Chapter 8 Opportunities for Best Practice in Various Settings
1. Illustrate certified occupational therapy assistant (COTA) practice in traditional and emerging practice settings.
2. Become familiar with the Occupational Therapy Practice Framework (second edition) and the COTA’s role during occupational therapy (OT) service delivery.
3. Understand the need for service competency for COTAs and continued competency for occupational therapy practitioners: COTA and registered occupational therapist (OTR).
client-centered practice, COTA/OTR partnership, occupational therapy practice framework, service competency, continued competency, geropsychiatric unit, inpatient rehabilitation, adult foster home, skilled nursing facility (SNF), assisted living, home health, adult day care, hospice, emerging practice
[T]he defining contribution of occupational therapy is the application of core values, knowledge, and skills to assist clients (people, organizations, and populations) to engage in everyday activities or occupations that they want and need to do in a manner that supports health and participation.1
Marta works with elders in a geropsychiatric unit, assisting elders and families to manage daily life activities on the ward and at home. Arianna works with elders in an adult foster home, helping the elders engage in leisure and social activities throughout their week. Rachel works in an inpatient rehabilitation unit, helping elders to regain their competence in basic activities of daily living (ADL). Jean works as a resident services coordinator at an assisted living facility, overseeing the delivery of services. Drew works with elders in an SNF, facilitating their ability to participate in basic and instrumental daily activities and regain former roles. Amanda works on-call for SNFs and is exploring the possibility of including OT services at the independently owned hospice where she volunteers. Manisha works in home health, helping elders engage in a routine of needed and desired daily life activities within their homes. Carlos works at an adult day care center, assisting elders engage in a routine of productive and leisure activities and achieve life satisfaction.
These COTAs attended a reunion for graduates from the Occupational Therapy Assistant (OTA) program at Blue Lake Community College, established 20 years ago. Of the 150 COTAs in attendance, the majority work with elders in one capacity or another, reflecting the U.S. national trends of 75% of COTAs working with rehabilitation/disability/productive aging populations and 50% working in SNFs.2 Some COTAs work in more traditional settings, such as an SNF or geropsychiatric unit; others work in emerging practice settings, such as adult foster homes and assisted living facilities. Despite working in different settings, the common thread is that the COTAs are assisting elders engage in daily activities and meaningful occupation. Although the settings differ, the focus and process of delivering OT services are similar.
This chapter addresses the role of COTAs, emphasizing the similar focus and process of OT service delivery with elders across different practice settings, using the Occupational Therapy Practice Framework (hereafter known as the Framework)1 as a guide.* Other initial concepts presented are the importance of the COTA/OTR partnership, service competency, continued competency, and practice issues during OT service delivery. A series of vignettes follow that describe COTAs’ work with elders in specific settings and illustrate best practice for COTAs, that is, when OT practitioners deliver services “based on knowledge and evidence that reflect the most current and innovative ideas available.”3
Occupational Therapy Practitioners: A Collaborative Partnership
To support elders to achieve health, well-being, and life satisfaction through participation in a meaningful occupation, the COTA/OTR team provides valuable OT services. Even though OTRs are ultimately responsible for OT service delivery and for supervising COTAs, the delivery of occupational services occurs collaboratively between the two partners.4 According to AOTA,4 supervision is defined as “a cooperative process in which two or more people participate in a joint effort to establish, maintain, and/or elevate a level of competence and performance.”4 This supervisory relationship is necessary to ensure the safe and effective delivery of OT services and to promote the professional development of the COTA. Moreover, OT service provision is done in accordance with the Occupational Therapy Code of Ethics,5 continuing competency and professional development guidelines, relevant workplace policies, and state laws and regulations.4,6
Together, the COTA/OTR partners should decide the type of contact (direct or indirect) and frequency of supervision4 and then develop and document a supervisory plan that details what type of supervision is needed, what areas should be addressed, and how often to meet. For example, a COTA/OTR team works in an SNF and meets face-to-face (direct contact) once a week for an hour to review and discuss their clients’ concerns and status. In addition, they discuss specific ways to foster the COTA’s professional expertise, such as developing advanced therapeutic skills when working with elders experiencing depression and better ways to incorporate the learning–teaching process when working with an elder’s family members, significant others, and caregivers. In other settings, such as home health, the COTA and OTR meet face-to-face several times a month for an hour; however, during the week, they keep in frequent contact through telephone calls and e-mail messages (indirect contact). Although these contacts focus primarily on service delivery for clients, they also discuss areas for professional development. The frequency, methods, and focus of supervision vary according to the skills of the COTA and OTR, the needs and complexity of clients, the service setting’s needs and requirements, and state regulatory requirements.4
To establish a collaborative partnership and deliver quality services, the COTA and OTR need to value their common beliefs and skills and honor their different contributions during service delivery.7 A respectful relationship occurs when partners communicate openly, trust each other, share each other’s knowledge, and are willing to learn from each other.8 Sue, a COTA, worked at a rehabilitation unit for 3 years when Steve, an OTR and recent graduate, joined the team. Steve appreciated Sue’s expertise to identify, plan, and adapt therapeutic activities related to elders’ specific interests and needs, particularly leisure, household, and community activities. Sue appreciated the way Steve fostered her understanding of elders’ specific emotional, cognitive, and physical conditions and how to apply this knowledge during evaluation and intervention. Sue taught Steve new and different ways of engaging clients in activities while Steve modeled a client-centered approach when interacting with elders. Steve trusted Sue to carry out interventions, particularly those focusing on adaptation, and share her thoughts and professional opinion, and Sue felt comfortable asking Steve for additional supervision when needed. Sue and Steve were respectful of each other without their partnership being a hierarchical relationship.
Establishing a strong collaborative COTA/OTR partnership is an ongoing process that requires active participation by the COTA and OTR to identify the partnership’s strengths and areas of improvement.8 To assist with the process, COTAs and OTRs should identify each other’s competencies, as well as the common knowledge and skills they share. This requires a comprehensive understanding of the role and responsibilities of COTAs and OTRs during the evaluation, intervention, and outcomes process of service delivery. To understand this, the second (and most recent) edition of the Framework1 and its relation to the COTA/OTR team process is presented in the following section.
Occupational Therapy Practice Framework
In 2002, AOTA introduced the Occupational Therapy Practice Framework: Domain and Process, a document designed to assist OTRs and COTAs to more clearly affirm and articulate OT’s unique focus on occupation and daily life activities and to illustrate an intervention process that facilitates clients’ engagement in occupation to support their participation in life.9 Because the Framework is an official AOTA document, it is reviewed every 5 years; consequently, a second edition was published in 2008.1 Following is a brief overview of the two major areas from the second edition—(1) Domain of Occupational Therapy and (2) Process of Occupational Therapy—that COTAs and OTRs should be familiar with when working with elders. Because the following sections focus on only highlights from the Framework, occupational therapy practitioners are encouraged to obtain the most recent edition for use in practice.
Domain of Occupational Therapy
Occupational therapy practitioners assist “clients (people, organizations, and populations) to engage in everyday activities or occupations that they want and need to do in a manner that supports health and participation.”1 Engagement in everyday occupation (the breadth and meaning of everyday activity) is the focus of occupational therapy, encompassing both subjective and objective aspects of engagement. Thus, the meaning and purpose of engaging in occupation is unique to each client.
In occupational therapy practice, the terms occupation and activity are used interchangeably, and in the Framework, the term occupation encompasses activity, making no real distinction between the two terms.1 Some professionals, however, do differentiate occupation from activity.10,11 For example, an elder enjoys creating wooden toys in his workshop for his granddaughter, deriving pride in his skill as a craftsman and from the pleasure the toys bring to his granddaughter. For another elder, that same activity may not hold the same meaning. In fact, some elders may view making wooden toys as a chore or childish. If so, then making wooden toys would be considered merely an activity, one without the meaning that would make it a personal, meaningful occupation.
Although the distinction between activity and occupation is not always clear, it can be helpful for occupational therapy practitioners to consider the distinction between activity and occupation when working with elders. If only an elder’s occupation is considered, there may be important activities in the elder’s life that are not adequately addressed during intervention. For example, when using the toilet, it may be important for an elder to assist to the best of his or her ability to reduce the physical and emotional stress on the caregiver. If an OT practitioner does not address toileting because the elder does not think it is important to become as independent as possible, then both the elder and the caregiver are at risk for physical injury and emotional distress. However, if an OT practitioner focuses solely on an elder’s performance in activities and ignores the elder’s engagement in meaningful occupation, an important contribution to the elder’s health, well-being, and life satisfaction may be ignored. For example, focusing therapy on increasing an elder’s independence in dressing when he or she does not find much personal meaning in this objective may not only damage the therapeutic relationship, but also the OT practitioner may miss an opportunity to enhance the elder’s health, well-being, and life satisfaction through assisting the elder to engage in meaningful occupation. Enhancing the elder’s engagement in occupation that has meaning to him or her, such as tending to tomato plants, walking the dog around the block twice a day, or washing the dishes after a meal his or her spouse has prepared, may be of greater benefit than achieving “independence” in dressing. The important aspect is that all activities and occupations addressed during OT intervention consider the contexts in which the elder lives, loves, works, and plays.
