chapter 12 Addressing Sexual Activity of Elders
1. Discuss the ways that values can influence attitudes about elder sexuality.
2. Identify primary myths about elder sexuality.
3. Discuss how elder homosexuals have been ignored by society.
4. Describe normal, age-related, sexual, physiological changes.
5. Describe sexually transmitted diseases and the elder population.
6. Discuss the treatment team members’ roles in addressing elders’ sexual concerns.
7. Discuss the ways elders’ sexuality is commonly dealt with in nursing facilities.
8. List the components of the permission, limited information, specific suggestions, and intensive therapy model (PLISSIT), and discuss ways that the certified occupational therapy assistant (COTA) can apply this model.
9. Identify strategies for elder sexual education.
10. List intervention and safety sides for addressing sexual concerns of elders who experience strokes, heart disease, and arthritis.
11. Increase personal comfort to discuss elder sexual concerns.
sexuality, values, myths, homosexuality, sexually transmitted diseases, physiological changes, nursing facilities, permission, limited information, specific suggestions, intensive therapy model
Heather is a COTA employed at an acute care hospital. A large part of her caseload is elders who have sustained total hip replacements. Intervention approaches are routine, and transfers, home situation, and safety precautions are typically addressed with people who have total hip repairs. One day a circumstance happened that resulted in Heather changing her intervention approach. Heather was working with Sam, an elder who had sustained a right total hip replacement. After Heather went through the protocol for total hip replacements, she asked him if he had any questions. “Yes,” he responded, “my wife and I want to know when we can have intimate relations.” Heather felt a surge of emotions. She felt perplexed because she did not know how to respond. She recalled blushing with embarrassment, stammering through a sentence stating that she would get back with Sam and abruptly leaving the room. Afterward Heather reflected about the situation. She wondered why she felt so embarrassed and what she could have done differently. She questioned whether she harbored feelings that elders should not be sexually active. After further reflection, Heather took the initiative to learn more about sexuality and elders and to incorporate this knowledge into intervention.
COTAs that provide thorough intervention first get to know elders as human beings and develop an understanding of the person’s daily life routines. Part of the daily life routines of many elders may involve sexual functioning. Sexual activity is categorized as an activities of daily living (ADL) function, according to the second edition of the Occupational Therapy Practice Framework: Domain and Process1 and is defined as “engaging in activities that result in sexual satisfaction.”1 Sexual expression can be an important part of a person’s life at any age and is related to a person’s self-concept, self-esteem, and body image (Figure 12-1).2 However, despite sexuality being so integral to human sexual expression, it may be ignored in clinical intervention for many reasons, including discomfort with one’s own sexuality or with an elder or disabled person remaining sexually active. Other reasons may include a lack of understanding of normal sexual changes with aging and a lack of knowledge about sexual function with regard to age and disability. Dealing with the elder’s concerns about sexual function should be part of intervention. This chapter helps the COTA learn about this important but often ignored area of ADL intervention. Furthermore, the chapter helps clarify myths and misconceptions.

Values about Sexuality
Each generation has certain values reflective of society, although such values are not necessarily uniformly held by all members of that generation. All individuals also have their own value systems.1 The Traditionalists (born between 1922 and 1945) are from a generation that was generally not well educated on sexuality and often did not discuss sexuality freely.3,4 For some members of this generation, sex was considered only a necessity for procreation and not a source of enjoyment. These are deeply held values that can influence the elder’s comfort level when discussing sexual feelings during clinical intervention. In addition, COTAs may feel uncomfortable discussing sexual concerns with elders because sexuality may not have been an open topic for some members of their generation either. But generational values change, and it is predicted that the Baby Boomer generation, especially the women from that generation, may embrace more openness about sexuality.5 Exercises 12-1 and 12-2 should be completed before further reading to explore values regarding elders and sexuality.
Exercise 12-1: Generational Sexual Attitudes/Values Inventory
Answer the following questions while considering your generation, the Baby Boomer generation (born between 1946 and 1964), and the Traditionalist generation (born between 1922 and 1945). Fill in “yes” or “no” for each question, then discuss or contemplate your findings. (For more information on generational cohorts, please refer to Chapter 1.)
| 1. It is appropriate to openly discuss sexual needs and concerns. | Your generation | Current elder generation |
| Yes (Acceptable) ___ | Yes (Acceptable) ___ | |
| No (Unacceptable) ___ | No (Unacceptable) ___ | |
| 2. Sexual activity is acceptable in a non-marriage situation. | Your generation | Current elder generation |
| Yes (Acceptable) ___ | Yes (Acceptable) ___ | |
| No (Unacceptable) ___ | No (Unacceptable) ___ | |
| 3. Sexual activity is appropriate if the purpose is physical pleasure. | Your generation | Current elder generation |
| Yes (Acceptable) ___ | Yes (Acceptable) ___ | |
| No (Unacceptable) ___ | No (Unacceptable) ___ | |
| 4. Sexual activity is for procreation only. | Your generation | Current elder generation |
| Yes (Acceptable) ___ | Yes (Acceptable) ___ | |
| No (Unacceptable) ___ | No (Unacceptable) ___ | |
| 5. The naked body is very private. Nudity is unacceptable. | Your generation | Current elder generation |
| Yes (Acceptable) ___ | Yes (Acceptable) ___ | |
| No (Unacceptable) ___ | No (Unacceptable) ___ | |
| 6. Women should discuss their sexual needs with their partners. | Your generation | Current elder generation |
| Yes (Acceptable) ___ | Yes (Acceptable) ___ | |
| No (Unacceptable) ___ | No (Unacceptable) ___ | |
| 7. It is appropriate for women to initiate sex. | Your generation | Current elder generation |
| Yes (Acceptable) ___ | Yes (Acceptable) ___ | |
| No (Unacceptable) ___ | No (Unacceptable) ___ | |
| 8. Masturbation is a normal sexual act. | Your generation | Current elder generation |
| Yes (Acceptable) ___ | Yes (Acceptable) ___ | |
| No (Unacceptable) ___ | No (Unacceptable) ___ | |
| 9. Sexual activity between people of the same sex is acceptable. | Your generation | Current elder generation |
| Yes (Acceptable) ___ | Yes (Acceptable) ___ | |
| No (Unacceptable) ___ | No (Unacceptable) ___ | |
| 10. Sexual activity between adults of different generations is unacceptable. | Your generation | Current elder generation |
| Yes (Acceptable) ___ | Yes (Acceptable) ___ | |
| No (Unacceptable) ___ | No (Unacceptable) ___ |
These questions are adapted from a module by Goldstein, H., & Runyon, C. (1993). An occupational therapy module to increase sensitivity about geriatric sexuality. Physical and Occupational Therapy in Geriatrics, 11(2), 57-75.
