5 The thorax
At the end of this chapter you should be able to
1. Find, recognize and name the constituent bony components of the thorax, including the clavicle, scapula, ribs and vertebrae, noting their size and position.
2. Palpate many of the bony features, being able to relate one to another.
3. Locate, name or number the spines and transverse processes of all the thoracic vertebrae.
4. Recognize and palpate all 12 of the ribs, noting their extent.
5. Name all the joints in which the clavicle, scapula, ribs, sternum and vertebrae are involved and palpate the joint lines where possible.
6. Give the class and type of all the joints named.
7. Demonstrate any accessory movements which may be possible in the joints of the thorax.
8. Locate and name the muscles which cover the thorax.
9. Draw the shape of the muscle on the surface and give its attachments.
10. Demonstrate the actions of all of the muscles covering the thorax.
11. Describe the position and attachments of the diaphragm.
12. Give an account of its actions and functional significance.
13. Demonstrate the cutaneous distribution of the thoracic nerves, giving an outline of the course each takes.
14. Describe the arrangement of chambers in the heart.
15. Give the surface markings of the main boundaries of the heart.
16. Describe the arrangement of the main arteries in the thorax, giving their surface markings.
17. Describe the arrangement of the main veins in the thorax, giving their surface markings.
Bones
The thoracic cage
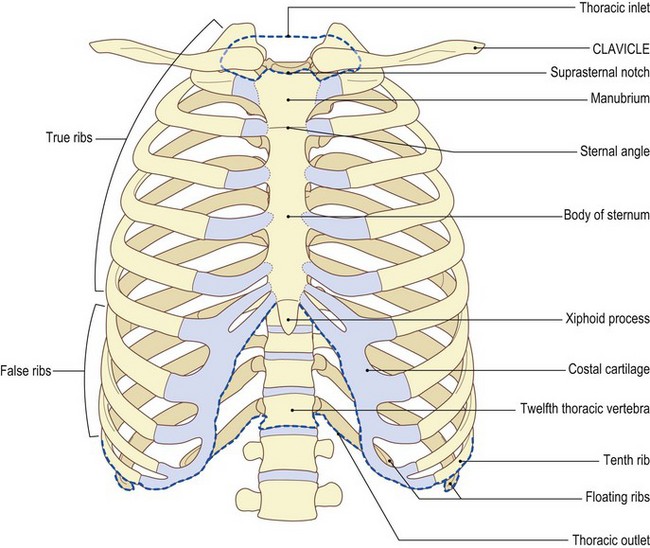
The bony structure of the thoracic cage consists of:
• the sternum [stereos (Gk) = solid, hard] anteriorly
• the twelve thoracic vertebrae [vertebra (L) = joint; from verto – I turn] posteriorly, the first thoracic vertebra being the smallest and the twelfth the largest (see Figs 5.2–5.4), and
• the twelve ribs on either side linking the vertebrae with the sternum.
The sternum is angled forward at the manubriosternal joint and angled backwards at the xiphisternal joint, forming a concavity backwards. The ribs are concave inwards and the vertebral column is concave forwards in this region. This forms a large cavity for the protection of vital organs such as the heart and lungs.
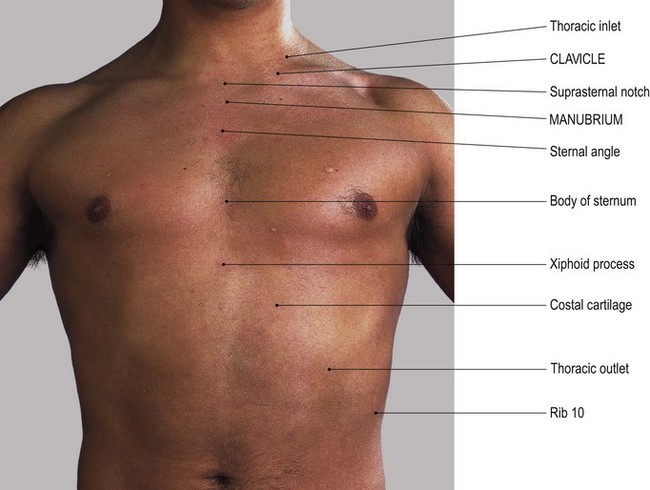
The rib spaces are filled with a musculofibrous sheet made up of the intercostal muscles and membrane. This forms a sealed unit in front, to the sides and behind. There are, however, openings at the top and bottom. The former is smaller and consists of the first thoracic vertebra posteriorly, the first rib on either side and the manubrium sterni anteriorly. This is termed the ‘thoracic inlet’. Below there is a much larger opening: the ‘thoracic outlet’. This comprises the twelfth thoracic vertebra posteriorly, the xiphoid anteriorly and the costal cartilages of ribs 7, 8, 9 and 10, the tip of rib 11 and the full length of rib 12.
The sternum
The sternum lies centrally at the front of the chest. It comprises three flat plates of bone: the manubrium [manubrium (L) = a handle; the sternum, as a whole, resembles a sword] superiorly, the body centrally and the pointed xiphoid [xiphos (Gk) = a sword] process inferiorly. The xiphoid usually remains cartilaginous until approximately 40 years of age.
The clavicle and scapula
The clavicle lies almost horizontal, articulating with the superolateral part of the manubrium. Posterolaterally the scapula rests on the second to eighth ribs, with the acromion at the lateral end of the spine articulating with the lateral end of the clavicle at the acromioclavicular joint (see Fig. 2.7).
Palpation
For palpation in this region, the model can be in either the sitting or standing position.
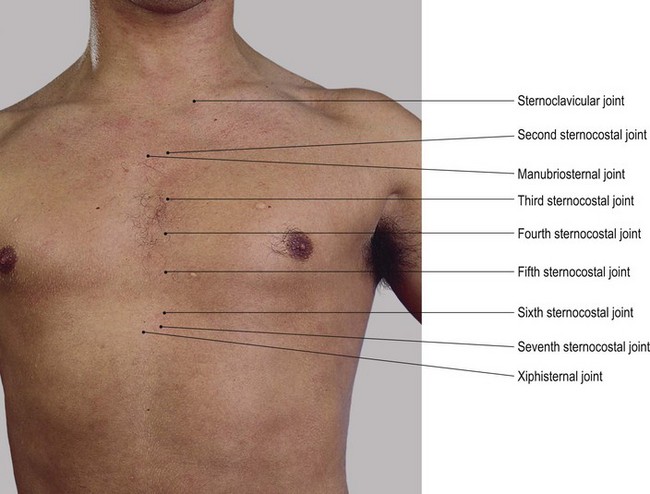
• The suprasternal notch. Identify the suprasternal notch which can be located at the upper border of the manubrium (Fig. 5.1a, b).
• The medial ends of the clavicle. On either side of the suprasternal notch, palpate the medial ends of the clavicle which project above the line of the manubrium sterni.
• The first rib. Just below the medial end of the clavicle, find the enlargement at the lateral end of the manubrium sterni. This is actually the anterior end of the first rib.
• The sternocostal joint. With careful palpation, you will be able to locate the joint between the first rib and the manubrium sterni running vertically, concave laterally 1 cm below and 1 cm lateral to the medial end of the clavicle.
• The manubriosternal joint (sternal angle). Trace down the anterior surface of the manubrium until you find a raised horizontal line. This is where it joins the body of the sternum at the manubriosternal (sternal angle) joint (Fig. 5.1a, b). The reflex angle between the manubrium and body of the sternum is of the order of 200°, changing some 5–7° between full inspiration and full expiration.
• The costal cartilages of the second ribs. On either side of the manubriosternal junction the costal cartilages of the second ribs can be palpated, with the lateral border of the manubrium just above.
• Ribs 3–6. Continue to trace down either side of the sternum and identify the third to sixth ribs and their costal cartilages with the lateral border of the sternum lying between their medial ends.
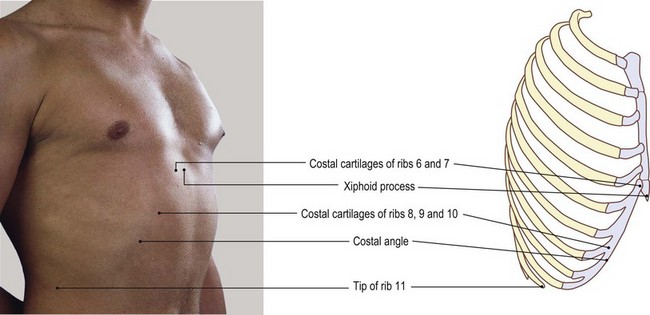
• The xyphoid process of the sternum. The sternum narrows inferiorly and usually dips inwards to join the cartilaginous xiphoid process. The costal cartilage of the seventh rib usually articulates with the sternum at the xiphisternal junction.
• Note 1. The whole of the sternum is subcutaneous and is commonly used to take samples of bone marrow.
• Note 2. The xiphoid process varies in its formation: it may appear to be pointed, double pointed or even rounded. Normally it projects forwards and can therefore easily be palpated. Occasionally it projects downwards and backwards and is then difficult to palpate.
