The Cardiovascular System
The cardiovascular system functions in coordination with the pulmonary system to circulate oxygenated blood through the arterial system to all cells. The deoxygenated blood is then collected from the venous system and delivered to the lungs for reoxygenation (Fig. 12-1). Pathologic conditions of the cardiovascular system are varied, multiple, and complex. This chapter presents cardiovascular structure and function according to how diseases affect each individual part, including diseases of the heart muscle, cardiac nervous system, heart valves, pericardium, and blood vessels.
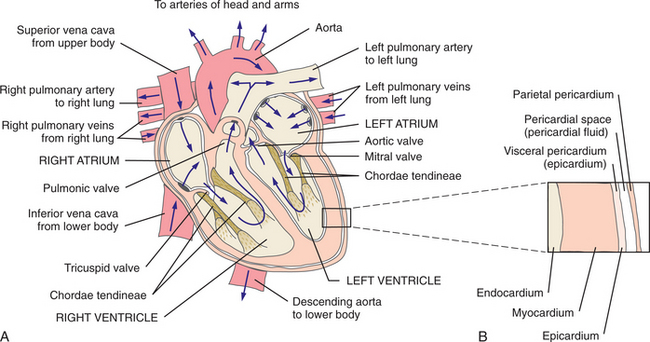
Figure 12-1 A, Structure and circulation of the heart. Blood flows from the superior and inferior venae cavae into the right atrium through the tricuspid valve to the right ventricle. The right ventricle ejects the blood through the pulmonic valve into the pulmonary artery during ventricular systole. Blood enters the pulmonary capillary system, where it exchanges the carbon dioxide for oxygen. The oxygenated blood then leaves the lungs via the pulmonary veins and returns to the left atrium. From the left atrium, blood flows through the mitral valve into the left ventricle. The left ventricle pumps blood into the systemic circulation through the aorta to supply all the tissues of the body with oxygen. From the systemic circulation, blood returns to the heart through the superior and inferior venae cavae to begin the cycle again. B, Sagittal view of the layers of the heart wall.
Other factors, such as surgery, pregnancy, and complications from other pathologic conditions (e.g., acquired immunodeficiency syndrome [AIDS], cancer treatment, metabolic diseases, collagen vascular diseases [now more commonly referred to as diffuse connective tissue diseases; see Box 12-17]) can also adversely affect the normal function of the cardiovascular system. Discussion of these additional factors is limited in this chapter (see specific chapters for each subject).
A section reporting gender differences as these relate to the cardiovascular system and diseases has been added. Whenever possible, ethnicity as it relates to cardiovascular diseases is included in each section. Ethnic differences are an area just coming under closer review, and the knowledge available is limited at this time.
SIGNS AND SYMPTOMS OF CARDIOVASCULAR DISEASE
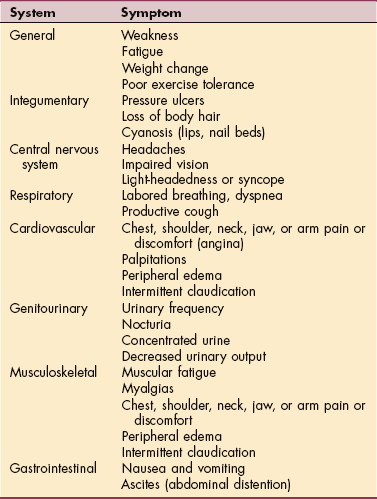
Cardinal symptoms of cardiac disease usually include chest, neck, or arm pain or discomfort; palpitations; dyspnea; syncope (fainting); fatigue; cough; and cyanosis. Edema and leg pain (claudication) are the most common symptoms of the vascular component of cardiovascular pathologic conditions. Symptoms of cardiovascular involvement should be reviewed by system as well (Table 12-1).
Chest pain or discomfort (e.g., tightness, pressure sensation) is a common presenting symptom of cardiovascular disease and must be evaluated carefully. Chest pain of systemic origin may be cardiac or noncardiac and may radiate to the neck, jaw, upper trapezius, upper back, shoulder, or arms (most commonly the left arm). Radiating pain down the arm is in the pattern of ulnar nerve distribution. Noncardiac chest pain can be caused by an extensive list of disorders and is not covered in this text.
Cardiac-related chest pain may arise secondary to ischemia, myocardial infarction (MI), pericarditis, endocarditis, mitral valve prolapse, or aortic dissection with or without aneurysm. Location and description (frequency, intensity, duration) vary according to the underlying pathologic condition (see each individual condition).
Chest pain is often accompanied by associated signs and symptoms, such as nausea, vomiting, diaphoresis, dyspnea, fatigue, pallor, or syncope. Cardiac chest pain or discomfort can also occur when coronary circulation is normal, as in the case of anemia causing lack of oxygenation of the myocardium (heart muscle) during physical exertion, although this situation is uncommon.
Angina (see Angina Pectoris section for more details) is a chest pain or discomfort occurring when a heart muscle does not get enough oxygen. It is a symptom of coronary artery disease (CAD). It usually starts behind the breastbone, but it may project in the arm, shoulder, neck, jaw, throat, and back. It is described as pressure, squeezing, or tightness in the chest. Some people may mistake it for indigestion. Shortness of breath, weakness, light-headedness, and sweating may occur.
Palpitations, the presence of an irregular, fast, or “extra” heartbeat, may also be referred to as arrhythmias or dysrhythmias, which may be caused by a relatively benign condition (e.g., mitral valve prolapse, caffeine, anxiety, exercise, athlete’s heart [increase in left ventricular mass as a result of intensive training])261 or a severe condition (e.g., CAD, cardiomyopathy, complete heart block, ventricular aneurysm, atrioventricular valve disease, mitral or aortic stenosis).
Palpitations may occur as a response to the bursts of adrenaline that occur with drops in estrogen levels, as a response to excess or erratic production of adrenaline-type compounds associated with panic disorder, or as a result of hyperthyroidism through other mechanisms. Up to one third of heart transplant recipients are aware of their resting heartbeat, despite the absence of cardiac innervation.32
Palpitations have been described as a bump, pound, jump, flop, flutter, butterfly, or racing sensation of the heart. Associated symptoms may include light-headedness or syncope. Palpated pulse may feel rapid or irregular, as if the heart has skipped a beat. Some people report fluttering sensations in the neck rather than in the chest or thoracic area.
Dyspnea, also referred to as breathlessness or shortness of breath, can be cardiovascular in origin, but it may also occur secondary to pulmonary pathologic conditions (see also Chapter 15), trauma, fever, certain medications, or obesity. Early onset of dyspnea may be described as a sensation of having to breathe too much or as an uncomfortable feeling during breathing after exercise or exertion. Shortness of breath with mild exertion (dyspnea on exertion [DOE]) can be caused by an impaired left ventricle that is unable to contract completely. The result is an abnormal accumulation of blood in the pulmonary vasculature. Pulmonary congestion and shortness of breath then ensue. With severe compromise of the cardiovascular or pulmonary system, dyspnea may occur at rest.
Dyspnea may be a predictor of death from cardiac or other causes. In a large study of over 17,000 adults undergoing myocardial perfusion single-photon emission computed tomography (SPECT) during stress and at rest, those with no history of CAD who presented with dyspnea had four times the risk of sudden death from cardiac causes compared to asymptomatic individuals. They also had twice the risk compared to participants already diagnosed with typical angina.2
The severity of dyspnea is determined by the extent of disease; the more severe the heart disease, the more readily episodes of dyspnea occur. More extreme dyspnea includes paroxysmal nocturnal dyspnea and orthopnea. Paroxysmal nocturnal dyspnea, which is sudden, unexplained episodes of shortness of breath, awakens a person sleeping in a supine position, because the amount of blood returning to the heart and lungs from the lower extremities increases in this position. This type of dyspnea frequently accompanies congestive heart failure (CHF).
During the day, the effects of gravity in the upright position and the shunting of excessive fluid to the lower extremities permit more effective ventilation and perfusion of the lungs, keeping the lungs relatively fluid free, depending on the degree of CHF. Orthopnea is the term used to describe breathlessness that occurs during recumbency and is relieved by sitting upright, using pillows to prop the head and trunk. Orthopnea can occur anytime during the day or night.
Cardiac syncope (fainting or, in a milder form, light-headedness) can be caused by reduced oxygen to the brain when the heart’s pumping ability becomes compromised. Conditions resulting in cardiac syncope include arrhythmias (particularly short bursts of ventricular tachycardia), orthostatic hypotension (sudden drop in blood pressure), aortic dissection, hypertrophic cardiomyopathy, CAD, vertebral artery insufficiency, and hypoglycemia. When the heart does not pump as much blood, blood pressure drops low enough to cause fainting.
Predictors of cardiac syncope include a history of stroke or transient ischemic attacks, use of cardiac medication, and high blood pressure. Marginally associated risk factors also include lower body mass index (BMI), increased alcohol intake, and diabetes or elevated plasma glucose level. Any client with aortic stenosis (a condition in which an aortic valve becomes narrowed or constricted) is more likely to experience light-headedness associated with postural hypotension as a result of a sudden change in position or increased intraabdominal pressure (Valsalva maneuver).
During the period of initiation and regulation of cardiac medications (e.g., vasodilators), side effects such as orthostatic hypotension may occur. Implantable loop recorders are available to assess falls associated with syncope of unknown cause. Implantable recorders allow for continuous electrocardiogram (ECG) monitoring for recurrent but infrequent syncope.
Noncardiac conditions, such as anxiety and emotional stress, migraine headaches, seizures, or psychiatric conditions, can cause hyperventilation and subsequent light-headedness.
Vasovagal syncope is a term that is used for persons who have a very strong parasympathetic response that leads to vasodilation throughout the body. It can occur after a prolonged period of sitting or standing. Normally, in such a situation, blood tends to pool in the legs, requiring a heart rate and vasoconstriction sufficient to push the blood back to the heart, but when vasovagal syncope occurs, it is because the heart rate slows and vessels dilate, causing hypotension and cerebral hypoperfusion with subsequent fainting and/or falling.
The individual has a vagal response to the vascular system and passes out but regains consciousness right away (after being recumbent). Some individuals may experience this type of parasympathetic reaction when having blood drawn for testing or when donating blood. This type of syncope is not as serious as cardiac syncope (except as a potential source of injury from falling).
Fatigue provoked by minimal exertion indicates a lack of energy that may be cardiac in origin (e.g., CAD, aortic valve dysfunction, cardiomyopathy, myocarditis), or it may occur secondary to neurologic, muscular, metabolic, or pulmonary pathologic conditions. Often fatigue of a cardiac nature is accompanied by associated symptoms, such as dyspnea, chest pain, palpitations, or headache.
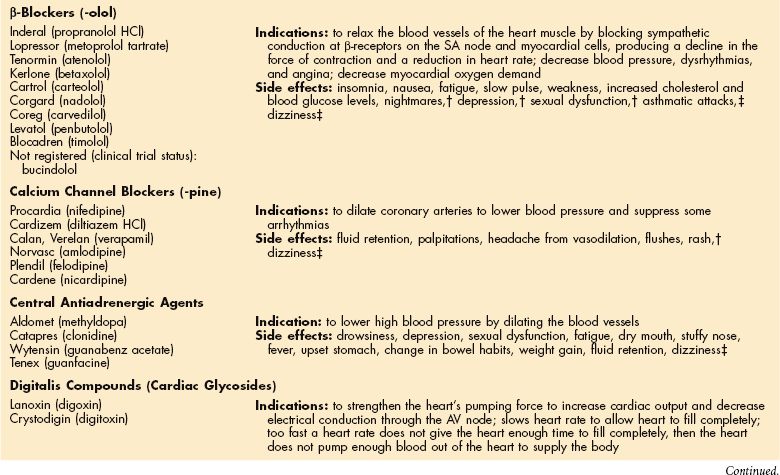
Cough (see also Chapter 15) is usually associated with pulmonary conditions but may occur as a pulmonary complication of a cardiovascular pathologic condition. Left ventricular dysfunction, including mitral valve dysfunction as with resulting pulmonary edema, may result in a cough when aggravated by exercise, metabolic stress, supine position, or paroxysmal nocturnal dyspnea. The cough is often hacking and dry when associated with left ventricular dysfunction and failure. Cough may be productive of large amounts of frothy, blood-tinged sputum in full-blown pulmonary edema. In the case of CHF, cough develops because a large amount of fluid is trapped in the pulmonary tree, irritating the lung mucosa. A persistent, dry cough can develop as a side effect of some cardiovascular medications (e.g., angiotensin-converting enzyme [ACE] inhibitors) (see Table 12-5).
Table 12-5
Common Cardiovascular Medications
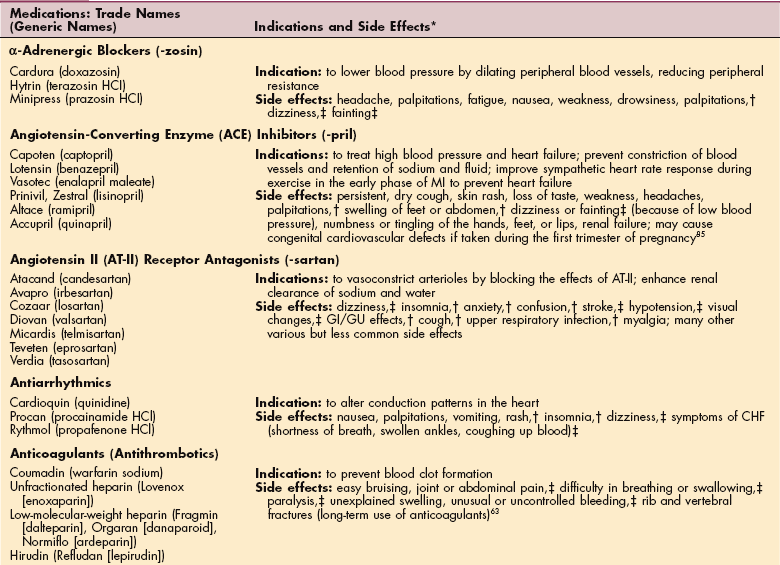
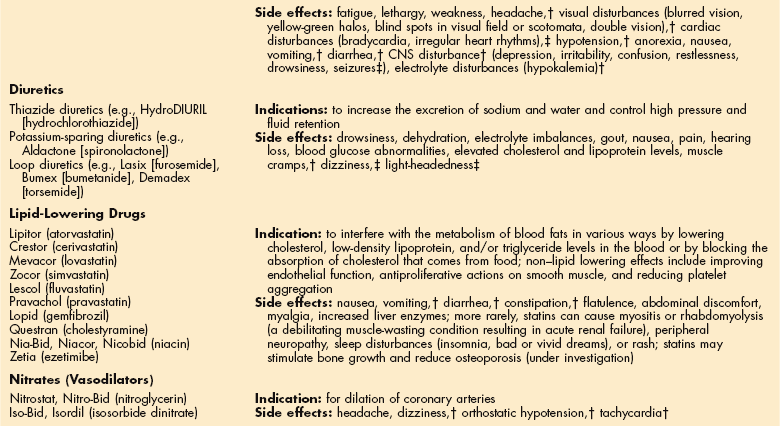
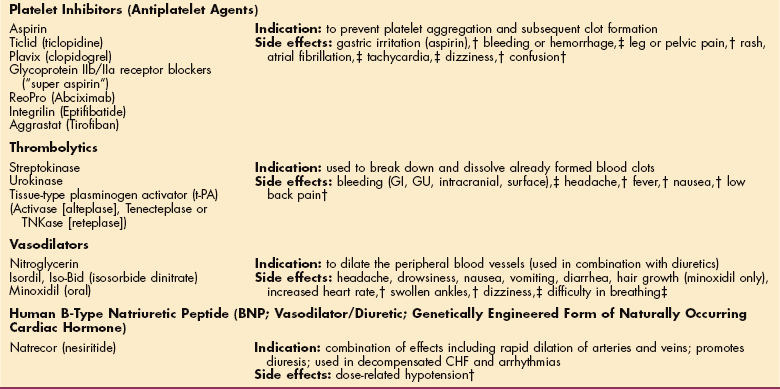
MI, Myocardial infarction; HCl, hydrochloride; GI, gastrointestinal; GU, genitourinary; CHF, congestive heart failure; SA, sinoatrial; AV, atrioventricular; CNS, central nervous system.
*The therapist is more likely to see potential side effects not otherwise present since these develop when the person is physically challenged. Any unusual signs or symptoms and potential side effects should be documented and reported to the prescribing physician.
†Document and call physician when possible.
‡Call physician immediately; document findings.
Cyanosis is a bluish discoloration of the lips and nail beds of the fingers and toes in the Caucasian population that accompanies inadequate blood oxygen levels (reduced amounts of oxygenated hemoglobin). Look for grey color tones (instead of pink/red) along the gum line (buccal mucosa) in the mouths of African Americans, Hispanics, or other dark-skinned individuals. Although cyanosis can accompany cardiac, pulmonary, hematologic, or central nervous system (CNS) disorders, visible cyanosis most often accompanies cardiac and pulmonary problems.
Peripheral edema is the hallmark of right ventricular failure; it is usually bilateral and dependent and may be accompanied by jugular venous distention (JVD; see Fig. 12-13), cyanosis (of lips, appendages), and abdominal distention from ascites (see Fig. 17-5). Right upper quadrant pain, described as constant, aching, or sharp, may occur secondary to an enlarged liver with this condition. Right-sided heart failure and subsequent edema can also occur as a result of cardiac surgery, venous valve incompetence or obstruction, or cardiac valve stenosis. Noncardiac causes of edema include pulmonary hypertension and lung dysfunction resulting in right-sided heart failure, as well as kidney dysfunction, cirrhosis, burns, infection, lymphatic obstruction, and allergic reaction.

Figure 12-13 Jugular venous distention occurs bilaterally if there is a cardiac cause such as congestive heart failure; a unilateral distention indicates a localized problem. (From Daily EK, Schroeder JP: Techniques in bedside hemodynamic monitoring, ed 2, St Louis, 1981, Mosby.)
Claudication, sometimes described as cramping or leg pain, is brought on by a consistent amount of exercise or activity. It develops as a result of peripheral vascular disease (PVD) (arterial or venous), often occurring simultaneously with CAD.68 Claudication can be more functionally debilitating than other associated symptoms, such as angina or dyspnea, and may occur in addition to these other symptoms. The presence of pitting edema along with leg pain is usually associated with venous disease. Pitting edema leaves a dent on the skin after the area has been pressed with a thumb for several seconds. This happens due to fluid collected in the tissue. The dent will slowly fill back.
Other noncardiac causes of leg pain (e.g., sciatica, anterior compartment syndrome, gout, peripheral neuropathy, pseudoclaudication) must be differentiated from pain associated with PVD. Low back pain associated with pseudoclaudication often indicates spinal stenosis. The typical person affected is approximately 60 years old and bothered less by back pain than by a discomfort occurring in the buttock, thigh, or leg that (like true claudication) is brought on by walking but (unlike true claudication) can also be elicited by prolonged standing. The discomfort associated with pseudoclaudication is frequently bilateral and improves with rest or with flexion of the lumbar spine.
