12 Surgical aids to orthodontics and surgery for dentofacial deformity
ASSUMED KNOWLEDGE
It is assumed that at this stage you will have knowledge/competencies in the following areas:
If you think that you are not well equipped in these areas, revise them before reading this chapter or cross-check with texts on those subjects as you read.
THE ORTHODONTIC/ORAL SURGERY INTERFACE
Oral and maxillofacial surgery, in the context of this chapter, includes a wide spectrum of procedures ranging from the removal and exposure of unerupted teeth to bimaxillary osteotomies. In planning these procedures, it is essential to involve the specialist orthodontist and the patients themselves from an early stage.
Surgery in the orthodontic patient will often be an integral part of a protracted treatment programme which may, especially in the case of adult fixed-appliance therapy, take 2 years or more to complete. It is essential, at the planning stage of the dentoalveolar surgery, that patients understand (and are willing to comply with) the extent and duration of the proposed therapy.
This prolonged treatment may relate either to the creation of space for eruption or to the application of external mechanical force to stimulate/induce the eruption of malpositioned teeth. Patients with dental indicators of poor motivation such as irregular attendance, high caries rates and inadequate oral hygiene should have appropriate treatment plans. The treatment administered should be simplified as far as possible to reflect the anticipated extent of cooperation from the patient and to expedite any prescribed treatment. Whilst in the past orthodontics has principally been undertaken in adolescents, adult orthodontics is becoming increasingly popular. Any relevant medical history will influence the type of treatment the patient is offered and the mode of anaesthesia.
The interface between oral surgery and orthodontics is difficult to define accurately but relates to those patients whose treatment decisions lie within both specialties. There will always be cases where choices must be made—to recommend orthodontics alone, surgery alone, a combination of the two or whether no intervention should be recommended. Decision-making in complex cases requires a combination of skill and experience and must be taken with the patient’s best interests as the fundamental starting point.
MANAGEMENT OF UNERUPTED AND IMPACTED TEETH
Nowhere is the practice of dentoalveolar surgery and orthodontics more closely related than in the management of unerupted and impacted teeth. The teeth most frequently affected by failure of eruption are generally the last to erupt in a particular series—wisdom teeth, canines and second premolar teeth. The management of third molar teeth is discussed in Chapter 5.
Assessment of unerupted teeth—clinical
In orthodontic cases it is unusual for patients to suffer any symptoms from unerupted teeth; they are far more frequently noted after clinical examination or as incidental radiographic findings. Careful monitoring of the eruption of the dentition is essential and the general dental practitioner is best equipped to perform this task. The combined oral surgery and orthodontic treatment options for unerupted teeth are threefold: extraction, exposure ± orthodontics and autotransplantation (most frequently of canines). In some cases (e.g. mesiodens when no orthodontics is planned) unerupted teeth may be left in situ. The autotransplantation of teeth is performed far less frequently than it was in the past due to unpredictable results and the reliability of osseointegrated implants and adhesive bridgework.
The timing of extractions or exposure is dependent on the age of the patient and the stage of development of the dentition. The principal treatment decision in the management of unerupted teeth is whether to extract. In general terms the rationale for removal of unerupted/malpositioned teeth resembles that for wisdom teeth (see Ch. 5). The principal indications for extraction are:
There is some evidence that timely extraction of deciduous teeth may prevent later impaction, particularly in the case of upper canines.
The surgical and radiographic assessment of unerupted teeth in orthodontic cases is based upon determining:
Whilst the crowns of these teeth are frequently in communication with the oral cavity, even where the teeth are not directly visible, clinical examination and palpation of the alveolus will often demonstrate a bulbosity associated with crowns of unerupted teeth, thereby giving an indication of their position. Additionally, the inclination of adjacent teeth may give some important clue to the position of the crown of an unerupted tooth. Radiographic analysis, however, is essential to determine the apex position, morphology and pathologies associated with unerupted teeth.
Assessment of unerupted teeth—radiographic
Radiographic assessment of the unerupted tooth will provide several valuable pieces of information in planning its management: stage of tooth development, crown/root morphology and angulation and the presence or absence of local disease. Most orthodontic assessment will include an orthopan-tomogram (OPT) and a lateral cephalometric view. Intraoral views are essential, however, for the management of unerupted maxillary anterior teeth due to the poor definition of the OPT in this region. In this situation, the OPT will usually be supplemented with periapical and/or upper anterior occlusal films. The use of ‘parallax’ analysis, in which two periapical views of the same area are taken from different angles (see Ch. 5), can be useful in determining whether the impacted teeth are buccal or palatal and therefore in planning the surgical approach to the teeth. In radiographic analysis, the stage of tooth development must also be carefully considered because it is inappropriate to expose teeth whose development is incomplete.
Exposure of unerupted teeth
The assessment of whether unerupted teeth are suitable for exposure is beyond the scope of this text and should be undertaken in conjunction with an orthodontic specialist. The decision to expose or not, however, is principally based on three factors: the angulation of the unerupted tooth, the depth of impaction and the relationship to other teeth. In general terms there are four treatment options:
The principles of treatment planning are discussed below in relation to the anterior maxillary region but can equally be applied in relation to unerupted teeth at other sites (most commonly mandibular second premolar teeth or even wisdom teeth).
