chapter 1 Aging Trends and Concepts
1. Define relevant terminology regarding elders.
2. Describe the relation between aging and illness.
3. Discuss components of health and chronic illness.
4. Discuss a client-centered approach.
5. Describe the three stages of aging, and define their differences.
6. Describe the effects of growth of the elder population on society.
7. Discuss the effects of an increasingly large number of elder women on society.
8. Describe the problems and needs of the oldest old populations—that is, those elders 85 years and older, including the centenarians.
9. Describe living arrangements of elders and living trends, such as aging in place.
10. Discuss the significance of economic trends on the elderly.
11. Relate implications of demographical data for occupational therapy practice.
12. Discuss current trends impacting elders in America and implications for occupational therapy practice.
13. Describe the importance of intergenerational contact for occupational therapy intervention.
14. Explain the importance of understanding generational cohorts for intervention.
15. Describe the concept of “ageism” in today’s society and the effect of the views of the American youth culture on aging.
gerontology, geriatrics, cohort, health, illness, chronic illness, young old, mid old, old old, demography, trends, aging in place, intergenerational, generational cohorts (Traditionalists, Baby Boomers, Generation X, Generation Y), ageism
Eric is a 25-year-old certified occupational therapy assistant (COTA) practicing in a skilled nursing home facility. He provides daily occupational therapy (OT) intervention for 5 days a week. Most of the elders are in some stage of recovery from an acute illness and are participating in OT to regain functional abilities. Many of the elders are quite frail and some have cognitive impairments. As a student, Eric observed Mark, a COTA working in an independent living facility. Mark was part of a team providing wellness programming for elders. Most of Mark’s clients were quite active at the facility and in the community. Eric especially enjoyed watching Mark lead Tai Chi groups with the residents. On weekends, Eric visits his grandparents, both of whom are 75 years of age and are also independent, active members of the community. One spring break Eric had the opportunity to accompany his grandfather to an AARP advocacy meeting. He was proud to watch his grandfather and others asking questions that reflected critical thinking about policy issues. Eric often thinks about his grandparents, the elders at the AARP meeting and the independent living facility, as well as the nursing home residents. He contemplates about who are the typical elders.
Lea is a 20-year-old occupational therapy assistant student in an OTA program. As one of her course requirements, class members participate in intergenerational book discussion groups at an independent living facility. The specific readings focus the book discussions on intergenerational values and beliefs. Lea is surprised to identify generational differences and similarities. The elder generations discuss the influences that World War II (WWII) and post-war America had on their lives. Her instructors also participate in the groups. They discuss growing up in the 1960s and 1970s and the influence of the media, the Civil Rights Movement, the Women’s Movement, the assassination of President John F. Kennedy, and the Vietnam War on their generation. Lea and some of her classmates often comment on the strong influence that technology has had on their generation. All of the generations commonly share the impact of the terrorist attacks on September 11, 2001, and the economic downturn of 2008. Lea notes that within each generation there are a variety of perspectives based on individual life experiences. These lively discussions have increased each participant’s awareness of intergenerational commonalities and differences, as well as the individual uniqueness of each group member. The discussions have created a strong bond among the group members. Lea feels that as a result of participating in the intergenerational book discussion group, she will be more comfortable working with elders in a clinical practice.
Lea has a strong desire to go into practice with elders. She remembers helping her grandmother recover from a stroke. When she studied the content about elders in her course work, Lea was surprised to learn of the diversity among the elder population. She realized that just as her OTA class represents diversity among age groups and cultural groups, so does the elder population. She also recognized misconceptions she had about the elder generation. Some were based on clinical observations at a nursing home and informal observations from visits to her grandmother. One misconception was that all elders are sick and frail. Another misconception was that most elders have cognitive impairments. Through her participation in course experiences with well elders in community settings, Lea learned that many elders are healthy and active, especially the younger generation of elders (those 65 to 75 years of age). Lea also learned that cognitive impairment affects a small portion of the elder population, primarily the oldest of the old (those 85 years and older).1
COTAs may easily acquire a skewed image of the elder population, especially in a nursing home setting, which is the second largest area of practice for COTAs.2 Elders in nursing homes tend to be representative of a sicker, older, and frailer elder population. Elders in nursing homes often have circulatory, cognitive, and mental disorders, and most residents require assistance with activities of daily living (ADL).3 In reality, only 4.4% of all elders at any one time reside in nursing homes.4 OT practice continues to change with a movement toward community-based practice, where the majority of elders reside. Therefore, COTAs must have a broader perspective about elders to work effectively with a diverse, continuously changing elder population. This chapter provides relevant background information as it relates to OT practice and to the overall elder population.
The term gerontology comes from the Greek terms geron and lojas, which mean “study of old men.” Gerontology is often thought of as the study of the aged and can include the aging process in humans and animals. The field of gerontology is broad and includes the historical, philosophical, religious, political, psychological, anthropological, and sociological issues of the elder population. The term geriatrics is often used to describe medical interventions with the elderly. In OT practice, geriatrics sometimes refers to an area of clinical specialty. The term cohort refers to “a collection or sampling of individuals who share a common characteristic, such as members of the same age or the same sex.”5 In gerontological literature, the elder generation may also be referred to as the elder (or aged) cohort compared with younger cohorts. Different terms used in this book refer to the geriatric population as the aged, older, or the elder population.
Health, Illness, and Well-Being
Although health, illness, and well-being are familiar terms, they require expanded definitions for OT practice in geriatrics. One part of a definition for health is “the absence of disease or other abnormal condition.”5 Few elders would be considered healthy with this general definition. However, a theory of well-being can be developed if health is considered the optimal level of functioning for a person’s age and condition. Many individuals have chronic illnesses to which they have adjusted and are able to live optimally. These people should be considered as being in a state of well-being. For example, to live optimally, individuals with lifelong disabilities, such as multiple sclerosis, need health care system services such as OT home evaluations for environmental adaptations even though they are not ill. These individuals do not think of themselves as ill and may resent being labeled as “patients” and placed in this role by health care professionals.
The biological systems of elders may change. Some changes that result in disease or dysfunction may be treated through medication or surgery. Other biological changes, such as decreased balance, can be handled with environmental adaptations such as installing brighter lights in stairwells and removing loose rugs and electrical cords from traffic areas in the home. Some sensory changes can be partially resolved with glasses and hearing aids. These biological and sensory changes should not be thought of as illnesses. They are changes that elders adjust to and incorporate into their daily lives.
Chronic Illness
Many medical conditions of elders are chronic—that is, they cannot be cured, but they can be managed. The physician may not cure heart disease, but the pain and debilitating consequences can be managed for years with medications, diet, exercise, surgery, and technology. COTAs can provide ideas to help elders manage their chronic conditions to maintain involvement in occupations (see Chapter 5). In these cases it could be said that, although the disease has not been cured, the elder’s life has been extended in a qualitatively meaningful way.
Most elders have a minimum of one or more chronic conditions. Recent data indicate the most prevalent conditions for elders are hypertension (53%), arthritis (49%), hearing impairments (42%), heart disease (32%), cancer (22%), diabetes (18%), visual impairments (17%), and asthma (11%).6 The incidence of chronic illness may be greater in minority elder groups than in white elders. Blacks and Hispanics over age 65 report higher levels of diabetes than whites. Hypertension is also more prevalent among blacks than whites.6
The following examples illustrate the way one elder learns to adapt to a chronic illness. Henry has osteoarthritis and needs assistance with some ADL functions. He continues to maintain his apartment and values his independence. He takes frequent breaks to rest while doing housekeeping tasks. Because of his decreased endurance, he uses a lightweight upright vacuum, which also helps reduce upper extremity strain. Henry has an active social life outside of his home. He maintains mobility in the community by taking a bus to activities. Henry has osteoarthritis, a disease that cannot be cured. However, most COTAs would say that Henry is not sick.
Miriam is 89 years old. She lives with her 97-year-old husband in the same house that they moved into after they got married. She has a chronic blood condition called thrombocytopenia, along with osteoporosis and hearing loss. She has been admitted several times to the hospital for complications related to the thrombocytopenia. After she returns home and when she gets her energy back, she assumes her normal routine of managing cooking, housework, and walking every morning for 3 miles around the neighborhood. Through her walks she has met many of her younger neighbors and established friendships. Miriam desires to stay in her home, and she enjoys being in an intergenerational community. Again with this example most COTAs would say that Miriam is not sick.
