11 Surgical aids to prosthodontics, including osseointegrated implants
ASSUMED KNOWLEDGE
It is assumed at this stage that you will have knowledge/competencies in the following areas:
If you think that you are not well equipped in these areas, revise them before reading this chapter or cross-check with texts on those subjects as you read.
INTRODUCTION
Although many advances in dental health have been made over the past few decades, it is nevertheless rare for an individual to retain a full complement of natural teeth for life. Teeth are lost for various reasons, notably periodontal disease, dental caries, pathological conditions of the jaws and trauma. Prosthodontics aims to restore not only the function and aesthetics of the dentition after tooth loss but also the aesthetics of the facial form.
A well-constructed removable prosthesis that replaces missing teeth will restore function and appearance. A removable prosthesis should be stable and have adequate retention and stability. To achieve this, the prosthesis should be seated onto well-shaped alveolar ridges with adequate basal bone and a healthy oral mucosa. There will ideally be no major vertical or horizontal skeletal discrepancy, which can compromise denture stability.
Preprosthetic surgery is a term used for surgical procedures that aim to improve the condition of the oral tissues to enable a removable denture to rest on a sound base, free from marked bony protuberances or undercuts, with no interfering muscle attachments, flabby soft-tissue excess or hyperplastic oral mucosa. To achieve the best results, the skills of the oral surgeon and the prosthodontist are combined in a team approach.
Endosseous implants are commonly placed in suitable patients to improve the stability and retention of removable dentures as well as fixed prostheses. Implants may avoid the need for more complex surgery to improve an otherwise unsatisfactory edentulous ridge.
AIMS AND OBJECTIVES OF PREPROSTHETIC SURGERY
The aim of preprosthetic surgery is to prepare the soft and hard tissues of the jaws for a comfortable prosthesis that will restore oral function, aesthetics and facial form.
The objectives of preprosthetic surgery are to help to:
Non-surgical options should always be considered first (e.g. remaking a technically unacceptable prosthesis, relining, adjusting the occlusal face height or extending the denture flanges to improve retention and stability) before preprosthetic surgery is undertaken.
Preprosthetic surgery may be undertaken to:
PHYSIOLOGICAL CHANGES IN THE ORAL TISSUES AND MASTICATORY APPARATUS ASSOCIATED WITH AGE
The oral tissues undergo physiological changes with advancing age, some of which may influence the outcome of prosthodontic rehabilitation:
As we age the blood supply to the jaws becomes increasingly dependent on the circulation in the periosteum, rather than from the arteries. This is largely due to age changes leading to narrowing of the lumen of vessels such as the inferior alveolar artery. Consequently, it is important to preserve the periosteum and its blood supply wherever possible, to minimize the risk of ischaemic necrosis of under-lying bone.
Physiological changes in the oral tissues are sometimes a consequence of hormonal changes. For example, oral discomfort may occur in women without overt clinical signs, and denture wearing may aggravate the symptoms in some patients. In a few cases, oral discomfort may be attributed to the menopause, and the symptoms may resolve after hormone replacement therapy. It is therefore necessary to obtain a comprehensive history from the patient in order to identify accurately the cause of any oral discomfort associated with denture wearing. Nutrition can also play a part in oral discomfort; some patients with sore mouth may be anaemic.
ANATOMICAL CONSEQUENCES OF TOOTH LOSS
Loss of alveolar bone
Changes occur in the morphology of the jaws after tooth loss (Fig. 11.1). The jaws are composed of alveolar and basal bone. The alveolar bone and periodontium support the teeth, but neither have a physiological function once the teeth are lost, and are therefore resorbed. Alveolar bone changes shape significantly with tooth loss, in both the horizontal and vertical planes, but the overall pattern of resorption is largely predictable. In the maxilla and in the anterior aspect of the mandible bone loss occurs typically in both the horizontal and vertical planes. In the posterior mandible the bone loss is mostly in the vertical plane.
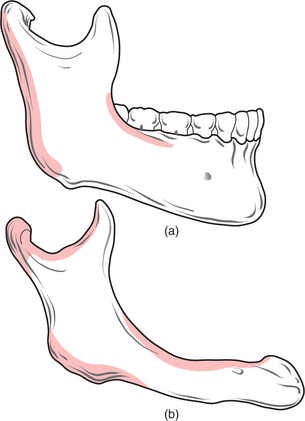
Fig. 11.1 (a) A dentate mandible, illustrating the extent of supporting (alveolar) bone around the teeth. (b) An edentulous mandible, illustrating the extent of resorption of alveolar bone that occurs following loss of the teeth. Note also that the angle between the ascending ramus and body of the mandible is more obtuse than in (a), and the mental foramen is also closer to the crest of the edentulous ridge. The shaded areas in this illustration indicate areas of resorption of mandibular bone with advancing age.
After physiological resorption has occurred, the remaining jaw structure is termed the ‘residual ridge’. The bone that remains after alveolar bone has resorbed is termed ‘basal bone’. Marked resorption sometimes affects the entire mandible (Fig. 11.2). Basal bone does not change shape significantly unless it is subjected to excessive local forces, for example, in the edentulous anterior maxilla in association with retained natural lower incisors.
Other affected anatomical structures
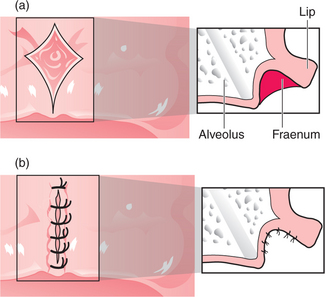
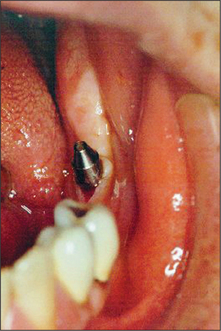
Other anatomical structures may become more prominent with tooth loss. The genial tubercles and their muscle attachments may become prominent in a patient with extensive resorption of the mandible, sometimes compromising denture stability. Maxillary or mandibular tori may also cause instability of a denture, or may be traumatized by it. A prominent fraenum (Fig. 11.3) can displace a denture during function, and may weaken the denture base so that it fractures through flexing.

