15 The maxillary antrum
ASSUMED KNOWLEDGE
It is assumed that at this stage you will have knowl-edge/competencies in the following areas:
If you think that you are not competent in these areas, revise them before reading this chapter or cross-check with relevant texts as you read.
INTENDED LEARNING OUTCOMES
At the end of this chapter you should be able to:
THE IMPORTANCE OF THE MAXILLARY ANTRUM TO DENTAL SURGERY
The maxillary sinus is often referred to as the maxillary antrum (or more simply the ‘antrum’). It is important to the dental surgeon because of its close relationship to the posterior maxillary teeth (generally from first premolar to third molar). The proximity varies between individuals (Fig. 15.1) but tends to increase with age as the antrum enlarges. The antrum can encroach into alveolar bone after tooth extraction, and periapical bone loss resulting from dental disease may further decrease the amount of bone separating it from the teeth. This close anatomical relationship can lead to diagnostic difficulties because both the antrum and the maxillary teeth are innervated by branches of the maxillary division of the trigeminal nerve. In addition, infection may spread from the periapical region of the posterior maxillary teeth to the antrum (and in the opposite direction) and the antrum is at risk of iatrogenic damage during certain dental procedures.
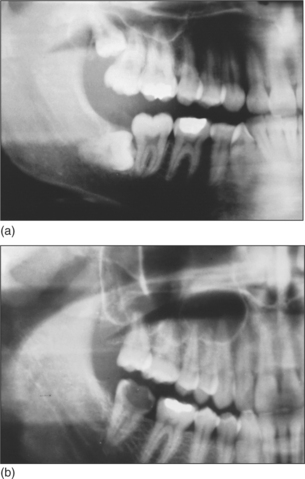
Fig. 15.1 (a) A small maxillary antrum that does not reach the apex of the second premolar. (b) A large maxillary antrum that reaches to the apex of the lateral incisor.
The ability to distinguish between dental and antral symptoms enables the dental surgeon to decide when dental treatment is indicated and when referral (e.g. to a general medical practitioner, an oral and maxillofacial surgeon or an ear, nose and throat (ENT) surgeon) is appropriate.
The antrum is visualized on oral and facial radiographs (notably periapical views of the posterior maxillary teeth, orthopantomogram (OPT) and occip-itomental views) and a knowledge of its normal radiographic appearance is essential in the diagnosis of both dental and antral disease. Evidence of antral pathology may be incidentally discovered by the general dental practitioner (GDP) on these radiographs.
Although the GDP is unlikely routinely to perform elective surgery within the antrum, there will be occasions when dentoalveolar surgery with a degree of antral involvement is necessary—for example, to repair a newly created oroantral communication. It is necessary for the GDP to be able to recognize and deal with problems such as oroantral communication and foreign body in the antrum and he or she should be capable of explaining the commonly performed antral investigations and surgical procedures to a patient who requests information. The GDP may also recommend other procedures that involve antral surgery (e.g. ‘sinus lift’/alveolar ridge augmentation procedures used prior to the placement of osseointegrated implants).
Summary of the importance of the maxillary antrum to dental surgery
DISTINGUISHING SIGNS AND SYMPTOMS OF DENTAL PATHOLOGY FROM THOSE OF SINUSITIS
Maxillary sinusitis is common and the dentist needs to be able to distinguish it from dental disease. It is usually an acute condition, but chronic sinusitis may also develop following an acute episode and may persist or recur if drainage from the antrum to the nasal cavity is poor or when a foreign body is retained.
Acute sinusitis may affect any of the paranasal sinuses but is usually confined at any one time to a single sinus. It is a bacterial infection and typically occurs after a viral upper respiratory tract infection (URTI) (Haemophilus, Pneumococcus, Streptococcus, Staphylococcus species and anaerobes are commonly found).
Maxillary sinusitis is usually related to impaired antral drainage, which may be caused by:
Accumulated secretions become infected, allowing a collection of pus to develop in the antrum.