Some health care practitioners may dismiss an elder’s complaints with comments such as “It’s your age; it’s your problem; what do you expect from me? I can’t cure you.” They are likely to overlook important ways to treat and to reduce symptoms that may increase the length and quality of that elder’s life. Generally, health professionals are educated to cure illness, and some may be less knowledgeable about illness management. Thus, some health care practitioners feel uncomfortable treating elders who cannot be cured, and thus in response the health care practitioners develop a dismissive approach.
The alternative to a dismissive approach is a collaborative approach, or what has been referred to in OT literature as client-centered therapy.7 In this approach, emphasized in the second edition of the Occupational Therapy Practice Framework: Domain and Process,8 registered occupational therapists (OTRs) and COTAs partner with their clients to help determine therapy goals and intervention activities. They spend time getting to know clients by hearing their stories through assessments such as the Canadian Occupational Performance Measure (COPM)9 and making an occupational profile. An occupational profile helps gain a better understanding of the elder’s personal history and viewpoints.8 Elders are central to the management of their own health and well-being. By using a client-centered approach, elders identify meaningful intervention activities and thus are more invested in intervention.10
A partnership involves the OTR, COTA, and the elder working together to help determine meaningful intervention goals that enhance the elder’s quality of life. The following example illustrates this partnership.
Sadie is an 86-year-old widow with arthritis and living in a senior citizen housing. Her daily life is a balance of self-maintenance, simple meal preparations, visits with neighbors in the community recreation room, telephone calls to family members, and watching television. Sadie has reported decreasing vision, weakness, and joint pain to her primary care physician. General anxiety and depression also appear to be features of her condition. She comments to her physician, “I think that I belong in a nursing home. I’m old, and I’m having difficulty taking care of myself.”
Placing Sadie in a nursing home may manage some of her medical conditions, as well as provide care and social opportunities. However, the medical team also can evaluate additional supports to maintain independent living in the community if that is what Sadie really desires. The physician can adjust drug dosages for the management of Sadie’s arthritis and order an OT evaluation and intervention. The OTR and COTA decide to first screen Sadie using the COPM to obtain a clearer picture of Sadie’s concerns. With the COPM Sadie mentions that she would really like to remain home and identifies her main concerns as having difficulties with meal preparation and reading the newspaper. Both concerns are related to her low vision. In addition, she has difficulty getting dressed because of arthritis. On the basis of this information, the OTR, COTA, and Sadie collaborate to develop the following intervention recommendations:
1. A kitchen evaluation for suggestions for low vision
2. A lighted magnifier to improve visual function with reading
3. Arthritis education that includes joint protection and mobilization, energy conservation, work simplification, and adaptive devices to improve dressing
A client-centered approach can address the elder’s chronic conditions, interests, and desires. Elders with multiple chronic diagnoses that often accompany acute conditions or changes in functional status are not unusual. When managed properly, all interventions work smoothly to improve the elder’s independent status and occupational well-being. The elder may need to adjust to a different status of functioning with different occupational roles. The OT interventions suggested in the example may result in improved functional abilities in many areas of life and decreased anxiety about independent living. The accumulation of medical conditions does not necessarily lead to decreased function and increased disability. Despite the “graying of America,”11 elder citizens are experiencing less disability and are living longer and better.12
The Stages of Aging
What age constitutes “old age”? The federally mandated age to collect Social Security varies between 65 and 67 years based on year of birth. The age that most retirement communities set as the minimum for their residents is 55 years. At age 50 years, one can join the AARP, and by age 40 years, Americans are protected by the Age Discrimination in Employment Act. The third stage of aging, called senescence, which social gerontologists define as a stage of biological decline, begins at age 30 years.
One definition of old age classifies 65 to 75 years of age as young old, 75 to 85 as mid old, and 85 and greater as old old.* This may help COTAs think of old age in terms of occupational role performance and expectations. However, COTAs should use this classification as a guideline because every person ages differently and every elder does not fit neatly into one of these three categories. Socioeconomic factors, societal changes, cultural factors, and personality considerations can largely influence the way each elder approaches aging. As the Baby Boomers enter the aging population, these categories may change and, ultimately, this generational cohort may change how aging is defined as they desire to stay youthful. Along with maintaining youthful attitudes, their life expectancy has increased.12 Yet as the following discussion indicates, Baby Boomers will also inevitably experience changes with an aging body.
Young Old (65 to 75 years of age)
Elders who are young old may be recently retired and enjoying the results of their years of employment, their essential role as grandparents, and their continuing role as parents in the growth of their adult children. They have increased leisure time to pursue interests and to develop new ones. They may choose to do volunteer work with a community service, return to school, or travel. Some elders, however, because of economic issues or other personal reasons, will choose to remain in the workforce.15 Others, because of family circumstances, may reassume the role of raising children with their grandchildren. The young old must often cope with chronic conditions such as osteoarthritis, hypertension, and cardiovascular disease. However, these chronic conditions are often managed medically and usually do not represent a major barrier to functioning or satisfactory occupational role performance.
Mid Old (75 to 85 years of age)
In the mid old period of life, more changes may be evident. These elders may make modifications in their occupational role performance. They may reduce or simplify their lives in various ways, including resting during the day, volunteering less, traveling less, and limiting distance of trips. They may rely more on social systems such as Meals on Wheels, public transportation, and family for some assistance with ADL (Figure 1-1). COTAs may provide interventions when necessary. The frequent loss of significant others brings affective stressors and additional role changes (see Chapter 2 for a discussion of specific theories explaining the stages of aging).

Old Old (85 years of age and older)
During the old old period of life, elders may reflect on the meaning of their lives, the quality of their relationships, and their contributions to society. They may think about the losses they are experiencing and about their own deaths. This may be a time of peace and generosity; elders in the old old period of life may find it meaningful to give valued objects to loved ones who will treasure them. Conversely, it can be a period of fear and anger resulting from unresolved conflicts. Resolution of these conflicts can make this the most spiritual and fulfilling period for elders. Personal growth and reflection continue throughout life.
This time in an elder’s life is usually a period of further systemic change affecting the sensory, motor, cardiac, and pulmonary systems. Chronic conditions impair self-maintenance capacities, and elders in the old old stage may need personal assistance with bathing, mobility, dressing, and money management that COTAs can provide. If these elders live independently, they may need some family member support.
An alternative health care delivery option to help frail elders primarily in the old old age group is a national demonstration project called Program for All-Inclusive Care of the Elderly (PACE). PACE addresses elders’ preventive, acute, and long-term health care needs, providing medical and support services to help keep elders in their homes after they have been certified to need nursing home care.16 PACE is financially supported by monthly capitation payments from Medicare and Medicaid or by private pay. In general, the goal of the project is to demonstrate that elders remain independent longer when their health care delivery system is sensitive and responsive to their medical, rehabilitative, social, and emotional needs. This project provides alternative models of long-term care such as adult day care, primary health care, rehabilitation, home care, transportation, housing, social services, and hospitalization. An interdisciplinary team handles case management. OTRs and COTAs are important team members with their strong skills of prevention, adaptation, and restoration of function.
As of 2008, there were 61 PACE programs operating in 29 states.16 PACE has been demonstrated to reduce costs “by delaying nursing home care and shortening hospital stays” (p. 1).17 It may be one answer to the ethical and economic dilemmas regarding ways to meet the increasing needs of elders as they live longer in a health care climate of declining resources and advancing technology.
Demographical Data and the Growth of the Aged Population
Demography is “the study of human populations, particularly the size, distribution, and characteristics of members of population groups.”5 Demographical data clearly suggest that the aged population is growing. This growth is often referred to in the literature as “the graying of America.”11 The portion of the elder population that consists of those 65 years or older comprises 12.6% of the total U.S. population. This population is expected to continue growing; it “will burgeon between the years 2010 and 2030 when the ‘baby boom’ generation reaches age 65” (p. 3).4 The elder generation is projected to be 19.3% of the total population by the year 2030.4 Minority elder populations also are growing rapidly and are projected to represent 28% of the elder population by the year 2030 compared with 18% of the elder population in 2003.18 Future generations of elders will be more ethnically and racially variant than the current elder population. By 2050, the elder white population is projected to decline from 81% to 61% of the total elder population. The growth of the minority populations will be greatest among Hispanics, who are projected to account for 18% of the elder population in 2050.6 Many factors contribute to this significant population growth, including a declining mortality rate, advances in medicine and sanitation, improved diet, improved health expectancy with fewer chronic illnesses among Baby Boomers,12 and improved technology. Figure 1-2 illustrates the growth of the elder population.
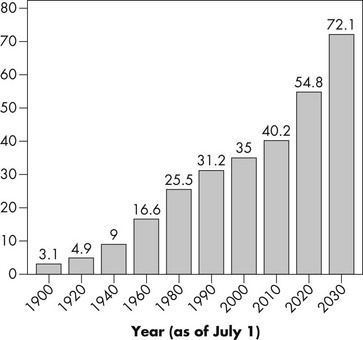
FIGURE 1-2 Number of persons age 65 years and older: 1900 to 2030.