AGING AND THE CARDIOVASCULAR SYSTEM
Cardiovascular disease, especially coronary atherosclerosis, is the most common cause of hospitalization and death in the older population in the United States. With the aging of America, by the year 2030 nearly 50% of all Americans will be 45 years old or older. By that time the number of people 65 years and older will more than double and the population 85 years and older is expected to triple.235 With this increase in the number of older persons, cardiovascular disease is likely to be even more of a major health problem in the future, as it accounts for over 80% of cardiovascular deaths in people aged 65 years and above.186
Specific Effects of Aging
Aging of the heart is associated with a number of typical morphologic, histologic, and biochemical changes, although not all observed changes with age are associated with deterioration in function. The high prevalence of hypertension and ischemic heart disease makes distinction between normal aging changes and the effects of underlying cardiovascular disease processes difficult.
Disease-independent changes in the aging heart associated with a reduction in function include (1) reduction in the number of myocytes and cells within the conduction tissue, (2) the development of cardiac fibrosis, (3) a reduction in calcium transport across membranes, (4) lower capillary density, (5) decreases in the intracellular response to β-adrenergic stimulation (sometimes referred to as blunted β-adrenoceptor responsiveness), and (6) impaired autonomic reflex control of heart rate.186
Other characteristic changes, such as epicardial fat deposition and “brown atrophy” caused by intracellular lipofuscin deposits, appear to be signs of the aging process but without any obvious effects on function. The hearts of older persons, even fit, healthy, and active adults, pump less blood to the skin and require the heart of the older person to work much harder under the same circumstances (e.g., exercise in warm environments) than that of a younger person.
Although the specific organ changes associated with aging are discussed here, disease and lifestyle may have a greater impact on cardiovascular function than aging. Research now shows that even children need to control their modifiable risk factors for heart disease.
Heart studies of adolescents and young adults who have died from accidental causes demonstrate that heart disease begins earlier than formerly expected. Cholesterol deposits and blood vessel changes have been demonstrated in early adolescence with substantial changes observed by age 30 years in some people.
As the arteries age, increased collagen and calcium content and progressive deterioration of the arterial media combined with atherosclerotic plaque formation result in stiff arterial walls, increased systolic blood pressure, and increased fatigue of arterial walls, all of which accelerate arterial damage, producing a self-perpetuating cycle.
Effects of Aging on Function
None of the changes described earlier has clinical relevance at rest but may have considerable consequences during cardiovascular stress, such as occurs with increased flow demand (e.g., exercise, postoperative), demand for acute autonomic reflex control (e.g., change in posture), or severe disease (e.g., uncontrolled hypertension, tachyarrhythmias, myocardial ischemia). Physiologic aging is accompanied by a progressive decline in resting organ function. Consequently, the reserve capacity to compensate for impaired organ function, heat, drug metabolism, and added physiologic demands is impaired, and functional disability will occur more quickly and take longer to resolve.249
According to experts at the National Institute on Aging, age is the greatest risk factor for cardiovascular disease.186,234 The heart also undergoes some changes associated with advancing age in individuals who do not exercise and who have risk factors for cardiac disease. Moderate thickening of the left ventricular wall (exaggerated in hypertensive clients) and increased left atrial size occur as a result of myocyte enlargement (hypertrophy) or replacement by fibrous tissue. Decreased ventricular filling compensated by increased systolic blood pressure occurs as a result of the changes in the ventricular wall. Left ventricular functioning is compromised in the presence of stress such as vigorous exercise or disease. Arrhythmia or hypertension may occur as a result.
The vasculature changes with aging as the arterial walls stiffen with age and the aorta becomes dilated and elongated. The incidence and severity of atherosclerosis do increase with aging, and this contributes to changes in vasculature function.
Calcium deposition and changes in the amount of and loss of elasticity in elastin and collagen most often affect the larger and medium-sized vessels. The unpredictable interaction between age-related and disease-associated changes in all organ functions (including the heart) and the altered neurohormonal response to various forms of stress in the aging older adult may result in atypical clinical presentations of disease that delay diagnosis and medical intervention.198,249
Resting cardiac function (e.g., cardiac output, heart rate) shows minimal age-related changes. Changes in functional capacity are more apparent during exercise than at rest. The maximal heart rate or the highest heart rate during exercise does decline with age, possibly because of a decreased cardiovascular response to catecholamines. This decline in maximal heart rate is reflected in the target zone heart rates for exercising senior citizens. See Appendix B for calculation of target heart rates for sedentary and physically fit older adults. The effect of the Frank-Starling mechanism is unaltered with age and is used effectively during exercise to maintain cardiac output through a higher stroke volume.
The Frank-Starling law states that the greater the myocardial fiber length (or stretch), the greater will be its force of contraction. The more the left ventricle fills with blood, the greater will be the quantity of blood ejected into the aorta. This is like a rubber band: the more it is stretched, the more strongly it recoils or snaps back. Thus a direct relationship exists between the volume of blood in the heart at the end of diastole (the length of the muscle fibers) and the force of contraction during the next systole.
Effects of Exercise on Aging
It is commonly accepted that a decline in maximal oxygen uptake, heart rate, and reduced maximal cardiac output with aging occurs during exercise, even in older athletes. These cardiovascular alterations parallel changes that occur with deconditioning or disuse, including the decrease in maximal oxygen intake and maximal cardiac output. These functions normalize with increased activity, and exercise can reverse some of the age-associated changes in the heart at least partially,186 supporting the hypothesis that age-related cardiovascular changes are simply the result of inactivity.
In older people, aerobic exercise training lowers heart rate at rest, reduces heart rate and levels of plasma catecholamine at the same absolute submaximal workload, improves heat tolerance,331 and, at least in men, improves left ventricular performance during peak exercise.298 It may be that the effect of training is relatively greater in older subjects.
Finally, although the benefits of physical activity and exercise among older persons are becoming increasingly clear, the role of exercise stress testing and safety monitoring for older people who want to start an exercise program is unclear. Current guidelines regarding exercise stress testing may not be applicable to the majority of adults aged 75 years or older who are interested in restoring or enhancing their physical function through a program of physical activity and exercise.
Recommendations and precautions to minimize the risk of adverse cardiac events among previously sedentary older adults who do not have symptomatic cardiovascular disease and are interested in starting an exercise program are available.124 The therapist is very instrumental in conducting an examination and performing exercise testing to identify the specific level of pathology, impairment, or functional limitations.34 An individual exercise prescription is made (mode, intensity, duration, frequency) based on the results of the examination and testing.108,192
GENDER DIFFERENCES AND THE CARDIOVASCULAR SYSTEM
Interest in gender differences in all of medicine but especially the cardiovascular system has come to the forefront in the new millennium. Only a small, representative portion of the new information now available can be presented here; the reader is referred to other more complete sources.194,195
Female hearts not only are smaller than male hearts but also are constructed differently and respond to age and hypertrophic stimuli differently. Structural differences in the mitral valve may explain why women are more prone to mitral valve prolapse than men. At puberty, a young woman’s QT interval lengthens, and the woman with a long QT interval is at greater risk for a serious form of ventricular arrhythmia (known as torsades de pointes) and sudden cardiac death, especially when taking drugs that prolong the QT interval.36
The QT interval is a measure of the duration of ventricular depolarization and repolarization. A prolonged period of time for depolarization prolongs the suprathreshold period of an action potential and upsets the critical influx and efflux of electrolytes during action potential activity that may predispose a person to ventricular tachycardia.
Left ventricular mass increases with age in healthy women but remains constant in men. Under increased cardiac loading conditions (e.g., hypertension, aortic stenosis) this disparity between genders is even more obvious, especially in adults older than 50 years.145 The risk for drugs other than cardiac and psychotropic ones to cause prolongation of the QT interval has recently been recognized. Women also have a three times greater risk of potentially fatal arrhythmias from some cardiac and psychotropic medications. It is anticipated that the list of drugs known to produce such effects will grow.296 Complications from antiarrhythmic drug use are most common during the first 3 days or after a dosage increase.
Women also tend to have a higher incidence of bleeding episodes from thrombolytic agents (see Table 12-5). Women also have different outcomes with surgery and percutaneous transluminal coronary angioplasty (PTCA), with more repeat procedures of PTCA, possibly due to smaller arteries, more advanced disease compared to men, or different tolerance to medications.190 Women, in contrast to men, with premature coronary disease are at higher risk of developing vascular and ischemic complications after percutaneous coronary intervention.189
Coronary Artery Disease in Women
It was long believed that CAD was a more benign process in females, but this has been soundly disproved. A woman presenting with angina postmenopausally has the exact same mortality as a man presenting with angina in his sixties. CAD is the single leading cause of death and a significant cause of morbidity among women in the United States.
Certain characteristics and clinical conditions may place women at higher risk of CAD development or progression, such as depression, being black, menopausal status, age, type 2 diabetes mellitus, and thyroid function. In addition, female gender may adversely influence the relative benefits of some risk modification interventions in older adults (e.g., cholesterol lowering, sedentary behavior, smoking cessation).164,349
Underrecognition and underdiagnosis of CAD in women contribute to the high mortality rate,222 and underuse of guideline-based preventive and therapeutic strategies for women probably contributes to their less favorable CAD outcomes.355 Researchers are actively studying specific risk factors for women.
A new predictive model for women that combines newer risk markers with traditional risk factors and family history is being investigated. A family history of heart attack prior to age 60 has been added to the list of risk factors of which women should be aware. The Reynolds Risk Score could help target women who could benefit from more aggressive preventive treatment, including diet, exercise, and a statin or other cholesterol-lowering medication.281 You can calculate your own score if you are a woman, or help your female clients do so, at www.reynoldsriskscore.org.
Coronary Microvascular Dysfunction
A “stealth” form of heart disease called coronary microvascular dysfunction or disease (previously called syndrome X) has been identified in women. This type does not show up on angiograms. Classic signs of reduced blood flow to the heart (ischemia) are not present. Instead there are false-positive stress test results (significantly abnormal results on the stress test but clear arteries on an angiogram). It may be that the tiny blood vessels to the heart become constricted, reducing blood flow.
Scientists suspect ischemia may have different effects on women compared to CAD (Table 12-2). It was previously believed that women with chest pain but clear arteries had an aggravating case of coronary microvascular syndrome but it was not considered harmful.
Table 12-2
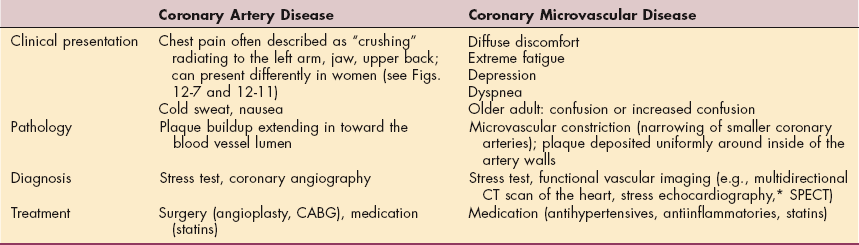
*Stress echocardiography uses ultrasound to produce images of the heart after an exercise stress test.
Data from Harvard Women’s Health Watch: New view of heart disease in women, Harv Womens Health Watch 14(6):1-3, 2007. CT, Computed tomography (serves as a noninvasive angiogram; moves around the heart generating a three-dimensional image of the heart and coronary arteries); SPECT, single-photon emission computed tomography (injects a radioactive tracer into bloodstream to chart the flow of blood in the heart and coronary vessels); CABG, coronary artery bypass graft.
Research in the Women’s Ischemia Syndrome Evaluation (WISE) study, a federally funded investigation into ischemic heart disease in women, is ongoing to explain this phenomenon.31,271,305,306 Autopsy comparisons of women and men have shown that women who die of heart attacks are more likely to have plaque buildup uniformly around the inside of the blood vessel, possibly as a result of chronic inflammation. Inflammation may not be the only cause of coronary microvascular dysfunction. Risk factors such as anemia and polycystic ovarian syndrome have been identified as well.141 Women with this type of heart disease are at increased risk for heart attack, stroke, and reduced quality of life.
Gender Differences
Many studies have suggested that women with acute MI receive less aggressive therapy than men and have a poorer outcome when treatment is received. Until recently, women in all age groups have been less likely to undergo diagnostic catheterization than men, and this difference was especially pronounced among older women (more than 85 years). Women have been less likely than men to receive preventive care (drug treatment for lipid management; risk factor management through exercise, nutrition, and weight reduction), invasive treatments (revascularization procedures), and thrombolytic therapy within 60 minutes of heart attack (or stroke).118,355
Women delay longer than men before seeking help for symptoms of acute MI, referred to as decision delay, further compromising effective treatment and improved outcomes.288 This is especially true given the evidence that first heart attacks in women may be more severe and that women are more likely to die in the first weeks and months after a heart attack. The WISE study has provided detailed evaluation of gender-related risk factors for ischemic heart disease.306
For many years, women and minorities were underrepresented in studies conducted on heart disease and stroke, but this has changed over the last decade along with concomitant expansion of prevention and educational outreach programs for heart attack, stroke, and other cardiovascular diseases in women. The use of noninvasive testing in women was controversial because of a perception of diminished accuracy, limited female representation, and technical limitations.
Large observational studies now report marked improvements in the accuracy of results for women undergoing exercise treadmill, echocardiography, and nuclear testing as a result of expanding risk parameters in the test interpretations and improved diagnostic accuracy of such tests.222 Because of technologic advances, improved surgical techniques, greater awareness of gender differences in heart disease, and increased funding for gender-based research, these trends are improving, and women now seem to do as well as men after surgical (revascularization) procedures to restore blood flow to the heart.
Although the American Heart Association reports a decline in death rates in women for CAD and stroke, women are still twice as likely as men to die within 1 year of having a heart attack, and women are at greater risk for second heart attacks and for disability because of heart failure. The death rate among black women is 33.7% higher for stroke and 69% higher for heart disease than among white women.12,17
Many women die of CAD without any warning signs, and by age 65 years one in four women has heart disease (the same proportion as in men). CAD claims the lives of nearly 250,000 women annually in the United States,222 compared with 40,200 for breast cancer and 63,000 for lung cancer. Despite these statistics, misperceptions still exist that cardiovascular disease is not a real problem for women and that, despite the fact that some risk factors for CAD can be prevented, CAD is not curable. For these reasons, education and prevention228 are vitally important to reduce risk of heart disease.
Coronary Artery Surgery and Women
The number of women undergoing coronary artery bypass graft (CABG, pronounced “cabbage”) has continued to increase (from 146,000 in 1995 to 427,000 in 2004).13,15 Women may experience more chest wall discomfort as a common side effect of CABG than men; it is most often reported in those women who had an internal mammary artery (IMA) graft.
Women undergoing bypass surgery have a death rate about twice as high as that of men.39 This has been attributed to the fact that women generally have smaller bodies, meaning smaller coronary arteries on which it may be technically more difficult to operate. Data from the WISE study also suggest that women may have both CAD and unrecognized microvessel disease, in which case, opening the arteries is not sufficient.
Hormonal Status
Influence of Hormones on Coronary Artery Disease
Estrogen has been considered to have a cardioprotective benefit for women via a variety of mechanisms. It stimulates the formation of high-density lipoprotein (HDL), the good cholesterol, which carries plaque away from the artery wall and back to the liver to be broken down and excreted, while also stimulating low-density lipoprotein (LDL) receptors in the liver and possibly the blood vessel walls. These receptors bind the LDL, the bad cholesterol, and remove it from the circulation, preventing its damaging effects in plaque formation.
Estradiol acts as a calcium channel blocker to relax artery walls, which helps dilate the arteries, improves blood flow throughout the brain and body, and helps to reduce blood pressure. Estrogen maintains the normal balance of prostacyclin and thromboxane, two chemicals that regulate clot formation. Estrogen increases arterial wall production of prostacyclin, which improves blood flow and reduces platelet aggregation. Estrogen receptors locate different regulatory molecules that attract and bind to estrogen in the cells of the smooth muscle layer of blood vessels. Atherosclerosis may develop because blood vessel cells cannot extract needed estrogen from the blood without the necessary receptors.
Another possible mechanism by which estrogen protects against heart disease before menopause is the release of endothelium-derived relaxing factor (EDRF, thought to be nitric oxide), a chemical stimulated by estrogen and responsible for dilating blood vessels to maintain normal pressure and flow. As women lose the biologically active estradiol, gender differences become gender similarities and the incidence of cardiovascular disease increases dramatically, matching the incidence among men within 10 years of menopause without hormone replacement therapy.
Myocardial ischemia may be more easily induced when estrogen concentrations are low, a finding that may be important for timing the assessment and evaluating treatment in women with CAD. The early follicular phase, when estradiol and progesterone concentrations are low, may be associated with poor exercise performance as measured by onset to myocardial ischemia. These findings are preliminary and have not been reproduced or confirmed.
Hormone Replacement for Postmenopausal Women
The use of hormones for cardioprotection has been under investigation for many years. Because heart attacks tend to occur 10 years later in women than in men, it was assumed that the protective effect of estrogen was responsible. Exogenous (externally administered) estrogen has been reported to improve plasma lipid profiles, carbohydrate metabolism, and vascular reactivity, but surprisingly, hormonal therapy does not alter the progression of CAD or protect against MI or coronary death. The Heart and Estrogen/Progestin Replacement Study (HERS) failed to demonstrate cardioprotection and even showed an early adverse outcome in women with documented CAD who received daily hormone replacement therapy (HRT). Several large randomized clinical trials for primary and secondary prevention showed mixed results.347
Fifty percent of all women who have had a hysterectomy (without removal of the ovaries) and all women who have an oophorectomy (ovary removal) become endocrinologically menopausal by 3 years after surgery, regardless of age. Their heart disease risk increases when they become menopausal regardless of their age or the means by which menopause occurs.
Oral Contraceptives
Studies show that women smokers over 35 years who use oral contraceptives are much more likely to have a heart attack or stroke than nonsmokers who use birth control pills. In the last 20 years, cardiovascular complications in all women taking oral contraceptives have become less common because current contraceptives contain the lowest dose of estrogen possible without breakthrough bleeding.17
At this dose, the risk of thromboembolic disease is reduced to about 40 events per 100,000 women per year, approximately the same risk as in the general population.55 However, much debate continues about the use of so-called third-generation (newest) oral contraceptives containing low doses of estrogen and a type of progestin known as desogestrel. Women taking this contraceptive are twice as likely to develop superficial venous blood clots compared to women taking second-generation oral contraceptives containing progestins, such as levonorgestrel and norethindrone. It is estimated that 425 ischemic strokes can be attributed to oral contraceptive use each year in the United States, even with the newer low-estrogen preparations.125
Hypertension in Women
More women than men eventually develop hypertension in the United States because of their higher numbers and greater longevity. White coat hypertension (rise in blood pressure when being evaluated by a physician or other health care worker) is more prevalent among women, and black women are more likely to have hypertension than black men.
