires from spreading or twisting the incisors. The acrylic band wrapping around the labial surface of the upper incisors and the orthodontic wires hold the acrylic firmly in the roof of the mouth. The acrylic is formed with the curved, rostral edge of the metal plate resting on the occlusal surface of the upper incisors and the caudal, straight edge of the plate level or slightly more ventral in the mouth than its rostral edge. This creates a flat or inclined surface for the lower incisors to contact (Fig. 19.11C). This inclined plate frees the mandible from caudal force imposed on it by the upper incisors and creates a slight rostral pull on the mandible as the lower incisors slide over the plate during chewing. As the foal chews, upward pressure is applied to the upper incisors and premaxillae, forcing them into a more normal position (Fig.19.12).

Fig. 19.11 (A) Parrot-mouthed foal placed in dorsal recumbency with orthodontic retention wires in place. An aluminum plate is cut and sized to fit the occlusal surface of the upper incisors while projecting caudally to contact the occlusal surface of the lower incisor arcade. A dam of paraffin rope has been built to retain the acrylic mouth piece. (B) Acrylic and thin plate in place. (C) Lateral view showing final placement of wires and acrylic mouth piece.
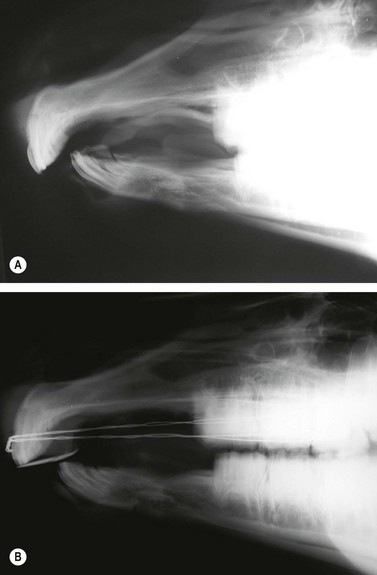
Fig. 19.12 (A) Lateral radiograph of the rostral skull of a 4-month-old foal with an overjet and overbite just prior to surgery (B) Lateral skull radiograph of foal with orthodontic retention wires placed behind the upper third premolar and encircling the upper incisor arcade. The metal incline plate has not been sloped for this first application of retention wires because creating a slope would have caused a gap in the premolar arcades. The second appliance will have a slope or mechanical incline to encourage rostral growth of the mandible.
The foal is allowed to recover from anesthesia after the acrylic sets and is returned to the dam. Most foals quickly learn to nurse with the appliance in place. Foals that do not nurse well should be supplemented with a complete foal ration and weaned.
Postoperative care consists of keeping the skin wounds clean until healing is complete. Most foals are administered omeprazole orally for 4–5 days, while they adjust to the orthodontic appliance, to help prevent gastric ulcers. Most foals begin to eat and nurse well within 1–2 days after surgery. The plate and wires should be checked daily by personnel at the farm to determine if the wires are loose or broken or if the acrylic appliance has loosened. The foal should be examined monthly by a veterinarian to ensure that the appliance is secure and is not causing oral lesions. At the same time, the cheek teeth should be inspected so that abnormal wear patterns can be detected and corrected by careful floating.
The appliance eventually loosens, so that by 3–6 months the appliance and wires must be removed. If correction is not complete by this time, the wires and acrylic appliance are reapplied and maintained until desirable results are achieved. The gap between the upper and lower incisors decreases, for most horses, by about 5 mm every 3–6 months. The most rapid correction is noticed when the procedure is performed when the horse is 2–8 months old; improvement is slow after the horse is 8 months old and ceases by the time the horse is 19 months old. Complications from orthodontic wiring and bite plate application are rare. They can include trauma to the dorsal buccal nerve, damage to the greater palatine artery, postoperative pain and nursing problems, and nasal curvature from unilateral wire breakage.50
Adult horses suffering from parrot mouth experience long-term adverse effects on dentition and mastication. The molar arcades may develop a hook on the rostral aspect of the upper 06s and/or a hook and/or ramp on the caudal aspect of the lower 11s, and the cheek teeth of both the upper and lower jaws may develop abnormal, exaggerated transverse ridges. The combination of abnormalities of the cheek teeth and elongated incisors tends to limit free, lateral excursion of the jaw, which can lead to a steep angle of the occlusal surface of the cheek teeth or, in some cases, to bilateral shear mouth.
Some parrot-mouthed horses function quite well if they receive regular dental equilibration and if their diet is modified. Dental equilibration entails reduction of rostral and caudal hooks, abnormal exaggerated transverse ridges, and steep molar angles. Unopposed upper and lower incisor arcades should be shortened to allow more normal, unobstructed motion of the lower jaw. Deciduous incisors can be shortened with little risk of damaging the pulp chambers. Permanent incisors, especially long ones, should be reduced in stages.
In addition to having its teeth equilibrated, a parrot-mouthed horse should also have its diet altered or modified. Some parrot-mouthed horses have difficulty foraging short grass; others have difficulty masticating any type of roughage, and so, to maintain these horses in good body condition, feeding processed or extruded feeds may be beneficial.
Monkey mouth
The term monkey mouth refers to the condition where the premaxillae/maxillae are shorter than the mandible, leading to an incisor underbite. This condition has also been termed sow mouth, hog mouth, undershot jaw, underjet, underbite, or mandibular prognathism, but the official term is a Class 3 malocclusion (MAL3). Retrognathism is a term defined, using human anatomical nomenclature, as a condition where the mandible is located posterior to its normal position in relation to the premaxillae/maxillae or a condition where one or both jaws lie posterior to normal in their craniofacial relationship.
The forward projection of one or both jaws in relation to the craniofacial skeleton has been referred to as prognathism. This condition is seen more commonly in miniature horses and has been associated with achondroplastic dwarfism in cattle.51–53 Prognathism is also seen in other breeds of horses, especially those with a dished face, such as the Arabian breed. This congenital anomaly has been reported to occur with other deformities of the head and musculoskeletal system. Owners should receive genetic counseling before therapy is undertaken to correct monkey mouth (Fig. 19.13).

Principles of therapy in the young, growing horse should consist of:
• encouraging or accelerating growth of the maxillae and premaxillae
• supporting the nasal bones and nasal septum
• slowing rostral growth of the mandible
• preventing the upper incisor arcade from interfering with the lower incisor arcade, and
Adult horses with a hook on the rostral aspect of the lower 06s can develop a slightly undershot lower jaw. This abnormality can be corrected by periodically floating the cheek teeth to remove the hooks and by reducing the incisors.
Wry nose
Wry nose, or campylorrhinus lateralis, is a congenital deviation of the maxillae, premaxillae, and nasal septum (Fig. 19.14). It is an infrequently reported condition sometimes associated with other congenital anomalies, such as cleft soft palate (palatoschisis), umbilical herniation, and contracted tendons of the limb.54 Affected foals may have difficulty suckling, but most seem to thrive until dyspnea appears when they are several months old. The degree of dyspnea is related to the severity of the nasal septal deviation. Severely affected foals may require a permanent tracheostomy or a nasal dilation tube to ventilate properly. Horses affected with wry nose usually encounter difficulty prehending and masticating grass forage when they are weaned. Lateral excursion of the lower jaw is usually limited to movement to the convex side of the deformity, causing abnormal wearing of cheek teeth, which may lead to shear mouth.
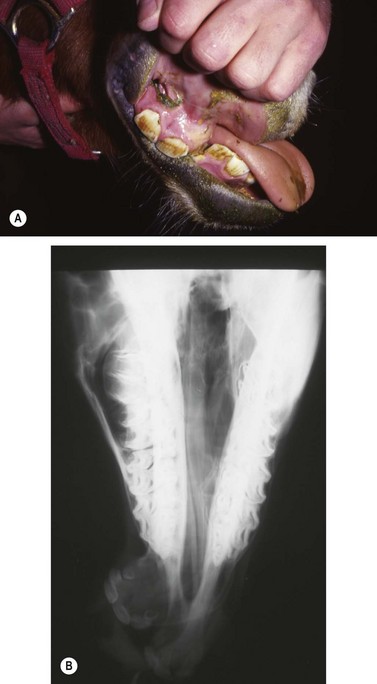
Fig. 19.14 (A) Four month old wry nose foal. (B) Dorsoventral radiograph of a wry nose foal. The maxilla is deviated at a 65° angle to the mandible.
Wry nose is thought by some to be a heritable condition because it seems to be seen most often in the Arabian and miniature horse breeds,52–54 but these claims are not supported by scientific evidence. The authors are aware of a mare that produced two foals affected with wry nose, during successive pregnancies, when bred to the same stallion (Dr Chris Johnson, personal communication, 2008).
Mildly affected foals have been managed using unilateral orthodontic wiring with good results. More severely affected foals have been treated successfully using principles of orthognathic surgery, as detailed later in this chapter, and many of these treated foals have developed into successful athletes and productive breeders.11,13,55,56
Foals should be evaluated carefully for aspiration pneumonia and to rule out associated congenital defects. The degree of the deformity can be determined by oral radiographic examination, and computed tomography of the skull might be useful to confirm the position and degree of premaxillary/maxillary deviation and nasal obstruction (Fig. 19.15). Dental impressions of the upper and lower arcades from the premolars to the incisors can help the surgeon determine the amount of space created on the concave side of the premaxillae/maxillae when the deformity is corrected and the upper and lower incisor arcades are brought into proper occlusion (Fig. 19.16). Occlusal abnormalities of the premolars causing wear should be corrected prior to surgery. This involves re-establishing a normal occlusal angle on the premolar arcades and leveling the incisors (Fig. 19.17).
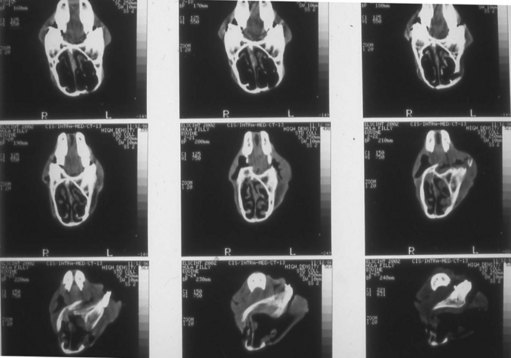
Fig. 19.15 Computed tomography images of transverse scans through the head of a 7-month-old Thoroughbred filly with wry nose. The filly is positioned in dorsal recumbency, and serial images, beginning at the second premolar and advancing rostrally, demonstrate the premaxillary curvature and progressive narrowing of the right nasal cavity.

Fig. 19.16 Plaster of Paris dental model of the upper arcade from a wry-nosed foal. The model has been cut and straightened to bring the upper and lower incisor arcade into proper occlusion. The white wedge indicates the angle of rostral and lateral displacement required to correct the deformity.
