Documentation in the Age of the Electronic Health Record
At the end of the chapter, the reader will be able to:
1 Identify five purposes for documentation.
2 Discuss electronic health records (EHRs) as part of a larger electronic Health Information Technology (HIT) system.
3 Discuss the need for coding and nursing taxonomy in the use of EHRs.
4 Identify how use of clinical pathways and electronic HIT systems improves client outcomes.
5 Identify legal aspects of documenting in client records.
6 Discuss how evidence-based clinical practice may change the way nursing is practiced and documented.
7 Discuss why “use of technologies to assist in effective communication in a variety of healthcare settings” is listed as an expected nurse competency by nursing organizations
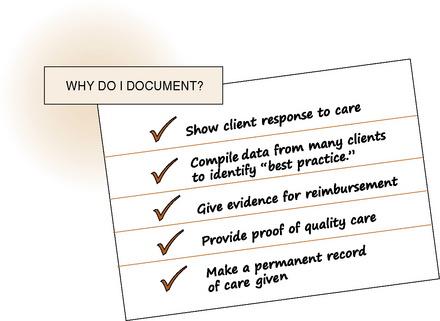
The process of obtaining, organizing, and conveying client health information to others in print or electronic format is referred to as documentation. As illustrated in Figure 25-1, documentation serves five purposes: communicates to others care received or not received; conveys pertinent information about the client’s condition and response to treatment interventions; substantiates the quality of care by showing adherence to care standards; provides evidence for reimbursement; and serves as source of data, which can be aggregated and analyzed for client care research to establish “best practice” interventions. Documentation should show evidence of effective care and client outcomes during accreditation reviews.
This chapter focuses on electronic health records (EHRs) and documenting client care. In recent years, computerization of records in hospitals has gone from a leading-edge experiment to mainstream management. Regulatory and ethical implications of documentation, use of coding and of nursing taxonomies, as well as use of clinical pathways are also discussed in this chapter. The newest technology devices for medical communication at the point of care, including clinical decision support, remote monitoring, secure messaging, and telehealth, are discussed in Chapter 26.
Basic concepts
Documenting client information
Documentation of client care must be complete and accurate. Standards of documentation must meet the requirements of government, health care agency, professional standards of practice, accreditation standards, third-party payers, and the legal system. Every health care agency has its own version of clinical documentation, but in the United States, Medicare has published guidelines for primary providers affecting advanced nurse practitioners. This documentation includes a client history (a database that often includes a summary list of health problems and needs); physical examination findings; a description of the presenting problem; and rationales for decision making, counseling, and coordination of care in a client-centered care plan. These guidelines specify what is to be examined in each body system. Nursing documentation also includes a Nursing Care Plan, daily records of client progress, and evaluation of outcomes. These daily records may include flow sheets, nursing notes, intake and output forms, and medication records.
Computerized health information technology systems
A major communication revolution in health care is under way internationally, made possible by the increased use of computers. The U.S. Health Information Technology for Economic and Clinical Health Act of 2009 provides major resources to care providers to assist them in computerization of client care information. Computers make information more accessible to all who are involved, including your client. The U.S. Federal Government, the American Nurses Association, and the Institute of Medicine, among others, believe computerization offers opportunities to improve the quality of health care and to reduce its cost. This use of Health Information Technology (HIT) involves creation of a whole new electronic interactive system. It is far more than just putting existing documentation, as in paper charting, on a computer. HIT is designed to support the multiple information needs required by today’s complex client care by providing you with assistance such as clinical decision support. Refer to Table 25-1 for a list of EHR components. Despite the federal government mandate that every American’s health records be electronic by 2014, hospitals in the United States have been amazingly slow to adopt fully integrated computerized health systems. By 2008, less than 11% of hospitals and 20% of physician offices had even basic EHR systems, in contrast with 98% in the Netherlands and 89% in Great Britain (Carter, 2008; Silva, 2009).
TABLE 25-1
Components of a Health Information Technology System
• An integrated, accessible electronic repository of client data with easy access by a variety of health care providers and agencies
• Client health record history, physical examination findings, medications, laboratory tests, imaging files with real-time access at the point of care
• Electronic clinical documentation of care available to nurses, physicians, other providers
• Computerized provider (or physician) order entry (CPOE)
• Clinical decision support alerts and reminders, standard “best practice” protocols that monitor your care and send you prompts if care is not recorded
• Ease of access to allow aggregation of data from many clients
Advantages of computerized client electronic health records
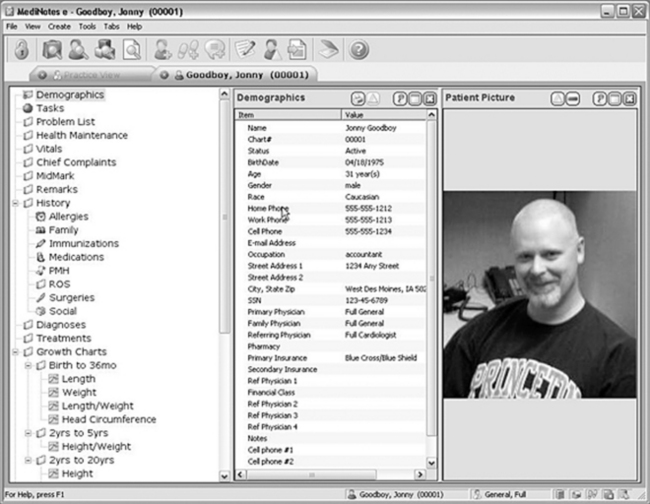
EHRs, as one part of the overall computerized HIT system, are now the accepted process for documenting care. The authors use the term EHR in this book, although electronic records are also known as electronic clinical records, electronic patient records, person-centered health records, or electronic medical records (Figure 25-2).
Interagency Accessibility: Electronic records are more durable than paper charting and easily transferable. For example, during Hurricane Katrina in 2005, the New Orleans Veterans Administration (VA) was able to send their 50,000 client health records to a secure site, while untold thousands of paper records at other New Orleans hospitals were destroyed by flood waters. The VA record system is fully integrated with the Department of Defense. Therefore, if a soldier is wounded abroad, diagnosed and treated, shipped home, and eventually discharged, his record including computed axial tomography (CAT) scans are seamlessly available to his VA doctor. Another example might be a client who travels across the country on vacation. His records are potentially available if he is admitted to an emergency department in another state.