The objective of exposing an unerupted tooth is to move it into a good functional and aesthetic position. In assessing teeth for exposure one of the prime considerations is the available space into which the tooth can erupt. This may be estimated by comparing the crown width of the unerupted tooth with the available space, either directly from the radiograph (with reference to the magnification in the system) or by measurement of the crown width of the contralateral corresponding tooth.
Surgical technique
Exposure at its simplest consists of removal of the soft tissues overlying the crown of an unerupted tooth under local anaesthetic. The exposure of teeth in this fashion has major disadvantages:
Attempts should be made to retain the keratinized tissues by employing displacement of the attached gingiva with apically or, occasionally, laterally repositioned flaps. The apically repositioned flap retains the mucogingival collar around the tooth and is displaced apically and sutured into place. The bunched gingiva will remodel as wound healing occurs (Fig. 12.1). If the tooth is misaligned, a bracket and gold chain may be etched to the canine to direct its eruptive path appropriately (Fig. 12.2).

Fig. 12.1 An erupted canine 3 months after exposure using an apically repositioned flap. The irregular gingival contour will gradually diminish with the passage of time.

Fig. 12.2 A bracket and gold chain bonded to the buccal surface of an exposed canine. The chain can be attached to a fixed appliance to direct the tooth into the correct location.
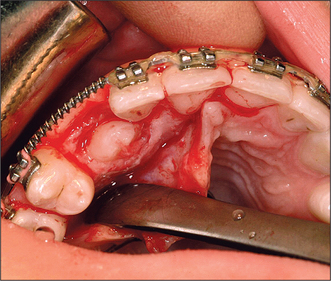
Although simple exposure is satisfactory for superficially placed teeth situated close to the surface and impacted in soft tissue alone, most unerupted teeth are located more than 3–4 mm from the oral mucosal surface and the crown cannot be seen completely after raising a flap (Fig. 12.3). As impaction of unerupted teeth usually involves hard tissue as well as soft tissue, all bone covering the tip of the crown as far as the maximum width of the tooth should be carefully removed. If the tooth is superficial and covered by thin bone this can often be undertaken using a scalpel blade. Where bone coverage of the unerupted tooth is more extensive, a small rose head bur or hand-held chisel may be used to clear overlying bone from the crown. Extreme caution must be taken to avoid damaging the tooth crown and the roots of the adjacent teeth. Unnecessary removal of bone should also be avoided. Whilst soft- and hard-tissue exposure of unerupted teeth is in some instances successful, most commonly (and especially in the case of deeply impacted teeth) the created surgical defect will become re-epithelialized if patency is not maintained. The defect is, therefore, packed with an antiseptic gauze dressing or a glass-ionomer cement bonded to the tooth crown in order to inhibit contraction and re-epithelialization (Fig. 12.4). Postoperative antibiotics are seldom indicated unless there is a known increased risk of wound infection, e.g. patients with insulin-dependent diabetes mellitus.
Mechanical traction and unerupted teeth
The application of mechanical force to stimulate and guide eruption of buried teeth is frequently necessary because the angulation of the root of an unerupted tooth is frequently unfavourable. This mechanical force may be employed in a number of ways: gold chains, steel or elastic ligatures and even magnets attached to an orthodontic appliance have all been used to induce the eruption. Mechanical traction is indicated:
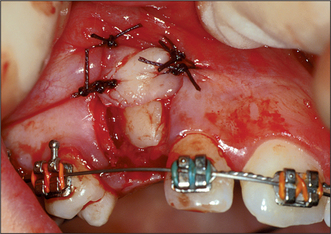
If the crown tip of a maxillary canine is beyond the midline of the lateral incisor root, spontaneous eruption will not usually occur and mechanical traction will be necessary. Bonding of the bracket to the tooth following its exposure (Fig. 12.5) involves a sequence of etching, washing, drying and bonding similar to that employed in conventional adhesive dentistry. Bonding is best performed in collaboration with an orthodontist to ensure the angulation and position of the bracket is appropriate in relation to the force to be applied to the tooth. During the procedure maintenance of a meticulously dry field is essential and this is facilitated by careful suction and local infiltration of epinephrine-containing local anaesthetic.
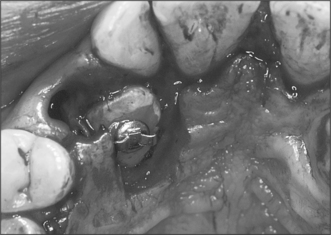
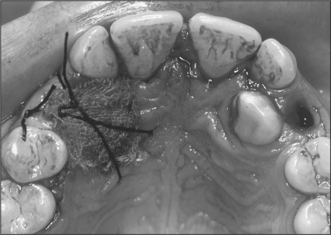
Fig. 12.5 A bracket bonded to the palatal surface of an unerupted canine. Either wires or elastics can be attached to the cleat.