With a primary focus on a client’s engagement in occupation, the Framework outlines six major elements that constitute the primary domain of OT (Table 8-1). No one element is considered more important than the other. OT practitioners need to consider all elements when focusing on the targeted outcome of OT intervention: the client’s health, participation in life, and engagement in occupation.1
TABLE 8-1 Domain of Occupational Therapy
| Performance in areas of occupation | |
| Performance skills | |
| Performance patterns | |
| Organization and population | |
| Contexts and environments | |
| Activity demands | |
| Client factors |
Based on data from American Occupational Therapy Association (AOTA). (2008). Occupational therapy practice framework: Domain and process. American Journal of Occupational Therapy, 62(6), 625-683.
The first element, areas of occupation, identifies the primary categories of occupation that OT practitioners consider when working with individuals, organizations, or populations.1 These categories represent the primary focus of OT: a client’s engagement in ADL, instrumental activities of daily living (IADL), rest and sleep, education, work, play, leisure, and social participation. Depending on the specific setting in which a COTA works, some areas may be emphasized more than others. For example, after an acute care hospitalization for pneumonia, it is important for elders to be able to manage their ADL when they return home. Although this may be a major area of concern for discharge, the Framework prompts occupational therapy practitioners to also address other potential areas, such as leisure and social participation, which may be equally important to an elder after discharge.
The second element, client factors, represents the underlying characteristics and capacities (i.e., values, beliefs, and spirituality; body functions; and body structures) specific to each client and that influence a client’s performance in occupation.1
The third element, activity demands, signifies the particular features of an activity required to engage in that specific activity1 and reflect a unique skill that occupational therapy practitioners possess: the ability to analyze activities.12 Each activity “possesses” specific demands—some activities require a large outdoor physical environment, such as a lawn to play croquet, whereas other activities require a relatively quiet indoor environment that promotes conversation, such as a living room where coffee and pastries can be served for church members. Furthermore, each activity will demand more or less of a particular body function or structure—some activities require more fine motor coordination, such as needlepoint, whereas others require greater strength, such as vacuuming.
The fourth element, performance skills, is the “abilities clients demonstrate in the actions they perform”1 and reflect the interaction of the underlying client factors. OT practitioners use their observation skills to identify those skills that are effective or ineffective when a person is engaging in occupation. For example, a COTA and an elder are in a pharmacy where the COTA is primarily interested in the elder’s communication and social skills while picking up a prescription. Throughout the process, the COTA observes the elder’s skill to project his voice to the pharmacist behind the counter and effectively ask questions about a medication’s side effects.
The fifth element, performance patterns, reflects the configuration of habits, routines, rituals, and roles as clients engage in occupation.1 An important factor for clients is the ability to engage in a series of activities over time that sustains engagement in occupation. For example, a COTA working with an elder experiencing mild memory loss might assist the elder to develop a consistent routine to safely prepare toast and coffee each morning.
The sixth (and final) element, context and environment, refers to the varied conditions and surroundings under which people engage in occupation. Engaging in occupation is influenced by cultural, personal, temporal, virtual, physical, and social conditions. For example, a cultural norm that a family values and follows may forbid female individuals from providing personal, intimate care for male elders, such as bathing, toileting, or dressing.
Process of Occupational Therapy: Evaluation, Intervention, and Outcome
OT practitioners view occupation as both the means and end of OT intervention.13 With this in mind, service delivery begins with an evaluation of a client’s occupational needs, problems, and concerns, continues with an intervention process that emphasizes the therapeutic use of occupations, and ends with a review of outcomes to identify whether the client’s occupational needs, problems, and concerns were resolved.1 The Framework contains three major elements that represent the process of delivering OT services.
The first element, evaluation, represents the first stage and focuses on understanding what the client wants and needs to do with respect to engaging in occupation and identifying the features that support or hinder the client’s engagement in occupation.1 To do so, OT practitioners must consider those elements identified in the Framework domain—client factors, activity demands, performance skills, performance patterns, and context and environment—and how they influence the client’s concerns about engagement in occupation and performance of activities.
The evaluation process consists of two steps: (1) creating an occupational profile and (2) conducting an analysis of occupational performance. Using a client-centered approach, OT practitioners gather information to create an occupational profile that clarifies what is important and meaningful to a client, focusing on the client’s occupational history and experiences, patterns of daily living, interests, values, and needs.1 The process to create a client’s occupational profile will vary, depending on the client and the setting, but the focus remains the same: What are the client’s current priorities and problems relative to engaging in occupation? Information from the occupational profile guides the next stage in the evaluation process: analysis of occupational performance. This involves observing clients engage in activities and occupation and requires an understanding of the complex and dynamic interaction of the client’s performance skills and patterns, the contexts and environments in which occupation needs to occur, the activity demands, and client factors. To analyze a client’s performance, specific activities (and the contexts and environments in which they occur) are identified, and the client is observed performing the activities. During this process, the occupational therapy practitioner notes the effectiveness of the client’s performance skills and patterns. Using other information gathered during the evaluation process, the OT practitioner then interprets the data to identify what supports and/or hinders the client’s engagement in occupation. OTRs are ultimately responsible for initiating and completing the evaluation. COTAs, supervised by an OTR, assist during the evaluation process according to their skill level (Table 8-2).1
TABLE 8-2 Certified Occupational Therapy Assistant/Registered Occupational Therapist Responsibilities During Process of Occupational Therapy Service Delivery
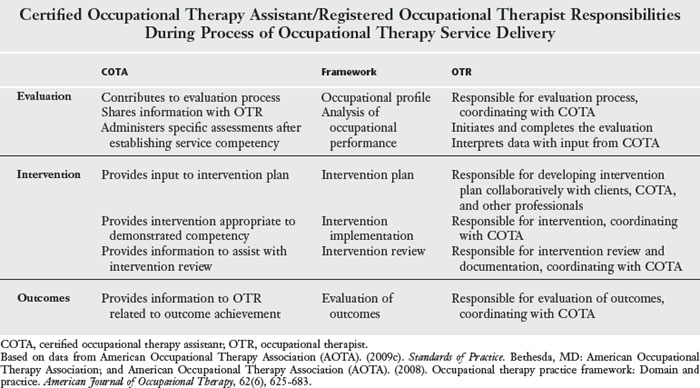
The second element, intervention, consists of three steps: (1) developing the plan, (2) intervention implementation, and (3) intervention review. Although OTRs are ultimately responsible for developing the intervention plan, COTAs may contribute during the plan’s development.1 The intervention plan, developed in collaboration with clients (and other professionals), focuses on OT approaches to create, promote, establish, restore, maintain, or modify clients’ engagement in occupation or prevent future problems engaging in occupation. An essential element of the intervention plan is the collaboration between clients and OT practitioners to identify and set goals for intervention that focus on specific aspects of a client’s occupation that could improve or be maintained over the course of intervention.
Interventions are then implemented to address the client factors, activity demands, performance skills, performance patterns, contexts, and environments that hinder the client’s engagement in desired activities and occupations.1 Again, this is a collaborative process between clients and OT practitioners and focuses on facilitating a change in the activity demands, the contexts and environments, client factors, and/or a client’s performance skills and patterns that directly result in improved or maintained engagement in occupation. Throughout intervention implementation, the process is monitored for its effectiveness and progress toward the identified goals and is modified accordingly. Intervention implementation is when COTAs are most active in their role as OT practitioners, using their skills to promote engagement in occupation.7
The final element, outcomes, focuses on identifying the success of the intervention.1 Did intervention foster an improvement with a client’s engagement in occupation? Were future problems with a client’s engagement prevented? Methods to evaluate outcomes should be used during the evaluation process and throughout intervention to identify what progress, if any, a client is making toward the goals and priorities identified at the beginning of OT intervention. As with evaluation and intervention, COTAs and OTRs work collaboratively to monitor intervention outcomes.
