Infectious Disease
Although human beings are continually exposed to a vast array of microorganisms in the environment, only a small proportion of those microbes are capable of interacting with the human host in such a way that infection and disease result. With the steady advances being made in medicine, people are living longer, but infection is still a frequent cause of hospital admission and remains an important cause of death, especially in the aging population.
From 1950 until 1980 the management of communicable infectious diseases was well under control; morbidity and mortality from infectious diseases such as yellow fever, cholera, typhus, malaria, typhoid fever, and plague were no longer serious threats in the United States.
The widespread availability and use of sulfa drugs and antibiotics successfully treated tuberculosis, syphilis, gonorrhea, bacterial meningitis, scarlet fever, rheumatic fever, and nosocomial (hospital-or nursing home–acquired) infections. Organized efforts to immunize all children lowered the incidence of vaccine-preventable diseases such as measles, mumps, rubella, diphtheria, tetanus, and poliomyelitis; more recently children have also been vaccinated against chickenpox (varicella) and hepatitis.
Unfortunately, this period of reduced morbidity and mortality secondary to infectious disease did not last, and in the 1970s and 1980s new infectious agents appeared. Legionella, human immunodeficiency virus (HIV), antibiotic-resistant organisms, Avian flu, and a resurgence of tuberculosis are examples of infectious processes that have returned focus to the prevention and treatment of infectious diseases. Infectious diseases are spreading more rapidly throughout the world than in the past, facilitated by a combination of environmental disruption and increasing human mobility.
At the same time, infectious agents are suspected in the predisposition of chronic disorders such as heart disease, mental illness, and autoimmune diseases.31,85,148 In addition, an area of major public health concern is the continued emergence of antibiotic-resistant microorganisms that appear in hospitals and communities. The presence of these multidrug-resistant organisms in health care facilities limits the number of effective antimicrobials available for treatment.99
The most common of these resistant bacteria are methicillin-resistant Staphylococcus aureus (MRSA); vancomycin-resistant enterococci (VRE), and multidrug–resistant Mycobacterium tuberculosis. Additionally, a strain of S. aureus is developing a resistance to vancomycin, which will make treatment of this organism extremely difficult.
Multidrug resistance in Pseudomonas aeruginosa is increasing, and carbapenem-resistant Klebsiella strains are emerging. Recent increases in the frequency and severity of Clostridium difficile–associated illness are associated with the emergence of a hypervirulent C. difficile strain with increased resistance to the fluoroquinolones.99
The cause of antibiotic resistance is primarily associated with the misuse and overuse of antibiotics in treatment of infections or potential infections. Other variables include large numbers of children in daycare facilities; a sicker population base when hospitalized (therefore more susceptible to infection); and modern agriculture’s reliance on antibiotics to boost growth and limit disease among cattle, chickens, and other animals, leading to the spread of more dangerous microbes. The resistant organisms spread quickly and easily when inadequate precautions are taken to prevent transmission (e.g., poor use of handwashing and contact precautions).1
Although a number of new infectious diseases have appeared in recent years, a worldwide resurgence of longstanding diseases once thought to be well controlled has occurred. Among infectious diseases in the world, M. tuberculosis is the second leading cause of death in adults, killing 2 million people a year. Organisms travel on the shoes of tourists, in the ballast of cargo ships, within the confines of jetliners, and in the blood of human beings.
When natural systems are weakened or altered by ecologic stresses (e.g., pollution, habitat destruction, weather disasters, climate change, famine), they become more vulnerable to damage or destruction by invading organisms, which can result in the spread of infection. Opportunistic organisms take advantage of the weakened defenses.
All health care professionals must maintain a vigilant attitude to preventing infectious disease. This requires an understanding of the infectious process, the chain of transmission, and selected aspects of control. In this chapter, a basic understanding of these concepts is provided along with a discussion of a few infectious diseases. Other pertinent infectious diseases are presented in appropriate chapters according to the primary clinical pathology (such as pneumonia in Chapter 15, bacterial meningitis in Chapter 29, and Sjögren’s syndrome in Chapter 27).
SIGNS AND SYMPTOMS OF INFECTIOUS DISEASES
Clinical manifestations of infectious disease are many and varied depending on the etiologic agent (e.g., viruses, bacteria) (see the section on Types of Organisms in this chapter) and the system affected (e.g., respiratory, central nervous system [CNS], gastrointestinal [GI], genitourinary).
Systemic symptoms of infectious disease can include fever and chills, sweating, malaise, and nausea and vomiting. Changes in blood composition may occur, such as an increased number of leukocytes or a change in the types of leukocytes. Older adults may experience a change in mentation (e.g., confusion, memory loss, difficulty concentrating). When observing any person for early signs of infection, the therapist will most likely see one or only a few symptoms (Box 8-1).
A change in body temperature is a characteristic systemic symptom of infectious disease, but fever may accompany noninfectious causes such as inflammatory, neoplastic, and immunologically mediated diseases (Box 8-2). Fever, a sustained temperature above normal, can be caused by abnormalities of the hypothalamus, brain tumors, dehydration, or toxic substances affecting the temperature-regulating center of the hypothalamus. Certain protein substances and toxins can cause the set point of the hypothalamic thermostat to rise. This results in activation of the hypothalamus to conserve heat and increase heat production. Substances that cause these effects are called pyrogens.
In infectious disease the endotoxins of some bacteria and the extracts of normal leukocytes (cytokines) are pyrogenic. They act to raise the thermostat in the hypothalamus, thus raising the body temperature. Fever patterns may differ depending on the specific infectious disease present and occur clinically on a continuum from fever associated with an acute illness lasting 7 to 10 days, to sepsis and ongoing infection lasting longer than 10 days, to fever of unknown origin associated with a possible infectious origin lasting at least 3 weeks.
Other causes of fever of unknown origin include neoplasm (lymphoma and leukemia are the most common); autoimmune disorders such as Still’s disease, systemic lupus erythematosus, and polyarteritis nodosa; and miscellaneous diseases, including temporal arteritis, sarcoidosis, alcoholic hepatitis, and drug-induced fever, among others.75
A general rule, the 102° F rule, divides conditions into two groups: those that do not cause temperature elevations exceeding 102° F (39° C) and those that regularly exceed 102° F. Table 8-1 reflects hospital data; the outpatient population is more likely to experience fever accompanied by generalized arthralgias and myalgias associated with a self-limiting illness or fever with localized symptom(s), such as a sore throat, cough, or right lower quadrant pain, as occurs with bacterial infection. Temperature elevation to 104° F (40° C) may cause delirium and seizures, particularly in children. An extremely high fever may damage cells irreversibly.
Table 8-1
Most Common Causes of Prolonged Fever*
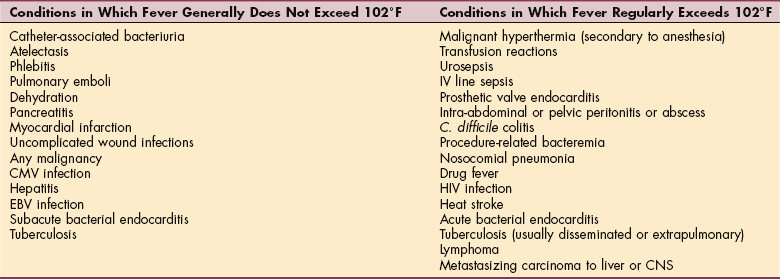
*The evaluation of fever magnitude with the 102° F rule is most often done in the acute care setting. This is a general guideline that must be taken into consideration with other presenting factors.
It is important to note that some people with serious infection do not initially develop fever but instead become tachypneic, confused, or develop hypotension. Most often this situation occurs in older adults, hospitalized individuals with a nosocomial infection, or in immunocompromised persons.
Inflammation and its exudates may remain localized, permeate the tissue, or spread throughout the body via the blood or lymph. Infection can develop, as is the case with an abscess, a localized infection and inflammation with purulent exudate. Leukocytes form a wall around the organisms. The abscess deepens as more leukocytes are drawn into the area, more organisms are killed, and more necrotic tissue is dissolved. The exudate may eventually be autolyzed and resorbed by the body, in which case the inflammation and infection are resolved. Rupture of the abscess and drainage into other tissues can spread the infection to other areas of the body.
For example, infectious abdominal disorders (e.g., diverticulitis, appendicitis), tuberculosis of the spine, pelvic inflammatory disease (PID), vertebral osteomyelitis, septic arthritis of the sacroiliac joint, and tumor of the thigh can result in abscess formation in the space between the posterior peritoneum and the psoas and iliac fascia.49,92 A psoas abscess is usually confined within the psoas fascia, but occasionally, because of anatomic relations, infection extends to the buttock, hip, or upper thigh.
Such an abscess causes true musculoskeletal symptoms of back pain, or pain referred to the hip or knee, and limited range of hip motion from an underlying systemic cause. Flexion contracture of the hip (positive Thomas test) may develop from reflex spasm, and extension of the thigh is very painful; hip abduction and adduction evoke minimal discomfort. An unexplained limp may be the initial symptom, an important clinical clue when taking a history (see Figs. 16-14 and 16-15). Only days to weeks later does lower abdominal pain develop, and the person becomes acutely ill with a high fever.
Rash with fever can result from an infectious process caused by any microbe that has successfully penetrated the stratum corneum (see Fig. 10-1) and multiplied locally. Skin rashes may also occur with infection elsewhere in the body unrelated to local skin disease (e.g., scarlet fever caused by streptococci, also called scarlatina).