The vertebrae
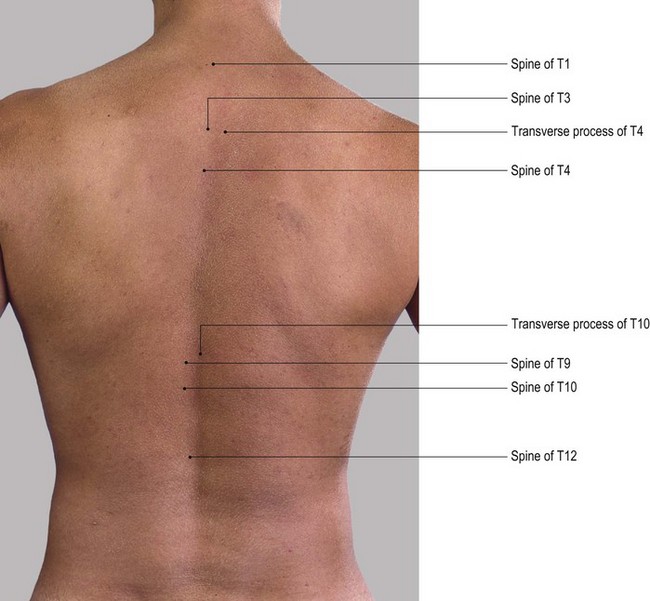
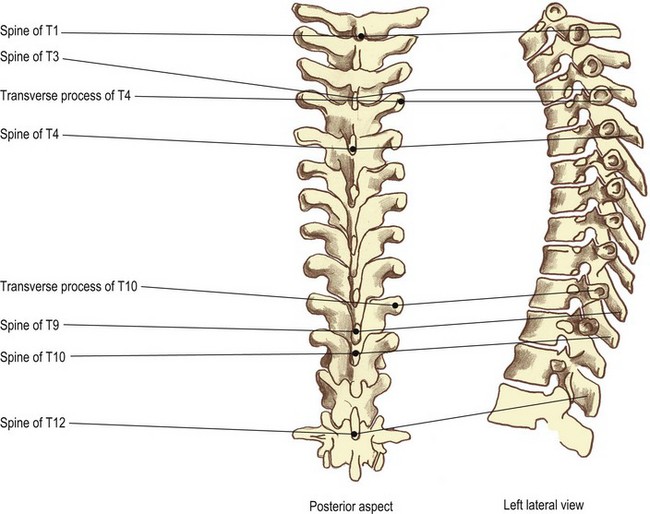
The thoracic part of the vertebral column can only be palpated posteriorly where it presents spines and transverse processes. These either overlap each other or are covered with strong, thick muscles and fascia, and so prove difficult to identify, even by an experienced practitioner.
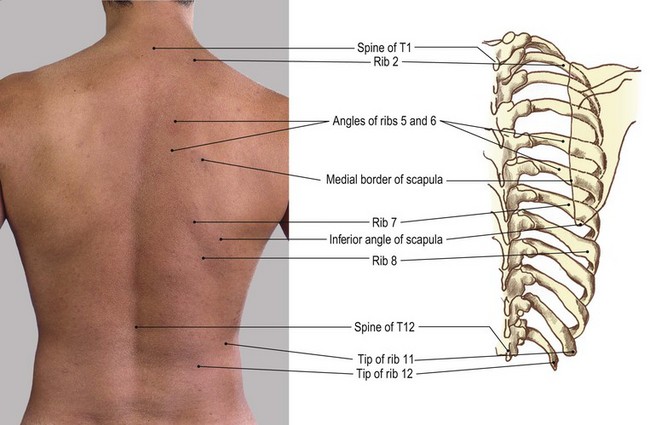
The spines form a line of tubercles down the midline of the thorax. They are not uniform in length but pass downwards and backwards with a tendency to overlap the spine below. The tips of those near the upper part of the thorax are level with the upper surface of the vertebral body below. The lower vertebrae have longer spines which reach to the lower border of the vertebra below. The tip of the spine of T3 is roughly level with the root of the spine of the scapula; that of T7 is level with the inferior angle of the scapula. The spine of T12 is atypical as it is squared posteriorly and resembles that of a lumbar vertebra. It is level with the disc between T12 and L1. Accurate location of these spines must therefore be carried out by palpation. The usual method is to count down from an identifiable point above or below.
The transverse processes are much more difficult to palpate as they are covered by strong, thick muscles even in the leaner subject. The tips of the transverse processes are level with the upper border of their own vertebral body (Fig. 5.2).
Palpation
For palpation in this region, the model is in the slump sitting position.
• The thoracic spines. The back is rounded by asking the model to place the chin on the chest. In this position, the tips of the spines become more identifiable.
• The spines of C7 and T1. First, identify the spines of C7 and T1: these are the two most prominent spines at the base of the neck.
• The thoracic spines. Carefully count down the tips of the spines, being sure to mark the upper spine with the fingers of one hand while seeking the spine below with the other. Each spine will feel quite pointed until the level of T12 where the spine becomes flattened. This is because the spine has features similar to those of a lumbar vertebra.
• Note. If you find that palpation is difficult, use the technique suggested on p. 6 where the fingertips are moved rapidly up and down the spine, in a scanning manner. This method of palpation is useful for locating and mapping structures which lie below the surface. It is, however, rarely used, as it gives the impression of merely moving the skin on the underlying structures. It amounts to the building up of a total picture by adding together many disparate pieces of information. Use the pads of all fingers of one hand (the most sensitive) if possible, to sweep across an area, allowing your fingers to move the skin and superficial fascia on the deeper structures. By using this technique, you will be building up a picture similar to that which would be achieved by the scanning beam of a video camera. Use the other hand to mark certain points and mark from where the previous information was obtained. More refined palpatory techniques can then be used on selected areas.
• The lateral tips of the thoracic transverse processes. These lie 3 cm lateral and parallel to the spines.
• Note. The tip of the spine lies 1 cm below the level of the transverse process of the vertebra below. This measurement remains constant because the shorter spines in the upper thorax are compensated for by the transverse processes being slightly raised.
• The costotransverse joints. Lateral to the tips of the transverse processes is a groove marking the line of the costotransverse joints.
The ribs (Fig. 5.3)
There are 12 ribs on either side. They are convex outwards, the eighth being the longest and the twelfth the shortest. The upper seven ribs articulate with the vertebral bodies and transverse processes posteriorly by the facets on their heads and tubercles. The first, tenth, eleventh and twelfth ribs have only one facet; the rest have two. The eleventh and twelfth ribs have no tubercles. Ribs 1–7 articulate with the sternum anteriorly via a varying length of costal cartilage. These are termed ‘true’ ribs. Ribs 8–10 articulate anteriorly via their costal cartilage, with the costal cartilage above, and are termed ‘false’ ribs. Ribs 11 and 12 do not articulate with their transverse process posteriorly and are free anteriorly. They are therefore termed ‘floating’ ribs (see Fig. 5.1).
Palpation
To facilitate the palpation of the ribs, the back muscles need to be relaxed. This is best achieved if the model is in the prone lying position.
• The posterior section of the ribs. Just lateral to the tip of each transverse process the posterior section of each rib can be palpated, being separated from the transverse process by a depression.
• Ribs 1–10. Ask the model to hang the arm over the side of the plinth (i.e. the pectoral girdle is in protraction). Now find and trace the first to tenth ribs laterally. The rib angle lies approximately 3–4 cm lateral to the tips of the transverse processes. It can readily be palpated in the mid-thoracic region, becoming less clear above and below. The first rib does not possess an angle and those of the eleventh and twelfth ribs are slight if present.
• Ribs 1–12 and the intercostal spaces. Each rib, together with the intercostal spaces above and below, can be traced anteriorly to where it joins the sternum. The second to seventh or eighth ribs are usually hidden posterolaterally by the scapula, while the eleventh and twelfth ribs only exist posterolaterally.
• The first rib. This rib is the most difficult to palpate. It lies deep to the clavicle anteriorly and deep to the trapezius and levator scapulae muscles posteriorly. If you apply deep pressure immediately below the clavicle, 1 cm lateral to its medial end, you will be able to palpate the junction of the rib with the manubrium. By applying deep pressure above the middle of the clavicle in the supraclavicular fossa, it is possible to feel the lateral border of the first rib.
• Note. This area is particularly tender and may produce unpleasant reactions in the upper limb due to pressure on the trunks of the brachial plexus and subclavian artery.
• The neck and tubercle of the first rib. Posteriorly, the neck and tubercle of the first rib can be palpated running downwards and laterally approximately 2 cm lateral to the tip of the spine of C7. This, however, is dependent on the thickness of the upper fibres of trapezius.
• Ribs 8–10 and the costal angle. The costal cartilages at the anterior end of the eighth to tenth ribs form the anterior part of the costal margin, running superomedially to join the xiphoid process. At the level of the ninth costal cartilage an angle and projection are formed: the ‘costal angle’. This lies on a level with the transpyloric plane, in common with the spine of L1 and the tip of the twelfth rib.
• Ribs 11 and 12. Just above the twelfth, the eleventh rib can easily be identified, ending in a point just anterior to the mid-axillary line.
Joints
The thoracic vertebral column (Fig. 5.4)
The joints of the thoracic vertebral column are similar to those in the cervical region. They do not, however, possess uncovertebral joints. They do have facets on the side of all of the bodies and the upper 10 transverse processes for the articulation of the ribs. The vertebral bodies articulate centrally by a series of intervertebral discs. These joints are complex cartilaginous symphyses. The intervertebral discs are made up of an outer ring of fibrous bands passing obliquely from one body to the other (the annulus fibrosus) and a central nucleus (the nucleus pulposus) composed of a soft highly hydrophilic substance. These discs are supported by many ligaments, including the very strong anterior and posterior longitudinal ligaments.
