Guidelines for Activity and Exercise
Frequently, older adults with orthopedic dysfunction are inactive, hypertensive, and have multiple risk factors for comorbidities. These factors often are not documented, and the client is treated as an orthopedic case without regard for the past medical history or current cardiopulmonary (or other) condition.
For these reasons, the health care provider must view the effect of other systems on the client’s orthopedic condition and rehabilitation outcome. A thorough evaluation may be necessary, and monitoring cardiopulmonary responses to exercise may be required. Postoperative considerations for various conditions are important when planning a rehabilitation program; these guidelines are listed in each section throughout this text whenever possible.
Exercise should be specific to the functional and medical needs of each individual. Whenever possible, physical activity and exercise should be at a level that causes minimal to no symptoms, and progression should be built into the program. For the aging adult, physiologic homeostasis may be altered by stress, medications, illness, and exercise. To assist in balancing and maintaining homeostasis, 1 day of rest between each day of exercise may be recommended for some individuals.
Interval training, consisting of short-term periods of ambulation followed by rest, is now recommended. Such a program activates the oxygen transport to skeletal and circulatory systems for completion of an activity of daily living to develop endurance. Progress slowly by increasing duration to 30 minutes before increasing intensity. Encourage the client to keep an exercise diary that includes any symptoms that may occur during or after exercise. Review the diary and compare this report to the client’s verbal report, because the person may forget or deny important information.
MEDICATIONS AND EXERCISE
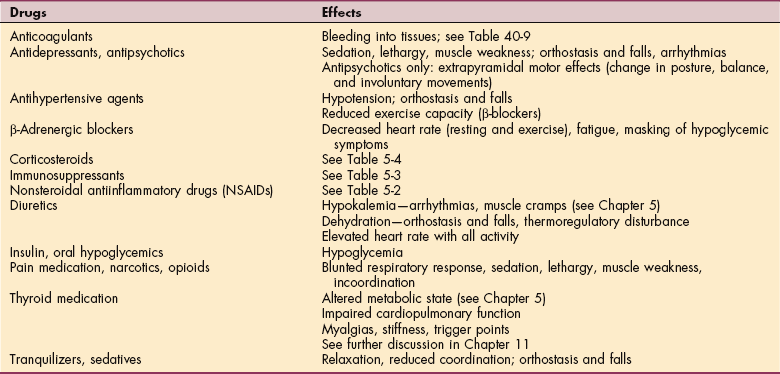
Some clients may be taking medications that can have considerable side effects and interactions when combined with other medications, including effects on exercise parameters such as heart rate, blood pressure, or respiratory rate. Medications can also affect balance, posture, motor control, sleep, and mood, which may affect the individual’s performance in rehabilitation. Common drugs with side effects that may affect an exercise program are listed in Table B-1.
People who are taking drugs that can cause volume depletion or orthostatic hypotension should have their blood pressure and pulse checked in both reclining and standing positions. Avoiding sudden postural changes or activities, limiting activities that promote vasodilation, and providing an adequate warm-up and cool-down period are essential. See also Special Implications for the Therapist: Orthostatic Hypotension in Chapter 12. Therapeutic intervention, especially exercise, should be scheduled according to medication peak blood levels to minimize effects on participation and to enhance rehabilitation performance.
GUIDELINES FOR MONITORING VITAL SIGNS
It is important to know normal responses to movement and activity (including exercise) to be able to identify abnormal responses in the client with a medical diagnosis. Safe and effective exercise can be measured in part by monitoring vital sign responses (temperature, heart rate, respiratory rate, blood pressure, oxygen saturation, pain levels). Such data can be used as specific outcome measures to substantiate decision making. For example, how quickly the heart rate returns to normal is an outcome measurement of fitness and conditioning.
Anyone with a significant past medical history of cardiovascular or pulmonary disease requires monitoring of vital signs and perceived exertion during exercise. The more coronary risk factors present (see Table 12-3), the greater the need for monitoring. For any client with known coronary artery disease and/or previous history of myocardial infarction, exercise testing should be performed before an exercise program is undertaken.
If this testing has not been accomplished and baseline measurements are unavailable for use in planning exercise, the therapist must monitor the client’s heart rate and blood pressure and note any accompanying symptoms during exercise. Too rapid a rise in heart rate, respiratory rate, or blood pressure for the workload is a general indication for modifying the activity or exercise program (see later discussion under Abnormal Heart Rate Response and Abnormal Respiratory Rate Response).
Type of exercise may make a difference in the changes observed in vital signs in older adults. Measurement of heart rate and blood pressure responses to typical isometric, isokinetic, and eccentric resistance-training protocols in older adults showed that changes in blood pressure, arterial pressure, and rate-pressure product were significantly greater during isometric exercise than during eccentric exercise. Clinically, an isokinetic eccentric exercise program enables older adults to work at the same torque output with less cardiovascular stress than isometric exercise.17
Temperature
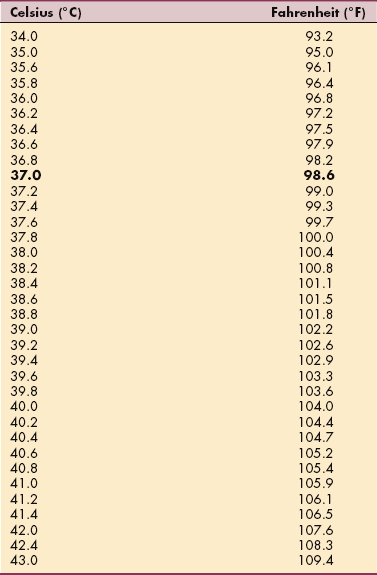
Normal body temperature is not a specific number but a range of values that depends on factors such as the time of day, age, medical status, and presence or absence of infection. Oral body temperature ranges from 96.8° to 99.5° F (36° to 37.5° C) with an average of 98.6° F (37° C) (Table B-2).
