10 Malignant disease of the oral cavity
ASSUMED KNOWLEDGE
It is assumed that at this stage you will have knowledge/competencies in the following areas:
If you think that you are not competent in these areas, revise them before reading this chapter or cross-check with relevant texts as you read.
INTENDED LEARNING OUTCOMES
At the end of this chapter you should be able to:
ORAL AND OROPHARYNGEAL CANCER
In global terms, oral/oropharyngeal cancer is the sixth most common malignancy. In the Western world it accounts for only 2–4% of all malignant tumours although there is now good evidence to show that the incidence is increasing, particularly in younger people. By contrast, in Asia oral/oropharyngeal malig-nancy is the most common malignant tumour, which in parts of India accounts for no less than 40% of all malignancy. It is estimated that globally nearly 500 000 new cases develop annually and that in the year 2000 there were 1.5 million people alive with oral cancer at any one time.
Oral/oropharyngeal cancer is an almost entirely preventable disease, being caused by use of tobacco (with or without alcohol). In the West this is mostly cigarette smoking combined with alcohol abuse; the risk caused by both in combination is greater than the summation of the risks of each individually. In Asia and the Far East the use of Pan in its various forms and reverse smoking are the major aetiologic agents: epidemiological evidence strongly suggests that it is the presence of tobacco in the betel quid which is the major agent, although there seems also to be some relationship to the source of slaked lime and the areca nut itself. In the West, the incidence in women appears to be increasing and there is a worrying increase in the number of young patients, mostly male and particularly with tongue cancer, after a gradual fall earlier this century. This recent trend seems not to be related to tobacco and alcohol consumption and has been observed throughout Europe and North America. The general dental practitioner has a major role in prevention by advising and helping patients to cease tobacco smoking or chewing and moderating alcohol consumption.
Local control of disease at the primary site and the management of neck disease has improved; yet, despite this, cure rates and survival rates have only improved marginally in 40 years, remaining at approximately 55% survival at 5 years. Both recurrence of local disease and failure to control lymphatic metastases in the neck are early events and are a major cause of death. There is no doubt, however, that during the past 20 years great advances have been made in the management of oral cancer, and persistence of local disease and lymphatic metastasis are now less common. Why then have cure rates not improved? Field changes in the upper aerodigestive tract result in the phenomenon of multiple primary cancers. The longer a patient survives a first tumour, the greater the risk of developing a second or third primary tumour either elsewhere in the oral cavity or in the larynx, bronchus or oesophagus.
Even a patient who does not develop a second primary tumour is at risk of developing distant metastatic disease. Metastasis via the bloodstream is a relatively early event in oral cancer, although until recently rarely recognized during life. Currently 20% of all cancer-related deaths in patients with a tumour in the oral cavity/oropharynx are due to distant metastasis with no evidence of disease in the head or neck. Thus oral cancer is a ‘systemic’ disease from an early stage.
Resection
Surgical advances have been mainly in techniques of access surgery and in reconstruction. The widespread adoption of lip splitting and mandibulotomy has facilitated safe three-dimensional resections of tumours in the tongue and floor of the mouth in continuity with the lymphatics in the neck. A better understanding of the patterns of invasion of the mandible by adjacent tumour has allowed the development of rim resections, avoiding the sacrifice of mandibular continuity in many cases, without risking local recurrence. In recent years the development of skull base access surgery using well-established oral and facial osteotomy techniques has rendered previously inoperable tumours operable. This is particularly true for tumours extending into the pterygoid, infratemporal and lateral pharyngeal regions.
Reconstruction
Primary reconstruction is now the rule, and this is to the great benefit of patients. Earlier techniques were often unreliable and when bony reconstruction was involved it was often delayed. It was reasonably felt that before embarking on such prolonged and insecure techniques a period of time should be allowed to elapse, to demonstrate that local recurrence was unlikely before reconstruction was attempted. With current techniques based largely on muscle flaps—pectoralis major, trapezius and latissimus dorsi—and free tissue transfer based on microvascular techniques—radial forearm, lateral thigh, scapular, fibula and groin—primary reconstruction is not only reliable but produces acceptable functional and cosmetic results.
Radiotherapy
Megavoltage X-ray beams or electron beams are able to penetrate tissues and can cause cell death by producing lethal damage to DNA. Irradiated cells die as they attempt to divide and because malignant cells generally divide more rapidly than normal cells there is differential cell death. With careful planning and adjustment of dosage and frequency of treatment the tumour cells can be destroyed whilst sparing sufficient normal tissues to allow healing and repair. A typical regimen for an oral carcinoma would be a total dose of 55 Gray given by daily treatments on Monday to Friday over a 6-week period. The daily dose (fraction) is therefore only small and allows for repair of normal tissues between treatments. In most centres, surgery is the primary modality for most patients. Radiotherapy is used as a supplement when the surgical margins of the tumour are not clear or there is extensive nodal metastasis in the neck.
Although treating a cancer with radiotherapy avoids major surgery it has disadvantages:
An alternative way of treating tumours with radiotherapy is to implant radioactive materials into the tumour (brachytherapy). Radioactive iridium wires are the most commonly used implants. There is a rapid fall-off of dose with distance, and the technique continuously delivers very high-dose local irradiation with very little damage to adjacent tissues. Therefore the adverse effects of conventional radiotherapy are largely avoided.
Chemotherapy
Although many single agents or combinations of drugs can result in a response rate of around 60%, there is no evidence that this results in an increase in survival time or cure rate. Some centres advocate the use of induction chemotherapy before surgery but again there is no evidence, based upon prospective studies, that this improves survival. Palliative chemotherapy using agents such as cisplatinum and 5-fluorouracil are sometimes helpful for painful or fungating tumours.