Following the bonding, the flap is apically repositioned (see earlier) or may simply be closed as both compare favourably if external traction is to be applied. If traction is not to be applied immediately, the ligatures or chains may be sutured to the mucosa or orthodontic appliance using non-resorbable material. This minimizes any discomfort from the loose chain.
Although bonding could be undertaken as a second procedure following exposure, this results in greater inconvenience and discomfort to the patient. Whilst simple exposures can typically be undertaken under local anaesthesia, bonding (where the procedure is more protracted and requires excellent moisture control in the operative site) is generally best performed under general anaesthesia.
Autotransplantation and surgical repositioning of teeth
In the past, autotransplantation was a popular treatment for unerupted canine, premolar and even molar teeth but there are some considerable biological problems associated with the technique to be overcome. Although individual studies have suggested clinical and radiographic success rates as high as 80% for the transplantation (at 1–5 years following surgery), most transplanted teeth will develop evidence of root resorption or even ankylosis if they are not root-treated. The success rate of transplantation can be maximized by careful handling of the tooth and preparation of the socket with minimal trauma. Resorption is directly influenced by the extent of trauma to the periodontal tissues on the root surface and care must be taken to minimize this during the removal of the tooth. For this reason, transplantation should be undertaken only on young, medically fit patients and should exclude all teeth which will be difficult to extract or those with hooked apices which will preclude simple elevation.
During the removal of the unerupted tooth only the crown of the tooth should be manipulated with instruments and whilst the socket is being prepared the tooth is ‘stored’ in the buccal or palatal sulcus beneath the flap. When preparing the ‘socket’, bone removal should be undertaken very carefully, with particular reference to not generating heat. A slow-running, well-irrigated bur is the preferred option to achieve this, although some surgeons use small chisels or osteotomes to remove the bone or expand the socket.
The repositioned tooth should be secured free from occlusion and splinted in place, usually by direct bonding using orthodontic brackets or wire and composite. Alternatively a thin vacuum-formed splint can be constructed and cemented in place. Following removal of the splint (usually after 3 weeks) the tooth should be root-filled with calcium hydroxide and reviewed clinically and radiographically at regular 3-month intervals for at least 1 year to check for resorption or ankylosis. Although the technique appears to be reasonably successful in the short term, the advent of adhesive bridgework and osseointegrated implants offers far more reliable, less inconvenient alternatives to management of missing maxillary canines. These techniques also avoid the inexplicable ‘late loss’ of transplanted teeth, which may occur after 10–15 years.
SUPERNUMERARY TEETH AND ODONTOMES
Supernumerary teeth may occur as teeth with normal morphology (supplemental) or with abnormal or rudimentary form. Supplemental teeth may be left in situ if they are cosmetically and functionally acceptable.
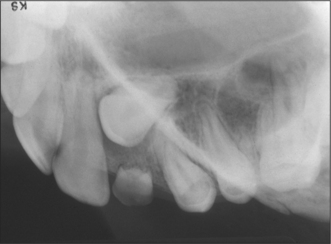
Supernumerary teeth and odontomes often must be removed as they can delay eruption or impede orthodontic tooth movement, particularly of maxillary incisors. If supernumerary teeth are removed from the path of eruption, the underlying teeth will often erupt given sufficient space. It has been estimated that this will occur spontaneously in approximately 60% of cases. If the underlying teeth fail to erupt, a second operation will be required to expose the teeth and apply mechanical traction. To avoid this risk some clinicians advocate the application of mechanical traction to the underlying permanent teeth when the overlying supernumerary teeth are removed. It is increasingly being recognized, however, that deeply buried supernumerary teeth in fully developed dentitions can be left in situ (Fig. 12.6) and require nothing more than occasional radiographic review. If these teeth are to be removed then careful surgical technique is essential to minimize risk of damage to adjacent unerupted teeth or the roots of erupted teeth (see Ch. 5).
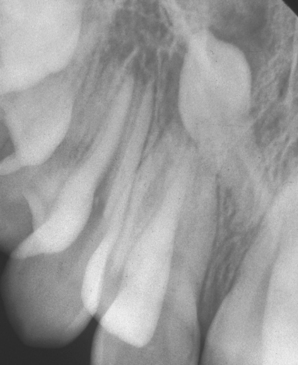
Fig. 12.6 An inverted supernumerary tooth—usually referred to as a mesiodens if it occurs in the incisor region. It should only be removed if there is a genuine clinical indication.
Odontomes are less common than supernumerary teeth, although the differentiation between the two is considerably blurred. Odontomes may be simple (tooth-like), compound (multiple tooth-like) or complex composite (containing elements of the tooth germ in a disorganized fashion). All true odontomes are benign, do not grow and are not true tumours. Like unerupted teeth, odontomes need only be removed if there are clinical indications (infection, they are obstructing eruption of other teeth, etc.).