Certified Occupational Therapy Assistant/Registered Occupational Therapist Competencies with Evaluation, Intervention, and Outcome Process
Continuing competence is a process by which OT practitioners “develop and maintain the knowledge, performance skills, interpersonal abilities, critical reasoning, and ethical reasoning skills necessary to perform current and future roles and responsibilities within the profession.”12 Demonstration of continuing competency is a requirement of most regulatory boards, employers, and accrediting bodies. The American Occupational Therapy Association12 serves to ensure that OT practitioners are providing services based on current knowledge and skills. Establishing continuing competency is ongoing and may involve various methods, such as (a) professional service (e.g., volunteering, peer review, and mentoring), (b) completing workshops/courses/independent learning (e.g., attending seminars, lectures, and conferences; reading peer-reviewed journals and textbooks), (c) presenting (e.g., presenting at state, national, and international conferences; serving as adjunct faculty), (d) fieldwork supervision (e.g., Level I or II), and (e) publishing (e.g., journal articles and book chapters).14 For example, Rachel attended a workshop specifically for COTAs that focused on incorporating a neurodevelopmental approach when providing OT services for elders with strokes. After returning to the rehabilitation center, she directly applied the knowledge and skills from the workshop with elders who had experienced a stroke (see Chapter 19). One elder, Elmer, liked to restore vintage cars and Rachel asked his wife to bring one of their cars to the rehabilitation center. While Elmer polished the car, Rachel worked with him and his wife so that Elmer could learn how to incorporate more normal movement patterns (performance skills) and inhibit muscle tone (client factors).
Establishing competence to practice begins after graduating from an accredited OTA program, successfully completing fieldwork, and passing a nationally recognized entry-level examination for OT assistants.15 In the United States, OT assistants are initially certified by the National Board of Certification in Occupational Therapy (NBCOT).14 Initial certification permits the use of the COTA credential for 3 years. After this period, COTAs may choose to recertify, a requirement to continue using the COTA credential after their name and identify themselves to the public as a certified occupational therapy assistant. Re-certification also requires the completion of professional development units, indicating continuing competency.14
A unique feature within the COTA/OTR partnership is the establishment of service competency for COTAs. Establishing service competency is the process by which a COTA collaborates with an OTR to demonstrate and document that the COTA’s reasoning, judgment, and performance is satisfactory for specific evaluation and intervention methods.4,7 For example, to establish service competency, an OTR may observe a COTA administer the Canadian Occupational Performance Measure (COPM)16 several times with different elders. If the COTA consistently administers the COPM according to the manual’s instructions and the OTR concurs that the results are accurate with each administration, then the COTA has demonstrated service competency to perform this specific assessment. After this time, the COTA may independently perform the assessment and share the results with the OTR, although the COTA may not interpret the results.7 In essence, with the establishment of service competency, less direct supervision is required. Documentation of service competency is recommended and is required by many state regulatory agencies.17
When reentering the workforce or changing practice areas, the demonstration of continued competency is important and likely a statutory requirement.17 For example, Drew had worked in a school setting for 1 year. He always had an interest in working with elders and accepted a job offer from an SNF. Before he began work, he attended a workshop to become familiar with Medicare guidelines and the prospective payment system (see Chapter 6). He also attended study groups with three other COTAs who worked in SNFs, where they focused on specific skills, such as transfer techniques, use of adaptive equipment, and application of hip precautions during ADL. In doing this, Drew was actively demonstrating continuing competency relevant to his new area of practice and meeting state regulatory requirements.
Issues Related to Certified Occupational Therapy Assistant Practice
Overuse and underuse of COTAs in the workplace may occur. COTAs may be underused when employers, as well as supervising OTRs, do not understand a COTA’s degree of skill and knowledge. Restricting a COTA to tasks below his or her skill level, such as those performed by a restorative aide, does not allow COTAs to work to their greatest potential. Tasks such as transporting and scheduling patients, keeping inventory of bath equipment, and assisting patients to eat meals do not reflect the greater knowledge and skills that COTAs acquire during their education. COTAs are underused when they are not permitted to fully contribute when delivering OT services. COTAs are qualified to provide safe and effective OT services under the supervision of and in partnership with an OTR, including conducting assessments and reporting observations; selecting, implementing and modifying therapeutic interventions; and contributing to the transition/discharge process.15
Overuse may occur when COTAs are asked to contribute beyond the scope of their competency and qualifications. Accepting referrals, conducting initial OT evaluations, and interpreting data are examples of tasks that OTRs are required to complete.15 In some instances, this may occur when COTAs are encouraged to take on tasks beyond the legal and ethical scope of practice. For example, an OTR may say “I don’t have time to see the client. Why don’t you start the initial evaluation?” In other instances, COTAs may be asked to perform these tasks when there is inadequate supervision or not enough practitioners to provide OT services.18 For example, the facility administrator may ask the COTA to complete the discharge summaries because he or she wants to employ an OTR only 4 hours a week. In these cases, the COTA must advocate for proper use of COTAs and discuss the issues with the OTR and others who need to understand the legal, ethical, and professional responsibilities of a COTA/OTR partnership.
Certified Occupational Therapy Assistants Working with Elders in Various Settings
During the class reunion, Chris Henson, the OTA instructor for the adulthood and aging course, invited graduates to share their work experiences with the OTA students during a series of class presentations. She was particularly interested in graduates who worked in traditional and emerging practice settings. A synopsis of each of the presentations is presented and integrates concepts from the Framework.1
Geropsychiatric Unit
Marta has worked at a 15-bed geropsychiatric unit in a small urban town for 7 years where she enjoys working with elders admitted with varied psychiatric diagnoses such as dementia, bipolar disorder, and schizophrenia. Although most elders are admitted directly from their homes, typically for behaviors with which their family members can no longer cope, such as aggression and confusion, Marta does not let these behaviors become the focus of her practice. Instead, she views each elder as a unique occupational being, focusing on those daily life activities and occupations of priority and concern to elders and their family members. Marta recently worked with one elder, José, a 62-year-old former migrant farm worker born and raised in Mexico who was admitted to the unit with suspected early-onset dementia. After she and Noel, the OTR with whom she collaborates, discussed the information from José’s occupational profile, they realized that José no longer walked to and visited with friends within the local Hispanic community, one of his most meaningful occupations. José’s family had become increasingly concerned about his memory loss and confusion and was afraid to let him leave the house for fear he would become lost or have an accident. Furthermore, they wanted to preserve José’s dignity and did not want his friends and acquaintances to know about his increasing confusion and memory loss. Although José was admitted to the unit for suspected early-onset dementia, Marta viewed José as an occupational being who was experiencing the loss of meaningful occupations, rather than as a confused man who was becoming a burden to his family.
With Marta’s 9 years of experience as a COTA, the staff relies on her judgment to identify those daily activities and occupations in which elder patients can successfully engage and which aspects of their daily routine present additional challenges and require support and assistance. Marta said that the elders “often look okay and say that they don’t have any problems but the reality is they can get into trouble carrying out simple daily life tasks, if they chose to do them at all.” To restore and maintain more successful engagement in routine activities, Marta relies on her skill to analyze an elder’s performance of activities and occupations, identifying those factors that support or hinder the elder’s successful engagement. Although Noel, the OTR, works with the elders during the morning, Marta works from 2:30 p.m. to 8:00 p.m. during the week, providing her with opportunities to observe elders during their early evening routine of eating dinner, undressing, bathing, toileting, and preparing for bed because performance patterns are important to support successful engagement in activities.19-21 Marta works closely with families and staff to establish consistent routines and habits for elders on the ward, focusing on creating a physical and social environment that promotes success and decreases confusion. With José, she and Noel worked closely with his family so they could create a routine of activities and meaningful occupations when he returned home to help reduce José’s confusion and his verbal outbursts.
Because Marta begins her workday at 2:30 p.m. and Noel ends his at 4:30 p.m., they have little scheduled time for consultation and supervision. Both agree, though, that this time is essential, not only to meet state regulatory requirements, but also to ensure that patients receive quality OT intervention. After her meeting with Noel, Marta leads group activities at 3:30 in the afternoon. Depending on the needs of the group of elders at any one time, Marta will lead groups that focus on life skills, such as craft and cooking groups. Because of the elders’ short stay on the unit, often less than 2 weeks, Marta finds that engaging them in activities that are familiar and not too challenging helps them to make sense of their daily life in the unit. Marta particularly enjoys leading the reminiscence group activity where she engages elders with the use of familiar scents, pictures, and objects, encouraging them to interact and share their personal stories. The gardening group activity is particularly enjoyable because Marta can adjust the challenge of the activity to each elder’s capability. For those elders who experience difficulty potting a plant on their own, Marta decreases the activity demands, such as asking an elder to help scoop dirt out of the bag or holding a pot while someone else scoops in the dirt. For others, merely sitting at the table and smelling the flowers is enough of a challenge. Those elders who are more able can choose what they would like to plant and carry out the process more independently, often sharing their own gardening expertise with Marta and other elders. No matter what capacity an elder may possess, Marta always ensures that all elders have a potted plant at the end of the group activity that they can give to a family member or friend during evening visits.
After leading groups in the afternoon and completing her notes on each elder’s participation, Marta works with the unit staff during the evening dinner hour, observing each elder’s ability to eat meals. Because Marta successfully achieved AOTA Specialty Certification in Feeding, Eating, and Swallowing,22 and she and Noel have agreed she has achieved service competency to manage eating and feeding problems with elders on the unit, Marta is responsible for identifying successful strategies to encourage elders to eat their meals and conveys those strategies to staff members for all meals and snacks. As needed, she will suggest and monitor the use of adaptive equipment. Although it can be challenging at times, Marta also works to create a pleasant and supportive environment during the dinner hour in which elders can successfully interact with family members when they choose to visit.