Clinical aspects
Oral cancer has a predilection for certain sites within the mouth, mostly the lateral margins and ventral tongue, floor of mouth, retromolar trigone, buccal mucosa and palate. Most—more than 85%—are mucosal squamous cell carcinomas. Malignant tumours arising in the minor salivary glands are next in frequency, with lymphomas, malignant melanomas, sarcomas and metastatic tumours making up the remainder.
PREMALIGNANT LESIONS
The association of oral carcinoma with other oral mucosal lesions has been recognized for many years. Often these lesions are in the form of white plaques (‘leukoplakia’) or bright red velvety plaques (‘erythroplakia’), which may be present for periods of months to years before the onset of malignant change and often will be present together with the carcinoma when the diagnosis of malignancy is made. Because of this association, it has been assumed that such lesions lead directly to invasive carcinoma and hence are themselves premalignant. Some white plaques do have a potential to undergo malignant transformation and an examination of established carcinomas will show many to exist in association with white plaques. However, most oral carcinomas are not preceded by, nor associated with, leukoplakia.
Although historically oral leukoplakia has been recognized as premalignant, the risk of malignant transformation is not as great as was previously thought. Early literature suggested a 30% or higher incidence of malignant transformation of these lesions whereas more recent authors quote an incidence of 3–6%. The following oral lesions are now considered to carry a potential for malignant change:
A further group of conditions, although not themselves premalignant, are associated with a higher than normal incidence of oral cancer:
There remains a further group of oral conditions about which there is still some doubt as to whether their association with oral cancer is causal or casual:
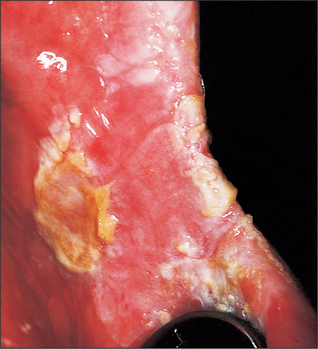
Leukoplakia (Fig. 10.1)
Using the term leukoplakia either in a histological or clinical context is a matter of defining what is meant by the term. The World Health Organization (WHO) has defined leukoplakia as ‘any white patch or plaque that cannot be characterized clinically or pathologically as any other disease’. This definition has no histological connotation.

Clinical features
Clinically leukoplakia may vary from a small, circumscribed white plaque to an extensive lesion involving wide areas of the oral mucosa. The surface may be smooth or it may be wrinkled and many lesions are traversed by cracks or fissures. The colour of the lesion may be white, yellowish or grey; some are homogeneous whilst others are nodular or speckled on an erythematous base. Many lesions are soft whereas other thicker lesions feel crusty. Induration (hardening) suggests malignant change and is an indication for immediate biopsy. It is important to recognize that it is the speckled or nodular leukoplakias which are the most likely to undergo malignant change.
Potential for malignant change
The incidence of malignant change in oral leukoplakia increases with the age of the lesion. One study showed a 2.4% malignant transformation rate at 10 years, which increased to 4% at 20 years. It also showed that as the age of the patient increased so did the risk of malignant transformation: for patients younger than 50 years it was 1%, whereas for those between 70 and 89 years it was 7.5% during a 5-year observation period. Kramer et al. (1978) have shown that in Southern England leukoplakia of the floor of the mouth and ventral surface of the tongue, so-called ‘sublingual keratosis’, has a particularly high incidence of malignant change. Their study suggested that this occurrence was due to pooling of soluble carcinogens in the ‘sump’ of the floor of the mouth.
Aetiology
Tobacco smoking or chewing are undoubtedly important aetiological factors. In Indians who smoke or chew tobacco (often as a component of the betel quid) the incidence of leukoplakia in those of 60 years of age is 20%, whereas in those who neither smoke nor chew tobacco the incidence is 1%.
The role of alcohol in the development of oral leukoplakia is difficult to assess. Few studies have been reported, but it has been shown that in patients with leukoplakia the incidence of excessive alcohol consumption is greater than in those without leukoplakia.
Management
In any patient presenting for the first time with oral leukoplakia a careful history—particularly looking for aetiological factors—and a detailed clinical examination should precede the histological examination of biopsies of any suspicious areas. Suspicion is aroused by any areas of ulceration, induration or where the underlying tissues are bright red and hyperaemic. Vital staining with toluidine blue can be used to guide the clinician to those sites most suspicious of malignant change.
If there is a history of tobacco consumption then the patient should be persuaded to stop immediately. It has been shown that if the patient stops smoking entirely for 1 year the leukoplakia will disappear in 60% of the cases.
Whenever severe epithelial dysplasia or carcinoma-in-situ is present, surgical excision or CO2 laser excision of the lesions is mandatory. Small lesions may be excised, the margins of the adjacent mucosa undermined and the defect closed by advancing the margins. For larger defects the area should be left to epithelialize spontaneously (alternatively the area can be skin-grafted). On the tongue the graft is quilted onto the raw area, whereas on the cheek, floor of the mouth or palate the graft can be retained in place by suturing a suitable pack overlying it.
When only mild to moderate epithelial dysplasia is present the patient should be followed up at 4-month intervals and details of the lesions recorded in the notes either photographically or diagrammatically.
