chapter 17 Strategies to Maintain Continence in Elders
1. Determine the prevalence and cost associated with incontinence.
2. Indicate common causes of incontinence.
3. Review the normal anatomy and physiology of urination and defecation.
4. Identify the different types of urinary and fecal incontinence.
5. Explain the effect of the Omnibus Budget Reconciliation Act in dealing with the problem of incontinence in nursing homes.
6. Specify the role of each team member, emphasizing the importance of an interdisciplinary approach.
7. Identify the certified occupational therapy assistant’s (COTA’s) role in the management of incontinence.
Sara is a COTA who has been treating Mrs. Smith since her arrival at the nursing home 2 months earlier following a stroke. Sara works with Mrs. Smith both morning and after lunch. To start each afternoon session, per Mrs. Smith’s usual routine, Sara assists Mrs. Smith with going to the restroom. However, the past few sessions that Sara has worked with Mrs. Smith, Sara has noticed that Mrs. Smith has been incontinent each time. When Sara questions Mrs. Smith about it, Mrs. Smith states, “I just can’t seem to get to the bathroom in time, and lately no one has been helping me go before lunch like they used to do.” Additionally, Sara observes that Mrs. Smith’s bathroom door is always closed and blocked shut by the bedside table, making access to the restroom difficult. Oftentimes, her call light is not within reach.
Sara is concerned about the noticeable increase in Mrs. Smith’s incontinence. She feels that, as a COTA, it is her responsibility to educate both Mrs. Smith and the nursing staff on some tips that may help Mrs. Smith decrease her incontinence episodes. As a result, Sara has begun working with the nursing staff to create a timed voiding schedule for Mrs. Smith. Sara has also made a checklist that reminds nursing staff of simple ways to reduce some of the environmental barriers contributing to Mrs. Smith’s incontinence. After implementing a few simple techniques and educating both Mrs. Smith and the nursing staff on some simple tips regarding incontinence, her episodes of incontinence have decreased.
Incontinence of urine and stool is a common problem many elders face. Bowel and bladder management, toilet hygiene bowel, as well as other areas of related occupations are discussed in the Occupational Therapy Practice Framework (2nd ed.)1 Incontinence is often considered part of the normal aging process and is therefore accepted but not treated. Society’s acceptance of this condition is manifested by the availability of absorbent products and high-fiber foods found in local stores. Some elders afflicted with this problem may feel ashamed and embarrassed, which may lead to psychological conditions such as depression and avoidance of social relations or activities. Other elders may think the problem will correct itself, or they may fear that it will lead to a surgical procedure. Prolonged hospitalizations are common when incontinence is left untreated. Incontinence may even be a primary reason that caregivers decide to place elders in long-term care facilities.
During the normal aging process, bladder capacity and the ability to delay urination and defecation decrease. These changes can increase the risk for incontinence, especially with medical conditions such as pneumonia and chronic heart failure. Often, fecal incontinence results from changes in sphincter musculature and hormonal imbalances.
Urinary and Fecal Incontinence
Prevalence
The prevalence of urinary incontinence in the nursing home setting has been reported to range from 22% to 90%, with the average near 56%.2 For non-institutionalized older adults, the range is 15% to 38%.3 In general, women are twice as likely as men to experience this problem.3 Additionally, urinary incontinence is thought to be widely underdiagnosed and underreported.4
Cost
In the United States, the estimated total annual cost of managing urinary incontinence is $16.3 billion per year. For the elderly in nursing homes managing urinary incontinence is estimated at 5.34 billion dollars per year.5 In other words, cost of incontinence is approximately $10,000 per patient each year.6 This cost can be itemized to include routine care such as labor, supplies, laundry, and diagnostic and medical evaluation; treatment such as surgery and pharmacy and drug costs; incontinent consequences such as skin erosion, urinary tract infection, and falls; and added admissions resulting from incontinence.2
Private insurance companies and government programs will usually pay for only urodynamic evaluation, surgical procedures, catheterization,7 and sacral nerve stimulation.8 Consequently, management of incontinence is routine care. Elders and their families may feel financially strained if incontinence is the only reason for institutionalization. Therefore, poor reimbursement encourages management of incontinence rather than determination of the underlying problem and provision of the most effective intervention.
