Orthodontics I
Development, assessment and treatment planning
Overview
Orthodontics relates to facial and occlusal development as well as to the supervision, interception and correction of occlusal and dentofacial anomalies. The practice of orthodontics, therefore, spans from birth into adulthood, with current practice aiming to establish optimal and stable occlusal relationships with dentofacial harmony. An appreciation of facial and occlusal development is fundamental to understanding the possible aetiology of some orthodontic problems as well as being critical for their assessment and the planning of any likely treatment.
This chapter commences with an account of the rudiments of facial and occlusal development. It then details the elements of comprehensive clinical and cephalometric orthodontic assessment. Finally, the principles of treatment planning are considered.
9.1 Craniofacial growth and occlusal development
An understanding of both craniofacial growth and occlusal development is essential to orthodontic practice as the former has a significant impact on the latter.
Craniofacial growth
Pattern of craniofacial growth
At birth, the face and jaws are underdeveloped compared with those in the adult. More growth, therefore, occurs of the facial skeleton than of the cranial structure postnatally. Growth patterns have been established for four major body tissue systems – lymphoid, neural, general or somatic, and genital – and it is important to have an appreciation of these as some patterns are followed by tissues involved in craniofacial growth (Fig. 9.1). Lymphoid growth is rapid up to about 10 years but undergoes involution as the genital growth is accelerating at puberty. Neural growth, however, is virtually complete by 6–7 years, while somatic growth increases in early childhood, then slows, before increasing dramatically at puberty.
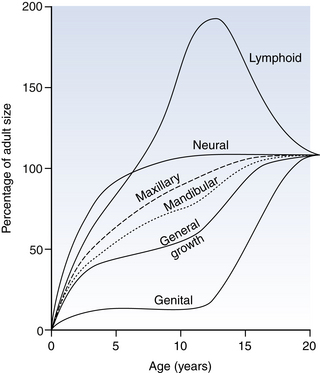
Fig. 9.1 Postnatal growth curves of various tissue types with superimposed maxillary and mandibular curves.
The pattern of neural growth affects skeletal growth of the calvarium and orbit, whereas the somatic growth pattern is followed approximately by the mandible and maxilla. More precisely, the jaw growth pattern falls between that followed by the neural and general body tissues, with the mandible aligning itself more to the latter than the maxilla. The spurt in jaw growth at puberty almost coincides with the spurt in height, on average at 12 years in girls and 2 years later in boys, although considerable individual variation exists.
For both the maxilla and mandible, on average, growth in width is completed in advance of that in length, which ceases before growth in the vertical dimension. The transverse dimensions of the jaws and dental arches do not tend to alter during puberty, as growth in width is largely completed before the growth spurt. Growth in length usually continues until 14–17 years in girls and 17–19 years in boys, while vertical growth may extend into the late teens in girls and into the twenties in boys. For males and females, growth of the maxilla in all dimensions is completed before that of the mandible.
Growth continues into adult life, with vertical changes in the facial skeleton predominating over anteroposterior changes, and least change taking place laterally. In the twenties, growth tends to resume slightly in females who overall exhibit a backward mandibular rotation. Although a late resumption of growth is not witnessed in males, a forward rotation of the mandible is usual in adulthood. Irrespective of the direction of mandibular growth rotation, compensatory adjustment occurs in the occlusal relationships. Facial growth should, therefore, be seen as a process that continues well into adult life and not as one that is complete in the late teens.
Control of facial growth
Both genetic and environmental factors impact on the regulation of craniofacial growth but the exact mechanisms are unclear. In theory, genetic control may be expressed primarily via bone, cartilage or the adjacent soft tissues (‘functional matrix theory’); the current concept is a merging of these second and third theories, bone largely having being discounted. Sutures and periosteal tissues do not determine craniofacial growth primarily, as sutural growth is reactive rather than inherently programmed. The maxillary sutures are not growth centres, but rather growth sites. The synchondroses of the cranial base and the nasal septum, to a lesser degree, probably act as independent growth centres but the cartilage of the mandibular condyle appears to react to, rather than initiate, growth.
Growth of the cranium and of the orbit in direct response to growth of the brain and of the eyes respectively lend support to the ‘functional matrix theory’. Growth of the cranial base, although mainly by endochondral growth coupled with bony replacement at the synchondroses, may be influenced by growth of the brain. Cartilaginous growth of the nasal septum and growth of the surrounding soft tissues probably contributes to moving the maxillary position forward but the amount apportioned to the former is unknown.
The soft tissues, including the masticatory muscles, are also contributors to spatial translation of the mandible and to addition of new bone at the condyle.
Growth prediction
At present, no method is available to predict accurately the amount, direction and timing of facial growth. Instead, the assumption is usually made that for most patients whose direction and amount of facial growth are about average, the likelihood is that their growth pattern will follow the same pattern through orthodontic treatment.
Methods attempting to predict the pattern of facial growth to assist orthodontic treatment planning include:
• superimposition of a template with average annual growth increments on the patient’s cephalometric tracing
• digitisation of a cephalometric film followed by computer addition of average annual growth increments.
As the amount and direction of growth may not be ‘average’ in an individual, there is a considerable amount of imprecision with regard to ascertaining clinically useful growth prediction. The assumption is often made, however, that the direction of mandibular growth rotation is likely to continue.
Growth of the craniofacial skeleton
Craniofacial growth can be considered conveniently in relation to the calvarium, the cranial base, the maxillary complex and the mandible.
Calvarium: The precursors to the skull bones develop in membrane, and six open spaces (fontanelles) that exist at birth are eliminated by 18 months. Contact between the bones is at sutures. Bone apposition occurs at these periosteum-lined sites in response to brain growth and they fuse eventually in adulthood. The contour of the cranial vault also changes by periosteal remodelling at the inner and outer surfaces. The growth in size of the calvarium is complete by 7 years.
Cranial base: The cranial base forms initially in cartilage, which is transformed to bone by endochondral ossification. Sutural growth and surface remodelling occur laterally in response to brain growth. Of greater significance are primary cartilageous growth sites (synchondroses): sphenoethmoidal, intersphenoid and, most importantly, the spheno-occipital. The spheno-occipital synchondrosis grows until the early to mid-teens in females and somewhat later in males (15–17 years), having a profound impact on the anteroposterior skeletal pattern; it finally fuses at about 20 years. Because of its location in front of the temporomandibular joints but behind the anterior cranial base, both growth in length and in shape of the cranial base affects the maxillary–mandibular relationship. A long cranial base or large cranial base angle is associated with a class II skeletal pattern, while the converse is generally associated with a class III pattern (see Section 9.3 for definitions).
Maxillary complex: The frontal process and a mesenchymal condensation in the maxillary processes of the first pharyngeal arch form the maxilla which then ossifies intramembraneously, starting in the lateral aspects of the cartilagenous nasal capsule. Growth of the maxilla occurs via:
• bone apposition at the circum-maxillary suture system
• passive displacement from its articulation with the cranial base
Growth at the maxillary sutures assumes a greater role after age 7 years, when neural growth is complete and growth at the cranial base synchondroses lessens. As the maxilla moves downwards and forwards in response to growth of the surrounding soft tissues, the space opened at the superior and posterior sutures is obliterated by bone deposition on either side of the suture. Resorption of the anterior maxillary surface occurs simultaneously. Displacement of the maxilla inferiorly is accompanied by bone resorption from the nasal floor and deposition on the palate, while the alveolar process also develops vertically with tooth eruption. Bone is deposited also at the midline suture in response to lateral displacement of the maxillary halves, leading to an increase in midfacial width. The increase in maxillary dimensions lag behind those of the nasal structures, especially at puberty where a 25% differential is recorded. Maxillary growth is complete by about 17 years in males and on average 2 years earlier in females.
Mandible: Like the maxilla, the mandible is derived from the first pharyngeal arch. It begins development as a mesenchymal condensation just lateral to Meckel’s cartilage. Ossification proceeds intramembraneously, spreading posteriorly along Meckel’s cartilage without directly replacing it by newly formed bone. Condylar cartilages are formed distant to the mandibular body but fuse with it at about 4 months. These secondary cartilages are not primary instigators of mandibular growth but respond to other controlling influences. Endochondral ossification at the condyles accounts, in part, for mandibular growth. Elsewhere, bone apposition and remodelling are responsible for an increase in size and shape. As the mandible is translated downwards and forwards, largely in response to muscular forces, contact with the base of the skull is maintained by cartilagenous growth at the condylar heads, which increases ramal height. The alveolar processes also increase in height with tooth eruption.
Mandibular length is increased by periosteal apposition along the posterior border and simultaneous bone removal from the anterior aspect of the ramus. An increase in mandibular width occurs principally by remodelling posteriorly. The chin is almost passive as a growth area but, by the late teenage years, it has become more prominent particularly in males. On average, mandibular growth is complete by about 17 years in females and 2 years later in males, but it can proceed for longer.
Growth rotations
The trend is for the facial skeleton to grow downwards and forwards away from the cranial base, although implant studies have indicated that rotations of both the maxilla and mandible occur during growth. These have more marked effects on the mandible than on the maxilla, where remodelling disguises their true impact. Mandibular growth rotations represent a growth imbalance in anterior and posterior facial heights. The direction of condylar growth and the vertical magnitude of growth at the spheno-occipital synchondrosis influence posterior facial height. Growth of the masticatory and suprahyoid musculature, including associated fascia and influenced partly by the vertical growth changes in the spinal column, affects the anterior facial height together with the eruption of teeth.
While mandibular growth rotations occur in all individuals, these are particularly different where the vertical facial proportions are markedly reduced or increased. A forward rotation, characterised by greater growth in posterior than in anterior facial height, is more common than a posterior growth rotation, where the change in facial height ratio is opposite to that observed in forward rotation (Fig. 9.2). Where forward rotation of the mandible is extreme:
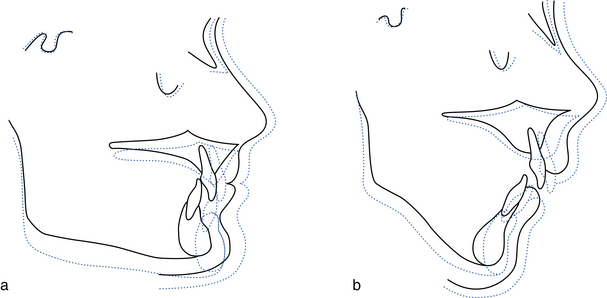
Fig. 9.2 Growth rotation.
(a) Forward growth rotation owing to greater increase in posterior than in anterior facial height, resulting in an increased overbite. (b) Backward growth rotation owing to a greater increase in anterior than in posterior facial height, resulting in a reduced overbite.