Exercise 12-2: Personal Values Assessment
This exercise helps identify personal values and attitudes. Answer the following questions. On completion of this exercise, any uncomfortable feelings may be handled by using this chapter as an educational tool to help dispel myths and misconceptions and to clarify normal physiological changes resulting from aging. After reading the chapter, the COTA can retake this personal value assessment to determine whether uncomfortable feelings have decreased.
| Agree | Disagree | |
| 1. Elders in nursing facilities should not be sexually active. | Agree | Disagree |
| 2. My grandparents (or parents) should not be sexually active. | Agree | Disagree |
| 3. It is acceptable for elder men to remain sexually active. | Agree | Disagree |
| 4. It is acceptable for elder women to remain sexually active. | Agree | Disagree |
| 5. It is immoral for elders to engage in recreational sex. | Agree | Disagree |
| 6. Sexual education is not necessary for elders. | Agree | Disagree |
| 7. Sexual education is not necessary for nursing facility staff. | Agree | Disagree |
| 8. Nursing facilities should provide large enough beds for couples to sleep together. | Agree | Disagree |
| 9. Nursing facilities should provide privacy for residents who desire sexual activity. | Agree | Disagree |
These questions are adapted from a scale developed by White, C. B. (1982). The aging sexuality knowledge and attitudes scale (ASKAS): A scale for the assessment of attitudes and knowledge regarding sexuality in the aged. Archives of Sexual Behavior, 11(6), 491-502.
Myths about Elders and Sexual Functioning
The media have provided people with misinformation and myths about elder sexual functioning. Television, magazines, and Internet advertisements encourage people to ignore or to cover up the aging process. Greeting cards make fun of aging and suggest that lying about age is acceptable. Some media sources encourage myths about sexuality such as “the dirty old man syndrome.” In addition, myths can be perpetuated by family members, peers, or elders themselves. With this inundation of misinformation, many people believe myths instead of truths about the sexual functioning of elders. Exercise 12-3 helps determine personal myths about elders and sexuality.
Exercise 12-3: Myths about Geriatric Sexuality
For each question below, answer T if the statement reflects a myth or F if the statement does not reflect a myth.
| Question | True | False |
| 1. Elders are no longer interested in sexuality. | True | False |
| 2. Elders no longer engage in sexual activity. | True | False |
| 3. Elders engage in a wide variety of sexual activity, including intercourse, cuddling, caressing, mutual stimulation, and oral sex. | True | False |
| 4. Elders in nursing facilities should be segregated according to sex; sexual functioning should be prohibited. | True | False |
| 5. Elder women are unattractive. | True | False |
| 6. More elder men remain sexually active than elder women. | True | False |
| 7. Elders are too frail to engage in sexual activity. | True | False |
| 8. Inability to maintain an erection (erectile dysfunction) is not a natural consequence of aging. | True | False |
| 9. All elders are heterosexual. | True | False |
Data from Comfort, A., & Dial, L. (1991). Sexuality and aging: An overview. Clinics in Geriatric Medicine, 7(1), 1-7; Goodwin, A. J., & Scott, L. (1987). Sexuality in the second half of life. In P. B. Doress & D. L. Siegal (Eds.). The Midlife and Older Women Book Project: Ourselves Growing Older. New York: Touchstone; Hammond, D. (1989). Love, sex, and marriage in later years. In E. S. Deichman & R. Kociechki R. (Eds.). Working with the Elderly: An Introduction. Buffalo, NY: Prometheus; Morrison-Beedy, D., & Robbins, L. (1989). Sexual assessment and the aging female. Nurse Practitioner, 14(36); and Pfeiffer, E., Verwoerdt, A., & Wang, H. S. (1968). Sexual behavior in aged men and women. Archives in General Psychiatry, 19, 753-758.
Answers to Exercise 12-3 questions: 1. T; 2. T; 3. F; 4. T; 5. T; 6. F; 7. T; 8. F; 9. F.
Discussion of Myths
Findings from a recently updated survey study in 2005 by the American Association of Retired Persons (AARP) (n = 1682)6 provide perspective about some of these myths about geriatric sexuality. A key finding was that 56% of persons age 45 and older of both sexes considered sexual relationships as contributing to their quality of life.6 However, a greater percentage of elder men and younger male respondents than women valued sexual activity as contributing to their quality of life.6 Nevertheless, sexuality was perceived as an integral part of these elders’ lives, not something they avoided. Furthermore, many elder men and women found their partner to be attractive; men 70 years of age or older reported this 53% of the time, whereas women of the same age reported this 49% of the time.6 In addition, women older than 70 years were more likely to describe their partners as romantic as compared with their younger counterparts (41% older than 70 years compared with 34% 45-49 years and 38% 50-59 years).6 Thus, these findings contradict the societal myths that equate age with unattractiveness and lack of romance. Health decline and lack of partners were major contributing factors to decreased sexual activity.6
The AARP study6 together with other literature7,8 suggest that for women sexual activity often stops because of lack of a partner. Kinsella and colleagues9 found in 2006 that only 40% of women age 65 and older were married compared to 72% of men in the same age group. When examining elders age 75 and older the gap between women and men grows even larger, with 28% of women and 68% of men reporting being married.9 In addition, some elder women believe the myth that they are unattractive and therefore should remain abstinent from sexual relationships. Previous research by AARP10 found that the current elder generation’s values are strongly against women being sexually active without a husband, but more current research conducted by AARP6 shows this trend is changing among the elder population. The results of the 2005 AARP study found a 7% decrease from the 1999 study in the viewpoint of opposition for sexual relations outside of marriage in individuals age 45 years and older.6,10
Both older men and older women may experience pressure from their children to remain abstinent. Some adult children may find it difficult to think of their parents as having normal sexual desires, especially if the parent is in a nursing facility.4,11
Most men experience occasional impotence or erectile dysfunction by the time they are elder12,13 because of fatigue, stress, illness, or alcohol.14 However, erectile dysfunction is not considered to be a normal part of aging.8 In the AARP study, 15% of men age 45 years and older admitted to being diagnosed with erectile dysfunction.6 Men can continue to have normal sexual activity throughout their lives. Minor physiological changes may have some effect on sexual functioning. For example, a benefit from physiological aging can be delayed ejaculation, which can increase sexual pleasure for the partner.15,16
For elder men who have erectile dysfunction, medications can help, such as Viagra (Pfizer U.S. Pharmaceuticals Group, New York), which increases the vascular flow to the genitals. However, caution must be taken in prescribing Viagra or any other medication because erectile dysfunction is complex, involving physical and psychological factors. In addition, Viagra, like any medication, has side effects and interactions with other medications.12,13 The elder should discuss with a physician the benefits as well as the risks involved in taking Viagra or other medication for erectile dysfunction. Media coverage using promotions by celebrities about taking Viagra has had a positive impact on opening discussions about erectile dysfunction.15
Most elders, especially the young old (that is, those 65 to 75 years of age), have active lives in which sexuality can remain an important component. Most likely, if a couple has always been sexually active, they will continue to be so as they grow older. As with any age group, communication is important for a positive sexual relationship. Frailty and disability do not automatically necessitate cause for an elder to be abstinent, although as findings from the AARP study suggest, having a disability or health problem does contribute to decreased sexual activity.6
Elder Homosexuals
Society has often ignored homosexuality in elders. Overall, society has embraced a “heteronormativity” viewpoint, or “a general perspective which sees heterosexual experiences as the only, or central view of the world.”17 Obviously, the elder cohort is diverse in terms of income, race, health status, and sexual orientation. Within this cohort the elder homosexual population also has a diverse background.18 The invisibility of the homosexual population is reflected in the paucity of research about homosexual elders.19,20 In occupational therapy literature, only a few articles have considered the homosexual experience,21-24 and even fewer have considered elder homosexuals.17 Progress in occupational therapy research and literature in these areas has been minimal, considering the growing number of elders identifying themselves as homosexual.