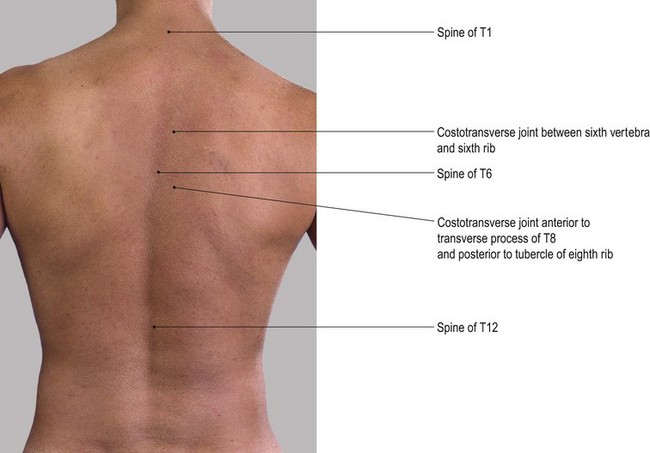
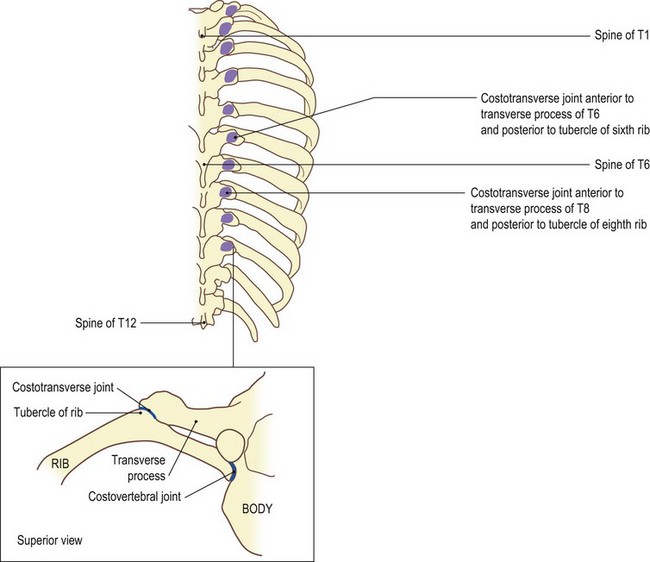
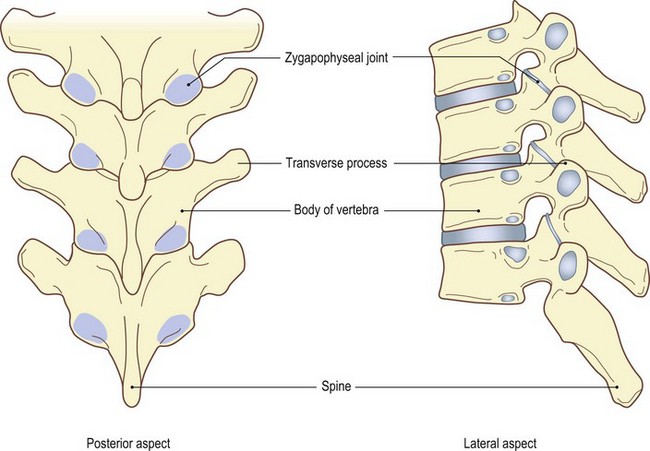
Fig. 5.4 (d, e) Zygapophyseal joints of thoracic spine. Shaded areas show joint surface deep to inferior articular processes
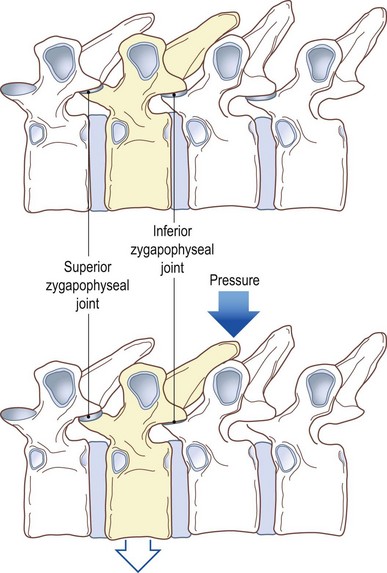
Fig. 5.4 (f, g) Vertebrae in horizontal position showing effect of pressure on spine in direction of arrow
On either side are the zygapophyseal joints (Fig. 5.4d, e) between the articular facets, two above and two below. In addition there are costovertebral joints (Fig. 5.4c) between the heads of the ribs and the side(s) of the body of the vertebrae and costotransverse joints between the tubercle of the rib and the transverse process (Fig. 5.4 a–c). The zygapophyseal, costovertebral and costotransverse joints are all synovial, surrounded by a capsule which is lined with synovial membrane and supported by ligaments. (For detailed study refer to Palastanga et al 2002.)
Palpation
All but the costotransverse and possibly the zygapophyseal joints are impossible to palpate.
For palpation in this region, the model is in the prone lying position with the forehead resting on the backs of the hands.
• The costotransverse joints. These joints lie in the furrow between the transverse processes and the ribs. They can be located either by following backwards along the line of a known rib to the point where it is obscured by the transverse process or finding the tip of the spinous process of a known vertebra and tracing out laterally to the furrow mentioned above.
• Note. Due to the length of the spines in the thoracic area, the transverse process you can feel is that of the vertebra below.
• The laminae of the thoracic spines. The joints between the articular facets of the thoracic vertebrae lie at the upper edge of the lamina as it meets the lamina above. The joint is virtually impossible to palpate but the lamina can be traced a little laterally from the spines. Slip your fingers down the side of the spinous process. Note that the lamina you feel is that of the vertebra below.
Accessory movements
As stated above, pressure on the lamina of one vertebra can part the zygapophyseal joint surfaces above and compress those below on the ipsilateral side (Fig. 5.4c).
• Posterior-to-anterior pressure to a thoracic spine. Applying this technique to the tip of a thoracic spine causes it to act as a lever, parting the upper zygapophyseal joint and compressing the lower (Fig. 5.4f, g).
• Lateral pressure. Pressure applied to the lateral side of the spinous process causes rotation of the body of the vertebra to the opposite side. This results in gapping of the upper zygapophyseal joint on the side to which the spine is moved, but compressing the lower joint. It has the opposite effect on the joints of the ipsilateral side.
• Traction. Traction on the thoracic intervertebral joints is difficult to produce, resulting in virtually no movement. To a limited extent, movement certainly does occur during lumbar or cervical traction.
• Pressure on the rib angles. Laterally, the heads of the ribs articulate with the bodies of the vertebrae; the tubercles of the ribs articulate with the transverse processes of the vertebrae (Fig. 5.4). Pressure on the angle of the rib will part the costotransverse joint. If you move your thumbs slightly medially to an area just lateral to the joint, the gapping is increased.
• Note. If you apply pressure even more medially, it will encroach upon the back of the transverse process, producing exactly the opposite effect and resulting in compression of the costotransverse joint (Fig. 5.4c).
The joints of the anterior end of the ribs
Anteriorly, the upper seven ribs articulate with the sternum via their costal cartilages. These are termed true ribs. The costal cartilages of ribs eight to ten articulate with the costal cartilage above and are termed false ribs. The two lower ribs are only capped with costal cartilage and do not link up with the sternum and are termed floating ribs.
There are three sets of joints in this area: the costochondral, the interchondral and the sternocostal joints.
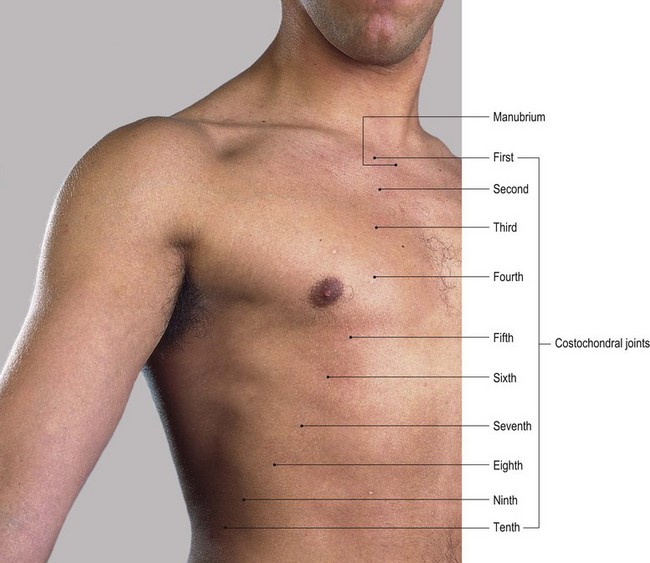
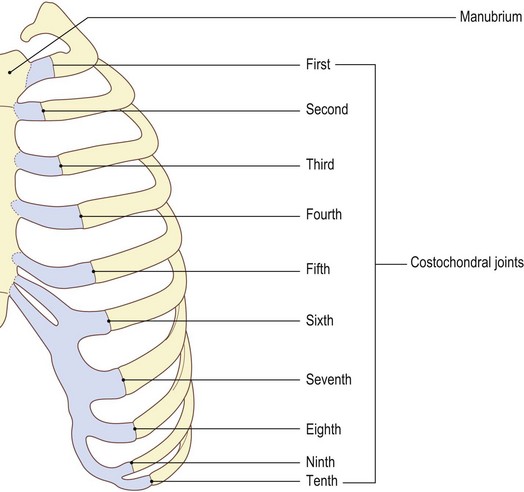
The costochondral joints
These joints are really the junction between the rib and its cartilage. The rounded end of the cartilage fits into the depressed roughened end of the rib. Its periosteum is continuous with its perichondrium.