• the lower border is convex with a reduced mandibular plane angle
Conversely, a backward rotational pattern of mandibular growth results in:
• a pronounced antegonial notch with a high mandibular plane angle
The pattern of rotation has an impact on treatment. Whereas a forward rather than a backward rotation aids correction of a class II skeletal discrepancy, it also tends to increase overbite. Where the rotation is marked, overbite reduction is more difficult. Growth rotations also influence the inclination and anteroposterior position of the lower incisors. A forward growth rotation leads to retroclination of the lower incisors and an increase in lower labial segment crowding. With a posterior mandibular growth rotation, the incisors become upright, shortening the dental arch and producing crowding of the lower incisor area. Lower labial segment crowding is common in late teens particularly where mandibular growth continues after maxillary growth has ceased but other factors are likely contributors (see below).
Soft tissue growth
At birth, the orofacial musculature is well developed to allow suckling and breathing, and it soon responds to other functional demands of mastication, speech, facial expression and changes to the swallowing pattern. The light pressures from the lingual and buccolabial musculature affect tooth position, guiding the teeth towards a functional relationship and compensating, where possible, for any skeletal discrepancy. However, where a severe skeletal discrepancy or abnormal soft tissue behaviour exists (e.g. a lip trap with a class II division 1 malocclusion), the dento-alveolar compensatory mechanism will be insufficient.
Facial musculature lengthens with facial growth which increases the likelihood of lip competence. In girls, the greatest overall changes in soft tissues occur between 10–15 years but nasal growth is complete generally by age 16. In boys, however, the greatest soft tissue changes usually occur later (from 15 years) and most will be complete by late teens. In adulthood, soft tissue profile changes take place in both sexes in concert with, but are much larger than, those of the facial skeleton. Notably, the nose tends to lengthen and the lips move down relative to the teeth so, over time, less of the maxillary and more of the mandibular incisors become exposed on smiling; the fullness of the lips also decreases. An increase in chin prominence is common in males, whereas in females, the chin may become more retrusive or show minor change.
Occlusal development
What follows is an account of normal occlusal development: the changes one would expect to see in the ‘average’ child. It is important to appreciate the range that exists within normal boundaries, so that developing problems may be recognised early and appropriate orthodontic intervention planned, if required. A thorough knowledge of the calcification and eruption dates of the 20 primary and 32 permanent teeth is essential (see Tables 7.1 and 7.2, p. 194). As well as allowing comparison of dental and chronological age, this information also helps to identify the timing of any insult that has led to alterations in the enamel or dentine mineralisation and indicates if a tooth that is absent radiographically is likely to develop.
Development of the primary dentition
The gum pads, containing the primary teeth, enlarge and widen following birth, with the lower lying slightly behind the upper by the time the first primary teeth (lower incisors) start to erupt at about 6 months of age. These are followed closely by the other incisors. The first primary molars erupt 3–4 months later, followed by the primary canines and the eruption of the second primary molars at about 3 years. The incisors tend to be upright, and anterior spacing is normal. Spacing is most common mesial to the upper canine and distal to the lower canine – the anthropoid or primate spaces. With a 1–2 mm increase in the intercanine distance, spacing between the incisors often increases as the child grows. In the absence of generalised spacing of the primary teeth, crowding of the permanent teeth is likely. The overbite, which is often initially ‘deep’ in terms of lower incisor crown coverage, reduces, and by 5 years of age an edge-to-edge occlusion with incisor attrition is common.
Development of the permanent dentition
At about 6 years, the eruption of the first permanent molars, followed by the permanent incisors, signifies the transition from the primary to the permanent dentition, commonly referred to as the ‘mixed dentition phase’. The permanent successors are slightly larger than the primary teeth and the first permanent molars need to be accommodated. Existing space is present between the primary teeth. Additional space is provided by minor modifications in arch length, arch width and intercanine distance (Table 9.1). Once the primary dentition is fully erupted, however, the dental arch size remains more or less constant anteriorly apart from a modest change in shape with some growth in the intercanine distance. In addition, growth at the back of the arches is necessary to accommodate the permanent molars and to maintain the arch relationship while the face grows vertically.
Table 9.1
| Characteristic | Measurement | Developmental changes |
| Arch length | Perpendicular distance from 1/1 contact point to a line contacting the distal surfaces of e/e or 5/5 | Maxilla: slight increase 6–10 years; followed by a 1–2 mm decrease Mandible: no increase 6–10 years; at 10–17 years, 1–2 mm decrease |
| Arch circumference | Line drawn through the buccal cusps and incisal edges of the teeth from the distal surface of e/e or 5/5 | Maxilla: ~1 mm increase in male; ~0.5 mm increase in female Mandible: ~3.5 mm decrease in male; ~4 mm decrease in female |
| Intercanine width | Distance between the cusp tips of c/c or 3/3 | Maxilla: ~1–2 mm increase from 3–6 years; ~3.5 mm increase from 6–12 years Mandible: ~1–2 mm increase from 3–6 years; ~3 mm increase from 6–10 years |
| Arch width | Distance from the palatal/lingual cusps of second primary molars or 5 | Maxilla: ~2–3 mm increase from 3–18 years; greater in males than females Mandible: ~3.6 mm increase from 3–18 years in both males and females |
The permanent lower incisors develop lingual to their predecessors and are frequently misaligned on eruption, but this usually resolves with intercanine growth. The upper anterior teeth develop palatal to their primary predecessors and are accommodated:
• by the existing spacing in the arch
• by erupting downwards and slightly forward so that they are placed on a wider arc
• by a small increase in intercanine distance (see Table 9.1).
The upper permanent lateral incisors usually move distally and labially with eruption of the central incisors, but they may be trapped palatally in crowded arches. The upper central incisors are often distally inclined when they first appear. An associated diastema tends to reduce as the lateral incisors erupt. At this time, the upper central and, to a greater extent, the lateral incisors are divergent, the latter because of pressure on their roots from the unerupted canines; this has been referred to as the ‘ugly duckling’ phase of dental development, terminology that is best avoided in the company of concerned parents.
The maxillary canines migrate from their palatal developmental position to lie labially and distally above the roots of the lateral incisors, leading to approximation of the incisor crowns as they erupt.
The combined mesiodistal widths of the primary canines and molars in each quadrant are slightly greater than those of the permanent canines and premolars. This difference in dimension is known as the ‘leeway space’ and is about 1 mm in the upper arch and 2.5 mm in the lower arch. The larger leeway space in the lower arch, probably in combination with mandibular growth, allows greater forward movement of the lower first permanent molar, converting a ‘flush terminal plane’ relationship of the primary molars to a class I occlusion (see below).
Six features (keys) of a good (‘ideal’) permanent occlusion have been described by Andrews:
• Molar relationship: the mesiobuccal cusp of the upper first molar lies in the groove between the mesiobuccal and middle cusp of the lower first molar; the distal surface of the distobuccal cusp of the upper first molar contacts the mesial surface of the mesiobuccal cusp of the lower second molar; the mesiolingual cusp of the upper first molar occludes in the central fossa of the lower first molar.
• Crown angulation: mesial for all teeth.
• Crown inclination: labially for incisors; lingually for canines through molars.
In addition, the following functional occlusal relations should exist:
Maturational changes in the occlusion
The occlusion of any child must be seen as dynamic and responding to changes in the facial skeleton. As the face continues to grow throughout the late teens and into adulthood, changes in the dentition and occlusion follow:
• There is an increase in lower incisor crowding. This has been observed even in children with previously well aligned, spaced arches and can be regarded as normal. Factors implicated in its aetiology are listed in Table 9.2.
Table 9.2
Factors implicated in late lower incisor crowding∗
| Factors | |
| Skeletal | Increase in mandibular prognathism Mandibular growth rotations Minimal forward maxillary growth |
| Soft tissue | Increase in soft tissue tone of lips and cheeks Trans-septal fibre contraction |
| Dental/occlusal | Lack of approximal attrition Dento-alveolar disproportion Tooth size Mesial drift secondary to anterior component of occlusal force, eruptive force of third molars Uprighting of posterior teeth in response to increase in lower facial height Third molars prevent posterior teeth shifting distally relative to the mandibular body in late mandibular growth |
• The interincisal angle increases, with uprighting of the incisors.
• There is a tendency for the overbite to reduce.
• A slight increase occurs in mandibular prognathism in males; in females there is a slight increase in mandibular retrusion.
9.2 Malocclusion: classification and aetiology
Malocclusion is an unacceptable deviation either aesthetically and/or functionally from the ideal occlusion. Prevalence of malocclusion varies with age and racial origin as well as according to the assessment methods, but not all malocclusion requires treatment.
Classification of malocclusion
Angle’s classification: Angle’s classification is based on the first permanent molar relationship (Fig. 9.3).
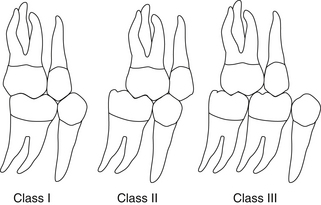
Class I (also referred to as neutrocclusion). The mesiobuccal cusp of the upper first permanent molar occludes in the buccal groove of the lower first permanent molar. Discrepancies no greater than half a cusp width were also regarded as class I by Angle.
Class II (also referred to as postnormal occlusion or distocclusion). The mesiobuccal cusp of the upper first permanent molar occludes anterior to the buccal groove of the lower first permanent molar.
Class III (also referred to as prenormal occlusion or mesiocclusion). The mesiobuccal cusp of the upper first permanent molar occludes posterior to the buccal groove of the lower first permanent molar.
Angle believed that the anteroposterior dental base relationship could be assessed reliably from the first permanent molar relationship, as its position, he maintained, remained constant following eruption. As this tenet is incorrect and difficulties arise in classification where mesial drift or loss of a first permanent molar has occurred, other classification systems are now used to categorise the anteroposterior dental base relationship.
British Standards Institute classification: The British Standards Institute classification relates to the incisor relationship (Fig. 9.4).
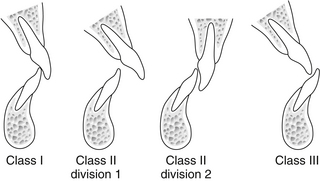
Class I. The lower incisor edges occlude with, or lie immediately below, the cingulum plateau (middle third of the palatal surface) of the upper central incisors.
Class II. The lower incisor edges lie posterior to the cingulum plateau of the upper incisors.
Division 1. The upper central incisors are proclined or of average inclination and there is an increase in overjet.
Division 2. The upper central incisors are retroclined; the overjet is usually minimal but may be increased.
Class III. The lower incisor edges lie anterior to the cingulum plateau of the upper incisors. The overjet is reduced or reversed.
Classification to assess treatment need and treatment outcome
Index of Orthodontic Treatment Need (IOTN): The IOTN was developed to help to identify those malocclusions most likely to benefit in dental health and appearance from orthodontic treatment. It comprises two components.