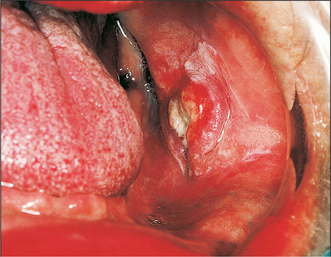
Erythroplakia (Fig. 10.2)
Erythroplakia is defined as ‘any lesion of the oral mucosa that presents as bright red velvety plaques which cannot be characterized clinically or pathologically as any other recognizable condition’. Such lesions are usually irregular in outline, although clearly demarcated from adjacent normal epithelium. The surface may be nodular. In some cases erythroplakia coexists with areas of leukoplakia. The incidence of malignant change in erythroplakias is 17 times higher than that in leukoplakia. In nearly every case of erythroplakia there are areas of epithelial dysplasia, carcinoma-in-situ or invasive carcinoma. Clearly all erythroplakic areas must be completely excised, either surgically or with a CO2 laser, and the specimens submitted for careful histological examination.

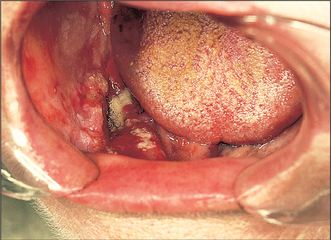
Chronic hyperplastic candidiasis (Fig. 10.3)
In chronic hyperplastic candidiasis, dense chalky plaques of keratin are formed, the plaques being thicker and more opaque than in non-candidal leukoplakia. Such lesions are particularly common at the oral commissures, extending onto the adjacent skin of the face. In 1969 attention was drawn to the high incidence of malignant transformation in these candidal leukoplakias, suggesting that the invasive candidal infection is the cause of the leukoplakia, and not merely a superimposed infection. It has also been suggested that in such patients there may be an immunological defect which allows the Candida albicans to invade the epithelium and may render the patient susceptible to malignant change.
It is thought that treatment with antifungal agents to eliminate the candidal infection will reduce the risk of malignant change. However, treatment may be necessary for many months to eliminate the organisms and reinfection is a constant problem. Surgical excision is recommended for persistent lesions.
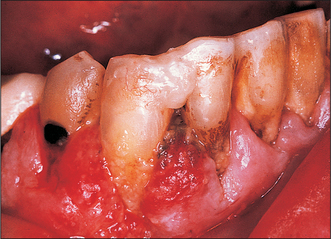
Oral submucous fibrosis (Fig. 10.4)
Oral submucous fibrosis is a progressive disease in which fibrous bands form beneath the oral mucosa. These bands progressively contract so that ultimately opening is severely limited, speech becomes hypernasal due to changes in the soft palate and swallowing is disturbed. Tongue movement may also be limited. The condition is almost entirely confined to Asians. Histologically it is characterized by jux-taepithelial fibrosis with atrophy or hyperplasia of the overlying epithelium, which also shows areas of epithelial dysplasia. Paymaster, in 1956, first discussed the precancerous nature of submucous fibrosis (see Langdon and Henk 1995). He noted the onset of a slowly growing squamous cell carcinoma in one-third of such patients. The changes are due to crosslinking of the collagen fibres caused by various alkaloids, particularly arecholine, which leach out of the arecha nut and penetrate the oral mucosa.

The scar bands of submucous fibrosis that result in difficulty in mouth opening can be treated either by intralesional injection of steroids or by surgical excision and grafting, but this has little effect in preventing the onset of squamous cell carcinoma in the generally atrophic oral mucosa. Any aetiological factors should, of course, be eliminated.
Syphilitic glossitis
Before the antibiotic era, syphilis was an important predisposing factor in the development of oral leuko-plakia and oral cancer. The syphilitic infection produces an interstitial glossitis with an endarteritis that results in atrophy of the overlying epithelium. This atrophic epithelium appears to be more vulnerable to those irritants that cause oral cancer or oral leukoplakia. As these changes are irreversible there is no specific treatment, although active syphilis must be treated. Regular follow-up is essential. It should be noted that squamous cell carcinomas may arise in syphilitic glossitis, even in the absence of leukoplakia.
Sideropenic dysphagia (Plummer-Vinson syndrome, Paterson-Kelly syndrome) (Fig. 10.5)
In 1936 Ahlbom showed the relation between sideropenic dysphagia and oral cancer (Langdon and Henk 1995). Sideropenic dysphagia is particularly common in Swedish women, and accounts for the high incidence of cancer of the upper alimentary tract in this group and the higher incidence of women with oral cancer in Sweden. Of women with oral cancer in Sweden, 25% were sideropenic. The pathogenesis of oral cancer in such patients may be similar to that of syphilitic glossitis. The sideropenic dysphagia leads to atrophic epithelium, which is particularly vulnerable to carcinogenic irritants. Although the anaemia will respond to treatment with iron supplements, it is not known whether such treatment reduces the risk of subsequent malignant change.

Oral lichen planus (Fig. 10.6)
Some reports have stated that in erosive or atrophic lichen planus there is a risk of malignant transformation; a 1.2% incidence of malignant change has been found in a series of 570 patients with oral lichen planus followed up for a mean of 5.6 years. If there is an association between lichen planus and oral cancer, the relation exists only with atrophic or erosive lichen planus, and patients with these conditions should be carefully reviewed. Erosive lichen planus should be treated with topical steroids, and in severe cases systemic steroids may be necessary.

Discoid lupus erythematosus
The oral lesions of discoid lupus erythematosus consist of circumscribed, somewhat elevated white patches, usually surrounded by a telangiectatic halo. Epithelial dysplasia may be seen on histological examination and this may lead to malignant transformation, usually on the labial mucosa adjacent to the vermilion border and more often in men than in women. Patients with discoid lupus erythematosus should be advised to avoid bright sunlight and, when in the open air, to apply an ultraviolet barrier cream to the lips.