Cost Savings: Initial transition from paper records is expensive, but cost reduction is expected to occur in the long run. Administrators estimate that the cost of using paper records in an agency is 25% of total health care costs. In addition to the actual paper and printing costs, there are costs involved in record transcription, filing, storage, and retrieval of information. Under Medicare and Medicaid reimbursement, hospitals maximized reimbursement through use of the computer-driven MS-DRG system.
Increased Access to Client Information: A client’s EHR may be stored so that it is accessible to all of a client’s care providers. Electronic records support telehealth, for example, in the case of a fully computerized medical record that includes graphic files (e.g., sonograms, x-ray scans, and other diagnostic imaging) that can be sent and analyzed by specialists hundreds of miles away. Information is instantly available to a variety of users. Results of your client’s laboratory tests, posted in the laboratory, can be accessed by you from the client’s inpatient unit, by the community health nurse, and by the primary physician’s office as soon as the laboratory technician enters them into the hospital computer system. Your clients also can have access to some areas of their EHR. For example, Kaiser Permanente’s nearly 9 million members can access their immunization records at any time from anywhere. When seeking care outside their own health system, clients can carry their entire health record on a flash drive until we achieve universal interoperatibility.
Efficiency and Ease of Use: The potential impact of EHRs on nursing efficiency is measured by a reduction in the amount of time you spend doing activities other than direct care of your client (Thompson, Johnston, & Spurr, 2009). Computer-assisted charting can reduce the time you spend charting. This allows you to spend more time with your client, possibly increasing client satisfaction. In a meta-analysis by Poissant et al. (2005), nurses reduced their time documenting by 24%, an average of almost an hour of their time in an 8-hour workday. Though there are some study results showing that computer charting takes a nurse more time, the Agency for Healthcare Research and Quality reports that there is up to a 50% decrease in time spent charting.
EHR also improves the quality of charting (Moody et al., 2004). Duplication is eliminated, increasing efficiency. This includes eliminating duplication in questioning your client about his history, as his answers about his medical history are available to you from admission. A greater impact on nursing efficiency is the elimination of duplication when charting.
Efficiency is increased because providers across all agencies have immediate access to client information. Some Canadian provinces and states such as Minnesota are examples of regions with integrated electronic health infrastructures, attained by legislating and financing a region-wide system. Thompson and colleagues (2009) list HIT benefits that improve nursing efficiency in other “downstream” ways beyond what is apparent in documentation activities, such as medication record resolution, automatic medication calculations, automatic downloading of bedside monitoring records, automated nursing discharge summaries, and so forth.
Computers should be easy to use. Your terminal may be located at the nurses’ station, in your client’s room, or it may be portable wherever you go, including to a client’s home or a community clinic. When charting, you type in your password/identification number, scan your identity card, or scan your fingerprint. Then you enter data into the client’s computer file. Some systems use a mouse or light pen to select from a menu of standard groupings or categories in documenting client care information. Many systems have template outlines to prompt you, for example, when you are doing your intake interview. Capability to document your care from your client’s bedside or home is known as “point of care” and is described in Chapter 26.
Enhanced Quality of Care and Communication: A comprehensive computer information system changes the way information flows through the health care delivery system. Communication is more rapid. For example, after the client’s admission to an acute care hospital, a physician’s orders entered into the computer are transmitted simultaneously to the pharmacy, the laboratory, and the nursing unit. HIT can be used to communicate quickly among doctors, nurses, client, families, and across agency departments.
Quality of care can be maximized with clinical decision-making electronic “prompts” that remind you to do complete care or to chart comprehensively. This prompt function also enhances the quality of care by reminding you about the specific standards of care that may apply to your client. Most electronic client monitors, such as those recording blood pressure, pulse, and oxygenation, record this information directly into the client’s EHR. This saves charting time and eliminates transcription errors. The computer sends you an “alert” to notify you about increases in your client blood pressure or other abnormalities. Records over time can be examined to determine the percentage of time you delivered care that was “best practice.” In another example, your diabetic client’s insurance company may be able to monitor whether his physician is appropriately checking his HbA1c levels routinely. Your client may also have limited access to his own health record, for example, to check results of his laboratory tests, his immunization records, and so on. Participation in Centralized Disease Registries can give real-time feedback to providers of care. For example, participants in the National Cancer Data System can receive electronic “alerts” if “best practice” care is not started within a certain time frame. So if the standard of care for your postoperative lumpectomy client for diagnosed early-stage breast cancer is to begin radiation within a week, the registry notifies the hospital and the physician if this fails to happen.
Communication among health professionals coordinating client care can also be improved with HIT use. For example, Nemeth’s study (2007) showed that point-of-care access to current laboratory tests allowed providers to discuss changes in care at the time of the visit. An example might be instant access to laboratory results on blood clotting time, allowing you to contact the physician for a change in medication levels while you are still at your client’s home.
Safety: As discussed in Chapter 22, one of the most important reasons for computerizing is to reduce errors. HITs force standardization of nursing terminology, eliminate use of inappropriate abbreviations, and avoid problems of illegibility. Errors are prevented because assistance is given with drug calculations, and in assisting with decision support such as checking drug incompatibility, allergies, and so on.
Aggregated Data: Computerized systems offer ease of access to aggregate (combine together) information from many clients for reports, disease surveillance, and to research best practice nursing care. An audit trail promotes greater accountability. Aggregated information from a number of records can be analyzed to determine outcomes, for example, the number of postoperative infections that have occurred on your unit. Access time to records is also enhanced. For example, when using paper files, it took a lengthy time to do audits for agency quality assurance or by insurance companies verifying reimbursement.
In addition to documentation, nurses use HIT systems to identify contributions nurses make to attain better client outcomes. By combining data, nurses identify better treatment methods and transfer this new knowledge to colleagues (Gruber, Cummings, Leblanc, & Smith, 2009). It is crucial to nursing that nursing terminologies become embedded into EHRs, both to improve communication between nurses, such as at change of shift, and to allow data to be extracted to describe nursing care. In the past, EHRs did not contain nursing terminologies (Westra, Delaney, Konicek, & Keenan, 2008). Thus, no data could be aggregated to identify best practice nursing care.