(From Administration on Aging: Profile of older Americans, 2009, Department of Health and Human Services.)
Accompanying the “graying of America” is a growth of the female aged population. For every 100 men older than 65 years, there are 143 women. This ratio increases with age. There are 114 women for every 100 men in the 65- to 69-year age group and 210 women for every 100 men in the 85 years and older age group.4 Women, though, are much more likely to live with a disability, which is often defined as “having difficulty with” ADL19 and indicates a need for OT intervention.
About 42% of women older than 65 years are widows, and there are over four times as many widows as widowers4; these statistics have broad sociocultural implications. A major consequence for some elder women with the loss of a spouse is an increased risk for poverty. In 2003, older single women, mostly widows, were more than twice as likely as older married women and more than three times as likely as older men to be poor or near poor.18
The Aging of the Aged Population
The fastest growing segment of the elder population is the 85 years and older cohort. As of 2006, elders older than 85 years numbered 5.3 million, and their size is projected to increase to 21 million by 2050.6 The 85 years and older cohorts have their own unique needs because they may have more difficulty with physical and social functioning.20 The 85 years and older cohorts are at risk for health problems such as cardiovascular disease and vision and hearing problems.20 The risk for serious injuries from falling increases as aging progresses because the number of risk factors increases.21 Risk factors for falls can include issues like having a chronic condition or poor lighting in the home.21 In addition, the risk for severe cognitive impairment is much greater in the 85 years and older age group. Approximately 32% of those 85 years and older experience moderate to severe memory impairment compared with 5.1% of elders between 65 and 69 years of age.22 The prevalence of Alzheimer’s disease is increasing with a trend toward more elders having the condition.23 Not surprisingly, the 85 years and older group uses a large amount of health, financial, and social services provided by public policies such as Medicare.6 The current elder population, one of many groups of Americans who can qualify for Medicaid, spends the highest amount of Medicaid funds.24 This large usage of federal money, along with concerns about increasing costs, may have future implications for continual modifications of public policies.
The 85 years and older age cohort is more likely to be institutionalized compared with their younger age cohorts. Although only 4.4% of the 65 years and older population are in nursing homes, 15.1% of those 85 years and older reside in institutional settings.4 The need for long-term care is anticipated to increase as this age group grows,25 especially for those with no living children or those living alone without other supports.
Although there are more elders among the 85 years and older population than in any age cohort who live in nursing homes and other long-term care facilities, the majority still reside in the community (Figure 1-3). Living in the community presents challenges because the need for assistance with ADL functions dramatically increases with age.4 “ADLs include bathing, dressing, eating, and getting around the house. Instrumental activities of daily living (IADL) include preparing meals, shopping, managing money, using a telephone, doing housework, and taking medication.”4

Many elders require a support system to have assistance with ADL. Currently, half (49%) of women 75 years and older live by themselves in households, and only 30.1% of women 75 years and older live with a spouse.4 Many members of this age cohort also live with family members such as adult children who provide assistance with ADL functions. The majority of care in the community is provided informally by family members, usually adult daughters.25 A future trend that may influence the type of caregiving needed for some members of the Baby Boom generation when they become the elder generation is a larger percentage of couples that are childless. These Baby Boomers should plan ahead and learn about community resources before they need them.26
Another important factor to consider is that some elders, particularly the old old age group, have relatively minimal formal education. However, the education level of all elders is increasing.6 The number of elders completing a high school education increased from 24% in 1965 to 76% in 2007. Approximately 19% of elders have a baccalaureate degree or higher.6 Knowing the educational level of their clients will help COTAs adjust or determine the instruction or training.
The Oldest of the Old: The Centenarians
An even older and more quickly growing group of elders are the centenarians, or those elders living beyond 100 years.27,28 Researchers are fascinated about factors contributing to this longevity. Lifestyle, genes, environment, and attitude are researched contributors to longevity.29-32 Of these factors, lifestyle appears to strongly impact longevity,27 although further research is warranted.30,31 Centenarians mainly experience a rapid decline in health status in their final years of life.30 Some centenarians, though, have been in good health throughout their lives.30,31 Compared to younger cohorts, centenarians tend to escape or delay chronic illnesses during their lifetimes.33
Living Arrangements
COTAs working in geriatric practice need to consider the elder’s home environment because housing problems can negatively affect the elder’s physical and psychological well-being.6 The majority of noninstitutionalized elders live in family households,34 and 30.2% live alone.4 Age influences living arrangements. Over half of people over age 65 live with spouses. A majority of elders living alone are women who outlive their husbands.34
There are a variety of living options available for elders. For elders with few economic resources, low-income housing is available. However, the number of units is limited, and there may be long waiting lists or lottery systems for applicants. Continuing Care Residential Communities and Life-Care Community Housing are other alternatives for elders with low incomes. In some cases, residents are required to contribute all of their assets. Residents have contracts for housing, supportive services, and often a continuum of services that include health and nursing homes.
Assisted living facilities are the fastest growing living option for seniors and have been available in the United States since the mid-1980s.35 Assisted living facilities focus on frail elders or adults with disabilities. With assisted living, elders receive care management and supportive services to enable maximal independence in a homelike setting. Assisted living residents need some help to remain independent but do not require the same level of 24-hour care provided in nursing home facilities.36 Typical residents are ambulatory 86-year-old women who require help with approximately two ADL.37 Most residents use private funds to finance assisted living.38 In some states, elders with less income can finance assisted living with Medicaid.39 The growth of assisted living is attributed to the increase in the aged population, the desire of elders to have their own home and not go into nursing homes, and state policies that limit access to nursing home facilities.38 There is much variability in the types of facilities. This variability in facilities and the expensive costs for residents are areas of discussion.38 Additionally, because there are no federal regulations for assisted living facilities and variability in the way that states regulate them,40 it would be beneficial for COTAs who practice in them to determine their state regulations.
Board and care homes, personal care, adult day care, adult foster care, family care, and adult congregate living facilities are other alternative care options in the community. Board and care homes service elders, many of whom have been deinstitutionalized. Adult day care is a community-based group program designed to meet the needs of functionally impaired elders. This structured, comprehensive program provides a variety of health, social, and related support services in a protective setting during any part of the day but provides less than 24-hour care. Adult foster homes are family homes or other facilities that provide residential care for elderly or physically disabled residents not related to the provider by blood or marriage. Adult congregate living facilities provide seniors with high-rise living accommodations with innovative service delivery options such as team laundry, cleaning, shopping, congregate meals, and home-delivered meals. Home health services are also available but are usually restricted to more acute episodic needs and require some level of homebound restrictions for reimbursement by Medicare.41
For those elders with assets, retirement communities include a variety of services such as leisure activities, congregate meals, laundry, transportation, and possibly health care. Some retirement communities may require entrance fees that could range from $20,000 to $400,000. Monthly payments may be as low as $200 or as high as $2,500.42 In these communities, COTAs can act as activity directors, using their skills to select, analyze, and adapt activities to the abilities and interests of the residents (see Chapter 8).43
Aging in place or staying in one’s current household with adequate support44 is a trend expected to influence present and future elder generations.12 Aging in place can be perceived as involving more than just an elder’s home, including also the broader community45 or an elder’s context and environment.8 Goals of aging in place is to allow elders a good quality of life by enabling them to stay in their homes and participate in their communities and to modify their homes to permit aging in place.46 Along with aging in place is the phenomenon of Naturally Occurring Retirement Communities (NORC), which are apartments or communities comprising more than 50% of elder populations.45 Elders living in NORCs can work together to provide enough resources to help the residents maintain a quality of life.47 Some health care professionals are choosing to become Certified Aging in Place Specialists (CAPS). With this certification developed by the National Association of Home Builders Remodelers Council (NAHB) along with AARP, health care practitioners are trained in understanding the specific needs of elders for home modification.48
Aging in place is also sometimes perceived as a market-driven concept where elders in a facility receive various levels of care. Thus, an elder might start out on an independent living unit and, when his or her functional status changes, move to an assisted living unit and eventually to a nursing home unit or even an Alzheimer’s disease unit, all in the same facility.49 COTAs working in these facilities can provide continuity of care as the resident’s functional status changes.