Alcohol, obesity, and oral contraceptives are important causes of rise in blood pressure among women. Alcohol is known to have specific toxic effects on heart muscle fibers, and excessive alcohol consumption is increasing in women; yet women are less likely than men to be identified as alcohol abusers at early stages of the illness and are less often referred for alcohol treatment until later stages of abuse, when cardiac and other severe complications have occurred.341
Women with left ventricular hypertrophy are at greater risk of death than men. ACE inhibitors and angiotensin receptor blockers are contraindicated in pregnancy and should be avoided in women with childbearing potential.272 A recent study found that infants who were exposed to the ACE inhibitors during the first trimester were at increased risk of major congenital malformations that affected the cardiovascular and nervous systems.85
In the WISE study, early onset of high systolic blood pressure or pulse pressure (the difference between systolic and diastolic blood pressures) has been linked with a higher risk of having significant CAD.
Cholesterol Concerns for Women
Total cholesterol is broken into HDL, or good cholesterol, which carries cholesterol away from the cells, and LDL, or bad cholesterol, which carries cholesterol to the cells. A helpful way to remember the function of these is to think of HDL as “Healthy” or beneficial cholesterol and LDL as “Lousy” or detrimental cholesterol. Lipoproteins are complexes that help dissolve, transport, and utilize the cholesterol molecule.
The National Heart, Lung, and Blood Institute estimates that more than half of all women over age 55 years need to lower their blood cholesterol. Reference guides for cholesterol testing and recommendations based on lipid levels have not been standardized for women with the exception of the HDL. The recommended level for initiating treatment in women is less than 50 mg/dl and for men is less than 40 mg/dl. Whether the current established guidelines on other lipids (based on data derived from studies of men) are most appropriate for women remains unknown.
After menopause, women have higher concentrations of total cholesterol than men do, but the significance of this finding remains unknown. Research results at this time suggest that women need higher levels of the good cholesterol (HDL) for protection against heart disease and that other blood markers, such as serum triglycerides and C-reactive protein (CRP), may play more meaningful roles in defining women’s heart disease risk. Low levels of HDL cholesterol are predictive of CAD in women and appear to be a stronger risk factor for women older than 65 years than for men of the same age.229
DISEASES AFFECTING THE HEART MUSCLE
Coronary arteries carry oxygenated blood to the myocardium. When these arteries become narrowed or blocked, the areas of the heart muscle supplied by that artery do not receive sufficient amount of oxygen and become ischemic and injured, and infarction may result. Major disorders of the myocardium owing to insufficient blood supply are collectively known as ischemic heart disease, coronary heart disease (CHD), or coronary artery disease (CAD).
Despite improved clinical care, heightened public awareness, and widespread use of health innovations, atherosclerotic diseases (resulting in narrowing of arteries) and their thrombotic complications remain the number one cause of mortality and morbidity in the United States (see Table 2-1).
An estimated 12 million persons in the United States have CAD. Of the 1.1 million CAD events that occurred during 2001, approximately 650,000 were first events and 450,000 were recurrences. Each year approximately 220,000 fatal CAD events occur suddenly among unhospitalized people. Eleven million Americans who are alive today have a history of angina pectoris, MI, or both, and an estimated 2 million middle-aged and older adults (more than 75 years) have silent myocardial ischemia.226
Although CAD death rates in the United States have decreased since reaching a peak during the late 1960s (146.2 cases per 100,000 in 1948 with a peak of 220.3 in 1963 to 87 cases per 100,000 in 1996), a decline in the incidence of coronary disease has not been achieved. In 1940, the rate of cardiovascular disease was 26.4 per 100,000 people compared to 173.5 in 2000.16
The declining mortality rate does not apply to those adults with diabetes and has been attributed to improvements in lifestyle (e.g., reduced smoking in men, improved treatment for lipid lowering, improved coronary care), whereas the increased incidence may be related to the increasing number of people who are surviving past age 65 years.
Nonatherosclerotic causes of coronary artery obstruction and subsequent ischemic heart disease are uncommon (Box 12-1). For example, mediastinal radiotherapy for left-sided breast cancer, Hodgkin’s disease, or non-Hodgkin’s disease may be an independent risk factor in the development of ischemic heart disease.
Radiotherapy causes cardiac perfusion defects 6 months after treatment in most people, but it remains unknown if these changes are transient or permanent. Improvements in radiation technique have reduced com- plications, especially late cardiac deaths. At the present time, the benefit of treatment for operable breast cancer for individuals who may be cured of the disease appears to outweigh the risks of long-term cardiac sequelae.367 Researchers continue to investigate the need to optimize adjuvant radiotherapy for early breast cancer by considering the dose both to the cancer and to the heart.
Arteriosclerosis
Arteriosclerosis represents a group of diseases characterized by thickening and loss of elasticity of the arterial walls, often referred to as hardening of the arteries. Arteriosclerosis can be divided into three types: (1) atherosclerosis, in which plaques of fatty deposits form in the inner layer or intima of the arteries; (2) Mönckeberg’s arteriosclerosis, involving the middle layer of the arteries with destruction of muscle and elastic fibers and formation of calcium deposits; and (3) arteriolosclerosis or arteriolar sclerosis, characterized by thickening of the walls of small arteries (arterioles). All three forms of arteriosclerosis may be present in the same person but in different blood vessels. Frequently the terms arteriosclerosis and atherosclerosis are used interchangeably, although technically atherosclerosis is the most common form of arteriosclerosis.
Atherosclerosis
Atherosclerosis, defined as thickening of the arterial wall through the accumulation of lipids, macrophages, T lymphocytes, smooth muscle cells, extracellular matrix, calcium, and necrotic debris, can affect any of the arteries in a condition known as cardiovascular disease.
When the arteries of the heart are affected it is referred to as coronary artery disease (CAD) or coronary heart disease (CHD); when the arteries to the brain are affected, cerebrovascular disease develops. Atherosclerosis of blood vessels to other parts of the body can result in PVD, aneurysm, and intestinal infarction. Atherosclerosis as it affects the heart vessels is discussed in this section. The effect of atherosclerosis on other blood vessels is discussed individually elsewhere.
Etiologic and Risk Factors.: In 1948, the U.S. government decided to investigate the etiologic factors, incidence, and pathologic findings of CAD by studying residents of a typical small town in the United States: Framingham, Massachusetts. In 1971 a second generation of adult children and their spouses of the original participants were added. Results from this ongoing research have identified important modifiable and nonmodifiable risk factors associated with death caused by CAD.
Modifiable risk factors that can be controlled are referred to now as “risk factors for which intervention has been shown to reduce incidence of CAD”; other risk factors that can be managed are now referred to as “risk factors for which intervention is likely to reduce incidence of CAD” or “risk factors for which intervention might reduce incidence of CAD.” Some risk factors cannot be altered (nonmodifiable), such as age, gender, family history of heart disease, ethnicity, and exposure to infectious agents (Table 12-3).
Table 12-3
Coronary Artery Disease Risk Factors
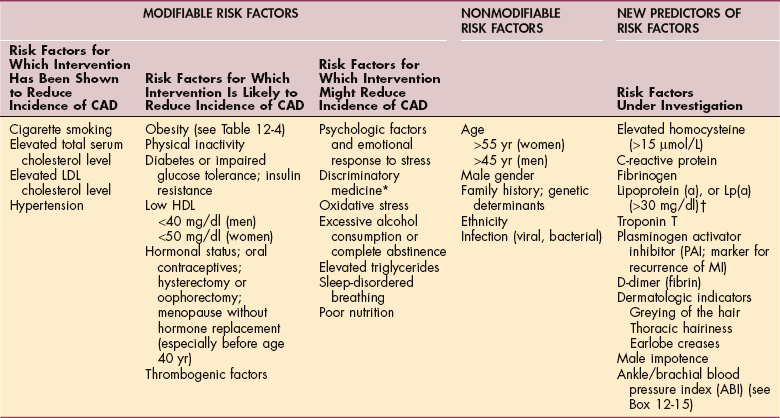
CAD, Coronary artery disease; LDL, low-density lipoprotein; HDL, high-density lipoprotein; MI, myocardial infarction.
*Discriminatory medicine is not technically a risk factor for CAD but rather results in a different natural history for some individuals.
†Applies to whites and Asians but not to blacks.
As the Framingham study continues to gather and analyze new data, results are reported that help modify existing health risk appraisal models relating risk factors to the probability of developing CAD. With these new models, blood lipid levels, diabetes, and, in women, systolic blood pressure and cigarette smoking are emphasized once again as independent predictors of risk.
The Framingham study is engaged in quantifying the independent contributions of plasma homocysteine (an amino acid by-product of protein metabolism); lipoprotein (a) (Lp[a]), a cholesterol-rich plasma lipoprotein that encourages overgrowth of cells in the artery walls; insulin resistance; small, dense LDL; CRP, a producer of inflammation; fibrinogen; and genetic determinants of cardiovascular disease.174
In a national sample of older women and men (65 to 84 years), black and Mexican American women and black men were at the greatest risk for cardiovascular disease. These findings parallel a previously documented increased risk of cardiovascular disease among younger ethnic minority populations. Differences in socioeconomic status (as measured by educational level and family income) do not explain the higher prevalence of cardiovascular disease risk factors in these ethnic minority groups.320
Higher prevalence of certain risk factors in black women, particularly diabetes and obesity, may explain their increased risk of CAD, but ethnic differences in CAD for Hispanics remain unknown. The Newcastle Thousand Families Study confirms that adult lifestyles are more important than socioeconomic variables,187 but further research to identify ethnic differences in cardiovascular disease risk factors is needed.
Modification of Risk Factors That Reduce Incidence of Coronary Artery Disease.: Cigarette smoking remains the leading preventable cause of CAD. Tobacco products increase heart rate and blood pressure; decrease the oxygen-carrying capacity of blood; increase poisonous gases and elements of the blood such as carbon monox- ide, cyanide, formaldehyde, and carbon dioxide; cause narrowing of blood vessels; and increase the work of the heart.
Nicotine enhances the process of atherosclerosis by a direct effect on the blood vessel wall, increasing the circulating levels of fibrinogen and tendency for plaque formation in the coronary arteries. Nicotine also increases the expression of LDL receptors on smooth muscle cells lining the plaque, priming the cells for the entry of LDL cholesterol. By-products of tobacco products in the blood act as potent oxidizing agents. This oxidation damages the intimal lining of the arterial walls, exposes collagen, and results in platelet aggregation. People who quit smoking will reduce their risk of CAD by one half after 1 year and equalize their risk of CAD to that of a nonsmoker in 15 years (see Table 3-4).
Elevated total serum cholesterol levels (more than 200 mg/dl) place a person at greater risk for heart disease; this risk doubles when cholesterol levels exceed 240 mg/dl and the ratio of total cholesterol to HDL cholesterol is more than 4.5 (Table 12-4). It is now well known that therapy to lower LDL levels can stabilize, reduce, or even reverse the progression of atherosclerotic plaques and coronary stenosis and reduce recurrent cardiac episodes. Cholesterol levels are influenced by heredity, diet, exercise, alcohol consumption,91,183 obesity, medications, menopausal status, thyroid function, and smoking. Impaired thyroid function is a cause of elevated cholesterol and arterial stiffness, especially in women older than 50 years who smoke.248,343
Table 12-4
Heart Disease Prevention Target Measurements*
*These target measures are for healthy adults without evidence of heart disease.
†The current standard for all adults is set at ≥35 mg/dl. Proposed targets of ≥40 mg/dl for men and ≥50 mg/dl for women are the new guidelines from the American Heart Association300 and are developed for adults and children over age 2 (no upper age limit). Some experts recommend 55 mg/dl or higher for women, but this remains unproven and is under investigation.
Hypertension, or high blood pressure, causes the heart to work harder and may injure the arterial walls, making them prone to atherosclerosis. Epidemiologic studies document a strong association between high levels of both systolic and diastolic blood pressure and risk of CAD (and stroke) in both men and women.
Hypertension is aggravated by obesity and is associated with diabetes and regular alcohol use. It can be initiated or aggravated by the use of oral contraceptives, especially in women who smoke. Women who have undetected or uncontrolled hypertension are five times more likely to experience angina, heart attack, or sudden death than women with normal blood pressure. Weight reduction, dietary interventions, and pharmacologic intervention have important roles in the prevention and treatment of hypertension.
Modification of Risk Factors That Are Likely to Reduce Incidence of Coronary Artery Disease.: Physical inactivity, sedentary lifestyle, and obesity are parallel, interrelated epidemics in the United States that contribute to increased risk of CAD.
Obesity (see discussion in Chapter 2) alone can lead to CAD, because the excess weight makes the heart work harder to pump blood throughout the body. Obesity is commonly associated with diabetes mellitus, high blood pressure, and high fat (triglycerides and cholesterol) levels. The prevalence of obesity has increased among both men and women in the United States in the past decade. More than one half of adult Americans are overweight or obese, and more than one half of this population is overweight with associated medical conditions.238
The U.S. Department of Health and Human Services reports that one out of every five children is obese, and the obesity rates have increased 147% from 1971 to 1994 among children ages 6 to 11 years.69 Target body measurements (adults) for the prevention of heart disease are listed in Table 12-4. Increasing research and knowledge related to nutrition have led to identification of several dietary factors that influence CAD risk. The epidemiologic evidence confirms that diets low in saturated fat and high in fruits, vegetables, whole grains, and fiber are associated with a reduced risk of CAD.
Physical inactivity is a major risk factor equal to cholesterol, cigarette smoking, and high blood pressure. Because a higher proportion of U.S. adults lead a sedentary lifestyle (60%) than have hypertension (10%), have hypercholesterolemia (excessive cholesterol in the blood) (10%), or smoke one pack or more of cigarettes per day (18%), increasing the general population’s physical activity level may have a greater effect on reducing the incidence of CAD than the modification of the other three risk factors.
Regular aerobic exercise lowers resting pulse rate and blood pressure, improves the ratio of good to bad cholesterol, and helps prevent and control diabetes and osteoporosis. The risk of heart attack and death from heart disease declines steadily as the frequency of vigorous exercise increases. Occasional exercise (one or two times per week) reduces the risk of heart attack by 36%, moderate exercise (three or four times per week) reduces it by 38%, and regular, vigorous exercise (five or more times per week) reduces it by 46%. The benefit of habitual exercise toward reducing heart attack was greatest among those who worked out for 11 to 24 minutes and did not change or increase further after 24 minutes of exercise.5
Impaired glucose metabolism (e.g., insulin resistance, hyperinsulinemia, glucose intolerance) is reported to be atherogenic. Diabetes mellitus, impaired glucose tolerance, and high-normal levels of glycated hemoglobin are powerful contributors to atherosclerotic cardiovascular events in the Framingham study.363
The association is complex, and the pathways by which elevated insulin adversely affects both CAD risk factors and the risk of developing CAD remain unknown. The risk for CAD in participants younger than 65 years was double in men and triple in women with diabetes compared with their nondiabetic counterparts. Individuals with type 2 diabetes mellitus have a risk of MI equivalent to that of someone without diabetes who has had a previous MI.
Diabetes confers the same risk of cardiovascular disease as aging 15 years.42 Kidney disease accompanied by hypertension is a serious complication affecting the cardiovascular system among people with diabetes. More than 80% of persons who have diabetes die of some form of cardiovascular disease. Bypass surgery provides significantly better survival than angioplasty for individuals with diabetes in some subgroups. This may be attributed to the more extensive CAD among people with diabetes and the greater tendency for their arteries to restenose after angioplasty.
Low levels of HDL cholesterol (and high levels of triglycerides) produce twice as many cases of CAD as any other lipid abnormality; this effect is exaggerated in women (see Table 12-4). Hormonal status in the menopausal or postmenopausal woman is now known to be a likely contributing risk factor in the development of CAD. The mechanism through which a protective effect is mediated by estrogen has not been explained completely (see previous discussion in this chapter).
Modification of Risk Factors That Might Reduce Incidence of Coronary Artery Disease.: Psychologic factors andemotional stress (e.g., depression, anxiety, personality factors and character traits, social isolation, chronic life stress) contribute significantly to the pathogenesis and expression of CAD. People who are negative, insecure, and distressed (type D personality) are three times more likely to experience a second heart attack than non-D types.96
Other personality traits likely to affect the heart are free-floating hostility associated with anger and a sense of time urgency (two major components of the type A personality). The long-held belief that anger can increase the risk of acute MI and can be an immediate trigger of heart attacks has been verified.361
The relationship between these entities and CAD can be divided into behavioral mechanisms, whereby psychosocial conditions contribute to a higher frequency of adverse health behaviors such as poor diet and smoking, and direct stress-induced pathophysiologic mechanisms, which contribute to neuroendocrine activation, hemodynamic and catecholamine responses, and platelet activation.316 Personality traits are more difficult to change than other psychologic risk factors, such as depression or anxiety.96
Improved technologies and research demonstrate that acute mental or emotional stress triggers myocardial ischemia, promotes arrhythmogenesis, stimulates platelet function, and increases blood viscosity through hemoconcentration. Moderate to severe depression is associated with altered cardiac autonomic modulation, including elevated heart rate, elevated norepinephrine, and reduced heart rate variability, known risk factors for cardiac morbidity and mortality.
In the presence of atherosclerosis in people with CAD, acute stress also causes coronary vasoconstriction. Hypersensitivity of the sympathetic nervous system to perceived adversity (manifested by exaggerated heart rate and blood pressure responses to psychologic stimuli) is an intrinsic characteristic among these individuals; in addition, the calming response of the parasympathetic nervous system is diminished in persons who are hostile and the parasympathetic counterbalance does not stop the effects of adrenaline on the heart.
These emotions trigger the stress response, increasing blood pressure and heart rate and altering platelet function. Increasing evidence suggests that cognitive behavioral therapy and anger management may benefit cardiac clients by improving medical outcome. (See also Special Implications for the Therapist: Stress, Coping, and Self-Efficacy in Chapter 2.)
Discriminatory medicine, the idea that women (and minorities) are treated less aggressively than men for heart problems, has been strongly debated. On the one hand, it has been suggested that a woman’s symptoms are more likely to be misinterpreted, overlooked, or dismissed as psychosomatic and that women are less likely to undergo diagnostic procedures. On the other hand, lower rates of cardiac catheterization among women may be related to women’s lower rate of positive exercise test results and older age at the time of symptomatic presentation rather than bias based on gender. As mentioned earlier in this chapter, there is evidence to suggest that this trend is changing toward improved gender equity. Research to understand ethnic differences remains limited.
Oxidative stress, or the oxidation of LDL particles as part of the atherosclerotic formation, is under active investigation. Oxidative stress is considered a significant risk factor for cardiovascular disease. However, antioxidant nutrients failed to provide benefits for cardiovascular disease in several human trials.