FRAENECTOMY
Fraenectomy—the surgical removal of fraenal attachments (usually in the midline) in the upper or lower jaw—may be a valuable surgical adjunct to orthodontic therapy (its use is also discussed in Ch. 11). Its use has been questioned over recent years and certainly the case for early surgical intervention has largely been dismissed. However, there are some instances when surgery is indicated; these are discussed below.
Labial fraenectomy
Upper labial fraenectomy aims to remove or reposition the entire labial fraenum, including its attachment to bone, and to remove all interdental tissue. It must be remembered that spacing of the incisors in children is a normal developmental process and is present until the eruption of the permanent canine teeth in adolescents. Labial fraenectomy should usually be delayed until after orthodontic treatment, unless the labial fraenum prevents closure of a diastema or displays evidence of trauma. The technique is usually performed if the fraenum extends to the incisive papilla and contributes to post-treatment stability of the orthodontically closed diastema. The pronounced fraenal attachment extending into the palate may often be viewed radiographically as a V-shaped depression. There are differing surgical techniques to remove the labial fraenum; one is outlined in Fig. 12.7 (see also Figs 11.7, 11.8).
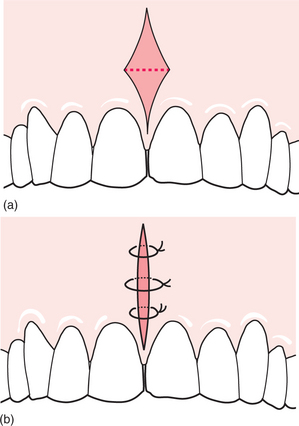
Under local anaesthesia the upper lip is firmly retracted, demonstrating the extent of the fraenal attachment. If the fraenum is particularly fibrous, its whole length is outlined and excised with a scalpel using an elliptical or rhomboid incision. The remaining fibres attached to the exposed bone can be curetted or gently removed with a bur but care must be taken not to damage the roots of adjacent teeth. The mucosa is then undermined and the defect closed with simple interrupted sutures. Patients are normally reviewed in 5–7 days.
Lingual fraenectomy
Lingual fraenectomies are occasionally recommended in younger children to assist in phonetic development or to avoid functional embarrassment. In older patients it may also be undertaken if tongue movement is so restricted that patients cannot lick the buccal surfaces of their upper molars to aid oral hygiene.
The procedure is usually performed under local anaesthesia. The surgical technique is similar to that of a labial fraenectomy although minimal tissue removal, if any, is required. The tongue is grasped and pulled upwards and the fraenal attachment is released using a single horizontal incision. The defect may be closed with two or three simple, interrupted, resorbable, 3/0 catgut sutures. Care must be taken to avoid damaging the submandibular salivary duct openings, either in the incision or when suturing the wound. Rarely, failure to undertake a lingual fraenectomy leads to periodontal problems in later life (Fig. 12.8).

ASSESSING THE NEED FOR SURGERY FOR DENTOFACIAL DEFORMITY
The development of the dentition and the facial skeleton is a series of complex and inter-related processes, beginning with the early embryological formation of the branchial arches and continuing through life with the growth of the skull, mandible and maxilla and the eruption of two dentitions. Between the ages of 6 and 12 years, the dentition is mixed and it is during these years that many of the problems of facial disproportion and malocclusion become apparent.
In addition, the cranium grows more rapidly than the rest of the skeleton and its pattern of growth (as is that of the facial skeleton) is highly complex. As such, it is perhaps surprising that in the vast majority of individuals harmonious growth occurs in three dimensions, resulting in broadly symmetrical faces with functional occlusions. Despite this, however, there is an enormous variability in forms and dimensions between sexes, individuals and cultures. Since such variation is universal, it is impossible to consider any particular pattern of growth—either the process or the end result—as ‘normal’.
Assessing the need for any surgical intervention must be on the basis of understanding the technical requirements and considering the relevant cultural, racial and ethical issues. Distinguishing between normal and abnormal variations is not always possible. However, it is possible in general terms to categorize the different types of anomalies as:
In each of these cases the variations may be symmetric or asymmetric, congenital or acquired. Treatment planning may be affected accordingly, although the general principles of treatment are not just dependent on aetiology. In all cases, however, the assessment of the need for surgical intervention must be based on a variety of factors, the principal one being the patient’s own desire for some form of treatment. Assuming this is the case, it is important to be able to recognize which cases are treatable with orthodontics alone and which will also require surgical intervention.
In general terms, orthodontics alone is unlikely to be adequate in patients:
This list is not exhaustive and does not preclude some patients from having treatment that may, at least in technical terms, be a compromise. However, most patients with any of the above problems will require surgery, and it then becomes important to determine the diagnosis of their anomalies. These will be considered in the same order as listed at the start of this section. Many technical terms have been devised to describe the jaw relationships which are useful in considering orthognathic surgery; these are italicized.
Mandibular anomalies
In relation to a normal upper jaw, the lower jaw can be too big or too small. When the mandible is too large the condition is referred to as prognathism; when it is too small it is termed retrognathia—literally, backwards positioning of the jaw. A genuinely diminutive mandible is probably better referred to as micrognathic although this term is usually reserved for cases where there is a failure of the ramus to develop. Such cases are often associated with various syndromes of the face including Apert’s and Treacher-Collins’ syndromes.
