chapter 2 Biological and Social Theories of Aging
Megan is a certified occupational therapy assistant (COTA) employed in an assisted living center that offers several levels of care. Her daily work involves treating elders who have a variety of diagnosed conditions and the planning of occupation-based activities. Megan has observed that although many of the elders require rehabilitation, each reacts differently to illness and the aging process. At least once a week, Megan meets with Kelly, a registered occupational therapist (OTR), for a supervision session in which they thoroughly discuss each person participating in occupational therapy (OT).
After reviewing the caseload during one particular session, Megan and Kelly began a lively discussion about the complexities of aging. Megan noted that some of the elders whom she treats as part of her caseload seem active and vigorous, whereas others seem withdrawn and lack energy to participate in therapeutic tasks. She also commented that some of the elders seem older than their chronological ages, whereas others seem to be their age or younger. Kelly encouraged Megan to review theories about aging to form a context in which to think about the elders. The next week Megan and Kelly discussed the application of the theories to their work with elders who are part of their caseloads.
Questions like Megan’s regarding reasons for aging and the differences in aging can be answered in multiple ways because aging research consists of many different studies and perspectives. COTAs need to understand various theories because the theoretical concepts attempt to go beyond the data to the fundamental biological, social, or psychological processes. Furthermore, theories explain what is observed or experienced and why and how it is important.1 A growing trend over the last 10 years has been interdisciplinary collaboration to merge profession-specific concepts into a unified theory to explain the aging phenomena.
This chapter uses the format of current biological, social, and psychological theories to provide insight on social aspects of aging. (The physical and psychological changes that occur with the aging process are described in Chapters 3 and 4.)
Biological Theories of Aging
As many as 300 or more aging theories have been presented in the literature over the past several decades; however, not all have stood up to scrutiny and in-depth scholarly investigation.2 The major biological theories that attempt to explain the individual differences in aging fit into one of two categories: genetic aging, which presumes that aging is predetermined or programmed, and nongenetic aging, which presumes that aging events occur randomly and accumulate with time.3,4 Four genetic aging theories are programmed aging, somatic mutation, free radical, and neuroendocrine theories. A nongenetic theory is the wear and tear theory. One or multiple theories may explain the aging process and characteristics as a wide range of factors that may affect aging such as genetics, random events, environment, lifestyle, and/or habits.
Genetic Theories
Programmed aging
The premise of the programmed aging theories is that the human body has an inherited internal “genetic clock” that determines the beginning of the aging process. This genetic clock may manifest as a predetermined or limited number of cell divisions, called the Hayflick limit (also known as replicative senescence or cellular senescence).5-8 The Hayflick limit does not affect all cells in the body as germ cells (sperm or egg), and cells in some tumors (cancer) seem to divide infinitely.7,9 The theory of cellular aging explains why many older adults have one or multiple conditions related to decreased or impaired client factors (sensory, neuromusculoskeletal, cardiovascular, respiratory, digestive, metabolic, and reproductive) and why it is rare to find any of these impairments in a young adult.10 The perception that cellular senescence is not programmed aging of the whole person explains why such conditions are not universal among older adults.7
Somatic mutation theory
According to the somatic mutation theory, stochastic (random) chromosomal changes occur as a result of miscoding, translation errors, chemical reactions, irradiation, and replication of errors; these mutations result in changes in the ribonucleic acid (RNA) deoxyribonucleic acid (DNA) code sequences.7,9,11 Mutations of the genetic material within a cell can accumulate if the alterations are not repaired when the code is being transcribed (reading process to make the building blocks of proteins).8 The accumulation of mutations can alter the genetic sequence of a cell in such a way that the “safe guard” to control the proliferation of cellular growth is deactivated, resulting in unrestrained cell division, sometimes leading to tumorigenesis and/or cancer.9,12 Mutations can occur in the expression of the genetic code or the way that the code is read without directly changing the RNA or DNA sequence; the expression of the genetic code is the epigenome, and the mutations are epimutations.7,13
Free radical theory