This apparent paradox between the role of antioxidants in reducing oxidative stress and the failure of many antioxidant supplementations warrants further research. Meanwhile, according to the current American Heart Association scientific statement, antioxidant vitamin supplements to prevent cardiovascular disease are not recommended.199 See further discussion of the oxidation process in Chapter 6.
Moderate alcohol consumption decreases the risk of heart disease in some people. This is attributed to alcohol’s beneficial effects on hemostasis, including platelet aggregation, coagulation factors, and fibrinolytic system.289 Alcohol intake increases activity of an enzyme called tissue-type plasminogen activator (t-PA) that helps to keep blood flowing smoothly by initiating dissolving of clots (fibrinolysis). The highest levels of endogenous t-PA protein have been found among daily consumers of red wine, and the lowest levels have been found among subjects who never (or rarely) consume alcohol.3
Although a small amount of alcohol taken daily with meals may elevate levels of HDL cholesterol and the bioflavonoids in red wine reduce atherosclerosis, most researchers oppose recommending drinking as a public health measure to fight heart disease and stress that no one, particularly people with a personal or family history of alcohol abuse, should drink alcohol to improve cholesterol. It should always be remembered that heavy alcohol consumption and binge drinking increase risk of blood clot formation, cardiac arrhythmia, elevated blood pressure, and cardiovascular disease. Dietary supplements containing flavonoids and antioxidants are now available without the sugar in grape juice or the alcohol in wine.
The cardioprotective benefits appear to be effective only in men over age 45 years and women over age 55 years when limited to one or two drinks per day.151 Greater concentrations of alcohol cause direct coronary artery constriction, which may explain the relationship between ethanol and sudden coronary ischemia that is seen clinically. In addition, the depressive effect of excessive alcohol on the function of myocardial cells decreases myocardial contractility and can be very disabling. Chronic abuse of alcohol is also related to a higher incidence of hypertension, which places greater stress on a heart already compromised by CAD. Chemical dependency is also associated with increased stress on the diseased heart.
In addition, several epidemiologic studies have suggested that sleep-disordered breathing is a risk factor for cardiovascular disease, particularly hypertension, stroke, and heart failure.
Nonmodifiable Risk Factors.: The risk of cardiovascular disease or CAD increases with increasing age, and the person older than 40 years is more likely to become symptomatic. Gender as a nonmodifiable risk factor is reflected in the fact that heart disease is more prevalent among men; women generally experience heart attacks 10 years later than men, possibly because of the biologic protection factor provided premenopausally by estrogen.
By age 45 years, heart disease affects one woman in nine. By age 65 years, this ratio becomes one in three, more closely approximating rates among men. These statistics represent the outcome when no hormone replacement therapy is initiated, but as previously mentioned, the effectiveness of hormone replacement therapy in reducing morbidity and mortality associated with CAD is still under investigation.
A family history of cardiovascular disease (i.e., one or more members of the immediate family with the disease) is associated with increased incidence of heart disease. It is proposed that a mix of environmental and genetic factors leads to atherosclerosis of the coronary arteries in a complex, unpredictable, and unknown series of interactions. For selected individuals, genetic predisposition, especially abnormalities in lipoprotein metabolism, can play a very important role in their risk of developing atherosclerosis.
Current research is exploring the possibility of “candidate genes” that may be associated with an increased risk of CAD. Current technology and information from the Genome Project now allow linkage in family studies to be supplemented with accurate localization of a disease-causing or susceptibility (candidate) gene.
For example, apolipoprotein E-4 (apo E-4), one of three forms of a gene involved in clearing cholesterol from the body, is associated with an increase in LDL and total cholesterol. Another candidate gene (DSCAM) present in individuals with Down syndrome and CAD has been identified, and a mutation in the ABC-1 (adenosine triphosphate [ATP]–binding cassette transporter 1) protein involved in lipoprotein metabolism can disrupt normal transport and processing of cholesterol. In the future, inherited markers in combination with traditional risk factor assessment will be used first to prevent and then to manage vascular disease through better utilization of diagnostic testing and individualized pharmacologic intervention.
Ethnicity is a risk factor, and certain ethnic groups have a higher rate of heart disease. The risk of heart disease is highest among blacks, who are three times more likely to have extremely high blood pressure, a major risk factor for CAD, and who have a higher prevalence of other risk factors, such as diabetes mellitus, obesity, and cigarette smoking.
Native Americans have an unusually high rate of diabetes and obesity, although lower total and LDL cholesterol levels appear to offset the difference. Conflicting comparisons of CAD mortality between Mexican Americans and non-Hispanic whites have been reported. Despite their adverse cardiovascular risk profiles, especially a greater prevalence of diabetes, Mexican Americans are reported to have lower mortality rates from CAD. However, when death certificates are more carefully examined and coded, Mexican Americans have rates equal to or higher than those of non-Hispanic whites.253 Hispanics are less likely than whites to receive catheterization and angioplasty procedures.109
Infections (bacterial and viral) as a cause of atherosclerosis and thereby CAD in some people have been supported by experimental and clinical data. This discovery came about as researchers identified the presence of a common virus (cytomegalovirus) in arterial plaque as a contributing factor to angioplasty failure. Atherosclerosis, now recognized as an inflammatory process, and injury to the inner layer of the artery may be triggered by acute or chronic infection, particularly in more susceptible disease states such as diabetes.
Epidemiologic studies have suggested a link between chronic Helicobacter pylori infection260 or prior infection with Chlamydia pneumoniae and ischemic heart disease, but this idea is speculative, and research results have been correspondingly conflicting. Although C. pneumoniae infection has been associated with the initiation and progression of atherosclerosis, results of clinical trials investigating antichlamydial antibiotics as adjuncts to standard therapy in patients with CAD have been inconsistent,23 and evidence available to date does not demonstrate an overall benefit of antibiotic therapy in reducing mortality or cardiovascular events in adults with CAD.
New Predictors.: Investigators may have identified markers for heart disease present in apparently healthy people, that is, components of blood or other factors that can help identify risk of CAD before symptoms develop (see Table 12-3). Serum cholesterol has been used for a long time, but many more potential predictors of risk are being examined. Homocysteine (Hcy), an amino acid that is generated as the body metabolizes another amino acid, methionine (found in animal-derived foods), occurs naturally in blood and tissues and is more common in people with CAD. Elevated levels of homocysteine may be as much of a risk factor as high cholesterol or smoking.
High-sensitivity C-reactive protein (hsCRP), an acute-phase reactant that reflects low-grade systemic inflammation, is produced by the liver in response to trauma, tissue inflammation, and infection, and seems to predict hypertension, diabetes, heart attacks, and strokes before they occur.280 People with even slightly elevated blood levels of CRP appear to be at increased risk for CAD and its complications regardless of age, gender, general health, or the presence of other CAD risk factors.
Cigarette smokers have elevated levels of CRP, and individuals experiencing a heart attack who have high levels of CRP have a slower than normal response to antithrombotic medication. Preliminary data suggest that the relative effectiveness of secondary preventive therapies, such as cholesterol-lowering drugs and aspirin, may depend on an individual’s baseline CRP level.6
Fibrinogen, a blood protein essential for proper clotting, may predict first heart attacks (and strokes) in people with unstable CAD and is a risk factor for future cardiovascular problems in those who have not yet developed CAD.
Lipoprotein (a), (Lp[a]), an LDL cholesterol particle with an additional protein attached, slows the breakdown of blood clots. People with high levels of Lp(a) are at greater risk for MI than those with lower levels of Lp(a).
Pulse pressure (less than 60 mm Hg), a measure of arterial stiffness (systolic blood pressure less diastolic blood pressure), has been investigated as an independent predictor of CHD risk. Pulse pressure has been shown to predict risk for cardiovascular events in men; this association has not been well established in women. Results of postmenopausal women with CAD evaluated in the Heart and Estrogen/Progestin Replacement Study showed that pulse pressure has a predictive value for heart failure and stroke, but is not associated with mortality associated with CAD.233
Dermatologic indicators of coronary risk, such as greying of the hair, hair loss (baldness), thoracic hairiness, and diagonal ear lobe crease are additional but weak risk indicators of CAD in men under age 60 years, independent of age and other established coronary risk factors. Short stature may also be an early indicator of heart disease risk. Available data on the mentioned skin conditions as markers for elevated coronary disease risk have come under question.30,138
Erectile dysfunction (impotence) is a hemodynamic event that can warn of ischemic heart disease in some men. Researchers may eventually call impotence a “penile stress test” that can be as predictive as a treadmill exercise stress test.246
Metabolic syndrome has received increased attention within the last few years (see also discussion in Chapter 11). Several terms have been proposed previously for it: the “deadly quartet,” syndrome X, insulin resistance syndrome, and hypertriglycemic waist.135 The term metabolic syndrome is most commonly used in the cardiovascular field.
Metabolic syndrome can be viewed as an aggregation of multiple cardiovascular risk factors of endogenous origin in one individual. Until recently, the metabolic syndrome has been considered a complex disorder (not a discrete entity with a single cause but truly a syndrome, i.e., a grouping of the risk factors) with no single factor as a cause.135
However, latest research using confirmatory factor analysis, while supporting the current clinical definition of the metabolic syndrome, suggests the existence of a single latent factor that underlies all of the core components of the metabolic syndrome.267 The existence and the nature of this single factor remain to be proved.
Metabolic syndrome is a group of interrelated factors of metabolic origin—metabolic risk factors—that appear to directly promote the development of the atherosclerotic cardiovascular disease. Another group of factors, the underlying risk factors, can precipitate the metabolic syndrome.
Metabolic risk factors include dyslipidemia (elevated serum triglycerides, apolipoprotein B, and LDL; low level of HDL cholesterol), elevated blood pressure, and elevated plasma glucose, a prothrombotic state, and a proinflammatory state.135 The most important underlying risk factors are abdominal obesity and insulin resistance; other associated conditions include physical inactivity, aging, hormonal imbalance, and genetic or ethnic predisposition.135 Excess visceral fat is considered more strongly associated with the metabolic syndrome than any other adipose tissue compartment.66,157
People with the metabolic syndrome have a twofold increase in relative risk for cardiovascular events, and in individuals without established type 2 diabetes mellitus, a fivefold increase in risk for developing diabetes as compared with people without the syndrome.
In 2001 the National Cholesterol Education Program (NCEP) Adult Treatment Panel III (ATPIII)236 proposed a set of diagnostic criteria based on common clinical measures, including waist circumference, triglycerides, HDL, blood pressure, and fasting glucose level (Box 12-2). Abnormalities in any three of these five measures constitute a diagnosis of the metabolic syndrome. Presently, the American Heart Association and the National Heart, Lung, and Blood Institute adhere to the NCEP ATPIII criteria.135
Most of the time, metabolic syndrome is manifested in the presence of some degree of obesity and physical inactivity. In addition to the lifestyle changes (exercise, smoking cessation) drug therapy for risk factors may be required.
The primary goal of clinical management of the metabolic syndrome is to reduce the risk for atherosclerotic cardiovascular disease. When encountering clients presenting with abdominal obesity, physical therapists should appreciate that waist circumference may be associated with lipid abnormalities.157
A possible link has been recently demonstrated between psychosocial stressors from everyday life and the metabolic syndrome. Employees with chronic work stress have more than double the odds of the syndrome compared with those without the stress.73
Pathogenesis.: The exact mechanism by which the development of cardiovascular disease/CAD can be explained has yet to be determined. The recent implication of infectious agents in initiating the inflammatory cascade may help explain the pathogenesis in some (but not all) cases.293 Clinical and laboratory studies have shown that inflammation plays a major role in the initiation, progression, and destabilization of atheromas. CRP has been found in a variety of cardiovascular diseases. However, whether CRP is a contributing cause or an aftereffect remains undetermined.
Mutations in the PCSK9 gene (chromosome 1) have been linked with naturally high levels of LDL in some people. Other PCSK9 variations have been discovered that cause naturally low levels of LDL by increasing the number of LDL receptors in the liver, making the liver better able to attract excess LDL.78
Many new studies emphasize the fact that cholesterol deposits are only one of many mechanisms through which acute CAD develops. New information points to the endothelium as a modulating factor in the pathogenesis of CAD through the production of nitric oxide and angiotensin II, which maintain the homeostatic environment influencing the progression of CAD. This imbalance tends to promote CAD in individuals who have multiple risk factors.
Endothelium-derived nitric oxide is an important mediator of exercise-induced changes in skeletal muscle blood flow. This molecule, composed of one nitrogen atom and one oxygen atom, is responsible for the natural dilation of blood vessels.
Nitric oxide is an antilipid that provides a nonstick coating to the lining of blood vessels, much like Teflon. These two effects have helped explain how nitric oxide might prevent heart attacks and strokes and why nitroglycerin works—nitroglycerin is converted to nitric oxide inside vascular tissue, where it relaxes smooth muscle in arteries and causes blood vessels to dilate.
In the normal artery, the endothelial lining is tightly packed with cells that allow the smooth passage of blood and act as a protective covering against harmful substances circulating in the bloodstream. The normal endothelium presents a nonreactive surface to blood, but injury triggers the thrombotic process.
In the earliest stage of atherosclerosis, damage to arteries arises from a combination of factors. In some cases, the initial damage comes from LDL cholesterol that has been modified by free radicals (see Fig. 6-2). Free radicals are abundant in people who smoke and who have high blood pressure or diabetes. In other cases, high levels of homocysteine or bacteria may contribute to early damage of arterial linings.
In general, most current theories include the following major events in the development of an atherosclerotic plaque (Fig. 12-2): Arterial wall damage occurs either from injury caused by harmful substances in the blood or by physical wear and tear as a result of high blood pressure. This injury to the blood vessel wall permits the infiltration of macromolecules (especially cholesterol) from blood through the damaged endothelium to the underlying smooth muscle cells. Naked collagen acts like flypaper for platelets, causing them to aggregate at the site of injury and plug up the wound.

Figure 12-2 Updated model of atherosclerosis. Atherosclerosis begins with an injury to the endothelial lining of the artery (intimal layer) that makes the vessel permeable to circulating lipoproteins. New technology using intravascular ultrasound shows the entire atherosclerotic plaque and has changed the way we view things. The traditional model held that an atherosclerotic plaque in the blood vessel, particularly a coronary blood vessel, kept growing inward and obstructing flow until it closed off and caused a heart attack. This is not entirely correct. A, It is more accurate to say that in the normal vessel B, penetration of lipoproteins into the smooth muscle cells of the intima produces fatty streaks and the start of a coronary lesion forms. C and D, The coronary lesion grows outward first in a compensatory manner to maintain the open lumen. This is called positive remodeling. The blood vessel tries to maintain an open lumen until it can do so no longer. A little roof or “fibrous cap” separates the plaque from the inside of the lumen. A blood clot called an intraplaque thrombosis can form inside the plaque; the clot may never leave the plaque. E, The plaque (atheroma) begins to build up, gradually pressing inward into the lumen with obstruction of blood flow and possible rupture and thrombus potentially leading to myocardial infarction or stroke. Capped plaques are not as likely to rupture as the softer type packed with viscous cholesterol and white blood cells but only capped with a thin layer of collagen. F, Vascular disease today is considered a disease of the wall. Some researchers like to say the disease is in the donut, not the hole of a donut, and that is a new concept. (From Goodman CC, Snyder TE: Differential diagnosis for physical therapists: screening for referral, ed 4, Philadelphia, 2007, Saunders. Data from Horn HR: Insulin resistance, diabetes, and vascular disease: the rationale for prevention. Available on-line at http://www.medscape.com/viewarticle/466799_2. April 2007.)
The core of a coronary thrombus (clot) is composed of platelets, forming a so-called white thrombus. Early-stage plaque formations known as fatty streaks consist of foam cells (white blood cells coated with LDL particles, smooth muscle cells that move in from deeper layers of the artery wall, and platelets).
Cholesterol-filled plaques can take decades to form, sitting snugly in an artery wall for years. What makes a plaque break open and leak its contents into the bloodstream, causing a clot that can block an artery supplying the heart or brain, remains unknown. Experts speculate it could be a spike of high blood pressure or a surge of chemical messages that accompany anger, stress, or other intense emotion. It could be the result of cholesterol crystallization inducing cap rupture and/or erosion.1,203
Although platelet activation is a normal response to injury, in atherosclerosis, once the platelets adhere, they also release chemicals that alter the structure of the blood vessel wall, so that what starts out as a small erosion in the wall can end up a swollen mound of platelets, muscle cells, and fibrous clots, a process called proliferation that obstructs the flow of blood through the vessel.
After a thrombus forms and causes static or reduced blood flow in the vessel, the clot stabilizes with fibrin. This is commonly referred to as a red thrombus because of the presence of entrapped red blood cells. Within the thrombus is thrombin, which remains active and can activate platelets. Platelets also release plasminogen activator inhibitor 1 (PAI-1), a potent natural inhibitor of fibrinolysis, and vasoactive amines that can lead to vessel spasm, further platelet aggregation, and thrombus formation or reocclusion. This cycle of injury, platelet activation, and lipid deposition can lead to complete blockage of a vessel and result in ischemia and necrosis of tissue supplied by the obstructed blood vessel.
Clinical Manifestations.: Atherosclerosis by itself does not necessarily produce symptoms. For manifestations to develop, there must be a critical deficit in blood supply to the heart or other structures supplied by affected blood vessels. For example, symptoms of CAD may not appear until the lumen of the coronary artery narrows by 75%. Then, pain and dysfunction referable to the region supplied by an occluded artery may occur.
When atherosclerosis develops slowly, collateral circulation develops to meet the heart’s needs. Complications from atherosclerosis occur because it is a progressive disorder that results in more severe cardiac disease if it is not prevented or untreated. Common sequelae of atherosclerosis affecting coronary arteries include angina pectoris, MI or heart attack, and sudden death.
Men experience angina as the first symptom of CAD in one third of all cases and heart attack or sudden death in the majority of cases, whereas one half of all women experience angina and remain asymptomatic or present with atypical symptoms in the remaining cases.
Atypical symptoms of angina in women include breathlessness, pain in the left chest, upper abdominal pain, and back or arm pain (more rarely, isolated pain in the right biceps muscle) in the absence of substernal chest pain. The pain may be more diffuse and is described as sharp or fleeting, unrelated to exercise, unrelieved by rest or nitroglycerin but relieved by antacids, and characterized by palpitations without chest pain. The pain may be repeated and prolonged. Chest pain in women with chronic stable angina is more likely to occur during rest, sleep, or periods of mental stress.
MEDICAL MANAGEMENT
Overwhelming evidence indicates that cardiovascular disease and CAD are largely preventable; therefore whenever possible, prevention of cardiovascular disease and CAD is the goal for everyone. And atherosclerosis is not a disease of middle to old age; it begins in adolescence and young adulthood and develops slowly but progressively throughout the body.