Prognathism is usually due to excessive growth of the mandible between the ages of 8 and 17 years but occasionally becomes apparent after an adolescent growth spurt. Features of prognathism include reversal of the mandibular/maxillary relationship, a reverse overjet and a diminished or absent overbite. The lower incisors tend to be retroclined and the upper incisors proclined, although they are also less visible on smiling. In addition to the increased horizontal length of the mandible there may be an increase in the vertical length. This vertical excess can be very variable and its management may be addressed by either mandibular shortening or maxillary impaction osteotomies. In addition to the simple excessive developmental growth there are other causes of prognathism, including hormonal disturbances such as would be found in cases of acromegaly. In all cases the enlargement of the mandible is basically symmetrical, although some lateral difference is always possible and the variation in the vertical dimension can be considerable.
It is also possible to have a normal skeletal base relationship (i.e. the teeth in a normal occlusal relationship) and yet have a marked protrusive or retrusive appearance in profile. This is caused by the failure of the chin to develop in proportion to the skeletal bases, excess development being termed progenia and underdevelopment retrogenia. An inadequate depth of bone between the apices of the anterior teeth and the base of the mandible is correctly termed microgenia but the term is frequently confused with retrogenia. The opposite condition, macrogenia, is also seen on occasion and all these conditions can be treated with different types of genioplasty (surgical sectioning and repositioning of the chin).
In some cases the jaw forms an asymmetric excess; this occurs commonly in condylar hyperplasia. This idiopathic condition is usually seen in patients between the ages of 20 and 40 years although it is not restricted to any age. Asymmetric loss of bone can also occur, for example, as a result of trauma or as a result of certain pathological conditions such as hemifacial microsomia, Still’s disease (juvenile rheumatoid arthritis) or severe hemifacial atrophy. Fortunately such conditions are relatively rare; they should be treated in a specialist unit. It should also be noted that asymmetry can be the result of soft-tissue changes such as masseteric hypertrophy, fibrous dysplasia or benign tumours such as neurofibromata.
Maxillary anomalies
The mid-face actually comprises some 23 bones, of which the two maxillae are fused to form the major part. The articulation of the mid-facial skeleton is complex and for many years orthognathic surgery was directed towards the mandible when the problems were really maxillary (mid-facial). Modern orthognathic surgery addresses the concept of the whole facial skeleton and the need to achieve a balance of the hard and soft tissues in three dimensions—lateral, vertical and anterior-posterior. Additionally, in developmental terms, the formation of the maxillary hard and soft tissues is complex and it is of little surprise that congenital defects in the form of cleft lip and/or palate are the world’s second most common congenital defect (see later).
Abnormal vertical development of the posterior maxilla
Increased posterior facial height may result in the anterior teeth failing to meet (i.e. a reverse overbite, which is commonly referred to as an anterior open bite). A similar condition may result from suppressed eruption of the incisors, such as that caused by thumb-sucking, but the two conditions are treated completely differently with only the former requiring surgical intervention. Isolated instances of reduced vertical dimensions of the maxilla are less common but they often accompany maxillary retrusion.
Bimaxillary anomalies
Bimaxillary anomalies are the most common type of facial variation because the growth of one jaw is always, to some extent, dependent on the other. This is clearly demonstrated in children who have cleft lips and palates. Inadequate surgical repair of the cleft in infants often inhibits growth of the maxilla in later years. This may then allow excessive growth of the mandible, resulting in a pronounced class 3 occlusion.
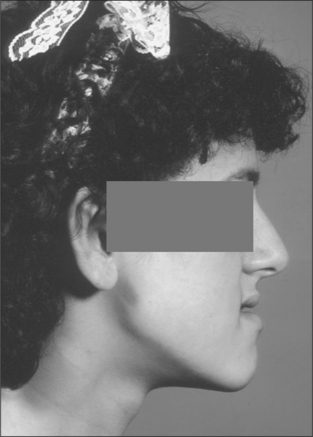
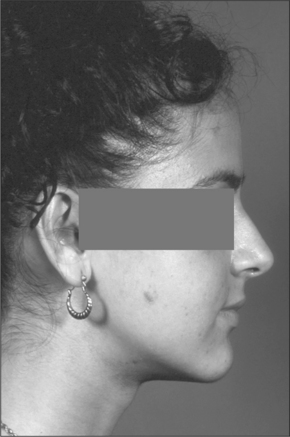
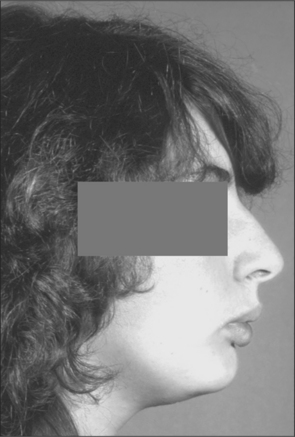
However, it is difficult to justify performing bimaxillary osteotomies when only small movements of two jaws are required; it is therefore sometimes necessary to operate on one jaw and compromise on which jaw is likely to give the best result. Conversely, single-jaw operations when movements in excess of 10 mm are required are more prone to significant relapse. Bimaxillary surgery, when indicated, usually gives more aesthetically and functionally pleasing results and it is always better to avoid compromise when at all possible (Figs 12.9, 12.10).