Because Marta works a later shift, she is responsible for meeting with family members and educating them not only about their elder’s diagnosis, but also about what level of care is currently required. She is particularly adept at identifying what aspects of activities each elder can do on his or her own and what aspects with which he or she requires assistance. Occasionally, family members may want to protect and help the elder too much and Marta works with them to preserve the elder’s independence and dignity while teaching family members to provide the right amount of support.
Although Marta relies primarily on informal observation to gather important information about the elders, she occasionally administers the Allen Cognitive Level (ACL) screening tool23 for which she has established service competency. Although Noel interprets the results, together they share the information with other team members. This information is useful because it provides insight into an elder’s cognitive abilities and his or her capacities in specific tasks or groups. Most of the time, though, Marta relies on her skills to analyze an elder’s performance of activities during groups and their evening routine. These informal observations provide her with the valuable information that she needs to help the elders and their family members plan to return to their own homes.
Inpatient Rehabilitation
After graduating from Blue Lake Community College 5 years ago, Rachel moved to a large metropolitan city and began full-time work at an inpatient rehabilitation facility. She and Beth, the OTR with whom she works, share a caseload of 12 patients, the majority of whom are elders who have experienced a cerebrovascular accident (CVA). Rachel, who does not consider herself a “morning” person, nonetheless arrives at work Monday through Friday at 7:30 a.m. She starts her day working with patients in their rooms, assisting them to achieve greater independence and satisfaction with their morning ADL, such as eating, grooming, dressing, toileting, and bathing (Figure 8-1). One of her favorite elders was Glen, with whom she worked after he experienced a CVA. When Rachel was assisting Glen in the mornings to get ready for the day, Glen would become frustrated because he could never find his hearing aide. One day it would be in the drawer under his clothes and the next it would be under the bed sheets. Rachel communicated with the evening nursing staff to ensure that Glen always put his hearing aide in the top right drawer before he went to bed. Although this seemed like such a small thing to do, Glen was much happier each morning because he could easily locate his hearing aide. Rachel works extra hard to establish routines for elders on the ward, recognizing that establishing performance patterns is particularly important for elders when they are away from their usual home environment.

FIGURE 8-1 Certified occupational therapy assistants work with those personal activities of importance to the elder.
During the initial OT evaluation conducted by Beth, the OTR, Glen raised a concern that he did not want to be a burden on his wife when he returned home. During Glen’s short 12-day admission, Rachel worked diligently to ensure that Glen’s wife would be comfortable and safe assisting Glen at home. Thus, although independence with toileting, dressing, and bathing was not the ultimate goal, during Glen’s morning routine Rachel and Beth focused on developing Glen’s performance skills so it would be easier for both Glen and his wife when Glen returned home. Although Glen was not pulling up his pants on his own by discharge, Rachel had worked out a system whereby Glen was able to stand upright on his own and safely stabilize himself on a solid counter while his wife pulled up his pants and fastened them for him.
After morning ADL and during the remainder of the day, Rachel and Beth work together to help the elders reach their goals, collaborating to share the responsibility for gathering initial evaluation information, implementing intervention, and evaluating outcomes. During her level II fieldwork, Rachel had observed her supervisor administer the COPM,16 although Rachel had never done it herself. Because the COPM is an open-ended interview requiring the OT practitioner to solicit the occupational performance issues of concern to the client, Rachel and Beth developed a plan for Rachel to become comfortable and achieve service competency to administer the COPM and other standardized assessments.
When Rachel interviewed Glen using the COPM,16 Glen identified that he still wanted to be able to take care of his 5-year-old grandson Brandon because Glen and his wife provide child care 3 days a week. Because this was a priority for Glen, the afternoon OT sessions were devoted to help Glen develop the performance skills needed for Glen to play catch and read story books with Brandon. Rachel worked with Glen to develop the specific motor skills necessary to play catch, such as bending and reaching for a ball on the ground and grasping and lifting the ball with his affected arm and hand. Rachel also worked with Glen on skills necessary to read story books, such as manipulating the pages and coordinating his affected arm with his other arm to hold the book. On the basis of the occupational profile completed during the initial evaluation, Rachel knew that Glen enjoyed challenging physical activities because he considered himself a sportsman. She particularly enjoyed working with Glen to identify various physical activities, both within the OT department and outside of the hospital, which would further develop his motor skills to help him reach his personal goals. Rachel was able to draw on Glen’s strengths, specifically his relatively good communication, social, and cognitive skills to help Glen improve his ability to perform daily life activities.
An important aspect of Rachel’s work, although not her favorite, is documentation. To demonstrate the need for OT intervention, Rachel and Beth have worked together to develop their documentation skills. They have attended conference workshops and met with local insurance representatives to explain the focus of OT and to understand the insurance representative’s point of view. Rachel and Beth share responsibility to write progress notes for their caseload. Although the OTR is ultimately responsible for documenting outcomes,15 Rachel contributes to the process, sharing her understanding of what has occurred during intervention. Because Beth and Rachel agree it is important that clients also express their views regarding their progress, Rachel often readministers the COPM16 before discharge. Although Glen did not make much progress with his morning ADL in terms of physical independence, the use of the COPM revealed that he was more satisfied with his performance because he believed that he was no longer as much of a burden to his wife. Although he did not believe he was entirely able to take care of his grandson, he felt he was far better than when admitted to the rehabilitation unit. By using a standardized assessment such as the COPM, Rachel and Beth have more credible evidence to document an elder’s progress and communicate the outcomes and benefit of OT services to help elders achieve their personal goals.
Adult Foster Home
After graduating 2 years ago, Arianna reflected about what aspects of OT practice she liked. She decided she liked working with elders and particularly enjoyed group activities. Because she had the opportunity during her professional education to explore settings that were not based on a medical model, Arianna also recognized that she preferred more nontraditional settings. During her course on adulthood and aging, she spent time at a local senior center where she helped with an exercise program for people with arthritis. Through this experience, she became a certified instructor in exercise and aquatics, which qualified her to teach exercise classes and swim classes.24 Moreover, a portion of her fieldwork was spent at an assisted living center where she spent time running groups with the activity director. She was able to incorporate the skills and knowledge she learned in her OTA classes, such as designing and organizing groups, leadership strategies, group dynamics, and stages of group process, as well as meeting the individual needs of the group participants.25
She noticed an adult foster home in her neighborhood and approached the owners, Elizabeth and Danny, about providing group activities for the elders. Arianna knew, per state regulations where she lived, that adult foster homes are required to provide 6 hours of activities a week for each resident, not including television and movies. Because the state requires the activities to be of interest and meet each elder’s abilities, her COTA skills to identify, adapt, and implement appropriate activities for elders were exactly what the owners needed. Arianna talked about her experience working with elders and her abilities to develop and lead group activities. She explained to the owners that, although she was a COTA, the services she would provide would not be considered OT. She would use expertise that did not require OTR supervision, such as making sure that elders were seated securely with their feet flat on the floor and using activities that incorporated full range of motion. Elizabeth and Danny were interested because they had been trying to provide activities without any outside help. After clarifying her intent with the state licensing board, Arianna began working, providing 2 half days of activity programming and consultation per week.
Most of the seven elders at the adult foster home were ambulatory; only one elder used a wheelchair. Anthony and Florence were legally blind, Maria had a severe hearing loss, Alfred used oxygen 24 hours a day for his chronic obstructive pulmonary disease, Herbert had Parkinson’s disease, and Leona and Alfonso had mild dementia. Arianna met with each elder individually to get to know them and identify their interests. She used her COTA skills to develop a profile that noted each elder’s interests and dislikes, as well as information related to medical needs, such as dietary restrictions, allergies, and “do not resuscitate” status. She also developed a form to document the type of group activity, the length of time each elder participated, the degree of participation, how each elder responded during the activity, and whether he or she declined to participate that day. This form was left at the adult foster home at the end of the month for the owners and served the purpose of documenting participation, as well as a time sheet for her hours worked. The owners employed other people so a payroll tax system was already in place. Because Arianna’s husband’s employer provided health insurance coverage for spouses, she was fortunate in not having to worry about this.
To provide a solid basis when designing group activities, Arianna organized and implemented a variety of activities, following Howe and Schwartzberg’s25 guidelines for group process. Arianna began each group with small talk, encouraging each resident to discuss current events. Arianna would then incorporate warm-up activities to encourage movement, such as telling a story with the elders acting out the movements. Activities such as marching in a parade or playing balloon volleyball were popular with the elders. Then the main activities would follow, focusing on those activities of interest to the elders, such as preparing the salad for the evening meal, planting herbs in pots, making place mats for holiday meals, and learning new card games. Each group activity closed, by asking the elders to help plan future activities.