The most common types of skin lesions associated with infectious disease are maculopapular eruptions (e.g., classic childhood viral illnesses such as measles, rubella, roseola, fifth disease), nodular lesions (e.g., streptococcus, Pseudomonas), diffuse erythema (e.g., scarlet fever, toxic shock syndrome), vesiculobullous eruptions (e.g., varicella, herpes zoster), and petechial purpuric eruptions (e.g., Epstein-Barr virus [EBV] and cytomegalovirus [CMV]). Specific types of skin lesions are discussed in Chapter 10.
Red streaks radiating from an infection site, known as blood poisoning, in the direction of a regional lymph node may be associated with lymphangitis secondary to an infection such as cellulitis. Lymphangitis, an acute inflammation of the subcutaneous lymphatic channels, usually occurs as a result of hemolytic streptococci or staphylococci (or both) entering the lymphatic channels from an abrasion or local trauma, wound, or infection. The red streak may be obvious, or it may be faint and easily overlooked, especially in dark-skinned people. The nodes most often affected are the submandibular, cervical, inguinal, and axillary nodes, in that order. Involved nodes are usually tender and enlarged (greater than 3 cm).
Inflamed lymph nodes can be associated with other infectious diseases and may be palpated by the therapist, especially in cervical, axillary, or inguinal areas when presenting musculoskeletal symptoms are evident in those areas. For example, intraoral infection may cause an inflamed cervical node leading to spasm of the sterno cleidomastoid muscle, causing neck pain. Palpation may appear to aggravate a primary spasm as if originating in the muscle, when in fact a lymph node under the muscle is the source of the symptom.
In acute infections, nodes are tender asymmetrically, enlarged, and matted together. The overlying skin may be erythematous (red) and warm. Unilaterally warm, tender, enlarged, and fluctuant lymph nodes sometimes associated with elevated body temperature may be caused by pyogenic infections and require medical referral.
Supraclavicular and inguinal nodes are also common metastatic sites for cancer. Nodes involved with metastatic cancer are usually hard and fixed to the underlying tissue. Any suspicious lymph node (e.g., changes in size greater than 1 cm; changes in shape, such as matted together; or changes in consistency, such as rubbery) or the presence of painless, enlarged lymph nodes must be evaluated by a physician. (See the section on lymph nodes in Special Implications for the Therapist: Anatomy of the Lymphatic System in Chapter 13.)
Joint effusion, usually of one joint (monarticular), associated with infectious arthritis can occur as a result of bacterial, mycobacterial, fungal, or viral etiologic agents. Streptococcal bacteremia from any cause can result in suppurative arthritis (inflammatory with pus formation). Bone and joint infections are discussed more completely in Chapter 25.
AGING AND INFECTIOUS DISEASES
As a group, older adults are more susceptible to infectious diseases and experience increased morbidity and mortality compared with younger people; this is especially noted in the frail and debilitated older adult.67 This increased susceptibility is most likely multifactorial, encompassing immune function as well as comorbidities.
The immune system is complex and requires well-orchestrated adaptability and responsiveness. With aging, there are modest changes in cell-mediated or T-cell function with a decrease in the number of naive T cells but an increase in the number of memory T cells. These memory cells, however, are slower to respond and require a stronger stimulus. There is also a decrease in the productivity of proinflammatory cytokines.
Diminished cell-mediated immunity results in the reactivation of dormant infections, such as herpes zoster and tuberculosis, as well as a decreased response to vaccines. While studies are lacking, it appears most older adults retain antigen-presenting cell function, although the frail elderly with significant chronic illness may have decreased function as well. Chronic illness or comorbidities (e.g., renal, cardiac, or lung disease) play a role in decreased immune function and may be a better indicator of immune function than age alone.21
Extrinsic factors apart from the immune system can lead to increased susceptibility to infection in the older adult. Atrophic skin is more easily damaged, decreased cough and gag reflexes make it more difficult to control secretions, and decreased bronchiolar elasticity and mucociliary activity contribute to the development of pneumonia.20
In many aging people, physical decline or psychologic impairment may result in indifference to personal hygiene and loss of manual dexterity, body mobility, or vision. This may lead to an increased risk for falls, with accompanying injuries and fractures. Denture-associated infections may occur in up to 60% of older adult denture-wearing clients. Predisposing factors include flaccid, sagging cheeks; deepened labial angles constantly moistened by saliva; and ill-fitting dentures, often worn for a considerable time without replacement or repair.41
Many types of infections are seen in the aging adult, but early recognition of infection in the older adult is difficult because people underreport symptoms, the presentation is often vague or atypical, and symptoms are difficult to assess. The older adult may be unable to describe the present illness or past history or list the medications being taken. A complete physical examination may be difficult because of the person’s uncooperativeness, cognitive impairment, neurologic deficits, or physical impairments. Pain may be poorly localized or absent, or it may be confused with preexisting conditions, such as in septic arthritis in a client with degenerative joint disease.
There is one other important reason recognition of infection in older adults can be difficult: the increasing frequency of implanted devices such as joint prostheses,15 hardware, defibrillators, peripherally inserted central catheter lines, stents, grafts, and so on. If an implanted device develops a biofilm, there may be no immediate response. This is because the organism is attached to inorganic material.
The aging person also can have more serious infections with little or no fever because of an impaired thermoregulatory system or the masking effects of drugs such as aspirin, other antiinflammatory drugs, and corticosteroids.
Fever in older people may not be high enough to cause concern because the basal body temperature is low. A lower threshold for infection should be used (e.g., oral temperature of 99° F or 100° F), especially if the person is taking a medication that masks fever. Watch for (or ask family about) any recent episodes of confusion, memory loss, or other change in mental status; these may be the first symptoms of infection.
If the febrile response is absent in an older adult with a serious infection, it is a grave sign. Acute infections in the older adult may cause delirium or a sudden change in mental status. Chronic infections of the lungs, bone, skin, kidneys, and CNS may cause mental status changes perceived as dementia.127
Many frail elderly are in acute or extended-care settings and are therefore more likely to be exposed to nosocomial pathogens such as aerobic gram-negative bacilli, S. aureus, and VRE.20
INFECTIOUS DISEASES
Infection is a process in which an organism establishes a parasitic relationship with its host. This invasion and multiplication of microorganisms produces an immune response and subsequent signs and symptoms. Such reproduction injures the host by causing cellular damage from microorganism-producing toxins or intracellular multiplication or by competing with the host’s metabolism.
The host’s immune response may compound the tissue damage; such damage may be localized (e.g., as in infected pressure ulcers) or systemic. However, in some instances, microorganisms may be present in the tissues of the host and yet not cause symptomatic disease. This process is called colonization of organisms. The person with colonization may be a carrier and transmit the organisms to others but does not have detectable symptoms of infection.
The development of an infection begins with transmission of an infectious organism (agent, pathogen, pathogenic agent) and depends on a complex interaction of the pathogen, an environment conducive to transmission of the organism, and the susceptibility of the human host. Even after successful transmission of a pathogen, the host may experience more than one possible outcome.
The pathogen may merely contaminate the body surface and be destroyed by first-line defenses such as intact skin or mucous membranes that prevent further invasion, or a subclinical infection may occur in which no apparent symptoms are evident other than an identifiable immune response of the host. A rise in the titer of antibody directed against the infecting agent is often the only detectable response. Antibiotic treatment is not necessary, although infection control procedures remain in force to prevent spreading the bacteria to others.
A third possible outcome is the development of a clinically apparent infection in which the host-parasite interaction causes obvious injury and is accompanied by one or more clinical symptoms. This outcome is called infectious disease and ranges in severity from mild to fatal depending on the organism and the response and underlying health of the host.72
The period between the pathogen entering the host and the appearance of clinical symptoms is called the incubation period. This period may last from a few days to several months, depending on the causative organism and type of disease. Disease symptoms herald the end of the incubation period. A latent infection occurs after a microorganism has replicated but remains dormant or inactive in the host, sometimes for years (e.g., tuberculosis, herpes zoster). The host may harbor a pathogen in sufficient quantities to be shed at any time after latency and toward the end of the incubation period. This time period when an organism can be shed is called the period of communicability.
From this concept of communicability, communicable diseases can be defined as any disease whereby the causative agent may pass or be carried from one person to another directly or indirectly. It usually precedes symptoms and continues through part or all of clinical disease, sometimes extending to convalescence; but it is important to note that an asymptomatic host can still transmit a pathogen. The communicable period, like the incubation period and mode of transmission, varies with different pathogens and different diseases.144
Types of Organisms
A great variety of microorganisms are responsible for infectious diseases, including viruses, mycoplasmas, bacteria, rickettsiae, chlamydiae, protozoa, fungi (yeasts and molds), helminths (e.g., tapeworms), mycobacteria, and prions. All microorganisms can be distinguished by certain intrinsic properties such as shape, size, structure, chemical composition, antigenic makeup, growth requirements, ability to produce toxins, and ability to remain alive (viability) under adverse conditions such as drying, sunlight, or heat.
These properties provide the basis for identification and classification of the organisms. Knowledge of the properties permits diagnosis of a specific pathogen in specimens of body fluids, secretions, or exudates. All these properties are important to consider when looking for ways to interfere with the mechanisms of transmission.
Viruses are subcellular organisms made up only of a ribonucleic acid (RNA) or a deoxyribonucleic acid (DNA) nucleus covered with proteins. They are the smallest known organisms, visible only through an electron microscope. Viruses are completely dependent on host cells and cannot replicate unless they invade a host cell and stimulate it to participate in the formation of additional virus particles.