Dental diseases (including periapical pathology, infected odontogenic cysts and periodontal disease) may also cause sinusitis. Other possible causes include the presence of contaminated foreign bodies, trauma or infections of non-odontogenic cysts or malignant tumours.
Signs and symptoms of sinusitis
Symptoms of acute sinusitis usually appear a few days after the acute cold symptoms have resolved. Pain, headache, nasal obstruction, a purulent nasal secretion and ‘postnasal drip’ (a discharge of ‘mucopus’ into the pharynx) are commonly found and there may also be fever and malaise. The pain is dull, heavy, throbbing and located over the cheek and in the upper teeth. It may resemble toothache but is not related to hot, cold or sweet stimuli, although it may be increased by biting. Typically all of the posterior teeth on the affected side are painful and tender to percussion, although often no obvious dental cause can be found. Leaning the head forwards increases the pain (as it leads to an increase in venous congestion which, together with collected secretions, occludes the ostium and increases pressure within the antrum). However, leaning the head backwards reduces congestion, allowing the ostium to become patent, reducing internal antral pressure and consequently relieving pain. Although the pain usually overlies the affected sinus it may be referred from the antrum to the frontal and retro-orbital regions.
THE INVESTIGATION OF ANTRAL DISEASE
A diagnosis of sinusitis can usually be made from the findings of the history and examination. The teeth and surrounding tissues should be examined for disease (although remember that sinusitis may itself have a dental cause). Transillumination, using a torch shone from inside the mouth, may demonstrate antral congestion but this is a rather crude test and may fail to detect tumours. Radiographs are not usually required to confirm the diagnosis of sinusitis as the diagnosis can be made on clinical grounds alone. Radiographs are only required to exclude the possibility of dental disease, trauma or pathology within the antrum. If pathology or trauma is suspected, occipitomental radiographic views are often taken in specialist centres. A ‘fluid level’ may be visible which represents a collection of pus, although following trauma it may be due to the presence of blood and suggests that there is a fracture of the wall of the antrum. Opacities due to polyps, cysts, thickened antral lining, tumours and radio-opaque foreign bodies may also be demonstrated.
Other useful radiographs include:
Much useful information can be gathered by endoscopy of the antrum. This is better performed by someone with experience of endoscopy in the region (such as an ENT surgeon).
DENTAL EXTRACTIONS AND THE ANTRUM
The following complications may occur during the extraction of posterior maxillary teeth because of their close proximity to the maxillary antrum:
Maxillary premolars and permanent molars are most frequently implicated, although permanent canines may occasionally be very close to the antrum. Complications may also occur during the surgical removal of impacted partially erupted or unerupted teeth (e.g. canines, premolars and third molars). The extraction of deciduous teeth does not present a risk due to the relatively small size of the antrum in children and the presence of the developing permanent teeth.
An assessment of the size and proximity of the antrum before extraction or periapical surgery on a posterior maxillary tooth may help to anticipate and avoid these complications. When a complication does occur, it should be recognized and dealt with promptly.
The following factors should be taken into account during clinical and radiographic examination in order to anticipate and avoid complications:
If the dental history reveals the creation of an oroantral communication during a previous extraction there is likely to be an increased risk of this complication occurring during the subsequent extraction of adjacent or contralateral teeth. Similarly, if there is a history of difficult extractions, due perhaps to hypercementosis or dense bone, there may be an increased risk of tuberosity fracture.
OROANTRAL COMMUNICATION AND FISTULA
An oroantral communication (OAC) is an abnormal connection between the oral and antral cavities; an oroantral fistula (OAF) is an epithelialized OAC (although the terms OAC and OAF are often used interchangeably).
