CHAPTER 9 The knee
Biomechanics of the extensor mechanism
The patella is the largest sesamoid bone in the body. It is attached above to the quadriceps tendon, below to the patellar tendon, and medially and laterally to the patellar retinacula. The breadth of the pelvis and close proximity of the knee creates a valgus angulation to the femur. Coupled with this, the direction of pull of the quadriceps is along the shaft of the femur and that of the patellar tendon is almost vertical (Fig. 9.1). The difference between the two lines of pull is known as the Q angle and is an important determinant of knee health. Normal values for the Q angle are in the region of 15–20°, and knees with an angle greater or less than this can be considered malaligned.

Definition
The Q angle is the difference between the direction of pull of the quadriceps along the shaft of the femur, and the direction of pull of the patellar tendon, which is almost vertical.
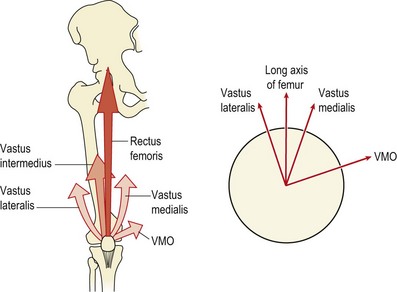
As the knee flexes and extends, the patella should travel in line with the long axis of the femur. However, the horizontal force vector created as a result of the Q angle tends to pull the patella laterally, a movement which is resisted by the horizontal pull of the lower fibres of vastus medialis. This coupled pull causes the patella to follow a curved path as the knee moves from extension to flexion.
The lower fibres of the vastus medialis can be considered as a functionally separate muscle, the vastus medialis oblique (VMO) (Speakman and Weisberg, 1977). The quadriceps as a whole have been shown to undergo reflex inhibition as the knee swells (de Andrade, Grant and Dixon, 1965; Stokes and Young, 1984). However, the VMO can be inhibited by as little as 10 ml effusion while the vastus lateralis and rectus femoris require as much as 60 ml (Arno, 1990). Minimal effusion occurs frequently with minor trauma and may go unnoticed by the athlete. However, this will be enough to weaken the VMO and alter the biomechanics of the patella.
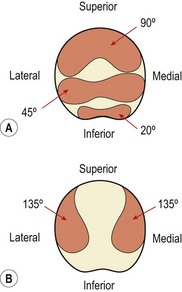
Patellar contact area
In full extension the patella does not contact the femur, but lies in a lateral position. As flexion progresses, the patella should move medially. If it moves laterally it will butt against the prominent lateral femoral condyle and the lateral edge of the patellar groove of the femur. As flexion progresses, different areas of the patella’s undersurface are compressed onto the femur. At 20° flexion the inferior pole of the patella is compressed, and by 45° the middle section is affected. At 90° flexion, compression has moved to the superior aspect of the knee. In a full squatting position, with the knee reaching 135° flexion, only the medial and lateral areas of the patella are compressed (Fig. 9.2). Compression tests of the patella to examine its posterior surface must therefore be performed with the knee flexed to different angles.
Patellofemoral loads may be as high as three or four times body weight as the knee flexes in walking, and nine times body weight when descending stairs (Cox, 1990). While the posterior surface of the patella is compressed, the anterior aspect receives a tensile force when seen in the sagittal plane (Fig. 9.3B). The effect of the Q angle is to create both horizontal and vertical force vectors which tend to compress the lateral aspect of the patella but submit the medial aspect to tensile stress (Fig. 9.3A). Clearly, alterations in Q angle will change the pattern of stress experienced by the patellar cartilage.
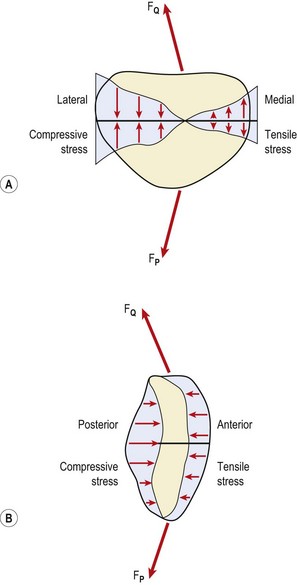
Figure 9.3 Patellar stress. (A) The Q angle causes the lateral edge of the patellar cartilage to be compressed, while the medial aspect is subjected to tensile stress. (B) The posterior surface of the patella is compressed. FQ, quadriceps pull; FP, patellar tendon.
From Cox (1990), with permission.
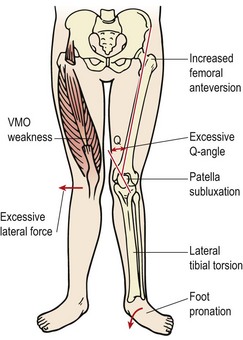
Knee angles in the stance phase of walking or running will be altered by foot and hip mechanics through the closed kinetic chain. Excessive foot pronation and hip internal rotation and adduction (causing a ‘knock-knee’ posture) have been linked to patellofemoral pain syndrome (PFPS—see below).
Patellofemoral pain syndrome
Pathology
Pain to the undersurface of the patella is variously called anterior knee pain, chondromalacia patellae, patella malalignment syndrome and patellofemoral pain syndrome (PFPS). The last term is used in this text. It is a condition affecting the posterior surface of the patella, and is sometimes attributed to cartilage damage and, on occasion, incorrectly seen as a direct precursor to osteoarthritis. Since hyaline cartilage is aneural, changes in the patellar cartilage surface itself would not result in PFPS. Furthermore, at arthroscopy cartilage changes are often seen in patients who have no PFPS. If cartilage degeneration does occur with this condition, it is to the ground substance and collagen at deep levels on the lateral edge of the patella. This results in a blistering of the cartilage as it separates from the underlying bone, but the cartilage surface itself is still smooth (Gruber, 1979). In osteoarthritis (OA) the initial changes occur to the cartilage surface of the odd facet (medial) and are followed by fibrillation.
The retinacula supporting the patella may be a major source of pain (Fulkerson, 1982), or the subchondral bone of the odd facet (Hertling and Kessler, 1990). As we have seen, the odd facet is only occasionally compressed in a full squatting position, and so its subchondral bone is less dense and weaker. Lateral movement of the loaded patella could pull the odd facet into rapid contact with the patellar surface of the femur, causing pain. Sources of pain are summarized in Table 9.1.
Table 9.1 Source of pain in PFPS
PFPS has a multifactorial etiology. Associated factors may be categorized as local and remote (Crossley et al., 2007). Local factors are those directly associated with the patella structure; remote factors have an effect on the patella through other structures. Table 9.2 shows some of the most common factors associated with PFPS.
Table 9.2 Factors associated with patella femoral pain syndrome (PFPS)
| Factor | Clinical sign |
|---|---|
| Remote | |
| Internal rotation of femur | Squinting patella due to femoral internal rotation |
| Knee valgus increased | Knock knee position, more noticeable during squatting. Often associated with poor gluteus medius tone |
| Tibial rotation | Often associated with foot biomechanics |
| Foot (subtalar) pronation | Drop foot or high arch position linked to tibial rotation |
| Muscle flexibility | Hamstrings, rectus femoris, ITB/TFL, gastrocnemius |
| Local | |
| Patella position | Patellar resting position and passive motion |
| Soft tissue characteristics | Compliance of medial and laterally placed tissues |
| Muscular control of quadriceps | Muscle wasting/weakness. Timing of VMO contraction. Tracking of patella |
ITB/TFL—iliotibial band/tensor fascia lata; VMO—vastus medialis obliqus.
From Crossley et al. (2007).
Muscular factors
Flexibility and strength of the knee tissues and muscles will often reveal asymmetry. The relationship between the hamstrings and quadriceps (HQ ratio) is particularly important and may require isokinetic assessment of peak torque values. Isokinetic testing also demonstrates characteristic changes in the PFPS patient (Fig. 9.4). Eccentric torque production during knee extension is often poor (Bennett and Stauber, 1986) and the torque curve may be irregular (Hoke, Howell and Stack, 1983). Both changes have been suggested to represent a deficiency in motor control, which would explain the often rapid response to quadriceps training that is achieved in these patients. One possibility is that malalignment and patellofemoral (PF) pressure alterations may result partly from subtle shifts in the timing or amount of VMO activity, in particular parts of the movement range (Reid, 1992). The aim of rehabilitation is therefore more a case of motor skill acquisition than pure strength training.
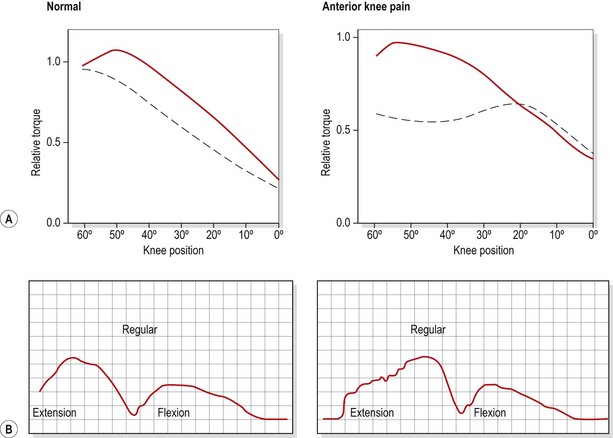
Figure 9.4 Characteristic changes in isokinetic evaluation with anterior knee pain. (A) Relative torque. (B) Shape of torque curve.
Keypoint
In PFPS patella dysfunction may result from a shift in the timing of VMO (vastus medialis obliquus) activity during movement. Retraining depends on re-educating the motor skill involved in knee movement rather than pure strength.
Weakness or malfunction in the VMO will allow the patella to drift laterally as the quadriceps contract. Using ultrasound imaging Herrington and Pearson (2008) were able to show medial displacement of the patella (6.8 mm) with VMO contraction and lateral displacement (5.6 mm) with vastus lateralis (VL) contraction in vivo. Normally the ratio of VMO to VL is approximately 1 : 1, and VMO activity is that of a stabilizing muscle in that it is tonic (Reynolds et al., 1983). In the PFPS patient the VMO to VL ratio is less than 1 as the VMO weakens. In addition, its contractile nature becomes phasic, as its endurance capacity is reduced.
Strengthening has traditionally been achieved by the use of short-range quadriceps exercises and straight leg raising exercises. However, these are both open chain movements and as the knee is in closed chain motion during the stance phase of gait, closed chain actions are more likely to carry over into functional activities.
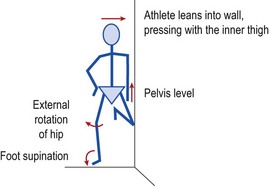
Closed chain VMO re-education may be carried out by performing limited range squats (1/4 squat exercise) or lunges moving the knee from 20–30° flexion to full extension. Step downs from a single stair are useful as they can retrain correct knee motion. The patient should be instructed to keep the knee over the centre of the foot (avoiding adduction and medial rotation) throughout the movement. The use of surface electromyography (sEMG) can help with re-education. The sEMG electrode is placed over the VMO and the patient is taught to activate the muscle in standing and then to maintain this activation throughout the 1/4 squat exercise. The full motor pattern is of foot supination, slight hip abduction and external rotation while maintaining VMO contraction. This may be achieved by standing side on to a wall with the injured leg on the outside (Fig. 9.5). The inner knee and hip are flexed to 45° and this knee presses against the wall, enabling the athlete to hold the trunk vertical while standing on one leg. This body position places significant loading on the gluteus medius of the outer leg to maintain the horizontal pelvic alignment. The foot is supinated, leg turned out and knee slightly flexed to 20°. EMG biofeedback is used over the VMO, and palpation is used to facilitate gluteus medius activity (McConnell, 1994).
In cases where genu recurvatum is present, strengthening of the hamstrings may be required in an attempt to correct the knee hyperextension. In addition to knee musculature, hip strength is particularly important. The hip abductors and lateral rotators warrant special attention as weakness here has been associated with this condition (Beckman, Craig and Lehman, 1989). It is common for young athletes to allow the knee to adduct and medially rotate when descending stairs. This may be due to weakness in the hip abductors, particularly gluteus medius, causing the iliotibial band (ITB) to overwork and tighten. This structure in turn pulls on the patella laterally, displacing or tilting it. Manual muscle testing of the gluteus medius in a side-lying position will often reveal weakness in the affected leg, and tightness in the ITB should be evaluated.
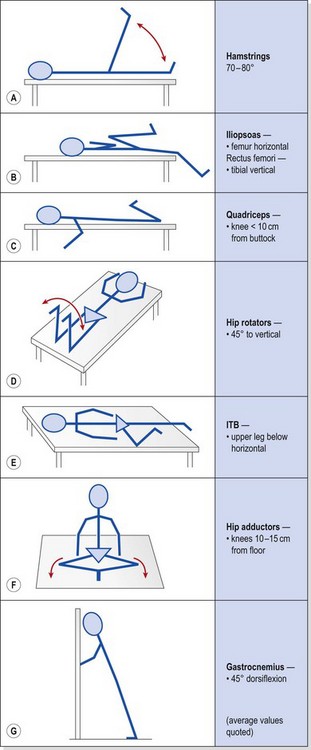
Muscle tightness must be evaluated. The hamstrings, ITB, quadriceps, hip flexors (iliopsoas and rectus femoris), hip rotators and gastrocnemius should all be addressed, as tightness in these structures can alter both knee alignment and gait. Tests, which may also be used as stretching exercises, are shown with average values in Table 9.3. ITB tightness may pull the patella laterally during flexion, while tight hamstrings could result in increased knee flexion and a resultant increase in patellofemoral compression forces. A tight gastrocnemius, in addition to increasing or prolonging knee flexion during gait, will also cause compensatory subtalar pronation.
Table 9.3 Flexibility tests/exercises used in the management of anterior knee pain
Foot biomechanics
During normal running gait (see Chapter 7), the subtaloid joint (STJ) is slightly supinated at heel strike. As the foot moves into ground contact, the joint pronates, pulling the lower limb into internal rotation and unlocking the knee. As the gait cycle progresses, the STJ moves into supination, externally rotating the leg as the knee extends (locks) to push the body forward. This biomechanical action is combining mobility and shock absorption (STJ pronation and knee flexion) with rigidity and power transmission (STJ supination and knee extension), and shows the intricate link between foot and knee function.
If STJ pronation is excessive or prolonged, external rotation of the lower limb will be delayed. At the beginning of the stance phase, STJ pronation should have finished but if it continues the tibia will remain externally rotated, stopping the knee from locking. The leg must compensate to prevent excessive strain on its structures, and so the femur rotates instead of the tibia and the knee is able to lock once more. As the femur rotates internally in this manner, the patella is forced to track laterally.
In certain circumstances the patella can cope with this extra stress, but if additional malalignment factors exist, they are compounded (Fig. 9.6). Anteversion of the femur (internal rotation), VMO weakness and tightness of the lateral retinaculum may all increase the lateral patellar tracking causing symptoms (Tiberio, 1987). For PFPS to be treated effectively therefore, a biomechanical assessment of the lower limb is mandatory. If hyperpronation is present, it must be corrected. This will involve assessment of sports footwear, patient education and orthotic prescription.
Keypoint
Hyperpronation of the foot can be corrected with an orthotic device in cases of patellofemoral pain syndrome.
Although clinically patients with PFPS often improve with the prescription of orthoses, the evidence for their use is poor. In a study comparing physiotherapy management (PF mobilisation, taping, quadriceps muscle re-education) with physiotherapy and orthoses, Collins et al. (2009) studied 179 participants and found contoured foot orthosis to be superior to flat shoe inserts in the short term, but to be no better than physiotherapy with a follow-up of 52 weeks.
Patella position
A number of forces are imposed on the patella as a result of active and passive structures (Fig. 9.7). The vastus lateralis pulls at 12–15° to the long axis of the femur, while the vastus medialis longus pulls at 15–18° and the VMO at 50–55° (Lieb and Perry, 1968). The medial and lateral retinacula, if tight, may tilt the patella (Norkin and Levangie, 1992). The ITB attaches to the patella via a small slip from its lower end called the iliopatellar band (Terry, Hughston and Norwook, 1986). The ITB has a connection to the biceps femoris through the lateral intermuscular septum. Loading the ITB has been shown to both displace the patella laterally and move the contact area of the patellofemoral joint laterally. In addition the pull of the ITB imparts a lateral rotation stress onto the tibia (Kwak et al., 2000). Subjects with PFPS have been shown to have a significantly tighter ITB on their symptomatic side (Hudson and Darthuy, 2009). Lateral patella displacement has been shown to correlate with ITB length when measured using a modified Ober test where the upper leg is straight and pelvic position is monitored using pressure biofeedback (Herrington, Rivett and Munro, 2006).
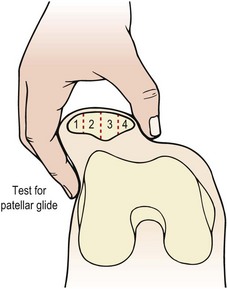
Quantifying the position of the patella is important because, as we have seen above, excessive pressure on the odd facet may result if the patella position is at fault. McConnell (1986) described four different patellar position faults which could be assessed with the patient in the supine position with the quadriceps relaxed. By using the patellar poles as landmarks and comparing their position to the planes of the femur, any malalignment becomes evident. In addition, accessory patellar movements can be assessed with particular emphasis on medial and lateral gliding.
Patellar glide occurs when the patella moves from a neutral position. The distance from the centre of the patella to the medial and lateral femoral condyles is assessed. A difference in the medial distance compared to the lateral of greater than 0.5 cm is significant (Fig. 9.8A). Tightness in the lateral retinaculum, a frequent occurrence in PFPS sufferers, will cause lateralization of the patella. Patellar tilt evaluates the position of the medial and lateral facets of the patella, with PF pain patients frequently showing a more prominent medial facet with difficulty actually palpating the lateral and posterior edge of the patella (Fig. 9.8B). Patellar rotation occurs when the inferior pole of the patella deviates from a neutral position. Medial (internal) rotation occurs when the inferior pole of the patella lies medial to the long axis of the femur. Lateral (external) rotation is present when the inferior pole of the patella lies lateral to the long axis of the femur (Fig. 9.8C). Anteroposterior (AP) tilt exists when both the superior and inferior poles are not clear to palpate, indicating that one is lower in the surrounding soft tissue (Fig. 9.8D).
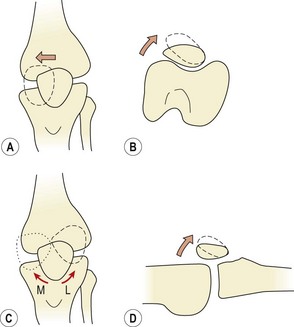
Figure 9.8 Patellar position. (A) Medial and lateral glide. (B) Medial and lateral tilt. (C) Rotation − M: medial, L: lateral. (D) Anteroposterior tilt.
Clinical measurement of patella position has been shown to be reliable and valid. Using 20 experienced manual therapists Herrington (2000) was able to show good agreement between testers when assessing medial and lateral orientation of the patella (r = 0.91 medial measurement, r = 0.94 lateral measurement). In addition validity has been assessed using MRI as the criterion measure, and a good correlation found between clinical examination and MRI measurement (McEwan, Herrington and Thom, 2007).
Measurement of patellar glide is made easier and more accurate by placing a piece of zinc oxide tape over the patella (Fig. 9.9A&B). The knee is flexed to 20° to fix the patella in the trochlea groove of the femur. The medial and lateral epicondyes are marked on the tape together with the mid position of the patella. The tape is removed and the distance between the patella central position and the epicondyles measured.