The dental health component: Malocclusion is categorised into five grades (Table 9.3) based on the severity of occlusal characteristics that could increase the morbidity of the dentition and impair function. Grading, in relation to treatment need, is according to the single worst feature of a malocclusion.
Table 9.3
The Index of Orthodontic Treatment Need: dental health component
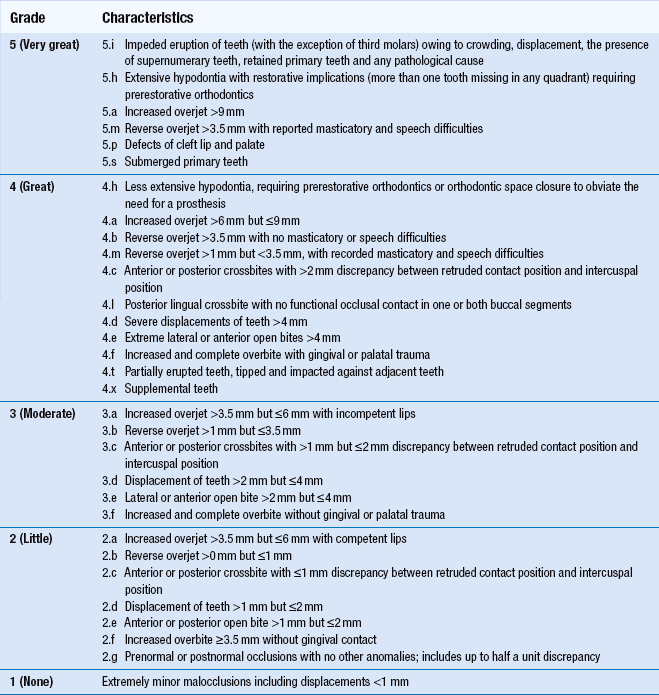
Reprinted from Brook P.H. and Shaw W.C., The development of orthodontic treatment priority, European Journal of Orthodontics, 1989, 11(3): 309-320, by permission of Oxford University Press
Table 9.4
Definition of commonly used cephalometric points and planes (Fig. 9.11)
| Points and planes | Definition |
| S | sella: midpoint of sella turcica |
| N | nasion: most anterior point of the frontonasal suture (may use the deepest point at the junction of the frontal and nasal bones instead) |
| P | porion: uppermost, outermost point on the bony external auditory meatus (upper border of the condylar head is at the same level, which helps location) |
| O | orbitale: most inferior anterior point on the margin of the orbit (use average of the left and right orbital shadows) |
| ANS | tip of the anterior nasal spine |
| PNS | tip of the posterior nasal spine (pterygomaxillary fissure is directly above, which helps location) |
| A | A point: most posterior point of the concavity on the anterior surface of the premaxilla in the midline below ANS |
| B | B point: most posterior point of the concavity on the anterior surface of the mandible in the midline above pogonion |
| Pog | pogonion: most anterior point on the bony chin |
| Me | menton: lowermost point on mandibular symphysis in the midline |
| Go | gonion: most posteroinferior point at the angle of the mandible (bisect the angle between tangent to the posterior ramus and inferior body of the mandible to locate) |
| S–N line | line drawn through S and N |
| Frankfort plane | line connecting porion and orbitale |
| Maxillary plane | line joining PNS and ANS |
| Mandibular plane | line joining Go to Me |
| Functional occlusal plane | line drawn between the cusp tips of the first permanent molars and premolars/primary molars |
To facilitate the grading process, a ruler (Fig. 9.5) has been developed. Occlusal features are assessed in the following order:

Fig. 9.5 The IOTN ruler (not drawn to scale).
Occlusal features are assessed in the order given by the acronym MOCDO. M = missing teeth; O = overjet; C = crossbite; D = displacement of contact point (i.e. crowding); O = overbite. (Reproduced by kind permission of Ortho-Care (UK) Ltd.)
The order above gives rise to the acronym MOCDO. With practice, it is possible to ascribe reliably and easily the treatment need category to a given malocclusion.
The aesthetic component: The aesthetic component of the IOTN (Fig. 9.6) consists of a set of ten photographs of anterior teeth in occlusion with increasing aesthetic impairment. These comprise class I and class II malocclusions; class III malocclusion and anterior open bite are not represented. Depending on whether the assessment is made clinically or from study models (with the anterior teeth in occlusion), colour or black and white photographs are used respectively. To categorise the treatment need, a score is given by selecting the photograph thought to be of an equal aesthetic handicap (and likely psychological impact on the patient), but judgement is very subjective. For this reason, treatment need tends to be based primarily on the dental health component of IOTN.
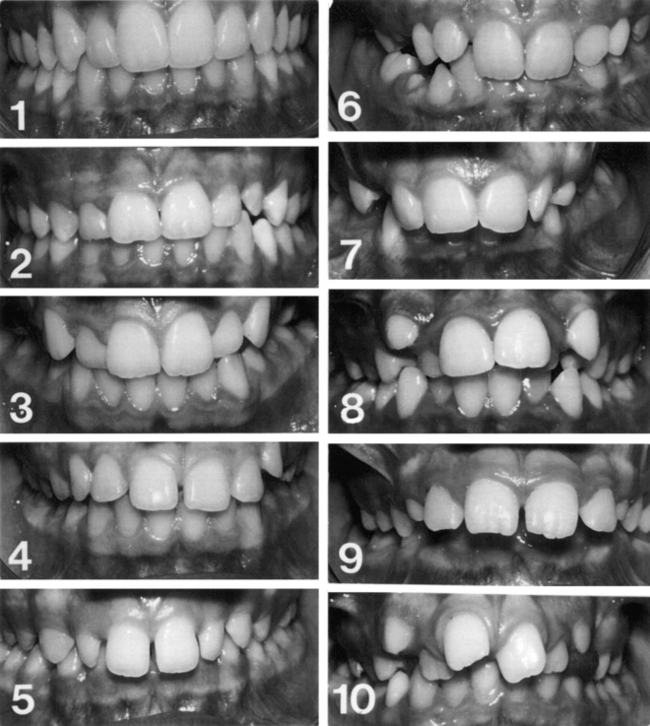
Fig. 9.6 The aesthetic component of the IOTN.
The need for treatment is categorised by subjective judgement based on the photographs: Score 1 or 2 = no need; 3 or 4 = slight need; 5–7 = moderate/borderline need; 8–10 = definite need. The Aesthetic Component was originally described as “SCAN” and was reprinted from Evans, R., and Shaw, W., Preliminary evaluation of an illustrated scale for rating dental attractiveness, European Journal of Orthodontics, 1987, 9(4):314-318, by permission of Oxford University Press
To assess treatment outcome: Assessment can be carried out objectively by applying the dental health component of IOTN and subjectively by application of the aesthetic component. In addition, the Peer Assessment Rating (PAR) may be recorded. A score is given to the pre- and post-treatment occlusion from the study models. The components and their weightings (by which the score is multiplied) are: crowding (×1), buccal segment relationship in anteroposterior, vertical and lateral planes (×1), overjet (×6), overbite (×2) and centrelines (×4). Measurement is facilitated by use of a specially designed ruler.
The percentage change in PAR score, obtained from the difference in pre- and post-treatment scores, is a measure of treatment success. A reduction of greater than 70% indicates a ‘greatly improved’ occlusion while a ‘worse/no different’ assignment is indicated by less than or equal to 30%.
To assess treatment need and complexity of treatment: In recent years, a new index, the Index of Complexity, Outcome and Need (ICON), has been developed. This incorporates scores for: the aesthetic component of IOTN (x7); upper arch crowding/spacing (x5); crossbite (x5); overbite/open bite (x4) and buccal segment relationship (x3). To indicate the improvement grade which reflects the outcome of treatment, 4× the post-treatment score is subtracted from the pretreatment score (intended to reflect need for and likely complexity of treatment).
Aetiology of malocclusion
A general overview of the aetiology of malocclusion is presented here while specific aspects related to the aetiology of each malocclusion type are considered in Chapter 10.
The aetiology of malocclusion is often the result of several interacting factors. These are principally genetic and environmental, although the precise role of inherited factors is not fully understood. Whereas the craniofacial dimensions and both size and number of teeth are largely determined genetically, the dental arch dimensions are influenced more by environmental factors.
Specific congenital defects with a genetic basis, which involve the maxilla or mandible, are rare, as is malocclusion caused primarily by trauma or pathology.
Skeletal problems
The majority of anteroposterior skeletal problems are caused by inherited jaw proportions, which are strongly genetically determined. Inherited characteristics (e.g. mandibular deficiency) account for almost all of moderate class II malocclusion, while the added insult of environmental soft tissue influences is likely in more severe cases. For class III malocclusion, mandibular prognathism has a strong racial and familial tendency although mandibular posturing, possibly caused by tongue or pharyngeal size, may stimulate growth and influence jaw size secondarily. Maxillary deficiency is also most likely due to inherited jaw dimensions and a simple environmental factor seems unlikely, but its exact aetiology is almost completely unidentified.
Vertical jaw proportions are also inherited, but soft tissue postural effects (e.g. anterior tongue position or mandibular postural changes induced by partial nasal obstruction) may contribute in particular to anterior open bite. Other environmental influences, such as a high lower lip line, may contribute to deep overbite.
A unilateral crossbite with displacement is often caused by a functional alteration, but it is usual for a skeletal crossbite to have an additional genetic input.
Crowding
Crowding is the most common orthodontic problem and is caused in part by a reduction in jaw and tooth size over the centuries. Interpopulation breeding has also been implied as arch width is influenced by jaw size, which is under tight genetic control.
Environmental influences, for example early loss of primary teeth due to caries or trauma or a digit-sucking habit, may also be instrumental in the aetiology of crowding. Also implicated is a softer, less abrasive modern diet which results in less interproximal tooth wear and less demands on jaw function; the latter may have added to a general tendency for smaller jaw size which was already happening. Soft tissue pressure of sufficient duration (more than 6 hours per day) in combination with the developmental tooth position may be responsible for a localised crossbite or malalignment.
9.3 Patient assessment in orthodontics
Orthodontic diagnosis consists of a list of all aspects that deviate from normal in relation to a particular occlusion. It is a prelude to treatment planning as it allows the relationship between the various factors and their likely impact on treatment and prognosis to be considered. Diagnosis is based on the accurate gathering of information about the patient from a logical case assessment.
Assessment
Timing: At 7–8 years, an assessment of the developing occlusion should be undertaken to note, in particular, the form, position and presence of the permanent incisors and to plan appropriate intervention should an abnormality be detected that is likely to interfere with the normal eruption sequence. The prognosis of the first permanent molars should be assessed routinely from age 8 years, and palpation of the maxillary permanent canines is carried out on a regular basis from about 10 years. Early detection of a skeletal discrepancy will allow also for optimal timing of treatment to maximise growth potential but, in most children, assessment is delayed until the permanent dentition has erupted.