The free radical theory of aging stemmed from the study of unstable atoms in living cells and the damage they caused as they tried to stabilize.14,15 Free radicals are highly reactive because of the unpaired electron(s) that seek to be paired but, in turn, damage cells, proteins, lipids, and DNA (by altering their structures).16 Free radicals happen naturally in the body whenever metallic ions, enzymes, or cellular materials combine with oxygen and are also introduced into the body through toxins, pollutants, and tobacco smoke. Low-level, free radical damage is theorized to accumulate over time, especially mutations in mitochondrial DNA (mtDNA), resulting in aging characteristics.16,17 Most organisms have defense mechanisms to limit the effects of free radicals and to repair the damage left behind, but because not all of the repairs can be fixed, the damage accumulates.11,15 The accumulated mutations of the mtDNA result from a decrease in or loss of function of the natural antioxidant defense layer in the body and cells. However, Harman17 highlights some studies that show a decrease in the loss of mtDNA through the consumption of coenzyme Q10 and other antioxidants such as Ginkgo biloba. Ames18 discusses the importance of nutrient balance, specifically of iron, copper, zinc, vitamin B6, biotin, and pantothenate. Too much of these nutrients tend to increase oxidative stress and mtDNA damage. However, these nutrients are important for mtDNA repair and cellular function, so too little of these nutrients decreases function and the repair of oxidative damage. The direct effect of the free radical theory on aging and dysfunction continues to be questioned and studied, but it is clear that the presence of oxidative damage from free radicals increases through the life span.15,16
Neuroendocrine theory
The neuroendocrine theory suggests that the central nervous system is the aging pacemaker of the body.19,20 Modification of metabolism or reproductive function affects the life span, and the hypothalamus is predicted to be one possible starting point for neuroendocrine-related changes because it influences the regulation of the metabolic and reproductive systems.20
Nongenetic Theory
Wear and tear theory
The wear and tear theory proposes that cumulative damage within the body leads to the death of cells, tissues, organs, and, finally, the organism.21 Wear and tear are natural from living things to inanimate objects, and organisms are able to repair wear and tear.21 The wear and tear theory is studied with identical twins. Identical twins are nature’s natural clones in that they have identical genotypes (genetic information); however, upon closer inspection there are phenotypic (physical) differences.22 It was found that epigenetic differences were greater between older monozygotic twins than younger pairs, even if external variables were almost identical.22 Cases in which the time of death varies between twins indicate that environmental factors may be as important as genetic factors in determining life span.23 Therefore, it can be concluded that internal and external factors play roles in aging and, like other biological aging theories, wear and tear within the body accumulate through the years.21,22
Social Theories of Aging
Longer life spans and an increased number of elders in U.S. society have resulted in greater attention to the aging process. Quality of life and successful aging are becoming important areas of study. The disengagement, activity, and continuity social theories each present a different process of aging and focus on different aspects of successful aging. The next three social theories, which consist of Erikson’s and Peck’s stages of psychological development and the life course, place more emphasis on the developmental stages of aging. The last social theory of aging, the theory of exchange, examines perceptions regarding the value of interactions and the ways that these perceptions affect elders’ relationships.
Researchers on the major social theories of aging—activity theory, disengagement theory, and continuity theory—have not consistently demonstrated accuracy in identifying behaviors at various stages. The disengagement theory, activity theory, and continuity theory seem to manifest from each other as elaborations or “glass half full” versus “glass half empty” arguments,24 as the following discussion illustrates.
Disengagement Theory
Disengagement occurs when people withdraw from roles or activities and reduce their activity levels or involvement.25 While completing an interest checklist with the COTA, an elder might indicate former activities and roles with various social clubs or organizations that they found meaningful.10 When asked for the reason for withdrawal from these activities, the elder might state that it was because of age. On the basis of their research in Kansas City, Missouri, in the 1950s, Cumming and Henry26 theorized that the turning inward typical of aging people produces a natural and normal withdrawal from social roles and activities, an increasing preoccupation with self, and decreasing involvement with others. They perceived individual disengagement as primarily a psychological process involving withdrawal of interest and commitment. Social withdrawal was a consequence of individual disengagement, coupled with society’s push for the withdrawal of the elderly manifested in such things as retirement plans and pensions.25
The disengagement theory resulted in increased research. The proposition of withdrawal being normal challenged the conventional wisdom that keeping active was the best way to deal with aging. Streib and Schneider27 suggested that differential disengagement was more likely to occur than total disengagement. For example, people may withdraw from some activities but increase or maintain their involvement in others. Troll28 found that elders often disengage into the family—that is, elders often cope with lost roles by increasing involvement with their families. Atchley and Barusch29 present that disengagement can also be due to increased frailty or disability such as decreased visual acuity, so elders choose not to attend sports events but rather stay home to hear the news cast of the events. People are seldom completely engaged or disengaged. Rather, they strike a balance between the two states that reflects their individual preferences, often mediated by social encouragement or discouragement from others.