Many elder homosexuals may be uncomfortable sharing about their sexuality, having grown up in a time when overt prejudice was expressed toward homosexuals.12,19 Homosexuality was defined as a mental illness by the American Psychiatric Association until 1973.12 Discrimination continues to exist with examples of lesbian couples who want to live together in long-term care facilities being denied rooms.19 Social Security does not recognize a lifelong companion for benefits, and many medical and other legal decisions are made by family members rather than a person’s partner.18
COTAs can help dispel myths by simple actions such as the use of more inclusive language. As Harrison17 suggests, asking who are the significant others in a person’s life rather than who is a person’s spouse can help create a more open conversation. Times are changing and there are now organizations that advocate for elder homosexuals, such as the National Association of Lesbian and Gay Gerontology, Lesbian and Aging Issues Network, and a Lesbian and Gay Aging Network with the American Society on Aging.17,18
Normal Age-Related Physiological Changes in Men and Women
With normal aging, physiological changes might affect sexual functioning. Knowledge of these changes may help the COTA counsel the elder (Box 12-1). Not all of these changes happen to every elder, and the degree varies among individuals.31 Lindau and colleagues7 surveyed 3,005 adults ranging from ages 57 to 85 years and found that 39% of women reported issues with vaginal lubrication and 34% of women were unable to reach an orgasm; erectile dysfunction (37%) ranked the highest among men.7 In addition, COTAs should be aware of the concept “use it or lose it.” Elders who remain sexually active may not experience some of these physiological changes or not to the same degree as elders who do not remain sexually active. Furthermore, these physiological changes are just one aspect of sexuality. Sexuality, including sexual functioning, is complex and involves psychological, spiritual, social, and cultural dimensions of a human being.2,32 The ways a person reacts to and perceives these physiological changes ultimately affect sexual functioning. COTAs can apply this knowledge to educate elders. For example, a commercially available lubricant can supplement decreased vaginal secretion and can help reduce abrasion from thinning of the vaginal lining. Lubrication may also prevent dyspareunia, or painful intercourse.26 Kegel exercises (pelvic floor exercises) help preserve vaginal tone in women, can aid in the intervention of erectile dysfunction in men, and can reduce symptoms of incontinence in both genders.33-35 COTAS can instruct the elder to do these exercises several times daily, such as three times daily for 10 increments with tightening the muscles for 3 to 4 seconds. Instruct the elder to think about holding back urine to do the exercise correctly.36
BOX 12-1
Age-Related Physiological Changes and Sexual Responses
Women
1. Decrease in rate and amount of vaginal lubrication may possibly lead to painful intercourse.8,15,25
2. Orgasmic phase decrease may occur in elder women, resulting in a decrease in orgasm intensity.15,16
3. Structural changes or atrophy may occur in the labia or uterus, in addition to a reduction in the expansion of the vagina width and length.8,16,25,26
4. Thinning of the lining of the vagina can result in irritation and painful intercourse.8
5. Sexual stimulation from the nipples, clitoris, and vulva may decrease with age due to a decrease in sensation.15
Men
1. Erection is slower, less full, and disappears quickly after orgasm. Erection has a longer refractory period. A man in his eighties may need to wait several days as compared with a man in his twenties, in whom refractory period is a few minutes.27,28
2. Elder men may experience a decrease in penile rigidity.27,28
3. A decreased volume of sperm occurs; although fertility level is decreased, men do not become sterile.16,29
4. Decreased penile sensitivity results in increased need for direct penile stimulation over other forms of stimulation such as visual, psychological, or manual.28,30
5. Ejaculatory control enhanced, and ejaculation may occur every third episode of sexual activity as a result of less concern about orgasm.16
6. Ejaculation and orgasm is less strong.8,16
7. Decrease in ejaculatory testosterone occurs, although most elder men have the minimal level for sexual functioning.8
8. Reduced size of testicles and increased size of prostate gland.28,30
Adapted from Goldstein, H., & Runyon, C. (1993). An occupational therapy module to increase sensitivity about geriatric sexuality. Physical and Occupational Therapy in Geriatrics, 11(2), 57-75.
Sexually Transmitted Diseases among the Elder Population
An often overlooked aspect of sexual activity in the elder population is the prevalence and prevention of sexually transmitted diseases (STDs). The AARP study6 shows increasing numbers of elders are sexually active without being married, which puts them at a risk for STDs. A Centers for Disease Control and Prevention (CDC) study37 estimated 15% of new diagnoses of HIV/AIDS in 2005 were among individuals age 50 or older.6 A lack of information among the elder population about sexual activity poses a risk for transmitting STDs. Without the risk of pregnancy, many older adults forgo using safe sex techniques such as condoms.38
Prevention and education with elders should be incorporated with intervention. Promoting the use of condoms and other safe sex techniques is important in discussions of sexuality with elders. COTAs working in long-term care facilities can educate elders on the importance of safe sex techniques as well as the proper use of condoms. COTAs can also collaborate with other health care professionals to facilitate education on safe sex among the elder population.
Role of Intervention in Sexual Education
COTAs, registered occupational therapists (OTRs), and elders should collaborate to address concerns about sexuality. In addition, COTAs should be aware of other team members’ areas of expertise. Sexual dysfunction such as erectile problems, ejaculatory disturbances, anorgasmia (lack of orgasm), and pain during intercourse may be caused by side effects of medication and other physiological reasons.39 The physician and pharmacist must be notified about these concerns. Sexual dysfunction has a psychological component.40 Therefore, the client should be referred for counseling with a social worker or psychologist who has expertise with elders who have disabilities and sexual dysfunction. In addition to the OTR/COTA team, some physical therapists and nurses may educate the client about sexual positioning. Speech therapists may assist elders who have difficulties with communication.41,42
Addressing Elder Sexuality in a Nursing Facility
Trends in public policy and in professional literature suggest a more accepting attitude of sexual activity in nursing facilities (Figure 12-2). Federal laws regulate privacy for institutionalized patients, namely the Omnibus Budget Reconciliation Act43 passed in 1987.44 Professional literature since the 1990s has generally encouraged a more accepting attitude of sexuality in nursing home settings.11 However, despite these positive trends, challenges still exist in nursing home facilities. These challenges include availability of privacy,11 dealing with sexual behavior of residents who have cognitive impairments,44-46 and addressing sexual concerns of residents with chronic conditions.47 In addition, negative attitudes and viewpoints against sexual activity of elders are expressed by some staff,4,44,45 spouses, and residents.11 Staff may express their disapproval in many ways. One subtle way is by joking about sexual activity, which may serve as a means to make elders conform to the expectation of asexuality in some nursing facilities.
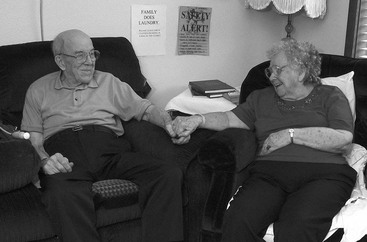
FIGURE 12-2 Sharing a room in a long-term care facility, these elders are able to enjoy the companionship of their lifelong spouse.
In some institutional settings, envisioning elders being interested in sex is difficult, and the elders themselves may be intolerant of peer engagement in sexual behavior.11,15 Generational beliefs or societal expectations may influence these attitudes.47 Mulligan and Palguta48 found that male elders in nursing home facilities displayed continued interest in sex and were sexually active if a partner was available.
Sexuality does not only include sexual intercourse. It also involves kissing, touching, hugging, masturbation, and expressing oneself as a sexual being.49,50 COTAs participating in program planning can suggest dances and other social events that encourage romance and human touch. They can encourage elders to be well dressed and well groomed. In addition, COTAs should always be aware of respecting client privacy. Shutting a curtain between beds or going to another room for intervention with personal ADL functions helps preserve privacy rights.