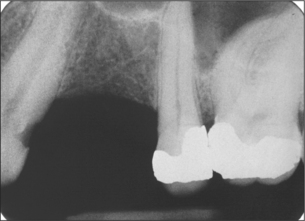
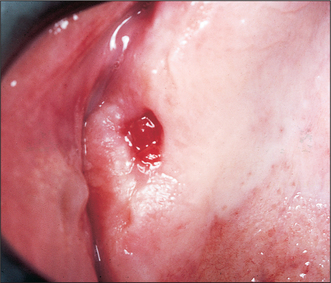
The creation of an OAC most commonly follows the extraction of a maxillary tooth closely related to the antral floor (typically the first molar (Fig. 15.2), which lies close to the lowest point of the antral floor, although any premolar or molar may be affected). An OAC may also form as a result of an alveolar fracture running through the antral floor or wall, or be due to direct trauma from a bur or chisel. Left untreated, an OAC may heal spontaneously or persist as an OAF (Fig. 15.3).
The following signs indicate OAC formation:
Investigation of a suspected OAC
The presence of an OAC can often be confirmed by careful examination using a mirror and a good light, although bleeding may obscure visibility. The interior of the antrum may be visible or there may be a bony defect lined by intact antral mucosa. Gentle suction applied to the socket often produces a characteristic hollow sound. The temptation to confirm the presence of a suspected OAC by probing or irrigation (to demonstrate transfer of fluid through the OAC into the antrum and nose) should be resisted. Both methods carry the risk of causing sinusitis by introducing oral flora or pushing contaminated bone fragments or other foreign bodies into the antrum. Even gentle probing may breach an intact antral floor or mucosal lining to create an OAC where one previously did not exist. It may also increase the size of an existing OAC, lessening the chances of spontaneous closure and complicating future surgical repair.
To test for a suspected OAC, a patient may be asked to attempt to blow the nose whilst pinching the nostrils. Air, which is unable to escape through the closed nostrils, is forced into the mouth through any OAC, producing bubbles of blood or saliva. Established OAFs often have small slit-like or pinhole oral openings concealing much wider underlying bony defects. They can also be detected using the above test and if sinusitis is present pus may be expressed or may discharge spontaneously into the mouth.
A patient with an untreated OAC or established OAF will typically give a history of an upper molar or premolar extraction followed by the development of:
Radiographs (e.g. periapical views or OPT) are useful to confirm the diagnosis of OAC/OAF and to assess the size of the bone defect, although small defects may not be demonstrated.
Prevention of OAC formation
Where the risk of OAC formation is anticipated, the patient should be warned preoperatively and steps should be taken to avoid this complication. Surgical exodontia is preferable to forceps extraction because it allows more control over bone removal and, by tooth division, enables individual roots to be delivered away from the thin antral floor. If a mucoperiosteal flap is raised its design should allow it to be adapted for OAC repair if necessary.
The diagnosis and enucleation of cysts near the antrum can be problematic, as an extension of the antrum may be mistaken for an odontogenic cyst during the preoperative assessment and at operation. Both have a similar radiographic appearance, although a radio-opaque line can usually be seen to separate a cyst cavity from the antrum, whereas an extension of the antrum will appear continuous with the main antral cavity. Because the healthy antrum contains air but a cyst contains fluid, the following simple test is often useful to distinguish between the two at operation. The thin bony wall is pierced using a wide-bore needle connected to a large syringe and the cavity contents aspirated. Air is aspirated if the antrum has been pierced; fluid would be recovered from a cyst. Unfortunately, this test is not foolproof as pus may be aspirated from an infected antrum or the contents of a cyst may be too thick to enter the needle, giving the impression of an empty cavity.
Treatment of OAC and OAF
The immediate treatment of a new OAC is aimed at preventing the development of a persistent OAF and chronic sinusitis. Larger communications require surgical closure although small defects (up to 5 mm wide) may heal spontaneously (it is likely that many close without being detected). However, early surgical closure is recommended whenever possible as it is difficult to predict when spontaneous healing will occur.
Immediate treatment of new OAC
This aims to encourage the regeneration of new bone between the oral and antral cavities. Treatment is directed at protecting the blood clot within the socket whilst organization and bone formation take place and at preventing infection of the wound or antrum.
Where further surgery is delayed or contraindicated an acrylic base plate or extension of an existing denture can be used to support the clot, or a dressing such as ribbon gauze (soaked in an antimicrobial agent) may be sutured across (not into) the defect. In smokers this has the advantage of protecting the clot from disturbances due to the changes in intraoral pressure associated with inhalation. However, care must be taken not to force impression material through the OAC into the antrum (the defect can be covered with sterile gauze while the impressions are taken).