Anatomy and Physiology
The anatomic structures of the male lower urinary tract primarily responsible for normal urination include the bladder neck, prostate gland, pelvic floor musculature, and urethra. In women, the structures include the bladder neck, proximal urethra (internal sphincter), and the pelvic floor muscles that provide the strength needed to maintain the pelvic floor tone and urethra resistance.
The bladder fills and empties. The normal bladder capacity averages about 500 ml. The urinary bladder can normally hold between 250 and 350 ml of urine before the individual feels the urge to void. As the urinary bladder reaches its holding capacity, the bladder becomes strong enough to activate the stretch receptors, which, in turn, send a message to the nervous system, the pelvic floor and sphincter sense the increased pressure, and the individual feels the urge to void.9 The urethra then relaxes, allowing the bladder to empty.
The anatomical structures involved with normal defecation include the pelvic floor muscles, anal sphincter mechanisms (internal and external), colon, rectum, and anal canal. A stool of an appropriate consistency is delivered to the rectum and anal sphincter through the gastrointestinal (GI) tract and colon. The normal sensory system acknowledges that the rectum is filling and alerts the structures of the type of rectal content (that is, solid, liquid, or gas). Once the stool passes the rectum, the internal sphincter relaxes, allowing the stool to pass.
Etiology
Causes of urinary and stool incontinence may be pathological, anatomical, or physiological. The most common potential causes of urinary incontinence are transient or reversible. These include delirium, infection such as symptomatic urinary tract infection or vaginitis, excessive urine production, and psychological factors such as depression.9 Hypercalcemia, hyperglycemia, diabetes insipidus, chronic heart failure, lower extremity venous insufficiency, and drug-induced ankle edema are other causes of transient incontinence.8
Pharmaceutical causes of transient incontinence are sedative hypnotics (that is, benzodiazepines); diuretics, leading to polyuria; calcium channel blockers; anticholinergic agents (that is, antihistamines, antidepressants, antipsychotics, antiparkinsonian agents, and alpha-adrenergic agents); sympathomimetics; and sympatholytics. Potential causes of fecal incontinence include abnormal delivery of feces to the rectum, which may be drug-induced, metabolic, or caused by infection; sphincter dysfunction from trauma, diabetes mellitus, or inflammation; reduced rectal compliance such as rectal ischemia or fecal impaction; and anatomical derangement such as from a tumor or from third-degree hemorrhoids or injury. Other causes of fecal incontinence include muscular and neuromuscular disorders such as congenital or hereditary myopathy, behavioral and developmental dysfunction such as mental retardation or psychiatric disorders, and neurological impairment such as with the central nervous system, spinal system, or peripheral nervous system.2
Types of Urinary Incontinence
Urge or Urgency Incontinence
Elders commonly have a combination of types of urinary incontinence. Urgency urinary incontinence (UUI) is defined as the involuntary leakage of urine accompanied by a sudden urgency to have to go to the bathroom.9 Elders may experience a massive and sudden loss of urine without warning and often strain to empty the bladder. This type of urge incontinence is common at night and is referred to as nocturnal incontinence. Urge incontinence may also occur when elders hear water trickling or when they drink small amounts of water. Uncontrolled contraction of the detrusor (bladder muscle), a condition that is also referred to as neurogenic detrusor overactivity, may be part of the problem.9
Stress Urinary Incontinence
Stress urinary incontinence (SUI) is considered more prevalent in women than in men. Elders with stress incontinence experience uncontrolled loss of urine when intra-abdominal pressure is placed on the bladder. This type of incontinence can occur while coughing, laughing, sneezing, exercising, bending, lifting a heavy object, or arising from a chair.9 A child sitting on an elder’s lap may place sufficient pressure on the elder’s bladder, which can lead to incontinence. Stress incontinence is usually caused by weakened pelvic floor musculature as a result of the childbirth process in women, or a weakened or damaged sphincter mechanism. In men, stress incontinence is often the result of a radical prostatectomy performed for the treatment of prostate cancer.4
