Chapter 66 Shoulder dystocia
Introduction
Shoulder dystocia is an obstetric emergency with a potentially catastrophic outcome. It refers to deliveries where manoeuvres other than gentle downward traction are needed to complete the delivery of the anterior shoulder (Resnik 1980).
Mechanism
In a normal labour the shoulders enter the pelvic brim in the oblique or transverse diameter. (For a complete description of the normal mechanism of labour, see Ch. 37.) In shoulder dystocia there is an arrest of the normal mechanism of labour as the shoulders attempt to enter the pelvis in the anteroposterior diameter of the pelvic brim. The diameter of the fetal shoulders or bisacromial diameter is 12.4 cm and should fit comfortably through the widest diameter of the pelvic brim. Shoulders are sufficiently flexible to allow those of even a large baby to negotiate the pelvis.
There is no current agreement on a definition for shoulder dystocia. Smeltzer (1986) suggests that shoulder dystocia is a failure of the shoulders to spontaneously traverse the pelvis after the fetal head has been delivered.
Some or all of the following will alert midwives to suspect that shoulder dystocia has occurred:
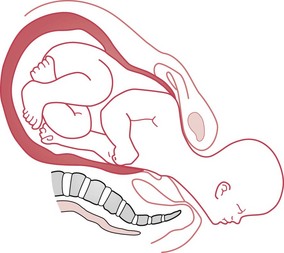
The turtle sign is caused by reverse traction from the shoulders. The anterior shoulder is wedged onto the symphysis pubis and the posterior shoulder may still be above the pelvic brim (Fig. 66.1). Pulling to deliver the anterior shoulder is likely to impede delivery by wedging the infant’s anterior shoulder more firmly onto the symphysis pubis and can cause damage to the brachial plexus (see Fig. 66.10).
The midwife must recognize shoulder dystocia and summon help immediately from midwifery, obstetric, paediatric and anaesthetist colleagues, as the outcome for both mother and infant is potentially very serious.
The midwife’s anxiety is likely to be communicated to the mother even if little is said. The midwife should remain calm and in control of the situation, and maintain communication with the mother and her partner.
Incidence and risk
The incidence of shoulder dystocia is around 0.6% at term, but the risk increases to 1.3% by 42 weeks’ gestation (Johnstone & Meyerscough 1998, RCOG 2005). However, a lack of agreement over the definition affects the number of cases reported (Johnstone & Myerscough 1998).
The risk of shoulder dystocia rises with increasing birthweight and length of gestation, birth order and maternal age (Acker et al 1986, Gross et al 1987, Johnstone & Myerscough 1998). Johnstone & Myerscough (1998) point out that half of all babies with shoulder dystocia weigh less than 4 kg and are not considered to be large, and only 4% of large babies suffer shoulder dystocia.
Mortimore & McNabb (1998) suggested that some practitioners may use the term shoulder dystocia to describe any general difficulty with the delivery of the shoulders. If RCOG (2005) diagnostic criteria for shoulder dystocia cannot be fulfilled, then ‘difficulty with delivery of the shoulders’ should be recorded to avoid overdiagnosis (Mahran et al 2008).
Identification of risk factors
Ideally, all potential cases of shoulder dystocia would be identified antenatally; the associated maternal and neonatal morbidity and mortality could then be prevented. The sensitivity of single predictive risk factors is poor. At present, midwives and obstetricians can do no more than anticipate the problem by identifying those factors which give a strong index of suspicion.
Maternal obesity is a frequently occurring factor associated with shoulder dystocia (maternal BMI >30 at booking, or weight at delivery >90 kg) (RCOG 2005). The greater the maternal weight, the higher the risk (Athukorala et al 2007).
Maternal diabetes and gestational diabetes are associated with asymmetrical fetal growth. The body and particularly the shoulders are larger than in babies of mothers who are not diabetic (Acker et al 1985).
Spellacy et al (1985) studied the data from 33,545 deliveries and concluded that women with either insulin-dependent or gestational diabetes are more likely to deliver a macrosomic infant and are therefore at a higher risk of a delivery complicated by shoulder dystocia.
Fetal macrosomia is the strongest independent risk factor for shoulder dystocia (Athukorala et al 2007). Infants of non-diabetic mothers who have birthweights of 4000–4449 g have a 10% risk of shoulder dystocia, while infants of the same weight born to diabetic mothers have a 31% risk of developing shoulder dystocia, because of their asymmetrical growth (Acker et al 1985, Spellacy et al 1985).