Craniofacial anomalies
The details of craniofacial anomalies are outside the scope of this book, but it is important for the dental profession to be aware of the rare conditions such as Crouzon’s syndrome and Apert’s syndrome, which can result in severe facial deformity.
Much of the pioneering work on these groups of patients was carried out by Paul Tessier. It is now possible to perform complex craniofacial reconstructions to ameliorate the worst of the anomalies.
THE PLANNING OF OSTEOTOMIES, IN THEORY AND PRACTICE
Treatment planning for orthognathic surgery is a process that must take account of the wishes of the patient in relation to the whole of the facial complex—the facial skeleton, the occlusion and the soft tissues which they support. The tissues must be considered both individually and collectively in relation to the patient, whose wishes and aspirations are of fundamental importance. The general principles of collecting data through history, clinical examination and special investigations should be followed. The patient’s medical and social history and psychological profile are also important in considering surgery that will significantly change their facial appearance.
A detailed history should reveal the patient’s principal complaints and the extent to which they concern him or her. These can generally be classified as functional or, more usually, aesthetic—although a combination of the two (in variable proportions) is common. It is important to try to grasp the true concerns of a patient because surgical intervention aimed at addressing the wrong issue carries obvious risks. Patients’ perceptions of their appearance are heavily influenced by upbringing, culture, race and their own psyche. If there is any doubt about a patient’s real motive for requesting surgery, a psychiatric assessment should be sought.
Surgical interventions should ideally, therefore:
In addition to the history of the problem, a detailed medical and social history should be taken. Patients considering orthognathic surgery undertake a major personal commitment and require as much support as possible. Any relevant medical condition or social pressure point should be assessed in relation to the overall treatment plan.
Clinical examination should be undertaken thoroughly but systematically—beginning with the general and working towards the specific. Examinationof the face requires considerable experience in being able to categorize anomalies. For example, maxillary hypoplasia and mandibular prognathism are often difficult to distinguish, even to the trained eye. Similarly, asymmetric development is not always easy to define unless it results in a marked midline shift; and even in such cases the dentition can be the result of excessive or inadequate growth. For example, condylar hyperplasia on the left side of the jaw results in a midline shift of the mandible to the right side; a similar displacement also occurs in right-sided condylar hypoplasia or ankylosis.
Generally, certain features of the face are relatively constant (Fig. 12.11). Horizontally, a line drawn between the pupils bisects the head and will cross the upper insertion of the ear. Vertically a line drawn perpendicularly to the midpoint of the interpupillary line will pass through the middle of the nose, the columella, the philtrum, the upper and lower central incisors and the midpoint of the chin. Various other relationships which define anterior and posterior facial height exist.
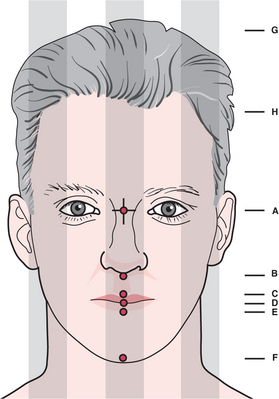
Fig. 12.11 The ideal proportions of the head and face. The vertical lines shown divide into fifths (alternatively vertical lines bisect each pupil to create thirds). The following lengths also correspond: AF = AG; AD = BF; CD = DE; AH = AD = DF. In addition, BD = 0.5 × DF and BF = 0.55 × AF. In reality, very few people fit the exact figures shown, yet the degree of overall conformity is extremely high despite the multiplicity of facial forms.
In all cases, it is essential that the face is viewed as a three-dimensional structure even though virtually all the analyses currently available are two dimensional. It is important to realize that ‘moving’ one part of the face affects the whole facial balance. For example, reducing the length of the mandible in a case of prognathism invariably results in the nose appearing larger. The converse is true for a forward-sliding maxillary osteotomy.
Special investigations relevant to orthognathic surgery include a full orthodontic assessment, radiology of the craniofacial skeleton and photography. Historically, matched cephalometric radiographs and photographs were used to ‘predict’ the desired outcomes of surgery. The radiographs and photographs were made as full-size transparencies and were cut to shape. They were then related to plaster models on which the desired movements were assessed. The method was crude and not always effective but it gave a rough idea of the expected profile after surgery. Nowadays, such analyses are undertaken by computer, using digitized cephalometric radiographs and photographs, with sophisticated software (Fig. 12.12). This enables the surgeon to ‘try out’ a variety of treatment options, including possible operations and orthodontic movements. The ‘occlusal fit’ still must be assessed on models but the accuracy of the predictions is fairly dependable. It is, however, still only an assessment of the profile and many have questioned the value of this from the patients’ viewpoint because this is a view they would rarely see. Full-face predictions will undoubtedly be possible but the software for this is not yet commercially available.