Fig. 11.3 A prominent labial fraenum causes displacement of the denture. If the denture flange is eased to fit round the fraenum, the denture may be weakened. Excision of the fraenum (fraenectomy) is indicated.
Forces transmitted through the teeth during mastication are absorbed by the supporting structures (the periodontium and alveolar bone). In an edentulous patient, forces exerted by a denture are transmitted through the oral mucosa to the underlying bone. A denture must therefore fit well if trauma to the oral mucosa overlying an edentulous ridge is to be avoided.
Facial aesthetics are affected by tooth loss. The facial profile collapses (the nose and chin appear too close together) after tooth loss and consequent edentulousness. The loss of face height can be restored with dentures.
CLASSIFICATION OF THE EDENTULOUS JAWS
Cawood and Howell (1988) classified the edentulous jaws according to the state of ridge resorption after tooth loss (Table 11.1). There are other classifications, but this one has been adopted internationally as a means of assisting communication and assessment of a patient’s edentulous state.
Table 11.1 A classification of the edentulous jaws
| Class | Description |
|---|---|
| I | Dentate |
| II | Immediately postextraction |
| III | Convex ridge form, adequate in height and width |
| IV | Knife-edge ridge form, adequate in height but inadequate in width |
| V | Flat ridge form, inadequate in height and width |
| VI | Loss of basal bone, which may be extensive but follows no predictable pattern |
THE IDEAL EDENTULOUS RIDGE
A removable denture requires a firm bone support with a smooth contour, adequate to provide stability, with access to the vestibule for a peripheral seal, and without any soft-tissue excess (e.g. flabby maxillary tuberosities) likely to cause displacement or weakness of the denture.
Most patients tolerate the loss of their natural teeth and subsequent denture wearing without difficulty. However, there may be extensive loss of alveolar bone after tooth extraction, resulting in an atrophic (flat or knife-edged) edentulous ridge (Fig. 11.4). In some patients this can make denture wearing difficult or uncomfortable. The prosthodontist may be able to modify a denture design to enhance its stability and retention, but this is not always possible. Surgery may therefore be required to enhance retention and stability of the prosthesis.

TREATMENT PLANNING
History
The history will indicate the patient’s principal concerns and expectations of treatment. The age and health of the patient influence the treatment plan’a young person with severely resorbed alveolar ridges might tolerate more complex surgery than would a mature patient with similar jaw morphology.
Clinical examination
This will include general extraoral and intraoral assessment of the hard and soft tissues, and specific analysis of the denture-bearing areas.
The height, width and general shape of the alveolar ridges are assessed, with an emphasis on the presence of bony undercuts and the position of anatomical structures such as the mental neurovascular bundle. The depth of the buccal sulci, the position and size of fraenal and muscle attachments and the condition of the alveolar ridges are documented. The dentures should be technically acceptable before considering preprosthetic surgery.
Special investigations
Radiographs are taken to assess the condition of the underlying bone. A panoramic film is useful to assess the overall condition of the edentulous ridges and to identify any retained dental roots or other pathology (e.g. cysts of the jaws). A lateral cephalostat may be taken to demonstrate the anteroposterior skeletal relationship and the height of the alveolar ridges anteriorly. Periapical views are desirable if retained roots are to be removed before construction of a denture.
Articulated study casts facilitate treatment planning and are helpful when explaining the surgical procedure to a patient. A diagnostic wax-up of the prosthesis is desirable to demonstrate the anticipated final aesthetic result to the patient, and as a medicolegal record of the proposed treatment.
PREPROSTHETIC SURGERY PROCEDURES
Various techniques may be used, either alone or in combination, to preserve or improve the denture-bearing area. There are three broad categories of preprosthetic surgery procedure:
Some of the procedures described below may be included in more than one category.
Soft-tissue procedures
Excision of hyperplastic tissue
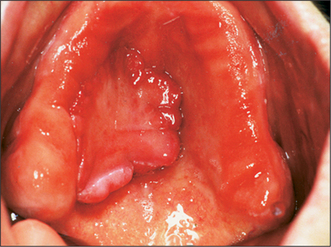
Hyperplastic oral mucosa under or adjacent to a removable denture usually arises in response to chronic irritation, for example, from an overextended denture flange or a deficiency in the fitting surface of a denture, trauma from a sharp cusp on an acrylic tooth or an ill-fitting denture clasp. Poor denture design may also cause mucosal hyperplasia (Figs 11.5, 11.6). Surgery may be unnecessary if the cause of the hyperplastic tissue is identified and eliminated; the hyperplastic tissue will then usually diminish in size or resolve completely. Any residual tissue that inter-feres with denture construction can be removed via an elliptical incision as for an excision biopsy (see Ch. 8, p. 109). Where possible (e.g. in the buccal sulcus or on the cheek), the incision may be closed by suturing the wound edges together (primary closure). On the edentulous ridge, the periosteum is elevated to undermine the edges of the wound, and the edges of the mucoperiosteal flaps can then be advanced to achieve wound closure. A split-thickness skin graft may be required to cover extensive areas of denuded oral mucosa. A keratinized-free mucosal graft may be harvested from the hard palate for smaller areas. It is often beneficial to place a temporary soft lining in the existing denture after surgery, to minimize the likelihood of further irritation, prior to remaking the prosthesis.

Prominent labial fraenum
The flange of a denture may traumatize a prominent labial fraenum or muscle attachment (Fig. 11.3). If the fraenum is relatively small, this may be managed by trimming back the labial or lingual denture flange. However, the denture may be weakened and it might fracture if extensive trimming is undertaken to relieve the fraenum. Excision of the fraenum (fraenectomy) may be indicated to avoid this.