For those elders who desire to remain in their homes and communities, support services such as adult day care, meal programs, senior centers, and transportation services can help them age in place.50 Aging in place is a trend that OT practitioners should pay close attention to for as Yamkovenko states, “A part of the 2017 Centennial Vision of the American Occupational Therapy Association (AOTA) is to meet society’s occupational needs. Occupational therapy practitioners can meet the needs of an aging population by helping them age in place, stay healthy, and lead full lives.”46
Most of these discussed living options require having adequate financial assets and good retirement planning because long-term care is costly. In 2009, the average cost for living in an assisted living apartment was $2,825 per month or approximately $34,000 a year.51 Nursing home yearly costs vary across the country with an average cost of $183 daily or almost $67,000 yearly for a semi-private room.51 Medicare does not generally cover long-term care.50 Some elders have shifted their finances to qualify for Medicaid, a program that provides some long-term care coverage for the indigent. However, the Deficit Reduction Act of 2005 now imposes a period of ineligibility for elders who give away assets or resources in order to qualify for Medicaid.52 At the time of this writing a positive addition with health care reform is an optional benefit for long-term care support called the Community Living Assistance Services and Supports Program (CLASS). This program helps pay for nonmedical services to support community residency such as “housing modification, assistive technologies, personal assistance services and transportation” for a person with functional limitations.53
Most federal funds for elders go toward institutional care rather than home and community services. Funding for community services for elders comes from a variety of programs such as Medicaid and the Older Americans Act.50,54 Long-term care insurance is an option to help people plan for their future long-term care needs. Plans differ but usually cover a variety of long-term care options such as assisted living, nursing home, Meals on Wheels, and home health. Coverage is usually based on the criteria of having difficulty with a set number of ADL. Generally, it is more financially advantageous to purchase a plan when one is younger, which results in lower premiums. Unfortunately, it is estimated that 85% of Americans over age 45 do not have any form of long-term care insurance.55 Federal and state governments do provide tax incentives for private long-term care insurance, but primarily affluent elders actually benefit from these incentives because of the set up of tax deductions.56
Finally, recent data on community-resident Medicare beneficiaries suggest that over 27% had difficulty with performing ADL, and an additional 12.5% had difficulty with one or more IADL.4 These data point to one strong reason for OT intervention in any of the discussed settings.
Economic Demographics
Most elders are not impoverished. Data from 2006 suggest that medium- and high-income elders account for more than two-thirds of the total elders.6 The economic status of the elder population has been variable over the past 40 years. The poverty rate in 1959 for elders was 35.2%.57 By 2003 the rate was reduced to 10.2%.57 It is easy to see that the elder poverty rate has “declined substantially” (p. 946).58 The current poverty rate for the elder population is 9.7%,4 which is close to the working age population’s (ages 18 to 64 years) level of poverty.6 General indicators of becoming impoverished after retirement are work history, occupational type, residence in rural areas,59 and preretirement income.60 Working in professional occupations with higher earnings and cognitive requirements may result in better retirement planning.59
Elder women have a greater poverty rate than elder men. Approximately 12% of elder women are poor compared with 6.6% of elder men.4 The economic statuses of elder men and women differ as a result of many factors. When they were younger, elder women of the current oldest generational cohort, the Traditionalists, were generally housewives or worked occasionally at paid employment. This resulted in fewer Social Security benefits and smaller or no pensions. When women become widowed, their chances of becoming impoverished increase, especially if they lose their spouse’s pension funds.58 Minority widows are especially at risk because they may have accrued fewer assets during their working years.61
Although there are differences across ethnic groups in rates of poverty, a wide economic disparity exists between white elders and elders of minority groups. Approximately 7.4% of white elders are poor, compared with 23.2% of black elders and 17.1% of Hispanic elders. Elder Hispanic and black women living alone have the highest poverty rates at 39.5% and 39%, respectively.4
Public policy influences the elder population’s economic status. Social Security, which provides retirement income for elders, and Supplemental Security Income, which provides some financial support for lower income elders,62 help elders. Ninety percent of people over age 65 live in families with income from Social Security.6 Overall, these public policies have proven to be antipoverty measures for elders.63
Changes are projected to occur because of concerns related to the economic solvency of Social Security. Amendments to the Social Security Act in 1983 increased the age in which upcoming generations of elders can start receiving social security.64 The current retirement age of 65 years will eventually increase to 67 years.65 This change, which will be gradually phased in, is applicable to workers who are 62 years of age in the year 2000 (McBride, 1996, personal communication). The economic solvency of Social Security is related to an increasing aging population with less tax dollars in the federal budget to pay for benefits. Discussed reforms are higher taxes, less benefits, or the privatization of retirement funds. Social Security reform will be an important discussion throughout this century.57
Changes in the Medicare and Medicaid policy also will continue to affect the economic status of the elder population, especially if elders are required to pay more money for health care. Adding new benefits such as prescription medication may result in cutbacks in other areas of Medicare or increased costs. At the time of this writing, with health care reform some positive benefits for Medicare beneficiaries are improved coverage for prescription medication and coverage for preventive services, such as annual physicals. Yet cost cuts are planned with other areas of Medicare, such as payment adjustments for home health care agencies.66 Other factors such as the increasing costs of health care and the general state of the American economy also influence the economic status of elders. For example, after the events of September 11, 2001, and in 2008, the stock market took a downswing, which decreased many retirement funds (see Chapter 6 for a discussion about public policy).
Additional Trends and the Influence of Aging Trends on Occupational Therapy Practice
COTAs working with elders need to be aware of aging trends. This section discusses three additional trends that impact elders and their possible influence on COTA practice. One growing trend is elders raising grandchildren. Grandparents in a parenting role can range in age from thirties to seventies.67 Approximately 5.1 million children were living with a grandparent in 2006.68 Grandparents raising grandchildren occurs in all socioeconomic and ethnic groups.68 However, grandparent-headed households are more likely to be living in poverty than other family units.67 Reasons for this phenomenon vary and can result from substance abuse, teen pregnancy, divorce, incarceration, death or disability, and the increasing number of single-parent families.67
Grandparents raising children can experience major challenges. For example, some elders may be dealing with their own health or financial issues along with the stresses of caregiving. It can be difficult to learn to set limits as they did with their children.67 However, some grandparents in a parenting role may find it rewarding to provide a sense of stability and predictability for their grandchildren.67 COTAs working with elders in this situation need to be sensitive to the demands and enjoyment of this parenting role.
A second trend will be an increase in elders remaining in the workforce. Data from 2006 indicate that 29% of workers ages 65 to 69 years old and 11% of workers age 70 years and older remain in the workforce.6 A 2009 survey indicated that 27% of people ages 55 to 64 plan to postpone retirement,15 and 27% of people ages 45 to 54 are seeking new jobs because of economic uncertainty. Another study by AARP found that 80% of Baby Boomers intend to continue working either for an economic reason or for self-gratification.69 The percentages of elders remaining employed have varied over the past 40 years with the greatest percentage occurring in the 1960s. A gradual decrease in workforce participation took place before the early 1980s.6 Since the late 1990s, the percentage of elders remaining in the workforce has gradually increased,6 and projections are for a continual growth of elders in the workforce, especially from the Baby Boomer generation70 and because of economic times.15 Many older workers choose to stay in the workplace “to feel useful and productive” and “live independently” (p. 2).71 In addition, public policy such as changes in the Social Security Act from the 1983 amendments will influence the next generation of elders to remain in the workforce. These amendments allow increases in payment if retirement is delayed between ages 65 and 69. As discussed earlier, full Social Security benefits will be extended until a person is 67 years old.65 The Age Discrimination in Employment Act of 1967 and its amendments along with the removal of required retirement laws also help elder workers remain in the workforce.
Though it has not been the case in the recent past, currently, most employed elders work full-time.72 Older workers tend to have less education and make less money than younger workers, but both of these trends are changing.72 The influence of an aging labor force on OT practice remains to be seen. However, innovative therapists may identify new areas of practice to ensure continual success of elders in the workforce.
A third trend influencing elders is the increased usage of computer technology. Approximately 41% of those age 65 and older have a computer at home, and 33% have Internet access at home.73 The usage of computers by elders has many advantages, such as decreasing isolation and providing telemedical support.74 Computers can assist elders with making purchases, which is a helpful benefit for those who are homebound (Figure 1-4). Adaptive computer programs aid elders with disabilities. For example, voice programs help elders who have arthritis and have difficulty with keyboarding. Elders with low vision can benefit from many computer programs geared for their visual needs. Elders who desire more intergenerational contact can achieve this contact through e-mail and instant messaging.74 Li and Perkins75 found that a majority of elders have a positive view of technology and are willing to learn necessary skills, but few have taken steps to do so. COTAs can suggest computer resources in the community, such as state sites supported by the Assistive Technology Act, which provides computer training, or libraries. They can suggest appropriate software to assist elders with functional concerns and can make adaptations to allow computer usage.