Alternative measurements of patellar position
Arno (1990) attempted to quantify the patellar position clinically with a description of the A angle. This relates patellar orientation to that of the tibial tubercle. The poles of the patella are palpated and a line is drawn bisecting the patella. Another line is drawn from the tibial tubercle to the apex of the inferior pole of the patella and the angle of intersection forms the A angle (Fig. 9.10). The same author argued that an A angle greater than 35° constituted malalignment when the Q angle remained constant.
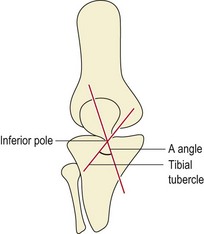
From Arno, S. (1990) The A angle: a quantitative measurement of patella alignment and realignment. Journal of Orthopaedic and Sports Physical Therapy, 12(6), 237–242. With permission.
Radiographic assessment of patellar position is more reliable than clinical measurements (Larsen et al., 1995). Three common measurements are used (Fig. 9.11). Patellofemoral congruence angle (PFCA) is the angle formed between a line bisecting the sulcus angle and a line connecting the apex of the sulcus to the lowest aspect of the patellar ridge. Lateral patellofemoral angle (LPFA) is the angle between lines drawn joining the summits of the femoral condyles and the patellar poles. Lateral patellar displacement (LPD) is the distance between the highest point of the medial femoral condyle and the most medial border of the patella.
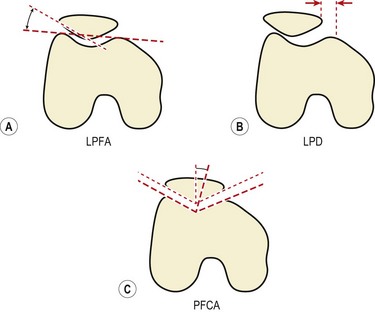
Figure 9.11 Radiographic measurements of patellar position.
Modified from Crossley et al. (2000) with permission.
Using these measurements, patellar malalignment is considered to exist when the LPD is greater than 1 mm, the PFCA is > +5° or the LPFA equals 1° (Crossley et al., 2000).
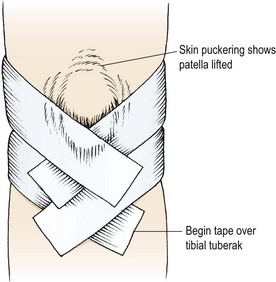
Patellar taping
Pain relief may often be provided by temporarily correcting any underlying fault in patella position through taping. Exercising with this taping in place may re-educate correct muscle sequencing to improve patellar alignment (McConnell, 1994). Initially, open web adhesive taping is applied to protect the skin against excessive tape drag. The pull of the final taping is applied using 5 cm zinc oxide tape. Decreased medial glide is corrected by pulling a piece of tape from the lateral border of the patella (Fig. 9.12A). The soft tissue over the medial femoral condyle is lifted towards the patella to give a skin bunching appearance. Lateral tilt is corrected again by a medially orientated tape. This time, however, the tape covers only the medial half of the patellar face, and again the medial soft tissue is lifted towards the patella (Fig. 9.12B). Rotation is corrected by pulling the patella around its central axis. Internal rotation is corrected by attaching the tape to the upper inner quadrant of the patella. The tape is pulled down medially to rotate the patella clockwise (Fig. 9.12C). External rotation is corrected by placing the tape over the lower inner quadrant of the patella and pulling anti-clockwise. A posterior tilt of the inferior pole should be corrected first to elevate the pole away from the fat pad. The tape is placed over the upper pole of the patella and the patella is taped medially (Fig. 9.12D).
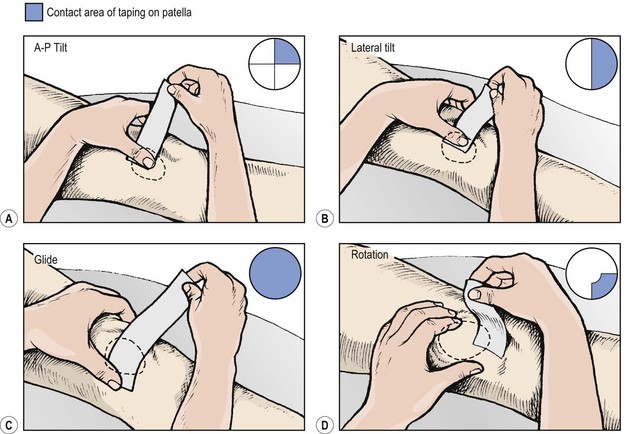
Figure 9.12 Correction of patellar position using tape.
After McConnell, J. (1992) McConnell Patellofemoral Course, London. With permission.
Evidence exists to support the clinical use of patellar taping. Roberts (1989) found a change in LPFA (1.2°) and a reduction in LPD of 1.1 mm in taped knees. Somes et al. (1997) showed a significant improvement in LPFA in weight bearing but none in non-weight bearing with taped knees. Larsen et al. (1995) showed improved PFCA in healthy subjects with taped knees, but this change lessened after 15 minutes of vigorous exercise.
One of the functions of patellar taping is to facilitate selective recruitment of the VMO in the belief that patellar pain patients contract their VMO after the VL (McConnell, 1986). Some studies have supported this hypothesis (Christou and Carlton, 1997; Millar et al., 1999), but others have not (Herrington and Payton, 1997). Interestingly, patellar taping seems to enhance proprioception, but only in those subjects where proprioception is poor to begin with (Callaghan et al., 2000).
Surgery
Before surgery is considered, conservative management must be attempted. Indeed, Insall (1979) stated that surgery was only indicated when continuous pain limited normal activities for at least 6 months and the condition had not responded to conservative management.
Keypoint
Surgery for patellar pain should only be considered after conservative management has been tried and has failed.
The complex aetiology of the condition has led to a number of different surgical procedures (Fig. 9.13).
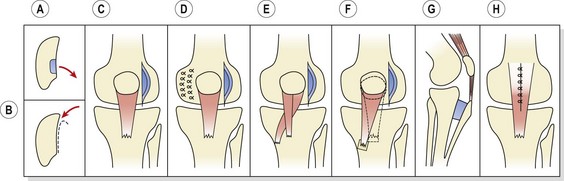
Figure 9.13 Surgical procedures used in anterior knee pain treatment. (A) Excision of diseased area (chondroplasty). (B) Shaving (debridement). (C) Lateral release. (D) Lateral release and medial reefing. (E) Release and transfer of part of tendon (Goldthwait). (F) Release and transfer of entire extensor insertion (Hauser). (G) Tibial tubercle elevation (Maquet). (H) Patellectomy.
From Apley and Solomon (1993), with permission.
Release of tight lateral retinaculum is performed through a small incision or arthroscopy to divide the retinaculum from the lower fibres of the vastus lateralis. Although this technique may be used to decrease a patellar tilt greater than 12° (Zachazewski, Magee and Quillen, 1996), the procedure has been shown to be ineffective at treating subluxation (Post and Fulkerson, 1992) or articular degeneration (Shea and Fulkerson, 1992).
Patellar debridement/shaving has been carried out to remove degenerate articular cartilage on the patella undersurface. Small areas of cartilage may be removed en bloc or larger areas shaved (chondroplasty).
Realignment procedures involve structural transfer to reduce or alter compression forces on the patella. The Maquet operation elevates the tibial tubercle to reduce patella reaction forces and the Hauser manoeuvre uses distal and medial transfer to reduce the valgus vector acting on the patellofemoral joint. The Goldthwait procedure involves release and transfer of part of the patellar tendon. Proximal realignment, by moving the attachment of the vastus medialis, aims at increasing the mechanical advantage of the VMO. This technique is used in the young where alteration of the tibial tuberosity will detrimentally affect the apophysis. Facetectomy involves excision of all or part of a single patellar facet, and patellectomy entails excision of the whole patella. It should be noted that the results for surgical treatment of PFPS are generally poor (Crossley et al., 2007).
Patellar fracture
Patellar fractures in sport occur most frequently in adolescent athletes, usually as a result of jumping. Fracture may occur at the pole of the patella, or as transverse, vertical or comminuted injuries. In the young, the bony fragment may pull off a substantial amount of articular cartilage from the patella undersurface, giving a ‘sleeve’ fracture. Stress fracture at the distal third of the patella has been reported after sprinting (Jerosch, Castro and Jantea, 1989). Conservative treatment, consisting of immobilizing the limb in a cast for 2–3 weeks, is sufficient in 50–60% of cases (Exler, 1991). Surgical treatment involves internal fixation of the patellar fragments, and hemipatellectomy or total patellectomy in the case of comminuted injuries, combined with immobilization in a cast.
Following immobilization, mobility exercises and quadriceps strengthening is started. Strengthening begins with quadriceps setting (QS) exercises and straight leg raising. An extension lag is common in these patients. The leg is locked from a long sitting position, and as it is raised, the tibia falls 2–3 cm as the patient is unable to maintain locking.
Definition
An extension lag occurs when the straight (locked) leg is lifted from a sitting position and the tibia drops slightly. The leg continues to lift but the unlocked position is maintained, because the quadriceps are unable to pull the leg into its final degrees of extension and initiate the screw home effect.
Re-education of the knee-locking mechanism may be achieved in a side-lying (gravity eliminated) position. This is followed by knee bracing with a rolled towel under the knee, the patient being instructed to ‘push down’ on the towel with the back of the knee and, at the same time, to lift the heel from the couch surface. Short range movements over a knee block using a weight bag is the next progression. When 60–90° knee flexion is achieved, light weight training on a universal machine with a relaxation stop, or isokinetic training, is used before closed chain activities.
Patellar dislocation
Patellar dislocation may occur traumatically with any athlete, but is more frequently seen in children between the ages of 8 and 15 years and in middle-aged women who are overweight and have poor muscular development of the quadriceps. Biomechanically, individuals are more susceptible to this condition if they demonstrate genu valgum, femoral anteversion or external rotation of the tibia, and if the VMO is weak. Patellar mobility may be assessed by lateral gliding. If the patella is divided into quadrants (Fig. 9.14), reduced mobility occurs when the patella can only glide laterally by 1 quadarant. Increased mobility and therefore susceptibility to dislocation is present when the patella glides by 2 quadrants or more. In this case, more than half of the patellar surface moves over the femoral condyle (Magee, 2002).
The injury usually occurs when the knee is externally rotated and straightened at the same time, such as when the athlete turns to the left while pushing off from the right foot. In this position the tibial attachment of the quadriceps moves laterally in relation to the femur, increasing the lateral force component as the muscle group contracts. The patella almost always dislocates laterally and is accompanied by a ripping sensation and excruciating pain, causing the knee to give way. As the knee straightens, the patella may reduce spontaneously with an audible click.
Keypoint
Patellar dislocation usually occurs when an athlete turns and pushes off at the same time, combining external rotation and extension of the knee.
Swelling is rapid due to the haemarthrosis, causing the skin to become taught and shiny. Bruising forms over the medial retinaculum, and the athlete is normally completely disabled by pain and quadriceps spasm. On occasion the VMO may avulse from the patella, revealing a hollow, and little tissue resistance to palpation, along the medial edge of the patellofemoral joint.
Initial treatment is to immobilize the knee completely and apply the RICE protocol. Aspiration may be required if pain is intense, but usually swelling abates with non-invasive management. Quadriceps re-education plays an important part in the rehabilitation process, with VMO strengthening being particularly important. The medial retinaculum must be allowed to heal fully, and it is a mistake to allow these athletes to mobilize unprotected too soon. Only when 90° knee flexion is achieved and the patient is able to perform a straight leg lift with 30–50% of the power of the uninjured leg are they ready to walk without support.
Early quadriceps exercises
The question of which quadriceps exercise to use at the beginning of rehabilitation is one of considerable debate within physiotherapy. The decision depends on a number of factors including PF reaction forces, the efficiency of an exercise to emphasize the VMO, and the relevance of an exercise movement to functional requirements (see Training specificity, Chapter 4).
The choice is often between open and closed chain movements, and bracing or lifting leg actions. In the gait cycle, the quadriceps are active during leg loading as the opposite leg moves into the swing phase, and to a lesser extent at the beginning of toe-off. In jumping, these muscles create very large concentric and eccentric forces in closed chain format. In a fast kicking action they work in an open chain action, but most of the work is from the two-joint rectus femoris (Richardson and Bullock, 1986). Both open chain and closed chain actions are important, but for early stage rehabilitation closed chain action emphasizing stability is more appropriate.
Comparing the leg extension with the leg press, Steinkamp et al. (1993) found PF joint stress, PF reaction force and quadriceps force to be significantly greater in a leg extension exercise from 0–30°, but significantly greater in a leg press action from 60–90°. These authors concluded that the leg press was more appropriate because it placed minimal stress on the PF joint in the functional range of motion and simulated normal movement patterns.
Keypoint
Closed chain movements reduce patellofemoral (PF) joint forces during inner range of the quadriceps. In addition they are more functional than open chain actions because they simulate the normal weight-bearing activities of daily living.
It is often argued that QS with isometric hip adduction will increase the recruitment of the VMO because some of the VMO fibres originate from adductor magnus (Reid, 1992). However, Karst and Jewett (1993) compared quadriceps setting (QS), straight leg raising (SLR), SLR with the hip laterally rotated, and SLR with isometric hip adduction with resistance equivalent to 5% bodyweight. These authors found that QS elicited a greater degree of activity than SLR. In addition, SLR with either hip adduction or lateral rotation failed to increase emphasis on the VMO over that of the rest of the quadriceps.
ITB friction syndrome
The ITB is a non-elastic collagen cord stretching from the pelvis to below the knee. At the top it is attached to the iliac crest where it blends with the gluteus maximus and tensor fascia lata. As the tract descends down the lateral side of the thigh, its deep fibres attach to the linea aspera of the femur. The superficial fibres continue downwards to attach to the lateral femoral condyle, lateral patellar retinaculum and anterolateral aspect of the tibial condyle (Gerdy’s tubercle). A large amount of the lateral retinaculum actually arises from the ITB to form the iliopatellar band having a direct effect on patellar tracking (Zachazewski, Magee and Quillen, 1996).
In standing, the ITB lies posterior to the hip axis and anterior to the knee axis, and therefore helps to maintain hip and knee extension, reducing the muscle work required to sustain an upright stance. As the knee flexes to 30° the ITB passes posterior to the knee joint axis, and in so doing it glides over the lateral femoral condyle. In running, during the swing phase the ITB lies anterior to the greater trochanter and hip flexion/extension axis, reducing the workload required for hip flexion.
Aetiology
Tightness of the ITB can occur in a number of patient groups. The tall, lanky teenager who has recently undergone the adolescent growth spurt may experience pain if soft tissue elongation lags behind long bone development. Tightness in adolescent females is a consistent factor in PFPS, although the relationship between the ITB and the patella has been debated by some authors (Rouse, 1996). The second major group of sufferers are adult athletes, particularly distance runners. A number of factors can contribute to problems within this group. Running on cambered roads and using shoes worn on their lateral edge will increase varus knee angulation and may overstretch a tight ITB. Rapid increases in speed or hill work can place excessive stress on the structure. In addition, imbalances of muscle strength and flexibility around the knee and hip may lead to the gradual onset of symptoms.
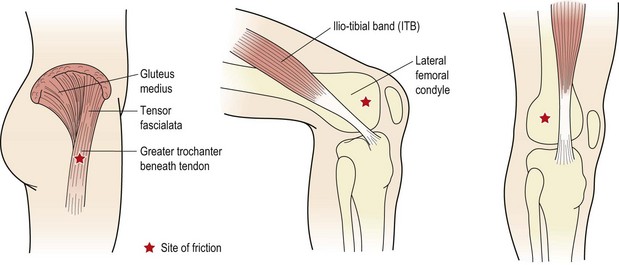
Pain normally occurs over either the trochanteric bursa or the lateral femoral condyle (Fig. 9.15). Pain is experienced to palpation, but also to limited range squats or lunges on the affected leg. As the knee flexes and the ITB passes over the lateral femoral condyle, friction may occur, causing pain of increasing intensity. Flexibility tests, particularly the Ober manoeuvre and Thomas test, often reveal pain and a lack of flexibility. In addition, compressing the ITB over the proximal part of the lateral femoral condyle with the knee flexing and extending to 30° may elicit pain (Noble, 1980). Where the ITB is tight and the tensor fascia lata overactive, the gluteus medius muscle is normally lengthened. Both muscles must therefore be addressed in treatment.
Management
The initial inflammation of this condition responds to anti-inflammatory modalities, but the underlying cause must be addressed. Modifications include alterations of running surface and footwear, and changes to training intensity, frequency, duration and content. Where limited range motion is identified, stretching procedures are called for. Hip flexor and extensor flexibility is regained by using exercises previously described, and the ITB itself is stretched using an adaptation of the Ober manoeuvre.
The ITB insertion at the knee is first heated with hot packs or diathermy. The pelvis is stabilized by the patient flexing and holding the lower knee. The affected upper leg is initially abducted and extended at the hip and flexed at the knee. From this position, hip extension is maintained and the leg is pushed downwards into adduction, and held for 30–60 seconds, with the stretch being repeated four or five times. As adduction commences, the patient’s pelvis will tend to tilt and an assistant should press down on the rim of the ilium to stabilize the pelvis and increase the stretch.
Between treatment sessions the patient should attempt this procedure at home. The weight of the leg may be used to press it into adduction, and a weight bag on the knee will assist this. In addition, a training partner or family member can be taught to help maintain lumbopelvic stability.
Weakness in the hip abductors may allow the pelvis to tilt or ‘dip’ during the stance phase of walking or running. This often gives the impression of a mild Trendelenburg gait, and may be habitual following lower limb injury. Gait re-education and abductor strengthening are called for. The abductors may be strengthened from an open chain or more functional closed chain starting position. Open chain strengthening is performed using a weight bag in a side-lying hip abduction exercise. Closed chain strengthening is carried out with the athlete standing on the affected leg, and keeping it locked. The unaffected leg is flexed at the knee. From this position, the pelvis is allowed to drop towards the unsupported side and pulled back to the horizontal position by hip abductor action (Fig. 9.16).
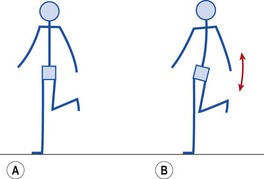
Figure 9.16 Hip abductor strengthening. (A) Athlete stands on affected leg. (B) Allowing the opposite hip to drop and then pulling it up works the abductors of the weight-bearing limb.
The gluteus medius muscles, if lengthened, should be worked using combined abduction and lateral rotation (clam shell exercise) of the hip to target the posterior fibres especially.
Collateral ligament injuries
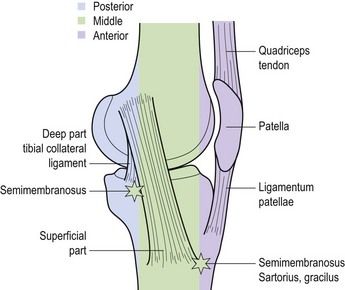
The medial collateral ligament (MCL) is a broad flat band about 8 or 9 cm in length. It travels downwards and forwards from the medial epicondyle of the femur to the medial condyle and upper medial shaft of the tibia. At its femoral attachment some fibres continue into the adductor magnus muscle. The ligament has both deep and superficial fibres, with the deep fibres attaching to the medial meniscus, and the superficial fibres extending below the level of the tibial tuberosity. The posterior border of the deep ligament is associated with an expansion from the semimembranosus muscle adding strength to this portion of the joint capsule. The superficial fibres have anterior, middle and posterior portions.
Keypoint
The medial collateral ligament has both deep and superficial fibres. The deep fibres attach to the medial meniscus. The superficial fibres have anterior, middle and posterior portions which must all be considered in treatment.
When the knee is in full extension, it is in close pack formation. The medial femoral condyle is pushed backwards, and the medial epicondyle lifts away from the tibial plateaux, tightening the posterior part of the MCL. As the knee is flexed, the posterior part of the ligament relaxes, but the anterior and middle parts remain tight. By 80–90° flexion, the middle of the ligament is still tight, but the anterior and posterior portions are lax. In this way, the strong middle section of the ligament remains tight for most of the range of movement. The changing distribution of tension strain in the ligament means that the section which is affected through injury will depend on the knee joint angle when the injury occurred, so an accurate history is extremely helpful.
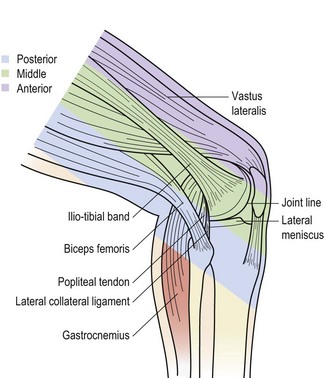
The lateral collateral ligament (LCL) is a round cord about 5 cm long, which stands clear of the joint capsule. It travels from the lateral epicondyle of the femur to the lateral surface of the head of the fibula. In some subjects the ligament is continuous with the peroneus longus muscle. The ligament splits the tendon of biceps femoris, and is separated from the joint capsule by the popliteus muscle, and the lateral genicular vessels and nerve (Palastanga, Field and Soames, 1989). The lower end of the lateral ligament is pulled back in extension, and forwards in flexion of the knee.
Damage to the MCL can result from excessive valgus angulation of the knee coupled with external rotation, while LCL damage is normally through varus strains coupled with internal rotation. MCL damage usually gives pain over the medial epicondyle of the femur, the middle third of the joint line or the tibial insertion of the ligament. With LCL damage, pain is normally over the head of the fibula or lateral femoral epicondyle.
Palpating the collateral knee structures
The joint line of the knee can be found by sliding one finger up the patellar tendon and palpating the apex (lower part) of the patella. Rest one finger horizontally across this point and the joint line lies at the lower edge of the finger tip.
Keypoint
To find the knee joint line, slide one finger up the patellar tendon until it touches the lower part of the patella. Rest the finger horizontally across this point and the joint line is felt as a shallow groove at the lower edge of the finger tip.
Palpation of the medial aspect of the knee is made easier by dividing the area into thirds (Fig. 9.17). The anterior third comprises the edge of the patellar tendon and extensor retinaculum and the superficial border of the MCL. Inferior and medial to the tibial tubercle are the insertions of semi-tendinosus, sartorius and gracilis (pes anserine structures). The middle third comprises the MCL and the coronary ligaments. The posterior third comprises the deep part of the MCL and the diverse expansion from the semi-membranosus. Palpation of the lateral aspect of the knee may be similarly divided into thirds (Fig. 9.18). The anterior third consists of the lateral edge of the patellar tendon and the lateral retinaculum. The middle third is dominated by the ITB and the posterior third consists of the fibular collateral ligament, the tendon of biceps femoris, the lateral head of gastrocnemius and popliteus.
Ligament tests
The integrity of the ligaments is tested by applying a varus and valgus stress to the knee flexed to 30°. Performing the same test with the knee locked is ineffective as this is the close pack position, and nearly 50% of medial and lateral stability is provided by the cruciate ligaments and joint capsule.
Pain and/or laxity to valgus and varus stress implicates structures other than the collateral ligaments. Valgus (abduction) stresses places tension on the MCL, posterior oblique ligament and posteromedial capsule. Varus (adduction) stress places tension on the lateral collateral ligament, posterolateral capsule, arcuate ligament and ITB. Diagnosis must therefore be made using several tests and the patient’s history.
The easiest way to perform the varus/valgus test is with the patient’s hip abducted, thigh supported on the couch or a rolled towel and the lower leg over the couch side. Where a lower couch is used the practitioner may need to use his/her own thigh to rest the patient’s leg (Fig. 9.19). The practitioner’s hands are positioned for maximum leverage with pressure coming through the forearms rather than from the hands alone. The limb is tightly controlled by holding close to the joint line and supporting the leg against the practitioner’s body.