If there is sufficient soft tissue, the opposing palatal and buccal mucosa may be held together with mattress sutures. A strong, preferably non-resorbable, suture material should be chosen (e.g. 3/0 black silk) and sutures retained for 10–14 days to ensure that healing is complete before they are removed. Reducing the height of the bony socket edges with a bur and slightly undermining the tissue margins helps to bring the margins together where there is a shortage of soft tissue. However, there is often insufficient mucosa for this simple technique and because the sutures are unsupported by bone there is a risk of wound dehiscence. If there is insufficient mucosa a buccal mucoperiosteal advancement flap is used to cover the defect. This is a more demanding procedure, which should be undertaken by a general dental practitioner only if he or she has adequate training, experience and facilities.
Further options for the treatment of OAC/OAF
If the immediate measures are insufficient or fail to lead to healing of an OAC (e.g. in the case of a large OAC) further treatment becomes necessary. Tissue from local flaps is most often utilized to close oroantral defects, although distant flaps (e.g. from the tongue) and grafting are also possible. The choice of method depends on the size and position of the communication. Of the variety of local flaps which have been described the most common is the buccal advancement flap.
Buccal advancement (Rehmann’s) flap (Fig. 15.4)
This technique is suitable for the closure of new OACs and chronic OAFs.
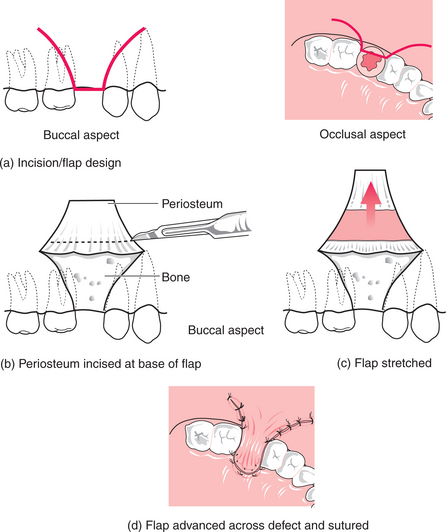
This is a simple, well-tolerated procedure with a good success rate. It can be performed under local anaesthesia in a cooperative patient and may be performed in general dental practice if adequate skill and facilities are available. Although this technique initially reduces sulcus depth, this is usually temporary.
In OAFs with large bony defects or where previous surgical closure has been unsuccessful, more complicated surgery may be required to close the defect. An adaptation of the buccal advancement flap utilizing a buccal fat pad (BFP) graft is often used. This is performed under GA in order to achieve adequate analgesia and as surgery is more prolonged. A broad-based three-sided mucoperiosteal flap is raised and periosteum incised (Fig. 15.4). The BFP is then located using a vestibular incision in the region of the upper first permanent molar and mobilized using blunt dissection with artery forceps. This tissue is then advanced to cover the bony defect and the mucoperiosteal flap is sutured using a non-resorbable material. A high success rate using the BFP graft has been reported.
Palatal rotation flap (Fig. 15.5)
This is used less commonly than the buccal advancement flap.
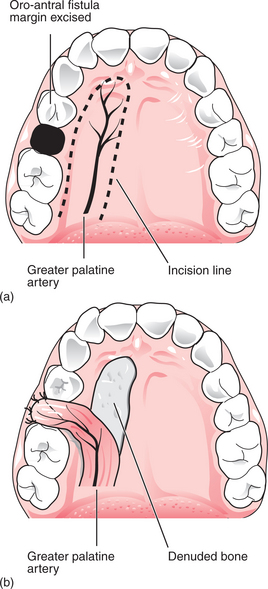
This technique provides a thick, strong repair, which heals readily due to its good blood supply and does not adversely affect the buccal sulcus. However, palatal flaps are relatively inelastic and can be difficult to raise and mobilize. In addition, it can be difficult to judge the precise length of tissue required. Under local anaesthesia, this procedure is more unpleasant for the patient than the buccal advancement flap is and a raw area of exposed palatal bone is produced. Although, it could be tackled in general dental practice under local anaesthesia it is more commonly performed in a specialist setting under GA.