As with well-designed groups, the elders would often direct the activities themselves. For example, while making strawberry shortcake, Leona began reminiscing about growing up in an area where there were many berry farms. She lamented that a community college and housing development now occupy the berry fields. Others joined in and talked about how they had to pick berries to earn money to buy their school clothes. Despite her memory loss, Leona shared her mother’s favorite jam recipe and asked if the group could make the jam at the next meeting. During another activity, Florence shared how she used to enjoy playing Bingo but is currently not able to get out to games and cannot see the cards well enough to play. Arianna took note and another activity was designed where the elders made Bingo cards with large black numbers so that everyone could see and participate. Arianna also purchased poker chips to cover the numbers because Herbert had trouble picking up small disks. The elders’ favorite activities, though, were ones that included cooking or baking. They took pride in preparing meals and inviting family members. Even Alfred, who “never cooked a meal in his life,” participated and took pride in telling his daughter that he made the cornbread by himself (even though he did require some help!). During the majority of the time, Arianna planned activities for all residents to participate. She also made sure that when an elder did not want to participate in group activities, she would offer alternative solitary activities.
Not all of the activities were confined to the foster home. The owners had a van and would occasionally take the elders to eat at local restaurants because they enjoyed getting out and eating their favorite foods. On those occasions when Arianna accompanied them, she sat close to Florence and Anthony, both legally blind, and suggested that they orient the food on their plate like a clock. Elizabeth took note and followed through with this suggestion at home with the elders. She reported that both Florence and Anthony were much happier with not needing someone to hover over them during meals. Arianna also suggested a weighted cup for Herbert and provided the phone number of a local vendor. As Arianna became more familiar with the residents, she suggested other community outings such as a trip to a lilac garden, a drive to see Christmas lights, a picnic in the park, and attending local music events at the senior center.
After working at the foster home for 3 months, Arianna expanded her services to other local adult foster homes. The owners were happy with her services and passed along Arianna’s business card to other adult foster home owners. Arianna now provides group activities to five foster homes and hopes to find another COTA who is interested in this work to expand the business. Moreover, with senior centers becoming an emerging practice setting for occupational therapy practitioners,26 Arianna is considering approaching the local senior centers to discuss the development of educational programs. She wants to again contact her state licensing board, however, to understand the parameters under which she can provide health promotion services while also licensed as a COTA.
Skilled Nursing Facility
After graduating 1 year ago, Drew moved to a rural city of 30,000 people and now works full-time at an SNF. At the reunion, he shared that, although he is frustrated at times with the facility rules and insurance regulations, he enjoys working with family members to help elders return home as soon as possible. He shared, “It’s tough working toward discharge right away, but then you realize most people’s priorities are to get home as soon as they can.” Drew primarily sees elders with CVA, as well as those with hip fractures and recent surgeries. Many have secondary health conditions, such as high blood pressure, diabetes, or pneumonia.
Drew particularly enjoys working with elders and their families to figure out the best way to manage ADL at home, including the need for adaptive equipment; thus, the primary intervention approaches he uses with elders are restore and modify. One of the most problematic issues for elders leaving the SNF is toileting and bathing at home. Drew particularly prides himself on his ability to analyze each elder’s performance. When observing an elder on the ward, Drew recognizes that the elder’s home environment may be very different from the accessible and well-equipped rooms at the SNF. For example, he recently worked with Clarence, an elder who was admitted with a severe case of pneumonia and long-standing arthritis. Clarence and his partner were concerned about Clarence still being able to get in and out of his bathtub and soak in the warm water to relieve his arthritic pain. As best he could in the OT bathroom, Drew re-created the layout of Clarence’s bathroom at home. He then observed Clarence’s partner assisting Clarence to get in and out of the tub. After they tried out different methods, Drew identified the safest and least painful transfer method, which they practiced until Clarence and his partner felt confident. Drew also identified which specific equipment would best meet their needs at home. This was particularly important because many elders may not start home health immediately after discharge from the SNF, and all necessary equipment needs to be in place before their departure.
Although a main focus of the SNF is promoting independence with ADL, Drew also addresses other roles that are important to the elder (Figure 8-2). Because Clarence was a retired veterinary technician, he was also concerned that he could not take care of his many birds at home. Drew worked with Clarence and his partner to figure how Clarence could safely stand and easily reach while feeding and watering the birds and cleaning the cages. Drew also arranged with the staff for Clarence to play with the resident dog and cat as often as possible when he was not scheduled for therapy. Because Clarence also sang in the church choir, Drew worked with Clarence and his partner to develop a plan so that Clarence could conserve enough energy to attend church twice a week.

FIGURE 8-2 Instrumental activities of daily living are often important for elders for when they return home.
In addition to his direct work with the elders, Drew has additional responsibilities. He participates in the weekly team meetings, sharing the reporting responsibilities with Sheryl. Drew and Sheryl also collaborate to leave clear instructions for Brooke, the COTA who works weekends. Drew also spends part of his time working with restorative aides, ensuring that they can follow through with intervention plans. Drew and Sheryl agree that he would assume the primary responsibility to be aware of current regulatory and reimbursement issues related to SNF (see Chapter 6) and share the information with Sheryl and Brooke.
Assisted Living Facility
Jean has been a COTA for 17 years. After graduating, she took a job at a local rehabilitation hospital and worked mainly with adults experiencing neurological disorders. She enjoyed the work, but, because of budgetary problems, her position was eliminated. She then worked at a large long-term care facility where her level of responsibilities increased over time. Having established service competency with the OT evaluation and intervention methods used at the facility, she worked fairly autonomously with occasional OTR supervision. Four years ago, Jean returned to school on a part-time basis to complete her bachelor’s degree in health care administration. As Jean was learning management skills, she decided to apply for a position as the director of the OT department. Given her competency as a COTA and her current interest and skills in management, she was offered the position. Jean was now responsible for running the department, including scheduling therapy, coordinating the training and supervision of the employees, and maintaining communication between OT and the other services offered at the facility.
After graduation and the completion of her business degree, she began to seriously consider her future. She enjoyed the management skills that she had learned and developed over the past few years as OT director. She was not sure that remaining in her current position would allow her to grow further so she began looking at other possibilities. First, Jean compiled a list of her abilities that she could bring to the job. She tried to be as realistic as possible and asked for assistance from her husband, parents, and friends who knew her professionally. She felt that she had good supervisory, interpersonal, verbal, and written communication skills. Finally, she was familiar with health care and rehabilitation in particular. However, her challenges were that she had limited experience in marketing, operations management beyond the OT department, and budgeting.
At first, Jean looked for jobs related to OT, rehabilitation, and health care delivery and was discouraged by what she had found. Then, she expanded her search after talking with her neighbor, whose mother was living in an assisted living complex. Jean searched the Internet for information about assisted living facilities and found the website for a corporation that operated a number of facilities in her area. She learned that there were three categories of positions: activities coordinator, executive administrator, and resident services coordinator.
Jean downloaded the three job descriptions and compared them to her list of abilities. The first job description that Jean reviewed was for activities coordinator (Table 8-3). Jean believed that this job was not challenging enough. Moreover, according to state regulations, if a perception existed that she was providing direct OT services, she would require OTR supervision. Besides, she felt this was not the type of job that interested her enough to leave her current position at the long-term care facility.
TABLE 8-3 Activities Coordinator Job Description
| Job position | Activities Coordinator |
| Primary purpose | This person is responsible for the development and coordination of individual activity programming for each resident. Responsibilities include planning and coordinating appropriate resident activities, day-to-day operations, supervising staff, and ensuring program quality. |
| Qualifications/skills needed | Prefer an individual with a minimum of 2 years geriatric experience. Experience working with people with Alzheimer’s disease/dementia is essential. Experience in staffing and managing the day-to-day operations is preferred. Must demonstrate good interpersonal skills and excellent written and verbal communication. Reports to resident services coordinator. |
The next position that she reviewed was for executive administrator (Table 8-4). Jean compared the job expectations with her abilities and realized that she was lacking in several categories. Although she has had experience at managing a small department, she lacked the marketing, budgeting, and operational management background required for this position.