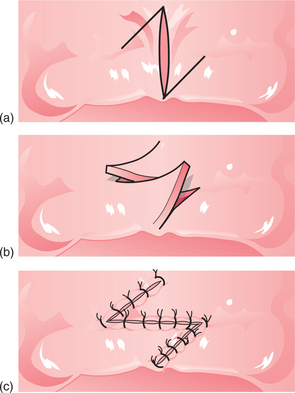
For the fraenectomy procedure (also described in Ch. 12) vertical incisions are made parallel to the fraenum, extending into the sulcus from the residual ridge to form a rhomboid-shaped wound (Fig. 11.7). The incisions are widest at the base of the labial sulcus. The insertion of the fraenum into the alveolar ridge is held with either a suture or a pair of toothed tissue forceps and the fraenum is dissected, leaving periosteum covering the surface of the bone. Interrupted sutures are inserted through the mucoperiosteal flap to achieve wound closure. A modification of this procedure incorporates a Z-plasty, to preserve sulcus depth (Fig. 11.8). However, the Z-plasty can be technically more difficult than the fraenectomy technique described above.
Fibrous enlargement of the maxillary tuberosity
Ideally, the maxillary tuberosities are firm for denture support. If they are flabby and mobile, the soft tissues of the tuberosities may displace during impression-taking for a new denture, making denture construction difficult. Fibrous enlargement of a maxillary tuberosity may be reduced (Fig. 11.9) by making two incisions along the crest of the alveolar ridge to form an ellipse, angled towards the centre of the ridge down to bone. A triangular-shaped wedge of tissue is excised, and a ‘fillet’ of soft tissue is excised from each flap. The wound edges are then sutured together.
Hard-tissue procedures
Dentoalveolar procedures
Care is taken when extracting teeth or dental roots with forceps or via a surgical approach to ensure preservation of alveolar bone and oral mucosa. Buccal bone may fracture and remain adherent to a tooth root after extraction. This is most likely to occur with canine teeth if there has been minimal bone loss through periodontal disease. Use of a dental elevator will minimize the risk of fracture of alveolar bone before delivery of a tooth with extraction forceps. Fracture of the maxillary tuberosity during tooth extraction may result in extensive bone loss leading to poor denture stability.
The periotome (Fig. 11.10) is increasingly being used to extract teeth before implant surgery (cf. extraction instruments described in Ch. 4). This device is composed of a narrow, flat blade which is pushed down into the gingivae, and breaks down the periodontal fibres supporting the tooth. Periotomes preserve the alveolar bone, which is essential when placing an immediate endosseous implant after tooth extraction (web sites include http://www.citagenix.com, http://www.klsmartinusa.com/OfficeProducts/periotome.htm).
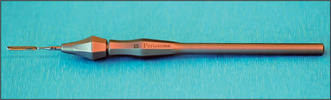
Fig. 11.10 An example of a periotome. The flat blade inserted into the handle is interchangeable with other blades. The blade is inserted into the periodontal ligament and through continuous manipulation, the periodontal fibres are cut around the tooth until it is extracted.
If alveolar bone is displaced during tooth extraction, it is repositioned by digital pressure after tooth delivery. Loose fragments of alveolar bone in the socket are removed to prevent delayed healing. Larger fragments with an intact periosteal blood supply are left in situ.
Alveoplasty
This procedure is performed to recontour an uneven alveolar ridge. Alveoplasty is undertaken either at the time of tooth extraction (primary) or after the alveolar ridge has healed (secondary). Alveoplasty removes the least amount of bone necessary to achieve a smooth bone contour.
Primary alveoplasty involves the exposure of a tooth socket to allow trimming of bone fragments with bone rongeurs or a bur to create a smooth, rounded socket outline. When several adjacent teeth are removed, alveoplasty may be combined with interseptal alveolotomy to eliminate bony undercuts (Fig. 11.11).
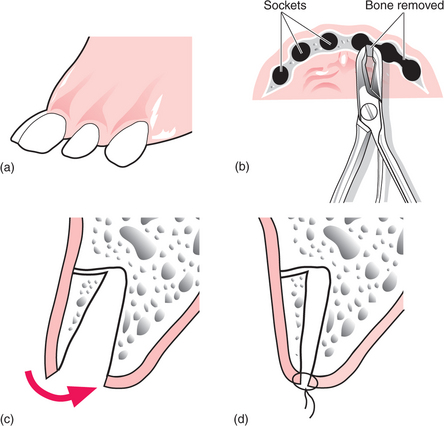
Fig. 11.11 (a) Reduction of an alveolar undercut by removal of the interseptal bone (interseptal alveolotomy). This might be required in the anterior maxilla in a patient with proclined incisor and canine teeth. (b) After extraction, rongeurs (bone nibblers) or bone shears are used to remove the interseptal bone. (c) Using digital pressure the buccal alveolar bone (still attached to the periosteum) is ‘in-fractured’ to reduce the bony undercut. (d) Sutures are placed to close the wound.
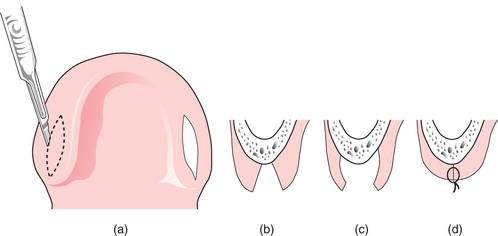
After tooth extraction, a bony protuberance may exist on the edentulous ridge or a bony undercut may be present several months later, compromising denture stability. Secondary alveoplasty is then undertaken. An incision is made along the crest of the ridge to expose the alveolar bone surface. The bony prominence or undercut is smoothed with a bur, bone file or a chisel to achieve the desired contour (Fig. 11.12), and after palpating the reshaped ridge to ensure a smooth contour, the wound is closed with sutures.
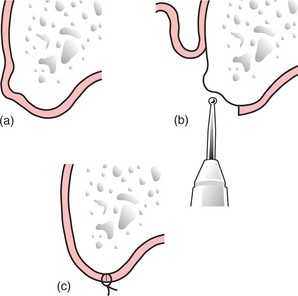
Fig. 11.12 (a) Reduction of a bony protuberance that is interfering with denture fitting. (b) An incision has been made along the crest of the alveolar ridge. A mucoperiosteal flap has been raised, and a round surgical bur is used to smooth the protuberance. (c) The wound is debrided and the flap is sutured back into position.
