chapter 7 Occupational Therapy Practice Models
1. Explain the importance and use of practice models in occupational therapy intervention with elders.
2. Briefly summarize the Occupational Therapy Practice Framework (2nd edition) and three occupational therapy practice models as they relate to aging, including Facilitating Growth and Development, Cognitive Disabilities, and the Model of Human Occupation.
3. Demonstrate the ways certified occupational therapy assistants can incorporate theoretical principles into practice with elders.
clinical practice models, values, dysfunction, skills, occupation, function, assessment, task, roles, performance, culture, environment, self-care, work, play and leisure, intervention, context, cognition, maturation, motor action, subsystem, habits
Deepak was admitted to the rehabilitation center with a severe infection in the left knee that had been replaced just 3 months earlier. Deepak had been looking forward to his recent retirement. As an executive for a large firm, he and his family had lived in 10 different countries around the world. Now that all of his children had graduated from college, he was planning a peaceful life in a small town by the ocean where he and his wife could play golf every day, attend cultural events in a nearby city, and occasionally go deep-sea fishing. A few days after he was admitted to the rehabilitation center he received news that his wife had fallen and fractured a hip. While preparing her for surgery at a different hospital, the doctors had discovered that she had a very aggressive cancer that had metastasized throughout her body. There was no hope for recovery, and she was discharged home under the care of her daughter and a hospice service. Deepak spoke to his wife on the telephone twice a day, and often was tearful during his conversations with her. The purpose of Deepak’s hospitalization was that he become independent in his self-care and in his mobility while not bearing any weight on his left leg. The weight-bearing restrictions were expected to be necessary for at least 10 weeks while his infection cleared and his knee was replaced again.
Martha is a small, frail woman in her late sixties who has been living in a skilled nursing facility for more than a year. When she was in her late twenties her automobile had been hit by a train and she sustained a head injury that resulted in her inability to speak and left hemiplegia. She had regained the ability to do her self-care and to walk without assistance, although over the years she had suffered many falls because of poor balance. For more than 40 years she had lived with her sister. When her sister died, Martha attempted to live on her own for some time but became ill with pneumonia. Her relatives insisted she live at a skilled nursing facility because they were not able to care for her. Because of another bout with pneumonia, Martha is very weak and is unable to bathe and dress herself without assistance. She is also not able to walk.
Ursula was recently referred to an adult day care center in the downtown area of a large city. Her Alzheimer’s disease has progressed to the point where she needs supervision 24 hours a day. Ursula’s husband has been working at a local bookstore to make some money to supplement his retirement income. Ursula and her husband were prisoners in a Nazi concentration camp in their youth, and in the last month Ursula has seemed to be reliving that experience, often becoming quite agitated and isolated at the center.
Carlos immigrated to the United States from Cuba nearly 30 years ago. Although he is in his late sixties, he continued to work running a family-owned restaurant until 5 days ago when he had a stroke. Because of his stroke, Carlos seems unable to understand and speak in English and continually repeats the same two lines of a Spanish song whenever he does speak. He also is unable to hold himself in midline and does not seem aware of one side of his body. Nearly every day his room in the acute care hospital has been full of relatives and friends, many of whom bring food. Carlos has a fever, and the doctors suspect he is having difficulty swallowing.
Deepak, Martha, Carlos, and Ursula represent the diversity of people who seek occupational therapy (OT) intervention because they are not able to carry out the activities that are important to them in their daily lives. The certified occupational therapy assistant (COTA) needs tools to address all of these unique needs according to basic OT philosophy and theoretical principles. The OT programs for these individuals must not consider only the physical and cognitive limitations that affect their ability to care for themselves. These programs must also take into account the whole history of these individuals and the adjustments that are needed because of dramatic changes in their environments. Deepak’s wife is dying, and his children no longer live at home. Martha has been moved against her will from her familiar home to a skilled nursing facility where she knows no one. Carlos has gone from spending nearly all of his waking hours at his business to a hospital room, and Ursula’s mind has gradually replaced her physical surroundings for dreadful ones that reside in her memory. Although these OT programs must maintain a common thread that identifies them as “occupational therapy,” they also should be flexible enough to provide individual meaning for each client. OT clinical practice models are intended to connect professional philosophy and theory with daily practice.
Overview of Practice Models
This chapter provides an overview of several conceptual models in which occupation is described as the principal feature of any OT intervention. First, the Occupational Therapy Practice Framework1 is reviewed, which articulates the general domain and process of intervention of the OT profession and gives the broadest look at how we might go about understanding Deepak’s life and current needs. Second, an overview of Llorens’s2 Facilitating Growth and Development model is provided, which, although published nearly 3 decades ago, is still the only conceptual model that emphasizes a developmental perspective in the practice of OT with adult clients. This model can help us understand how to consider Martha’s stage in life. Third, the Cognitive Disabilities Model3,4,5 is described, which helps us understand how cognitive process affects the performance of occupation and will be particularly useful in working with elders such as Ursula, although it certainly also has applications for Deepak, Martha, and Carlos. Finally, the Model of Human Occupation6 is discussed as a model that makes an effort to assist practitioners to consider clients holistically. This model will help us understand elders like Carlos as people with dynamic abilities and needs who actively interact with their environments.
The common link among all forms of OT intervention cannot be overemphasized. The philosophy of OT practice includes values, beliefs, truths, and principles that should guide the general practice of the profession. One tenet of this philosophy is that the human being is inherently active and can influence self-development, health, and environment with purposeful activity. Thus, the human is able to adapt to life’s demands and become self-actualized. Dysfunction occurs when the human being’s ability to adapt is impaired in some way. OT intervention seeks to prevent and remediate dysfunction and facilitate maximal adaptation through the use of purposeful activities.7 The use of meaningful and purposeful activity, or occupation, is the common thread for every OT intervention.
Since the OT profession began, the term occupation has described the individual’s active participation in self-care, work, and leisure,8 which constitute the ordinary, familiar things people do every day.7 The person must use combinations of sensorimotor, cognitive, psychological, and psychosocial skills to perform these occupations.9 Specific environments and different stages of life influence these occupations. Kielhofner10 defined occupation as “doing culturally meaningful work, play or living tasks in the stream of time and in the contexts of one’s physical and social world.”
To understand the concepts of occupations and use them to facilitate function and adaptation, COTAs must have broad knowledge of the biological, social, and medical sciences in addition to OT theoretical premises. OT practice models provide organized frameworks for that knowledge, which allow the therapist to apply pertinent information to a specific client’s problem. Thus, practice models guide the therapist in creating individual intervention programs that are culturally meaningful and age-related and that facilitate development of sensorimotor, cognitive, psychological, and psychosocial skills. By using a practice model for guidance, the four COTAs assisting the patients discussed earlier can ensure professional intervention programs that are tailored to meet the needs of each client.