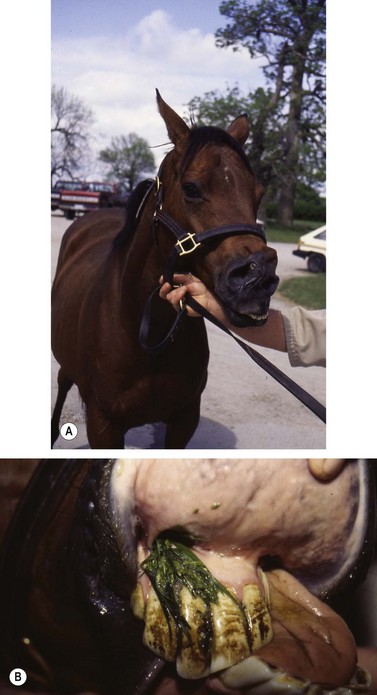
Fig. 19.17 (A) and (B) Twelve-year-old Thoroughbred mare with a wry nose. A ‘permanent’ tracheostomy as a yearling allowed the mare to breathe with no signs of respiratory distress. She had produced six normal foals while being bred to six different stallions. The uncorrected dental and facial deformity caused the mare difficulty with prehension and mastication. She had a severe shear mouth on the concave (right) arcades.
Conclusion
All undesirable traits and pathologic conditions present at birth were at one time thought to be entirely genetic in origin. Our knowledge of birth defects has evolved to the point that we now know that many, if not most, congenital defects are the result of intrauterine events that result from extrauterine influences. Congenital defects do not indicate inheritance but simply that the defect was present at birth.
Some characteristics of horses are genetically influenced, and horses have been selectively bred for centuries to promote or discourage these characteristics. The selection for or against inherited tendencies is the basis for our current breed registries. Size, power, color, speed, conformation, and many other characteristics that are genetically influenced, are selected for or against by certain breed registries. Variations from ideal may be undesirable, but they are not genetic defects.
The American Veterinary Medical Association (AVMA) recently restated a policy saying that surgical correction of ‘genetic defects’ for the purposes of concealing the defect is unethical.57 This AVMA statement refers specifically to correction of genetic defects. By definition, a genetic defect is a pathologic condition of proven genetic origin.
Although equine practitioners should support the intent of the AVMA statement, the policy should be applied only to horses with a genetic defect and not misapplied to horses with a congenital defect for which a genetic cause has not been proven or to horses with inherited tendencies. Equine practitioners should considered surgical treatment of horses with a debilitating condition if the condition is amendable by surgical correction. There is no doubt that correction of debilitating dental malocclusions and facial deformities is in the best, long-term interest of the horse’s oral health. Some equine breed registries require certain undesirable traits and/or conditions commonly considered to be a ‘genetic defect’ to be indicated on the affected horse’s registration certificate. This requirement should be brought to the attention of an owner or breeder when a severe malocclusion is diagnosed. An attempt to correct a known genetic defect to allow an owner to misrepresent the horse in the show ring or breeding shed should be considered unethical.
Clinical observation and detailed documentation promote understanding of why and how malocclusions and malrelationships between the jaws occur and how they can be prevented or treated. The equine practitioner can benefit greatly from the new human biomedical discoveries. Genetic studies to detect the chromosomal factors that play a role in head shape could influence genetic consultation and mating engineering. Such studies and/or research may help reduce the incidence of equine dental malocclusions.
Equine orthodontic principles are at work in the mouth starting in utero and continuing well into old age. Changes occur as the deciduous teeth erupt, the jaws grow and develop, deciduous teeth are shed, permanent dentition erupts, and the hypsodont teeth wear. The equine practitioner who is familiar with the principles of diagnosis and documentation of malocclusion is better able to use the controlled movement of teeth and adjustments of jaw growth for treatment. Knowledge obtained through observation, diagnosis, documentation, and appropriate adjustments provides the equine dental patient with the best possible occlusion and helps maintain proper oral health.
Surgery of the paranasal sinuses
Sinusotomy
Surgery of the paranasal sinuses is performed most commonly to determine the cause of clinical signs of disease referable to the paranasal sinuses, such as facial deformity or chronic, unilateral nasal charge. It is also performed to excise or biopsy abnormal tissue, such as an osteoma, cyst, progressive ethmoidal hematoma, fungal granuloma, or neoplasm, or to evacuate inspissated exudate, usually from the ventral conchal sinus. It is sometimes performed to expose the apex of a diseased tooth so that the tooth can be repulsed into the oral cavity or receive endodontic treatment. The paranasal sinuses can be exposed through one or more trephine openings or through an osteoplastic flap. Although the paranasal sinuses can be examined endoscopically through one or more trephine holes, treatment of the horse for a disease identified endoscopically is often not possible, unless the trephine opening is huge, in which case the horse may be left with facial deformity. Surgery of the paranasal sinuses is, therefore, usually performed through one or more large osteoplastic flaps that are replaced at the end of surgery.
The two types of osteoplastic flaps are the frontonasal flap and the maxillary flap. The frontonasal flap is the most versatile because it is easy to create and provides direct or indirect access to all compartments of the ipsilateral paranasal sinuses. The maxillary flap is more difficult than the frontonasal flap to create and provides poor access to the ventral conchal sinus, at least in horses less than 6 years old. The maxillary flap provides good access to the rostral and caudal maxillary sinuses, however, and is most commonly used to expose the apex of the first or second maxillary molar (Triadan 09 and 10). The apex of the third maxillary molar (Triadan 11) is often best exposed through a frontonasal flap. The surgeon should have a good understanding of the boundaries and anatomical features of the paranasal sinuses before performing sinusotomy.
Frontonasal flap
To create a medially-hinged, osteoplastic frontonasal flap, a three-sided incision through the skin, subcutaneous tissue, and periosteum, with rounded corners, is created within the confines of the boundaries of the frontal and dorsal conchal sinuses (i.e., the conchofrontal sinus; Fig. 19.18). The caudal portion of the incision begins on the dorsal midline, at a point midway between the supraorbital foramina and the medial canthi of the eyes, and extends laterally, perpendicular to the long axis of the head, to a point about 1.5–2 cm medial to the most medial aspect of the rim of the orbit. The rostral portion of the incision also begins on the dorsal midline, at a point 1–2 cm caudal to the plane where the nasal bones begin to diverge, and extends laterally, perpendicular to the long axis of the head, to an imaginary line extending from the medial canthus of the eye to the nasoincisive notch. The lateral portion of the incision connects the lateral extent of the rostral and caudal portions of the incision and courses parallel to the midline. The incision should not cross the path of the nasolacrimal duct, which courses between the medial canthus of the eye and a point midway between the infraorbital foramen and the nasoincisive notch. The rostral aspect of the lateral segment of the incision can be angled medially, if necessary, to avoid crossing the duct. Periosteum is reflected several millimeters from the underlying frontal and nasal bones with a periosteal elevator.

Fig. 19.18 To create a medially hinged, osteoplastic frontonasal flap, a three-sided incision extending through periosteum is created within the confines of the boundaries of the conchofrontal sinus.
The incision is extended through bone using an oscillating bone saw, a motorized cast cutter with a sharp, oscillating blade, or a mallet and osteotome. The blade of the saw should be cooled with sterile, normal saline solution, while cutting, to avoid overheating bone. The bone is cut at a 45° angle so that the flap’s external lamina is slightly larger than its internal lamina. The flap is elevated sufficiently, using a chisel or osteotome, to allow the fingers of one hand to be introduced beneath the flap, and the flap is fractured at its base, close to the dorsal midline. The flap remains attached to the skull by skin, subcutaneous tissue, and periosteum.
Elevating the flap exposes the conchofrontal sinus, which communicates ventrally with the caudal maxillary sinus through the large frontomaxillary aperture. Provided that the architecture of the sinuses is not distorted by disease, the bulla of the ventral conchal sinus, which forms a portion of the maxillary septum, is usually seen protruding into the caudal maxillary sinus beneath the rostral margin of the frontomaxillary aperture (Fig. 19.19). Occasionally, this structure is obscured by the caudal portion of the floor of the dorsal conchal sinus. To expose the rostral maxillary and ventral conchal sinuses, a portion of this bulla is excised with scissors. After creating a hole in the bulla, the ventral conchal sinus is seen medial to the infraorbital canal, and the rostral maxillary sinus is seen lateral to the canal. The infraorbital canal is supported by a thin plate of bone that separates these two compartments. All or a portion of the reserve crowns of the 3rd, 4th, and 5th cheek teeth (Triadan 08–10) completely fill the rostral maxillary sinus of horses less than 4 years old. To better expose the ventral conchal and rostral maxillary sinuses, the rostrolateral portion of the floor of the conchofrontal sinus and the closely associated dorsolateral portion of the ventral conchal bone can be excised using a scissors or a bone rongeur.
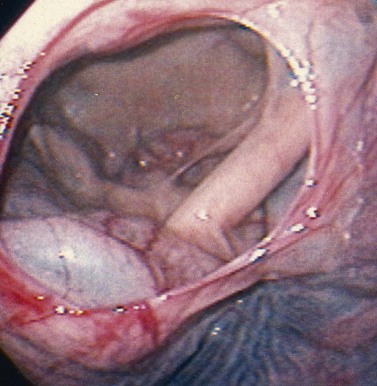
Fig. 19.19 The bulla of the ventral conchal sinus is seen protruding into the caudal maxillary sinus beneath the rostral margin of the frontomaxillary aperture. The bulla structure is sometimes obscured by the caudal portion of the floor of the dorsal conchal sinus.
The medial wall of the dorsal or ventral conchal sinus is often perforated, or a portion of it is excised, to establish a portal for drainage of the paranasal sinuses into the nasal cavity, and creating this portal is generally accompanied by substantial hemorrhage. A portal for drainage need not be established if the nasomaxillary aperture is patent, provided that the mucosa of the sinuses is not grossly thickened. Patency of the aperture can sometimes be determined by threading a 5- to 8-Fr, male dog urinary catheter into the caudal opening of the nasomaxillary aperture, located between the floor of the dorsal conchal sinus and the bulla of the ventral conchal sinus at the rostral aspect of the frontomaxillary aperture. The end of the catheter exits the ipsilateral external naris. Threading a catheter through the nasomaxillary aperture can sometime be difficult or even impossible, but blood or lavage fluid seen exiting the nasal cavity can also be used as evidence that the nasomaxillary aperture is patent. Rarely is the nasomaxillary aperture obstructed.
A portal to remove gauze packing or to allow lavage of the sinuses can be created in the frontal bone, adjacent to flap, through a 2-cm, longitudinal, skin and periosteal incision, using a 9.5-mm ( -inch) Galt trephine. Alternatively, the portal can be created in the maxillary bone about 2 cm ventral and 2 cm rostral to the medial canthus of the eye.
-inch) Galt trephine. Alternatively, the portal can be created in the maxillary bone about 2 cm ventral and 2 cm rostral to the medial canthus of the eye.
After returning the flap to its normal position, at the end of surgery, the subcutaneous tissue is apposed with 4–6, widely-spaced, simple interrupted, absorbable sutures. Because the bone in the flap is beveled, it need not be attached to surrounding bone, and suturing the fragile, inelastic periosteum is difficult to impossible. The margins of the skin incision are apposed with staples, and the surgical site is compressed with a Stent bandage or with gauze swabs anchored by elastic, adhesive tape placed in a figure-of-eight fashion around the head. Gauze packed into the sinuses can be removed through the trephine hole, usually within 12 hours, and the Stent or elastic bandage is removed at 5–7 days. The portal created for lavage of the sinuses or to remove the gauze packing can be closed with staples or sutures after the portal is no longer required.