In summary, these three highlighted trends are examples from many trends influencing elders. As the elder generation continues to grow and as society continues to change, it will be paramount that COTAs remain aware of aging trends and consider them in terms of society and OT practice.
Implications for Occupational Therapy Practice
Because of continued growth of the elder population, the need will increase for OTRs and COTAs working with them. The effects of all of the demographics, issues, and trends discussed in this chapter on OT practice remain to be seen. However, it can be assumed that in the future, dilemmas related to limited resources will affect the practice arena. In the coming decades, as the Baby Boom cohorts reach 85 years of age, Ericson, Toohey, and Wiener25 expect that “burdens on families and institutions will increase substantially” (p. v). At this time, no one can predict whether there will be adequate funding and social services to meet the needs of a growing elder population and whether there will be enough health care resources to address this population’s health care needs. The increasing cost of health care,76 the ever changing economy, and the tenuous state of Social Security are current concerns that have future implications for the aged population. OT personnel will continue to be challenged to provide quality intervention in a cost-constrained environment. New models of OT geriatric care will evolve in the future, especially in community settings where the majority of elders remain. All OT personnel should be at the front end of this evolution.
Intergenerational Concepts and Generational Cohorts
In today’s society, same-age cohorts socialize, for the most part, among themselves and have minimal intergenerational contact. When they work in a nursing home, COTAs may have little daily interaction with well elders in the community. COTAs treat elders who are often two or three generations removed. Yet COTAs must have meaningful contact, either informally or formally, with both well and frail elderly to work effectively with the elder population. Many benefits are mentioned in the literature about formal intergenerational programs. Some of these benefits include a better understanding of the elder generation from a historical perspective and their values and beliefs,77 increased positive views of elders,78,79 improved social skills and academic performance for youth, and increased socialization and emotional support for elders.80
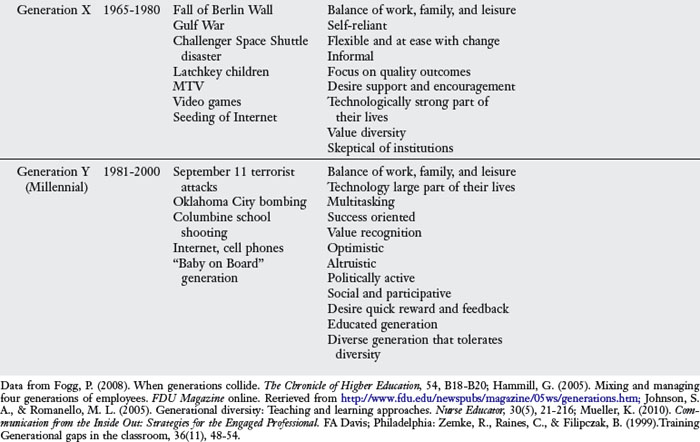
In recent literature there has been much discussion about generational cohorts or a “group of people whose birthdates fall between specified dates and who move through life together” (p. 103).81 Other classical defining factors of generational cohorts are being from the same area and experiencing similar historical and social events.82 Thus, generational cohorts experience comparable social and historical occurrences that predispose them to related life perspectives.83 From an OT standpoint context and environmental factors8 are some considerations with a population of generational cohorts. Current generations are divided into the several groups, each with its own characteristics (Table 1-1). In reviewing this table, consider generational traits and historical/social factors that influenced the generational cohort that you are from as well as from the generations that you will work with in intervention. Table 1-1 also emphasizes concepts about approaching intervention with the current elder generations—the Traditionalist and the entering elder generation of Baby Boomers. Some consideration for intervention is how each generation approaches work, reward, communication, learning, and authority. Contemplate how you can capitalize on the generational characteristics to maximize interventions. Also, when reading this discussion, keep in mind that there is individual variation in any generational cohort based on each individual’s life experiences. Individuals born closer to the end or beginning of a generational cohort may take on traits from their own or the previous or next generational cohort. So ideas presented in this discussion should be viewed as general guidelines.
TABLE 1-1 Intergenerational Factors to Consider with Therapy with the Current Elder Generational Cohorts
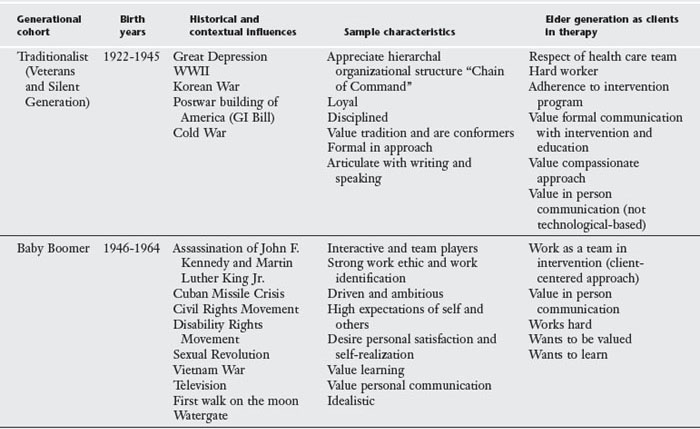
Think about the influence that the Great Depression, WWII, and the Korean War had on the current oldest elder generation. That generation, the Traditionalists, which came of age during WWII, was used to the military being of their lives and therefore embrace a hierarchal approach, are formal in their interaction approach, respectful of authority, value conformity, and believe in working for the greater good.84-86 Based on these traits, Traditionalists in an intervention situation may be very respectful and adherent to the suggestions of “the authorities” on the health care team. It will be important to ask these elders how they want to be addressed because many Traditionalists embrace a formal communication style and prefer titles, such as Mr. Jones, instead of being addressed by a first name.87 Because the Traditionalists value formality and conformity, COTAs should be particularly cognizant of their dress and language. Additionally, Traditionalists grew up at a time when physicians were more personal with house calls and may desire a compassionate approach.87 Having experienced the Great Depression, Traditionalists may be frugal about spending their money, such as for adaptive equipment.
Now think about the Baby Boomer generation that came of age during a time in American history when there was much optimism, prosperity, and yet societal angst and turbulence. Growing up in a secure time of post-WWII, Baby Boomers experienced the benefits of an expanding American society with many advances in science and technology. They also experienced the assassination of President Kennedy, the Vietnam War, and related unrest. The defining events of President Kennedy’s assassination and the Cuban Missile Crisis may have contributed to the Baby Boomers’ focus on living for the moment and personal gratification.12 Additionally, many societal changes were happening, such as the reformation of Congress to be more liberal, the Civil Rights Movement, and the Disability Rights Movement, along with the deinstitutionalization of people with mental illness and people with developmental disabilities. Growing up in such a prosperous time, many members of the Baby Boomer generation were more educated than those of previous generations.12 Generational slogans developed during the youthful period of the Baby Boomers reflected their beliefs. The slogan “Make Love Not War” suggested the unrest of the time about the Vietnam War and the sexual revolution. “Don’t Trust Anyone Over Thirty” reflected the distrust that the Baby Boomer generation had of people in authority. Current Baby Boomers still do not like to think of themselves as aging and desire to stay young.12
According to generational cohort literature, the Baby Boomer generation currently entering the aged population is very different from the present oldest of the aged population, the Traditionalists, based on their life experiences. Baby Boomers value a team approach rather than the authoritative leadership approach that the Traditionalist generation desires.88,89 However, similar to the Traditionalists, Baby Boomers value hard work.88 Baby Boomers are very driven in what they do, often being thought of as achievers.86 Baby Boomers desire personal gratification with life’s occupations,89 like to learn for learning’s sake,88,90 and want to be valued.86 Johnson and Bungum90 found in their research that the Baby Boomer subjects wanted to learn new activities because of multiple reasons, such as providing more social options and relationships, improving health and length of life, and obtaining educational goals. Research indicates that Baby Boomers want to age in place in their homes and remain in their own communities or move to a community that is designed for their aging needs.91
COTAs contemplating intervention approaches with Baby Boomers, based on generational cohort theory, would recognize that elders from this generation may need to be approached differently than elders from the current generational cohort, the Traditionalists. With Baby Boomers, COTAs might strongly integrate a client-centered approach or a team partnership with intervention based on this generational cohort values about work and leadership. In addition, COTAs might recognize that Baby Boomers would want in-depth education about their condition because of valuing learning and that they may have already researched their condition before therapy. The OTR/COTA therapy team will have a strong role helping elders from the Baby Boomer generation who desire to age in place or perhaps helping design homes in communities for elders.