Preventing heart disease means controlling LDL before atherosclerosis gets a chance to do much damage. Reduction in the plasma level of LDL (at or below 100 mg/dl) throughout the lifespan through the use of diet, exercise, and statins or other cholesterol-lowering drugs is the proposed ways to do this.78
Healthy People 2010 has identified the following goals for heart disease and stroke: improvement of cardiovascular health and quality of life through the prevention, detection, and treatment of risk factors; early identification and treatment of heart attacks and strokes; and prevention of recurrent cardiovascular events. An excellent guide to evidence-based primary prevention of cardiovascular disease and similar recommendations for prevention of cerebrovascular disease (i.e., stroke) are available.131,136,148,258,259
Health perceptions, health care–seeking behavior, and willingness to participate in long-term preventive therapies are significantly influenced by age, cultural, and socioeconomic factors. Many physicians underestimate the life expectancy in older adults. For example, the average 65-year-old can expect to live an additional 15 to 20 years and function independently for more than 70% of this time.
Adults older than 80 years can expect to live 7 to 10 more years and function independently for one half of that time. Older individuals are less likely to be referred to cardiac rehabilitation and exercise-training programs and less likely to attend than younger adults. Therefore, preventive cardiology, including primary and secondary preventive efforts directed at the older adult, is important.193
Primary and secondary prevention programs are needed that are modified for the language, cultural, and medical needs of people of all age groups and ethnic backgrounds but especially for older ethnic minorities who are at increased risk for cardiovascular disease.320 Ethnic comparisons of health behaviors and prevalence of risk factors among teenagers support the need for health promotion intervention among urban ethnic teenagers.105
Women are less likely than men to receive health care advice on risk reduction while they are still healthy (i.e., before a significant cardiac event), even though they are more likely to die with the first heart attack. For this reason, new guidelines for prevention of heart disease in women were published in 2007.229
The bottom line is that even for people with a strong genetic component, modifying risk factors can slow the growth and spread of atherosclerotic plaque and reduce the risk of heart attack or stroke. The goal is to prevent cholesterol-filled plaque from rupturing, a key event that leads to the formation of blood clots that can block a coronary or carotid artery. Many people with significant nonmodifiable risk factors for heart disease but who follow a heart-healthy lifestyle live longer and in better health with better quality of life compared with those individuals who do not follow a heart-healthy plan.
DIAGNOSIS.
Current national guidelines advise everyone over age 20 to have his or her cholesterol checked to establish a baseline with follow-up (retesting) once every 5 years (more often for those with risk factors for heart disease).
Advances in technology are rapidly changing the diagnostic tools available to physicians for diagnosing and evaluating CAD. Coronary angiography (angiogram or arteriogram; x-ray examination of the arteries with dye injection) has been the most widely used anatomic test to assess the degree of obstructive coronary disease and left ventricular contractility.
Angiograms are limited by their inability to detect which plaques represent vulnerable sites for rupture, and all forms of chest pain in women are associated with a lower prevalence of positive findings on angiography, making the diagnosis challenging. Tests using ultrasound or nuclear agents are less reliable in women because signals are blocked by breast tissue. Angiography is much more accurate than echocardiography; echocardiography improves the diagnostic accuracy of stress tests.
Echocardiography is a group of interrelated applications of ultrasound imaging (including Doppler, contrast, stress, and real-time three-dimensional [RT-3D] echocardiography). Advances in echocardiography have expanded its use in assessment of regional myocardial function, analysis of diastolic function, and quantification of regional myocardial function in different pathologic conditions, including ischemic heart disease.
Echocardiography has the potential to image myocardial perfusion along with wall motion and wall thickening. Stress echocardiography showing responses of the heart can be performed during or after a number of different physical stressors. This is important, because responses of the heart to stressors are probably even more important than how the heart functions at rest.
Until this technology is available everywhere, exercise treadmill testing to record symptoms and the electrical activity of the heart under stress continues to offer a means of assessing risk of future cardiac events in most groups (obese, sedentary, middle-aged or older men and women; studies among ethnic groups are under way).130
Heart rate recovery after submaximal exercise has been confirmed as a predictor of mortality. This measurement is routinely obtained during exercise testing; it is determined by subtracting the heart rate 2 minutes after exercise from the heart rate at the end of exercise. Abnormal heart rate recovery is defined as a reduction of 12 beats/min or less from the heart rate at peak exercise as compared to the heart rate measured 2 minutes after exercise cessation.
People with an abnormal heart rate recovery are four times as likely to die as those with a normal heart rate recovery. This screening tool can be used with healthy adults as well as with those who have known heart disease.79,80 A delay in decline of systolic blood pressure after graded exercise is another independent correlate of CAD.
Other diagnostic test procedures available include ultrafast computed tomography (fast CT; “heart scan”), which allows for a computer image accommodating for the heart’s pumping cycle. Multidirectional or multidetector CT (also referred to as the “new angiogram”) generates up to 64 slicelike images of the heart. A computer then reconstructs these slices to create a detailed 3D image of the heart and coronary arteries. Although less expensive, this new technology is not yet considered a replacement for angiography as it exposes people to increased doses of radiation compared to a traditional coronary angiogram.
Magnetic resonance angiography (MRA) uses a powerful cylinder-shaped magnet able to vibrate in distinctive ways to create a signal that is translated into a picture. This technique is also synchronized to the heart cycle, able to detect plaques. High-speed rotational angiography may be the next technologic diagnostic technique. High-speed rotational angiography is a newly available angiographic modality that gives a dynamic multiple-angle perspective of the coronary tree during a single contrast injection.205
With a standard angiogram, the camera is placed at different angles and takes a series of pictures of the heart. Dye is injected with each angle photographed. High-speed rotational angiography allows the camera to sweep across the heart in an arc taking all the (digital) pictures with one injection. The digital component allows the cardiovascular surgeon to stop and look at each frame.
In the future advanced technology may be able to determine which plaques are most likely to rupture. Thermography using probes to check the temperature of arteries may also reveal vulnerable plaques that are at risk for rupture, since these will be inflamed with elevated temperatures. The routine measurement of newer predictors, such as Lp(a) and CRP, is not recommended at this time for prognostic use and will be delayed until the clinical benefits of altering these concentrations are made available.
MODIFICATION OF RISK FACTORS.
Modifying risk factors whenever possible can decrease the risk of cardiovascular disease/CAD, especially prevention or cessation of cigarette smoking, management of diabetes and hypertension, and modification of diet. For example, folate deficiency was believed to be a major determinant of the increased risk of cardiovascular disease related to elevated total homocysteine (tHcy) because these nutritional components benefit both the vascular wall structure and the blood coagulation system.101
Folate, riboflavin, vitamin B6, and vitamin B12 are essential in homocysteine metabolism. But recent studies using folic acid supplements, though successful in reducing homocysteine levels, did not lower the risk of recurrent cardiovascular disease after acute MI. A harmful effect from combined B vitamin treatment was observed. The American Heart Association no longer recommends folic acid supplements for individuals with elevated levels of homocysteine.
Changing dietary habits by reducing fat intake can result in regression and disappearance of fatty streaks consisting of lipid-laden macrophages, T lymphocytes, and smooth muscle cells before these components progress to form a fibrous plaque.
Dietary changes are recommended for everyone, including children and adults, since it is now recognized that blood vessel changes associated with heart disease begin as early as 15 years of age and the progression of the lesions is strongly influenced by the same risk factors that predict risk of clinically manifest coronary disease in middle-aged adults.317,368 In addition, at least 25% of all Americans under age 19 years are overweight or obese.
There is a need for early and aggressive control of all risk factors in young persons for long-range prevention of CAD and related diseases. The Unified Dietary Guidelines have been published as nutritional guidelines by experts from the American Heart Association, American Cancer Society, American Dietetic Association, American Academy of Pediatrics, and National Institutes of Health.93
In addition, an excellent guide to risk reduction outlining goals, screening, and recommendations for lifestyle factors and pharmacologic interventions is available.229 The National Heart, Lung, and Blood Institute also has a validated health risk appraisal instrument (ATPIII scale) that is easy to use.239
EXERCISE AND PHYSICAL ACTIVITY.
Exercise and physical activity according to recommendations from the Centers for Disease Control and Prevention (CDC) (i.e., moderate-intensity exercise for at least 30 minutes on most days of the week) have been shown to reduce the risk for coronary events, ischemic stroke,154 metabolic syndrome and insulin resistance, and diabetes mellitus for men and women.209,344
The American College of Sports Medicine’s position on the quantity and quality of exercise for developing and maintaining cardiorespiratory and muscular fitness and flexibility in healthy adults recommends aerobic endurance training at least 2 days/wk at 50% or higher VO2 and for at least 10 minutes. VO2 is a measure of oxygen uptake sometimes described as aerobic capacity, ventilatory uptake, or physical working capacity. Maximal oxygen consumption is referred to as VO2max. This measurement reflects the integration of three components of the delivery system that transports O2 from the outside air to the working muscles: pulmonary ventilation, blood circulation, and muscle tissue.
In recent years the view that physical activity has to be vigorous to achieve a reduction in risk of CAD has been under question. Substantial evidence supports the benefit of continued regular physical activity that does not need to be strenuous or prolonged and includes daily leisure activities, such as walking or gardening. Taking up regular light or moderate physical activity in middle or older age confers significant benefit for cardiovascular disease.343
The National Runners’ Health Study reports that substantial health benefits occur (in men) at exercise levels that exceed the CDC guidelines, suggesting that intense exercise offers one set of benefits whereas lengthy exercise provides another.362 Other studies report the benefits of shorter periods of physical activity in decreasing the risk of CAD as being equal to one longer, continuous session of exercise, as long as the total caloric expenditure is equivalent.132
The effect of exercise on cholesterol has been documented, but it remains unclear which component of exercise is the underlying beneficial mechanism. Exercise frequency may be more important than intensity in improving HDL cholesterol and cholesterol ratios,179 and resistive exercise training has been reported to raise HDL cholesterol levels, but studies in these areas have been limited.128,263 Even so, many health benefits from physical activity can be achieved in shorter bouts at less intensity.10
More studies are required to identify the ideal prescriptive exercise. Interestingly, endothelial damage has been reported after intense aerobic exercise, raising additional questions about exercise for athletes with cardiovascular risk factors.37 It is likely that in the future, different exercise regimens for specific heart disease risk factors will be individually prescribed.
Exercise alone independent of weight loss or diet changes can have significant beneficial effects on cardiovascular risk factors in overweight people with elevated cholesterol levels.53 Exercise is the one single intervention with the ability to influence the greatest number of risk factors (e.g., aids in smoking cessation, alters cholesterol levels, reduces blood pressure, helps control blood glucose levels, reverses the effects of a sedentary lifestyle, contributes to weight loss, helps in managing stress-induced increases in heart rate and blood pressure).
In fact, researchers at the University of Texas using RT-3D echocardiography to compare the effects of medications with the effects of exercise on coronary artery perfusion declare exercise to be “the most powerful drug available in preventing cardiac events.”74 Exercise can lessen depression, anger, and stress, which frequently interfere with recovery, and heart attack survivors who follow the CDC exercise guidelines reduce their risk of a fatal second episode by up to 25%.165
PHARMACOTHERAPY AND CHEMOPREVENTION.
Chemoprevention is an established method in the primary and secondary prevention of cardiovascular (and cerebrovascular) disease. Clinical trials have proven conclusively that both fatal and nonfatal coronary events and strokes can be prevented.336 Pharmacologic management is used to reduce the risk of clotting, to treat hypertension, and to decrease serum cholesterol level when it exceeds 200 mg/dl.
Medications are now available (3-hydroxy-3-methylglutaryl coenzyme A [HMG-CoA] reductase inhibitors, better known as “statins”) that have been proven effective not only in lowering LDL levels and raising HDL levels but also in reducing cardiac events (primary and secondary prevention of MI).
However, caution has to be executed when a combination of drugs is used. Recent findings showed increased rate of death in patients receiving atorvastatin (Lipitor) in combination with torcetrapib, an HDL booster, compared with those receiving the Lipitor alone. The drug company subsequently halted clinical drug trials of experimental cholesterol treatment with torcetrapib. Target measurements to reduce risk factors developed by the American College of Cardiology and the American Heart Association are listed in Table 12-4.
Low-dose aspirin, 75 to 81 mg/day, was found to be just as effective in prevention of cardiovascular disease as high doses that result in increased incidence of bleeding events, primarily related to gastrointestinal (GI) tract toxicity.61 The American Heart Association now recommends low-dose aspirin therapy of 81 mg/day or 100 mg every other day for all women age 65 or older. Studies show that aspirin will not prevent heart attacks in low-risk women under age 65, but it may be considered for all women at risk for stroke who are not at increased risk of bleeding.
TREATMENT.
Medical management is directed toward the specific blood vessel occlusion and depends on complications, for example, occlusive disease of the peripheral vasculature, arterial disease in diabetic clients, occlusive cerebrovascular disease, or visceral artery insufficiency (intestinal ischemia) (see discussion of each individual complication).
Surgery.
Surgical management of atherosclerosis of the coronary arteries may include PTCA (Fig. 12-3), CABG (Fig. 12-4), and coronary stents (Fig. 12-5). The current generation of drug-coated stents are bare metal covered with a polymer (plastic) coating that holds and releases a drug to inhibit the growth of endothelial cells. Several companies are working on polymers that are more compatible with the body and less likely to trigger clots. Others are testing polymers that dissolve and disappear after some time.
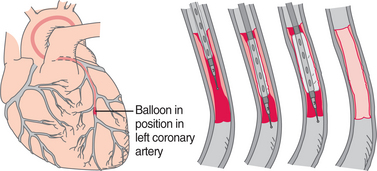
Figure 12-3 Percutaneous transluminal coronary angioplasty (PTCA) can open an occluded coronary artery without opening the chest, an important advantage over bypass surgery. A, Once coronary angiography has been performed to determine the presence and location of an arterial occlusion, a guide catheter is threaded through the femoral artery into the left coronary artery. B, When the angiography shows the guide catheter positioned at the site of occlusion, the uninflated balloon is centered in the obstruction. C, A smaller double-lumen balloon catheter is inserted through the guide catheter. D, The balloon is inflated, compressing the plaque against the arterial wall and deflated until the angiogram confirms a reduced pressure gradient in the vessel. E, The balloon is removed, and the artery is left unoccluded.
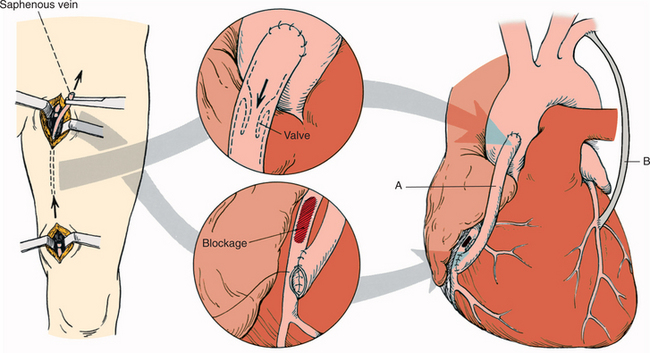
Figure 12-4 Coronary artery bypass graft (CABG). This procedure involves taking a portion of a vein or artery from the chest or leg and grafting it onto the coronary artery. In this illustration, (A) a section of the saphenous vein is used as a graft to route blood around areas of blockage. Bypassing the clogged vessel provides an alternative route (B) for blood to reach the heart muscle. The internal mammary artery can be used as an alternate vein site for grafting. CABG has been a major surgery requiring a sternotomy but is being refined to possibly become an off-pump bypass grafting through a partial sternotomy. It is considered most effective in individuals who have several severely blocked coronary arteries and a previously damaged heart muscle or when repeated revascularization has failed. (From Black JM, Hawks JH, Keene AM: Medical-surgical nursing: clinical management for positive outcomes, ed 6, Philadelphia, 2001, Saunders.)
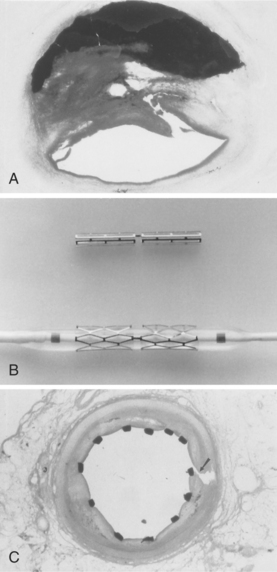
Figure 12-5 Application of the coronary stent. A, Cross-section of a severely occluded coronary artery. B, Blocked coronary artery can be held open using a balloon-expandable device called a coronary stent. C, Stent shown here is in place to maintain opened vessel, allowing blood to pass through freely. Biodegradable stents are under development to reduce or eliminate problems associated with metal stents.342 Delivery of drugs or gene therapy to inhibit intimal hyperplasia and prevent postangioplasty restenosis is under investigation.83,107 (Courtesy Thomas Jefferson University, Philadelphia.)
Angioplasty is performed 10 times more often than bypass surgery; angioplasty combined with a stent reduces the incidence of restenosis, especially for people with diabetes who have a high restenosis rate when treated by standard balloon angioplasty.337 The use of a combined antiplatelet treatment with aspirin and glycoprotein IIb/IIIa receptor blockers (Table 12-5) is a standard pharmacologic regimen after coronary artery stenting for the prevention of thrombosis (thrombosis is the formation of a clot; thrombus is the clot).
For the person with significant coronary and carotid artery disease, the importance of treating symptomatic stenosis of the carotid artery as a means of stroke prevention is now widely accepted. Carotid artery angioplasty and stenting constitute a procedure that is an alternative to carotid endarterectomy, especially for people considered at high risk for postoperative complications.
Blockages that are heavily calcified and that involve long stretches of coronary artery are difficult to treat successfully with angioplasty or stenting. In such cases, rotational atherectomy can be accomplished using a device called a rotoblator (catheter tipped with a tiny rotary blade). This procedure makes sharp cuts in plaque, shaving away the blockage and producing a relatively smooth luminal surface.
Other surgical techniques such as mechanical thrombectomy using a device (AngioJet System) that removes blood clots in the coronary (or carotid) arteries before angioplasty are viable options in some cases but carry a higher rate of major complications, especially for women.
Intravascular ultrasound, a technology that combines echo with catheterization, may eventually allow diagnosis and therapy to be combined as the cardiologist uses a camera on the tip of a catheter to precisely target atherosclerotic blockage. In keeping with the new data on the time of day that cardiac events occur (i.e., thrombus formation is more likely to occur in the morning hours), researchers are now investigating the possibility that postoperative complications are related to the time the procedure takes place.327
Although surgical intervention has been a mainstay for the treatment of CAD, researchers are questioning the necessity of heart surgery and studying the benefits of pharmacologic intervention combined with exercise and lifestyle changes. The role of exercise in the prevention of atherosclerosis has been discussed, but the role of exercise as a treatment modality is equally important.
Cardiac Rehabilitation.