Surgery of the paranasal sinuses is usually performed with the horse anesthetized and recumbent, but most surgeries of the paranasal sinuses that can be performed through a frontonasal flap can also be performed with the horse standing, thereby eliminating the risks and expense of general anesthesia (Fig. 19.20). Repulsion of a tooth, however, is most safely performed with the horse anesthetized. Creating a frontonasal flap causes minimal hemorrhage, regardless of the position of the horse, but performing surgery within the sinuses with the horse standing seems to cause less hemorrhage than surgery performed with the horse anesthetized and recumbent.58 Performing surgery of the horse’s sinuses with the horse standing and its head elevated may result in less venous congestion in structures of the paranasal sinuses, and hence less hemorrhage, than if the same surgery were performed with horse recumbent. Another advantage of performing surgery of the sinuses with the horse standing is that the structures within the sinuses are oriented in a normal position.

Fig. 19.20 A progressive ethmoidal hematoma exposed through a conchofrontal, osteoplastic flap created with the horse sedated.
A horse selected to receive surgery of the sinuses while standing should be compliant and should not resent movement of hands and instruments about its head. When performed with the horse standing, surgery of the paranasal sinuses is most safely and conveniently performed with the horse restrained in stocks; cross-tying the horse’s halter to the stocks provides added restraint. The horse is sedated with detomidine HCl (0.01–0.02 mg/kg IV or 0.03–0.04 mg/kg intramuscularly) and butorphanol tartrate (0.02–0.05 mg/kg IV) or morphine (0.15 mg/kg IV). When administered intramuscularly, detomidine should be administered 15–20 minutes before surgery. The horse can be re-sedated during surgery with xylazine (0.5 mg/kg IV) or detomidine (0.01 mg/kg IV), when needed, to minimize movement. If a long procedure is anticipated, constant rate infusion of detomidine (0.02 mg/kg/hour) and butorphanol (0.012 mg/kg/h) can be administered to provide a prolonged, constant state of sedation, after first administering a loading dose of detomidine (0.008 mg/kg IV) and butorphanol (0.02 mg/kg IV).59 The horse can also be sedated using constant-rate infusion of morphine (0.15 mg/kg/h) after first administering a loading dose of morphine (0.15 mg/kg IV). After the horse is sedated, its head should be supported on a stand or small table so that the site of sinusotomy is at a comfortable level for the surgeon.
The proposed site of incision is infused subcutaneously with local anesthetic solution, and the paranasal sinuses are desensitized, either by infusing 30–40 ml of local anesthetic solution into the sinuses or by anesthetizing the ipsilateral maxillary nerve. Instilling local anesthetic solution into the paranasal sinuses usually desensitizes the mucosa sufficiently to permit most procedures to be performed without causing severe discomfort to the horse. The local anesthetic solution is infused through a small hole created several centimeters medial to the medial canthus of the eye with a Steinmann pin in a Jacob’s chuck or with a steel 14- or 16-gauge hypodermic needle driven through a stab incision in the skin and frontal bone with a mallet. A plug of tissue is often retained within the shaft of the needle and can be extruded into the sinuses with a smaller gauge, spinal needle inserted through the shaft of the larger needle.
The paranasal sinuses can be desensitized more effectively by anesthetizing the maxillary nerve at the pterygopalatine fossa, where it passes through the maxillary foramen to enter the infraorbital canal as the infraorbital nerve. To anesthetize the maxillary nerve, a 20-gauge, 8.9-cm (3.5-inch) spinal needle is inserted just ventral to the zygomatic process at the level of the lateral canthus of the eye, perpendicular to the long axis of the head until the needle strikes bone. Ten–fifteen milliliters of local anesthetic solution is deposited at this site.
The paranasal sinuses can also be desensitized by depositing 10 ml or more of local anesthetic solution into the rostral aspect of the infraorbital canal. This large volume anesthetizes the infraorbital nerve, which courses through the canal, as far caudally as the maxillary foramen. To locate the infraorbital foramen, the thumb (or middle finger) is placed in the nasomaxillary notch, and the middle finger (or thumb) is placed on the rostral end of the facial crest. The foramen is located with the index finger halfway between and 1.5 to 2.5 cm (0.5–1 inch) caudal to an imaginary line between these points (Fig. 19.21). The bony ridge of the foramen can be palpated by pushing the ventral edge of the levator nasolabialis muscle dorsally. A 20- or 22-gauge, 3.8 cm (1.5 inch) needle is inserted through the skin about 2.5 cm (1 inch) rostral to the foramen after elevating the levator nasolabialis muscle. The shaft of the needle is inserted about 1 inch into the canal. Although anesthetizing the infraorbital nerve is easier and more reliable than anesthetizing the maxillary nerve, the infraorbital nerve block is not tolerated well by the horse, and so great care should be taken during its administration. Anesthesia of the infraorbital nerve or maxillary nerve at the maxillary foramen desensitizes the paranasal sinuses on that side of the head, but desensitization of the skin at the proposed site of incision by subcutaneous infiltration of local anesthetic solution is still required.
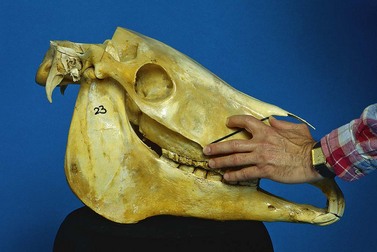
Fig. 19.21 The infraorbital foramen is located by placing the thumb (or middle finger) in the nasomaxillary notch, and the middle finger (or thumb) on the rostral end of the facial crest. The foramen is located with the index finger halfway between 1.5 and 2.5 cm caudal to an imaginary line between these points.
After the horse’s paranasal sinuses and skin at the proposed site of incision are desensitized, the surgical site is prepared for surgery. The surgical site should not be draped, so that the horse’s reactions to the procedure can be monitored. A twitch should be applied to the horse’s upper lip when the bone is cut to prevent the horse from moving, but the twitch can usually be removed after the flap is fractured. The paranasal sinuses are inspected, and the horse is treated for disease encountered. If the maxillary nerve was not desensitized with local anesthetic solution before surgery, the horse may react to manipulations within the sinuses, especially if the infraorbital canal is touched with instruments.
An alternative method of exposing the paranasal sinuses with the horse standing is to create a hole into the conchofrontal sinus through a cutaneous, periosteal flap, using a 5-cm (2-inch) diameter trephine (Arnolds Veterinary Products Ltd, Harlescott, Shrewsbury, UK), as described by Quinn et al (2005).60 The site of trephination is centered 5 cm axial to an imaginary line between the medial canthus of the eye and the nasoincisive notch, 2 cm below a line drawn between the medial canthi, and 4 cm lateral to the dorsal midline. Bone of the forehead is exposed through an abaxially based, curved, cutaneous incision created 1–1.5 cm axial to the intended site of trephination. This incision is extended through the periosteum, and the cutaneous, periosteal flap is reflected abaxially. The edge of the trephine is aligned 10 mm inside the skin incision. The disc of bone excised with the trephine is discarded. At the end of surgery, four or five, simple-interrupted, widely-spaced sutures are placed to approximate the skin and periosteum in a single layer, and the skin incision is stapled. Using a large trephine, rather than an oscillating saw, to expose the sinuses simplifies surgery, while still providing adequate exposure for removal of diseased tissue, but removing the large section of bone sometimes imparts a marked concavity to the horse’s forehead.
Maxillary osteoplastic flap
The apex of a maxillary molar is often exposed through an osteoplastic maxillary flap. Creating a maxillary flap, rather than a trephine hole, to expose the apex of a maxillary molar provides opportunity for visual examination of a large extent of the paranasal sinuses and permits easier manipulation of dental instruments within the sinuses. The most common indication for creating a maxillary osteoplastic flap is repulsion of a tooth.
To create a dorsally hinged, osteoplastic maxillary flap, a three-sided incision through the skin, subcutis, and periosteum, with rounded corners, is created within the confines of the boundaries of the rostral and caudal maxillary sinuses (Fig. 19.22). The caudal boundary of the maxillary sinuses extends from the middle of the eye to the facial crest, and the ventral boundary extends along the facial crest to below the middle of the eye. The rostral boundary is a line that extends from the infraorbital foramen to the rostral border of the facial crest, and the dorsal boundary is a line that extends from the medial canthus of the eye to the infraorbital foramen.
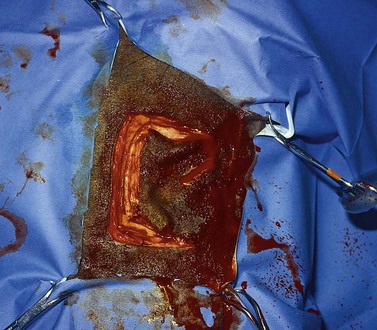
Fig. 19.22 To create a dorsally hinged, maxillary flap, a three-sided incision extending through the periosteum is created within the confines of the boundaries of the rostral and caudal maxillary sinuses.
The caudal portion of the cutaneous incision begins at a point about 1 cm rostral to the eye, slightly below the medial canthus, and extends ventrally to a point about one centimeter dorsal to the facial crest. The incision is extended rostrally, parallel to the facial crest to a point about one centimeter caudal to the rostral end of the facial crest. The incision is turned dorsally and extended to a point about one centimeter caudal to the infraorbital foramen. The rostral portion of the incision extends into the nasolabialis and levator labii superioris muscles and may transect the angularis oculi artery and vein. Periosteum is reflected about 3 mm to the inside of the three-sided incision, and the maxillary bone is cut along the incision using an oscillating saw or a mallet and an osteotome. The bone is cut at a 45° angle, so that its external lamina is slightly larger than its internal lamina. Care should be taken when cutting the bone at the dorsal, rostral end of the incision to avoid damaging the infraorbital canal and the infraorbital nerve contained within. After the rostral, caudal, and ventral sides of the flap have been cut, the flap is pried upward until it fractures dorsally to expose the interior of the rostral and caudal maxillary sinuses. Septal attachments on the interior surface of the bone flap sometimes must be severed with the osteotome before the flap can be pried dorsally. The flap is hinged dorsally by skin, subcutis, and periosteum. Besides repelling a tooth through a maxillary flap, inspissated exudate in the ventral conchal sinus can also be removed through a portal into this compartment created below the infraorbital canal, provided that the horse is more than 6 years old (Fig. 19.23). The sagittal bony plate beneath the infraorbital canal and the lateral wall of the ventral conchal sinus are penetrated using a small trephine or a bone rongeur. The reserve crowns of the first and second maxillary molars of horses less than 6 years old obscure this bony plate and lateral wall of the sinus. The ventral conchal sinus can be exposed by deforming the conchomaxillary aperture, located medial to the infraorbital canal, with a finger.61 The ventral conchal sinus of horses less than 6 years old is most easily penetrated at its bulla, which is exposed through a frontonasal, osteoplastic flap. Inspissated exudate in the ventral conchal sinus most commonly results from primary bacterial sinusitis, but it can also accompany sinusitis secondary to dental infection.
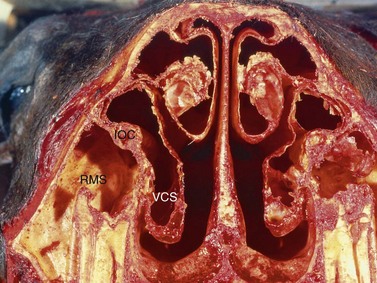
Fig. 19.23 Inspissated exudate in the ventral conchal sinus can also be removed, through a portal in the sagittal bony plate and the lateral wall of the ventral conchal sinus located beneath the infraorbital canal, provided that the horse is older than 6 years. The reserve crowns of the first and second maxillary molars of horses less than 6 years old obscure this bony plate and lateral wall of the sinus. VCS, ventral conchal sinus; RMS, rostral maxillary sinus; IOC, infraorbital canal.