Overflow Incontinence
An individual with overflow incontinence experiences frequent or constant dribbling of urine, voiding only small amounts at a time. The bladder is always full, and the elder is never able to completely empty it. The elder cannot sense its fullness. The cause is often an underactive detrusor muscle. In men this type of incontinence is common when there is a blockage in the bladder, such as an enlarged prostate.9
Mixed Incontinence
Mixed urinary incontinence (MUI) is a combination of urge and stress incontinence. In other words, there is involuntary leakage in conjunction with a sense of urgency and increased bladder pressure. Approximately 80% of urinary incontinence cases are in this category.9
Functional Incontinence and Other Types
Functional incontinence is related to impaired cognitive functioning and mobility. With functional incontinence, lower urinary tract function is intact, but decreased cognitive functioning prevents individuals from recognizing the need to use the restroom or decreased mobility impacts the ability to reach the restroom in time.4 This type of incontinence often warrants occupational therapy (OT) intervention to help with environmental and other adaptations. Other types of incontinence, which are not as common, include reflex incontinence, detrusor instability, and iatrogenic incontinence. Reflex incontinence is a storage and emptying problem resulting from a spinal cord lesion. Detrusor instability is common in individuals diagnosed with dementia. With this type of incontinence, the bladder contracts before it is full. Iatrogenic incontinence is caused by an outside medical intervention or treatment such as a new medication.4
Fecal Incontinence
Fecal incontinence is often a result of problems with the GI tract and colon. GI problems cause changes in the consistency and volume of stools, leading to problems such as diarrhea and constipation.4 Diarrhea is defined as “the frequent passage of loose, watery stools.”10 Associated symptoms are abdominal pain and cramping. Diarrhea can be a symptom of problems such as dietary intolerance, malabsorption syndromes, inflammatory bowel disease, fecal impaction, gastroenteritis, and GI tumors.
An individual with constipation will complain of abdominal pain and fullness in the rectum. Defecation usually occurs infrequently, and consistency of the stool is hard and dry. Constipation can result from intestinal obstruction, diverticulitis, tumors, dehydration, lack of exercise, and a poor diet.
Omnibus Budget Reconciliation Act and Related Research
The Agency for Healthcare Policy and Research, currently referred to as the Agency for Healthcare Research and Quality (AHRQ), was created as a result of the Omnibus Budget Reconciliation Act (OBRA) to conduct research on diseases and disorders. The following are the initial guidelines for information on urinary incontinence developed as a result of studies conducted by the AHRQ panel:
1. Improve education and dissemination of urinary incontinence diagnosis and treatment alternatives to the public and to health care professionals
2. Educate the consumer to report incontinence problems once they occur
3. Improve the detection and documentation of urinary incontinence through better history taking and health care record keeping
4. Establish appropriate basic evaluation and further evaluations
5. Reduce variance among health care professionals
6. Encourage further biomedical, clinical, and cost research on prevention, diagnosis, and treatment of urinary incontinence in the adult11
This special panel concluded that most elders were improperly diagnosed for urinary incontinence and ineffectively treated. Both urinary and fecal incontinence are areas that surveyors look at closely during their annual inspections because of the secondary complications such as skin erosion and falls associated with these problems. For COTAs working in nursing home practice with the Minimum Data Set (MDS) Version 3.0 bladder and bowel are addressed in Section H. (Figure 17-1). Section G of the MDS includes the functional status of toileting for which therapists may provide input. Refer to Chapter 6 for more information on the MDS According to OBRA guidelines, the goal with incontinence is to encourage the nursing home staff to use a rehabilitative model.12
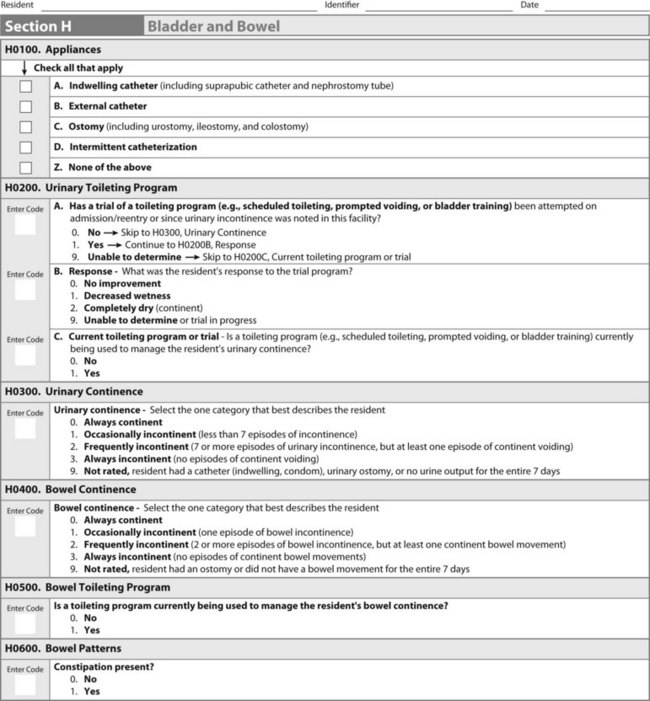
FIGURE 17-1 Minimum Data Set (MDS; 3.0) form section H. Form is used by nursing staffs to rate incontinence.