The estimated 400 viruses that infect human beings are classified according to their size, shape (spherical, rod shaped, or cubic), or means of transmission (respiratory, fecal, oral, or sexual). Viruses are not susceptible to antibiotics. However, antiviral medications can mitigate (moderate) the course of the viral illness. For example, acyclovir, an antiviral medication used for herpesvirus, interferes with DNA synthesis, causing decreased viral replication and decreasing the time of lesional healing.
Mycoplasmas are unusual, self-replicating bacteria that have no cell wall components and very small genomes. For this reason, antibiotics that are active against bacterial cell walls have no effect on mycoplasmas. At present, mycoplasmas remain sensitive to some antibiotics. They require a strict dependence on the host for nutrition and sustenance and are able to pass through many bacteria-retaining filters or barriers because they are very small.10
Bacteria are single-celled microorganisms with well-defined cell walls that can grow independently on artificial media without the need for other cells. Bacteria can be classified according to shape. Spherical bacterial cells are called cocci, rod-shaped bacteria are called bacilli, and spiral-shaped bacteria are called spirilla or spirochetes.
Bacteria can also be classified according to their response to staining (gram positive, gram negative, or acid fast), motility (motile or nonmotile), tendency toward capsulation (encapsulated or nonencapsulated), and capacity to form spores (sporulating or nonsporulating) (Fig. 8-1).
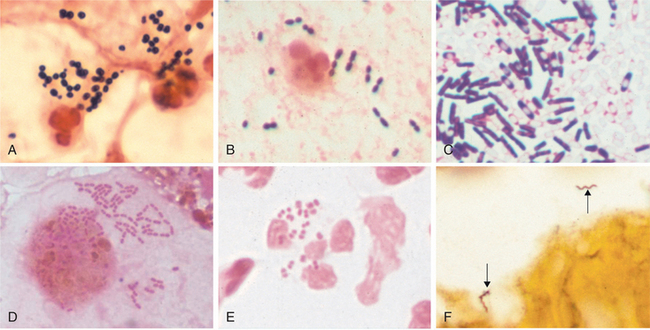
Figure 8-1 A variety of bacterial morphology. A, Gram stain of sputum from person with pneumonia. There are gram-positive cocci in clusters (Staphylococcus aureus) with degenerating neutrophils. B, Gram stain of sputum from an individual with pneumonia. Gram-positive, elongated cocci in pairs and short chains (Streptococcus pneumoniae) and a neutrophil are seen. C, Gram stain of Clostridium sordellii grown in culture. A mixture of gram-positive and gram-negative rods, many of which have subterminal spores (clear areas), are present. Clostridia species often stain as both gram positive and negative, although they are true gram-positive bacteria. D, Gram stain of a bronchoalveolar lavage specimen showing gram-negative intracellular rods typical of Enterobacteriaceae such as Klebsiella pneumoniae and E. coli. E, Gram stain of urethral discharge from someone with gonorrhea. Many gram-negative diplococci (Neisseria gonorrhoeae) are present within a neutrophil. F, Silver stain of brain tissue from a person with Lyme disease meningoencephalitis. Two helical spirochetes (Borrelia burgdorferi) are indicated by arrows. The panels are at different magnifications. (A to C, Reprinted from Kumar V, Abbas AK, Fausto N: Robbins and Cotran: pathologic basis of disease, ed 7, Philadelphia, 2005, Saunders, courtesy Dr. Kenneth Van Horn. D, Courtesy Karen Krisher, Clinical Microbiology Institute, Wilsonville, OR.)
Bacteria can also be classified according to whether oxygen is needed to replicate and develop (aerobic) or whether they can sustain life in an oxygen-poor (anaerobic) environment. Anaerobic bacteria are organisms that require reduced oxygen tension for growth.
Normal human flora are primarily anaerobic, and disease can be produced when these normal organisms are displaced from their usual tissue sites (e.g., mouth, skin, large bowel, female genital tract) into other tissues or closed body spaces.128 Other common anaerobic organisms include the spore-forming bacilli such as Clostridium botulinum or C. tetani that thrive in a strictly anaerobic environment.
Rickettsiae are primarily animal pathogens that generally produce disease in human beings through the bite of an insect vector such as a tick, flea, louse, or mite. They are small, gram negative, obligate intracellular organisms that often cause life-threatening infections. Like viruses, these microorganisms require a host for replication. Three categories of the family Rickettsiaceae are Rickettsia, Coxiella, and Bartonella.16
Chlamydiae are smaller than rickettsiae and bacteria but larger than viruses. They, too, depend on host cells for replication, but unlike viruses they always contain both DNA and RNA and are susceptible to antibiotics.
Protozoa have a single cell unit or a group of nondifferentiated cells loosely held together and not forming tissues. They have cell membranes rather than cell walls, and their nuclei are surrounded by nuclear membranes. Larger parasites include roundworms and flatworms. Fungi are unicellular to filamentous organisms possessing hyphae (filamentous outgrowths) surrounded by cell walls and containing nuclei (eukaryocyte). Fungi show relatively little cellular specialization and occur as yeasts (single-cell, oval-shaped organisms) or molds (organisms with branching filaments). Depending on the environment, some fungi may occur in both forms. Fungal diseases in human beings are called mycoses.
Prions are proteinaceous, infectious particles consisting of proteins but without nucleic acids. These particles are transmitted from animals to human beings and are characterized by a long latent interval in the host. When reactivated, they cause a rapidly progressive deteriorating state in the host (e.g., Creutzfeldt-Jakob disease, bovine spongiform encephalopathy or “mad cow disease”).43
The Chain of Transmission
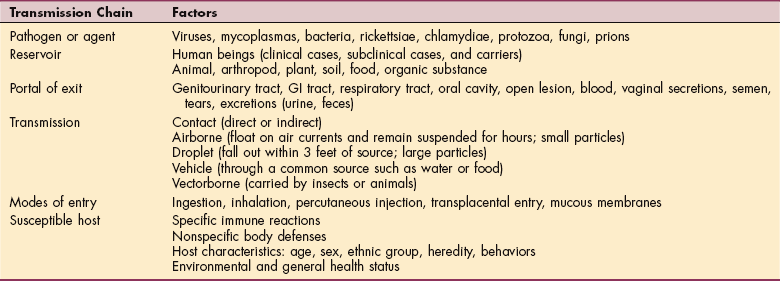
Infection begins with transmission of a pathogen to the host. Successful transmission depends on a pathogenic agent, a reservoir, a portal of exit from the reservoir, a mode (mechanism) of transmission, a portal of entry into the host, and a susceptible host. This sequence of events is called the chain of transmission (Table 8-2).
Nosocomial infections are infections acquired during hospitalization. In the United States, about 5% of people who enter the hospital without infection will acquire a nosocomial infection. Transmission can be through any of the possible routes discussed in this section. Nosocomial infections result in prolongation of hospital stays, increase in cost of care, significant morbidity, and a mortality rate of about 5%.77
The most common infections are urinary tract infections (usually associated with Foley catheters or urologic procedures) and bloodstream infections. Bloodstream infections can occur as a result of indwelling intravenous (IV) catheters or surgical wound infections, abscesses, pneumonia (especially in intubated individuals or those with altered levels of consciousness), and GI and genitourinary infections.
In general, increases in nosocomial infections can be related to more frequent use of invasive devices for monitoring or therapy, more colonization and infection by multidrug–resistant organisms (both viral and bacterial), and greater debilitation and severity of illness of hospitalized clients who acquire these infections.
The increased use of invasive and surgical procedures, immunosuppressants, antibiotics, and the lack of handwashing predispose people to such infections and superinfections. At the same time, the growing number of personnel who come into contact with the client makes the risk of exposure greater.
Prevention is of critical importance in controlling nosocomial infections. The concept of standard precautions emphasizes that all clients must be treated as though each one has a potential bloodborne, transmissible disease; thus all body secretions are handled with care to prevent disease. Handwashing has been cited as the easiest and most effective means of preventing nosocomial infection and must be done routinely even when gloves are used.12 See further discussion under Control of Transmission in this chapter.
Pathogens
Humans coexist with many microorganisms in complex, mutually beneficial relationships. Even so, many organisms are parasitic, maintaining themselves at the expense of their host. Some parasites arouse a pathologic response in the host and are called pathogens or pathogenic agents. A pathogen is defined as any microorganism that has the capacity to cause disease.126 As such, pathogens are ineffective parasites because they stimulate a disease response, which may harm the host and eventually kill the pathogen.
The ability of a pathogen to stimulate an immune response in the host (antigenicity) varies greatly among organisms, depending on the site of invasion, the number of pathogenic organisms, and the dissemination of organisms in the body. The immune status of a person plays the largest role in determining the risk for infection and the ability of the host to combat organisms that have gained entry.
The mode of action of a pathogen refers to how the organism produces a pathologic process. Great variation exists among the various pathogens. Some intracellular pathogens, like viruses, invade cells and interfere with cellular metabolism, growth, and replication, whereas others invade and cause hyperplasia and cell death. Yet other organisms, such as the influenza virus, have the potential to alter their antigenic characteristics. This virus is capable of extensive gene rearrangements, resulting in significant changes in surface antigen structure. This ability allows new strains to evade host antibody responses directed at earlier strains.
Some viruses (e.g., all members of the herpesvirus group) cause a persistent latent infection that can be reactivated in certain circumstances. HIV causes immunosuppression by destroying helper T lymphocytes. Some pathogens, such as the tetanus bacillus, produce a toxin that interferes with intercellular responses. Some bacteria, such as diphtheria and tetanus, secrete water-soluble antigenic exotoxins that are quickly disseminated in the blood, causing potentially severe systemic and neurologic manifestations. Larger parasites such as roundworms cause anemia and interfere with the function of the GI system.