If the sinuses require lavage after maxillary sinusotomy, the portal for lavage can be created over the frontal bone into the conchofrontal sinus or through the maxillary bone into the caudal maxillary sinus, caudal to the flap, about 1.5 cm ventral to the most ventral aspect of the orbit. Packing the paranasal sinuses to achieve hemostasis after repelling a tooth is seldom, if ever, necessary. A trephine portal large enough to accommodate a 24 Fr Foley catheter is created into the conchofrontal sinus through a 3- or 4-cm longitudinal cutaneous incision created over the frontal bone, 2–3 cm medial to the medial canthus of the eye. Fluid instilled into the conchofrontal sinus through the Foley catheter exits the sinuses into the nasal cavity through the nasomaxillary aperture.
After returning the flap to its normal position, after the tooth has been repelled, the subcutaneous tissue is apposed with 4–6, widely spaced, simple interrupted, absorbable sutures. Attaching the flap of bone to surrounding bone is not necessary, because the flap is beveled. Only the subcutis and skin are sutured, because the inelastic periosteum is difficult to appose. The cutaneous margins of the flap are apposed with staples, and the surgical site is compressed with a Stent bandage or with gauze swabs anchored by elastic, adhesive tape placed in a figure-of-eight fashion around the head. The Stent or elastic bandage is removed at 5–7 days. The portal created for lavage of the sinuses can be closed with staples or sutures after the portal is no longer required.
Partial mandibulectomy
The most common indication for partial mandibulectomy is to remove a neoplastic lesion of the rostral aspect of the mandible. The most commonly encountered mandibular neoplasm is the juvenile ossifying fibroma, and this neoplasm is most commonly found on the mentum (Fig. 19.24). Consequently, the mentum is that portion of the mandible that is most frequently amputated. Other neoplasms sometimes encountered on the mentum include the carcinoma (Fig. 19.25) and ameloblastoma. Another indication for amputation of the rostral aspect of the mandible is fracture of the mentum not amenable to repair.

Fig. 19.24 The juvenile ossifying fibroma is the most commonly encountered mandibular neoplasm and is most commonly found on the mentum.

Fig. 19.25 Laterolateral radiograph of the skull of a horse with a carcinoma of the mandible. The rostral portion of the mandible of this horse was amputated caudal to the symphysis.
The rostral portion of the mandible can be amputated with the horse anesthetized and in dorsal recumbency or with the horse sedated using local or regional anesthesia to desensitize the mentum. The horse should receive an antimicrobial and an anti-inflammatory drug prior to surgery. If the procedure is performed with the horse anesthetized using gas anesthesia, the endotracheal tube should be inserted into the trachea through a nasal cavity so that the oral cavity is maximally exposed. Administering a bilateral mental nerve block after the horse is anesthetized allows the horse to be maintained at a lighter depth of anesthesia. To perform the surgery with the horse standing, the mandibular alveolar nerves are desensitized by injecting local anesthetic solution through a needle inserted through the mental foramen into the mandibular canals. If deformity of the mentum from disease makes inserting a needle into the canals difficult, the mentum can be desensitized by infusing the submucosa around the site at which the mandible is to be amputated with local anesthetic solution.
The horse’s mouth is maintained in an opened position with a wedge speculum inserted between the cheek teeth, and the rostral aspect of the mandible prepared for surgery. The gingiva is incised horizontally at the ventral margin of the abnormal bone, and the incision is extended through the periosteum. Each end of the incision is directed dorsally to the center of the right and left interalveolar spaces. At the dorsal aspect of the horizontal ramus of each hemimandible, each end of the incision is redirected rostrally to the corner incisor and then medially until the ends of the incision meet on the midline caudal to the central incisors. The mucoperiosteal flaps created are reflected 15–20 mm beyond the margin of the abnormal bone using a curved, periosteal elevator.
The mandible is transected caudal to the lesion but rostral to the caudal margin of the symphysis using an oscillating saw or obstetrical wire (Figs 19.26 & 19.27). If necessary, hemorrhage from the mandibular stump can be ameliorated by applying bone wax to the cut edge of the bone. Sharp edges of bone are smoothed with a rongeur. The submucosa and periosteum of the lingual flap are apposed to the submucosa and periosteum of the labial flap, using 2-0 or 0-absorbable suture in a simple-continuous or cruciate suture pattern, and the mucosal margins of the flaps are apposed with simple-interrupted, cruciate, or vertical mattress sutures using the same suture material (Fig. 19.28). Inserting a Penrose drain into the space between the two flaps through a stab incision created on the ventral aspect of the mentum prevents formation of a hematoma between the two flaps. Phenylbutazone should be administered twice daily for at least several days after surgery to provide analgesia.

Fig. 19.26 The mandible is transected caudal to the lesion but rostral to the caudal margin of the symphysis using an oscillating saw or obstetrical wire.
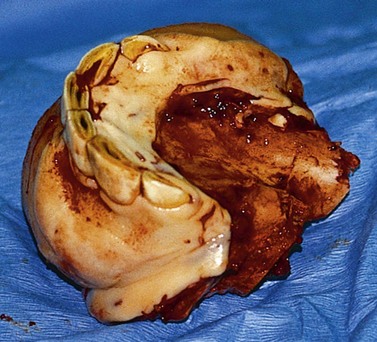

Fig. 19.28 The lingual flap and labial mucoperiosteal flaps are apposed in two layers using absorbable sutures.
The appearance of a horse that has had the rostral aspect of its mandible amputated in this fashion is nearly normal, but the procedure imparts slight flaccidity of the lower lip (Fig. 19.29). Horses are able to prehend grain and grass normally.62 Initially, the tongue may protrude intermittently between the lips.

Fig. 19.29 The facial appearance of a horse that has had the rostral aspect of its mandible amputated is nearly normal, except for slight flaccidity of the lower lip.
If a portion of the symphysis is left intact, the need for internal fixation of the mandibles is avoided, but if the rostral portion of the mandible must be amputated caudal to the symphysis, fixing the right and left hemimandibles to each other may be necessary, using a spacer, such as a portion of rib, at the site of amputation to maintain the proper relationship of the dentition of each hemimandible to its opposing maxillary dentition. However, one of us (JS) amputated the rostral portion of a horse’s mandible caudal to the symphysis, without fixing the hemimandibles to each other, and this horse suffered no postoperative complications.
Premaxillectomy
Indications for premaxillectomy are the same as those for partial mandibulectomy, but the procedure is not performed as frequently as is partial mandibulectomy because ossifying fibroma is not as commonly encountered on the premaxillae as it is on the mandible.
Premaxillectomy is performed in a manner similar to that described for partial mandibulectomy, but the procedure is best performed with the horse anesthetized because, with this procedure, the large palatine arteries are transected. Administering a bilateral infraorbital nerve block after the horse is anesthetized allows the horse to be maintained at a lighter depth of anesthesia. The horse should receive antimicrobial and anti-inflammatory drugs prior to surgery. To perform premaxillectomy, the horse is anesthetized, and an endotracheal tube is inserted nasally, rather than orally, so that the oral cavity is maximally exposed. Anesthesia is best maintained using gas anesthesia. The horse is positioned in dorsal recumbency, and the oral cavity and surrounding skin are prepared for surgery. The upper lip is retracted and attached to the skin over the nasal bones with a towel clamp to expose the vestibule. The horse’s mouth is maintained in an opened position with a wedge speculum inserted between the maxillary and mandibular cheek teeth (Fig. 19.30).

Fig. 19.30 In preparation for premaxillectomy, the upper lip is retracted with a towel clamp to expose the vestibule. The horse’s mouth is maintained in an opened position with a wedge speculum inserted between the maxillary and mandibular cheek teeth.
A horizontal incision through the gingiva and periosteum is made on the labial surface of the premaxillae at the dorsal border of the mass, and each end of the incision angled caudoventrally to the right and left interalveolar spaces aiming toward the caudal border of the canine teeth. Both ends of the incision are redirected rostrally from the alveolar border of the hard palate to the corner incisors and then medially until the ends of the incision meet on the midline caudal to the central incisors. Hemorrhage is controlled by ligating or cauterizing blood vessels. Using a periosteal elevator, the upper lip and nostrils are elevated from the labial surface of the premaxillae and maxillae to at least 1 cm beyond the intended site of transection. The palatine, mucoperiosteal flap is also elevated to its base at the interalveolar space to expose the palatine surface of the premaxillary and maxillary bones and the palatine processes of the premaxillae.
The exposed bone of the upper jaw is then excised, caudal to the lesion, using obstetrical wire or an oscillating saw. The palatine arteries are ligated, and hemorrhage from the maxillae is ameliorated, if necessary, by applying bone wax to the cut edge of bone. If the canine teeth were transected, the portion of each tooth that remains embedded within the maxillae is removed by using a bone gouge. Sharp edges of bone are smoothed with a rongeur, and the submucosa and periosteum of the labial, mucoperiosteal flap are apposed to the submucosa and periosteum of the palatine, mucoperiosteal flap with 2-0 or 0-absorbable suture in a simple-continuous or cruciate suture pattern, and the mucosal margins of the flaps are apposed with simple-interrupted, cruciate, or vertical mattress sutures using the same suture material (Fig. 19.31). Phenylbutazone should be administered twice daily for at least several days after surgery to provide analgesia. Removing a lesion that extends beyond the canine teeth using this technique is difficult without entering the nasal cavities or removing a portion of the nasal septum.
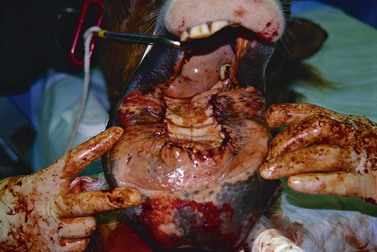
Fig. 19.31 The palatal and labial, mucoperiosteal flaps are apposed in two layers with absorbable sutures.
The facial appearance of a horse that has had a premaxillectomy performed in the manner described is nearly normal (Fig. 19.32). Horses can prehend hay and grain, and can graze tall grass without difficulty but may have difficulty grasping short grass.63 Initially, the horse’s tongue may protrude intermittently between its lips.
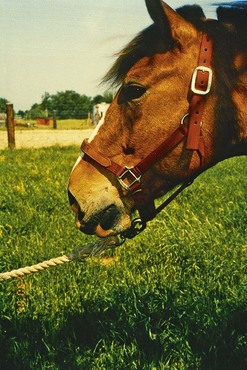
Wry nose
Wry nose, or campylorrhinus lateralis, is a congenital deviation and shortening of the rostral aspect of the bones of the nose (i.e., maxillae, premaxillae, nasal bones, vomer bone, and nasal septum; Fig. 19.33). Wry nose has been reported to occur in a wide variety of horse breeds, but the malformation may be most prevalent in the Arabian breed, causing speculation that the condition may be genetic.64 Inheritance of wry nose, however, has not been reported. Failure of the uterus, particularly that of primiparous mares, to expand to accommodate the fetus as it grows has also been hypothesized to be responsible for the anomaly.31
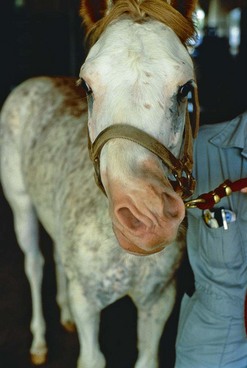
The nose of the affected horse may be deviated mildly or severely (e.g., up to 90°) causing all or some of the premaxillary incisors to fail to contact the mandibular incisors, but the deviation typically does not involve the maxillary cheek teeth. An affected foal may have trouble nursing,65 and its nasal septum may be so severely deviated that it has stertorous respiration, even when resting. The nasal cavity on the convex side of the deviation is the most severely obstructed. Wry nose may be accompanied by other abnormalities, such as cleft palate (i.e., palatoschisis) and abnormal arching of the nasal bones and hard palate.