Keepnews, Capitman, and Rosati (2004) demonstrated that one computer charting system could be used to obtain reports about predictors of client outcomes in home health care. For example, you can easily get information identifying the most effective specific nursing interventions to establish best practice and identify other interventions that need to be changed. Combining data from many clients quickly can speed identification of adverse outcomes. For example, public health agencies analyze information about illness to generate epidemiologic information such as the spread of influenza across the world. In another example, Kaiser Permanente was able to analyze information from 1.3 million clients receiving Vioxx to identify potential harm from this medication, which led to its removal from the market.
Disadvantages of computerized patient electronic health records
In 2009, the American Health Information Management Association published a citizen’s Health Information Bill of Rights, which states that all clients have the right to secure and accurate electronic records which they can access free of charge. Other professional organizations and governments advocate protection and privacy of client information, including electronic records.
Initial Cost: Barriers to adoption of the EHR include high start-up costs. In the United States, several government statutes provide financial incentives for adopting EHR, but beginning in 2014, there are penalties for not e-prescribing. Future changes in technologies associated with your client care will necessitate expensive software periodic revisions. These may be offset by the increased efficiency and the improved ability to capture billing levels.
Lack of Legal Guidelines: Your client’s record is a legal document. Few nations have adequate laws governing information misuse of EHRs. In the United States, government Health Insurance Portability and Accountability Act of 1996 (HIPAA) regulations provide some privacy guidelines for your client’s records, limiting with whom you can share this information, and these will be expanded to include associated businesses. More rigorous penalties will be imposed. When computers are located at the bedside, the screen displays information to anyone who stops by the bedside. You need to be alert to this potential violation of your client’s privacy.
Lack of Uniform Standards and Universal Client Identifier Numbers: Although many countries use the same universal number to identify the client in all their agencies, in the United States, our clients often have multiple identity numbers across agencies. Proposals for using one’s Social Security number have received criticism, with some favoring a separate national identification number. During the transitional phase-in stage, some information is still in paper charts whereas other data are in a computer.
Problems with System Function: Vendors created systems that were incompatible with competing software. The Office of the National Coordinator for HIT created a certification process to harmonize EHR products for better interoperatibility. Not only must EHRs be integrated in multiple departments such as pharmacy, radiology, physical therapy, and nursing, they must be accessible across agencies. A number of companies are now marketing software applications to maximize interoperatibility.
User Frustration: Incompatibility of software would make it difficult to follow care from acute treatment to rehabilitation to home care. The lack of standardized data terminology and classification in the past was a key barrier to EHR information sharing. As with the medical profession, the nursing profession has been intensely engaged in developing standardized languages for their practice.
Insurance companies, banks, and others have been doing business electronically for years. But initially, health care providers complained that software was difficult to use. Staff do have a challenge, particularly those who work in multiple agencies having different computer systems, such as nurses who float to several hospitals. New users complain HIT is time consuming, but once use is mastered, their efficiency increases. Periodic system upgrades also require readjustment.
A staff nurse on a busy unit might not have a computer terminal immediately available. Client files are routinely backed up usually once a day. If there is a dysfunction or glitch and your computer crashes, you get frustrated. Computer systems require “downtime” for storing records on backup software or while technicians service system hardware. Any time the computer is unavailable for entering your documentation, you need alternative documentation forms.
Misuse of Technology: Several articles have addressed the potential possibility of abusing the unique capabilities of computer entry, such as a temptation to “cut and paste” an old client care entry when documenting today’s care (Siegler & Adelman, 2009).
Confidentiality Issues: Confidentiality and legal issues are by far the biggest areas of concern. Whenever there are multiple users, there are risks that others not involved in a client’s care may access confidential information. This is particularly true for computerized data, but it is also a concern with any data transmitted electronically (e.g., information sent by fax or through telehealth networks). Ensuring privacy and developing security safeguards have become a requirement for electronic records. Procedures requiring passwords, preset log-on time limitations, and internal computer system safeguards to prevent tampering with or unauthorized access to client data are now routine expectations of nursing documentation.
Classification of care: use of standardized terminologies
The nursing profession has been very active in developing coding systems for the classification of nursing care. If nursing cannot categorically classify the care provided and the outcomes of that care, there is little hope that the profession will be able to effectively communicate, document nursing care electronically, or get reimbursed for its essential role in the health care of the individual, family, and community.
Goal for the classification of nursing care
Problem statements, interventions, and outcomes recorded using a standard language communicate a commonly understood message across a variety of health care settings. These terms, consistent with the scope of nursing practice, are necessary to electronically document our care. When standardized language is used to document practice, we can compare and evaluate effectiveness of our care, regardless of which nurse in which setting is delivering this care. In the past, nursing has been unable to describe the units of care, its effect on client outcome, or to establish a cost for its contributions to client care. Nowhere on a client’s hospital bill does the cost of our nursing care appear. It traditionally has been part of the “room charge.” The goals of developing standardized terminology and classification codes are to improve communication, to make nursing practice visible within (computerized) health information systems, and to assist in establishing evidenced-based nursing practices.
Developing classifications for coding
Use of a standardized nursing classification language can save time by clearly describing clients’ needs, interventions used, and the outcomes of care; by improving communication among staff members, in writing nursing care plans and nursing notes; and in conferring with health team members across the continuum of primary care, acute care, and home care practices. Use of standard language is instrumental in describing nursing practice. The time spent teaching, providing support, and assisting in grieving are the types of nursing activities that nurses spend considerable time doing, yet they rarely show up in the medical record. In home health records, nurses most often document nursing problems or diagnoses related to the medical diagnosis, but some report they spend most of their care in client teaching.
Taxonomies: Standardized Language Terminology in Nursing: The challenge for nursing is to communicate clearly. For decades, efforts have been made to improve communication among nurses caring for the same clients, as well as those working across different health care settings and different cultures. Our profession is building a scientific knowledge base so we can identify, teach, and give “best care” that creates the best possible outcome for our clients. With the shift to electronic records, terms must also be codable. Utilization of standardized nursing terms to describe nursing practices and their outcomes accomplishes this (Rutherford, 2008). The American Nurses Association recognizes a number of different taxonomies for describing nursing care, based on specific criteria. In 1998, McCormick and Jones predicted that because no one system could meet the needs of nurses in all areas of practice, technologic applications would be developed that would communicate across classification systems.
Taxonomy is defined as a hierarchical method of classifying a vocabulary of terms according to certain rules. Various taxonomies have been developed to be used in communication and comparisons across health care settings and providers, insurers/payers, and policy makers who set priorities and allocate resources. So far, the international nursing community has not agreed on one common terminology. Research by Muller-Staub and colleagues (2007) found North American Nursing Diagnosis Association International (NANDA-I) to be the best researched and most widely implemented nursing classification internationally.