A previous delivery complicated by shoulder dystocia is a predictive risk factor, with a recurrence rate of around 10% for subsequent deliveries (Olugbile & Mascarenhas 2000, Smith et al 1994).
Use of ultrasound to predict the macrosomic fetus
Ultrasonic estimation of fetal weight is widely used, as it is objective and can be reproduced (Combs et al 1993). However, Chauhan et al (1992) suggest that ultrasonic diagnosis of the large infant is generally no more accurate than clinical estimation and that if a woman has had a baby before, her own estimate is likely to be as good as an ultrasound measurement. Elective induction for infants diagnosed as macrosomic on ultrasound scan increases the risk of caesarean section and does not prevent shoulder dystocia (Hall 1996, RCOG 2005).
In spite of the inadequacy of ultrasound estimation of fetal weight, it is currently used along with clinical judgement to assess the safest method of delivery, especially for the postmature, large for gestational age or suspected macrosomic fetus.
Prediction of impending shoulder dystocia
Most labours preceding shoulder dystocia are normal (McFarland et al 1995). In some cases the first hint of trouble the midwife may experience during a delivery is the slow extension of the baby’s head and then the chin remaining tight against the mother’s perineum (Coates 1995). In spite of current technology, shoulder dystocia usually occurs unexpectedly (RCOG 2005).
Unfortunately, the absence of risk factors cannot be relied upon to exclude the possibility of shoulder dystocia. It is therefore important that the midwife has a sound knowledge of the interaction between the physiology and mechanism of labour and the manoeuvres that may be used to complete the delivery in the shortest time possible. This is to ensure the best outcome for the mother and her infant. All members of the labour ward team should be familiar with the agreed protocol, and ‘drills’ should be practised on a regular basis by all grades of staff (Draycott et al 2008, MCHRC 1998).
Manoeuvres for management of shoulder dystocia
The following descriptions of manoeuvres are arranged from the simple, requiring only movement of the mother, to the complex, where direct manipulation of the baby is required. These manoeuvres cannot really be learned or fully understood by reading alone and it is suggested that the reader works through the manoeuvres using a doll and pelvis or phantom.
McRoberts’ manoeuvre
This is the first choice of manoeuvre in most circumstances as it has been proven to be safe and effective. The manoeuvre (Fig. 66.2) requires the mother to lie flat on her back (or with a slight lateral tilt to prevent supine hypotension), then she is assisted into an exaggerated knee–chest position (Gonik et al 1983).

Once the mother has adopted this position, the midwife should be able to proceed with a normal delivery of the shoulders. Smeltzer (1986) suggests that this manoeuvre:
This was supported by later radiological studies (Gherman et al 2000).
Maternal and fetal models were used by Gonik et al (1989) to assess the forces used to extract the fetal shoulders. The McRoberts’ manoeuvre was compared with the lithotomy position and consistently required less force to remove the shoulders.
RCOG (2005) advocates the use of the McRoberts’ manoeuvre as a first step if shoulder dystocia is diagnosed, and, if the manoeuvre is unsuccessful at the first attempt, to try it a second time before attempting other manoeuvres.
All-fours position
When there is a minor degree of shoulder dystocia, movement of the mother can dislodge the obstruction so the shoulders can negotiate the pelvis normally; assisting the mother into an all-fours position can work in this way. The all-fours position (Fig. 66.5) also can be used to optimize the space in the sacral curve for the midwife to undertake the direct or rotational manoeuvres as described below. Generally, this position, which acts as an ‘upside-down McRoberts’ position’ carries the same positive effects as above, and will allow the posterior shoulder to deliver first (Macdonald & Day-Stirk 1995).

If a mother is already on all fours and shoulder dystocia is encountered, then the midwife should assist her to move into the McRoberts’ position. If this is not possible, then direct manoeuvres can be undertaken whilst the all-fours position is maintained.
The all-fours position can only be used if the woman is willing and able to manoeuvre onto her knees, and is not suitable for women who have a dense epidural block. Whilst the woman is in the all-fours position it is difficult to maintain eye contact and the midwife must ensure that good clear verbal contact is maintained. It is a useful position for a larger or overweight woman, who may find it difficult to adopt the McRoberts’ position.
