Chapter 64 Malpositions and malpresentations
After reading this chapter, you will be able to:
Introduction
This chapter considers the recognition, management and care of the fetus when it presents in an occipitoposterior (OP) position, by the breech, face or brow and when an oblique or transverse lie results in a shoulder presentation. Compound presentation is also discussed.
Malposition and malpresentations of the fetus can occur in both pregnancy and labour. The midwife has a key role in identifying these, using best evidence to inform and support the mother and effective skills to undertake safe management and care. With associated higher rates of maternal and perinatal morbidity and mortality, it is essential that careful attention be given to the diagnosis of malposition and malpresentations in order to maximize fetal outcomes (Baxley 2001, Cheng & Hannah 1993, Hannah et al 2000, Pritchard & MacDonald 1980).
While primarily a practitioner of the ‘normal’, the midwife must be fully conversant with the problems and practicalities that both malposition and malpresentations can present. In such circumstances, skills are often tested to the limit and the midwife’s ability to gain the confidence of the woman and to work effectively with the wider healthcare team is paramount in achieving a safe and successful outcome for both mother and baby (ALSO 2003). In dealing with malpositions and malpresentations of the fetus, the midwife needs to be knowledgeable about the latest evidence or lack of it, that will help to inform a woman’s decisions in relation to her care and provide her with the options available (Evans 2007).
This may be difficult and, in spite of the evidence, some women may choose a path, for personal, cultural or religious reasons, that is not in keeping with the recommended evidence or accepted institutional practices. Nevertheless, it is a woman’s right to choose for herself and the midwife needs to ensure that in such circumstances, the woman continues to receive the relevant information, advice and support necessary. In achieving this, the midwife should consult with her supervisor of midwives and, with the woman’s permission, share the proposed plan of care with her and the lead obstetrician. All discussions with the woman must be clearly documented in her maternity notes and accurately reflect the advice given, the options available and choices she has made.
Identifying Malpositions and Malpresentations of the Fetus
Midwives must be able to employ a range of skills to assist them in identifying the fetus in:

These require midwives to take a detailed history, keenly observe the woman’s body and behaviours, and carry out a considered and careful clinical examination. Above all, they must be able to draw the findings together in order to analyse and make sense of them. From this, the midwife can then make a diagnosis, upon which discussions with the woman, clinical decisions and further professional judgements will be based.
Incidence
The incidence of malpositions and malpresentations varies according to lifestyle, gestation and parity, as well as the condition of the mother and fetus. The midwife needs to consider the likelihood and the reasons why these presentations might occur as part of the assessment, diagnosis and plan of the woman’s care.
It is essential that the midwife recognize that a malposition is the commonest cause of non-engagement of the fetal head at term in a primigravida. It is the commonest cause of prolonged labour and mechanical difficulties associated with the birth. Persistent OP position was a significant factor in caesarean section and instrumental deliveries with less than half of the OP labours ending in a spontaneous birth of the baby (Fitzpatrick et al 2001).
Clinical Assessment
In identifying malpositions and malpresentations, the midwife should take into account the gestational age of the fetus, the woman’s parity, and any history that might suggest the likelihood of such anomalies or abnormalities. The clinical skills of abdominal and vaginal assessment that the midwife may perform as part of a woman’s antenatal and intrapartum care, are central to the recognition of the presentation, engagement, attitude, lie and position of the fetus. Underlying this is the need to be fully conversant with the anatomy of the maternal pelvis, the engaging diameter of the fetal presentations, and the implications of these for the birthing process.
Malposition of the Occiput
The fetus is in an occipitoposterior position (OPP) when the fetal occiput lies adjacent to the sacroiliac joint and occupies either the left or right posterior quadrants of the mother’s pelvis with the brow directed anteriorly.
Occipitoposterior positions occur in approximately 10–25% of pregnancies during the early stage of labour and in 10–15% during the active phase, most of which end normally (Gardberg & Tuppurainen 1994a).
Causes of OPP include the following:
Sutton and Scott (1996) highlighted the use of optimal fetal positioning (see website) in helping women to increase their chances of normal childbirth. Other work suggests that such strategies for reducing persistent OPP at birth may be more complex (Hunter et al 2007) (see website).
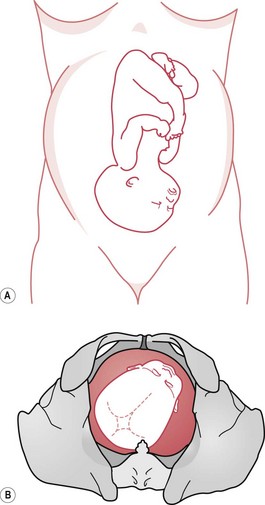
Occipitoposterior positions (Fig. 64.1) throw a heavy responsibility on the midwife, but being overly pessimistic does little to help the mother. Where the labour is progressing satisfactorily, the outcome is likely to be spontaneous rotation to an anterior position followed by a normal vertex delivery.
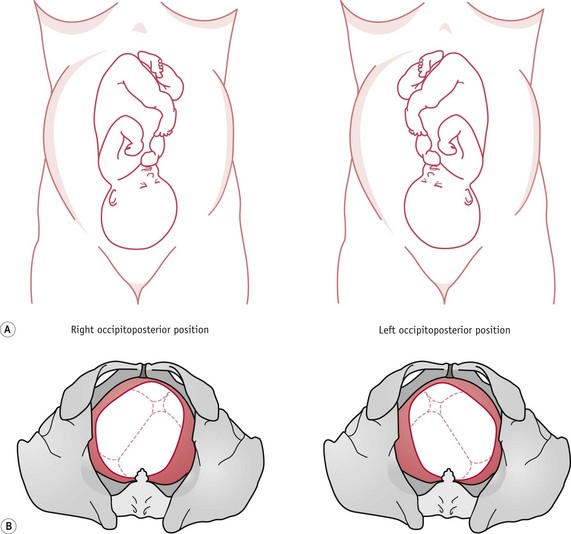
Figure 64.1 Occipitoposterior positions. A. Abdominal findings – the anterior shoulders are well out from the midline or fetal limbs are easily palpable. This may cause a misdiagnosis of multiple pregnancy. B. Vaginal findings – on vaginal examination, the anterior fontanelle is easily felt and recognized by its shape and size.
While malpositions can and do resolve, the midwife should be aware of the potential for delay and the possibility of adverse outcomes that may arise when the labour is prolonged or the OPP persists.
Slow progress should alert midwives to the possibility of abnormal labour and they must be vigilant to promptly recognize any complications that may arise and call for assistance. They should be ready to act and make decisive professional judgements when indicated by the maternal or fetal condition, poor progress of labour, or the mother’s psychological state and frame of mind. In the presence of an obstetric urgency or emergency, such as deep transverse arrest (DTA) or cord prolapse, the midwife must seek immediate medical assistance.
In caring for a woman in prolonged labour, the midwife has the exacting task of maintaining a close watch on the progress she is making, attending to her physical care and providing the encouragement, reassurance and emotional support that the woman needs.
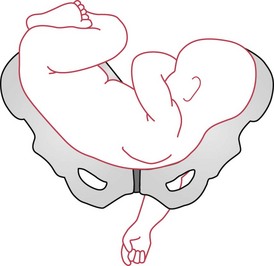
The midwife also needs to be aware of the altered mechanism of a fetus in a posterior position, during which the fetus tends to be in a deflexed attitude, with the anterior fontanelle immediately over the internal cervical os. The fetal spine is towards the forward curve of the maternal lumbar spine, so that the fetus finds it difficult or impossible to adopt a flexed position. As the fetal spine straightens, the fetus tends to ‘square’ the shoulders and raise the chin from the chest, resulting in a deflexed, erect ‘military’ attitude of the fetal head, as shown in Figure 64.2.
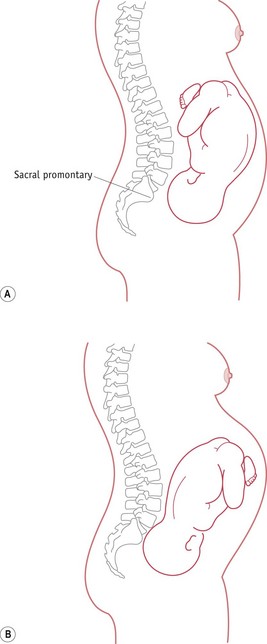
Figure 64.2 The ‘military’ posture of the fetus in an occipitoposterior position. A. Well-flexed fetus. B. OP position. Deflexed with straight spine and wider engaging diameter.