Four of the most commonly used nursing taxonomies are briefly discussed: NANDA-I, the Nursing Interventions Classification system (NIC), the Nursing Outcomes Classification system (NOC), and the Omaha system.
The first three terminologies (NANDA-I, NIC, and NOC), are used together to plan and document nursing care, sometimes referred to as NNN. NNN use creates a systematic schema for implementing the nursing process. Table 25-2 presents an example of the linkages for the nursing diagnosis of chronic pain, linking nursing diagnosis, intervention, and outcome aids in developing electronic records so that for each diagnosis there are specific interventions and outcomes that can be selected and saved into a client database.
TABLE 25-2
Example of Linkages of North American Nursing Diagnosis Association, Nursing Interventions Classification, and Nursing Outcomes Classification
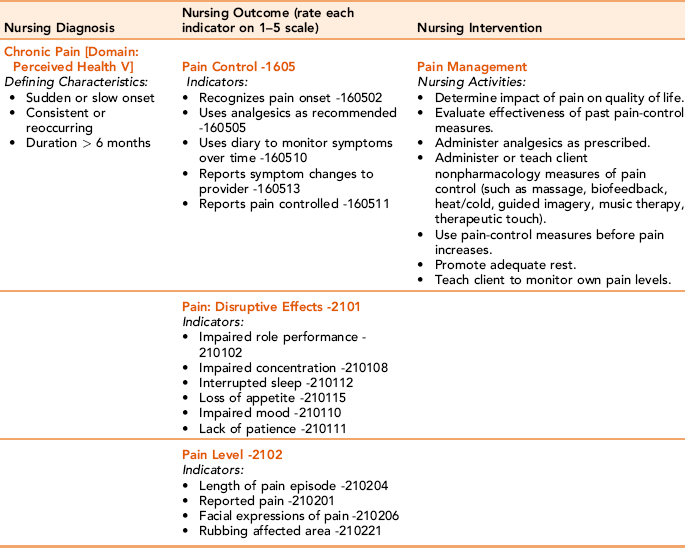
Modified from Bulechek GM, Butcher HK, Dochterman J [McCloskey]: Nursing classification (NIC), ed 5, St. Louis, 2008, Mosby/Elsevier; Johnson M, Bulechek G, Dochterman JM et al: Nursing diagnosis, outcomes, and interventions: NANDA, NOC, and NIC linkages, St. Louis, 2001, Mosby; and Moorhead M, Johnson M, Maas M, Swanson E: Nursing outcomes classification (NOC), ed 4, St. Louis, 2008, Mosby/Elsevier.
North American Nursing Diagnosis Association International: NANDA uses domains based on Gordon’s Functional Health Patterns with diagnoses of actual problems, at-risk for diagnoses, potential problems or syndromes in illness, as well as wellness diagnoses. A nursing diagnosis is a clinical judgment and is the basis for your selection of nursing interventions. Diagnosis domains are health promotion, nutrition, elimination, rest/activity, perception/cognition, self-perception, role relationships, sexuality, coping-stress tolerance, life principles, safety/protection, comfort, and growth and development. NANDA has approved for clinical testing and refinement more than 150 standardized terms to describe nursing diagnoses. Initially designed to classify the problems of hospitalized ill clients, nursing diagnoses have been expanded to include community nursing, especially in areas used by home health nurses
A nursing diagnosis is not another name for a medical diagnosis; rather, it delineates areas for independent nursing actions. When a physician orders a primary intervention, the nursing actions are collaborative, secondary interventions that include monitoring and managing physician-prescribed interventions. A sample list of NANDA-I diagnoses is provided in Box 25-1, with the intent of generating enough material for application in the accompanying learning exercises. Refer to books on nursing diagnoses for complete information. Writing nursing diagnoses takes practice.
Nursing Interventions Classification: This classification of nursing interventions was developed as a standardized language that names and defines an intervention you will use to give direct and indirect care. The interventions are actions that nurses perform in settings relevant to illness prevention, illness treatment, and health promotion. The NIC is used to communicate a common meaning across settings. Its focus is on describing nursing behaviors in the logical order you use to improve client outcomes. There are 542 recognized nursing interventions that are classified in 7 domains. The domains are physiologic basic, physiologic complex, behavioral, safety, family, health systems, and community. Under each domain are classes, and under the classes are the specific interventions. For example, in the domain of physiologic basic there is a class called “immobility management.” Specific intervention activities include bedrest care, cast care maintenance, physical restraint, positioning, splinting, traction, and transport. You can use or modify these interventions to meet your client’s need. Each nursing intervention has a unique code number, and thus can be computerized and potentially could be used to reimburse the nurse. In one example relevant to mobility, the code for “Body mechanics promotion” is 0140, under Class A “Activity and exercise management” (Park, Lu, Konicek, & Delaney, 2007). More than half of the most common nursing interventions are in the physiologic domain. The following case example demonstrates how NIC is used.
NIC experts identify core nursing interventions. A partial list is presented in Box 25-2 (refer to the Elsevier Evolve Web site for complete information). Identification of core interventions provides nurse educators and clinicians with a focus for developing entry-level competencies for nursing practice.
Nursing Outcomes Classification: NOC provides a standard language to name and define client outcomes attained through nursing actions to communicate among nurses and across settings. NOC complements NANDA-I and NIC, and provides a language and coding numbers for evaluating the nursing process. NOC experts identified 385 nursing-sensitive outcomes. An outcome assesses the client’s actual status on specific behaviors (indicators) using a five-point scale, ranging from 1 (severely compromised function) to 5 (function not compromised). The following case example demonstrates how NOC is used.
The Omaha System: In the 1970s, Omaha System research was initiated to address the needs of community health nurses, managers, and administrators. The Omaha System is a comprehensive practice, documentation, and information management tool used by nurses and other health providers (Martin, 2005). Studies show it can also be used in acute care situations. Categories cover common transitional care problems as clients move from hospitalized care to long-term or home care. Transitional care problems include categories such as nutrition, communication, pain, physical activity, and medication administration.