Theorists have articulated many practice models or approaches. Those presented here are certainly not the only ones that can provide guidance for OT intervention with elders. For example, the Kinesiological Model,11,12 also referred to as the Biomechanical Approach, provides insight into how elders move based on mechanical principles of range of motion, muscle strength, and physical endurance. Concepts of this approach help us restore movement to an elder after a stroke or apply hip precautions during participation in occupation after a hip replacement (refer to Chapters 19 and 22 for examples of applications of this approach). Another example is the Sensory Integration Model,13,14 which addresses dysfunctions that make it difficult for the brain to modulate sensory stimulation. Intervention guided by this model provides strategic sensory stimulation designed to organize the central nervous system and promote adaptive responses according to the person’s neurological needs (refer to Chapter 20 for an understanding of intervention guided by this model).
OT practice models do not offer concrete plans for improvement of function. Instead, these models suggest the use of various graded occupations that demand the development of performance abilities, thereby improving function. COTAs may use the information in the practice models to formulate questions to assess the client’s needs, interests, and meanings; select assessment tools; and accordingly design a unique intervention strategy. COTAs should be familiar with several practice models because each model usually has a specific focus and does not address all dimensions of occupational functioning.
Occupational Therapy Practice Framework
The Occupational Therapy Practice Framework: Domain and Processes (subsequently referred to as “the Framework”1) represents the latest effort of the AOTA to articulate language with which to describe the profession’s focus. As such, the Framework is intended to help occupational therapy practitioners analyze their current practice and consider new applications in emerging areas. In addition, the Framework was developed to help the external audience (physicians, payers, community groups, and others) understand the profession’s emphasis on function and participation in social life.
The domain of concern of a profession refers to the areas of human experience in which practitioners of the profession help others (Figure 7-1). According to the Framework, the focus of the OT profession is “the promotion of health and participation of people, organizations, and populations through engagement in occupation.”1 For OT, the breadth of meaningful everyday life activities is captured in the notion of “occupation.” OT practitioners help people perform meaningful occupations that affect their health, well-being, and life satisfaction. These occupations and activities permit desired or needed participation in home, school, workplace, and community life. Notably, personal meaning is emphasized as the central characteristic of occupation. The degree to which personal meaningfulness is decreased may render a therapeutic intervention as merely purposeful (i.e., achieving a goal a client understands but in which he is not particularly invested) or simply inconsequential.
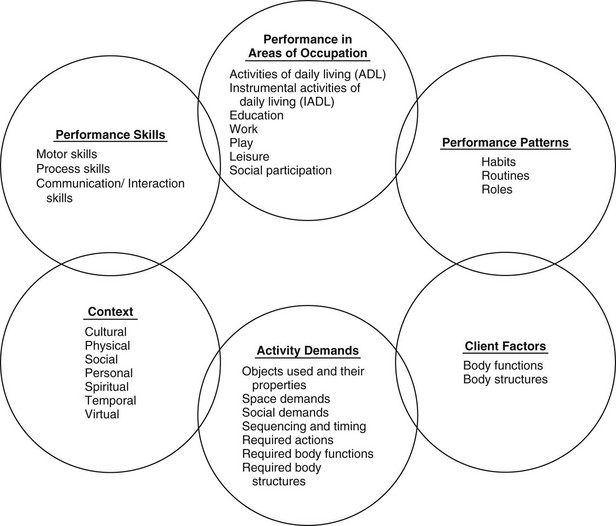
FIGURE 7-1 Domain of occupational therapy.
(Adapted from American Occupational Therapy Association. (2008). Occupational therapy practice framework: Domain and processes, 2nd ed. American Journal of Occupational Therapy, 62, 625-683.)
According to the Framework, meaningfulness of occupation is tightly intertwined with the contexts in which the person lives. The Framework recognizes that “occupational engagement occurs individually or with others.”1 Thus, the many types of occupations in which the client might engage should be addressed in OT intervention. The Framework has organized the many occupations in which an individual, group, or population may engage into broad categories called areas of occupation (Table 7-1). Engagement in these areas depends on the client’s perspective, needs, and interests as well as his or her specific abilities, characteristics, or beliefs, which the Framework identifies as client factors because they reside within the client. For example, to tie one’s shoes (a dressing activity within the ADL area of occupation) one must, among many things, possess sufficient body functions supported by body structures and performance skills to maintain an erect posture while bending and reaching one’s foot, and then one must manipulate the laces and pull on them with sufficient force to tighten them but not enough to break them (all examples of motor and praxis skills). This sequence of actions is carried out by one’s ability to plan and sequence events (examples of cognitive skills). A fascinating feature of human occupation is that many combinations of performance skills (Table 7-2) are integrated and choreographed into automatic or semiautomatic patterns that enable one to function on a daily basis without demanding undue attention. After one has tied his or her shoe laces with sufficient frequency, he or she can often do it without thinking or looking at the laces because it has become a habit. Broader habits can be said to become organized into routines (e.g., one might dress in a certain way and take a particular route to get to work), and frequently routines correspond to the variety of roles in which one functions (e.g., because one is the supervisor of an office, one might routinely meet with employees each morning at a certain time). The Framework notes that “when practitioners consider the client’s patterns of performance, they are better able to understand the frequency and manner in which performance skills and occupations are integrated into the client’s life.”1
| Areas | Types of occupations |
|---|---|
| Activities of daily living | |
| Instrumental activities of daily living | |
| Rest and sleep | |
| Education | |
| Work | |
| Play | |
| Leisure | |
| Social participation |
Adapted from American Occupational Therapy Association. (2008). Occupational therapy practice framework: Domain and processes, 2nd ed. American Journal of Occupational Therapy, 62, 625-683.
| Skill* | Examples |
|---|---|
| Motor and praxis | |
| Sensory-perceptual | |
| Emotional regulation | |
| Cognitive | |
| Communication and social |
*Skills listed as verbs to denote they imply action.
Adapted from American Occupational Therapy Association. (2008). Occupational therapy practice framework: Domain and processes, 2nd ed. American Journal of Occupational Therapy, 62, 625-683.
As stated earlier, the Framework emphasizes the importance of considering the environments and contexts in which a person engages in occupation. Environments are the external physical and social surroundings in which the client’s daily life occupations take place. Contexts refer to the “variety of interrelated conditions that are within and surrounding the client.”1 Contexts, therefore, can be cultural (customs, beliefs, activity patterns, behavior standards, and expectations), personal (age, gender, socioeconomic, and educational level), temporal (stage of life, time of day/year, duration, rhythm of activity, or history), and virtual (simulated interactions absent of physical contact). These contexts offer opportunities for occupational engagement, but at the same time they restrict it; for example, a theater may offer an elder the opportunity to watch a theatrical performance but not to swim or ride a horse, whereas a swimming pool may offer the opportunity to swim but not to watch a theatrical performance.