The characteristics of the organism and the susceptibility of the host influence the likelihood of a pathogen producing infectious disease and the type of disease produced. Not all pathogens have an equal probability of inducing disease in the same host population. Principal pathogens regularly cause disease in people with apparently intact defense systems.
Opportunist pathogens do not cause disease in people with intact host defense systems but can clearly cause devastating disease in many hospitalized and immunocompromised clients.126 Organisms that may be harmless members of normal flora in healthy people may act as virulent invaders in people with severe defects in host defense mechanisms.91
Pathogenicity, the ability of the organism to induce disease, depends on the organism’s speed of reproduction in the host, the extent of damage it causes to tissues, and the strength of any toxin released by the pathogen. Virulence refers to the potency of the pathogen in producing severe disease and is measured by the case fatality rate (i.e., the number of people who die of the disease divided by the number of people who have the disease). Virulence provides a quantitative measure of pathogenicity. The amount and destructive potential of released toxin are closely related to virulence.
Reservoir
A reservoir is an environment in which an organism can live and multiply, such as an animal, plant, soil, food, or other organic substance or combination of substances. The reservoir provides the essentials for survival of the organism at specific stages in its life cycle. Some parasites have more than one reservoir, such as the yellow fever virus, which can maintain life in human beings and other animals. Some parasites require more than one reservoir at different growth stages and still others, such as most sexually transmitted organisms, require only a human reservoir.
Human and animal reservoirs can be symptomatic or asymptomatic carriers of the pathogen. A carrier maintains an environment that promotes growth, multiplication, and shedding of the parasite without exhibiting signs of disease. Hepatitis is a common example of this carrier state in human beings.
Portal of Exit
The portal of exit is the place from which the parasite leaves the reservoir. Generally, this is the site of growth of the organism and corresponds to the system of entry into the next host. For example, the portal of exit for GI parasites is usually the feces, and the portal of entry into a new host is the mouth. Exceptions to the case include hookworm eggs, which are shed in the feces but enter through the skin of a person walking barefoot in soil containing hatched eggs.
Common portals of exit include secretions and fluids (e.g., respiratory secretions, blood, vaginal secretions, semen, tears), excretions such as urine and feces, open lesions, and exudates such as pus from an open wound or ulcer. Some organisms, such as HIV, have more than one portal of exit. Knowledge of the portal of exit is essential for preventing transmission of a pathogen.
Mode of Transmission
For infection to be transmitted, the invading organism must be transported from the infected source to a susceptible host. Microorganisms are transmitted by several possible routes, and the same microorganism can travel by more than one route. The five main routes of transmission are contact, airborne, droplet, vehicle, and vector borne.
Contact transmission occurs directly or indirectly. Direct contact is the direct transfer of microorganisms that come into physical contact either by skin-to-skin contact or mucous membrane–to–mucous membrane contact (e.g., sexual contact, biting, touching, kissing).
Indirect contact involves transfer of microorganisms from a source to a host by passive transfer from an inanimate, intermediate object, called a fomite. Inanimate objects can include items such as the telephone, sphygmomanometer, bedside rails, tray tables, countertops, and other items that come into direct contact with the infected person, thus emphasizing the need for thorough handwashing at all times.
An example of indirect transmission is transfer of human immunodeficiency virus from a contaminated source to a host through a needlestick. Another example of indirect contact includes oral-fecal transmission by the ingestion of enteric pathogens from a food prepared by a person who does not wash his or her hands.72
Airborne transmission occurs when disease-causing organisms are so small (less than 5 microns) that they are capable of floating on air currents within a room and remain suspended in the air for several hours. They are often propelled from the respiratory tract through coughing or sneezing. A host then inhales the particles directly into the respiratory tract (e.g., tuberculosis, chickenpox, rubeola measles).54
Droplet transmission is different from airborne transmission because droplets are larger particles (greater than 5 microns) than airborne particles and they do not remain suspended in air but fall out within 3 feet of the source. They are produced when a person coughs or sneezes and then travel only a short distance. A common example of droplet-spread infection is influenza. Those people who are in closest proximity to the infected source have the highest risk for infection.72
Vehicle transmission occurs when infectious organisms (e.g., salmonellosis) are transmitted through a common source (e.g., contaminated food, water, and IV fluid) to many potential susceptible hosts. Vectorborne transmission of infectious organisms involves insects and/or animals that act as intermediaries between two or more hosts. Lyme disease and Rocky Mountain spotted fever are examples of vectorborne diseases.
Portal of Entry
A pathogen may enter a new host by ingestion, inhalation, or bites or through contact with mucous membranes, percutaneously or transplacentally. Infectious diseases vary as to the number of organisms and the duration of exposure required to start the infectious process in a new host.
Host Susceptibility
Each person has his or her own susceptibility to infectious disease, and this susceptibility can vary throughout time. A susceptible host has personal characteristics and behaviors that increase the probability of an infectious disease developing.
Biologic and personal characteristics such as age, sex, ethnicity, and heredity influence this probability. General health and nutritional status, hormonal balance, and the presence of concurrent disease also play a role. Likewise, living conditions and personal behaviors such as drug use, diet, hygiene, and sexual practices influence the risk of exposure to pathogens and resistance once exposed.
Older adults in hospitals and long-term care facilities are already susceptible hosts, especially if poorly nourished. Immunosuppressive agents and corticosteroids decrease the body’s ability to resist infection. Inadequate or absent handwashing or other breaches of aseptic technique result in spread of microorganisms from health care workers (HCWs) to clients and between individuals receiving health care.
Surfaces of equipment can become contaminated and then transmit microorganisms that cause infection. Incorrect isolation procedures such as leaving doors open to rooms in which airborne precautions are in effect or not using masks increase the risk of transmitting organisms that cause nosocomial infections.
The presence of underlying medical disorders (e.g., malignancy, diabetes, renal failure, acquired immune deficiency syndrome [AIDS], and cirrhosis) decreases T-cell– and B-cell–mediated immune function. Breaches of body integrity such as nasogastric and chest tubes, intubation, urinary catheters, and IV devices impair the body’s defense mechanisms, decreasing the ability of the integumentary, GI, genitourinary, and respiratory systems to resist invasion by microorganisms.174
Lines of Defense.: Susceptibility is also influenced by the presence of anatomic and physiologic defenses, sometimes called lines of defense. The first-line defenses are external, such as intact skin and mucous membranes; oil and perspiration on skin; cilia in respiratory passages; gag and coughing reflexes; peristalsis in the GI tract; and the flushing action of tears, saliva, and mucus.
These first-line defenses act to inhibit invasion of pathogens and remove them before they have an opportunity to multiply. The chemical composition of body secretions such as tears and sweat, together with the pH of saliva, vaginal secretions, urine, and digestive juices, further prevents or inhibits growth of organisms. Compromise in any of these natural defenses increases host susceptibility to pathogen invasion.
Another important first-line defense is the normal flora of microorganisms that inhabit the skin and mucous membranes in the oral cavity, GI tract, and vagina. These organisms occur naturally and usually coexist with their host in a mutually beneficial relationship. Through a mechanism called microbial antagonism they control the replication of potential pathogens.
The importance of this mechanism is evident when it is disturbed, as happens when extensive antibiotic therapy destroys normal flora in the oral or vaginal cavity, resulting in Candida albicans, an overgrowth of yeast. Some normal flora can become pathogenic under specific conditions such as immunosuppression or displacement of the pathogen to another area of the body. Displacement of normal flora is a common cause of nosocomial infections. This can occur when Escherichia coli, ordinarily normal flora in the GI tract, invade the urinary tract. Invasive procedures increase the risk of displacing these organisms.
The second-line defense, the inflammatory process, and the third-line defense, the immune response, share several physiologic components. These include the lymphatic system, leukocytes, and a multitude of chemicals, proteins, and enzymes that facilitate the internal defenses.
Once a microorganism penetrates the first line of defense, the inflammatory response is initiated. Inflammation is a local reaction to cell injury of any type whether from physical, chemical, or thermal damage, or microbial invasion. As a response to microbial injury, inflammation is aimed at preventing further invasion by walling off, destroying, or neutralizing the invading organism.
The early inflammatory response is protective, but it can continue for sustained periods in some infections, leading to granuloma formation. The production of new leukocytes may be stimulated for weeks or months and is reflected in an elevated white blood cell count. However, sustained inflammation can become chronic and result in destruction of healthy tissues. Extensive necrosis from persistent inflammation can increase tissue susceptibility to the infectious agent or provide an ideal setting for invasion by other pathogens.
The first-and second-line defenses are nonspecific; that is, they operate against all infectious agents in the same way. In contrast, the immune system responds in a specific manner to individual pathogens as long as the organism has antigenic characteristics. Generally, antigens are proteins, large polysaccharides, or large lipoprotein complexes that stimulate an immune response.
Not all microorganisms are antigenic, but some are bound by complement or other host-produced substances to form an antigen that elicits an immune response. An immune response is triggered after foreign materials have been cleared from an area of inflammation. For specific details regarding cell-mediated versus humoral immune responses, see Chapter 7.
Control of Transmission
Much can be done to prevent transmission of infectious diseases, including the use of barriers and isolation; comprehensive immunizations, including the required immunization of travelers to or emigrants from endemic areas; drug prophylaxis; improved nutrition, living conditions, and sanitation; and correction of environmental factors.
Breaking the transmission chain at any of these links can help control transmission of infectious diseases. The link most amenable to control varies with the characteristics of the organism, its reservoirs, the type of pathologic response it produces, and the available technology for control. The general goal is to break the chain at the most cost-effective point or points—that is, the point at which the greatest number of people can be protected with available technology and the least amount of resources.