Excision of a maxillary or mandibular torus
A torus (Figs 11.13, 11.14) is a developmental bone exostosis, present typically either on the midline of the hard palate or on the lingual aspect of the mandible above the mylohyoid ridge (usually bilat-erally). Patients are often unaware of their existence. There are other causes of bony expansion of the jaws, some of which may have a history of slow onset and gradual enlargement. A neoplastic lesion (usually of minor salivary gland origin) sometimes develops on the hard palate, and it has been known for a dentist to ease a denture to accommodate an enlarging malignant growth. If there is doubt about the nature of any lesion, the patient is referred for a specialist opinion.
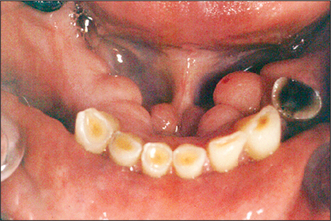
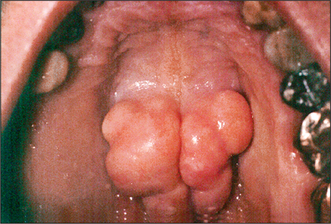
Fig. 11.13 Lingual tori are typically bilateral, although the patient is often unaware of their existence.
A denture rubbing on a torus may cause ulceration of the overlying oral mucosa and pain. Removal of a torus may therefore be indicated if the denture cannot be constructed to avoid it.
Radiographs are taken before excision of a maxillary torus to examine its structure. If a maxillary torus has an air space within it that communicates with the floor of the nose, then excision of the torus might result in an oronasal fistula, which can be difficult to treat.
Limited surgical access or a pronounced gag reflex might compromise treatment under local anaesthesia. General anaesthesia is sometimes indicated, particularly for maxillary surgery.
Surgical access to a palatal torus is gained via a midline incision over the lesion, with short (avoiding the greater palatine artery) relieving incisions at either end (Fig. 11.15). The flaps are raised to expose the torus, and the mass is excised either with a rotary bur, a chisel or both. Destruction of the torus with a rotary bur (e.g. a large acrylic bur) ensures safe, gradual removal of the mass. Alternatively a flat fissure bur is used to section the torus into smaller pieces, which are freed with a chisel and a surgical mallet. After suturing the flaps, an acrylic surgical stent (cover plate) may then be placed to cover the wound, to help prevent haematoma formation.
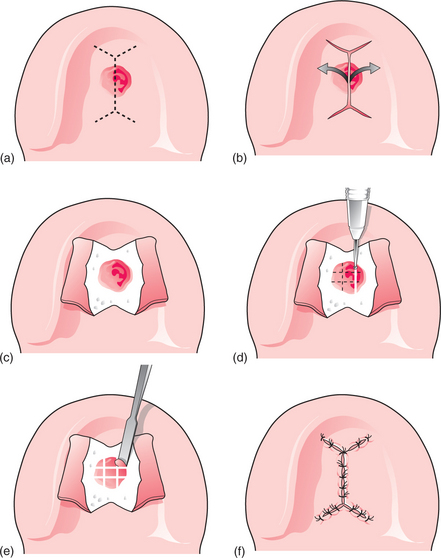
Fig. 11.15 Removal of a palatal torus. (a) A midline incision is made across the bony mass, with lateral extensions anteriorly and posteriorly. (b, c) The mucoperiosteal flaps are reflected to expose the bony mass. (d) A bur is used to divide the torus into small pieces. (e) A chisel is used to elevate the small fragments of bone from the hard palate. (f) The wound is debrided and the bone is smoothed with a bur, then sutures are placed to close the wound.
A mandibular torus is exposed by raising a lingual flap, releasing the gingival margin around any teeth adjacent to the torus. If the patient is edentulous, the incision is along the crest of the alveolar ridge, avoiding the mental neurovascular bundle (Fig. 11.16). A surgical bur or chisel and mallet may then be used to divide the torus from the surface of the mandible. After removal of the excess bone, the osteotomized surface is palpated to ensure a smooth outline before the lingual flap is replaced and sutured (a surgical stent may be placed to prevent dead space and haematoma formation).
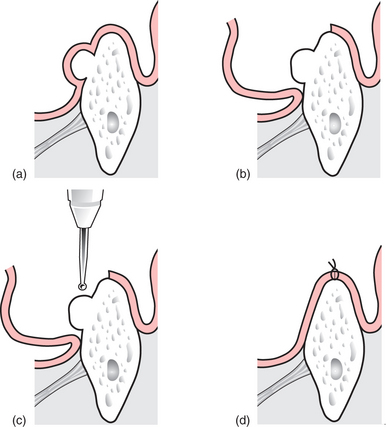
Fig. 11.16 (a) A lingual torus is covered by thin oral mucosa, and considerable care is required to avoid accidental perforation of the flap. (b) The mucoperiosteal flap is raised to expose the entire bony mass. (c) A surgical bur or chisel may be used to remove the bony torus. Conscious patients may find the sensation of the chisel being used unpleasant, but in experienced hands the technique is quick and safe. (d) The wound is closed with multiple resorbable sutures.
Restoration of grossly deficient denture-bearing areas
Many surgical procedures have been devised to augment atrophic jaw bone. A key problem with bone augmentation is the resorption that follows such surgery, leaving the patient without significant gain in function. Bone grafting on its own is insufficient to improve a patient’s deficiency. When undertaken in combination with endosseous implants, the outcome of bone grafting is often highly encouraging.
OSSEOINTEGRATED (ENDOSSEOUS) IMPLANTS
Endosseous implant surgery offers considerable flexibility in preprosthetic surgery, but the practitioner should gain experience in minor oral surgery procedures before contemplating implant surgery. Further training is required to acquire the additional diagnostic and surgical skills required. Implant companies will not usually sell implant components to a dentist who has not undertaken training in their implant system.
There are three main types of jaw implant:
Endosseous implants
In the past few decades the management of tooth loss has been revolutionized through endosseous implant surgery. Brånemark and colleagues pioneered research on the integration of titanium implants with direct bone contact in the 1960s. Most endosseous implants are constructed from pure titanium because of its ideal biological performance characteristics as an implant material.
Osseointegration is a clinical and histological concept that describes the natural apposition of bone to an implant with a subsequent ability of the implant to sustain loading and transfer the load to and within the adjacent bone (Fig. 11.17). Stringent clinical and technical standards are required to achieve osseointegration. Survival rates for titanium implants in excess of 86% in the mandible and 78% in the maxilla at 15 years have been reported. Recent advances in implant design and surface treatment technology have improved the survival rates.