Fig. 12.12 The use of the ‘Dentofacial planner’—computerized software which enables predictive projections for various surgical and orthodontic options.
In the future, three-dimensional analyses and laser images that can be manipulated may well become the norm. Pseudo-three-dimensional images can already be created using computed tomography, and this can easily be extended to milling machine technology, allowing the construction of prostheses, models or attachments which can assist in both the planning and the surgery itself.
The detail of orthognathic surgery is outside the scope of this book and readers are advised to study the textbooks listed at the end of the chapter for further information.
THE NATURE OF THE BASIC OSTEOTOMY PROCEDURES, INCLUDING THEIR MANAGEMENT, RISKS AND COMPLICATIONS
Surgery to the mandible
As orthognathic surgery began on the lower jaw it is perhaps not surprising that a variety of procedures have been described and many of them modified as time has passed. There are several basic principles that should be observed in all orthognathic procedures.
Surgery of the mandible can be applied to any point on the ramus, body or the dentoalveolar segment, although ramus surgery is the most common. The two classical operations—the sagittal split osteotomy (SSO) and the vertical subsigmoid (VSS)—have been adapted and modified in various ways from those originally described.
Sagittal split surgery—where the ramus and posterior part of the mandible are sectioned between the buccal and lingual surfaces—can be used to treat both the severe class 2 and class 3 malocclusion, whereas the VSS is used only to correct relatively mild prognathism. The sagittal split is performed via an intraoral approach (Figs 12.13, 12.14). The lingual tissues are retracted posteriorly and retained using one of the special retractors developed for this purpose. Buccally, the periosteum is retracted to the lower border of the mandible in the second molar region. The lingual bone cut is made horizontally, through the cortical plate, above the level of the lingula; in the past it was extended to the posterior margin of the ramus but this degree of extension is not necessary and may contribute towards relapse. The sagittal cut is made as lateral as is practicable on the external oblique ridge and extended as far forwards as necessary to ensure adequate contact of the split surfaces after repositioning. Finally the buccal cut is made vertically to the lower border. Bone cuts can be undertaken with burs but reciprocating and oscillating saws are more efficient and less likely to cause soft-tissue damage. Once the cuts have been completed the mandible is carefully split using ultra-fine osteotomes. The inferior dental nerve should be identified (usually towards the buccal aspect) during this process and gently dissected away from its canal.
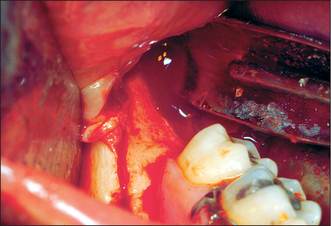
Fig. 12.13 A sagittal split osteotomy being performed intraorally. The cuts can be made with a bur or a reciprocating or oscillating saw.
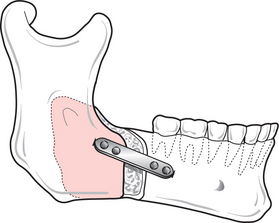
Fig. 12.14 Forward-sliding sagittal split osteotomy. Fixation with miniplates improves stability, and reduces morbidity and the risk of relapse.
On completion of both sides the jaw can be repositioned using an acrylic wafer to locate the mandibular teeth accurately into the maxillary arch. The mandible is then stabilized with intermaxillary fixation and plates and/or screws are used to stabilize the fragments in their new position.
The other common mandibular osteotomy (the VSS) can be approached intraorally or extraorally. A carefully performed VSS carries little risk of damage to the inferior dental nerve because the bone cuts are made distal to the lingula, unlike the SSO, which frequently results in neuropraxia (and occasionally neurotmesis), causing profound anaesthesia in the distribution of the nerve distal to the point of trauma.
Other mandibular osteotomies using different cuts have been described but are beyond the scope of this book. Surgery of the dentoalveolus alone was popular for a short time in the 1970s and 1980s but its use has diminished considerably because ‘dentoalveolar’ surgery was often undertaken to correct an anomaly in the opposing jaw (or of apparently abnormal tooth position) and did not, therefore, really address the underlying problem in the basal bone adequately.
Surgery to the maxilla
When orthognathic surgery was first developed, surgical procedures on the maxilla were very limited, usually being restricted to anterior dentoalveolar procedures. The first attempts at total maxillary osteotomies at the Le Fort I level (see Fig. 13.2) were carried out through small multiple vertical incisions because of concern for the vascularity of the maxilla and the presumed risk of total exfoliation of the osteotomized segment. In reality this has not proved problematic and the Le Fort I osteotomy is now a common operation. Higher-level osteotomies at Le Fort II or III level can also be carried out using bicoronal flaps for access. The latter are only necessary for complex cases such as Crouzon’s and Apert’s syndromes (where intracranial surgery may also be necessary), and most simple orthognathic surgery on the maxilla can be carried out via a Le Fort I osteotomy. As with the mandible, surgery restricted to the alveolus has lost its popularity and anterior segmental osteotomies (such as the Wassmund and Wunderer procedures) are becoming uncommon.