The frequency of disengagement is very much the product of the opportunity for continued engagement. For example, elders may wish to continue many activities, but, because they believe that other people may think they are “too old,” they withdraw. For elders in facilities who think they are too old or unable to continue activities, the COTA could discuss with them doing activities that would be similar to former interests. For example, if elders are interested in gardening, they could assist with the plants in and out of their residence. If elders are interested in communicating with friends, perhaps an introduction to e-mail would be a meaningful activity.
Activity Theory
The activity theory was proposed as an alternative view of the disengagement theory to explain the psychosocial process of aging.24 Havighurst, Neugarten, and Tobin30 articulated an activity theory of aging, which held that unless constrained by poor health or disability, elders have the same psychological and social needs as people of middle age. Hochschild31 presented that the changing of activities was the result of changed meaning in the activities as seen through the life span. An example is parents regularly attending PTA meetings for their child’s school. As the child grows and moves away, the parents begin to read more because there is no longer meaning in the PTA meetings. Thus, the adults embrace the activity of reading for pleasure without the need to monitor children.10 Menec32 purported “different types of activities may have different benefits. Whereas social and productive activities may afford physical benefits, as reflected in better function and greater longevity, more solitary activities, such as reading, may have more psychological benefits by providing a sense of engagement with life” (p. 74).
The activity theory has received a great deal of criticism in that it excludes elders’ physical well-being, past lifestyle, and personality attributes. It also does not account for the value or the personal meaning that the elder may find in activities. Instead, it most often quantifies the number of roles and the amount of involvement in these roles.25,33,34 In addition, the belief that it is better to be active than inactive is a bias derived from the Western culture.25,34 Much of OT is based on the assumption that our value of human beings comes from what we know and do, rather than on who we are and have been.10,35
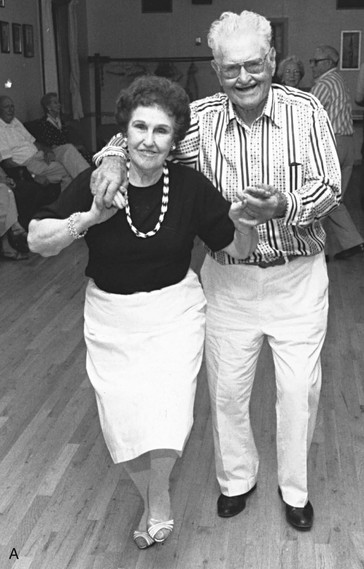
A further component of the activity theory considers the preferences of elders and the extent to which they wish to be active. Setting aside time for quiet reflection may be equally as important as more active pursuits for some elders. COTAs should remember this when attempting to get everyone involved in an activity. Some elders may welcome participation in physical activities such as bowling and walking (Figure 2-1, A), and others may be content with listening to quiet music and reading (Figure 2-1, B).

Continuity Theory
The premise of the continuity theory is that elders adapt to changes by using strategies to maintain continuity in their lives, both internal and external. Internal continuity refers to the strategy of forming personal links between new experiences and memories of previous ones.29,36,37 External continuity refers to interacting with familiar people and living in familiar environments.29,37,38 According to this theory, elders should continue to live in their own homes as long as possible. If this is not possible, the family should attempt to locate housing for the elder in the same general area to maintain friendships and familiar environments. Many elders continue to be independent as long as they are in familiar surroundings. Some families have noted that once they moved their elder family member from a familiar area, the elder was confused and disoriented.
Continuity of activities and environments helps the individual concentrate energies in familiar areas of activity. Practice of activities can often prevent, offset, or minimize the effects of aging. Atchley and Barusch29 state that by maintaining the same lifestyle and residence, an older person is able to meet instrumental activities of daily living needs. Continuity of roles and activities is effective in maintaining the capacity to meet social and emotional needs for interaction and social support. Maintaining independence is important for continued good self-esteem. Continuity does not mean that nothing changes; it means that new life experiences occur, and the elder must adapt to them with familiar and persistent processes and attributes. New information is likely to produce less stress when an elder has memories of similar experiences. This may be one reason new information does not have the same weight for both younger and older generations and may help explain the reason that some elders seem more conservative than others. For example, an elder may reject learning to use a computer to order home supplies and to be in contact with others despite being isolated in a rural location because the activity involves a new way of performing a task.
Practice should not be based on one theory but a combination of theories as they apply and are appropriate to our clients. For instance, it may be dangerous to allow an elder to withdraw by considering it a normal function of aging or to push meaningless activity with a disinterested elder. COTAs may want to discuss with elders what activities have meaning to them and allow elders to reminisce about past activities, or perform client-centered assessments such as an interest checklist or the Canadian Occupational Performance Measure.39 The information gleaned from the individual could give COTAs more insight into a selection of activities that are most appropriate.