Elders should reside in a supportive environment that encourages sexual expression and involvement in sexual activity.47 Residents should have a say in nursing home standards, especially setting standards for sexual behavior within the community11,51 because most nursing home residents and staff support sexual rights.47
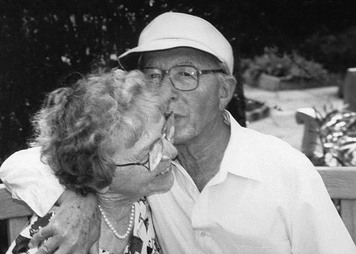
Finally, education can help dispel myths and misconceptions about sexuality and elders.52 COTAs who have positive attitudes and are educated about sexuality and elders can help dispel the ageist attitudes sometimes held by nursing home staff, family members, or the elders themselves (Figure 12-3).
Educating and Counseling the Elder Client
The Permission, Limited Information, Specific Suggestions, and Intensive Therapy Model
Intervention models may help provide sexual education to elders. The permission, limited information, specific suggestions, and intensive therapy (PLISSIT) model developed by Annon53,54 is a useful format for presenting sexual education information (Box 12-2).
BOX 12-2
The PLISSIT Model
 This stage involves listening in a nonjudgmental, knowledgeable, and relaxed manner as the client discusses sexual concerns. General questions can be asked in an intake or screening evaluation (for example, “Do you have any concerns about the effects of your disease on sexual function?”).
This stage involves listening in a nonjudgmental, knowledgeable, and relaxed manner as the client discusses sexual concerns. General questions can be asked in an intake or screening evaluation (for example, “Do you have any concerns about the effects of your disease on sexual function?”).
At this level, elders can be educated about normal physiological changes with aging, myths and stereotypes about the elder population, and sexuality and psychosocial factors that may inhibit or stress the elder.
At this level, COTAs may make appropriate suggestions for improved sexual functioning. Elders also may need to be referred to specialists such as social workers, psychologists, and physical or occupational therapists.
This level of counseling involves the expertise of a skilled social worker, psychologist, or psychiatrist.
Data from Annon, J. S. (1974). The behavioral treatment of sexual problems: Brief therapy [brochure]. Honolulu, HI: Kapiolani Health Services; Annon, J. S. (1976). The Behavioral Treatment of Sexual Problems: Brief Therapy. New York: Harper & Row; and Lohman, H., & Runyon, C. (1995). Counseling the Geriatric Client about Sexuality Issues in Counseling and Therapy: Lesson 5. New York: Hatherleigh.
COTAs can use the first, second, and third stages of this model during intervention. The elder must be assured of confidentiality throughout the educational process. In the first stage of the PLISSIT model, permission, the COTA applies therapeutic listening skills. The verbal and nonverbal body language of the COTA must show comfort with the topic. COTAs can ask questions using clear and direct language in a nonthreatening manner to encourage communication about sexual functioning during the ADL assessment.4 In addition, the COTA can convey that sexuality is a normal part of every human’s needs throughout a lifetime.55 Elders who are interested in discussing sexuality may have general questions about normal sexual changes with aging or common myths. The spouse or partner should be encouraged to join the discussion.
In the second stage of the model, the COTA can apply limited information by relating knowledge of sexuality gleaned from this chapter and other relevant sources. The COTA can provide specific suggestions in the third stage. Many suggestions to help elders who have disabling conditions and their partners maintain sexual function are discussed in the chapter. The COTA should refer the elder who needs psychological support at any point of the education process to the appropriate counselor. The fourth stage of the model, intensive therapy, involves the skills of a trained counselor and is especially important for those elders experiencing sexual dysfunction.
Role of the Certified Occupational Therapy Assistant in Sexual Education
To provide elders with adequate sex education, COTAs must have a general knowledge about medical conditions, awareness of psychological issues, and an understanding of the importance of good communication. Understanding the effects of a disease or disabling condition on sexual performance is necessary. COTAs must remember that the manifestations of a disease or condition differs with each person, and often sexual functioning has to do with how a person adapts to life changes.14 The following are some general education suggestions:
1. Encourage elders to maintain good communication with their partners in all aspects of their lives, not just about sexuality.16
2. Encourage elders to experiment with different sexual positions for comfort.16
3. Provide instruction on energy conservation techniques. Suggest resting before sexual activity.56
4. Encourage elders with decreased energy to explore other forms of sexual expression such as caressing, masturbation, and oral sex.16
5. Reassure elders that once they are medically stable and their physician has assessed them, they can reassume sexual activity.33
6. Talk with elders about any fears that they may have about resuming sexual functioning.38
The specific sexual concerns of elders who have experienced cerebrovascular accidents (CVAs), heart disease, and arthritis are discussed in the following sections.
Safety Considerations with Sexual Activity
Medications, drugs, alcohol, and smoking can be a cause of sexual dysfunction. COTAs should encourage elders to consult with their physicians or pharmacists to discuss sexual dysfunction related to these areas.
Elders who sustained strokes may have motor, sensory, and psychological dysfunctions. Sensory and motor dysfunctions should be considered with suggestions for positioning with sexual activity.
With a cardiac condition, encourage elders to consult with physicians before returning to sexual activity. COTAs should educate elders on the precautions for sexual activity after a cardiac condition: chest pain, shortness of breath, excessive fatigue, and continuous increase in blood pressure after sex or heart palpitations lasting longer than 15 minutes after sex.33,57,58 If elders experience these symptoms, they should seek immediate medical assistance.
Arthritis can cause pain, fatigue, and joint inflammation during sexual activity. Elders should be instructed on sexual positions that reduce the risk of these debilitating factors.
Safety concerns with sexual activity and other activities are necessary for elders to follow after total hip replacements. Review with elders that with any sexual or life activity they should not flex the affected hip more than 90 degrees59,60 and that the affected hip should not be adducted or externally rotated.59,61
COTAs need to recognize when to refer elders with sexual concerns that would benefit from additional services to appropriate professionals (Box 12-3).
BOX 12-3 Intervention Gems and Elder Sexual Activity
Sexuality activity is an ADL listed in the Occupational Therapy Practice Framework II.1 It is a normal part of aging and should be incorporated into intervention if elders desire. Generational values as well as individual values influence attitudes and beliefs about sexuality.
The current generation of elders, the Traditionalists, grew up in a time when sexuality was not openly discussed. With some members of the Baby Boomer generation, sexuality may be more openly discussed in intervention sessions.
Discussing sexuality and sexual activity is a sensitive subject and may cause some health care professionals to become uncomfortable. COTAs must be comfortable discussing sexuality with intervention, including sexual positioning, sexual orientation, and psychological aspects of sexuality.
Develop a rapport with elders before discussing sexual activity, and address sexuality based on the PLISSIT Model.
Elders may not have an adequate amount of knowledge about sexual activity after sustaining a condition, and therefore education is an important aspect of intervention. Education about positioning, energy conservation, sexually transmitted diseases, and safe sex techniques can be incorporated into an elder’s intervention.
COTAs can also collaborate with the treatment team as well as educate staff of the importance of incorporating sexuality within the elder’s intervention plan.