Such movements bring the fetal head into a more difficult relationship with the inlet of the maternal pelvis. Misaligned above the pelvic brim, the fetal head is slow to engage as its larger diameters present. This ill-fitting presentation may also result in early rupture of the membranes and the danger of cord prolapse.
There is a loss of fetal axis pressure, contractions are not effectively stimulated and descent is delayed. This can lead to slow, uneven cervical dilatation and prolonged labour. In the process of birth, the engaging diameter of the fetal head is reduced, with that at right angles being elongated. In an occipitoposterior position, the fetal head is compressed in unfavourable diameters, resulting in ‘sugar loaf’ moulding, creating a greater risk of damage to the tentorium cerebelli and the likelihood of intracranial haemorrhage. With a persistent occipitoposterior position, these wider diameters may also result in increased trauma to the woman’s vagina and perineum.
Diagnosis of the occipitoposterior position
During pregnancy
The diagnosis is often made by abdominal examination. On inspection, the abdomen appears flattened, or slightly depressed, below the umbilicus (see Fig. 64.3). On palpation, the fetal head is commonly high. If the fetus is almost occipitolateral, the deflexed head may feel large, because the occipitofrontal diameter is palpated.
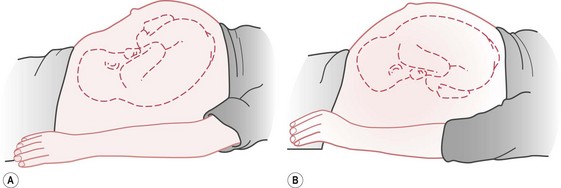
Figure 64.3 Abdominal contour: A. when the fetus is in the occipitoposterior position, compared to B. the more rounded contour of the occipitoanterior position.
The occiput and brow may be felt at the same level at the pelvic inlet, while the fetal back can be palpated out in the flank. If the occiput is markedly posterior, the high head feels small, as the bitemporal diameter is palpated; movements of the fetal limbs can often be seen or easily felt and it may be impossible to feel the back (see Fig. 64.1). The fetal heart sounds can be heard in the midline just below the umbilicus. If the heart sounds are audible in one flank, it suggests that the fetal back is directed towards that side.
During labour
The diagnosis may be made by abdominal examination, though as labour advances, the head may become flexed and engaged. The cephalic prominence of the sinciput can be felt above the pubic bone and on the opposite side to the fetal back. The midwife should be alert whenever the cephalic prominence is felt on the same side as the fetal back and should consider the possibility of a face or brow presentation and seek to exclude these. A deflexed head prior to or in the process of engagement in the maternal pelvis can become extended to a brow, or hyperextended to a face presentation. ‘Coupling’ of contractions is associated with occipitoposterior positions (ALSO 2003). The midwife may identify this phenomenon when she palpates the mother’s abdomen or else on the tocograph tracing if electronic fetal monitoring is in progress.
On vaginal examination the findings depend on the degree of flexion of the fetal head. Palpation of the anterior fontanelle is usually diagnostic of an occipitoposterior position. When the head is partially or well flexed, the anterior fontanelle is felt towards the front of the pelvis, while occasionally the posterior fontanelle is just within reach at the back. With a deflexed head, the anterior fontanelle is almost central and, unless obscured by caput, easily recognizable by its size and shape.
Progress in labour
The progress of labour will depend upon the regularity and strength of uterine contractions and the degree of flexion of the fetal head. The shape of the maternal pelvis and the maternal position may be significant in determining how the fetus negotiates the pelvic inlet, cavity and outlet.
Flexion of the fetal head
If the head is flexed, labour will probably be completely normal. The engaging diameter is the suboccipitofrontal (10 cm). The occiput reaches the pelvic floor and rotates anteriorly through three-eighths of a circle and the baby is born with the occiput anteriorly (Fig. 64.4).
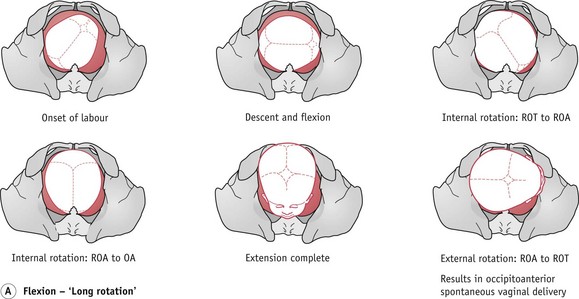
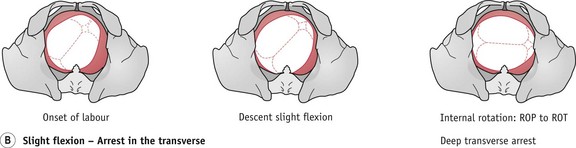
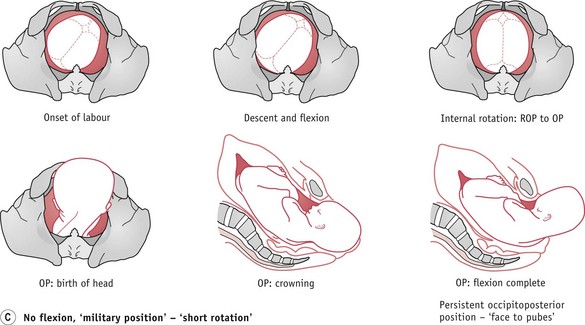
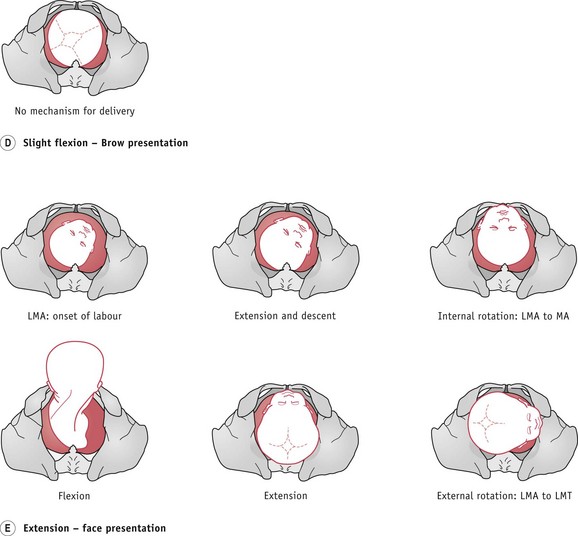
Figure 64.4 Possible outcomes of an occipitoposterior position. The fetal head enters the pelvis with the occiput posteriorly.
When the head remains deflexed, it tends to remain high or is slow to engage. Labour is slow to become established, with hypotonic and irregular uterine contractions. However, flexion may improve, and once the head becomes flexed, labour usually accelerates and continues normally, with a long internal rotation and an occipitoanterior birth (Fig. 64.4A).
Deflexion of the fetal head
The midwife needs to be fully conversant with the mechanism of the persistent occipitoposterior position and how this translates into what the woman experiences. If the head remains deflexed, labour is likely to be prolonged and painful, with backache a prominent characteristic. The outcome is then dependent on the size, shape and dimensions of the pelvis in relation to those of the fetal skull.
Persistent occipitoposterior position (POP)
The mechanism is that the lie is longitudinal, presentation vertex and attitude deflexed – the engaging diameter is the occipitofrontal and measures 11.5 cm. The position may be either right or left occipitoposterior and the presenting part is the anterior aspect of the right (ROP) or left (LOP) parietal bone. Descent takes place with deficient flexion and the biparietal diameter of the fetal head is held up on the sacrocotyloid diameter of the maternal pelvis, so that the sinciput becomes the leading part. When the sinciput meets the resistance of the pelvic floor, it rotates forward one-eighth of a circle (Fig. 64.4C). The sinciput passes under the pubic arch and the occiput into the hollow of the sacrum. With good contractions, spontaneous delivery ensues and, with flexion, the occiput sweeps the maternal perineum and, once the glabellar is visible, the brow and face are delivered by extension. The rest of the mechanism follows that of a normal, vertex presentation (see Ch. 37). This is called persistent occipitoposterior position or ‘face-to-pubes’ delivery and is often associated with an anthropoid pelvis (Fig. 64.4C).
Deep transverse arrest (DTA)
DTA (Fig. 64.4B) may occur if the head remains deflexed. The fetal head may attempt a long rotation, but because of wider diameters and prominence of the ischial spines, it can become caught in the transverse diameter of the obstetric outlet, between the ischial spines.