Two other elements may affect how a person engages in occupation. A person may not be able to meet the demands inherent in an activity (e.g., without a fair amount of conditioning, an elder might not be able to climb up a mountain), or the person may find the demands too low (e.g., a champion chess player may find it quite boring to play Tic Tac Toe). Activity demands include such things as the objects used in the activity and the characteristics of these objects, space and social demands, required actions, and required body functions and structures. For example, the activity of playing golf requires balls and golf irons; takes place on a golf course; is often played with others and therefore requires taking turns; involves a sequence of tasks from placing the ball, hitting it, and then locating it in the distance; and requires the bodily functions of joint mobility and muscle power to swing the iron while not letting the iron fly away and harming someone standing nearby. Furthermore, playing golf involves the person’s cardiovascular system while walking, vestibular functions while turning one’s trunk and following through with the swing, and a variety of other body structures and functions. Interestingly, engagement in occupation is not only affected by these functions and structures, but also it may affect them in turn; for example, an elder’s cardiovascular and neuromuscular functions become conditioned while gradually increasing the time spent walking in a golf course.
The Framework describes the OT process as consisting of three dynamic and interactive phases: evaluation, intervention, and outcome.1 Evaluation consists of the initial step of obtaining the client’s occupational profile and a second step of analysis of the client’s occupational performance. The occupational profile is focused on the person’s history, experiences, daily living patterns, values, needs, beliefs, and so on. The profile consists, essentially, of understanding what the person finds important and meaningful and, therefore, of high priority. Although obtaining contextual information is important throughout the whole intervention process, it is particularly essential at this stage because it will provide the foundation for specific evaluation of occupational performance and certainly for the selection of intervention strategies later in the OT process. For example, if an elder who has had a mild stroke states that he has assembled and collected fishing flies during his whole life, a detailed assessment of fine motor skills may be indicated to ascertain whether he has the necessary motor skills to manipulate the small pieces used in this meaningful occupation. Likewise, an analysis of any other areas of occupational performance that may negatively influence the person’s engagement in meaningful occupation should be performed. Notably, barriers to participation in occupation may not necessarily reside in the client but may be located in the client’s context. For example, although an elder may like to tie fishing flies, his family may not make the materials available to him because they cannot imagine him going fishing any time soon. In this case, they may not understand the meaningfulness of the occupation of fly tying and therefore create a barrier for his participation in the occupation.
The occupational profile and analysis of occupational performance guide the identification of OT intervention goals and strategies. Thus, the intervention phase is centered around what the client finds most meaningful in life and of greatest priority. An intervention plan will include strategies to address performance skills, patterns, contexts, activity demands, and client factors that may be hindering performance. An ongoing collaboration among the OTR, COTA, and client is indispensable to assure that goals, intervention strategies, and progress are continually evaluated and adapted to meet the client’s priorities.
According to the Occupational Therapy Practice Framework, OTRs and COTAs “determine the client’s success in achieving health and participation in life through engagement in occupation.”1 This means that it is the responsibility of OT practitioners to assure that their interventions lead to actual participation in life situations and not simply to improvement in performance skills. In the earlier example of the elder who found tying fishing flies meaningful, it is not sufficient to help him develop the motor skills necessary to maintain this interest. The ultimate goal of OT is for the elder to actually engage in fly tying in the most natural context possible. Thus, instructing the elder to exercise his fingers with elastic bands may contribute to his skills but cannot be the limit of OT intervention. Likewise, using fly fishing to develop dexterity can be considered insufficient intervention if the elder never has the opportunity to use the product of his hands in a meaningful way.
Deepak: The Framework in use
The Framework can help us understand Deepak’s life situation and plan intervention that best supports his participation in all areas of life. According to the Framework, the initial phase of evaluation should involve obtaining an occupational profile. By asking Deepak about his current concerns related to engaging in occupations and daily life activities, as well as about his work history, life experiences, family traditions, and other personal facts, we find out that he has relied heavily on his wife to help with the family’s transition from country to country. Deepak now has a great sense of debt toward her and some guilt for having spent much time working away from home. The physician has recommended that Deepak not put any weight on his left leg for 6 weeks. Deepak’s main concern is that, because of his left knee infection, he will not be able to be of any assistance to his wife in her last weeks of life.
Understanding Deepak’s main concern will help us establish a collaborative relationship with him while we evaluate his skills and environment. If, for example, we had proceeded to evaluate his ability to dress and bathe himself and assessed his endurance and joint range of motion without knowing about his concerns, we might have further reinforced his sense of uselessness and limited potential for social participation. Instead, we can now identify which activities he believes would be the most important for him to be able to do to convey caring for his wife. For Deepak, these include being able to help her move in bed, get in and out of a bed and a chair, run errands for her and, if necessary, help her eat. Thus, we can proceed by evaluating his endurance, balance, and strength, all needed to help his wife move in bed or get in and out of a chair. We can help adapt the environment and teach him body mechanics to have the maximum leverage while moving his wife. We can further evaluate his ability to complete activities of daily living (ADL) because he will need to be dressed to run errands outside of the home.
Naturally, there are many other areas for assessment and intervention with Deepak. However, the previous illustrates how the central concern for him is related to an area of occupation rather than to a body structure. OT intervention can still be organized to address many client factors, but the intervention is not likely to seem meaningful unless Deepak is able to understand that it contributes to his main concern.
Facilitating Growth and Development
The Facilitating Growth and Development Model views the OT practitioner’s role as one “concerned with facilitating or promoting optimal growth and development in all ages of man.”2 An individual’s growth and development may be threatened by disease, injury, disability, or trauma. The OT practitioner may be required to assist the individual in coping with illness, trauma, or disability, or to help with rehabilitation. The OT practitioner also may seek to prevent maladaptation and promote health maintenance.
This model requires the OT practitioner to understand the developmental tasks and adaptive skills that are usually mastered at different ages. The model describes the belief that the human being “develops simultaneously in the areas of neurophysiological, physical, psychosocial and psychodynamic growth, and in the development of social language, daily living, sociocultural, and intellectual skills during the life span.”2 The way the individual integrates and organizes these areas of development to perform in work, education, play, self-care, and leisure activities during each stage of life is of primary concern to OT. In addition to understanding the individual’s development, the OT practitioner must understand the ways illness, disease, trauma, and disability may threaten that development. Finally, OT addresses the environmental variables necessary to support the development and maintenance of the important adaptive skills cited by Llorens.2
The Facilitating Growth and Development Model synthesizes the work of numerous authors who have contributed to the understanding of human maturation.2 The model includes descriptions of the adaptive skills mentioned during each life stage, including infancy to age 2 years, ages 2 to 3 years, ages 3 to 6 years, ages 6 to 11 years, adolescence, young adulthood, adulthood, and maturity. Each stage is built on the foundation of the stages that the person has completed (Table 7-3). This text, however, focuses on the last stage.