For all methods of OAC/OAF closure, the patient should be warned not to blow the nose during the first 10 postoperative days, as this raises pressure within the antrum and may disrupt the healing tissue. Compliance with this instruction may be greater if a patient is given a simple explanation for it. Prophylactic antibiotics and nasal decongestant drops are prescribed by some surgeons to prevent infection and encourage antral drainage.
FOREIGN BODIES IN THE ANTRUM
This complication occurs when teeth or roots are closely related to the antrum. Roots of maxillary premolars and molars are the most common foreign bodies although whole teeth may also be displaced into the antrum. Their entry into the antrum occurs during attempts at removal and is associated with OAC formation. Other foreign bodies include materials introduced during root-filling procedures, via an OAF (food, impression material, cotton buds) and during trauma.
The displacement of a root into the antrum occurs because of:
As a root can be pushed through a very thin antral floor using the lightest touch it is essential to avoid applying any upward pressure. The risk is particularly high when an elevator is used blindly within a socket. Root removal should therefore be performed under direct vision using a transalveolar approach. Elevators are used to apply gentle pressure towards the mouth (never towards the antrum) and forceps should not be applied without a clear view of both the palatal and buccal root surfaces. Consideration may be given to leaving a small (less than 3 mm) vital root fragment rather than risk displacing it into the antrum. If this decision is taken the patient should be informed and the reasons explained, relevant radiographs should be taken to confirm the size and position of the retained root and an entry should be made in the patient’s notes. The root should be reviewed periodically and removed if symptoms develop. Whole teeth may be pushed into the antrum, with partially erupted and unerupted teeth, especially those with a single conical root, being at the greatest risk (e.g. upper third molars, impacted canines and premolars).
A root not removed with the tooth must be accounted for, due to the dangers of inhalation and infection. First look in the oral cavity, socket and adjacent tissues, next search extraorally and then take radiographs if necessary. Radiographs that are suitable for demonstrating a root in the antrum include periapical (Fig. 15.6) and oblique occlusal views or an OPT. The presence of a root canal confirms that a radio-opaque image represents a root.

Roots should be removed from the antrum as soon as possible to prevent an OAF and chronic sinusitis from developing. If left they may become embedded in granulation tissue, polyps or fibrous tissue or an antrolith (antral ‘stone’) may form around them. They are occasionally expelled through an OAF into the mouth or through the ostium into the nose from where they may be inhaled or expelled by sneezing. In general dental practice, the recommended immediate treatment for a root in the antrum is to provide simple treatment for the OAC (see above), inform the patient and arrange prompt referral to an oral and maxillofacial surgeon.
Roots can sometimes be removed through the extraction socket, although often access is better via a window in the anterior antral wall, made using the Caldwell-Luc operation. As an alternative, consideration should be given to possible removal of small roots by endoscopy.
Surgical removal via an extraction socket
If a root in the antrum is near its socket, it can sometimes be removed by raising a buccal flap and removing the buccal wall of the socket to create an enlarged opening into the antrum. Suction and irrigation are used to locate the root, which is then recovered. The defect is closed by advancing a buccal flap across it.
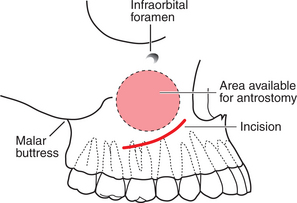
Caldwell-Luc operation (Fig. 15.7)
This gives surgical access to the interior of the antrum though the mouth and is usually performed in hospital under GA. It can be used to remove roots, teeth and other foreign bodies from the antrum.
Summary of extractions and the maxillary antrum
FACIAL FRACTURES INVOLVING THE ANTRUM
Fractures of the antral walls occur in several common types of facial fracture including zygomatic complex, mid-third (Le Fort I, II and III), orbital blow-out and alveolar fractures (see Ch. 13). The presence of a fracture through the antral wall does not preclude the extraction of a maxillary molar or premolar, although forceps should be avoided in favour of a surgical approach in the initial 6 weeks following trauma.