TABLE 8-4 Executive Administrator Job Description
| Job position | Executive Administrator |
| Primary purpose | This person is responsible for the creation of resident-focused work teams that support the philosophy of partnering with families. Responsibilities include staffing, training, program implementation, budgeting, sales, marketing, and community relations. |
| Qualifications/skills needed | Prior experience managing senior resident services is required along with a bachelor’s degree. Experience in marketing, operations management, and budgeting is essential. Strong leadership skills, including organization and interpersonal skills, are a must. Excellent verbal and written communication skills required, as well as computer experience. Occasional travel required. |
The final job description Jean reviewed was for services coordinator (Table 8-5). Jean studied the job description and compared it to her list of abilities. Because she believed that this was the right position, Jean contacted the assisted living corporation and requested an application. She applied and was contacted for an interview. Before the interview, Jean wanted to clarify that the services she would provide in this position were not those of a COTA requiring OTR supervision. She contacted her state’s OT licensure board and asked them to review the job description. On careful review, the Board determined the following: (1) Her status as a COTA in this position did not violate state laws and regulations; (2) although the position oversaw the coordination of programs, including OT, it did not require Jean to perform hands-on OT; and (3) Jean could use her COTA initials after her name (she had kept her NBCOT certification up to date) as long as it was understood that she could not provide any OT services without the supervision of an OTR.
TABLE 8-5 Resident Services Coordinator Job Description
| Job position | Resident Services Coordinator |
| Primary purpose | This person is responsible for overseeing the delivery of resident services and supervising the resident assistant staff. As a member of the management team, responsibilities include supervising unit teams, staff development, and monitoring quality of resident service and staff recruitment. Reports to executive administrator. |
| Qualifications/skills needed | Person should possess a bachelor’s degree in a health-related field. Five years experience in senior resident services, including staff supervision, is required. Excellent organizational and interpersonal skills are a must. Strong verbal and written communication skills are essential. Computer proficiency is strongly preferred. |
Meanwhile, Jean prepared for the interview by identifying the major points she wanted to emphasize. First, she wanted to stress the importance of addressing the elders’ needs, including physical, social, emotional, cognitive, and spiritual, and how this belief would guide staff recruitment and development. Second, she wanted to demonstrate how she would coordinate the services in a manner that supported the corporation’s philosophy of partnering with families. Third, she wanted to show that her background as a COTA brought a unique perspective on quality of life for elders. She located information that identified that life satisfaction is multifaceted for elders27 and that the manner in which elders occupy their time contributes to their health, well-being, and quality of life.28,29
During the interview, Jean did well and was offered the position. Since then, she has been working with the new executive administrator, assisting with recruitment and development of the resident service teams. One of the first tasks she undertook was to develop a screening tool to identify the physical, social, emotional, cognitive, and spiritual needs of the residents. Her goal was to match the services with the identified needs and eventually demonstrate how the residents’ overall needs were being met.
Home Health Agency
Manisha recently changed jobs after working 9 years in an acute care hospital when she obtained a job at a home health agency within a major metropolitan city. Because Manisha used only public transportation before this job, she needed to purchase her first car, one that was spacious enough to carry needed equipment and supplies. Furthermore, Manisha needed to brush up on her map reading skills because her new supervisor emphasized that she would be traveling extensively, often up to 80 miles a day. Because this agency recently converted to a computer-based documentation system, Manisha signed up for a computer course at a local community college. An important issue emphasized during her interview was client confidentiality. Although Manisha was aware of this issue from her work in acute care, Manisha would be visiting many elders during the day, carrying the required documentation from house to house, and would need to take extra care to ensure that that information was kept confidential during her visits.
During her first few weeks on the job, she traveled with different team members, including nurses, physical therapists and physical therapist assistants, social workers, nutritionists, and home health aides. During these visits, Manisha was surprised by how different things were in the elders’ home environment than what she imagined when she worked in acute care. Sometimes, solutions that were proposed in the hospital (similar to those proposed by Manisha when she worked there) turned out to be impractical or the elders just did not want to use them. Recognizing this, Manisha was excited to be working with elders in their own homes where she could assist them to achieve their goals within their familiar home environment, focusing on practical solutions in context (Figure 8-3). Manisha looked forward to working with elders and their caregivers to achieve their goals, such as getting out in the back garden on their own, emptying the trash, getting the mail, operating the radio, or using the telephone to reorder prescription medications.

One elder, Irene, had lived by herself in a one-room apartment and was getting along fairly well despite her legal blindness. Irene recently broke her foot while getting off a high stool in her kitchen. After receiving the doctor’s referral, Antonio, the OTR with whom Manisha worked, completed the initial evaluation. Antonio shared the initial evaluation results and developed the intervention plan with Manisha, stressing that her input was important to monitor the effectiveness of the plan. Manisha then assumed primary responsibility for implementing the intervention plan and monitoring the achievement of outcomes. Although Manisha would be on her own visiting Irene over the next month, Manisha would consult as needed with Antonio when they were both in the office in the morning. Furthermore, she frequently communicated with him, as well as with Irene’s social worker and physical therapist, through cell phone calls throughout the month.
One of Irene’s first priorities was to prepare her own meals rather than rely on the Meals on Wheels initially organized by the social worker. Although it was important to Irene that she prepare her own meals, she did not want to spend a lot of time doing so. After Manisha’s first visit, Irene searched for recipes that would be easy to prepare and nutritious and arranged for her neighbor to purchase the necessary ingredients. During the next visit, Manisha and Irene problem solved how to safely prepare simple meals that would not compromise her fractured foot, such as safely using a low chair and safely maneuvering within the kitchen. To make it easier to transport items, Manisha also arranged for Irene to purchase a basket for her walker and to practice safely carrying her recycling items and trash down the hallway.
Because Irene was a volunteer at the blind commission, it was important for her to be able to use public transportation as soon as possible to return to her monthly meetings. Although Irene’s home visits would end as soon as she became more mobile, she and Manisha problem solved how best to manage her walker while using the bus. They practiced skills such as managing doors, stepping up and down different levels while using the walker, and folding up her walker once she was seated. Another priority of Irene’s was to plan and be able to execute an emergency exit from her third-floor apartment. She and Manisha developed a plan with Irene’s neighbors to deal with different types of emergencies. For some situations, a buddy system would be used; for other situations, Irene could make the necessary arrangements through a telephone call.
Because Irene’s broken foot presented additional challenges to safely maneuver within her apartment, Manisha and she worked together to rearrange her living and dining room to make it easier and safer for her to listen to the radio and books on tape, as well as use her computer. Although Manisha works most of the time with individual elders, such as Irene, on occasion she is called in to an adult foster home to recommend environmental modifications. For example, she has recommended suitable bath and toilet equipment and more appropriate furniture arrangement to prevent falls. Manisha understands the significant meaning that home has for many elders,30 and so when recommending environment modifications, she always considers the elders’ viewpoints.
Manisha enjoys working in home health because it provides a lot of variety. She visits four to five people a day, the majority of whom are elders. Because she visits elders in their own homes, Manisha is particularly sensitive to being a guest, respecting the elders’ privacy and following their lead to establish intervention priorities. This includes collaborating with elders and their families/caregivers as to the best approach to achieve their priorities. Many times this involves working closely with family members to provide education and training, emphasizing safety for not only the elders, but also for the caregiver (see Chapter 11). Because Manisha is skilled with body mechanics and safety concerns/issues, she is responsible for home health aide staff training, providing them with information and skills to safely assist elders (e.g., while toileting, dressing, and bathing).
One of the most important skills that Manisha brings to this particular job is that of observation. Because she has been the primary OT practitioner working with the elder, Manisha must provide accurate information to the OTR. Often, detailed information is required per regulatory and facility guidelines.31 In Irene’s case, to complete the discharge summary, Manisha needed to provide information to Antonio, not only about Irene’s ADL status, but also such factors as Irene’s ability to accurately express herself, whether any sanitation hazards were present in the home, which social supports she consistently relied on, and whether she was capable of making safe decisions.
Free Standing Hospice
When Amanda graduated from Blue Lake Community College 14 years ago, her children were toddlers. To balance her work and family life, she chose to work on-call 2 to 3 days a week at various local SNFs, which she continues to do. For the past 10 years, she has volunteered at Riverview House, an independently owned hospice that provides end-of-life care for individuals who cannot receive services at home. Amanda appreciates the approach at Riverview House where staff and volunteers focus on enhancing a person’s quality of life, paying equal attention to the spiritual, emotional, and physical aspects of life. The pace at Riverview House is unhurried with an emphasis on quality time until death. Amanda finds great personal reward in her volunteer work.
Almost 2 years ago, Amanda faced the prospective of death in her own family. Her favorite aunt, Paula, was diagnosed with ovarian cancer and expressed a wish to stay at home. Amanda decided that she could help fulfill her aunt’s wish. Her volunteer experience at Riverview House, as well as her COTA experience working in SNFs, provided her with the capacity to feel comfortable with terminally ill individuals and the ability to cope with loss. Moreover, having attended an in-service at Riverview Hospice that emphasized strategies to prevent burnout in hospice personnel,32 Amanda knew that it was important to maintain her physical well-being, engage in hobbies and interests, take time away from her caregiving, talk with others, and engage in meaningful activities. Amanda arranged for her daughter and niece to provide respite care several times a week so she could spend time with her partner and friends and go to the gym. She and her partner also spent time each week engaged in contemplative activities, walking the labyrinth at a nearby Buddhist retreat and meditating at the local church.