The Le Fort I osteotomy is a versatile procedure, which can be performed at different levels above the apices of the teeth, entering the nasal cavity at the base or higher up on the lateral wall. The only limiting structure of note is the infraorbital nerve, which must be avoided. Posteriorly, care must be taken in separating the pterygoid plates from the posterior wall of the maxilla because any improper use of the chisel may damage the maxillary artery, the consequence of which may be profuse bleeding. Rarely, it is necessary to transfuse a patient because of excessive blood loss, although the likelihood of this can be minimized by careful surgical technique, local anaesthetic with vasoconstrictor and general anaesthesia with induced hypotension.
The actual technique involves a horizontal incision from molar to molar regions. The height of the incision can be varied but there is some evidence that there is less relapse when the incision is made well above the level of the apices. Anteriorly, the floor of the nose, the septum and lateral walls all need to be exposed carefully so as not to tear the nasal mucoperiosteum. The buccal bone cuts are normally made with a bur or reciprocating saw, whilst the septum, the lateral nasal walls and the pterygoid plates are detached with specifically designed chisels and osteotomes (Fig. 12.15). After mobilizing the fractured bones, as in mandibular osteotomies, an acrylic wafer between the upper and lower teeth should be used with intermaxillary fixation to establish the new position of the jaw. Care must be taken to avoid unwanted rotational movements before stabilizing the maxilla in its new position with titanium miniplates. Maxillary osteotomies with at least four miniplates in situ are relatively stable and intermaxillary fixation can be replaced with elastic fixation postoperatively. Any cyanosis of the buccal tissues should rapidly resolve at this stage, before the wounds are closed with interrupted or continuous sutures.
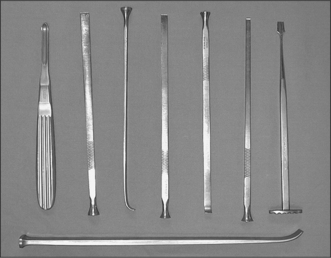
Fig. 12.15 A selection of special chisels and osteotomes designed for use in orthognathic surgery. Many more designs exist, each with a special function.
CLEFT LIP AND PALATE
The incidence of cleft lip and palate varies considerably around the world but is estimated by the WHO to be the second most common birth defect. It is, however, difficult to classify since it could refer to anything from a bifid uvula to a complete bilateral cleft affecting the upper lip, nasal floor and whole of the palate. Cleft lip and palate are extremely important because:
Details of the surgical management of cleft patients are outside the scope of this book but it is important to be aware of the stages of treatment so that parents can be reassured and in order to encourage dental development as normally as possible. Previous generations have sought to repair clefts at the earliest possible opportunity but much of our current thinking has been based on the work of two French surgeons (Malek and Delaire). The latter particularly promoted the concept of functional repairs—establishing normal anatomy insofar as was possible which was never the purpose of the original surgical techniques such as the Millard lip repair. This is probably best achieved once a baby has reached the age of 4–6 months but it requires considerable support for parents who (for obvious reasons) wish to pressurize surgeons into earlier intervention.
Surgery to the palate is usually completed by the first birthday and, for the next few years, further surgery should be avoided giving more attention to speech, social and educational development. Alveolar clefts in the canine region respond well to bone grafting and, when this is required, it should be undertaken well before the canine is due to erupt—usually around the age of 9–10 years.
Finally, when the child reaches the age of 14–15 years he/she should be assessed with a view to orthodontic treatment + orthognathic surgery. Orthodontic treatment in severe cases can take in excess of two years and so should be timed for completion once growth of the facial skeleton can be expected to have finished (17–18 years of age). Recent improvements in the care of cleft babies and children have focused on the establishment of regional centres with teams of specialists and sub-specialists. This, and the much closer attention to research and outcomes, has undoubtedly raised the standards of care available to cleft patients in the UK.
Becker A., Shpack N., Shteyer A. Attachment bonding to impacted teeth at the time of surgical exposure. European Journal of Orthodontics. 1996;18:457-463.
Epker B.N., Stella J.P., Fish L.C. Dentofacial deformities, 2nd edn. St Louis, MO: Mosby, 1995.
Henderson D. A colour atlas of orthognathic surgery. London: Wolfe Medical, 1985.
McBride L.J. Traction—a surgical/orthodontic procedure. American Journal of Orthodontics. 1979;76:287-299.
Schatz J.P., Joho J.P. Long-term clinical and radiologic evaluation of autotransplanted teeth. International Journal of Oral and Maxillofacial Surgery. 1992;21:271-275.
Vermette M.E., Kokich V.G., Kennedy D.B. Uncovering labially impacted teeth: apically repositioned flap and closed eruption techniques. Angle Orthodontist. 1995;65:23-32.
SELF-ASSESSMENT


Answers on page 267.