CHAPTER 19 Gait
What is gait?
Gait is a highly energy efficient method of locomotion necessary for most daily activities. It involves rhythmical, reciprocal movements of the lower limbs and in terms of biomechanics reflects a destabilizing phase followed by a stabilizing phase (Magee 2006). Commonly, the gait cycle is described in terms of a stance phase (approximately 60% of time) and a swing phase (approximately 40%). The tasks involved in gait include: progression within space but also the achievement of a stable alternating one leg stand and postural stability to maintain an upright stance during all phases. Although for the majority of time gait is automatic, requiring no conscious thought, it actually comprises complex patterns of movement involving the whole body. The rhythmic, repetitive components of gait are thought to be initiated and controlled by central pattern generators within the spinal cord (S2.13). However, when changes in the internal and external environment occur, higher level centres are required to integrate and coordinate the motor response. Therefore, if the central nervous system is damaged the functional ability of a patient to walk is likely to be impaired.
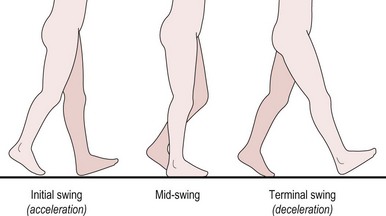
The normal gait cycle is defined as the sequence of motions between two consecutive contacts of the same foot, e.g. heel strike of the left foot to heel strike of the left foot. Stance phase involves heel strike to toe off of the same lower limb (LL), while swing phase includes an initial acceleration phase through to a terminal deceleration phase. An understanding of the normal gait cycle (Figs 19.1, 19.2) and its biomechanics in terms of joint angles and muscle activity is vital to completing a sound assessment, with insufficient knowledge leading to incorrect analysis. A detailed description of normal gait is beyond the scope of this text, however a brief overview of the mechanics of the lower limb is noted below. It should be stressed that all the elements described are integrated in real-time during gait and the therapist should not forget to consider the head/neck, trunk and upper limbs, which are integral in efficient gait.
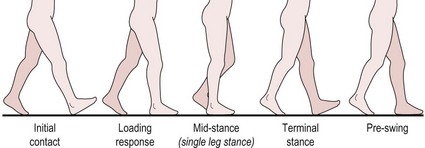
Stance phase (Fig. 19.1)
Swing phase (Fig. 19.2)
Why do I need to assess gait?
Gait dysfunction is common in neurologically impaired patients and can occur from a myriad of different signs and symptoms associated with the pathology. The factors influencing gait may be a direct result of the pathology such as changes in muscle tone, sensation or cognitive and perceptual deficits or due to secondary disuse and inactivity. For example, muscle weakness, alteration of soft tissue extensibility, reduced exercise tolerance or reduced confidence. (For more detail on how specific impairments affect gait, the reader is referred to Chapter 14 in Shumway-Cook and Woollacott 2007).
Dysfunction of gait is one of the earliest and commonest problems reported by patients, with the inability to move around the environment being stated as a critical factor in individuals becoming more dependent and suffering a reduced quality of life. The ability to walk is often, but not always, the goal most eagerly pursued by patients.
Therefore, a detailed assessment of a patient’s gait is essential in order to set a benchmark from which appropriate goals can be set and an efficient gait pattern achieved. A more efficient gait is likely to be more energy efficient and safer in terms of falling. It may also prevent or at least limit secondary musculoskeletal complications.
How do I do gait analysis?
Observation
Gait analysis may be carried out in many ways and the method chosen should be based on what the individual therapist finds most helpful. One method is highlighted below.
Patient
Initially the therapist needs to establish how the patient chooses to move without any intervention.
Therapist
 Clinical hints and tips
Clinical hints and tipsRecording
A text description of the deficits of gait may be structured under the relevant phase of gait or related to body segments. The example below relates to Figure 19.3.
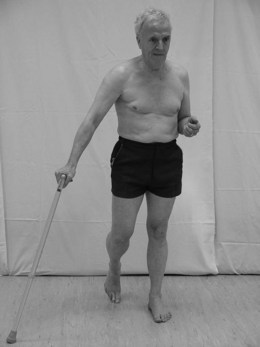
Example
Pt X walks independently with a walking stick carried in the right hand. Using a reciprocal pattern with a 3-point gait.
Analysis
In terms of clinical reasoning, the gait analysis itself may allow the therapist to produce a hypothesis as to the causes of any deviation from normal, however this will need to be tested and confirmed in Part 3 of the objective assessment (S3.20–34).
In the above example, the gait analysis may lead the therapist to suspect (1) an area of instability (trunk, hip/pelvis) on the left side which leads the patient to lack confidence or the ability to transfer weight over the affected left lower limb and achieve terminal hip extension. The associated reaction could also reflect the instability acting as a balance mechanism for an alignment that lacks equilibrium. Or (2) the foot/ankle may also be causal as the inability to gain flat foot could also produce the malalignments described above.
Outcome measures
Research
In recent years technology has developed high quality accurate measurement tools in relation to kinematic or kinetic data by which any movement can be objectively analysed. The use of this technology improves the quality and rigour of gait analysis for the assessment.
References and Further Reading
Holland A, Lynch-Ellerington M. The control of locomotion. In: Raine S, Meadows L, Lynch-Ellerington M, editors. Bobath concept: theory and clinical practice in neurological rehabilitation. Oxford: Wiley-Blackwell, 2009.
Magee DJ. Orthopaedic physical assessment, ed 4. Canada: Elsevier Sciences; 2006.
Moore S, Schurr K, Wales A, et al. Observation and analysis of hemiplegic gait: stance phase. Australian Journal of Physiotherapy. 1993;39:259-267.
Moore S, Schurr K, Wales A, et al. Observation and analysis of hemiplegic gait: swing phase. Australian Journal of Physiotherapy. 1993;39:271-278.
Shumway-Cook A, Woollacott MH. Motor control: translating research into clinical practice, ed 3. Philadelphia: Lippincott Williams and Wilkins; 2007.
SiliconCOACH. SiliconCOACH Coaching solutions for a digital age [online]. New Zealand www.siliconcoach.com, 2004. (Accessed 1 September 2006)