Although Amanda previously experienced the challenges and responsibilities of caring for dying persons, she soon found herself physically and emotionally drained. She was distraught as her aunt experienced a loss of control, diminished ability to engage in her favored daily activities, and physical and emotional pain. As her aunt’s condition worsened, home care hospice services were formally instituted. Although a substantial commitment, Amanda decided she wanted to continue as her aunt’s primary, live-in caregiver, a usual requirement for home-based hospice services. She also decided to attend a caregivers’ support group at the local hospital to help cope with such a challenging, emotional endeavor. Aunt Paula lived long enough to attend the college graduation of her great grandson and died at home with family by her side.
After her aunt died, Amanda spent time recuperating, re-engaging in projects she had put on hold during the 8 months she cared for her aunt and taking a month-long vacation with a close friend. When she returned, she contacted the director at Riverview Hospice to initiate discussions about the potential inclusion of OT services. Because the director was familiar with Amanda’s volunteer work, she was happy to meet and discuss her ideas. Amanda shared how the philosophy and approach of hospice were very compatible with those of occupational therapy.33 She then shared her vision of how OT services might further enhance hospice care.
Amanda emphasized the skills that OT practitioners possess to facilitate participation in daily activities that people find meaningful, such as cooking simple meals, engaging in art projects, and writing in journals. Amanda then shared one of her volunteer experiences. She was with Joe, an elder who previously enjoyed fishing and camping and who was complaining that there was nothing he could do now. Amanda gently suggested that Joe might consider barbecuing a trout for the staff at Riverview House; he agreed and contacted his wife to bring in his secret spices to prepare the trout. Meanwhile, Amanda made arrangements with staff to make it easier for Joe to safely use the backyard barbecue. Connecting to his love of fishing and camping through the simple preparation of a barbecued trout provided Joe with a sense of self, and connecting his current self to his past life.
Amanda went on to explain that occupational therapy practitioners work with individuals throughout the life span, death and dying being one phase among many. Amanda discussed her experience with Vivian, a lively woman with a sense of humor and quick wit. Vivian enjoyed being with others, especially her family. When she was diagnosed with terminal breast cancer, she decided to move from another state to be near her family of four generations. She would live at Riverview Hospice until her death, where her care could be provided without being a burden to her family, a point she was emphatic about. Vivian was thrilled to be near her 3-year-old great-grandson with whom she shared a special bond (Figure 8-4). She looked forward to his daily visits but soon found herself exhausted and in pain by the time he usually arrived in mid-afternoon. Amanda suggested whether it might be possible for Vivian’s family to arrange for her great-grandson to arrive during lunch, where they could eat together and cuddle afterward during a nap. Moreover, Amanda suggested that Vivian listen to some relaxation tapes just before lunch to help alleviate her pain before her great-grandson arrived. Amanda explained that it was important to not only schedule rest periods, but also to consider when to schedule valued activities throughout the day.

FIGURE 8-4 A special bond existed between Vivian and her 3-year-old great-grandson.
(Courtesy Sue Byers-Connon).
Amanda went on to explain that OT practitioners are committed to facilitating the process of enhancing the quality of life of individuals and that they have particular expertise to modify a person’s performance so that he or she can engage in desired activities. She shared the story of Cora, who was experiencing end-stage congestive heart failure and neuropathy in her fingers, making it difficult for her to hold eating utensils. Amanda knew that changing the silverware would make it easier for Cora to eat, but she also understood the enjoyment that eating meals with others can bring. The next week she brought in some silverware with sticky handgrips (which still looked normal) and asked if she could join Cora for lunch in her room. She showed the silverware to Cora and asked if she would like to give them a go. Cora agreed and found eating a bit easier; however, she still chose to eat in her room. A few weeks later, Amanda gently asked if Cora would join her in the dining room for lunch. Cora agreed, and when lunch was over, asked if Amanda would come back next week. When Amanda returned the following week, she discovered that Cora had been eating her meals in the dining room. Because Amanda gradually modified Cora’s engagement, Cora was able to enjoy her meals, socializing with other residents and family members in the dining room.
The director was impressed with Amanda’s understanding of the compatibility of OT with the practice of hospice and realized that other professional practitioners exist who bring important skills that support the hospice philosophy. Amanda and the director agreed to continue meeting and discuss the possibility of instituting formal OT services at Riverview House, including the need for an OTR/COTA partnership to fully realize the potential of OT services with elders at the end of life.
Adult Day Care
Carlos, who graduated 4 years ago, works at an adult day care center in an urban setting. This particular setting has a continuum of care that also includes assisted living, independent apartment living, and adult foster homes. The elders attend day care 5 days a week from 9:00 a.m. until 3:00 p.m., receiving lunch, health services, and activities in which to participate. Carlos has a dual role within this setting. His primary role is as an activities director, in that he identifies and plans individual and group activities for the day care participants throughout the week.34 In his other role, he works with Sydney, an OTR, in providing OT services for all clients along the care continuum.
To determine whether an elder requires individual OT intervention, Sydney, the OTR, begins the initial evaluation with an occupational profile, identifying what is currently important and meaningful in regard to the elder’s occupational needs. Mr. Kirov, a new day care attendee, had recently fractured his humerus and was having difficulty performing activities with only one arm and hand; consequently, Sydney conducted an initial evaluation. As a result, specific OT intervention was initiated to address his problems with performing activities. To identify which group and individual activities would be appropriate for each elder attending the day care center, Carlos (in his role as the activities director) meets with each elder (and the family, when possible). Carlos also met with Mr. Kirov who identified that he enjoyed using his hands to make things and that he liked to talk with people. From this, Carlos recommended that he participate in the craft activities and other activities that included discussion, such as current events and reminiscence. Note: In his role as the activities director, Carlos does not provide OT services.
Carlos starts off his day by attending a team meeting. At this center, the bus drivers, the chaplain, the custodial staff representative, and home health aides attend, as well as the more typical team members, such as nurses, social workers, physicians, and physical and OT practitioners. Everyone contributes during the team meetings. Recently, the bus driver reported that Mrs. Chang experiences shortness of breath while getting on the bus, and a home health aide shared the progress that Millie has made with feeding her cat by herself. After the team meeting, Carlos divides his time—he provides one-on-one occupational therapy intervention under the supervision of Sydney and designs and implements group and individual activities for the day care attendees. Because social participation is integral to an elder’s health and well-being,35,36 Carlos uses his COTA background to plan and implement groups to ensure that the elders engage in culturally rich and sensitive social activities that they enjoy and find meaningful. One of the most popular groups is the Helping Hands group. The theme of this group is to provide the elders with a sense of contribution to the community. In the past, they have put together gift baskets for migrant workers, solicited grooming and hygiene products for military personnel, read to preschool children, and stuffed envelopes for a local school board election. Carlos enjoys this group because he knows that elders enjoy engaging in altruistic activities in which they help other people.37,38 Other groups that Carlos plans and implements weekly and monthly are gardening, music, reminiscence, movement, and crafts. In addition, Carlos makes an extra effort to contact family members to discuss options for activities at home in which the elders can successfully engage and enjoy.
During one-on-one OT intervention, Carlos addresses specific concerns with performance of daily living activities and occupations. Recently, Carlos worked with Mrs. Chang after she began experiencing increased breathlessness caused by her chronic bronchitis. Mrs. Chang’s family reported that during the weekends she wanted to help her daughter and son-in-law with household chores and would push herself too far and become breathless. Because Mrs. Chang valued her role as a family member, Carlos worked with her and her family to identify which activities she considered important and which activities her family felt comfortable allowing her to do. Carlos then worked with Mrs. Chang and her family to develop a routine, incorporating energy conservation techniques that would allow her to complete activities without becoming breathless and tired.39 Within a month, Mrs. Chang’s family reported that she was helping with household chores without getting tired and breathless. More importantly, she was extremely happy to be able to make a valuable contribution to the family and felt that her health, well-being, and life satisfaction was better than before. Because health promotion is a primary focus of the organization, Carlos also works with other team members to deliver a falls prevention program during which elders meet in small groups for 7 weeks.40 Carlos is particularly proud that he is the team member responsible for the follow-up home visit to oversee the implementation of safety strategies by the group participants in their home environment. In doing so, Carlos can see first-hand the important role that COTAs can play to promote health for elders.
Conclusion
Over the next 3 to 4 decades, the population of elders will increase significantly, the number of elders with disabilities living in the community will expand sharply, and the percentage of elders (particularly those over age 85 years) residing in SNFs will rise dramatically.41 Such trends suggest that COTAs will continue to work with elders in both traditional and emerging practice settings, focusing on daily life activities that are meaningful to elders. In doing so, COTAs will continue to provide a valuable contribution during the delivery of OT services.