TABLE 7-3 Characteristics of Maturity
| Neurophysiological and physical development | Possible alterations in sensory functions (visual, auditory, tactile, kinesthetic, gustatory, and olfactory), motor behavior (coordination of extremities), information processing (higher level integration, including conceptualization and memory), and physical endurance |
| Psychosocial—ego integrity and maturity | Acceptance of life experiences and the life cycle |
| Psychodynamic | Coping with continued growth after middle age, decision making regarding growth or death (giving up on life), dealing with insincerity of friends and acquaintances, inner life trends toward survival, possible decrease in efforts to maintain false pride, often a reduction in defenses, more suspiciousness, and necessity of dealing with psychological deterioration |
| Sociocultural | Group affiliation: family, social, interest, civic |
| Social language development | Predominantly verbal use, some use of nonverbal behavior to communicate |
| Activities of daily living and developmental tasks | Adjustment to decreasing physical strength and health, adjustment to retirement and reduced income, adjustment to death of spouse, adjustment to one’s own impending death, establishment of affiliations with own age group, and meeting of social obligations |
| Ego-adaptive skills | Ability to function independently; ability to control drives and select appropriate objects; ability to organize stimuli, plan, and execute purposeful motion; ability to obtain, organize, and use knowledge; ability to participate in primary group; ability to participate in a variety of relationships; ability to experience self as a holistic, acceptable object; ability to participate in mutually satisfying relationships oriented to sexual needs |
| Intellectual development | Possible neurophysiological and physical development alteration and return of egocentrism |
Adapted from Llorens, L. A. (1976). Application of a Developmental Theory for Health and Rehabilitation. Rockville, MD: American Occupational Therapy Association.
During the OT process, the OTR and COTA assess the client’s development and determine potential disruptions in each adaptive skill area. The OTR and COTA analyze this information to determine the effects on age-appropriate occupational performance in the areas of work, education, self-care, and play and leisure. The OTR and COTA may then devise intervention strategies that facilitate development of a specific skill needed for successful occupational performance (Table 7-4). Matching the client’s needs with the right therapeutic activities requires careful analysis of inherent requirements of each activity.
Data from Llorens, L. A. (1976). Application of a developmental theory for health and rehabilitation. Rockville, MD: American Occupational Therapy Association.
Depending on the client’s needs, selected activities may include sensory, developmental, symbolic, and daily life tasks. These activities are combined with the social interaction that is most beneficial for the client. Sensory activities are those that primarily influence the senses through human action, such as touching, rocking, running, and listening to sounds. Developmental activities involve the use of objects such as crafts and puzzles in play, learning, and skill development situations. The client develops specific performance skills by engaging in these types of activities. Symbolic activities are designed to help the client satisfy needs and elicit and cope with emotional responses. Examples include gouging wood and kneading clay, which may release muscle tension and help process anger. Another example of a symbolic activity is leading a group in a task. This activity may satisfy the client’s need to be heard and feel competent. The emotional response from leading a group may be improved self-esteem. Daily life tasks, also called activities of daily living, include tasks such as brushing teeth, getting dressed, cooking, and cleaning. Finally, social interaction includes participation in dyads with the therapist or another person and groups. These activities encourage the development of sociocultural competence and language and intellectual skills.
According to the Facilitating Growth and Development Model, OT intervention should continue until the client reaches sufficient competence in performing the skills and activities described as developmentally appropriate. The OTR and COTA continually monitor and reevaluate the client’s progress in improving, maintaining, or restoring areas of occupational performance and therefore clearly know when the client no longer requires specialized OT services.
Martha: The model in use
Llorens’s2 developmental model can help give us a more complete picture of Martha’s life and occupational needs. She has lived for more than half her life with the disability that resulted from her head injury. However, she has been relatively healthy and independent. She now is facing the neurophysiological and physical alterations that are normal with maturity but that seem to compound the occupational performance challenges brought by her disability. Her bouts with pneumonia have left her debilitated, and she has been moved to a skilled nursing facility.
According to Llorens’s developmental model,2 a life priority for Martha is to accept life experiences and the life cycle, not to distinguish which of her problems are caused by her age and which by her head injury. Of great importance will be for her to continue developing coping skills to deal with both her limitations in function and the changes in her environment now that she no longer lives with her sister. She has the opportunity to participate in a variety of relationships with fellow patients and staff. Finally, of great importance will be to stimulate her continued intellectual development. Although her ability to bathe and dress herself independently is important, that need should not overshadow the other needs she has as a developing human being.
Cognitive Disabilities
As its name indicates, the Cognitive Disabilities Model is concerned with OT services that are designed for clients with cognitive impairments. These impairments may be the result of psychiatric illness, medical diseases, brain traumas, or developmental disorders. Psychiatric illnesses such as depression and schizophrenia have associated cognitive impairments. Alzheimer’s dementia and cerebrovascular accidents are examples of medical conditions that result in cognitive impairments, and closed head injuries are an example of trauma to the brain that can also result in a brain disorder. Brain dysfunction also may result from use of prescribed medications or other drugs. The cognitive impairment that results from these conditions may be short-term or long lasting.
Assertions of the Cognitive Disabilities Model are based on information from neuroscience, biology, psychology, and traditional OT theory.5 According to this model, occupation is synonymous with voluntary motor action. Observing voluntary motor actions such as dressing, completing a craft, or preparing a simple meal is of primary interest to the OT practitioner because of the inferences that can be made about brain function. Voluntary motor actions are “behavioral responses to a sensory cue that are guided by the mind.”3 That is, voluntary motor actions occur as a consequence of the relation among the external physical environment of matter, which provides sensory cues; the internal mind, which provides purpose; and the body, which produces behavior in the form of motor activity. Observing a person’s voluntary motor action gives the OT practitioner insight into the relation among these three domains. Each domain is further described by subclassifications.
Based on extensive research, the Cognitive Disabilities Model proposes a categorization of six cognitive levels that describe the way an individual relates matter, behavior, and mind as demonstrated in performance of voluntary motor actions (Table 7-5).3,5 Level 1 represents the greatest degree of impairment, and level 6 represents normal performance. As this model has evolved, each cognitive level has been expanded to include several subcategories or modes. Only the global characteristics of each level are described in this text. This practice model may be used to describe client performance and to guide selection of activities or tasks that permit the client to function consistently at the greatest possible level. (Other chapters in this text describe conditions associated with elders for whom the application of the cognitive disabilities model may be appropriate, including the aging process in Chapter 3; side effects of medication in Chapter 13; malnutrition and dehydration in Chapter 18; strokes in Chapter 19; Alzheimer’s dementia in Chapter 20; depression, schizophrenia, and drug addiction in Chapter 21; and brain tumors in Chapter 25.)