COTAs should familiarize themselves with the characteristics of all generations, including their own, because they may have a positive influence on intergenerational interactions. The exercise in Figure 1-5 demonstrates that each generation has certain values and attitudes that are influenced by similar generational experiences and historical events.92 Yet each person has his or her own story to tell. This exercise can be completed as a group or individually. The exercise in Box 1-1 will help pull together concepts about working with the entering aged population of Baby Boomers.
(Adapted from Davis, L. J., & Kirkland, M. (1987). ROTE: The role of occupational therapy with the elderly: Faculty guide. Rockville, MD: American Occupational Therapy Association, with permission.)
BOX 1-1 Active Learning Exercise
You have been asked to be on a marketing committee to redesign an assisted living facility to meet the needs of the Baby Boomer generation. What will be your suggestions? Consider concepts of context and environment from the Occupational Therapy Practice Framework II with this exercise.8
Ageism, Myths, and Stereotypes about the Aged
“If you are a man and you are prejudiced against women, you will never know how a woman feels. If you are white and you are prejudiced against blacks, you will never know how a black person feels. But if you are young and you are prejudiced against the old, you are indeed prejudiced against yourself, because you, too, will have the honor of being old someday” (Lewis).93
“Ageism is an attitude that discriminates, separates, stigmatizes, or otherwise disadvantages older adults on the basis of chronological age.”5 Ageism is a form of prejudice because it promotes general assumptions, or stereotypes, about a group of people. These assumptions are not true for all members of the elder population and may change to some different expressions of ageism with the Baby Boomer population. Following are some stereotypes expressed with ageism:
 Elders are useless because they can’t see, hear, or remember.
Elders are useless because they can’t see, hear, or remember.
Elders are slow when they move about.
Elders cannot learn new things.
Elders drain the economy rather than contribute to it; they are unproductive.
Elders are too old to remain part of the workforce.
Elders cannot perform or enjoy sexual activity.
Elders prefer being with and talking with other elders.
Many of these statements have been challenged by research. With any stereotype, there may be a small amount of truth for some members of the group. For example, it is true that elders frequently need glasses as aging progresses; however, the need for glasses does not render an elder useless. An unfortunate result of these myths is that some elders may believe them. For example, whereas young persons may joke about becoming forgetful, elders may seriously question their cognitive abilities as a result of the stereotype that elders have trouble remembering.
These stereotypes may develop as a result of fear of the unknown, or from a lack of contact with the aged. American culture often focuses on youth. Youth is seen as beautiful, as something to aspire to and maintain at any cost. Young is sexy, and old is not.
The medical system in the United States also has been focused on youth. The goal of this system has traditionally been to find a cure for all illnesses. This goal has prompted significant contributions to the world’s health care; however, the belief in a cure for all ills may conflict with the care elder citizens need. With the United States’ current technological knowledge, some chronic illnesses of old age can be managed only, not cured.
In the health care system, references to ageism often occur as a response to a medical diagnosis. OT documentation that begins, “This 91-year-old female was admitted with the diagnosis of total hip replacement,” may trigger preconceived ideas based on age bias, such as the opinion that the client is too old for intervention. Readers of this type of documentation may question the benefits versus risks of surgery or OT intervention for this elder.
In day-to-day interactions, language can encourage ageism. People working in the health care field may unintentionally be condescending when they refer to elders as “dear” or “sweetie.” This type of “elderspeak” can contribute to more negative images of aging and lead to worse functional health over time.94 Simply referring to a person as “the older stroke patient in Room 570” dehumanizes the person. Stating that a person is incapable of doing a task because of being old or having some deficits without a true understanding of the person’s functional abilities also promotes ageism. The following story illustrates this concept. At an assisted living facility there were several elders who had mild to moderate cognitive deficits. The COTA knew each elder as a human being and had an understanding of each person’s identified meaningful occupations. For elders who valued cooking, the COTA organized a cooking group followed by a party. She adapted the activity so that all of the elders would be successful. Before the cooking activity, the team leader expressed negative feelings because she felt that the elders would be incapable of cooking. The team leader was surprised to observe that the cooking activity turned out to be beneficial and successful for the elders. The leader later honestly remarked that oftentimes her feelings of being “protective” of the residents got in her way. Feeling protective of elders promotes ageism. A protective attitude can encourage assumptions, such as elders are incapable or elders are like children. Sometimes staff working with elders who have cognitive deficits and have regressed in their function can inadvertently talk to them in a childish manner. Unprofessional actions also can reflect ageism. One COTA who had a very full day skipped an appointment with an elder assuming that the elder had a cognitive deficit and would not remember. Later that day the elder called the COTA to inquire about what happened. The COTA learned a hard lesson from that experience about her own ageism. As these stories illustrate, reflection often helps people realize their own stereotypical beliefs and attitudes. A way to be more aware of ageism and general attitudes is to record in a journal one’s feeling about contact with elders. Box 1-2 provides reflection questions about ageism that COTAs should ask themselves.
Perspectives are changing as reflected in initiatives such as the International Classification of Functioning, Disability and Health, or ICF,95 and Healthy People 2020.96 The ICF is an “international standard to describe and measure health and disability.”95 The ICF focuses on the impact of disability rather than cause and considers not just the disease but also the environmental context in which people live.95
The Occupational Therapy Practice Framework: Domain and Process, second edition, reflects perspectives from the ICF. The Practice Framework considers the intervention process within the broad “domain” of OT.8 Similar to the ICF, the Practice Framework takes into account the influence of context and environment on occupation. Context and environment includes “cultural, personal, temporal, virtual, physical, and social” (p. 645) dimensions.8 As Youngstrom97 stated, “Occupational therapists [need] to understand their role within a larger societal and health context in order to position themselves in changing traditional areas and to take advantage of opportunities in emerging areas” (p. 607). In the second edition several changes were made, including considering clients as persons, organizations, or populations. (See Chapter 7 for more information about the Occupational Therapy Practice Framework.)
Healthy People 2020 envisions “a society in which all people live long, healthy lives.”96 It is based on the following four goals: (1) Attain high quality, longer lives free of preventable disease, disability, injury, and premature death; (2) achieve health equity, eliminate disparities, and improve the health of all groups; (3) create social and physical environments that promote good health for all; and (4) promote quality of life, healthy development, and healthy behaviors across all life stages.96 All goals impact the elder population.
Many aspects of American society, including housing, employment, and recreational resources, are geared toward youth. However, that focus is slowly changing with the emergence of the senior citizen as a powerful political and economic force and with the growth of the aged population. Who knows what changes the next generation of entering elders of Baby Boomers will bring to society!
1. Define the terms gerontology, geriatrics, and cohort.
2. What is the relation between aging and illness?
3. What is a client-centered approach? How might it affect client care?
4. What considerations should be taken for managing clients with chronic illnesses?
5. What factors are related to the significant population growth of the elder generation?
6. What is a result of more widows than widowers among the elder population?
7. What are some of the needs of the 85 years and older generation?
8. What does the COTA need to know about the educational level of any elder for intervention?
9. What age group has the highest poverty rate and why?
10. How has public policy influenced the economic status of elders?
11. What are some implications of the demographical data for future OT practice?
12. How do you think the three discussed trends (grandparents raising children, aging workforce, and increased computer usage) can impact OT practice?
13. How do you keep abreast of aging trends?
14. What is ageism? Provide examples of it in today’s culture. How do you think expressions of ageism might differ or stay the same with an aging population of Baby Boomers?
15. What were misconceptions you had about growth of the aged population, minority elders, the old old (85 years and older), economic demographics, and living arrangements before reading this chapter?
16. What are some of your ideas about what will happen when the Baby Boomers become the elder generation?
1 Burnstein A.B., Remsburg R.E. Estimated prevalence of people with cognitive impairment: Results from nationally representative community and institutional surveys. The Gerontologist. 2007;47:350-354.
2 American Occupational Therapy Association. occupational therapy compensation and workforce study. Bethesda, MD: AOTA Press; 2010.
3 Jones A.L., Dwyer L.L., Bercovitz A.R., Strahan G.W. The National Nursing Home Survey: 2004 overview. National Center for Health Statistics. Vital Health Stat. 13(167), 2009.
4 U. S. Department of Health and Human Services (DHHS). A profile of older Americans. http://www.hhs.gov/, 2008.
5 Mosby’s Dictionary of Medicine, Nursing, and Health Professions, seventh ed. St. Louis, MO: Mosby, 2006.
6 Federal Interagency Forum on Aging-Related Statistics, 2008. Older Americans 2008: Key indicators of well-being. Federal Interagency Forum on Aging-Related Statistics.
7 Law M., Mills J. Client-centered occupational therapy. In: Law M., editor. Client-Centered Occupational Therapy. Thorofare, NJ: SLACK Inc; 1998:1-18.