Most affected foals are capable of nursing and can survive without treatment, but severely affected foals may be unable to nurse and may require immediate, intensive management. A slightly deviated nose may straighten as the horse matures,31 but for horses with moderate or severe deviation, surgical treatment is required to improve respiratory capacity, occlusion of the incisors, and cosmetic appearance. To surgically correct the deviated nose, the maxillae/premaxillae and nasal bones are transected at their point of maximum curvature and stabilized in proper alignment, and a portion of the nasal septum is excised. The nasal bones can be straightened and a portion of the septum removed 2 or 3 months after the premaxillae/maxillae are straightened,13 but to decrease time of convalescence and expense associated with the procedure, the entire deviation can be corrected during one anesthetic period.11
The deviation is corrected with the horse anesthetized, preferably using gas anesthesia, and positioned in dorsal recumbency. The gas anesthetic agent should be delivered through an endotracheal tube inserted through a temporary tracheostomy, rather than orally, to provide maximal exposure of the oral cavity. The horse should receive an antimicrobial and an anti-inflammatory drug prior to surgery. The horse can be administered a bilateral infraorbital nerve block after anesthetic induction, so that it can be maintained at a lighter depth of anesthesia.
Before straightening the maxillae/premaxillae, a section of rib to be grafted at the site of maxillary/premaxillary osteotomy is harvested. After preparing the right or left aspect of the thorax for aseptic surgery, a 10 cm long, cutaneous incision is created over one of the most caudal ribs. The incision begins at the costochondral junction and extends dorsally, through the skin, subcutaneous tissues, and periosteum, along the longitudinal axis of the rib. Periosteum is reflected from the exposed rib, and a 2- to 4 cm long section of rib is transected using obstetrical wire or an oscillating saw. The section of rib is stored in gauze sponges soaked in normal saline solution (0.9 % NaCl) until it is inserted later, at the site of premaxillary/maxillary osteotomy, as a graft. Instillation of bupivacaine around the surgical site to desensitize the intercostal nerve of the rib may diminish pain associated with the rib resection after the horse recovers from anesthesia. The periosteum, musculature, and subcutaneous tissue are sutured separately with 2-0 absorbable suture placed in a simple-continuous pattern, and the skin is stapled. A Stent bandage sutured over the site of surgery may decrease swelling associated with the resection of the rib.
To straighten the premaxillae/maxillae, the horse’s mouth is maintained in an opened position with a wedge speculum inserted between the cheek teeth or with a Guenther oral speculum inserted between the incisors. The upper lip is retracted and attached to the skin over the bridge of the nose with a towel clamp to expose the vestibule, which is cleansed with an antimicrobial soap and rinsed with water. A 3-cm, longitudinal, mucosal incision centered at the point of greatest curvature is created in each interalveolar space over the ventral aspect of each premaxilla/maxilla (Fig. 19.34). The incision extends through the periosteum, which is elevated from the medial and lateral surfaces of the premaxilla/maxilla using a periosteal elevator.
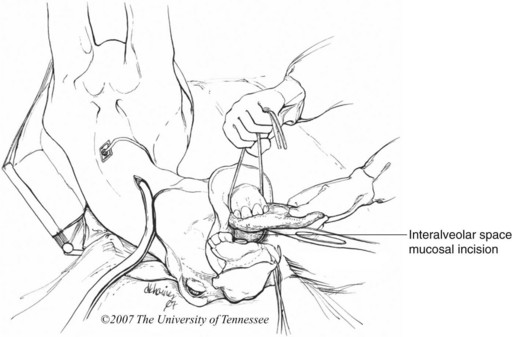
Fig. 19.34 The ventral border of each premaxilla/maxilla is exposed through a longitudinal mucosal incision at the interalveolar space centered at the site of greatest curvature.
(From Schumacher J, Brink P, Easley, J, et al. Surgical correction of wry nose in four horses. Vet Surg 37:142–148, 2008. Illustrations by D.K. Haines
The premaxillae/maxillae and palatine processes of the premaxillae are transected though the mucoperiosteal incisions using an oscillating saw (Fig. 19.35). The oral speculum is removed, and the transected, rostral portion of the upper jaw is rotated toward the sagittal plane of the head until the premaxillary and mandibular incisors are properly aligned. A piece of bone, 1–3 cm long, that corresponds in length to the length of the gap created on the concave side of the jaw when the maxillae/premaxillae are straightened is cut from the harvested section of rib using an oscillating saw, and this piece of bone is inserted tightly into the gap.
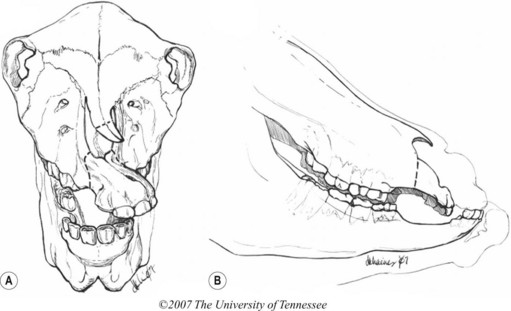
Fig. 19.35 Dashed lines indicate sites of transection of the premaxillae/maxillae and nasal bones.
(From Schumacher J, Brink P, Easley, J, et al. Surgical correction of wry nose in four horses. Vet Surg 37:142–148, 2008. Illustrations by D.K. Haines
The transected segment of the upper jaw is stabilized with 2, trocar-point Steinmann pins (6-mm diameter), using a high-speed, pneumatic drill (Figs 19.36 & 19.37). Each pin is inserted between the reserve crowns of the deciduous central and intermediate incisors, dorsal to the gingival margin, and driven through the medullary cavity of the transected segment of the ipsilateral premaxilla into the medullary cavity of the ipsilateral maxilla. The pin inserted on the concave side of the jaw also penetrates the medullary cavity of the rib graft. Pins are cut flush with the gingiva using a hacksaw or a bolt cutter, and the pins are driven beneath the gingiva using a mallet and a punch. The sites of gingival penetration of the pins are left unsutured to heal by second intention. The gingival incisions at the interalveolar space are closed with 2-0 absorbable suture placed in a simple-interrupted or simple-continuous pattern.
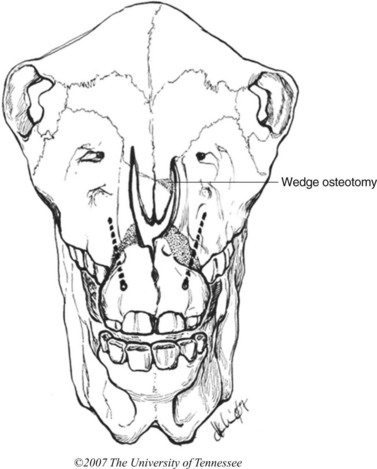
Fig. 19.36 Rostral view. Dashed lines show path of Steinmann pins for fixation of the transected premaxillae/maxillae. Stippled pattern shows gap in premaxillae/maxillae and nasal bones created by transection and realignment of the bones. The gap created when the transected nasal bones are realigned along the longitudinal axis of the skull is eliminated by performing a wedge osteotomy at the convex side of the nasal bones at the site of transection.
(From Schumacher J, Brink P, Easley J, et al. Surgical correction of wry nose in four horses. Vet Surg 37:142–148, 2008. Illustrations by D.K. Haines
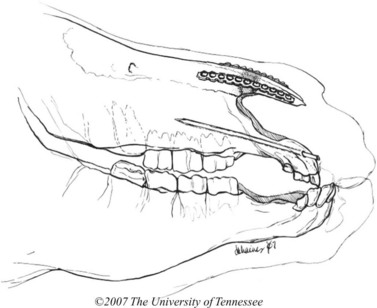
Fig. 19.37 The transected end of each nasal bone can be fixed to its parent nasal bone using a dynamic compression plate or a reconstruction plate.
(From Schumacher J, Brink P, Easley J, et al. Surgical correction of wry nose in four horses. Vet Surg 37:142–148, 2008. Illustrations by D.K. Haines
To straighten the nasal bones and remove the nasal septum, either during the same anesthetic period or 6–8 weeks later, the horse is positioned in lateral recumbency, with the concave side of the deviation uppermost. The dorsal aspect of its head is tilted 45° using a sand bag. After preparing the bridge of the nose for surgery, a 6- to 10 cm, longitudinal, curved, cutaneous incision, centered over the site of maximum deviation of the nasal bones, is made between the two deviated nasal bones. The nasal bones are exposed using a self-retaining retractor, and the periosteum is incised longitudinally, along the midline of each nasal bone, and the margins of the periosteal incisions are reflected.
The nasal bones are transected perpendicular to their long axis at their point of maximum curvature by using an oscillating saw, being careful not to penetrate the underlying parietal cartilage. The gap created on the concave side of the deviation when the bones are rotated into proper alignment can be eliminated by inserting a wedge-shaped segment of one of the cortices of the harvested section of rib into the gap, or the gap in the nasal bones can be eliminated by performing a wedge osteotomy at the convex side of the nasal bones at the site of transection by using an oscillating saw (Fig. 19.36).
The transected end of each nasal bone is fixed to its parent bone using a 2.7 mm reconstruction plate (Fig. 19.38). The plates are fixed with 8-mm long, 2.7-mm cortical screws. The transected segments of the nasal bones can also be fixed to the parent nasal bones with 1-mm diameter Kirschner wires by using a high-speed drill. These Kirschner wires are inserted, caudal to rostral, between the internal and external laminae of the thin, transected end of each nasal bone so that each emerges through the dorsal surface of the nasal bone and skin at the level of the external nares. The wires are then inserted retrograde, between the internal and external laminae of the parent nasal bones. The exposed ends of the wires are cut flush with skin. The Kirschner wires are more difficult to implant because the thickness of the nasal bones is not much more than the diameter of the pins, making insertion of the pins between the internal and external laminae of the bones, without penetrating the nasal or facial surface of the bone, difficult. The subcutaneous tissue is sutured with 2-0 absorbable suture in a simple continuous pattern, and the skin is stapled. A Stent bandage, composed of gauze swabs, is sutured over the surgical site.