Cardiac rehabilitation exercise training consistently improves objective measures of exercise tolerance, without significant cardiovascular complications or other adverse outcomes. Appropriately prescribed and conducted exercise training is recommended as an integral component of the treatment of atherosclerosis and CAD.4 See further discussion in Special Implications for the Therapist, this section.
Results from the Stanford Coronary Risk Intervention Project (SCRIP) conducted over 4 years have demonstrated that intensive multifactor risk reduction favorably alters the rate of luminal narrowing in coronary arteries of men and women with CAD and decreases hospitalizations for clinical cardiac events. In cases of low-risk, stable CAD, aggressive lipid-lowering therapy is at least as effective as angioplasty in reducing the incidence of ischemic events.54
Numerous other trials (e.g., Leiden Intervention Trial, Heidelberg Diet and Exercise Study, St. Thomas’s Atherosclerosis Regression Study, Cholesterol Lowering Atherosclerosis Study [CLAS]) have focused on the effect of diet-induced reductions in LDL cholesterol and the resultant changes in CAD. Restricting the intake of saturated fat and cholesterol has a favorable result in changing the course of coronary atherosclerosis.
In addition, dietary and lifestyle interventions slowed CAD progression, decreased the incidence and severity of angina, and reduced the number of cardiac events. Anyone with CAD, a family history of CAD, or other risk factors should read the American Heart Association scientific statement Diet and Lifestyle Recommendations Revision 2006.199 Exercise-based cardiac rehabilitation is effective in reducing cardiac deaths, but the effect of exercise alone without a comprehensive cardiac rehabilitation intervention has not been evaluated.167
Because pharmaceutical agents, surgery, and lifestyle changes including diet and exercise have been unable to maintain blood flow without restenosis in some people, new technologic approaches to intervention are being investigated. Emerging treatments for reclosure (restenosis) include antiproliferative (drug)–coated stents and photoangioplasty.
Drug-coated stents resist colonization of the stent (smooth muscle cells cover the surface) and prevent restenosis but can lead to the formation of blood clots. The drugs that prevent the accumulation of scar tissue around the stent also delay healing over the stent site. When tissue does not heal quickly, blood collects and thickens around the stent site, causing a stent-related thrombosis that can cause a heart attack. People with drug-coated stents often take antiplatelet medication (e.g., clopidogrel [Plavix] in combination with aspirin) to prevent this from happening.
Photoangioplasty uses a photosensitive drug that selectively accumulates in atheromatous plaque and remains inactive until exposed to an endovascularly delivered far-red light that reduces or destroys the deposits without damage to the normal vessel wall.143
Gene Therapy.
Gene therapy (i.e., gene transfer–based antirestenosis therapy) is one strategy with the potential to prevent some of the sequelae after arterial injury, induce growth of new vessels, or remodel preexisting vessels.107 Several groups have injected a gene that makes a protein called vascular endothelial growth factor (VEGF). When injected directly into the heart, this gene prompts the heart to sprout tiny new blood vessels to bypass the blocked vessels, a process referred to as therapeutic angiogenesis or biologic revascularization.243,368
Alternatively, endothelial stem cells derived from bone marrow and injected into the region bordering an infarction have been shown to regenerate new myocardium or new blood vessels in animal studies. The increase in oxygen and nutrients accompanying this new tissue formation has the potential of preventing death of myocardial cells, reducing myocardiac remodeling and scarring, and improving heart function by levels of 30% to 40%.116,247
Genetic approaches will continue to identify genes and pathways involved in the predisposition to and pathophysiology of atherosclerosis. Targets for therapeutic intervention based on gene profiling continue to be the focus of research at this time.223
Complementary and Integrative Medicine.
Finally, a review of alternative or complementary integrative medicine, sometimes referred to as mind-body therapies, and their effects on heart disease, blood pressure, lipid levels, morbidity, and mortality is available.202
These techniques remain under investigation and include prayer or meditation and/or religious attendance at church or services; yoga, Tai Chi, and other forms of martial arts; acupuncture; social support and/or support groups; cognitive-behavioral therapy; imagery; hypnosis; physiologic quieting; relaxation techniques; music therapy; and others (Table 12-6).
Table 12-6
Medical Management of Cardiovascular Conditions*
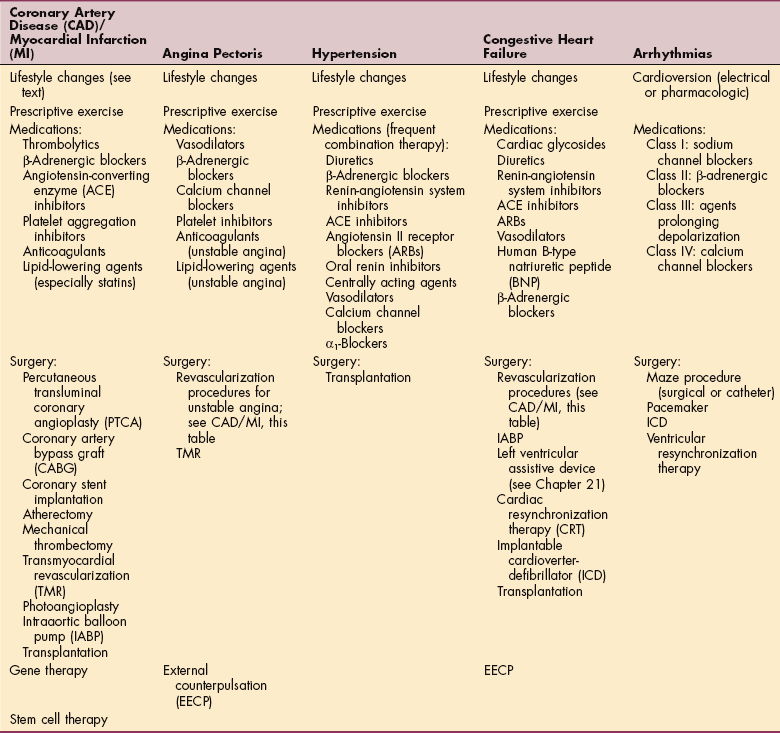
The term blocker is synonymous with antagonist.
Platelet aggregation inhibitors, anticoagulants, and thrombolytics are used to treat overactive clotting but have distinct uses and mechanisms of action. Platelet aggregation inhibitors block platelet aggregation and platelet-induced clotting, anticoagulants inhibit the synthesis of clotting factors, and thrombolytics facilitate clot breakdown after the formation of a clot.
*The use of complementary-integrative therapies in the adjunctive treatment of each of these conditions is under investigation at this time (see text discussion in Atherosclerosis: Treatment). Research centered on pharmacologic and surgical approaches to these conditions is changing rapidly. This information represents a broad overview and may not include every option available.
Adapted from Susan Queen, PT, PhD, University of New Mexico, Albuquerque, NM, 2007, with permission.
PROGNOSIS.
The American Heart Association reports compelling scientific evidence that comprehensive risk factor interventions in people with cardiovascular heart disease extend overall survival, improve quality of life, decrease the need for interventional procedures, and reduce the incidence of subsequent MI. Even so, despite the well-documented benefit of preventive measures and cardiac rehabilitation, compliance with recommendations for reducing risk factors and utilization rates of rehabilitation programs remain low, especially among women.229
Prognosis depends on the site and extent of myocardial necrosis, but nearly 500,000 deaths each year in the United States are attributable to CAD/CHD. Fatality rates for CAD remain low before age 35 years, but these figures increase exponentially until age 75 years, with men generally experiencing mortality at approximately twice the rate of women until age 65 years. Total CAD mortality in women after age 65 years now exceeds that of men. Of the nearly 20,000 persons eligible for heart transplants, only 10% receive a new heart each year. Advanced atherosclerosis is usually fatal if vessels to the brain or heart are affected, but new technology and new surgical intervention may reduce mortality in the decade ahead.
Surgical procedures are considered safe, and although complications can occur, the rates of complications (e.g., reintervention or repeat procedures, reexploration for bleeding) following CABG surgery have declined substantially in the last 15 years despite higher client risks. In the case of angioplasty, the risks of failure, reoperative procedures, and operative mortality are higher with advanced age, female gender, diabetes mellitus, elevated serum cardiac enzymes following the procedure, and impaired left ventricular dysfunction.314
PTCAs are associated with greater rates of restenosis, especially among women, who are at greater risk for complications and have a higher mortality rate. Most studies attribute the higher mortality rate to the fact that women more often undergo the surgery during an emergency, they are usually older at the time of diagnosis than men, they are more likely to have other complicating conditions (e.g., hypertension, diabetes), and they may have smaller, more delicate coronary arteries, making surgery more difficult.
The higher rates of morbidity and mortality associated with angioplasty have resulted in the use of the balloon-expandable stent, which is associated with a low restenosis rate and a favorable clinical outcome with event-free survival rate at 1 year. The need for repeat revascularization has also been significantly reduced.
Angina Pectoris
As blood vessels become obstructed by the formation of atherosclerotic plaque, the blood supply to tissues supplied by these vessels becomes restricted. When the cardiac workload exceeds the oxygen supply to myocardial tissue, ischemia occurs, causing temporary chest pain or discomfort, called angina pectoris. The exact incidence of angina is unknown, although it is considered common, especially in people age 65 years and older; it occurs more often in men.
Overview
There are several types of anginal pain (Box 12-6). Chronic stable angina, classified as classic, exertional angina, occurs at predictable levels of physical or emotional stress and responds promptly to rest or to nitroglycerin. No pain occurs at rest; and the location, duration, intensity, and frequency of chest pain are consistent over time (60 days). New-onset angina describes angina that has developed for the first time within the last 2 weeks and is also considered unstable. Nocturnal angina may awaken a person from sleep with the same sensation experienced during exertion and is usually caused by increased heart rate associated with dreams or in response to underlying CHF.
Postinfarction angina occurs after MI when residual ischemia triggers an episode of angina. Preinfarction angina or unstable angina, also known as progressive angina or crescendo angina, is unpredictable and is characterized by an abrupt change (increase) in the intensity and frequency of symptoms or decreased threshold of stimulus. This angina lasts longer than 15 minutes and is a symptom of worsening cardiac ischemia.
Prinzmetal’s, vasospastic, or variant angina produces symptoms similar to those of typical angina, but it is caused by coronary artery spasm. These spasms periodically squeeze arteries shut and keep the blood from reaching the heart. In this type of angina, coronary arteries are usually clear of plaque or free of physiologic changes that cause obstruction of the vessels. The pattern of Prinzmetal’s angina is characterized by early morning occurrence, frequently at the same time each day, and it occurs at rest (i.e., it is unrelated to exertion).
Prinzmetal’s angina is more common in women younger than 50 years; it is often associated with various types of arrhythmias or conduction defects. It is not a benign condition but is less likely to lead to a heart attack than angina caused by atherosclerosis because most heart attacks are caused by the rupture of an atherosclerotic plaque.
Decubitus or resting angina is considered atypical; it occurs most often when at rest and frequently occurs at the same time every day. This type of anginal chest pain is atypical in that it is paroxysmal in nature, not brought on by exercise, and not relieved by rest, but it is reduced when the person sits or stands up.
It is more prevalent among women, particularly those who have undergone hysterectomy. Microvascular angina associated with insulin resistance syndrome affects the microcirculatory system, a network of tiny blood vessels that branch from the large coronary vessels and that provide oxygen to each of the millions of myocardial cells. Why these vessels spasm and cause decreased blood flow remains undetermined; the cause may be a decrease in estrogen during menopause or a specific trigger from within the heart. Long-term survival rates are not reduced in women with this syndrome.
Etiologic and Risk Factors
Any condition that alters the blood (oxygen) supply or demand of the myocardium can cause ischemia (Table 12-7). Increased oxygen needs of the heart, increased cardiac output, or reduced blood flow to the heart can cause angina. CAD accounts for 90% of all cases of angina, although other conditions affecting normal vessels can also cause angina. Disorders of circulation, such as relative hypotension secondary to spinal anesthesia, antihypertensive drugs, or blood loss, can also result in decreased blood return to the heart and subsequent ischemic pain.
Table 12-7
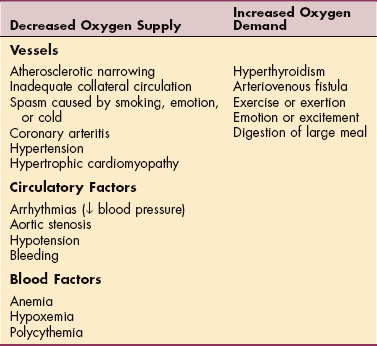
From Goodman CC, Snyder TE: Differential diagnosis in physical therapy, ed 3, Philadelphia, 2000, Saunders.
Onset of angina may be triggered by physical exertion or exercise, especially involving thoracic or upper extremity muscles or walking rapidly uphill; increase in pulse rate or blood pressure (e.g., psychologic or emotional stress); or vasoconstriction. The threshold for angina is often lower in the morning or after strong emotion; the latter can provoke attacks in the absence of exertion. Angina may also occur less commonly during sexual activity, at rest, or at night during sleep.
Pathogenesis
Angina is a symptom of ischemia usually brought on by an imbalance between cardiac workload and oxygen supply to myocardial tissue usually secondary to CAD (see previous discussion on pathogenesis of atherosclerosis). Disruption of a formed plaque with sudden total or near-total arterial occlusion may bring on unstable angina. Rupture leads to the activation, adhesion, and aggregation of platelets and the activation of the clotting cascade, resulting in the formation of an occlusive thrombus. If this process leads to complete occlusion of the artery, then MI occurs. If the process leads to severe stenosis but the artery remains open, then unstable angina occurs.
Metabolites within the ischemic segment of the myocardium (e.g., histamines, bradykinin, prostaglandins) and buildup of lactic acid or abnormal stretching of the myocardium irritate myocardial fibers, resulting in myocardial pain. Afferent sympathetic fibers of the autonomic nervous system enter the spinal cord from levels C3 to T4 (Fig. 12-6), accounting for the varied locations and radiation patterns of anginal pain. The effects of temporary ischemia are reversible; if blood flow is restored, no permanent damage to or necrosis of the heart muscle occurs.
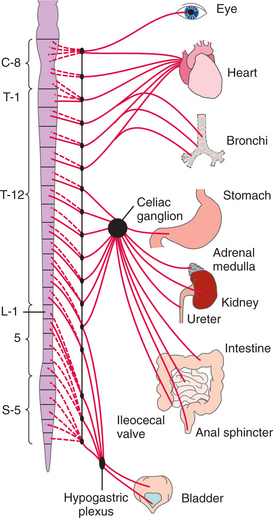
Figure 12-6 Diagram of the autonomic nervous system. The visceral afferent fibers mediating cardiac pain travel with the sympathetic nerves and enter the spinal cord at multiple levels (C3 to T4). This multisegmental innervation results in a variety of pain patterns associated with myocardial ischemia and infarction.
Clinical Manifestations
Angina is characterized by temporary pain or, more often, discomfort that starts suddenly in the chest (substernal or retrosternal) and sometimes radiates to other parts of the body, most commonly to the left shoulder and down the ulnar border of the arm to the fingers. Pain or discomfort may also be referred to any dermatome from C3 to T4, presenting at the back of the neck, lower jaw, teeth, left upper back, interscapular area, abdomen occasionally, and possibly down the right arm (Fig. 12-7).
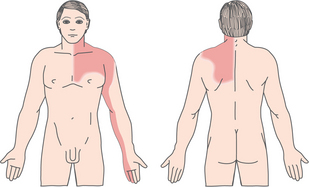
Figure 12-7 Pain patterns associated with angina. Left, Area of substernal discomfort projected to the left shoulder and arm over the distribution of the ulnar nerve. Referred pain may be present only in the left shoulder or in the shoulder and along the arm only to the elbow. Right, Occasionally, anginal pain may be referred to the back in the area of the left scapula or the interscapular region. See Fig. 12-11 for pain pattern associated with myocardial ischemia or infarction experienced by some women (see text for complete description).
The sensation described is often referred to as squeezing, burning, pressing, heartburn, indigestion, or choking. It is usually mild to moderate (rarely reported as severe); it usually lasts 1 to 3 minutes, sometimes 3 to 5 minutes, but can persist up to 15 to 20 minutes. Symptoms are usually relieved by rest or nitroglycerin; in women, symptoms may be relieved by taking an antacid.
Recognizing symptoms of myocardial ischemia in women is more difficult, since the symptoms are less reliable and do not follow the classic pattern described. Many women describe the pain in ways consistent with unstable angina, suggesting that they first become aware of their chest discomfort or have it diagnosed only after it reaches more advanced stages. Some experience a sensation similar to that of inhaling cold air, rather than the more typical shortness of breath. Other women note only weakness and lethargy, and some have observed isolated pain in the midthoracic spine or throbbing and aching in the right biceps muscle.
MEDICAL MANAGEMENT
The diagnosis of angina pectoris is strongly suspected by history and is supported if sublingual nitroglycerin shortens an attack and if prophylactic nitrates permit greater exertion or prevent angina entirely. Medical evaluation includes examination for signs of diseases that may produce angina or contribute to or accompany atherosclerotic disease (see the previous section on Clinical Manifestations).
Early and accurate triage to assess risk (low, intermediate, high) can help identify those people for whom medical therapy will probably fail and lead to better outcomes through a more appropriate management strategy. ECG is normal in about 25% to 30% of people with angina, so the exercise tolerance test is a more useful noninvasive procedure for evaluating the ischemic response to exercise in the client with angina. Diagnostic testing continues as for CAD (see the previous section on Atherosclerosis: Diagnosis and the section on Myocardial Infarction: Diagnosis later in the chapter).
PREVENTION AND TREATMENT.
Prevention of attacks is the first step after the acute attack subsides. Treatment of underlying disorders such as hypertension is essential. The client is also encouraged to avoid situations and stressors that precipitate angina. This usually requires modifying all possible risk factors through changes in lifestyle and modifications of lifelong habits.
Short-acting sublingual nitroglycerin is the drug of choice for the acute attack, usually relieving symptoms within 1 to 2 minutes. Nitroglycerin oral spray is also available in a metered delivery system, which is especially useful for anyone having difficulty handling or swallowing pills. The spray is also easy to use in the dark and is more rapidly acting. Long-acting nitrates (e.g., oral sustained-release nitroglycerin, transdermal nitroglycerin patches, nitroglycerin ointment) are especially useful for people for whom sudden drop in blood pressure associated with taking nitroglycerin is not desirable (i.e., people with hypotension).
Pharmacologic therapy may include other vasodilators, such as β-blockers (i.e., β-adrenergic receptor blockers) and calcium channel blockers (see Table 12-5). Intravascular thrombosis is a key element in the pathophysiology of unstable angina and its progression to MI. Anticoagulation therapy using aspirin and/or heparin is an important part of treatment for unstable angina.