The clinical implications of fever and approach to fever vary considerably from person to person, institution to institution, and physician to physician. For example, there is a tendency among the aging population to develop an increase in temperature on hospital admission or in response to any change in homeostasis. Alternatively, fever in older adults residing in extended care facilities may suggest an infectious process, whereas postoperative fever can indicate a surgical complication, such as intraabdominal abscess, leaking anastomosis with peritonitis, or an infected surgical site or prosthesis (e.g., valve, joint, graft). Fever response in adults older than 75 years is often blunted and sometimes even absent.
Others who may remain afebrile in the presence of significant infectious pathology include those who are immunocompromised (e.g., transplant recipients, corticosteroid users, individuals with cancer undergoing treatment), alcoholics, individuals with chronic renal insufficiency, and anyone taking excessive antipyretic medications. Establishing a basal body temperature and monitoring for changes in temperature (of more than 2.4° F [1.3° C]) can assist in early detection of infection (see Box 8-1 for other manifestations of infection).7,28
Single temperature spikes (sudden elevation that returns to normal without intervention) is usually of no diagnostic significance unless it occurs in an immunocompromised individual.10 Common causes of sustained fever are listed in Box 8-2 and Table 8-1. Unexplained fever in adolescents may be a manifestation of drug abuse or endocarditis.
The therapist should use discretionary caution with anyone who has a fever. Exercise with a fever stresses the cardiopulmonary and immune systems, which may be further complicated by dehydration.
Heart Rate (Pulse Rate)
Measuring the heart rate by taking the pulse is really a measurement of the pulse rate. A true measure of the heart rate requires measurement of the electrical impulses of the heart. Resting heart rate is age dependent, with minimal variation for each individual within the normal ranges.
The normal range for the resting pulse rate is 60 to 100 beats/min (or bpm). A rate above 100 beats/min indicates tachycardia; below 60 beats/min indicates bradycardia. Some variations occur with age and training (Table B-3). For example, a well-trained athlete whose heart muscle develops along with the skeletal muscle may have a resting heart rate of less than 60 beats/min.
Table B-3
Normal Resting Pulse Rates Across Age Groups
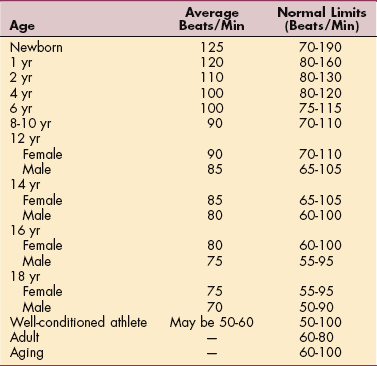
From Behrman RE, Kliegman RM, Jenson HB: Nelson textbook of pediatrics, ed 17, Philadelphia, 2004, Saunders.
The force of the pulse represents the strength of the heart’s stroke volume. A weak, thready pulse reflects a decreased stroke volume, such as occurs with hemorrhagic shock. A full, bounding pulse indicates an increased stroke volume, possibly associated with anxiety, exercise, or some pathologic condition. The pulse force (pulse amplitude) is recorded using the following three-point scale (some physicians/nurses use a four-point scale):
| 3+ | Full, bounding |
| 2+ | Normal |
| 1+ | Weak, thready |
| 0 | Absent |
The pulse should be measured before and during the activity using the same position both times. Count for 6 seconds and add a 0 to that number for a beats-per-minute count or count for 10 seconds and multiply by 6. Heart rate response should increase gradually with an increase in the workload of the heart. Once a steady state has been achieved, little change should occur in heart rate during sustained endurance activities (e.g., water aerobics, riding a stationary bicycle). Factors affecting heart rate responses are listed in Box B-1.
Heart rate responses are different in the deconditioned person because the resting heart rate is higher to begin with. The heart rate increases more rapidly for the same workload compared to the change in a healthy individual. A rapid heart rate may occur during activity in response to dehydration, because the decreased plasma volume results in decreased blood volume and subsequent decreased blood to the heart.
A decreased stroke volume (volume ejected per heartbeat) is compensated for by a higher heart rate to match the demands for oxygen caused by the activity. Cardiac muscle dysfunction is the term used when a decreased stroke volume occurs as a result of diseased cardiac muscle that can no longer contract and pump blood out of the heart normally. Decreased stroke volume results in a more rapid rise in heart rate unless the person is taking β-blocking medication.
Aging is accompanied by a decreasing maximum heart rate. The age-predicted method for calculating the predicted maximal (target) heart rate (PMHR) is 220-age. For example, for a 70-year-old the PMHR = 220-70, or 150 beats/min. This principle is based on the fact that the heart’s maximal rate is 220 beats/min and that this maximal rate declines by one beat each year (probably as a result of the heart’s stiffening and becoming less compliant).19
Some concern about the use of this formula has been raised; some consider it inaccurate because it was based on early research that only examined sedentary men under the age of 60. The formula does not take into account female gender, older age, diagnosis, fitness level, or the presence of comorbidities. It has been suggested that the standard formula underestimates maximum heart rate in older adults. This would have the effect of underestimating the true level of physical stress imposed during exercise testing and the appropriate intensity of prescribed exercise programs.27
This method should not be applied to individuals with peripheral neuropathies, those with chronotropic incompetence (irregular contraction of the heart), or clients taking β-blockers for hypertension and angina. The β-blockers are medications that block the sympathetic nervous system’s input to the β1-receptors in the heart, therefore affecting heart rate and contractility. The net effect is a decrease in the resting and exercise heart rate (drug-induced bradycardia).