Palpation
• The costochondral joints (Fig. 5.5a, b). These joints can be identified in some subjects. They lie approximately 3 cm lateral to the sternum at the second rib, progressing to some 12 cm from the xiphoid at the seventh rib and approximately 18 cm from the xiphoid process at the tenth rib.
• Note. Pressure on the anterior surface of these joints can often be unpleasant and too much palpation may lead to the area becoming very tender, the symptoms lasting for some time.
Accessory movements
The model is in the supine lying position.
• Compression of the joints. Applying pressure to the sternal area of the chest achieves quite marked compression of the joints. This is due in part to the flexibility of the ribs and costal cartilage and in part to the slight gliding and bending movements occurring between the costochondral, interchondral, sternocostal and intersternal joints.
• Movement of individual joints. It is possible to produce movement of each individual joint. Using two thumbs, apply pressure to the rib or to the costal cartilage close to either side of the joint. The movement is minimal in some joints, such as that of the first and second ribs with the sternum. It is quite considerable lower down the thorax, particularly at the interchondral joints.
• Note. Some of these joints can be traumatized and become inflamed. This is usually following a blow on the chest or stress on the rib cage due to resting heavily against a beam or bar. This produces acute pain over that area of the chest. If the pain is over the area of the heart, it may erroneously be associated with a heart attack.
The sternocostal (chondrosternal) joints (Fig. 5.5c, d)
These are the joints between the anterior rounded end of the costal cartilages of the upper seven ribs and the small hollow cavities on the side of the sternum.
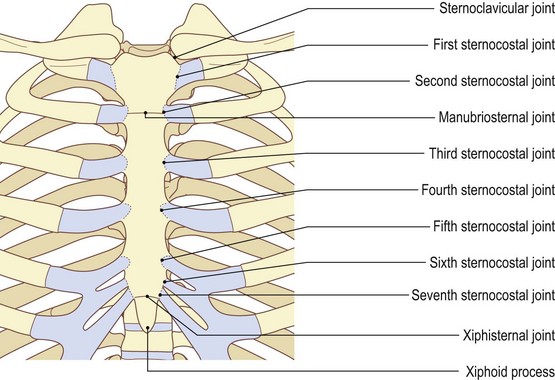
The first articulates with the side of the manubrium just below the clavicular notch. It is a synarthrosis and has a similar structure to a symphysis, so forming a fairly rigid union. It is close to the midline of the body, a location where most symphyses are found.
The second to the seventh are all synovial joints. They are surrounded by a capsule which is lined with synovial membrane and supported by ligaments that radiate from the front of the cartilage on to the anterior aspect of the sternum (the sternocostal radiate ligaments). The second costal cartilage joins the sternum at the side of the manubriosternal joint. It has the extra support of an interosseous ligament which attaches to the disc of the manubriosternal joint. The seventh costal cartilage joins a small shallow facet formed by the lower part of the sternum and the xiphoid process. It is supported in front and behind by costoxiphoid ligaments. This synovial joint is often replaced by a symphysis.
Palpation
• The costomanubriosternal joint. At the side of the manubriosternal joint, approximately 7 cm below the sternal notch, you can palpate the articulation of the second costal cartilage, the manubrium (Fig. 5.5b) and body of the sternum. It is identified as a small V-shaped notch, with the concavity facing laterally.
• Ribs 3–7 and costal cartilages. Below this, on either side, the third to seventh ribs and their costal cartilages can be palpated as they articulate with the lateral border of the sternum at the costosternal or chondrosternal joints. The section of the sternum between each costal cartilage is concave laterally, being the anterior limit of the intercostal spaces.
• The manubriocostal joint. The joint between the first rib and the manubrium lies 1 cm below, and 1 cm lateral to, the medial end of the clavicle and is more difficult to identify. You can, however, palpate the anterior limit of the rib.
• Ribs 8–10 and their costal cartilages. The costal cartilage of the eighth to tenth ribs can be identified. They articulate medially, with the costal cartilage above, at the interchondral joints and form the costal margin.
Joints of the sternum
The sternum is composed of three segments: the manubrium superiorly, the body centrally, and the small, pointed xiphoid process inferiorly. The joints between these sections are secondary cartilaginous symphyses.
Palpation
• The manubriosternal joint (Fig. 5.5c, d). This joint is easy to identify. It is approximately 7 cm below the upper border of the sternum at the sternal angle. It is level with the articulation of the second costal cartilage with the sternum.
• The xiphisternal joint (Fig. 5.5c, d). The joint between the body and the xiphoid process is more difficult to palpate, although the body and the xiphoid are both easily identifiable.
Accessory movements
• Bilateral pressure. There is very little accessory movement of the manubriosternal joint, although pressure on either the body or the manubrium, close to the joint, will produce slight angling of the two sections.
• Anterior-posterior pressure. At the xiphisternal joint, however, the xiphoid process can normally be moved backwards some considerable distance by pressure applied to its anterior surface. This produces an angling at the joint.
Muscles
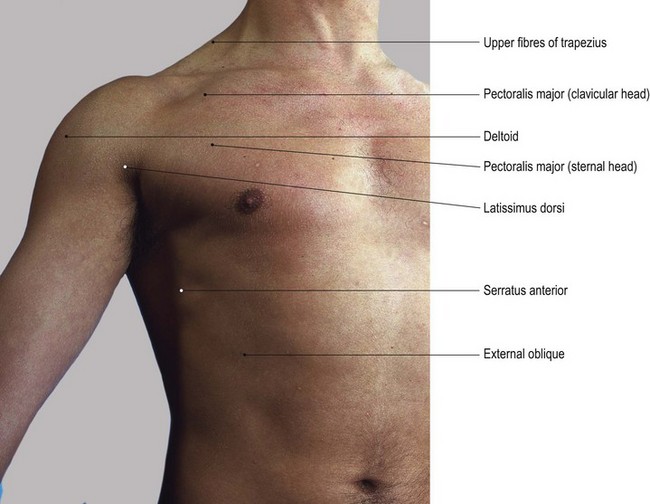
The anterior aspect of the chest
The muscle that dominates the upper part of the chest is pectoralis major. Lying deep to it are pectoralis minor and the upper intercostal muscles. In the lower part of the chest, rectus abdominis and the external oblique muscle of the abdomen have their upper attachment (see Fig. 6.5).
Pectoralis minor is a triangular muscle. Its base attaches to the third, fourth and fifth ribs at approximately the mid-clavicular line; its apex attaches to the coracoid process of the scapula. It is very difficult to palpate. The intercostal muscles attach to the lower border of the rib above and to the upper border of the rib below. They are easier to palpate in the lower region of the chest (see p. 199).
The external oblique muscle attaches above to the external surface of the lower border of the lower eight ribs.
The rectus abdominis attaches above to the fifth, sixth and seventh costal cartilages just lateral to the sternum.
Palpation
• Rectus abdominis. Place your fingers just below the rib cage just lateral to the xiphoid process. Now ask the model to raise the head. Immediately the powerful contraction of the muscle will be palpated. (See also p. 229.)
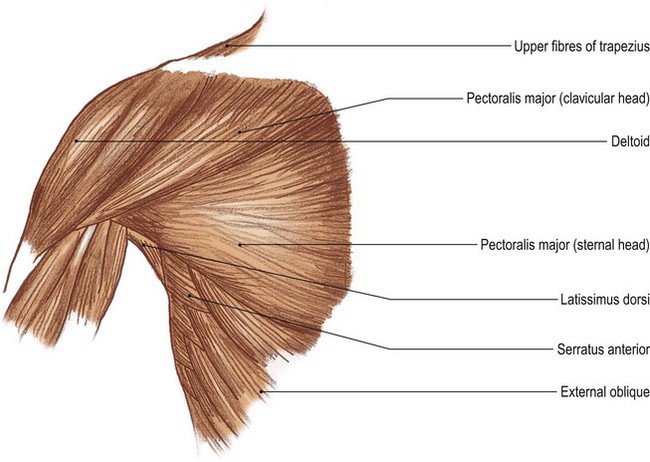
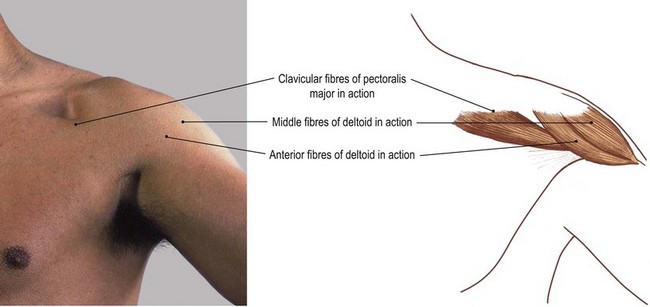
Pectoralis major
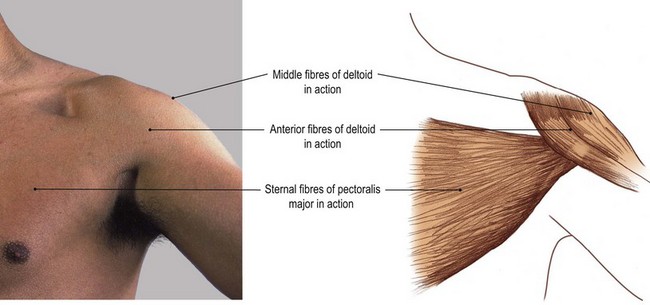
Pectoralis major (Figs 5.6 and 5.7) is a large, thick triangular muscle situated on the upper anterior area of the chest wall. It is composed of two main groups of fibres: clavicular and sternal. The clavicular fibres attach medially to the anterior surface of the medial half of the clavicle. The sternal fibres attach the anterior surface of sternum on the same side, the anterior surface of the upper seven costal cartilages and the upper part of the aponeurosis covering the abdominal muscles. Both sets of fibres pass laterally, leaving a small space between them, and join together laterally to form a bilaminar tendon which attaches to the lateral lip of the intertubercular groove of the humerus. The lower sternal fibres tend to fold up behind the upper fibres to form the double bilaminated tendon. The muscle forms a lower border which becomes the anterior border of the axilla laterally.