The Omaha System includes an assessment, or Problem Classification Scheme. This consists of four levels: (a) the major domains (environmental, psychosocial, physiologic, and health-related behaviors), (b) specific problems, (c) modifiers, and (d) signs and symptoms. The Intervention Scheme is similarly organized into categories: (a) teaching guidance and counseling, (b) treatments and procedures, (c) case management, and (d) surveillance. Each domain has targets of the intervention. Lastly, it has an outcome component, the Problem Rating Scale for Outcomes. This consists of a five-point ordinal scale assessing the client’s knowledge, behavior, and condition (the status or symptoms of the identified problem). The outcomes rating scale can be applied as a baseline and then reevaluated after the intervention to measure change in knowledge, related behaviors, and symptoms of the originally identified problem (Martin, 2005).
Advantages of nursing classification systems
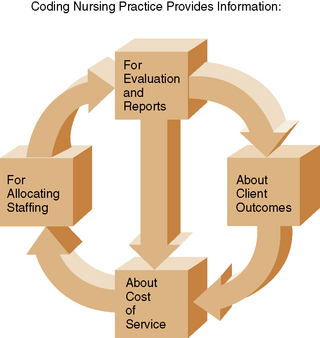
Nursing classification systems provide a standard and common language for nursing care so that nursing contributions to client care become visible and define professional practice. The ANA has issued a position statement stating that standards for terminology are an essential requirement for a computer-based patient record (ANA, 1995b). A standardized language of nursing can help develop realistic standards of care. Groups of client records can be analyzed to describe the client population (e.g., to discover the most common interventions used for a specific nursing diagnosis). Analyzing client records in this way can lead to developing benchmarks that set the desired outcomes for a condition or diagnosis and then measure the client’s actual level of achievement. Agencies could use a nursing classification system to bill for specific nursing care and build further accountability into the care and its documentation. Figure 25-3 shows how coding allows a client’s data to be easily aggregated with other cases to produce a larger picture describing health care delivered by the agency.
Disadvantages of nursing classification systems
Standardized nursing languages need to convince the business and medical interests managing health care agencies of the need to incorporate nursing classification codes as part of their information technology systems. The greatest problem has been that nursing classifications have not yet been thoroughly incorporated into many agency clinical records. Other difficulties include awkward syntax, lack of completeness, and problems with portability to other cultures. As is true of medical classification systems, nursing classification systems continue to evolve and develop as they are used in practice.
Other coding systems in health care
The National Library of Medicine maintains a meta-thesaurus for a unified medical language. Because of the complexity of health care and the variety of providers involved, multiple medical classification systems have emerged. Often providers use several in combination. A major drawback for nursing is that use of computerized documentation systems based on medical code numbers often forces nurses to use classification systems designed to describe medical practice instead of describing nursing assessment and care of clients. In doing so, the richness of the nursing care provided often goes undocumented. Four common medical classification and coding systems are described here.
International classification of diseases
One of the most common medical coding systems is the ICD codes. Classifications in use include ICD-9-CM, ICD-10-CM (codes for inpatient and outpatient diagnoses), and ICD-10-PCS (codes for procedures). The World Health Organization (WHO) published a revised 10th edition in 1994, but the United States did not mandate use until 2013.
Generally, diseases are classified according to body system. ICD-10 uses three to seven digits in an alphanumeric code that begins with a letter to record diagnosis and care interventions, and has 3,000 more categories than ICD-9, which used a 4-digit numeric code. The first digit is always alpha. For example, fractures are coded beginning with S, so a displaced fracture of the neck of the right radius in an initial treatment for closed fracture is S52.131a. In another example, respiratory diseases are all classified beginning with the letter J. Pneumonia is listed in this grouping. Death from pneumonia and influenza is classified under ICD-9 as 480, but under ICD-10 code, it is J10, while to the right of this decimal, the coder can enter codes that identify very specific information, such as the type of pneumonia, which lung was affected, and so on. It is crucial when documenting care to provide enough specificity so that information management workers can correctly and accurately code. Data management and reimbursement depend on the accuracy of this coding.
ICD-10-PCS (Codes for procedures)
These new codes replace CPT codes, which were originally developed by the American Medical Society to provide coding for diagnostic procedures. The client’s record must provide sufficient information about a diagnosis so that the insurance company computer accepts the diagnostic test as relevant and necessary for reaching a correct diagnosis. For example, the ordering of a digoxin level by a provider would be appropriate related to a diagnosis with a code for hypertension with congestive failure, but would not be appropriate or reimbursable for a diagnosis code for epilepsy.
Diagnosis-related groups
Diagnosis-related groups [DRGs] were originally developed for use in prospective payment for the Medicare program. Diagnosis-related group coding provided a small number of codes for classifying client hospitalizations based on diagnosis and severity of illness.
Diagnostic and statistical manual of mental disorders, fourth edition, text revision
The Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision (DSM-IV-TR) is the standardized diagnostic classification for mental illness. The DSM-IV-TR is organized using five axes describing psychiatric diagnosis and functional status. It provides a comprehensive assessment and labeling of psychiatric and mental health–related conditions. The five axes are clinical disorders, personality disorders, general medical conditions, psychosocial and environmental problems, and global assessment of functioning (American Psychiatric Association, 2000).
Joint commission computerized documentation guidelines
Electronic Clinical Information Systems promote entry, storage, and linkage of all information about a client’s health care. Ideally, any Clinical Information System allows ease of access to one client’s information as inputted by any of the client’s health care providers, including the hospital and community. The Joint Commission on Accreditation of Healthcare Organizations has developed standards for uniform data for agencies it accredits. In the past, the Joint Commission required that nurses repeat information recorded by the physician. Now, nursing documentation may consist merely of updating.
Outcome and assessment information set
Beginning in 1998, home care agencies phased in a new requirement to complete a functional health assessment on all Medicare clients before they begin care. The results of the assessment feed into a standardized database. The Health Care Financing Administration (HCFA) developed the Outcome and Assessment Information Set (OASIS) assessment for the purpose of describing home care clients, developing outcome benchmarks, and providing feedback regarding quality of care to home health agencies.
The OASIS assessment is required for home health agencies to receive reimbursement for the care provided to Medicare recipients. Home health care agencies are sent reports comparing their client populations and functions with benchmarks established through analysis of multiple home health agency clients. OASIS can be used to establish standards of quality. The report can also be used by individual home health agencies to monitor and improve outcomes of care. The components of OASIS are essential items for documenting a comprehensive assessment of functional health status of adult home care clients. The assessment documentation is used by HCFA to analyze the health status and needs of Medicare recipients.