(From Nursing Home Quality Initiatives, Centers for Medicare & Medicaid Services. Baltimore, MD, 2010, US Department of Health & Human Services.)
More recently, in 2005, the Centers for Medicare and Medicaid Services (CMS) came out with new surveyor guidance regarding long-term care on urinary incontinence. The purposes of all of these guidelines are intended to help with the diagnosis, assessment, and management of urinary incontinence so that individuals can benefit from early screening and intervention.9
Interdisciplinary Team Strategies
Only half of elders residing in the community actually relate incontinence problems to their physicians to receive treatment.9 When the problem is reported, many health care professionals treat incontinence as a disease rather than determine the underlying cause, often attributing the incontinence to old age or normal body changes. However, incontinence should never be considered normal.9
Health care providers involved in the treatment of incontinence in elders include urologists, gynecologists, psychiatrists, nurses, psychologists, social workers, dietitians, pharmacists, and enterostomal therapists (ET nurses). Other health professionals include OT practitioners and physical and speech therapists. All members of this team work together to determine the most effective plan of care, and each provides a unique role in the interdisciplinary team.
Physicians begin care of elders with incontinence by taking a thorough medical history, performing a physical examination, and scheduling laboratory tests. They may refer the client to a specialist such as an urologist or gynecologist, if the problem is recurrent. However, a conservative approach is usually initiated. The primary preference is the use of behavioral techniques followed by pharmacological approaches. Because of potential complications, surgery is considered the last resort. Surgery for stress incontinence in women, which requires repositioning the bladder neck, has a success rate of 69% to 94%, depending on the type of procedure.2 The success rate of surgery in men with overflow incontinence, which requires removal of the cause of blockage, is similar.8,13 Surgery for fecal incontinence is indicated for traumatic, idiopathic, neurogenic, congenital, and medical problems. Surgery may consist of a sphincter repair, gracilis muscle transfer, and artificial anal sphincter placement.2
Medications are often prescribed to improve incontinence by treating infection, replacing hormones (estrogen), decreasing abnormal bladder contractions, and tightening sphincter muscles. This type of treatment is effective primarily with urge incontinence resulting from detrusor hyperactivity. Anticholinergics such as atropine, antispasmodics, tricyclic antidepressants, and calcium channel blockers are the drugs commonly prescribed. Antidiarrheal agents such as loperamide and fecal softeners and lubricants are common medications used to treat problems with defecation.2
The dietitian can determine hydration or nutrition patterns in the elder’s diet that may be contributing to both urinary and stool incontinence. Recommendations such as a high-fiber diet2 and liquid intake of 48 to 64 oz per day help maintain proper functioning of the bowel and bladder.3,14 Caffeine intake should be limited because it acts as a diuretic.
A nurse should complete a bowel (Figure 17-2, A) and bladder (Figure 17-2, B) profile indicating the length of time that incontinence has been present and the frequency and timing of episodes. The nurse usually initiates behavioral approaches.