The most accurate way to determine maximum heart rate is a stress test in consultation with a cardiologist. Since this is not practical or cost effective, the therapist can teach the client how to use rating of perceived exertion (RPE) as a more user-friendly method. For most clients, it is best to wait until the person has exercised for at least 5 minutes before applying the formula. When using the 6 to 20 scale (very, very light effort to very, very hard effort), multiply the RPE number that matches the client’s effort and multiply by 10. This figure gives a close estimate of the actual heart rate; cardiovascular (aerobic) exercise should be in the 11 to 14 RPE range.5
There is a revised formula that may be more accurate: 208-(age × 0.70).27 For a 70-year-old, using this formula would suggest a maximum heart rate of 159 beats/min. This method does require accurate measurement of the pulse and a calculator and may still be off by up to 8 beats/min. For the active, healthy older adult, another formula has been proposed: PMHR = 205-½ age.26 For example, evaluating the same 70-year-old under these conditions would be 205-½(70), or 205-35 (PMHR = 170).
Keep in mind that anyone taking cardiac medications may not be able to achieve a target heart rate above 90 beats/min. Therefore symptoms of shortness of breath or the use of RPE is a much better guideline for determining exercise intensity. Many individuals who are compromised need more time to work up to the exercise load and to cool down. Using RPE still requires close monitoring of heart rate and blood pressure.
Other methods for prescribing exercise intensity by target heart rate include the Heart Rate Reserve (Karvonen) Method, which takes into account the person’s resting heart rate; the rate-pressure product method (valid indicator of myocardial oxygen uptake); maximal oxygen consumption (VO2max or maximal functional capacity); and the systolic blood pressure method. Information on each of these methods and their recommended applications and known limitations is available.19
Most methods for determining exercise intensity are based on target heart rates that are 40% to 85% of VO2max. However, there are some people for whom exercise intensity should not be prescribed by a target heart rate method, such as those who are deconditioned. In such cases exercise should be prescribed at the lower end of the intensity continuum.
A safe rate of exercise will allow the heart rate to return to the resting level within 5 minutes after stopping exercise (blood pressure returns to resting levels after heart rate). Avoid increases of more than 20 beats/min over resting heart rate. (See Exercise and Antihypertensive Medications, Chapter 12.) Do not remove telemetry immediately after exercise (wait 5 to 10 minutes); in the case of cardiac transplantation, cool down may take up to 1 hour (warm-up should last 30 to 45 minutes).
Abnormal Heart Rate Response
Heart rate should increase commensurately with exercise; as the intensity of exercise increases, the heart rate increases (e.g., like blood pressure, heart rate also increases according to metabolic equivalent [MET]; only a minimal increase in heart rate would be expected with a low-MET activity). The MET system provides one way of measuring the amount of oxygen needed to perform an activity: 1 MET = 3.5 ml of oxygen uptake, which a person requires when resting.
If the pulse is irregular, count the pulse for a full minute and document the number of beats per minute as well as the number of irregular beats (see next section). Abnormal heart rate responses include a rapid rate of rise in heart rate (judging from the activity, age, and training history) or a decreased heart rate with activity (e.g., arrhythmias or pauses in pulse). For example, a doubling of the heart rate with walking on a flat surface (no incline) would be considered outside normal parameters.
A decreased heart rate with activity may occur as a normal response when the person is sympathetically overloaded before treatment. For example, a person who takes inhalants for asthma just before therapy or who drinks more than three cups of coffee within 2 hours of the therapy appointment may have an artificially elevated baseline heart rate. Over the course of therapy, without further stimulation, this person’s heart rate may decrease, especially if the therapy session has no exercise component. Factors such as these require individual evaluation of abnormal responses for each person.
Pulse amplitude (weak or bounding quality of the pulse) that fades with inspiration and strengthens with expiration is paradoxic (paradoxical pulse) and should be reported to the physician. When there is compression or constriction around the heart (e.g., pericardial effusion, tension pneumothorax, pericarditis with fluid, pericardial tamponade) and the person breathes in, the increased mechanical pressure of inspiration added to the physiologic compression from the underlying disease prevents the heart from contracting fully and results in reduced pulse. When the individual expires, the pressure from chest expansion is reduced and the pulse increases. A pulse increase of over 20 beats/min lasting for more than 3 minutes after rest or changing position should also be reported.
If ischemia occurs as evidenced by angina or (on visual readout) depression of ST segment on electrocardiogram, the person should rest and then return to an activity level below ischemic level. For example, if the ST segment drops below baseline with activity or the client experiences angina when the heart rate is at 140 beats/min, the activity level should be reduced so that the heart rate remains below 140 beats/min.
Heart Rhythm
For the person with an abnormal heart rhythm, the pulse should be palpated throughout the activity if no electrocardiogram or Holter monitor reading is available during exercise. If any abnormal pulse beats are noted (e.g., absent, irregular), the number of pauses per minute should be counted at rest and during activity. There should be no more than six abnormal or absent beats per minute. The normal heart rhythm should not change, and individuals with arrhythmias at rest should not show an increase in number of irregular heartbeats with increased activity.