The effects of a stroke can have motor, sensory, and psychological manifestations that may affect an elder’s ability to participate in sexual activity. Common compensatory techniques for sexual intercourse include lying on the affected side so the unaffected arm is free, using pillows under the affected side, the use of touch for individuals with aphasia, and a non-distracting environment for individuals with cognitive impairments.
Elders with cardiac condition may have fear of sustaining a recurrent heart attack during sexual activity. Elders with cardiac conditions should consult a physician before beginning sexual activity. If cleared to resume sexual activity, COTAs can instruct elders on the use of relaxation techniques and energy conservation during sexual activity.
Pain, fatigue, joint inflammation, and anxiety can all hinder sexual activity with elders who have arthritis. COTAs can instruct elders with arthritis to use energy conservation techniques and rest to decrease pain during sexual activity. Heat pads or warm baths can be effective preparatory methods to decrease pain during sexual activity.
Elders with hip replacements should be instructed to abide by hip precautions during sexual activity.
Elders with knee replacements often prefer a side-lying position for comfort. Pillows can also be used with elders with knee replacements to maintain comfort and for safety.
Effects of Health Conditions on Elder Sexuality
Cerebrovascular Accident
COTAs commonly work with elders who have sustained CVAs or strokes. Dealing with sexual concerns after a stroke is often ignored.41,62,63 Addressing sexuality should be one of many aspects of a thorough evaluation. Just as the outcomes after a stroke are complex and different for each person, so are the impacts of a stroke on sexuality. It is not unusual for someone after a stroke to experience a decreased desire for sexual activity and decreased satisfaction with sexual activity.12,64,65 A study of 109 men who had a stroke found a decrease in erectile function, sexual desire, and ejaculatory function after stroke, but a lack of sexual desire was the main cause of limitations in sexual intercourse.66 Changes after a CVA have been linked to a person’s attitude about sexual activity and to fears about having erectile dysfunction, experiencing rejection, or having another stroke.41,65-67 Changes in one’s body image and one’s coping skills can be psychological manifestations.41,67,68 Being aphasic, having functional changes, displaying difficulties in arousal, and taking certain medications that have side effects on sexual performance also can influence sexual activity.69 Many of these changes may indicate a need for intervention about sexuality, and COTAs can play a strong role because of their background in working with people who have had CVAs. However, in considering any intervention, COTAs should keep in mind the concept that sexual dysfunctions after a CVA will likely result from multiple causes67; therefore, use of clinical reasoning skills70 and a team-based approach41 will be important.
COTAs should observe for motor abnormalities and other symptoms that can affect sexual function, including hemiplegia; perceptual, cognitive, and visual spatial disturbances; speech problems; emotional manifestations; and sensory deficits. For example, if elders are depressed, they may have no interest in sex. Anxiety may cause sexual performance problems such as male impotence and decreased female lubrication leading to painful intercourse. If elders have unilateral neglect, they may ignore one side of the body during sexual performance. Expressive aphasia may result in difficulty stating sexual needs. Sensory deficits such as esthesia or hyperesthesia on the affected side may affect sexual pleasure.41,71 Motor disturbances such as muscle weakness or hypertonia can make sexual performance awkward.41,71 (See Chapter 19 for a detailed discussion about CVA.)
After identifying the symptoms that affect sexual performance, the OTR and the COTA should collaborate with the elder to develop specific intervention suggestions. For example, clients with hemiplegia are sometimes advised to lie on the affected side so that the unaffected arm is free to caress the partner,41,72 or to just find a comfortable position.16 Simple adaptations such as using pillows under the affected side, use of a vibrator, raising the headboard, and adding a bed trapeze can help with motor manifestations of the CVA.41,71 Touch and other forms of nonverbal communication are useful with elders who have expressive aphasia.16 The partners of elders with visual field deficits should be encouraged to approach from the impaired side and use touch on both sides. Minimizing environmental distractions during sexual activity may help elders with cognitive deficits involving concentration.73
Beyond the physical effects of a CVA, some elders may experience low self-esteem and depression. These symptoms can affect sexual desire and performance.41,67,74 Elders who are in some way dependent on a partner may feel ambivalent about resuming a sexual relationship because of role changes.41,75 In addition, elders may worry about sustaining another CVA.67,76 Results of a study of 103 individuals who had a stroke for the first time found 65% of the individuals had a fear of experiencing another stroke while engaging in sexual activity.76 Elders with these psychological manifestations may require counseling.
Heart Disease
Heart disease is one of the most common chronic ailments affecting the elder population.77 Elders can have acute cardiac conditions, such as myocardial infarctions (MI), or chronic cardiac conditions, such as hypertension. With either type of cardiac condition the possible impact on sexuality should not be ignored. Elders should consult their physician for recommendations about sexual activity and cardiac conditions.30 DeBusk and colleagues78 developed a classification system to use as a guideline for physician’s recommendations to manage sexual activity in patients with cardiac disease. With this classification system, patients are divided into low, medium, or high cardiac risk. Patients with low risk, such as having controlled hypertension or mild stable angina, are recommended to safely resume sex. Patients with moderate risk, such as sustaining a recent MI or displaying moderate angina, require further cardiac evaluation. Patients in the high-risk category, such as having unstable angina or hypertension, are recommended to be stabilized before reassuming sexual activity.
Once stabilized, some elders with cardiac conditions may be instructed to resume sexual activity in a gradual manner.58 For elders who gradually reassume sexual activity, alternative forms of sexuality other than intercourse can be suggested. However, before reassuming sexual activity, elders should be instructed by the medical team about precautions and when to notify their physician.
Examples of precautions for sexual activity are chest pain, shortness of breath, excessive fatigue, and continuous increase in blood pressure after sex or heart palpitations lasting longer than 15 minutes after sex.33,58,62 The medical team also should be aware of negative side effects of common cardiac medications, herbal supplements, or illicit drugs that can influence libido or result in sexual dysfunction.33,58,79
Sustaining a cardiac condition can impact a person psychologically, resulting in fears about resuming sexuality. The resumption of sexual activity after a heart attack is believed by some people to cause future cardiac incidents and even death.58,80 Findings from a study (n = 1774) published in the Journal of the American Medical Association helps clarify anecdotal information.81 Sexual activity was found to contribute to MIs in a small number of the subjects (0.9%), and regular exercise was related to a decreased risk.81 Elders need to be educated that the physical demands of sexual activity are equal to mild to moderate exercise (“heart rate rarely increases to greater than 130 beats per minute and systolic blood pressure is rarely greater than 170 mm Hg”78).
Relaxation is important because fears and anxieties are common after cardiac incidents, especially about resuming sexual relationships.82 In addition, it is not uncommon to be depressed.83 Sexual dysfunctions can develop because of these anxieties.16,79 Sexual dysfunctions such as erectile problems also can result from physical reasons such as arteriosclerosis (hardening of the arteries).27,63 Furthermore, one must consider the sexual activity of the person before the cardiac incident.14 Using positions that require less energy expenditure and encouraging relaxation with sexual activity are helpful suggestions.83 COTAs can teach elders stress reduction techniques. Energy conservation techniques also may be helpful for those who are gradually building up their endurance. It is also beneficial to wait 1 to 3 hours after meals to allow the heart to pump blood to assist with the digestive process.58,83 Per the PLISSIT model,53,54 COTAs may need to refer the elder to an expert to address any sexual dysfunction. (See Chapter 23 for a more detailed discussion about cardiac concerns and the elderly.)