Fig. 11.17 Photomicrograph showing the intimate relationship between newly formed bone and a titanium endosseous implant (shown in black) embedded within cancellous bone of the jaws for 12 weeks.
Factors that influence the success of endosseous implants
Implant systems
There are many different implant systems. In selecting a suitable system, manufacturers’ claims about the superiority of a particular system should always be supported by laboratory data and published clinical trials. Most are based on a cylindrical or screw design. Implant systems are usually placed as a single-stage fixture (the implant or its healing abutment protrudes into the oral cavity on insertion) or two-stage (the implant is buried beneath the oral mucosa for several months to osseointegrate before it is exposed; a fixture that protrudes into the oral cavity is then inserted). The trend now is for implants to be loaded immediately on insertion or after a relatively short period of osseointegration (a few weeks).
Treatment planning for endosseous implants
A complete history and examination will establish the patient’s suitability for implants. A standard proforma for implant surgery will ensure a comprehensive, systematic history and examination. The medical history will identify possible contraindications for implants. An appraisal of the remaining dentition, the periodontal tissues and the standard of oral hygiene is required. Surgical access to the implant site is also assessed (Fig. 11.18). The type of anaesthesia is discussed with the patient at an early stage; intravenous sedation with local analgesia may be preferred in the outpatient or dental practice setting.

Fig. 11.18 Access to the implant site should always be assessed before embarking on implant surgery. At the beginning of site preparation there is little room to get the drill in a good position.
Contraindications for endosseous implants
Endosseous implants are not recommended for patients below the age of 16 because of the potential for further growth of the jaws; the implant is ankylosed in the bone, and therefore it will become sub-merged as the jaws grow. There is no absolute upper age limit for endosseous implants.
A patient’s medical history will determine their suitability for endosseous implants. For example, a poorly controlled diabetic is at risk of infection and soft-tissue breakdown around an implant, which may contraindicate implant surgery. The patient may have a history of psychosis, or there may be an ongoing history of drug or alcohol abuse. Such patients are unsuitable for implant surgery. Referral for a specialist opinion is recommended if there is doubt about the suitability of a patient with medical problems for implant surgery.
Poor oral hygiene will compromise implant provision because of peri-implant inflammatory disease (which is destructive in a manner similar to periodontitis). Patient education can effectively improve oral hygiene status in some patients. A patient must demonstrate consistency in maintaining their oral hygiene over several months; only then can implants become a feasible option. Smoking is a relative contraindication, because some smokers are at increased risk of losing the implant through inflammation of the peri-implant mucosa, and increased resorption of peri-implant bone. This manifests clinically as an increase in the bleeding index, the peri-implant pocket depth, the degree of peri-implant mucosal inflammation and radiographic evidence of bone resorption mesial and distal to the implant. There is emerging evidence of an increased risk for implant loss in patients on bisphosphonates, though the risk for patients on oral bisphosphonates seems to be less than for patients having intravenous doses (see Ch. 4, p. 42 concerning osteonecrosis following tooth extraction).
Special investigations
The height, width and overall shape of the residual ridge are evaluated from study models and radiographs to ensure adequate bone to support the implant. Articulated study casts are required to evaluate the occlusion; there should be no excessive forces on the implant during lateral or protrusive excursions of the jaws. A preliminary assessment of the ideal position and angulation of implants may be made from the study casts, in conjunction with a surgical stent (Fig. 11.19). Radiographs (Fig. 11.20) will determine the quality of the bone and help in assessing suitable sites for implants. The radiographs should adequately demonstrate important structures (the inferior alveolar neurovascular bundle, the floor of the nose, the maxillary antrum and adjacent teeth).
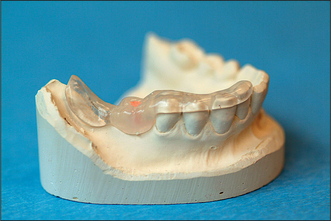
Fig. 11.19 An acrylic stent is placed in the mouth before radiography to evaluate the quality and quantity of bone at the desired site of implant insertion. Gutta percha inserted into a bur hole cut into the acrylic stent will assist in radiographic planning. The dimensions of the gutta percha and the angulation of the bur hole permit accurate assessment of the proposed implant site.
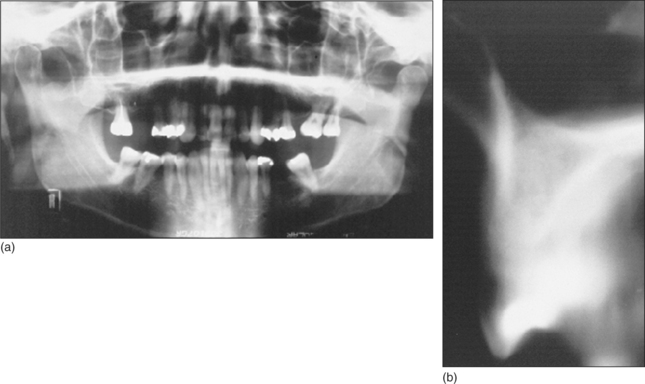
Fig. 11.20 (a) A panoramic radiograph yields much information about the teeth and jaws, but is unhelpful in determining the suitability of the bone at the proposed site of an implant in tooth 16 position. (b) A tomographic view of the bone in the tooth 16 area gives more information about the quality of the bone and the height of the maxillary sinus.
It is necessary to establish whether an implant can be placed with the desired stability within bone and satisfactory soft-tissue aesthetics. If there is insufficient bone, then bone grafting must be considered. Bone may be grafted from the patient, e.g. from the chin (Fig. 11.21), tuberosity region or retromolar region in the mandible. Proprietary bone scrapers facilitate the collection of autogenous bone by scraping the cortical surface. Blocks of cortical bone may be taken, or cancellous bone chips may be harvested, depending on the extent of bone deficiency at the implant site.