8 American Occupational Therapy Association. Occupational therapy practice framework: Domain and process, second ed. American Journal of Occupational Therapy. 2008;62(6):625-683.
9 Law M., Baptiste S., Carswell A., McCall M.A., Polatajko H., Pollock N. Canadian Occupational Performance Measure, third ed. Ottawa, Ontario, Canada: CAOT Publications ACE; 1998.
10 Law M. Identifying occupational performance issues. In: Fearing V.G., Clark J., editors. Individuals in Context: A Practical Guide to Client-Centered Practice. Thorofare, NJ: SLACK Inc; 2000:31-45.
11 McLean C. The graying of America. Oregon Starter. 1988;11:11-17.
12 Greenblatt A. Aging Baby Boomers: The issues. CQ Researcher. 2007;17(37):857-887. Retrieved from http://www.agingsociety.org/agingsociety/publications/public_policy/cqboomers.pdf
13 Lazer W. Inside the mature market. American Demographics. 1985;7(3):48.
14 Neugarten B.L. Age groups in American society and the rise of the young-old. Annals of the American Academy of Political and Social Sciences. 1974;415:187-188.
15 Walker B.S. Uncertain economy changes outlook on job status. AARP Bulletin Today, Retrieved from http://bulletin.aarp.org/yourmoney/work/articles/uncertain_economy_changes_outlook_on_job_status.html, 2009.
16 National PACE Association. What is PACE? Retrieved from http://www.npaonline.org/website/article.asp?id=12, 2009.
17 Petigara T., Anderson G. Program of all-inclusive care for the elderly. Health Policy Monitor. Retrieved from http://www.npaonline.org/website/download.asp?id=3034, 2009, April.
18 U.S. Census Bureau. 65+ in the United States: 2005. Retrieved from http://www.census.gov/prod/2006pubs/p23-209.pdf, 2005.
19 Bould S. Oldest old. In The Encyclopedia of Health and Aging. Retrieved from. http://www.sage-ereference.com.cuhsl.creighton.edu/aging/Article_n206.html, 2007.
20 Schoenborn C.A., Heyman K.M. Health characteristics of adults aged 55 years and over: United States, 2004-2007. National Health Report Statistics. 16, 2009, July 8. Retrieved from http://www.cdc.gov/nchs/data/nhsr/nhsr016.pdf
21 Stevens J.A. Injury, fourth ed. Schultz R., editor. The Encyclopedia of Aging: A Comprehensive Resource in Gerontology and Geriatrics. New York: Springer. 2006;vol. 1:591-593.
22 Federal Interagency Forum on Aging-Related Statistics, 2006. Older Americans 2006: Key indicators of well-being. Federal Interagency Forum on Aging-Related Statistics.
23 Fernandez A. Alzheimer’s disease: Is our healthcare system ready? Retrieved from http://www.sharpbrains.com/blog/2009/09/21/alzheimers-disease-is-our-healthcare-system-ready/, 2009.
24 Sommers A., Cohen M. Kaiser Commission on Medicaid and the Uninsured. Medicaid’s high cost enrollees: How much do they drive program spending? 1-18. Retrieved from http://www.kff.org/medicaid/upload/7490.pdf, 2006.
25 Ericson R.W., Toohey D., Wiener J.M. Meeting the long-term care needs of the Baby Boomers: How changing families will affect paid helpers and institutions. The Retirement Project. Washington, DC: The Urban Institute, 2007. Retrieved from http://www.urban.org/UploadedPDF/311451_Meeting_Care.pdf
26 Snyderman N. Aging without children—who provides care? NBC News. 2007, May 2. Retrieved from http://www.msnbc.msn.com/id/18444782/ns/nightly_news_with_brian_williams-trading_places
27 MacKnight C. Centenarians, fourth ed. Schultz R., editor. The Encyclopedia of Aging: A Comprehensive Resource in Gerontology and Geriatrics. New York: Springer. 2006;vol. 1:196-198.
28 Poon L.W., Jang Y. Centenarians. In The Encyclopedia of Health & Aging. Retrieved from. http://www.sage-ereference.com.cuhsl.creighton.edu/aging/Article_n55.html, 2007.
29 Adams E.R., Nolan V.G., Andersen S.L., Perls T.T., Terry D.F. Centenarian offspring: Start healthier and stay healthier. Journal of the American Geriatrics Society. 2008;56(11):2089-2092.
30 Willcox D.C., Willcox B.J., Wang N., He Q., Rosenbaum M., Suzuki M. Life at the extreme limit: Phenotypic characteristics of supercentenarians in Okinawa. Journal of Gerontology Series A: Biological Sciences & Medical Sciences. 2008;63A(11):1201-1208.
31 Power C., Koch T., Kralik D. Exploring longevity with Australian centenarians. Geriaction. 2006;24(4):5-14.
32 Perls T.T. The different paths to 100. American Journal of Clinical Nutrition. 2006;83(5):484S-487S.
33 Poon L.W. The Georgia Centenarian Study: A study of longevity and survival of the oldest old. The University of Georgia Gerontology Center. Retrieved from http://www.geron.uga.edu/pdfs/CentStudyBooklet.pdf, 2005.
34 Angel J.L., Lewis E. Living arrangements. In The Encyclopedia of Health & Aging. Retrieved from. http://www.sage-ereference.com.cuhsl.creighton.edu/aging/Article_n157.html, 2007.
35 Assisted Living Federation of America. Assisted living today—a brief overview of senior living care. Retrieved from http://www.alfa.org/alfa/About_ALFA.asp?SnID=1357427202, 2009.
36 Mitty E.L. Nursing homes, fourth ed. Schultz R., editor. The Encyclopedia of Aging: A Comprehensive Resource in Gerontology and Geriatrics. New York: Springer. 2006;vol. 2:842-853.
37 National Center for Assisted Living. Resident profile. Retrieved from http://www.ahcancal.org/ncal/resources/Pages/ResidentProfile.aspx, 2009.
38 Hawes C., Phillips C.D., Hutchison L.L. Assisted living, fourth ed. Schultz R., editor. The Encyclopedia of Aging: A Comprehensive Resource in Gerontology and Geriatrics. New York: Springer. 2006;vol. 1:87-91.
39 American Association of Homes and Services for the Aging. About assisted living. Retrieved from http://www.aahsa.org/article.aspx?id=3836, 2009.
40 Kreiser J. Assisted living, erratic regulation. Retrieved from http://www.cbsnews.com/stories/2006/11/13/cbsnews_investigates/main2177892.shtml, 2006.
41 Medicare.gov. Home health compare: Medicare coverage of home health care. Retrieved from http://www.medicare.gov/HHCompare/Home.asp?dest=NAV|Home|About|MedicareCoverage#TabTop, April 1, 2007.
42 American Association of Retired Persons (AARP). Continuing care retirement communities. Retrieved from http://www.aarp.org/families/housing_choices/other_options/a2004-02-26-retirementcommunity.html, 2009.
43 Ryan S.E., Sladyk K. The occupational therapy assistant as activity director. In: Ryan S.E., Sladyk K., editors. Ryan’s Occupational Therapy Assistant: Principles, Practice Issues, and Techniques. fourth ed. Thorofare, NJ: SLACK Inc; 2005:517-528.
44 Mitty E., Flores S. Aging in place and negotiated risk agreements. Geriatric Nursing. 2008;29(2):94-101.
45 Black K. Health and aging in place: Implications for community practice. Journal of Community Practice. 2008;15(1):79-95.
46 Yamkovenko S. Occupational therapy: Helping America age in place. Retrieved from n.d. http://www.aota.org/News/Centennial/40313/Aging/Aging-in-Place.aspx
47 Seniorresource.com. Aging in place. Retrieved from n.d. http://www.seniorresource.com/ageinpl.htm
48 Ageinplace.com. Introduction to Certified Aging in Place Specialists (CAPS). n.d. http://ageinplace.com/certified-aging-in-place-specialists-caps/
49 Seniorresource.com. Aging in place. Retrieved from http://www.seniorresource.com/ageinpl.htm#ageinpltop, 2009.
50 Agency for Healthcare Research and Quality. Your guide to choosing quality healthcare: Long-term care. Retrieved from http://www.ahrq.gov/consumer/qnt/qntltc.htm, 2009.
51 Genworth Financial, Inc. Genworth 2009 cost of care survey. Retrieved from http://www.genworth.com/content/etc/medialib/genworth_v2/pdf/ltc_cost_of_care.Par.8024.File.dat/cost_of_care.pdf, 2009.