DTA should be suspected if there is delay in the second stage of labour. On vaginal examination, the sagittal suture is found in the transverse diameter of the pelvis with a fontanelle at each end, close to the ischial spines. In such circumstances, appropriately skilled midwifery or medical assistance should be obtained and, with the use of vacuum extraction (ventouse), the fetal head may be rotated to an anterior position and delivered. Manual rotation of the occiput may also be considered. The midwife should be knowledgeable about this procedure (NMC 2008), and needs to explain the procedure fully to the woman, obtaining informed consent (see website). This should not delay summoning additional assistance.
Occasionally, caesarean section is necessary to deliver the fetus in an occipitoposterior position. This is likely when complications such as cord prolapse and fetal distress occur, or when true cephalopelvic disproportion is diagnosed.
Extension of the fetal head
It is possible that the fetal head may either be in a slightly extended position, or may adopt this as labour progresses, resulting in a brow presentation (Fig. 64.4D). Unless the fetus is particularly small or preterm, then it is unlikely that it will be born vaginally. Full extension of the fetal head may lead to a face presentation, which, if mento-anterior, may deliver vaginally (Fig. 64.4E).
Complications of OPP
Midwives need to carefully consider complications that might arise (Table 64.1) and be fully aware of what action should be taken to prevent or minimize these occurring in their management and care of a woman whose baby is in an occipitoposterior position.
Table 64.1 Complications of occipitoposterior (OP) position
| Complication | Reason |
|---|---|
| Early rupture of the membranes | Poorly fitting presenting part and uneven pressure on the forewaters |
| Cord prolapse | As with any ill-fitting presenting part, the membranes tend to rupture early and the cord may prolapse |
| Prolonged labour | This is associated with a deflexed head, poorly fitting presenting part and misaligned fetal axis pressure. A slightly contracted pelvis may compound this. Hypotonic and inefficient or over-efficient uterine contractions may result. In such circumstances, the development of either fetal or maternal distress is more likely and operative intervention and anaesthesia are often necessary. Postpartum haemorrhage is therefore an added risk |
| Retention of urine | This may occur with prolonged labour and the pressure on the urethra that results from the wider diameters of the OP position |
| Premature expulsive effort | The wider diameter of the OP position results in pressure on the sacral nerves and the woman may feel the need to push before full dilatation of the cervix. Early distension of the perineum and dilatation of the anus can also occur while the head is still high |
| Infection | This is more likely because of early rupture of the membranes, especially if labour is prolonged, and can be compounded by an increased number of vaginal assessments |
| Trauma to the mother’s soft tissues | The risk of trauma is increased with the wider diameter of the OP position. When this is persistent, the biparietal diameter and large occiput distend the maternal perineum. Instrumental delivery may also increase the risk of maternal trauma |
| Post-traumatic stress disorder or postnatal depression | Prolonged, difficult, painful and traumatic labour might result in mental ill-health. This can be exacerbated when the mother has no control over events and is not involved in decision-making. This, together with maternal exhaustion and an unsettled baby, may lead to difficulty in maternal–infant bonding |
| Maternal exhaustion | In prolonged labour, maternal exhaustion may follow the birth |
| Unsettled or difficult-to-feed infant | In an OP position and a prolonged labour, the baby’s head will have been compressed in an unnatural angle, resulting in discomfort and pain |
| Fetal intracranial haemorrhage | Upward moulding of the fetal skull may lead to stretching and damage of the tentorium cerebelli and consequent tearing of the great vein of Galen, resulting in haemorrhage and intracranial damage |
| Increased perinatal mortality and morbidity | This might result from cord prolapse, prolonged labour, instrumental delivery, infection and intracranial haemorrhage, and is increased because of hypoxia and birth trauma |
Malpresentations of the Fetus
Malpresentation refers to the orientation of the fetus and may be diagnosed during pregnancy or in labour. Any presentation other than vertex is termed a malpresentation and this therefore includes breech, face, brow and shoulder. When midwives encounter a malpresentation of the fetus, they will draw upon similar knowledge and many of the skills they use in the care and management of women whose babies were in an occipitoposterior position.
In all malpresentations there is commonly an ill-fitting presenting part: often associated with early rupture of the membranes because of uneven pressure on the bag of forewaters. This results in an increased risk of cord prolapse. An ill-fitting presenting part is also associated with poor uterine action and slower cervical dilatation, and therefore labour may be prolonged with the concomitant risk of infection and operative intervention.
Breech presentation
A breech presentation occurs when the fetal buttocks lie lowermost in the maternal uterus and the fetal head occupies the fundus. The lie is longitudinal, the denominator is the sacrum and the presenting diameter is the bitrochanteric, which measures 10 cm.
Breech presentation is common before 37 weeks’ gestation, with a suggested incidence of 15% at 29–32 weeks’ gestation reducing to 3–4% at term (Hannah et al 2000, MIDIRS 2008). One fetus in four will present by the breech at some stage in pregnancy. In preterm labour it is not surprising to find the breech presenting and these infants comprise a quarter of all babies born by the breech. However, by the 34th week of pregnancy, the majority will have turned to a vertex presentation.
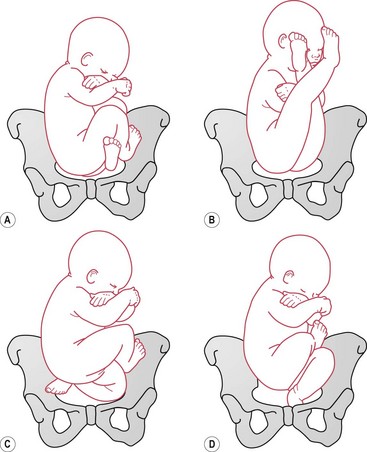
Types
Four types of breech presentation are described (Fig. 64.5). They are determined by the way in which the fetal legs are flexed or extended, and these have implications for the birth.
There is a higher perinatal mortality and morbidity rate with breech presentation, which is largely due to prematurity and congenital abnormalities of the fetus, as well as birth asphyxia and birth trauma (Cheng & Hannah 1993, Hannah et al 2000). The clinical setting, failure to respond to delay and lack of clinical experience may also contribute to poorer outcomes (Kotaska et al 2009).
In providing care, the midwife needs to be conversant with the latest developments surrounding the management and optimal mode of delivery. While the outcomes of the ‘Term Breech Trial’ have dominated the discourse around the mode and management of breech births (Hannah et al 2000) and significantly influenced practice in the United Kingdom and abroad, the evidence is at best uncertain, conflicting and contradictory (Glezerman 2006, Goffinet et al 2006, Hofmeyr & Hannah 2003, Kotaska 2004, Kotaska et al 2009, Van Idderkinge 2007, Waites 2003, Whyte et al 2004).
However, as Shennan & Bewley (2001) point out, the need to provide expertise in vaginal breech delivery will not disappear. Some women present too late, even when a policy of planned caesarean section is in place, and some women will reject the choice of a planned caesarean section and choose to have a vaginal breech birth in either the hospital or home setting because of personal, cultural or religious reasons.
Causes
The fetus may adopt the breech position for a variety of reasons, though the true cause is often unknown. Waites (2003) found that in most cases no single cause can be identified, and it may result from a random occurrence (Bartlett & Okun 1994). The most common cause is likely to be a ‘benign error of orientation’ in which the fetus sits in the breech for no known cause and without any obvious abnormalities. Other causes include:
See Table 64.2.