All general dentists should be able to carry out a basic orthodontic assessment for their patients and recognise when referral to a specialist is appropriate. When dental and/or occlusal development deviates from normal, or when significant discrepancies in established dentofacial or occlusal relationships concern the patient and may compromise dental health over the long term, referral is indicated.
Apart from basic personal details, including relevant history with regard to medical, dental and social factors, the referral letter should give a brief summary of the salient features of the malocclusion incorporating the incisor and molar classifications (see Section 9.2). It should also include specific reference to:
• the patient’s perception of the problem
• the level of dental awareness including that of the parents (if appropriate)
Any recent radiographs should be forwarded with the referral. Study models are also of great assistance with treatment planning.
Demand for treatment: The demand for orthodontic treatment is influenced by two main factors:
• Patient/parent factors, which include patient gender, age, level of self-esteem, self- and peer-perception of any occlusal or skeletal discrepancy, social class and parental desires.
• Awareness by dental professionals and the health care system.
In general, demand for treatment is greatest when the orthodontist:population and orthodontist:general dentist ratios are small. Overall demand is increasing in adults, is higher in females, in those from better socioeconomic backgrounds and when a lower orthodontist:population ratio exists, as appliances become more common and their acceptance increases.
Initially the dentist must identify:
It is important to document whether the patient is unconcerned with the appearance of their teeth, particularly in the presence of obvious malocclusion, as any attempt to persuade the patient to undertake treatment is likely to be met with indifference. Attitude to treatment is best assessed from response to enquiries about their perception of orthodontic treatment for their peers, and by observing carefully their reaction when shown photographs or examples of appliances. Adults usually have a high level of dental awareness, are able to specify their concerns and motivation is high for treatment.
Medical history
A health questionnaire should be completed by each patient or a parent, and the findings verified by a clinical interview. Several medical conditions may impact on orthodontic treatment. Some are given below; where any uncertainty exists, liaison with the relevant medical specialist(s) is required.
Rheumatic fever/congenital cardiac defects: It is wise to consult the patient’s cardiologist to ascertain the need for antibiotic prophylaxis.
Recurrent oral ulceration: Appliance therapy should be avoided until this condition has been investigated thoroughly. Depending on the frequency and nature of ulceration, limited appliance treatment may be possible.
Epilepsy: Due to the risk of airway obstruction from appliance parts fractured during an epileptic attack and the difficulty with tooth movement in the presence of gingival hyperplasia, no orthodontic appliance should be fitted until the epilepsy is well controlled and the gingival condition healthy.
Diabetes: Patients with diabetes are more prone to periodontal breakdown, and active appliance therapy should be withheld until the periodontal condition is sound and the diabetes is stabilised.
Hay fever: Hay fever may interfere with the wearing of functional appliances over the summer months. An alternative approach to treating the malocclusion may be sought.
Nickel allergies: In patients with a confirmed severe hypersensitivity to nickel, nickel-free brackets and wires should be used; in some cases, clear aligner therapy may be considered as an alternative.
Latex allergy: Latex-free gloves, elastomeric separators, modules/chain, intraoral elastics and headgear components should be used.
Bleeding diatheses: If extractions are necessary, special medical arrangements will need to be in place.
Severe physical/mental handicap: In selected patients, extractions only may produce an improvement in dental aesthetics and facilitate tooth-cleaning measures. Appliance therapy is invariably not a viable option.
Arthritis or osteoporosis: Because juvenile or adult-onset rheumatoid arthritis often requires management with chronic steroid administration, lengthy orthodontic treatment is inadvisable due to the increased possibility of periodontal problems arising.
Oral doses of prostaglandin inhibitors or resorption-inhibiting agents (bisphosphonates) may be administered to adults being treated for arthritis or osteoporosis respectively; tooth movement may be affected. Orthodontic treatment and extractions are contraindicated if bisphosphonates are given intravenously due to the osteonecrosis risk.
Dental history
The nature, extent and frequency of previous dental treatment together with the level of patient co-operation should be recorded, along with details of daily oral hygiene practices. A history of early loss of primary teeth or of incisor trauma should be noted. If orthodontic treatment has been carried out previously, details relating to extractions and appliance type should be recorded. If treatment was abandoned, the patient must be questioned carefully for the reasons.
Clinical examination
Before the child patient takes a seat in the dental chair, it is often worthwhile to attempt to estimate their chronological age from their height and general level of physical maturity. This may give some indication of future growth potential. If the patient is accompanied by a parent, obvious familial malocclusion traits may be observed. The purpose of the clinical examination is to assess and record facial, dental, occlusal and related functional aspects of a patient in order to request appropriate diagnostic aids. An extraoral followed by an intraoral examination should be performed.
Extraoral examination
The skeletal pattern, soft tissues of the lips, tongue position during swallowing, speech, temporomandibular joints and mandibular path of closure should be assessed and the presence of any habits noted.
The relationship of the mandible to the maxilla should be assessed in all three planes of space: anteroposteriorly, vertically and laterally. Before proceeding, it is important to ensure that:
• the patient is seated upright with the head in the natural postural position or with the Frankfort plane (a line joining the upper border of the external auditory meatus to the inferior aspect of the bony orbit) horizontal; natural head posture may be obtained by asking the patient to look straight ahead focusing on the horizon
Anteroposterior plane: The relationship of the mandible to the maxilla in the anteroposterior plane is assessed by observing the patient in profile. In most cases, an indication of the skeletal pattern in this dimension may be gained from the soft tissue facial profile, allowing the following classification to be made (Fig. 9.7).
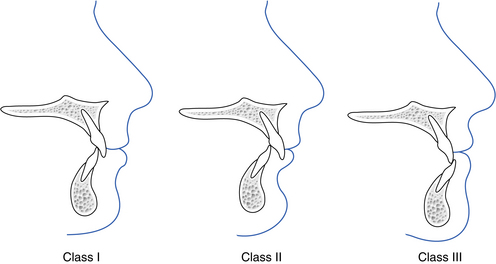
Class I: the mandible lies 2–3 mm behind the maxilla.
Class II: the mandible is retruded in relation to the maxilla.
Class III: the mandible is protruded in relation to the maxilla.
No indication, however, is given as to where a skeletal discrepancy may lie as the classification reflects solely the position of the mandible and the maxilla relative to each other.
This method is not always reliable because of variation in lip thickness, and palpation of the alveolar bases over the apices of the upper and lower incisors in the midline has been claimed to give a better estimate of skeletal pattern. In essence, any significant discrepancy in the anteroposterior dental base relationship should be investigated more thoroughly by taking and analysing a lateral cephalometric film (see below).
Vertical plane: Two assessments of the vertical relationship of the face should be made (Fig. 9.8).
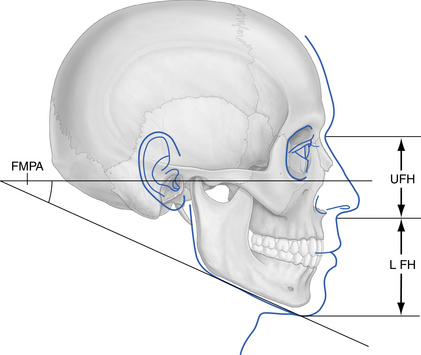
Fig. 9.8 Assessment of the vertical facial relationships.
Lower facial height (LFH) compared with upper facial height (UFH) and Frankfort–mandibular planes angle (FMPA).
Assessment of lower facial height: In a well-balanced face, the upper facial height (distance from the mid-eyebrow level to the base of the nose) should be equal to that of the lower facial height (base of the nose to the inferior aspect of the chin). The lower facial height may, therefore, be assessed as average (when these measurements are equal), reduced (when lower facial height is less than upper facial height) or increased (when lower facial height is greater than upper facial height).
Assessment of the Frankfort–mandibular planes angle (FMPA): With one hand, or the handle of a dental mirror, along the inferior aspect of the mandible and another hand along the Frankfort plane, these two lines can be projected backward in the imagination to give an estimate of the FMPA. Where the vertical dimensions of the face are normal, both lines should meet at the back of the skull (occiput) and the FMPA is regarded as average. If the FMPA is reduced, the lines will meet beyond the occiput and, if the FMPA is increased, they will meet anterior to it.
Transverse plane: Obvious facial asymmetry may be assessed first from in front of the patient and then, if present, by standing directly behind the patient and looking down across the face, checking the coincidence of the midlines of the nose, upper and lower lips and midpoint of the chin. In most people, some degree of facial asymmetry is present and may be regarded as normal. Marked asymmetries, however, require further investigation. The location and extent of any marked asymmetry (e.g. upper, middle or lower facial third) should be recorded.
Soft tissues of the lips and tongue: Eight aspects should be assessed in relation to the lips and tongue:
• Lip form and fullness: form may be described as vertical, average or everted, and fullness in terms of whether the lips are full or thin.
• Lower lip position in relation to the upper incisors: the upper incisors may lie behind, on, or in front of the lower lip.
• Lower lip coverage in relation to the upper incisors: at rest, on average, the lower lip should cover at least one-third to one-half of the upper incisor teeth.
• Upper lip level in relation to the upper incisors: the length of the upper lip and amount of exposure of the upper incisors at rest should be assessed; in males 1–2 mm display of the incisors is average, with slightly more in females.
• Whether the lips are together (competent) or apart (incompetent) at rest: if lips are apart, it should be noted if they are slightly or wide apart, and if the patient makes any habitual effort to hold them together; markedly incompetent lips confer a poor prospect for stability of a corrected overjet in patients with class II division 1 malocclusion.
• Tongue position at rest: should be assessed throughout the examination and particular note made if it lies in contact with the lower lip as this is likely to contribute to an incomplete overbite.
• Lip and tongue behaviour during swallowing and speech: abnormal tongue activity on swallowing, or marked hyperactivity of the lower lip, should be noted.
• Attractiveness of the smile. An attractive smile has the following components: visibility of the full crown length of the upper incisors and related interproximal gingivae; the curvature of the upper incisors, matches but does not touch, the lower lip; the smile extends laterally to include the upper first premolars but it should be borne in mind that the width of the upper dental arch on smiling should be in proportion to that of the mid-face.
Speech: Obvious defects such as a lisp will be noticed during general questioning of the patient, and specific assessment by a speech therapist is rarely indicated in patients referred for orthodontic advice.
Habits: The tell-tale signs of finger- or digit-sucking habits are generally easy to ascertain:
• Proclination of maxillary incisors.
• Retroclination of mandibular incisors.
• Incomplete overbite or open bite, often asymmetric.
• Tendency to bilateral buccal segment crossbite, often resulting in a unilateral crossbite with displacement.