Reflective activity 66.1
Using role play, with one of you ‘playing’ the woman and one the midwife, work with a colleague and try:
Practise the instructions that you might have to give to a mother moving from one position to another. Consider how easy/difficult it was getting into these different positions, and how you could prepare women antenatally for such an emergency.
Suprapubic pressure
The application of suprapubic pressure is intended to adduct and then displace the anterior shoulder away from the symphysis pubis and so allow it to enter the pelvis in an oblique diameter (Fig. 66.6). Pressure is applied by either the midwife or assistant, using the flat of the hand against the baby’s back in the direction that the baby is facing.
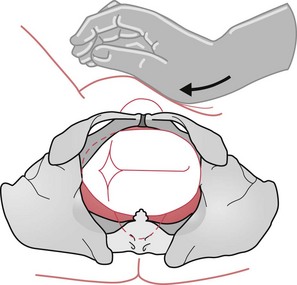
Figure 66.6 Diagram to illustrate the use and direction of suprapubic pressure when the back is on the woman’s left.
Suprapubic pressure can be used on its own or with other non-invasive manoeuvres, such as the McRoberts’ or all-fours manoeuvre. It may also be used with the Rubin manoeuvre or the Woods’ manoeuvre (see below).
Non-invasive procedures have been shown to be effective in up to 69/76 (91%) of cases of shoulder dystocia (Luria et al 1994). However, if the non-invasive manoeuvres described have been unsuccessful, then direct rotational manoeuvres are required. It is at this stage that extra analgesia or anaesthesia may be required. Meanwhile, the midwife should not delay attempting to complete the delivery.
Episiotomy
Shoulder dystocia is a bony dystocia and as such is not greatly affected by soft tissue. An episiotomy may prevent injury to the mother’s pelvic floor and perineum during any direct manipulation of the fetus and/or accommodate the midwife’s or obstetrician’s hand whilst undertaking direct rotational manoeuvres.
Woods’ manoeuvre and Rubin manoeuvre
Woods’ manoeuvre
To undertake the Woods’ or the Rubin manoeuvre, the midwife should assist the woman into the lithotomy position with her buttocks well over the edge of the bed so that there is no restriction to the sacrum or coccyx during the manoeuvre. If this is not possible, in a home confinement for instance, then the McRoberts’ or all-fours position should be used. These are practical positions for undertaking further manoeuvres and remove restrictions to the sacrum and coccyx that are present when the mother is in the dorsal or semi-recumbent position.
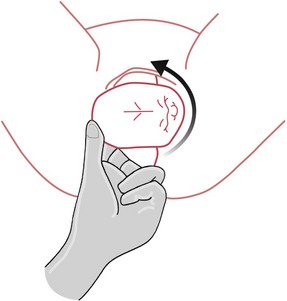
The method Woods (1943) used to relieve shoulder dystocia involves applying one hand to the mother’s abdomen, putting firm but gentle pressure onto the fetal buttocks, and inserting as much of the hand as is necessary into the vagina to locate the anterior surface of the posterior shoulder (clavicle). The shoulder is then rotated through 180 degrees in the direction of the fetal back (Fig. 66.5), which actually causes an abduction (see website) of the fetal shoulders.
This rotation may dislodge the anterior shoulder and enable the posterior shoulder to enter the pelvic brim. The posterior shoulder becomes the anterior following the rotation, and may be delivered by normal downward traction and the delivery completed.
Rubin manoeuvre
Rubin (1964) emphasized the importance of having both of the infant’s shoulders adducted, and presented measurements to demonstrate that in this position the circumference of the baby’s body is less than if the shoulders were abducted. To achieve the Rubin manoeuvre, a hand must be inserted into the vagina as far as is necessary to locate a shoulder. Then, working from behind the fetus, the shoulders are pushed into the oblique diameter (see website). Once the shoulders are in the oblique diameter and free of the symphysis pubis, then delivery can be completed (Fig. 66.7).
O’Leary (2009) suggests that both the Woods’ and Rubin manoeuvres may be more successful if they are used in conjunction with gentle but firm suprapubic pressure in the direction that facilitates the vaginal rotation (see Fig. 66.6).