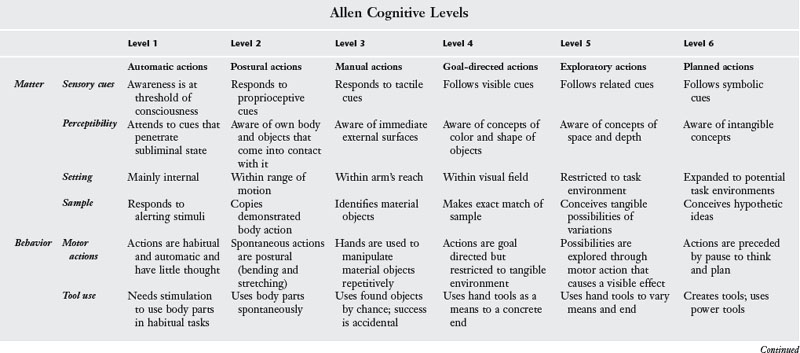
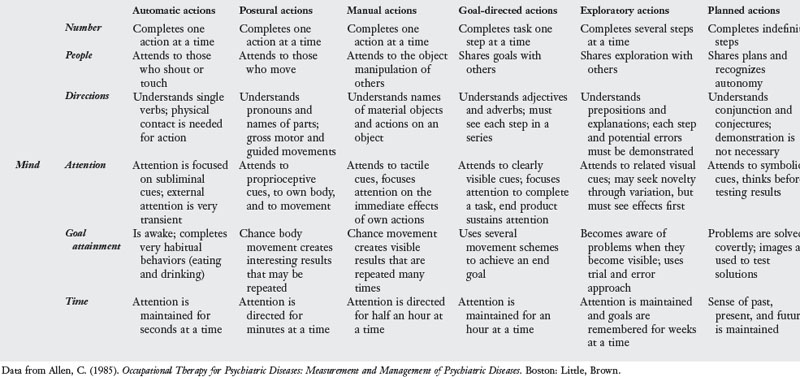
Observing clients perform activities and tasks that are part of their daily routines is ideal during assessment because these activities are usually important to the client and caregivers. These activities also allow the OTR and COTA team to separate issues related to learning a new activity, which might not accurately convey the client’s current cognitive performance. Consequently, task assessment should be preceded by information obtained from the client and caregivers regarding the client’s most familiar tasks. After observing the client, the OTR and COTA team can compare the performance with the characteristic behaviors for each cognitive level. The OTR and COTA must remember that a client may function at a variety of levels depending on familiarity with the task and the time of day. Knowledge of the client’s optimal functional level helps the OTR and COTA team design intervention strategies that maximize the client’s abilities.
Several standardized tests may be used to determine cognitive level, including the Expanded Routine Task Inventory (RTI)3,15 and the Allen Cognitive Levels (ACL) Test.5,16 The RTI evaluates the individual’s ability at each of the six levels to complete a variety of routine tasks along a physical scale, such as grooming, dressing, bathing, walking, exercising, feeding, toileting, taking medication, and using adaptive equipment; a community scale, such as housekeeping, obtaining and preparing food, spending money, doing laundry, traveling, shopping, telephoning, and taking care of a child; a communication scale, such as listening, talking, reading, and writing; and an employment scale, such as maintaining pace and schedule, following instructions, performing simple and complex tasks, getting along with coworkers, following safety precautions and responding to emergencies, and supervising and planning work. The ACL test helps determine cognitive level by assessing the response to verbal instructions and problem-solving techniques when a client is presented with a leather lacing project.3 The large ACL was developed to compensate for visual loss in the elder population, and the Cognitive Performance Test was developed to provide a standardized, ADL-based instrument for the assessment of functional level in Alzheimer’s dementia.
Once the client’s cognitive level has been determined, the OT intervention goals must be considered.4 Allen states that participation in an occupation does not necessarily mean the client will improve.3 This assumption fails to recognize other possible reasons for recovery, including that the client may recover spontaneously without any intervention. Consequently, the purpose of OT intervention should be to document alterations and improvements in functional abilities, sustain current performance, and reduce pain and distress associated with the symptoms. Goals are not intended to improve cognitive level but to ensure consistency of performance at the safest and least restrictive level. The case of Ray illustrates this point. Ray is a 70-year-old man with Alzheimer’s dementia. An OTR and COTA team determined that he is currently functioning at cognitive level 4. This means that Ray can spontaneously complete tasks when cues are clearly visible. A goal for Ray to live independently would not be appropriate because he does not deal with cues that are not within his field of vision and consequently can easily place himself in danger. Appropriate OT goals for Ray according to this model may include consistent initiation of daily self-care routines, initiation of laundry washing, consistent monitoring of Ray in unfamiliar environments, and provision by his caregivers of appropriate cues to maximize his performance.
Once the client’s goals have been determined, the COTA may select a variety of activities that match the characteristics of the matter, mind, and behavior domains appropriate to the client’s cognitive level. The COTA must be adept at analyzing a task to know precisely the way it requires matter, mind, and behavior to interact for the client to successfully perform a voluntary motor action. Tasks are selected by the degree of demand on the client to perform consistently at a particular cognitive level. The OTR and COTA team evaluated Ray and determined he was at cognitive level 4. Consequently, he can understand basic goals of activities, can purposefully use objects placed within his field of vision, and is able to match examples of tasks demonstrated to him. To reinforce his ability to maintain a sense of accomplishment, the COTA may select a simple woodworking project for Ray. The COTA can place all materials for this project on a table in front of Ray and instruct him to sand the wooden pieces. Telling him to pick up the sandpaper, hold it so the grain comes in contact with the wood, and rub it against the wood is unnecessary. These steps would be obvious to Ray because the materials are in his field of vision. Once Ray completes the sanding, the COTA may instruct him in a similar way to glue the pieces together as shown in the sample, stain the stool, and varnish it. Ray lacks the foresight to plan for potential problems; consequently, the COTA should demonstrate the amount of glue, stain, and varnish needed in addition to the application procedures.
Once the client is performing at a level that most consistently demonstrates remaining task abilities and the environment has been structured to compensate for the client’s limitations, skilled OT services should be discontinued. Discharge considerations are made from the beginning of OT intervention. The cognitive disabilities model specifically focuses on preparing the client for discharge to the least restrictive environment.5 Therefore, the COTA must observe voluntary motor actions to understand the way each client interacts with the environment. The COTA and OTR should recommend that the client be discharged to the setting that best supports the client’s task abilities.