First and second degree injuries are generally treated conservatively. Third degree injuries (complete rupture) have been treated surgically, but some authors argue that stability of the knee is not improved to a greater extent than with non-operative intervention (Keene, 1990). First degree injuries are generally treated partial or full weight bearing with the ligament supported by strapping. Second and third degree injuries are managed non-weight bearing.
Initially, the aim is pain relief, swelling reduction and the start of mobile scar formation. Isometric quadriceps drill is begun and modalities used to reduce pain and swelling (Table 9.4). At night a knee brace may be used to protect the ligament. By the third or fourth day after injury (sometimes earlier with a first degree and later with a third degree injury) gentle mobility exercises are begun, either in a side-lying starting position or in the pool. Gentle transverse frictions are used to encourage mobile scar formation. The sweep should be quite broad and a large section of the ligament treated. Free or light resisted exercises are begun to the knee, hip and calf musculature within the pain-free range. Isokinetics may be used with the aim of restoring the HQ ratio to that of the uninjured limb.
Table 9.4 Guidelines for medial collateral ligament rehabilitation
* Criterion for progression to phase three: no joint effusion; minimal pain to direct ligament palpation; full or near full painless range of motion; knee stable to hop/hop and turn tests. After Reid (1992), with permission.
When 90° of pain-free movement is obtained (usually 10–14 days after injury with a grade 3 sprain), the rehabilitation programme can be progressed further to include more vigorous activities, and increased mobility and strength training. An exercise cycle or light jogging may be used, and swimming (not breaststroke) started. Weight training is progressed to use leg machines, and some power training is added. Towards the end of this period, depending on pain levels, shallow jumping, bench stepping, circle running and zig-zagging in the gym are used to gradually introduce rotation, shear and valgus stress to the knee. In addition to improving strength and power, these exercises build confidence and provide an assessment of knee stability.
Occasionally, anteroposterior X-ray will show a bony plaque under the femoral attachment of the MCL (Pellegrini-Stieda disease). The attachment of the adductor magnus onto the adductor tubercle may also be partially avulsed. The condition is normally due to ossification of the haematoma formed at the time of injury (Apley and Solomon, 1993), and MCL injuries which do not improve or get worse with treatment should be examined radiographically to check for this condition. Infrequently it may occur in the absence of apparent trauma. The condition will normally resolve with rest, but where pain is continuous, surgical removal is required.
Cruciate ligaments
Structure and function
The cruciate ligaments are strong rounded cords within the knee joint capsule, but outside its synovial cavity. The ligament fibres are 90% collagen and 10% elastic, arranged in two types of fasciculi. The first group travels directly between the femur and tibia, as would be expected, but the second set spiral around the length of the ligament. This structure enables the ligament to increase its resistance to tension when loaded. Under light loads only a few of the fasciculi are under tension, but as the load increases, the spiral fibres unwind, bringing more fasciculi into play and effectively increasing the ligament strength.
The anterior cruciate ligament (ACL) is attached from the tibia, anterior to the tibial spine. Here, it blends with the anterior horn of the lateral meniscus and passes beneath the transverse ligament. Its direction is posterior, lateral and proximal to attach to the posterior part of the medial surface of the lateral femoral condyle. As it travels from the tibia to the femur, the ligament twists in a medial spiral. The posterolateral part of the ACL is taut in extension and the anteromedial portion is lax. In flexion, all of the fibres except the anteromedial portion are lax.
The posterior cruciate ligament (PCL) arises from the posterior intercondylar area of the tibia and travels anteriorly, medially and proximally, passing medial to the ACL to insert into the anterior portion of the lateral surface of the medial femoral condyle. The majority of the PCL fibres are taut in flexion, with only the posterior portion being lax, and in extension the posterior fibres are tight but the rest of the ligament is lax.
The ACL provides 86% of the resistance to anterior displacement and 30% to medial displacement, while the PCL provides 94% of the restraint to posterior displacement and 36% to lateral stresses (Palastanga, Field and Soames, 1989).
Injury
Of the two ligaments, the ACL is far more commonly injured in sport, with over 70% of knee injuries with acute haemarthrosis involving ACL damage (Noyes, Bassett and Grood, 1980). The athlete has often participated in either a running/jumping activity or skiing. The history is usually of a non-contact movement such as rapid deceleration, a ‘cutting’ action in football, or a twisting fall. The combination is frequently one of rotation and abduction, a similar action to that which causes MCL or medial meniscus damage, and the three injuries often coalesce to form an ‘unhappy triad’.
Following injury, swelling is usually immediate as a result of haemarthrosis, leaving a hot, tense, inflamed knee within 1 or 2 hours after injury. This contrasts with simple effusion which may take many hours to form (normally overnight). In addition, the athlete often describes ‘something going’, ‘popping’ or ‘ripping’ inside the knee as it gave way. Rapid swelling, a feeling of internal tearing and giving way are essential elements of the history of injury with this condition. The classic anterior draw test is often negative at this stage due to hamstring muscle spasm and effusion. The high strain rates encountered in sports situations cause the majority of injuries to occur to the ligament substance rather than the osseous junction and so x-ray is usually unrevealing.
Manual testing
Diagnosis relies heavily on clinical history and tests for instability, the latter being the subject of some debate. The two most common tests are the anterior draw test and modifications of this, and the pivot shift.
The classic anterior draw test (Fig. 9.20) involves flexing the patient’s knee to 90° and stabilizing the foot with the examiner’s bodyweight. The proximal tibia is pulled anteriorly and the amount of movement compared to the ‘normal’ value of the uninjured leg. Various grades of movement may be assessed, grade 1 being up to 5 mm of anterior glide, grade 2, 5–10 mm and grade 3 over 30 mm. The test can, however, give false negatives if haemarthrosis prevents the knee being flexed to 90°. Movement can also be limited by protective hamstring spasm or if the posterior horn of the medial meniscus wedges against the medial femoral condyle.