Anticoagulants, such as aspirin and heparin, prevent clot formation, whereas antithrombotic agents (thrombolytics), such as urokinase and streptokinase, break down clots already formed. Aspirin blocks platelet cyclooxygenase, preventing the formation of thromboxane A2, thereby inhibiting platelet aggregation. Heparin binds to an enzyme inhibitor, antithrombin III, enabling it to inactivate clotting factors such as thrombin or factor X.
Second-line alternatives to aspirin (sometimes referred to as “clot busters” or “super aspirins”; e.g., ticlopidine, clopidogrel) are more effective than aspirin in preventing platelet aggregation and thereby reducing the combined risk of ischemic stroke, MI, or death from vascular disease and may be useful in preventing coronary stent thrombosis.
Revascularization procedures are recommended for persons who do not become ischemia free on medical therapy, especially clients with progressive unstable angina. Surgical intervention, such as PTCA, has been shown to relieve angina, but it does not halt the progress of atherosclerosis. CABG can diminish the probability that ischemia will lead to necrosis and lethal infarction.
For people who are not good candidates for any of the proven procedures or whose angina persists despite angioplasty or bypass surgery, transmyocardial revascularization (TMR) may be recommended. In TMR, a computer-controlled laser drills tiny channels through the wall of the left ventricle while the chamber is filled with oxygenated blood. In theory, this allows blood to flow through the channels to the oxygen-deprived tissue, relieving angina. The openings on the heart’s surface scar over quickly, but it is not known how long the channels stay open on the inside of the heart; long-term results remain unknown.
TMR is still considered experimental and may not be available in all centers, but studies consistently report success in relieving severe angina that has been refractory to medical and surgical intervention.169 This procedure is performed through a 4-inch incision between the ribs and does not require a bypass machine; efforts to develop noninvasive techniques for TMR using fiberoptic catheters are under investigation.
PROGNOSIS.
Myocardial ischemia leaves the heart vulnerable to arrhythmias and MI, which can be fatal. About one third of all people who experience angina pectoris die suddenly from MI or arrhythmias. Prognosis depends primarily on left ventricular function (i.e., ejection fraction) but is influenced by type of angina, ability to prevent angina, and severity of underlying disease, such as hypertension or atherosclerosis.
Hypertensive Cardiovascular Disease
Hypertensive cardiovascular disease includes hypertensive vascular disease and hypertensive heart disease. Other conditions affecting the heart caused by an underlying pulmonary pathologic condition (e.g., pulmonary hypertension, pulmonary heart disease) are discussed in Chapter 15.
Hypertension (Hypertensive Vascular Disease)
Definition and Overview.: Blood pressure is the force exerted against the walls of the arteries and arterioles; diastolic pressure (bottom number) is the pressure in these vessels when the heart is relaxed between beats, and systolic pressure (top number) is the pressure exerted in the arteries when the heart contracts. Between ages 55 and 60 years, diastolic blood pressure often begins to plateau and may even decline, whereas systolic blood pressure often starts to rise.
Hypertension, or high blood pressure, is defined by the World Health Organization (WHO) as a persistent elevation of diastolic blood pressure (higher than 90 mm Hg), systolic blood pressure (higher than 140 mm Hg), or both measured on at least two separate occasions at least 2 weeks apart (i.e., sustained elevation of blood pressure). Recent evidence supports a systolic blood pressure threshold of 140 mm Hg for even “low-risk” individuals. In high-risk persons, there is evidence for lower thresholds.358
Based on epidemiologic data from the Framingham Heart Study, the development of hypertension is neither inevitable nor beneficial; both systolic pressure and diastolic pressure are important determinants of cardiovascular sequelae.
Hypertension can be classified according to type (systolic or diastolic), cause, and degree of severity. Hypertension can also be classified based on risk according to the most recent guidelines (Table 12-8).75
Table 12-8
Classification of Blood Pressure for Adults
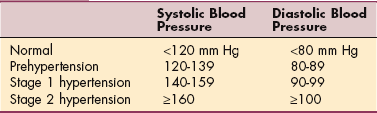
The relationship between blood pressure (BP) and risk of cardiovascular disease (CVD) events is continuous, consistent, and independent of other risk factors. The higher the BP, the greater the chance of heart attack, heart failure, stroke, and kidney disease.
For individuals 40-70 yr of age, each 20 mm Hg incremental increase in systolic BP or 10 mm Hg in diastolic BP doubles the risk of CVD across the entire BP range from 115/75 to 185/115 mm Hg.
From The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. NIH publication no. 03-5233, Bethesda, MD, May 2003, National Heart, Lung, and Blood Institute. Available on-line at www.nhlbi.nih.gov. Accessed April 21, 2008.
Primary (or essential) hypertension is also known as idiopathic hypertension and accounts for 90% to 95% of all cases of hypertension. Secondary hypertension accounts for only 5% to 10% of cases and results from an identifiable cause. Intermittent elevation of blood pressure interspersed with normal readings is called labile hypertension or borderline hypertension. Malignant hypertension is a syndrome of markedly elevated blood pressure (diastolic blood pressure of more than 125 mm Hg) with target organ damage (e.g., retinal hemorrhages, papilledema, heart failure, encephalopathy, renal insufficiency). The elevation of systolic blood pressure independently of change in the diastolic blood pressure is now recognized as a medical condition referred to as isolated systolic hypertension.
Incidence.: The incidence of hypertension varies considerably among different groups in the American population, but it is estimated that one in four adult Americans (50 million) have high blood pressure. Hypertension is twice as prevalent and more severe among blacks than whites. This phenomenon has been attributed to heredity, greater environmental stress, and greater salt intake or salt sensitivity (i.e., responsiveness to changes in sodium balance and extracellular fluid and volume status), although the actual cause is not clear; reduced access to health care increases the prevalence of untreated hypertension.
Blood pressure control rates vary in minority populations and are lowest in Mexican Americans and Native Americans.75 Socioeconomic factors and lifestyle may be important barriers to blood pressure control in some minority individuals.
Classification of Blood Pressure for Children and Adolescents
| Normal | <90th percentile; 50th percentile is the midpoint of the normal range |
| Prehypertension | 90th-95th percentile or if blood pressure is greater than 120/80 (even if this figure is <90th percentile) |
| Stage 1 hypertension | 95th-99th percentile + 5 mm Hg |
| Stage 2 hypertension | >99th percentile + 5 mm Hg |
From National Heart, Lung, and Blood Institute: Fourth report on the diagnosis, evaluation, and treatment of high blood pressure in children and adolescents, Pediatrics 114(2):555-576, August 2004.
Hypertension control rates are no longer improving and fell short of the U.S. Healthy People 2000 goal of blood pressure control in 50% of all hypertensive adults. These goals have now been modified for Healthy People 2010 to include the following: (1) reduce the proportion of adults ages 20 years and older with high blood pressure from the current incidence (28%) to 16% and (2) increase the proportion of adults ages 18 years and older with high blood pressure whose blood pressure is under control from current rates of 18% to a target rate of 50%.146
Etiologic and Risk Factors.: Primary (essential) hypertension has no established etiology but is probably related to genetics and other risk factors, such as smoking, obesity, high cholesterol levels, and being of black descent. In the recent past, hypertension research shifted strongly in the direction of molecular genetics.
A familial association with hypertension has been documented, possibly attributable to common genetic background, shared environment, or lifestyle habits. Using the candidate gene approach, allelic variants in the genes for angiotensinogen, β2-adrenergic receptor, mutation in the β subunit of the epithelial sodium channel, and several others have been identified, but the mecha- nisms by which these contribute to hypertension have not been identified.210
Small arteries branching from the aorta, called arterioles, regulate blood pressure. Any condition that can narrow the opening of these arterioles can increase the blood pressure in the arteries. A variety of specific diseases or problems, such as chronic renal failure, renal artery stenosis, or endocrine disease, can cause secondary hypertension (Box 12-7). The risk for cardiovascular disease in adults with hypertension is determined not only by the level of blood pressure but also by the presence or absence of target organ damage or factors such as smoking, dyslipidemia, and diabetes. Isolated systolic hypertension has very distinct causes, often not directly vascular and often related to a specific organ or tissue, such as aortic diseases, heart malformations, or thyrotoxic crisis.
Risk factors for hypertension may be modifiable or nonmodifiable (Box 12-8). The risk of hypertension increases with age as arteries lose elasticity and become less able to relax. Hypertension occurs slightly more often in men than in women and at an earlier age, but after age 50 years, hypertension begins to develop in more women than men. In all groups the incidence of hypertension increases with age, with a poorer prognosis for people whose hypertension begins at a young age.
White coat hypertension increases the risk of heart disease, because rise in blood pressure occurs in other anxiety-provoking situations as well. Personality traits such as hopelessness and hostility are important factors in cardiovascular disease, including hypertension; research is under way to identify the neuroendocrine and CNS mechanisms underlying these associations and to identify other possible risk-associated personality traits.103 Hypertension itself represents a significant risk factor for the development of CAD, stroke, CHF, and renal failure, preceding heart failure in 90% of all cases and increasing in all other associated conditions.
The influence of nonsteroidal antiinflammatory drugs (NSAIDs) on blood pressure in normotensive and hypertensive persons remains in question. At the very least it has been determined that there is always the potential for NSAIDs to interact with antihypertensive agents, most notably diuretics, β-receptor antagonists, and ACE inhibitors.
Given the high prevalence of NSAID use by older adults, especially for conditions such as arthritis, gout, and similar problems, the association between this drug use and blood pressure must be observed carefully (see Special Implications for the Therapist: Hypertension, section on Medications). Alcohol has been estimated to be responsible for as many as 10% of all cases of hypertension and may be the actual unknown cause of “essential” hypertension.115
Blood pressure is linked to salt intake and modulated by the “salt gene” (angiotensinogen) in some people. Those who are salt sensitive (including those who do not yet have high blood pressure) may have an increased risk of death. Salt sensitivity is a measure of how blood pressure responds to sodium and is independent of other risk factors (including elevated blood pressure) for death from cardiovascular disease.
Inadequate sleep has been identified as a risk factor for hypertension among adults in their fourth to sixth decades who sleep less than 5 hours each night. Short sleep duration is also a risk factor for obesity and diabetes, two conditions commonly linked with hypertension. Men are more likely than women to report getting fewer than 6 hours of sleep, although women are more likely to have trouble falling asleep or getting back to sleep after waking up early.102,119
Pathogenesis.: Blood pressure is regulated by two factors: blood flow and peripheral vascular resistance. Blood flow is determined by cardiac output (strength, rate, rhythm of heartbeat; blood volume). The resistance to flow is primarily determined by the diameter of blood vessels and, to a lesser degree, by the viscosity of blood.
Increased peripheral resistance as a result of the narrowing of the arterioles is the single most common characteristic of hypertension. Constriction of the peripheral arterioles may be controlled by two mechanisms, each with several components: (1) sympathetic nervous system activity (autonomic regulation) and (2) activation of the renin-angiotensin system.
In the case of the sympathetic nervous system, norepinephrine is released in response to psychogenic stress or baroreceptor activity. The blood vessels constrict, which increases peripheral resistance. At the same time, epinephrine is secreted by the adrenal medulla, resulting in increased force of cardiac contraction, increased cardiac output, and vasoconstriction.
With prolonged hypertension, the elastic tissue in the arterioles is replaced by fibrous collagen tissue. The thickened arteriole wall becomes less distensible, offering even greater resistance to the flow of blood. This process leads to decreased tissue perfusion, especially in the target organs of high blood pressure (i.e., heart, kidneys, brain). Atherosclerosis is also accelerated in persons with high blood pressure.
Within the renin-angiotensin system, vasoconstriction results in decreased blood flow to the kidney. Whenever blood flow to the kidney diminishes, renin is secreted and angiotensin is formed, causing vasoconstriction within the renal system and increased total peripheral resistance. Angiotensin also stimulates the secretion of aldosterone, which promotes sodium and water retention by the kidney tubules, causing an increase in intravascular volume. All these factors increase blood pressure.
Evidence from animal, clinical, and epidemiologic studies points to an association between high blood pressure and abnormal calcium metabolism, leading to increased calcium loss, secondary activation of the parathyroid gland, increased movement of calcium from bone, and increased risk of urinary tract stones and osteoporosis.62
Clinical Manifestations.: Hypertension is frequently asymptomatic; this creates a significant health care risk for affected people. When symptoms do occur, they may include headache (usually occipital and present in the morning, worse on waking, and slowly improving with activity), vertigo, flushed face, spontaneous epistaxis, blurred vision, and nocturnal urinary frequency. Elevated blood pressure when measured, especially in the early stages, may be the only sign of hypertension.
Sleep-disordered breathing is also associated with systemic hypertension in middle-aged and older individuals of both genders and different ethnic backgrounds.242 Progressive hypertension may be characterized by cardiovascular symptoms (dyspnea, orthopnea, chest pain, and leg edema) or cerebral symptoms (nausea, vomiting, drowsiness, confusion, and fleeting numbness or tingling in the limbs). Hypertensive encephalopathy, a neurologic syndrome that occurs as a result of a sudden sustained rise in blood pressure, may be accompanied by nonspecific neurologic symptoms, such as confusion, headache, nausea, and even coma. It is also well recognized that end-stage renal disease (ESRD) is associated with accelerated and malignant hypertension; hypertension is associated with increased urinary calcium excretion and subsequent bone loss and osteoporosis, especially at the femoral neck.38
MEDICAL MANAGEMENT
The American Society of Hypertension recommends that everyone, regardless of age, know his or her blood pressure (the actual numbers). An annual blood pressure check is important for everyone; more frequent blood pressure measurements should be taken in anyone with risk factors or known hypertension. Elevated blood pressure in a younger adult (less than 50 years) can cause long-term accumulated damage, irreversible by age 50 or 60 years; therefore, any elevation in blood pressure at any age must be addressed.
The most important prevention factor is physical activity and exercise; other key variables include weight control, limitations on salt and alcohol intake, and modification of other risk factors present (see Box 12-8). Combining a low-sodium diet with the DASH (Dietary Approaches to Stop Hypertension) diet (high intake of fruits, vegetables, and low-fat dairy foods) helps reduce blood pressure more than the DASH diet alone, both for healthy people and for those with high blood pressure. Reducing salt intake also lowers the risk of osteoporosis and possible fracture, since a high salt intake increases urinary calcium excretion and hypertension has been found to be associated with bone loss.
DIAGNOSIS.
In the past, hypertension was diagnosed primarily on the basis of the diastolic measurement, which was considered a better representation of the overall condition of the circulatory system. The rise of systolic pressure with age was considered to be normal and therefore not a risk factor. Today, it is recognized that although diastolic hypertension (higher than 90 mm Hg) is common and usually controllable, systolic hypertension (higher than 140 mm Hg) is the most common in older adults and the most powerful risk factor for stroke and is strongly linked with heart attack, heart failure, and kidney failure even when the diastolic blood pressure is within normal limits. Systolic pressure measures the maximal strain on the heart and blood vessels and is a more precise measure of future damage to the system.
Blood pressure varies over the course of any single day depending on exertion, emotional state, ingestion of food, medications, and the presence of risk factors described previously. Thus it is important that blood pressure be measured at several different times and under consistent circumstances before a diagnosis of hypertension is made. Twenty-four–hour blood pressure monitoring using a portable device that automatically takes blood pressure readings at regular intervals is available and especially helpful in mapping out labile hypertension.
The individual maintains a log of activities and emotions corresponding to the times when readings are taken; this information is compared with the computer-generated map of blood pressures generated from the data collected by the measurement device. No other tests are specific for essential hypertension.
Studies used in the routine evaluation of hypertension may include a complete blood count (CBC); urinalysis; serum potassium, cholesterol, and creatinine assays; fasting blood glucose level; ECG; and chest radiography. Other more specific tests may be needed for secondary hypertension, and more complete cardiac assessment may be required for selected individuals.
TREATMENT.
Once diagnosed, hypertension requires ongoing management (see Table 12-6) despite the absence of symptoms. According to the Joint National Committee,26 the goal is to achieve and maintain the lowest safe arterial blood pressure (without side effects); the intended target goal is to reduce blood pressure to less than 135/85 mm Hg or 130/80 for people with diabetes or kidney disease.26
The decision to treat and the method and intensity of intervention are based on the concept of total risk, not just blood pressure measurements. This approach takes into account cardiovascular risk factors in people with hypertension (see Box 12-8) and the presence of target organ damage or clinical cardiovascular disease (e.g., prior coronary revascularization, MI, stroke, PAD, retinopathy).
The WHO has published guidelines for the management of hypertension that review the management of risk factors in detail and prognosis based on risk stratification.358 In addition, a comprehensive list of recommendations on the treatment of hypertension in the prevention and management of ischemic heart disease is available from the American Heart Association.287
Management of hypertension may begin with a “stepped care” approach including smoking cessation and other nonpharmacologic interventions through lifestyle modification as initial therapy for primary hypertension (including those with blood pressure on the high side of normal or a family history of hypertension). This approach has been shown effective in lowering blood pressure and can reduce other cardiovascular risk factors.
Even when lifestyle modifications alone are not adequate in controlling hypertension, they may reduce the dosage of medication needed to manage the condition.75 This program may include weight reduction; smoking cessation; a regular program of aerobic exercise; moderation of alcohol, dietary fat, caffeine, and dietary sodium; administration of nutritional supplements (e.g., potassium, calcium, magnesium); and behavioral cognitive therapy for those with hypertension associated with certain personality traits. See the previous section on Atherosclerosis: Treatment.
If nonpharmacologic measures fail to produce the desired results or if the blood pressure is very high at the time of diagnosis, blood pressure–lowering medications are prescribed starting with the lowest effective dose (to avoid intolerable side effects) and modifying accordingly. Antihypertensive medications can be classified by mode of action as diuretics, adrenergic blockers, vasodilators, ACE inhibitors, and calcium antagonists (see Table 12-5).
More than 50% of cases of mild hypertension can be controlled with one drug; a combination of medications may be required for others. Diuretics are often the first step in the pharmacologic management of hypertension. Although these drugs decrease plasma volume, potassium depletion and renal complications may require the use of β-blockers, calcium channel blockers, or ACE inhibitors.
Oral renin inhibitors such as aliskiren (Tekturna) are a new class of antihypertensive medication that can be used as a single treatment or in combination with other antihypertensive drugs. Aliskiren blocks the action of renin, a key kidney enzyme that helps regulate blood pressure. The blocking action takes place at the beginning of the renin-angiotensin-aldosterone system by directly inhibiting the renin released from the kidneys, thereby preventing conversion of angiotensinogen to angiotensin I. This is different from most other antihypertensive medications, which take action later in the renin-angiotensin-aldosterone system.
Black people are generally more responsive to calcium antagonists and diuretics than to β-blockers, ACE inhibitors, or the new oral renin inhibitors. Older adults with hypertension are generally equally responsive to all classes of antihypertensive medications, but they have an increased likelihood of side effects. Pharmacologic therapy is individualized, matching the individual’s clinical presentation with medications available.