Table 64.2 Causes of breech presentation
| Primigravidae | Firm abdominal and uterine muscles may prevent flexion of the fetal legs, especially when they are already extended. |
| Uterine anomalies | Bicornuate uterus may restrict fetal movement. Previous breech birth may also be strongly associated with a uterine anomaly. |
| Oligohydramnios | Reduced liquor volume restricts the ability of the fetus to turn in the uterus. The condition may also be associated with fetal anomalies and fetal compromise. |
| Placental location | Placenta praevia may prevent the fetal head from fitting into the lower uterine segment and entering the pelvis. A placenta situated in one or other cornua of the uterus reduces the breadth of space in the upper segment and can lead to a breech presentation. |
| Uterine fibroids | These can interfere with fetal activity or when situated in the lower uterine segment can prevent the fetal head from entering the lower pole of the uterus. |
| A contracted pelvis | The fetal head is unable to enter the pelvic brim. |
| Fetal anomalies such as trisomy 21 and hydrocephalus | These can lead to fetal hypotonia in which the lack of movement, reduced or restricted fetal activity makes it difficult for the fetus to turn. Hydrocephalus can prevent the fetal head engaging in the pelvis. |
| Multiple pregnancy | There is usually insufficient space to turn. Twins may present vertex and breech and, as such, spontaneous version is unlikely. |
| Maternal alcohol or drug abuse | May lead to fetal hypotonia in which the lack of movement, reduced or restricted fetal activity makes it difficult for the fetus to turn. |
| Grande multiparity | Lax abdominal and uterine muscles allow movement and may lead to an unstable lie. |
| Polyhydramnios | Overdistension of the uterus enables the fetus to be more mobile. |
| Prematurity | Increased incidence at earlier gestation. Smaller fetus with greater space within the uterus to adopt a breech position. |
| Impaired fetal growth, short umbilical cord and fetal death | Compromised fetus may result in decreased fetal activity. May be associated with fetal or maternal conditions having an adverse effect on the fetus, which results in reduced or restricted fetal mobility. |
Diagnosis during pregnancy
The midwife needs to be alert to the gestational age of the fetus but should not be unduly concerned prior to 36 weeks’ gestation. A history of a previous breech presentation may be significant, and if the breech persists, then referral to an obstetrician should be made and the likely cause identified.
The woman may give a history of discomfort under the ribs due to the presence of the hard fetal head or describe fetal movements in the lower pole of the uterus. Her description of her baby’s movements and how she feels can be valuable elements in the diagnosis of a breech presentation (Banks 2000).
Abdominal examination
usually allows the diagnosis to be confirmed. It may be difficult to distinguish between a breech and a vertex presentation and a high index of suspicion is an asset for diagnosis (ALSO 2003).
The method of conducting the abdominal examination may have consequences for detecting a breech presentation or finding a ballottable fetal head in the uterine fundus.
Although inspection of the maternal abdomen usually reveals nothing that indicates a breech presentation, occasionally fetal movements can be seen in the lower pole. On palpation the presenting part feels firm but less hard and less rounded than the head. The diagnosis is usually made by feeling the hard, round and ballottable head in the fundus of the uterus.
Over time, the sequence in which Leopold manoeuvres (see website) have been applied during abdominal palpation have changed, with identification of the lie often taking place before palpation of the presenting part. In such circumstances, especially at term, the uterus might be stimulated, increasing tone or even stimulating a contraction. This results in the presenting part feeling hard, and the fetal head, if in the uterine fundus, becomes fixed and more difficult to ballot. As a consequence, breech presentations can be missed.
A primigravida with an extended breech may simulate a cephalic presentation. The woman’s firm abdominal muscles brace the extended legs and compress the breech, allowing it to enter deep into the pelvis. The presenting part may be out of reach of the midwife’s palpating fingers and can be mistaken for the deeply engaged head. The baby’s feet, lying under the chin, make ballottement more difficult. If the placenta is situated on the anterior uterine wall, identification of the fetal head is further obscured.
Fetal heart sounds, classically heard above the umbilicus in breech presentations, may be heard at maximum intensity in an extended breech where the heart sounds are commonly heard in a vertex presentation: halfway between the superior anterior iliac spine and the maternal umbilicus.
Ultrasound imaging is helpful in:
Vaginal examination
may be carried out by the midwife or obstetrician to exclude a deeply engaged head and confirm breech presentation. If the head is deeply engaged, the shoulders palpate just above the pelvic brim and are sometimes difficult to distinguish from the breech. On vaginal examination, an extended breech has a hard, compressed presenting part similar to a cephalic presentation, and the cleft of the buttocks may imitate the line of the sagittal suture.
Midwives should be aware of these deceptive findings and unless certain that the presentation is vertex, should be cautious. If in doubt or convinced that the presentation is breech after 36 weeks’ gestation, they should seek confirmation by ultrasound examination, informing the woman of the findings. Where a breech presentation exists, the midwife should discuss the evidence and implications and, as appropriate, refer to a senior obstetric colleague.
Diagnosis during labour
In labour the presenting part may initially be high. On vaginal examination the breech feels soft and irregular and no sutures or fontanelles are palpable. The hard sacrum and the anus should be felt and it is important to distinguish the breech from a face presentation.
The midwife will note that in a breech presentation the landmarks of the fetal ischial tuberosities are on either side of the fetal anus and form a straight line. This differs from a face presentation, in which the fetal mouth and malar prominences form a triangle (ALSO 2003).
Fresh, ‘toothpaste like’, thick meconium may be found on the examining finger and is diagnostic of a breech presentation. The fetal genitalia are soft and not easily recognized because they become oedematous.
In a flexed breech, the feet may be palpable alongside the buttocks, but these usually fall back behind the presenting part as labour advances. On vaginal examination, the features of the foot that distinguish it from a hand are: shorter digits, larger size but limited range of movements of the big toe, and the presence of a heel.
Associated risks
Breech presentation carries increased risks to a healthy mother and fetus from either a complicated vaginal delivery or caesarean section (Cheng & Hannah 1993, Hofmeyr 1991, Kotaska et al 2009, Van Idderkinge 2007). A high incidence of childhood handicap following breech presentation has also been identified and found to be similar in those infants delivered after a trial of labour and following an elective caesarean section (Danielian et al 1996). Poor outcomes following vaginal breech delivery, therefore, might result from some underlying condition causing breech presentation rather than damage during delivery (Hofmeyr & Hannah 2003). A study following up the ‘Term Breech Trial’, found no differences in long-term neonatal morbidity between babies born by vaginal birth and those born by caesarean section (Whyte et al 2004).
Care and management – pregnancy
The midwife who diagnoses a breech presentation should, depending on the woman’s preferences, either refer her to a senior obstetrician or discuss the case with her Supervisor of Midwives. The midwife must inform the woman as to her options of care and these, together with the mother’s choices, should be clearly documented in her maternity record.
The three options she will need to consider are:
Spontaneous cephalic version of the breech
While the vast majority of breech presentations will have turned to the vertex by term – 57% of pregnancies after 32 weeks’ gestation and 25% after 36 weeks’ gestation (Westgren et al 1985) – it occurs with diminishing frequency as pregnancy advances.
The use of alternative approaches and techniques to promote spontaneous cephalic version has been widely reported, though the effectiveness of these has yet to be confirmed. There is insufficient evidence from well-controlled trials to support the use of postural management in converting breech to cephalic presentations (Hofmeyr & Kulier 2000). Moxibustion – used in traditional Chinese medicine to encourage fetal activity and version of the fetus in breech presentations (Budd 2000, Cardini & Weixin 1998) – was found, in a systematic review (Coyle et al 2005), to have insufficient evidence to support its use to correct breech presentation.
External cephalic version (ECV)
is strongly advocated (RCOG 2006a) and well evaluated (Collins et al 2007, Hofmeyr & Kulier 1996a) (see website). The procedure is considered both safe and effective, reducing the chance for breech presentation at birth and caesarean section. Tocolysis is also associated with fewer failures of ECV (Hofmeyr & Gyte 2004). ECV should be offered to all women with an uncomplicated breech presentation at term. This role could be undertaken by appropriately trained and supported midwives and obstetric colleagues, and could significantly reduce the incidence of breech presentation (Taylor & Robson 2003).
Mechanism of vaginal breech delivery
Although caesarean section is increasingly considered as the optimal mode of delivery for the breech presentation (Hannah et al 2000), women may still choose to have a vaginal breech birth or may present in advanced labour with an undiagnosed breech. Midwives must be fully conversant with the management and mechanisms of breech presentation and be able to orientate themselves to the position that the mother adopts in labour (RCM 2008).
There are six positions in breech presentation. The denominator is the sacrum, and its relationship to the maternal pelvis determines the position. The positions are the same as the vertex presentations, substituting the sacrum for the occiput (Fig. 64.6):
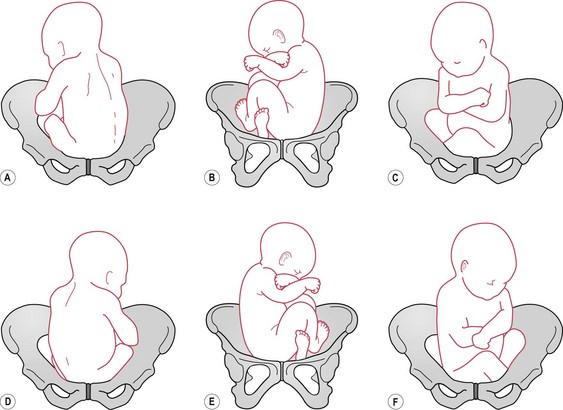
Figure 64.6 Breech positions. A. Left sacroanterior (LSA). B. Left sacrolateral (LSL). C. Left sacroposterior (LSP). D. Right sacroanterior (RSA). E. Right sacrolateral (RSL). F. Right sacroposterior (RSP).