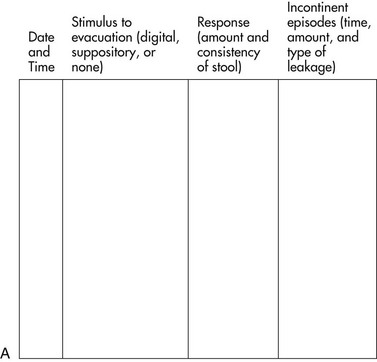
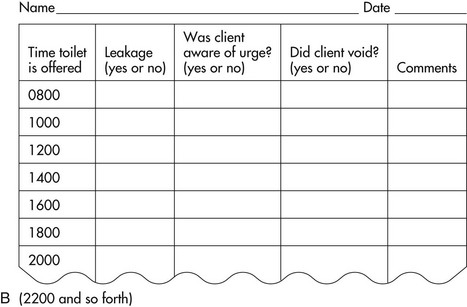
FIGURE 17-2 Sample recording charts. A, A diary of bowel function. B, A diary of bladder function.
(From Doughty, D. B. (2006). Urinary and Fecal Incontinence Nursing Management. St. Louis, MO: Mosby.)
Social service specialists and psychologists are important in determining the family dynamics and support available to elders. They may help determine the effect that incontinence has on the involvement of elders in social activities and relationships. They may also provide counseling to assist elders in expressing feelings about their incontinence problems.
Speech and language therapists are involved in evaluating elders’ abilities to communicate either verbally or nonverbally to make their needs known in a timely and effective manner. These professionals assist elders in compensating for impaired communication by providing instruction in the use of gestures and communication aids. Specific training is also provided to the caregiver to ensure proper carryover.
Physical therapists are involved in completing a comprehensive musculoskeletal and functional mobility assessment to ascertain range of motion, muscle strength, bed mobility, sitting balance, and gait. The treatment provided by physical therapists may also include teaching and instruction on the use of an assistive device such as a walker, cane, or brace to improve the elders’ abilities to ambulate to the bathroom. Caregiver training by physical therapists may include the proper use of a mechanical lift or sliding board with transfers or encouraging elders to carry over a program involving range of motion and strengthening exercises. Electrical stimulation to strengthen the muscles in stress incontinence, biofeedback, and Kegel exercises may all be part of the physical therapy intervention. These approaches also may be applied by the COTA with demonstrated competency and according to any state licensure guidelines.
COTAs work closely with the other disciplines to determine the cause of incontinence and to develop an effective intervention plan. Understanding how incontinence fits in with the Occupational Therapy Practice Framework (OTPF) can be helpful in recognizing the role of COTAs with incontinence. According to the OTPF: Domain and Process (2nd ed.) bowel and bladder management and toileting hygiene are areas of occupations, or more specifically activities of daily living (ADL).1 COTAs have a responsibility to their patients to address ADL that are pertinent to them.
The following intervention techniques can be provided by members of the treatment team, including COTAs, to help increase voiding, thus leading to increased independence in ADL.
Timed Voiding and Habit Training
Timed voiding and habit training consist of establishing a fixed schedule that requires the client to void every 2 hours. Toileting is adjusted according to the client’s normal pattern and is determined after approximately 2 weeks of monitoring. To make timed voiding easier, associate the schedule with certain parts of the elder’s daily routine, such as before/after a meal, or activity.9 Attempts are made to increase the intervals between voiding. This habit training often is used in the nursing home setting and is successful with neurologically impaired residents.
Prompted Voiding
Prompted voiding is commonly used in the nursing facility and is recommended for frail or cognitively impaired individuals. Caregivers are responsible for documenting whether the client is wet or dry on a regular basis, usually every 1 to 2 hours. Caregivers are encouraged to ask whether elders have a need to void.
Bladder Training
Bladder training is recommended as a first step with stress, urge, and mixed incontinence.2 While some studies have shown a 10% to 15% improvement rate in urinary continence using bladder training,8,13 a recent Cochrane review of the literature was able to conclude only that bladder retraining may be a beneficial intervention for urinary incontinence.2 The goal of bladder training is to decrease the frequency of voiding and lengthen the intervals between voiding. Caregivers instruct elders to resist the urge to urinate and to follow a planned time schedule rather than to respond immediately to the urge.