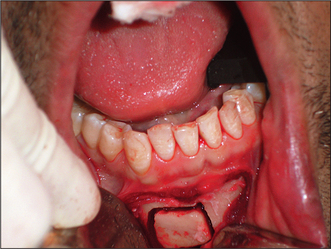
Fig. 11.21 A block cortical bone graft is being harvested from the patient’s chin to augment an atrophic upper central incisor socket. The block graft will be fixed with a bone screw at the recipient site.
When the soft tissue is deficient, a connective tissue or mucosal graft might be indicated. Such soft-tissue grafts are taken from the hard palate. Connective tissue grafts e.g. Alloderm (an acellular dermal matrix derived from donated human skin tissue) can also be purchased for use in such situations. The key objective with a soft-tissue graft is to re-establish the gingival contour for aesthetic reasons.
Determining the optimum length of an implant
Most X-ray units do not give 1:1 magnification of the image: this must be borne in mind when planning the optimum dimensions of an implant from the radiographs. An acrylic stent may be used to determine the planned location of an implant. The stent is fitted over the teeth or edentulous jaw (Fig. 11.19) when the radiograph is taken.
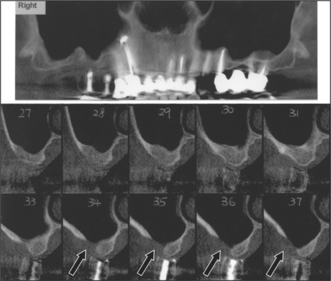
CT scans (Fig. 11.22) are gaining popularity in the assessment of a patient before implant surgery. Cone-beam CT scan units offer improved functionality and convenience over conventional CT scanning units (http://www.imagingsciences.com/pro_iCAT_features.htm). In the above illustration, a patient requesting implants in the right posterior maxillary sextant has undergone an I-Cat scan to assess the bone. There is a deficiency in the buccal bone in sections 34–36, and clearly bone grafting is required before implants can be placed.
Planning the site of the implants from the radiograph
Endosseous implants are positioned within healthy bone, with an adequate height and width of bone. Forces applied to an implant should be axial rather than lateral, to avoid forces that might result in implant failure.
A radiograph is a medicolegal document and should not be altered in any way. A copy of the radiograph is therefore made (either a digital copy or a copy made on tracing paper from the original) and the teeth and other anatomical structures such as the inferior alveolar canal, the floor of the nose and the maxillary antrum are highlighted on the copy. A transparent stencil (fixture guide) is superimposed on the tracing to plan with accuracy the proposed position of the implant. The fixture guide offers various magnifications depending on the X-ray unit used. The tracing may be used to illustrate the treatment plan to the patient.
The morphology of the residual ridge and the thickness of overlying mucosa are determined at the proposed site for the implants. Unless sophisticated CT scanning is available, a suitable implant cannot otherwise be selected reliably, and the procedure might have to be abandoned if there is inadequate bone. The depth of the oral mucosa cannot be assessed from a periapical or panoramic radiograph, because the image records the residual ridge only in two dimensions. Ridge mapping (Figs 11.23, 11.24) is simple and reliable, but may cause temporary mucosal trauma and discomfort.
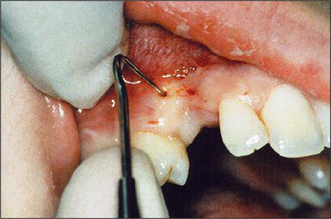
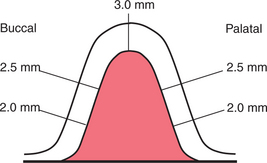
Ridge mapping
Under local anaesthesia, a probe with millimetre markings along its tip is inserted into the oral mucosa overlying the alveolar ridge. The depth of the soft tissue is noted at all sites (Figs 11.23, 11.24). This information is transposed to a study model, and the shape of the residual ridge is recorded by trimming back the model stone to the corresponding depth of soft tissue.
Diagnostic wax-up
Having planned the position of the implants, a diagnostic wax-up (Fig. 11.25) will ensure that the desired aesthetic result can be achieved. If retained roots or other lesions are present, implant surgery must be deferred for 4–6 months after surgical intervention, to ensure satisfactory healing.

Informed consent
A complete discussion with the patient of all aspects of surgery, prior to commencing treatment is a requisite for consent for any operative procedure (see Ch. 2). For procedures which are lengthy, expensive and irreversible, such as implant surgery and subsequent prosthodontic rehabilitation it is doubly important. Only when the patient fully understands what is proposed can they establish realistic expectations of the treatment. Misunderstandings about implant therapy can be avoided when a written outline of the treatment proposed is given to the patient to read and sign. An individual having high (unreal-istic) expectations may be disappointed by the outcome of surgery, and litigation may ensue. Written documented evidence of informed consent will help to avoid legal proceedings.
SURGICAL PROCEDURE FOR ENDOSSEOUS IMPLANTS
There is a trend towards flapless surgery. The clinician will decide preoperatively whether a flap is required, based on past experience and clinical circumstances.
Flap design
Access is usually gained to the alveolar bone via a broad-based flap to ensure good visibility and reduce the risk of ischaemic necrosis of the flap extremities. The wound will be closed around a single-stage (transmucosal) implant, and the incision should take into consideration the site of the implant. For a two-stage implant the flap is extended palatally, and a rim of soft tissue is preserved around the cervical margin of adjacent teeth. Incisions are placed to avoid friction from a denture during healing.
The mucoperiosteal flap is incised; it may be tightly bound to an edentulous alveolar ridge, and flap elevation is sometimes difficult. Damage to the periosteum may result in postoperative pain and swelling of the tissues and delayed healing. If the flap is perforated, dehiscence or wound infection may result. Extensive exposure of the implant site is usually unnecessary; the blood supply to mandibular bone is dependent on intact periosteum and muscle insertions into the bone.
Insertion of implants immediately after tooth extraction
Immediate implant insertion is gaining popularity, with good outcomes. In some circumstances it may be possible to insert an implant immediately after tooth extraction. Although undertaken by some operators with good results, this technique is not recommended routinely; each case is planned according to clinical circumstances. For example, the prognosis for successful osseointegration is poor in the presence of apical pathology prior to implant insertion. Other problems likely to be encountered include differences between the width of the natural tooth root and the endosseous implant and insufficient bone at the coronal aspect (a bone graft may be required to close the defect). A further disadvantage is that non-keratinized mucosa may have to be advanced to cover the implant.