The activity and continuity theories are compatible with OT in that they assume that performance of meaningful activities promotes competence, independence, and well-being. Kielhofner40 states that human beings are occupational in nature; therefore, occupation is vital for our well-being. The Model of Human Occupation incorporates this assumption and is a valuable theory of OT for aging.40 What a person does depends on individual factors such as level of interest, values, personal causation, health, socioeconomic status, and prior occupations.
Life Span/Life Course Theory
The life span, or life course, perspective is a recent approach to human development by theorists interested in the social and behavioral processes of aging (Box 2-1). Life course is defined by Elder, Johnson, and Crosnoe41 as “an age-graded sequence of socially defined roles and events that are enacted over historical time and place” (p. 15). This theory was influenced by the age stratification model, which emphasizes the significant variations in elders, depending on the characteristics of their birth cohort. Some researchers believe that this is not actually a theory, but rather a conceptual framework for conducting research and interpreting data.
BOX 2-1
Key Elements of the Life Span Framework

From Passuth, P., & Bengtson, V. (1988). Sociological theories of aging: Current perspectives and future directions. In J. Birren & V. Bengtson (Eds.). Emergent Theories of Aging. New York: Springer.
Most elders who experienced the Great Depression seem to have a different perception of the meaning of “poor.” Many elders reject offers of help because they compare what little they had in the past with what they currently have, which seems sufficient. In addition, some elders who are eligible for Social Security insurance may not accept it. This viewpoint may vary with subsequent generations of elders.
Elder, Johnson, and Crosnoe41 reported considerable consensus on age-related progression and sequence of roles and group memberships that individuals are expected to follow as they mature and move through life. The stages of the adult life course as defined by this group are middle age, later maturity, and old age. Unlike Erikson’s and Peck’s stages, life course stages are related to specific chronological ages. Age norms generally define what people within a given life stage are “allowed” to do and be at certain ages. Many norms are established by long traditions. Others are often the result of compromise and negotiation. In addition, a series of assumptions related to the capabilities of the people in a given life stage underlies age norms. Thus, opportunities may be limited for some elders because others assume they are not strong enough or lack education or experience.29,38 Elders who achieve greatness beyond expectations for their life stages are perceived as unique or different. Their accomplishments elicit comments about their endeavors being met by a person of “their age.” Many older elders, such as the current group of centenarians, are considered pioneers because few prescribed behaviors or age norms exist for them. Franklin and Tate24 stated, “A large body of research and theoretical literature confirms that physical, cognitive, and social functioning, broadly speaking, are key factors of successful aging and that multiple lifestyle choices, behaviors, and psychosocial factors influence them” (p. 8).
Erikson’s Theory of Human Development
Erik Erikson’s theory of human development over the life span is one of the most influential descriptions of psychological change.21,42 Erikson’s stages of ego development are familiar to most students of psychology (Table 2-1).
TABLE 2-1 Erik Erikson’s Stage of Ego Development
| Time period | Stage |
|---|---|
| Early infancy | Trust versus distrust |
| Later infancy | Autonomy versus shame and doubt |
| Early childhood | Initiative versus guilt |
| Childhood middle years | Industry versus inferiority |
| Adolescence | Ego identity versus role confusion |
| Early adulthood | Intimacy versus isolation |
| Middle adulthood | Generativity versus stagnation |
| Late adulthood | Ego integrity versus ego despair |
From Erikson, E. (1985). Childhood and Society. New York: WW Norton.
Erikson’s framework addresses the developmental tasks at each stage of the life cycle. The stage most commonly identified with aging is that of integrity versus despair. In this stage, the elder comes to terms with the gradual deterioration of the body but at the same time may reflect on the acquisition of wisdom associated with life experiences. Ego integrity involves the elders’ ability to see life as meaningful and to accept both positive and negative personality traits without feeling threatened. Integrity provides a basis for elders approaching the end of life with a feeling of having done their best under the circumstances. Despair is the elder’s rejection of self and life experiences, and it includes the realization that there is insufficient time to alter this assessment. The despairing elder is prone to depression and is afraid to die. COTAs can play a vital role in assisting elders to master this developmental stage. Helping elders develop self-empathy, the ability to bounce back from change, and a focus on the completeness of their lives supports elders’ efforts to deal with this life stage.