Effects vary depending on whether the finger or thumb is placed in a median or paramedian position and on whether one or more digits are sucked. An adaptive tongue thrust is common. Inspection of the hands will usually identify the offender. The patient and parent should be made aware of the effects of the habit on the dentition and occlusion. Note also if the patient is a nail biter or bruxist.
Temporomandibular joints: Opening and lateral mandibular movements should be assessed by first observing the patient from in front and, second, by palpation of the condylar heads while listening for the presence of crepitus, or a joint click. Normal findings should be recorded as a baseline for future reference. Palpation of the masticatory muscles is not required unless symptoms are present.
Mandibular path of closure: The path of closure from rest position to maximum interdigitation should be assessed, noting any anterior or lateral mandibular displacement. This may be difficult to detect in a young and anxious patient where a habitual posture has developed to avoid a premature contact, often from an instanding incisor. Applying gentle backward and upward pressure to the chin while instructing the patient to touch the back of the mouth with the tip of the tongue usually gets around this problem.
Intraoral examination
The soft tissues of the buccal mucosa, floor of the mouth, tongue and the attachment of the maxillary labial frenum should be observed and any abnormality noted. A general dental examination should be carried out prior to assessing the individual arches of teeth and the occlusal relationships. The following should be charted:
• Standard of oral hygiene and caries rate.
• Gingival condition, paying particular attention to any area of gingival recession or attachment loss.
• All erupted teeth, noting those with abnormal shape or size. A quick way to assess if an anterior tooth-size discrepancy exists is to compare the mesiodistal widths of the upper and lower lateral incisors. The upper laterals should be larger than the lower incisors, but only discrepancies of greater than 1.5 mm should be recorded as these are likely to affect treatment planning.
• Teeth with untreated caries, hypoplasia, large restorations or previous trauma. The condition of the first permanent molars should be examined, in particular, and a record made of any cervical decalcification (buccally on the uppers or lingually on the lowers), or large areas of hypoplasia, which may indicate a poor prognosis.
• The presence of erosion on the palatal surfaces of the upper incisors. In these cases, the patient should be questioned about frequency of dietary intake of acidic or carbonated drinks.
• Marked attrition of the dentition. This is likely to be present in individuals with a bruxing habit.
The lower arch followed by the upper arch should then be assessed independently.
Assessment of the upper and lower arches:
Symmetry and overall alignment: Include here the presence of rotations (classified by the surface furthest from the line of the arch).
Angulation of the lower labial segment to the mandibular plane: By placing the index finger of the right hand along the mandibular body and gently everting the lower lip, the angulation of the lower incisors may be assessed as average (if they appear to make almost a 90° angle with the mandibular plane), retroclined or proclined.
Inclination of the canines: These may be described as upright, mesially inclined or distally inclined.
Presence and site of spacing or crowding including the magnitude of each: The degree of spacing/crowding may be assessed by performing a space analysis on the study models. This only takes account of any space discrepancy anterior to the first permanent molars and is usually carried out as described below.
For each quadrant: Measure with dividers the distance from the mesial surface of the first permanent molar to the distal surface of the permanent lateral incisor, and from there to the midline. Add these measurements for each arch to give the space available.
Measure the mesiodistal width of each tooth and add these together to calculate the space required. Where the canines and premolars have not erupted, on average 21 mm in each lower quadrant and 22 mm per quadrant in the upper arch is an estimate of their space requirements.
Assessments with the teeth in occlusion: With the teeth in maximum intercuspation, the remaining aspects should be recorded.
Incisor relationship: This may be categorised according to the British Standards Institute classification (see Section 9.2).
Overjet (the horizontal overlap of the upper over the lower incisors): This is usually measured (in millimetres) from the mesial of the upper central incisors to the lower incisors. If there is a marked difference for each upper central incisor, both measurements should be noted.
Overbite (vertical overlap of the upper over the lower incisors): This is measured (in millimetres) – an indication should be given as to whether it is complete, incomplete or if there is an anterior open bite or traumatic overbite. The overbite is complete when the lower incisors occlude with the opposing maxillary teeth or with the palatal mucosa; it is incomplete if there is no contact with the opposing surfaces. The extent (in millimetres) of an anterior open bite should be noted and the site of mucosal ulceration recorded (either palatal to the upper incisors, labial to the lower incisors or in both locations) in the presence of a traumatic overbite.
Centrelines: Upper and lower centrelines should be coincident with the midline of the face and in line with each other; any centreline shift should be recorded (in millimetres) with a note to indicate the direction of the shift.
Molar relationship: Providing a corresponding molar is present in the opposing arch, the molar relationship may be categorised according to Angle’s classification (see Section 9.2).
Where the first permanent molar is missing in either arch, the premolar or canine relationship may be assessed.
Canine relationship: This should be recorded in addition to the molar relationship, as although they are often the same, on occasion discrepancies are present.
The presence of anterior or posterior crossbite (bucco-lingual discrepancy in arch relationship): Is the crossbite buccal or lingual, bilateral or unilateral (Fig. 9.9)? For the premolar and/or molar teeth, a buccal crossbite exists when the buccal cusps of the lower tooth occlude buccally to the buccal cusps of the upper teeth. A lingual crossbite exists when the buccal cusps of the lower tooth occlude lingually to the palatal cusps of the upper teeth. A unilateral crossbite affects teeth on one side of the arch while teeth on both sides of the arch are affected with a bilateral crossbite. Often a unilateral crossbite is associated with a mandibular displacement (Fig. 9.10).
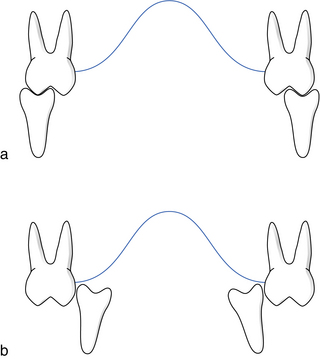
Fig. 9.9 Buccolingual discrepancies.
(a) Bilateral buccal crossbite. (b) Bilateral lingual crossbite.

Special investigations
Sensibility tests: Traumatised incisors or other teeth with suspect vitality should be sensibility tested, the most accurate of which is probably electric pulp testing, and their status recorded.
Radiography – conventional or digital: All radiographs should be justified on clinical grounds. Radiographs forwarded by a referring practitioner may provide sufficient information to supplement the clinical findings but often the following views are needed.
An orthopantomographic radiograph or right and left lateral oblique views: These are good screening radiographs. The bony architecture of the maxillary and mandibular bases as well as that of the mandibular condyles (if included) should be checked first to exclude any dentally-related, or other, pathology. All teeth should be identified and counted. It is a good routine to start in one area (e.g. upper right third molar area) and follow systematically through the upper left, lower left and finally lower right quadrants to ensure that nothing is missed. Then the condition of each tooth should be checked for caries, hypoplasia or resorption. All unerupted teeth should be charted, noting their developmental stage and position. Teeth previously extracted, those congenitally absent and any pathology should be recorded. Although large carious lesions will be obvious on a panoramic film, a more thorough assessment should be made from bitewing or periapical films if required.
Cephalometric analysis
Cephalometric analysis involves the evaluation and subsequent interpretation of both lateral and posteroanterior views of the skull although, in practice, it is usually confined to the former because of difficulty in interpreting the posteroanterior view.
To allow comparison of measurements recorded for the same patient at different times, or between patients, attempts have been made to standardise the radiographic technique. Originally developed by Broadbent and Hofrath independently in 1931, the radiograph is taken with the Frankfort plane horizontal, the ear posts positioned in the external auditory meati and the teeth in centric occlusion. The central ray should pass through the ear posts. Importantly, the X-ray source to midsagittal plane distance and the midsagittal plane-to-film distance should be standardised to facilitate reproducibility and to minimise magnification (7–8%). To allow accurate calculation of magnification, a steel rule of known length should be placed at the midsagittal plane and recorded on each film.
It is now common practice to collimate the X-ray beam, thereby avoiding radiation exposure to areas of the head not required for lateral cephalometric analysis. To enhance the soft tissue profile, the beam intensity can be reduced by placing an aluminium filter between the X-ray source and the patient.
Uses of lateral cephalometric analysis
Lateral cephalometric analysis is used:
A diagnostic aid: Lateral cephalometric analysis sheds light on the dental and skeletal characteristics of a malocclusion, thereby allowing its aetiology to be determined and focusing attention on the aspects that require correction. It also serves as a useful reference of pretreatment incisor position, especially if anteroposterior movement is intended. In some patients, particularly those with class III skeletal bases, growth may be checked from serial radiographs and treatment considered at the appropriate time. Assessment of skeletal age, based on the characteristics of cervical vertebral maturation, has also been developed which indicates where an individual is with regard to the peak growth at adolescence. Unerupted teeth may also be located accurately, soft or hard tissue pathology identified and upper incisor root resorption observed.
A means of checking treatment progress: During treatment with fixed or functional appliances, it is customary to check incisor inclinations and anchorage considerations. Any change in the position of unerupted teeth may be checked also.
A means of assessing treatment and growth changes: If films are to be compared, they must be superimposed on some stable area or points. As orthodontic treatment is generally carried out during the growth period, no natural fixed points or planes exist. The following, however, are reasonably stable areas and are used commonly for superimposition:
• Cranial base: after 7 years of age, the anterior cranial base is found to be relatively stable. The S–N (sella–nasion) line is a close approximation to the anterior cranial base (N is not on the anterior cranial base), and holding at sella allows the general pattern of facial growth to be assessed; superimposition on de Coster’s line (the anatomical outline of the anterior cranial base) reflects more accurately changes in facial pattern but requires greater skill to carry out.
• Maxilla: superimposition on the anterior vault of the palate shows changes in maxillary tooth position.
• Mandible: changes in mandibular tooth position may be assessed by superimposition on Bjork’s structures. These are the inner cortex of the symphysis, the tip of the chin, the mandibular canal outline and the third molar tooth germ before root development.
Aim and objective of cephalometric analysis
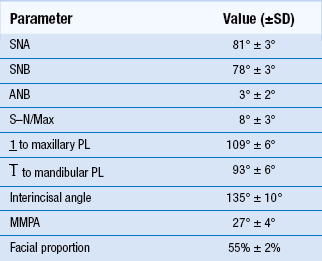
The aim of cephalometric analysis is to assess the anteroposterior and vertical relationships of the upper and lower teeth with supporting alveolar bone to their respective maxillary and mandibular bases, and to the cranial base. The objective is to compare the patient with normal population standards appropriate for his/her racial group, identifying any differences between the two. The technique used is outlined in Box 9.1.
It is important, however, to remember that irrespective of whether cephalometric measurements are made directly from a digitiser or indirectly from a tracing, the cephalometric technique and its subsequent analysis are open to error. The technique relies on reducing the three-dimensional facial skeleton to a two-dimensional X-ray film. Bilateral landmarks, therefore, are superimposed. The validity of the analysis depends upon the ability of the operator to identify points accurately and reproducibly, which in turn is dependent on the film quality and operator experience.