More aggressive early treatment of people with diabetes and elevated blood pressure is recommended. Hypertensive people who tend to be hostile may be told to take their medication at bedtime to avoid the sharp rises in blood pressure in the early morning hours associated with heart attacks. The use of home monitoring devices is an important part of the management program both to monitor the blood pressure and to evaluate the effect of antihypertensive medication.
Home monitoring can also distinguish between sustained hypertension and white coat hypertension and improves program compliance. In individuals with hypertension, the blood pressure readings taken in a clinic setting tend to be 5 to 10 mm Hg higher than measurements taken at home. Recommended frequency of readings is twice daily (morning and evening) on work and nonwork days for anyone newly diagnosed or in whom antihypertensive medication has recently been initiated or changed. Anyone with stable hypertension can take blood pressure reading several days per week.
Obesity has long been associated with hypertension and is an independent risk factor for cardiovascular disease and CAD as well. Regular exercise enhances weight loss and reduces blood pressure independent of weight loss. (For further discussion see Special Implications for the Therapist: Hypertension, section on exercise.)
Older individuals, blacks, and hypertensive individuals are more sensitive to change in dietary sodium chloride than are other individuals. A reduction of sodium intake alone may be enough to control blood pressure in persons with mild hypertension and may reduce the medication requirements in those who require drug therapy.
It is also recommended that individuals with high blood pressure limit their intake of alcohol to 2 oz of liquor, 10 oz of red wine, or 24 oz of beer per day. Women and lighter-weight men should limit alcohol intake to half of these amounts per day.75
Dietary potassium deficiency may have a role in increasing blood pressure; individuals may also become hypokalemic from increased urinary magnesium excretion during diuretic therapy and require additional potassium. Magnesium and calcium influence vascular tone because magnesium acts to relax blood vessels and calcium assists in blood vessel contraction.
A proper balance of these two substances is essential, since they compete for entry into the cell. When magnesium is low, an abnormally large amount of calcium enters the cells so that blood vessels begin to lose their ability to relax. Progressive vasoconstriction and subsequent spasms result in elevated blood pressure and eventual ischemia. Muscle weakness with depressed tendon reflexes may accompany this condition. A fall in serum potassium level also enhances the effects of digitalis, increasing the risk of digoxin toxicity (see Table 12-5).
PROGNOSIS.
Hypertension is a major risk factor for atherosclerosis, implicating hypertension as a common cause of death in the United States. Among black Americans, hypertension is also the most common fatal familial disease. More than one half of persons with angina pectoris, sudden death, stroke, and thrombotic occlusion of the abdominal aorta or its branches have hypertension.
Three fourths of people with CHF, dissecting aortic aneurysm, intracerebral hemorrhage, or rupture of the myocardial wall also have elevated blood pressure. If it is untreated, nearly 50% of people with hypertension die of heart disease, 33% die of stroke, and 10% to 15% die of renal failure.
When a person with hypertension achieves the target blood pressure, it must be emphasized that blood pressure control does not equal cure. Adherence to treatment and follow-up monitoring must be continued on an ongoing basis. Unfortunately, the cost of antihypertensives, side effects, and lack of symptoms sometimes lead to poor compliance with treatment. Treatment prolongs life, and antihypertensive medications have dramatically reduced the mortality rate associated with hypertension. See also the section on Atherosclerosis: Prognosis (especially regarding pulse pressure as the newest predictor of mortality).
Hypertensive Heart Disease
Definition and Overview.: The term hypertensive heart disease is used when the heart is enlarged as a result of persistently elevated blood pressure (hypertension) (see previous discussion). Left ventricular hypertrophy and diastolic dysfunction are found in 10% to 30% of the adult population with chronic hypertension, and it may present with many of the signs and symptoms of CHF. Both the prevalence and the severity of the disease are greater in blacks than in whites. In all adults, it increases progressively with age.
MEDICAL MANAGEMENT
DIAGNOSIS, TREATMENT, AND PROGNOSIS.
Cardiac enlargement and left ventricular hypertrophy, best viewed with echocardiography, are diagnostic of hypertensive heart disease. Treatment is as for hypertension unless heart failure develops, in which case treatment is as for heart failure (see the sections on each of these conditions for more discussion). The most common cause of death in hypertensive heart disease is CHF, accounting for 40% of all deaths from hypertension.
Myocardial Infarction
MI, also known as a heart attack or referred to as a “coronary,” is the development of ischemia with resultant necrosis of myocardial tissue. Any prolonged obstruction depriving the heart muscle of oxygen can cause an MI. MI occurs in 1½ million persons each year and represents the leading cause of death (500,000 deaths annually) in the adult American population. See the previous section on Ischemic Heart Disease in this chapter.
Etiologic and Risk Factors
Etiologic and risk factors are the same as for all forms of cardiovascular disease, especially angina pectoris associated with CAD (see the previous section on Angina Pectoris). Eighty percent to ninety percent of MIs result from coronary thrombus at the site of a preexisting atherosclerotic stenosis. New cases of MI occur in many people with only a borderline risk profile or even lack of known risk factors, suggesting other unidentified risk factors.
Other causes may include cocaine use (causes vasoconstriction of the coronary arteries), vasculitis, aortic stenosis, or aortic root or coronary artery dissection. Smokers have more than twice as many heart attacks as nonsmokers, and sudden cardiac death occurs two to four times more frequently in smokers. After an infarction, smokers have a poorer chance of recovery than nonsmokers. Exertion-related MI, which may include weakness or shortness of breath while working with the arms extended overhead in habitually inactive people, has also been reported associated with single-vessel rather than triple-vessel disease.126
It is a well-established fact that heart attacks occur more frequently in the early morning hours. This peak incidence is attributed to an increase in catecholamines with the resultant increased blood pressure, increased workload of the heart, as well as increased clotting factors in the early morning. Heart attacks also occur in a seasonal pattern with an increased incidence between Thanksgiving and New Year’s Day across all ages, in both genders, and across geographic regions. Whether this can be attributed to mood changes, weather, circadian rhythms, large quantity of food consumed, or some other mechanism remains unknown.
Upper respiratory tract illnesses have been associated with an increased risk of ischemic heart disease and stroke, especially during the flu season in adults 65 years old and older who have not received a flu shot. Studies show a reduction in the risk of hospitalization and mortality for heart disease as well as cerebrovascular disease, pneumonia, and influenza among elderly adults receiving flu vaccine.240,241
The association between periodontal disease (e.g., gingivitis, periodontitis) and acute MI is under investigation. There is a definite association between common forms of periodontal disease and cardiovascular disease and stroke, but the causal relations have not been identified.265
Researchers have found that bacteria in the mouth spill into the bloodstream and can be found in the walls of major arteries. Recent research showed that intensive periodontal treatment may reverse atherosclerosis by improving elasticity of the arteries, or endothelial function,333 suggesting that periodontal treatment may reduce cardiovascular risk.
Acute respiratory tract infections, such as the common cold, flu, and bronchitis, may also increase the risk of a heart attack’s occurring within 2 weeks of a first heart attack and may account for some cases of MI, although researchers point out that early symptoms of heart attacks may be mistaken for acute upper respiratory tract infection.217
Silent ischemia is highly prevalent among people with diabetes; increased PAI-1 activity has been identified as a risk factor for MI in persons with diabetes as well as for postmenopausal women not receiving hormone replacement therapy. PAI-1 is a naturally occurring substance that inhibits another natural substance, t-PA; t-PA is an enzyme released endogenously as part of the body’s defense against thrombosis; it lyses fibrin and dissolves the forming blood clot (thrombus). The effect of PAI-1 on t-PA is to prevent clot destruction in the bloodstream.
Research now shows that diabetic clients have higher PAI-1 activity than nondiabetic clients, both at hospital admission for acute MI and at follow-up 1 year later. Raised PAI-1 activity may predispose diabetic clients to MI and may also impair pharmacologic and spontaneous reperfusion after acute MI, contributing to the poor outcome in this population.324
Pathogenesis
The myocardium receives its blood supply from the two large coronary arteries and their branches (Fig. 12-8; Table 12-9). One or more of these blood vessels may become occluded by a clot that forms suddenly when an atheromatous plaque ruptures through the sublayers of a blood vessel or when the narrow, roughened inner lining of a sclerosed artery becomes completely filled with thrombus. In most cases, infarcts result from an occlusive thrombus superimposed on an atherosclerotic plaque.
Table 12-9
Blood Supply to the Myocardium
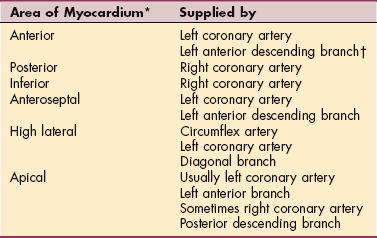
*Most commonly affected arteries and the area of myocardium supplied are listed in order of decreasing frequency of blockage.
†Often referred to as the “widow maker,” untreated blockage of the left anterior descending branch leads to permanent heart damage if the individual does not die first.
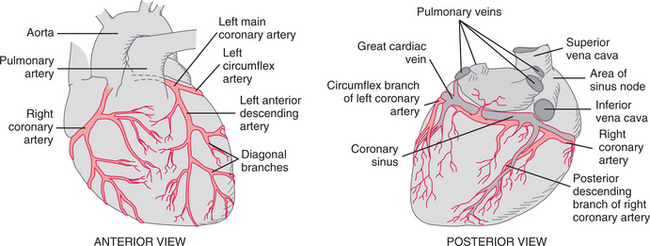
Figure 12-8 Areas of myocardium affected by arterial insufficiency of specific coronary arteries. The right and left coronary arteries branch off the aorta just above the aortic valve and normally supply the myocardium with oxygenated blood. The most commonly affected arteries and the area of myocardium supplied are listed in Table 12-9.
Researchers have found that plaque most likely to rupture (vulnerable plaque) is comprised of the soft form of cholesterol (cholesteryl ester) and is vulnerable to mechanical forces such as occur with the increase in hormones early in the morning or even the vibration of the heartbeat.
Rupturing plaque does not always result in an MI. It is likely that plaque breaks off frequently without triggering a heart attack, and the large plaques visible on angiograms are often the healed-over and more stable plaques. Although these plaques occlude the coronary vessels, resulting in obstruction, ischemia, and angina, they are not as likely to cause rupture and sudden death as happens with the soft, smaller, and usually undetected plaques.
The most common site involved is the left ventricle, the chamber of the heart with the greatest workload. Thrombosis of the anterior descending branch of the left coronary artery is the most common cause of infarction and affects the anterior left ventricle (Fig. 12-9).
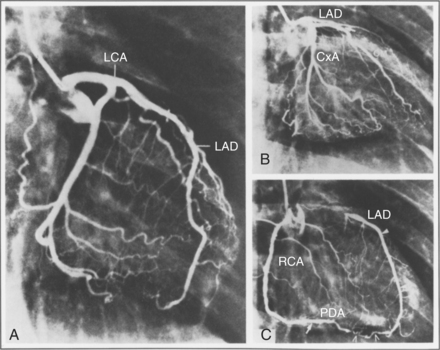
Figure 12-9 A, Angiogram of a normal left coronary artery (LCA). B, Angiogram of a totally obstructed left anterior descending (LAD) coronary artery. C, Angiogram of the right coronary artery (RCA) and its major branch, the posterior descending artery (PDA) (same heart as in B). The LAD is seen because of collateral vessels connecting the LAD and the RCA system. (From Boucek R, Morales A, Romanelli R, et al: Coronary artery disease: pathologic and clinical assessment, Baltimore, 1984, Williams & Wilkins, pp 4, 9.) Williams & Wilkins
Occlusion of the left circumflex artery produces anterolateral or posterolateral infarction. Right coronary artery thrombosis leads to infarction of the posteroinferior portion of the left ventricle and may involve the right ventricular myocardium and interventricular septum. The arteries supplying the atrioventricular node and the sinus node more commonly arise from the right coronary artery; thus atrioventricular block at the nodal level and sinus node dysfunction occur more frequently during inferior infarctions.
Myocardial ischemia/reperfusion injury is accompanied by an inflammatory response involving three major components: (1) molecular oxygen, (2) cellular blood elements (especially neutrophils), and (3) activated complement system. When the myocardium has been completely deprived of oxygen, cells die and the tissue becomes necrotic in an area called the zone of infarction (Fig. 12-10; see also Figs. 6-5 and 6-6). In response to this necrosis, leukocytes aid in removing the dead cells, and fibroblasts form a connective tissue scar within the area of infarction. The remaining heart muscle cells enlarge to compensate for the loss in heart pump function (see also the section on Cell Injury in Chapter 6; a complete discussion of the role of oxidative stress and complement activation in heart disease is available71,99). Usually the formation of fibrous scar tissue is complete within 6 to 8 weeks (Table 12-10; see Fig. 6-6).
Table 12-10
Tissue Changes After Myocardial Infarction (MI)
| Time after MI | Tissue Changes |
| 6-12 hr | No gross changes; healing process has not begun |
| 18-24 hr | Inflammatory response; intercellular enzyme release |
| 2-4 days | Visible necrosis; proteolytic enzymes remove debris; catecholamines, lipolysis, and glycogenolysis elevate plasma glucose and increase free fatty acids to assist depleted myocardium recovery from anaerobic state |
| 4-10 days | Debris cleared; collagen matrix laid down |
| 10-14 days | Weak, fibrotic scar tissue with beginning revascularization; area vulnerable to stress |
| 6 wk | Scarring usually complete; tough, inelastic scar replaces necrotic myocardium; unable to contract and relax like healthy myocardial tissue |
Modified from McCance KL, Huether SE: Pathophysiology: the biologic basis for disease in adults and children, ed 5, St Louis, 2006, Mosby.
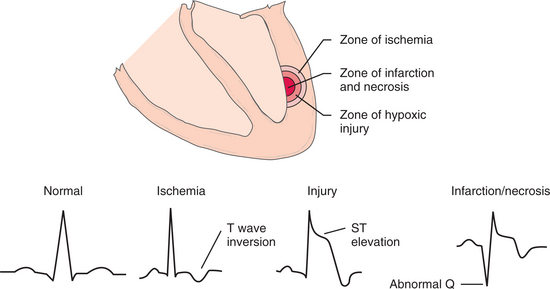
Figure 12-10 Electrocardiographic (ECG) alterations associated with the three zones of myocardial infarction (MI).
Immediately surrounding the area of infarction is a less seriously damaged area of injury called the zone of hypoxic injury. This zone is able to return to normal, but it may also become necrotic if blood flow is not restored. With adequate collateral circulation, this area may regain its function within 2 to 3 weeks. Adjacent to the zone of hypoxic injury is another reversible zone called the zone of ischemia. Ischemic and injured myocardial tissues cause characteristic ECG changes; as the myocardium heals, the ST segment and T waves gradually return to normal, but abnormal Q waves may persist.
Oxygen deprivation is accompanied by electrolyte disturbances, particularly cellular loss of potassium, calcium, and magnesium. Myocardial cells deprived of necessary oxygen and nutrients lose contractility, thereby diminishing the pumping ability of the heart. Normally the myocardium takes up varying quantities of catecholamines (epinephrine, norepinephrine), which are released when significant arterial occlusion occurs. Released catecholamines predispose the individual to serious imbalances of sympathetic and parasympathetic function, irregular heartbeats (arrhythmia), and heart failure.
Clinical Manifestations
The most notable symptom of MI is a sudden sensation of pressure, often described as prolonged crushing chest pain, occasionally radiating to the arms, throat, neck (as high as the occipital area), and back (Fig. 12-11). The pain is constant, lasting 30 minutes up to hours, and may be accompanied by pallor, shortness of breath, and profuse perspiration. Catecholamine release resulting in sympathetic stimulation may produce diaphoresis and peripheral vasoconstriction that cause the skin to become cool and clammy. Angina pectoris pain can be similar, but it is less severe, does not last for hours, and is relieved by cessation of activity, rest, or nitrates.
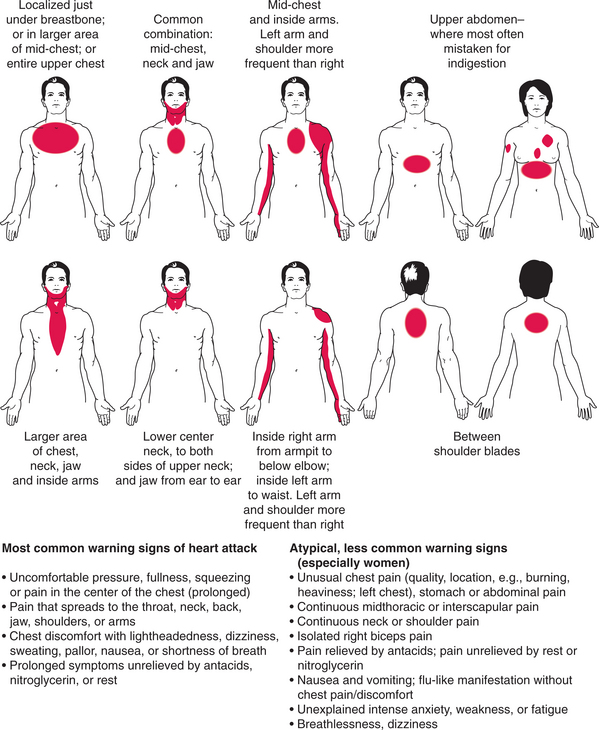
Figure 12-11 Early warning signs of a heart attack. Multiple segmental nerve innervation shown in Fig. 12-6 accounts for the varied pain patterns possible. A woman can experience any of the various patterns described but is more likely to develop atypical symptoms of pain as depicted here. (Modified from Goodman CC, Snyder TE: Differential diagnosis for physical therapists: screening for referral, ed 4, Philadelphia, 2007, Saunders.)
Symptoms do not always follow the classic pattern, especially in women. Two major symptoms in women are shortness of breath, sometimes occurring in the middle of the night, and chronic, unexplained fatigue. Atypical presentation may include continuous pain in the midthoracic spine or interscapular area, neck and shoulder pain, stomach or abdominal pain, nausea, unexplained anxiety, or heartburn that is not altered by antacids.
Silent attacks (painless infarction without acute symptoms) are more common among nonwhites, older adults (more than 75 years), all smokers, and adults (men and women) with diabetes, presumably because of reduced sensitivity to pain. Nausea and vomiting may occur because of reflex stimulation of vomiting centers by pain fibers. Fever may develop in the first 24 hours and persist for a week because of inflammatory activity within the myocardium.
Postinfarction complications include arrhythmias, CHF, cardiogenic shock, pericarditis, rupture of the heart, thromboembolism, recurrent infarction, and sudden death. Arrhythmias, affecting more than 90% of individuals, are the most common complication of acute MI and are caused by ischemia, hypoxia, autonomic nervous system imbalances, lactic acidosis, electrolyte imbalances, drug toxicity, or alterations of impulse conduction pathways or conduction defects.