Ursula: The model in use
Ursula’s Alzheimer’s disease has progressed to the point where there is a clear cognitive deficit. Therefore, the Cognitive Disabilities Model is ideal to help us develop a suitable intervention plan. The first step is to determine the cognitive level at which Ursula is functioning. During the RTI, Ursula shows that she performs at cognitive level 4. This is consistent with her husband’s report, who states that at home Ursula follows his visible cues and seems to pay attention to only objects within her immediate visual field. He notes that she does not seem able to find items she needs even though they are in plain view in the room. However, once she finds the item, she is able to use it correctly.
The OT program for Ursula should consist of activities at level 4 that encourage her to complete steps of repetitive tasks after they have been demonstrated for her. For her safety, the environment should be structured so that all of the items she needs are in plain view in front of her. She should be given one instruction at a time, and instructions should focus on the motor actions rather than on the abstract goal of projects. Examples of suitable projects include simple printing or painting tasks, woodworking kits with few and large pieces, and simple food preparation tasks that do not require use of a stove or other potentially dangerous appliances. For her safety, Ursula should never be left alone or unattended.
Model of Human Occupation
The Model of Human Occupation was designed for use with any individual experiencing difficulties in performing an occupation. This model evolved from earlier research by Reilly17 on occupational behavior. Using concepts from General Systems Theory, Open Systems Theory, and Dynamical Systems Theory, this model gives an explanation for the way occupation is motivated, organized, and performed, thereby emphasizing the human system’s spontaneous, purposeful, tension-seeking properties and acknowledging its creative properties.6 In addition, this model provides a view of the degree of intimacy between the environment and the performance of occupation.
Human beings maintain constant interaction with the environment and receive many types of input such as olfactory and sensory stimulation and behavior expectations. The individual uses that input in many ways (e.g., food becomes energy; sensory stimulation may translate to touch, pain, or temperature; and words are interpreted). This process is known as throughput. Part of the result of the process of input and throughput is that a behavior, or output, is produced. Finally, as the person performs the behavior, the experience of doing it and any results from it form the process of feedback, which becomes a new source of input into the system. The Model of Human Occupation explains occupation as the cumulative and highly dynamic expression of this process. For example, in meal preparation, the cook sees the food items (input), considers what recipe to use (throughput), prepares the food items (output), feels arm movement, and sees the result of the preparation (feedback). While seeing that feedback, the cook notices that the food is beginning to turn brown (input), decides it is burning (throughput), removes the pan from the stove (output), and experiences moving the pan until it is off of the stove (feedback). To further explain this dynamic interaction between the individual and the environment from which the occupation arises, the Model of Human Occupation describes external and internal environments of the human being as composed of several subsystems.
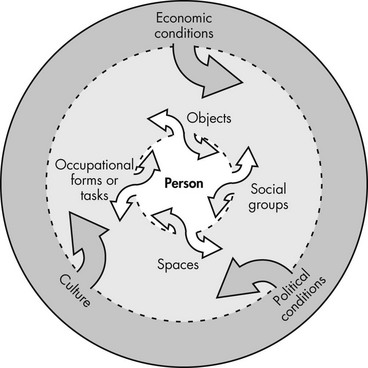
According to this model, the external environment offers opportunities for certain behaviors while requiring others. For example, the institution of school offers the teacher a room in which to walk around, speak, write on the chalkboard, and sit in a chair. At the same time, the school requires from the teacher the behavior of instructing the students. The teacher will be fired if those requirements are not met. Providing opportunity and requiring behavior is a complementary relationship. The influence of this relationship comes from several sources in the environment, including the physical realm, such as objects and built or natural structures; the social realm, which includes the tasks deemed appropriate and desirable and the social groups sanctioning the behavior; the settings or spaces in which occupation occurs, such as home, neighborhood, school, workplace, and gathering, recreation, and resource sites; and the overall culture, such as values, norms, and customs, which affect the individual’s life. In addition, political forces and socioeconomic conditions of the society in which a person lives have an impact on the person’s occupation by making resources available or restricting access to them. For example, a person in a wheelchair may not be able to access an entertainment venue if the society does not mandate the presence of cut curbs, ramps, and elevators in public spaces. However, the presence of adapted environments will not make much difference if the person lacks economic means to obtain a wheelchair in the first place (Figure 7-2).
The earlier example of meal preparation can be used to further elaborate on these external environment concepts. To perform this occupation, the cook requires several objects, including food ingredients and seasonings, a knife, some pans, and the stove. The processes of dicing, chopping, stirring, and frying the food are all tasks recognized as cooking. Because of health concerns, the cook may choose to prepare a meal consisting only of vegetables for his or her family (social group). The setting of the meal is the cook’s home, where he or she can exercise creativity in preparing and seasoning the food and presenting the meal. In addition, the choice of vegetables only may be influenced by a cultural value that an athletic body is preferable to an obese one. If the cook were performing the occupation of cooking as the main task of his or her job at a restaurant, however, the objects, tasks, social group, setting, and possibly cultural expectations may present completely different opportunities and behavior expectations. There he or she might use industrial-size knives and tools, prepare large amounts of fried fish, be part of a team of cooks, and work in a restaurant that specializes in ethnic food.
The Model of Human Occupation describes the individual’s internal environment as composed of interrelated components (Figure 7-3). Volition is responsible for guiding the individual through occupation choices throughout the day. According to this model, occupation choice is influenced by the individual’s disposition about expected outcome and by self-knowledge, or awareness of the self as an active participant in this world. Both of these influences determine the way the individual anticipates, chooses, and experiences occupation. These concepts are illustrated by George and Pam, an elder couple residing in a senior housing community. Every Saturday night they dress in their best clothes and walk to the common hall to play bridge with other members of their community. They choose to do this because they anticipate the pleasure of friends’ company and because they believe they are capable bridge players. Helen, who lives in the same community as George and Pam, chooses not to play bridge. Although she is a champion player, she anticipates feeling out of place because she is a widow and does not have a regular partner.