Cephalometric interpretation
The following aspects may be assessed from the cephalometric analysis.
Anteroposterior skeletal pattern:
ANB angle: This is determined by the difference between SNA and SNB (the relative positions of the maxilla and mandible to the cranial base respectively) and allows the following broad classification:
The ANB value should be considered along with the measurement for SNA, as ANB is affected by variation in the position of nasion. In cases where the SNA value is above or below the average value of 81° and provided the S–N/maxillary plane angle is within 8 ± 3°, a correction may be employed to the ANB value as follows: for every degree SNA is greater than 81°, substract 0.5° from the ANB value, and vice versa.
The Wits analysis: This is an alternative means of assessing the skeletal pattern in which the distance (in mm) is measured between perpendiculars from A and B point to the functional occlusal plane (a line joining the cusp tips of the permanent molars and premolars or primary molars). The average values for males and females are 1 ± 1.9 mm and 0 ± 1.77 mm, respectively. No indication is given, however, of the relation of the dental bases to the cranial base and the functional occlusal plane is difficult to locate. In some cases, however, it may be a useful check to complement that made from the ANB value.
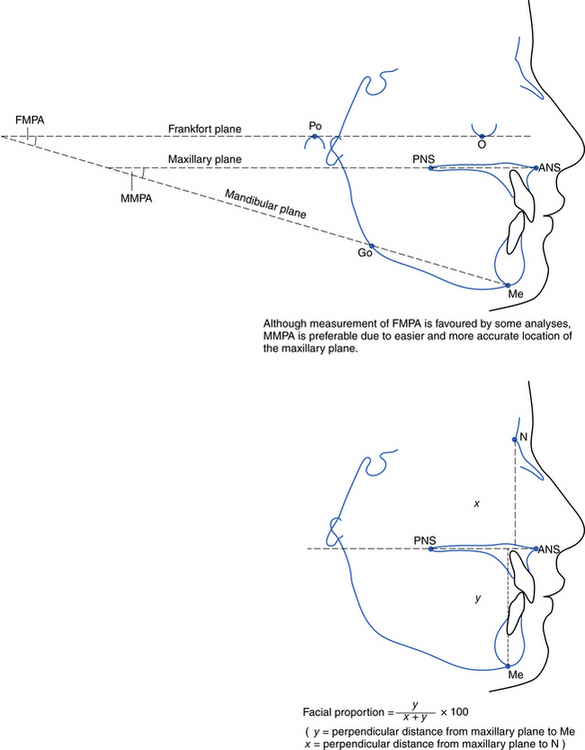
Vertical skeletal pattern (MMPA and facial proportion) (Fig. 9.12): Both anterior and posterior lower facial heights are considered in the MMPA whereas facial proportion assesses the contribution of lower anterior facial height to total facial height. The facial proportion should lend support to the value obtained for the MMPA; a reduced facial proportion is usually consistent with a low MMPA and vice versa. Where there is disagreement between these two assessments, the tracing should be checked to identify the cause.
Angle of the upper incisor to the maxillary plane: The mean value for this angle is 109 ± 6°; the incisors may be classified as retroclined or proclined relative to the mean value. In class II division 1, it is often helpful to carry out a ‘prognosis tracing’ to indicate if correction of the incisor relationship may be undertaken by tipping or bodily movement (Fig. 9.13). An alternative method is to apply the following rule of thumb: for every 1 mm of overjet reduction, subtract 2.5° from the upper incisor to maxillary plane angle. Provided the final upper incisor angulation is not likely to be less than 95° to the maxillary plane, tipping rather than bodily movement may be acceptable.
Angle of the lower incisor to the mandibular plane: This must be looked at in conjunction with the ANB and MMPA angles as the lower incisor angulation may compensate for discrepancies in the anteroposterior and vertical skeletal pattern. Under the influence of the soft tissues, the lower incisors may procline in class II malocclusion or retrocline in class III malocclusion. There is also an inverse relationship between the lower incisor angulation (LIA) and the MMPA: for every degree the LIA is greater than the average (93°), the MMPA is 1° less than the average (27°); the opposite holds true when the LIA is less than the average. Alternatively, the lower incisor angle is determined by subtracting the MMPA from 120°.
Lower incisor to A–pogonion line: This has been used as an aesthetic reference line for lower incisor positioning (average 0–2 mm) but it is unwise to lend too much credence to this measurement for treatment planning purposes. Both point A and pogonion may shift with treatment or growth, and orientating the lower incisors correctly with respect to the A–pogonion line does not improve the prospect of a stable result.
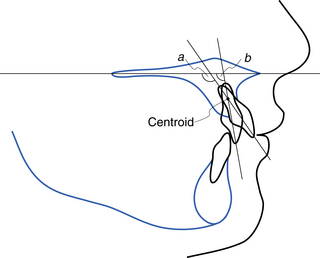
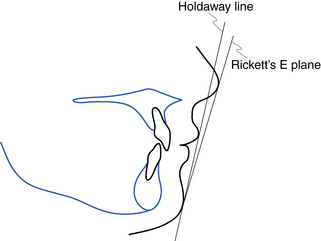
Analysis of soft tissues: Various reference lines, regarded as indicators of pleasing facial appearance, have been suggested to assess the relationship of the soft tissues of the nose, lips and chin. These lines are more helpful in orthognathic surgical planning than in planning conventional orthodontic treatment. Two lines are shown in Figure 9.14.
9.4 Principles of orthodontic treatment planning
Problem list and treatment need
The first stage in treatment planning is to summarise the features of a patient’s malocclusion to produce a problem list of the pathological and developmental (orthodontic) problems. Then the need for treatment on dental health and aesthetic grounds must be considered (see Section 9.2). Only if appliance therapy and/or extractions can confer significant benefit to dental health and/or appearance of the dentition should treatment be undertaken. If there is any doubt, treatment is best withheld.
Potential benefits and limitations of orthodontic treatment
Dental health and function: Overall, the oral health-related benefits of orthodontic treatment are rather limited.
Caries: No significant relationship has been found between dental caries experience and malocclusion. Orthodontic treatment could not be claimed to prevent caries.
Periodontal disease: In general, crowding is weakly associated with periodontal disease and improvement in oral hygiene techniques/motivation are more likely than orthodontic treatment to reduce susceptibility to periodontal disease. Where an occlusal relationship is causing periodontal trauma, e.g. displacing occlusal contacts leading to gingival recession and mobility in relation to an incisor crossbite or deep overbite producing palatal or labial gingival trauma, periodontal health is improved by corrective orthodontic treatment. Otherwise, in terms of long-term periodontal health, orthodontic treatment brings neither harm nor benefit.
Incisor trauma: The risk of trauma to the upper anterior teeth is twice as great when the overjet is increased more than 3 mm. Trauma is more common in boys and when the lips are incompetent. Early orthodontic treatment, however, has been shown not to affect the incidence of incisor trauma.
Tooth impaction: Unerupted teeth may cause resorption of the adjacent teeth or dentigerous cyst formation but these sequelae are rare. Supernumerary teeth may prevent eruption of the related permanent tooth/teeth.
Speech: Speech is a complex process involving mutual compensation between the contributing organs (brain, lips, tongue and laryngeal muscles) so drawing firm conclusions regarding the correlation between a speech disorder and malocclusion is difficult. No guarantee could be made that correction of malocclusion (e.g. severe class II or class III malocclusion or anterior open bite which may be associated with lisping) would improve a speech impediment.
Masticatory function: In those with marked anterior open bite, increased or reverse overjet, incising food may be difficult or even impossible.
Temporomandibular joint dysfunction syndrome (TMJDS): Research has linked, although weakly, crossbites, class III malocclusion, asymmetry, class II mandibular retrusion and open bite with TMJDS. Orthodontic treatment, with or without extractions, will not cure or cause TMJDS.
Social/psychological wellbeing: In adolescents presenting for treatment, quality of life and that of their parents are affected negatively by the presence of upper anterior spacing or increased overjet. Bullying has been significantly associated with an increased overjet but improved self-concept and reduction in negative experiences have been reported following correction in 8–10 year olds. Long-term longitudinal assessment in adulthood of orthodontic treatment undertaken during childhood indicated only limited positive impact on psychological health or quality of life. Furthermore, occlusal status in adulthood appears to have limited association with psychological factors and quality of life.
Summary: Dental health is likely to benefit long term where any of the following exist: impacted teeth with a risk of resorption, increased overjet, mandibular displacement in the presence of a crossbite and traumatic overbite. Psychosocial wellbeing/quality of life is also likely to improve with treatment in childhood of upper anterior spacing or an increased overjet. The impact of orthodontic treatment on long-term social/psychological wellbeing appears limited.
Limitations of orthodontic treatment
Orthodontic treatment, like all forms of dental treatment, has some limitations, and these should be borne in mind when the aims of treatment and treatment plan are being devised.
• Tooth movement is confined to cancellous bone.
• Limited differential eruption of anterior or posterior teeth may be used successfully to aid correction of malocclusion, but there is limited evidence on the permanency of any alteration in vertical skeletal pattern.
• Some small restraint or redirection of maxillary and/or mandibular growth is possible with headgear or functional appliance therapy; with rapid maxillary expansion, some orthopaedic increase in maxillary dental base width is possible.
• The effect of tooth movement on the facial profile is modest, with the growth of the nose and chin having a greater effect.
• Tooth movement is generally more efficient in a growing child but may still be undertaken in the adult.
• Growth may aid or hinder correction of a malocclusion and attempts to modify its expression, even though this is limited, may be considered on occasion in the early mixed dentition.
• Removable appliances tip teeth, whereas fixed appliances may bodily move, tip, intrude, extrude, rotate or torque teeth.
• Functional appliances alter arch relations through a combination of actions that involves tipping of teeth, differential eruption and possibly some restraint or stimulation of maxillary and/or mandibular growth, depending on the specifics of the design.
• Headgear restrains or redirects growth of the maxillary complex depending on the force magnitude and direction employed.
• Treatment success is dependent on:
• correct diagnosis, treatment planning including assessment of anchorage, and proficiency in whatever appliance system is selected on the part of the operator
• regular attendance, compliance with all instructions regarding appliance wear and maintenance of a high standard of oral hygiene by the patient
• a stable result is only possible if the forces from the soft tissues, occlusion and periodontium are in equilibrium and facial growth is favourable.
Aims of treatment
The aims of treatment lists in a logical sequence the steps required to achieve the final occlusal result. For example, in a patient with a class II division 1 malocclusion with moderate upper and lower arch crowding as well as a half unit class II molar relationship, these would often be as follows:
• Alignment within the arches.
• Closure of residual spacing and correction of molar relationship to class I.