The fetus may be positioned in a direct anterior or posterior position.
With the breech in either the left or right sacroanterior position and good contractions, there is descent. The mechanism of the right sacroanterior position is illustrated in Figure 64.7. The fetus engages with the bitrochanteric diameter (10 cm) in the right oblique diameter of the pelvic brim and descends into the pelvic cavity.
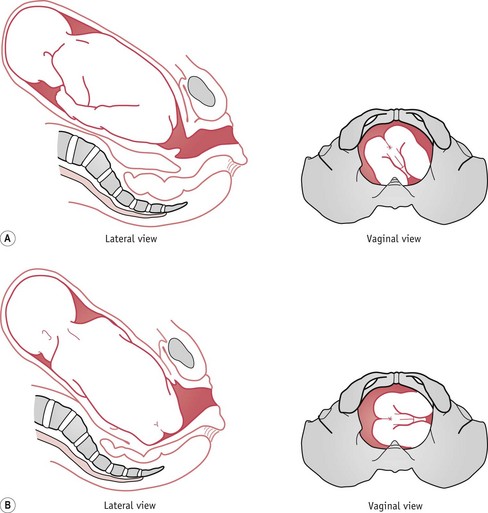
Figure 64.7 Right sacroanterior position. A. Onset of labour. B. Descent and internal rotation of the buttocks.
With further contractions, the anterior buttock meets the resistance of the pelvic floor and rotates forwards through one-eighth of a circle (45 degrees) and comes to lie behind the symphysis pubis. The bitrochanteric diameter now lies in the anteroposterior diameter of the outlet. Lateral flexion of the trunk allows the continued descent of the buttocks along the curve of the birth canal (Fig. 64.8). The anterior buttock normally passes under the symphysis pubis and ‘rumps’, followed by the posterior buttock, which sweeps over the perineum.
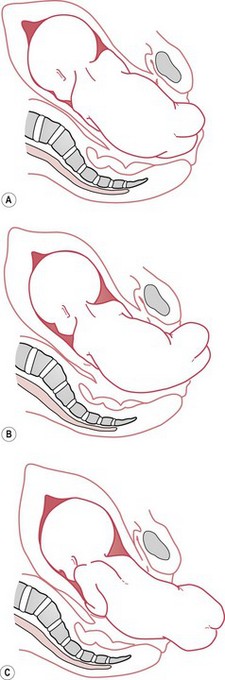
Figure 64.8 Birth of the buttocks. A. Breech crowning or ‘rumping’. B. Birth of posterior buttock. C. Birth of anterior buttock.
With the birth of the buttocks the shoulders descend into the pelvis with the bisacromial diameter (11 cm) in the right oblique diameter of the brim. Internal rotation of the shoulders through one-eighth of a circle brings the anterior shoulder behind the symphysis. The right (anterior) shoulder and arm escape under the symphysis and the left (posterior) shoulder and arm pass over the perineum (Fig. 64.9).
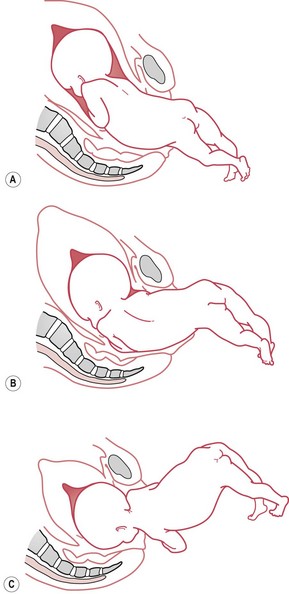
Figure 64.9 Birth of the shoulders. A. Feet born, shoulders engaging. B. Descent and internal rotation of shoulders. C. Posterior shoulder born; head has entered the pelvis.
The flexed head engages with the suboccipitobregmatic (9.5 cm) or suboccipitofrontal diameter (10 cm) lying in the right oblique or transverse diameter of the brim. Internal rotation of the head carries the occiput behind the symphysis. The face now lies in the hollow of the sacrum. External rotation of the buttocks and shoulders is produced by the internal rotation of the head. The back of the baby’s head and body now face in the same direction as the mother’s abdomen.
It is essential that the back of the fetus orientates in the same direction as the mother’s abdomen, and if it does not, it is gently assisted to do so. The chin, face, vertex and occiput are born over the perineum by a movement of flexion to complete the delivery (Fig. 64.10).
Management of breech labour
When a woman chooses to have a vaginal breech birth, the midwife needs to ensure that she does so from an informed position. A careful history should be taken to ensure that there are no medical or obstetric contraindications for vaginal breech birth and that both woman and baby are in good health.
If possible, a detailed ultrasound scan should be carried out to:
A thorough clinical assessment of pelvic capacity should be performed. Today, pelvimetry to measure maternal pelvic diameters for safe delivery is deemed unnecessary, with good progress in labour being indicative of adequate fetal–pelvic proportions (Kotaska et al 2009).
Even when labour is established, consideration should be given to performing an ECV in an attempt to alter the presentation of the fetus to cephalic. While it is preferable for a vaginal breech labour to be conducted in hospital and under the supervision of an experienced obstetrician or midwife, this may not always be possible; maternal choice, as well as unexpected and rapid delivery, sometimes prevents transfer to hospital. Supervisors of midwives also have a role in facilitating the woman’s admission to hospital and in supporting those midwives with the relevant skill to accompany her if requested to do so by the mother.
First stage of labour
This differs little from that of normal labour. If the breech is not engaged, as is probable in a flexed breech, there is a risk of early rupture of the membranes and prolapse of the umbilical cord. The midwife must be vigilant and immediately exclude the possibility of cord prolapse when the membranes rupture. Where the breech is engaged, the legs are probably extended and the risk of cord prolapse reduced.
The value of upright positions, ambulation and support in labour are equally pertinent to women labouring with a breech presentation. The midwife provides continued support and continuity, carefully monitoring the progress of labour and the condition of the woman and fetus. A close working relationship with the wider maternity care team is also essential, and while the experienced midwife may conduct the breech delivery, the support of a senior obstetrician should be readily available if necessary.
Because of the associated risk in breech presentation, continuous monitoring of the fetal heart should be offered and recommended in breech labour (NICE 2007, RCOG 2006b). Some women who pursue a vaginal birth may reject this evidence, and opt for intermittent monitoring. In such circumstances, observations on the maternal condition and progress in labour should be carried out in keeping with the recommended guidelines for intermittent monitoring (NICE 2007).
In most cases, the first stage of labour progresses normally. Augmentation may be required should uterine action be hypotonic. This must be done with extreme caution – in some units, breech presentation may be considered a contraindication for augmentation. There is no evidence that epidural anaesthesia is essential, and its use depends upon the wishes and needs of the woman.
Occasionally, the breech may begin to descend through the cervix before the cervical os is fully dilated and this gives the woman a desire to push. Although uncommon, the buttocks may then descend easily, but the larger head cannot pass through the incompletely dilated cervix and dangerous delay results. The use of epidural anaesthesia makes this less likely as the woman does not experience the premature urge to push; however, a large retrospective study on breech presentation found that epidurals were associated with a longer duration of labour, increased need for augmentation and a significantly higher caesarean section rate in the second stage (Chadha et al 1992).
Second stage of labour
When full dilatation of the cervical os has been confirmed, the mother may adopt a semi-recumbent, all-fours, upright or supported squatting position aiding expulsive efforts and the descent of the fetus.
Standing positions for the birth should be treated with caution because of an association with premature separation of the placenta. Midwives experienced in the management of breech birth advocate women adopting an all-fours or a forward-leaning ‘prayer position’ for the birth (Cronk 2005, Evans 2005).
Where an obstetrician is conducting the delivery, the woman is usually in the lithotomy position. The woman can mobilize prior to the onset of the second stage and lithotomy may be delayed until the breech is visible.