Palpation
For palpation in this region, the model is in the sitting position.
• Pectoralis major. This muscle is easily recognizable and palpable in even the less muscular subject. Ask the model to press the hands against the iliac crest and feel the contraction of the whole muscle.
• The sternal fibres. Identify the lower border of the anterior wall of the axilla. This is rounded due to the lower sternal fibres of pectoralis major twisting upwards posterior to its upper fibres. The muscle can be traced medially and inferiorly on to the anterior aspect of the chest as far down as the costal cartilage of the seventh rib and xiphoid process. Now ask the model to extend the arm from the flexed position against resistance. Palpate the lower sternal fibres. These are identifiable as a thick triangular shape forming the lower boundary of the muscle which can be traced out laterally to the intertubercular groove of the humerus (Fig. 5.7c, d).
• Note. The bulk of the muscle forms a rounded shape on the upper anterior chest wall. It is the muscle that men try to develop to produce a characteristic shape to the upper part of the chest. It is almost entirely covered by the breast in the female, particularly in its lower section.
• The clavicular fibres. Now ask the model to flex the arms against resistance. Palpate the clavicular fibres which are easily identified, just below the medial half of the clavicle, as a column of muscle standing clear of the chest wall (Fig. 5.7a, b) passing downwards and laterally.
• The sternal and clavicular fibres together. To observe the two sets of fibres working in concert, ask the model to press the two hands together in front of the chest. Palpate both sets of fibres which will now stand clear of the chest wall.
Functional anatomy
It is interesting to note that pectoralis major has two functionally distinct sets of fibres, a bilaminal tendon, and is supplied through two nerves (lateral and medial pectoral). In addition, it is involved in two actions which appear to oppose each other. The clavicular fibres will flex and the sternal fibres will extend the shoulder joint. In prone kneeling, both sets of fibres act to stabilize the upper trunk posture, preventing sway either forwards, backwards or from side to side. In crawling, the limb is taken forwards by the clavicular fibres and backwards by the sternal fibres. This important muscle must have had a greater significance in our evolution and recognition of its residual function may help in its re-education.
In patients suffering from respiratory embarrassment, pectoralis major may be used as an accessory muscle of inspiration. In this case the arms have to be fixed, as in gripping a post or beam, thus fixing the lateral attachment of the muscle to the humerus. The medial attachment of the muscle may then be used to expand the chest a little more.
Comparative anatomy
The pectoralis muscle(s) also play an important role in the animal, bird, fish, reptile and insect worlds. In the quadruped this muscle acts as a stabilizing muscle for the forelimb in the standing position, similar to that in the human prone kneeling position, and because of its shape takes part in both the propulsive and recovery phase of the forelimb in locomotion. It also acts as a sling for the thorax, holding it up between the two limbs. In the bird and insect it creates the enormous thrust for take-off and flight, while at the same time controlling the intricate movements of the wings. In the fish it controls the fine movements of the pectoral fin in a comparatively simple up-and-down motion, but occasionally may have fibres which are extended into the neck region. The pectorals in the forelimb of a reptile normally have the adaptability of being functional in water and on land.
Biceps brachii and coracobrachialis (see Ch. 2)
Palpation
For palpation in this region the model is in the sitting position.
• Biceps brachii and coracobrachialis tendons. Running vertically from the coracoid process the combined tendon of the biceps brachii and coracobrachialis can be palpated just below the coracoid process but is soon hidden by the broad tendon of pectoralis major. It emerges below and can be identified passing down into the anteromedial aspect of the arm and splitting into its anterior (bicipital) and posterior (coracobrachialis) section.
• The intercostal muscles. Place your fingers between the ribs and identify a tight membranous sheet. This consists of the external and internal intercostal muscles and their covering fascia. These are most easily palpated just below pectoralis major and slightly lateral to the line of the nipple. On muscular subjects they are possibly hidden by larger, more superficial muscles.
The posterior aspect of the chest
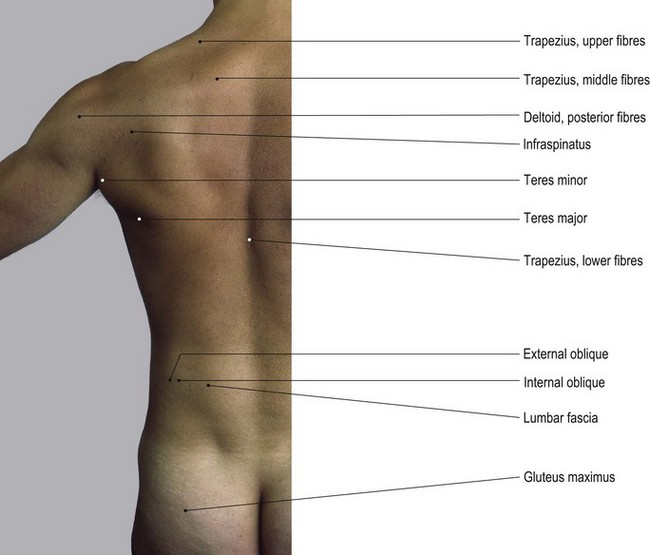
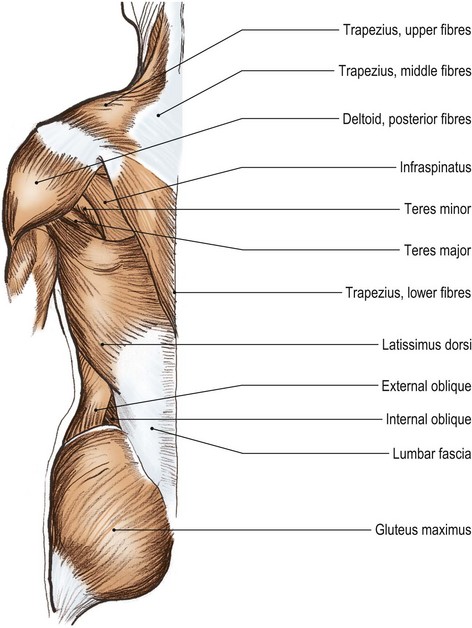
Trapezius (Fig. 5.8a, b)
The two trapezius muscles cover most of the posterior aspect of the neck and upper thorax, connecting the skull, ligamentum nuchae, seventh cervical and all the thoracic spines to the lateral end of the clavicle, acromion and superior border of the spine of the scapula.
Palpation
For palpation in this region, the model is in the sitting position.
• The upper fibres of trapezius. These are easier to identify if the model is asked to shrug the shoulders: raising the shoulder girdle. They can be palpated halfway between the external occipital protuberance and the acromion process, forming the contour of the upper lateral aspect of the shoulder.
• The middle fibres of trapezius. These are easier to identify if the model is asked to retract the shoulder girdle. They can be palpated between the upper border of the spine of the scapula and the lower cervical and upper thoracic regions.
• The lower fibres of trapezius. These are more difficult to identify as they pass from the lower thoracic spines to the medial end of the spine of the scapula. Palpation is, however, facilitated if you ask the model to depress the shoulder girdle.
Levator scapulae, rhomboid major and rhomboid minor
These muscles lie deep to the trapezius. Levator scapulae attaches above to the transverse processes of the upper four cervical vertebrae and below to the upper part of the medial border of the scapula. The rhomboid muscles attach above to the lower part of the ligamentum nuchae, the spine of the seventh cervical vertebra and the spines of the upper five thoracic vertebrae. They pass downwards and laterally to attach to the lower two-thirds of the medial border of the scapula.
Supraspinatus and infraspinatus
Supraspinatus arises from the supraspinous fossa of the scapula, passing laterally to the top of the greater tuberosity of the humerus. Infraspinatus arises from the infraspinous fossa, passing laterally to the posterior aspect of the same tuberosity.
Teres major and latissimus dorsi
These two muscles are triangular in shape and cover the lateral border of the scapula, teres major actually arising from the border. Latissimus dorsi comes from an extensive attachment to the spines of the lower six thoracic vertebrae, the thoracolumbar fascia and the posterior section of the iliac crest. It passes over the inferior angle of the scapula, taking a few fibres of origin, and then twists under the axilla with teres major to attach to the floor of the intertubercular groove of the humerus. Teres major attaches to its medial lip.