One should always aim for the ideal plan initially but keep an open mind, as sometimes this plan may require alteration (e.g. if the patient does not wish to wear a fixed appliance or headgear). Importantly, where a compromise plan is proposed, the patient must benefit and not suffer long term.
Treatment planning
All pathological problems (e.g. caries and periodontal disease) must be addressed before any orthodontic treatment is considered. In broad terms, the following series of steps will be useful for treatment planning purposes in most malocclusions (refer to the sections covering management of each malocclusion).
Plan the lower arch
In general, the lower arch form is to be accepted, particularly the anteroposterior position of the lower labial segment, which lies in a narrow zone of balance between the lips and tongue. Movement beyond this narrow zone is likely to lead to an unstable result apart from in certain circumstances (where thumb sucking has retroclined the lower incisors, class II division 2 malocclusion, class III camouflage treatment and bimaxillary proclination); these invariably require specialist management. The general and local factors that govern the need for and choice of any extractions are described below.
Imagine the lower canine repositioned for alignment of the lower labial segment: If the canine is mesially inclined in a crowded arch, it will upright spontaneously following the extraction of a first premolar, thereby providing space for alignment of the lower labial segment. Most improvement occurs within the first 6 months following extraction, and if the premolars are removed as the canines are erupting. If the canine is upright or distally inclined, a fixed appliance will be necessary for its retraction.
Plan the upper arch
Mentally correct 3 position to a class I relationship with the aligned lower canine: This is done assuming that the lower labial segment is not spaced and that the upper incisor teeth are all of normal size and not retroclined. The space needed may come from extractions, arch expansion or distal movement of the buccal segment. Importantly, if all of an extraction space is required to achieve a class I canine relationship, anchorage will need to be reinforced. The appliance type needed to achieve the desired canine relationship can be assessed also.
Consideration should be given as well to relief of upper labial segment crowding, reduction of the overjet and/or overbite and the appliance type necessary to achieve correction.
Plan the final buccal segment relationship and the need for closure of any residual spaces
In most cases, if corresponding teeth have been extracted in each quadrant, the final buccal segment relationship should be class I; however, if only upper arch extractions or lower arch extractions have been undertaken, the final relationship will be class II or class III, respectively. The potential for spontaneous space closure depends on:
• the degree of initial crowding
• the vertical pattern of facial growth (space closure tends to occur more rapidly in patients with increased Frankfort–mandibular planes angle compared to those with a reduced angle).
Alternatively, space closure may be produced mechanically by applying intramaxillary (from within the same arch), intermaxillary (from the opposing arch) or extraoral traction.
Plan the mechanics and consider the anchorage demands
Removable appliances are limited to tipping movements, whereas bodily movement is possible with fixed appliances. Functional appliances are generally confined to correction of class II malocclusion in growing children and mostly produce tipping rather than bodily movement of teeth.
Tipping movements make only modest demands on the balance between the desired tooth movements and the space available (i.e. anchorage), whereas bodily movements place greater strain on anchorage. Where all the space available from extractions is required to relieve crowding, reduce an overjet or both, anchorage is at a premium and will need reinforcement.
Treatment timing
Intervention in the mixed dentition is advisable in some circumstances (Section 9.3). Certain orthodontic treatments rely on growth for success. For example, overbite reduction and functional appliance therapy and treatment is usually best started in the late mixed dentition. However, where a severe skeletal problem exists that is likely to be exacerbated by growth, treatment is best deferred until the late teens when a combined orthodontic/surgical approach can be considered.
Retention
A phase of retention is usually required following tooth movement with appliance therapy to allow consolidation of the new tooth positions through adaptation of the alveolar bone, gingival and periodontal tissues. Planning the retention phase of treatment requires an appraisal of the original features of the malocclusion as well as:
The likely retention regimen should be individualised for each patient, taking these factors into account, and must be explained to the patient before treatment starts. Specific guidelines in relation to retention are included in the management of each malocclusion type and appliance treatments (Section 11.4).
Final presentation
The final presentation should outline clearly the objectives of each stage of treatment in a form that is understandable to the patient and/or parent or guardian. If there is more than one plan possible, the ‘pros’ and ‘cons’ of each should be explained. Good colour photographs of any appliance to be used are very helpful. If anchorage reinforcement by headgear or temporary anchorage devices (TADs) is required, this must be explained. An outline of the likely appointment intervals and their length, together with an estimate of the overall duration of treatment and likely cost, is also necessary.
The need for maintenance of a high standard of oral hygiene as well as the importance of maintaining regular dental attendance for routine dental care throughout appliance treatment should be emphasised to the patient, together with the level of co-operation expected in relation to wear of intraoral elastics or specific appliance types, e.g. functional appliance or headgear. The potential risks of each treatment plan (e.g. root resorption, decalcification and alveolar bone loss) should be explained to the patient and parent or guardian, taking care to put them in context and not dramatise sequelae that are usually of minor significance (Table 9.6). If there is a risk attached to undertaking no treatment, this must also be highlighted.
Table 9.6
Risks of orthodontic treatment
| Risks | |
| Root resorption | 0.5–1 mm loss of root length common, but large individual variation Suggested risk factors are force magnitude and method of application, length of treatment, appliance type (more with fixed than removable appliances), history of trauma, previous root resorption, blunt or pipette-shaped roots Current evidence indicates heavy forces and comprehensive treatment with fixed appliances increase incidence and severity Previous trauma and unusual root shape unlikely causes |
| Decalcification | Greater risk with fixed than removable appliances Risk increases with poor oral hygiene and frequent intake of sugary foods/drinks |
| Periodontal disease | Palatal gingival inflammation common with removable appliances if oral hygiene poor Marginal gingivitis common with fixed appliances; tends to resolve on appliance removal Occasionally 1 mm loss of attachment and 0.25–0.5 mm loss of alveolar bone adjacent to extraction sites |
| Pulpal/soft tissue damage | Loss of pulpal vitality, particularly if overactivation of appliance and previous history of trauma Abrasion/ulceration of oral mucosa, more common with fixed than removable appliances |
| Temporomandibular joint dysfunction syndrome (TMJDS) | Orthodontic treatment with or without extractions is not a cause of TMJDS Stress often acts in conjunction with parafunction promoted by occlusal factors TMJDS associated with crossbites, class III malocclusion, open bite |
| Iatrogenic effects | Greater risk with inexperienced operator (e.g. anchorage loss, inappropriate treatment mechanics) |
Informed consent should then be obtained, although this may have to be deferred until a later date if the patient wishes time to consider the options presented. An information leaflet for the patient to take away is helpful.
Creating space for desired tooth movement
This entails evaluating the space required and space to be created during treatment; for the latter, the treatment aims need to be finalised. The following require space: relief of crowding; overbite reduction; overjet correction; centerline correction; contracting the arch width; adjusting incisor tip or torque. The mesiodistal width of the misaligned teeth compared to the space available in the arch allows the magnitude of crowding to be assessed and classified (see Section 9.3). Where the depth of the curve of Spee is 3 mm, 1 mm is required for correction; more space will be required where the curve is deeper. Each mm of overjet reduction requires 2 mm of space. Proclination of incisors will create space (2 mm for each mm of proclination). Space required for changes in incisor angulation or inclination are generally small.
Extractions
Extraction of teeth is required to provide space for either relief of crowding and/or to camouflage a class II or class III skeletal discrepancy. In general, to preserve symmetry, teeth are usually extracted from both sides of the same arch. The decision to extract teeth is governed by:
Profile considerations: Attempts to expand the arches anteroposteriorly to relieve crowding and improve facial aesthetics are unlikely to be inherently stable over the long term. Indeed, the extraction of premolars rather than second permanent molars may produce only 1–2 mm of retraction of the lips. Differences in lip thickness and growth pattern between individuals are likely to have greater bearing on the soft tissue profile than whether or not extractions are undertaken as part of treatment. However, where there is a marked class II skeletal discrepancy, retraction of the incisors is likely to produce a very unsatisfactory facial profile, and specialist advice should be sought.
Incisor relationships: In class I or class II, it is usual to extract at least as far forward in the upper arch as in the lower, but the opposite holds true in class III. Where the overbite is deep (curve of Spee 5 mm or more), about 2 mm of space will be required for its reduction. Centreline discrepancies require greater space on one side of the arch than on the other to facilitate correction. To camouflage a moderate class II or class III skeletal problem, extraction of only upper first or lower first premolars, respectively, may be indicated.
Appliance to be employed: In crowded mouths, extraction of the same tooth from each quadrant encourages mesial drift and spontaneous space closure, but the choice of extraction is not so critical if fixed appliances are to be used for correction of the malocclusion.
Anchorage requirements: Bodily movement of teeth, particularly apical torque, is more demanding on anchorage than tipping movement, so space near to the site of the intended tooth movement is desirable. In addition, the anchorage balance (best thought of in terms of the combined root surface area posterior and anterior to the extraction site) is unfavourable for aligning crowded incisors the further posterior in the arch extractions are undertaken.
The condition of the teeth: Teeth with poor long-term prognosis should be considered for extraction even if treatment is made more difficult or prolonged as a result.
Site of crowding: Crowding in one part of the arch is more easily corrected if extractions are carried out in, or close to, that part of the arch. This is not true for the incisor areas: extraction of an incisor is not usually undertaken for relief of crowding because of the poor appearance that would result. First premolars, located midway between the front and back of the arches, often provide space for relief of crowding in both locations, whereas second permanent molars may be extracted for crowding confined to the posterior regions.
Degree of crowding: In the mixed dentition, mild crowding may resolve with the leeway space, but after this stage has passed, appliance therapy to either expand the arches or to move the buccal segments distally will be required to provide space. Where space shortage is of the order of 4 mm per quadrant, it may be dealt with without extractions, but extractions will be warranted for more severe crowding.
Extraction of teeth in the buccal segment:
First premolars: These teeth are most commonly extracted for relief of moderate-to-severe crowding. Maximum spontaneous labial segment alignment is likely if first premolars are extracted as the canines are erupting, provided they are mesially inclined.
Second premolars: Extraction of these teeth is indicated in the following situations:
• Mild to moderate crowding, as the anchorage balance favours space closure by mesial movement of the molars; fixed appliances will be required for this.
• When the teeth are hypoplastic (usually as a result of an apical infection of the overlying second primary molar; Turner’s hypoplasia), carious or absent.
• In those in whom one or more second premolar is absent and crowding is mild to moderate, the second premolar may be extracted in the other quadrant(s), thereby balancing and/or compensating for the extractions; fixed appliances will be required to align the remaining teeth and close any residual spacing.
• One or more second premolar excluded from the arch either palatally or lingually following early loss of the second primary molar; the contact between the first permanent molar and the first premolars should be acceptable.
First permanent molars: See Section 10.1.