Biofeedback
Biofeedback offers elders visual and auditory information to teach voluntary control of certain functions. Most elders are taught to relax the detrusor and abdominal muscles while contracting the sphincter muscle. An improvement rate of 20% to 25% in urinary incontinence has been noted for individuals using this technique.8 A 70% to 90% success rate is reported with fecal incontinence.15
Pelvic Floor Exercise
Pelvic floor exercises are also known as Kegel, or childbirth, exercises. Kegel exercises are commonly used and have a 30% to 90% success rate in women with stress incontinence.8,13 Elders are taught to relax the abdominal muscles while contracting the pelvic floor muscles. After assistance is given to identify the correct muscles, elders are told to complete a minimum of 60 contractions of the pelvic floor muscles per day working up to 150 contractions per day, if possible.3 This technique is commonly used to improve fecal incontinence and increase muscle tone in the pelvic floor to prevent stool leakage.2 Physical and occupational therapists can initiate these exercises.
Environmental Adaptations
The ability to be continent resides heavily on being able to reach the restroom or commode. Often there are environmental barriers that contribute to incontinence. Many residents in long-term care facilities experience incontinence simply because of the inability to obtain help with toileting in a timely fashion. In most cases, changes in the physical environment must be initiated by caregivers.2 When considering problems with functional mobility, COTAs are encouraged to look at the elder’s environment to determine whether modifications are necessary to facilitate independence and to ensure safety while toileting (Box 17-1). COTAs should make recommendations for improvement where required (Table 17-1). (See Chapter 14 for more information on fall prevention.)
BOX 17-1 Considerations for Environmental Adaptations to Help with Incontinence
1. Does the client need or use side rails to assist with bed mobility?
2. Is the call light easily accessible to the client?
3. Is the height of the bed appropriate for safe transfers?
4. Is the client restrained in bed or in the wheelchair, which would limit mobility to the bathroom?
5. Is there adequate lighting to and from the bathroom? (A 60-year-old elder requires three times brighter lighting than a 20-year-old adult.)
6. Are there any obstacles or clutter that would interfere with safe mobility?
7. Is the client able to manage the door leading into the bathroom?
8. Are the floors highly waxed, which could cause a fall?
9. Is the doorway leading into the bathroom wide enough to allow proper clearance for a wheelchair or walker?
10. Is the height of the toilet appropriate?
11. Are there any grab bars or support to assist with a transfer to the toilet?
TABLE 17-1 Environmental and Safety Adaptations to Help with Incontinence
| When implemented appropriately, the following safety adaptations are ideas that may be used to make it easier for the elders to maneuver around in their environment. |
Data from Miller, C. (2009). Nursing for Wellness in Older Adults, 5th ed. Philadelphia: Lippincott Williams & Wilkins.
Many environmental modifications can be made in the bathroom. For example, grab bars can be mounted either in a 45-degree horizontal fashion to assist in pushing up or in a vertical position to facilitate pulling up. The length of the bars should be between 24 and 36 inches on the back wall and 42 inches on the side wall.16
Physical restraints can sometimes be used by caregivers in nursing facilities to prevent individuals from falling out of bed or the wheelchair. However, the use of a restraint may cause increased agitation for many reasons, including elders being unable to take care of bathroom needs if call lights are not answered in a timely manner. Because of the original OBRA law, the use of restraints is carefully monitored. Restraints are recommended only to encourage more functional independence, to decrease the risk for a life-threatening medical problem, or to promote a better anatomical seating position that is minimally restrictive.17 OBRA protects the rights of elders to freedom of movement and access to the body. COTAs must work closely with other staff members in deciding on a restraint program that allows the client to remain continent while minimizing the use of restraints (see Chapter 14).