Erikson originally proposed eight stages of psychosocial development. As Erikson himself reached later life, he noted that the predominant image of old age was quite different from when he had first formulated his theory. To fit with the increasingly older population, Joan M. Erikson43 published a ninth stage of development. This ninth stage, applicable to elders in their eighties and nineties, enhanced her husband’s well-known eight-stage theory of development.43,44 It is felt that in the ninth stage elders may also revisit unresolved crisis issues from earlier stages in a different manner. For example, elders in the ninth stage may perceive the first stage of trust versus mistrust as trust in their own physical and mental abilities with functional activities.43 Erikson also discusses the concept of gerotranscendence in which elders deal with their aging selves and consider life satisfaction as they move beyond materialistic concerns to spiritual or as Lars Tornstam stated, “cosmic and transcendent” thoughts.45
Brown and Lowis44 purported that the results of surveying individuals near or in the ninth stage showed a sense of peace and acceptance, decreased fear of death, closeness to those who have gone before, acceptance of the age-related changes, and increased understanding of the meaning of life. Reminiscence groups and other life review activities conducted as part of an intervention program by COTAs can be effective in helping elders work through developmental stages.
As increasing numbers of people reach very old age, tasks and other aspects of psychosocial development that were not systematically described in Erikson’s original formulations are emerging. Positive resolution of crisis is the elder’s confidence in the continuity of a personal contribution beyond death. For example, an elder who handcrafts rocking chairs may pass on those skills to children, who may pass them on to their children. Tasks of this stage include coping with the inevitable physical changes that accompany aging. The elder may be increasingly obliged to turn attention from the more interesting aspects of life to the demands of the body. In addition, the very old may have to shape new patterns for adapting to late life because few norms for behavior and few responsibilities are established for elders who reach a very old age. Numerous articles on persons older than 100 years show a fascination with the many activities of this fastest growing age group. Most of these elders attribute their longevity to keeping their minds, not their bodies, stimulated.46,47
Peck’s Stages of Psychological Development
Robert Peck48 believed that Erikson’s eighth stage, integrity versus despair, was intended to “represent in a global, nonspecific way all of the psychological crises and crisis-solutions of the last forty or fifty years of life” (p. 88). He suggested that it might be more accurate and useful to take a closer look at the second half of life and divide it into several different psychological stages and adjustments (Table 2-2).
TABLE 2-2 Robert Peck’s Psychological Stages in the Second Half of Life
| Time period | Stage | |
|---|---|---|
| Middle age | First stage | Wisdom versus physical powers |
| Second stage | Socializing versus sexualizing | |
| Third stage | Cathectic flexibility versus cathectic impoverishment | |
| Fourth stage | Mental flexibility versus mental rigidity | |
| Old age | First stage | Ego differentiation versus work-role preoccupation |
| Second stage | Body transcendence versus body preoccupation | |
| Third stage | Ego transcendence versus ego preoccupation | |
From Peck, R. (1968). Psychological developments in the second half of life. In B. Neugarten (Ed.). Middle Age and Aging. Chicago: University of Chicago Press.
Peck48 proposed four stages that occur in middle age and three stages in old age. He avoided establishing a chronological period for these stages, suggesting instead that they might occur in different time sequences for different individuals.
The first stage of old age is ego differentiation versus work-role preoccupation. The effect of retirement, particularly for men in their late sixties, is the issue at this stage. In U.S. culture, identity tends to be tied to the individual’s work role. Retiring individuals must reappraise and redefine their worth in a broader range of role activities (Figure 2-2, A). Retirement also affects women, regardless of whether their careers were inside or outside of the home. As more working women from the Baby Boomer generation retire, it will be interesting to see how they redefine their roles. The housewife’s work role changes drastically when the husband retires and is suddenly always in “her” domain (Figure 2-2, B). With economic downturns and policy changes associated with the Social Security Act, this stage may move to later years as more elders remain or return to the workforce (see the discussion on elders in the workforce in Chapter 1).
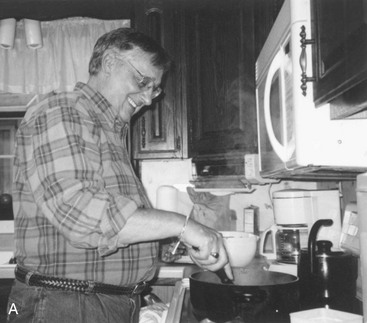

FIGURE 2-2 Changing roles. A, This retired man enjoys his new role as he prepares the family meal. B, The housewife’s work role can change when the husband retires and is suddenly in “her domain.”
(A Courtesy of Sue Byers-Connon, Mt. Hood Community College, Gresham, OR.)