Second permanent molars: Extraction of lower second permanent molars may be considered for relief of slight premolar crowding or to compensate for upper second permanent molar extractions, being undertaken to facilitate distal movement of the buccal segments. First permanent molars must have a good prognosis. The best chance of providing space to disimpact a lower third molar successfully occurs when:

However, even when these criteria are met, the final position of  is unpredictable.
is unpredictable.
Extraction of teeth in the labial segment:
Lower incisors: Rarely extraction of a lower incisor produces an acceptable solution for crowded incisors. Crowding of three lower incisors may occur due to a reduction in the lower intercanine width and a tendency for the labial segment to move lingually. Fitting six upper anterior teeth around five lower anteriors may lead to a reduction in the upper intercanine width and upper labial segment crowding. Therefore, extraction of a lower incisor is usually best considered only in the following situations:
• Poor prognosis due to caries, trauma or gingival recession.
• Severe crowding with one incisor excluded from the arch.
• Distally inclined canines with fanning of the lower incisors.
• Mild class III malocclusion in an adult with aligned buccal segments.
• Class I buccal and incisor relationships with severe lower incisor crowding; here subsequent changes in arch dimensions are likely to be minimal.
• Tooth size discrepancy in the upper labial segment (i.e. small upper lateral incisors).
When extraction of a lower incisor is an option, it is wise to see what the final result is likely to be by carrying out a diagnostic set-up on a set of working casts. In each case, a lower fixed appliance is usually required to align and approximate the remaining teeth.
Upper incisors: A permanent central incisor is never a tooth of choice for extraction but may be considered if dilacerated or of poor prognosis due to trauma. Extraction of an upper lateral incisor is not recommended except in the following circumstances:
• 2 on opposite side of the arch absent or abnormally formed
The canine should be of good size, shape and colour to allow optimal dental aesthetics in the upper labial segment.
Lower canines: These should only be removed if the tooth is severely displaced or ectopic with good contact between first premolar and lateral incisor.
Upper canines: See Section 10.1.
Interproximal stripping
Using abrasive strips, 0.25 mm of enamel can be removed from each proximal surface of the anterior teeth to give 2 mm of space. An extra 3–6 mm is possible per arch through enamel removal from the buccal segment teeth using a high-speed handpiece; space should be created between the teeth before this is carried out and fluoride applied after all enamel removal.
Arch expansion (lateral or anteroposterior)
In the upper arch, treatment of a unilateral buccal segment crossbite with displacement may provide sufficient space (~0.5 mm per 1 mm of expansion) to obviate the need for extractions. In the absence of such a crossbite, lateral arch expansion is unlikely to be stable. Correction of a lingual crossbite by lower arch expansion is possible in some cases. For each mm of incisor proclination (anteroposterior arch expansion), ~2 mm of space is obtained in the arch.
Distal movement of the buccal segments
Space lost to unilateral mesial drift of the molars following early loss of primary teeth may be regained in the upper arch by use of a removable appliance with a screw and headgear support (Fig. 9.15). Bilateral distal movement of the upper buccal segments is possible in well-motivated individuals, requiring excellent co-operation, and usually with headgear wear. However, without removal of the upper second permanent molars, it is unlikely that more than 2–3 mm of space per quadrant can be gained. To avoid the use of headgear, TAD(s) may be used in combination with a fixed appliance to bring about the movement required.
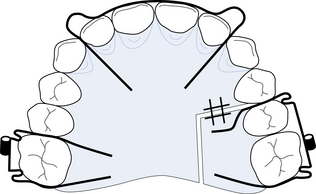
Fig. 9.15 An upper removable appliance (URA) with screw and headgear support to regain space lost to unilateral mesial drift.
URA to move |56 distally. Screw section to |56; single Adams’ clasp 6/ and double Adams’ clasp |56 (both 0.7 mm SS wire); tubes for headgear soldered to clasp bridges; labial bow 2 1 | 1 2 (0.7 mm wire).
Distal movement of the lower first permanent molar is more difficult to achieve but may be attempted if the lower second permanent molar is considered for extraction. Treatment is best carried out with a fixed appliance, perhaps assisted by use of a TAD.
 Self-assessment: questions
Self-assessment: questions
Multiple choice questions (True/False)
a. Is derived from the second pharyngeal arch
b. Completes growth in length before growth in width
c. Grows partly by passive displacement of its articulation with the cranial base
d. Is translated downwards and forwards by the condylar cartilage
a. Is derived from the first pharyngeal arch
b. Ossifies medial to Meckel’s cartilage
c. Has a predictable pattern of growth in each individual
3. Marked anterior mandibular growth rotation:
a. Occurs when growth in posterior face height is less than in anterior face height
b. Is more common than backward growth rotation
c. Is often associated with a deep overbite
d. Is associated with an increased maxillary/mandibular plane angle
4. In the dental development of the ‘average’ child:
a. Calcification of the primary incisors commences 6–8 months in utero
b. Root calcification of the primary teeth completes 2–2.5 years after eruption
c. Primary incisors erupt in contact and proclined
d. Calcification of the first permanent molars commences at 8–10 months after birth
e. The ‘leeway space’ is greater in the upper than in the lower arch
5. Space for the permanent upper incisors:
a. Is obtained mostly by eruption palatal to their predecessors
b. Is obtained by use of existing primary labial segments spacing
c. Is obtained by intercanine width growth
d. Is likely to be adequate where the primary incisors are crowded
6. Normal maturational changes in the dentition include:
a. A reduction in lower labial segment crowding
b. An increase in upper labial segment crowding
7. Clinical assessment of the anteroposterior dental base relationship:
a. Is undertaken by viewing the patient from in front
b. Should be undertaken with the teeth just out of occlusion
c. Is best carried out with the patient supine
8. A class II skeletal pattern:
a. Is present when the mandible is protruded relative to the maxilla
b. Can be assessed from the SNB angle
c. Is usually associated with a retrognathic maxilla
d. Can be assessed from the first permanent molar relationship
9. The maxillary/mandibular planes angle (MMPA):
b. Reflects the anteroposterior skeletal pattern
c. Indicates the vertical skeletal pattern
d. Reflects posterior lower facial height and anterior lower facial height
10. Class II division 2 malocclusion:
a. Is defined by a half unit class II buccal segment relationship
b. Exists when the lower incisor edges occlude anterior to the cingulum of the upper incisors
c. Is characterised by retroclined upper central incisors
11. A lateral cephalometric radiograph:
a. Is taken with the head tilted up
b. Is recorded with tube-to-midsagittal plane distance typically of about 15 cm
c. Is an exact record of facial dimensions
d. Is essential for orthodontic diagnosis
e. May be useful in localising the position of an unerupted tooth
Extended matching items questions
For each of the clinical problems (a–e), select from the list below (1–25) the most appropriate cephalometric input to assist in your assesment (more than one may be correct). Each variable can be used once, more than once or not at all.
3. Lower incisor angulation to mandibular plane.
4. Superimposition on Bjork’s structures.
8. Upper incisor angulation to maxillary plane.
13. Lower incisor tip to A–pogonion line.
14. Superimposition on S–N, holding at S.
19. No cephalometric assessment.
22. Superimposition on anterior vault of the palate.
a. A 12-year-old girl presenting for treatment planning of her moderately severe class II division 2 malocclusion; you are asked to give priority to planning the lower labial segment position.
b. An 18-year-old male patient on review for his worsening class III malocclusion, where an overall assessment is required of facial changes which have occurred in the 2 years since he was last seen (a cephalometric film is available from that time).
c. A 14-year-old girl with a class II division 1 malocclusion seen for treatment planning, where it is necessary to evaluate upper incisor angulation and decide between tipping or bodily tooth movement for overjet correction.
d. A 13-year-old male patient presenting for assessment of his class I malocclusion who indicates no desire to undertake orthodontic treatment.
e. A 20-year-old female patient with an anterior open bite, class I skeletal and incisor relationships.
Case history question
A 13-year-old female patient presents with a class I malocclusion with moderate upper and lower mid-arch crowding on a class I dental base with average FMPA. There is a history of recurrent oral ulceration.
Picture questions
Examine the records in Figure 9.16.
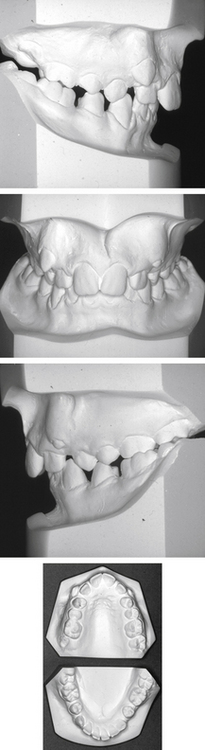
1. Classify the incisor relationship.
2. Classify the right and left molar relationships.
3. Classify the degree of crowding in the maxillary and mandibular arches (all permanent teeth are present).
4. What are the likely causes of this malocclusion?
5. What is the IOTN (DHC) score? (Additional information: no mandibular displacement associated with the crossbite; overjet 6 mm; lips competent.)
Picture 2
Examine the records in Figure 9.17.
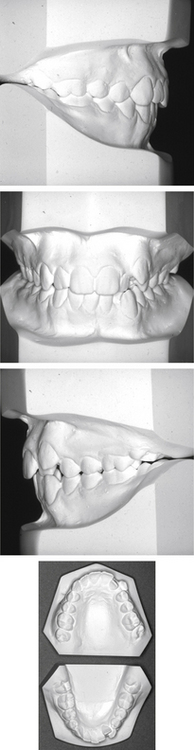
1. Classify the incisor relationship.
2. Classify the right and left molar relationships.
3. Assess the degree of crowding in the upper and lower arches.
4. What is the most likely cause of the upper arch crowding?
5. What is the IOTN (DHC) score? (Additional information: no mandibular displacement associated with |2 or |7 crossbites.)
Data interpretation question
Given the following cephalometric values: SNA = 78°; SNB = 85°; SN to maxillary plane 7°; MMPA = 30°; 1 to maxillary plane = 130°;  to mandibular plane = 75°, answer the following questions, explaining your reasoning.
to mandibular plane = 75°, answer the following questions, explaining your reasoning.
Short note questions
1. Angle’s classification of malocclusion
2. the dental health component of the Index of Orthodontic Treatment Need (IOTN)
3. the aesthetic component of IOTN
4. methods of creating space for relief of crowding other than by extraction.
1. What are the potential benefits/risks of orthodontic treatment? How would you assess the need for treatment?
2. Describe the occlusion of an average primary dentition in a child aged 5 years. What changes occur up to the age of 14 years leading to the establishment of a ‘normal’ permanent occlusion?
3. What factors should be considered when obtaining informed consent from a patient prior to orthodontic treatment?
 Self-assessment: answers
Self-assessment: answers ); class I on the left.
); class I on the left.