Isolation and barriers can be used to prevent the transmission of microorganisms from infected or colonized people to other unaffected people. In hospital or institutional settings, the purpose of isolating individuals or residents is to prevent the transmission of colonized or infectious microorganisms among clients, visitors, and HCWs. In 1996 the Centers for Disease Control and Prevention (CDC) and the Hospital Infection Control Practices Advisory Committee issued a revision of the isolation guidelines.
The new guidelines outline a two-tiered approach with standard precautions that apply to all clients and transmission-based precautions that apply to anyone with documented or suspected infection or colonization with specific microorganisms.
These transmission-based precautions are defined according to the major modes of transmission of infectious agents (contact, airborne, and droplet) in the health care setting (Table 8-3). Standard precautions have replaced universal precautions. Barrier precautions stipulate that gloves should be worn to touch any of the following: blood; all body fluids; secretions and excretions except sweat, regardless of whether these are visibly bloody; nonintact skin; and mucous membranes. Infectious waste is defined as free-flowing blood or body fluids present in sufficient quantity to drip, splash, or flake from dressings or containers (Box 8-3).
Table 8-3
Type of Transmission-Based Precautions and Prevention Guidelines
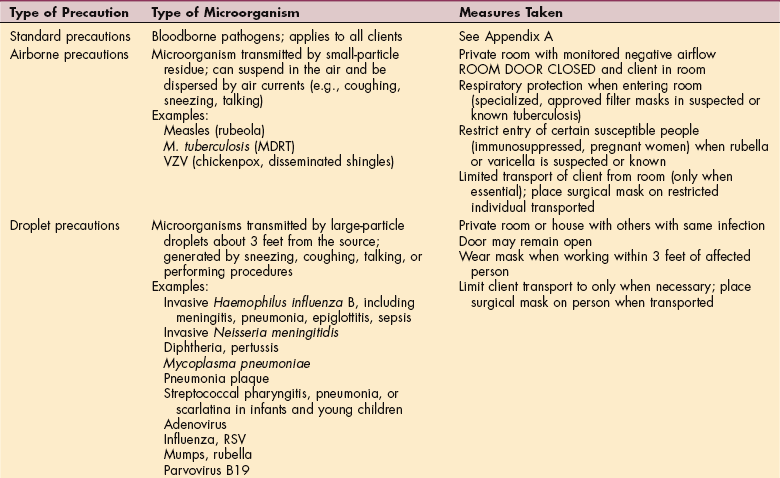
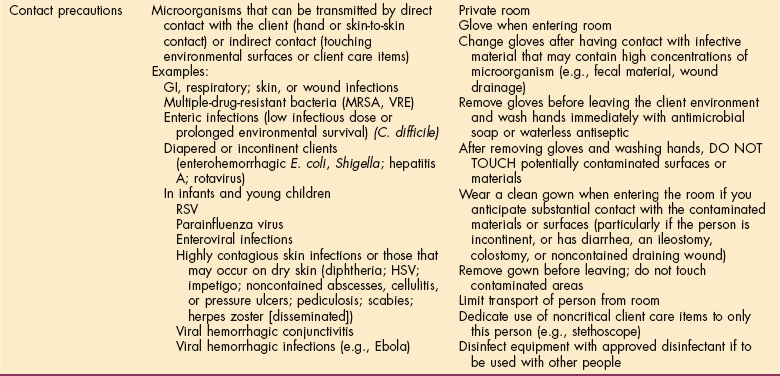
MDRT, Multiple-drug-resistant tuberculosis; RSV, respiratory syncytial virus; MRSA, methicillin-resistant Staphylococcus aureus; VRE, vancomycin-resistant enterococci.
Modified from Centers for Disease Control and Prevention: Guidelines for infection control in health care personnel, Am J Infect Control 26(3):289-343, 1998.
Hands must be washed immediately after gloves are removed and between clients. For procedures that are likely to generate splashes or sprays of body fluid, a mask with eye protection or a face shield and gown should be worn. Gowns should be of a material that prevents penetration by microorganisms and subsequent contamination of the skin or clothing.54,179 Needles should not be recapped, bent, or broken, but should be disposed of in a puncture-resistant container.45
Handwashing is an integral part of reducing transmission of harmful microbes in a health care setting. Streptococci and coagulase-negative staphylococci are the most common bacteria residing on the skin. HCWs can transiently obtain other pathogens after patient care or from the areas immediately surrounding a client, which can then be transmitted to other clients. Transient organisms are more likely to be transmitted to others than are resident flora of the skin.
Handwashing significantly reduces transient bacteria on HCW hands and the risk of transmitting infection. Different studies have been done looking at actual barriers to proper handwashing, while others concentrated on perceived barriers.
In one large study, nonadherence to recommended handwashing was highest in areas where adherence was crucial (such as intensive care units), whereas adherence was highest in areas where there was a lower need for stringent hand hygiene. Perceived reasons for nonadherence included skin irritation caused by the detergents, high client/HCW ratio (less time), unavailable or inconvenient location of supplies, forgetfulness, glove use, and incorrect information regarding proper hand hygiene.121
The CDC has reevaluated hand hygiene and made recommendations allowing HCWs to achieve more realistic goals of proper hand hygiene.12 Soap (antimicrobial or non-antimicrobial) and water should be used when hands are visibly soiled with blood or other body fluid, before and after eating, and after using the restroom (Box 8-4).
If hands are not visibly soiled, decontamination may be accomplished by using an alcohol-based rub for the following instances: before and after routine contact with a client, before putting on gloves and after removing gloves for a nonsurgical procedure or client contact, and after contact with a body fluid or skin that is not intact and before moving to a clean part of the same person. During outbreaks of C. difficile–associated disease (CDAD), washing hands with an antimicrobial soap and water after removing gloves is advised (Box 8-5).13
No recommendations are available for the use of non–alcohol-based rubs since data are lacking. Antimicrobial towelettes are an alternative but not a substitute for handwashing with soap and water or alcohol-based rubs.
Other pertinent recommendations have been made by the CDC in regard to wearing jewelry or gloves and having long or artificial nails (acrylics). Although rings have been shown to harbor organisms, more studies are needed to determine if this leads to an increase in transmission of these microbes; the CDC has not made specific recommendations in this area.
The Occupational Safety and Health Administration has mandated that gloves be worn by HCWs when caring for clients when they may be exposed to blood or body fluids that can be contaminated with blood. Gloves have been shown to reduce contamination of hands as well as reduce the transmission of pathogens by HCWs. However, gloves do not completely protect against hand contamination; therefore decontamination of the hands after use is essential.
Available studies suggest that the areas under the fingernails contain significant amounts of bacteria, especially coagulase-negative staphylococci and gram-negative rods. Artificial nails harbor even larger concentrations than natural nails. It is unknown if long or artificial nails contribute to transmission of these organisms, although a few reports have linked outbreaks of Pseudomonas to artificial nails worn by nurses. More studies are needed to determine the significance of artificial nails, but the CDC recommends that artificial nails should not be worn if the HCW is in contact with clients at high risk for infection.
Immunization, by decreasing host susceptibility, can now control many diseases, including diphtheria, tetanus, pertussis, measles, mumps, rubella, some forms of meningitis, poliomyelitis, hepatitis A and B, pneumococcal pneumonia, influenza (certain strains), and rabies. Each year the CDC issues updated information on the vaccine and antiviral agents available for controlling influenza during the current influenza season.
Vaccines, which contain live but attenuated (weakened) or killed microbes, induce active immunity against bacterial and viral diseases by stimulating antibody formation.
These molecules lock onto specific proteins made by a virus or bacterium, which are often those proteins lodged in the microbe’s outer coat. Once antibodies attach to an invading microbe, other immune defenses are evoked to destroy it. Immune globulins contain previously formed antibodies from hyperimmunized donors or pooled plasma and provide temporary passive immunity. Passive immunization is generally used when active immunization is life threatening or when complete protection requires both active and passive immunization (e.g., immunoglobulins used for hepatitis B or for tetanus) (see Table 7-1).
Side effects to immunization can occur, but the incidence of significant adverse effects of immunization among human beings remains very small.1,3,4 The potential increase in susceptibility to influenza and death from respiratory illness in high-risk people (e.g., those with rheumatoid arthritis, the aging adult, and chronically ill or immunosuppressed individuals) suggests that the influenza and pneumococcal vaccines should include these groups in standard immunization programs.3
Prophylactic antibiotic therapy may prevent certain diseases and is usually reserved for people at high risk of exposure to dangerous infections (e.g., Pneumocystis carinii pneumonia in clients with HIV/AIDS, postexposure of HCWs to percutaneous contamination from individuals with HIV, preoperatively before joint replacement surgery).56
Antibiotic-resistant bacteria are on the rise in part because antibiotics have been misused and overused. This is only a small part of the total picture regarding this issue. Other components of this problem include the extensive use of antibiotics in animals later consumed or whose products are consumed (e.g., milk products). Crowded conditions (e.g., day care centers, hospitals, military barracks, and prisons) and prior antibiotic therapy are the principal factors predisposing to colonization and disease.
Some bacteria, such as enterococci, which cause wound and blood infections, have developed mutant strains that do not respond to any antibiotic therapy. Enterococcal infections are primarily limited to hospitals. At present, certain strains of pneumococcus are resistant to only one antibiotic, so other antibiotics remain effective against these pneumococci. If those strains become resistant to other (currently effective) antibiotics, there may be no treatment available. Before 1980, only a few cases of pneumococcus were resistant to penicillin, but within a year strains resistant to penicillin were reported everywhere and are now common throughout the world.