Palpation
• Teres major. Ask the model to extend the arm from a flexed position against resistance. The triangular bulk of teres major lies over the lateral border of the scapula.
• Latissimus dorsi. Again, ask the model to extend the arm from a flexed position against resistance. The tendon of latissimus dorsi can be traced, laterally and forwards, forming the posterior wall of the axilla. This tendon can be traced to its muscle fibres medially over the dorsum of the chest and lumbar area. Ask the model to cough and palpate the muscle.
Serratus anterior (see Fig. 5.6a, b)
Serratus anterior is a flat but powerful muscle attaching to the whole of the medial border of the scapula. Passing deep to the scapula, it attaches anteriorly to the lateral aspect of the first to eighth ribs at the mid-axillary line. Most of the muscle is concealed beneath the scapula, but palpation of its anterior attachment to the ribs is possible.
Palpation
• Serratus anterior. Ask the model to protract the shoulder girdle. Now place your fingers behind the mid-axillary line but in front of the scapula. The anterior attachment of serratus anterior to the ribs can be identified.
• Note. Care must be taken to observe the contraction when the pectoral girdle is retracted and begins to move forwards. Once the lateral border of the scapula has passed beyond the mid-axillary line, the muscle is hidden.
The diaphragm (Figs 5.9 and 5.10)
The diaphragm is a musculotendinous sheet separating the thoracic and abdominal cavities. It forms a double cupola within the thorax, with the heart resting upon its central tendinous part. Anteriorly it attaches to the xiphisternum, laterally to the inner aspect of the lower six ribs on a line with the inner surface of the costochondral joints, and posteriorly to the vertebral column. It is the main muscle of inspiration and moves downwards on inspiration and upwards on expiration. It is therefore more useful to indicate its surface markings after full expiration and then after a deep inspiration. The attachments to the xiphisternum, ribs and vertebral column remain constant, but the two cupolae and central tendon vary in height. It must also be remembered that the position of the diaphragm is influenced by other factors: it lies at a higher level with respect to the rib cage when lying supine than when standing; its downward movement is restricted by food and gas in the stomach, and by increased pressure in the abdominal cavity, for example during pregnancy; in side lying it is pushed up into the thoracic cavity on the lower side by the contents of the abdomen; and in prone lying the liver tends to restrict its downward movement on the right side.
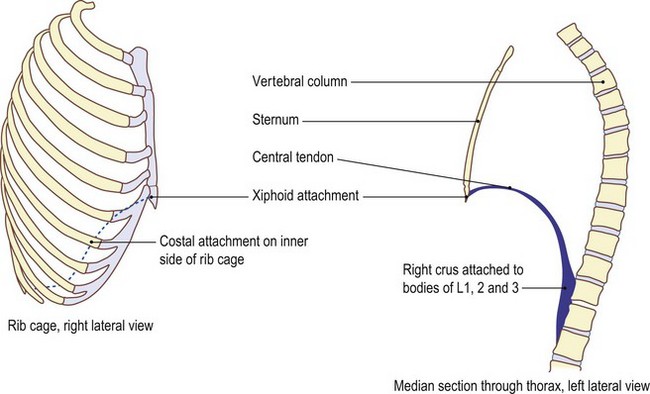
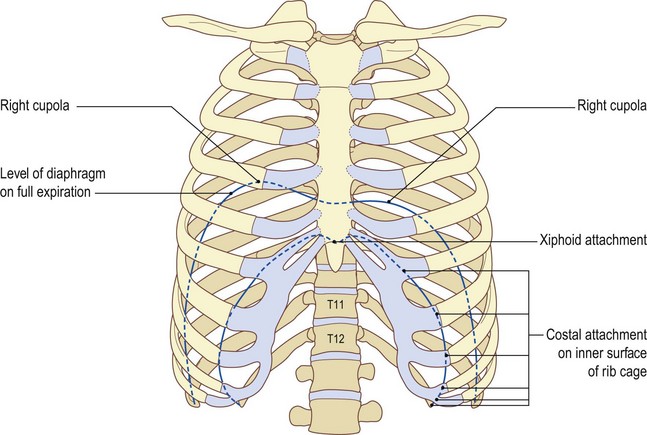
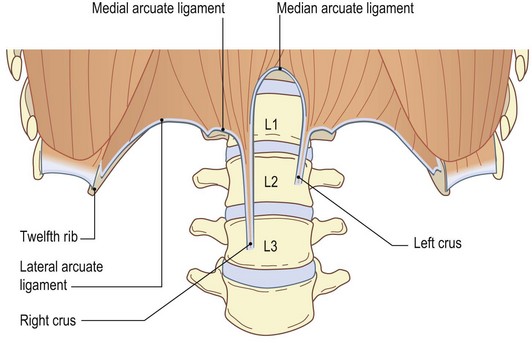
Fig. 5.10 The diaphragm. (a) The rib cage (anterior aspect). (b) Attachments of diaphragm to the vertebrae and twelfth rib (anterior aspect viewed from inside rib cage)
On full expiration, the right cupola rises to the level of the fourth rib, the left to the fourth intercostal space and the central tendon to the level of the fifth costal cartilage. On full inspiration – which may produce a 6 cm descent of the cupolae – the diaphragm may reach the level of the sixth or seventh ribs. In quiet respiration, the diaphragm normally only moves up and down 1–2 cm.
Palpation
surface marking
It is impossible to palpate the diaphragm. On full inspiration there is a bulging of the abdomen between the two costal margins. Although this is produced by the diaphragm, it is actually the upper section of the abdominals.
• The diaphragm: surface marking. The attachment of the diaphragm to the inside of the chest wall can be marked by an oblique line drawn from the xiphoid process, anteriorly, downwards and laterally slightly concave downwards. It follows the line of the sixth costal cartilage, attaching to the inner surface and anterior end of the sixth to tenth ribs (Fig. 5.9a). It then attaches to the inner surface of the eleventh and twelfth ribs. Its vertebral attachment is marked by a line running down the lateral side of the bodies of the first and second lumbar vertebrae on the left and the first to third lumbar vertebrae on the right (Fig. 5.10b). These can be represented by two vertical lines, 2 cm lateral to the first and second lumbar spines on the left and the first to third lumbar spines on the right.
Nerves (Figs 5.11 and 5.12)
The only nerves that become superficial in the thoracic region are those that supply the skin covering the ribs and intercostal spaces. By the time they reach the surface they are fine filaments and impossible to palpate.
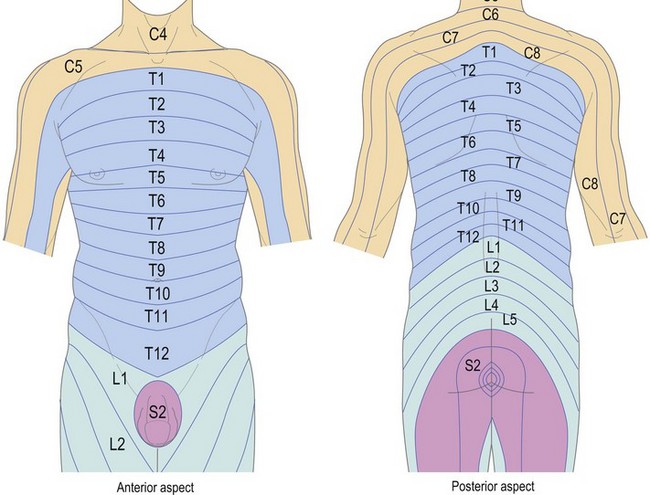
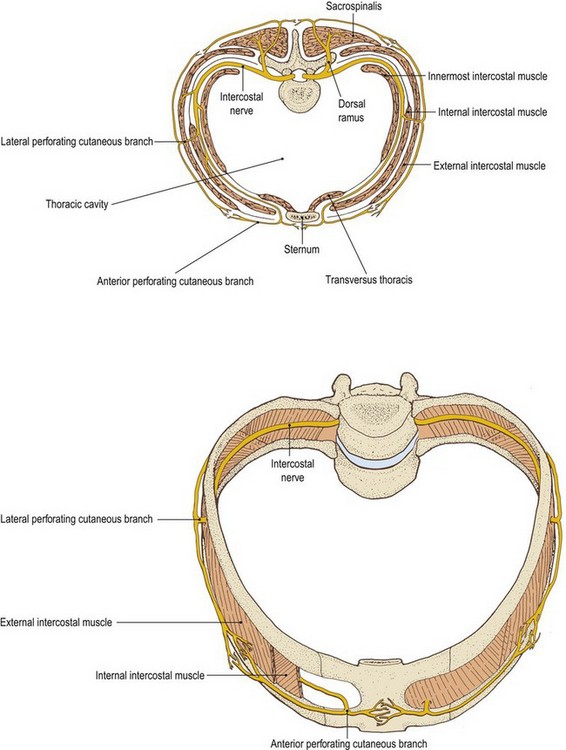
Each intercostal nerve passes around the inside of the rib cage deep to the internal intercostal muscle, normally giving off a lateral branch at approximately the mid-axillary line. The area of skin supplied by each nerve usually includes that covering the rib above and below, including the external intercostal muscle passing between. Therefore there is an area of overlap of the cutaneous nerves, so that the loss of sensation from one nerve only leaves an area of paraesthesia not anaesthesia.