Respiratory Rate
Normal resting respiratory rates are presented in Table B-4. The ratio of pulse rate to respiratory rate is fairly constant (4:1). The respirations can be counted at the same time that the pulse is counted. If an abnormality is suspected, these measurements should be taken for a full minute. A normal pulmonary response to exercise is an increase in breathing rate and depth based on body type and disease present. Factors that can affect respiratory rate include the following:
Table B-4
Normal Resting Respiratory Rates
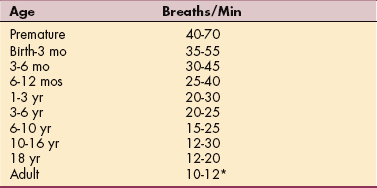
*Typical for average, healthy adult; low for older adult.
From Behrman RE, Kliegman RM, Jenson HB: Nelson textbook of pediatrics, ed 17, Philadelphia, 2004, Saunders.
• Altered lung compliance (chronic obstructive pulmonary disease [COPD], hyaline membrane disease) or any other restrictive condition
• Alterations in lung volumes/lung capacity (smokers, persons with emphysema or occupational lung disease)
• Body position (diaphragm cannot drop down enough to expand the lungs in the fully supine position in the pregnant, obese, or spinal cord–injured client)
Abnormal Respiratory Rate Response
An abnormal respiratory rate response is usually characterized by too rapid a rise in respiratory rate for the activity and medical condition of the client. Increases in respiratory rate greater than 10 respirations/min must be monitored carefully. Measuring the respiratory rate may be difficult. The client must be observed for how much work is required to breathe, and whenever possible, a pulse oximeter should be used to measure arterial oxygen saturation noninvasively (Fig. B-1).
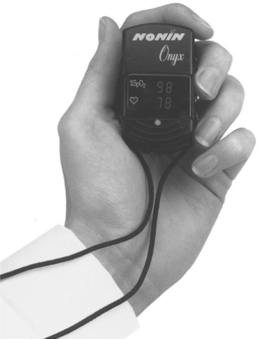
Figure B-1 Noninvasive monitoring of oxygen saturation (SaO2), sometimes referred to as the fifth vital sign, can be done with a pulse oximeter. A finger probe is used most frequently during stationary activities. This compact unit (Onyx) is small enough to carry and ideal for spot checks anytime. The person slips this digital pulse oximeter onto a finger for an immediate pulse rate and oxygen saturation percentage. An ear probe (not shown) can be used to measure oxygen saturation continuously during exercise. (Courtesy Nonin, Inc., Plymouth, MN.)
Pulse Oximetry
The saturation of hemoglobin with oxygen can be measured via pulse oximetry (SpO2) or arterial blood gas (ABG) analysis (SaO2). A normal SpO2 or SaO2 value is 95% or higher. An SaO2 or SaO2 value below 90% means the PaO2 is below 60 mm Hg, indicating the person is not adequately oxygenated (PaO2 is a measure of the pressure of oxygen dissolved in plasma as measured by ABG analysis).
The PaO2 at rest may decline with age because of a loss of surface respiratory space for ventilatory exchange, especially in adults 70 years old or older. The PaO2 increases with activity in older adults as blood volume and respiratory volume increase.8
Using a pulse oximeter with the pulmonary population can provide an outcome measure with exercise for documentation. Oxygen saturation values must be interpreted within the context of the person’s medical status as well as respiratory and metabolic status (as determined by ABG measurements). Respiratory and metabolic status are taken into consideration, because shifts in the oxyhemoglobin curve caused by factors such as temperature fluctuations or acidosis will change the affinity of oxygen to the hemoglobin.
Normal oxygen saturation is 98%, with no change in this measurement during activity or exercise. Clients with chronic respiratory disease may experience a drop in oxygen saturation that is considered normal for them, but this represents a normal response to pathology and is not truly normal.
There has been some question as to whether nail polish can affect the accuracy of pulse oximetry readings. Studies to date have not shown a statistically or clinically significant difference in readings with nail polish of any color (including colorless) in healthy or critically ill and mechanically ventilated individuals.6,9,16,24
Activity should be terminated if oxygen saturation drops to 90% or less in the acutely ill individual or 86% in the person with chronic lung disease. Individuals with decreased oxygen saturation may require more time to accomplish tasks and often experience fatigue and/or shortness of breath. Panic values may vary according to institution and physician. Increased oxygen during activity may prevent such drops but should be discussed with the physician before it is instituted.
At all times, other vital signs should be monitored (heart rate, respiratory rate, and blood pressure) to assess how well the person is tolerating the activity and oxygen desaturation. In the event of large changes in oxygen saturation as determined by pulse oximetry with no changes in vital signs, the pulse oximetry may not be accurate, thus requiring a mechanical check.