Peck48 states that a critical requisite for successful adaptation to this stage may be the establishment of varied sets of valued activities and self-attributes. These activities and attributes allow the individual to have satisfying and worthwhile alternatives to pursue. Participation in voluntary organizations, such as the AARP, formally the American Association of Retired Persons, can provide meaningful activities. Involvement in the AARP can be initiated as early as 50 years of age and continues after the formal work role has ended. This organization provides opportunities for driver refresher courses through AARP Driver Safety, help with filing of tax returns through AARP Tax-Aide, travel at reduced cost, and many other discounted products and services. In addition, it offers medical insurance plans to supplement private insurance and Medicare and the choice to become a volunteer advocate for improved health care, long-term care, consumer protection, financial and retirement security, transportation, housing, and other areas (Lanner, April 7, 2010, personal communication).
Peck’s second stage of old age is body transcendence versus body preoccupation. Physical decline, along with a marked decline in recuperative powers and increased body aches and pains, occurs in many elders in this stage. To those who especially value physical well-being, this may be the most difficult period of adjustment. For some elders, this adjustment means a growing preoccupation with their bodily functions. However, others have learned to define comfort and happiness in human relationships or creative mental activities. For them, only complete physical destruction can deter these feelings.
The third stage is ego transcendence versus ego preoccupation. With this stage of old age comes the certain prospect of death. Successful adaptation is not compatible with passive resignation or ego denial. It requires deep, active effort on the part of the elder to make life more secure, meaningful, and happy for those who will live after the elder’s death. These elders experience a gratifying absorption in the future and are interested in doing all that is possible to make the world better for familial or cultural descendants. In practice COTAs may work with elders to do life review activities, such as developing a video to leave for future generations.
Exchange Theory
In clinical practice the OT practitioner may find it more rewarding to work with an elder who is motivated and has a “fun” personality than with an elder who does not relate well with others. COTAs may observe that the client who displays a winning personality receives more attention from everyone. This is an example of exchange theory.
Exchange theory, as originally developed by Homans,49 assumes that people attempt to maximize their rewards and minimize their costs in interactions with others. The major attempts to use exchange theory in work with elders are attributed to Dowd.50,51 Elders are viewed from the perspective of their ongoing interactions with a number of persons. Continuing interaction is based on what the elder perceives as rewarding or costly. Elders tend to continue with interactions that are beneficial and withdraw from those perceived as having no benefit. Rewards may be defined in material or nonmaterial terms and could include such components as assistance, money, information, affection, approval, property, skill, respect, compliance, and conformity. Costs are defined as an expenditure of any of these.
In American culture, more emphasis is often placed on resources a person is assumed to have rather than on the actual exchange resources. The concept of ageism includes assumptions about elders, such as that elders have less current information, outdated skills, and inadequate physical strength or endurance. If elders are perceived as having few resources to contribute to a relationship, an issue over power can result, with the elder at a distinct disadvantage. Elders may be seen as powerless actors who are forced into a position of compliance and dependence because they have nothing of value to withhold to get better intervention.29,38 Many elders accept the validity of these assumptions and fear dependency on others more than death.52
Thriving: A Holistic Life Span Theory
For several years, gerontologists have become concerned with failure to thrive in elders, which is a sharp decline for no real physical or illness-related reason. A nursing research group was brought together to explore the phenomenon. The group broadened its vision from the syndrome failure to thrive to a more holistic life span concept called thriving. This theory seems quite applicable to our OT approach because we profess to view our clients holistically. This theory considers three interacting factors in a continuum: the person, the human environment, and the nonhuman environment. Critical to thriving are “social connectedness, ability to find meaning in life and to attach to one’s environment, adaptation to physical patterns, and positive cognitive/affective function” (p. 22).53
1. Scenario one: Ethel Shanas, a very famous gerontologist, once said that if you want to live a long time, you should choose your grandparents carefully. Which aging theory or theories support Dr. Shanas’ suggestion?
2. Scenario two: Megan, the COTA introduced at the beginning of this chapter, decided to include reminiscence and life review as part of her therapeutic interventions with elders in the nursing home. Which aging theory supports the selection of these activities?
3. Scenario three: The family of one of Megan’s elderly clients is upset because the elder insists on planning her own funeral and asking for specific clothes in which to be buried. In addition, she has made a list of all of her furniture and other property and has designated which of her children or grandchildren is to inherit these items. Although this client has accepted her terminal illness, her family has not. Which aging theory would Megan use to explain to the family what is happening with their relative?