Below the sixth rib the nerves continue obliquely around the abdominal wall in the same direction as the ribs between which they commenced.
• Note. In the condition herpes zoster (shingles), the sensory component of an individual thoracic nerve is often affected by the virus and this leads to small pustules appearing over the area supplied by this particular nerve. The patient presents with a strip around the chest or abdomen following the line of its distribution (Fig. 5.11). Although this condition commonly appears to affect a single thoracic nerve it may affect any nerve in the body.
Structures within the thoracic cage
Although the structures contained within the thoracic cage are almost totally hidden by the ribs, sternum and vertebral column, it is of some importance to be able to indicate the surface markings of the major organs and vessels. Owing to considerable movement during life, no surface marking can be constant; nevertheless, each organ stays within certain boundaries. These will be indicated by the locations given.
Palpation
surface marking
For palpation in this region, the model is in the sitting, standing or supine lying position.
The lungs (Fig. 5.13)
The lungs almost totally fill the thorax on either side of the heart.
The apices of the lungs. The apex of each lung can be palpated, on deep inspiration, as it rises behind the middle third of the clavicle. These are the only areas of the lungs which are palpable and may prove to be elusive in some individuals.
Each lung takes on the shape of the deep surface of the rib cage and intercostal muscles, being convex laterally and concave medially and inferiorly. Each lung presents anterior, posterior and inferior borders medially. The borders divide the lung into lateral, medial and inferior surfaces.
Palpation
surface marking
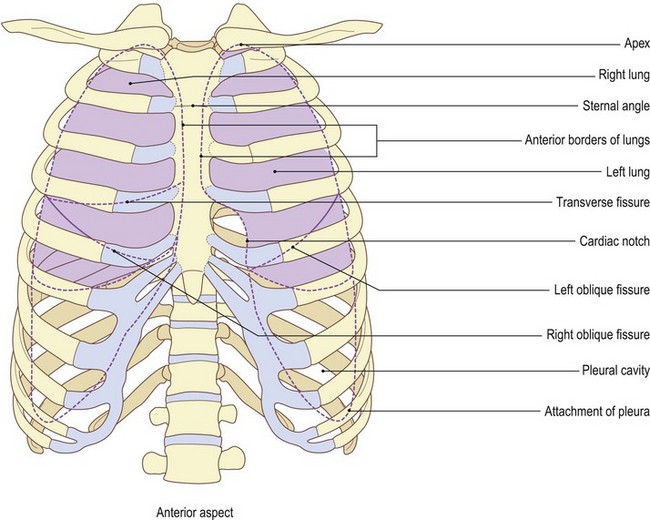
• Both lungs. The surface markings of the anterior borders of the two lungs differ slightly. Both descend from the apex of the lung, behind the sternoclavicular joint of the appropriate side, to come together behind the sternal angle. They then pass downwards close to the midline until the level of the fourth costal cartilage.
• The left lung. At the level of the fourth costal cartilage the left anterior border passes laterally in a C-shaped curve concave medially (the cardiac notch) to reach the inferior border behind the sixth costal cartilage in the mid-clavicular line.
• The right lung. The right medial border passes straight downwards, reaching the inferior border at the sixth chondrosternal joint (Fig. 5.13a).
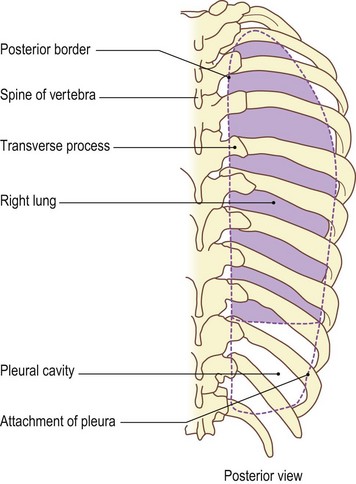
• Both lungs. The posterior borders of both lungs pass vertically downwards in front of the necks of the ribs, approximately 2 cm either side of the spines of the vertebrae, from the apex of the lung to the level of the tenth rib (Fig. 5.13c).
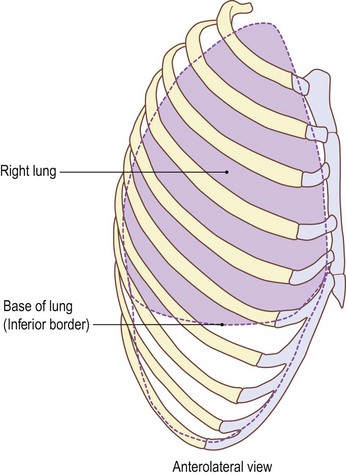
• Both lungs. The inferior border of each lung passes almost horizontally around the chest wall, being level with the sixth costal cartilage anteriorly, crossing the eighth rib in the mid-axillary line and the tenth rib posteriorly.
• The right lung. The base of the right lung is usually slightly higher than the left owing to the presence of the liver below it (Fig. 5.13a–c).
• The pleura. Parietal pleura lines the thoracic cage of each side and covers each lung in parts. The lower part of this pleura, however, is prolonged downwards for some 5 cm below the lower border of the lung to the twelfth rib posteriorly, the tenth rib at the mid-axillary line and the sixth costal cartilage anteriorly (Fig. 5.13a–c). This is termed the pleural cavity.
The fissures of the lungs
Each lung is marked by an oblique fissure; the right lung, in addition, has a transverse fissure. These mark the junctions between the various lobes of each lung; the left therefore possesses two lobes, upper and lower, while the right possesses three, upper, middle and lower.
• The oblique fissures. Each oblique fissure can be marked on the chest wall by a line drawn obliquely downwards and forwards from a point 2 cm lateral to the spine of T3, crossing the mid-axillary line at the fifth rib, to reach the inferior border of the lung at the costal cartilage of the sixth rib, 7 cm from the midline (Fig. 5.13a). A good guide for the direction of this line is given by the medial border of the scapula when the arm is raised above the head.
• The transverse fissure. Only the right lung has a transverse fissure, which marks the division of the upper and middle lobes. It is indicated by a line from the fifth rib in the mid-axillary line to the fourth costal cartilage 3 cm from the median plane, essentially running along the lower border of the fourth rib.
The heart (Fig. 5.14)
The heart is a roughly cone-shaped double muscular pump situated behind the sternum with its apex downward and to the left and its base upward and to the right. It is composed of specialized contractile muscular tissue (myocardium) contained within a double layer of serous pericardium, which is joined around the area where the great vessels enter the heart. The outer layer of the pericardium is attached to the central part of the upper surface of the diaphragm and the inner layer is connected to the heart musculature. The two pumps, although pumping together, are completely separate and are often referred to as the ‘left heart’ and the ‘right heart’. Each pump is composed of an upper receiving chamber, the atrium, and a lower more powerful muscular chamber, the ventricle.
The heart is a rhythmically contractile tissue which is controlled by nerve impulses. The upper chambers or atria are completely separated from the lower ventricles by a fibrous non-conductive layer. The only communication between the two is by a bundle of specialized tissue.
Palpation
surface marking
The position of the heart within the thorax is variable, to some extent, depending on the posture adopted, so that its surface markings are slightly higher when lying compared with standing and sitting.
The projection of the heart on to the anterior surface of the chest is as follows (Figs 5.14 and 5.15).
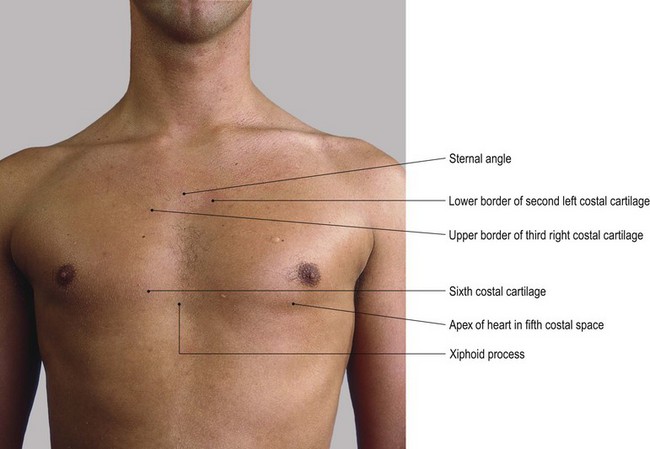
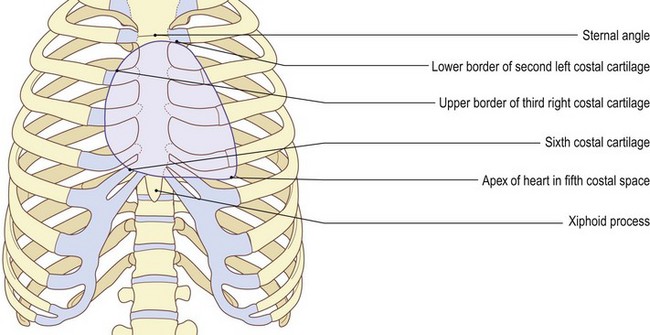
• The apex. The apex of the heart points downwards and to the left and can be palpated 9 cm from the midline in the fifth left intercostal space. The model is in the sitting position. Ask the model to lean slightly forward; in this position, the pulsations are enhanced because the apex of the heart is pressed against the chest wall.