Arthritis
Arthritis is another common chronic condition among elders. All types of arthritis, including osteoarthritis and rheumatoid arthritis, can influence sexual function with physical and psychological effects. Physical concerns can be pain, functional limitations, fatigue, medication side effects, and genital lesions with some types of arthritis. Psychological problems include but are not limited to depression, anxiety, and loss of self-esteem.84-86 In addition, less opportunity to meet potential partners because of isolation and physical separation from one’s partner because of repeated hospitalizations is another psychological concern.84,85
Elders with joint inflammation and pain may be particularly prone to sexual performance problems. A common intervention goal for people with rheumatoid arthritis is to maintain or increase functional abilities in all areas of life,86,87 including sexual function. COTAs can make specific suggestions to help elders reduce joint pain and discomfort and preserve energy. Exercises to increase and maintain muscle strength affect the motor aspect of sexual performance. Elders should be encouraged to use a heating pad or tub bath before sexual activity to help decrease joint pain and inflammation. Elders and their partners also may experiment with various sexual positions that decrease joint pressure. Rest and energy conservation techniques may help make sexual performance less fatiguing. Finding the best time of day for sexual activity when the elder is less fatigued helps sexual performance.60,86
Joint Replacements
Elders with a history of arthritis commonly sustain joint replacements. Elders after total hip replacements are counseled to follow certain precautions in all areas of their lives, including sexuality. For an elder who has had a total hip replacement (posterolateral approach), it is important to review that with any sexual activity, or life activity, the elder should not flex the affected hip more than 90 degrees59,60 and that the affected hip should not be adducted or externally rotated.59,61 After the customary healing period of approximately 6 weeks and with physician approval, these elders can resume sexual activity as long as they follow precautions.
For intercourse, it is preferable with either sex that the elder with the total hip replacement be positioned supine (on back) with hips abducted (apart), knees in extension (straight), and legs in neutral (toes pointed up), and not in external rotation (toes pointed out).60 Intercourse in a side-lying position for the involved elder woman is accomplished by lying on her unaffected side with a minimum of two pillows between her legs to keep them abducted. The involved man using a side-lying position should also lie on his unaffected side and should “use his partner’s legs to support his affected leg.” Thus, the man’s affected leg is on top of his partner’s leg during sexual intercourse. The elder man’s partner should have a minimum of two pillows between her legs for support and to help her partner follow precautions.60 Other suggestions are pillows between the knees to help maintain the hip joints in abduction,88 and pillows under the knees while in a supine position can prevent extreme external rotation.61
After a total knee replacement, elders should be instructed to find the most comfortable position for intercourse. When the involved person is in a supine position, pillows can be placed under the knee, and the person can bend the knee within a comfortable range.60 A side-lying position is often most comfortable after surgery, and pillow support under the knee is beneficial.60. Exercise 12-4 is a role play exercise to overview many of the concepts discussed in in the chapter. Its purpose is to help increase comfort level in addressing sexual concerns of clients in practice.
Exercise 12-4: Role Play
Addressing sexual concerns in intervention will become more comfortable with practice for COTAs. The purpose of this role-play exercise is to increase comfort levels when discussing sexual issues. It also serves as a review of chapter material. To begin the exercise, choose four people to be part of a radio talk show panel made up of knowledgeable professionals who are experts on the sexuality of elders. Then choose people who will read the scenarios listed in the following. Members of the radio talk show panel are allowed to consult notes and have a commercial break if they want to discuss a situation before responding.
Another method is to role play doing a live show on the Internet site Skype found at http://www.skype.com. Role play a synchronous session in which elders (played by students) from several community facilities call in their questions about sexuality, either using a webcam or a microphone.
I am 78 years of age and have rheumatoid arthritis. Over the years, I have developed increasingly painful joints, particularly in my hips. I am currently a widow but will soon marry a wonderful man. I would like to enjoy my new sexual relationship. Do you have any suggestions?
I am a 65-year-old man who had a heart attack 8 weeks ago. My doctor says that it is safe to begin sex again. Still, I have tremendous fears. Are these fears normal, and what can I do about them?
I am a nurse’s aide who works in a nursing facility. I have recently noticed male and female patients taking an interest in each other. They are constantly holding hands and have been observed kissing. The other aides make fun of them and have told them to stop, but they continue openly expressing their affection. I feel that they have a right to express their romantic side. Who is right?
I am an 82-year-old man. My wife and I continue to have a satisfying sexual relationship. However, I have noticed in recent years that my first erection is slower and it takes me even longer to achieve an erection the second time. I am afraid to ask my physician about this. Am I normal?
I am a 64-year-old man who had a heart attack 2 years ago. I have been impotent since getting out of the hospital. What should I do?
I have a two-part question. I am 65 years old and have recently had a minor stroke. I am uncomfortable asking my physician about this. I have noticed over the years that sexual activity with my lover has become painful because of less vaginal lubrication. Is this normal, and is there anything I can do about it? Concerning the stroke, my left side is impaired and weakened. Do you have any suggestions for sexual positioning?
I am an 87-year-old lesbian. I can now more openly state that fact because times are changing. However, in most of my lifetime I have had to hide my sexuality. Because of having arthritis and high blood pressure, I have found it more difficult to get around and am now looking into relocating to an assisted living facility with my partner. With interviews at the facilities we have been open about our sexual relationship. Although none of the directors has directly stated that they do not want us to move into their facility, it has been obvious from their body language that we are less than welcome. We realize that we will likely experience some prejudice from other residents wherever we move. Do you have any suggestions on how to approach finding a place? Also, as long as you are consulting, do you have suggestions about my arthritis and maintaining sexual relations with my partner?
1. Discuss common myths related to elder sexuality.
2. Discuss the viewpoint held by society about elder homosexuals.
3. Discuss issues related to STDs and the elder population.
4. Identify some of the normal age-related physiological changes for women and some simple intervention suggestions for them.
5. Identify some of the normal age-related physiological changes for men.
6. List the members of the treatment team and discuss ways the team can work together to address elders’ sexual concerns.
7. Discuss the ways that attitudes of health care workers in nursing home facilities affect elder sexuality.
8. Describe ways COTAs help facilitate elder sexual expression in a nursing home setting.
9. List and describe the parts of the PLISSIT model.
10. Describe ways COTAs may apply the PLISSIT model in intervention.
1 American Occupational Therapy Association. Occupational therapy practice framework: Domain and process, second ed. American Journal of Occupational Therapy. 2008;62:625-683.
2 Pangman V.C., Sequire M. Sexuality and the chronically ill older adult: A social justice issue. Sexuality and Disability. 2000;18(1):49-50.
3 Goodwin A.J., Scott L. Sexuality in the second half of life. In: Doress P.B., Siegal D.L., editors. The Midlife and Older Women Book Project: Ourselves Growing Older. New York: Touchstone; 1987:79-99.
4 Langer N. Late life love and intimacy. Educational Gerontology. 2009;35(8):752-764.
5 Jacoby S. Retrieved from http://www.aarpmagazine.org/lifestyle/relationships/sex_in_america.html/page=1, 2005, July/August. Sex in America. AARP the Magazine 1-2
6 American Association of Retired Persons (AARP). Sexuality at midlife and beyond: 2004 update of attitudes and behaviors [WWW page]. URL http://assets.aarp.org/rgcenter/general/2004_sexuality.pdf, 2005.
7 Lindau S., Schumm P., Laumann E., Levinson W., O’Muircheartaigh C., Waite L. A study of sexuality and health among older adults in the United States. New England Journal of Medicine. 2007, August;357(8):762-774.