OASIS data items include the sociodemographic, environmental, support system, health status, and functional status attributes of nonmaternity adult clients, as well as the attributes of health service utilization. OASIS was not developed as a comprehensive health assessment tool, and home care agencies need to supplement the assessment items. The items of OASIS have evolved over time.
Home health agencies are required to submit OASIS data to a designated state site. The state agency then has the responsibility of collecting OASIS data that can be retrieved from a central repository. These data provide a national picture of health status, outcome, and cost of Medicare enrollees who require home health care. To learn more, visit HCFA’s Medicare Web site (www.HCFA.gov).
Reference terminology systems that exchange data between classification systems
The American Nurses Association recognizes two reference terminologies that can translate the terms between the various classification systems. These allow us to retrieve data even when agencies use several different classification systems.
Systematized nomenclature of medical-clinical terms
Systematized nomenclature of medical-clinical terms (SNOMED-CT) is the most comprehensive reference of medical terminology from many health care languages. Originally developed by American pathologists and the U.K. Department of Health (National Health Service), its goal is to accurately record health care encounters to avoid the injuries or deaths arising from poor communication between health care practitioners. It is endorsed by the American Nurses Association and is used in several other countries including Australia (www.ihtsdo.org/snomed-ct/).
Logical observation identifiers names and codes
Logical Observation Identifiers Names and Codes (LOINC) was developed originally to provide electronic exchange of laboratory data but evolved to include data from lots of classification systems. For example, it includes terms from the Omaha System and the Nursing Management Minimum Data Set (Westra et al., 2008).
Charting formats for documenting nursing care
Use of structured documentation has been found to be associated with more complete nursing records, better continuity of care, more meaningful nursing data, and perhaps with better client outcomes. Use of EHRs has made written charting formats, such as the narrative Problem-Oriented Record (POR), the SOAP format, and so on, obsolete. Still, the focus of the POR on the client’s identified list of health problems can be adapted for electronic charting. A problem list typically consists of medical diagnoses. In POR, nurses refer to the problem list and chart their observations by referring to the listed problem. Information about the client’s progress in each problem area is documented when some measurable change occurs.
In charting electronically, the nurse can call up a preformulated template to record today’s data. There is some evidence that use of EHRs that provide reminders or “prompts” results in more complete documentation (Gunningberg, Fogelberg-Dahm, & Ehrenberg, 2009).
Electronic charting can use flow sheets with predefined client progress parameters based on written standards with preprinted categories of information. They contain daily assessments of normal findings. For example, in assessing lung sounds, the nurse needs to merely check “clear” if that information is normal. Deviations from norm must be completely documented. By marking a flow sheet, you are saying all care was performed according to existing agency protocols. The best example of this format is known as critical pathways or clinical pathways.
Clinical pathways are a documentation system based on standardized plans of care. They are derived by aggregating computerized assessment and outcome data from client records. Locally developed by consensus, they incorporate national evidence-based best practice recommendations. A “pathway” is created, with benchmark milestones clients are expected to achieve within an identified time frame. Each specific disease or procedure has a standard path developed by an interdisciplinary team. The path describes expected care for each day and also permits the nurse to record care given. This improves communication and reduces unnecessary variations in care.
The trend toward more streamlined yet comprehensive and meaningful charting is exemplified in clinical pathways. The goals are to provide a structured tool for planning the highest quality of care; encourage interdisciplinary communication; decrease the time spent charting, because you are charting by exception; focus care on expected client outcomes; and facilitate quality assurance evaluations. Most agencies give the client a copy of the pathway at the time of admission, so that he understands what is expected each day (Figure 25-4). Thus, the pathway becomes a teaching tool for client education and a tool to measure quality.
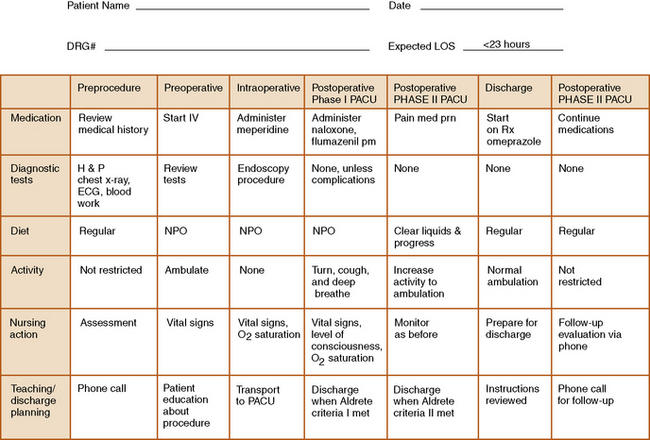
Figure 25-4 Clinical pathway for endoscopy.
DRG, Diagnosis-related group; ECG, electrocardiogram; H&P, history and physical; IV, intravenous; LOS, length of stay; NPO, nothing by mouth; O2, oxygen; PACU, postanesthesia care unit; prn, as needed. (From Monahan FD: Phipps’ Medical-Surgical Nursing: Health and Illness Perspectives, ed 8, 2007, Mosby.)
The clinical pathway is truly an interdisciplinary tool. It allows the entire health team to monitor the client’s progress compared with a standard time frame for progress. A variance or exception occurs when a client does not progress as anticipated or an expected outcome does not occur. A variance is a red flag, alerting staff of a need for further action to assist the client.
Advantages
Use of clinical pathways provides a concise method for documenting routine care. Nurses direct attention to abnormal or significant findings, rather than spending time detailing normal findings. This documentation method is efficient and cost-effective. Multiple studies show it takes less nursing time. Use of pathways is associated with fewer complications and reduced length of hospital stays (Barbieri et al., 2009). Loeb et al.’s 2006 study in nursing home clients showed use of pathways was associated with fewer admissions to hospital, again showing pathways to be cost-effective.
Disadvantages
Charting by exception does not allow for qualitative information. If you fail to perform even one step of the protocol, you are guilty of falsifying the client’s record. Legal decisions in the early 1990s found that certain nurses charting by exception were negligent by virtue of items not charted. Clinical pathways are labor-intensive to develop, and they require “buy-in” by both physicians and nursing staff.
Ethical, regulatory, and professional standards
The use of electronic medical records and storage of personal health information in computer databases has refocused attention on issues of ethics, security, privacy, and confidentiality. For example, a nurse in one unit of a hospital who accesses the electronic medical record of a client who is in another unit and for whom the nurse has no responsibilities for care is violating confidentiality. Ethical professional practice requires that you do not allow others to use your access log-on. Other ethical issues with electronically generated care plans and standard orders center on how to determine who is responsible for the computer-generated care decisions.