Because resistance to many commonly used antibiotics has developed, including resistance to vancomycin, a search is underway for novel and more effective antimicrobial agents. Cellular enzymes such as synthetases that are universal and essential for cellular viability are being studied as one of the targets for new antibiotics.136 Experiments are also underway to find molecules that are effective in binding small, untranslated RNA, causing plasmid elimination and reducing resistance.171 Gatifloxacin, a newer fluoroquinolone, continues to retain susceptibility to most gram-negative organisms, but increasing resistance to Streptococcus spp., including S. pneumoniae, is worrisome.46,111
In April 2000 the Food and Drug Administration (FDA) approved linezolid for the treatment of individuals with infections caused by gram-positive bacteria. Linezolid comes from the first completely new class of antibiotics to reach hospitals in 35 years, the oxazolidinones. Linezolid is indicated for adults and children in the treatment of numerous gram-positive organisms, including MRSA and Enterococcus spp.119
Although studies are lacking, linezolid may have efficacy in treating M. tuberculosis, including strains resistant to the usual antituberculotic agents.44 Current research is focused on the epidemiology of resistant bacteria, including investigation about the receptors and mechanisms of cellular action and resistance. The study and potential use of inhibitors of resistance mechanisms is an area that might prove useful as a new direction in drug development.101,185
Improved nutrition, living conditions, and sanitation through the use of disinfection, sterilization, and antiinfective drugs can inactivate pathogens such as S. aureus. This is important because drug-resistant strains of S. aureus have developed. One strain of staphylococcus, MRSA, is resistant to most antibiotics.
Over the past 10 years, MRSA and other resistant strains of S. aureus have become the most common causes of hospital and community-acquired infections. MRSA usually develops when multiple antibiotics are used in the treatment of infection and in older adults who are debilitated, having surgery or multiple invasive procedures, or being treated in critical care units.
Transmission to a new portal of entry can be prevented by environmental disinfection, use of barrier precautions (gloves, masks, condoms), proper handling of food, and protection from vectors. Decreasing host susceptibility can be achieved through personal hygiene and avoidance of high-risk behaviors (unsafe sex practices, injection drug use, recapping needles) and effective handwashing.
Maintaining the first-line defense is an important consideration for the client whose health status has already been compromised by disease or diagnostic and treatment procedures. Some ways to accomplish this include preoperative and postprocedure assistance to encourage deep breathing;, coughing, ambulation, and skin care; maintaining adequate hydration, fluid, and electrolyte balance; and providing proper nutrition to strengthen resistance.
Correction of environmental factors, particularly water treatment; food and milk safety programs; and control of animals, vectors, rodents, sewage, and solid wastes, can best eradicate nonhuman environments (reservoirs) and thus control pathogens.
Other prevention methods in this category include proper handling and disposal of secretions, excretions, and exudates; isolation of infected clients (doors must remain closed, especially in negative-pressure rooms); and quarantine of contacts.
The CDC has recommended specific transmission precautions based on knowledge of the transmission chain for individual infections. The precautions were designed to prevent transmission of pathogens among hospitalized people, HCWs, and visitors (see Table 8-3). Specific recommendations have been made for individual diseases.
Diagnosis of Infectious Diseases
Five basic laboratory techniques can be used in the diagnosis of infectious diseases: (1) direct visualization of the organism, (2) detection of microbial antigen, (3) a search for clues produced by the host immune response to specific microorganisms, (4) detection of specific microbial nucleotide sequences, and (5) isolation of the organism in culture. Each technique has its use and each has associated advantages and disadvantages.
In many infectious diseases, pathogenic organisms can be directly visualized by microscopic examination of readily available tissue fluids, such as sputum, urine, and pus as well as pleural, peritoneal, and cerebrospinal fluid (CSF). Detection of specific antigens establishes the presence of some diseases such as meningitis, hepatitis B, and some respiratory and genitourinary tract infections.
Histopathologic examination of biopsied or excised tissue often reveals patterns of the host inflammatory response that can provide clues to narrow down the diagnostic possibilities. Some viral infections, such as skin or respiratory infections caused by herpesviruses or pneumonia due to CMV, produce characteristic changes in host cells visible on cytologic examination.
Recent techniques to amplify microbial DNA or RNA sequences for detection have been used to diagnose some infections and are expected to be developed enough to diagnose numerous other infectious diseases. Finally, isolation of a single microbe from an infected site is generally considered evidence that the infection is caused by this organism.
SPECIFIC INFECTIOUS DISEASES
Most infections are confined to specific organ systems. In this book, many of the important infectious disease entities are discussed in the specific chapter dealing with the affected anatomic area. Only the most commonly encountered infectious problems not covered elsewhere are included in this chapter.
Bacterial Infections
Overview.: Clostridium difficile (C. difficile, “C diff”) is becoming an important public health issue as a cause of nosocomial and community-based diarrhea. It is an anaerobic, spore-forming bacillus recognized as occurring exclusively in the presence of exposure to antibiotics; it is the only anaerobe that poses a nosocomial risk.9
CDAD is increasingly recognized among residents of long-term care facilities but has especially been reported with increasing frequency in acute care or short-stay hospitals because of the high rates of antibiotic use in hospitals.100
Incidence.: CDAD rates and severity appear to be increasing rapidly in the United States and Canada and show no sign of decline. U.S. hospital discharges for which C. difficile was listed as a diagnosis doubled from 82,000 in 1996 to 178,000 in 2003, with the highest rate reported in adults aged 65 years or older. Incidence is an estimated 228 cases per 100,000 persons.150
Etiology, Transmission, and Risk Factors.: Transmission of C. difficile occurs primarily in health care facilities via the fecal-oral route following contamination of the hands of HCWs and patients with oral ingestion of the causative organism. Contamination of the patient care environment also plays an important role.162 Nonhuman reservoirs such as water, raw vegetables, and animals can also cause infection.5 Tube feeding is also a risk factor.52
The reason for rising rates of CDAD is unknown. Several possible explanations have been offered, including new and evolving patterns of antimicrobial drug use (e.g., increased use of fluoroquinolones), promotion of alcohol-based hand sanitizers (these may not be as effective as soap in removing C. difficile), and the emergence of more virulent strains of C. difficile better able to cause transmission and disease.100
Age (65 years and older) is a definite risk factor, especially when linked with antibiotic use and residence in acute or long-term health care facilities, where exposure is increased through physical proximity of residents and with their health care providers, or admittance to a room that housed someone with CDAD during the last 10 to 14 days.27,52
Older adults may also have decreased host defenses to protect them from CDAD such as decreased stomach acid as part of the aging process (achlorhydria) or decreased immune responsiveness. There is also an increased use of medications such as H2 receptor blockers or proton-pump inhibitors, which are becoming increasingly recognized in association with CDAD.42
Pathogenesis.: Change in the protective flora of the enteric system induced by antibiotics may produce acute diarrhea by overgrowth and toxin production by C. difficile. Gastric acid constitutes a major defense mechanism against ingested pathogens. Loss of stomach acid has been associated with colonization of the normally sterile upper GI tract.
In the healthy person, the C. difficile organism is inactive in the spore form. It is assumed that antibiotic-induced change in the competing intestinal flora promotes a conversion from a spore state to the vegetative forms, which then replicate and produce toxins, causing cellular damage of the intestinal mucosa and increased gut permeability.9
A more virulent strain of C. difficile is associated with more frequent and more severe disease with higher rates of toxic megacolon, shock, and even death. The variant strains of C. difficile are resistant to fluoroquinolones, producing up to 23 times more toxins than other strains.9
Clinical Manifestations.: CDAD is easily recognized by persistent diarrhea following antibiotic consumption. The patient may not have a fever, but an elevated white blood cell count is common. Manifestations of CDAD can range from uncomplicated diarrhea to sepsis and even death from toxic megacolon. Antibiotic-associated colitis is discussed further in Chapter 16.
MEDICAL MANAGEMENT
Diagnosis is typically confirmed by identifying toxins in the stool of the infected individual. Colonoscopy identifying pseudomembranous lesions present late in the disease may help identify difficult-to-diagnose cases.
Standard treatment consists of prompt discontinuation of the antibiotic agent with administration of oral metronidazole (Flagyl), an antibiotic effective against anaerobic bacteria. In some cases, oral vancomycin is the antimicrobial treatment of choice. Individuals with the fulminant form of colitis may not respond to this treatment. Management of diarrhea is essential to prevent electrolyte imbalance and subsequent sequelae.
PREVENTION.
Prevention of this nosocomial infection is imperative to reduce patient morbidity and mortality and reduce health care costs associated with infection control, medication, and excess hospital days.
C. difficile is a bacteria commonly present in our everyday environment in natural water sources, soil, animals, and raw vegetables.5 CDAD is, by and large, a nosocomial disease and therefore most prevention and control efforts take place in the health care setting. Proven strategies include hand hygiene, barrier precautions, environmental disinfection, and antimicrobial stewardship.150
Contact precautions are recommended to prevent the transmission of C. difficile in the health care setting consisting of using private rooms or rooms shared by CDAD patients, using gloves and gowns for all contact, and using disposable equipment or cleaning equipment between use with each patient.55 The primary means of reducing risk is through the careful use of antimicrobial drugs.58
Preventing oral ingestion of the C. difficile organism is important whenever suction devices are used in the oral cavity (mouth). A strong correlation has been noted between ventilator-associated pneumonia rates and CDAD rates in the critical care population, emphasizing again the importance of cleanliness of anything introduced into a patient’s mouth and stomach.151
Staphylococcal Infections
Overview and Incidence.: Staphylococci bacteria are among the most common bacterial pathogens normally residing on the skin. Although there are more than 30 species of staphylococci, only a few are clinically relevant.