Clothing Adaptations and Management
Clothing management before and after toileting is a functional independence measure. This measure is often used to evaluate toileting and bowel and bladder management at admission to and on discharge from inpatient rehabilitation facilities.18 COTAs can help elders improve clothing management by providing activities that use fine motor coordination, such as increasing dexterity with manipulation of zippers or buttons. Range of motion and strengthening exercises may facilitate pulling pants over the feet and hips. Another option is to suggest that elders wear clothing that can be easily manipulated, such as clothing with Velcro or elastic waistbands.3
Adaptations for Clients with Functional Incontinence
An increased incidence of incontinence is often seen in elders with dementia. In addition to an inability to manage their clothing, these elders also have difficulty locating the bathroom and toilet. Some may have problems with their strength, coordination, range of motion, and sense of balance, which affect their abilities to toilet in a timely and safe manner. They may be seen urinating and defecating in inappropriate places. This level of functioning is described by Allen and colleagues19 as Allen Cognitive Level 3 (see Chapter 7 for more information on this theory). Elders with dementia might perform part of the toileting task but become confused at some point and require verbal or physical assistance, or both, to continue. COTAs can encourage maximal functioning by determining what tasks the client can do and by training caregivers to assist with only those tasks that become difficult.
Impaired functional mobility of elders can be addressed by COTAs in conjunction with physical therapy. The goal is to improve functional mobility skills and train caregivers to provide the proper physical and verbal cues needed for elders to become successful with safe mobility.
Prevention of Skin Erosion
One of the secondary effects of incontinence mentioned earlier is skin erosion. Caregivers must be educated on a bowel and bladder program, a repositioning schedule, and proper wound care. Skin integrity may be improved by placing a special mattress on the bed or an incontinence cushion on the sitting surface.
Nutrition is extremely important in wound healing. COTAs must consider elders’ abilities to feed themselves. Elders may need to learn how to use adaptive equipment to aid this procedure. Elders must be able to obtain and drink fluids to maintain hydration.
Case Study
Ricardo was recently admitted to a skilled nursing facility (SNF) from his home, where his aging partner Paul was attempting to care for him. Ricardo’s urinary and bowel incontinence was becoming burdensome, and with little support and inconsistent in-home services, the daily routine had become too much for Paul. The situation was also causing a strain on their relationship.
On admission to the SNF, Ricardo was diagnosed with early-stage Alzheimer-type dementia, rheumatoid arthritis, and long-term low back pain. In addition, Ricardo had the beginning of a pressure sore forming on his coccyx. The nursing home physician reviewed Ricardo’s medical history and performed a physical examination. He determined that Ricardo’s incontinence was not caused from medications, but rather was related to the Alzheimer’s disease process and pain associated with movement. OT and physical therapy were ordered to evaluate and provide appropriate intervention for Ricardo.
The findings from the OT evaluation were as follows:
2. Limited mobility and ambulation secondary to pain
3. Limited upper extremity range of motion
Josie, the COTA at the SNF, was assigned to provide OT treatment five times a week. She was to assess bed and wheelchair positioning, adaptive equipment needs, fine motor skills, and toileting tasks and transfers. It was determined through the interdisciplinary team process that nursing would assist with pain management, including appropriate medications. Nursing would also implement scheduled toileting and begin intervention to heal the pressure ulcer. The dietitian would provide suggestions for a proper diet, intake, and suggest nutritional supplements to promote healing of the pressure ulcer. Physical therapy would address bed mobility, sitting and standing balance, and safe ambulation.
By the end of the first week of intervention, Josie recommended a higher bed to ease Ricardo’s transfer process and to decrease the amount of pain associated with transfers. A bedside commode was placed in Ricardo’s room until his ability to ambulate to the bathroom in his room could be evaluated. Because of his dementia, Ricardo was unable to complete pericare; however, with verbal cueing he was able to assist with clothing management before and after toileting. Josie also recommended a pull-up incontinent undergarment to be used because Ricardo was able to assist with clothing management. She also provided positioning equipment for the bed and wheelchair to assist in the healing of and prevention of further pressure ulcers. This included a bed wedge to help Ricardo maintain side-lying during scheduled turning when in bed and a gel cushion with a coccyx cut-out for his wheelchair to decrease heat and shear.
Paul began to make regular visits, and the social worker helped them adjust to the changes in their lives.