4. Scenario four: Margaret’s children decide to move her away from her current home town to a new assisted living facility in the town where they reside. Since the move Margaret seems more depressed and is having difficulty adapting to her new living arrangements. What aging theory explains her behavior?
5. The risk for having cancer increases significantly as people grow older. Use an aging theory to explain a possible reason for this.
6. Dr. Alex Comfort, a famous gerontologist, suggested that 2 weeks is about the ideal time to retire. What does he mean by this statement? Discuss the theory that supports your suggestion.
7. Some older adults may become extremely depressed once they retire. What could you suggest, other than antidepressant medications that may improve their outlook on life? Discuss the theory that supports your suggestion.
8. An 80-year-old man recently made headlines because he entered the Boston marathon. Why did this make the news? How do cultural age norms influence the persistence of ageism?
9. An 85-year-old woman with severe Parkinson’s disease has requested that during her activities of daily living session the COTA help her dress herself and put on makeup. The woman’s doctor has suggested that she is “too old for rehab” and is thinking of discontinuing her OT. Justify her intervention with a theory, and then explain how you would convince the doctor that it is important.
10. According to the exchange theory, why does an elder feel dependent on his or her relatives?
1 Bengtson V.L., Silverstein M., Putney N., Gans D. Theorizing about age and aging. In Bengtson V.L., editor: Handbook of Theories of Aging, 2nd ed, New York: Springer, 2009.
2 Medvedev Z.A. An attempt at a rational classification of theories of ageing. Biological Reviews of the Cambridge Philosophical Society. 1990;65:375-398.
3 Abrams W., Beers M., Berkow R. The Merck Manual of Geriatrics. Whitehouse Station, NJ: Merck Research Laboratories; 1995.
4 Beers M.H., Berkow R., Bogin R.M., Fletcher A.J., Rahman M.I. The Merck Manual of Geriatrics, 3rd ed. Whitehouse Station, NJ: Merck Research Laboratories; 2000.
5 Hayflick L. Biological theories of aging. In: Maddox G., editor. The Encyclopedia of Aging. New York: Springer, 1987.
6 Hayflick L., Moorhead P. The serial cultivation of human diploid cell strains. Experimental Cell Research. 1961;25:585-621.
7 Kirkwood T.B.L. Time of Our Lives: The Science of Human Aging. Oxford: Oxford University Press; 1999.
8 Kirkwood T.B.L. Understanding the odd science of aging. Cell. 2005;120:437-447.
9 Campisi J., d’Adda D.F. Cellular senescence: When bad things happen to good cells. Nature Reviews: Molecular Cell Biology. 2007;8:729-740.
10 American Occupational Therapy Association. Occupational therapy practice framework: Domain and process, 2nd ed. American Journal of Occupational Therapy. 2008;62:625-683.
11 Holliday R. Aging: The Paradox of Life. Amsterdam: Springer; 2007.
12 Finkel T., Serrano M., Blasco M.A. The common biology of cancer and ageing. Nature. 2007;448:767-774.
13 Bird A. Perceptions of epigenetics. Nature. 2007;447:396-398.
14 Harman D. Aging: A theory based on free radical and radiation chemistry. Journal of Gerontology. 1956;11:298-300.
15 Shringarpure R., Davies K.J.A. Free radicals and oxidative stress in aging. In Bengtson V.L., Gans D., Putney N.M., et al, editors: Handbook of Theories of Aging, 2nd ed, New York: Springer, 2009.
16 Muller F.L., Lustgarten M.S., Jang Y., Richardson A., Van Remmen H. Trends in oxidative aging theories. Free Radical Biology & Medicine. 2007;43:477-503.
17 Harman D. Free radical theory of aging: An update. Increasing the functional life span. Annals of the New York Academy of Sciences. 2006;1067:10-21.
18 Ames B.N. Delaying the mitochondrial decay of aging. Annals of the New York Academy of Sciences. 2004;1019:406-411.
19 Cristofalo V. An overview of the theories of biological aging. In: Birren J., Bengtson V., editors. Emergent Theories of Aging. New York: Springer, 1988.
20 Finch C.E., Ruvkun G. The genetics of aging. Annual Review of Genomics & Human Genetics. 2001;2:435-462.
21 Moody H.R. Aging: Concepts and Controversies, 6th ed. Thousand Oaks, CA: Pine Forge Press; 2010.
22 Fraga M.F., Ballestar E., Paz M.F., Ropero S., Setien F., Ballestar M.L., et al. Epigenetic differences arise during the lifetime of monozygotic twins. Proceedings of the National Academy of Sciences of the United States of America. 2005;102:10604-10609.