CLINICAL PRESENTATION AND DIAGNOSIS OF ORAL CANCER
Oral cancer arises from the surface mucosa, and the clinical diagnosis should be easy. Early detection should lead to better outcome. Oral lesions, unlike those at many other sites in the body, give rise to early symptoms. In general, patients become aware of and usually complain about tiny lesions within the mouth and biopsy may be carried out under local analgesia. Yet, despite all the above, between 27 and 50% of patients present for treatment with tumours greater than 4 cm in diameter. Many of these patients are elderly and frail and therefore delay the effort of visiting their doctor or dentist: they are often denture wearers, accustomed to discomfort and ulceration in the mouth and thus see no urgency in seeking treatment. Furthermore, the practitioner may not be suspicious that a lesion is malignant. Not all oral cancers present as classical non-healing ulcers with heaped-up margins: they can start as small areas of ulceration in the depth of fissures in the tongue, as superficial mucosal erosions, as areas of induration in the absence of discernible ulceration or even as gingival hyperplasia mimicking gingival infection. The lesion is often treated initially with antifungal therapy, antibiotics, steroids and mouthwashes, thus causing further delay in the ultimate diagnosis and treatment. Another factor is that oral cancer is not usually painful until such time as either the ulcer becomes secondarily infected or the tumour invades sensory nerve fibres.
The time scale of development of oral cancer is generally weeks to months, by comparison with the scale of a few days seen with acute infective conditions (see p. 88).
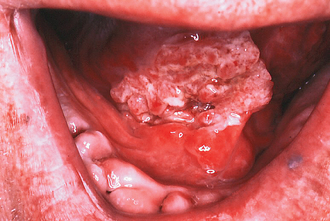
The tongue (Fig. 10.7)
Most tongue cancers occur on the middle third of the lateral margins, extending early in the course of the disease onto the ventral aspect and floor of the mouth. Approximately 25% occur on the posterior third of the tongue, 20% on the anterior third and only very rarely on the dorsum.
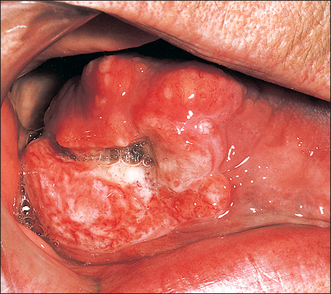
Fig. 10.7 An advanced cancer of the tongue presenting as an ulcer with heaped-up margins and a central area of necrosis.
Early tongue cancer may manifest in a variety of ways. Often the growth is exophytic with areas of ulceration. It may occur as an ulcer in the depths of a fissure or as an area of superficial ulceration with unsuspected infiltration into the underlying muscle. Leukoplakic patches may or may not be associated with the primary lesion. A minority of tongue cancers may be asymptomatic, arising in an atrophic depapillated area with an erythroplakic patch with peripheral streaks or areas of leukoplakia.
Later in the course of the disease a more typical malignant ulcer will usually develop, often several centimetres in diameter. The ulcer is hard in consistency (indurated) with heaped-up and often everted edges (Fig. 10.7). The floor is granular, indurated and bleeds readily. Often there are areas of necrosis. The growth infiltrates the tongue progressively, causing increasing pain and difficulty with speech and swallowing. By this stage pain is often severe and constant, radiating to the neck and ears. Lymph node metastases at this stage are common—indeed 50% of patients may have palpable nodes at first attendance. Because of the relatively early lymph node metastasis of tongue cancer, 12% of patients may present with no symptoms other than ‘a lump in the neck’.
Floor of the mouth (Fig. 10.8)
The floor of the mouth is the second most common site for oral cancer. It is defined as the U-shaped area between the lower alveolus and the ventral surface of the tongue; carcinomas arising at this site involve adjacent structures very early in their natural history. Most tumours occur in the anterior segment of the floor of the mouth to one side of the midline.
The lesion usually starts as an indurated mass, which soon ulcerates. At an early stage the tongue and lingual aspect of the mandible become infiltrated. This early involvement of the tongue leads to the characteristic slurring of the speech often noted in patients with such cancers. The infiltration is deceptive but may extend to reach the gingivae, tongue and genioglossus muscle. Subperiosteal spread is rapid once the mandible is reached. Lymphatic metastasis, although early, is less common than with tongue cancer. Spread is usually to the submandibular and jugulodigastric nodes and may be bilateral.
Floor of mouth cancer is associated with a pre-existing leukoplakia more commonly than cancer at other sites.
Gingiva and alveolar ridge (Fig. 10.9)
Carcinoma of the lower alveolar ridge occurs predominantly in the premolar and molar regions. The patient usually presents with proliferative tissue at the gingival margins or superficial gingival ulceration. Diagnosis is often delayed because a wide variety of inflammatory and reactive lesions occur in this region in association with the teeth or dentures (Fig. 10.9). Indeed, there will often be a history of tooth extraction with subsequent failure of the socket to heal before definitive diagnosis is made. Another common story is that of sudden difficulty in wearing dentures. Regional nodal metastasis is common at presentation, varying from 30 to 84%, although false-positive and false-negative clinical findings are common.
The buccal mucosa (Fig. 10.10)
The buccal mucosa extends from the upper alveolar ridge down to the lower alveolar ridge and from the commissure anteriorly to the mandibular ramus and retromolar region posteriorly. Squamous cell carcinomas mostly arise either at the commissure or along the occlusal plane to the retromolar area, most being situated posteriorly. Exophytic, ulcerative and verrucous types occur. Tumours are subject to occlusal trauma, with consequent early ulceration, and often become secondarily infected. The onset of the disease may be insidious, the patient sometimes presenting with trismus due to deep neoplastic infiltration into the buccinator muscle. Extension posteriorly involves the anterior pillar of the fauces and soft palate, with consequent worsening of the prognosis. Infiltrating lesions will often involve the overlying skin of the cheek, resulting in multiple sinuses. Lymph node spread is to the submental, submandibular, parotid and lateral pharyngeal nodes.