Case Study Questions
1. Why would a pull-up incontinence product be the most appropriate recommendation for Ricardo?
2. What is the advantage of using a gel cushion?
3. List three possible reasons why a pressure ulcer was developing before Ricardo’s admission to the SNF.
4. Identify two reasons why an elder in Ricardo’s situation benefits from scheduled turning.
5. Why would Ricardo’s incontinence cause strain on his relationship with his partner Paul?
6. Why is timely pain medication helpful?
7. Identify one reason why improved nutrition is important in Ricardo’s situation.
1. List the members of any incontinence team.
2. Describe how OBRA has affected the management of incontinence in the nursing facility.
3. Discuss whether urinary and fecal incontinence are part of the normal aging process.
4. What type of incontinence is more prevalent in women?
5. Describe the effect of incontinence on nursing home placement.
6. Which behavioral technique is commonly used for incontinence training with an elder who has dementia?
7. What are some of the secondary complications associated with incontinence?
8. What is the role of the COTA in the management of incontinence?
9. What are some environmental modifications that can improve continence?
10. Discuss the various ways that incontinence can be addressed by using Table 17-1, areas of occupation in the OTPF.1 Consider beyond the categories of bowel and bladder management and toilet hygiene to other categories that could be related to incontinence.
1 American Occupational Therapy Association. Occupational therapy practice framework: Domain and process, 2nd ed. American Journal of Occupational Therapy. 2008;62:625-683.
2 Doughty D. Urinary and Fecal Incontinence, 3rd ed. St. Louis, MO: Mosby; 2006.
3 Miller C. Nursing for Wellness in Older Adults, 5th ed. Philadelphia: Lippincott Williams & Wilkins; 2009.
4 Smeltzer S., Bare B., Hinkle J., Cheever K. Brunner and Suddarth’s Textbook of Medical-Surgical Nursing, 12th ed. Philadelphia: Lippincott Williams & Wilkins; 2009.
5 Palmer M. Urinary incontinence quality improvement in nursing homes: Where have we been? Where are we going? Urologic Nursing. 2008;28(6):439-444. 453
6 Fink H., Taylor B., Tacklind J., Rutkus I., Wilt T. Treatment interventions in nursing home residents with urinary incontinence: A systematic review of randomized trials. Mayo Clinic Proceedings. 2008;83(12):1332-1343.
7 Hu T.W. Impact of urinary incontinence on health-care costs. Journal of the American Geriatric Society. 1990;38(3):292-295.
8 U.S. Department of Health and Human Services. Urinary incontinence in adults. Rockville, MD: U.S. Department of Health and Human Services; 1999.
9 Newman D., Wein A. Managing and Treating Urinary Incontinence. Baltimore, MD: Health Profession Press; 2009.
10 Mosby’s Dictionary of Medicine, Nursing, and Health Professions, 7th ed. St. Louis, MO: Mosby, 2006.
11 Hood F.J. Coverage of urinary incontinence. Southern Medical Journal. 2002;95(2):198-201.
12 NovaCare, Inc. OBRA guidelines for occupational therapy and physical therapy clinicians. (Pamphlet). King of Prussia, PA; 1993.
13 Centers for Medicare and Medicaid Services. Deficiency decision-making and severity scope determination (draft). Baltimore, MD: Centers; 2001.
14 Beers M., Berkow A., editors. The Merck Manual of Diagnosis and Therapy, 17th centennial ed, Whitehouse Station, NJ: Merck & Co, 1997.
15 Blaivas J.G., Romanzi L.J., Heritz D.M. Urinary incontinence: Pathophysiology, evaluation, treatment, overview, and nonsurgical management. In: Walsh P.C., Retik A.B., Vaughan E.D.Jr., Wein A.J., editors. Campbell’s Urology. Philadelphia: WB Saunders; 1998:1007-1036.
16 Schmitz T. Environmental assessment. In O’Sullivan S.B., editor: Physical Rehabilitation: Assessment and Treatment, 4th ed, Philadelphia: FA Davis, 2001.
17 Health Care Financing Administration. Omnibus Budget Reconciliation Act. Baltimore: Administration; 1995.
18 Uniform Data System for Medical Rehabilitation. Guide for the uniform data set for medical rehabilitation (Adult FIM). Buffalo, NY: Uniform Data System for Medical Rehabilitation; 2001.
19 Allen C., Earhart C., Blue T. Occupational Therapy Treatment Goals for the Physically and Cognitively Disabled. Rockville, MD: American Occupational Therapy Association; 1992.