The midwife should ensure that appropriate and experienced help is at hand and that a paediatrician and senior obstetrician are present or readily available and that an anaesthetist can be quickly in attendance in case operative intervention suddenly becomes necessary.
If the fetal breech and body descend well, then it is likely that spontaneous breech delivery will occur with little assistance from the midwife or obstetrician. This is more common in multigravidae or when the fetus is small and preterm.
Assisted breech delivery
A medically managed vaginal breech birth employs techniques to assist the delivery with the woman predominantly in the lithotomy position. The bladder is emptied prior to delivery. When the posterior buttock distends the perineum, the perineum is infiltrated with local anaesthetic (unless an epidural anaesthetic or a pudendal block is employed) and an episiotomy is performed. The posterior buttock then emerges and the breech advances more quickly.
As the trunk descends, the back will rotate anteriorly, allowing the fetal shoulder to enter the maternal pelvis in the transverse or oblique diameter of the inlet. Traction on the fetus is not a part of British practice, as this can give rise to extension of the head and nuchal displacement of the arms. There should be no interference and, increasingly, obstetricians, like midwives, apply the rule of ‘hands off the breech’ and will try to avoid unnecessary manipulations.
Once the umbilicus is visible, previous practice dictated gently pulling down a loop of the umbilical cord to relieve any tension. This is no longer advocated. At this stage, compression of the cord is likely and time is an imperative.
From the complete delivery of the buttocks, some authorities advocate that the baby should be delivered within 15 minutes. Some believe that in vaginal breech birth, there may be benefits from rapid delivery of the baby to prevent progressive acidosis. This needs to be weighed against the potential trauma of a quick delivery. To date, there is insufficient evidence to evaluate the effects of expedited vaginal breech birth (Hofmeyr & Kulier 1996b).
If the fetal legs do not deliver spontaneously, inserting the index finger behind the thigh to flex the knee and abduct the leg may gently disengage them. However, if the practitioner is prepared to wait, they will usually deliver as the trunk descends.
With the next contraction, the shoulder blades appear; the arms, which are normally flexed across the chest, will usually slip out on their own and the shoulders are born in the anteroposterior diameter of the pelvic outlet. The head at this stage is entering the transverse or oblique diameter of the pelvic inlet. Some authorities advocate that from complete delivery of the baby’s body until full delivery of the head, no more than 5 minutes should elapse.
At this stage, a number of manoeuvres may be used to facilitate the delivery of the head. If all is proceeding well, spontaneous, but controlled, delivery may be used when the head is at the pelvic outlet. Midwives who assist women to give birth using a forward-leaning position, use the analogy of ‘getting the woman to move from a Christian prayer position to a Muslim prayer position’ as this aids release of the head, facilitating its delivery. It has been observed that when the fetus begins to draw up its knees, the fetal head also flexes. If the woman then moves forward as described above, her pelvis rotates over the fetal head, causing its spontaneous release (Evans & Cronk, personal communication, 2002).
Alternatively, the Mauriceau–Smellie–Veit or Burns–Marshall manoeuvre may be used.
Mauriceau–Smellie–Veit manoeuvre
is an effective method of delivering the fetal head, and the underlying principle is that of ‘flexion before traction’ (Fig. 64.11). It offers good control of the head and may also be used when there is delay in the descent of the head.
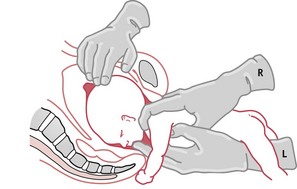
The manoeuvre involves a combination of jaw flexion and shoulder traction and can be used for any breech delivery, but is of particular value when the fetal head is extended and forceps may be difficult to apply.
The practitioner supports the baby with the legs straddling their left arm (Fig. 64.11); three fingers slide into the vagina, feeling for the baby’s cheekbones (malar bones). Originally, the middle finger was inserted into the baby’s mouth in order to maximize traction but this is not recommended as it can result in dislocation of the jaw (ALSO 2003). Instead, the ring and index fingers rest on the cheekbones while the middle finger applies pressure to the chin.
The index and ring fingers of the practitioner’s right hand are hooked over the baby’s shoulders, to apply traction, while the middle finger presses on the occiput to aid flexion. An assistant may apply suprapubic pressure if needed.
As gently as possible, the baby’s head is flexed and aided through the pelvic cavity to the outlet, after which the trunk is raised to bring the mouth into view. The air passages are then cleared and the birth of the head completed in the usual way.
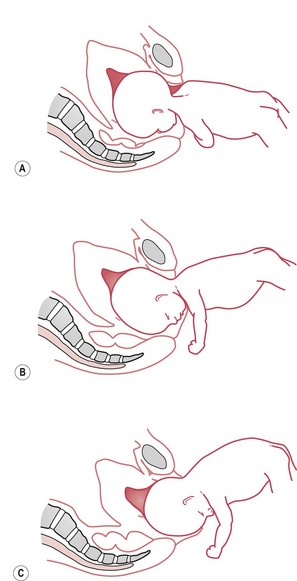
Burns–Marshall manoeuvre
is a medical procedure. Once the body is born, the baby is allowed to hang by his own weight for a few moments to facilitate descent and flexion of the head. When the nape of the neck and hairline come into view, the head is ready to be delivered (Fig. 64.12). Grasping the baby by the ankles and using slight traction, the practitioner directs the trunk upwards in a wide arc over the woman’s abdomen.
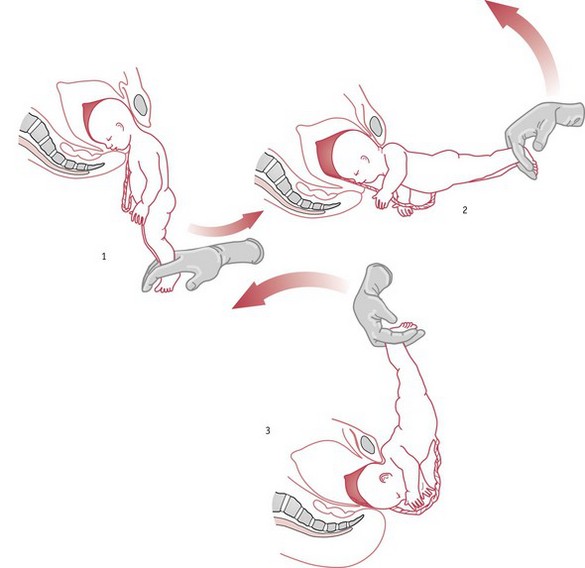
The perineum should then be depressed with the fingers to expose the mouth of the fetus and allow it to be cleared of any blood or mucus, enabling the baby to breathe freely.
The birth of the head then proceeds very slowly to avoid any sudden release of pressure that might give rise to an intracranial haemorrhage. To avoid this danger, Wrigley’s or Neville–Barnes forceps may be applied to the aftercoming head, which allows careful control of the speed with which the head is born.
Complications of vaginal breech delivery
Extended arms
If the baby’s arms are not flexed across the chest, they are likely to be stretched up alongside the head. It is not possible for head and arms to enter the pelvis together, so the arms must come first and then the head. This is best achieved by Lövset’s manoeuvre, shown in Figure 64.13. With the baby in a right sacrolateral position, the manoeuvre depends on the fact that the posterior shoulder is below the sacral promontory and anterior shoulder above the symphysis pubis.
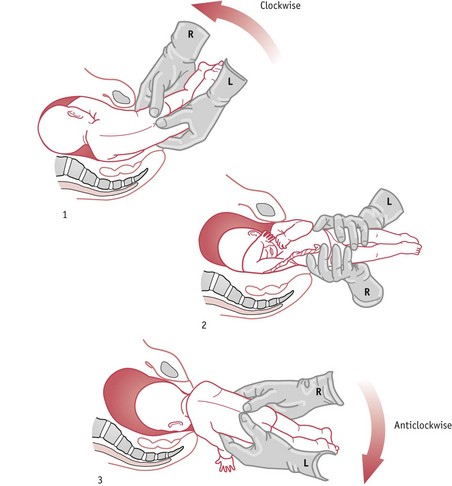
The practitioner grasps the baby’s thighs with thumbs over the sacrum, and, being careful to avoid pressure above the pelvic girdle, which could cause abdominal injury, pulls the baby gently downwards, at the same time turning him, back upwards, through a half circle (180 degrees). The former posterior shoulder now becomes anterior and is released under the symphysis pubis, while at the same time; the other shoulder is brought into the pelvic cavity. The baby is then turned back through a half circle in the opposite direction and the other arm is released in the same way.