Caution is advised when using a finger probe on an individual with cold, discolored hands (blue or white), which is an indication that blood has already been shunted from the fingers. Pulse oximetry as a measure of oxygen saturation would not be accurate in such a situation.14 Peripheral arterial vasoconstriction during the early phases of treadmill exercise has been documented in individuals with vascular pathology secondary to atherosclerosis.25
Supplemental Oxygen
Supplemental oxygen is given if an individual has documented or suspected hypoxemia or deficient oxygenation of the blood, defined as a PaO2 below 60 mm Hg, an SaO2 or SpO2 below 90%, or either value below the desirable range for the clinical situation.23
Other times supplemental oxygen may be needed include severe trauma, acute myocardial infarction, during or after labor and delivery, and as part of procedural sedation or general anesthesia. The therapist should be alert for any signs of increasing hypoxia (reduced tissue oxygenation despite adequate perfusion) indicating a possible need for supplemental oxygen. These include increasing tachypnea and dyspnea, skin color changes (pale, cyanotic), increasing tachycardia, hypertension, restlessness, and/or disorientation.23
Oxygen supplementation in anyone with COPD must be prescribed and monitored very carefully to avoid oxygen toxicity and absorption atelectasis. The therapist should watch for blunting of the respiratory drive. Too much oxygen can depress the respiratory drive of a person with COPD. For example, in the person with emphysema, low arterial oxygen levels are the respiratory drive triggers. For this reason, too much oxygen delivered as an intervention can depress the respiratory drive, which is now reliant on lower levels of arterial oxygen.
The drive to breathe in a normal person results from an increase in the arterial carbon dioxide level (PCO2). Since the individual with COPD chronically retains excessive amounts of carbon dioxide, an increased arterial PCO2 is no longer an effective respiratory drive mechanism.22
If oxygen flow rate must be increased during exercise for individuals with chronic lung disease, oxygen flow rate must be returned promptly to its set value at the end of exercise. Failure to return flow rate to the value determined by the physician may result in hypoventilation, retention of carbon dioxide, and respiratory acidosis.
Blood Pressure
To monitor blood pressure effectively, the therapist must be familiar with normal (see Table 12-8; Table B-5) and abnormal blood pressure responses to exercise and must keep in mind that arterial blood pressure is a general indicator of the function of the heart as a pump and a measure of the peripheral arterial resistance. Systolic pressure measures the force exerted against the arteries during the ejection cycle, and diastolic pressure measures the force exerted against the arteries during rest or against peripheral resistance.
Table B-5
Normal Blood Pressures for Children*
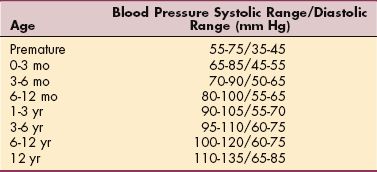
*Normal blood pressure values for children and adolescents of various ethnic groups are under investigation.
From Behrman RE, Kliegman RM, Jenson HB: Nelson textbook of pediatrics, ed 17, Philadelphia, 2004, Saunders.
Systolic blood pressure normally rises with increased exertion in proportion to the workload (approximately 7 to 10 mm Hg/MET) with little or no change in diastolic blood pressure,2 and it rises more quickly in males than in females. For example, during endurance activities, the systolic blood pressure gradually increases, but with sustained activity no further change should occur. Exercise involving a small total muscle mass, such as a single extremity, typically elicits minimal incremental changes in systolic blood pressure and greater increases in diastolic blood pressure.4
Diastolic blood pressure may increase or decrease a maximum of 10 mm Hg due to adaptive dilatation of peripheral vasculature. A highly trained athlete may exhibit more than a 10 mm Hg drop in diastolic blood pressure as a result of increased vasodilation, but this would be considered an abnormal response in an older or untrained adult. A sustained elevation of the diastolic blood pressure during the recovery phase of activity is also considered abnormal. More specific abnormal responses to activity are discussed in detail elsewhere.15
If the resting blood pressure is excessively high (systolic blood pressure 200 mm Hg or diastolic blood pressure 105 to 110 mm Hg), physician clearance should be obtained before continuing with evaluation or treatment. Exercise should be terminated if blood pressure becomes excessively high (systolic blood pressure higher than 250 mm Hg or diastolic blood pressure higher than 110 mm Hg). Systolic blood pressure rise during exercise (19.7 mm Hg/min of exercise duration) and a relatively slow recovery in systolic pressure after exercise are associated with the risk of any stroke and of ischemic stroke.18
Blood pressure should always be measured in the same position, because it can drop quickly with cessation of activity (e.g., do not measure blood pressure while the client is sitting, then ambulate, and recheck blood pressure in the standing position; measure in the standing position, ambulate, and remeasure while standing). In fact, because blood pressure changes can occur within 10 seconds, a truly accurate postexercise blood pressure may be difficult to obtain. Always observe for associated symptoms, such as shortness of breath, dizziness, palpitations, or increase in heart rate.
Pediatrics
A child’s blood pressure is usually much lower than an adult’s. Children are at risk for developing high blood pressure if they exceed the guidelines listed in Table B-5. About 1% of children (including very young babies) have blood pressure that is too high. The cause is often unknown. When a child’s high blood pressure is severe, it is often because of another serious condition, such as kidney disease or heart disease.
Children can inherit high blood pressure from their parents. Overweight children are also at higher risk. Children who both have a family history of hypertension and are overweight should be screened for aberrant blood pressure. The American Heart Association recommends that all children 3 years of age and older have their blood pressure checked once a year.
A child’s sex, age, and height are used to determine age-, sex-, and height-specific systolic and diastolic blood pressure percentiles (see Table 12-8). This approach provides information that lets researchers consider different levels of growth in evaluating blood pressure. It also demonstrates the blood pressure standards that are based on sex, age, and height and allows a more precise classification of blood pressure according to body size. More importantly, the approach avoids misclassifying children at the extremes of normal growth.1
The therapist can provide an important service by including this type of assessment. In children, even a mild elevation of blood pressure can lead to serious medical conditions such as cardiomyopathy and kidney or visual impairments. Medical evaluation and monitoring for signs of early organ damage are needed for any child or adolescent with high blood pressure.