After the series of presentations at Blue Lake Community College, the OTA students were excited and enthusiastic about the variety of opportunities waiting for them after graduation. Their instructor, Chris Henson, emphasized that their unique COTA skills and knowledge prepared them to work with elders in traditional settings such as SNFs, rehabilitation centers, geropsychiatric units, and home health. She went on to say that the job opportunities did not stop there. As Arianna and Jean had demonstrated, they used their COTA background to create new job opportunities in emerging practice areas. Chris Henson concluded that Carlos, who worked in adult day care, was a good example of a COTA who works in collaboration with an OTR to provide OT services but also can use his COTA background to assist elders in engaging in meaningful activities that do not require the direct supervision of an OTR. In all cases, whether in typical or emerging practice settings, the Blue Lake Community College graduates were engaged in opportunities that brought satisfaction to themselves and quality services for elders.
1. Discuss service competency and continued competency for COTAs and ways to establish each.
2. A COTA and OTR work together in a rehabilitation setting and have different ideas regarding intervention for elders. Suggest three ways that they can learn from each other and form a collaborative partnership.
3. A COTA who is a new graduate and an OTR who recently moved from another state are working to develop a supervision plan. Locate three resources to assist them, develop this plan, and explain what information they would seek from each resource.
4. Identify three activities that you consider meaningful (an occupation) and identify three that you consider merely an activity. Explain the differences.
5. Explain why it is important to focus on both occupations and activities to enhance an elder’s health, well-being, and life satisfaction.
6. Why should COTAs consider the caregiver/significant other/spouse/family when collaborating to develop an intervention plan for an elder?
7. Three COTAs have been hired to work in an SNF. One is a new graduate, one has 5 years of experience working in a rehabilitation setting, and one previously worked in an outpatient adolescent psychiatric unit. Develop a continued competency plan for each COTA.
8. Identify three different potential emerging practice settings in which COTAs might consider working. List five skills for each setting that COTAs receive during their education that would be helpful to secure a position in that specific setting.
9. What previous experience should a COTA have before considering hospice work?
1 American Occupational Therapy Association. Occupational therapy practice framework: Domain and practice. American Journal of Occupational Therapy. 2008;62(6):625-683.
2 National Certification Board for Certification in Occupational Therapy. Executive summary for the practice analysis study: Certified occupational therapy assistant, COTA. Gaithersburg, MD: Author; 2009.
3 Dunn W. Best practice philosophy for community services for children and families. In: Dunn W., editor. Best Practice Occupational Therapy: In Community Service with Children and Families. Thorofare, NJ: Slack, 2009.
4 American Occupational Therapy Association. Guidelines for supervision, roles, and responsibilities during the delivery of occupational therapy services. American Journal of Occupational Therapy. 2009;63(6):797-803.
5 American Occupational Therapy Association. Occupational therapy code of ethics. American Journal of Occupational Therapy. 2005;59(6):639-642.
6 American Occupational Therapy Association. Scope of practice. Bethesda, MD: American Occupational Therapy Association; 2009.
7 Sands M. The occupational therapist and occupational therapy assistant partnership. In Crepeau E.B., Cohn E., Schell B.A.B., editors: Willard and Spackman’s Occupational Therapy, 10th ed, Philadelphia: Lippincott Williams & Wilkins, 2003.
8 Dillon T.H. Practitioner perspectives: Effective intraprofessional relationships in occupational therapy. Occupational Therapy in Health Care. 2001;14(3-4):1-15.
9 American Occupational Therapy Association. Occupational therapy practice framework: Domain and practice. American Journal of Occupational Therapy. 2002;56(6):609-639.
10 Christiansen C., Townsend E. An introduction to occupation. In: Christiansen C.H., Townsend E.A., editors. Introduction to Occupation: The Art and Science of Living. Upper Saddle River, NJ: Prentice Hall, 2000.
11 Pierce D. Untangling occupation and activity. American Journal of Occupational Therapy. 2001;55(2):138-146.
12 American Occupational Therapy Association. Standards for continuing competence. American Journal of Occupational Therapy. 2005;59(6):661-662.
13 Gray J.M. Putting occupation into practice: Occupation as ends, occupations as means. American Journal of Occupational Therapy. 1998;52(5):354-364.
14 National Board for Certification in Occupational Therapy. Certification Renewal Handbook. Gaithersburg, MD: Author; 2010.
15 American Occupational Therapy Association. Standards of Practice. Bethesda, MD: American Occupational Therapy Association; 2009.
16 Law M., Baptiste S., Carswell A., Polatajko H., Pollock N. Canadian Occupational Performance Measure, 4th ed. Toronto: Canadian Association of Occupational Therapists; 2005.
17 AOTA State Affairs Group. Occupational therapy assistant supervision requirements. Bethesda, MD: American Occupational Therapy Association; 2006.
18 Black T. COTAs and OTRs as partners and teams. OT Practice. 1996;1(3):42-47.
19 Gitlin L.N., Corcoran M., Chee Y.K. Occupational therapy and dementia care: The home environmental skill-building program for individuals and families. Bethesda, MD: American Occupational Therapy Association; 2005.
20 Rogers J. Habits: Do we practice what we preach? Occupational Therapy Journal of Research. 2000;20(Suppl 1):119S-122S.
21 Rowles G.D. Habituation and being in place. Occupational Therapy Journal of Research. 2000;20(Suppl 1):52S-67S.
22 American Occupational Therapy Association. Board and specialty certification. Retrieved July 12, 2010, from www.aota.org/Practitioners/ProfDev/Certification.aspx, 2010.
23 Allen C.K., Austin S.L., David S.K., Earhart C.A., McCraith D.B., Riska-Williams L. Allen Cognitive Level Screen-5 (ACLS-5) and Large Allen Cognitive Level Screen-5 (LACLS-5). Camarillo, CA: ACLS and LACLS Committee; 2007.
24 Arthritis Foundation. Offering life improvement series programs: Program instructors/leaders. Retrieved June 30, 2010, from www.arthritis.org/leaders-instructors.php, 2010.
25 Howe M.C., Schwartzberg S.L. A Functional Approach to Group Work in Occupational Therapy. Philadelphia: Lippincott Williams & Wilkins; 2001.
26 American Occupational Therapy Association. Occupational therapy’s role in senior centers. Bethesda, MD: American Occupational Therapy Association; 2006.
27 McPhee S.D., Johnson T. Program planning for an assisted living community. Occupational Therapy in Health Care. 2000;12(2-3):1-17.
28 Horowitz B.P., Vanner E. Relationships among active engagement in life activities and quality of life for assisted-living residents. Journal of Housing for the Elderly. 2010;24(2):130-150.
29 McKenna K., Broome K., Liddle J. What older people do: Time use and exploring the link between role participation and life satisfaction in people aged 65 years and over. Australian Occupational Therapy Journal. 2007;54(4):273-284.
30 Tanner B., Tilse C., de Jonge D. Restoring and sustaining home: The impact of home modifications on the meaning of home for older people. Journal of Housing for the Elderly. 2008;22(3):195-215.
31 Glantz C.H., Richman N. OTR-COTA collaboration in home health: Roles and supervisory issues. American Journal of Occupational Therapy. 1997;51(6):446-452.
32 Swetz K.M., Harrington S.E., Matsuyama R.K., Shanafelt T.D, Lyckholm L.T. Strategies for avoiding burnout in hospice and palliative medicine: Peer advice for physicians on achieving longevity and fulfillment. Journal of Palliative Medicine. 2009;12(9):773-777.
33 Cooper J. Occupational Therapy in Oncology and Palliative Care. Chichester, England; Hoboken, NJ: Wiley; 2006.
34 Krawcyk A. The certified occupational therapy assistant as an activity director. Occupational Therapy in Health Care. 1988;5(2-3):111-118.
35 Herzog A.R., Ofstedal M.B., Wheeler L.M. Social engagement and its relationship to health. Clinics in Geriatric Medicine. 2002;18(3):593-609.
36 Martinez I.L., Kim K., Tanner E., et al. Ethnic and class variations in promoting social activities among older adults. Activities, Adaptation & Aging. 2009;33(2):96-119.
37 Cipriani J. Altruistic activities of older adults living in long-term care facilities: A literature review. Physical & Occupational Therapy in Geriatrics. 2007;26(1):19-28.
38 Williams A.L., Haber D., Weaver G.D., Freeman J.L. Altruistic activity: Does it make a difference in the senior center? Activities, Adaptation & Aging. 1997;22(4):31-39.
39 Dreiling D. Energy conservation. Home Health Care Management and Practice. 2009;22(1):26-33.
40 Peterson E.W., Clemson L. Understanding the role of occupational therapy in fall prevention for community-dwelling older adults. OT Practice. 2008;13(3):CE1-CE8.
41 Administration on Aging. Aging into the 21st century. Retrieved June 20, 2010, from www.aoa.gov/AoARoot/Aging_Statistics/future_growth/aging21/health.aspx, 2009.