Verrucous carcinoma occurs as a superficial proliferative exophytic lesion with minimal deep invasion and induration. Often the lesion is densely keratinized and presents as a soft white velvety area mimicking benign hyperplasia. Lymph node metastasis is late and the tumour behaves as a low-grade, squamous cell carcinoma.
The hard palate, maxillary alveolar ridge and floor of antrum (Figs. 10.11, 10.12)
These three sites are anatomically distinct, but a carcinoma arising from one site soon involves the others. Consequently it can be difficult to determine the precise site of origin. Except in countries where reverse smoking is practised, cancer of the palate is relatively uncommon. Most squamous cancers in this site arise in the antrum and later ulcerate through to involve the hard palate (see Ch. 15, p. 225.). The majority of malignant tumours arising from the palatal mucosa are of minor salivary gland origin. Palatal cancers usually present as sessile swellings, which ulcerate relatively late. In contrast to mandibular alveolar tumours, deep infiltration into the underlying bone is uncommon.

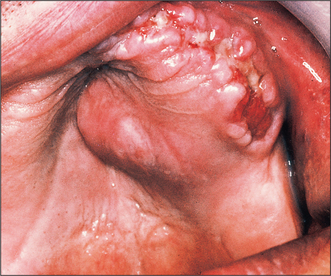
Fig. 10.12 This patient with an antral carcinoma first attended his dental practitioner complaining of loosening of the teeth, which were then extracted. Carcinoma can be seen growing through the sockets from above.
Carcinomas arising in the floor of the maxillary antrum often present as palatal tumours. Although an extensive antral carcinoma is difficult to miss, the early symptoms are non-specific and may mimic chronic sinusitis. Patients with tumours of the lower half of the antrum complain of ‘dental’ symptoms because of early alveolar invasion. The most common features are pain, swelling or numbness of the face. Later symptoms of unilateral nasal obstruction, discharge or bleeding and dental symptoms such as painful or loose teeth, ill-fitting dentures, oroantral fistula or failure of an extraction socket to heal may follow. Lymph node metastasis from carcinomas of the palate and floor of the antrum occurs late but carries a poor prognosis.
DIAGNOSIS
The diagnosis of intraoral carcinoma is primarily clinical, and a high index of suspicion is necessary for all those clinicians seeing and treating patients with oral symptoms. A careful and detailed history, with particular attention to recording the dates of the onset of particular signs and symptoms, must precede the clinical examination. All areas of the oral mucosa should be carefully inspected and any suspicious lesion palpated for texture, tethering to adjacent structures and induration of underlying tissue. Any ulcer persisting for more than 2 weeks, any induration or spontaneous bleeding (particularly in a patient over 50 years who smokes and/or drinks alcohol) requires urgent referral for expert opinion. Dental practitioners should make a full mucosal examination of the mouth and oropharynx part of their routine ‘dental inspection’.
INVESTIGATION
Surgical biopsy
A clinical diagnosis of oral cancer should always be confirmed histologically (see Ch. 8), but this should not be undertaken in general dental practice, because a biopsy will alter the appearance of the lesion and make it more difficult for the hospital specialist to assess the tumour. The general dental practitioner should refer the patient with a suspicious lesion immediately to an oral and maxillofacial surgeon.
Within the oral cavity a surgical biopsy can usually be obtained using local anaesthesia: incisional biopsy is recommended in all cases. Whenever possible the patient should be seen at a combined clinic by a surgeon and radiotherapist before even the biopsy is carried out but, provided careful records are made, an initial incisional biopsy is acceptable—and may indeed save time in the planning and initiation of subsequent therapy. The biopsy should include the most suspicious area of the lesion and some normal adjacent mucosa. Areas of necrosis or gross infection should be avoided as they may confuse the diagnosis.
Fine-needle aspiration biopsy
This technique (see Ch. 8), which is often used in hospital, is applicable mainly to lumps in the neck, especially suspicious lymph nodes in a patient with a known primary carcinoma. It consists of the percutaneous puncture of the mass with a fine needle and aspiration of material for cytological examination. The method of aspiration needs no specialized equipment (although devices to enable controlled and prolonged traction on the plunger of the syringe may make it much simpler) and is fast, almost painless and without complications. The accuracy can be improved by using ultrasound to guide the needle into the suspicious mass.
Radiography
Plain radiography is of limited value in the investigation of oral cancer. Only in very advanced lesions involving bone will changes be visible on conventional radiographs: at least 50% of the calcified component of bone must be lost before any radiographic change is apparent. Furthermore, the facial bones are of such a complexity that confusion from overlying structures makes radiographic diagnosis more difficult. However, rotational pantomography of the jaws can be helpful in assessing alveolar and antral involvement provided that the above limitations are understood.
Computed tomography and magnetic resonance imaging
The increasing availability of computed tomography (CT) scanning and magnetic resonance imaging (MRI) has been of great benefit in the investigation of head and neck tumours. For the evaluation of antral tumours, particularly assessment of the pterygoid regions, CT and MRI have superseded plain radiography and conventional tomography. CT is also of value in the investigation of metastatic disease in the lungs, liver and skeleton. Positron emission tomography (PET) scanning is a newer modality which relies on the fact that tumours have a higher rate of metabolism of glucose. A radioactive glucose analogue is injected. This is taken up selectively by the tumour and subsequently imaged.
CLASSIFICATION AND STAGING OF ORAL CANCER
Before starting treatment for a patient with oral cancer the disease must be carefully evaluated. Clinical assessment includes a detailed history, physical examination and laboratory and imaging studies, the purposes of which are to determine the extent of the tumour and the presence or absence of regional lymph node involvement or distant metastasis.