Current guidelines for children may not be very accurate. “Normal” blood pressure values may be different for children and adolescents of various ethnic groups. Heretofore, values have been established without consideration of ethnicity and/or culture and were based mostly on normal values for Anglo children. Investigation to establish more accurate norms and to verify standards for current blood pressure guidelines set by national committees are under way.21
Abnormal Blood Pressure Response
An abnormal blood pressure response may result in hypotension or hypertension as reflected by any of the following responses:
• Too rapid a rise in systolic blood pressure for the workload; in the healthy adult, the systolic blood pressure should go up by 20 mm Hg with minimal to moderate exercise and 40 to 50 mm Hg with intensive exercise. These values are less likely with cardiac clients.
• Very little change in systolic blood pressure with excessive workload in an unfit or deconditioned person.
• Progressive rise of diastolic blood pressure.
• Diastolic blood pressure should remain the same or change slightly (less than 5 mm Hg increase/decrease should be noted); a drop of more than 10 mm Hg in diastolic blood pressure is considered abnormal.
• Drop in systolic pressure (or both systolic and diastolic pressure) of 10 to 20 mm Hg or more associated with an increase in pulse rate of more than 15 beats/min (depleted intravascular volume).
• Narrowing of pulse pressure (systolic blood pressure-diastolic blood pressure).
An increase in diastolic blood pressure of 20 mm Hg or more may be a sign that the person has exceeded cardiac reserve capacity and that blood flow to the liver, kidneys, and digestive tract has been critically reduced. A decrease in diastolic blood pressure may occur as a result of rapid vasodilation, an effect of training in the athletic individual.
A drop in diastolic blood pressure may also indicate normalization in a hypertensive individual as a result of vasodilation and decreased peripheral resistance. For example, this may occur if the hypertensive person experiences a calming effect as a result of participating in a regular routine of exercise after driving in heavy traffic to get to the clinic on time. Other factors that affect blood pressure are listed in Box B-2.
GUIDELINES FOR AQUATIC PHYSICAL THERAPY
Paula Richley Geigle and Charlotte O. Norton
The decision to include aquatic physical therapy in a treatment regime is made for each client based on the Guide to Physical Therapist Practice.12 For each individual a risk-benefit analysis is completed at each intervention point, wellness through tertiary care.20 Sound clinical decision making is required to determine if the positive impact of hydrostatic principles offsets any potential risks created by the aquatic environment.13
The clinician must consider the static properties of water, including density and specific gravity, hydrostatic pressure, and the effects of buoyancy on each client. The effects of time-dependent properties such as viscosity, laminar flow, turbulent flow, and their effects on the amount of resistance encountered with water activity are additional critical elements considered in the thought process determining whether to include or not include aquatic therapy and, if included, under what conditions the therapist develops the program.3 Additionally, thermodynamics and its respective interaction with varied client presentations plays a key role in directing the appropriate use of aquatic physical therapy.
In each practice environment, therapists must assess the precautions and contraindications for each respective clientele category. Precautions for aquatic physical therapy participation include but are not limited to the conditions listed in Table B-6.13
Table B-6
Precautions and Contraindications for Aquatic Physical Therapy
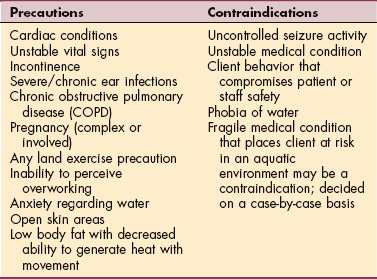
Courtesy Paula Richley Geigle, PT, PhD, and Charlotte Norton, DPT, ATC, CSCS, 2006. Used with permission.
An overview of examination components, organized by Guide categories and systems review, is provided in Table B-7. The therapist can use this tool to guide the examination performed prior to aquatic intervention. Categories of test and measurement tools are also included from which clinicians can choose to complete these additional assessment components.