Delivery of the posterior arm
The technique is to insert a hand into the vagina along the curve of the sacrum and locate the posterior arm or hand. The fetal arm should then be swept over the chest and delivered (Fig. 66.8).
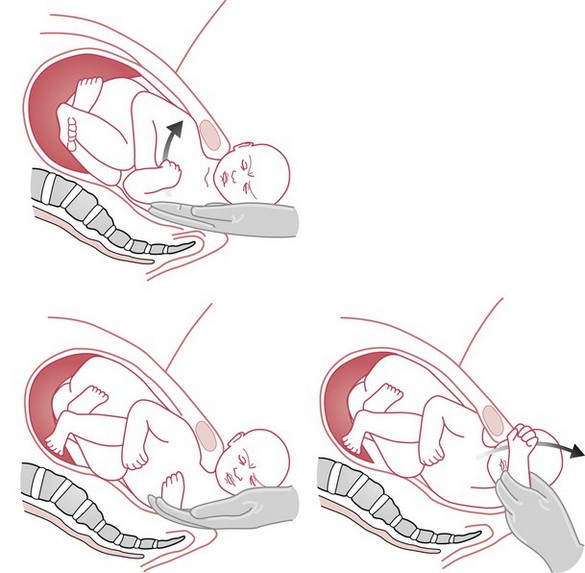
If this manoeuvre fails once the posterior arm has been delivered, the fetus may be rotated using either the Woods’ or Rubin manoeuvre so that the shoulder and arm that have been delivered are rotated to the anterior position, thus unlocking the obstruction (this is similar to the Burns–Marshall manoeuvre as described in Chapter 64).
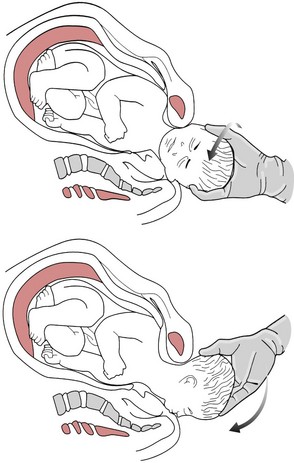
Zavanelli manoeuvre
The Zavanelli manoeuvre is a revolutionary concept (Sandberg 1985). Unlike the other manoeuvres described, it reverses the whole mechanism of delivery. Cephalic replacement is followed by a caesarean section. Whilst it is unlikely that a midwife would ever need to undertake this manoeuvre, it may be a last resort if practising in a remote area away from immediate obstetric support.
To carry out the manoeuvre, the fetal head is returned to the pre-restitution position of either direct occipitoanterior or direct occipitoposterior. The head is then manually flexed and returned to the vagina (Sandberg 1985) (Fig. 66.9). Delivery is then completed by caesarean section.
The role of the midwife in such circumstances would normally be to support the mother, monitor and record the condition of both the mother and the fetus, and ensure that all the personnel necessary are called to deal with this obstetric emergency.
Sandberg (1985:482) suggests that the Zavanelli manoeuvre ‘must occupy the bottom priority until its virtue and applicability … can be confirmed’. The Zavanelli manoeuvre must remain the last resort; however, it has proved to be a life-saving procedure. Midwives should understand the mechanisms of the Zavanelli manoeuvre and hope that they will never need to use it.
Reflective activity 66.2
When you believe that you are familiar with the manoeuvres, use a doll and pelvis to reinforce your knowledge of the pelvic angles achieved with each manoeuvre. Try to undertake the direct manoeuvres with the pelvis in the correct position for an all-fours delivery. Ask a colleague to hold the pelvis in the correct position for you whilst you try to undertake the manoeuvres and note the different degrees of force which may be used.
Use the mnemonics in Boxes 66.3 and 66.4 if you find that they help you, or make up your own mnemonic to memorize the sequences of the manoeuvres.
Other procedures
Symphysiotomy
Surgical separation of the symphysis pubis to enlarge the pelvis for delivery has been proven clinically useful for cephalopelvic disproportion but is associated with high maternal morbidity. Although symphysiotomy has been used for the relief of shoulder dystocia, the few cases reported reveal high maternal morbidity (Broekman et al 1994).
Cleidotomy
A clavicle can fracture spontaneously during a normal delivery of a normal-weight infant or a delivery complicated by shoulder dystocia. Deliberate fracture of the clavicle is a difficult procedure, especially in a large, mature fetus. O’Leary (1992:78) points out that although clavicular fracture is often mentioned, ‘its use has never been substantiated’ to resolve shoulder dystocia.