Keypoint
The classic anterior draw test can give a false negative result if haemarthrosis prevents the knee being flexed to 90°. Movement can also be limited by protective hamstring muscle spasm.
Lachman test
The Lachman test, a modification of the anterior draw, has been shown to be highly reliable (Donaldson, Warren and Wickiewicz, 1985). The test is performed with the patient lying supine. The examiner holds the patient’s knee in 20° flexion, minimizing the effect of hamstring spasm and reducing the likelihood of meniscal wedging. The reduced angle of flexion compared with the anterior draw test is less painful for the patient, and comfort can be further enhanced by placing the knee over a pillow. One hand stabilizes the femur and the other applies an anterior shearing force to the proximal tibia, avoiding medial rotation (Fig. 9.21A).
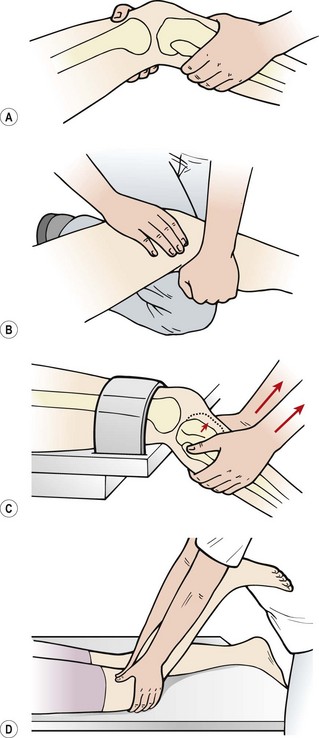
Figure 9.21 The Lachman test and modifications. (A) Standard test. (B) Patient’s leg supported over the therapist’s knee. (C) Patient’s leg over couch end and supported by a strap. (D) Reverse Lachman’s.
Clinically, the test may be modified in a number of ways to avoid holding the weight of the whole leg. The therapist may place his or her flexed knee on the couch and rest the patient’s leg over it (Fig. 9.21B). Alternatively, the patient’s femur may be supported on the couch with the tibia over the couch end. The femur is stabilized with a strap, leaving both of the therapist’s hands free to shift the tibia (Fig. 9.21C). If anterior translation of the tibia is felt, the test is positive. The movement is compared to the uninjured knee, both for range and end-feel, an ACL tear giving a characteristically soft end-feel. The same grading system is used as with the anterior draw test.
With the anxious patient who is unable to relax, the reverse Lachman test may be used (Rebman, 1988). Here, the patient is in prone lying with the knee flexed to 20°. The examiner grasps the patient’s tibia with the forefingers over the tibial tubercle and the thumbs over the politeal fossa (Fig. 9.21D). Anterior displacement, rather than being felt (as in the classic Lachman test) is actually seen with this modified test.
Pivot shift tests
Another frequently used test is the pivot shift, and its adaptations (Galway, Beaupre and MacIntosh, 1973). These work on the basis that the ACL-deficient knee will allow the lateral tibial plateau to sublux anteriorly (Fig. 9.22). By applying forces to enforce this and then moving the knee, the tibia can be made to reduce rapidly, causing a ‘thud’. The pivot shift test starts with the affected leg in full extension. The examiner grasps the ankle of this leg with his or her distal hand and the outside of the ipsilateral knee with his or her proximal hand. The ankle and tibia are forced into maximum internal rotation, subluxing the lateral tibial plateau anteriorly. The knee is slowly flexed as the proximal hand applies a valgus stress. If the test is positive, tension in the ITB will reduce the tibia at 30–40° causing a sudden backward ‘shift’. The major disadvantage with this test is that the patient must be relaxed throughout the manoeuvre, a situation often not possible because of pain. Donaldson, Warren and Wickiewicz (1985) tested over 100 ACL-deficient knees preoperatively and found the pivot shift test to be positive in only 35% of cases. The same examination carried out under anaesthesia (muscles completely relaxed) gave 98% positive results.
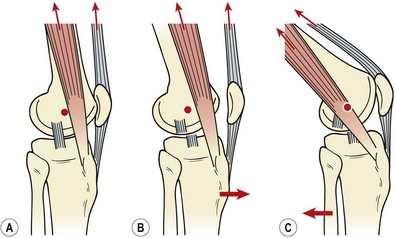
Figure 9.22 The pivot shift test. (A) In the normal knee at rest, anterior pull of the quadriceps and iliotibial band (ITB) is resisted by the intact anterior cruciate ligament (ACL). The ITB lies in front of the knee pivot point. (B) In the ACL-deficient knee the tibia is drawn forwards, pushing the ITB anterior to the pivot point of the knee. (C) In the ACL-deficient knee the pivot point of the knee moves backwards (closer to the ITB) allowing the tibia to reduce with a thud.
From Reid (1992) with permission.
Keypoint
The pivot shift test is only accurate if the patient remains relaxed throughout the movement. Accuracy is increased from 35% for the conscious patient to 98% when the test is performed under anaesthetic.
This test is reversed in the jerk test (Table 9.5), while the flexion rotation draw (FRD) test eliminates the need for a valgus force by using gravity to sublux the tibia. A reliability of 62% has been reported for the FRD, rising to 89% with the anaesthetized patient (Jensen, 1990). The Slocum (ii) test (Slocum, James and Larson, 1976) uses a side-lying position to perform a pivot shift and is particularly suitable for heavier patients.
Table 9.5 Manual laxity tests of the knee
| Anterior draw | Knee flexed to 90°, foot stabilized, tibia drawn forwards |
| Lachman | Knee flexed to 20°, femur stabilized, tibia drawn forwards |
| Pivot shift (MacIntosh) | Knee extended, foot/tibia internally rotated, valgus strain on knee as it is flexed |
| Jerk (reverse pivot shift) | Knee flexed to 90°, valgus stress on knee, internally rotate tibia and extend knee |
| Flexion/rotation drawer | Leg held by tibia only, knee in 20° flexion posterior force on tibia, then flex knee |
| Slocum | (i) Knee and hip flexed, anterior drawer test in 30° external rotation. AMRI if medial condyle still moves forwards |
| (ii) Patient on uninjured side, pelvis rotated posteriorly. Ankle on couch. Knee flexed to 10°, apply valgus stress and push further into flexion. Tests for ALRI. Knee flexed to 45°, tibia externally rotated. | |
| Losee | Knee extended, and valgus force applied, allowing tibia to internally rotate |
AMRI—anteromedial rotary instability, ALRI—anterolateral rotary instability.
Adapted from Jensen (1990). Manual laxity tests for anterior cruciate ligament injuries. Journal of Orthopaedic and Sports Physical Therapy, 11(10), 474–481.
Since the ACL has two functionally separate portions (see above), depending on the knee angle at the time of injury, only one portion may be damaged, resulting in a partial ligament tear. If the anteromedial band is damaged but the posterolateral portion is intact, the Lachman test may be negative but the anterior draw positive. This is because the anteromedial portion is tightened as the knee flexes, and so will be tighter (and therefore instability will be more apparent) with the 90° knee angle of the anterior draw. Similarly, if the posterolateral band is disrupted (the more usual situation), the anterior draw may be negative but the Lachman positive, as this portion of the ligament becomes tighter as the knee approaches extension.
Partial tears usually remain intact and show good long-term results. However, Noyes et al. (1989) argued that progression to complete deficiency, although unlikely in knees which have sustained injury to one quarter of the ligament, may be expected in 50% of knees with half ligament tears and 86% of those with three-quarter tears.
Combined instabilities
Most ligament tests assess instability in only one plane, but various combinations of instability exist in two or more planes (Fig. 9.23). The two most common instabilities are anteromedial, in which the medial tibial plateau moves anteriorly on the femur, and anterolateral, where the lateral tibial plateau moves anteriorly. Movement of the lateral tibial plateau posteriorly (posterolateral instability) or the medial tibial plateau posteriorly (posteromedial instability) may also occur. Anteromedial instabilities may be assessed using a modified anterior draw and anterolateral instabilities by the pivot shift (above).
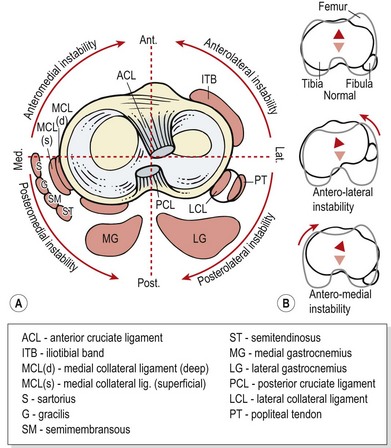
Figure 9.23 (A) Structures contributing to combined instabilities of the knee. (B) Movement directions.
From Magee (2002), with permission.
For the modified anterior draw test or Slocum (i), the patient sits with the hip and knee flexed. The test is to perform the anterior draw initially with the tibia in neutral and then with tibial rotation. The degree of anterior movement of the medial tibial condyle is assessed using the standard draw test and then the tibia is externally rotated to 15–30°. The external rotation tenses (‘winds up’) the anteromedial structures, and if the tibial rotation fails to reduce the anterior movement of the medial condyle the test is positive.
Arthrometer testing
An arthrometer measures joint motion. The most commonly reported arthrometer in the literature for assessing knee joint motion is the KT-1000 (Med Metrics Corp. Inc., San Diego, California, USA). To perform anteroposterior testing, patients are placed in the Lachman test position (see above) with the knee flexed to 30°. In this position the patella is engaged in the trochlea, so that it does not move during assessment of tibial movement relative to the femur. The arthrometer unit is placed on the anterior tibia and held in place with Velcro straps around the calf. Leg rotation is avoided by supporting the heel in a shallow rubber cup on the couch.
The arthrometer handle applies a force to the tibia usually of 67 N (15 lb) and 89 N (20 lb). The difference in anterior displacement between the two forces is called the ‘compliance index’ and is a frequently quoted measure of knee joint stability. Alternatively, maximal manual force may be used and the injured and non-injured legs compared (side-to-side measurement). Tibial translation (to the nearest 0.5 mm) is measured by the change in relative alignment of pads placed on the tibial tuberosity and patella. However, the translation values seen with arthrometry do not represent actual bony motion specifically. When arthrometer readings are compared with stress radiographs, different values are obtained (Staubli and Jakob, 1991), suggesting that an amount of tissue compression is occurring.
Arthrometer measurement has been found to be consistently accurate. Using maximal manual testing and side-to-side measurement, 90% of conscious and 100% of anaesthetized patients with acute ACL tears had measurements greater than 3 mm (Daniel, Malcom and Losse, 1985). Using 141 uninjured subjects, Bach, Warren and Wickiewicz (1990) showed 99% to have side-to-side measurements less than 3 mm using a force of 89 N.
A number of factors can influence measurement consistency and accuracy. First, muscle relaxation must be obtained. Comparing conscious and anaesthetized patients at force values of 67 N and 136 N, Highgenboten, Jackson and Meske (1989) found side-to-side differences greater than 2 mm in 64% and 81% in conscious patients, but 72% and 83% in anaesthetized patients, respectively. Greater muscle relaxation can be obtained as patients become familiar with the testing procedure, and repeated measurements have certainly been shown to be more effective than isolated tests (Wroble et al., 1990). In addition, arthrometer measurement has been found to be operator dependent (Forster and Warren-Smith, 1989). Consistently accurate results will only be obtained with trained testers who have gained significant expertise. Larger testing forces tend to produce better reproducibility, with maximal manual testing giving the most accurate results with all instruments (Torzilli, 1991; Anderson et al., 1992).
Management
First and second degree injuries may be immobilized initially and then subjected to intense rehabilitation to re-strengthen the supporting knee musculature. A de-rotation brace may be used to protect the knee until muscle strength is sufficient. Third degree injuries, with marked instability, may be treated surgically, although some authors argue that rehabilitation alone is the better solution (Garrick and Webb, 1990).
General guidelines of indications for surgery include combined injuries (ACL, MCL and/or meniscus), and high degrees of anterior shear (Feagin et al., 1995). Isolated injuries treated conservatively seem to remain functional. Jackson, Peters and Marczyk (1980) reported a retrospective study with a mean follow-up of 10 years. Of those patients treated non-operatively, 80% of isolated ACL injuries had no functional deficit, compared to only 10% of those with combined injuries. In a later study (Evans et al., 2001), 90% of those with isolated injuries who were treated non-operatively reported that they were satisfied with the result compared to 60% for those with combined injuries.
Patients treated non-operatively are often presumed to be at risk of developing meniscal injury and joint degeneration (Kannus and Jarvinen, 1989). However, x-ray examination and bone scan of patients treated both operatively and non-operatively has shown an increased incidence of degenerative joint disease in the surgically treated group. However, the explanation for this finding is the subject of debate (Woo et al., 1994).
Surgery
Surgery involves repair and reconstruction, most authors agreeing that the latter is more appropriate. Reconstruction techniques may be either extracapsular, intracapsular or a combination of the two. In the UK, 58% of orthopaedic surgeons use bone−patellar tendon autografts and 33% semitendinosis/gracilis autografts (Kapoor et al., 2004).
Extracapsular reconstruction has been described using the MacIntosh procedure (Wilson, Lewis and Scranton, 1990). A 10 × 1 cm strip of the ITB is passed beneath the fibular collateral ligament, under the lateral attachment of the gastrocnemius, and then looped back on itself. The knee is flexed to 60° and the leg externally rotated before the ITB is pulled tight and secured with sutures.
Alternatively, a graft may be cut from the middle third of the patellar tendon, to include both non-articular patellar and tibial tubercle bone (bone−patellar tendon autograft). This has the advantage that it leaves other structures around the knee intact. Tunnels are then drilled in the tibia and femur, travelling through the attachments of the ACL. The graft is passed through the bone tunnel and attached to the lateral aspect of the lateral femoral condyle and the tibial tubercle. The graft is secured with cancellous screws and sutures. This procedure gives a very strong graft, but may have the complication of patellar pain following surgery. Flexion contraction of 5° or more may be present in almost one quarter of these patients (Sachs et al., 1989), and PF irritability can result. Where contracture is a likelihood, rehabilitation should place a greater emphasis on maintaining full knee extension. A similar technique has been described by Wilson and co-workers (1990) using the semitendinosus tendon instead of the patellar tendon, to avoid patellar complications (semitendinosis/gracilis autograft).
Several structures may be used for grafts, and Noyes, Butler and Grood (1984) showed the patellar tendon graft to have a strength of 168% of the ACL while the semitendinosus had only 70%, gracilis 49% and the quadriceps/patellar retinaculum only 21%. Synthetic tissues, such as polytetrafluoroethylene (PTFE), are now used more frequently, and mobility may be attained more rapidly following surgery using these materials. However, synthetics are generally only used where intra-articular reconstructions have failed. Bovine substances have been used, but problems have been caused by reactive synovitis following these operations. Allogenic tendon grafts from cadavers and amputation specimens have been used to good effect with patients suffering chronic ACL insufficiency (Shino et al., 1986).
Guidelines for rehabilitation following ACL reconstruction
Rehabilitation will depend very much on the particular surgical procedure which has been performed. As synthetic grafts do not need to redevelop a blood supply, they can be rehabilitated more quickly than autogenous grafts. Intra-articular repairs weaken with revascularization, so the repairing ligament will reach only 25–50% of its ultimate strength by 6–12 weeks following surgery. In contrast, extra-articular grafts regain approximately 75% of their original strength in the same time (Reid, 1992). Tendon grafts often suffer fewer complications and the patellofemoral joint remains mobile, while extracapsular grafts require more restraint on movement. Patellar tendon reconstructions tend to be the strongest grafts but cause greater morbidity due to the anterior surgical approach (Briggs, Sandor and Kenihan, 1995). Arthroscopic repairs will recover more quickly than open repairs as the knee joint is less affected. There is less swelling and a reduced likelihood of complications.
The dichotomy is that immobilization is thought desirable for healing of the graft, but early mobility is required to avoid cartilage degeneration, soft tissue contracture and muscle atrophy. To overcome the combined problem of healing and mobility, the patient is mobilized early, providing the movement used does not overly stress the graft.
Keypoint
Early mobilization is required to avoid cartilage degeneration, soft tissue contracture and muscle atrophy. However, any movement used must not overly stress the graft.
The range of motion possible without placing undue tension on the graft must be established, and a protective brace may be used to limit undesirable movements. Sandberg, Nilsson and Westlin (1987) showed the time needed to return to sport to be 5 weeks shorter and range of motion significantly better following the use of a hinged cast allowing knee flexion from 20° to 70°. Noyes, Mangine and Barber (1987) mobilized patients on the second day after surgery and found no adverse effects on the ligament reconstruction. Some authors even begin weight bearing immediately (Shelbourne and Nitz, 1990).
Early rehabilitation (up to 4 days following surgery) focuses on avoiding the standard complications following general surgery, and reducing pain (Table 9.6). Simultaneous contraction of the hamstrings and quadriceps are used to aid the leg muscle pump, but isolated quadriceps exercises and straight leg raising are avoided. Isolated quadriceps bracing has been shown to place considerable stress on the ACL whereas isolated hamstring actions actually reduce strain (Renstrom, Arms and Stanwick, 1986). Prone-lying leg hanging (Fig. 9.24A) is a useful exercise for regaining terminal extension while placing minimal stress on the healing tissues. The patient lies prone, with the thigh supported on a folded towel, leaving the anterior knee free. The weight of the tibia presses the knee into extension. Resistance may be supplied by a small weight bag attached to the heel. The patient then performs eccentric hamstring actions, allowing the tibia to lower as far as pain will allow. A wedge may be used below the tibia as a relaxation stop.
Table 9.6 Guidelines for ACL rehabilitation
After Reid (1992).
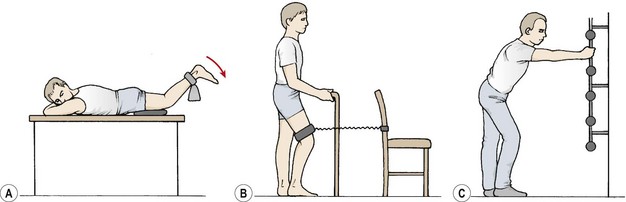
Figure 9.24 Staged anterior cruciate ligament (ACL) exercises. (A) Prone leg hang—to regain terminal extension while working the hamstring muscles. (B) Closed chain co-contraction of quadriceps and hamstrings. (C) Adding trunk flexion increases hamstring muscle work.
From 5 to 14 days following surgery, co-contraction activities of the quadriceps and hamstrings are performed by using simple closed chain actions. Co-contraction of the hamstrings and quadriceps has been shown to place 15% of the quadriceps tension on the ACL at 5° knee flexion. By the time flexion had increased to a mean angle of 7.4° this force is reduced to zero. As the angle of flexion increases still further, a posterior draw force is imposed (Yasuda and Sasaki, 1987).
Closed chain terminal leg extension is a useful exercise for co-contraction of the quadriceps and hamstrings (Fig. 9.24B). The athlete stands predominantly on the unaffected leg, placing sufficient weight on the injured leg to prevent the foot from moving. An elastic resistance band attached to a wallbar is placed around the mid-thigh, and the action is to extend the hip and knee simultaneously. Adding trunk flexion (Fig. 9.24C) has been shown to increase hamstring activity on surface EMG (Ohkoshi et al., 1991).
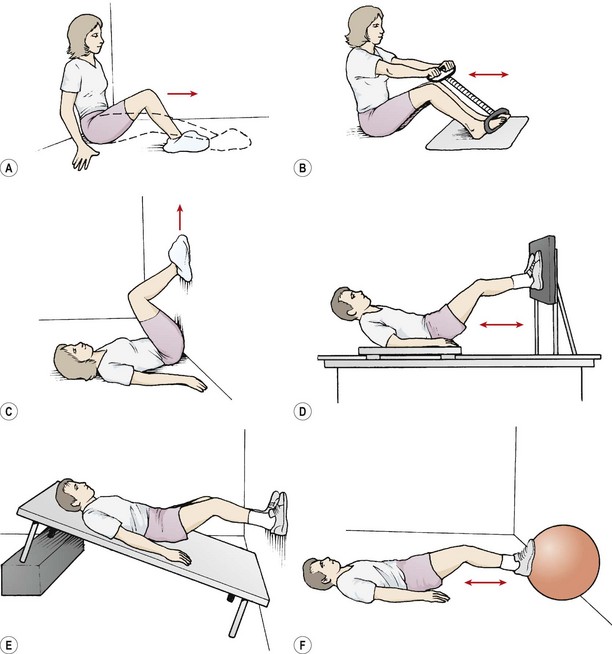
The heel slide against a wall or on the floor is useful at this stage (Fig. 9.25A). This exercise may be progressed by performing it against isometric resistance using a large diameter Swiss ball or isotonic resistance against rubber tubing. Shuttle exercises may be used on a sliding platform or low friction surface. A declined bench is useful and a linoleum surface or the ‘slide trainer’ used in popular exercise classes, both provide suitable low friction surfaces. Static cycles and step machines provide useful closed kinetic chain actions in a partial weight-bearing starting position, and will also improve cardiopulmonary fitness.
Muscle imbalance and proprioception in the ACL deficient knee
Excessive hypertrophy of the quadriceps relative to the hamstrings will lead to a muscle imbalance which will alter ACL loading (Fig. 9.26). The normal even distribution of pressure on the femoral articular surface seen with balanced musculature has been shown to change to a focused high pressure point in the absence of opposing hamstring coactivation (Baratta et al., 1988).
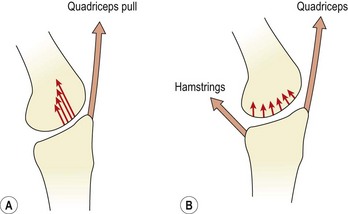
Figure 9.26 Articular surface pressure distribution with muscle co-activation. (A) Focused high pressure point at the anterior articular surface in the absence of opposing hamstring co-activation. (B) Low, evenly distributed articular surface pressure with hamstring co-activation.
After Baratta, R. et al. (1988) Muscular coactivation: the role of the antagonist musculature in maintaining knee stability. American Journal of Sports Medicine, 16, 113–122. With permission.
However, functional return is not related directly to hamstring strength, but rather to reflex contraction (Seto, Orofino and Morrissey, 1988). Co-contraction of the agonist and antagonist muscles of a joint will enhance stability. As the knee extends, the muscle spindles in the hamstrings will be stretched, leading to mild hamstring contraction (Ambrosia: Solomonow, Baratta and D’, 1989). In addition, mechanical stress on the ACL has an inhibitory effect on the quadriceps, but will simultaneously excite the hamstrings (Baratta et al., 1988). A reflex arc from the ACL mechanoreceptors may allow dynamic torque regulation during ligament loading, and mechanoreceptor stimulation from muscles and the joint capsule causes hamstring stimulation to stabilize the knee (Reid, 1992).
Both tension and mechanoreceptors are present in the ACL. Failure of the feedback system from these structures can result in a loss of reflex muscular splinting and the increased likelihood of reinjury (Kennedy, Alexander and Hayes, 1982). Normally there is a minimal, 2%, variation in the threshold to detection of passive movement (TTDPM) between the two knees. With ACL-deficient knees variation values as high as 25% have been found (Kennedy, Alexander and Hayes, 1982). The proprioceptive deficit seems to be increased at near terminal range of motion. Lephart and Fu (1995) reported longer TTDPM in the involved knee tested at 15° knee flexion, but no significant difference when tested at 45°.
Hamstring contraction of ACL-deficient patients occurs earlier in the gait cycle and is of longer duration (Kalund et al., 1990; Sinkjaer and Arendt-Nielsen, 1991). Clinically, ACL deficient patients have an increased hamstring contraction latency—the time interval between displacement of the tibia and reflex reaction of the hamstrings (Fig. 9.27). ACL-deficient patients have been found to have a mean contraction latency of 90.4 ms compared to the normal uninjured knee with a mean latency of 49.1 ms (Beard et al., 1994).
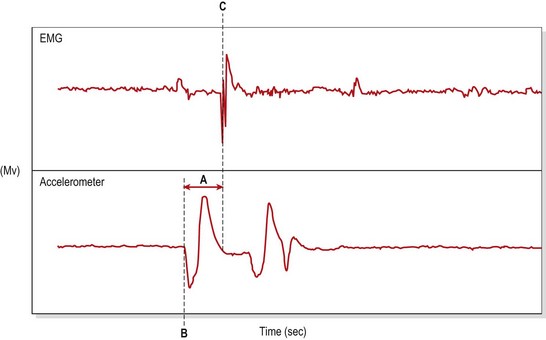
Figure 9.27 Reflex hamstring contraction latency is the time interval between the initial tibial displacement and the first measurable reaction of the hamstrings. A. Reflex hamstring contraction latency. B. First recorded displacement of the tibia (accelerometer). C. First reflex reaction of the hamstrings (EMG).
Adapted from Beard et al. (1994) with permission.
Definition
Hamstring contraction latency is the time interval between displacement of the tibia and reflex reaction of the hamstrings attempting to stabilize the knee.
Quadriceps exercises using short range (from 45° to full extension) should be preceded by isometric hip extension to facilitate hamstring contraction (Seto, Brewster and Lombardo, 1989). Indeed, the use of a standard leg extension regime using a sitting position has been severely criticized (Palmitier et al., 1991). Contraction of the quadriceps from this open chain position places considerable anterior shear on the knee and may stretch the ACL. When performing leg extension on an isokinetic dynamometer, an anti-shear device will greatly reduce shear forces generated with the exercise (Malone, 1986; Timm, 1986). When using weight training, however, closed chain motions such as the squat or leg press movement are more appropriate as they produce co-contraction of the quadriceps and hamstrings to reduce shear.
Proprioceptive exercises for the knee include three components. First, sudden alterations in joint position are employed to retrain reflex stabilization. Secondly, general posture and balance activities are used. Finally, joint-positioning skills form the basis of retraining for automatic motor control.
Definition
Proprioceptive exercises for the knee use: (i) sudden alterations in joint position, (ii) general posture and balance activities, and (iii) joint-positioning skills.
Single-leg standing activities begin the training, progressing from positions with the eyes open to those with eyes closed. These activities may be performed on an uneven surface (thick mat and then mini trampette) and later in combination with trunk and upper limb movements. Reflex hamstring contraction may be performed in crook sitting (Fig. 9.28A). A towel is placed under the patient’s heel. The patient must hold the towel in place with a sudden downward pressure (hip extension and knee flexion) as the therapist pulls on the towel suddenly. Similar actions may be performed on a low stool (Fig. 9.28B). The patient stands on the affected leg only, eyes closed. The therapist produces a very small but sudden displacement of the stool. Partner activities include single leg standing (eyes closed) with a partner suddenly pushing on the patient’s shoulders from any direction. Again, the movement, while rapid, is of small amplitude.