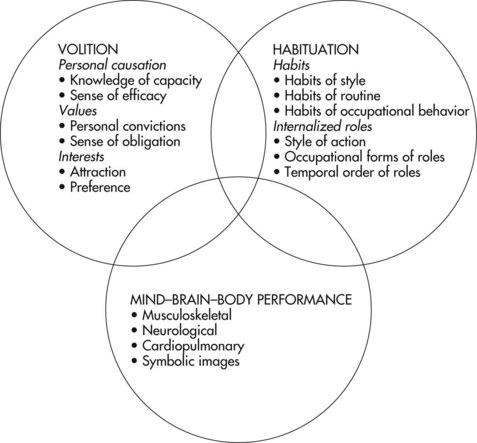
Volition is composed of personal causation, values, and interests. Personal causation refers to the awareness individuals have of their abilities (i.e., knowledge of capacity) and to individuals’ perceptions that they have control over their behavior (i.e., sense of efficacy). An individual is more likely to engage in an occupation he or she feels capable of doing. Values refer to the convictions people have that help them assign significance and standards of performance to the occupations they perform. Each individual has values that form the individual’s views of life. These values elicit a sense of obligation to do what the individual believes is right. Finally, interests refer to the desire to find pleasure, enjoyment, and satisfaction in certain occupations. Interests may also be attractions that people feel toward certain occupations and preferences regarding ways that occupations are performed. For example, George, Pam, and Helen each has a sense of themselves as good or effective bridge players (personal causation). This sense was developed through experience over time, so that after playing as partners for more than 30 years, George and Pam have a specific playing style (preference) and are attracted to the opportunity to play bridge on Saturday nights rather than staying home and watching television. Although Helen may have developed the same interest and personal causation, she believes that playing bridge is most meaningful with your spouse as your partner. Because she has no spouse, this value is sufficient to deter her from participating in the Saturday night games at the senior housing community.
In contrast to volition, which has to do with conscious choice and motivation of occupation, habituation has to do with the routine ADL. These routines require little deliberation because they are built on repetition. Habituation is composed of habits and internalized roles. Habits have to do with the typical way an individual performs a particular occupation and organizes it within a typical day or week and the unique style the individual brings to performance. For example, going to the common hall on Saturday night to play bridge is part of George and Pam’s weekly routine. While playing bridge, both drink coffee. George typically puts one teaspoon of sugar in his cup before pouring in the coffee, and Pam pours her coffee first and then mixes in the sugar. During the game, George is talkative and Pam is quiet, but both break into song when they win the game.
Internalized roles refer to typical ways in which an individual relates to others. Roles are the identities and behaviors that people assume in various social situations. These roles are based on the individual’s perceived expectations of others. Thus, roles involve obligations and rights of the individual in the various social contexts. According to the Model of Human Occupation, the specific occupational behaviors that encompass a role, the style in which actions in a role occur, and the way an individual’s roles are prioritized are of particular interest to the OT practitioner. George, Pam, and Helen each have an image of the role of bridge player. For George and Pam, this role includes the occupations of dressing nicely, walking to the common hall, playing by the rules, and sitting around a table conversing with others. Helen may view the role in a similar way, but she has the additional sense that the role of bridge player requires having one’s spouse as partner. Because she is a widow, Helen has abandoned the role of bridge player. Conversely, George and Pam routinely enter this role on Saturday nights.
The final element of the human being’s internal environment is the mind–brain–body performance capacity component. As its name implies, this component represents the complex interplay among the musculoskeletal, neurological, perceptual, and cognitive abilities required to actually perform an occupation or enact a behavior. Interaction with the environment occurs through this subsystem. The individual perceives challenges and opportunities in the environment through the perceptual system and processes this information in the brain. According to the meaning ascribed to the perception, the brain plans an action, which is carried to the muscles, joints, and bones of the limbs that perform the action. Whereas an occupation’s meaning is ascribed by volition and the social context is determined by habituation, the related actions are enabled though the person’s performance capacity. George and Pam like to play bridge (volition subsystem) and do so every Saturday night (habituation subsystem). During the bridge game, George and Pam keep in mind the rules and play accordingly. They sit with others around a table and maintain a grasp on the cards (performance subsystem). The complex interplay between mind, brain, and body inherent in the performance of any occupation occurs through specific skills, including motor skills, process skills, and communication–interaction skills (Table 7-6). Performance capacity, however, entails more than simply possessing intact body structures and functions upon which the actions of occupation are built. The person’s subjective experience or sense of being oneself in one’s own body, significantly shapes what occupations are engaged in and the quality of such engagement. This involves knowing things, knowing how to do things, and then, finally, actually doing things. The Model of Human Occupation refers to this as mid-body unity, in which the bodily experience of doing is intricately intertwined with the embodied mind.
| Motor domains and skills | Posture | |
| Mobility | ||
| Coordination | ||
| Strength and effort | ||
| Energy | ||
| Communication and interaction domains and skills | Physicality | |
| Language | ||
| Relations | ||
| Information exchange | ||
| Process domains and skills | Energy | |
| Knowledge | ||
| Temporal organization | ||
| Organization | ||
| Adaptation | ||
| Social interaction domains and skills | Acknowledging | |
| Sending | ||
| Timing | ||
| Coordinating |
A strength of the Model of Human Occupation is the holistic view that it provides of any dysfunction. Traditional health practice often focuses on one or two particular traits of a dysfunction rather than on all of the contributing factors. All of the effects of dysfunction on an individual’s life are rarely fully explored.6 This lack of understanding the whole situation may be particularly detrimental to the elder. For example, Calvin is a 78-year-old man recently admitted to the hospital after falling and fracturing his left femur. On admission, an x-ray examination was done, Calvin was taken to surgery, and an open reduction of the fracture was performed. A cast was put on Calvin’s leg, and he was referred to physical and OT for a brief rehabilitation course. The physical therapist focused rehabilitation on getting in and out of bed and walking with the reduced weight-bearing guidelines recommended by the physician. The OTR evaluated Calvin and identified difficulties in dressing and toileting because of the cast and weight-bearing precautions. The OTR asked the COTA to train Calvin to dress and toilet with adaptive equipment, to which Calvin easily complied. Calvin was discharged to return home in 2 days, at which time the OTR and COTA team documented that Calvin was independent in dressing and toileting with necessary equipment and was aware of home modifications needed to avoid further falls. Unfortunately, nobody on the health team carefully investigated the reason that Calvin fell. Although he can care for himself, he finds living alone unbearably lonely. In addition, three of Calvin’s lifelong friends died in the past year. Thus, Calvin has a deep sense of hopelessness. He occasionally tries to alleviate his feelings of loneliness and despair by drinking alcohol. He fell after one of these drinking episodes. When the admitting health worker at the hospital asked him if he consumed alcohol, Calvin responded truthfully that he did so only occasionally. During his hospital stay, Calvin appeared bright and friendly because he received much desired social contact. A more systematic evaluation of Calvin’s life would have revealed a deeper problem related to his volition and habituation subsystems. Instead, the OTR and COTA team focused on the obvious performance subsystem problem, which actually was only a symptom of a more complex issue. The team’s care also should have addressed Calvin’s feelings of hopelessness (volition) and the reduced number of roles he has to help himself organize his days (habitation). Furthermore, the COTA and OTR should have helped Calvin explore community resources.