This procedure does not require an anaesthetic, can be carried out by a midwife, and, correctly performed, is safe and successful, even in cases where the baby has one arm at the back of the neck (nuchal displacement).
Extended head
After the birth of the shoulders, the baby is allowed to hang from the vagina to facilitate descent and flexion of the head. If the neck and hairline are not visible within a few seconds, the most likely reason is extension of the head. The head may be delivered by the Mauriceau-Smellie–Veit manoeuvre, described above.
Entrapment of the fetal head
This is an extremely rare but dangerous situation in the term breech. It occurs when the breech is delivered and the cervix is not fully dilated and traps the fetal head. In this situation, the midwife must call for urgent medical assistance. The obstetrician will try to release the head from the cervix, but mortality and morbidity rates are high. Although more commonly used in shoulder dystocia, McRobert’s manoeuvre (see Ch. 66) has been used as a means to facilitate release of the fetal head (Shushan & Younis 1992).
It is possible, for a variety of reasons, for a midwife to be faced with an unexpected and emergency breech delivery. In community practice, the midwife should, with the mother’s consent, make every effort to transfer her into hospital. When labour is not advancing very quickly, this is usually possible.
If the labour is progressing rapidly, however, delivery may be imminent and the risks of transfer considerable. If the contractions are strong and effective, there is every chance that the breech will deliver easily, though the midwife should call for skilled help as unexpected complications may still occur. The midwife’s management of the breech birth is as described above.
Face presentation
Face presentation occurs when the head and neck are hyperextended but the limbs flexed, so that the fetus lies in the uterus in a curious S-shaped attitude with the occiput against its shoulder blades and the face directly over the internal os (Fig. 64.14). The presenting portion is between the orbital ridges and the chin, with the latter being the denominator (Chitra & Marino 2010). Face presentation is uncommon, and occurs in 1 of every 600–800 live births, averaging about 0.2% of live births.

Primary face presentation is present before the onset of labour and causative factors are similar to those leading to general malpresentation and those that prevent head flexion or favour extension (Chitra & Marino 2010), including:
Secondary face presentations develop in labour. Causes include:
The presenting diameters of the face presentation are to some degree favourable (i.e. 9.5 cm); however, the initial reason for the fetus adopting this position, the risk of the fetus being in a mentoposterior position, and the reduced ability of the facial bones to mould, carry additional risks to the fetus (see Table 64.3).
Table 64.3 Complications that may occur with a face presentation
| Complication | Reason |
|---|---|
| Cord prolapse | Ill-fitting presenting part and early rupture of the membranes. |
| Obstructed labour | The face does not mould and therefore cannot overcome minor degrees of cephalopelvic disproportion. A persistent posterior face presentation leads to obstructed labour. |
| Emergency operative delivery | As a result of obstructive labour or fetal distress. |
| Severe perineal trauma | Wider diameters: although the presenting diameter is the submentobregmatic at 9.5 cm, it is the submentovertical of 11.5 cm that distends the vagina and perineum. Risk of operative delivery. |
| Intracranial haemorrhage | Anoxia and abnormal moulding of the fetal skull. |
| Facial bruising and oedema | The inability of the face to mould and injury to the soft tissue. |
Identification in pregnancy
Face presentation is not easily diagnosed in pregnancy, but should be suspected if a deep groove is felt between the fetal head and back and when the cephalic prominence and the fetal back are palpated on the same side.
If heart sounds are heard through the anterior chest wall on the side where the limbs are palpated, these may seem unusually loud and clear when the position is mentoanterior (MA). In mentoposterior (MP) positions, the fetal heart sounds are more difficult to hear.
When face presentation is suspected, ultrasound should be used to confirm the clinical diagnosis.
During labour, the high presenting part may give rise to suspicion. The diagnosis can be made on vaginal examination, when gentle palpation will reveal the orbital ridges and the gums within the mouth. Occasionally, the fetus will further help the diagnosis by sucking the examining finger.
Once a face presentation is diagnosed, it is essential to determine the position of the chin, whether it is anterior or posterior. A posterior face presentation, unless it rotates to an anterior position, will lead to obstructed labour. When the midwife diagnoses a face presentation, a senior obstetrician should be informed as soon as possible. If the chin is lateral or posterior, the urgency of the situation must be stressed.
As labour progresses, it becomes increasingly difficult to distinguish facial landmarks on vaginal examination because the face becomes oedematous. Vaginal examinations must be carried out with great care to avoid trauma to the eyes.
Mechanisms
The lie is longitudinal, the presentation is the face, the denominator is the chin and the attitude is hyperextended. The engaging diameter is submentobregmatic (9.5 cm). There are six positions in which the face may present (Fig. 64.15).
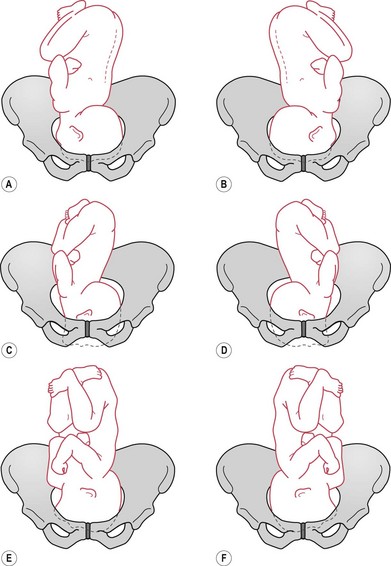
Figure 64.15 Face presentations. A. Right mentoposterior. B. Left mentoposterior. C. Right mentolateral. D. Left mentolateral. E. Right mentoanterior. F. Left mentoanterior.
Face presentation develops before the head is engaged in the pelvis. The mentum is anterior in 60–80% of cases; transverse in 10–12%; and posterior in 20–25%, with most rotating to the anterior (Chitra & Morino 2010).
In a mentoanterior position, the extended head enters the brim of the pelvis with the face presenting. The chin points to the iliopectineal eminence, and the sinciput to the opposite sacroiliac joint (Fig. 64.16).
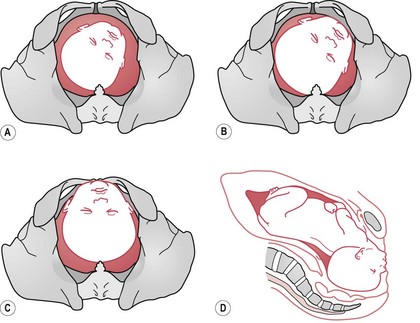
Figure 64.16 Mechanism of labour of anterior face presentation. A. LMA – onset of labour. B. Extension and descent. C. Vaginal view. D. Lateral view.
The submentobregmatic diameter (9.5 cm) engages and the face descends into the pelvis. The chin, being the lowest part, meets the resistance of the pelvic floor and rotates through one-eighth of a circle to escape under the pubic arch. The face appears at the vulval outlet (Fig. 64.17). Further uterine contractions drive the vertex and occiput over the perineum, and thus, by a movement of flexion, the head is born. Restitution and external rotation take place.
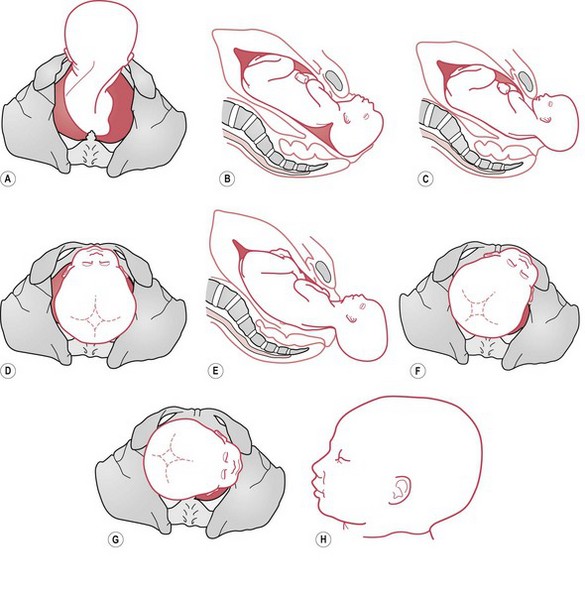
Figure 64.17 Mechanism of labour of anterior face presentation – birth of the face. A. Flexion. B. Flexion beginning. C. Flexion complete. D. Vaginal view. E. Lateral view. F. Restitution – MA to LMA. G. External rotation – LMA to LMT. H. Moulding.