Figure 9.28 Rehabilitation of reflex hamstring contraction. (A) Therapist pulls towel suddenly, athlete must rapidly flex knee to stop movement. (B) Therapist minimally displaces stool suddenly, athlete must maintain balance.
Posture and coordination activities include backward walking, zig-zags, crossover drills of varying complexity and figure-of-eight running. Running on uneven surfaces and lateral step-ups are useful, as is speed walking and uphill walking. Multidirectional running skills based on the functional tests used for the knee also form part of the rehabilitation at this stage.
Accurate static joint repositioning uses cognitive skills and is helpful at various stages of rehabilitation. This may be performed by passive movement on a one-to-one basis with the therapist, or on a dynamometer which shows a display for range of motion. In each case, the patient is encouraged to reposition the joint exactly in the range that the limb rested in before movement began.
A variety of apparatus is useful for proprioceptive rehabilitation. Standard rocker boards and wobble boards, used so frequently for ankle re-education, are also of use for the knee. The ‘slide trainer’ (Forza Fitness Equipment, London) and ‘fitter’ machine (Fitter International, Calgary, Canada) are also helpful.
Proprioceptive training using balance boards has also been shown to reduce the incidence of ACL injuries in soccer players. In a study of 600 soccer players, those who included 20 minutes per day of a progressive regime of five different proprioceptive exercises (Table 9.7) had an incidence of 0.15 ACL injuries per team year compared to 1.15 in the control group (Caraffa et al., 1996).
Table 9.7 Proprioceptive training to prevent ACL injuries in soccer players
| Phase | Exercise |
|---|---|
| 1 | Single leg standing for 2.5 mins four times each day |
| 2 | Single leg training (1/2 step exercise) on a rocker board for 2.5 mins |
| 3 | Single leg training on balance board |
| 4 | Single leg training, combined rocker and balance board |
| 5 | Single leg training on BAPS board |
From Caraffa, A. et al. (1996) Prevention of anterior cruciate ligament injuries in soccer. Knee Surgery, Sports Traumatology and Arthroscopy, 4, 19–21. With permission.
Keypoint
Proprioceptive exercises used for ACL rehabilitation have also been shown to reduce the incidence of ACL injuries. They should therefore form a part of a general training programme for ‘at risk’ sports, and are used to help protect the knee from ACL injury.
The early stages of rehabilitation emphasized hamstring activity to reduce shear forces imposed on the knee. Now, any imbalance between the quadriceps and hamstring muscle groups must be corrected with both concentric and eccentric quadriceps training. Again, the emphasis is on closed chain activity, but limited open chain activity may be introduced. With all activities, the shearing stress placed on the knee must be considered (Fig. 9.29), noting that downhill running and resisted isometric quadriceps activity at 20° flexion, for example, produce the greatest ACL elongation (Henning, Lynch and Glick, 1985).
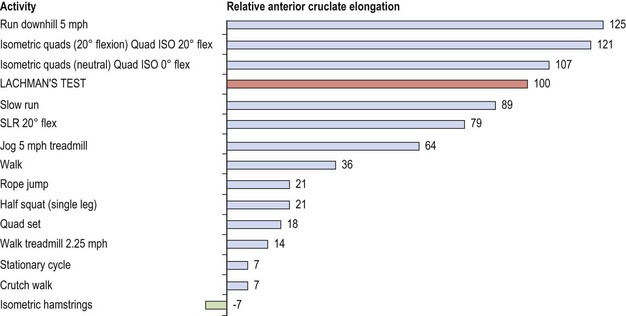
Figure 9.29 Anterior cruciate ligament (ACL) elongation relative to Lachman test (using an 80 lb pull).
After Henning, C.E. (1988) Semilunar cartilage of the knee: function and pathology. Exercise and Sport Sciences Review, 16, 67–75. With permission.
It must be remembered that following knee injury, there is a selective atrophy of type I muscle fibres, so endurance ability must be regained to ensure joint stabilization. Patients have been shown to be able to restore quadriceps strength 6 weeks after surgery (on a leg extension bench) but to still have a 20% deficit in endurance capacity (Costill, Fink and Habansky, 1977).
Neuromuscular training for knee injury prevention
Neuromuscular training (NT) has been used successfully in the prevention of knee injury. In a study of 457 floorball (indoor hockey) players followed up for 6 months, the NT group suffered 20 injuries against a control group of 52 injuries. The injury rate per 1000 hours was 0.65 and 2.08 for intervention (NT) and control group (normal sport training) respectively. The risk of non-contact leg injury was 66% lower in the NT group (Pasanen et al., 2008). This striking result confirms the importance of including training which prepares the body appropriately for sport specific actions.
Four exercise types may be used for NT in the prevention of knee injury—balance and movement control, running skills/footwork, specific strengthening and plyometrics (Table 9.8). The emphasis is on correct movement and alignment. For example during knee flexion actions such as lunges, squats and jumps the knee should pass over the centre of the foot rather than in inner aspect. Jumps should encourage shock absorption through the foot, knee and hip and should not be performed stiff legged. The hip hinge action is emphasized when angling the body forwards rather than lumbar flexion alone. Where movements are limited by flexibility issues (hamstring tightness in forward bending for example) stretching is used in parallel with movement re-education. Training is periodized. The total training period for NT is 20−30 minutes 2 or 3 times per week during the non-competitive season, and a single weekly maintenance period is used during the competitive season.

The squat exercise in knee rehabilitation
The squat is a controversial exercise in both rehabilitation and general training. Generally, the parallel squat (to a point where the femur is horizontal) rather than the full squat (buttock to heel) is recommended (Baechle, 1994), as it is claimed that less stress is placed on the knee using the reduced range of motion. When performing this exercise, less skilled individuals have been shown to produce a large initial drop velocity, to bounce in the low position, and to lean the trunk forwards while pushing the hips back (McLaughlin, Lardner and Dillman, 1979). This trunk angulation increases the leverage forces imposed on the lower back (Norris, 1993). The more skilled individual, by limiting trunk extension, places more stress on the quadriceps and reduces the leverage effect on the lower spine.
The squat has the advantage of being a closed chain activity, but is often said to ‘overstretch the knee ligaments’ and so is frequently derided. The squat has been shown to work the quadriceps, but significant co-contraction of the hamstrings has been questioned (Gryzlo et al., 1994). Heavy resistance squatting (130–200% bodyweight) used over a 21-week training period has not been shown to increase knee laxity (Panariello, Backus and Parker, 1994). Ligament stability was assessed in 32 professional football players using an arthrometer at 30° and 90° flexion after 12 and 21 weeks. Treatment note 9.1 details teaching points for the squat.
Treatment note 9.1 The squat exercise
Table 9.9 details common errors when performing a squat. They broadly fall into two categories: (i) lower limb alignment and (ii) lumbopelvic alignment. The foot should be turned out slightly (Fick angle) by about 15°.
Table 9.9 Common errors when performing a squat
| Error | Technique modification |
|---|---|
| Knees move inwards (knock knee) | Foot may be flattening too much (pronation). Wear more supporting shoes and practise the movement in front of a mirror. Aim to keep the knee over the foot. |
| Knees stay behind feet throughout movement | Ankle forward bending (dorsiflexion) may be limited. Place a 1–2 cm wooden block beneath the heels. Squat onto a bench without a weight and practise pressing the knee forwards. |
| Back angles too far forward | Keep the spine more vertical and monitor your posture by standing side on to a mirror. |
| Spine flexes between the shoulders (thoracic region) | Press the breastbone (sternum) forwards and draw the shoulder blades (scapulae) down and in using a bracing action. |
| Low back hollows excessively (increased lumbar lordosis) | Tighten the abdominal muscles and hold them tight throughout the movement. Practise hip flexor muscle stretching. |
| Heel lift | Position the squat in front of a mirror and use a horizontal line drawn on the mirror to line up the bar. |
| Bar dips to one side | Practise the squat in front of a mirror and use a horizontal line drawn on the mirror to line up the bar. |
| Bouncing in the low position | Practise squatting onto a bench and gradually lower the weight into the final position. |
From Norris, C.M. (2003) Bodytoning, A&C Black, Oxford.
Keypoint
The Fick angle is formed by the long axis of the foot (2nd toe to mid heel), relative to the sagittal axis of the body. Normal range is 5−18°.
As the knee bends the patella should face forwards and outwards slightly, but not pull inwards (knock knee) or outwards (bow legged) excessively. To check this position, ensure that the knee moves over the centre of the foot and not over the outer or inner edge. The spine should stay relatively upright and straight. There is often a tendency to angle forwards as the weight is lowered and extend the spine as the weight is lifted (Fig. 9.30). Where this happens the weight is generally too heavy and the spinal extensor muscles are being used excessively.


The knee should pass over the foot, showing that the ankle has dorsiflexed. Where the ankle is stiff, the shin may remain vertical. To maintain the line of gravity through the base of support the individual will be forced to angle the trunk forwards. This situation is corrected by placing a block beneath the heels.
In some individuals the trunk may lose alignment either flexing at the lumbar (Fig. 9.31) or thoracic (Fig. 9.32) spine or hyperextending at the lumbar spine, a position accompanied by anterior pelvic tilt (Fig. 9.33).