A solution to the technical problems described above is to remove the tooth or root and insert the implant 4–6 weeks after extraction, when the soft tissues will have healed but the alveolar bone will not have undergone excessive resorption.
Preparation of bone and insertion of the implant
The manufacturer’s recommended technique for preparation of the implant site is adhered to at all times. Important factors related to bone preparation are the cutting efficiency and speed of rotation of burs, the use of sterile coolant and the rate of bone cutting. The cutting efficiency of a bur will influence the survival of adjacent bone and the rate of healing. Surgical implant burs (Fig. 11.26) may be designed for single or multiple use; only sharp implant burs are used. Reusable burs are cleaned thoroughly before autoclaving to remove organic debris.
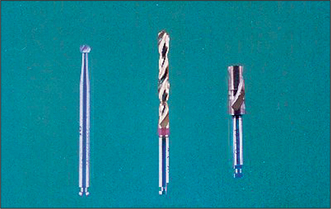
Fig. 11.26 Examples of burs used to prepare bone for an implant. The pilot hole is prepared with the bur on the left; the initial bone preparation is made with the bur in the centre and the cortical bone is cut with the bur on the right.
Sterile saline coolant is required at all times during bone cutting. The coolant itself may be refrigerated before use. Even when coolant is used, the temperature adjacent to drills may become excessive without due care; the threshold for tissue damage due to heat from friction during bone preparation is estimated to be 47°C for 1 minute. Gentle pressure is applied to the handpiece when cutting bone, and the bur is removed frequently from the bur hole and allowed to cool. With some implant systems an internal irrigation system may be used to direct coolant to the tip of the drill.
If the alveolar ridge is uneven where the implant is to be inserted, alveoplasty is undertaken before a pilot hole is created through cortical bone. An acrylic stent, prepared with a bur hole for the proposed site of the implant, is fitted over the teeth and the pilot hole is cut into bone through the hole in the stent. Fine bone shavings are often present in the grooves of the bur. If these are removed and stored in sterile saline, they may be used later as a graft to pack around the implant before wound closure. Bone chips may also be collected via the suction apparatus if a special collecting device is attached.
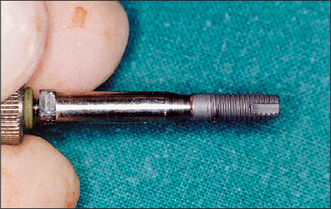
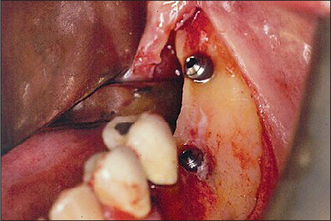
The pilot hole is progressively widened with burs of increasing diameters. If a self-tapping implant is to be inserted, the hole is prepared (Fig. 11.27) to accommodate the implant without excessive tightening force; otherwise the screw thread of the implant might shear. Insertion of a self-tapping implant generates heat through friction, and implant insertion is undertaken slowly. The implant is loaded onto its insertion tool (Fig. 11.28) and the surface of the implant is not touched, to avoid contamination. After insertion of the implant, the cover screw is placed (Fig. 11.29). Blood is washed out of the screw threads before a cover screw or healing abutment is placed; it may be difficult to remove later.
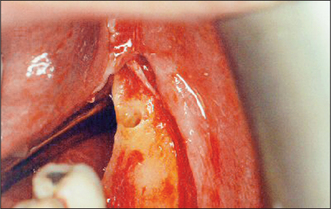
Fig. 11.27 A completed bur hole is irrigated with saline before checking its depth. The lingual aspect of the alveolar ridge should also be checked to ensure that the bur hole has not perforated lingual bone.
Wound closure
The choice of suture material depends on personal preference. If a resorbable suture is used, the suture should remain within the tissues sufficiently long for early wound healing. The ideal retention period for resorbable sutures is 5–14 days.
If single interrupted sutures are placed, care is taken to ensure that the wound edges are approximated accurately without tension. A vertical mattress technique is helpful if the mucosal incision is to be closed near to a muscle attachment (e.g. mentalis muscle), resulting in additional displacement forces on the flap. This will reduce the risk of wound dehiscence, which sometimes occurs in the edentulous mandible after insertion of an implant.
Postoperative care
The patient is reminded of the possibility of postoperative pain, swelling and bruising. There may also be loss of sensation in the oral mucosa, or discomfort relating to a prosthesis. Postoperative antibiotics may be prescribed if a single preoperative dose has not already been given. The patient must refrain from wearing a denture over the implant until the follow-up appointment at 1 week.
The patient will have a soft diet and will keep the wound clean by hot salt-water mouth bath irrigation. The patient should refrain from examining the wound because retraction of the lip may encourage wound dehiscence. A follow-up appointment is made for 7–10 days after surgery. A soft lining (e.g. Coe-Comfort) is recommended when a denture is re-inserted a week after surgery, after extensive trimming of the fitting surface. The patient is advised to remove and clean the denture at night.
The implant is allowed to osseointegrate before physiological loading (after approximately 10 weeks). However, the optimum time for osseointegration is influenced by factors such as the health status of the patient and the quality of the bone around the implant. Therefore, when deciding the most suitable time to load an implant, each case is considered on its own merits.
Second-stage surgery to expose an implant
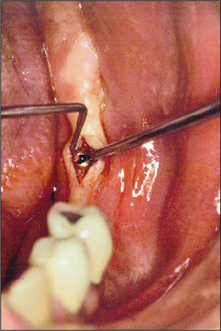
After the healing phase is complete it can sometimes be difficult to determine the exact location of a two-stage (submucosal) implant. A dental probe can be used to palpate the cover screw through the anaesthetized tissues. Once the cover screw is located, a crestal incision is made to expose it (Fig. 11.30). The cover screw is then removed and a healing abutment inserted. If necessary, resorbable sutures are placed to ensure close apposition of the oral mucosa to the healing abutment (Fig. 11.31). After a period of 7–10 days, the healing abutment is replaced with a suitable abutment that will subsequently be loaded.