Confidentiality and privacy
The Institute of Medicine defines confidentiality as the act of limiting disclosure of private matters appropriately, maintaining the trust that an individual has placed in an agent entrusted with private matters. In the United States, most states have laws that grant the client ownership rights to the information contained in the client’s health record. Electronic storage and transmission of medical records have sparked intense scrutiny over privacy protection. More than two thirds of consumers express concerns that their personal health records stored in an EHR with Internet connections will not remain private. Violations of confidentiality because of unauthorized access or distribution of sensitive health information can have severe consequences for clients. It may lead to discrimination at the workplace, loss of job opportunities, or disqualification for health insurance. Issues of privacy will dominate how nurses and other health care providers address clinical documentation in the years ahead. Currently, a personal medical identification number is used on client records. Hardware safeguards such as workstation security, keyed lock hard drives, and automatic log-offs are used in addition to user identification and passwords to prevent unauthorized access. Some advocate that clients be able to choose how much of their information is shared and be notified when their information is accessed. In the United States, federal law now requires clients be notified in the event of a breach of their EHR. Authorization is not needed in situations concerning the public’s health, criminal, or legal matters. Refer to Chapter 2 for Federal Medical Record Privacy Regulations (HIPAA).
Other legal aspects of charting
Management literature emphasizes the need for quicker documentation that still reflects the nursing process. At the same time, documentation must be legally sound. The legal assumption is that the care was not given unless it is documented in the client’s record. Malpractice settlements have approached the multimillion-dollar mark for individuals whose charts failed to document safe, effective care.
“If it was not charted, it was not done.” This statement stems from a legal case (Kolesar v. Jeffries) heard before Canada’s Supreme Court, in which a nurse failed to document the care of a client on a Stryker frame before he died. Because the purpose of the medical record is to list care given and client outcomes, any information that is clinically significant must be included. Legally, all care must be documented. Aside from issues of legal liability, third-party reimbursement depends on accurate recording of care given. Major insurance companies audit client records and contest any charges that are not documented. Every nurse should anticipate having their clients’ records subpoenaed at some time during their nursing career (refer to Box 25-3 for recommendations).
Any method of documentation that provides comprehensive, factual information is legally acceptable. This includes graphs and checklists. By signing a protocol, check sheet, pathway, and so forth, you are documenting that every step was performed. If a protocol exists in a health care agency, you are legally responsible for carrying it out.
Communicating medical orders
Nurses are required to question orders that they do not understand or those that seem to them to be unsafe. Failure to do so puts the nurse at legal risk. “Just following orders” is not an acceptable excuse. On the other hand, nurses can be held liable if they arbitrarily decide not to follow a legitimate order, such as choosing to withhold ordered pain medication. Reasons for such a decision would have to be explicitly documented. With computerization, it is possible to have standing orders, such as for administering vaccines. The computer is programmed to recognize the absence of a vaccination and then to automatically write an order for a nurse to administer. What might the legal implications be?
Persons licensed or certified by appropriate government agencies to conduct medical treatment acts include physicians, advance practice nurses, and physician assistants. These providers have their own state prescribing numbers and must abide by government rules and restrictions. To prescribe controlled substances they must also have a Drug Enforcement Agency (DEA) number. Nurse practitioners may choose not to apply for a DEA number. Consult your agency policy regarding who is allowed to write client orders for the nurse to carry out.
Faxed orders
The physician or nurse practitioner may choose to send a faxed order. Because this is a form of written order, it has been shown to decrease the number of errors that occur when transcripting verbal or telephone orders. However, there is the risk for violating client confidentiality when faxing health-related information. See the American Health Information Management Association’s general guidelines for faxing medical orders (Hughes, 2001).
Verbal orders
Often, a change in client condition requires the nurse to telephone the primary physician or hospital staff resident to obtain new orders. Most primary providers work in group practices, so it is necessary to determine who is “on call” or who is covering your client when the primary provider is unavailable. It may be necessary to call for new orders if there is a significant change in the client’s physical or mental condition as noted by vital signs, laboratory value reports, treatment or medication reactions, or response failure. Before calling for verbal orders, obtain the chart and familiarize yourself with current vital signs, medications, infusions, and other relevant data. Read Chapter 22 on using the SBAR format to communicate with doctors.
With the growth of unlicensed personnel, there is greater likelihood that a verbal order will be relayed through someone with this status. The legality is vague, but basically, if harm comes to the client through miscommunication of a verbal order, you (the licensed nurse) will be held responsible. The following case examples demonstrate typical scenarios you may encounter:
Applications
To practice nursing in coming years, you will need to continually upgrade your technology skills. As students, you learn skills such as data entry, data transmission, word processing, Internet accessing, spreadsheet entry, and use of standard language and codes describing practice. Voice recognition software may eventually revolutionize clinical documentation, making documentation easier for nurses.
Documenting on a client’s health record
Documenting electronically requires learning the specific system at your agency. There is a learning curve; that is, initially it may take longer, but as you become familiar with the system, EHRs should increase your nursing efficiency. Use Exercise 25-1 to stimulate discussion of appropriate documentation.
Confidentiality
Ethical and legal dilemmas inherent in use of computerized systems require continued vigilance, especially regarding the concern of protecting client privacy. As cases come to court, a body of case law will provide some guidance. HIPAA regulations mandating clients’ right to privacy are the current guidelines. You need to become aware of threats to privacy and your obligation to protect your clients’ privacy where possible. Discuss the ethical dilemma provided.
Use of universal nursing languages and codes
The need to identify and analyze outcomes of nursing practice requires computer-compatible frameworks. Adoption allows us to gather and analyze large amounts of information to identify which nursing interventions produce positive client outcomes. Interoperable computer coding applications help do this across health settings. Think about this “bigger picture” as you learn use of nursing terminology in your clinical practice.
Dochterman and colleagues (2005) were among the first to demonstrate that NIC-coded patterns of nursing interventions can be analyzed. They examined three types of interventions for older adults in 13,758 acute care hospitalizations. Data were obtained for interventions for clients with diagnoses of heart failure and hip fracture, and for fall prevention interventions. Results demonstrated that interventions occurred throughout the hospitalization period, were individualized, and could be classified into daily patterns (and potentially could produce better health outcomes). Information describing the type and amount of nursing care delivered could also potentially help staff managers plan for amount and type of staff needed on a unit.