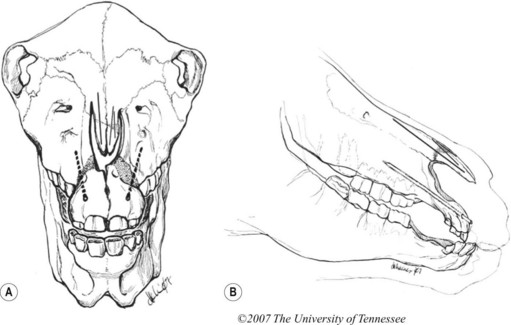
Fig. 19.38 (A) Rostral view. Dashed lines denote position of Steinmann pins. Thin lines in the nasal bones denote Kirschner wires. (B) Lateral view. Kirschner wires in nasal bones (denoted by thin lines) and Steinmann pins in the premaxillae and maxillae. Kirschner wires are inserted, caudal to cranial, through the transected end of each nasal bone, so that each pin emerges through the dorsal surface of the bone and skin at the level of the external nares. The wires are then inserted retrograde into the parent nasal bones.
(From Schumacher J, Brink P, Easley J, et al. Surgical correction of wry nose in four horses. Vet Surg 37:142–148, 2008. Illustrations by D.K. Haines
The nasal septum is removed with the horse in lateral recumbency with the dorsal aspect of its head elevated 45° with a sand bag, using a guarded chisel, a cartilage scissor, or obstetrical wire, using any one of various published techniques.66,67 Two–three centimeters of the rostral aspect of the septum are retained by the horse to provide support for the soft tissues at the rostral aspect of the nose. The caudal cut edge of the septum should lie within the nasopharynx. When only the rostral, deformed portion of the nasal septum is removed, the airways become obstructed if the caudal, cut edge of the septum thickens, because this edge lies between the conchae. The nasal chamber is packed tightly with rolled gauze, and the nostrils are sutured closed to retain the packing. The endotracheal tube is removed, either before or after the horse recovers from anesthesia, and replaced with a tracheotomy tube.
Gauze packing can usually be removed safely after 24 hours, after which the tracheostomy tube is no longer required. Phenylbutazone should be administered twice daily for at least 5 days after surgery to provide analgesia. Steinmann pins can be removed after 6 weeks, and plates or Kirschner wires can be left in situ. Because the upper jaw of most horses affected with wry nose is foreshortened, the horse is likely to require periodic dental care tailored to horses affected with prognathism.
Excising the nasal septum has been reported to result in collapse of the nasal bones into the nasal chamber, and collapse seems most likely to occur if the horse is <1 year old.67 Support of the nasal bones by anchoring each transected segment of nasal bone to its parent bone with either Kirschner wires or plates and screws prevents collapse of the nasal bones. Collapse of the alar folds and ventral aspect of the nasal diverticula resulting in abnormal respiratory noise or partial obstruction of the nasal passage may be evident after surgery.11 Resecting the alar folds may be necessary to resolve the abnormal respiratory noise and partial obstruction of the nasal passage.
Fixing the premaxillary incisors to the mandibular incisors with wire to increase stability at the sites of premaxillary/maxillary osteotomy has been recommended,68 but the additional stability provided by wiring incisors together is not necessary for healing, and horses can be returned to their normal diet as soon as they recover from anesthesia.
Distraction osteogenesis may be another effective method of correcting wry nose.69 Using this technique, the premaxillae/maxillae are partially transected at their point of maximum curvature, and a monolateral distraction external skeletal fixator applied to the concave side of the deformity is used to periodically distract pins inserted rostral and caudal to the osteotomy.69 Using this technique, the nasal bones and nasal septum, in addition to the premaxillae/maxillae, apparently also straighten. A disadvantage of using distraction osteogenesis to correct wry nose is that the horse must be hospitalized for a prolonged time so that the external fixator can be frequently adjusted to maintain a distractive force. Danger of injury to the dam from the protruding pins may prohibit use of the device to correct wry nose of a nursing foal.
Oromaxillary sinus fistula
A relatively common complication of repulsion of one or more of the caudal four maxillary cheek teeth is formation of an oromaxillary sinus fistula (orosinus or oro-antral fistula) resulting in contamination of the paranasal sinuses with feed.70,71 This complication occurs in up to 33 % of horses suffering apical dental infection of one or more of the caudal maxillary cheek teeth (Triadan 09–011) treated by repulsion of the infected tooth into the oral cavity.71An oromaxillary sinus fistula can also develop secondary to an acquired or developmental diastema between two of the caudal maxillary cheek teeth.72 During mastication, food is compressed into the diastema, causing destruction of the periodontium that may eventually result in formation of an oromaxillary sinus fistula, especially if the horse is old, because old horses have short cheek teeth.
Repulsing a maxillary molar or the fourth maxillary premolar creates a large communication between the oral cavity and the paranasal sinuses, and the coronal aspect of this communication is usually plugged with gauze or acrylic until its apical aspect fills with tissue. An oromaxillary sinus fistula results if this communication fails to fill with tissue. The communication may fail to heal if the alveolus becomes chronically infected, usually from sequestration of dental or osseous fragments that were either left in the alveolus at the time of surgery or from osseous sequestra that formed later due to damage to the blood supply of the alveolus caused by surgical trauma.
Premature loss of the alveolar plug or overfilling the alveolus so that the plug extends into the sinuses can also result in formation of an oromaxillary sinus fistula.70,71,73 When the alveolus is overfilled with the plug, the entire alveolus epithelializes around the plug, so that when the plug is removed or lost, the sinuses communicate with the oral cavity through an epithelialized alveolus. The alveolus of old horses is more likely to be overfilled than that of young horses because the alveoli of old horses are short.
Most horses with oromaxillary sinus fistula can be treated while sedated by lavaging feed and exudate from the sinuses through a trephine portal and temporarily plugging the coronal aspect of the vacant alveolus with gauze or acrylic until the apical aspect of the alveolus fills with tissue.72 Before sealing the oral aspect of the alveolus, epithelium that lines the alveolus and infected granulation tissue that fills it are removed by curettage. Horses with an oromaxillary sinus fistula that has occurred secondary to a diastema may also respond to plugging the oral aspect of the diastema with an acrylic, without removal of an adjacent tooth.72 The primary complication associated with this form of treatment is loosening or loss of the plug during the 2 to 3 weeks that it takes for granulation tissue to fill the fistula. The most effective plug is one composed of polymethylmethacrylate.72 To prevent the acrylic plug from loosening, the plug should not be in contact with the cheek teeth in the opposing arcade, and when the acrylic is applied, the surrounding dental structures should be clean and dry. The fistula should be surrounded by a tooth both rostrally and caudally because the acrylic requires a hard surface to attach to. The plug can be applied per os or through a sinusotomy. The plug should not extend into the apical aspect of the fistula. If an overgrowth or exaggerated transverse ridge is present on opposing cheek teeth, it should be reduced.
Horses with an oromaxillary sinus fistula that is refractory to treatment by plugging the coronal aspect of the fistula with acrylic can be treated by occluding the lumen of the alveolus with the end of a transposed muscle, such as the levator nasolabialis muscle74 or levator labii superioris muscle.75 The levator nasolabialis muscle is difficult to mobilize, and because it is flat, it fits poorly into the oromaxillary sinus fistula.75 The levator labii superioris muscle is ellipsoid in its transverse plane, making it ideal for filling an alveolus.
To transpose the levator labii superioris muscle to the oromaxillary sinus fistula, as described by Brink (2006),75 the horse is anesthetized, positioned in lateral recumbency with the affected side of the head uppermost, and prepared for surgery of the oral cavity and face.
The skin over the maxilla is incised longitudinally, with the incision centered over the apex of the oromaxillary sinus fistula, and the paranasal sinuses and the opening of the fistula into the sinuses are exposed through a trephine hole. The epithelial lining of the alveolus is removed by curettage, and the sinuses and fistula are lavaged with isotonic saline solution.
The palpable tendon of the levator labii superioris muscle is exposed through a 2-cm longitudinal skin incision created directly over the tendon and transected 2 cm rostral to its musculotendinous junction (Fig. 19.39). A locking-loop suture with long tails is placed in the tendon. The muscle and tendon are bluntly separated from the underlying maxillary and nasal bones and overlying subcutaneous tissue, using scissor dissection through the small incision created to expose the tendon and through the dorsal margin of the cutaneous incision over the maxilla, to the muscle’s origin rostral to the eye.
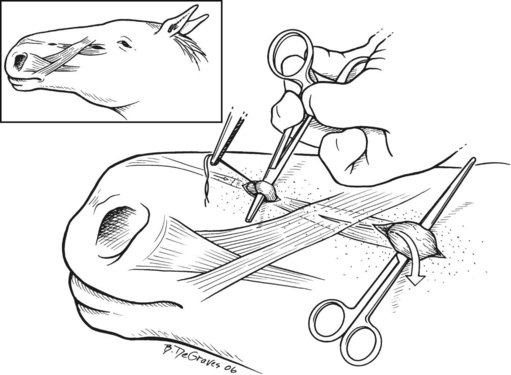
Fig. 19.39 This figure shows the site incisions created to expose the levator labii superioris muscle.
(From Brink P. Levator labii superioris muscle transposition to treat oromaxillary sinus fistula in three horses. Vet Surg 35:596–600, 2006.)
A grasping forceps is inserted subcutaneously at the dorsorostral margin of the incision over the maxilla and advanced rostrally beneath the levator nasolabialis muscle until it emerges at the incision created to expose the tendon of the levator labii superioris muscle. The ends of the suture in the tendon are grasped with the forceps, and by pulling them caudoventrally, the muscle and its tendon are retroverted into the incision over the maxilla (Fig. 19.40). A 2-cm, longitudinal, buccal skin incision is created adjacent to the oral aspect of the oromaxillary sinus fistula, and the jaws of a mosquito forceps are forced into the oral cavity through this incision. The suture ends are inserted through the oromaxillary sinus fistula into the oral cavity, and using hand assistance through the mouth, the suture ends are grasped with the forceps. By placing traction on the suture with the forceps, the tendon and muscle of the levator labii superioris are pulled into the oromaxillary sinus fistula and through the buccal incision so that the muscle completely occupies the oromaxillary sinus fistula (Fig. 19.41).
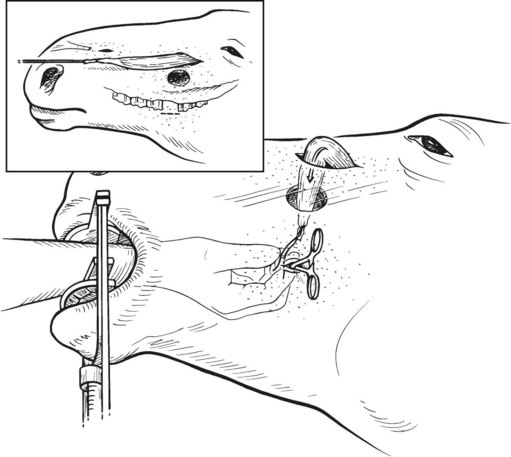
Fig. 19.40 Using a hand placed in the oral cavity, the levator labii superioris muscle is transposed through the maxillary sinus and orosinus fistula.
(From Brink P. Levator labii superioris muscle transposition to treat oromaxillary sinus fistula in three horses. Vet Surg 35:596–600, 2006.)