Table B-7
Aquatic Practice for the Physical Therapist
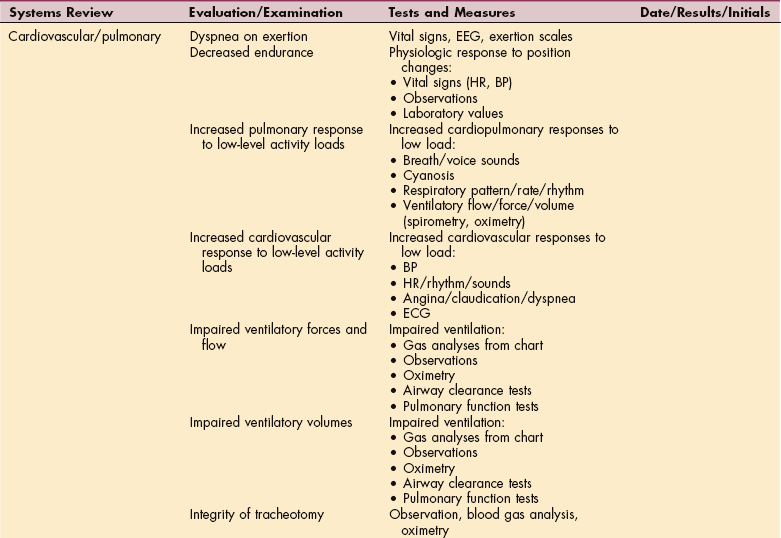
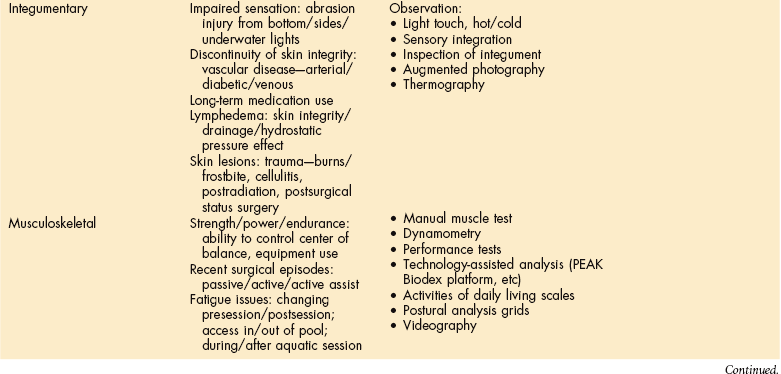
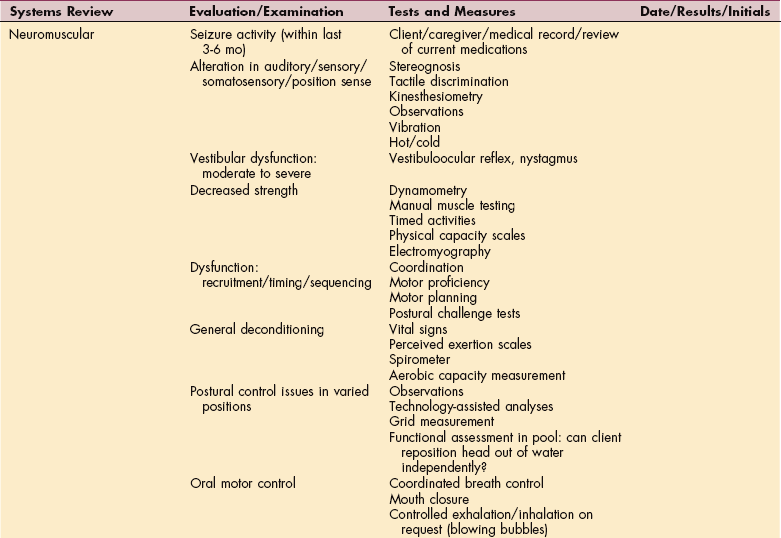
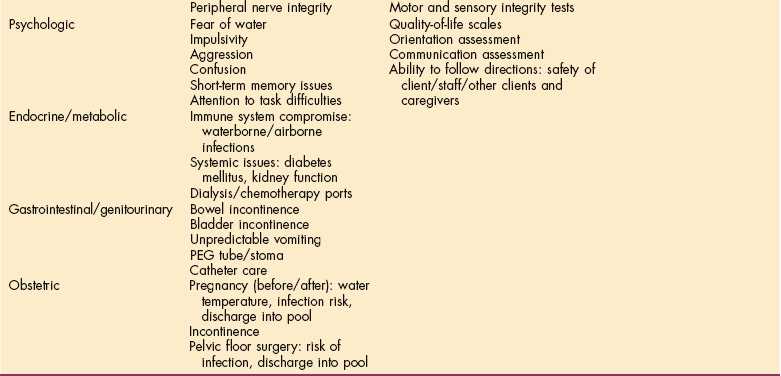
ECG, Electrocardiogram; HR, heart rate; BP, blood pressure; PEG, percutaneous endoluminal gastrostomy.
Courtesy Paula Richley Geigle, PT, PhD, and Charlotte O. Norton, DPT, MS, ATC, CSCS. Used with permission.
One example of the clinical decision-making process used in determining if and how the aquatic medium should be used in rehabilitation is the case of Viola, an 80-year-old woman living independently with her husband in a full-spectrum retirement community. She was referred to aquatic physical therapy for severe back pain, after having undergone several spinal fusions. The back pain was interfering with her activity level.
Viola participated in an initial land-based physical therapy examination and a course of therapeutic exercise and manual therapy. After a 3-to 4-week land-based physical therapy intervention, an aquatic physical therapy referral was recommended with the goals of reducing lumbar spasm and pain that interfered with her functional activities. Viola reported several comorbidities, including a 15-year history of Parkinson’s disease.
For Viola’s program, the clinician must consider the client’s body type and structure, and whether she demonstrates any changes in muscle tone as a result of Par- kinson’s disease. Changes in tone must be considered in relation to density and specific gravity, as both affect the amount of buoyancy support the person may need while participating in aquatic physical therapy.
The use of hydrostatic pressure and the effects of buoyancy in deeper water to minimize the effects of gravity may help decrease the amount of muscle spasm and pain (Guide Musculoskeletal category) Viola experiences from both her spinal involvement and tone changes from a longstanding neuromuscular pathology. The increased movement that buoyancy offers allows Viola to increase her cardiovascular reserve (Guide Cardiovascular/Pulmonary category) without increasing her back pain.
Scaling of speed and amplitude11 is enabled by the buoyancy principle, both from ease of movement and decreased fear of balance loss (Guide Neuromuscular and Musculoskeletal categories). In other words, the aquatic environment facilitates larger, full range-of-motion movement as a result of a decreased falling anxiety and the increased proprioceptive input from hydrostatic pressure.