23 Bank L., Jarvik L. A longitudinal study of aging human twins. In: Schneider E., editor. The Genetics of Aging. New York: Plenum Press, 1978.
24 Franklin N.C., Tate C.A. Lifestyle and successful aging: An overview. American Journal of Lifestyle Medicine. 2009;3(1):6-11.
25 Mabry B.J., Bengtson V.L. Disengagement theory. In: Palmore E.B., Branch L.G., Harris D.K., editors. Encyclopedia of Ageism. Binghamton, NY: Haworth Press, 2005.
26 Cumming E., Henry W. Growing Old. New York: Basic Books; 1961.
27 Streib G., Schneider C. Retirement in American Society. Ithaca, NY: Cornell University Press; 1971.
28 Troll L. The family of later life. Journal of Marriage and the Family. 1971;33:263.
29 Atchley R., Barusch A.S. Social Forces and Aging: An Introduction to Social Gerontology, 10th ed. Belmont, CA: Wadsworth/Thomson Learning; 2004.
30 Havighurst R., Neugarten B., Tobin S. Disengagement, personality, and life satisfaction. In: Hansen P., editor. Age with a Future. Copenhagen: Munksgaard, 1963.
31 Hochschild A.R. Disengagement theory: A critique and proposal. American Sociological Review. 1975;40:553-569.
32 Menec V.H. The relation between everyday activities and successful aging: A 6-year longitudinal study. The Journals of Gerontology: Series B. 2003;58(2):74-82.
33 Bonder B.R., Dal Bello-Haas V. Functional Performance in Older Adults, 3rd ed. Philadelphia: FA Davis; 2009.
34 Bonder B., Wagner M. Functional Performance in Older Adults. Philadelphia: FA Davis; 2001.
35 Rowles G. Beyond performance: Being in place as a component of occupational therapy. American Journal of Occupational Therapy. 1991;45:265-271.
36 Cohler B. Person narrative and life course. In: Baltes P., Brim O., editors. Life Span Development and Behavior. New York: Academic Press, 1982.
37 Atchley R. Continuity and Adaptation in Old Age. Baltimore: Johns Hopkins University Press; 1999.
38 Atchley R. Social Forces and Aging. Belmont, CA: Wadsworth; 1991.
39 Law M. Canadian Occupational Performance Measure, 4th ed. Ottawa, Canada: CAOT Publications ACE; 2005.
40 Kielhofner G. A Model of Human Occupation: Theory and Application, 4th ed. Baltimore: Lippincott Williams & Wilkins; 2007.
41 Elder G.H., Johnson M.K., Crosnoe R. The emergence and development of life course theory. In: Mortimer J.T., Shanahan M.J., editors. Handbook of the Life Course. New York: Springer, 2004.
42 Erikson E. Childhood and Society. New York: WW Norton; 1985.
43 Erikson J.M. The ninth stage. In: Erikson E.H., Erikson J.M., editors. The Life Cycle Completed. New York: WW Norton, 1997.
44 Brown C., Lowis M.J. Psychosocial development in the elderly: An investigation into Erikson’s ninth stage. Journal of Aging Studies. 2003;17:415-426.
45 Erikson J.M. Gerotranscendence. In: Erikson E.H., Erikson J.M., editors. The Life Cycle Completed. New York: WW Norton, 1997.
46 Stern C. Who is old? Parade. 1996;21:4.
47 Poon L.W., Jazwinski M., Green R.C., Woodard J.L., Martin P., Rodgers W.L., et al. Methodological considerations in studying centenarians: Lessons learned from the Georgia centenarian studies. In: Poon L.W., Perls T.T., editors. Annual Review of Gerontology and Geriatrics: Biopsychosocial Approaches to Longevity, Vol. 27. New York: Springer; 2008.
48 Peck R. Psychological developments in the second half of life. In: Neugarten B., editor. Middle Age and Aging. Chicago: University of Chicago Press; 1968:88-92.
49 Homans G. Social Behavior: Its Elementary Forms. New York: Harcourt Brace Jovanovich; 1961.
50 Dowd J. Aging as exchange: A preface to theory. Journal of Gerontology. 1975;30(5):584-594.
51 Dowd J. Exchange rates and old people. Journal of Gerontology. 1980;35(4):596-602.
52 Aitken M. Self concept and functional independence in the hospitalized elderly. American Journal of Occupational Therapy. 1982;36(4):243-250.
53 Haight B., Barba B., Tesh A., Courts N.F. Thriving: A life span theory. Journal of Gerontological Nursing. 2002;28(3):14-22.