Keypoint
A squat exercise, used correctly, will not overstretch the knee ligaments. It is a functional closed chain movement which, as well as working the knee, rehearses good lifting technique.
Knee stiffness
Knee stiffness is a common problem following ACL surgery. There are a variety of possible causes, including adhesions within the suprapatellar pouch and/or patellofemoral joint, quadriceps contracture and retraction of the alar folds (Reid, 1992). Furthermore, patients have been described with an involvement of the infrapatellar fat pads, producing infrapatellar contracture syndrome (Paulos, Rosenberg and Drawbert, 1987).
Initially, stiffness begins with inflammation, immobility and quadriceps weakness. Patients are unable to gain full extension and may complain of excessive pain. Patellar glide is restricted and pain may be located around the patellofemoral joint. Later, fat pad involvement may be noted and the patellar tendon may become rigid. Patellar mobility is virtually eliminated and both active and passive knee motion is severely restricted. Flexion contracture is often present by this time and the patient walks with an apparent ‘short leg’.
If progress in regaining knee mobility begins to slow, this must be recognized immediately and acted upon. Intense rehabilitation is the key to preventing development of this condition. Patellofemoral joint mobilization and the restoration of full knee extension is vital.
Posterior cruciate damage
The PCL is the strongest ligament in the knee (Baylis and Rzonca, 1988) and is much less frequently damaged in sport than the ACL. When an injury does occur, it may be the result of a posteriorly directed force onto a flexed knee (typically a road traffic accident), forced hyperextension, or forced flexion where the athlete falls into a kneeling position, pressing the ankle into plantarflexion (Keene, 1990). Unlike ACL injury, the athlete with a damaged PCL can usually continue playing and may only notice minimal swelling, but there is marked pain on the posterior aspect of the knee.
Posterior subluxation of the tibia often occurs during walking and standing. It may be seen clinically from the side if the knee is flexed to 90° (Fig. 9.34). This may be accentuated if the patient contracts the quadriceps against a resistance provided by the examiner. The patient is asked to ‘slide the foot down the couch’ (Daniel et al., 1988) as the examiner stabilizes the ankle. If not viewed from the side, the subluxation may be missed and the injury wrongly diagnosed as an ACL tear, the tibia moving forwards to reduce and mimicking an anterior drawer sign.
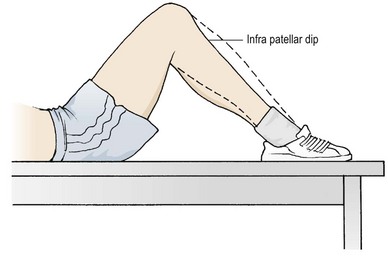
The posterior shift of the tibia moves the patellar tendon closer to the axis of rotation of the knee, reducing the mechanical advantage of the quadriceps (Fig. 9.35). The change in quadriceps muscle efficiency is reflected in the gait cycle. With the PCL deficient knee, athletes demonstrate quadriceps activity before heel strike, in contrast to normal individuals who show this contraction after heel strike (Reid, 1992).
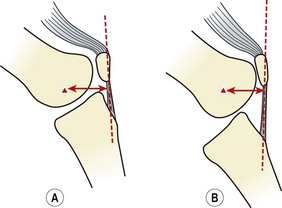
Figure 9.35 Alteration in mechanical advantage of the knee following posterior cruciate ligament (PCL) rupture. (A) Normal knee: axis of rotation to patellar tendon distance gives mechanical advantage. (B) PCL deficient knee: tibial shift gives reduced mechanical advantage.
Rehabilitation
As with ACL damage, conservative treatment involving intensive muscle strengthening is tried first. Isolated hamstring contractions will cause posterior shear of the tibia on the femur and so should be avoided. In addition, excessive external rotation of the tibia as the knee approaches full extension will stress the repaired tissue. As with ACL rehabilitation, co-contraction exercises should be favoured, with a greater emphasis on quadriceps rather than hamstring contractions where isolation movements are used.
The PCL is contained within a synovial sheath which enhances its ability to heal in continuity (Fowler and Messieh, 1987). Reconstruction may be attempted using a similar patellar tendon graft to that described above. This time, the graft is positioned lateral to the tibial attachment of the PCL and travels through the femur at the junction of the medial condyle and the intercondylar notch.
The knee with isolated PCL insufficiency producing unidirectional instability generally does well when treated conservatively, but when PCL damage is associated with additional tissue damage which results in multidirectional instability, surgery should be considered (Torg, 1989). In a study investigating the long-term effects of non-operative management of PCL damage, Parolie and Bergfeld (1986) assessed 25 athletes on average 6.2 years after injury. Of these, 84% had returned to their previous sport. Importantly, those who were not satisfied with their knee had less than 100% strength compared to the undamaged knee (measured as mean torque on an isokinetic dynamometer at varying angular velocities), and those who were satisfied had strength values greater than 100%. The importance of maintaining superior muscle strength following PCL injuries is therefore clear. Shelbourne et al. (1999) found that half of all patients treated non-operatively returned to the same sport at the same or even higher levels of activity. Those with greater PCL laxity do not generally have lower functional rating scores (Shelbourne and Muthukaruppan, 2005). The same authors found that even after long-term follow-up (7.8 years) 16% of patients were still improving and 40% scored excellent, 10% good and 6% fair measured on the Noyes knee survey.
Of those patients who are symptomatic enough to seek treatment, damage to the medial compartment is more common with chronic injuries, and to the lateral compartment with acute injuries (Geissler and Whipple, 1993). Damage includes meniscal tears and articular cartilage defects.
Functional testing of the cruciate ligament deficient knee
Functional testing may be used to assess stability, pain and confidence in the knee. Tests normally aim to reproduce some key aspect of a sport to enhance specificity. In each case the injured and uninjured sides of the body are compared.
For the crossover test the athlete stands on the affected leg and uses the unaffected leg to step in front and behind the injured one, imparting multiplane stress on the knee (Fig. 9.36). The test may also be performed with the injured leg on a small stool to increase flexion stress on the knee.
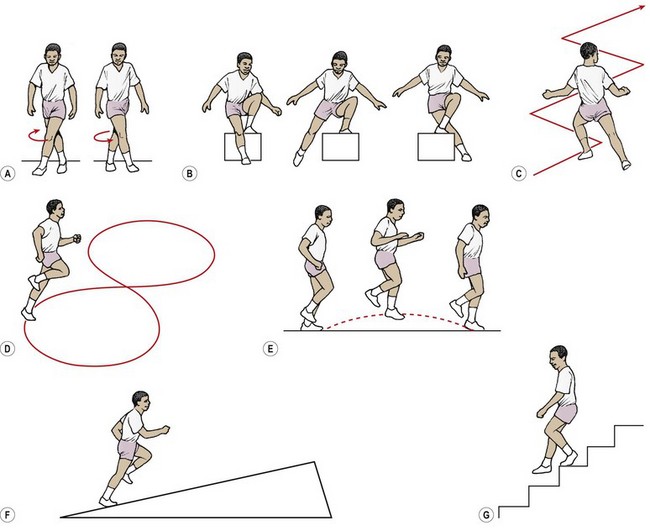
Figure 9.36 Functional testing of the knee. (A) Crossover. (B) Crossover on box. (C) Zig-zag. (D) Figure-of-eight. (E) Single leg hop. (F) Slope running. (G) Ascending and descending stairs.
The single-leg hop test measures the distance obtained on the injured side and divides this figure by that obtained for the uninjured side to obtain a ‘hop ratio’ which may be recorded throughout treatment (Reid, 1992). Combining straight hopping with hop-and-turn activities increases and varies the stress imposed on the knee, as does hopping down or up from a low stool.
Figure-of-eight, slalom and slope/stair running circuits are also useful. The figure-of-eight may be performed with a gradual curve or a sharp one to impose more or less stress on the knee. The knee on the outside of the circle is exposed to a varus stress as the body leans inwards. The slalom or zig-zag run imposes sudden direction changes and shear on the knee. This test is particularly suitable for assessing function in sports which involve ‘cutting’ actions. Slope/stair running may be performed on an inclined or declined surface, or on a camber. In each case repetitive shearing stress is imposed on the knee.
The menisci
The menisci are fibrocartilage structures which rest on the tibial condyles. They are crescent-shaped when viewed from above, but triangular in cross-section. Their peripheral border is formed from fibrous tissue and attached to the deep surface of the joint capsule. These same fibres attach the menisci to the tibial surface, forming the coronary ligaments. Anteriorly, the two menisci are joined by the transverse ligament, a posterior transverse ligament being present in 20% of the population (Palastanga, Field and Soames, 1989).
The medial meniscus is the larger of the two, semicircular in shape, and broader posteriorly. Its anterior horn is attached to the front of the intercondylar area of the tibia in front of the ACL. The posterior horn attaches to the posterior intercondylar area between the PCL and the lateral meniscus. It has an attachment to the MCL and the oblique popliteal ligament coming from semimembranosus (Fig. 9.37A). The upper part of the meniscus is firmly attached to the MCL, the fibres here forming the medial meniscofemoral ligament (Fig. 9.37B). The lower part, attached to the coronary ligament, is more lax. This has important functional consequences because the medial meniscus is anchored more firmly to the femur than to the tibia. In flexion/extension the femur is thus able to glide on the tibia, while in rotation, the meniscus can slide over the tibial plateau (Evans, 1986).
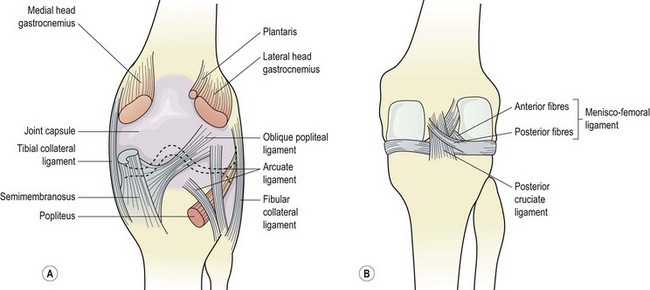
The lateral meniscus is more circular, and has a uniform breadth. Its two horns are attached close together, the anterior horn blending with the attachment of the ACL. The posterior horn attaches just anterior to the posterior horn of the medial meniscus. The meniscus has a posterolateral groove which receives the popliteus tendon, and a few fibres from this muscle attach to the meniscus itself. In addition, the tendon of popliteus partially separates the lateral meniscus from the joint capsule, a configuration which makes the lateral meniscus more mobile than its medial counterpart. The posterior part of the lateral meniscus has two ligamentous attachments, the anterior and posterior meniscofemoral ligaments (Fig. 9.38). These divide around the PCL, and in extreme flexion, as the PCL tightens, so do the anterior and posterior meniscofemoral ligaments. The lateral meniscus is thus pulled back and medially.
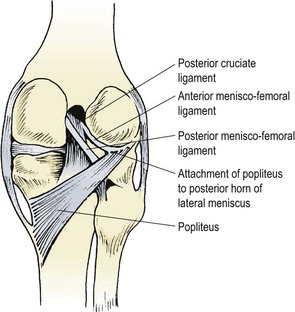
Keypoint
Because the lateral meniscus attaches through the meniscofemoral ligaments to the posterior cruciate, it is more mobile than the medial meniscus and so less likely to be trapped and torn.
The menisci receive blood flow from the inferior genicular arteries which supply the perimeniscal plexus (Fig. 9.39). Small penetrating branches from this plexus enter the meniscus via the coronary ligaments. Up until the age of about 11 years, the whole meniscus has a blood supply, but in the adult only 10–25% of the periphery of the meniscus is vascular. The anterior and posterior horns are covered by vascular synovium and have a good blood supply (Arnoczky and Warren, 1983). The peripheral vessels are within the deeper cartilage substance, the surface receiving its main nutrition via diffusion from the synovial fluid. A few myelinated and non-myelinated nerve fibres are found in the outer third of the menisci, but no nerve endings.
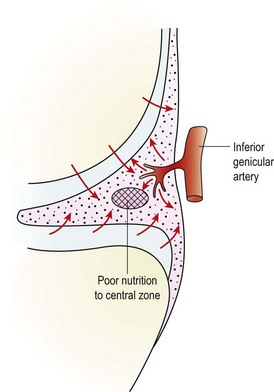
Because the menisci are held more firmly centrally, they are able to alter their shape and move forwards and backwards over the tibial plateau. The lateral meniscus has a greater amount of movement, and is often ‘pulled away from trouble’, leaving the medial meniscus to be more commonly injured in association with the MCL and ACL, to which it has attachments.
In flexion, the lateral meniscus is carried backwards, onto the steep posterior slope of the lateral tibial plateau, and with extension, it moves forwards again. In flexion/extension the medial meniscus is held firm until the last 20° of extension when the knee begins to rotate (screw home mechanism). As this happens, the medial meniscus is carried backwards. The lateral meniscus has the greater movement therefore—approximately 11 mm versus only 5 mm for the medial (Reid, 1992). In extension, the menisci are squeezed and elongated in an anteroposterior direction, and in flexion they become wider (Fig. 9.40).
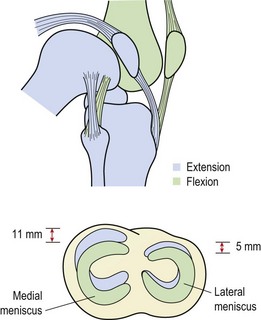
The menisci enlarge the tibiofemoral contact area, thus spreading the pressure taken by the subchondral bone (Fig. 9.41). It has been estimated that the menisci disperse between 30% and 55% of the load across the knee (Kelley, 1990). When only a portion of the meniscus is removed, the joint surface contact forces may increase by 350% (Seedhom and Hargreaves, 1979).
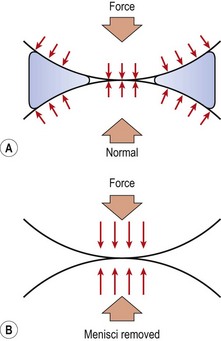
Figure 9.41 The effect of cartilage removal (meniscectomy) on the knee. (A) Forces on the normal knee. (B) Menisci removed. The bones take more jarring strain.
The menisci contribute substantially to knee stability. In the ACL deficient knee, the anterior drawer test may be positive in only 35% of knees with an intact medial meniscus, but in 83% when the meniscus is removed (Levy, Torzilli and Warren, 1982). The menisci limit sagittal gliding of the femur over the tibial plateau, a movement greatly increased in patients who have undergone meniscectomy. In addition, they allow a dual movement to occur, normally only possible in joints which are far more lax. The menisci also aid joint lubrication by spreading the synovial fluid over the surface of the articular cartilage.
Keypoint
When a portion of the meniscus is removed, the joint surface contact forces may increase by 350%. Following menisectomy bone adaptation will take time, and weightbearing should be progressed slowly. Shock absorbing padding should be used in all sports footwear.
Injury
It has been estimated that meniscal injury has a frequency of 61 per 100 000 individuals. The condition is three times more prevalent in males than females, with the medial meniscus being injured four times as often as the lateral (Kelley, 1990).
With ageing, degeneration and asymptomatic tearing occurs. Noble and Hamblen (1975) examined 400 cadaveric menisci and found 29% to have horizontal cleavage tears, and 60% to have a significant meniscal lesion of some sort.
In the active athlete, the history of injury is usually one which combines twisting on a semi-flexed knee with the foot fixed on the ground. The onset is sudden, and pain is felt deep within the knee, the patient often saying they ‘felt something go’. Effusion may be extensive after injury, and haemarthrosis may result if the injury occurs in combination with ACL or MCL damage. Tears may be to the periphery or body of the meniscus, running horizontally or vertically (Fig. 9.42). A longitudinal tear (bucket handle) of the medial meniscus may allow its lateral portion to slip over the dome of the medial femoral condyle causing blocked extension (true locking). Shakespeare and Rigby (1983) reviewed 272 patients found to have bucket handle tears at operation. Of these, 43% presented with true locking. When the knee unlocks, either spontaneously or through manipulation, anterior extension of the bucket handle tear, rather than meniscal relocation, may occur (Reid, 1992).
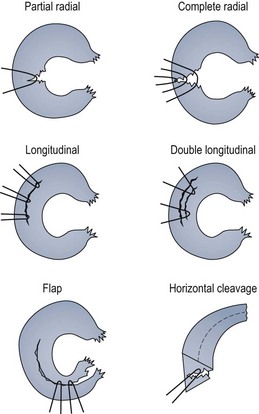
Figure 9.42 Common meniscal tears. The longitudinal tear may extend anteriorly to form a bucket-handle tear.
From Zuluaga, Briggs and Carlisle (1995), with permission.
On examination, effusion is apparent and tenderness is often found over the joint line, most usually medially. A capsular pattern may be noticeable (see Table 1.9), and terminal extension is often blocked with a springy end-feel if muscle spasm is not present. Various tests are used to assess the problem, of which the two most common are McMurray’s and Apley’s.
McMurray’s test (Fig. 9.43A) requires full flexion of the knee and so is not suitable for the acute joint. The medial joint line is palpated and from the fully flexed position the knee is externally rotated and extended, as a slight varus strain is applied. If positive, a painful click or thud is felt over the medial meniscus. The lateral meniscus can be similarly tested by extending the knee with internal rotation and a valgus strain, although the value of lateral testing in this way is questionable (see below). In each case only the middle and posterior portion of the meniscus is tested, and so a negative McMurray’s sign does not preclude meniscal damage, but when positive the test is clinically revealing.
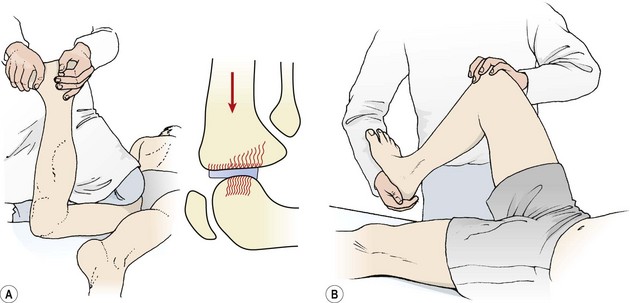
The McMurray’s test has been shown to be useful only with medial meniscal tears (Evans, Bell and Frank, 1993). In this evaluation the authors found that a thud elicited on the medial joint line was the only significant sign to correlate with meniscal injury. They showed the test to have a positive predictive value of 83% and a specificity of 98%.
Apley’s grinding test (Fig. 9.43B) involves placing the patient in a prone-lying position, flexing the knee to 90°, rotating the tibia and compressing it against the femur in an attempt to elicit a popping or snapping sensation. It is important not to force the movements too far, as this may further tear the already damaged meniscus (Garrick and Webb, 1990). The intention with this test is to help differentiate between meniscal and MCL damage at the joint line. Symptoms will be present as the knee is compressed when the meniscus is damaged but not if the MCL alone is injured, because this structure will be relaxed by the compression force (Apley and Solomon, 1989). Conversely, a distraction force stretches the ligament but disengages the meniscus, so giving pain where MCL damage has occurred in isolation.
The results of meniscal tests combined with the clinical history will indicate if damage is likely, in which case arthroscopy is called for to confirm the findings.
Management
If a meniscal tear is present, the choice is either non-operative management or surgical intervention involving removal or repair of the injured meniscus.
Non-operative management
Henning (1988) argued that meniscal tears of less than 10 mm in length and partial thickness injuries involving 50% or less of the vertical height of the meniscus could be treated non-operatively, providing the ACL was undamaged. Weiss et al. (1989) reported that stable vertical longitudinal tears in the vascular outer area of the meniscus had a good potential for healing, whereas stable radial tears did not. They performed a repeat arthroscopy on 32 patients (on average 26 months after the first procedure), and found that 17 longitudinal tears had healed completely. Five radial tears showed no evidence of healing and one had extended. No degenerative changes were found in the adjacent articular cartilage of the stable lesions.
Meniscal repair
The peripheral part of the meniscus has a blood supply sufficient to support healing. Initial healing in this region is by fibrosis with vessels from the capillary plexus and synovial fringe penetrating the area. Fibrous healing may be complete within 10 weeks, and the scar tissue can be remodelled into normal fibrocartilage within several months (Hammesfahr, 1989). The mid-portion of the meniscus is avascular and has been traditionally thought not to heal. However, Arnoczky and Warren (1983) demonstrated healing in canine tissue by cutting an access channel from the peripheral region to the mid-point of the meniscus. The peripheral vessels proliferated through the channel into the lesion, giving fibrovascular scarring throughout both areas.
The peripheral tear may be sutured, and healing improved by abrading the parameniscal synovium. Henning (1988) argued that healing may be further enhanced by injecting an exogenous blood clot into the injury site. Results are good when repair is limited to the vascular area of the meniscus and to vertical tears (Ryu and Dunbar, 1988). Weight bearing or full range motion will deform the menisci and so pull on the scar site. For this reason rehabilitation of the repaired meniscus is much less intense than that of a patient who has undergone meniscectomy. General recommendations for rehabilitation (DeHaven and Bronstein, 1995) include the restriction of weight bearing for 6 weeks, with no flexion allowed for the first 2 weeks. After 2 weeks, 20–70° flexion is allowed, with free motion allowed 4 weeks after surgery. Full weight bearing is allowed, and resistance exercises are progressed. Return to full sports is not permitted for 6 weeks.
For successful repair, DeHaven and Bronstein (1995) produced a number of recommendations. First, that the tear should lie within 3 mm of the meniscosynovial junction and that the overall contour of the meniscus should be normal. In addition, these authors stated that the tear should be at least 7 mm long and making the meniscus unstable. For tears further than 4 mm from the meniscosynovial junction and those with deformity, healing enhancement using fibrin clot was recommended. In general tears greater than 3 cm and transverse tears do not heal. Repair is either from the outside or inside of the meniscus. The ‘outside in’ procedure uses needles passed through the joint capsule, but placement of sutures is less precise. The ‘inside out’ procedure uses sutures placed arthroscopically from inside the knee.
DeHaven, Black and Griffiths (1989) reported follow-up results on 80 repaired menisci on average 4.6 years after surgery. Of these, 11% had torn again (only three at the repair zone), and these authors recommended meniscal repair in view of the degenerative changes following meniscectomy.
Meniscectomy
The preceding descriptions of non-operative management and meniscal repair make it apparent that meniscectomy is not the first choice in many cases of meniscal tearing.
Degenerative changes which have been described after total meniscectomy include joint narrowing, ridging and flattening (Fairbank, 1948). Follow-up after meniscectomy (Jorgensen, Sonne-Holm and Lauridsen, 1987) has shown patients to be increasingly dissatisfied with the knee. Incidence of complaint grew from 53% after 4.5 years to 67% after 14.5 years. A positive anterior draw sign was demonstrated in 10% after 4.5 years and 36% after 14.5 years, with 34% of the latter group giving up sport as a result of knee symptoms (Table 9.10).
Table 9.10 Follow-up after complete meniscectomy
| 4.5 years(n 5 131)% | 14.5 years(n 5 101)% | |
|---|---|---|
| Symptoms | ||
| Swelling | 19 | 29 |
| Pain | ||
| Weight-bearing | 38 | 30 |
| On stairs | 15 | 23 |
| When first walking | – | 23 |
| At rest | 12 | 13 |
| Sensation of instability | 20 | 21 |
| Signs | ||
| Crepitus | 18 | 38 |
| Quadriceps wasting | 7 | 12 |
| Positive anterior drawer | 10 | 36 |
| Joint line tenderness | 10 | 12 |
| Activity | ||
| Unchanged | 53 | 19 |
| Reduced because of knee | 12 | 12 |
| No sport because of knee | 15 | 34 |
After Jorgensen, U. et al. (1987) Long term follow up of meniscectomy in athletes: a prospective longitudinal study. Journal of Bone and Joint Surgery, 69, 80. With permission.
Where the meniscus is grossly damaged and the knee is unstable, however, a partial or total meniscectomy may be required. The minimum amount of tissue should be removed to reduce the biomechanical impairment to the joint.
The traditional method for meniscectomy (Donoghue: O’, 1976) is with the patient supine, knee flexed to 90° over the table end. For a medial meniscectomy a straight incision is often used, starting proximal to the lower pole of the patella and medial to the patellar tendon, and stretching parallel to the tendon. The retinaculum is split and the joint washed out (lavaged) with warm saline to remove any blood. The whole cartilage may be visible if the knee can be sprung open medially, but usually only palpation with forceps is possible. The bony attachment of the meniscus is dissected and the meniscus itself removed.
Arthroscopic removal of all, or part, of the meniscus is commonplace nowadays. An anterolateral or anteromedial approach may be taken, depending on which compartment of the knee the lesion lies in. The knee is held in 10° flexion and the joint is gapped by applying a valgus or varus stress. The joint is distended with fluid to allow easier inspection of the tissue surfaces. An initial incision is made into the anterior part of the meniscus, and the incision is then extended into the middle and posterior segments. The posterior horn is released, followed by the anterior horn, and the meniscus is removed. In cases where only part of the meniscus is removed, the edge of the remaining tissue is trimmed.
Results of arthroscopic partial meniscectomy are generally good, but are dependent on the amount of tissue damage which occurred at the time of injury. Investigating 67 patients on average 12.2 years after arthroscopic partial meniscectomy, Higuchi, Kimura and Shirakura (2000) found 79% to have a satisfactory outcome (52% excellent, 27% good, 10.5% fair). Osteoarthritic deterioration was noticed in 48% of patients the amount being dependent on the amount of cartilage degeneration noticed at the time of surgery. Of the original group, 39 had normal knee cartilage, and 28 had articular degeneration.
Arthroscopy, although commonplace, is not without risk of complication. The Committee on Complications of Arthroscopy of North America (1985) found a 0.8% complication rate in over 100 000 procedures, while Sherman et al. (1986) reported a complication rate of 8.2%. Neurological injury, poor wound healing, instrument breakage, intra-articular infection, knee ligament injury and pulmonary embolism resulting in death have all occurred. The patient’s age and the length of time that a tourniquet is used have been found to be the most significant factors in predicting problems (Sherman et al., 1986).
The use of arthroscopy with local anaesthesia is steadily increasing (Ngo et al., 1985; Besser and Stahl, 1986; Buckley, Hood and Macrae, 1989), and obviously removes the risk inherent in any procedure involving a general anaesthetic. In addition, complication rate is lessened, cost is reduced and the patient is discharged significantly earlier than when general anaesthesia is used. The skin puncture sites are injected with lidocaine (lignocaine) or similar, and the joint is distended with saline and anaesthetic solution. Studying 400 patients in total, Jacobson, Forssblad and Rosenberg (2000) compared results from elective knee arthroscopy using either local, general or spinal anaesthesia and obtained a 92% success rate using local anaesthesia in 200 of the patients. They concluded that the use of local anaesthesia was superior to either spinal or general anaesthetic in this group.
Following meniscectomy of any type, the initial aim is to limit effusion and pain (Table 9.11). As this is achieved, the leg musculature is progressively built up. Initially, open chain movements are used within the pain-free range, to protect the joint from excessive loading. Range of motion is gradually increased, and as this is achieved, closed chain movements are introduced. Functional activities and power training are used in late stage rehabilitation, with sports specific progressions forming the mainstay of pre-competitive work.
Table 9.11 Guidelines for post-meniscectomy rehabilitation
| Initial stage (0–2 weeks) |
| Intermediate stage (2–4 weeks) |
| Late stage (4–6 weeks)* |
| Pre-competition testing |
* Progress to late stage when no/minimal swelling is present and full range motion obtained. After Zuluaga, Briggs and Carlisle (1995) and Reid (1992).
Meniscal cysts and discoid meniscus
The discoid meniscus (Fig. 9.44) is more usually seen on the lateral side than the medial. Even so, the condition is unusual. Smillie (1974) reported a total of 467 discoid lateral menisci (and only seven medial) in 10 000 meniscectomies. In the fetus, the meniscus is disc shaped rather than semi-lunar. When this shape remains later in life, the discoid meniscus is said to be present.
Figure 9.44 Meniscal abnormalities. (A) Normal. (B) Partial discoid. (C) Complete discoid. (D) Cyst.
Definition
The meniscus of the knee in an unborn child is disc shaped rather than moon shaped. When this shape remains later in life, a discoid meniscus is present.
Discoid menisci may be classified as complete, incomplete (partial) or Wrisberg type (DeHaven and Bronstein, 1995). In the latter type the posterior osseous attachment of the meniscus is absent, leaving it attached only by the meniscofemoral ligament (Wrisberg’s ligament).
The abnormal shape of the meniscus subtly alters both the contact area between the tibia and femur and joint mobility. In the young, the discoid meniscus may be asymptomatic, with 65% of those who present with symptoms being over 18 years old (Reid, 1992). A clunk may be felt in the knee at 110° as it is bent, and at 10° as it is straightened again (Apley and Solomon, 1993). Surgical treatment may be by meniscectomy or repair.
Meniscal cysts (ganglia) are again more common in the lateral meniscus, with the posterior and mid-portion of the meniscus being affected. The cyst is associated with a horizontal tear, and may be the result of infiltration of synovial fluid through the tear, with the edge of the tear acting as a one-way valve (Barrie, 1979). In a series of 18 patients with MRI documented cysts, all were found to have horizontal cleavage tears at arthroscopy (Ryu and Ting, 1993).
The cyst generally begins as a small pedicle and gradually enlarges, the size fluctuating with varying activities. It is more easily seen with the knee flexed to 45°. Arthroscopic repair of the tear site is possible, allowing the cyst to decompress into the joint (DeHaven and Bronstein, 1995). Where no tear is identified, removal of the cyst is attempted. The meniscal rim is scarified and the perimeniscal tissue reattached, leaving the meniscus proper fully intact. Some cysts respond to direct aspiration (Reid, 1992).
Jumper’s knee
Jumper’s knee is traditionally described as a patellofemoral pain syndrome (PFPS) affecting the teno-osseous junctions of the quadriceps tendon as it attaches to the superior pole of the patella, and the patellar tendon as it attaches to the inferior pole of the patella and tibial tuberosity. It is, therefore, an insertional tendinopathy resulting in derangement of the bone–tendon unit (Colosimo and Bassett, 1990).
Definition
Jumper’s knee is patellar pain traditionally described as affecting the insertion of the patellar tendon into either the patella itself or the tibial tuberosity. Histologically it is a tendinopathy of the patellar tendon.
Jumper’s knee occurs more frequently in athletes who regularly impose rapid eccentric loading (traction) on the extensor mechanism of the knee, especially on hard surfaces. The condition affects the inferior pole of the patella in 80% of cases and is most common at this site in athletes over 40 years of age. The insertion of the quadriceps is more commonly affected in the over 40s, and the tibial tuberosity is the most common sight for jumper’s knee in children (David, 1989).
Repetitive stress on the T/O junction causes microtearing over time, and an insidious onset of pain. The condition progresses in a series of stages. Initially, pain is experienced only after intense activity, as a well-localized dull ache without a history of trauma. With time, pain occurs at the onset of activity and disappears when the athlete is warmed up, only to reappear when sport has finished. Eventually, pain is constant, with consequent impairment of performance, and as a final but rare scenario, the tendon may rupture completely.
On examination, quadriceps wasting is apparent in long-standing cases and pain occurs to resisted extension, with slight soreness to full passive flexion. Some swelling may be noticed around the patellar tendon in acute cases, with fluctuance present if the condition is severe. A non-capsular pattern is found.
Palpation is performed with the knee in full extension to relax the patellar tendon. Palpation to the lower pole of the patella is best performed by pressing with the flat of the hand onto the upper surface of the patella to tilt it. This brings the lower pole into prominence and enables the practitioner to reach the part of the T/O junction which lies on the undersurface of the angular lower pole.
Radiographic changes are usually apparent where symptoms have been present for more than 6 months (Colosimo and Bassett, 1990). An elongation of the involved pole of the patella may be seen, with calcification of the affected tendon matrix. Bone scan has indicated increased blood pooling and concentration of radioactive tracer in the affected area (Kahn and Wilson, 1987).
Aetiology
Both intrinsic and extrinsic factors have been implicated as possible causes. Intrinsic factors include biomechanical alterations in the extensor mechanism, such as hypermobility, altered Q angle and genu valgum or genu recurvatum. Changes in the HQ ratio and hamstring flexibility may also have a part to play and should be examined. Muscle imbalance, consisting of weakness of the glutei, hamstrings and abdominals, combined with hip flexor shortening, has been noted (Sommer, 1988). In addition, on landing, players who are susceptible to this condition, have a greater tendency to adduct the knee and internally rotate the leg (knock-knee posture).
Extrinsic factors include frequency and intensity of training, training surface and footwear. Ferretti (1986) showed a correlation between jumper’s knee and both hardness of playing surface and training frequency. In his study, 37% of players (matched for sport, playing position, and training type) using cement surfaces suffered from the condition, compared to only 5% of those using softer surfaces (Fig. 9.45A). In addition, the percentage number of players affected by the condition escalated as the number of training sessions per week increased. Only 3.2% of those with the condition trained twice each week, whereas nearly 42% trained four times or over (Fig. 9.45B).
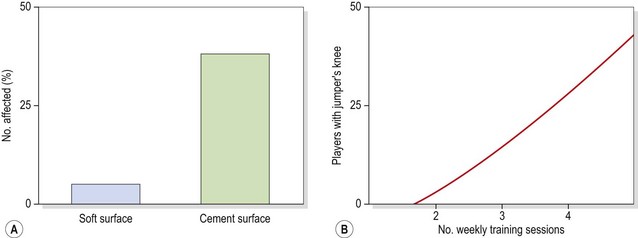
Pathological tendon changes
Four main pathological features are present in patella tendinopathy, affecting the tendon collagen, ground substance, cells and blood vessels (Table 9.12). The affected region of the patella tendon demonstrates mucoid degeneration, being a dull brownish tissue rather than the white glistening appearance characteristic of normal tendon tissue. Instead of the parallel fibres of healthy tendon, pathological tendon demonstrates disorganized fibre arrangement with microtearing, some necrotic fibres and vascular ingrowth which can be visualized on Doppler ultrasound.
Table 9.12 Main pathological features of patellar tendinopathy
| Feature | Characteristic |
|---|---|
|
Transverse disruption of collagen fibres and separation of bundles, leading to reduction of cross-links and weakening
|
From Cook et al. (2001).
Keypoint
Mucoid degeneration is a biological degrading of connective tissue into a gelatinous mucus-like substance.
Studies have shown an increased number of mast cells in patella tendinosis. Normal tissue showed 1.0 cells/mm2 and pathological tendon showed a threefold increase in cell numbers at 3.35 cells/mm2. In addition mast cell number was correlated to symptom duration with longer term conditions showing greater cell number. Increased vascular area was measured as 2.81% compared to a normal value of 1.2% in control subjects (Scott et al., 2008). The presence of mast cells is important as they release profibrotic factors including transforming growth factor (TGF) and interleukin-1 and -4. In addition mast cells interact with tenocytes causing tendon modification.
Management
As with any overuse syndrome, part of the management of the condition involves avoidance or modification of training. Athletes should be encouraged to warm up adequately, and practise flexibility exercises to both the quadriceps and hamstrings. Strength must be developed symmetrically, and footwear should incorporate shock-absorbing materials.
In the early stages of the condition these modifications, combined with ice application when pain is acute, are usually sufficient. Later, transverse frictional massage can be effective at relieving pain. Frictions to the T/O junction attaching to the patella (infrapatellar tendon) are performed with the patella tilted and pressure from the therapist’s finger is directed at a 45° angle to the long axis of the femur rather than straight down. Deep tissue mobilization of this type has been shown to be beneficial in the treatment of tendon pathology in the rat model. Increased fibroblast recruitment has been demonstrated following 3 minutes of soft tissue mobilization over four treatments (Davidson et al., 1997). Use of heavy pressure during soft tissue mobilization has been shown to significantly increase the fibroblast number compared to light pressure (Gehlsen, Ganion and Helfst, 1999).
Keypoint
Frictions to the teno-osseous (T/O) junction of the patella tendon are only effective if the patella is tilted. Pressure from the therapist’s finger is directed at a 45° angle to the long axis of the femur rather than straight down.
In chronic conditions, where scar tissue has formed at the T/O junctions, limitation in flexion may be apparent. Flexibility exercises will increase the range of movement, but more by stretching the quadriceps than the scar tissue. Where this is the case, a soft tissue manipulation may be required in an attempt to rupture the adherent scarring. If this procedure fails to produce a complete result surgery may be required. Various procedures have been described, some attempting to alter underlying malalignment and others to excise abnormal tissue.
Exercise therapy is the most important treatment clinically. Exercise on a decline board (Fig 9.46A−C) targets the extensor mechanism of the knee (Purdam et al., 2003). During a standard squat, tension in the calf musculature increases as the dorsiflexion angle of the ankle increases. This increased calf tension reduces the required workload of the quadriceps as the elastic response of the gastrocnemius will tend to lock the knee during the final degrees of extension. The eccentric squat should be used as a progression from a flat surface to decline and finally as a hop action in each case initially practised with both legs and then with a single (affected) leg. The single leg decline squat is an intense action which has been shown to be an accurate test to detect change in pain with a better discriminative ability than the standard squat (Purdam et al., 2003).