Standardization work is ongoing internationally, as evidenced by groups such as the Association for Common European Nursing Diagnoses, Interventions, and Outcomes. Try Exercise 25-2 to explore how you might apply information.
Summary
This chapter focuses on electronic documentation of care in the nurse-client relationship. Documentation refers to the process of obtaining, organizing, and conveying information to others in the client record. Discussion of new HIT including the nurse’s role in using EHRs emphasized their role in reducing redundancy, improving efficiency, reducing cost, decreasing errors, and improving compliance with standards of practice. Chapter 26 discusses technology that can facilitate communication among health care workers, increase client education, and assist the providers of health care with decision making.
References
American Nurses Association. ANA Position Statement No.12.22, On access to patient data http://nursingworld.org/readroom/position/joint/jtdata.htm, 1995.
American Nurses Association. ANA Position Statement No. 12.20, Position paper on computer-based patient record standards http://nursingworld.org/readroom/position/joint/jtcpri1.htm, 1995.
American Psychiatric Association. Diagnostic and statistical manual of mental disorders, ed 4. Washington, DC: Author, 2000. [text revision].
Barbieri, A., Vanhaecht, K., Van Herck, P., et al. Effects of clinical pathways in the joint replacement: a meta-analysis. BMC Med. 2009;7:32.
Bulechek, G.M., Butcher, H.K., Dochterman, J., [McCloskey]. Nursing classification (NIC), ed 5, St. Louis, Mosby/Elsevier, 2008.
Carter J.H., ed. Electronic health records, ed 2, Philadelphia: ACP Press, 2008.
Dochterman J.M., Bulechek G.M., eds. Nursing interventions classification (NIC), ed 4, St. Louis: Mosby, 2004.
Dochterman, J., Titler, M., Wang, J., et al. Describing use of nursing interventions for three groups of patients. J Nurs Scholarsh. 2005;37(1):57–66.
Gruber, D., Cummings, G.G., Leblanc, L., et al. Factors influencing outcomes of clinical information systems implementation, CIN. Comput Inform Nurs. 2009;27(3):151–163.
Gunningberg, L., Fogelberg-Dahm, M., Ehrenberg, A., et al. Improved quality and comprehensiveness in nursing documentation of pressure ulcers after implementing an electronic health record in hospital care. J Clin Nurs. 2009;18:1557–1564.
Hughes, G., Practice brief: facsimile transmission of health information (updated), AHIMA Practice Brief. J AHIMA, 2001;72(6):64E. 64F, Available online:, http://library.ahima.org/ xpedio/groups/public/documents/ahima/bok2_000116.hcsp?dDocName=bok2_000116.
Johnson, M., Bulechek, G., Dochterman, J.M., et al. Nursing diagnosis, outcomes, and interventions: NANDA, NOC, and NIC linkages. St. Louis: Mosby, 2001.
Keepnews, D., Capitman, J.A., Rosati, R.J., et al. Measuring patient-level clinical outcomes of home health care. J Nurs Scholarsh. 2004;35(1):79–85.
Loeb, M., Carusone, S.C., Goeree, R., et al. Effect of a clinical pathway to reduce hospitalizations in nursing home residents with pneumonia. JAMA. 2006;295(21):2503–2510.
Martin, K.S. The Omaha System: a key to practice, documentation and information management, ed 2. St Louis: Elsevier, 2005.
McCormick, K.A., Jones, C.B., Is one taxonomy needed for health care vocabularies and classifications? Online J Issues Nurs, 1998;3(2). manuscript 2 Available online:, www.nursingworld.org/MainMenueCategories/ANAMarketplace/ANAPeriodicals/OJIN/ TableofContents/Vol31998/No2Sept1998/Isonetaxonomyneeded.aspx. [Accessed December 6, 2009].
Moody, L.E., Slocumb, E., Berg, B., et al. Electronic health records documentation in nursing: nurses’ perceptions, attitudes and preferences. Comput Inform Nurs. 2004;22(6):337–344.
Moorhead, M., Johnson, M., Maas, M., et al. Nursing outcomes classification (NOC), ed 4. St. Louis: Mosby/Elsevier, 2008.
Muller-Staub, M., Lavin, M.A., Needham, I., et al. Meeting the criteria of a nursing diagnosis classification: evaluation of ICNP, ICF, NANDA, and ZEFP. Int J Nurs Stud. 2007;44(5):702–713.
Nemeth, L.S., Wessell, A.M., Jenkins, R.G., et al. Strategies to accelerate translation of research into primary care with practices using electronic medical records. J Nurs Care Qual. 2007;22(4):343–349.
North American Nursing Diagnosis Association (NANDA). Nursing diagnoses: definitions and classifications 2009–2011. Philadelphia: Wiley-Blackwell, 2009.
Park, H., Lu, D., Konicek, D., et al. Nursing interventions classification in systematized nomenclature of medical terms: a cross-mapping validation. CIN Comput Inform Nurs. 2007;25(4):198–208.
Poissant, L., Pereira, J., Tamblyn, R., et al. The impact of electronic health records on time efficiency of physicians and nurses: a systematic review. J Am Med Inform Assoc. 2005;12(5):505–516.
Rutherford, M.A., Standardized nursing language: what does it mean for Nursing Practice? OJIN, 2008;13(1). Available online:, www.nursingworld.org/MainMenuCategories/ANAMarketplace/ANAPeriodicals/OJIN/Table ofContents/vol132008/No1Jan08/ArticlePreviousTopic/StandardizedNursingLanguage.aspx.
Siegler, E.L., Adelman, R. Copy and paste: a remediable hazard of electronic health records. Am J Med. 2009;122(6):493–494.
Silva, C., Only 1.5% of non-Federal hospitals report having full EHRs. Am Med News 2009. April 6 Available online:, www.ama-assn.org/amednews/2009/04/06/gvsc0406.htm. [Accessed April 6, 2009].
Thompson, D., Johnston, P., Spurr, C., et al. The impact of electronic medical records on nursing efficiency. J Nurs Admin. 2009;39(10):444–451.
Westra, B.L., Delaney, C.W., Konicek, D., et al. Nursing standards to support the electronic health record. Nurs Outlook. 2008;56(5):258–266.