Fundal pressure
Fundal pressure together with traction provides the worst outcome for brachial plexus injury (Gross et al 1987). Fundal pressure will further impact the shoulder or shoulders and impede progress, can damage the brachial plexus and has also been associated with uterine rupture and maternal death (O’Leary 2009). Fundal pressure has also been implicated in uterine rupture, and thus maternal morbidity and mortality. It is therefore a practice which should not be used (RCOG 2005).
Maternal outcome
Shoulder dystocia is associated with a higher risk of physical and psychological morbidity and mortality for mother and baby:
Uterine rupture
Maternal deaths associated with shoulder dystocia have been caused by the use of fundal pressure resulting in uterine rupture and from haemorrhage during delivery or immediately postpartum (RCOG 2005).
Postpartum haemorrhage and/or shock
Benedetti & Gabbe (1978) described maternal morbidity from shoulder dystocia as considerable: in their study, 68% of cases had an estimated blood loss of more than 1000 mL. Others have recorded extensive vaginal, cervical and perineal lacerations, uterine rupture and vaginal haematoma as sequelae to shoulder dystocia (Gross et al 1987).
It is wise to anticipate postpartum haemorrhage if shoulder dystocia is encountered.
Soft tissue damage – cervix and vagina
Soft tissue damage may include vulval haematoma and minor and major lacerations. As these may cause a significant degree of blood loss, the midwife should examine the cervix, vagina and labia very carefully following delivery to diagnose any lacerations and take appropriate action (see Ch. 40).
Infection
Increased vaginal examinations, and manoeuvres are likely to increase the risk of infection for the woman. This may be exacerbated by soft tissue damage and blood loss.
The loss of the perfect birth and the perfect baby
Women will have had plans and expectations for the birth of the baby. It may be difficult for the woman to come to terms with the reality of a shoulder dystocia birth and its sequelae. As with any traumatic experience, the mother and her partner may wish to discuss the events surrounding the delivery. This is discussed further in Chapter 70.
Birth Injury and fetal outcomes
The most obvious and immediate consequence for the infant whose birth has been complicated by shoulder dystocia is asphyxia (MCHRC 1998, RCOG 2005).
Airway protective reflexes are reduced by asphyxia. Midwives should therefore prepare for the reception of an asphyxiated baby, and must call for a paediatrician to attend the delivery (Box 66.1). (Resuscitation of the newborn is described in Chapter 45.)
Careful examination of the newborn is always important but is imperative following a traumatic delivery (see also Ch. 41). The most commonly reported injuries following deliveries complicated by shoulder dystocia involve the brachial plexus.
Brachial plexus injury
The prevalence of congenital brachial palsy (CBP) is 1 : 2300 of all live births; 64% of CBP is associated with shoulder dystocia, compared with the normal population risk of 0.2–1% (RCPCH 2000). Whilst many brachial plexus injuries are associated with shoulder dystocia, high birthweight and assisted delivery, around 7.5% of cases have no associated risks reported (RCPCH 2000). There is no reliable method of predicting risk of either shoulder dystocia or brachial plexus injuries.
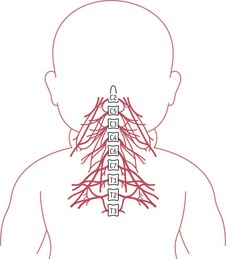
Erb’s palsy is the most commonly reported brachial plexus injury following shoulder dystocia. This is the result of damage to the nerve roots C5–6 (Fig. 66.10). The arm on the affected side lies in the classical ‘waiter’s tip’ position (Fig. 66.11).

Following delivery, if the baby has a flaccid arm or an unequal Moro reflex (see Ch. 41), then the midwife must suspect a brachial plexus injury and inform a senior paediatrician. Serious conditions are associated with congenital brachial plexus injury, such as cervical cord injury and cerebral injury, and these will require urgent treatment.
There are four degrees of injury to the brachial plexus:
Diagnosis may be complex as there may be a combination of injuries.
Treatment for congenital brachial plexus injury
The baby will be referred to a physiotherapist and the parents will be taught how to maintain the affected arm in a natural position until any bruising or swelling resolves. The physiotherapist will then teach the parents a series of exercises for the affected arm.