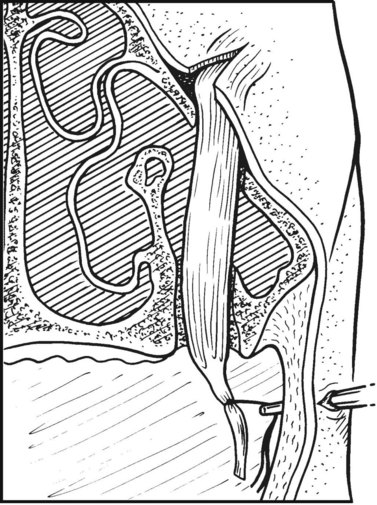
Fig. 19.41 Cross-section of head showing the position of the transposed levator labii superioris muscle and tendon through the maxillary sinus, orosinus fistula, and cheek.
(From Brink P. Levator labii superioris muscle transposition to treat oromaxillary sinus fistula in three horses. Vet Surg 35:596–600, 2006.)
A 5-mm, longitudinal skin incision is made about 2–4 cm ventral to the buccotomy, and using a curved mosquito hemostat inserted through the incision, the skin between this incision and the buccotomy is undermined. The ends of the suture in the tendon are grasped with the forceps and pulled subcutaneously, causing the tendon to emerge at the ventral incision (Fig. 19.42). The tendon is secured under slight tension to the skin and musculature at the ventral buccal incision with several, simple interrupted sutures.
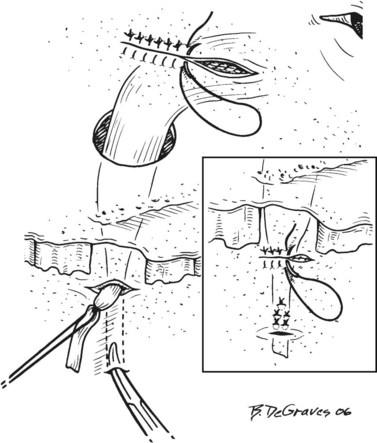
Fig. 19.42 The tendon of the levator labii superioris is tunneled subcutaneously beneath the buccotomy, exited through the buccal skin, and secured with sutures.
(From Brink P. Levator labii superioris muscle transposition to treat oromaxillary sinus fistula in three horses. Vet Surg 35:596–600, 2006.)
A drain tube is placed in the space formerly occupied by the levator labii superioris muscle (Fig. 19.43). One end of the drain exits a stab incision created about 1 cm rostral to the end of the incision created over the tendon of the levator labii superioris. Another drain is placed subcutaneously at the maxillary incision. One end of this drain exits a stab incision created 1–2 cm ventral to the rostral end of the maxillary incision, and the other end exits a stab incision created 1–2 cm ventral to the caudal end of the maxillary incision (Fig.19.43). Each end of each drain is secured with a simple-interrupted skin suture. If the sinuses must be lavaged, a Foley catheter is placed into the ipsilateral caudal maxillary sinus or conchofrontal sinus through a small trephine portal.
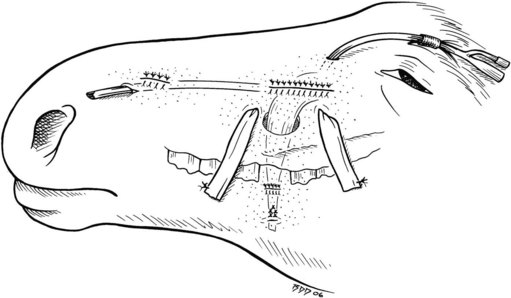
Fig. 19.43 This figure shows surgical drains placed subcutaneously and a Foley catheter placed into the paranasal sinuses for lavage of the sinuses.
(From Brink P. Levator labii superioris muscle transposition to treat oromaxillary sinus fistula in three horses. Vet Surg 35:596–600, 2006.)
The ventral buccal incision, through which the tendon of the levator labii superioris muscle protrudes, is left unsutured to heal by second intention. The other incisions are closed in two layers. A Stent bandage, composed of sterile gauze sponges, is sutured over the maxillary incision with heavy, non-absorbable suture. Any space at the oral aspect of the alveolus unoccupied by muscle is filled with a dental acrylic.
The drains in the rostral wound and the maxillary wound are removed when drainage ceases. The Stent bandage is removed after 3 or 4 days, and skin sutures are removed at 2 weeks. The paranasal sinuses are lavaged once or twice daily until lavage is no longer required. The portion of muscle located within the oral cavity sloughs at about a week, and is removed through the oral cavity, after cutting the sutures anchoring the tendon to the ventral buccal incision. The portion of muscle within the alveolus remains vital.
Transposing the levator labii superioris muscle and its tendon does not appear to have deleterious effects on labial and nasal function, but care should be taken when performing a lateral buccotomy to avoid damaging the dorsal buccal branch of the facial nerve because permanent damage to this branch of the facial nerve results in permanent flaccidity of the lip. Care should also be taken to avoid damage to the duct of the parotid salivary gland.
Sinocutaneous fistula
A sinocutaneous fistula is a permanent defect that extends from the skin into the paranasal sinuses (Fig. 19.44). Those that occur in horses are most commonly the result of an open, comminuted fracture involving facial bones, but they can also result when a sinus flap or trephine portal fails to heal.

Fig. 19.44 This horse has a permanent defect (i.e., sinocutaneous fistula) that extends from the skin into the paranasal sinuses.
Full-thickness defects over the sinuses decrease in size after injury by centripetal movement of the tissue surrounding the defect. When the defect is large, the skin heals to the mucosa of the sinus, forming a completely epithelialized surface that prevents the defect from closing completely. The size of the defect can sometimes be decreased by incising the mucocutaneous margin of the fistula and elevating the surrounding skin to initiate contraction of the wound. A sinocutaneous fistula that cannot be healed in this manner can be healed using transposed muscle, such as the temporalis muscle,76 the levator nasolabialis muscle,77 or the levator labii superioris muscle,75 or by covering the fistula with periosteum reflected from the margin of the fistula.78
Muscle transposed to cover a sinocutaneous fistula provides vascularized tissue to the wound that is capable of accepting a rotational skin flap or a free skin graft. The temporalis muscle is in close proximity to a sinocutaneous fistula involving the conchofrontal sinus, and the levator nasolabialis and levator labii superioris muscles are in close proximity to a sinocutaneous fistula involving the rostral or caudal maxillary sinuses. To heal a sinocutaneous fistula by transposing a muscle, the horse is anesthetized and positioned in lateral recumbency with the side of the head containing the sinocutaneous fistula uppermost. The dorsal aspect of its head is tilted 45° using a sand bag. The mucocutaneous margin of the fistula is incised, and the margin of the skin surrounding the fistula is elevated. A skin incision is made over or close to the insertion of the muscle to be transposed, and through this incision the muscle or its tendon is transected. A locking-loop suture with long tails is placed in the severed end of the muscle or tendon, and the muscle is bluntly freed from its fascial attachments, using scissor dissection through the small incision created to expose the muscle or tendon, and through the margin of the sinocutaneous fistula. A grasping forceps is inserted and advanced subcutaneously at the margin of the fistula until it emerges at the incision created to expose the muscle to be transposed. The ends of the suture in the muscle or tendon are grasped with the forceps, and by placing traction on them, the muscle is pulled beneath skin interposed between its transected end and the sinocutaneous fistula. The fistula is covered with the transposed muscle, and the muscle is sutured to fascia surrounding the fistula. The muscle is covered with a rotational skin flap or a free, full-thickness or split-thickness, meshed or non-meshed skin graft.
A sinocutaneous fistula can be healed with one large periosteal flap that covers the fistula or two, small periosteal flaps that are joined over the center of the fistula.78 This surgery is best performed with the horse anesthetized and in lateral recumbency with the side of the head containing the fistula uppermost. The dorsal aspect of the head is tilted 45° using a sand bag, and the skin around the defect is prepared for aseptic surgery. The mucosa is separated from the skin around the mucocutaneous border of the fistula with a scalpel, and skin surrounding the fistula is freed from its underlying subcutaneous tissue. The periosteum adjacent to the fistula is exposed by creating a rotational skin flap adjacent to the fistula. A curved incision is made through the periosteum on opposite sides of the fistula, unless periosteum is available on only one side. Each incision is slightly longer than the length of the fistula and curved away from the fistula. The periosteum within the curved incision on each side is elevated toward the fistula, creating two flaps, each of which remains attached at its base, which is the border of the fistula. The periosteal flaps are sutured together with the inner, or osteogenic, layer outermost over the defect, using simple interrupted, absorbable sutures. The rotational skin flap is sutured over the periosteal flap. Subcutaneous tissue exposed by covering the defect with the rotated skin flap can be covered with a full-thickness or split-thickness, meshed or non-meshed skin graft (Fig. 19.45). The full-thickness graft is harvested from the pectoral region and the split-thickness skin graft is harvested from the ventral aspect of the abdomen. A non-adherent dressing is placed over the surgery site, and the dressing is covered with a Stent bandage or gauze pads and elastic adhesive tape. The site from which the full-thickness graft was obtained is sutured in two layers.

Fig. 19.45 Same horse as in Fig. 19.44 after sinocutaneous fistula was closed using periosteal and rotational skin flaps. Subcutaneous tissue exposed by the rotational skin flap has been covered with a full-thickness, meshed skin graft procured from the pectoral region.
The osteogenic, or cambium, layer of the periosteal flaps forms new bone, and bone denuded of periosteum to create the periosteal flaps forms new periosteum.78 Cancellous bone, harvested from the sternum or wing of the ilium, can be used to augment periosteal bone formation, but is not necessary for the successful closure of the defect. Creating two small periosteal flaps, rather than one large flap, is more effective at preserving the blood supply to the edges of the flaps, but creating two flaps may be difficult if the fistula is in an area where periosteum is available on only one side of the lesion.
1 Roberts EW. Bone physiology, metabolism, and biomechanics in orthodontic practice. In: Graber TM, Vanarsdall RL. Orthodontic practice, current principles, and techniques. 2nd edn. St Louis: Mosby; 1994:193–234.
2 Fletcher B. Orthodontic treatment, case report update. Horse Dentistry and Bitting Journal. 2008;1:18.
3 Galloway SS. An expansion screw device to facilitate eruption of a mandibular premolar in a horse. In: Proceedings of the 22nd Annual Vet Dental Forum, Jacksonville, 2008, p. 105
4 Klugh DO. Acrylic bite plane for treatment of malocclusion in a young horse. J Vet Dent. 2004;21:84–87.
5 Easley J. Equine orthodontics. In: Proceedings of the American Association of Equine Practitioners Focus on Dentistry. Indianapolis, 2006, pp 118–126
6 Wiggs RB, Lobprise HB. Veterinary dentistry principles and practice. Philadelphia: Lippincott-Raven; 1997.
7 Nanci A. Ten Cate’s Oral histology, development, structures and function, 6th edn. St Louis: Mosby; 2003.
8 Wolff J, The law of bone remodeling. (Translation of 1892 German edition.), Verlag Springer, New York, 1986.
9 Graber TM. Functional appliances in orthodontics. In: Graber TM, Vanarsdall RL. Orthodontic practice, current principles, and techniques. 2nd edn. St Louis: Mosby; 1994:383–436.
10 Musich DR. Orthodontics and orthognathic surgery. In: Graber TM, Vanarsdall RL. Orthodontic practice, current principles, and techniques. 2nd edn. St Louis: Mosby; 1994:835–907.
11 Schumacher J, Brink P, Easley J, Pollock P. Surgical correction of wry nose in four horses. Vet Surg. 2008;37:142–148.