All classification systems have the aim of grouping together homogeneous and comparable elements which share similar prognostic significance. Throughout the world the TNM system is applied. This consists of assessing the size and extent of the primary lesion (T), the presence and condition of associated regional nodes (N) and the presence of distant metastases (M) (Table 10.1).
Table 10.1 Classification of oral cancers
| T | N | M |
|---|---|---|
| T0: No primary tumour detected | N0: No nodes detected | M0: No evidence of distant metastases |
| T1: Tumour less than 2 cm diameter | N1: Single ipsilateral node less than 3 cm | M1: Distant metastases present |
| T2: Tumour more than 2 cm but less than 4 cm | N2: (a) Single ipsilateral node more than 3 cm but less than 6 cm | — |
| (b) Multiple ipsilateral nodes not greater than 6 cm | ||
| (c) Bilateral or contralateral node or nodes not greater than 6 cm | ||
| T3: Tumour more than 4 cm | N3: Any node or nodes greater than 6 cm | — |
| T4: Adjacent structures invaded by tumour | — | — |
All gradations of prognosis can be demonstrated by grouping patients together on the basis of T, N and M into groups with similar survival rates. This is tumour staging (Table 10.2).
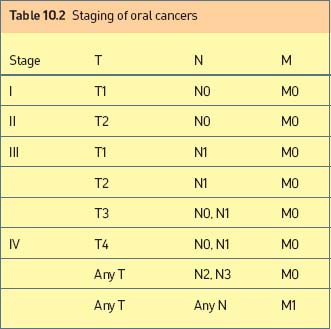
The prime purpose of staging is that, by knowing the prognosis, an appropriate treatment can be selected which will most favourably affect survival (Table 10.3).
Table 10.3 Prognostic significance of staging of oral cancer
| Stage | % 5-year survival |
|---|---|
| I | 57–84 |
| II | 49–70 |
| III | 25–59 |
| IV | 7–47 |
MANAGEMENT OF THE PRIMARY TUMOUR
Role of general dental practitioner before definitive treatment
Choice of treatment
The principal treatments available for primary tumours remain surgery and radiotherapy. The basic decision to be made is between radical radiotherapy and elective surgery. If the former is chosen surgery is reserved for ‘salvage’ (i.e. for biopsy-proven recurrent or residual disease). If surgery is chosen, radiotherapy may be used in an adjuvant manner, either before or after surgery, but the operation remains fundamentally the definitive curative procedure. Preferences for one or other policy vary considerably between treatment centres.
Many factors must be considered in deciding the optimum management for each individual patient. These include the site, stage and histology of the tumour and the medical condition and lifestyle of the patient. Ideally every patient should be seen at a joint consultation clinic by a surgeon and radiotherapist, who assess objectively and agree the optimum strategy of management for the particular individual. The following factors influence the decision on treatment policy.
Site of origin
The choice of treatment depends on the part of the mouth in which the tumour arises. The management of primary tumours at the various anatomical sites are discussed later (pp. 140–142). In general, surgery is preferred for tumours arising on or involving the alveolar processes; for other sites surgery and radiotherapy are alternatives.
Stage of disease
A small lesion which can be excised readily without producing any deformity or disability is in general best managed surgically. Surgery is also usually more appropriate for a very large mass or where there is invasion of bone, provided the tumour is operable, because of the low cure rates by radiotherapy in these circumstances. The management of lesions of intermediate stage (larger T1, most T2 and early exophytic T3 tumours) is more controversial, as policies of elective surgery or radical radiotherapy produce generally similar survival rates; hence discussion centres on the likely functional results and morbidity of either approach. When there is involvement of cervical lymph nodes the primary tumour and nodes are usually both treated surgically.
Previous irradiation
It is not advisable to retreat with radiotherapy a tumour arising in previously irradiated tissue. Such a tumour is likely to be relatively radioresistant because of limited blood supply. Also re-irradiation of normal tissue is very likely to result in necrosis of all the tissues in the area.
Field change
Where multiple primary tumours are present, or if there is extensive premalignant change, surgery is the preferred treatment. Radiotherapy in these circumstances is unsatisfactory; irradiation of the entire oral cavity causes severe morbidity and may not prevent subsequent new primary tumours arising from areas of premalignant change.
Histology
The histology report on a biopsy specimen has little influence on choice of treatment. The less common adenocarcinoma and melanoma are relatively radioresistant and therefore should be treated surgically whenever possible. The histological differentiation of a squamous carcinoma does not usually influence its management, there being little evidence to suggest that a well-differentiated primary should be treated differently from a poorly differentiated one.
Age
The patient’s age is often quoted as an important factor which must be taken into account when deciding on a course of management. With a young patient there is the fear that if radiotherapy is given it may induce a malignancy in years to come; in fact this risk is very small compared with the mortality of the disease itself. Elderly patients tend to be poor surgical risks, but on the other hand they also tend to do badly with radiotherapy, especially external radiotherapy, and often deteriorate and may die as a result of the debility and poor nutritional status induced by the irradiation. Chronological age per se should not necessarily be regarded as a contraindication to surgery.
TREATMENT ISSUES SPECIFIC TO SITE OF OCCURRENCE
Carcinoma of the lip
Carcinoma of the lip most commonly arises at the vermilion border of the lower lip, away from the line of contact with the upper lip: only 15% arise from the central third and commissure regions, and 5% from the upper lip. Initially the tumours tend to spread laterally rather than infiltrating deeply; eventually, if uncontrolled, they can spread into the anterior triangle of the neck and invade the mandible. Lymph node metastases occur late. Both surgery and radiotherapy are frequently employed and are highly effective methods of treatment, each giving cure rates of about 90%.