52 Gosselin J. Medicaid planning. Aging Well. 2009, September/October;2(4):26. Retrieved from http://www.agingwellmag.com/archive/083109p26.shtml
53 Kaiser Family Foundation. Focus on health reform: The Community Living Assistance Services and Supports (CLASS) Act. Retrieved from http://www.kff.org/healthreform/upload/7996.pdf, 2009.
54 Administration on Aging. Home and community-based long-term care. Retrieved from http://www.aoa.gov/AoARoot/AoA_Programs/HCLTC/index.aspx, 2009.
55 Meiners M.R. Long-term care insurance. In The Encyclopedia of Health & Aging. Retrieved from. http://www.sage-ereference.com.cuhsl.creighton.edu/aging/Article_n163.html, 2007.
56 Baer D., O’Brien E. Federal and state income tax incentives for private long-term care insurance. AARP Public Policy Institute. Retrieved from http://www.aarp.org/research/ppi/ltc/ltc-ins/articles/2009-19-tax-incentives.html, 2009.
57 Clark R.L. Economics, fourth ed. Schultz R., editor. The Encyclopedia of Aging: A Comprehensive Resource in Gerontology and Geriatrics. New York: Springer. 2006;vol. 1:348-351.
58 Bensing K.M. Poverty, fourth ed. Schultz R., editor. The Encyclopedia of Aging: A Comprehensive Resource in Gerontology and Geriatrics. New York: Springer. 2006;vol. 2:946-949.
59 McLaughlin D.K., Jensen L. Work history and U.S. elders’ transition into poverty. The Gerontologist. 2001;40(4):469-480.
60 Holden K.C.A., Kim M. Poverty, third ed. Atchley R.C., editor. The Encyclopedia of Aging: A Comprehensive Resource in Gerontology and Geriatrics. New York: Springer, 2001;vol. 2.
61 Angel J.L., Jimenez M.A., Angel R.J. The economic consequences of widowhood for older minority women. The Gerontologist. 2007;47(2):224-234.
62 Social Security Online—The official website of the U.S. Social Security Administration. Supplemental security income (SSI). Retrieved from http://www.ssa.gov/ssi/, 2009.
63 American Association of Retired Persons (AARP). How social security keeps older persons out of poverty across developed countries. AARP Public Policy Institute. Retrieved from http://assets.aarp.org/rgcenter/econ/dd118_ss_poverty.pdf, 2005.
64 Social Security Online—The official website of the U.S. Social Security Administration. Historical background and development of social security. Retrieved from n.d. http://www.ssa.gov/history/briefhistory3.html/
65 Rix S.E. Employment, fourth ed. Schultz R., editor. The Encyclopedia of Aging: A Comprehensive Resource in Gerontology and Geriatrics. New York: Springer. 2006;vol. 1:362-368.
66 Intermill, M. (n.d.). Provisions of H.R. 3590 that reduce Medicare spending. AARP Nebraska.
67 American Academy of Child & Adolescent Psychiatry. Grandparents raising grandchildren. Retrieved from http://www.aacap.org/cs/root/facts_for_families/grandparents_raising_grandchildren, 2008.
68 U.S. Census Bureau. Grandparents day 2008: Sept. 7. U.S. Census Bureau News. Retrieved from http://www.census.gov/Press-Release/www/releases/pdf/cb08ff-14_grandparents.pdf, 2008, July 7.
69 Novelli W.E. The end of retirement. Retrieved from http://www.aarp.org/aarp/articles/novelliretirement_1.html, 2002.
70 Toossi M. Labor force projections to 2016: More workers in their golden years. Monthly Labor Review. Bureau of Labor Statistics. Retrieved from http://www.bls.gov/opub/mlr/2007/11/art3full.pdf, 2007, November.
71 Pew Research Center. America’s changing workforce: Recession turns a graying office grayer. Retrieved from http://pewsocialtrends.org/assets/pdf/americas-changing-workforce.pdf, 2009, September 3.
72 U.S. Bureau of Labor Statistics. Older workers: Spotlight on statistics. Retrieved from http://www.bls.gov/spotlight/2008/older_workers/, 2008.
73 Kaiser Family Foundation. e-Health and the elderly: How seniors use the Internet for health information. Retrieved from http://www.kff.org/entmedia/upload/e-Health-and-the-Elderly-How-Seniors-Use-the-Internet-for-Health-Information-Key-Findings-From-a-National-Survey-of-Older-Americans-Survey-Report.pdf, 2005.
74 Mundorf N., Mundorf J., Brownell W. Communication technologies and older adults, fourth ed. Schultz R., editor. The Encyclopedia of Aging: A Comprehensive Resource in Gerontology and Geriatrics. New York: Springer. 2006;vol. 1:242-247.
75 Li Y., Perkins A. The impact of technological developments on the daily life of the elderly. Technology in Society. 2007;29(3):361-368.
76 Congressional Budget Office. The long-term outlook for health care spending. Congress of the United States. Retrieved from http://www.cbo.gov/ftpdocs/87xx/doc8758/11-13-LT-Health.pdf, 2007.
77 Lohman H., Griffiths Y., Coppard B., Cota L. The power of book discussion groups in intergenerational learning. Educational Gerontology. 2003;29(2):103-116.
78 Chung J.C.C. An intergenerational reminiscence programme for older adults with early dementia and youth volunteers: Values and challenges. Scandinavian Journal of Caring Science. 2009;23:259-264. doi: 10.1111/j.1471-6712.2008.00615.x
79 Dunham C.C., Casadonte D. Children’s attitudes and classroom interaction in an intergenerational education program. Educational Gerontology. 2009;35(5):453-464.
80 Aging Initiative. Benefits of intergenerational programs. U.S. Environmental Protection Agency. Retrieved from http://www.epa.gov/aging/ia/benefits.htm, 2009.
81 Thompson J. Generational rights and duties. In: Intergenerational Justice: Rights and Responsibilities in an Intergenerational Policy. New York: Routledge; 2009:103.
82 Ryder N.B. The cohort as a concept in the study of social change. American Sociological Review. 1965;30(6):843-861.
83 Sessa V.L., Kabacoff R.I., Deal J., Brown H. Generational differences in leadership values and leadership behaviors. The Psychologist-Manager Journal. 2007;10:1-28.
84 Fogg P. When generations collide. The Chronicle of Higher Education. 2008;54:B18-B20.
85 Johnson S.A., Romanello M.L. Generational diversity: Teaching and learning approaches. Nurse Educator. 2005;30(5):21-216.
86 Zemke, R., Raines, C., Filipczak, B., 1999. Generational gaps in the classroom. 36 (11), 48-54.
87 Mueller K. Communication from the Inside Out: Strategies for the Engaged Professional. Philadelphia: FA Davis; 2010.
88 Coates J. Generational learning styles. River Falls, Wis: LERN Books; 2007.
89 Hahn J. Effectively manage a multigenerational staff. Nursing Management. 2009;40(9):8-10.
90 Johnson M.L., Bungum T. Aging adults learning new avocations: Potential increases in activity among educated Baby-Boomers. Educational Gerontology. 2008;34(11):970-996.
91 Metlife. New housing trends report: Most Baby Boomers prefer to age in place, but growing numbers head to age-restricted communities, say NAHB and Metlife Mature Market Institute. Retrieved from http://www.metlife.com/about/press-room/us-press-releases/2009/index.html?SCOPE=Metlife&MSHiC=65001&L=10&W=Aging%20Housing%20Place%20Whats%20in%20new%20&Pre=%3CFONT%20STYLE%3D%22background%3A%23ffff00%22%3E&Post=%3C/FONT%3E&compID=12912, 2009.
92 ROTE: The role of occupational therapy with the elderly: Faculty guide. In: Davis L.J., Kirkland M., editors. Module I: Teaching Resources Gerontology in Theory and Practice. Rockville, MD: American Occupational Therapy Association; 1987:71-79.
93 Lewis C. How the myths of aging impact rehabilitative care for the older person. Occupational Therapy Forum. 1989;10:10. 11, 14, 15
94 Leland J. In “sweetie” and “dear,” a hurt for the elderly. The New York Times. Retrieved from http://www.nytimes.com/2008/10/07/us/07aging.html, 2008, October 6.
95 World Health Organization. International Classification of Functioning, Disability, and Health (ICF). Retrieved from http://www.who.int/classifications/icf/en/, 2010.
96 U.S. Department of Health and Human Services (DHHS). Healthy people 2020 framework. Retrieved from http://www.healthypeople.gov/HP2020/Objectives/framework.aspx, 2009.
97 Youngstrom M.J. The occupational therapy practice framework: The evolution of our professional language. The American Journal of Occupational Therapy. 2002;56(6):607-608.