12 Tucker MR. Correction of dentofacial deformities. In: Peterson LJ, Hupp J, Ellis E, III., Tucker MR. Contemporary oral and maxillofacial surgery. 2nd edn. St Louis: Mosby; 1993:613–656.
13 Valdez H, McMullan WC, Hobson HP, Hanselka DV. Surgical correction of deviated nasal septum and premaxilla in a colt. J Am Vet Med Assoc. 1978;173:1001–1004.
14 Verwilghen D, Galen G, Vanderheyden L, et al. Mandibular osteodistraction as a corrective method for deep bite II malocclusions in the horse. Vet Surg. 2008.
15 Uhlinger C. Survey of selected dental abnormalities in 233 horses. Proceedings of the 33rd Annual Meeting of the American Association of Equine Practitioners, 1987, pp 577–583.
16 Joest E, Handbuch der speziellen pathogischem Anatomie der Haustere. Verlag Paul Parey, Berlin, 1970;Vol. V/I.
17 Miles AEW, Grigson C. Colyer’s Variations and diseases of the teeth of animals, rev edn. Cambridge: Cambridge University Press; 1990.
18 Dixon PM. Removal of equine dental overgrowths. Equine Veterinary Education. 2000;12(2):68–81.
19 Dixon PM, The gross, histological and ultrastructural anatomy of equine teeth and their relationship to disease. Proceedings of 48th Annual Convention of the American Association of Equine Practitioners, 2002:421–437.
20 Dixon PM, Tremaine WH, McGorum BC, et al. Equine dental disease – a long term study of 400 cases, part 1: Introduction and disorders of incisor, canine and first premolar teeth. Equine Vet J. 1999;31:369–377.
21 Dixon PM, Tremaine WH, McGorum BC, et al. Equine dental disease – a long term study of 400 cases, part 2: Disorders of development, eruption and variations in position of cheek teeth. Equine Vet J. 1999;31:519–528.
22 Baker GJ. Oral diseases of the horse. In: Harvey CE, ed. Veterinary dentistry. Philadelphia: WB Saunders; 1985:220–221.
23 Faragella F. Rotated maxillary fourth premolar in a horse. J Vet Dent. 2004;21:226–227.
24 Earley ET. How to manage maleruptions of the upper forth premolars in the miniature horse. Proceedings of the 53rd Annual Convention of the American Association of Equine Practitioners, 2007, pp 487–497
25 DeBowes RM, Brachygnathia. Philadelphia. White AN, Moore JN, Lippincott JB. Current practice of equine surgery, 1990:469–472.
26 McIlwraith CW. Equine digestive system. In: Jennings PB, ed. The Practice of large animal surgery. Philadelphia: WB Saunders; 1984:558–560.
27 Burdach J, Mooney MP. The relationship between lip pressure following lip repair and craniofacial growth: an experimental study in beagles. Plastic and Reconstruction Surgery. 1984;73(4):544–555.
28 Petrovik AG, Experimental and cybernetic approaches to the mechanism of action of functional appliances of mandibular growth. (monograph). McNamara JA, ed. Malocclusion and the periodontium, Cranial Growth Series, 1984:15.
29 Easley J. Basic equine orthodontics. In: Baker GJ, Easley J. Equine dentistry. 2nd edn. Edinburgh: Elsevier; 2005:249–266.
30 Crowe MW, Swerczek TW. Equine congenital defects. Am J Vet Res. 1985;46:353–358.
31 Vandeplassche M, Simoens P, Bouters R, et al. Aetiology and pathogenesis of congenital torticollis and head scoliosis in the equine foetus. Equine Vet J. 1984;16:419–424.
32 McNamara JA. Neuromuscular and skeletal adaptations to altered function in the orofacial region. American Journal of Orthodontics. 1973;64:136. 189, 578
33 McNamara JA. Functional determinants of craniofacial and shape. European Journal of Orthodontics. 1980;2:131.
34 Hennet PR, Harvey CE. Craniofacial development and growth in the dog. Journal of Veterinary Dentistry. 1992;9(2):11–18.
35 Harvey CE, Penny RHC. Oral and dental diseases in pigs. In: Harvey CE, ed. Veterinary Dentistry. Philadelphia: WB Saunders; 1985:481–551.
36 Angle EH. The angle system of regulation and retention of the teeth and treatment of fractures of the maxillae, 5th edn. Philadelphia: SS White Manufacturing; 1899.
37 Hennet PR, Harvey CE, Emily PP. The angle classification of malocclusion: is it appropriate for use in veterinary dentistry? Journal of Veterinary Dentistry. 1992;9(3):10–12.
38 Academy of Veterinary Dentistry. Dental abbreviations, Equine dental abbreviations Suppl, 2007, pp 15–17
39 Carmalt JL. Understanding the equine diastema. Equine Veterinary Education. 2003;5(1):43–44.
40 Greene S, Basile JP, Recognition and treatment of equine periodontal disease. Proceedings of the 48th Annual Convention of the American Association of Equine Practitioners, 2002:463–466.
41 Vlaminck L, Post-extraction molariform tooth drift and alveolar grafting in horses. PhD thesis, University of Ghent, Ghent, 2007. pp 209–223
42 Vlaminck L, Hays L, Maes D, et al. Use of a synthetic bone substitute to retard moliform tooth drift after maxillary tooth loss in ponies. Vet Surg. 2006;35(7):587–588.
43 Carmalt JL, Townsend HGG, Allen LA. Effect of dental floating on the rostrocaudal mobility of the mandible of horses. J Am Vet Med Assoc. 2003;23:666–669.
44 Lear TL, Cox JH, Kennedy GA. Autosomal trisomy in a thoroughbred colt: 65, XY, +31. Equine Vet J. 1997;31(1):85–88.
45 McLaughlin GB, Doige LE. Congenital musculoskeletal lesions and hyperplastic goiter in foals. Canadian Veterinary Journal. 1981;22:130.
46 Becker E. Zähne. In Handbuch der speziellen pathologischen Anatomie der Haustiere, 3rd edn, Berlin: Verlag Paul Parey; 1970:83–313.
47 Duke A. Equine bit analysis. Annual Conference of American Veterinary Dental Society, Handout notes. New Orleans, 1989
48 Boero M. Correction of brachygnathism in foals. In: Allen T, ed. Manual of equine dentistry. St Louis: Mosby; 2003:173.
49 Pence P, Wilewski K. Newborn, weanling and adolescent horse dentistry. In: Pence P, ed. Equine dentistry: a practical guide. Lippincott. Baltimore: Williams and Wilkins; 2002:115–139.
50 Dixon PM, Hawkes C, Townsend W. Complications of equine oral surgery. Vet Clin North Am Equine Pract. 2009;24:499–514.
51 Jayo M, Leipold HW, Dennis SM, Eldridge FE. Brachygnathia superior and degenerative joint disease, a new lethal syndrome in Angus calves. Veterinary Pathology. 1987;24:148–155.
52 Mitz C, Allen T. Dentistry in miniature horses. In: Allen T, ed. Manual of equine dentistry. St Louis: Mosby; 2003:175–192.
53 Pence P, Mitz C. Miniature horse dentistry. In: Pence P, ed. Equine dentistry: a practical guide. Baltimore: Lippincott, Williams, and Wilkins; 2002:191–199.
54 Baker GJ. Problems involving the mouth. In: Reed S, Bayly W. Equine internal medicine. Philadelphia: WB Saunders; 1998:605.
55 Easter JL, Watkins JP. Diseases of the head and neck. In: Colahan PT, Merritt AM, Moore JN, Mayhew JG. Equine Medicine and Surgery. St Louis: Mosby; 1999:1669.
56 Stashak TS. Equine wound management. Philadelphia: Lea and Febiger; 1991.
57 American Veterinary Medical Association Membership Directory. Principles of veterinary medical ethics of the AVMA (1999 revision) IV. Therapies, Genetic Defects, 2003, 36
58 Schumacher J, Dutton DM, Murphy DJ, et al. Paranasal sinus surgery in sedated, standing horses. Vet Surg. 2000;29:173–177.
59 Doherty T, Valverde A. Management of sedation and anesthesia. In: Doherty T, Valverde A. Manual of equine anesthesia and analgesia. Ames, Iowa: Blackwell; 2006:206–208.
60 Quinn GC, Kidd JA, Lane JG. Modified frontonasal sinus flap surgery in standing horses: surgical findings and outcomes of 60 cases. Equine Vet J. 2005;37:138–142.
61 Schumacher J, Honnas C, Smith B. Paranasal sinusitis complicated by inspissated exudate in the ventral conchal sinus. Vet Surg. 1987;16:373–377.
62 Richardson DW, Evans LH, Tulleners EP. Rostral mandibulectomy in five horses. J Am Vet Med Assoc. 1991;199:1179–1182.
63 Schumacher J, Kemper DL, Helman RG, Edwards JL. Removal of the premaxillae of a horse. J Am Vet Med Assoc. 1996;209:118–119.
64 Baker GJ. Abnormalities of development and eruption. In: Baker GJ, Easley J. Equine dentistry. Philadelphia: WB Saunders; 1999:49–59.
65 McKellar GM, Collins AP. The surgical correction of a deviated anterior maxilla in a horse. Australian Veterinary Journal. 1993;70:112–114.
66 Doyle AJ, Freeman DE. Extensive nasal septum resection in horses using a 3-wire method. Veterinary Surgery. 2005;34:167–173.
67 Tulleners EP, Raker CW. Nasal septum resection in the horse. Veterinary Surgery. 1983;12:41–47.
68 Auer JA. Craniomaxillofacial disorders. In: Auer JA, Stick JA. Textbook of equine surgery. 3rd edn. Philadelphia: Elsevier; 2006:1341–1362.
69 Puchol JL, Herrán R, Durall L, et al. Use of distraction osteogenesis for the correction of deviated nasal septum and premaxilla in a horse. J Am Vet Med Assoc. 2004;224:1147–1150.
70 Baker GJ. Some aspects of equine dental disease. Equine Vet J. 1970;2:105–110.
71 Orsini PG, Ross MW. Retrospective study of tooth root abscesses in 110 horses. Proceedings of the 16th Annual Veterinary Surgical Forum, 1988
72 Dixon PM, Hawkes C, Easley J. Standing treatment of oronasal and orosinus fistulas. Proceedings of the American College of Veterinary Surgeons ACVS Symposium Equine and Small Animal, 2007
73 Prichard MA, Hackett RP, Erb HN. Long-term outcome of tooth repulsion in horses: a retrospective study of 61 cases. Vet Surg. 1992;21:145–149.
74 Orsini P, Ross M, Hamir A. Levator nasolabialis muscle transposition to prevent an orosinus fistula after tooth extraction in horses. Vet Surg. 1992;21:150–156.
75 Brink P. Levator labii superioris muscle transposition to treat oromaxillary sinus fistula in three horses. Vet Surg. 2006;35:596–600.
76 Campbell ML, Peyton LC. Muscle flap closure of a frontocutaneous fistula in a horse. Vet Surg. 1984;13:185–188.
77 Dart A, Best P, Peatfield J. Reconstruction of a maxillary sinus defect in a horse using a levator nasolabialis muscle flap. Australian Veterinary Journal. 1994;71:379–380.
78 Schumacher J, Auer J, Shamis L. The use of periosteal flaps to repair facial defects in two horses. Vet Surg. 1985;14:235–239.