Figure 9.46 Exercise therapy for knee extensor mechanism: (A) decline board, (B) incline board and (C) hop.
Keypoint
The decline squat action should be used as a progression in patella tendinitis from (i) flat, (ii) decline to (iii) hop, in each case from double leg to single leg.
The shock-attenuating function of the leg musculature must be enhanced, and re-education of correct lower limb alignment during take-off and landing patterns is useful. Any muscle imbalance must be identified and corrected. Eccentric loading is increased through progressive closed chain activities, using ‘drop and stop’ exercises of varying intensities. These are progressed initially to slow concentric−eccentric coupling and eventually to plyometrics.
Stretching and gradual eccentric strengthening of the anterior tibials has been shown to be effective (Reid, 1992). Passive plantarflexion is performed initially to stretch the musculature. Slow concentric activity is then used as the athlete actively dorsiflexes against manual resistance. Eccentric activity follows as the athlete controls the rate of plantarflexion against therapist resistance. The exact mechanism for the effectiveness of this programme is not known, but both infrapatellar ligament stretching, and quadriceps/foreleg strength ratio changes have been suggested (Reid, 1992).
Arthritis
The pathological processes involved in osteoarthrosis (OA) were covered in Chapter 1. Here, we will look at the relevance of OA to the knee in sport.
Arthritis secondary to sports injury
Joint cartilage is continually subjected to impact stress in sport. For example when running a marathon an athlete is said to take 38 000 steps and each time to subject the knee joint to between 4 and 8 times their bodyweight, which equates to almost 5000 tons force. After a 20 km run cartilage volume is seen to reduce by 8% in the patella, 10% in the meniscus and 6% on the tibial plateau, with all cartilage volumes returning to normal within 1 hour of cessation of exercise (Hohmann, 2006). Joint cartilage is open to continuous micro-damage. However, providing the cartilage repair mechanisms outweigh the damage process, the joint will remain healthy. If these repair mechanisms break down, however, the joint will degrade. The repair mechanism is carried out by chondrocytes which, are responsible for secreted proteoglycans and collagen.
Some of the changes which occur in OA, if detected early enough, may be reversible (Hertling and Kessler, 1990). Altered biomechanics of a joint, if corrected, can result in regrowth of fibrocartilage. However, subtle alterations in normal joint mechanics, which may remain long after an injury has ‘resolved’, may be largely undetectable to a patient or physician. It is not until these changes are well developed and limit physiological joint movement or cause deformity that they become readily apparent. Accessory movements, however, when limited, are detectable to a physiotherapist with good manipulation skills at a much earlier stage. It would seem logical therefore to assess and restore accessory movements after joint injury rather than simply full range physiological movement and muscle strength. In this way the onset of OA may be slowed or even avoided.
As an example of the importance of this principle, note a study by Sharma et al. (2001) which showed that a small change in alignment of the knee (10% increase in varus angle) changed the peak contact force from 3.3 times bodyweight to 7.4 times bodyweight, more than doubling the forces acting on the knee during running.
The use of biomechanical analyses after injury with apparatus such as video playback, isokinetic dynamometry and force plates is helpful to ensure that joint function has been restored.
Arthritis and exercise
Arthritis is often considered a normal ageing process. However, Panush and Brown (1987) cite a study of a population in the age range 70–79 years in which 85% had OA. Importantly, the data indicated that 15% of this age group did not suffer from OA, so it seems likely that although ageing is an important factor, other considerations must exist.
Animal studies have failed to show a direct link between exercise and arthritis. Radin, Eyre and Schiller (1979) found no evidence of cartilage deterioration in sheep forced to walk for 4 hours daily on concrete for 12 and 30 months. Videman (1982) found that running did not affect the development of OA in rabbits. Experimentally induced OA was not increased when the animals were forced to run over 2000 m per week for 14 consecutive weeks.
Studies on runners have also failed to show any significant difference from non-runners. Puranen et al. (1975) found less hip OA in Finnish distance runners than in non-runners of a similar age. Panush et al. (1987) found no greater clinical or radiological evidence of OA in male runners of average age 55 years, and Lane, Oehlert and Block (1998) concluded that runners and non-runners showed similar evidence of hip and knee OA.
Studies have linked OA of particular joints with specific sports. In a review on the subject, Panush and Brown (1987) cited studies describing OA in the cervical spine and lower extremities of ballet dancers, the upper limb of baseball pitchers, the hands of boxers, cricketers, and downhill skiers, and the ankles and feet of soccer players. Whether these results reflect overuse of the joints involved or altered mechanics following injury to these more frequently used body parts remains uncertain. In general, most authors agree that moderate habitual exercise will maintain joint integrity but sports which subject a joint to repetitive high impact and torsional forces increase the risk of articular degeneration and subsequent OA development (Eichner, 1999).
It would seem logical that maintaining the normal mobility and strength of a joint throughout life could help maintain the health of the joint structures and perhaps delay the onset of OA. Conversely, high impact loading of an already degenerating joint, such as may occur with running or aerobics on hard unforgiving surfaces, may exacerbate symptoms.
The advice to a patient with OA must be to reduce impact but maintain mobility and strength in a controlled fashion. Athletes must also be made aware of the danger of ‘running through the pain’ and training with an injury which alters the forces across a joint. Similarly, athletes must be conscious that the cessation of pain following injury does not indicate that full function has returned. Total rehabilitation has only occurred when normal joint mechanics has been restored.
Arthritis and obesity
Obesity is steadily increasing in the Western world; 55–60% of adults in the USA are overweight (BMI of 25 or more) and 20–25% are clinically obese (BMI 30 or more) (ACSM, 2001). As well as having an important effect on cardiovascular health, obesity has an effect on joints. A high percentage of subjects with end-stage hip OA have been shown to be overweight, with a mean BMI of 28.8 (Marks and Allegrante, 2002).
The weight-bearing joints of the lower limb (hip, knee and ankle) are especially at risk from obesity. Obese patients with arthritis of these joints should therefore be helped to lose weight, as this may significantly help the condition.
Definition
Body mass index (BMI) or ‘Quetelet index’ is a measure of body bulk. BMI is obtained by dividing a person’s weight (in kilograms) by their height (in metres) squared. A BMI below 20 is considered underweight, 20–25 normal, 25–30 overweight and over 30 obese.
Obese individuals have been shown to be more likely to develop OA, the increased risk being 4.8-fold in men and 4.0-fold in women. In addition, it has been suggested that obesity increases the risk of the development of bilateral rather than unliteral OA (Felson, 1997).
Treatment of the osteoarthritic knee
Cartilage repair
Articular cartilage damage is common in the general population with over 60% of patients showing damage on arthroscopic investigation. Of these, just over 10% may be suitable for cartilage repair (Aroen, Loken, and Heir, 2004). Damage may occur through trauma including contact sports, chronic repetitive trauma (overuse in the presence of biomechanical malalignment) or through disease states such as osteoporosis and osteoarthrosis.
Several surgical techniques may be used to aid repair of injury to articular cartilage (see Table 1.72. The joint surface may be debrided (scraped) and the joint itself washed out (lavaged) to remove fragments of cartilage or subchondral bone. Damaging enzymes produced through cartilage degeneration are also removed. New cartilage cells may be introduced into the damaged area to stimulate healing. Osteochondral grafts of this type may be taken from the patient (autografts) or from cadaveric donors (allografts). A number of tissues have been used for autografts including rib perichondrial cells, periosteum and chondrocytes themselves. The technique involves two surgical procedures. First the cells must be removed, then allowed to grow in a laboratory, and finally the cells must be replanted into the damaged cartilage. Allograft techniques can result in high degrees of rejection as a complication (Wroble, 2000) but only involve a single surgical procedure.
Definition
Autografts involve implanting cells or tissue taken from the patient. Allografts are taken from a cadaver (dead person).
Drilling, abrasion and microfracture all work by penetrating the subchondral bone and stimulating cell regrowth. The aim is to allow a conduit for clot formation containing mesenchymal stem cells capable of forming repair tissue (Steadman, Rodkey and Singleton, 1997). Unfortunately fibrocartilage rather than renewed hyaline cartilage is produced by these procedures, and this is less durable than hyaline cartilage.
The most commonly used technique for articular cartilage repair is autologous chondrocyte implantation (ACI), and Table 9.13 shows general indications for this type of surgery. This technique was developed in the 1980s and is now the most commonly used technique. In the first stage of the procedure a biopsy of cartilage is taken from a non-weight bearing area and the harvested tissue is sent to a laboratory where new chondrocyte cells are grown from it. As this is the patient’s own tissue, rejection is avoided. On average one million such cells are required per centimetre of chondral defect. In the second surgical stage a collagen membrane is sutured to the defect site to created a water tight region and the cultured cells are implanted into the hollow.
Table 9.13 Criteria for autologous chondrocyte implantation (ACI)
| Inclusion criteria | Exclusion criteria |
|---|---|
Outcome ratings are best for procedures involving the medial femoral condyle, with patella and trochlea regions being less successful. Treatment failure can occur especially if high impact sport is begun too early, and standard surgical complications to arthroscopy apply.
Rehabilitation following cartilage repair
Maturation and remodeling of the graft can continue for up to 24 months following surgery, an important factor to consider when structuring a rehabilitation programme. Return to weight bearing activities must be progressive and both range of motion and strengthening exercise is required. Intensity of rehabilitation is dependent on defect size, larger defects clearly having more tissue. The graft is at most risk for the first 12 weeks following surgery and is especially vulnerable to shearing stresses.
During rehabilitation there must be a balance between protection of the joint and encouraging function. Joint motion, intermittent loading (progressive) and tissue adaptation is encouraged, while repetitive friction, shearing stress and either overload or underload of the repaired joint are restricted (Hambly, 2009). In the initially post surgical stage reduction in swelling and pain are key components of rehabilitation while the joint is protected. A knee brace is worn and the patient may be non-weight bearing on crutches for 2−4 weeks. Gentle range of motion exercises are encouraged, but rotation actions on the knee such as kneeling or squatting are prohibited to prevent imparting shear forces onto the new tissue. Cartilage reattachment can take between 8 and 12 weeks, and during this time a progressive programme from non-weight bearing to partial weight bearing is used. Early full weight bearing (avoiding shearing) may be desirable. A study comparing an 11 week programme of full weight bearing to an accelerated 8 week programme (Ebert et al., 2008) showed that patients in the accelerated group achieved greater 6 minute walking distances and better improvement in knee pain measured using the Knee Injury and Osteoarthritis Outcome Score. The programmes caused no adverse effects in either group when investigated using MRI.
Sport which involves twisting and pivoting actions are generally limited for 3−5 months following surgery depending on the type of surgery performed. Small isolated defects will recover while larger defects, and those associated with other structural faults of the knee (traumatic debridement accompanied by cruciate or meniscal injury, for example), will take longer.
Non-weight bearing activity should include general mobility such as static cycling and pool exercise, while specific work addresses muscle imbalance around the hip and knee. Imbalance exercises such as the clamshell, hip hitch and mini squat are used together with walking re-education. It is also important to reinforce an appreciation of the amount of weight being taken through the limb in partial weight bearing activities. This can be achieved by having the athlete stand on two sets of scales (Hambly, 2009) and gradually increasing and reducing the amount of weight taken. As with all knee injuries requiring the athlete to walk with crutches, part of the training should be education on 3 point and then 4 point walking with correct heel−toe action and whole body alignment.
Hyaluronic acid injections
The use of hyaluronic acid (HA) injections of the knee is now widespread. Its use is based on the fact that in OA, the synovial fluid of the knee decreases in both elasticity and viscosity, as a result of a lowering of the molecular weight of the naturally occurring hyaluronic acid. The aim of HA injection is to counteract this effect. HA is a glycosaminoglycan (GAG) which acts as a lubricant and shock absorber. It supports the normal effect of GAG within the cartilage ground substance produced by chondrocytes. This has the effect of acting as a ‘molecular sponge’ as its molecules repel each other to form a lattice which attracts water into itself (Jackson, Sheer and Simon, 2001). Injection of HA into a joint is claimed to have a viscosupplementing effect (Wright, Crockett, and Dowd 2001). However the half life of HA has been shown to be less than 24 hours in sheep, suggesting that other effects may be important. It is thought that injected HA may stimulate the natural production of hyaluronate by synoviocytes, and that HA has a direct anti-inflammatory effect by blocking prostaglandin production and reducing levels of inflammatory mediators (Bobic, 2002). In addition pain relief occurs, possibly by inhibition of substance P (Watterson and Esdaile, 2000). Side effects are typical of any joint injection and include redness, local pain and effusion lasting 2−3 days. The risk of infection and synovitis also exists, but is minimized by clean technique. A Cochrane review (Bellamy et al., 2006) of 76 trials of viscosupplementation concluded that the technique was an effective treatment for OA of the knee. Pain on average changed by 26% from baseline and function improved by 23% from baseline during weeks 5−13 post injection. There was a longer term benefit compared to interarticular injection of corticosteroids.
Interestingly the use of oral supplementation with glucosamine shows similar results. A Cochrane review of the use of glucosamine therapy (500 mg three times daily) for treating osteoarthritis (Towheed et al., 2008) demonstrated a reduction in pain of 22% from baseline and an improvement of function of 11% from baseline.
Manual therapy, exercise therapy and acupuncture
Treatment note 9.2 Manual therapy techniques for the knee
Manual therapy techniques around the knee can be used either to relieve pain or to mobilize a stiff joint. The aim is to use either a sustained stretch or a small amplitude oscillation; for manipulation, a high velocity, low amplitude movement is used at end-range.
Abduction/adduction in extension
The patient lies supine with the couch raised to the hip level of the therapist. The therapist grasps the patient’s leg tucking the shin beneath their arm and gripping it into the side of their body with the elbow (Fig. 9.47). The leg is then supported with the hands either side of the knee, thumbs resting loosely over the top of the patella, fingers curled over the popliteal area of the knee. The action is to impart an abduction and adduction oscillation with the knee extended or minimally unlocked. The valgus stress to the knee can be increased by drawing the inner hand distally and the outer hand proximally and gapping the joint. Similarly a varus stretch may be applied by moving the inner hand proximally and the outer hand distally.