• The upper limit of the heart is marked by two points, one at the lower border of the second left costal cartilage, 3 cm to the left of the midline, and the other at the upper border of the third right costal cartilage, 3 cm to the right of the midline.
• The lower right border of the heart can be indicated on the lower border of the costal cartilage of the right sixth rib, 3 cm from the midline. The boundaries are curved, joining the above points and making an area approximately the size of the model’s clenched fist.
Function
The heart is responsible for pumping the blood around the body. The deoxygenated blood enters the right atrium from the systemic circulation through the large veins, e.g. the inferior and superior vena cavae. It is then pumped down into the right ventricle through the right atrioventricular (tricuspid) valve, which contracts, sending the blood into the pulmonary circulation and lungs, passing via the pulmonary valve.
Oxygenated blood is received into the left atrium from the lungs and is propelled down into the left ventricle through the left atrioventricular (mitral) valve. When full, the left ventricle contracts, pumping the blood through the aortic valve into the aorta and back into the systemic circulation. Equal volumes of blood must be expelled from the two ventricles at each stroke, the right into the pulmonary circulation and the left into the systemic circulation. This will maintain an equal rate of flow in both systems.
Major arteries (Fig. 5.15)
The aorta
The aorta is the main artery carrying oxygenated blood to the body. It leaves the heart at the base of the left ventricle, immediately giving off the two coronary arteries which supply the heart itself with blood. It passes upwards, slightly forwards and to the right before arching backwards and to the left over the right pulmonary vessels. It then passes inferiorly through the thorax on the left side of the vertebral bodies, behind the heart. As it does so it gradually comes to lie more in the midline, finally leaving the thorax in front, but slightly to the left of the body of T12, passing between the two crura and behind the median arcuate ligament of the diaphragm.
Palpation
surface marking
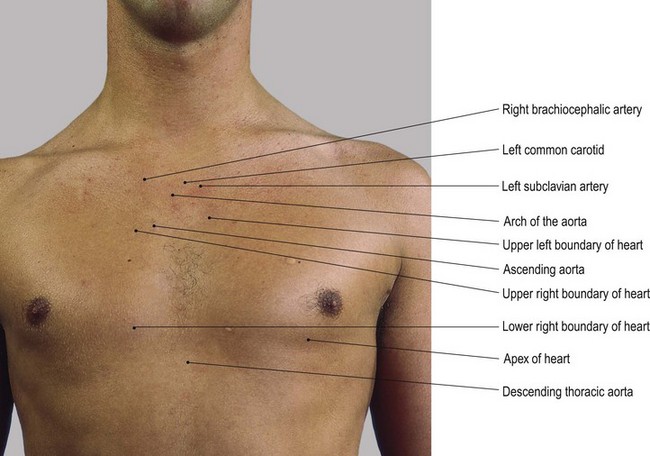
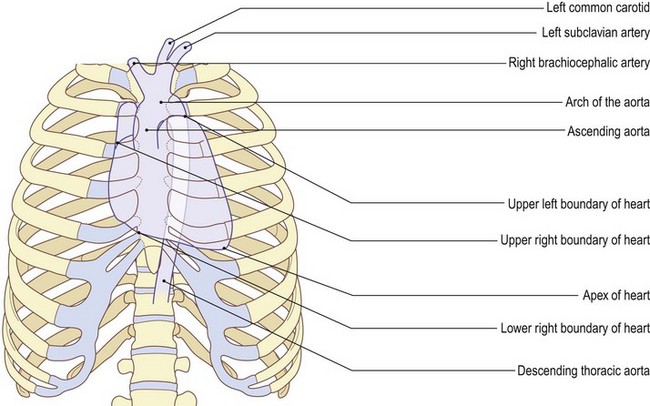
• The aortic valve. The aortic valve lies deep to the sternum adjacent to the third intercostal space. From here the ascending aorta, a band 2.5 cm wide, passes upwards and to the right as far as the second right chondrosternal joint.
• The aortic arch. The arch of the aorta then passes behind the sternal angle (and the lower part of the manubrium) over the heart, to end behind the second left costal cartilage.
• The descending aorta. This can be represented by a line extending from this point to its exit from the thorax just left of the midline and above the transpyloric plane, which is on a level with the tips of the ninth costal cartilages.
The brachiocephalic, left common carotid and left subclavian arteries
From the upper convexity of the arch of the aorta, three major vessels arise. The brachiocephalic (innominate) artery is anterior and to the right. Immediately behind and to the left is the left common carotid. Behind and to the left of the left common carotid is the left subclavian.
The brachiocephalic artery supplies oxygenated blood to the right side of the head and neck via the right common carotid artery through its internal and external branches. It also supplies blood to the right arm via the right subclavian artery. The left common carotid artery supplies blood to the left side of the head and neck via its internal and external branches. The left subclavian supplies blood to the left arm.
Palpation
surface marking
• The brachiocephalic artery. The brachiocephalic artery arises from the arch of the aorta behind the manubrium slightly right of centre and passes upwards, backwards and to the right for approximately 5 cm. It divides behind the right sternoclavicular joint into the right subclavian and right common carotid.
• The left common carotid artery. This artery arises from the aorta just to the left of the mid point of the manubrium and passes upwards, backwards and to the left for approximately 4 cm to enter the neck behind the left sternoclavicular joint.
• The left subclavian artery. This artery arises from the posterior part of the arch of the aorta behind the first intercostal space on the left, just lateral to the manubrium. It passes upwards and to the left for approximately 7 cm behind the first chondrosternal joint on the left to the inner borders of the left first rib. It passes over the rib en route to the left upper limb.
Veins (Fig. 5.16)
The large veins of the thorax are also situated deep within the thoracic cage and are impossible to palpate. Nevertheless, it is of some value to know where they lie in relation to palpable surface markings. It must, however, be remembered that the chest wall, the heart, diaphragm and lungs are all moveable structures and this will lead to small differences in their relationship to one another. Surface markings, therefore, will be as accurate as possible but a little leeway must be expected in this area.
Outline of the venous network
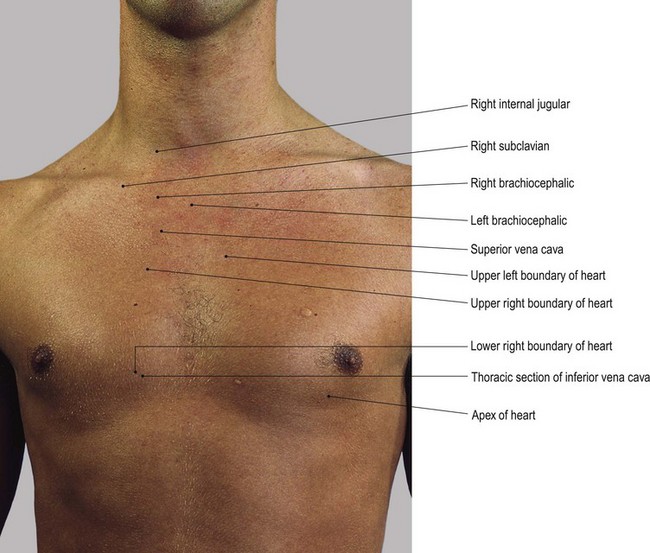
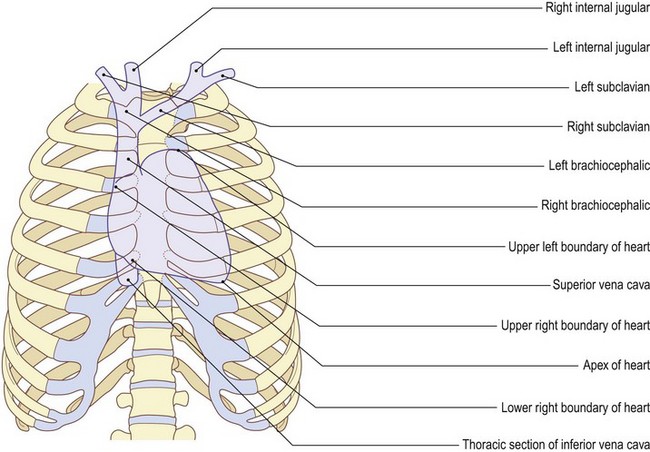
Venous blood from the head, neck, both upper limbs and upper trunk enters the left and right brachiocephalic (innominate) veins. It then passes into the superior vena cava and then into the upper part of the right atrium of the heart.
Venous blood from the two lower limbs and lower trunk passes, via the internal and external iliac veins, into the abdominal inferior vena cava, entering the thoracic cavity, for just a short distance, forming its thoracic section. This empties into the lower part of the right atrium of the heart.
Palpation
surface marking
• The innominate veins. In the upper thorax, the left and right brachiocephalic (innominate) veins are formed by the internal jugular and the subclavian veins of their respective sides, just lateral to each sternoclavicular joint.
• The left brachiocephalic vein. This vein passes downwards and to the right for approximately 6 cm to join the right brachiocephalic behind the sternal end of the first right costal cartilage. At this point they form the superior vena cava.
• The superior vena cava. This vein passes vertically downwards for approximately 7 cm from behind the costal cartilage of the first rib on the right to enter the right atrium behind the sternal end of the third costal cartilage.
• The inferior vena cava. In the lower thorax, the inferior vena cava enters the thoracic cavity through the upper fibrous part of the diaphragm, entering the lower part of the right atrium of the heart almost immediately, lying behind the sternal end of the sixth right costal cartilage.