ANTRAL CYSTS AND TUMOURS
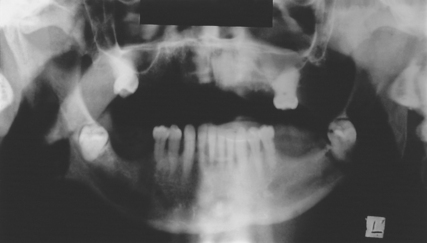
Antral mucosal cysts are frequently discovered as incidental findings on dental radiographs (Fig. 15.8). They are generally symptomless and have no long-term significance, but care should be taken to differentiate between truly antral lesions and cysts of odontogenic origin (apical cysts, dentigerous cysts and odontogenic keratocysts), which do require treatment.
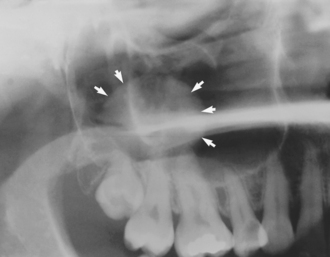
Fig. 15.8 A benign antral mucosal cyst (arrows) may be an incidental finding on a dental radiograph.
Benign tumours arising in the antrum include papillomas and osteomas. Although they rarely cause symptoms, they may interfere with antral drainage or cause nasal obstruction by growing through the ostium, and they occasionally herniate through an OAC. More often, however, they are discovered incidentally on radiographs.
Malignant tumours arising in the antrum are less common, but often have a poor prognosis as they tend to present at an advanced stage. This is because they develop in a concealed location and early symptoms may be absent, or mistaken for sinusitis. When symptoms of antral malignancy do develop, a patient may consult a dentist believing he or she has a dental problem. This makes it especially important that dentists are able to recognize the typical presenting signs and symptoms (see also Ch. 10, p. 136). These vary according to the direction in which the tumour is spreading (see box).
Radiographs of early malignant antral tumours appear normal or may show cloudiness or an irregular soft-tissue outline. Erosion of the antral wall is seen in later stages. Whenever antral malignancy is suspected referral should be made without delay to an oral and maxillofacial surgeon, initially by telephone or fax.
THE ANTRUM AND FACIAL PAIN
Sinusitis and antral malignancy both produce facial pain, which may not have an immediately obvious cause. These conditions should be included in the differential diagnosis of facial pain (their typical signs and symptoms are described above and facial pain is discussed in detail in Ch. 16).
Signs and symptoms of antral malignancy (dependent on direction of spread)
PHARMACOLOGICAL TREATMENT OF ANTRAL DISEASE
Antibiotics, decongestant nasal drops and steam inhalations are prescribed for the prevention of sinus infection following the creation of an OAC. Broad-spectrum antibiotics are useful in the treatment of acute sinusitis (although they are not a substitute for the drainage of pus) and decongestant nasal drops and steam inhalations can be used to encourage drainage. An analgesic such as paracetamol or ibuprofen may be recommended for relief of pain in acute sinusitis.
Decongestants
Sympathomimetic drops, such as ephedrine 0.5%, encourage antral drainage by causing vasoconstriction, which reduces vascular engorgement within the nasal mucosa. This decreases mucosal swelling and thus increases the patency of the ostium. Ephedrine drops should not be used for more than 7 consecutive days as rebound vasodilatation occurs with long-term use, leading to further mucosal congestion (also note that ephedrine should not be prescribed for a patient taking monoamine oxidase inhibitors). Pseudoephedrine tablets may be taken as an alternative.
Steam inhalations
Steam inhalations help to decrease the viscosity of mucus, allowing it to drain more easily (use hot rather than boiling water to avoid the risk of scalding). Menthol and eucalyptus may be added to the water to make this treatment more pleasant and, although this has no proven medical benefit, it increases patient compliance.
SELF-ASSESSMENT
Answers on page 269.