PROSTHODONTIC REHABILITATION AFTER IMPLANT SURGERY
Prosthodontic rehabilitation typically involves the use of ball attachments, magnets, a retentive bar with clips to support an overdenture, or the construction of a fixed prosthesis (e.g. a crown or bridge as seen in Fig. 11.32). Further discussion of the methods employed may be obtained from a suitable textbook on dental prosthetics.
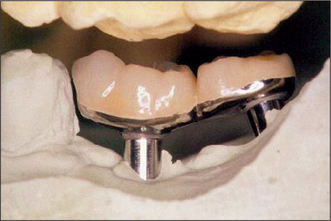
Fig. 11.32 The fixed prosthesis with the free-end saddle fabricated for the patient in Figs 11.27-11.31.
COMPLICATIONS OF ENDOSSEOUS IMPLANT SURGERY AND THEIR MANAGEMENT
Inappropriate placement of implants may be avoided by meticulous preoperative planning. Haemorrhage is unusual during surgery, but life-threatening haemorrhage has been reported after placement of mandibular implants (through accidental perforation of the lingual cortical plate and rupture of the sublingual artery). The morphology of the lingual aspect of the mandible is assessed before drilling. Trauma to the inferior alveolar nerve is another distressing complication, and immediate referral is advised to ensure appropriate specialist care.
Wound infection is unusual in the early healing phase, and is controlled with a suitable antibiotic. Chronic peri-implant infection may result from poor oral hygiene. However, the patient’s inability to maintain good standards of oral hygiene should have been identified early in the planning stage. Chronic peri-implant infection is difficult to control, and may result in loss of the implant if the patient’s oral hygiene standards do not improve.
Mandibular fracture is a rare complication after implant insertion, but can occur in the atrophic mandible. The dental surgeon should be vigilant, both during surgery and in the healing phase, to identify the signs of a mandibular fracture. Immediate referral to an oral and maxillofacial surgeon is appropriate.
MAJOR PREPROSTHETIC SURGERY
Many techniques to augment the edentulous jaws have been developed. However, most have fallen out of favour, principally because of the poor results obtained.
Orthognathic surgery has a role to play in the management of some jaw discrepancies (Fig. 11.33). The surgical techniques employed are described in Chapter 12.
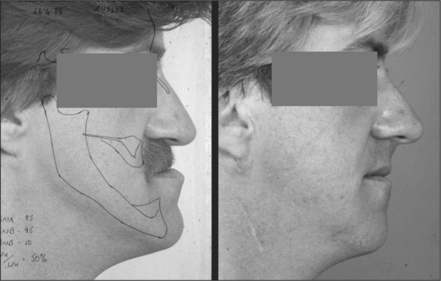
Fig. 11.33 Left: this edentulous patient underwent a vertical ramus osteotomy to correct his mandibular prognathism. Cephalometric tracings have been superimposed over the photograph to aid in planning the surgery. Right: the postoperative profile view. The patient was able to masticate more efficiently after correction of the mandibular prognathism and provision of new dentures.
Reconstructive surgery is indicated in a few patients to provide a stable bony base for a fixed or removable prosthesis, particularly after resection of oral cancer. These major procedures are outside the scope of practice of the general dental practitioner—referral to an oral and maxillofacial surgeon is appropriate. Reconstructive surgery for prosthodontic rehabilitation is described in contemporary oral and maxillofacial surgery textbooks.
Adell R. The surgical principles of osseointegration. In: Worthington P., Brånemark P.I., editors. Advanced osseointegration surgery: applications in the maxillofacial region. Chicago, IL: Quintessence; 1992:94-108.
Adell R., Eriksson B., Lekholm U., et al. Long-term follow-up study of osseointegrated implants in the treatment of totally edentulous jaws. International Journal of Oral and Maxillofacial Implants. 1990;5:347-359.
Berg R., Morgenstern N.E. Physiologic changes in the elderly. Dental Clinics of North America. 1997;41:651-668.
Brånemark P.I., Adell R., Breine U., et al. Intraosseous anchorage of dental prostheses. I. Experimental studies. Scandinavian Journal of Plastic and Reconstructive Surgery. 1969;3:81-100.
Brånemark P.I., Hansson B.O., Adell R., et al. Osseointegrated implants in the treatment of the edentulous jaw. Experience from a 10-year period. Scandinavian Journal of Plastic and Reconstructive Surgery. 1977;16(Suppl):1-132.
Cawood J.I., Howell R.A. A classification of the edentulous jaws. International Journal of Oral and Maxillofacial Surgery. 1988;17:232-236.
Fiske J., Davis D.M., Frances C., Gelbier S. The emotional effects of tooth loss in edentulous people. British Dental Journal. 1998;184:90-93.
Hildebrandt G.H., Loesche W.J., Lin C.F., Bretz W.A. Comparison of the number and type of dental functional units in geriatric populations with diverse medical backgrounds. Journal of Prosthetic Dentistry. 1995;73:253-261.
Lemons J.E., Laskin D.M., Roberts W.E., et al. Changes in patient screening for a clinical study of dental implants after increased awareness of tobacco use as a risk factor. Journal of Oral and Maxillofacial Surgery. 1997;55(Suppl 5):72-75.
Norton M. Dental implants—a guide for the general practitioner. Chicago, IL: Quintessence, 1996.
Terry B.C., Zarb G.A. Report on 4th International Congress on Preprosthetic Surgery, Palm Springs, FL, 18–20 April 1991. International Journal of Oral and Maxillofacial Surgery. 1991;20:314-316.
Verhoeven J.W., Cune M.S., Van Kampen F.M., Koole R. The use of the transmandibular implant system in extreme atrophy of the mandible; a retrospective study of the results in two different hospital situations. Journal of Oral Rehabilitation. 2001;28:497-506.
Wardrop R.W., Hailes J., Burger H., Reade P.C. Oral discomfort at menopause. Oral Surgery. 1989;67:535-540.
Wedgwood D., Jennings K.J., Critchlow H.A., et al. Experience with ITI osseointegrated implants at five centres in the UK. British Journal of Oral and Maxillofacial Surgery. 1992;30:377-381.