8 Meston C.M. Successful aging: Aging and sexuality. Western Journal of Medicine. 1997;167(4):285-290.
9 Kinsella K., Wan H., U.S. Census Bureau. An aging world: 2008 (Report No. P95/09-1). Washington, DC: U.S. Government Printing Office; 2009.
10 American Association of Retired Persons (AARP). AARP modern maturity sexuality survey—summary of findings [WWW page]. URL http://www.research.aarp.org/health/mmsexsurvey_l.html, 1999.
11 Gibson M.C., Bol N., Woodbury M.G., Beaton C., Janke C. Comparison of caregivers’, residents’ and community-dwelling spouses’ opinions about expressing sexuality in an institutional setting. Journal of Gerontological Nursing. 1999;25(4):30-39.
12 Allen W. Sexuality. In Ferrini A.F., Ferrini R.L., editors: Health in the Later Years, 4th ed, New York: McGraw-Hill, 2008.
13 Starr B.D. Sexuality, forth ed. Schulz R., editor. The Encyclopedia of Aging: A Comprehensive Source in Gerontology and Geriatrics. New York: Springer, 2002;Vol. 2.
14 Lerner S. Sexuality and myths: A study of aging factors. Focus on Geriatric Care and Rehabilitation. 2000;13(10):3-12.
15 Agronin M.E. Sexual disorders. In: Blazer D.G., Steffens D.C., Busse E.W., editors. The American Psychiatric Publishing Textbook of Geriatric Psychiatry. third ed. Washington, DC: American Psychiatric; 2004:303-317.
16 Laflin M. Sexuality and the elderly individuals. In Lewis C.B., editor: Aging: The Health-Care Challenge, fourth ed, Philadelphia: FA Davis, 2002.
17 Harrison J. “It’s none of my business”: Gay and lesbian invisibility in aged care. Australian Occupational Therapy Journal. 2001;48:142-145.
18 Kimmel D.C. Homosexuality, fourth ed. Schulz R., editor. The Encyclopedia of Aging: A Comprehensive Resource in Gerontology and Geriatrics. New York: Springer, 2006;vol. 1.
19 Wojciechowski C. Issues in caring for older lesbians. Journal of Gerontological Nursing. 1998;24:28-33.
20 Wright S., Canetto S. Stereotypes of older lesbians and gay men. Educational Gerontology. 2009;35(5):424-452.
21 Birkholtz M., Blair S. “Coming out” and its impact on women’s occupational behavior—a discussion paper. Journal of Occupational Science. 1999;62:68-74.
22 Jackson J. Sexual orientation: Its relevance to occupational science and the practice of occupational therapy. American Journal of Occupational Therapy. 1995;54:26-35.
23 Jackson J. Understanding the experience of non-inclusive occupational therapy clinics: Lesbians’ perspectives. American Journal of Occupational Therapy. 2000;54:26-35.
24 Walsh A., Crepeau E. “My secret life”: The emergence of one gay man’s authentic identity. American Journal of Occupational Therapy. 1998;52:563-569.
25 Zeiss A.M., Kasl-Godley J. Sexuality in older adults’ relationships. Generations. 2001;25:18-25.
26 Johnson L.E., Alline K.M. Sexual health. In: Ham R.J., Sloane P.D., Warshaw G.A., Bernard M.A., Flaherty E., editors. Primary Care Geriatrics: A Case-Based Approach. fifth ed. Philadelphia: Mosby Elsevier; 2007:401-407.
27 Tenover J.L. Sexuality, sexual function, androgen therapy, and the aging male. In: Hazzard W.R., Halter J.B., editors. Hazzard’s geriatric medicine and gerontology. sixth ed. New York: McGraw-Hill Medical Pub. Division; 2009:1634. Retrieved from http://www.accessmedicine.com.cuhsl.creighton.edu/content.aspx?aID=5118079
28 Schiavi R.C., Rehman J. Sexuality and aging. Urologic Clinics of North America. 1995;22(4):711-726.
29 LeVay S., Valente S.M. Human Sexuality, second ed. Sunderland, MA: Sinauer Associates; 2006.
30 Miracle A., Miracle T.S. Sexuality in late adulthood. In Bonder B.R., Bello-Haas V.D., editors: Functional Performance in Older Adults, third ed, Philadelphia: FA Davis, 2009.
31 Glass C., Dalton A. Sexuality in older adults: A continuing education concern. Journal of Continuing Education in Nursing. 1988;19:61-64.
32 DeLamater J., Karraker A. Sexual functioning in older adults. Current Psychiatry Reports. 2009, February;11(1):6-11. doi:10.1007/s11920-009-0002-4
33 Mueller L.W. Common questions about sex and sexuality in elders. American Journal of Nursing. 1997;97(7):61-64.
34 Sivalingam S., Hashim H., Schwaibold H. An overview of the diagnosis and treatment of erectile dysfunction. Drugs. 2006;66(18):2339-2355.
35 Weiss B.D. Selecting medications for the treatment of urinary incontinence. American Family Physician. 2005;71(2):315-322.
36 Mayo Clinic. Kegel exercises: How to strengthen pelvic floor muscles. Retrieved February 5, 2010, from n.d. http://www.mayoclinic.com/health/Kegel-exercises/WO00119
37 Centers for Disease Control and Prevention (CDC). HIV/AIDS among persons aged 50 and older [WWW page]. URL http://www.cdc.gov/hiv/topics/over50/resources/factsheets/over50.htm, 2008.
38 Atkinson P.J. Intimacy and sexuality. In: Meiner S.E., Lueckenotte A.G., editors. Gerontologic Nursing. third ed. St. Louis, MO: Mosby Elsevier; 2006:268-280.
39 Camacho M.E., Reyes-Ortiz C.A. Sexual dysfunction in the elderly: Age or disease? International Journal of Impotence Research. 2005;17:S52-S56.
40 Laumann E.O., Nicolosi A., Glasser D.B., Paik A., Gingell C., Moreira E., Wang T. Sexual problems among women and men aged 40-80 y: Prevalence and correlates identified in the global study of sexual attitudes and behaviors. International Journal of Impotence Research. 2005;17(1):39-57.
41 Farman J., Friedman J.D. Sexual function and intimacy. In Stroke Rehabilitation: A Function-Based Approach, 2nd ed, St. Louis, MO: Mosby; 2004:533-549.
42 Lohman H., Runyon C. Counseling the Geriatric Client about Sexuality Issues in Counseling and Therapy: Lesson 5. New York: Hatherleigh; 1995.
43 Omnibus Budget Reconciliation Act (OBRA). Health Care Financing Administration. Baltimore: Health Care Administration; 1987.
44 Reingold D., Burros N. Sexuality in the nursing home. Journal of Gerontological Social Work. 2004;43(2/3):175-186. doi:10.1300/J083v43n02_12
45 Doyle D., Bisson D., Janes N., Lynch H., Martin C. Human sexuality in long-term care. The Canadian Nurse. 1999;95(1):26-29.
46 Tzeng Y., Lin L., Shyr Y.L., Wen J. Sexual behaviour of institutionalised residents with dementia–a qualitative study. Journal of Clinical Nursing. 2009;18(7):991-1001.
47 Ghusn H. Sexuality in institutionalized patients. Physical medicine and rehabilitation: State of the art reviews, 9, 2. Philadelphia: Hanley & Belfus, 1995.