A face presentation can only be born spontaneously if the chin is anterior. There is no mechanism by which the chin can be born when it lies at the back of the pelvis. The neck is too short to span the length of the sacrum and is already at the point of maximum extension, and obstructed labour occurs. Spontaneous rotation of the head from the mentolateral or mentoposterior to the mentoanterior position can, and occasionally does, take place, and spontaneous delivery may then occur. See Figure 64.18.
In a face presentation with the chin to the front, an adequate pelvis, a healthy fetus and good contractions, the labour will usually progress normally, with a vaginal delivery rate of 60–70%. However, in spite of this, in developed countries in the 21st century there is a lower threshold to move to caesarean section when face presentation is identified.
Management
In a mentoanterior position, labour often proceeds normally, though, as in any malpresentation, the membranes may rupture early, prolapse of the cord is possible, and labour is sometimes prolonged. In the second stage, normal delivery is anticipated, aided by an episiotomy, since, although the submentobregmatic diameter is only 9.5 cm, it is the submentovertical of 11.5 cm which distends the perineum at the time of delivery.
If there is delay in the second stage, the obstetrician will apply forceps. If normal delivery occurs, extension is maintained by applying pressure on the sinciput until the chin has escaped under the symphysis pubis; the head is then flexed to allow the vertex and occiput to sweep the perineum.
At birth, the baby is usually in good condition, although the eyelids and lips will be grossly oedematous and the face congested. The bruising and unsightly appearance can cause the mother considerable alarm and anxiety. The midwife should warn her what to expect and describe how the baby might look. The mother should be reassured that the bruising and oedema will subside within a few days and suckling, which at first may be difficult, is usually normal in 48 hours.
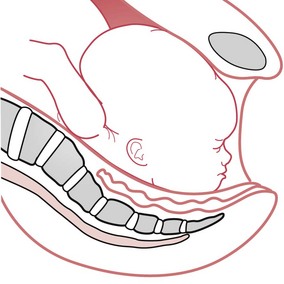
Brow presentation
Brow presentation (Fig. 64.19) is the least common presentation. The head is midway between flexion and extension, with the mentovertical diameter of 13.5 cm attempting unsuccessfully to enter the transverse diameter of the pelvic brim. A small head might enter a large pelvis only to be arrested in the cavity.
The incidence varies from 1 in 500 to 1 in 1400 deliveries. Brow presentation may be encountered early in labour but is usually a transitional state and converts to a vertex presentation after the fetal neck flexes. Occasionally, further extension may occur, resulting in a face presentation.
The causes are, with the exception of anencephaly, the same as in face presentation, and include (Chitra & Marino 2010):
These account for more than 60% of cases of persistent brow presentation.
Brow presentation, undiscovered and untreated, will lead to obstructed labour, uterine rupture, and raised perinatal and maternal morbidity and mortality.
Identification
On abdominal examination, the head is high and the presenting diameter unusually large. As with face presentation, a groove may be felt between the occiput and the back, and the cephalic prominence will be on the same side as the fetal back.
On vaginal examination, the presenting part may be too high to identify. If the brow is within reach, the orbital ridges may be felt on one side and the anterior fontanelle on the other. The diagnosis should be confirmed by ultrasound.
Management
In brow presentation, three outcomes are possible. The brow may:
The midwife must immediately call an obstetrician if a brow presentation is suspected or diagnosed in labour, and a woman at home should be alerted to the situation and its dangers and transferred into hospital.
As in all malpresentations, the membranes are likely to rupture early and there is a risk of cord prolapse; thus, a vaginal examination should be made as soon as the membranes rupture, to exclude this.
If a brow presentation is diagnosed early in labour, it may convert to a face presentation becoming fully extended or it may flex to a vertex presentation and deliver normally. If the brow presentation persists, however, and the fetus is a normal size, it will be impossible to deliver vaginally and a caesarean section will be performed.
Oblique and transverse lie leading to shoulder presentation
A shoulder presentation occurs as a result of a transverse or an oblique lie (Fig. 64.20). Shoulder presentation is not uncommon and is only problematic if the fetus is not cephalic by 36 weeks’ gestation. At term, an unstable or transverse lie presents a considerable risk to both mother and fetus, with cord prolapse being 20 times more common than with a flexed vertex presentation (Baxley 2001). If uncorrected, shoulder presentation will result in obstructed labour, and unless the lie is corrected, a caesarean section is the only mode of delivery.
Causes of an unstable lie and shoulder presentation are:
Identification
Abdominal examination and continuity are key to making the diagnosis of an oblique, transverse or unstable lie and therefore the presence of a shoulder presentation. The abnormal lie is easily diagnosed in pregnancy from the shape of the uterus, which appears too broad, with the fetal poles felt on either side of the abdomen, while the fundus is unusually low. Palpation will reveal the fetal head on one side and the breech on the other and no presenting part within the pelvis.
In an oblique lie, the fetal head, or breech, is found in one or other iliac fossa. If a non-longitudinal lie is found after the 36–37th week of pregnancy, an obstetrician must be informed. Ultrasound may be used to confirm the diagnosis, identify the presentation and detect the possible cause.
Management
As pregnancy advances, a non-longitudinal lie tends to revert to longitudinal and stabilize; however, if this does not occur, after 36 weeks’ gestation, the obstetrician will attempt to correct the lie by external version to a longitudinal lie and cephalic presentation. At term, labour may then be induced while the lie remains longitudinal and the presentation cephalic.
The likelihood of reversion to an oblique or transverse lie is high. The attendant risk is that the membranes may rupture and the cord or arm prolapse; or labour may commence before the lie is corrected. Often the woman is admitted to hospital for observation.
Ultrasound examination should exclude placenta praevia, and fetal or uterine abnormalities. A vaginal examination may be made to detect any pelvic abnormality such as a contracted pelvis. In labour, the lie is closely monitored and, if necessary, gentle lateral pressure may be applied to the uterus to help maintain a longitudinal lie.
Once labour is established and the fetal head enters the pelvis, the membranes can be ruptured. Labour should then progress normally. In cases where the woman has a poor obstetric history, or if complications occur in labour, there is likely to be early recourse to caesarean section as the safest mode of delivery.
If undetected or inadequately monitored, an unstable lie in labour is a serious obstetric emergency. With contractions, the fetal shoulder will be forced down into the pelvis, the membranes are likely to rupture, and the cord and/or the fetal arm may prolapse.
The midwife should recognize shoulder presentation during abdominal examination. Once placenta praevia has been excluded, vaginal examination can be carried out, and the fetal ribs or the hand may be felt. On detecting an unstable lie or shoulder presentation, the midwife must immediately inform an obstetrician, and if in the community, rapidly transfer the woman to hospital. Turning the woman onto all fours is of value in displacing the shoulder and reducing the mother’s urge to push. Where an arm or cord prolapses, this manoeuvre is essential (see Ch. 67). If the lie is uncorrected, caesarean section will be necessary and it may well be the safest mode of delivery even when the fetus has died.
Compound presentation
Compound presentation is a presentation in which a hand or foot lies alongside the head. Very rarely, both a hand and a foot come down. This tends to occur when the fetus is small and the pelvis large or when there is any condition preventing the descent of the head into the pelvis. Lower abdominal pain and a lack of fundal dominance is often noted. The pain experienced by the mother is best dealt with through effleurage, where the midwife applies light circular stroking movements to massage the mother’s lower abdomen. Compound presentation is only of significance in advanced labour when the membranes have ruptured. Usually, the presenting limb will recede as the presenting part descends. Labour usually ends in a normal or a low instrumental delivery, but where the compound presentation persists, there is an increased risk to the mother of vaginal and perineal trauma.
Conclusion
It is important that the midwife is knowledgeable about contemporary care and management of malpositions and malpresentations, and is able to impart this information to the woman in a realistic and accessible manner. Good preparation for labour and birth, and different strategies which might be required, should be discussed prior to labour if possible, and a plan agreed and documented, involving the whole maternity care team.
The midwife’s primary role is to monitor, support and enhance the experience of the pregnancy and birth, and where there are deviations from normal, make quick and appropriate referral. Midwives should be familiar with the mechanisms of malpositions and malpresentation and the manoeuvres which they may use in facilitating birth. It is important to inspire confidence in the mother, but midwives must also have confidence in themselves and in their ability to support the woman in her choice of birth and to manage this effectively when a malposition or malpresentation occurs.