Abduction/adduction in flexion
The therapist moves close into the couch and grips the patient’s ankle with the inner hand and rests the outer hand on the lateral aspect of the knee. The movement is one of flexion by pressing the heel towards the buttock (Fig. 9.48). An abduction force is applied by drawing the heel laterally or an adduction force by drawing the heel medially. These movements may be combined with either a lateral rotation (abduction) or medial rotation (adduction) by surrounding the calcaneus in the cup of the hand and using the fingers for leverage.

Anteroposterior (AP) glide
The patient’s thigh (femur) is placed on a block leaving the tibia free. The therapist lowers the couch below waist height and uses the heel of the hand to impart an AP glide to the tibia while the femur is blocked. For low grade movements both hands may be used surrounding the tibia; for high grade movements the motion is imparted through the straight arm (Fig. 9.49).

Posteroanterior (PA) glide
The patient is supported in crook lying with the knee flexed between 45° and 90°. The therapist lightly sits on the patient’s foot to prevent it slipping. The patient’s shin is gripped with the heel of the hands on the anterior aspect of the tibia and the fingers curled around the back of the calf (Fig. 9.50). The PA draw is performed by drawing the tibia forwards and may be combined with either external rotation (foot turned out) or internal rotation (foot turned in).

Lateral glide
In the crook lying position, a webbing belt is placed around the patient’s tibia and the therapist fixes the belt around his or her own waist standing to the side of the patient. The tibia is supported with one hand and the femur with the other (Fig. 9.51). The lateral glide movement is instigated by the therapist swaying backwards; movement may be monitored using the thumb over the lateral joint line.

Capsular stretch
A joint distraction or capsular stretch to flexion may be imposed using the therapist’s forearm as a pivot. The couch is raised above waist level and the patient sits in crook lying. The therapist places his or her arm under the popliteal area of the patient’s knee and the distal arm contacts the tibia. The action is to apply flexion against the pivot point of the forearm, in a ‘nutcracker’ action (Fig. 9.52). The flexion movement may be combined with internal or external rotation simultaneously.

Joint distraction
The couch is raised above waist height and the knee is placed in its open pack position of slight flexion. The patient’s shin is fixed beneath the therapist’s arm and the action is a distraction movement which is brought on by swaying the body back (Fig. 9.53).

For higher grade distraction movements, the patient begins side lying with the femur supported against the headboard of the couch. The therapist grasps the patient’s ankle and leans back with their full body weight to impart a distraction force (Fig. 9.54). This distraction force may be combined with rotation of the tibia to perform a loose body manipulation of the knee (Cyriax and Cyriax, 1983) muscles.

Manual therapy (see Treatment note 9.2), exercise therapy and acupuncture are techniques commonly used within physiotherapy for treatment of OA of the knee. Two manual therapy techniques are especially useful for OA, the capsular stretch (see Fig. 9.52) and joint distraction (see Fig. 9.53). Marked pain reduction and increased movement usually result from these procedures where flexion is substantially limited and pain occurs through prolonged standing especially.
Exercise therapy for pain reduction includes pendular swinging where the patient sits on a high bench with their feet off the ground. The action is to rhythmically swing the legs within mid range (knee flexion and extension). The exercise is continued for 2−3 minutes until pain reduces and the patient feels movement loosening. The capsular stretch mobilization may be followed up using a self-mobilization technique and home exercise. For the knee flexion self-mobilization, the patient places a soft rolled towel into the popliteal region of their knee. Overpressure is then placed on the knee by flexing the knee passively either using the hands holding the shin in lying, or pressing into flexion from a long sitting position. The kneeling sitback exercise is used as a follow-up procedure when pain has subsided below 2−3 on a visual analogue scale (VAS) and there is no visible swelling. The patient kneels (4 point kneeling) on a mat or cushion taking their weight mostly on the hands and uninjured knee. The action is to gradually press the hips backwards towards the heels (autoassisted knee flexion), easing into the movement gradually rather than forcing the motion range.
Acupuncture is often used by physiotherapists in the treatment of the osteoarthritic knee, and the results are generally good. In a systematic review of seven trials (393 patients) Ezzo et al. (2001) concluded that acupuncture was effective for both pain relief and restoration of function, and that real acupuncture was better than sham acupuncture. In a later systematic review of 13 RCTs (1334 patients) White et al. (2007) concluded that acupuncture was superior to sham acupuncture for improving pain and function with chronic knee pain. Effective treatment of pain and function is dependent on adequate treatment which normally includes more than 10 treatment sessions of 30 minutes duration, use of an appropriate treatment protocol, the patient feeling a dull aching sensation (deqi) travelling from the needling site and electrical stimulation of the needles (electroacupuncture). The acupuncture treatment technique for knee pain is covered elsewhere (Norris, 2001).
Sinding–Larsen–Johansson disease
In this condition the secondary ossification centre on the lower border of the patella is affected in adolescents. The epiphysis is tractioned, leading to inflammation and eventual fragmentation. Avascular necrosis is not usually present, but a temporary osteoporosis has been described (Traverso, Baldari and Catalani, 1990) during the adolescent growth spurt. This may weaken the inferior pole of the patella making avulsion more likely.
Definition
Sinding–Larsen–Johansson disease affects the secondary ossification centre on the lower border of the patella in adolescents. Inflammation, bone fragmentation and occasionally temporary (transient) osteoporosis may occur.
Sinding–Larsen–Johansson (SLJ) disease can easily be confused with chondromalacia on first inspection as it gives pain to the lower pole of the patella, especially when kneeling. However, on closer examination the differences are soon apparent, and x-ray confirms the bony change. Initially, no abnormalities are seen on x-ray, but after 2–4 weeks, irregular calcification is noted at the inferior pole. The calcifications are seen to coalesce later, and may finally be incorporated into the patella (Medlar and Lyne, 1978).
The condition may exist with Osgood–Schlatter’s syndrome (Traverso, Baldari and Catalani, 1990), and the conservative management of the two syndromes is largely the same, involving the use of pain relieving/anti-inflammatory modalities and training modification. Surgical removal of the lower pole of the patella has been recommended in persistent cases (Williams and Sperryn, 1976).
Osgood–Schlatter’s syndrome
This condition affects adolescents, especially males. Most often the patient is an active sportsperson who has recently undergone the adolescent growth spurt. With Osgood–Schlatter’s syndrome traction is applied to the tibial tubercle, eventually causing the apophysis of the tubercle to separate from the proximal end of the tibia. Initially, fragmentation appears, but with time the fragments coalesce and further ossification leads to an increase in bone. This gives the characteristic prominent tibial ‘bump’ often noticeable when the knee silhouette is compared to that of the unaffected side.
The infrapatellar tendon shows increased vascularization and, particularly where radiographic changes are not apparent, soft tissue swelling and infrapatellar fat pad involvement is noted. Pain is highly localized to the tibial tubercle and exacerbated by activities such as running, jumping and descending stairs. The condition may coalesce with patellar malalignment faults such as patella infera and patella alta. Patellar tendon avulsion can occur following this condition, and Levi and Coleman (1976) reported 26% of those seen with this type of fracture to have had a previous history of Osgood–Schlatter’s disease.
Initial management is by limiting activity in the acute phase. Pain relief and reduction of inflammation may be obtained by using electrotherapy modalities alone, or iontophoresis with an anti-inflammatory medication and local anaesthetic (Antich and Brewster, 1985). Injection of the tibial tubercle with hydrocortisone has been described (Grass, 1978). The use of local dry needling to the tibial tuberosity and trigger point acupuncture to the rectus femoris has been described (Norris, 2001). An infrapatellar strap to reduce the pull of the quadriceps onto the tibial tubercle has been used with some success (Levine and Kashyap, 1981).
Assessment of the lower limb musculature often reveals hypertrophy and inflexibility of the quadriceps. When passive knee flexion is tested, intense pain precludes the use of quadriceps stretching. However, when pain has subsided, flexibility of this muscle group must be regained. Where prolonged rest has given rise to muscle atrophy, strengthening exercises are indicated. Ice packs may be used to limit pain or inflammation following activity. Restoration of acceleration/deceleration mechanics in jumping and landing (closed chain) is as for jumper’s knee (see above).
Synovial plica
The synovial plica is a remnant of the septum which separates the knee into three chambers until the fourth intrauterine month. Three types of plica are seen. The infrapatellar plica (ligamentum mucosum) lies within the intercondylar notch and runs parallel to the anterior cruciate ligament. The suprapatellar plica is found on the medial aspect of the suprapatellar pouch, lying proximal to the superior pole of the patella. The mediopatellar plica extends from the medial suprapatellar pouch over the medial femoral condyle and onto the synovium covering the infrapatellar fat pad (Fig. 9.55). The mediopatellar plica is by far the most important in terms of pathology.
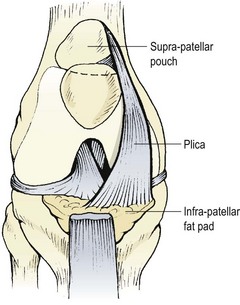
Definition
A synovial plica is a remnant of the tissue which separates the knee into three chambers in the unborn child. A mediopatellar plica is the most common type to give problems in sport.
A mediopatellar plica may be present in some 20–60% of knees (Amatuzzi, Fazzi and Varella, 1990), but does not necessarily cause symptoms. In a series of 3250 knee disorders, Koshino and Okamoto (1985) found only 32 patients to have the complaint (1%). The structure separates the knee joint into two reservoirs, one above the patella and the other constituting the joint cavity proper. The normal plica is a thin, pink, flexible structure, but when inflamed it becomes thick, fibrosed and swollen, loosing its elasticity and interfering with patellofemoral tracking.
These tissue changes are often initiated by trauma that results in synovitis, and is more common in athletes. Pain is usually intermittent and increases with activity. Discomfort is experienced when descending stairs and may mimic PFPS. However, pain of plical origin normally subsides immediately when the knee is extended. In addition, the ‘morning sign’ may be present. This is a popping sensation which occurs as the knee is extended, particularly on rising, but disappears throughout the day. The popping may be accompanied by giving way, and is caused by the thickened plica passing over the medial femoral condyle. As the day progresses, joint effusion pushes the plica away from the condyle. This sign may be reproduced with some patients by extending the knee from 90° flexion while internally rotating the tibia and pushing the patella medially. The pop is usually experienced between 45° and 60° flexion.
Keypoint
A popping sensation may be caused as the plica passes over the medial femoral condyle when the knee is extended. This may be reproduced by: (i) extending the knee from 90° flexion while (ii) internally rotating the tibia and (iii) pushing the patella medially.
Conservative treatment has been found to be effective in 60% of cases (Amatuzzi, Fazzi and Varella, 1990) and aims at reducing the compression over the anterior compartment of the knee, by using stretching exercises. The length of the hamstrings, quadriceps and gastrocnemius muscles should be assessed and these muscles stretched if noticeable shortening is found. Where conservative treatment fails and symptoms limit sport or daily living, surgery may be warranted. Koshino and Okamoto (1985) reported pain and symptom relief in 90% of knees treated surgically by plical resection, but did not quote figures for long-term follow-up.
Tendinitis
Tendinitis (inflammation within the tendon substance) and tendinopathy (swelling around but not within the tendon) of the knee occurs most commonly within the patellar tendon (jumper’s knee, see above), the semimembranosus and the popliteus.
Semimembranosus has a complex insertion consisting of five slips onto the proximal tibia (Williams, 1995), making direct palpation of an inflamed area difficult. The five insertions are:
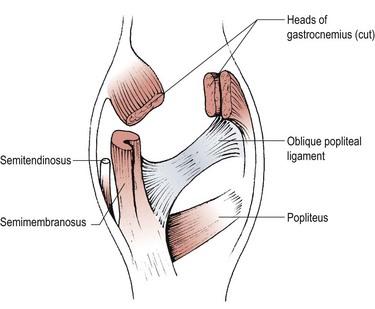
Tendinopathy of this muscle gives a persistent ache over the posteromedial aspect of the knee. It occurs as the semimembranosus tendon slides over the medial corner of the medial femoral condyle, and is distinct from semimembranosus bursitis which affects the area of the medial tibial condyle. Pain may occur within the tendon substance itself, or over the teno-osseous junction, when an insertional tendinopathy is present. Increased tracer uptake has been noted on bone scan with this latter condition (Ray, Clancy and Lemon, 1988).
Popliteus tendinopathy is related to increased pronation of the STJ and excessive internal rotation of the tibia (Brody, 1980). The increased internal rotation causes traction on the popliteus attachment to the lateral femoral condyle. The popliteus acts with the PCL to prevent forward displacement of the femur on the flexed tibia, and so will be overworked with downhill running (Baylis and Rzonca, 1988). On examination, tenderness is revealed over the popliteus just anterior to the fibular collateral ligament. The patient is examined in a supine position with the injured knee in the ‘figure of four’ position, that is affected hip flexed, abducted and externally rotated, knee bent to 90° and foot placed on the knee of the contralateral leg. The condition is differentiated from ITB friction syndrome by testing resisted tibial internal rotation with the knee flexed, and palpating the popliteus while internal rotation is resisted in extension (Allen and Ray, 1989).
Treatment for tendinopathy involves rest, anti-inflammatory modalities and training modification. Flexibility of the knee musculature and the biomechanics of the lower limb should be assessed and corrected as necessary.
Bursitis
The knee joint has on average 14 bursae (Table 9.14) in areas where friction is likely to occur, between muscle, tendon, bone and skin. Any of these can become inflamed and give pain when compressed through muscle contraction or direct palpation. Those most commonly injured in sport include the pre-patellar, pes anserine and semimembranosus.
Table 9.14 Bursae around the knee
| Bursa | Lying between |
|---|---|
| Subcutaneous prepatellar | Lower patella/skin |
| Deep infrapatellar | Upper tibia/patellar ligament |
| Subcutaneous infrapatellar | Lower tibial tuberosity/skin |
| Suprapatellar | Lower femur/deep surface of quadriceps (communicates with joint) |
| No specific name | Lateral head of gastrocnemius/capsule |
| Lateral collateral ligament/tendon of biceps femoris | |
| Lateral collateral ligament/popliteus | |
| Popliteus tendon/lateral condyle of femur | |
| Medial head of gastrocnemius/capsule | |
| Medial head of gastrocnemius/semimembranosus | |
| Pes anserine | Superficial to medial collateral ligament/ sartorius, gracilus, semitendinosus |
| No specific name | Deep medial collateral ligament/femur, medial meniscus |
| Semimembranosus | Semimembranosus/medial tibial condyle, gastrocnemius |
| No specific name | Semimembranosus/semitendinosus |
Pre-patellar bursa
The pre-patellar bursa is usually injured by falling onto the anterior aspect of the knee, or by prolonged kneeling (housemaid’s knee). Haemorrhage into the bursa can cause an inflammatory reaction and increased fluid volume. Enlargement is noticeable and the margins of the mass are well defined, differentiating the condition from general knee effusion or subcutaneous haematoma. Knee flexion may be limited, the bursa being compressed as the skin covering the patella tightens.
Keypoint
Falling directly onto the point of the knee may cause housemaid’s knee (pre-patellar bursitis). Only the anterior aspect of the knee is swollen, and pain is increased by knee flexion as the bursa is compressed.
Septic bursitis may result by secondary infection if the skin over the bursa is broken by laceration or puncture wound. If the condition becomes chronic, the bursa may collapse and the folded walls of the thickened bursal sac appear as small hardened masses on the anterior aspect of the knee. In these cases, erythema and exquisite tenderness are usually present.
Minor cases normally respond to rest and ice, but more marked swelling requires aspiration. Aspiration is carried out under sterile conditions, and a compression bandage applied.
Semimembranosus and pes anserine bursae
Semimembranosus bursitis gives rise to pain and swelling over the lower posteromedial aspect of the knee. Pain may be made worse by hamstring or gastrocnemius contraction against resistance, and in activities involving intense action of these muscles, such as sprinting and bounding.
Pes anserine bursitis gives pain and swelling over the metaphyseal area of the tibia, sometimes referred to the medial joint line (Baylis and Rzonca, 1988). The bursa may be injured by direct trauma (hitting the knee on a hurdle) or by overuse of the pes anserine tendons.
With both of the latter causes of bursitis, rest and anti-inflammatory modalities are required. Biomechanical assessment of the lower limb and analysis of the athlete’s training regime are called for where there is no history of injury.
Baker’s cyst
One condition often referred to as ‘bursitis’ is a Baker’s cyst. This is actually a posterior herniation of the synovial membrane into the bursa lying between semimembranosus and the medial head of the gastrocnemius (Fig. 9.57).
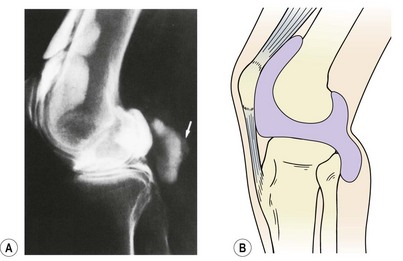
From Reilly, B.M. (1991) Practical Strategies in Outpatient Medicine. W.B. Saunders, Philadelphia. With permission.
The mass bulges into the popliteal space, and occurs particularly in rheumatoid arthritis. The posterior knee ligaments weaken and fail to support the joint capsule, allowing the herniation to occur. The cyst can be palpated over the medial side of the popliteal space beneath the medial head of the gastrocnemius.
Definition
A Baker’s cyst is a bulging (herniation) of the synovial membrane backwards into the bursa lying between semimembranosus and the medial head of the gastrocnemius.
When painless, the condition may be managed conservatively, but where the enlargement compromises venous return or causes severe pain, aspiration or excision of the mass is called for.
Fat pads
Fat pads consist of fat cells (adipose tissue) packed closely together and separated from other tissues by fibrous septa. They have an abundant blood supply, and are well innervated. Most significant to the knee is the infrapatellar fat pad, lying beneath the patellar tendon, and in front of the femoral condyles. The fat pad is intracapsular but extrasynovial, and a piece of synovial membrane (ligamentum mucosum, see above) may pass from the pad to the intracondylar notch of the femur. When the knee is fully flexed, the infrapatellar fat pad fills the anterior aspect of the intercondylar notch. As the knee extends, the fat pad covers the trochlear surface of the femur within the patellar groove (Hertling and Kessler, 1990).
The usual pathology of the infrapatellar fat pad is an enlargement causing increased pressure with resultant pain (Hoffa’s disease). Direct trauma can cause haemorrhage and local oedema, and swelling may also occur as a result of premenstrual water retention. Space occupying lesions, such as osteochondrotic fragments, may also cause enlargement, and Smillie (1974) described a case where a displaced bucket handle tear of the medial meniscus was forced into the infrapatellar fat pad of the knee.
Enlargement and entrapment of the patellar fat pad has been described by Finsterbush, Frankl and Mann (1989). The entrapped pad was shown to be in various stages of tissue degeneration, including fat necrosis and replacement of the fatty tissue with fibrinoid material. Complete fibrosis was later seen. Silver and Campbell (1985) described persistent inflammation of the knee fat pads as a cause of delayed recovery in dancers with knee injuries. Surgical removal of the pad resulted in restoration of full range motion at the knee. Tsirbas, Paterson and Keene (1990) described excision of the fat pad tip to relieve patellofemoral pain. Patients presented with a history of pain inferomedial, and sometimes inferolateral, to the patella. On examination, impingement pain occurred deep to the inferior pole of the patella at 20° flexion with resisted quadriceps contraction.
Relief of mild compression pain may be achieved with taping (McConnell, 1992). Taping begins over the tibial tubercle and extends laterally and medially in a ‘V’ shape. The tape is placed under traction to lift the patella in a cephalic direction. This effectively forms a sling to prevent the patella pressing into the fat pad (Fig. 9.58).