Staphylococci can be characterized as coagulase (a surface enzyme that converts fibrinogen to fibrin) positive or negative. Staphylococcus aureus is, almost without exception, the only significant staphylococcal species that is coagulase positive.
Several coagulase-negative bacteria may be pathogenic, such as S. epidermidis, but all are often collectively referred to as coagulase-negative staph (CoNS). S. aureus is very virulent, whereas the forms of CoNS are less virulent but still cause significant human infections. These organisms are nonmotile and anaerobic. They are hardy and able to survive on inanimate objects for an extended period.
Staphylococci bacteria are the leading cause of nosocomial and community-acquired infections, accounting for about 13% of all hospital infections each year. This figure translates into approximately 2 million hospital infections annually, resulting in 60,000 to 80,000 deaths each year. Staphylococcal species are the most common cause of infections, affecting all ages and involving the blood, skin, lung, soft tissue, joints, and bones. They are a leading cause of infective endocarditis. S. epidermidis is the most common cause of prosthetic device infections.
Risk Factors.: S. aureus spreads by direct contact with colonized surfaces or people. The most common location of human colonization of S. aureus are the nares (nasal passages), although the skin, axilla, perineum, vagina, and oropharynx can also be colonized. Approximately 25% to 50% of healthy adults are intermittently or perpetually colonized with S. aureus.
Colonization occurs more frequently in individuals with diabetes who are insulin dependent, individuals who are HIV positive, clients receiving hemodialysis, IV drug users, and persons with chronic skin lesions. Infections occur more frequently in individuals who are colonized than those who are not (typically with their own colonized strain).
Individuals more likely to develop a staph infection include surgical and burn patients (from damaged skin); individuals with diabetes who require insulin (from needlesticks, perhaps decreased leukocyte function); anyone who is neutropenic (PMNs dangerously low); and anyone with prosthetics, chronic skin disease, rheumatoid arthritis, catheters, or on corticosteroid therapy (unable to control local infections sufficiently).
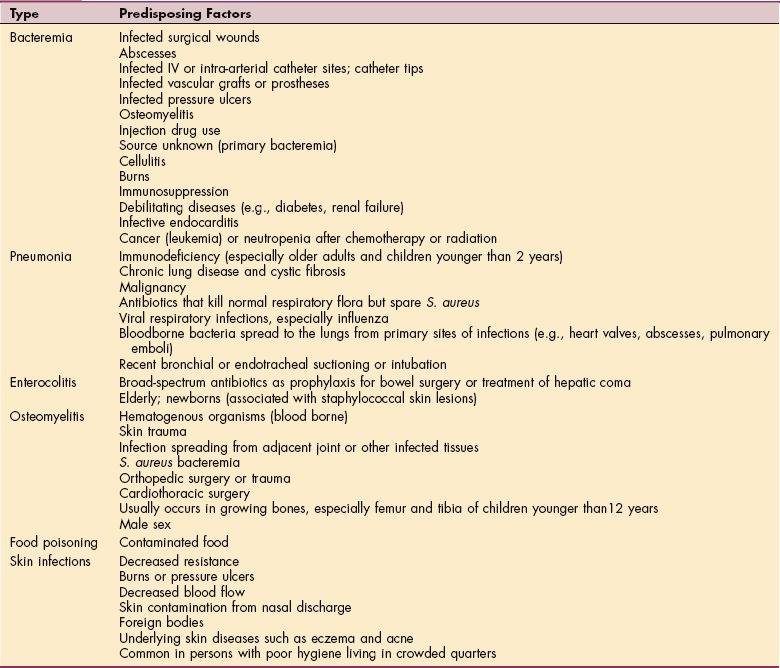
Predisposing factors are multiple and varied depending on disease location (Table 8-6). Transient contamination of HCWs’ hands can also transmit the bacteria to clients and is an important cause of spreading bacteria in health care settings.169
Pathogenesis.: S. aureus cannot invade through intact skin or mucous membranes; infection usually begins with traumatic inoculation of the organism. Once inside the body, the organism is a virulent pathogen, secreting membrane-damaging enzymes and toxins that harm host tissues. Staphylococci stimulate a significant host immune response, forming a suppurative or pustular local response. If the bacteria are then able to evade local host defenses, they can spread via the bloodstream to almost any location in the body. The bones, joints, kidney, lung, and heart valves are the most common sites of S. aureus infections.
Clinical Manifestations.: When S. aureus is inoculated into a previously sterile site, infection usually produces suppuration and abscess formation. The abscesses range in size from microscopic to lesions several centimeters in diameter filled with pus and bacteria (Fig. 8-2).

Figure 8-2 Staphylococcus skin abscess. (Reprinted from Braverman IM: Skin signs of systemic disease, ed 3, Philadelphia, 1998, W.B. Saunders.)
Infective syndromes include osteomyelitis, infections of burns or surgical wounds,143 respiratory tract infections (particularly in newborns and intubated or ICU patients), bacterial arthritis, septicemia, bacterial endocarditis, and toxic shock syndrome. Consumption of toxins produced by staphylococcal species in contaminated food is a common cause of food poisoning. Fever, chills, and symptoms associated with the affected area may accompany staphylococcal infection of any body part.
Acute S. osteomyelitis, usually in the bones of the legs, most commonly affects boys between ages 3 and 10 years, most of whom have a history of infection or trauma. Osteomyelitis presenting in the vertebrae affects adults older than age 50 years, often following staphylococcal infections of the skin or urinary tract, after prostatic surgery, or after pinning of a fracture. Clinical manifestations include abrupt onset of fever, shaking chills, pain and swelling over the infected area, restlessness, and headache (see the section on Osteomyelitis in Chapter 25).
Staphylococcus-associated skin infections include cellulitis (see the section on Cellulitis in Chapter 10), boil-like lesions (furuncles and carbuncles), and small macules that may develop into pus-filled vesicles. Associated symptoms may include mild or spiking fever and malaise. Scalded skin syndrome is typically seen in infants with exfoliation of skin secondary to staphylococcal-produced toxins.
CoNS is most often associated with prosthetic device infections: prosthetic cardiac valves and joints, vascular grafts, intravascular devices, and CNS shunts.96 CoNS does not typically produce fulminant symptoms. Individuals may present with mild fever, pain, and slightly elevated leukocytosis with a subtle course of illness.
MEDICAL MANAGEMENT
DIAGNOSIS, TREATMENT, AND PROGNOSIS.
Gram stain and culture of the organism from the infected site, blood, or other fluid is usually diagnostic; antibiotic sensitivity testing is important. Polymerase chain reaction (PCR)–based assays are becoming more available for rapid diagnosis of S. aureus, especially in areas where resistance is high. Since CoNS is ubiquitously found on the skin and is a common contaminant, the isolation of CoNS does not always indicate infection. In fact, blood cultures positive for CoNS are truly positive in only 10% to 25% of isolates.96
Isolation of S. aureus in blood cultures usually confirms bacteremia, and several positive blood cultures can be diagnostic of endocarditis in the presence of a new murmur or echocardiogram demonstrating valvular vegetations. Treatment may include drainage of any abscesses, removal of prosthetic devices, administration of antibiotics, and supportive therapy for the specific type and site.
MRSA is resistant to available antimicrobials except vancomycin, making vancomycin the preferred drug for staphylococcal infections, especially nosocomial ones. Reports of reduced susceptibility to vancomycin among strains of S. aureus (VISA strains) are on the rise.23,149
New classes of antistaphylococcal drugs have been developed to combat the multidrug-resistant S. aureus. Combinations of drugs have also been used to create multifaceted attacks to decrease resistance development.
Debate continues on the efficacy of preventing S. aureus using topical antimicrobial ointments to eradicate colonization in high-risk individuals. Studies are underway to develop an effective vaccine to prevent S. aureus. Although it may be several years before vaccines against S. aureus are available for human beings, immunization may represent an important step toward solving the problem of antimicrobial resistance.110
Prognosis is good with treatment, although antibiotic-resistant strains are increasingly associated with morbidity and mortality. Infective endocarditis with S. aureus remains a serious life-threatening illness, with 20% to 40% mortality. Visceral abscesses, osteomyelitis, and staphylococcal sepsis are illnesses that are potentially lethal.
Streptococcal Infections
Group A Streptococci.: Streptococcus pyogenes, the prototype of group A streptococci (GAS), is one of the most common bacterial pathogens of human beings of any age. It causes many diseases of diverse organ systems, ranging from skin infections to acute self-limited pharyngitis to postinfectious syndromes of rheumatic fever and poststreptococcal glomerulonephritis (Box 8-7).
The diseases caused by S. pyogenes may be considered in two categories: suppurative (formation of pus) and nonsuppurative. Suppurative diseases occur at sites where the bacteria invade and cause tissue necrosis and pus formation, inciting an acute inflammatory response. By contrast, nonsuppurative diseases are immune related and triggered by previous streptococcal infection.
GAS is typically transmitted via contact with respiratory droplets, although other, less-common mechanisms have been identified, such as foodborne. In health care settings, personnel may spread GAS after contact with clients who have infected secretions or may become infected themselves. The infected personnel subsequently acquire a variety of GAS-related illnesses (e.g., toxic shock–like syndrome, cellulitis, and pharyngitis).