Physiotherapy is used to maximize the use of the arm to prevent muscle contracture. Motion exercises develop strength and flexibility, and tactile stimulation is used to improve sensory awareness. It is important to keep the joints supple for the best outcome. However, these exercises are time consuming, and parents will require support and encouragement, in addition to as much information as is available concerning their baby’s condition. Parents should be referred to support groups (see website for contact addresses).
Most congenital brachial plexus injuries resolve within 6–12 months; those that have not resolved may need surgery to improve function.
Bony injury
Shoulder dystocia and high birthweight are considered risk factors for clavicular fractures. Clavicular fractures can also be unpredictable and unavoidable, and may occur in 2–4% of normal births (Roberts et al 1995). The baby may be in considerable pain and on examination an irregularity may be felt over the site of the fracture. However, if the fracture is not displaced, an irregularity may only be felt over the site of the fracture several days after birth as a callus forms as part of the healing process. The callus will resolve within a couple of months. If a midwife suspects that a clavicle has been fractured, a paediatrician must examine the baby. The paediatrician may order X-rays to confirm the diagnosis and to rule out other bony injury. An analgesic, such as paracetamol in a paediataric dosage, may be prescribed if the baby appears to be suffering any discomfort.
The humerus may have also been damaged following shoulder dystocia, especially if the posterior arm has to be delivered to release the impaction. Both arms should be examined carefully after delivery, and in the first weeks following delivery, to exclude bony injury and monitor CBP.
Careful examination of the newborn must be undertaken following any delivery, and special attention taken following a traumatic delivery, to exclude any injury not immediately apparent (see Box 66.2).
Notes and record-keeping
There are many events in midwifery that happen with alarming rapidity (NMC 2007) and as such are difficult to record contemporaneously. Accurate records are vital for all deliveries and especially following any emergency situation. The midwife must take care to record all events in chronological order. The important or main events in a case of shoulder dystocia are:
Education, training and development
Regular scenario training or ‘drills’ and thorough knowledge of local procedure for shoulder dystocia are recommended (Draycott et al 2008, MCHRC 1998). Most maternity units have instituted such educational and development strategies and have demonstrated improved staff performance and outcome.
The Advanced Life Support in Obstetrics (ALSO) training has been a useful means of gathering multidisciplinary groups together to practise emergency skills in a safe environment, and for the emergency of shoulder dystocia (Sokol et al 2003) has promoted the HELPERR mnemonic (see Box 66.3). Other mnemonics are in use (see Box 66.4).
If a mnemonic is in use, it should be underpinned by a clear evidence-based rationale and should be clearly understood by the whole team.
The nature of shoulder dystocia as a comparatively rare but serious emergency means that some practitioners may never have the experience of dealing with it, or may never observe a case before they have to deal with it as lead practitioner. It is therefore vital that following an incident of shoulder dystocia (and any other emergency) there is a forum to discuss the individual case and its management in a systematic and critically reflective way. This will highlight elements of good practice and communication, and identify areas that require additional attention. This forum should be multidisciplinary, and should at its heart have a non-blame and development principle (DH 2000).
Reflective activity 66.3
Review your local protocols and clinical guidelines. Are these up-to-date and evidence based? Is there a regular shoulder dystocia drill carried out locally? You may wish to work with colleagues to plan a regular drill as recommended by CESDI (MCHRC 1998) and the RCOG (2005) involving a range of colleagues, to practise the manoeuvres and management. Ensure that there is an opportunity to reflect together after the sessions.
Conclusion
Shoulder dystocia is a rare but serious complication of labour. Midwives should commit to memory a series of manoeuvres that have been proven to be effective and be aware of those manoeuvres that are ineffective or dangerous. Current knowledge of labour ward protocol or procedure is necessary for all members of the labour ward staff. All members of staff who may be involved in such an emergency should take part in practice ‘drills’ on the labour ward (MCHRC 1998, RCOG 2005, RCM 2000).
Permanent damage is rare. Babies who do suffer brachial plexus injury should be swiftly referred to a specialist centre, and parents provided with appropriate support and information to help them care for their child. The psychological impact of such a traumatic birth should be considered by the care team, and opportunities provided for debriefing and for further counselling, should this be necessary.