Examination of her postural control in a variety of positions with particular attention to safety issues (Guide Neuromuscular category) associated with Parkinson’s disease–related muscle tone fluctuations during positioning transitions will allow the clinician to determine the most appropriate application of viscosity and resistance for her exercise program. For example, Viola demonstrates the “typical” Parkinson’s rigidity when in a full supine position. Any horizontal aquatic techniques should place Viola in about 25 to 30 degrees of trunk flexion via flotation supports.
Finally, the clinician must consider the water temperature (Guide Neuromuscular category). Warmer temperatures, approximating 90° F (32.2° C), will facilitate relaxation of the muscles and help to reduce the rigidity associated with Parkinson’s disease and may increase the ease of spinal muscle activation.
Using the Guide to Physical Therapist Practice and hydrodynamic principles as a conceptual framework for clinical decision making, optimal aquatic care can be initiated. The Aquatic Physical Therapy Section of the American Physical Therapy Association provides current clinical information on its website and produces both a how-to manual on aquatic programming and a bibliography updated every 2 years (www.aquaticpt.org).
References
1. American Heart Association (AHA): High blood pressure in children. Available on-line at http://www.americanheart.org/presenter.jhtml?identifier=4609 Accessed August 8, 2007.
2. American Heart Association Committee on Exercise. Exercise testing and training of individuals with heart disease or at high risk for its development: a handbook for physicians. Dallas: American Heart Association, 1975.
3. Becker, BE, Cole, AJ, eds. ed 2. Comprehensive aquatic therapy. Boston: Butterworth-Heinemann; 1997.
4. Blomquist, CG, Lewis, SF, Taylor, WF, et al. Similarity of the hemodynamic responses to static and dynamic exercise of small muscle groups. Circ Res. 1981;48:187–190. [(suppl)].
5. Borg, G. Borg’s perceived exertion and pain scales. Champaign, IL: Human Kinetics Publishers, 1998.
6. Brand, TM. Enamel nail polish does not interfere with pulse oximetry among normoxic volunteers. J Clin Monit Comput. 2002;17(2):93–96.
7. Castle, SC, Norman, DC, Yeh, M, et al. Fever response in elderly nursing home residents: are the older truly colder? J Am Geriatr Soc. 1991;39:853–857.
8. Cerveri, I. Reference values of arterial oxygen tension in the middle-aged and elderly. Am J Respir Crit Care Med. 1995;152(3):934–941.
9. Chan, MM. What is the effect of fingernail polish on pulse oximetry? Chest. 2003;123(6):2163–2164.
10. Cunha, BA. Clinical implications of fever. Postgrad Med. 1989;85(5):188–200.
11. Farley, BG, Koshland, GF. Training BIG to move faster: the application of the speed-amplitude relation as a rehabilitation strategy for people with Parkinson’s disease. Exp Brain Research. 2005;167:462–467.
12. Guide to physical therapist practice. Alexandria, VA: American Physical Therapy Association; 2003. Available on-line at www.aquaticpt.org Developing an aquatic physical therapy program and Aquatic physical therapy bibliography..
13. Geigle, PR, Norton, CO. Medical screening for aquatic physical therapy. J Aquat Phys Ther. 2005;13(2):6–10.
14. Hillegass E: Personal communication, Atlanta, 2000, Emory University.
15. Hillegass, E, Sadowsky, S. Essentials of cardiopulmonary physical therapy, ed 2. Philadelphia: Saunders, 2001.
16. Hinkelbein, J. Effect of nail polish on oxygen saturation determined by pulse oximetry in critically ill patients. Resuscitation. 2007;72(1):82–91.
17. Huggett, DL. Comparison of heart-rate and blood-pressure increases during isokinetic eccentric versus isometric exercise in older adults. J Aging Phys Act. 2004;12(2):157–169.
18. Kurl, S, Laukkanen, JA, Rauramaa, R, et al. Systolic blood pressure response to exercise stress test and risk of stroke. Stroke. 2001;32(9):2036–2041.
19. Leutholtz, BC, Ripoll, I. Exercise and disease management. Boca Raton, FL: CRC Press, 1999.
20. Norton, CO, Jamison, LJ. Team approach to the aquatic continuum of care. Boston: Butterworth-Heinemann, 2000.
21. Park, MK. Oscillometric blood pressure standards for children. Pediatr Cardiol. 2005;26(5):601–607.
22. Pauwels, RA, Rabe, KF. Burden and clinical features of chronic obstructive pulmonary disease (COPD). Lancet. 2004;364(9434):613–620.
23. Pruitt, WC. Basics of oxygen therapy. Nursing2003. 2003;33(10):43–45.
24. Rodden, AM. Does fingernail polish affect pulse oximeter readings? Intensive Crit Care Nurs. 2007;23(1):51–55.
25. Rozanski, A, Qureshi, E, Bauman, M, et al. Peripheral arterial responses to treadmill exercise among healthy subjects and atherosclerotic patients. Circulation. 2001;103(16):2084–2089.
26. Sidney, KH, Shephard, RJ. Maximum and submaximum exercise tests in men and women in 7th, 8th, and 9th decades of life. J Appl Physiol. 1977;43:280–287.
27. Tanaka, H, Monahan, KD, Seals, DR. Age-predicted maximal heart rate revisited. J Am Coll Cardiol. 2001;37(1):153–156.
28. Yoshikawa, TT, Norman, DC. Approach to fever and infection in the nursing home. J Am Geriatr Soc. 1996;44(1):74–82.