HCWs who are GAS carriers have infrequently been linked to sporadic outbreaks of surgical site, postpartum, or burn wound infection and to foodborne transmission of GAS causing pharyngitis. Adherence to standard precautions or other transmission-based precautions can prevent nosocomial transmission of GAS to personnel. Restriction from client care activities and food handling is indicated for personnel with GAS (see Table 8-5).
Signs, symptoms, and complications of GAS depend upon the location of the infection.
Streptococcal Pharyngitis.: Streptococcal pharyngitis, commonly known as strep throat, occurs most commonly in children and accounts for 15% to 36% of all sore throats in children.87 It is also the only pharyngitis requiring antibiotic treatment. The infection occurs most commonly from October to April in children aged 5 to 10 years, but a recent increase has occurred among adults aged 30 to 50 years. This organism often colonizes in throats of people with no symptoms; up to 20% of schoolchildren may be carriers (pets may also be carriers).
The incubation stage is 1 to 5 days. Clinical manifestations vary but may include a fever, sore throat with pain on swallowing (may be severe), beefy red pharynx, edematous tonsils with exudate, swollen lymph nodes along the jaw line, generalized malaise and weakness, anorexia, and occasional abdominal discomfort (particularly in children). Up to 40% of affected children may have symptoms too mild for diagnosis.
Complications have significantly been reduced with the advent of antibiotics but may include otitis media, sinusitis, peritonsillar or retropharyngeal abscess, bacteremia, endocarditis, meningitis, pneumonia, and osteomyelitis. Poststreptococcal sequelae include acute rheumatic fever or acute glomerulonephritis. Diagnosis is usually by rapid diagnostic kits, but if negative a throat culture (the gold standard) should be performed. Treatment is with antibiotics to avoid poststreptococcal syndromes.
Scarlet Fever.: Scarlet fever usually follows untreated streptococcal pharyngitis but may also occur after wound infections. It is caused by a streptococcal strain that releases a pyogenic exotoxin and is most common in children aged 2 to 10 years old.
The streptococcus is acquired by inhalation or direct contact with oral secretions and presents with a sore throat, fever, strawberry tongue (white-coated tongue with prominent red papillae), and a fine erythematous rash that blanches on pressure and has been described as feeling like sandpaper. The rash first appears on the upper chest and then spreads to the extremities, sparing the soles and palms. After 6 to 9 days there may be desquamation of the skin of the soles and palms. The cheeks may be flushed, with pallor around the mouth. Rarely complications may include high fever, arthritis, and jaundice.
Impetigo.: Impetigo is principally caused by GAS, although other streptococcal or staphylococcal species may be involved. It occurs most commonly in children aged 2 to 5 years, especially in hot, humid weather. Predisposing factors include close contact in schools, overcrowded living quarters, poor skin hygiene, and minor skin trauma.
Colonization with GAS most often precedes the skin lesions, so good hygiene is essential. Small macules appear and rapidly develop into vesicles that become pustular and encrusted. Neither fever nor pain is typically a component of impetigo and if present suggests another diagnosis.
Scratching spreads infection and may develop into lymphadenitis or cellulitis. Lesions often affect the face although any area of the skin can be involved (see Chapter 10). Antibiotic treatment should cover both staphylococcal and streptococcal species. Untreated skin infections do not lead to rheumatic fever, although they can trigger poststreptococcal glomerulonephritis.
Erysipelas.: Streptococcal species and other organisms (such as S. aureus) may cause a type of cellulitis that may cause an acute infection of the skin accompanied by fever and chills. The skin may be very red, shiny, and swollen in appearance (Fig. 8-3). This type of cellulitis develops over a few hours; bullae may form in the affected areas after 2 to 3 days. The margins between normal and infected skin are well demarcated.
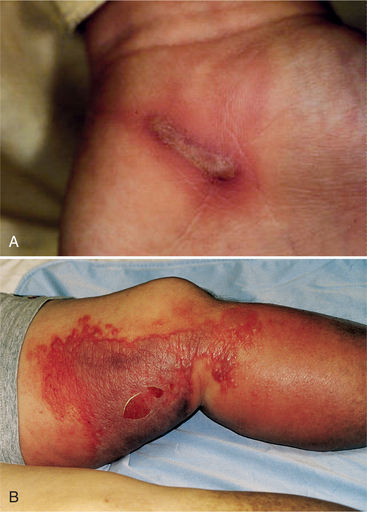
Figure 8-3 Cellulitis and lymphangitis. A. Infection in a wound is usually due to streptococcal bacteria, but often in combination with Staphylococcus. Infection can be local without streaking (cellulitis), local infection with streaking toward the heart (lymphangitis or blood poisoning), or pus forming (boil or abscess). This boy stuck a needle into a burn blister on his palm the previous day. Note the redness and the streaking. B, Erysipelas, a type of cellulitis, is more of a clinical diagnosis describing an infectious skin condition characterized by sharp, elevated, demarcated borders; redness; swelling; vesicles; bullae; fever; pain; and lymphadenopathy. Erysipelas affects the face and legs most often. It is almost always caused by GAS but can be caused by Staphylococcus. (A, Courtesy Bruce Argyle, Utah Mountain Biking, http://www.utahmountainbiking.com/firstaid/infect.htm. B, Reprinted from Black JM, Hawks JH: Medical-surgical nursing: clinical management for positive outcomes, ed 7, Philadelphia, 2006, W.B. Saunders.)
The most common areas affected include the face and legs, although erysipelas can occur anywhere. The disease is more common in women and may be especially severe in anyone with a debilitating condition.66 Antibiotics that cover GAS are the treatment of choice but may need to be broadened to include staphylococcal species.
Streptococcal Cellulitis.: Streptococcal cellulitis, an acute spreading inflammation of the skin and subcutaneous tissues, usually results from infection of burns, wounds, or other breaks in the skin, although in some cases no entry site is noted. Recurrent episodes of cellulitis may occur in extremities in which lymphatic drainage has been impaired (e.g., postaxillary node dissection, site of saphenous vein harvest).
Lymphangitis may accompany cellulitis or may occur after clinically minor or unapparent skin infection. Lymphangitis is readily recognized by the presence of red, tender, linear streaks directed toward enlarged, tender regional lymph nodes. It is accompanied by systemic symptoms such as chills, fever, malaise, and headache (see the sections on Cellulitis in Chapter 10 and Lymphangitis in Chapter 13).
Streptococcal Necrotizing Fasciitis.: Necrotizing fasciitis (NF) is a serious infection that progresses rapidly along fascial planes, usually in the legs, causing severe tissue damage as it spreads. The classification of soft-tissue necrotizing infections has changed over the years, and NF was previously known as streptococcal gangrene. There are different types of NF caused by various organisms but they often have overlapping features.
One classification separates NF into type I and type II. Type I is a polymicrobial infection that typically occurs following surgery when protective mucosa of the GI or genitourinary tract is damaged or when seeding occurs from an occult abscess. Gas formation may also form. S. pyogenes accounts for more than 60% of type II NF and often originates from a distal break in the skin or transient bacteremia. NF is a rare but serious complication of chickenpox and should be suspected in children with progressive pain, fever, and lethargy.30
NF may be difficult to diagnose initially. Pain and fever are present but the overlying skin often is without abnormalities. The infection spreads rapidly, causing edema and tenderness. Changes later occur in the skin as thrombosis of blood vessels occurs. The skin turns a dark red color with accompanying induration. Bullae form and fill with dark fluid. Later the skin becomes friable and turns a maroon or black color consistent with ischemia.
The bacteria produce several pyogenic endotoxins, causing severe breakdown of tissue in multiple organs. At least 50% of affected individuals experience toxic shock syndrome with hypotension, nausea, vomiting, and delirium.69 There is often renal and hepatic compromise as well as pulmonary infiltrates, leading to respiratory distress. Mortality rate is high (30% to 70%).
Immediate surgery with aggressive debridement of all necrotic tissue along with appropriate intensive IV antibiotics are essential to save muscles and limbs.141 Gram stain and culture of the site is essential to identify the organism(s) and antimicrobial susceptibility. Multiple procedures and serial debridement may be necessary with secondary closure since the demarcation line of infection is difficult to identify.
Gram stain is a laboratory staining technique used to distinguish between two groups of bacteria by identifying differences in the structure of their cell walls. The Gram stain was named after Danish bacteriologist Christian Gram, who developed this technique. Gram stain has become an important laboratory tool, distinguishing between so-called gram-positive bacteria, which remain colored after the staining procedure, and gram-negative bacteria, which do not retain dye.
Streptococcal Myositis.: Streptococcal myositis is a rare but potentially life-threatening entity characterized by severe pain and inflammation in the affected muscle with few abnormalities of overlying skin. Typically blunt, nonpenetrating trauma or hematologic seeding of bacteria to the muscle leads to the infection. Two forms of streptococcal myositis have been reported. The first is a slower, less-virulent process, while the second is more fulminant with systemic symptoms, high fever, bacteremia, and a high mortality rate.163
This condition can also be caused by other bacteria (usually S. aureus), mycobacteria, fungi, viruses, and protozoan forms. Clinical features of myositis and NF often overlap. Therapy includes aggressive surgical debridement and IV antibiotics (see the section on Myositis in Chapter 25 and Streptococcal Gangrene in this chapter).
Puerperal Sepsis.: Puerperal sepsis follows abortion or normal delivery when streptococci colonizing the woman or transmitted from medical personnel invade the endometrium and surrounding structures, lymphatics, and bloodstream. The resulting endometritis and septicemia may be complicated by pelvic cellulitis, septic pelvic thrombophlebitis, peritonitis, or pelvic abscess. Before the antibiotic era and the benefits of handwashing between clients were known, this disease was more common and associated with a high mortality rate.