48 Mulligan T., Palguta R.F. Sexual interest, activity, and satisfaction among male nursing home residents. Archives of Sexual Behavior. 1991;20(2):199-204.
49 Ginsberg T.B., Pomerantz S.C., Kramer-Feeley V. Sexuality in older adults: Behaviours and preferences. Age and Ageing. 2005, September;34(5):475-480.
50 Lyder C.H. Examining sexuality in long-term care. Journal of Practical Nursing. 1991;41(4):25-27.
51 Roach S. Sexual behaviour of nursing home residents: Staff perceptions and responses. Journal of Advanced Nursing. 2004;48(4):371-379. doi:10.1111/j.1365-2648.2004.03206.x
52 Lohman H., Aitken M. Influence of education on knowledge and attitude toward older adult sexuality. Physical and Occupational Therapy in Geriatrics. 1995;13:51.
53 Annon J.S. The behavioral treatment of sexual problems: Brief therapy [brochure]. Honolulu, HI: Kapiolani Health Services; 1974.
54 Annon J.S. The Behavioral Treatment of Sexual Problems: Brief Therapy. New York: Harper & Row; 1976.
55 Kessel B. Sexuality in the older person. Age and Ageing. 2001;30:121-124.
56 Hordern A., Currow D. A patient-centered approach to sexuality in the face of life-limiting illness. Medical Journal of Australia. 2003;179(Suppl. 6):S8-S11.
57 Miller C.A. Nursing for Wellness in Older Adults, 5th ed. Philadelphia: Lippincott Williams & Wilkins; 2009.
58 Steinke E.E. Sexual counseling after myocardial infarction. American Journal of Nursing. 2000;100(12):38-44.
59 Pratt E., Gray P.A. Total hip arthroplasty. In Maxey L., Magnusson J., editors: Rehabilitation for the Postsurgical Orthopedic Patient, second ed, St. Louis, MO: Mosby, 2007.
60 Whittington C., Mansour S., Sloan S.L. Sex After Total Joint Replacement: A Guide for You and Your Partner. Atlanta, GA: Media Partners; 2001.
61 Coleman S. Hip fractures and lower extremity joint replacement. In Pedretti L.W., Early M.B., editors: Occupational Therapy: Practice Skills for Physical Dysfunction, fifth ed, St. Louis, MO: Mosby, 2002.
62 Miller L. Let’s talk about sex. OT Practice. 2008, February 4;13(2):7-8.
63 Miracle A., Miracle T.S. Sexuality in late adulthood. In Bonder B.R., Wagner M.B., editors: Functional Performance in Older Adults, 2nd ed, Philadelphia: FA Davis, 2001.
64 Edmans J. An investigation of stroke patients resuming sexual activity. British Journal of Occupational Therapy. 1998;61(1):36-38.
65 Korpelainen J.T., Nieminen P., Myllyla V.V. Sexual functioning among stroke patients and their spouses. Stroke. 1999;30:715-719.
66 Jung J.H., Kam S.C., Choi S.M., Jae S.U., Lee S.H., Hyun J.S. Sexual dysfunction in male stroke patients: Correlation between brain lesions and sexual function. Urology. 2008;71(1):99-103.
67 Monga T.N., Ostermann H.J. Sexuality and sexual adjustment in stroke patients. Physical Medicine and Rehabilitation State of the Art Reviews. 1995;9(2):345-359.
68 Wilz G. Predictors of subjective impairment after stroke: Influence of depression, gender, and severity of stroke. Brain Injury. 2007;21(1):39-45.
69 Cheung R.T. Sexual dysfunction after stroke: A need for more study. European Journal of Neurology. 2008;15(7):641.
70 Mattingly C., Fleming M.H. Clinical Reasoning: Forms of Inquiry in a Therapeutic Practice. Philadelphia: FA Davis; 1994.
71 Zukas R., Ross-Robinson L. Sexuality and the disabled woman. Occupational Therapy Practice. 1991;2(4):1-12.
72 Burgener S., Logan G. Sexuality concerns of the post-style patient. Rehabilitation Nursing. 1989;14(4):178-195.
73 Neistadt M.E., Freda M. Choices: A Guide to Sexual Counseling with Physically Disabled Adults. Malabar, FL: Robert E. Krieger; 1987.
74 Somers K.J., Philbrick K.L. Sexual dysfunction in the medically ill. Current Psychiatry Reports. 2007, June;9(3):247-254.
75 Mooradian A.D. Geriatric sexuality and chronic diseases. Clinics in Geriatric Medicine. 1991;7(1):113-131.
76 Tamam Y., Tamam L., Akil E., Yasan A., Tamam B. Post-stroke sexual functioning in first stroke patients. European Journal of Neurology: The Official Journal of the European Federation of Neurological Societies. 2008;15(7):660-666. Retrieved from MEDLINE database
77 U.S. Department of Health and Human Services (DHHS). A profile of older Americans: 2008. Washington, DC: Author; 2008.
78 DeBusk R., Drory Y., Goldstein I., Jackson G., Kaul S., Kimmel S., et al. Management of sexual dysfunction in patients with cardiovascular disease: recommendations of The Princeton Consensus Panel. The American Journal of Cardiology. 2000;86(2):175-181. Retrieved from MEDLINE database
79 Steinke E.E., Jaarsma T. Impact of cardiovascular disease on sexuality. In: Moser D.K., Riegel B., editors. Cardiac Nursing: A Companion to Braunwald’s Heart Disease. St. Louis, MO: WB Saunders, 2008.
80 Mandras S.A., Uber P.A., Mehra M.R. Sexual activity and chronic heart failure. Mayo Clinic Proceedings. 2007, October;82(10):1203-1210.
81 Muller J., Mittleman M., Maclure M., Sherwood J., Tofler G. Triggering myocardial infarction by sexual activity. Low absolute risk and prevention by regular physical exertion. Determinants of Myocardial Infarction Onset Study Investigators. JAMA: The Journal of the American Medical Association. 1996;275(18):1405-1409.
82 Westlake C., Dracup K., Walden J., Fonarow G. Sexuality of patients with advanced heart failure and their spouses or partners. The Journal of Heart and Lung Transplantation: The Official Publication of the International Society for Heart Transplantation. 1999;18(11):1133-1138. Retrieved from MEDLINE database
83 American Heart Association, 2009. Sexual activity and heart disease or stroke [WWW page]. URL http://www.americanheart.org/presenter.jhtml?identifier=4714
84 Clinical Rheumatology. 2007;26;6:872-878.
85 Lim P.A.C. Sexuality in patients with musculoskeletal diseases. Physical Medicine and Rehabilitation: State of the Art Review. 1995;9(2):401-415.
86 Helewa A. Management of persons with rheumatoid arthritis and other inflammatory conditions. In: Walker J.M., Helewa A., editors. Physical Rehabilitation in Arthritis. second ed. St. Louis, MO: WB Saunders; 2004:191-212.
87 Yasuda Y.L. Rheumatoid arthritis and osteoarthritis. In Trombly C.A., editor: Occupational Therapy for Physical Dysfunction, fifth ed, Baltimore: Lippincott Williams & Wilkins, 2002.
88 Lawson S. Hip fractures and lower extremity joint replacement. In: Pendleton H.McHugh, Schultz-Krohn W., editors. Pedretti’s Occupational Therapy: Practice Skills for Physical Dysfunction. sixth ed. Philadelphia: Mosby; 2006:1020-1035.