Tongue
Surgery is the treatment of choice for early lesions suitable for simple intraoral excision, for tumours on the tip of the tongue and for advanced disease (when surgery should be combined with postoperative radiotherapy). For intermediate-stage disease surgery and radiotherapy have similar outcomes. When performing surgical excision of less than one-third of the tongue, formal reconstruction is not necessary: indeed, the best results are obtained by not attempting to close the defect or to apply a split skin graft. The base of the residual defect should be diathermied and then allowed to granulate and epithelialize spontaneously. Such treatment is relatively pain free and results in an undistorted tongue. When available, a CO2 laser may be used for the partial glossectomy. The postoperative course is relatively pain free, oedema is minimal and healing occurs with minimal scarring.
Any tongue carcinoma exceeding 2 cm in diameter requires at the very least a hemiglossectomy. Many such tumours will infiltrate deeply between the fibres of the hyoglossus muscle. Extensive tongue lesions often involve the floor of the mouth and alveolus. In any of these circumstances a major resection is indicated. Access is best via a lip split and mandibulotomy. The treatment will involve dissecting the neck in order to remove any lymph nodes that might be harbouring metastatic disease. The tongue defect requires reconstruction, usually with a free-tissue transfer using a radial forearm flap with microvascular anastomosis of the artery and vein.
Floor of the mouth
Floor of the mouth cancers spread to involve the under-surface of the tongue and the lower alveolus at a relatively early stage. Therefore surgical excision will nearly always include partial glossectomy and marginal resection of the mandible. The resultant defect must always be reconstructed with either a local or a distant flap. It is unacceptable to advance and suture the lateral margin of the residual tongue to the buccal mucosa because this tethers the tongue, causing severe difficulties with speech and mastication. Small tumours of the floor of the mouth that do not show deep infiltration can be treated by simple excision.
For larger lesions and those involving the ventral tongue and/or the alveolus, surgical access is gained via a midline or lateral (anterior to the mental foramen) mandibulotomy and lip split. As these extensive tumours have a high incidence of nodal involvement the resection must be undertaken in continuity with an ipsilateral neck dissection.
When there is evidence of gross tumour invasion of the bone, resection of the mandible is necessary. In order to avoid functional and cosmetic deformity, immediate primary reconstruction is essential. The choice lies between reconstruction with vascularized bone, a free corticocancellous graft or an alloplastic system usually supplemented with cancellous bone mush.
Buccal mucosa
Lesions confined to the buccal mucosa should be excised with a 2-cm margin, including the underlying buccinator muscle, followed by a split skin graft. Extensive lesions with complicated three-dimensional shapes—for example, lesions extending posteriorly to the retromolar area, maxillary tuberosity or tonsillar fossa—require reconstruction with a free radial forearm flap; this adapts very well to such shapes and remains soft and mobile postoperatively.
Lower alveolus
In general, surgery is the treatment modality of choice for all alveolar carcinoma, except for patients unfit for surgery. Access is achieved via a lip split approach. Now that the patterns of bone invasion are better understood, the continuity of the mandible can often be preserved by performing a marginal resection. If bone invasion is so extensive that the mandible must be resected in continuity with the tumour, primary reconstruction should always be undertaken, because the results are always better than those of delayed reconstruction.
Several techniques for immediate reconstruction of the mandible are available. Historically, free corticocancellous grafts harvested from the iliac crest or rib grafts have been used. Provided there is a good soft-tissue cover to the graft, results can be very satisfactory, although it is difficult to reconstruct the chin prominence with this technique.
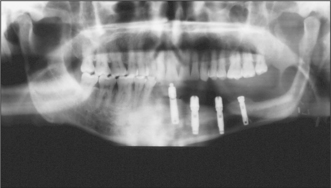
Microvascular tissue transfer is currently favoured for immediate mandibular reconstruction. The radial forearm flap with soft tissue and a section of the radius, the compound groin flap based on the deep circumflex iliac vessels and free fibula flaps have all been advocated. A problem with the radial flap is that the harvested bone, although restoring mandibular continuity, often does not provide sufficient bulk for prosthetic reconstruction. Both the fibula and the groin flap provide sufficient bone stock to allow the insertion of osseointegrated implants (Fig. 10.13) and thus full dental rehabilitation postoperatively.
Retromolar trigone
The retromolar trigone is defined as the anterior surface of the ascending ramus of the mandible. It is roughly triangular in shape, with the base being superior, behind the third upper molar, and the apex inferior, behind the third lower molar. Tumours at this site may invade the ascending ramus of the mandible. They may also spread upwards in soft tissue to involve the pterygomandibular space; this can be difficult to detect clinically or radiologically.
A lip split and mandibulotomy are needed to gain access to the retromolar region. Small defects can often be reconstructed with a masseter or temporalis muscle flap. Larger defects are best reconstructed with a free radial forearm flap, which can be made to conform very well to the shape of the defect at this site.
Hard palate and upper alveolus
These are considered together because they are adjacent and are rare sites of origin of primary squamous carcinoma. A squamous carcinoma presenting at either of these locations is more likely to have arisen in the maxillary antrum than in the oral cavity. An exception is on the Indian subcontinent where carcinoma of the hard palate occurs in association with reverse smoking. Malignant tumours of the hard palate are more likely to arise from the minor salivary glands.