According to the Model of Human Occupation, any traditional OT tool is valid for assessment and intervention. Not one single assessment or intervention tool can completely address the complexity of the individual. Some suggested evaluation tools include the Assessment of Communication and Interaction Skills,18 the Assessment of Motor and Process Skills,19 the Assessment of Occupational Functioning,20 the Occupational Case Analysis Interview and Rating Scale,21 and the Occupational Performance History Interview.22 Interest and role checklists, activity configurations, manual muscle tests, range-of-motion tests, and cognitive tests are among the many tools that may be used to evaluate each subsystem. Ultimately, data should be gathered regarding all subsystems of the individual’s internal and external environments. Once problems are identified, intervention is prioritized according to all subsystems that are interdependent. In Calvin’s case, if the volition and habituation issues had been identified, OT intervention could have focused on helping Calvin find other meaningful activities and resources for continued social contact, in addition to addressing his dressing and toileting needs.
Carlos: The model in use
Because Carlos is unable to speak, an observational assessment tool should be used to describe a baseline of occupational functioning. An Assessment of Motor and Process Skills19 can help us see that although Carlos is unable to speak, he is able to perform fairly complicated motor tasks. As part of the Assessment of Motor and Process Skills, Carlos was asked to make a fruit salad. Carlos positioned his body appropriately for the task, stabilized all objects, including the fruit and knife, maintained a secure grasp on the objects, chose the right tools, sequenced the task correctly, and cleaned the workspace without being asked to do so. This demonstrated that Carlos continued to consider his role as cook as very important and that he was motivated to remain active. When tasting the fruit salad, there was no coughing, and it became apparent that part of his problem may have been that his family was feeding him while he was in bed. By making the fruit salad, Carlos demonstrated to his family that he was not an invalid and that he was motivated to be upright and active. This allowed the family to step back and encourage him to increase his level of activity rather than overprotect him as they had been doing. In 2 days Carlos’s fever was gone and he was developing a system to communicate with his family members through gestures and pictures.
Conclusion
Building on the use occupation as a common thread for any OT intervention, each of the practice frameworks or models provides a unique way to organize and think about information regarding the individual’s function. In addition, each model guides the selection of intervention strategies appropriate for the specific needs of the individual. Finally, the use of practice models assists the COTA in looking beyond the obvious functional deficits, thereby ensuring a more holistic approach to care of complexities of an elder’s life.
1. Explain the meaning of occupation and why this concept should be at the core of any OT intervention.
2. Describe at least two ways in which a practice model can help the COTA work with elders.
3. Explain why it is important to consider context in an elder’s occupational performance.
4. Considering Llorens’s developmental model, explain the social interaction needs that an elder is likely to have when placed in a long-term care facility.
5. You have planned a task group for psychiatric clients during which you plan to carve pumpkins for Halloween. Using the Cognitive Disabilities Model, describe how you would modify the activity if the members of the group are functioning at a cognitive level 4.
6. Using the language of the Model of Human Occupation, explain how you would prioritize intervention for an elderly Native American elder who was admitted to the hospital after a car accident in which his wife and adult son died. He has severe fractures in all extremities, and there is the possibility of a mild head trauma. When you approach this gentleman, he refuses to speak and remains staring out the window.
1 American Occupational Therapy Association. Occupational therapy practice framework: Domain and processes, 2nd ed. American Journal of Occupational Therapy. 2008;62:625-683.
2 Llorens L. Application of a Developmental Theory for Health and Rehabilitation. Rockville, MD: American Occupational Therapy Association; 1976.
3 Allen C. Occupational Therapy for Psychiatric Diseases: Measurement and Management of Cognitive Disabilities. Boston: Little Brown; 1985.
4 Allen C., Earhart C., Blue T. Occupational Therapy Treatment Goals for the Physically and Cognitively Disabled. Rockville, MD: American Occupational Therapy Association; 1992.
5 Allen C., Earhart C., Blue T. Understanding cognitive performance modes. Ormond Beach, FL: Allen Conferences; 1995.
6 Kielhofner G. A Model of Human Occupation: Theory and Application, 4th ed. Baltimore: Lippincott Williams & Wilkins; 2007.
7 American Occupational Therapy Association. The philosophical base of occupational therapy. American Journal of Occupational Therapy. 1995;49:1026.
8 American Occupational Therapy Association. Position paper: Purposeful activity. American Journal of Occupational Therapy. 1993;47:1081.
9 American Occupational Therapy Association. Uniform terminology for occupational therapy—3rd ed. American Journal of Occupational Therapy. 1994;48:1047.
10 Kielhofner G. A Model of Human Occupation: Theory and Application, 2nd ed. Baltimore: Lippincott Williams & Wilkins; 1995.
11 Trombly C. Occupation: Purposefulness and meaningfulness as therapeutic mechanisms. Eleanor Clarke Slagle Lecture. American Journal of Occupational Therapy. 1995;49(10):960-972.
12 Ma H., Trombly C. Effects of task complexity on reaction time and movement kinematics in elderly people. American Journal of Occupational Therapy. 2004;58(2):150-158.
13 Ayers A.J. Sensory Integration and Praxis Test. Los Angeles: Western Psychological Services; 1991.
14 Mountain G. Occupational Therapy with Older People. Hoboken, NJ: Wiley; 2005.
15 Katz N. Routine Task Inventory: Expanded (RTI-E) manual, prepared, and elaborated on the basis of C. K. Allen. Unpublished manuscript available at www.allen_cognitive_network.org, 1989. unpublished
16 Pollard D., Olin D.W. Allen’s cognitive levels: Meeting the challenges of client-focused services. Monona, WI: SELECTone Rehab; 2005.
17 Reilly M. Occupational therapy can be one of the great ideas of 20th century medicine. American Journal of Occupational Therapy. 1962;16:1-9.
18 Salamy M., Simon S., Kielhofner G. The Assessment of Communication and Interaction Skills (research version). Chicago: University of Illinois; 1993.
19 Fisher G. Assessment of Motor and Process Skills, 3rd ed. Ft. Collins, CO: Three Star Press; 1999.
20 Watts J., Newman S. The assessment of occupational functioning. In Hempill-Pearson B., editor: Assessments in Occupational Therapy in Mental Health, 2nd ed, Thorofare, NJ: Slack, 2007.
21 Kalplan K., Kielhofner G. The Occupational Case Analysis and Interview and Rating Scale. Thorofare, NJ: Slack; 1989.
22 Kielhofner G., Mallinson T., Crawford C., Nowak M. A user’s guide to the Occupational Performance History Interview II (OPHI-II) (version 2.0). Chicago: Model of Human Occupation Clearinghouse, Department of Occupational Therapy, College of Applied Health Sciences, University of Illinois at Chicago; 1997.