A tumour confined to the hard palate, upper alveolus and floor of the antrum can be resected by a partial maxillectomy. A more extensive tumour confined to the infrastructure of the maxilla requires total maxillectomy. If the preoperative investigations indicate extension of disease into the orbit, pterygoid space or infratemporal fossa, a more extensive procedure is necessary. The chance of obtaining a cure by surgery alone is small and postoperative radiotherapy is essential. If the tumour extends superiorly to involve the dura within the skull then a combined neurosurgical procedure will be required. Following maxillary resection the resulting cavity should be skin grafted to ensure rapid healing and to prevent contracture of the overlying soft tissues.
Malignant melanoma
Oral melanomas are rare. The peak age incidence is between 40 and 60 years; nearly 50% are on the hard palate and about 25% are on the upper gingivae. About 30% of melanomas are preceded by an area of hyperpigmentation, often by many years. Pigmentation varies from black to brown, while rare non-pigmented melanomas (15% of oral melanomas) are red. Oral melanomas may be flat but are usually raised or nodular, and asymptomatic initially but may later become ulcerated, painful or bleed. Because of their rapid growth, most oral melanomas are at least 1 cm across. Approximately 50% of patients have metastases at presentation.
Size and rapid growth, particularly if associated with destruction of underlying bone or presence of metastases, are obvious indicators of a poor outcome. Once the diagnosis has been confirmed, the best hope of cure is provided by the widest possible excision followed by radical radiotherapy. There is no evidence that chemotherapy is of significant value except for palliation. Immunotherapy has been used successfully to prolong survival, sometimes for several years. The 5-year survival rate appears to be about 5%.
MANAGEMENT OF THE NECK
Patients staged N0
The regional lymph nodes, although clinically impalpable, sometimes contain occult foci of malignant cells. It seems reasonable to expect that removal or treatment of regional lymph nodes, even when clinically clear, would improve cure rates. Alternatively, it can be argued that treatment of the regional nodes in all cases is unnecessary, because only a minority have metastases in the nodes. In practice, whenever the surgery for the primary cancer involves opening the neck, a prophylactic neck dissection is undertaken. The submandibular triangle often must be opened as part of the resection of the primary, and therefore a function-sparing elective neck dissection for tumours in the floor of the mouth, lower alveolar ridge and tongue is advocated. In this dissection, structures such as the accessory nerve, internal jugular vein and sternocleidomastoid muscle are preserved.
The operation should preferably be seen as a staging procedure on which is based the decision to give radical postoperative radiotherapy. All patients with two or more positive nodes or extracapsular spread should be treated with postoperative radiotherapy.
Patients staged N1, N2a, N2b
Present evidence suggests that the treatment of choice is a full neck dissection wherever possible sparing the sternocleidomastoid muscle, the accessory nerve and the internal jugular vein, either alone or combined with postoperative radiotherapy if multiple nodal involvement or extracapsular extension is found in the resected specimen. In patients unfit for radical surgery, radical external beam irradiation is indicated.
Patients staged N2c
It is uncommon for patients with oral cancer to present with bilateral nodes. When they do so, there is often a large inoperable primary tumour, which is best treated by external radiation. It therefore seems logical to treat the neck also by irradiation. Occasionally, particularly in a young patient, bilateral neck dissection can be justified. A full radical neck dissection is undertaken on the ipsilateral side and the internal jugular vein is spared if possible on the contralateral side. Most often postoperative radiotherapy will be required for multiple nodal involvement or extracapsular spread. In such situations, severe post-treatment oedema or congestion of the face and tongue may be anticipated.
Patients staged N3
N3 indicates massive involvement, usually with fixation. Large fixed nodes are often associated with advanced primary disease with a poor prognosis. Surgery is not normally advisable: removal of the common or internal carotid artery with replacement, or extensive resection, of the base of the skull, although technically feasible, is seldom advisable. Treatment is most often by external radiotherapy. In a few younger patients with resectable primaries it is worth rendering a fixed mass in the neck operable by preoperative radiotherapy.
Nodal metastasis appearing after primary treatment
Provided that follow-up at regular intervals is rigorously maintained, it should be possible to detect a lymph node metastasis while it is still relatively small and therefore operable. Ultrasound-guided fine-needle aspiration cytology is particularly useful in this situation to confirm that the palpable node is a carcinoma rather than being enlarged due to reactive hyperplasia. Whenever positive, or if there is any doubt, a radical neck dissection is performed, followed by external irradiation if multiple involved nodes or extracapsular spread are found.
FOLLOW-UP
Approximately 50% of patients treated for oral cancer will die from the disease, approximately 20% of patients will develop a local recurrence at the site of the primary tumour; another 25% will develop nodal metastases. Both of these events are likely to occur within the first 2 years following treatment. A further 20% of patients with oral cancers will develop additional new cancers elsewhere in the upper aerodigestive tract due to field changes resulting from tobacco and alcohol abuse. For all these reasons careful and meticulous follow-up is essential. For the first 12 months following treatment the patient will be seen at the hospital monthly. During the second year the patient is seen at 2- to 3-month intervals and thereafter they are seen every 6 months.
The general dental practitioner has an ongoing role in monitoring and treating dental diseases, which might impact on the tissues treated because of cancer and in observing for any new malignant disease.
Kramer I.R.H., El-Laban N., Lee K.W. The clinical features and risk of malignant transformation in sublingual keratosis. British Dental Journal. 1978;144:171-180.
Langdon J.D., Henk J.M. Malignant tumours of the mouth, jaws and salivary glands. London: Edward Arnold, 1995.
Ord R.A., Blanchaert R.H. Oral cancer. The dentist’s role in diagnosis, management, rehabilitation and prevention. Chicago, IL: Quintessence, 1999.
Pindborg J.J. Oral cancer and precancer. Bristol, UK: Wright, 1980.
SELF-ASSESSMENT
Answers on page 266.